Covid 5/19/22: The Law of Five
post by Zvi · 2022-05-19T12:20:06.271Z · LW · GW · 2 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Physical World Modeling The participants who received the 50-µg dose had a 2.20-fold increase in their neutralizing antibody titers against Omicron after 28 days. Six months later, the participants still had 2.15 times the antibodies acquired with the original Moderna booster. Boost Your Children Well Prevention and Prevention Prevention Prevention The Bob Wachter Chronicles: Paxlovid Postscript The New Normal In Other News Ministry of Truth Proves False None 2 comments
If you’re five, you now get a booster. If you’re four, you still get no vaccine at all (while we ‘wait for more data’) and you’re often forced to take precautions that might make sense for senior citizens.
Because no one cares. And that truly continues to be the overall message. No one cares about the physical prevention or mitigation of Covid. Congress allocates zero dollars, doctors don’t prescribe Paxlovid and life mostly continues as normal because Omicron in a mostly-already-infected-and/or-vaccinated population simply isn’t that dangerous. Cases go up, but life goes on.
It’s pretty terrible that we’re not funding pandemic prevention or anything for the current pandemic, but at this point I don’t know that the most likely alternatives are even improvements.
(And of course, if you’re under one, thanks in large part to the FDA you may have also have a problem getting food.)
Florida did not report this week. I am retroactively smoothing out Florida’s numbers by giving 50% of its reporting weeks to its no-reporting weeks, now that this has happened three times in a six-week period. All future numbers and predictions will include this adjustment (assuming I remember to do it) and I will assume up front that when Florida reports we take 50% off the top. If I find time I’ll do a smarter adjustment, since this one is slightly flawed, but it’s much better than doing nothing.
Executive Summary
- Cases up.
- Boosters available for ages 5-11.
- No one cares and deaths are not rising yet.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 640,000 cases (+23%) and 2,100 deaths (+1%)
Results: 600,742 cases (+23% after adjusting Florida for both weeks, would have been +15% without the adjustment) and 2,004 deaths (+2% after Florida adjustment, -3% without the adjustment).
Prediction for next week:
Deaths
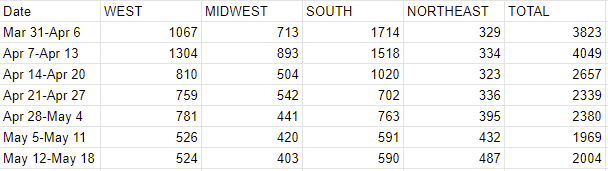
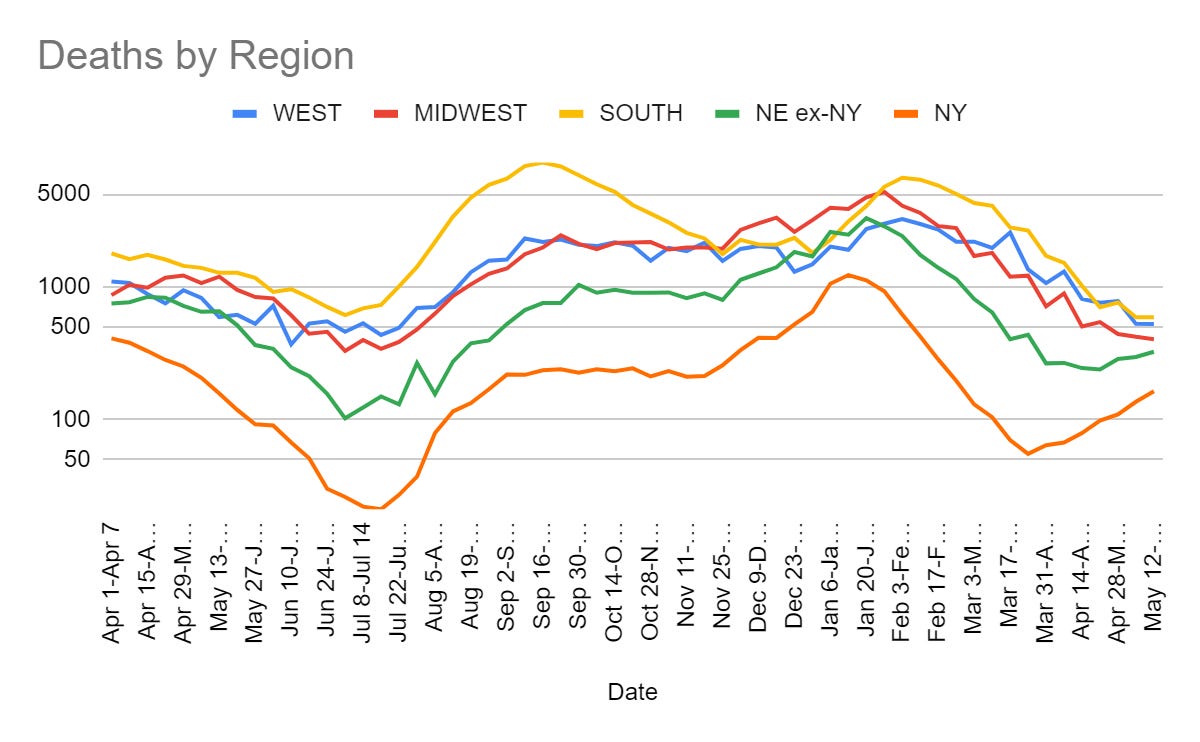
Deaths are rising in the Northeast and flat elsewhere, despite it being more than three weeks since cases began rising again. It seems clear that case fatality rates in this wave are going to be lower. It’s not great that thousands of Americans with Covid are dying each week, some of them from Covid as well. I wish it were not so, but I am glad we are not ruining our lives trying to stop this.
Cases
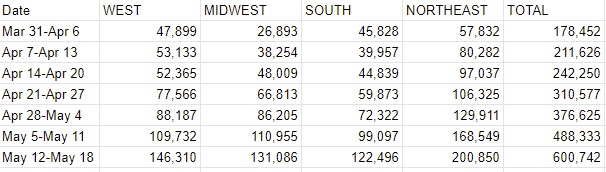
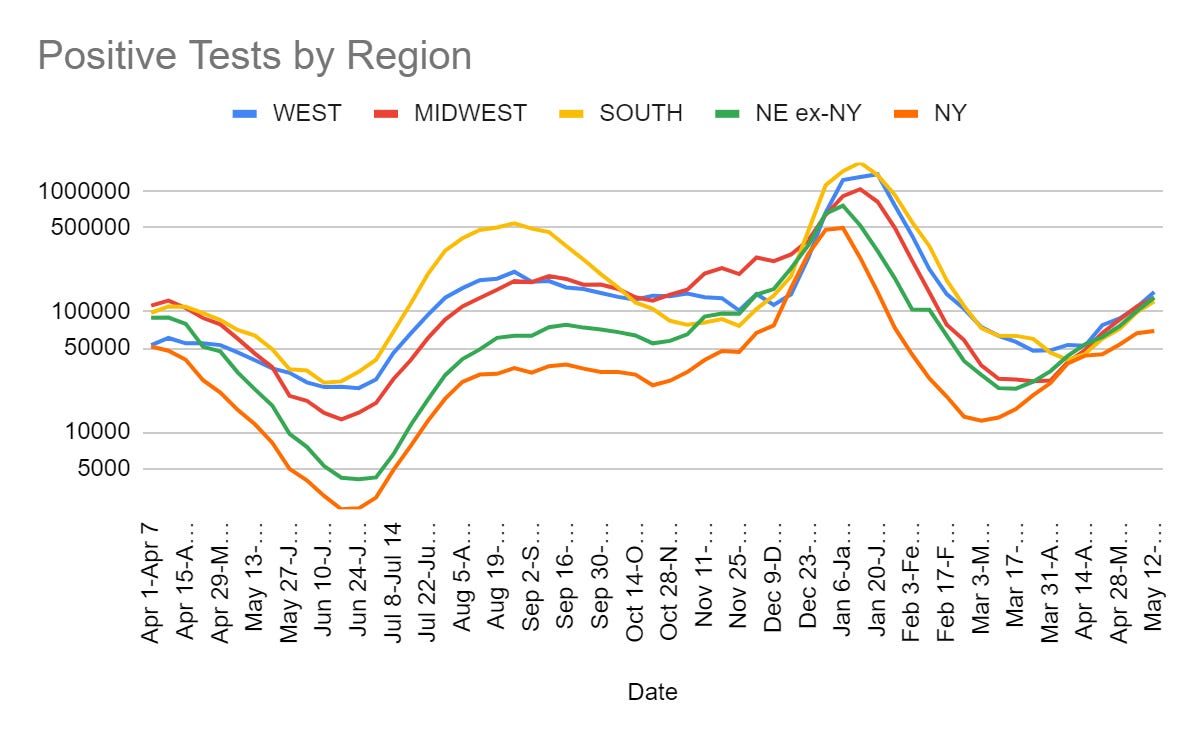
Enough weeks in a row with 20% weekly case growth and things get out of hand. We’re now triple our low point and back at a point similar to where we’ve been for most of the past year. I expect case growth to peak well before we get back to where things were in January, and even if we did get those case numbers back I expect less death to result from it, but certainly this is not where I hoped or expected to be in May.
The rise of BA.2.1.12 (and BA.4 and BA.5) are something I wasn’t predicting would happen, or at least would not happen so fast. Variants are inevitable, but this was unexpectedly quick, and Topol’s note below that this implies more future variants is well taken.
Is the pandemic over? In terms of cases, we have a clear no. In terms of deaths and people’s reactions, that remains to be seen. I still consider my pandemic over.
Physical World Modeling
Eric Topol describes our current approach as The Covid Capitulation. That name seems apt, for both good aspects and bad. The first half of the post is about how B.2.1.12 and B.4/5 bring both the new mutations and doom.
To recap, we have a highly unfavorable picture of: (1) accelerated evolution of the virus; (2) increased immune escape of new variants; (2) progressively higher transmissibility and infectiousness; (4) substantially less protection from transmission by vaccines and boosters; (5) some reduction on vaccine/booster protection against hospitalization and death; (6) high vulnerability from infection-acquired immunity only; and (7) likelihood of more noxious new variants in the months ahead
This is repeating ‘the virus mutates a lot’ over and over. It’s worth repeating, as it is central to modeling what will happen in the future. As one would expect, static vaccines and existing immunity decline in effectiveness as we accumulate mutations, and immunity from both infection and vaccination are now established as fading at least somewhat over time especially for purposes of initial infection.
The flip side of this is that there have been a massive number of infections, and there will continue to be a lot of them, without many deaths. This creates a cycle where immunity is renewed was time passes and variants give way to new variants and subvariants.
This graph is worth copying over, showing a clear decline in vaccine effectiveness and booster effectiveness. It is still showing vaccine and booster effectiveness, and all the usual biases in the samples continue to apply, but the ratios are no longer anything like as dramatic as they used to be.
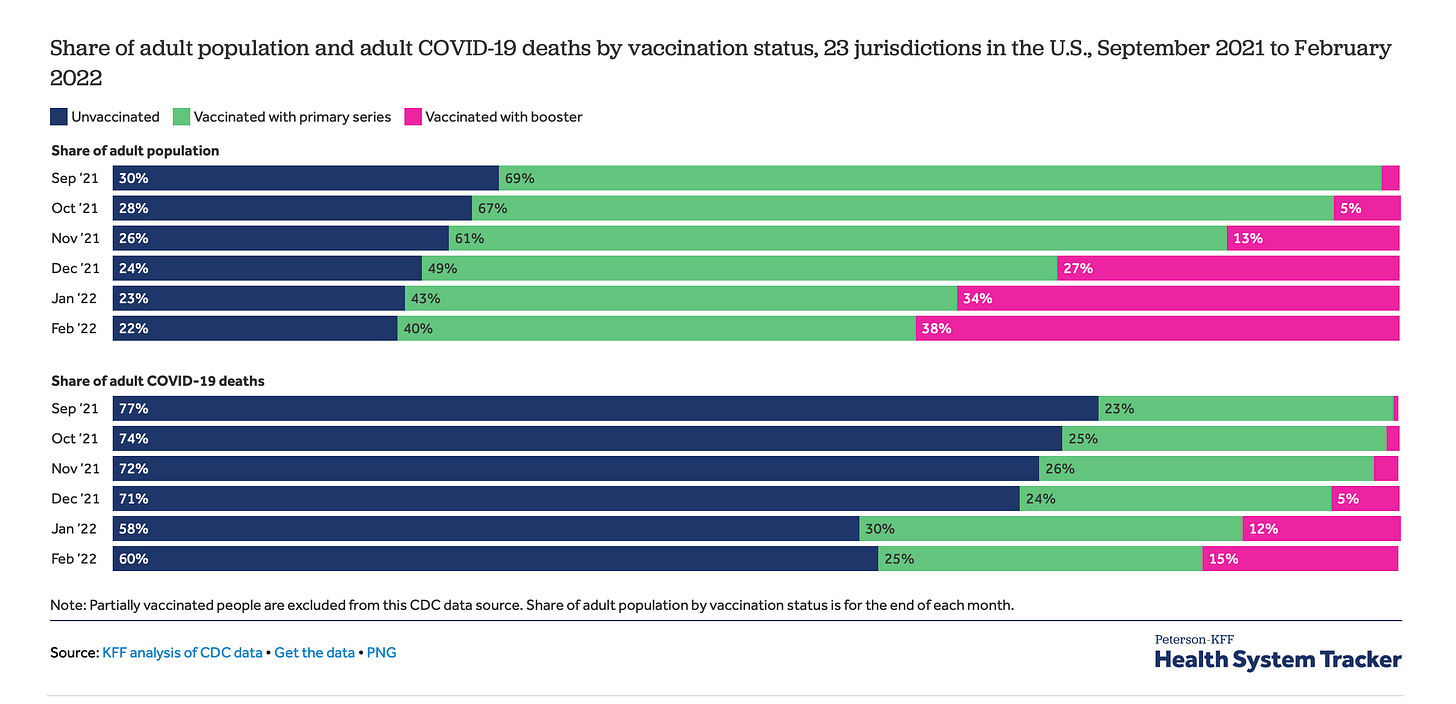
One reason for this is that previously almost all infections were first-time infections. Now many of them, perhaps a majority, are re-infections – by the math, they have to be, there have been roughly as many infections as we have people. A lot more of the unvaccinated group is going to have been previously infected, and especially been previously infected multiple times, and those infections will ‘buy more protection’ for them than they will for the vaccinated group. So this results in less of an advantage for the vaccinated even if underlying effects of vaccination hadn’t changed, and this is doubtless an important part of the story.
Topol comes out in favor of a policy of Zero Covid Deaths, as opposed to Zero Covid. The problem is that they’re the same policy. You can’t have a virus running around infecting lots of people and killing zero of them, no matter how good your vaccines and treatments. That’s not how the physical world works. So such slogans are always calls to Do More. But the core idea of shifting to mitigation of the death rate is clearly correct at this point.
The second half of the post is called A Delusional Congress and is about congress deciding to fund exactly nothing towards either the current pandemic situation, work to prepare for future variants, or future pandemic prevention.
In the opposite of news, I strongly agree with this central call.
We’re not just looking at running out of vaccines and antiviral medications. Congress should immediately allocate for an Operation Warp Speed (OWS)-like initiative to bring nasal vaccines over the goal line. Three of these are in late stage clinical trials and success of any would markedly ameliorate our problems of transmission, no less the alluring aspect of achieving mucosal immunity and being variant-proof. That brings us to catalyzing the efforts for a pan-β-coronavirus vaccine, previously reviewed, now that we have discovered tens of broad neutralizing antibodies but have limited traction of these in the form of advanced clinical trials.
What I disagree with is Topol’s characterization of why congress is failing us. Congress isn’t unusually delusional. They know that ‘what they are doing is wrong’ in the relevant sense. They just don’t… care. Not enough to act.
Did you know that the new version of the Moderna vaccine is more effective?
The booster candidate, mRNA 1273.211, was tested n 895 people against the currently approved mRNA 1273 booster. Some participants received a 50 micrograms (µg) dose, the same amount of viral RNA as the current boosters. Some received a 100 µg dose.
The participants who received the 50-µg dose had a 2.20-fold increase in their neutralizing antibody titers against Omicron after 28 days. Six months later, the participants still had 2.15 times the antibodies acquired with the original Moderna booster.
That’s not that great. Doubling your antibodies is a lot less than doubled effectiveness, as all of this needs to be thought about on a log scale. It’s still something we should be willing to spend a little money on to ensure it happens quickly and also at all.
The battle against Paxlovid continues. The most effective weapon is pure ignorance, followed closely by a race between confusion and an obsession with conserving supply and whether someone ‘needs’ it, since Covid isn’t all that dangerous for most people, you see. On the drug interaction front, Mina points us to good resources. Drug interactions are a worry, but they’re still relatively rare, applying to 2 of the 100 most prescribed drugs. The vast majority of people won’t have an issue.
Boost Your Children Well
If you are five years old, you can now get a Covid booster. Washington Post coverage is here.


If you are four years old, you can’t get the vaccine at all, often with maddening social consequences.
I do not notice that any particular urgency to get my eight year old son a booster.
Also, I continue to be impressed with the flexible definitions of the word ‘emergency.’
The FDA also announced plans to meet June 7 with its advisers to talk about an emergency authorization request for a coronavirus vaccine made by Novavax for people 18 and older.
Novavax submitted an application for emergency use authorization in late January.
It would be good to approve Novavax on principle. In practice I doubt anything changes. It’s great to know your emergency application will be handled only five months later.
There’s also this:
In addition, the FDA said it will convene an advisory committee meeting June 28 to discuss whether the composition of coronavirus vaccines should be modified for use in a potential vaccination campaign this fall.
Many experts say vaccines for the general population should be reformulated to keep up with the changing virus, but the question of whether, when and how remains unresolved.
So over a month from now they will convene to discuss whether to reformulate vaccines going forward. Presumably, this allows the FDA to say that there’s no hurry because congress isn’t funding further vaccinations, and the congress to say there’s no hurry because the FDA hasn’t approved updating the virus.
I remember when we said mRNA vaccines could be modified in a week.
I also remember when we designed them in a day.
But the CDC is worried. They’re worried that if we have an effective vaccine program, it might give the impression we don’t have an effective vaccine program?
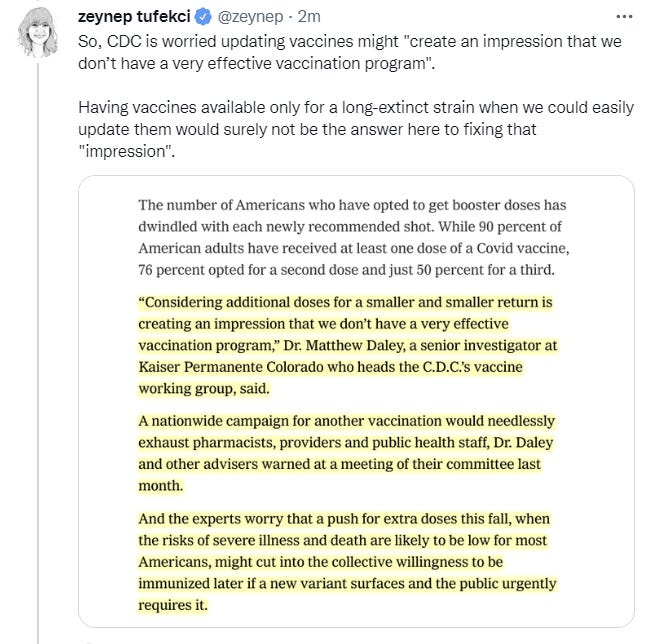
If I wanted to give people the impression I had an effective vaccine program and that vaccination was important, I would act like vaccination was important and do my best to have an effective vaccine program.
Every single time the Very Serious People sabotage our pandemic response in the name of ‘impressions’ people correctly get the impression that we are sabotaging our pandemic response. It backfires. Every. Single. Damn. Time.
That doesn’t mean you want to do a big push to tell everyone an additional booster is super important. The argument for ‘saving your powder’ on that front makes sense.
Prevention and Prevention Prevention Prevention
More free Covid tests are available. The last of our Covid money is being spent on this.
Covid-related entry requirements have been waived by many European countries, do nothing, waste a lot of time and money, are dumb, and we should scrap them.
New York City issues new mask advisory.
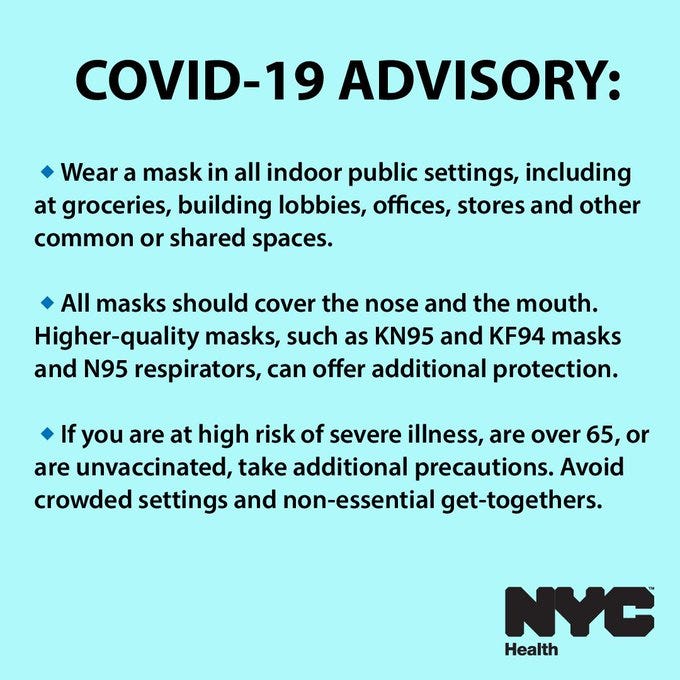
This continues to be brutal on young children, who are at almost zero risk yet are told to ‘avoid non-essential get-togethers’ also known as childhood, because they are not eligible for vaccination. My son still has to wear a mask each day. There’s also the continued baseline assumption of cloth masks rather than N95s, and no mention of masks better than N95s.
FDA Delenda Est has rejected the emergency use application for Fluvoxamine. They did so by looking around until they found a set of endpoints that had insufficiently strong results, and deciding those were the ones they cared about.
I didn’t expect better on Fluvoxamine, because all signs point to no one caring about Covid. It’s not enough of an emergency to let me (yet) vaccinate my kid, so why should I expect this decision to go any differently? Plus the FDA thinks that effects that aren’t sufficiently dramatic should be illegal – a ~35% reduction in severe disease seems a lot to them like a 65% chance of them getting blamed, and a lot of confusion they don’t want to deal with. Much better, they think, if we all pretend the whole thing has gone away.
What both these decisions have in common is that those who know better can ignore them. Fluvoxamine is already approved for psychiatric use, so you can still get a prescription if you care enough and work the system. An advisory is a rule you don’t have to follow. The real damage is from rules you have to follow.
The Bob Wachter Chronicles: Paxlovid Postscript
Last week Bob’s wife got Covid and had to decide what to do about it. This week, she took Paxlovid and she’s feeling better, but worrying about the situation is far from over. Another thread into the mind of the well-meaning, well-informed and overthinking Covid concerned – if you’re not here for it, skip ahead to the next section.
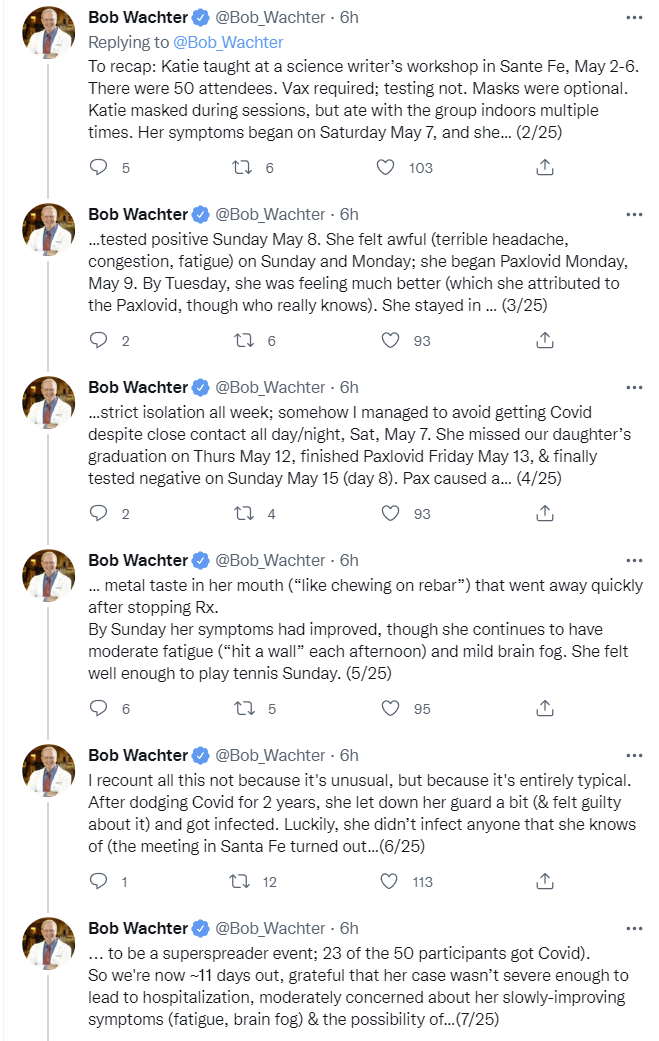
The Long Covid paranoia always makes my heart sink. In this case, it’s concern after getting Covid rather than before, so it will stress everyone involved out but at least won’t prevent them from living life. This was a (mild) symptomatic case so there’s certainly a non-zero chance.
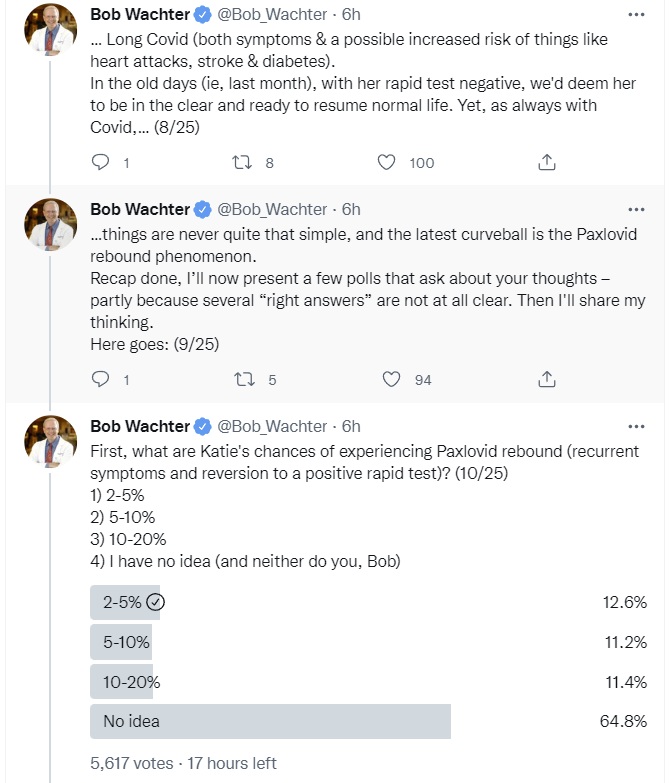
Then there’s the concern about Paxlovid rebound. This is the New Hotness concern. I see a decent number of tweets that have one particular case of it and say ‘not rare.’ That is… not how statistics works. There is some motivation for people to play this up, as part of the general motivation among health professionals to play down Paxlovid.
It’s worth noticing that the survey results above both don’t allow for answers below 2% despite 2% being the rate at which the effect has previously been reported, and also looks exactly like it would if people had actual no idea what the answer was.
What’s Bob’s answer?

Excuse me while I bang my head against the wall.
There’s the whole ‘we don’t know for sure so we have no idea’ thing but also:
A similar percentage was seen in the placebo group.
Technically it was 2% in the treatment group, 1.5% in the placebo group.
You know what this suggests? That we should be skeptical that most of the rebounds we observe have anything to do with Paxlovid. Yes, we have a reasonably good ‘just so’ story about them such that it makes sense that they happen. But what Bob is reporting is that the rebound effect was not associated with Paxlovid in the trial, at all. One could reasonably thus say both that Paxlovid is unlikely to cause that many rebounds, and that if you want to take this seriously than you should be worried about ‘rebounds’ in all Covid cases even without Paxlovid. Which we are totally not.
The good rebuttal to this that I have seen is that Omicron gives you symptoms faster, so Paxlovid is getting prescribed earlier, so we end up giving out Paxlovid ‘too quickly’ and thus rebounds are happening more often. That might even be an argument that you want to wait to take Paxlovid if you think you caught your case super quickly. In this case, Bob’s wife didn’t get started for about two days after detection, which means this likely isn’t a concern.
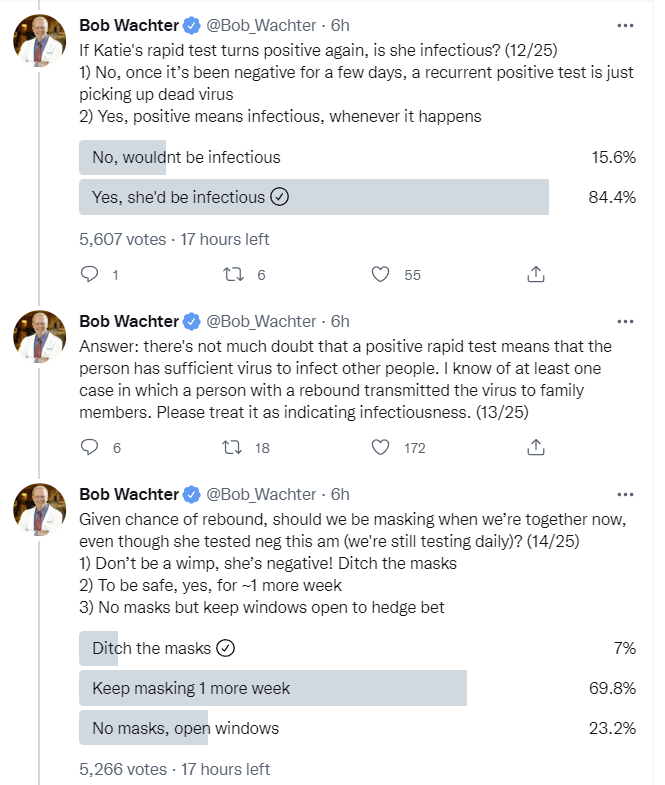
Bob’s right on the question in #12 here. If your test comes back positive, that implies you’re infectious and you should act accordingly.
However, in the question in#14, we’re not talking about what Bob should do if his wife tests positive again. We’re talking about what he should do given his wife is still testing negative, except that she previously got Covid, took Paxlovid on the 8th and tested negative three days ago. There’s no sign of a rebound case, and without a rebound she’s in the clear.
(Also note, they did a nine hour car ride together when she was definitely positive, using only N95s, but consistency is mostly not a reasonable ask.)
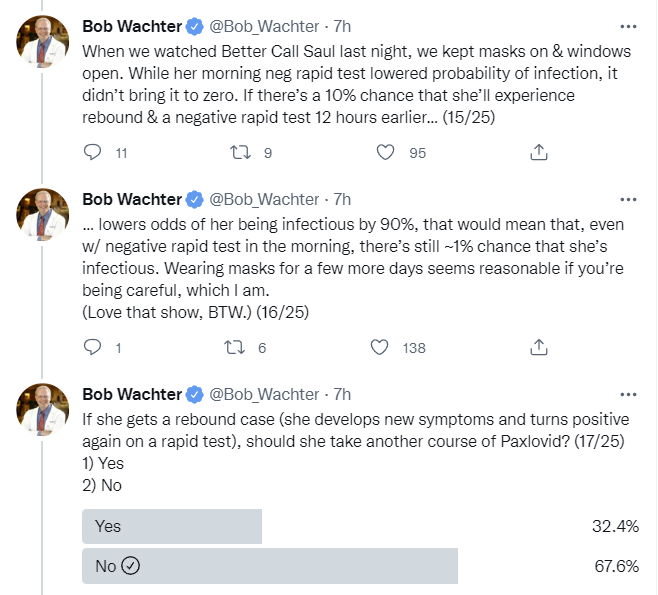
If our only prior is ‘got Covid and then took Paxlovid’ we could reasonably put his wife at a few percent to have a mild rebound case at some point, which might or might not make her infectious at this point, and which is reduced by all the days of negative testing so far. It’s also reduced by the details of her case. She had several days of symptoms, which makes the physical logic of a rebound seem much less likely. Thus I voted for option one, but I certainly won’t blame anyone who wants to open a window.
As you’d expect Bob chose to wear masks for an additional week. My guess is that given his emotional reaction in all scenarios, it was the right choice for him. If you’re ‘being careful’ this is part of the storytelling package of being careful.
(As a side note, everyone tells me Better Call Saul is terrific, and objectively that seems very right, but I noticed I wasn’t enjoying watching it so I stopped after a few episodes. I presume I should eventually push through that.)
My answer to the question of another round is no, because from what I know the rebound cases aren’t as serious, so there’s no need.
I consider the ‘not an FDA approved use’ justification here to be rather content-free. Yes, of course there haven’t been enough rebound cases for us to know if the second course is wise here, but we should be able to use our physical world models to figure that problem out.
On the last question, 3% is basically Lizardman Constant, so it doesn’t worry me. The 19% part does, yet it also raises a valid point. If using Paxlovid means several weeks of living as if you are positive, that’s a non-trivial downside. If that’s how you’re going to react, the calculus does not look as good. It still looks pretty great, though, if you’re in a medium-risk or high-risk group.
Here’s a link to that post. Her takeaway seems to be that yes we are seeing a lot of anecdotes, but that’s not inconsistent with a 2% rebound rate, and we have to wait for better data which will be hard to get.
The New Normal
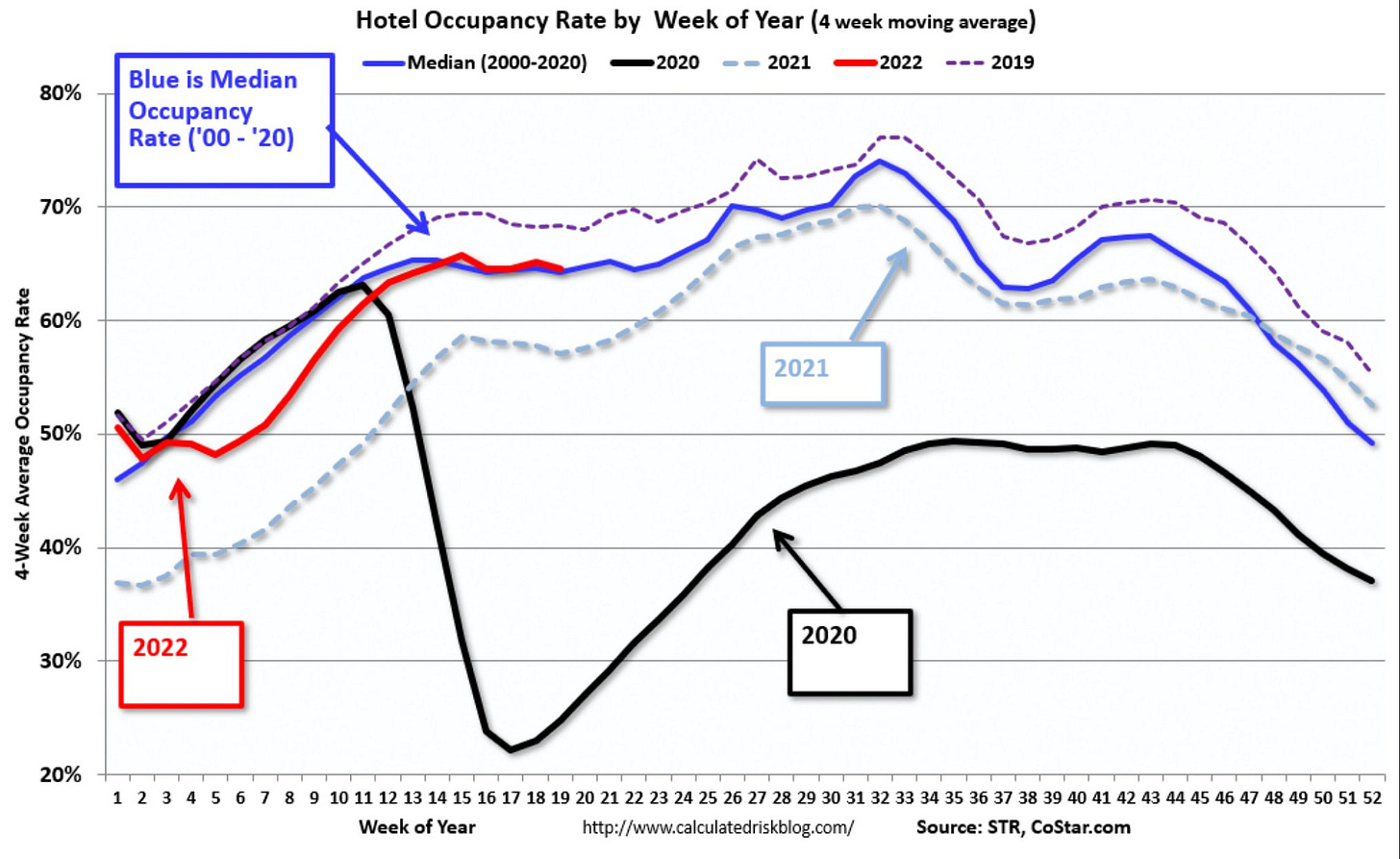
Hotel occupancy is back to pre-pandemic levels, but NYC subways very much are not.
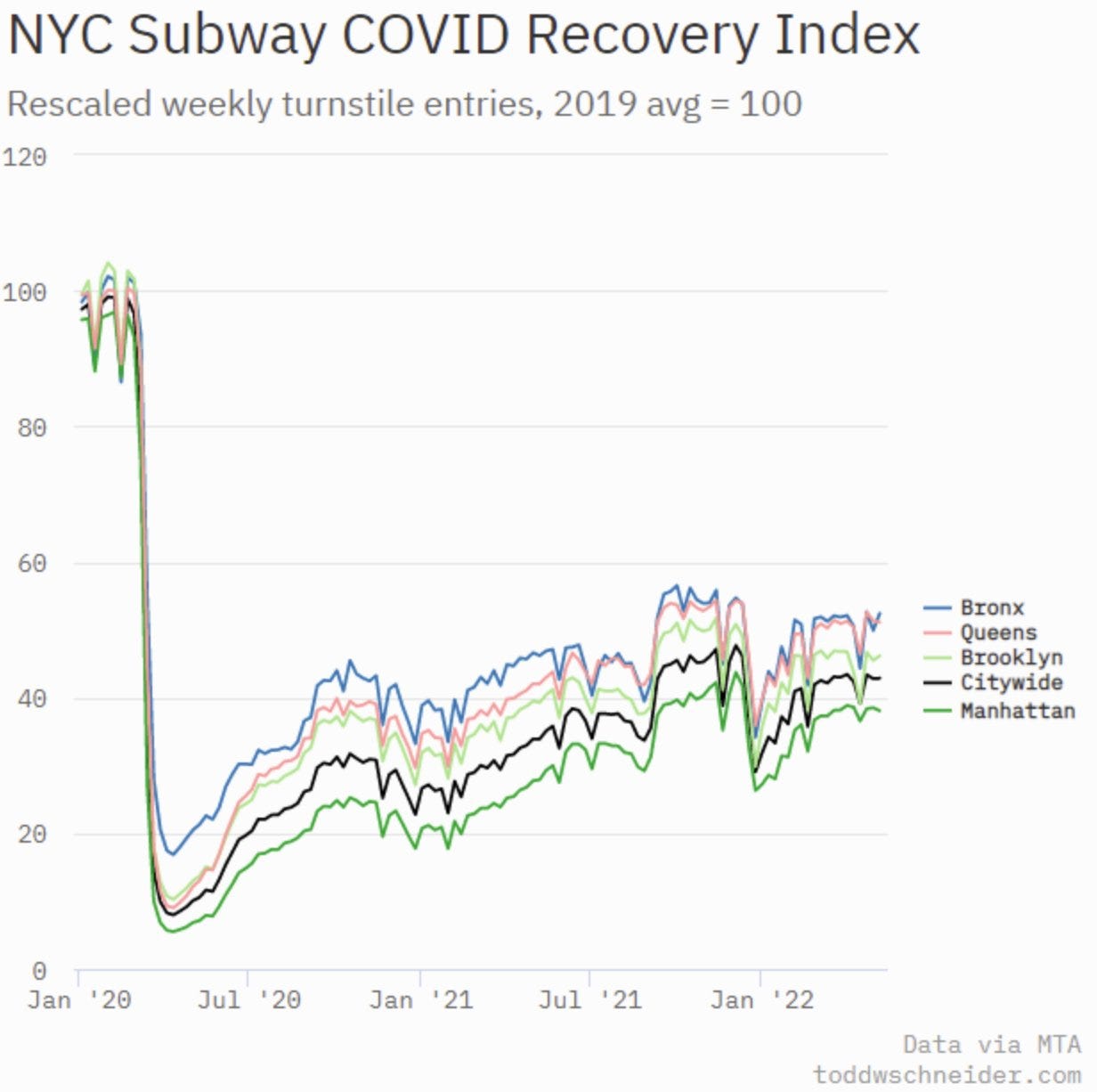
About half of subway ridership has vanished and so far it isn’t coming back. I buy that this is a shift towards massively more working from home and that the bulk of this change likely never reverses.
Whereas hotels represent activity that isn’t going away. Although there’s another explanation here, which is: Hotels, man. Capacity can be down, as can prices and profitability, and occupancy being at equilibrium may not mean much.
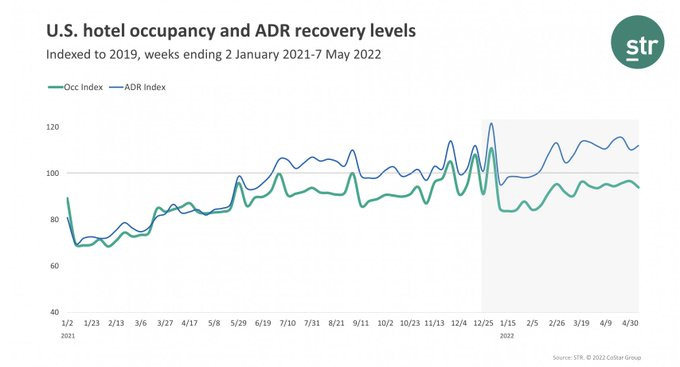

I asked someone who knows the business and he said inventory is down generally, so this is a ‘new normal’ of sorts but does not represent anything like a full rebound. But at the new supply levels prices look more like they used to look, whereas when I visited New York during the pandemic hotels were remarkably cheap.
In Other News
Well-earned congratulations are in order: Zeynep Tufekci accepts position at Columbia University as inaugural director of Center for Ethics and Security in Journalism. Turns out it was always about ethics in journalism.
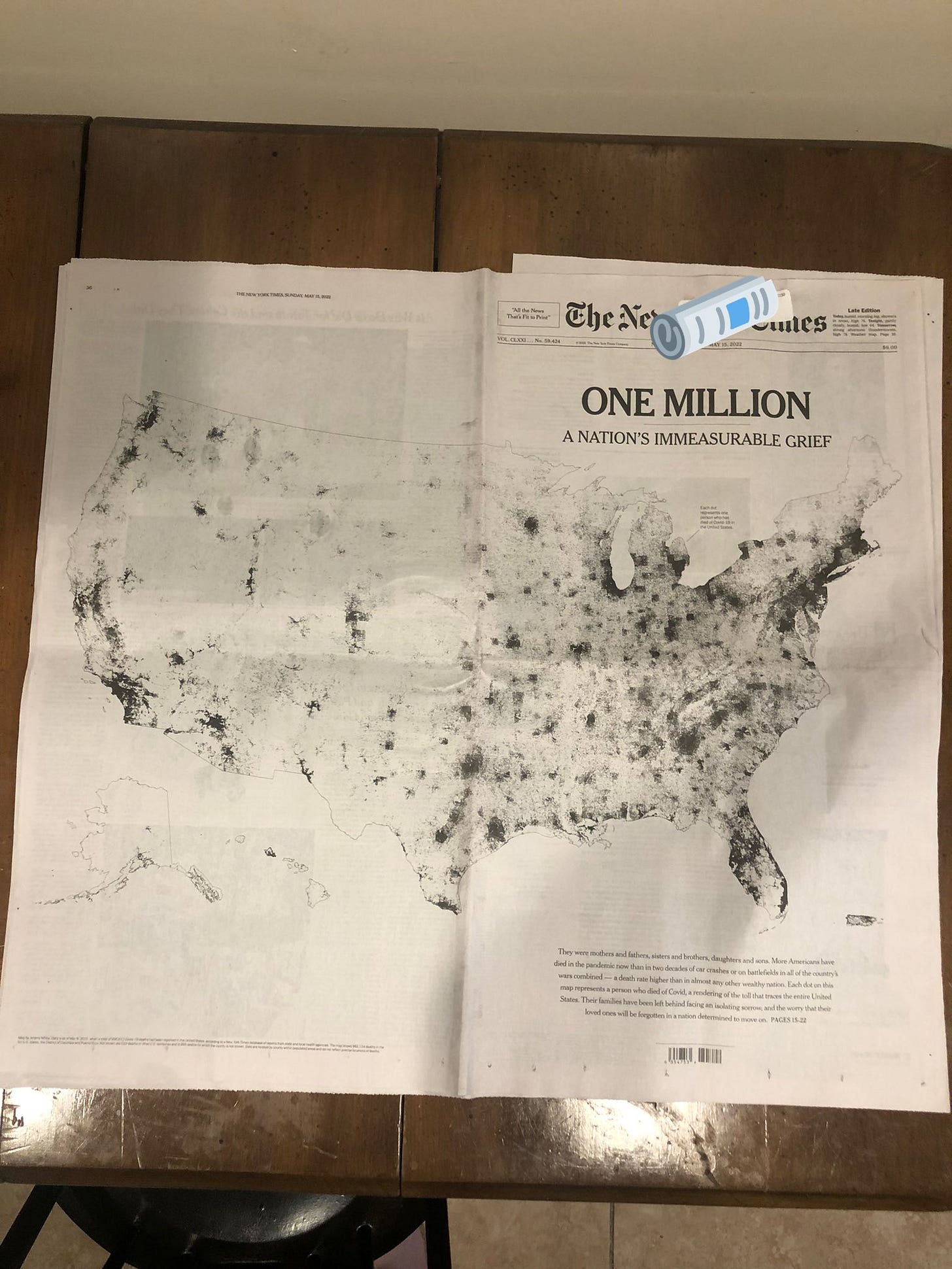
New York Times publishes helpful front page population density map of America.
Meat packing plants may have been a remarkably large share of early Covid infections.
Marriage rates declined 16% in 2020. I was very surprised that this effect was so small.
Ministry of Truth Proves False
Ministry of Truth closes its doors in wake of the sharing of information about the Ministry of Truth, the idea of creating a Ministry of Truth and its new would-be leader who has a history of calling for censorship of any speech she doesn’t like. The framing by the Washington Post was that this was an attack by exactly the kind of misinformation the board was to be deployed against.
Which tells you exactly what kind of misinformation the Ministry of Truth was designed to censor.
That the would be 33-year-old leader who has gone around calling for censorship is called a ‘well-respected expert’ in the field of misinformation tells you what it means to be a ‘well-respected expert’ these days.
Pirate Wires has more details and less generosity to offer, if that’s relevant to your interests.
I would like to better understand the mechanisms whereby this backlash resulted in the board shutting down. None of the reactions seem like they should have been unexpected, or like they should have any unexpected impacts. I notice I am (pleasantly) confused that they worked.
2 comments
Comments sorted by top scores.
comment by Daniel V · 2022-05-19T16:26:07.310Z · LW(p) · GW(p)
On fluvoxamine, the FDA's report includes additional analyses that even go beyond what I talked about regarding the NIH's [LW(p) · GW(p)]. Though I will say their discussion of the meta-analysis seemed a little disingenuous (though some comments in peer review can feel the same, so) - garbage in, garbage out is always a potential problem, and one should never hope for a meta-analysis to "substantially alter the assessment of the individual trials," so failing to deliver on that is just par for the course and should not be viewed as a negative.
But even just taking the meta-analysis at face value, the summarized evidence of efficacy is kinda weak (a reduction in severe disease that is consistent with reductions ranging from 0-50%...consistent with 0% means "While the FDA has concluded that the existing clinical data are insufficient to support the issuance of an EUA, these data suggest that further clinical investigation may be warranted." At least it's not consistent with, say, -10%-40%, in which case the FDA would presumably not have thrown that bone).