When to Get the Booster?
post by jefftk (jkaufman) · 2023-10-03T21:00:12.813Z · LW · GW · 15 commentsContents
15 comments
Let's say you're planning on getting a covid booster this fall: when's the best time to get it? The updated boosters ( targeting the XBB lineage) have been out since mid September, so there's not a new vaccine to wait for. Instead, I see the choice as balancing two considerations:
If you get it too soon it might have worn off too much by the time you most need it.
But if you're too late you might get infected in the meantime.
As a first approximation, you probably want to have the strongest protection when local levels be at their highest. When would that be? Wastewater monitoring is pretty good for this sort of thing because it's not dependent on people getting tested. Here's what I see on Biobot:
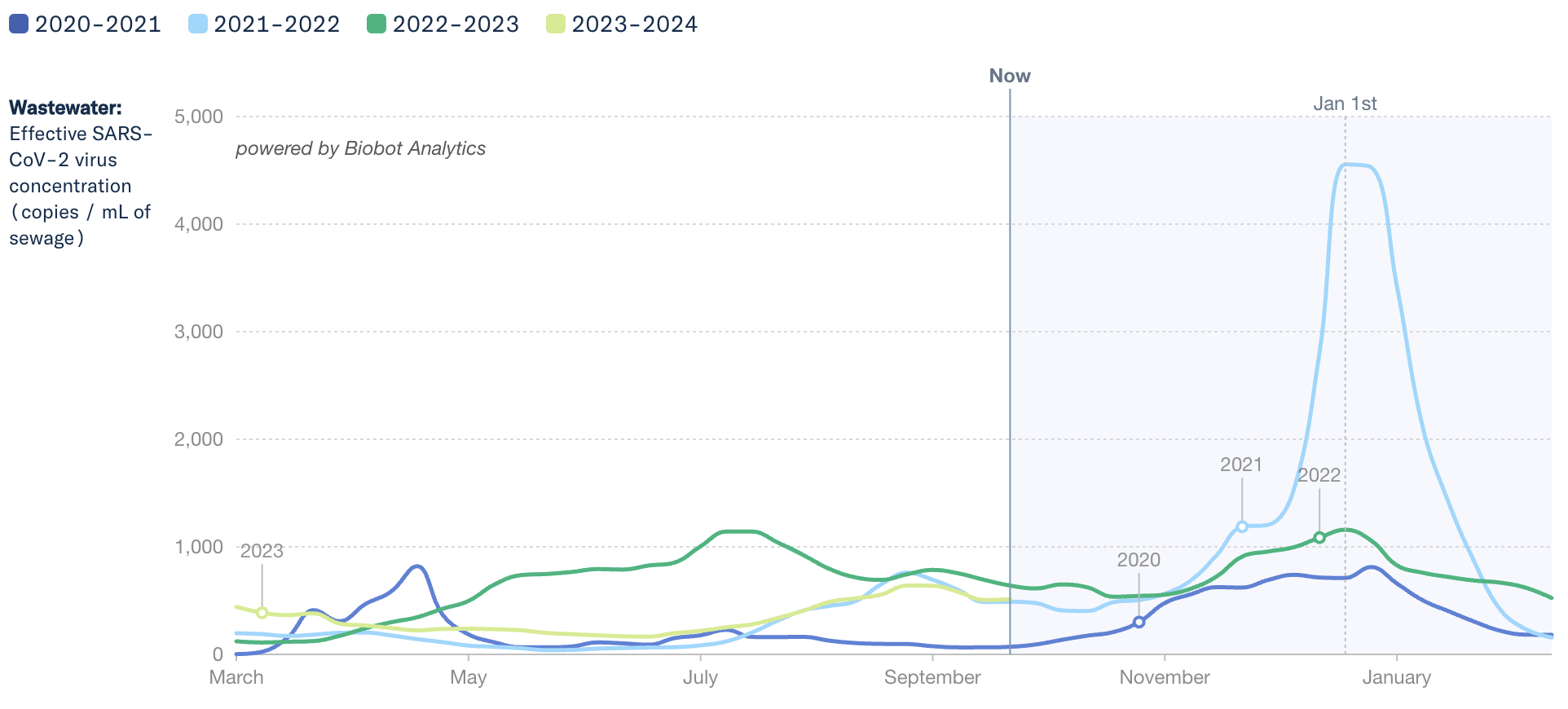
It looks like 2020-2021 and 2021-2022 were strongly concentrated around New Years, and 2022-2023 less so. On the other hand, 2023-2024 so far is following a trend very close to 2021-2022, so perhaps it will be up for the holidays again?
The other key question here is how quickly the vaccine wears off. It looks like the most recent meta-analysis here is Menegale et. al 2023, which found effectiveness decreased quite rapidly against Omicron (and everything now is a kind of Omicron):
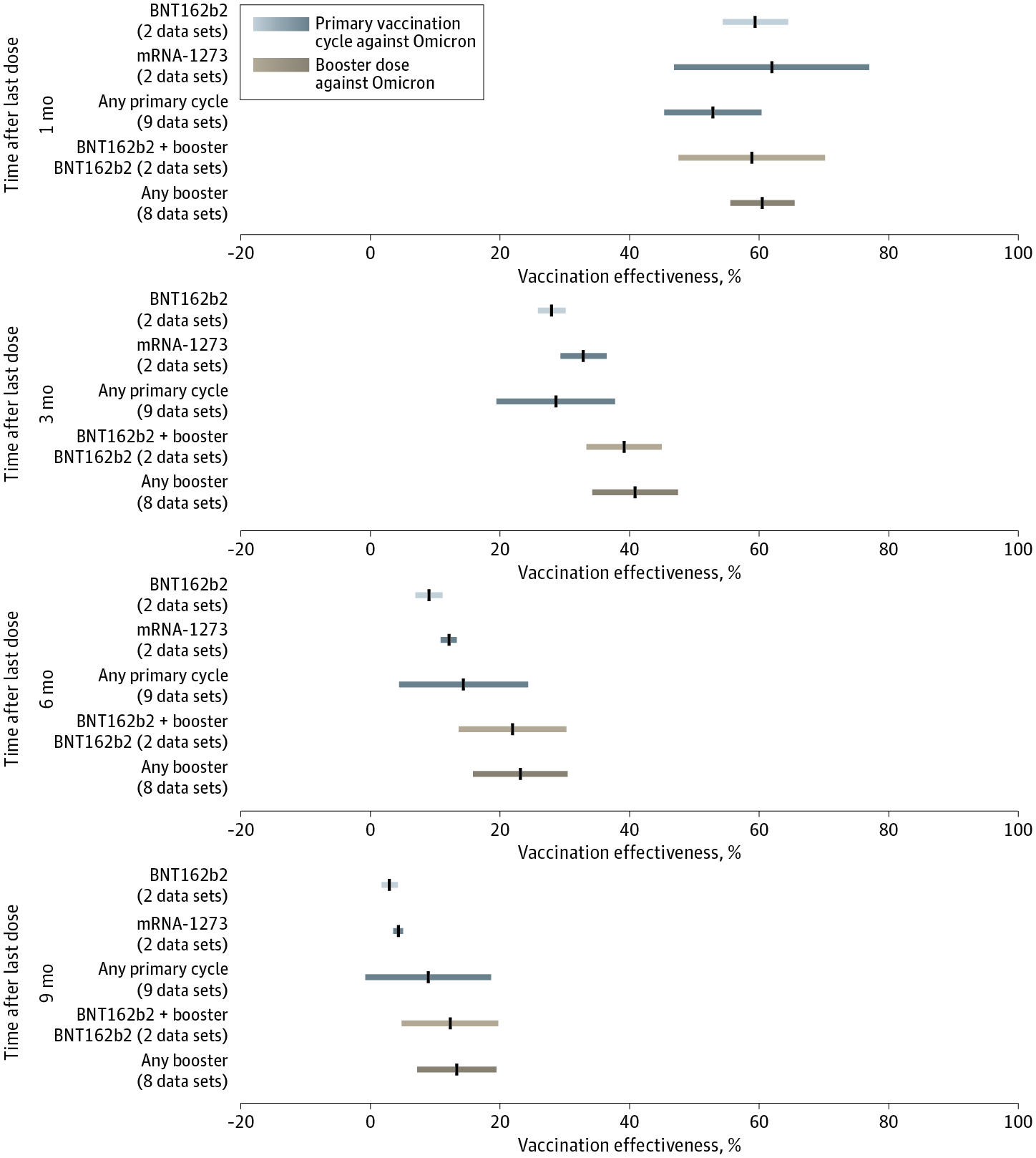
They estimated a half life of 111d [88-115d]. This means that if you got a shot on the first day they were made available this year (2023-09-12) you'd be down to 50% [42-51%] effectiveness at New Years. I wish the CDC would be more transparent about their reasoning so we could tell whether this was on purpose...
At this point I'd love to see a calculator that lets you put in when you last got a booster (or had covid) and then combined the half life data with the historical seasonality data to identify the covid-minimizing time to get a shot. It could even allow you to specify dates you want to not be sick for, or not get sick during, along with how important it is to you.
Unfortunately this calculator doesn't exist, so we'll have to eyeball it. I think most people would like to avoid infection around Thanksgiving and Christmas, historically high-infectious times that we especially don't want interrupted by covid and during which we're much more likely than usual to be getting together in large multigenerational groups. Getting a shot two weeks before Thanksgiving, 2023-11-09, would have you at most protected for Thanksgiving, and then still 82% [78-82%] of peak protection at Christmas. If more worried about infecting other people than getting infected yourself, such as if you're younger but visiting older people, subtract a week to model that you're trying to prevent infection in the week leading up and not during the holiday.
There are a lot of person-specific factors that could affect your decisions. For example, you might be about to travel to see an elderly relative or have an infant, in which case sooner is likely better. Or maybe you had covid recently or have something super important to you later in the season, in which case later could be better. In my case we're doing Thanksgiving early with my wife's family, leaving Boston 2023-11-09, so I'm thinking two weeks before that, less a week for being mostly worried about infecting other people, so around 2023-10-19.
Anything I'm missing?
(I do think it's worth most people getting the booster, even considered selfishly: I'd much rather suffer side effects at a time of my choosing than cancel holiday plans.)
Comment via: facebook, mastodon
15 comments
Comments sorted by top scores.
comment by Gordon Seidoh Worley (gworley) · 2023-10-04T01:17:03.429Z · LW(p) · GW(p)
For what it's worth, this matches my own plan, though arrived at more roughly. My thinking is flu and COVID vaccines seem to provide decent levels of immunity for about 6 months, the winter disease season ends roughly late March, it ramps up slowly at the start and there's some significant risk towards the end as immunity wanes, so mid October looks like the sweet spot for getting a booster to minimize risk through the season.
Replies from: florin-clapa↑ comment by Florin (florin-clapa) · 2023-10-04T19:23:15.829Z · LW(p) · GW(p)
You might want to consider adding additional protection measures (like a respirator), as the effectiveness of some vaccines can be moderate to non-existent. The effectiveness of the flu vaccine in years when its well-matched to the circulating strains is between 40% and 60%, and when the vaccine is not well-matched, it's protection against illness plummets, although it may still offer some protection against complications such as pneumonia. Vaccines don't exist for bad colds and the stomach flu.
comment by johnhalstead · 2023-10-04T18:30:35.937Z · LW(p) · GW(p)
Personally, I don't think it is worth getting the vaccine if you are under 40. According to this paper in the BMJ, for people aged 18-29, per covid hospitalisation prevented, an MRNA vaccine will cause at least 18.5 severe adverse events. A serious adverse event is: An adverse event that results in any of the following conditions: death, life threatening at the time of the event, inpatient hospitalisation or prolongation of existing hospitalisation; persistent or significant disability/ incapacity, a congenital anomaly/birth defect or a medically important event, based on medical judgement.
This decision also depends on what you think the risk of long covid is, but I personally think it is extremely low, as I discuss in the comments here [EA · GW].
It's worth noting that the JCVI in the UK, which I think has been one of the most sensible bureaus on vaccines doesn't offer the booster to people under the age of 65 unless they are in a high risk group or caring for someone in a high risk group.
Replies from: jkaufman, nathaniel-monson, Mark_↑ comment by jefftk (jkaufman) · 2023-10-04T19:54:58.046Z · LW(p) · GW(p)
I think this is assuming that someone under 40 would be considering getting the vaccine because they're concerned about getting hospitalized for covid, but that's very far down my list. Instead, the main things I want to prevent are (1) getting reasonably covid-cautious elderly relatives sick, where large family holiday gatherings are a decent portion of their annual risk and (2) having to cancel plans because I've contracted covid and am expected to isolate.
(Your comment also seems to conflate "under 40" and "under 30")
Replies from: johnhalstead↑ comment by johnhalstead · 2023-10-04T20:25:56.653Z · LW(p) · GW(p)
As mentioned in my other comment, unless the people you are visiting are hiding at home all the time, you are not going to have much effect on the chance they get covid over any six month period. you might just bring it forward a bit time. but if they are living a relatively normal life eg going to shops (as I think they should) then it's not going to make much difference since covid has been let rip in the US.
Re (1) I think you could do that with lateral flow testing rather than taking a vaccine that may be net harmful to your health. The false negative rate of a LFT is much lower than the protection against transmissible infection you would get at any point after having the vaccine.
I meant to say under 40. Given that the ratio of severe adverse events for 20s-30s is >18.5:1, I would also expect it to be bad to get the vaccine aged 30-40 given the extremely low health risks of getting covid in that age group.
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2023-10-05T01:00:50.141Z · LW(p) · GW(p)
> if they are living a relatively normal life eg going to shops (as I think they should)
They aren't: they are being very cautious.
> I think you could do that with lateral flow testing rather than taking a vaccine that may be net harmful to your health
Everyone in our family is already testing before each visit with our most vulnerable relatives, which is additional protection on top of the booster.
But even if this were not a factor in my life, (2) would still be sufficient.
↑ comment by Nathaniel Monson (nathaniel-monson) · 2023-10-04T19:09:49.307Z · LW(p) · GW(p)
Surely your self-estimated chance of exposure and number of high-risk people you would in turn expose should factor in somewhere? I agree with you for people who aren't traveling, but someone who, eg, flies into a major conference and then is visiting a retirement home the week after is doing a different calculation.
Replies from: johnhalstead↑ comment by johnhalstead · 2023-10-04T19:36:30.388Z · LW(p) · GW(p)
I don't think that makes much difference because I don't think it has much effect on the total number of infections - you would really be changing the time at which someone gets the virus given that we're not trying to contain it anymore.
One way round the concern about visiting the retirement home would be to do a lateral flow test before you go in. If you're seeing extremely vulnerable people a lot, then it might be worth getting the vaccine. But the IFR is now lower than the flu for all ages and I think should be treated accordingly
Replies from: nathaniel-monson↑ comment by Nathaniel Monson (nathaniel-monson) · 2023-10-04T21:26:39.679Z · LW(p) · GW(p)
I think the people I know well over 65 (my parents, my surviving grandparent, some professors) are trying to not get COVID--they go to stores only in off-peak hours, avoid large gatherings, don't travel much. These seem like basically worth-it decisions to me (low benefit, but even lower cost). This means that their chance of getting COVID is much much higher when, eg, seeing relatives who just took a plane flight to see them.
I agree that the flu is comparably worrisome, and it wouldn't make sense to get a COVID booster but not a flu vaccine.
↑ comment by Mark_ · 2023-12-15T06:26:38.533Z · LW(p) · GW(p)
Note that the serious adverse events (SAEs) that were recorded as attributable to the vaccine in the study were much more mild:
- Of the 12 SAEs reported in the intervention arm of the randomised controlled trial (RCT) for BNT162b2 (n=5055), three were found by blinded investigators to be attributable to the vaccine, providing a rate of 1 in 1685 (3/5055).19 The three SAEs considered vaccine related included: moderate persistent tachycardia, moderate transient elevated hepatic enzymes and mild elevated hepatic enzymes.
Seems a bit misleading to list those much scarier sounding SAEs (as the paper does as well) like death and birth defects when none of them occurred in the study.
comment by Jackson Wagner · 2023-10-05T03:11:17.809Z · LW(p) · GW(p)
Yeah, I am interested in this from the "about to have an infant" perspective (my wife is almost 20 weeks pregnant). Interestingly this means she will be able to get both the flu, covid, and newly-approved RSV shot.
- Presumably you want to space out the vaccines a lot -- I would guess two weeks at least, but maybe more?
- Is there a difference between when covid, flu, and RSV peak in activity, which might justify getting one before the other? (The RSV vaccine is apparently only approved for weeks 32 - 36 of pregnancy, so we will at least have to wait at least another 12 weeks I guess, which annoyingly takes us all the way past the holidays.)
- Like you say, I am thinking that earlier is better (rather "play it safe" and have some immunity, even if it later wears off), so she has already gotten her flu shot. (Does flu or covid immunity wane faster?)
- I think part of the reason RSV is only approved for the third trimester is to transfer some immunity to the child, so that the newborn is protected in its first months of life. Presumably that logic applies less for influenza (which is not particularly severe in newborns) or covid (which seems especially mild in children)?
comment by chasmani · 2023-10-07T09:27:24.010Z · LW(p) · GW(p)
I think I’m more concerned with minimising extreme risks. I don’t really mind if I catch mild covid but I really don’t want to catch covid in a bad way. I think that would shift the optimal time to take the vaccine earlier, as I’d have at least some protection throughout the disease season.
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2023-10-07T10:32:22.251Z · LW(p) · GW(p)
The half life I discuss on the post is for protection from infection. For protection from severe illness and death the half life is far longer. So unless you're writing that because you've not been vaccinated yet I don't think that's right?
comment by Yanjo · 2023-10-04T06:29:52.438Z · LW(p) · GW(p)
Only nit is that vaccine efficacy isn't at 100% right after the shot. Common wisdom was 2 weeks, though honestly, I don't remember if that was a robust claim, doesn't necessarily mean the same for the newest one.
Only affects your model if there's risks in the ~2 weeks after your otherwise "optimal" timing
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2023-10-04T19:56:21.333Z · LW(p) · GW(p)
Yes? Which is why I have "Getting a shot two weeks before Thanksgiving, 2023-11-09, would have you at most protected for Thanksgiving, and then still 82% [78-82%] of peak protection at Christmas".