Slightly More Than You Wanted To Know: Pregnancy Length Effects
post by JustisMills · 2024-10-21T01:26:02.030Z · LW · GW · 4 commentsThis is a link post for https://justismills.substack.com/p/slightly-more-than-you-wanted-to
Contents
The Inner Bullseye What’s In A Week? Study Dive: Gestational age at birth, chronic conditions and school outcomes: a population-based data linkage study of children born in England What about other studies? Any Countervailing Evidence? Why Does This Matter? None 4 comments
Pregnancy is most stressful at the beginning and at the end. First you try to conceive, and spend half of each month superimposed between two very different realities. Then there’s morning sickness, and you worry about miscarriage, which is far more likely early on.
Near the end, you can be pretty confident you’re having a baby. But there’s a wide range of when exactly that baby might come. Very early, and you’re looking at a long stay in the NICU, and maybe more problems later on. Very late, and you have to be medically induced for the health of both baby and mother, which is correlated with protracted labor.
Everyone agrees that pre-32 weeks is really bad, pre-37 weeks is pretty bad, and post-42 weeks is dangerous. In this post, though, I’ll focus on the sweet spot: the 37-41 week range. If you have a baby in this range, you’re basically in good shape, and should be grateful. But are you in slightly better shape in some parts of the window than others? Let’s find out.
(In case you were wondering, nothing in this blog post is medical advice.)
The Inner Bullseye
37-41 weeks may be the sweet spot, but 39-41 is sweeter. This fact is unambiguous and widely reported, though it only recently raised to the level of ironclad medical orthodoxy. This study from 2013 is a good example of the relevant research: basically, babies born a few weeks early have (some of) the same problems as babies born earlier still, only more subtle. For example:
Adverse outcomes experienced by the early term[1] babies included hypoglycemia (4.9 percent versus 2.5 percent of full-term babies), admission to the neonatal intensive care unit (8.8 percent versus 5.3 percent, the need for respiratory support (2.0 percent versus 1.1 percent), the need for intravenous fluids (7.5 percent versus 4.4 percent) intravenous antibiotics (2.6 percent versus 1.6 percent) and mechanical ventilation or intubation, which was required in .6 percent of early term babies versus .1 percent in full-term babies.
So to a first approximation, just hope for week 39 or later. Which is a shame, because the weeks after 37 are extra uncomfortable,[2] so expecting mothers have lots of kick-shaped reasons to feel conflicted.
Beyond this, we have to get speculative.
What’s In A Week?
When you’re trying to figure something out that really matters, I find a two pronged approach is best. On the one hand, you want to find high-quality research, and follow where it leads. But alas, high-quality research is hard to find, fraud and its lesser cousin p-hacking are everywhere, and often the best studies are in the future. So on the other hand, you want to develop a simple causal model, a story of your own that makes sense. If you have a simple causal model that points one direction, and some finicky studies that point the other, it’s hard to be sure what’s going on. But if they point the same direction, now you’re cooking.
We’ll get to a study in a second, but based on this post so far, a simple causal model of pregnancy duration should be obvious: you want more Dakka [LW · GW]. If 39 weeks is better than 38 weeks is better than 36 weeks is better than 32 weeks, the obvious guess is that 40 weeks is better still. So if the studies agree, you can be pretty confident.
Fortunately, they do.
Study Dive: Gestational age at birth, chronic conditions and school outcomes: a population-based data linkage study of children born in England
There are a few studies I could focus on, but the ones I’ve seen all point the same direction, and this one seems well designed.
First, intellectual attainment:
- At 37 weeks, 10.5% of babies later failed to meet a mathematics benchmark, versus 9.3% for week 38, 8.3% for week 39, 7.7% for week 40, and 7.6% or week 41.
- For a second, later benchmark, the numbers were 23.7% for week 37, 22.1% for week 38, 20.8% for week 39, 19.9% for week 40, and 20.0% for week 41.
- The percentage of children needing special education support is also included: this was 35.0% for week 37, 33.2% for week 38, 31.1% for week 39, 29.5% for week 40, and 29.0% for week 41.
Second, early-in-life chronic conditions:
- At week 39, 6.9% of babies had at least one recorded chronic condition by age two, versus 6.1% at week 40 and 5.8% for weeks 41-43. That last figure is surprising, since it’s lower than the week 40 figure despite weeks 42 and 43 generally being considered high risk.
- The trend is similar for babies with at least two recorded chronic conditions by the same age, with 0.7% at week 39, 0.6% at week 40, and 0.6% for weeks 41-43.
I’ll summarize this as: “outcomes obviously get better up to 40 weeks, then it’s very close or kind of ambiguous comparing 40 and 41”. My personal guess is that the 41st week continues to offer subtle benefits, but in practice these are sometimes outweighed by the risks.
What about other studies?
They generally agree.
This study of Danish babies shows the usual negative IQ effects for babies born before 32 weeks, but no major differences between siblings between weeks 39 and 40. To be more precise:
In a nested sub-cohort of full brothers with intelligence test scores, those born at 32-33, 28-31, and ≤27 gestational weeks showed a reduction in IQ points of 2.4 (95% confidence interval 1.1 to 3.6), 3.8 (2.3 to 5.3), and 4.2 (0.8 to 7.5), respectively, whereas children born at 34-39 gestational weeks showed a reduction in intelligence of <1 IQ point, compared with children born at 40 gestational weeks.
1 IQ point is a reassuring ceiling, but 1 is still more than 0, and indeed this graph from the study does suggest that those last few weeks still do (probably) have a modest benefit:
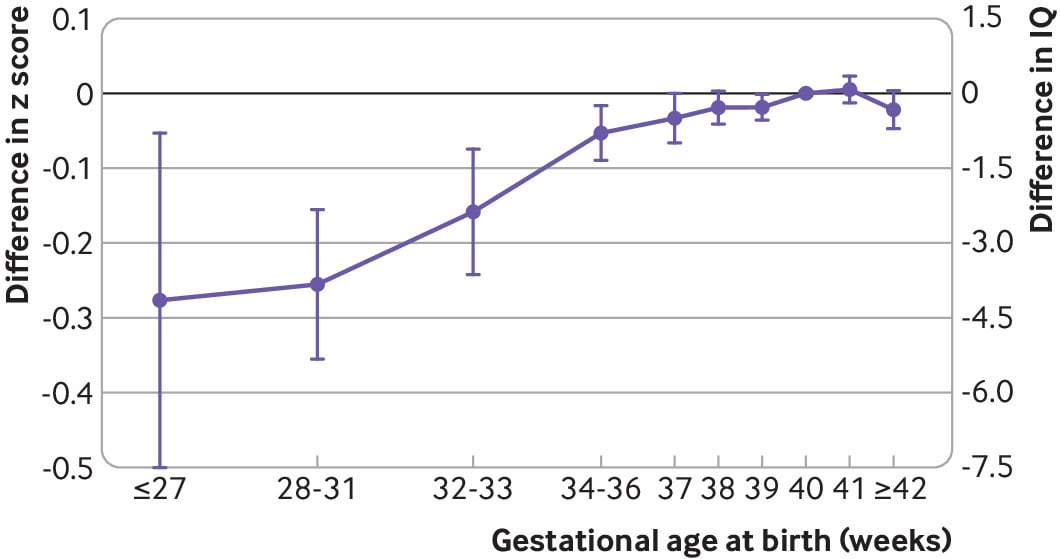
So I’ll say this study doesn’t contradict the British study (or our basic causal model), but does suggest a slightly weaker correlation.
This JAMA study is another point in favor, finding that “every week of gestation was significantly associated with increased IQ, but the strongest association was observed in the very preterm range, before 32 weeks gestation.”
Any Countervailing Evidence?
For 40 weeks being at least as good or better than 39, I’m not aware of any; most discussion I’ve found is arguing whether it’s “at least as good” or “better”.
Still, I’d be remiss not to mention this recent study out of China, which suggests that elective inductions at 39 weeks have better perinatal outcomes. But even they’re saying there are “complex tradeoffs” at play: in other words, the last week or two might offer benefits in the long run for the baby, but short-run birth complications can be serious for both mother and baby, and increase in severity post-term. They conclude:
Our findings indicate that elective induction of labor at 39 weeks’ gestation was significantly associated with lower risks for adverse short-term neonatal and maternal outcomes when compared with expectant management. Moreover, our study highlights the nuanced trade-offs in risks and benefits between elective induction at 39 weeks’ gestation and waiting for spontaneous labor or delayed induction at 40 or 41 weeks’ gestation, thus providing valuable insights for clinical decision-making in practice.
If I’m understanding correctly, you might induce at 39 weeks because you want to avoid the risk of having to induce at 41 or so weeks, though if you happen to have spontaneous labor at 40 weeks, great. Since this study was measuring perinatal outcomes specifically though, rather than long-run outcomes for the baby, I didn’t look at it as closely as the others and may be misunderstanding.
Why Does This Matter?
This is a great time for me to reiterate that none of this post is medical advice. That being said, there are applications to the question beyond “things to bite your nails about during pregnancy”. Specifically, OBGYNs may offer various induction options near a baby’s due date. For example, some will offer a membrane sweep around week 39: basically, they reach in there and mess around,[3] and your odds of spontaneous labor increase. And some women know in advance they’ll definitely need a c-section, and have leeway for when to schedule it.
Finally, in case any nervous expecting parents are reading this, first of all, I see you. It can be pretty tough, dealing with so much uncertainty about something so important! But I want to reiterate something from near the beginning of the post: anywhere after week 37, it makes sense to overall be grateful (and plenty of babies do great before then, too). Even if these studies all replicate perfectly, the IQ difference between weeks 39 and 40 is probably less than 1 point.[4] It might be decision-relevant in some edge cases (for the third time, not medical advice), but you shouldn’t let it keep you up at night.
For my part, we’re in the 40th week as of tomorrow. Wish us luck!
I write many more posts on Substack than I crosspost to LessWrong; if you want to read more posts like this, consider subscribing.
- ^
“Early term” is the technical - ahem - term for babies born between weeks 37-38, while “full term” is babies born between weeks 39-41. 42+ is called “post term”, though often induction is used to keep things from getting to that point.
- ^
Source: my wife. Also almost anyone who’s been pregnant who you ask about it, after a dark cloud crosses their face.
- ^
It’s as painful as it sounds, per Reddit.
- ^
IQ is often a good proxy for other health stuff, especially among younger children, so you don’t have to be obsessed with standardized test performance for this to move you.
4 comments
Comments sorted by top scores.
comment by johnswentworth · 2024-10-21T03:17:33.129Z · LW(p) · GW(p)
Huh. Sounds like longer gestation is straightforwardly pretty good for the baby, but is then counterbalanced by difficult birth if it gets too big, which would mean the baby-in-a-bag thing could actually yield some substantial benefits over a normal pregnancy. Like, you could maybe leave the baby in there a few extra weeks and it would be great.
Replies from: JustisMills↑ comment by JustisMills · 2024-10-21T23:48:43.042Z · LW(p) · GW(p)
Yeah, probably. There are a few things like "meconium aspiration" that would make a literal 1:1 womb substitute insufficient to give the baby a few more weeks, and for all we know some of the 42-43 issues are direct harms of marginal gestation. But I'd be rather surprised (<10% chance) if the optimal gestation-in-artificial-womb duration were less than 41 weeks.
comment by rotatingpaguro · 2024-10-21T16:19:54.056Z · LW(p) · GW(p)
Not sure if I missed something because I read quickly, but: all these are purely correlational studies, without causal inference, right?
Replies from: JustisMills↑ comment by JustisMills · 2024-10-21T23:47:29.016Z · LW(p) · GW(p)
They're correlational, though the broad cohorts help - not sure what you can do beyond just canvassing an entire birth cohort and noticing differences. There are possible pitfalls like the decision to induct early being made by people with genes that predict bad outcomes? But I really don't think that's major.