Covid 3/25: Own Goals
post by Zvi · 2021-03-25T13:50:00.989Z · LW · GW · 17 commentsContents
The Numbers Predictions Deaths Positive Tests Vaccinations AstraZeneca Vaccinations Resume In Europe I Will Not Invoke The Copenhagen Interpretation of Ethics AstraZeneca Vaccine Once Again Found Safe and Effective? Have You Tried Increasing Supply? The Safe Distance For Children Has Always Been Three Feet Talk To Your Kids About Covid-19 Public Broadly Supports Challenge Trials In Other News None 17 comments
AstraZeneca has made quite the mess of things. First they screwed up their initial studies in ways that kind of boggle the mind. Then, with the studies designed to repair trust, fix the problem and allow approval, they report incomplete results in order to make themselves look better, even though inevitably they were caught doing this within a day – it’s pretty inevitable that you’ll be caught when you do something in public that someone already warned you not to do, especially when that someone is also the regulatory authority. Oops.
In addition to AZ’s own goals, health officials continue to score additional own goals around the whole issue of blood clots (that don’t exist, and wouldn’t matter even if they did). Most but not all places have resumed vaccinations, but trust in the vaccine, and plausibly in all vaccines, is permanently damaged.
Those developments are infuriating, and also enlightening as to how the system of the world functions these days, but the main event remains the race between new strains and vaccinations.
In America the race is plausibly close. Cases are rising, and likely will continue to rise for several more weeks, especially if vaccination rates continue to stagnate. But that acceleration should start soon, and at an additional 3% protection per week that grows and compounds, the vaccinations won’t take that long to turn the tide even if they don’t accelerate much.
In Europe the race is not so close. Vaccinations are running far slower, with no short term hope for things to get much better. The recent own goals only made a bad situation worse, and in many European countries things are looking quite bad. Lockdowns are once again the order of the day in many places, most notably Germany, and yet the situation is getting rapidly worse, in some places reaching crisis proportions.
I spend a lot of focus on everything that’s wrong with our vaccine efforts, but as with many such things it’s equally vital to remember that things could be, and in almost all other places are, so much worse. We failed versus the standards of a fully functional civilization, but compared to the rest of Earth 2020, we passed with flying colors. We need to remember both results.
Let’s run the numbers.
The Numbers
Predictions
Last week’s prediction (WaPo numbers): Positivity rate of 4.3% (up 0.2%), deaths decline by 8%.
Result:
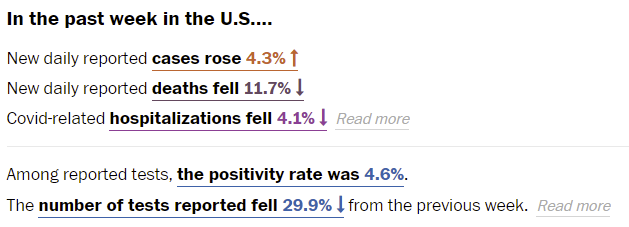
Pretty close. It’s worth noting that these changes don’t match the Wikipedia data, which only has a 2% or so drop in deaths. Based on regional changes I’d be inclined to believe the WaPo decline is more accurate.
The positivity rate was higher than I expected, and I presume that’s mostly because the number of tests fell by almost 30%. That’s a very scary drop to see while we’re seeing a rise in cases in the same data set. It’s much bigger than vaccinations could explain. What’s going on there? I certainly hope we don’t see another big drop until the need goes away.
Prediction for next week: Positivity rate of 4.9% (up 0.3%) and deaths fall by 7%. Deaths should continue to decline due to lag, but that effect should shrink. Vaccinations continue to help, but in the short term I’d expect new strains to have the bigger impact, so the short term situation should get somewhat worse.
Deaths
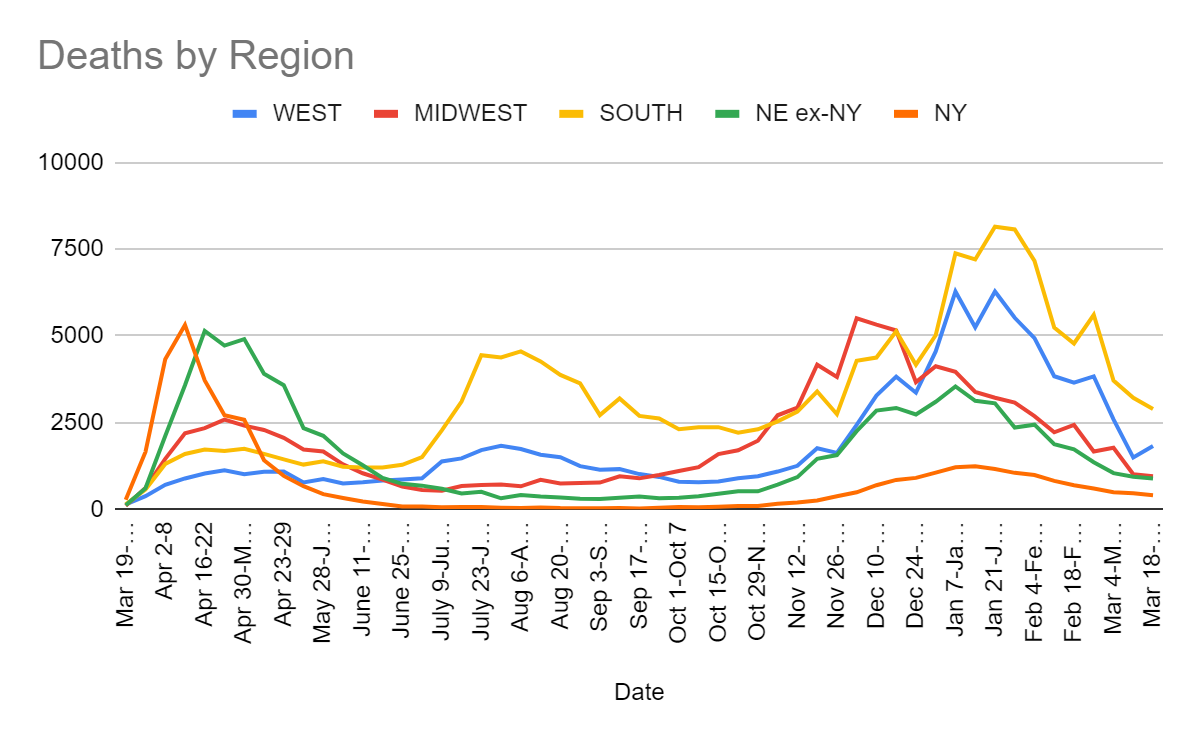
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Feb 4-Feb 10 | 4937 | 2687 | 7165 | 3429 | 18218 |
| Feb 11-Feb 17 | 3837 | 2221 | 5239 | 2700 | 13997 |
| Feb 18-Feb 24 | 3652 | 2433 | 4782 | 2427 | 13294 |
| Feb 25-Mar 3 | 3834 | 1669 | 5610 | 1958 | 13071 |
| Mar 4-Mar 10 | 2595 | 1775 | 3714 | 1539 | 9623 |
| Mar 11-Mar 17 | 1492 | 1010 | 3217 | 1402 | 7121 |
| Mar 18-Mar 24 | 1823 | 957 | 2895 | 1294 | 6969 |
The change in the West seems like it has to be timeshifted data messing things up, with the declines in the other regions closely matching the WaPo declines. Deaths are on a solid trajectory downwards.
Positive Tests
Remember that the number of tests went way down this week, so this is a much bigger deal than it appears to be.
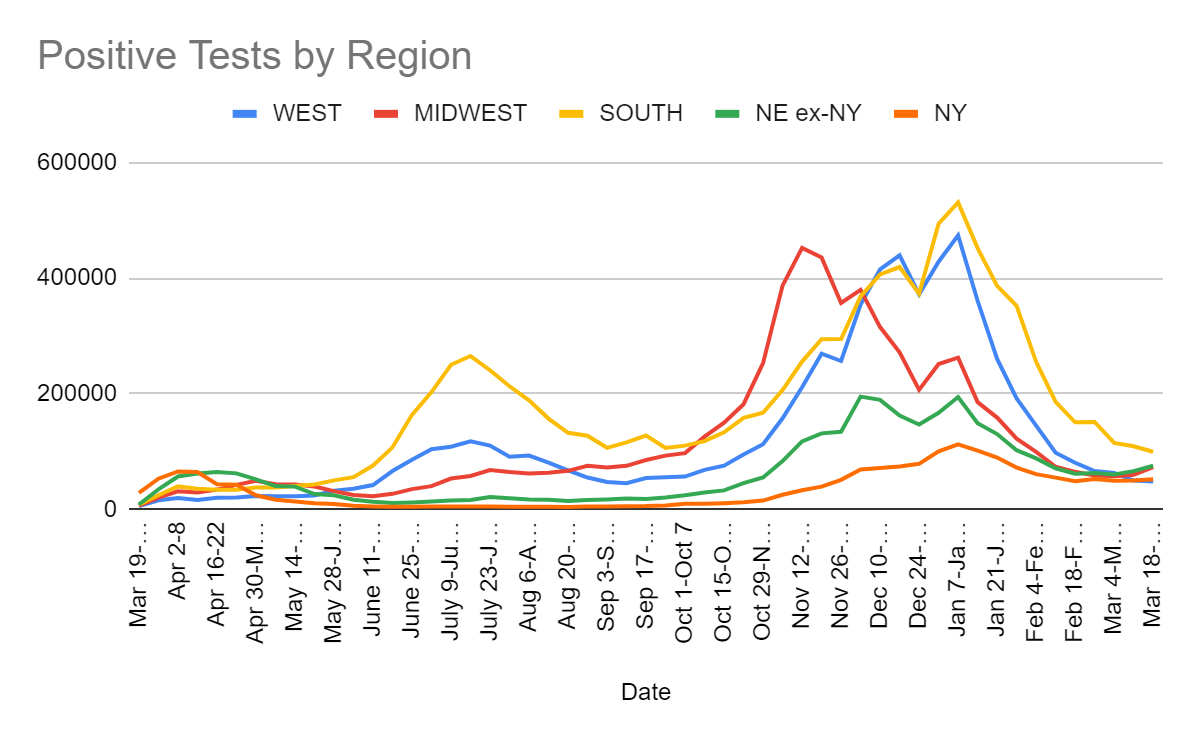
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Feb 11-Feb 17 | 97,894 | 73,713 | 185,765 | 125,773 |
| Feb 18-Feb 24 | 80,625 | 64,857 | 150,493 | 110,339 |
| Feb 25-Mar 3 | 66,151 | 58,295 | 151,253 | 115,426 |
| Mar 4-Mar 10 | 62,935 | 57,262 | 114,830 | 109,916 |
| Mar 11-Mar 17 | 49,696 | 59,881 | 109,141 | 115,893 |
| Mar 18-Mar 24 | 47,921 | 72,810 | 99,568 | 127,421 |
A number of states saw 20%+ rises in cases, including Michigan, Pennsylvania and Illinois.
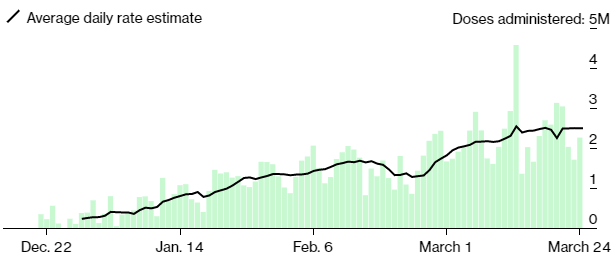
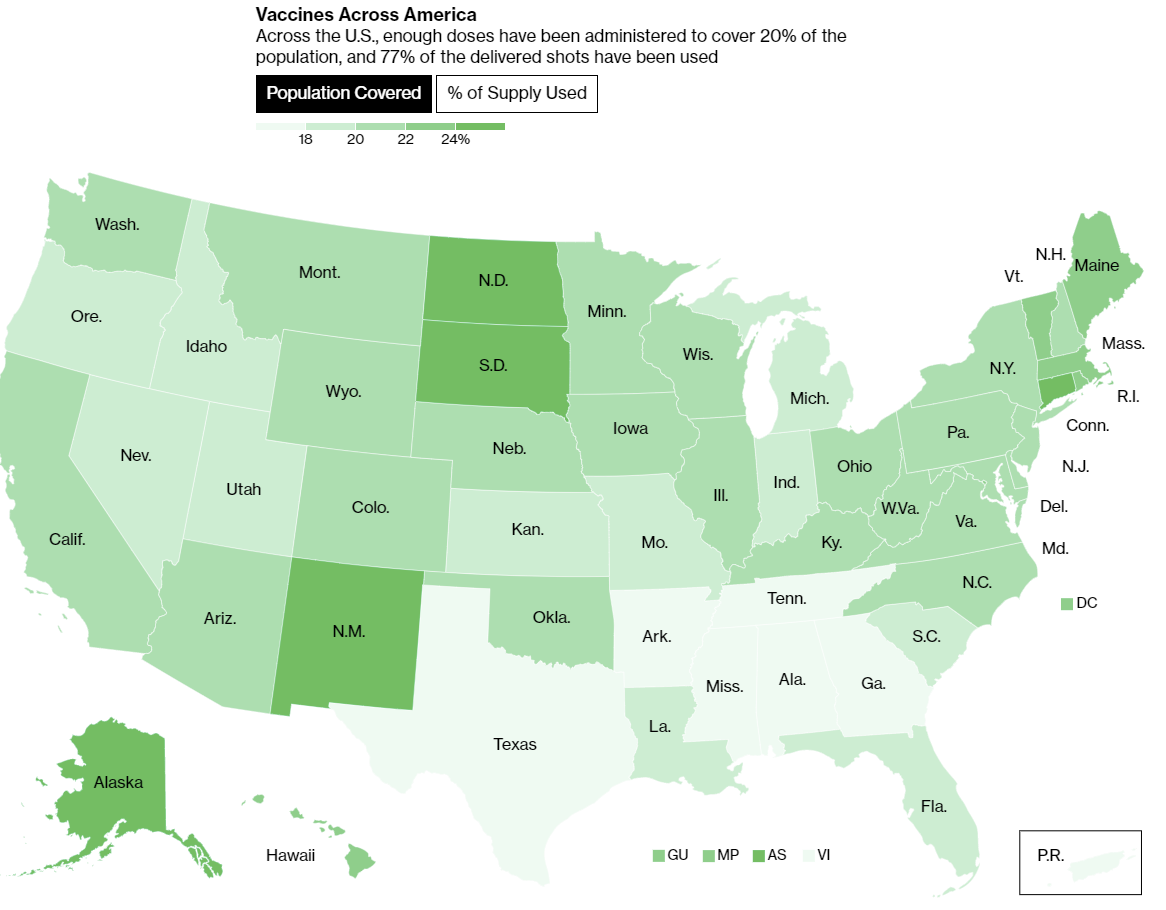
It’s also worth remembering, if you are unvaccinated, that these tallies include an increasing number of vaccinated people. Every week another 3% or so of the adult population gets vaccinated for what Bloomberg currently calls 20% overall vaccine coverage, and most of the infections are coming out of the remaining unvaccinated population. That’s an extra 25% effective risk above the numbers for anyone still fully vulnerable, compared to numbers from last year, and that gap will continue to rise. Take action accordingly.
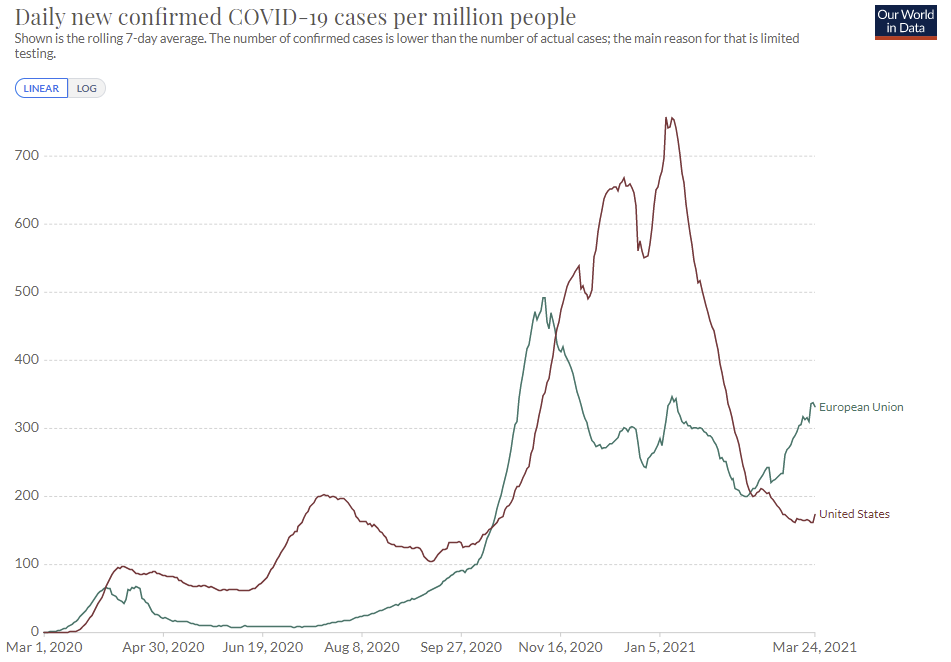
In Europe, the situation is rapidly getting worse despite strong lockdown efforts in many places. Rather than go with the previous hard-to-read multi-country graph, I’ll show only the European Union:
Vaccinations

When can anyone who wants a vaccine fail to load a crashing website where they will eventually be able to book an appointment? Here’s a handy guide.
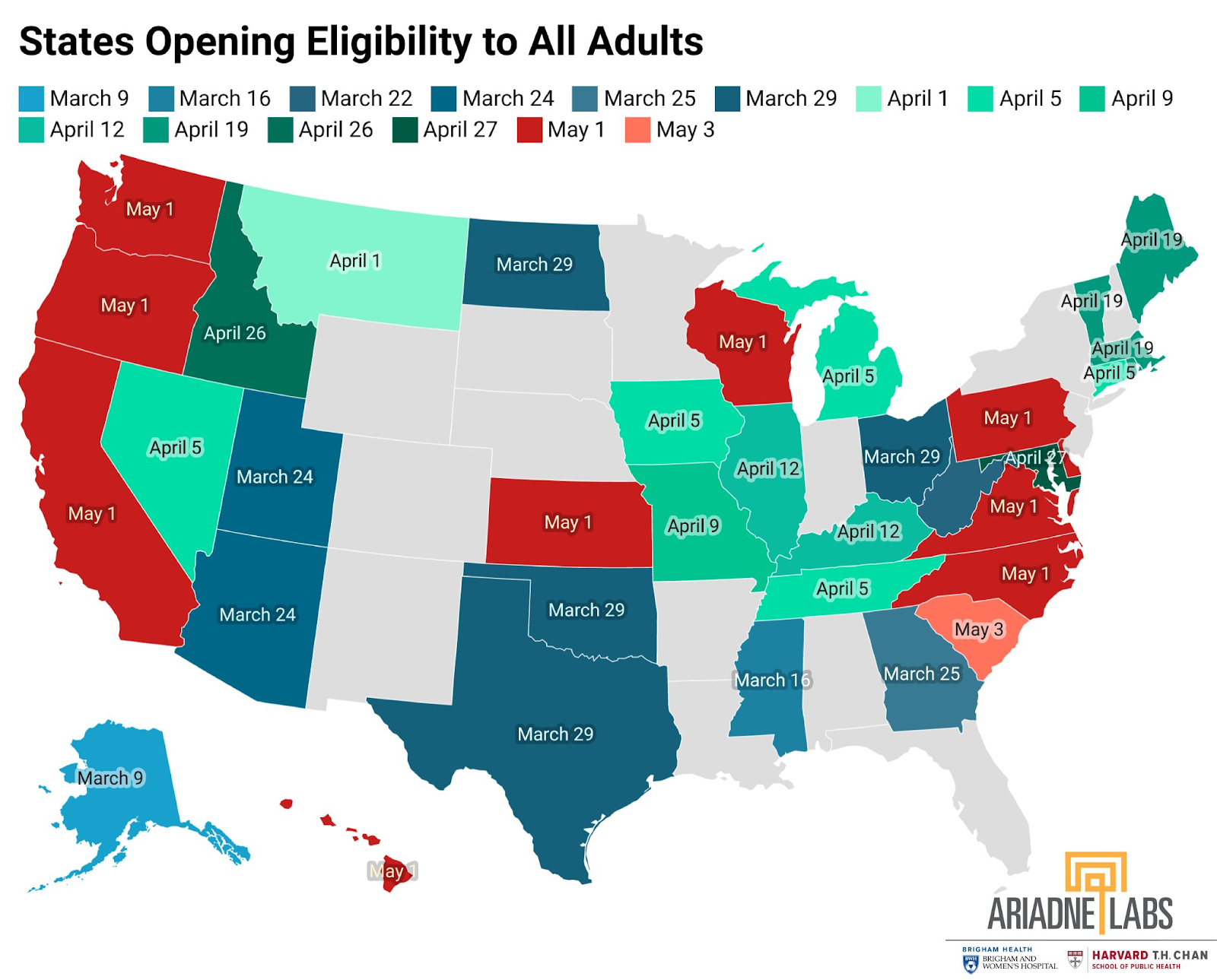
That means New York and Florida among other states so far have not heeded Biden’s call for universal May 1 eligibility. My guess is that they’ll do it anyway, but we’ll see.
On a similar note, I’m super late to the party but in case you also missed it, this is great and all too accurate: SNL’s So You Think You Can Get The Vaccine.
Here’s a piece on vaccine access and the problems people have in practice trying to get an appointment, by journalists who booked thousands of appointments and wrote up their experiences. Many strong takeaways, including several important practical takeaways, including that mostly the exact time of your appointment does not matter at the big sites so long as you’re there the same day. This is the way.
It does seem like appointment access is steadily improving. We have anecdotes like this:

Also thought I’d signal boost this even though it’s likely largely out of date:
If you want the Johnson & Johnson shot, that’s going less well. It seems that when officials said explicitly they have no plan, that did not bode so well.
That’s on top of J&J failing to produce that much supply, which is also not going well.
One source of that seems to be that a contract manufacturer Catalent they used needed its own emergency use authorization which they only got this week. That was holding back millions of doses, and the delay plausibly killed thousands. And that saga isn’t even over yet:
The whole debacle makes it clear that the FDA is causing far more delays in vaccine manufacturing and delivery with its red tape than one would guess only looking at the topline delays in authorizations.
Also, if you have gotten vaccinated, don’t forget to claim your free Krispy Kreme donuts. One free glazed any time you show your card, not even a one time deal. Being obese and thus at high risk for Covid-19 no longer matters to you, so it’s doubly good! Remember, the key is not eating several additional donuts while you’re there.
AstraZeneca Vaccinations Resume In Europe
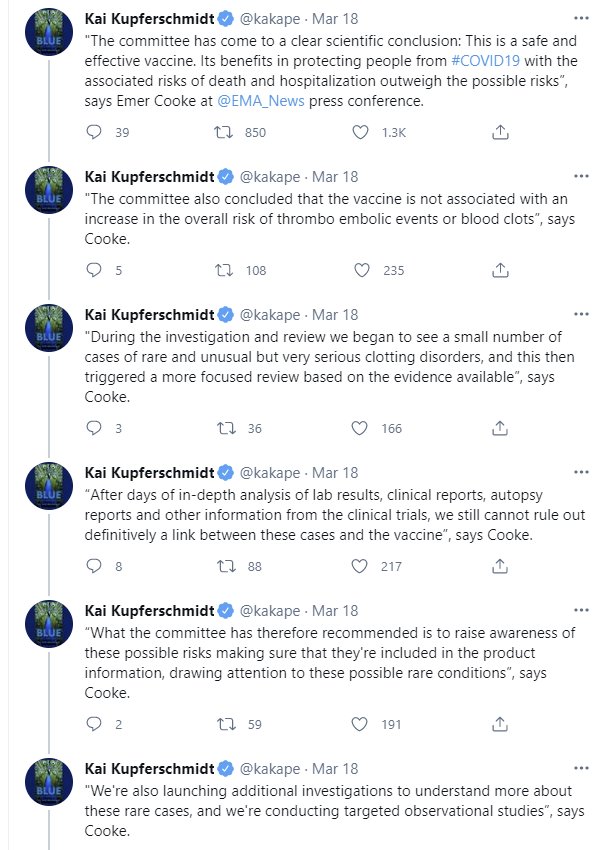
The pause is over and vaccinations have resumed, after the EMA issued its official decision shortly after last week’s post went up. This was a supremely overdetermined decision from a cost/benefit standpoint.
Here’s Kai’s summary of the statement, which somehow manages to call for everyone to still be concerned and calls for us to Raise Awareness of a phantom danger, which will have the primary effect of making people not get vaccinated (and almost no secondary effects).
As expected, elites that backed halting vaccinations in order to show how Very Serious they were got the Official Word right away and pivoted to explaining how important it was to be cautious for no reason, and how it’s now important to resume giving life saving medicine once the Official Word came down that the exact same information we had last week still contains no case whatsoever for halting vaccinations.
There seem to be two stories being told at once by the Very Serious. One is that the pause was necessary to assure people we were being Very Serious, and took potential risks seriously; if we didn’t signal we were willing to move the trolley to the track with thousands of people on it, in order to maybe save the handful of people who might be on the other track, who would trust vaccines? The other case is that we couldn’t possibly know anything until the Proper Authorities at the EMA say it in the proper form, so once safety had been thrown into official doubt, we needed to wait for Official Word to be sure we weren’t doing something awful.
I’m glad the full pause is over. I am highly confident that this did far more damage to vaccine confidence than would have been done without a suspension, and I am also highly confident that elites will continue to insist that this is not the case no matter what happens, and that they will keep patting themselves on the back for their actions.
I strongly endorse this strong prior:

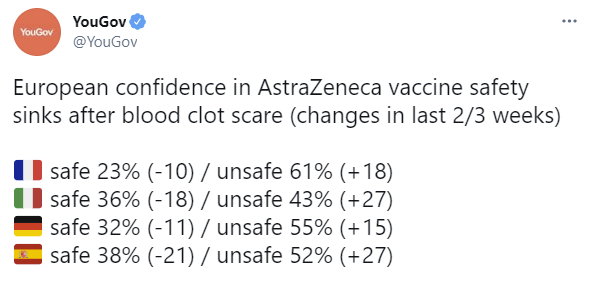
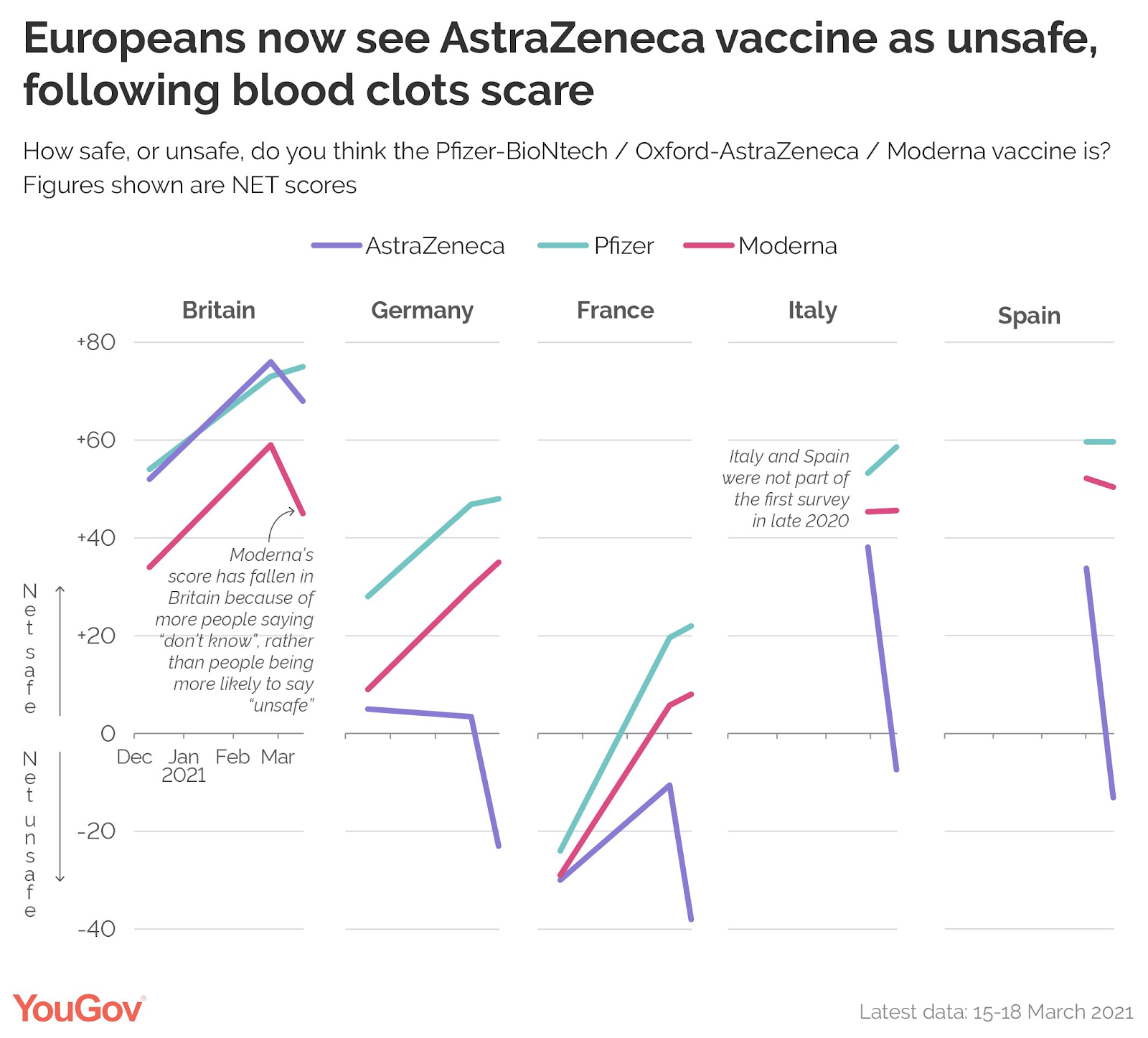
Here’s some concrete data on what’s happened to vaccine hesitancy in Europe. I don’t think Nate’s comment is entirely fair, in the sense that we’d expect increasing hesitancy right now under any scenario, but still, magnitude here is large.

Australia is trying the plausible-sounding gambit of telling people who have explicit blood clot issues to avoid the AstraZeneca vaccine. Which has essentially no first-order object-level consequences, because such conditions are super rare:

That’s unlikely to kill anyone directly on net given Australia’s situation, but what it does is send the clear message to everyone in Australia that the reasonable authority figures think there’s something wrong with the AstraZeneca vaccine.
Thus, I expect this approach, while far less bad than what Europe did, to still backfire.
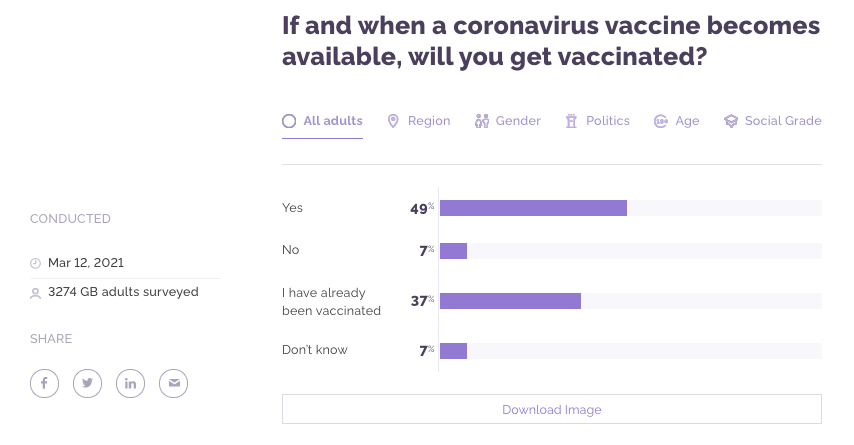
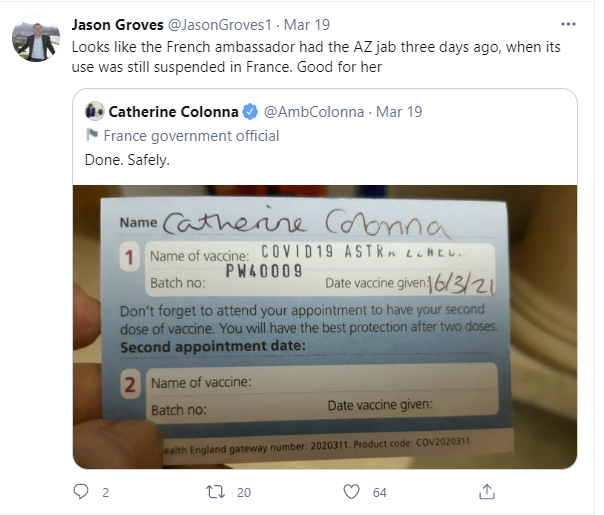
Whereas here’s how it’s going in the United Kingdom, which ignored the whole thing:
Lest we think this is fully over, the madness will continue until morale improves (WaPo), and I do not expect improved morale:
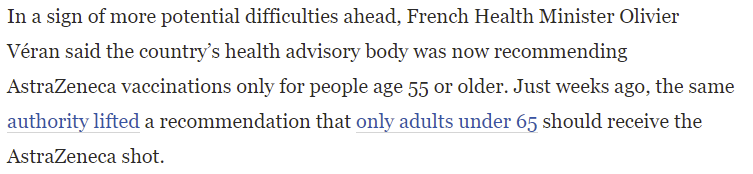

I can’t blame the people for getting confused and skeptical when they get these kinds of messages. Model what such authorities are thinking, and what they care about, based on what they say and do.
Plus things are still halted in some places:

Perhaps the most interesting part of the whole situation is the question of what is the ‘default’ action, which thus counts as inaction and is not blameworthy, versus what would constitute a non-default action, and thus be fully blameworthy for incurring even the theoretical risk of loss while getting zero credit for any gains? In other words, which track is the train already on when we decide whether to flip the switch?
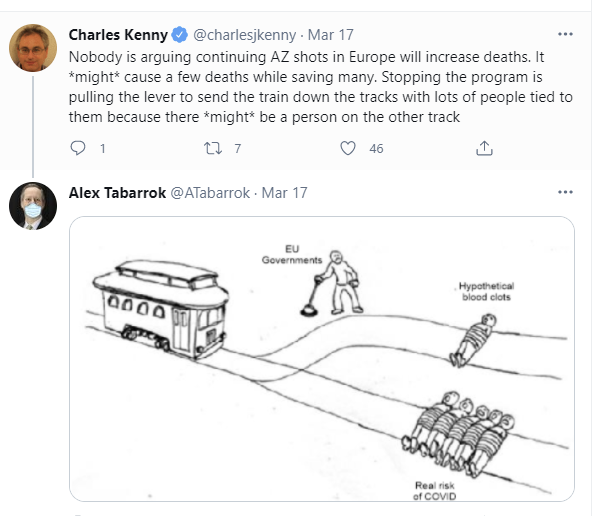
If we could get the ‘stopping AZ is flipping the switch’ intuition to stick, then no one would have flipped the switch. Somehow, elite and ‘ethicist’ wisdom got so internalized that halting vaccinations over a phantom in the wind effectively became the default action.
Meanwhile, if you’re European and still aren’t sure what happened, Johan Norberg provided a handy FAQ during the suspension, which would now need to be slightly modified since vaccinations have resumed, but still seems worth sharing in full:
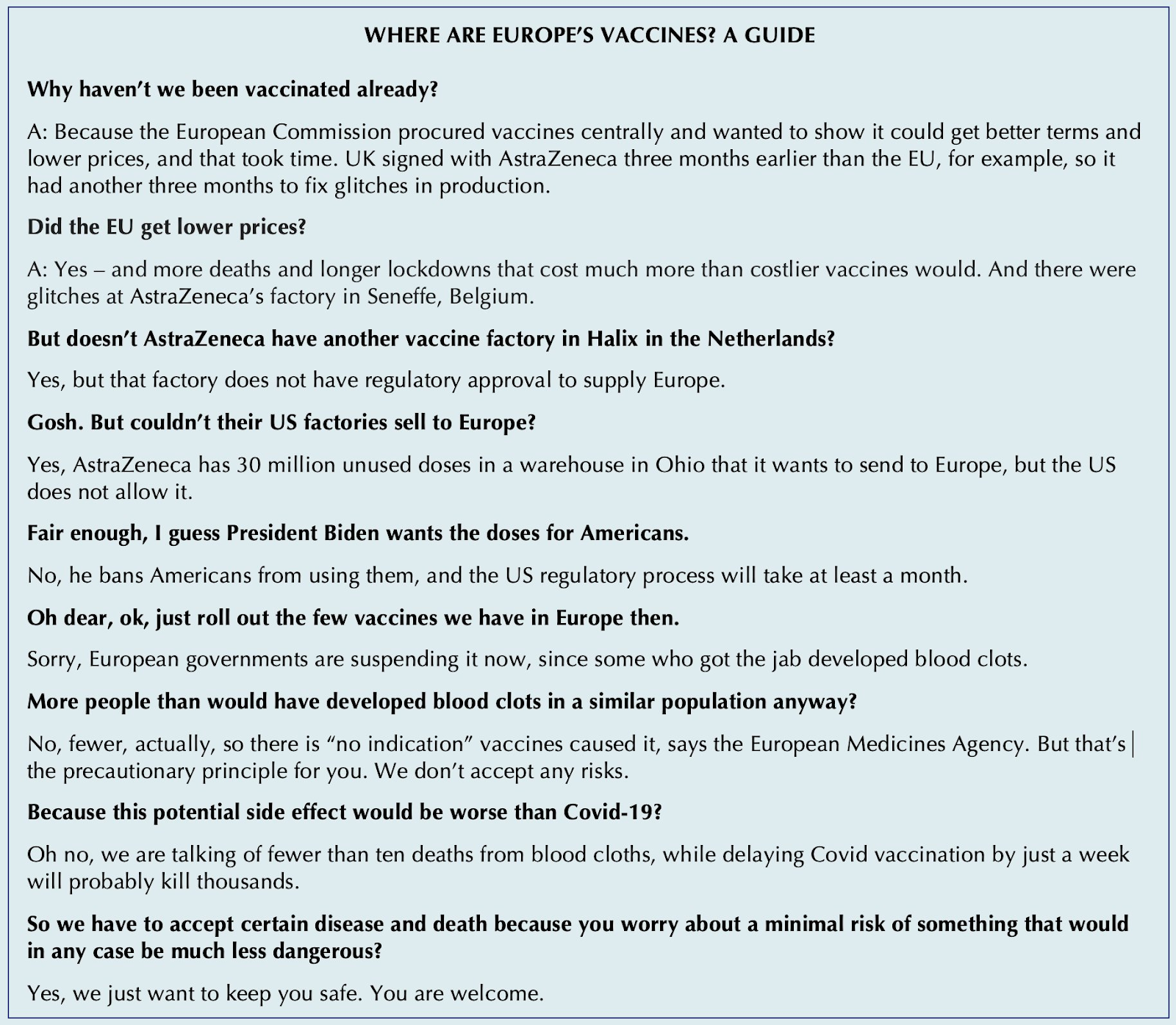
We also have MR’s take on Europe’s vaccine efforts.
And this is offered without further comment, beyond my congratulations:
I Will Not Invoke The Copenhagen Interpretation of Ethics
With 30-60 million doses in reserve, and no intention of approving or using the AstraZeneca vaccine until after we have enough vaccines without it (we’re getting closer than when I wrote this section, but not closer enough, see below), we generously agreed to send 4 million of them overseas.
I am glad to see that we saw a problem, and in response we did something good and helpful. Excellent. Nothing wrong here. Woo-hoo.
AstraZeneca Vaccine Once Again Found Safe and Effective?
It was looking to be very good news.
AstraZeneca’s American trial results were in (WaPo). Sample size of 32,449. The headline numbers are 79% effectiveness against symptomatic Covid-19 and 100% (once again!) against severe disease and death, although that was only 5 cases versus 0 cases so it doesn’t mean much.
Part of the justification for all this delay was the need to check various subgroups, both age and ethnicity. The study made extra effort to ‘look like America’ in these ways, and found essentially no variation between groups. This is of course rather silly, since if you actually cared mostly about such groups you’d want to overrepresent them, but theater, like war, never changes.

As one would expect, blood clotting was examined, and they found nothing:
We’ve managed to stall out the process long enough that we likely won’t need the vaccine once it gets approved, even if nothing unexpected goes wrong from here:
There were already real messaging issues with the AstraZeneca vaccine, as it is less effective than Moderna/Pfizer, and now the Europeans have muddied the waters further, to the point where introducing AstraZeneca in America might end up doing more harm than good via confusion and increasing overall vaccine reluctance. I’d still approve and use it if I could do so now, but if we’re going to wait weeks for an application then weeks for a review, we could plausibly be far enough along that it makes sense to ship all our AZ doses overseas anyway.
If it gets to be May 1, and we make everyone suddenly eligible while also approving AZ and making available 60 million doses, it’s going to be an interesting dilemma for unvaccinated people who can’t find an appointment for a better vaccine right away. With a vaccine surplus likely imminent at that point, the advice ‘get any vaccine you can as soon as you can’ no longer would obviously apply even to those who know the ‘risks’ involved are pure phantoms.
So, about that ‘nothing goes wrong from here’ line, there’s one little problem.
My consistent line on companies releasing their trial data has been that one can assume it’s right because if it isn’t right then officials will quickly figure this out and it would be a disaster within the two week blame horizon, so there’s no reason for them not to get it right.
AstraZeneca has decided to test that theory on multiple fronts. The part where we can trust the initial release was decisively disproven. The part where any deception would be quickly spotted seems strongly confirmed.
The mystery is how in the world AstraZeneca thought they would ever get away with this, especially on top of both the botched initial studies and the recent ongoing (completely unfounded and undeserved) doubts involving blood clots.
Or, alternatively, did Oxford really find a pharmaceutical company so incompetent that they did this by mistake, on top of giving an entire trial segment the wrong dose of vaccine the first time around? These are some rather epic screwups.
The safety board outright told AZ that they should be using a lower safety estimate, and AZ went ahead and used the higher number anyway (from WaPo).

There was a known actual 0% chance this would work.
The widespread response seems to similarly be disbelief that AZ could be this stupid.


This was worse than telling your mother you got an A in the course when you got a C overall and an A on one test. This is you telling your mother you got a C+ after your father already knows you got a C-, told you that you’d better not pretend you got a C-, and there’s no real consequences to you based on the slightly lower grade, and your father is standing right there during the conversation.
The rest of that WaPo article and the rest of the Stat article flesh out the details, with a heartwarming amount of scrambling to stop this debacle from sinking the vaccine’s approval or the public’s trust in it. My model of how this would normally work is that they’d be looking for ways to punish AstraZeneca for this, which is quite reasonable given that the incentives involved have to be maintained. Instead, everyone is doing their best to admit they are stunned but essentially turn around and say ‘la-la-la, I can’t hear you, I’m sure you said the right number, right?’ for practical purposes, and hope the public doesn’t notice.
I agree strongly that we need to do a bunch of whistling in the dark and get this approved anyway, even if it’s a little late to make that much difference, and to paper over the potential loss of trust in the vaccine. To the extent that I wrote a paragraph after this and then deleted it rather than give ammunition where it shouldn’t be given.
We still need to punish AstraZeneca the company, and hard. The default outcome is of course this:
And that’s completely unacceptable. The fine for this should be freaking huge. Enough to materially move the stock price. Heads at the company need to roll. And the next time they come to us for an approval, or issue a press release, we need to remember that this happened. No reputational bailouts, please.
What happened in the end, at least so far?
It looks like they’re now going with 76% effective as their new story, and so far it’s still sticking. That’s not that different from 79% for any regulatory purposes, so the whole thing really was a pure own goal.
Have You Tried Increasing Supply?
For a while it’s been clear that the world is capable of producing far more Covid-19 vaccine doses than it is producing. A few billion dollars would have bought us vastly greater production capacity, and it still could do so in time to impact the third world greatly, which would be highly worthwhile for direct impact and also selfishly wise for us to do purely in order to limit potential mutations. As Tyler Cowen puts it, trillions are bigger than billions.
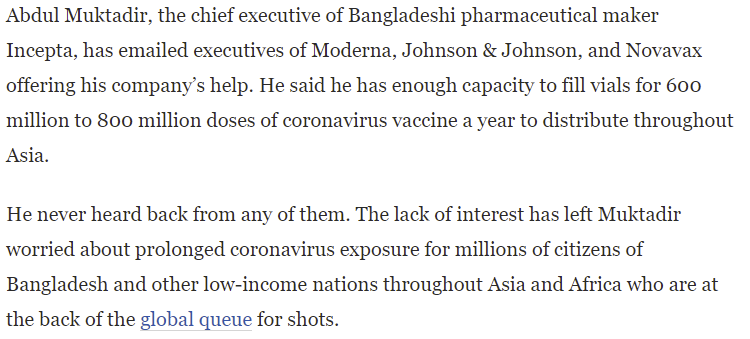
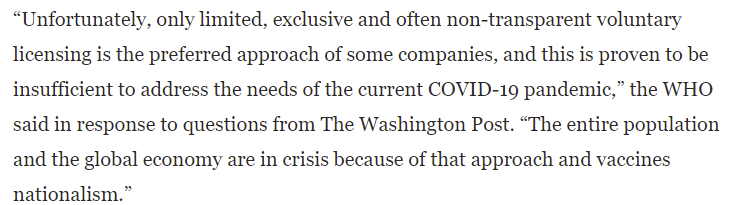
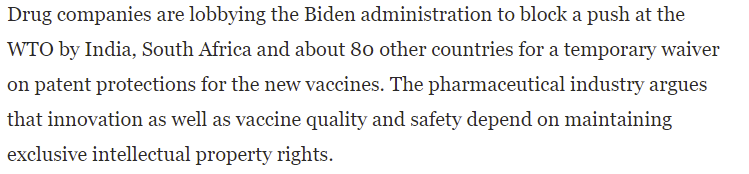
This week we have yet more evidence that there is lots of slack in the vaccine supply (WaPo) if we collectively paid what it would take to use it.
(Also, you gotta admire the chutzpah of saying vaccine manufacturers are ‘defending their monopolies’ when many vaccines still sit ready to go, safe and effective yet unapproved, the rest were delayed for needless months, and while companies are forced to accept fixed monopsony prices from governments who refuse to pay for more capacity or speed, and who pause for investigation and cripple public faith in all vaccines when there are side effects at below the rate in the general population. I mean, yeah, wow.)
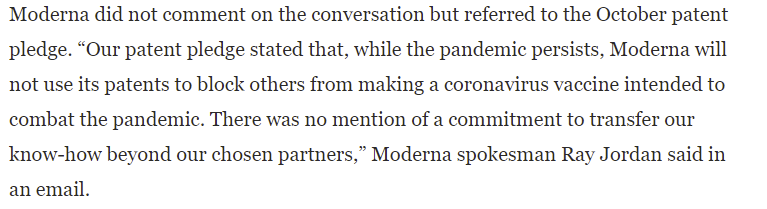
In particular, there are additional pharmaceutical firms capable of manufacturing vaccine doses if given the legal right to do so, and the holders of the relevant intellectual property are saying no.
Except, from how I read this, they’re not saying no because they want to preserve their patents – Moderna in particular already said they wouldn’t enforce theirs, and I doubt anyone else would either no matter what the drug companies wanted.
They’re saying no because they don’t want to teach other companies how to produce vaccines. They’re also concerned about quality control, and what would happen if another manufacturer made a mistake – it would doubtless still be a net huge win on first order grounds, but faith in vaccines in general, and in each company’s product in particular, is fragile.
.
Which all makes perfect sense from a business standpoint. Their technical expertise is their entire business, so is the trust in their brands, and it all transfers between products.
Here are some choice quotes from that piece, in which cases are made from all sides, from which I believe the overall picture becomes clear:

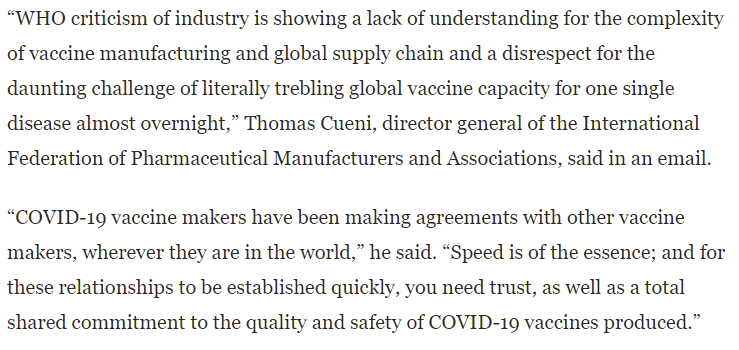
If we cared enough, we could pay off the necessary stakeholders and make all of this happen, as an extreme upper bound all the vaccine manufacturers have a combined market cap below a trillion dollars most of which is unrelated to any of this, but like paying to expand capacity, we are choosing not to do so or even seriously consider doing so. There’s still time to get the rest of the world vaccinated at a much faster pace than would otherwise happen, and in doing so save a lot of people and also dramatically lower our risk of mutations.
The Safe Distance For Children Has Always Been Three Feet
That is all.
Talk To Your Kids About Covid-19
An important fact about teenagers is that they mostly don’t underestimate the risks from activities like drunk driving. Instead, they mostly greatly overestimate those risks, then often decide they don’t care and do the stupid and dangerous stuff anyway, because they’re teenagers. The typical response strategy is to misleadingly scare kids even more so that they’ll end up acting more like we want them to act.
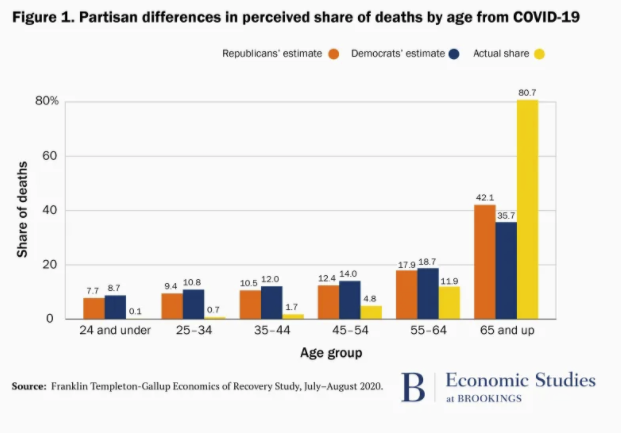
Why should Covid-19 be any different? In a thread that’s centered on explicit bothsidesism with regard to Covid mistakes, David Leonhardt drops this chart (source that has a lot of good data):
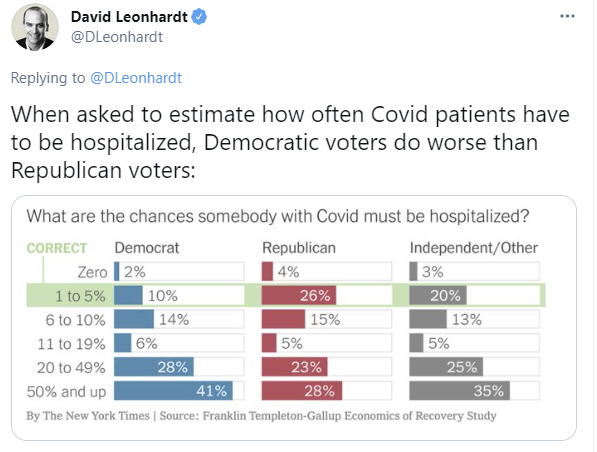
As usual, when one is tallying up points for who is doing better or worse and deserves more credit or blame, the lead gets buried. The lead is the implicit ‘overall’ chart that combines all three of these, and that the three charts aren’t fundamentally that different.
A large majority even of Republicans still are vastly overestimating the hospitalization rate, with half of them thinking at least one person in five needs hospitalization.
There’s a huge correlation with the Berlin Numeracy Score (and also sadly if you do the math not that many people scoring high on the Berlin Numeracy Score, looks like about 29% of Republicans and 27% of Democrats if my calculations are correct):
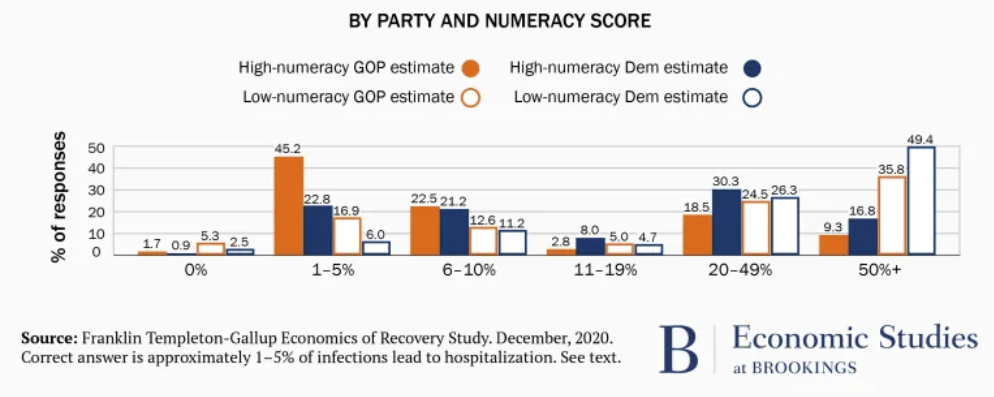
You see a similar thing here:
The small extent to which the Republican estimates here are better is much less interesting and important than the extent to which everyone’s estimates are way, way off, in the direction that would lead to people being far more cautious than they would otherwise be, and much closer to each other than to the right answer.
We don’t have the high vs. low numeracy chart for this one, but I’d be curious to see it.
My guess is that we can afford to mostly not treat the low-numeracy people as meaningfully having numbers assigned to things at all. When we ask them for numbers, we get garbage answers because they don’t think that way at all, and you get a detached wild guess slash attempt to give the right no-context social response to a question rather than anything that’s meant to represent reality.
For the high-numeracy people, the numbers likely at least mean something. They’re still wildly wrong, in ways that are more enlightening, and they are more different by party than the low-numeracy numbers rather than the reverse, which is interesting.
Should we score this as a clear win for Facui-style level-two thinking and communication (also known as ‘lying’)? That depends on people adjusting their behaviors based on their perceived risk levels, and on those adjustments being useful rather than not useful, plus a willingness to pay the costs involved in misrepresentation. I don’t think those questions have clear-cut answers. I do think that some sympathy for the devil is reasonable here, in a ‘if you told them the full truth and they understood it you wouldn’t like their answer’ kind of way. Humans often solve risk problems and collective action problems by having very false primary and intermediate values in their calculations, then doing incorrect manipulations to them that get tuned in various ways until they give reasonable answers. This is another illustration of all that.
The other question is, if we told people the truth, would they make all these errors anyway? Or to put it another way, if you listen to me say 1%, when asked for the answer write down 25%, but then tend to make decisions that make sense if the answer is 1%, and you’re not ever asked for explicit calculations in an impactful sense, where’s the mistake? In what sense are you really being wrong here?
I think that’s an excellent question and that we haven’t given it enough thought.
Public Broadly Supports Challenge Trials
Ethics is hard, but it’s nowhere near as hard as ‘ethicists’ think it is. The public knows better (source).

Challenge trials are super popular, and the concerns of ‘ethicists’ are simply wrong. Excellent.
In general, if something has 75% popular support, and those who best understand it give it 90% support, that’s a pretty popular thing, and when the only thing stopping it is that it’s illegal, supporting legalization seems like a very good political issue for either or both parties or any politician to take up and make their own.
I also wouldn’t worry about those ‘ethicists’ on any level. Not only are they always wrong and destructive in everything they do, they’ll fall in line on this when policy changes, and move on to trying to slow down and cripple the challenge trials the way they try to slow down and cripple every other type of experiment or other useful action. It’s their job, after all.
Going forward, the agenda is clear. Human challenge trials, always, in all things, as the standard, default way to test new vaccines or other applicable treatments in Phase III, with proper compensation to participants.
In Other News
Take me out to the ballgame, at the latest some time in May, concerts getting similar treatment, I’d prefer a higher percentage with only the vaccinated which seems better all around:


Take me out of the ballgame and keep me out long enough to fully recover, because Covid-19 is really nasty and you very much do not want to get it even if you know you’re not going to die. Article looks primarily at the NBA and the longer-term impact of Covid on its players, especially players who push hard to return quickly. Post includes reports of many athletes where there’s nothing physically wrong with them that can be identified, yet their performance levels haven’t corrected themselves for extended periods. Very hard to tell from things like this how frequent or severe such effects are in general, and how scared young people especially should therefore be of the virus.
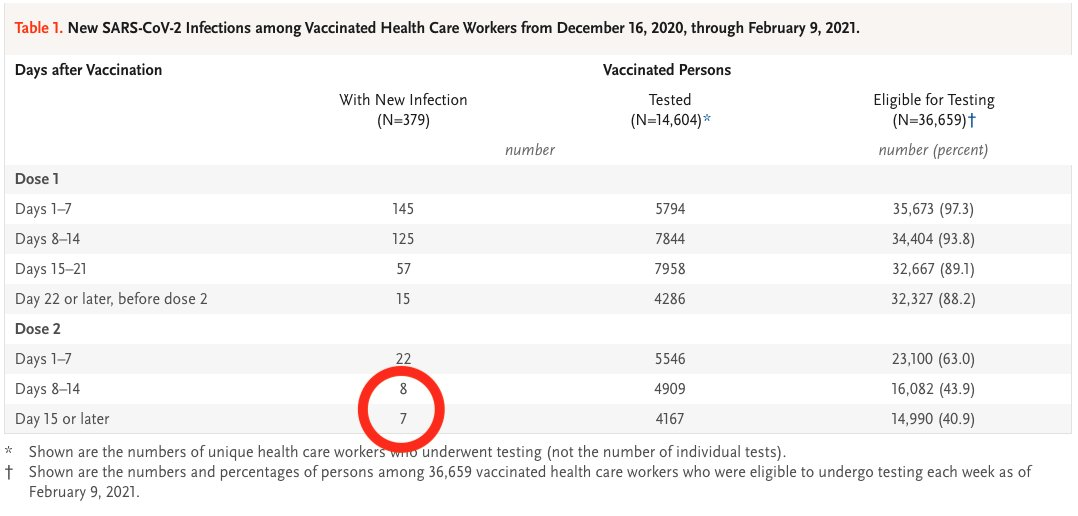
Data on infections post-vaccination among California healthcare workers. I’m doing a bunch more thinking on exactly how delayed we should treat the vaccine response. The initial trials strongly suggested very good protection after about day 10, whereas the in-the-wild data we have, both here and from Israel, suggest similar longer term results but that it takes longer to happen. I think I initially mostly dismissed the Israeli data for reasons that don’t hold up under scrutiny, and we should be more skeptical of how protected we are in the second and third weeks after vaccination – it’s still a lot, but probably not a 90%+ ‘hot damn look at this chart’ level of protection, and that’s likely due to real world conditions messing things up reasonably often, in ways the second shot still fixes.
New Zealand experiences the joys of vaccine prioritization by politics and power, except the relatively sane one both because New Zealand is relatively sane in general, and because they don’t have an ongoing pandemic so anyone not looking to leave the country can afford to wait a bit no matter how high-risk they would be.
Cuomo Watch: New York is over Covid and has its priorities straight:
(Yes, those are only budget priorities, but still. Also, I get it, it’s been a rough time and you gotta mello out, man.)
An analysis of a likely airborne infection inside the quarantine hotel in New Zealand. I’m not as blown away as the thread author is, and in general such things are unlikely, but I have little doubt that they happen.
Also Cuomo watch (WaPo):

Now that everyone’s truly out to get him, we should expect to find lots of abuses of power, because abuse of power should come as no surprise. Cuomo I do think was unusually abusive in all senses, but the main difference between Cuomo and similar others is mostly that Cuomo is now a scapegoat and thus is getting caught and called out, rather than that such behaviors are rare.
In other allocation by politics and power news, if your diversion of vaccines to your employees includes a place with the word Trump in its title, then maybe we’ll notice (WaPo). Doesn’t seem like the consequences for this are going to be much of a deterrent, even as the symbolic scapegoat case, and I presume this kind of thing happened a lot and mostly wasn’t caught.
Germany is imposing new restrictions. The explanation is something that perhaps they could have seen coming…
Merkel tried to go even farther this time, then backed down saying it wasn’t practical, and accepted responsibility for the overreach, providing good evidence that there isn’t much more slack left in the system in that direction.
Why did Germany previously loosen? Pandemic fatigue. I’m more sympathetic to this than Kai is, in the sense that if there are increasing costs over time eventually you can’t and won’t keep paying them, even if the consequences are dire. The vaccination campaign in Europe isn’t far enough along to give people a reasonable end point, and hoping to sustain harsh restrictions that long never seemed that likely to work.
Then there’s this from Austria, where similar dynamics seem to have forced the issue. At some point, all options become impossible for different reasons.
We shouldn’t feel superior on this, any more than Europe should have felt all that superior to us earlier. If our vaccine effort wasn’t where it is, would we be any different?
I hadn’t heard what was going on with Novavax for a while despite it looking like they had a proven safe and effective vaccine, found this article from early in March saying they’re on track to ship in June. Article in question doesn’t seem to notice this is a problem.
Paper finding cognitive function declines in face of prolonged social isolation. Social isolation costs are definitely being downplayed by many, with the ‘cognitive decline’ aspect seeming like a way to make a part of it legible so that at least part of it can be properly considered in decisions. Reminds me of other similar concerns that got ignored without quantification.
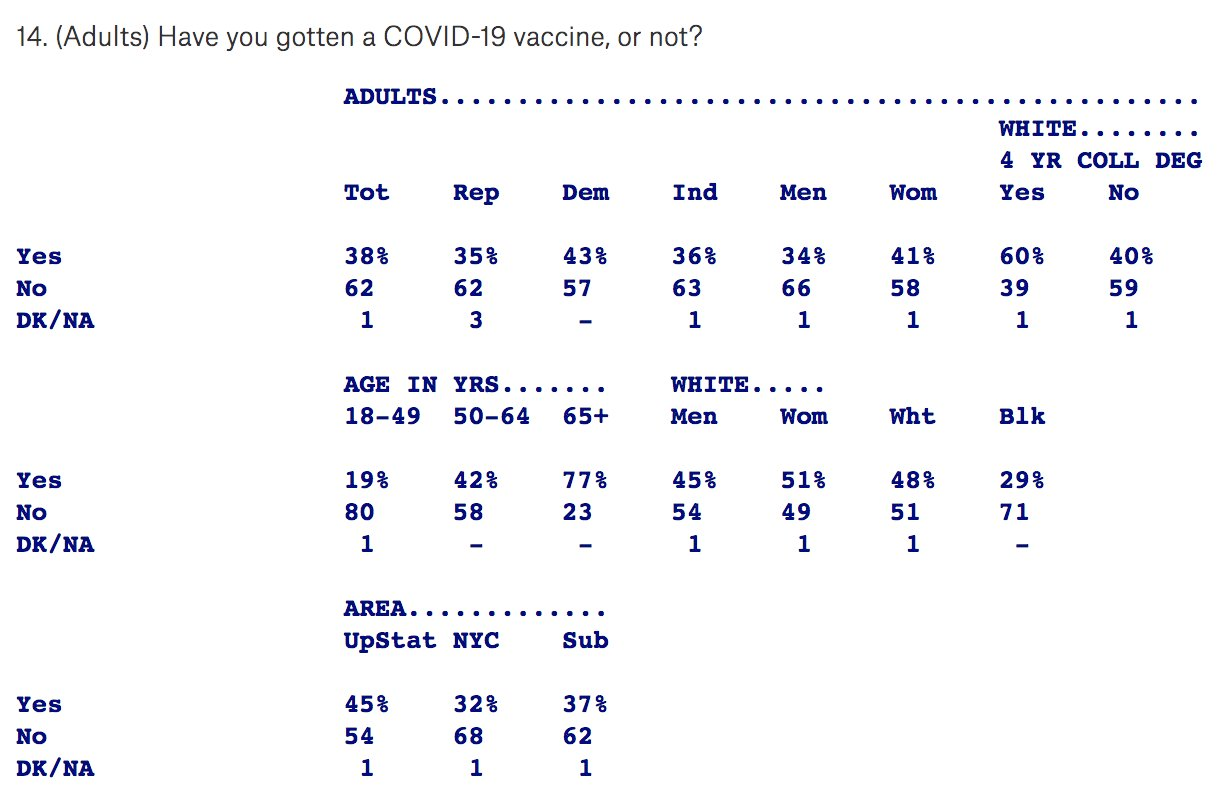
Getting vaccinated correlates to answering polls in a way that isn’t easy to correct for (poll).

Results are also interesting, with a bunch of different dynamics going on here and being combined. I’ll let the numbers speak for themselves, remember to adjust for who answers polls.
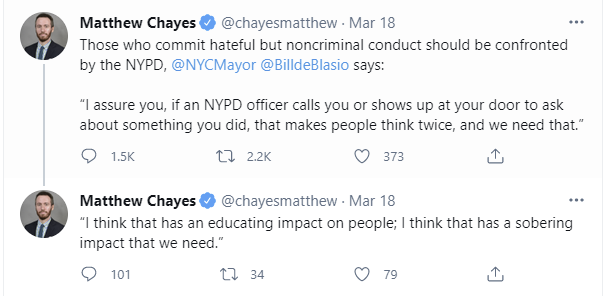
Not Covid, Not a Crime Either: Bill de Blasio calls for sending the police in when people are spotting committing wrongthink.
Twitter thread on Supreme Court rulings on Covid-19 restrictions, the opinions written in support of them, and how it is being treated as a gotcha when justices stop pretending they don’t know things, and illustrating what happens when there’s no such thing as knowledge or law but only blame avoidance.
This Vitamin D observational study is super weird. It’s saying that in black individuals vitamin D levels mattered, but in white individuals they didn’t, even for correlations and even for fully deficient levels of Vitamin D. This proves way, way too much, so I notice I’m confused. We have seen lots of studies showing correlations of D-levels with results in ways that ethnicity doesn’t screen off, and the counterarguments against it were along the lines of of course there’s a correlation because people in poor health have low D levels and to the extent D is doing work it could be by needing to not be deficient. Yet this is claiming to blow past all of that. What’s up here?
Retrospective called “How the West Lost Covid.”
Looks like there was a brief period where Danville was handing out vaccinations to whoever wanted it, but the health department shut it down.
A survey on how effective ‘reasonable prevention’ was at preventing Covid:
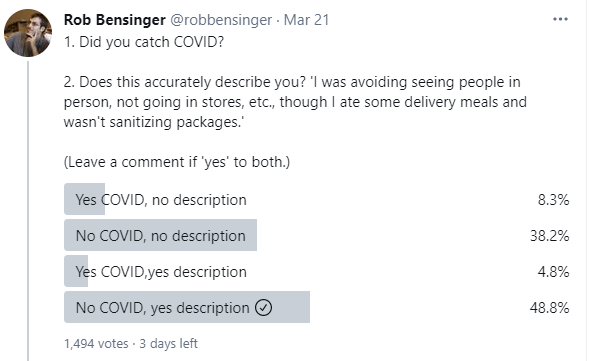
My worry here is that some people who were even more paranoid than that got put in the no category, and given who follows Rob I’m guessing that could be a sizable group, but it’s cool to see. This is an overall 13.1% rate of getting Covid, and 17.8% even in the “no” group, which is substantially lower than the nationwide average of about 30% (some people answering weren’t American, but still that’s a big gap), which supports the idea that this group is a lot more cautious than usual. The “yes” group had a 9% rate, about half of the “no” group.
Between people thinking they followed such rules when they didn’t, the lizardman constant slash misclicks/misunderstandings, false beliefs about having had Covid (which aren’t that rare) and the most cautious people of all being in the “no” group, that 2:1 ratio is almost certainly too low. I don’t think I’m the best person to repeat this quiz (since my followers largely read this) while fixing the wording (something like ending with the etc in the description on #2, and ideally with “USA only” on it and if desired a second copy for non-Americans) but I’d encourage those with enough and diverse enough Twitter followers to give it a shot. Would also be cool to see how often different groups did this level of prevention, in addition to the goal of being able to get effectiveness.
New analysis on how we could do the most important thing and speed up vaccination capacity. Le sigh.
Vaccination is a superpower, it even gives you the ability to fly, but no, it isn’t as cool as being bulletproof, even if you discount required secondary powers and healing factors involved. If one was bulletproof, one could change one’s behavior even more than you can when you’re vaccinated. Luke Cage is a lot more likely to get shot than Alex Tabarrok or even Trish Walker, and she’s not exactly doing proper social distancing.
This week I’ll once again be travelling into New York City, this time to get my second vaccine shot. It’ll be that much better not having to be so paranoid while I’m there. The third trip a few weeks from now will be even better.
17 comments
Comments sorted by top scores.
comment by magfrump · 2021-03-26T05:07:53.705Z · LW(p) · GW(p)
A friend of mine on Facebook notes that the instances of blood clots in Germany were concerning because in Germany mostly young health care workers are getting vaccinated, where it's both more possible to distinguish small numbers of blood clots from chance and more concerning to see extreme side effects.
The rate is still low enough that pausing vaccination is (obviously) a dangerous move, but dismissing the case that blood clots may be caused by the vaccine isn't a fair assessment of the evidence, and that may be important in maybe two years when supply of non-AZ vaccines is no longer a limit for the world.
comment by Cesare · 2021-03-27T12:16:41.446Z · LW(p) · GW(p)
I am writing from the UK (decent vaccination campaign) as an Italian person (horrible vaccination campaign), and agreeing with your critiques on the USA (pretty good vaccination campaign) is disheartening. Just why are we so bad at doing crucial things, as a society? It's so incredibly sad.
comment by Bucky · 2021-03-26T09:48:09.692Z · LW(p) · GW(p)
Or, alternatively, did Oxford really find a pharmaceutical company so incompetent that they did this by mistake, on top of giving an entire trial segment the wrong dose of vaccine the first time around? These are some rather epic screwups.
My experience working for a large company makes me not particularly surprised by this and I would give a decent amount of probability to this being an accident. I don't know enough about the specific procedures to be hugely confident but it does seem most likely to me.
If we're fairly confident that the wrong dose thing was an accident - I can't think of any reason to do this deliberately and then try to cover it up - then AstraZeneca obviously have the potential to make big mistakes.
One scenario would be that the person requesting / approving the press release is not the same as the person running the project but rather their boss or their bosses boss or even in another department. The press release approver is less involved in the minutiae and has remembered the 79% figure, maybe even goes so far as to check their e-mails that this is the correct figure (or check with someone else who checks their e-mails). Probably none of these people were in the meeting with the safety board.
I have had this experience myself on many occasions where my superiors have given information to customers that is outdated just from them not being as up to date or forgetting the latest results. Obviously I'd like to think something like this would have more care taken about it but the dosing debacle is suggestive that checking things isn't AstraZeneca's strong suit.
That combined with the 0% chance of this not being noticed suggests to me that this wasn't on purpose.
comment by Rob Bensinger (RobbBB) · 2021-03-25T22:31:51.097Z · LW(p) · GW(p)
My worry here is that some people who were even more paranoid than that got put in the no category, and given who follows Rob I’m guessing that could be a sizable group, but it’s cool to see. This is an overall 13.1% rate of getting Covid, and 17.8% even in the “no” group, which is substantially lower than the nationwide average of about 30% (some people answering weren’t American, but still that’s a big gap), which supports the idea that this group is a lot more cautious than usual. The “yes” group had a 9% rate, about half of the “no” group.
Between people thinking they followed such rules when they didn’t, the lizardman constant slash misclicks/misunderstandings, false beliefs about having had Covid (which aren’t that rare) and the most cautious people of all being in the “no” group, that 2:1 ratio is almost certainly too low.
The poll was retweeted by Aella, who has 65x my follower count, so the respondents are much less rationalist and academic than you might expect. Also, only 4 of the 72 people who answered "yes, yes" followed the instructions ("leave a comment"), and 2 of those 4 admitted to being misclicks. Between this and the other issues, I think the poll results are probably almost useless.
Replies from: Zvicomment by PatrickDFarley · 2021-03-25T20:19:41.422Z · LW(p) · GW(p)
your father already knows you got a C-, told you that you’d better not pretend you got a C-,
Second C- should be C+
comment by Primer (primer) · 2021-03-28T00:22:16.302Z · LW(p) · GW(p)
I agree that stopping Astrazeneca rollout was a very stupid thing to do, but once the damage is done, I'm not so sure about resuming Astrazeneca vaccinations without any changes to recommendations.
So far, about 70 women between 20-40yrs died due to Covid in Germany. About 85% of overall Covid deaths seem to appear in connection with comorbidities. It is probably safe to assume that comorbidities play a higher role in younger patients, but let's stay conservative: about 10 women between 20-40yrs without comorbidities died due to Covid in Germany. There are around 10 million women in Germany between 20-40yrs. Let's say 8 million without relevant comorbidities. We get a risk of death due to Covid of about 1 in 800000 for healthy women in that age group.
So far, about 15 women were diagnosed with cerebral vein thrombosis in connection with an Astrazeneca vaccination in Germany. Those numbers differ from the UK's because in the UK mainly older people were vaccinated with Astrazeneca. In Germany, many younger healthcare workers got Astrazeneca. 4 women between 18-55yrs died due to thrombosis, so we can assume 2 of those deaths appeared in women between 20-40yrs.
So far, about 1.8 million Germans have been vaccinated with Astrazeneca, most of them elderly and/or people with comorbidities. So let's assume, again conservatively, that 0.5 million of those doses went to women in healthcare between 20-40yrs. We get a 1 in 250000 risk of death due to vaccination with Astrazeneca in that age group.
All this is not considering severe illness and long Covid. But it is also not considering declining cases due to warmer temperatures and (very) slowly approaching herd immunity due to vaccinations.
I'm not sure at all whether I would recommend Astrazeneca to young, healthy women who do not have a considerably above average risk of infection. At least not without having a deeper and way more thorough look at those numbers first.
Replies from: Zvi, Cesare↑ comment by Zvi · 2021-03-28T12:14:29.987Z · LW(p) · GW(p)
You can argue that risk is so low that bothering with vaccination for young people isn't worth it on selfish grounds and it is somehow more ethical then to not recommend it. I would strongly disagree due to long term risks of Covid, which are much higher than any risks of vaccination.
But also, blood clots are a disease of aging. Young people are at almost no risk of those. So even if the danger were real, which it isn't and even if there it was stupidly tiny, it would be orders of magnitude lower here.
So any argument to not recommend would have applied before anyway.
Replies from: primer↑ comment by Primer (primer) · 2021-03-28T18:41:11.219Z · LW(p) · GW(p)
I'm not arguing vaccination vs. no vaccination for young people, I'm arguing that it might not be such a bad idea for young women with a corresponding risk profile to wait a few months (at least half of which will be spent in lockdown anyways) for Biontech or Moderna.
Should you skip Astrazeneca today in order to get Biontech tomorrow? I'd say yes. Should you skip Astrazeneca now for Biontech in September if you are a young healthy woman? Maybe.
↑ comment by Cesare · 2021-03-28T11:10:58.117Z · LW(p) · GW(p)
My main problem with this is the following: I would totally recommend Astrazeneca to everyone if the choice was between a) Astrazeneca, b) no vaccine.
But this is not the case (this has never been the case!). There are better, more effective vaccines - even not taking into account this CVT mess. In a world where we can produce infinitely many vaccines in 1 second, we'd have Pfizer/Moderna jabs for everyone.
So... why are we still producing Astrazeneca? It is the least likely to have an effect on transmission - we know for instance that it is less than 10% effective against B135, which is about 20% of the cases in Europe right now (see Luxembourg data). It does protect against severe disease from ancestral and B117 (still no data on B135 severe diseases), but... so does being young and healthy.
I think that we are using Astrazeneca as an emergency measure - we don't have enough Pfizer, and people are dying. This is fine. But then, as you correctly point out, it begs the question: why are we giving it to people with close-to-none chances of dying from Covid19?
↑ comment by Lukas Finnveden (Lanrian) · 2021-04-16T23:19:43.573Z · LW(p) · GW(p)
which is about 20% of the cases in Europe right now (see Luxembourg data)
Do you have a link? (I can't find one by googling.)
Replies from: Cesare↑ comment by Cesare · 2021-04-17T11:48:27.422Z · LW(p) · GW(p)
I had a better one, but a quick googling gave me this article: https://today.rtl.lu/news/luxembourg/a/1685866.html
(second paragraph)
comment by Dirichlet-to-Neumann · 2021-03-30T08:52:13.746Z · LW(p) · GW(p)
I'm a bit late with this but I think the French site https://covidtracker.fr/ should have everything you want in term of Covid data. It has a focus on France but also gives data for other countries (and the "World" page is in English).
comment by tailcalled · 2021-03-27T10:36:47.071Z · LW(p) · GW(p)
The framing of Europe flip-flopping for no reason on the safety of AstraZeneca's vaccine seems inaccurate. As you point out, Scandinavia still has it suspended, but it was also Scandinavia that kicked off the decision to suspend, with other European countries following. (It's still bad ofc, but y'know, less self-contradictory.)
comment by IrenicTruth · 2021-03-26T20:21:59.897Z · LW(p) · GW(p)
The Science Article mentions some ways it may understate the benefit of increasing production. But it misses an important benefit altogether. The chance of creating vaccine-resistant strains increases with the number of unvaccinated people. Vaccine-resistant strains make current capacity less valuable. So all capacity becomes more valuable the faster you vaccinate people because there is less chance of starting over.
comment by ejacob · 2021-03-26T05:45:02.226Z · LW(p) · GW(p)
Hey Zvi - What do you make of the Ted Cruz-reporter spat when he refused to put on a mask? I have mixed feelings, because I think he obviously has the wrong motivation (annoying the social distance warriors for its own sake) but accidentally expressed a reasonable idea (specifically, "we should not reasonably fear infection from vaccinated individual, especially when there is the option of stepping away," and more generally, "leave the vaccinated the hell alone!")
Replies from: Zvi