Covid 8/6: The Case of the Missing Data
post by Zvi · 2020-08-06T21:40:00.880Z · LW · GW · 3 commentsContents
Positive Test Counts Deaths Positive Test Percentages The Decline in Testing The One Dollar At-Home Covid Tests Some Baseball Players Who Exposed Themselves To Covid Got Covid In Case You Were Wondering Why We Can’t Have Nice Things: College Football Edition In Soviet Russia, Vaccine Injects You Is Giving People Hope For a Vaccine Helpful or Unhelpful? I Once Again Have The Power None 3 comments
Last time: Covid 7/30: Whack a Mole
Testing. One could sum up the entire failure on Covid-19 as a failure of testing.
We have failed to test individuals. We have failed to ramp up testing capacity fast enough. We have failed to deliver test results within the time frame necessary for them to stop the spread of the virus. We have failed to allow other forms of testing that could help us greatly.
We have also failed to test everything else. We still don’t reliably know how this virus is transmitted. We still don’t know what actions are safe or risky. We don’t know the right mask designs. Our knowledge of which drugs work is spotty at best. We don’t know how many people are actually immune or how that works. We don’t know if our vaccines work. We don’t know how people respond to different policies and options. We don’t know almost anything.
The reason these posts exist is to try and figure out something, anything. To let us navigate our lives, plan for the future and maybe even help improve he overall course of events. But also on general principles. It is good and right to figure out as best one can what is going on, and tell others, whether or not there is a concrete plan to cash that out into other benefits.
This week’s theme is testing because rather than the usual steady increase, this week saw a marked drop in the number of Covid-19 tests. It’s one thing to move forward too slowly. It’s a different matter to be going backwards. Meanwhile, the shutting down of additional means of testing by the FDA is back in the story as well.
The scariest part of all this is wondering whether this reduction in testing is on purpose.
It is a shame. I had hoped to focus on good news.
Let’s run the numbers.
Be careful with them this week.
Positive Test Counts
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| May 21-May 27 | 23979 | 39418 | 42977 | 37029 |
| May 28-June 3 | 32200 | 31504 | 50039 | 33370 |
| June 4-June 10 | 35487 | 24674 | 55731 | 22693 |
| June 11-June 17 | 41976 | 22510 | 75787 | 17891 |
| June 18-June 24 | 66292 | 26792 | 107221 | 15446 |
| June 25-July 1 | 85761 | 34974 | 163472 | 16303 |
| July 2-July 8 | 103879 | 40139 | 202863 | 18226 |
| July 9-July 15 | 108395 | 53229 | 250072 | 20276 |
| July 16-July 22 | 117506 | 57797 | 265221 | 20917 |
| July 23-July 29 | 110219 | 67903 | 240667 | 26008 |
| July 30-Aug 5 | 91002 | 64462 | 212945 | 23784 |
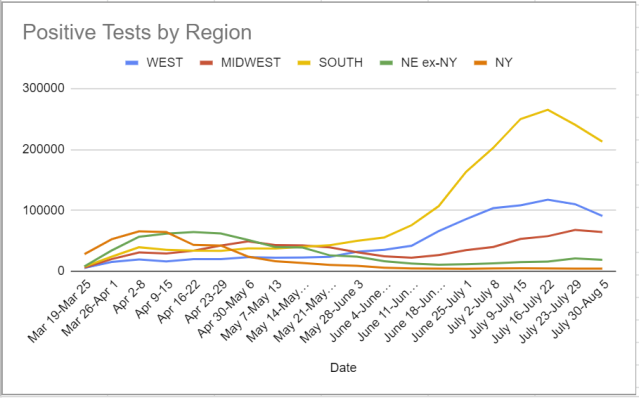
That looks amazing. But the gains are due to lack of testing.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Apr 30-May 6 | 775 | 1723 | 1290 | 3008 |
| May 28-June 3 | 875 | 1666 | 1387 | 2557 |
| June 4-June 10 | 743 | 1297 | 1230 | 1936 |
| June 11-June 17 | 778 | 1040 | 1207 | 1495 |
| June 18-June 24 | 831 | 859 | 1204 | 1061 |
| June 25-July 1 | 858 | 658 | 1285 | 818 |
| July 2-July 8 | 894 | 559 | 1503 | 761 |
| July 9-July 15 | 1380 | 539 | 2278 | 650 |
| July 16-July 22 | 1469 | 674 | 3106 | 524 |
| July 23-July 29 | 1707 | 700 | 4443 | 568 |
| July 30-Aug 5 | 1831 | 719 | 4379 | 365 |

That also looks much better than we had any right to expect. The South looks like it turned the corner. The drop in the Northeast is impressive. Too impressive. Something’s not right.
Positive Test Percentages
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| June 4-June 10 | 3,177,318 | 4.4% | 438,695 | 1.4% | 0.61% |
| June 11-June 17 | 3,446,858 | 4.6% | 442,951 | 1.1% | 0.66% |
| June 18-June 24 | 3,638,024 | 6.0% | 440,833 | 1.0% | 0.72% |
| June 25-July 1 | 4,331,352 | 7.1% | 419,696 | 1.2% | 0.82% |
| July 2-July 8 | 4,461,980 | 8.2% | 429,804 | 1.1% | 0.93% |
| July 9-July 15 | 5,196,179 | 8.4% | 447,073 | 1.1% | 1.06% |
| July 16-July 22 | 5,481,861 | 8.5% | 450,115 | 1.1% | 1.20% |
| July 17-July 29 | 5,757,290 | 7.8% | 448,182 | 1.1% | 1.34% |
| July 30-Aug 5 | 5,079,828 | 7.9% | 479,613 | 1.0% | 1.46% |
Oh no. Testing is way down. Positive test percentages aren’t down at all, despite Florida having a very steep testing decline. That’s not good at all. What happened?
The Decline in Testing
I expected six million tests. Instead, we got five million.
I did some spot checks to see where this was happening.
About 90k of the decline is from Florida, where they had to contend with a tropical storm. That’s only about 15% of the decline. Texas is about 70k of the decline, with a dramatic drop in test reporting the last four days, in a way that looks like incomplete reporting. I don’t know what their excuse is here. Arizona saw a small decline. Results from other states was a grab bag.
I haven’t seen an explanation as to why this happened to this degree. Weather is only a minor factor. Testing if anything declined more in places with worse outbreaks.
The scary question is whether testing is being sabotaged, perhaps because of the need to open schools, and the continuous fallacy that if the tests go away then that makes it all right to make everything worse.
The same question applies to deaths. Are we looking at longer-than-usual delays in reporting? Could a tropical storm be enough to explain this? Or are we looking at something else? It’s at least a week too early to plausibly have the South’s real death count stabilize. Reporting of deaths lags too much for that, and with the dramatic increases in deaths that come before, a small decline doesn’t seem plausible at all.
One possibility is that some deaths were reported faster than usual last week, shifting some of this week’s deaths backwards. That would be a relatively benign explanation.
For the Northeast, it’s clear New Jersey’s reporting this past week has been pretty terrible, which explains a third of the drop. Delaware seems to have dumped a bunch of past deaths on us last week, which gets us halfway home, and we did have some disruptions from the storm in New York and potentially other places. I’m going to say that this change mostly isn’t real, but also isn’t that suspicious.
For the South, I am worried. Florida’s death count actually increased, so the storm is not the issue, and it’s clear that there was no real turning of the corner since most of the South will turn its corner after Florida does. Arizona’s count also didn’t decline. Texas points to a potential partial explanation, as it dumped some extra deaths on us last week due to a methodological adjustment.
I have reasonable ‘hope’ that the death declines that don’t make sense are understandable flukes of data, and we actually do have overall relatively good news on that front, even if not as good as it looks at first glance.
The One Dollar At-Home Covid Tests
This week saw several renewed calls for cheap, plentiful at-home Covid-19 testing. The benefits of such a scheme are obvious.
It’s possible that the calls are the same every week, but that this week I happened to notice them more, slash my thoughts were more about inadequate testing than usual. The result is the same.
When I search, it seems the first news of such tests goes back several months to when they were tested in Senegal.
With plentiful tests, people could test themselves frequently whether or not they had any reason to suspect they were sick.
The FDA refuses to allow these tests unless they are proven to be at least as accurate and good in every way as PCR tests. It seems they are almost as good, and might be as good, but that’s not good enough.
The PCR tests cost several orders of magnitude more, that require taking a trip to see medical professionals, thus taking up a valuable resource and putting both yourself and others at further risk of infection, and which are so overloaded that results can take weeks to get back to a person.
This is transparently obviously a completely insane standard.
The correct response in a sane world would be that these tests are a hyper-efficient supply of very useful Bayesian evidence and that would be the end of that. We don’t live in anything like that world, so we need to break down exactly what would happen in practice.
As many have pointed out, if these tests are not sufficiently specific or sensitive, we don’t have to use them diagnostically. We use them instead as an early warning system to determine who should isolate.
If you get a positive strip test, you isolate, inform your contacts, and get a PCR test.
If you get a negative strip test, you don’t isolate without symptoms. You still get a PCR test if you are high enough priority that you would have gotten one anyway.
That’s it. That’s the rule.
The whole idea is to allow a large percentage of those who are infectious to isolate, and to find a better population on which to use your PCR tests, trading marginal cases for those who have a positive strip test.
You shift costly risk-avoidance behaviors away from people at less risk towards people at higher risk. You shift PCR testing from people at lower risk to people at higher risk.
If the FDA or anyone else is concerned that these tests will mess up the statistics? Fine, don’t count them in the official testing statistics.
Except, of course, even better would be to gather them as their own statistics, and aggregate them to faster and more accurately find places with rising numbers of cases. An office with enough positive strip tests could shut down. So could a school. With that possibility, a school or office that for now has to remain closed could instead open.
Instead, we continue to ban cheap Bayesian evidence whose central practical use case is obviously immensely helpful in multiple ways.
Given how close we are to R0 = 1, we likely could stop this virus in its tracks quickly using this strategy alone (if combined with what we are already doing) – all we would have to do is get a substantial fraction of infectious people to isolate more, even if we miss a lot of people and those who do isolate are not fully successful at doing that.
FDA delenda est.
Some Baseball Players Who Exposed Themselves To Covid Got Covid
I keep focusing on baseball both because it matters to me, and because it is a microcosm that can tell us about Covid in general.
There have now been two outbreaks, one with the Marlins and one with the Cardinals.
Both outbreaks have been traced to players flagrantly violating reasonable social distancing and responsible activity guidelines.
These were not unavoidable flukes. These were deeply irresponsible choices made by players who let their team and their country down.
They also were not cases in which an infection on one team spread to another team. We still have zero examples of this. As I argued last week, I don’t think actual baseball is risky across teams. The risk is in the dugout, in the celebrations, and otherwise avoidable.
Let’s take a closer look. Is baseball actually spreading Covid? Is it doing so more than other activities would in its place?
USA Today has a great feature that it keeps updating that lists who has been infected in MLB.
As of today, there were 97 reported positive tests. One of them was a free agent, Yasiel Puig, which likely had nothing to do with baseball, so let’s ignore that one. 96 positives.
First question. Is that a lot? There are 30 teams, each of which has 30 active players at a time. They can have 40-man rosters, towards which Covid-positive players don’t count. My guess is that this list only contains players who were on active rosters, but players move around and are injured. Let’s say there are about 1000 meaningful players here. We’re looking at a 9.6% positive rate.
How does that compare to the general population?
As always, it’s tough to know the actual base rate. Nate Silver has been suggesting using the estimates here. He suggests 20.6% total infection rate for New York, where I have 23.3% as my estimate, so it’s not too far off there from my general beliefs. For this purpose, it will do.
He has 12.4% total infected for the United States. That’s higher than baseball’s base rate.
But that’s not entirely fair, because baseball’s tests only started in July. The first positive test report is from July 2, and they don’t seem to be doing antibody tests even though they really, really should have done them. So we should be comparing their infection rate to the infection rate in the USA since when a new infection would show up on a test in July. Which is a lot lower. Let’s say you test positive for an average of two weeks after infection, so June 15 is our deadline. That means 5.9% were infected and wouldn’t have been detected, leaving 6.5% infected since then.
That means that MLB players have been infected at about 50% higher rates since their testing started, than the general population.
One could argue that baseball players have the resources and incentive to be more careful than others, but one could also argue that baseball players are young and athletes tend to be irresponsible.
How many of the extra positives are clearly due to baseball? Let’s assume that infection hasn’t crossed between teams, and look for clusters. There are 18 Marlins infected within the same week, and we can presume that 16-17 of them got it from teammates. We can assume 5 of the 6 Cardinals who tested positive in August probably got it from teammates too.
If we assume everyone who tested positive July 4-7 was infected before they arrived, then there’s only 1 additional plausible case of infection from a teammate, when two Royals tested positive on the same day.
Thus, we have an upper bound of 23 players who were infected by teammates so far. The other 73 are from other sources, at a rate similar to our best estimate of the population’s rate of infection.
We could also say that the infections measured in early July came from before Summer Camp, so we should ignore them, and only count tests from July 10 or after, and exclude anyone who didn’t report to camp until after they were clear of the virus. That would mean players who caught the virus at Summer Camp, on July 3 or after.
If we do that, we exclude 54 cases, leaving only 41. Of those 41, 23 look likely to be from teammates, 18 from other sources.
Using the same website we used earlier, we get a population estimate of 3.1% infected between July 10 and August 2 (since it takes about 5 days to show a positive result). MLB has a 4.1% positive rate in that period, with half of that from the Marlins cluster. If the Marlins cluster had been the size of the Cardinals cluster, MLB would be doing better than average, and even more above average given its locations.
A point of comparison is that 5.4% of baseball players tested positive upon arrival at camp or were still recovering and thus reported late. The data we’re using suggests that for the general population that number should have been more like 2.5%, at most around 3%. Thus, baseball players were clearly taking much above average risk before arriving to play baseball. Their risk seems, upon arriving, to have gone down in relative-to-America terms.
All this talk of MLB ‘failing’ or being on the brink or being irresponsible seems quite wrong to me. MLB could of course be doing much better. The Marlins outbreak was much larger than it needed to be, and players should be kept in much more of a bubble than they are, and on-field social distancing isn’t good enough. There is work to do. But there is work to do everywhere. This is actually a success story.
NBA is of course an even bigger success story. They’ve created a bubble in the heart of the epidemic, and so far it has held. Zero positive cases yesterday, games are being played. Let’s hope it continues.
Also consider this when reading about schools. I don’t think opening schools is a responsible thing to do. But that doesn’t mean that every time a kid has a positive test, it’s a systemic failure of the system.
There were these huge headlines of “school foolishly and irresponsibly reopens in Georgia and less than 24 hours later a student tests positive and his class has to quarantine.” If 2%+ of the population is infected at any one time, even if the rate among kids is a lot lower, of course there are going to be classrooms that have to shut down on the first day. It’s not a scandal. Or rather, the scandal lies outside the school.
Extend that to everything else, as well.
In Case You Were Wondering Why We Can’t Have Nice Things: College Football Edition
As I’ve made clear, the game must go on. No football, no peace. The needs of the many, together with the benefits to the few, hugely outweigh the risk to the few and I have little tolerance for the false righteousness that says otherwise. I don’t even think Covid-19 substantially changes the risk profile of playing football, at least at positions where one takes a lot of hits.
That, however, relies on a modicum of common sense and human decency. This is college football, so that’s not a safe assumption. We periodically get stories like this, h/t Seth Burn via Kevin Lytle. Here’s the money quote:
CSU football players and university athletic department staff say coaches have told players not to report COVID-19 symptoms, threatened players with reduced playing time if they quarantine and claim CSU is altering contact tracing reports to keep players practicing.
It is one thing to train for and play football knowing that some players will get Covid-19, and others will get Covid-19 that wouldn’t have had it if they hadn’t played football.
It is another thing to actively surpress players from reporting symptoms, or quarantining when they are sick or might be infectious, and to alter contact tracing reports.
As Seth puts it, that’s what you do when you actively want a Covid-19 cluster on campus. It’s criminal on multiple levels. Yes, it’s in line with how football teams often treat other health conditions, and I wish that were not so, but pandemics are different.
Even on a pure win-at-any-costs level, with no risk of being caught or called out on such actions and if everyone was totally fine with it, this still seems mighty grade-A stupid. All such policies do is guarantee widespread Covid-19 infection. The team’s health and performance will suffer. Why would you want to power through like this?
I can think of two explanations.
The first possible explanation is that no one involved is thinking about whether this actually benefits the team. They know that being tough and hiding medical conditions while having players practice, play and power through them is what winning teams do. It’s how you build character. That’s the football way. The idea that a pandemic might be a different case doesn’t cross their minds. Combine this with the instinct to get through the next day, the next week, while moving away from blameworthiness, and it’s easy to see why hiding the evidence could be the instinctual thing to do despite it making zero sense and on net costing the team wins.
The second possible explanation is that this is intentional variolation. The goal is to infect the whole team now so they’ll be ready for the season.
Think about it. It’s much less crazy than it sounds.
If you successfully shield the team now, then they’ll get Covid-19 later, because they’ll be jock college students who do jock college student things and then practice and play against others doing likewise. If there isn’t much to be done about that, better to get it over with now.
Of course, if that was your plan it would be much better to do it in a systematic and responsible way, rather than like this, but that option requires admitting what is going on, which isn’t available. So, this is what we get instead.
I’m not saying that’s what is happening. But it does seem to fit the data.
In Soviet Russia, Vaccine Injects You
Russia is preparing for mass vaccinations as early as October.
I am very happy that Russia is doing this, on multiple levels.
On a basic level, I expect this to be a positive expected value thing to do. There is some risk that the vaccine will not work, and even some risk that it will backfire and make people more vulnerable to infection. This is true. However, I have a hard time believing that the odds don’t favor acting now rather than waiting to act later.
On a broader level, this will tell us quickly whether the vaccine works. It’s a massive experiment with hugely valuable results. I consider it highly ethical, since I think it’s net positive to participate, but I would favor running the experiment at scale even if I didn’t think it was obviously net positive.
The worry that a failed vaccine might add fuel to the ‘anti-vaxers’ and prevent people from getting vaccinated is real. So is the worry that a failure here would make everyone generally more cautious doing pretty much everything vaccine-related, which would also be very bad. I get that. But I can’t advocate making mistake X because if I don’t make mistake X others might make mistake X in the future.
I also don’t think the success or failure of vaccines, or anything that might go wrong with them, would have a substantial effect on support for vaccination. The arguments on both sides will be the same. The case for vaccination will remain beyond overwhelming and obvious. Those who don’t want to vaccinate will point to the incident instead of other events, and their example will be somewhat more real, but I don’t think it matters. Those who care about whether the evidence is real at all will realize to forking vaccinate. Those who don’t care about whether the evidence is real will have nothing change.
There have been real vaccine failures in the past from moving fast and trying to do the most good despite the risks. That’s not what anyone ever talks about. They instead talk about completely false claims that resonate better with those that are vulnerable to such arguments.
If anything, the harm from failure stems from us setting a narrative up that a failure would strengthen resistance. That seems more like a self-fulfilling prophecy.
In any case, I salute you, people of Russia. You’re doing the world a great service. And if you hacked into our computers and stole that vaccine from us, you know what? Thank you for that, too.
Is Giving People Hope For a Vaccine Helpful or Unhelpful?
Whenever you see statements about anything in today’s world, and especially anything about Covid-19, a key question to ask is which simulacra level the statement is primarily functioning on.
When people talk about a vaccine, they could be talking on any of several levels.
Level one talk is about what is actually going to happen. When will a vaccine be ready? How long after that will I be able to get one? How long after that will this effectively be over? How likely are the vaccines to work? And so on.
My best guess right now seems to be ‘around October if everything goes well,’ ‘a few months after that, again if everything goes well,’ ‘not for a while after that but things will steadily get more and more normal’ and ‘actually pretty damn likely that at least one of them works pretty well and we figure that out.’
My confidence in all that is low, but that’s my best read of the situation.
Level two talk is about making people believe the thing you think will cause them to act the way you’d like them to.
Usually this means that someone wants everyone to wear a damn mask and otherwise act responsibly to contain the virus. Things that we’d like people to do whether or not the vaccine is coming.
Occasionally, it’s the opposite, and someone wants to argue for herd immunity strategies, but that’s rare.
Level three talk is about showing that you are in the right coalition and are the right type of person. This tends to be people talking about how vaccines are very difficult and complicated, and should not be treated as a ‘magic bullet,’ and can’t be relied upon. That vaccines must be Properly Approved after being Properly Tested using Proper Medical Ethics, and then Distributed Fairly, or else better to just let everyone sit around in their homes while the economy and many of those people die. This righttalkism is a large percentage of all vaccine talk.
Such level three talk often claims to instead be level two talk, with the goal of getting people to buckle down and act responsibly, because part of the coalition signal is to be advocating for things that cause people to act responsibly. It waves its hand towards being level one talk, but rarely with much conviction.
Or, alternatively, there are those who want to be in the group that thinks vaccines are an evil conspiracy, because that’s the world we live in. Or those who want to complain preemptively that the company that saves the world economy and hundreds of thousands of lives might end up turning a profit, or make Western civilization look good, or save us from having to deal with nature’s mighty wrath, or something. Which would all be just awful. Sigh. Beware righttalkism.
Level four talk here is about saying the types of things to say to give off the impression you want, without any intention to convince anyone of anything concrete or to take any subsequent actions or update any models. Thus, those who want to give general impression of awfulness or wonderfulness. The practical difference between this and vaccine level two talk is that level two talk is trying to convince people of things, and this isn’t.
Thus, we get arguments from both sides coming on all four levels, with a lot of it on the second and third levels.
Today’s discussion question comes from Nate Silver and concerns level two. When one says that a vaccine is unlikely to arrive soon, thus being a level three responsible person, what is the actual level two effect?
On the one hand, lack of hope could lull people out of a false sense of complacency. We can’t wait for the vaccine. We have to solve this ourselves! We can do it!
On the other hand, it could, lack of hope could cause despair. We can’t wait for a vaccine, so we can’t hope to keep up these awful lifestyle choices forever. We’ll never solve this ourselves! We can’t do it!
In the first case, you’re ‘helping.’ In the second case, you’re doing the opposite. Those engaging in such talk want people to think they are working to trigger the first effect. Nate speculated the second might dominate instead.
I’m not confident, but I think he’s right. At this point, what people ‘need to hear’ to encourage them to do what is necessary is that this is a fight that won’t last forever. That it’s a fight we can win.
Thus, anyone giving an awful future outlook is likely making the short-term situation worse slash encouraging a de facto herd immunity strategy (which might not be worse, depending on how things go), whereas anyone giving a hopeful future outlook is making the short-term situation better because it gives people the motivation and strength to carry on for a while longer. There’s a light at the end of the tunnel.
The more important point, of course, is that if our civilization is to survive then we can’t decide what story we are telling based on which psychological impact we expect to dominate. Two plus two equals four. Either the vaccines are likely coming or they’re not. Either a mask works or it doesn’t. Lying about such things backfires in the long run every time, and in the short run most of the time. Stop it.
I Once Again Have The Power
This week’s update was delayed slightly by our losing power here. Under the brave leadership of Andrew Cuomo, once again events beyond his control have conspired to cause damage in the great state of New York, and the not-at-all-a-blowhard-in-chief has called for an investigation as to how the power companies could have been so woefully unprepared for the storm. Somehow, the bad things that happen to New York are not due to poor state leadership. No, sir. Can’t be that.
This is the buck. It would like somewhere to stop. Please get back to it as soon as you can.
See everyone next week.
3 comments
Comments sorted by top scores.
comment by RamblinDash · 2020-08-07T13:41:24.410Z · LW(p) · GW(p)
One possible less-nefarious explanation for the reduced test numbers is that more tests were performed but fewer were processed because one or more central processing labs were affected by the storm. LabCorp and Quest, our national backlogged testing duopoly, have several major labs in Florida, Georgia, and North Carolina that could have been impacted, and this could affect test numbers for other non-storm states if they sent their tests to these labs.
comment by Dr_Manhattan · 2020-08-06T21:48:57.695Z · LW(p) · GW(p)
thought this was interesting
https://twitter.com/HealthAllegheny/status/1291466180386062340?s=20
comment by Viliam · 2020-08-07T22:21:53.274Z · LW(p) · GW(p)
The second possible explanation is that this is intentional variolation. The goal is to infect the whole team now so they’ll be ready for the season.
Think about it. It’s much less crazy than it sounds.
The crazy part will be watching people who can't breathe trying to play football.