Posts
Comments
Actually, cryogenic vessels do not really fail, in the sense I think you mean, over time - with the notable exception of liquid helium and liquid hydrogen storage vessels. Liquid helium has bizzare effects of metal (in addition to quantum tunneling) causing high strength steel to embrittle over time. It is thoought that this occurs due to the presence of helium in solid solution in the metal subjected to loading, and being present at a temperature sufficiently low to form grain boundary cracks as a result of sliding along grain boundaries (which contain steps developed as a result of prior intragranular shear).
Hydrogen "embrittlement" is due to migration of lone hydrogen atoms into the metal where they re-combine in sub-micron sized voids in the metal matrix to form hydrogen molecules. In so doing, they create pressure from inside the cavity where they are located which can increase in vulnerable areas of the metal (e.g., where it has reduced ductility and tensile strength) to the point where the metal develops first micro-cracks and then a large, macro-fracture resulting in castastrophic failure.
Liquid nitrogen storage containers kept dry and free from liquid oxygen accumulation, and which remain stationary, can and do last "indefinitely." They will require periodic re-hardening of the vacuum, but this is not due to structural failure, but rather is due to outgassing of materials from the reflective/convective barrier wrap and of hydrogen from hydrogen inclusions in the welds. If the units are not man-handled and are well cared for, there is essentially no work-hardening of the welds, or of the structural metal itself, and they may well last for many decades, or even centuries. If the nitrogen gas boil-off were used to create a dry nitrogen sheild around the exterior of the vessels, their lifespan would likely be in the range of many centuries. Work-hardening, hydrogen ingress into the metal from water condensed from the air and corrosion from atmospheric oxygen and water at the neck-tube are the three principal causes of structural cryogenic dewar failure. If the dewar is not moved about, and if water is eliminated from the environment, stainless steel dewars should last indefinitely. I've seen dewars in semen storage facilities that are 50 years old and have not yet required rehardening of their vacuum. Conversely, I've seen vessels in lab use and used to haul industrial gases fail after a few years, or even a few months of use. TLC is almost everything when it comes to liquid nitrogen dewars.
Probably the best example of how robust ultra-high pressure vessel engineering can be is to look to long range guns on battleships. These tubes are about 2" in diameter shy of being big enough to hold an average human and can withstand pressures in the range Maxikov is talking about. These "vessels" also have a breech and operate under horrible conditions wih respect to heat and corrosion. And yet, failure is almost unheard of. When failure means the loss of a battle ship, failure is not an option; consider that one turret on a 20th century battleship, exclusive of the guns, cost ~$1.5 million, U.S. These guns were made with mid-1920's technology and remained in service until the last decade of the past century. Then, there was the Paris-Geschütz (http://en.wikipedia.org/wiki/Paris_Gun) of Krupp, but that's another story...
Most of my childhood notes and cryo-memrobilia were lost when my house burned down in September, of last year. So, regrettably, I can't consult my notes from those experiments. However, as best I recall, the mortality rate in yeast frozen in distilled water was ~90%. No special treatment was required beyond removing them from the incubating medium and resuspending them in distilled water prior to freezing. Viability was determined indirectly by adding the frozen-thawed yeast in water to culture medium in an Erlenmeyer flask connected to a water displacement set-up very much like this:
http://herbarium.usu.edu/fungi/funfacts/respiration.jpg
{kind=link}
I later repeated this experiment with red cells (my own) which is much more sensitive and directly quantative of cell survival. You do, however, need a centrifuge and related equiupment to measure microhematocrit - things I could easily acquire back in the day (and in fact, still have).
If people did hands-on biology in the same way and to the same extent they do hands-onelectronics and programming, we'd all likely be either "immortal," or dead, by now.
Here is an experiment I am currently struggling to tool to do which may serve as an example. Recently, a very simple way was discovered to induce apoptosis in a significant fraction of senescent cells in vivo in rodents, and in human cell culture cells, as well: http://onlinelibrary.wiley.com/doi/10.1111/acel.12344/pdf. This results in partial rejuvenation of the animals because senescent cells release myriad toxic cytokines, chemokines and other pro-inflammatory and probably telomere shortening species. While there is as yet no evidence that eliminating senescent cells - or reducing their number - will increase lifespan, there is ample evidence that it will greatly increase healthspan. This new class of drugs has been dubbed the "senolytics" by their discoverers, Zu and Tchkonia. The nice things about these two drugs is that they are both small molecules which are readily available, FDA approved/GRAS and have very low toxicity. One is the OTC nutrient quercetin, and the other is the relatively exotic molecularly targeted antineoplastic agent dasitinib, marketed under the name of Sprycell by Bristol-Meyers-Squibb.
In mice, one dose of these agents in combination was effective at reducing the senescent cell burden dramatically, with benefits lasting for 7 months. The cost of a dose of dasitinib for an adult human is about $400 - eminently affordable (the cost of the quercetin required is a few cents). So, what's the problem? Well, if you are over 30, odds are that you have a significant burden of senesacent cells, and by the time you are 50, somewhere between 15 to 30% of your body mass may be senescent cells. In my days in ICU doing hemodialysis, I saw more than a few patients critically ill and in renal failure from something called "acute cell death syndrome" (ACDS) which most often resulted from chemotherapy given to lymphoma or leukemia patients too rapidly, resulting in a massive die-off of cancer cells. Large scale cell death is toxic and can be, and often is, lethal.
Animals treated with dasitinib+quercetin do not show signs of ACDS. However, careful monitoring of blood chemistrires during the treatment phase was not done and the animals so far studied were middle aged rodehts - not humans, and certainly not older, or elderly humans. Thus, additiional data are needed. In my opinion, dogs are ideal for such a study because they are available in abundance as old and very old (senile) animals, have large blood volumes which allow for harmless routine clinical laboratory evaluations, and have neurobehavioral faculties which are easily and reliably assessed by untrained humans. They also stand to benefit from the treatment if it does not prove lethal, or can be adjusted so that it is easily tolerated.
You have to "make" your own aged rodents and that takes years. And years are something many of us no longer have... Research begun now (or soon) will very likly yeild results that will be immediately clinically applicable to humans. Unfortunately, this research cannot practically be done anywhere in the West legally.
My pleasure!
I have a few (hopefully helpful) comments to add. I am a huge advocate of trying things yourself on a do-able scale. For instance, many years ago I had pretty much the same idea you did and I decided to it out, directly. I lived across the street from a mechanical engineer from Eli Lilly, Inc., named Bud Riever. I asked Bud to figure how much prsssure would be developed if I simply cooled a closed steel container which was completely filled with water to well below the frrezing point? The answer was about 2,000 atmospheres, or about 24,000 psi. As it turns out, a piece of steel pipe of the right thickness threaded on both ends and capped with screw on galvanized steel pipe caps will hold that pressure. And, since it is hydrostatic pressure with no gas present, if the pipe fails (splits), it will not fail explosively. My test subject was to be Baker's yeast, reconstituted in a dilute sugar solution and placed inside of a twist tied sawdwhich bag (no air bubbles) which was in turn placed inside the section of pipe which was then capped on the open end.
It took me forever to figure out that the only way to close the pipe with the yeast inside, whilst excluding also all air bubbles, was to do so in a galvanized metal wash tub filled with water. The cap on the pipe was screwed shut under water in tub. I could then cool my self-pressurizing chamber with a slush of dry ice and acetone. I broke several pipes before I found a thickness of steel that would take the pressure. Alas, my experiment showed only a little better survival of yeast under pressure than that which was achieveable under the same conditions with a vented pipe; i.e., almost none.
Maybe two years ago, I got the idea that inhaled hydrogen gas might be profoundly radioprotective. H+ should be available to neutralize the OH- radicals produced by the interaction of gamma rays and water, thereby acting as an "instantaneous" neutralizer of the bulk of radiation injury (the bulk of the non-hydroxyl radical injury occurs when high energy particles directly impact and disrupt DNA). I did a literature search and found nothing. I also asked a medical physicist friend and several other scientists whom I respected. I was told that this approach would not work in large measure because the addition of dissolved hydrogen would not deal with the problem of the hydrogen radical that would remain after the hydroxyl radical was neutralized. My hypothesis was that the hydrogen radical would react with oxygen to form another hydroxyl radical, and then subsequently be neutralized by the abundand molecular hydrogen.
After some months, I couldn't stand not knowing anymore so I found an industrial X-ray service with powerful enough X- and gamma ray sources to deliver ~16 gray of radiation to half a dozen mice in a reasonable pewriod of time and I cobbled up a test apparatus. The next step was to expose mice to supralethal doses of X- and gamma rays. Hydrogen gas at 80% of the breathing air (balance oxygen) was indeed profoundy protective. When I passed this information along to my medical physicist friend he quickly found cites of other (pretty obscure) work showing the same effect:
Qian LR, Cao F, Cui JG, Huang YC, Zhou XJ, Liu SL, Cai JM: Radioprotective effect of hydrogen in cultured cells and mice. Free Radic Res 2010, 44:275-282. PubMed Abstract | Publisher Full Text OpenURL
Qian LR, Li BL, Cao F, Huang YC, Liu SL, Cai JM, Gao F: Hydrogen-rich pbs protects cultured human cells from ionizing radiation-induced cellular damage. Nuclear Technology & Radiation Protection 2010, 25:23-29. PubMed Abstract | Publisher Full Text OpenURL
Alas, my dreams of a commercializable product that would render radiolgical exams effectively safe for children, young and middle aged adults vanished, well, as in a puff of hydrogen and oxygen igniting. But here (to me) is the really strange thing, despite the stunning degree of radiprotection inhaled hydxrogen gas proivides, as well as evidnce that it is pluripotent protect against ischemia-reperfusion injury, cancer and a variety of other free radical mediated pathologies (http://www.molecularhydrogeninstitute.com/studies/), no one I know has shown the slighest interest in it. So, even if you identify something that is workable and easy to implement, don't expect the world to beat a path to your door!
Nevertheless, DOING THINGS and actually carrying out experiments changes how you think, how you approach problem solving and how your brain is wired. These changes are, for the most part, empowering and make you better problem solver.
I'd say FUNDAMENTALS OF CRYOBIOLOGY, followed by Baust's ADVANCES in BIOPRESERVATION. However, you may find another starting point better. I recently felt the need (out of self defense) to learn about dentistry. That's a bit like saying I decided to learn about neurosurgery:that covers a lot of ground. However, mostly what I was interested in was plain old restorative dentistry and the much more exotic implant dentistry. There are easily half a dosen textbooks on basic, restorative dentistry... After perusing a number, I settled on one as a proper "read through" introduction. All were adequate, but only that one really communicated in my style. The good thing about most modern textbooks is that there are now study and review guides and, of course, mock-up Board exams. This kind of learning allows me to get a good basic grasp of what is being done to me and to overcome the "condescension" factor when speaking with the dental professionals treating me. Please note, it does NOT make me a dentist! I wish I could recommend the same thing vis a vis cryobiology or cryonics. But I can't. I've tried to get support to start a formal training college for cryonics professionals (I actually have some funding), but have been laughed at, or dismissed out of hand - perhaps justifiably so. Nevertheless, that is what needs to be done and textbooks, study guides, testing and certification do not occur until a discipline is professionalized and formally taught.
I was asked by several people to comment on this post/proposal. Clearly, Maxikov put a lot of time and effort into this post and, at least in part, there's the pity. When you find you have an idea which seems at once compelling and obvious (in tems of the science) in an already well explored field, the odds are very good that you weren't the first to reach that conjecture. And that almost always means that there is someting wrong with your premises. Very smart and capable people have been trying to achieve cryopreservation of cells, tissues, organs and organisms for over 50 years now and the physical chemistry of water under very high pressures and very low temperatures has been understood for far longer. This should be a hint that some careful searching of the literature is in order before going public with a proposal to "fix cryonics," and especially before spending a lot of time/energy on proposal like this.
Attempts to use extreme hydrostatic pressure to mitigate or eliminate freezing injury go back at least 60 years, and probably longer. As your phase diagram above shows, when the pressure is sufficiently high during cooling the expansiuon of water is prevented, but ice formation is not. What happens is that other allotropes of ice form which do not require expansion. However, this turns out to be a bad thing, since, as opposed to any of these ices being formed first in the interstitial spaces, as happens with Ice I, freezing occurs both intracellularly and extracellularly at the same time in the presence of other ice allotropes. Crystal formation inside cells results in devastating ultrastructural disruption - far worse than would occur if ice formed outside cells first, grew slowly and dehydrated the cells, and finally resulted in a vitrified cellular interior (providing that cryoprotectant is present).
However, the problem with this approach doesn't stop there. Extreme hyperbaria itself is directly damaging by at least two mechanisms: denaturation of cellular proteins (including critical enzymes and membrane proteins) and damage to cell membrane lipid leaflets resulting in permeabilization of the membrane to ions (Onuchic LF, Lacaz-Vieira F., Glycerol-induced baroprotection in erythrocyte membranes. Cryobiology. 1985 Oct;22(5):438-45.) Irreversible membrane damage occurs in mammalian red cells exposed to a pressure of 8000 atm (~117,600 psi) applied for ~10 minutes. Exposure of more comnplex mammamalian cells to far lower pressures~20,000 psi, results in loss of viability due to protein denaturation, and perhaphs due to alterations in the molecular structure of membrane lipids,as well. Interestingly, the same compounds that provide protection cellular (molecular) protection against freezing damage also confer substantial protection against baroinjury. Fahy, et al., have extensively explored the use of hyperbaria to augment vitrification in the rabbit kidney (http://www.freepatentsonline.com/4559298.pdf) and have further extended work from the 1980s demonstrating that cryoprotectives are also substatntially baroprotective.
The first work that I'm aware of to attempt to achieve organ cryopreservation using hyperbaria was that of the late Armand Karow, in the late 1960s - early 1970s (Karow AM Jr, Liu WP, Humphries AL Jr. Survival of dog kidneys subjected to high pressures: necrosis of kidneys after freezing.Cryobiology. 1970 Sep-Oct;7(2):122-8. PMID: 5498348). Karow was able to demonstrate the brief tolerance of dog kidneys to pressures of about ~18,000 psi, however, kidneys subjected to isothermal hyperbaric freezing, even in the presence of of moderate cryoprotection, did not survive.
When I started research and experimentation in cryobiology nearly 40 years ago, there was no Internet, no (affordable) photocopiers and the only way to do a "literature search" was with something called the Index Medicus (http://en.wikipedia.org/wiki/Index_Medicus) which was a veritable wall of bound volumes. I used 3" x 5" index cards to write down possible cites to look up - which then required a trip(s) to the "stacks" to look for the journals. Today, I have the Internet, Pubmed, the international patent database and on line library for 30 million books available. I currently have a digitial library of 12,000 mostly scientific and technical books which, at its current rate of growth, should double in size within a few months. My computer is almost constantly reading a book to me with software that cost me just under $5.00. One of the books I "read" recently was The Shallows: What the Internet Is Doing to Our Brains by Nicholas Carr. Carr argues that the Internet is fundamentally altering the way most people today process information - and not for the better. I don't use the Internet the way most people seem to, today. I rely heavily on books, especially textbooks, to educate me about areas with which I have little or no familiarity, and my approach is pretty much what it has been since I started my intellectual life; namely to study intensively and deeply until I achieve basic mastery of an area, and only then use skimming and browsing over large amounts of material to advance my knowledge. The tools of the information-digitial age have thus been a nearly unblemished advantage to me. If you want to reads Carr's book, click on this link:
http://www.mediafire.com/download/5s4wdr554ia4axn/Nicholas_Carr-The_Shallows__What_the_Internet_Is_Doing_to_Our_Brains_(2010).epub and then click on the green Download button.
I'm also posting links to a number of full text books on cryobioolgy which you can download, as per above:
ADVANCES IN BIOPRESERVATION: https://www.mediafire.com/?raccqhv0rrqfhmh
ADVANCES IN LOW TEMPERATURE BIOLOGY: https://www.mediafire.com/?4i6v9qublf3l8q2
FUNDAMENTALS OF CRYOBIOLOGY: https://www.mediafire.com/?pxq6mxbxvfib41j
CURRENT TRENDS IN CRYOBIOLOGY: https://www.mediafire.com/?pxq6mxbxvfib41j
CRYOPRESERVATION... https://www.mediafire.com/?pxq6mxbxvfib41j
LIFE IN THE FROZEN STATE: https://www.mediafire.com/?ydx3a89m2f47r7y
THE FROZEN CELL: https://www.mediafire.com/?ydx3a89m2f47r7y
Cheers, Mike Darwin
Next up for discussions is the issue of "hyperonconicity." Just as cells require a certain "tonicity" (electrolyte concentration) to maintain their normal volume, tissues with capillaries require a certain concentration (and type) of large (macro-) molecules (colloid) to avoid accumulating water between the cells and becoming swollen, or edematous. Hyperonconicity refers to any solution that has more ability to hold water in the circulatory system (circulating blood or perfusate) than would be the case under NORMAL conditions. The key word there is NORMAL. The macromolecules that comprise colloids can be thought of as molecular sponges that hold water in the capillaries and prevent it from accumulating in between cells as a result of the hydrostatic pressure of perfusion.
This water holding ability is quite complex and nuanced and depends upon the condition of the junctions between the cells in the capillary, the charge of the colloid, the unique chemical properties of the colloid (poorly understood), the configuration of the colloid molecule, and so on.
Onconicity and hyperonconicity are thus in actual practice, relative terms - relative to the condition of the capillary membrane. It is quite possible to have a markedly hyperoncotic perfusate and still have massive edema due to accumulation of water and of the colloid in between the cells! This is so because injured capillary membranes do not behave the same way as healthy or intact ones do - they leak! They leak colloid and with the colloid goes water. Simply cooling the organs (or bodies) of non-hibernating animals results in increased capillary permeability and the leakage of colloid and water into the spaces between cells. There is currently not a complete understanding of why this happens, or why some colloids do not leak as much in the cold as do others. In fact, only a very few species of colloid have been shown to leak less in hypothermia.
Capillary injury and consequent leakage of colloid from ischemia is vastly worse than that induced by hypothermia alone, and no colloid has been identified which is effective at inhibiting this leak, or even reducing it enough in clinical settings to meaningfully change outcome. In the setting of serious ischemic injury in the presence of high concentrations of cryoprotectant, NO COLLOID OR OTHER MOLECULAR SPECIES HAS BEEN SHOWN TO SIGNIFICANTLY REDUCE EDEMA - INCLUDING the PEGs OF VARIOUS MOLECULAR WEIGHTS. CI's own research associates had reported this to CI prior to Ben's decision to do an ad hoc experiment on a human patient with absolutely no prior laboratory animal or even bench testing of the perfusate. The only thing more unconscionable than such an uninformed and reckless action is the continued denial that it was such, and that his "mistake did not have the disastrous consequences implied by Mike Darwin."
Here is what Ben Best says about the outcome for Curtis Henderson in terms of cryoprotective concentration at the end of perfusion:
" The refractive index of the effluent was 1.366 after six liters of VM−1 had been perfused, and was 1.3586 at the end. Intermediate values were as low as 1.3586 and as high as 1.3651, but this was a small range with no trend, and is indicative of random variation. These values are well below the values of 1.416 for 60% VM−1 and 1.4275 for 70% VM−1 — and they showed no trend."
Based on the reported refractive indexes of the venous effluent, I would estimate that Curtis Henderson had approximately 20% to 20% cryoprotectant in his brain - most of which was ethylene glycol. That would (again roughly estimating) equate to about 1.5M to 2.0 M glycerol in terms of colligative cryoprotective effect. I have not yet posted the electron micrographs (EMs) of the damage incurred when 3M glycerol is used as a cryoprotectant in the cat brain, but the histology is posted here: http://wp.me/p1sGcr-lt . I can tell you that the EM's are vastly worse than are the light micrographs.
I have provided a detailed, and I believe accurate, scientific rebuttal to Ben Best's claims. For onto a decade I have privately urged CI to either stop advertising that they are perfusing human patients under conditions which yield 86.1% viability +/- 5.8% (for a 55% concentration CI-VM-1 at - 20 deg C FOR TEN MINUTES, followed by cooling to and rewarming from -130 degrees C at 0.3 degrees C/min) brain tissue viability and ultrastructure, when in reality they are treating patients with 70% VM-1 delivered at +7 (or higher) to -7 deg C (rarely) over far longer periods of time (hours) and in the presence of ischemic insults that typically run to many hours, or even days!
This isn't about elegance of writing, it's about facts, most of which are derived from CI's own website.
As you can see from the CI data above and below, patient temperatures never come anywhere near -7 degrees, let alone the -20 degrees C called out in either the original animal research, or in CI's own publicly posted protocol for how cryoprotective perfusion is to be administered. In fact, it is necessary to look a number of case reports to even document that CI is perfusing its p atients with VM-1 chilled in a mechanical freezer: "Perfusion with CI−VM−1 vitrification solution began at 3:04 A.M. The CI−VM−1 was at freezer temperature (about −20ºC) in contrast to the ethylene glycol, which was at refrigerator temperature (about 3ºC)" see: http://www.cryonics.org/reports/CI110.html In fact, this patient was one of the very few who achieved any subzero temperature during cryoprotective perfusion with VM-1:
Refractive Index values only taken during CI−VM−1 perfusion CI Patient 110: http://www.cryonics.org/reports/CI110.html
TIME (AM) Nasopharyngeal temperature (ºC) Flow rate(liters/minute) Pressure mm Hg RJVRI
3:07 8.25 1.07 102
3:08 6.9 1.06 101
3:09 5.3 1.07 100 1.3700
3:11 3.6 1.3769
3:16 4.3 1.39 101 1.3670
3:19 2.0 1.37
3:20 0.8 1.00 1.62 1.367
3:20 Perfusion Halted/Surgery
3:30 0.4 0.35 134 1.4166
3:33 −1.4 0.29 135
3:37 −2.6 0.26 120 1.42
3:40 −3.6 0.24 111 1.424
3:41 −1.4 0.29 135
3:43 −3.7 0.26 127 1.42
3:40 −3.0 0.28 126 1.454
3:45 −3.7 0.26 118
3:48 −3.9 0.28 128 1.4346
3:53 −5.3 0.28 125 1.4281
3:57 -5.6 0.27 122 1.4285
4:00 −5.8 0.26 120 1.4296
4:03 −5.8 0.26 117 1.4276
4:05 −5.8 0.26 117 1.4276
4:10 −5.7 0.26 115 1.4284
4:15 −4.6 0.26 114 1.4284
4:20 -3.8 0.26 109 1.4250
4:23 −3.0 0.27 86 1.4181
4:07 −2.3 0.34 82 1.4204
Since it is standard CI operating procedure (and a biological imperative to reduce toxicity) to pre-cool VM-1 in a freezer before use, and since PEG-VM-1 solutions invariably undergo gel formation/precipitation under such conditions, then how is it possible to say, as Ben Best does, "There is no incompatibility between DMSO and PEG"? In fact, there is, because PEG solutions with glycerol or ethylene glycol do NOT undergo this kind of transition - at least they didn't in my laboratory. Even more to the point, Aschwin & Chana deWolf, two researchers who work with CI reported this phenomenon to Best some weeks or months (as I recall) before he decided to conduct this ad hoc experiment on Curtis Henderson. I know this because i was a party to the correspondence.
Continued....
This Mickey Mouse operation results in perfusate that is at some (variable) subzero temperature when it is pumped through the perfusion circuit and delivered to the patient. While CI case reports are chaotic and inconsistent - some report temperature data during perfusion (http://www.cryonics.org/reports/CI97.html), some do not (http://www.cryonics.org/reports/CI75.html) - it is clear that even with the practice of pre-cooling the VM-1 perfusate in a freezer before perfusing it, CI patients never (so far as I can determine from published case reports, see: http://www.cryonics.org/refs.html#cases) reached subzero temperatures of -7 degrees C throughout VM-1 administration and in fact rarely reach subzero temperatures at all. This despite what CI says in its own description of how its patients are to be perfused with VM-1:
http://www.cryonics.org/research/CI-VM-1.html
"The Cryonics Institute protocol for perfusing the heads (brains) of cryonics patients is a 4-stage stepped open circuit perfusion:
(1) blood washout with carrier solution (4ºC) (2) 10% Ethylene Glycol (4ºC) (3) 30% Ethylene Glycol (4ºC) (4) 70% CI−VM−1 (−7ºC)"
I would also note that in the same document, it is stated that the positive research results achieved with VM-1 in rats were achieved only under these conditions:
*"To test the toxic effects of CI−VM−1 (with or without ice blockers) hippocampal slices were saturated with increasing concentrations of ethylene glycol at 0ºC and −7ºC before cooling to −20ºC for ten minutes of saturation with CI−VM−1 (with or without ice blockers). The DMSO in CI−VM−1 is less toxic at lower temperatures, and is least toxic when introduced at −20ºC. Adding the ethylene glycol first and cooling at 0.3ºC/minute ensured that the solution would not be frozen at −20ºC when the CI−VM−1 (with or without ice blockers) is introduced. The results of the toxicity test were as follows:
86.1% viability +/- 5.8% for 55% concentration CI-VM-1 without ice blockers 89.6% viability +/- 6.2% for 52% concentration CI-VM-1 with ice blockers*
Refractive Index values only taken during CI−VM−1 perfusion
CI Patient 97: http://www.cryonics.org/reports/CI97.htm
TIME (AM) TEMP (ºC) Flow rate(liters/minute) Pressure mm Hg RJVRI LJVRI
1:11 3.2 1.13 127
1:14 3.8 1.06 131
1:20 5.5 1.36 120 1.3976
1:26 7.0 1.07 117 1.3986
1:30 5.6 1.32 103 1.4017 1.4167
1:35 4.9 1.4048
1:37 4.1 1.4258 1.4242
1:40 3.5 1.4043 1.4183
1:45 2.5 1.4137 1.4209
1:47 2.0 1.4153 1.4224
1:50 1.6 1.15 139 1.4207 1.4236
1:52 Upper Body Perfusion Halted
2:00 Lower Body Perfusion Begun
2:00 0.5 0.42 121
2:03 0.5 0.32 136
2:05 0.5 0.32 134
2:10 0.5 0.31 143
2:13 0.5 0.40 200
2:15 0.5 0.46 185
2:20 0.5 0.46 175
2:25 0.5 0.48 191
2:33 0.5 0.48 174
Lower Body Perfusion Halted
Dry Ice Slurry Added to Head
2:37 −2.0
Refractive Index values taken during CI−VM−1 perfusion CI Patient 91: http://www.cryonics.org/reports/CI91.html
TIME (am) TEMP (ºC) RJVRI RBHRI LBHRI
9:35 7.0 1.4084
9:38 5.4 1.3655
9:40 4.2 1.4169
9:42 3.7 1.4198
9:46 2.1 1.4041
9:48 1.7 1.4138
9:50 1.8 1.4194
9:53 1.5 1.3721
9:55 1.1 1.4239
9:57 0.6 1.4206
10:00 0.4 1.3809
10:02 0.4 1.3830
10:07 0.7 1.4229
10:09 0.7 1.4233
10:11 0.6 1.3959
10:15 0.6 1.3971
10:16 0.8 1.4046
Continued....
This is a remarkable statement from Ben Best, and one that perhaps speaks best as to why CI is not a cryonics organization being run on a rational, scientific,or evidence based basis. When Ben Best writes: "There is no incompatibility between DMSO and PEG. The PEG make the solution hyperoncotic as the expected. My big mistake, and it was a bad one, I acknowledge, is that most of the vitrification solution was ruined because I was not aware that PEG would come out of solution when placed in a freezer," he is making a statement that has the following outright errors, misunderstandings or distortions in it:
First, DMSO and PEG are incompatible in that they cannot be used either safely or effectively under the conditions required to carry out cryoprotective perfusion in a clinical (or research) setting AS PRACTICED BY CI. The first fact to consider is that DMSO-PEG solutions will often undergo gel formation when cooled to temperatures above freezing if left under refrigeration long enough. This phenomenon has a variable time course and is akin to nucleation and freezing in supercooled solutions - such mixtures may remain clear for days, or undergo precipitation/gel formation within hours of cooling.
Second, the perfusate in question, VM-1, is designed to be administered at a SUBZERO temperature (-7 degrees C) in order to minimize toxicity. The final concentration of cryoprotectants in VM-1, a roughly equal mixture of DMSO and ethylene glycol (the latter is the principal ingredient in automotive antifreeze) and has a total concentration of these two agents of ~ 70%!
In the brain tissue slice experiments performed by CI's researcher Dr. Yuri Pichugin who invented VM-1, this very high concentration of agent was not introduced until the temperature of the brain tissue was -20 degrees C! CI's own protocol for human cryonics patients calls for the introduction of VM-1 at the lowest possible temperature that they can achieve (~ -7 degrees C), given that they have no heat exchanger in their patient perfusion circuit. The way CI attempts to get the temperature of the final pass of VM-1 below 0 degrees C, and as close to the ideal of -20 degrees C as possible, is by the expedient of placing bottles containing the perfusate into a standard household-type freezer. The pre-chilled bottles of perfusate are then loaded into picnic chests and the perfusate is dispensed from there.
Continued....
Brian, when you say: "Mike, let's be fair about this. Veterinary surgeons for thoracic surgery (after loss of Jerry Leaf) and chemists for running perfusion machines were also used during your tenure managing biomedical affairs at Alcor two decades ago. You trained and utilized lay people to do all kinds procedures that would ordinarily be done by medical or paramedical professionals, including establishing airways, mechanical circulation, and I.V. administration of fluids and medications. Manuals provided to lay students even included directions for doing femoral cutdown surgery," you are either not reading what I wrote or are not being fair yourself. I not only acknowledge that this was so, I go so far as to say it is completely acceptable with the caveat that such people are instructed, vetted and mentored properly. I'll go even further (as I have repeatedly, elsewhere) and state that the most highly qualified medical personnel can be dangerous, or even worse than useless unless they have been trained and mentored in human cryopreservation as a specialty. There's nothing remarkable about this; no reasonable person would want a psychiatrist or a dermatologist doing bowel or brain surgery.
Some of the same people who performed very well in the past, and who are not medically qualified, are still at Alcor. The individual people, per se (in this instance), are not the problem. Rather, it's the absence of the paradigm of cryonics as a professional medical undertaking that's missing. The evidence for that is present in Alcor's own case histories where highly qualified medical personnel do things like discontinue cardiopulmonary support on still warm patients in order to open their chests for cannulation (http://alcor.org/Library/pdfs/casereportA2435.pdf) or drill burr holes without irrigating the drilling site with chilled fluid to prevent regional heating of the brain under the burr. We are in complete agreement on these issues, as far as I can tell. Where we apparently differ is on how to resolve them.
The most interesting thing to me about this post from Brian is information it communicates for the first time. I follow Alcor's announcements, read its magazine and track its public blog, as I necessarily must, so I am surprised to learn that "In Alcor's O.R., Alcor is presently evaluating and training two board certified general surgeons to supplement the veterinary surgeon and neurosurgeon who have been used by Alcor for the past 15 years." This is the kind of information that I would expect to see showcased in the organization's literature and on its website, not disclosed here. This is the kind of thing that happens over and over and which degrades member confidence in the transparency of the organization. The next question is, who what, where and how? What are the details of this training? What kind of model is being used? What are the results to date?
Yes, SA does use pigs for training, but they use them in a non-survival mode - they get no robust feedback about errors, and no new insights. In fact, Brian might have mentioned that Alcor has used both animals and human cadavers in this manner, but I think he understood that the point I was making was about vetting your skills in an outcome driven fashion. That is not being done.
What's even more disturbing is that there is virtually no visibility into the outcome from even these training operations. SA and Alcor are both essentially black boxes - there is no data, no performance reports, not even any reports or internal scoring of how well simulated cases proceeded. There's at least one reason for this, and that is that there is no scoring system, internal or external. When things go wrong, well, it's oops, we shouldn't do that next time. And if that isn't the case, then I'd love to hear it and I want to see the data to document it. That is an eminently reasonable request.
It's great that Alcor can sometimes mount skilled perfusionists and highly skilled emergency vascular surgeons. But that isn't the issue. The issue is the framework of knowledge, understanding and consistent performance that is absent. A surgeon or a perfusionist are, absent mentoring (internship), TOOLS to be used by and within that framework. If a man tells me he has the best glass cutting tool money can buy, but he doesn't know how to cut glass, well, I'm going to be underwhelmed.
Alcor patient case reports are disorganized, inconsistent and erratic narratives that make objective evaluation impossible. No great genius is required to consistently collect and organize the key data that define how well a case went - or didn't. The first cryonics case report was done by a 17 year old and a 22 year old graduate student:
http://www.lifepact.com/images/MTRV3N1.pdf
Examples of competently executed cases and case reports are available on Alcor's own web site and the data captured, reduced and presented in these case reports was achieved using a tiny fraction of the financial and personnel resources Alcor currently has available:
http://www.alcor.org/Library/html/casereport8511.html
http://alcor.org/Library/html/fried.html
http://alcor.org/Library/html/casereportC2150.htm
http://alcor.org/Library/html/casereport8504.html
LOOK AT THESE CARE REPORTS CAREFULLY and then look at those on the Alcor website from 1997 forward: http://www.alcor.org/Library/index.html#casereports
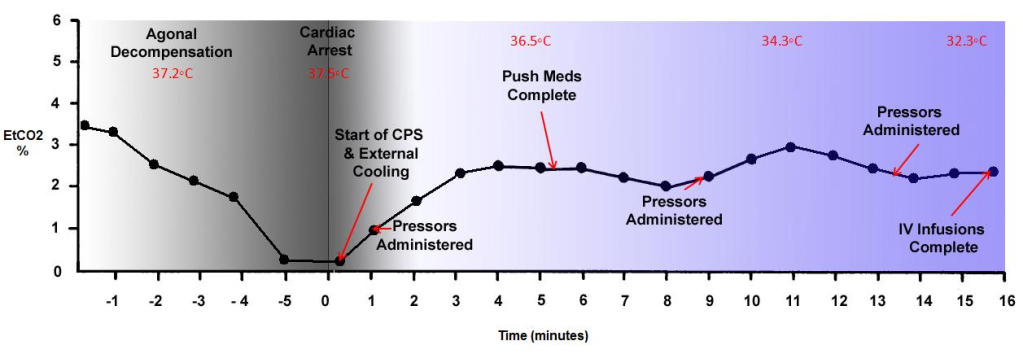
I'm not trying to be contrary, difficult, or unreasonable. What I am asking for is core competence, not perfection. There is nothing either exotic or impossible in that. For example, Alcor has a Novametrix CO2SMO capnograph and respiratory function analyzer. The device can effortlessly capture and write to disk over 60 different respiratory parameters and it measures the end-tidal expired carbon dioxide (EtCO2) in the patient's breath. The EtCO2 is the gold standard for determining how effective cardiopulmonary support (CPS) is. And if CPS is not effective, than that is both additional ischemic time the patient is experiencing and it is an opportunity to intervene and fix the situation. Or at worst, it offers the possibility of learning what caused inadequate CPS so that it might be avoided next time. The only skill required to use the device is to put the walnut sized sensor in line between the patient's airway and the ventilator on the LUCAS CPR machine: http://frankshospitalworkshop.com/equipment/documents/pulse_oximeter/user_manuals/Novametrix_8100_-_User_manual.pdf That should make it easily possible to produce graphic data like this:
http://i293.photobucket.com/albums/mm55/mikedarwin1967/EtCO2inCPSgraph.png
{kind=link}
THAT kind of data speaks definitively to how that patient was stabilized and transported, and in aggregate it provides a statistical dataset that speaks to the overall performance of the organization. It should be accompanied with graphic data for the patient's TEMPERATURE, mean arterial pressure (until the time of arrest), the SpO2 (pulse ox) and other relevant data. This was done in the past by stressed out, sleep deprived, mostly volunteer people who were trained in-house. If that kind of data collection and accountability are considered "perfectionist," or some kind of golden past no longer to be achieved, then I restate my opinion that something is terribly wrong.
Paramedics are taught that the single most important and most critical indication of the efficacy, or lack thereof, of CPR is the EtCO2 of the patient over time. Where is this data???? This is only one of countless examples I could use - but it is especially relevant because it is simple data to collect, and I know from Alcor's recent case reports that they have a CO2SMO and they are actually using it on patients during the peri-arrest hospice period. Again, where is the data? That data is the ONLY way anyone has to evaluate the quality of cryonics cases because the patients cannot speak to us.
If you want to stop my criticisms, you need only show me the data and offer me and everyone else the opportunity to be reasonably certain it is valid and representative.
My comments about economic, social and political matters don't speak to how people should invest in the market, or to who will win the coming election. They speak to the general condition of the economy and the culture over the long haul. As I've observed in print before, plenty of people will get rich, and millions of people have gotten richer, despite the fact that diversion of wealth from the people who primarily produce it is at an all time high. I am the first to acknowledge that it has been fantastic advances in productivity that have made this possible. But that doesn't make the reality go away that the system is increasingly thwarting innovation, overspending its resource base, and appropriating vast amounts of wealth which is used inefficiently, is wasted, or is actually used for contra-productive purposes.
All I have said, in addition to these fairly mundane observations, is that, sooner or later, something's got to give. To some extent this has already happened in that many trillions of dollars of wealth have disappeared, or been reallocated to cover "bad actions" of various kinds. The situation in Europe is actually much worse than it is here, and if it becomes impossible to maintain solvency of large EU nations such Greece, Italy and Spain, then the effect will, again, be felt in the US and elsewhere.
What I have no way of knowing is how much "re-assignable" wealth is present in the system - and just as importantly, if it will be reassigned to cover "bad acts." That' difficult to assess wealth covers a huge range of goods and actions, from the quality of food people eat, to whether they use paper towels or go back to using rags! I've never claimed any special insight in those matters, and for good reason; because the data to make those kinds of "forecasts" simply isn't available.
So, my position is very much like that of someone who warns that "crime doesn't pay." It doesn't - not in the long run, because it is destructive of productivity, and destructive of effective human social interaction. But the BIG question is, what exactly constitutes the "long run?" That's not a joke, and I am mindful that the Soviet Union ground on for 70 years. That's an economist's eternity, and then some. Pepsi Cola made millions betting that Soviet Russia would continue for decades. Do I think Fidelista Cuba is doomed? Absolutely. I also think it is a miserable, oppressive place. But I wouldn't care to give any odds on how long it will survive.
Finally, if all the "non-contrarians" on this matter are concerned with or about is financial gain, regardless of the system's characteristics or "meta-qualities," then I have nothing to say to them and their disappointment in my "judgment" is as understandable as it is mutual.
Umm, here's a suggestion: WHY DON"T YOU JUST ASK ELIZER HOW AND WHY HE MADE THE DECISION? Why speculate?
This post from Max More is the kind of post that I would expect to see voted off of LessWrong. I have not had a substantive conversation with Max More about cryonics, let alone my personal position, psychology, desires or motivations in over 20 years. We did correspond recently, and I have asked Max for permission to make that complete correspondence, minus personal incidentals not material to cryonics, public. He has flatly refused. Why, I do not know, but I do know that that is the only substantive communication he and I have had in decades and that it is completely documented in writing. Prior to that, at least to my knowledge, our relationship was cordial and not marred by any disagreements or conflicts. Nor do we have any confidants or intimates in common. Thus, the question arises, how would Max know anything about whether I am "envious that I'm not running things"? As he says, he doesn't know this, he can only speculate because he has refused to speak with me on these matters.
He then goes on to say something that I find remarkable to be left unchallenged here on LessWrong:
"That depth (of knowledge) and his most excellent writing skills often fool people into believing that his judgment is better than it is"
LessWrong, as I understand it, is a forum where people are mastering the craft and science of evaluating the logic and substance of the arguments put forth by people, including thinkers and writers here and elsewhere - not based on their style, cleverness of articulation, or their speculations. If anyone has questions about the assertions I make, feel free to ask for the evidence. We may not always agree on how to weight it, but the evidence will (hopefully) always be there, and it will be credible. Where I overstep or make a mistake, you will find me quick to acknowledge and apologize.
The first question you need to ask Yudkowsky (and yourself) is a damned difficult one to answer "simply," and that is what are the currently well known, well understood, and well documented BIOLOGICAL differences in outcome that are likely to pertain using the two different approaches in the reasonably optimum case. Reasonably optimum means that the member is experiencing medico-legal death under controlled conditions with competent cryonics organization personnel in attendance, My bet is that only a few people on the planet can answer that question, and that Yudkowsky isn't one of them.
Of course, if you do not believe the degree of molecular, histological or gross damage to the patient matters, within broad limits, then such differences are immaterial. For instance, if you think that several hours of warm ischemic injury, followed by 12 to 24 hours of cold ischemic injury, followed by reperfusion injury, followed by grossly inadequate cryoprotective perfusion/equilibration in the brain resulting in large areas of massively ice injured brain tissue will be easily repairable with Nanotechnology, then you will be largely insensitive to the differences between Ci and Alcor, or a well done cryoprotective perfusion and a poorly done one.
My question for such people is, "Why bother with perfusion at all? The ischemic delays are very damaging. Why not just have yourself packed in dry ice as soon as you are pronounced and get shipped off to CI? It would be about $10K to $15 cheaper and you'd only be faced with Nano-repair of cryoinjury?" No need for Nano, Nano, one Nano will do.
I'm in the final stages of preparing Part 3 of THE EFFECTS OF CRYOPRESERVATION ON THE CAT for publication on Chronosophere. Part 3 is the transmission electron microscopy of the tissues under different conditions of cryopreservation (Part 2 was the histology: http://chronopause.com/index.php/2012/02/14/the-effects-of-cryopreservation-on-the-cat-part-2/). You can look at those pictures of cell and tissue structure and decide for yourself which condition you'd rather be in.
Yes, unquestionably some of the "information" that constitutes your person hood is in your gut, your glands, your immune system and your peripheral nervous system. However, your position would seem to imply that these things, and things much more central to your identity, such as your brain structure, are like unchanging books or artifacts on a museum shelf. They aren't. In fact, by the time you are 80, you will have lost roughly a third of your brain mass and your brain will be a tattered "remnant" of what it once was. You're now losing roughly 80K neurons a day. The practical consequences of this will be a massive transformation of your personality and of your functional capabilities. If that change were to be imposed on you all at once, you would not only be horrified, you likely wouldn't even recognize the resulting individual as the same person. More likely, you'd consider that individual to be a cruel and sadistic parody of yourself.
The point is that your "identity" is a dynamic thing which is badly degraded over time by aging. This is important information to keep in mind, because it provides context for what I'm going to say now. I have known a good number of people who have no stomach or intestines. They could not eat food of any kind. They stayed alive by virtue of total parenteral nutrition (TPN) which provides for all their fluid and nutritional needs intravenously. These people did not undergo any perceptible change in memory, personality or person-hood. At least three such people I've known have also had kidney transplants. That's even more interesting, because we now know that many patients with successful, long term grafts become chimeric with the donor! Donor immune and stem cells colonize the patient! Similarly, any mother is chimeric for each of her fetuses. In fact, in animals, if you injure the mother's heart or brain during pregnancy, the fetal stem cells are the ones which repair the damage - massively remodeling the damaged organs. This chimerism seems to be an evolutionary adaptation to protect the mother against injury during pregnancy.
To my knowledge, no one is upset at the idea that a significant fraction of the stem cell population in such people is ALIEN. And those stem cells are genetically and functionally different from the native ones. Maybe more than the gut, the immune system is an extension of the brain - they interact dynamically and the immune system can and does profoundly effect mood and behavior.
So what is identity? Well, that's complicated, but one thing is clear, it is NOT static and a lot of the changes in the structures which determine it happen all the time as part of life, and you have little or no control over them. Where this intersects whole body vs. neuro is that you have the need (arguably the necessity) to decide just what parts of you are truly essential to your person-hood AND at what cost in risk to survival they can be taken along during cryopreservation.
If you are smart, cool, and rational, you'll try to determine just what parts of you are really you - are really essential to your person-hood. This would be an impossible black box of a task were it not for contemporary transplant and artificial organ medicine. There are tens of thousands of people on dialysis or who get kidney transplants. There are people with no hearts, or new hearts, and people with gut, liver, pancreas and renal transplants. There are countless people with bone marrow transplants and countless others whose spinal cord and peripheral nervous system have been functionally disconnected from their brains. Do these people constitute an acceptable degree of survival for you as persons? If so, I would suggest you delve into the logistics, economics and hard practical realities of cryopreservation that must endure over a period of many decades, or far more likely, a century or two. It is NOT easy to handle, move or care for whole body patients. They are a ball and chain and cannot be moved or evacuated quickly. They are subject to a large burden of state regulation which neuros are not, and they suffer additional injury to the brain as a result of compromises necessary to achieve cryoprotection and cooling.
If you think that those components of you identity present in your body are worth those added risks, then you should go whole body. However, my question is, where is the empirical evidence to support that belief? I've known many, many transplant patients well, and neither they nor I saw any noticeable transformation in their identity. Indeed, the transformation, such as it was, was the return to fully functioning person-hood which resulted from becoming chimeric with another human being or a machine.
No, and that's the trouble! Because, you see, if cryonics were like any other medical procedure, I'd simply point to the STATISTICS and to the MAIMED and DEAD patients. In fact, the errors and screw ups would be a huge public scandal, because people would have SUFFERED and DIED. Indeed, the patients themselves (who were not killed outright) would be hollering to high heaven via every available media outlet. Cryonics patients never complain because they can't.
Because no cryonics patient suffers, or dies, or experiences any other OUTCOME of any kind, your only choice, if you want to understand differences in procedures, quality of care, and so on, is to delve into the complex, technical specifics.
You don't have to learn the details of automotive engineering, metallurgy, and so on, to go pick out a good automobile. All of that huge body of technical and scientific knowledge is effectively INVISIBLE to you as a consumer (as well it should be) because you can look at PERFORMANCE as your guide to making a good buy. All that science and engineering gets reduced to miles per liter, road reliability and, of course, your comfort, convenience and safety while driving it! So "close" are the performance specs between automobiles that a significant part of what makes therm sell and out-compete each other is styling - just how the damn thing looks!
Think about that.
The major problems at Alcor are truly abysmal management, for which the Alcor Board of Directors is to blame, and lack of a professional culture and staff to administer the front end of cryopreservation. The situation is almost identical to one that would exist if the board of directors of a hospital tried to deliver medical services without physicians and nurses, but rather hired "the best they could find" to do these professionals' jobs. Thus, there might be a veterinarian doing cardiac and neurosurgery, a chemist operating the heart lung machine, and so on. The absence of credentials, per se, is not the core issue here, because it is perfectly possible for such individuals to do these tasks and to do them "reasonably" well.
Because cryonics did not become a mainstream medical, industrial, or business activity, it necessarily is in the realm of very small "visionary enterprises," like the early days of flight or radio, or perhaps in the realm of the dedicated (professional) amateurs. A good example of the latter is amateur astronomy, where the people involved are fantastic - mostly level headed, focused, responsible and astonishingly capable. Amateur astronomers have made more brass tacks basic discoverers of heavenly bodies than their professional counterparts, and they have made major contributions to the fundamental science, as well. There are essentially no kooks, and their equipment and facilities are often spectacular and demonstrate fabulous innovation and engineering skill.
The barnstormers at the start of flight were "crazy," extreme personalities, but the fact that they had to fly and thus had to work with real machines which could CRASH and KILL them, kept them on track. However, a careful observer of their history will note that their mortality rate was terribly high. Those that survived barnstorming and doing air mail runs were, in effect, a "filtered product" who represented the best of practical skills, engineering ability, risk taking, and bad-ass courage. In that respect, Lindbergh and Fred Chamberlain had personalities that were extraordinarily similar.
I've had considerable contact with HAM radio clubs and amateur astronomers and there is simply no comparison to cryonicists. Ditto for the pioneering ultralight aircraft guys of 25 years ago. If you spend any time around these kinds of groups, you quickly see that they attract as many dysfunctional, narcissistic personalities, as does cryonics, but 99.9% of the time these people flake away, almost instantly. In the HAM groups it happens during the run up to getting your basic license. It doesn't matter how much physics you know, or how smart you are, most of the test is FCC regulations, proper jargon, and things that you must memorize. The loonies flee!
Having said that, it's been interesting to watch the quality of amateur radio enthusiasts plummet in recent years. This is because the equipment is now all solid state, it is much less expensive, and the days of building you own radios from parts are over. Also, the requirement for Morse code was dropped from the entry level licensing exam.
If you, or I, or anyone else looked at a TV set, or an MP3 player, or even a modern HAM radio and said, "I'm going to build one of those; I can do it just as well as Samsung and much less expensively," we'd likely all just laugh and figure the poor guy was crazy. Nobody tries to do that because it is stupid, just like no one in their right mind says, "My wife needs open heart surgery and those bastards at the Medical Center want $50K to do it! That's ridiculous, I've seen it done on TV and my brother in law is a veterinarian, so we're going to do it ourselves." The hubris required to take such an action, let alone the lack of commonsense, is just indescribable.
Now, if your wife needs surgery, you cannot possibly find a doctor to do it, and you think you can learn the craft well enough to give her fighting chance, well that's another matter - depending upon how you go at it! If you have 5-6 years to prepare, you're willing to do the work and you're willing to kill a LOT of dogs, you can indeed teach yourself the basics and perhaps have a 25% chance of pulling it off - providing it is a SIMPLE surgical procedure that she needs. You can actually do this from books, journals and lots of failed attempts in the "dog lab." When I was kid in the late 1960s, several teens a little older than me (15-16 years old) actually set up and did do cardiac surgery in their garages on dogs, and the animals survived! They built their own heart lung machines (HLMs). Today, such an action would be illegal and it is impossible to imagine teenagers building their own heart lung machines! But, in fact, this really happened.
The first practical HLM was built by the maverick surgeon C. Walton Lillehei, and a colleague, Richard Dewall . Lillihei was the archetype of the founder of almost any daring new profession (in this case, cardiac surgery): he was brilliant, courageous - just an incredible man. He started doing open heart surgery BEFORE the HLM by using another human being as the HLM in a technique called "cross circulation." He'd hook up a volunteer to the patient and use the volunteer's heart and lungs to support the patient while he operated. This was brutally controversial at the time and, of course, eventually one of the volunteers died due to a technical error in the OR! It was almost the end of Lillehei, and he barely escaped criminal prosecution. I mention Lillehei because his first HLM was built from a commercial "finger" tubing pump, with the oxygenator made from PVC beer tubing, a cheap glass frit, some stainless steel pot scratcher pads, and other odds and ends. Their total cost, excluding the pumps, was ~ $15.00: http://i293.photobucket.com/albums/mm55/mikedarwin1967/m8jpg.jpg
{kind=link}
It worked brilliantly and was the design template for every HLM up until bubble oxygenators were replaced by membranes in the late 1980s. Now, if you look at the machine in that picture, it is something that anyone with a modicum of hand-skills could build. The pumps were standard, off the shelf industrial finger-pumps used in the food processing industry. So, a kid with some bucks really could build his own HLM - in fact, he could do it today. The difference is, as I previously pointed out, is that he'd be hauled off to jail if he tried to use it. And if you can't use it, why build it?
However, if you really want to master (simple) basic cardiac surgery, it will cost you a fortune in time, equipment, animals and supplies. The only way such a situation would make sense is if you were in a world where there were lots of doctors, medical supplies, equipment and so on, but you and your wife were banned from access to them. Your money wasn't any good and you had to "operate underground," literally. That's the situation cryonics was in and still is in, to a great degree.
The critical difference is that there is today in cryonics no perceived need to "get it right" with animals, or any other feedback-driven test system. It's like the guy I describe above who just decides he and vet brother in law will show up in the garage one day with whatever their idea of what is needed is, and they'll simply operate on his wife! But wait, what happens if they do that? Well, pretty clearly it will be a HORRIBLE MESS, not only will the wife die, but it will be a gruesome fuck up - just unimaginably bad - worse than if she were murdered with an ax. Then what happens? Well, they go to jail, there will be a huge outcry, it will be front page news. In short, they will get subjected to the CONSEQUENCES of their stupid and irresponsible acts.
However, if you are "freezing" your wife, well, who knows how it turned out? Who cares? She looks great! You feel real good about it! And if she does thaw out and rot, well, she was dead anyway, right? So, no harm and no foul. Certainly there are no social or legal consequences for any errors, oversights or failures. There isn't even any way to KNOW that such things might have (or indeed did happen).
THAT IS CRYONICS.
And when good quality people do come along, or people who sincerely want to put their money into cryonics, there is always some damned fool who will tell them how easy it is, how much more quickly THEY will show them results, and on and on and on. If you were doing anything else; running a dog food company, or making women's' handbags, you couldn't get away with that, because the product wouldn't sell and you might even be in court for killing peoples' pets with tainted food. But, not so with cryonics...
Cryonics came reasonably close to crossing the threshold into professionalism with Alcor in the 1980s, but that effort imploded. Jerry Leaf was cryopreserved and I left to pursue more conventional biomedical research (a terrible mistake, in hindsight). Absent a well defined and well established culture of professionalism that included self-correcting feedback mechanisms, Alcor fell back to become something broadly similar to CI. Instead of functioning as a hospital board of directors does, Alcor's Directors became de facto managers - arbiters of the technical details of care, by default. This has been a disaster, not only for those receiving such care, but because Alcor (much more than CI) now serves as a spolier to professionalism. The high tech veneer and the appearance of biomedical competence short circuit any perception that something is seriously wrong, and that things were once, and could again be, much better.
There's no mystery about why I have comparatively few criticisms posted about CI. My reasons for this are as follows:
1) Ci is what it is. What you see is pretty much what you get, and that this is so is evident from the discussion here. The perception of CI as a "mom and pop" outfit is but one example I could cite from this discussion. Ci does not project itself as using a medically-based model of cryonics. It's case histories are ghastly - and anyone who doesn't take the time to read them, or who can't see what the deficiencies are, well, you can't (as I've learned the hard way) fix clueless.
2) I am not a CI member. The reason I am not a CI member can be divined from my written criticisms and by looking over point #1, above. If I were a Ci member, I have no doubt that I would have posted reams of criticisms. Note that I said "posted," because, in fact, I have written reams of criticisms, suggestions, detailed technical advice and countless letters and personal communications on specific deficiencies at CI. I have also generated Power Point presentations and written many pages of material on how CI could improve its capabilities. To their credit, CI has at least listened to these suggestions and critiques; and they are responsive to same. This is not imply that they are receptive. But at least they listen and engage in dialogue. Alcor does not.
3) Since I am not a CI member, and I do not believe CI materially misrepresents itself, or its capabilities, and because they have invited private criticism in the past, I see no need to discuss their deficiencies publicly, beyond the (comparatively) brief remarks I've made from time to time. What would be the point of going further? The only exception I can think of is when CI takes actions that could, or which do materially impact the operation of cryonics as a whole. Some examples of that would be their submission to regulation by the Michigan Cemetery Board, their practice of accepting at need cases absent any defined standards for informed consent, and their practice of having morticians freeze, and if necessary, thaw cryonics "bodies," whilst claiming that cryonics "patients" haven't thawed out since the 1970s.
4) Because Alcor represents itself as a medically-scientifically based cryonics operation I believe that it is not only deserving of the criticism it has received, but of much more. While the care Alcor patients receive is, on average, much better than that available at CI, it is still, in my opinion, grossly substandard, frequently marred by inexcusable iatrogenesis, and not in keeping with the highly professional and medically sophisticated image that Alcor projects on its website, in its literature, and via the media. If anyone is truly interested, I'm wiling to discuss specifics - and in detail. In fact, shortly I will be posting a piece about research priorities in cryonics, which should give some perspective on just how Less Right Alcor has become.
5) The problem is deeper than the specifics at Alcor, it is inherent in cryonics itself. A simple introduction to the root problem can be found here: http://chronopause.com/index.php/2011/02/13/on-the-need-for-prosthetic-nocioception-in-cryonics/
A much more detailed analysis of the problems that have beset and thwarted cryonics can be found here :
http://cryoeuro.eu:8080/download/attachments/425990/Cryonics_Failure_Analysis_Part_2v5.2.pdf
http://cryoeuro.eu:8080/download/attachments/425990/Cryonics_Failure_Analysis_Part_3v5.4.pdf
[Please note that the server hosting the two files above is sometimes unavailable - please try again if you aren't successful.]
This post http://chronopause.com/index.php/2011/05/29/a-visit-to-alcor/ provoked outrage from Max More and in private correspondence, now many months ago, he told me he was working on a response that would demonstrate my criticisms were in error.. Apparently, he is still working on it.
I've posted a more detailed explanation of the problems vis a vis Alcor and cryonics as a response to this post.
Melatonin has a very short half life and is secreted as needed by the pineal gland. It's apparent primary biological function is as a signal transduction/regulatory molecule. It's unclear if this function is what is responsible for its protective effect in ischemia-reperfusion injury (IRI), because melatonin is also a powerful radical scavenger - and in fact, a particularly effective scavenger of the radical species associated with neuronal injury in IRI, such as peroxynitrite. Other factors to consider are the timing, route of administration and dose used in our studies. The drug was given intravenously in a micellized form to speed delivery across the blood brain barrier. This was done at the start of reperfusion. Finally, the effective dose given was very large (and was based on the stoichiometry of the radical species we wanted to scavenge). The drug was also given in conjunction with many others and, perhaps critically, in combination with the rapid induction of mild therapeutic hypothermia ( 3 deg C below normothermia). Next up on my agenda to test was whether the drug combination was effective without hypothermia since it is very problematic to achieve a 3 deg C reduction in body temperature in ~15 min or less! Unfortunately, that study was canned.
The point here is that the application of any such treatment in the setting of a critical illness would require that it be both an integrated and ACCEPTED part of the medical infrastructure. For instance, it was over 30 years ago that Peter Safar, et al., demonstrated that mild hypothermia AFTER cardiac arrest was profoundly effective in reducing ischemic brain injury, and it has been 9 years since ILCOR made post-cardiac arrest hypothermia the standard of care: http://circ.ahajournals.org/content/108/1/118.full. And yet, post-arrest hypothermia is used almost nowhere. So, even if a treatment is approved and demonstrated to be scientifically valid, it still may not see widespread clinical application for a host of reasons.
Sorry, you've spent a lot of time trying to address things that really aren't problems. I was in no way offended, or put off. It's axiomatic, but worth noting yet again, that correspondence in writing is a dangerous way to communicate, because it lacks the context of intonation, facial expressions, and other non-verbal cues.
The best way to deal with errors in my writing, thinking or actions, real or perceived, is directly, matter of factly, and with only such tact as common courtesy requires. Public statements can be dealt with publicly, privates ones are best dealt with privately...
I think this will also save you time (when you are correct), because a succinct critique of an error is a hell of a lot less draining than spending time and energy crafting a convoluted, or overly polite reply. I do understand that this site is about a rigorous way of way thinking.
Finally, in reading your response, I realize that my comment about why I've posted here extensively recently, and am unlikely to continue to do so, may have been misinterpreted. It should be taken at face value as the literal truth. My primary obligations in terms of time, energy and writing must necessarily be elsewhere for the foreseeable future. This is just the way it is and it has nothing to do with LW.
Thanks for your letter - I know it took a fair bit of time to write and I really do appreciate it ;and I appreciate even more the sentiments expressed!
I'll try to keep my response brief:
1) I respect the desire for precision in the use of words, and I understand that each culture has its own nomenclature and rules.Those here that I have seen so far seem eminently reasonable.
2) I have no interest whatsoever (and haven't for many years) in persuading anyone to sign up for cryonics - including friends and family. While it is an understandable error, my purpose here is not to convince, proselytize, or recruit, but rather to identify minds that are useful to my current endeavor. They will not need persuasion - they will 'know the lion by his paw.'
3) Forgive my levity, but in urging mono-topical posts of short duration, you pointed me to three dissertations dealing with a range of subjects within each essay, the shortest of which was ~1,400 words and the longest of which was 2,700 words - not including commentary.
4) For the record, I use the word disease in the context your writer specified: as .something unusual, abnormal, and I would add, deleterious to the normal functioning and survival of the organism. I know little about computing and have even less aptitude to learn. I use the word malware as software that damages or destroys data that the computer's owner doesn't want destroyed or degraded. I would add that given my predicament, when that happens it is a complex, difficult and thoroughly unpleasant thing to sort out which generally requires my machine spend time in "stasis" until the appropriate expertise can be brought to bear.
5) My posts here have been mostly confined to the subject of cryonics and were never intended to continue. I've really enjoyed the discussion and I've found this an interesting and rewarding forum. Many thanks!
In looking over the comments here, there are a few missed points that I believe heavily shift the balance in favor of having cryonics arrangements. The first is that the need for "cryonics," in the generic sense, is never likely to go away. While it is true that we can currently envision technologies to repair all of the pathological processes we currently understand, that does NOT mean that we understand all of the things that both can, and will go wrong with us in the future.
Let's assume that aging is conquered tomorrow. Within some definite (but unknown) period of time you are going to fill up your hard drive - or your "soft drive," if you prefer. Humans were not designed to store thousands of years of memories and experiences. And we may be doing just that, if the people with Superior Autobiographical Memory are any indication. So unless you are happy with eventually losing most, or all of your current memories, something will have to change…
A likely consequence of this limitation is that we are going to have to reconfigure our brains. I use this very conservative example, because it speaks to the NECESSITY of doing this. Probably most of the people on LW envision, and even desire, vastly more daring reworks of their identity-encoding hardware and software. That will inevitably carry associated risk. It is very easy (at least for me) to envision major and very complicated screw-ups in cognitive re-engineering that cannot be easily or rapidly sorted out. In fact, this sort of thing happens today on a small, but nevertheless sometimes lethal, and not infrequently very damaging way, when people become psychologically confused, or "existentially damaged." A good example is when seemingly normal people get taken over by ideas, or become ensnared in cults. Is "deprogramming" a treatment, or coercion? Malware, either deliberately designed or accidentally created, which badly damages programs and data are yet another example. So, leaving hardware out of consideration, it seems likely that people will still get very nasty “software” diseases that do a lot of damage in a short period of time, and that require that the “system” (person) be shut down until a solution can be found. Nanotechnology will not solve this problem because the problem is a meta-problem that is intrinsic to complex systems interacting in an open universe.
I also think it will also be a long time, if ever, before damage to "hardware" substrates becomes 100% repairable 100% of the time in REAL TIME. As long as it is possible to envision pathologies that render the individual into a degraded and nonfunctional state, which current technology cannot reverse, then you will need cryonics, regardless of what it is subsequently called or what preservation technology is used.
My next point is that there are a couple of implicit assumptions in the foregoing arguments which are demonstrably not true. The first is that cryonics is a discrete, consumable product, like a bag of crisps, a candy bar, or even a computer or a radio. Or that it is like an automobile maintenance contract, or an insurance policy that pays off when you need it.
It isn't.
All of those products and services can be assigned, with a high degree of precision, a probability as to how they will perform and what your likelihood is of being satisfied with them. They are fully developed products. And mostly, all you need to know about them is present, free for the asking in your culture in the form of "common knowledge," information from friends and family, and, of course, in advertising. You pay your money and that's it. Nobody needs to explain to you, or to or anyone else what a TV or broom are for, how to use them, and what might go wrong with them over time.
This is no way describes cryonics.
So, the first benefit you get by signing up is that you now have a proprietary interest in learning what it is that you just bought; and you will soon become aware that you need to KEEP LEARNING, because cryonics is an undeveloped, immature, and above all, experimental technique. I signed up with the Cryonics Society of New York (CSNY) when I was 15 years old. CSNY is long, long gone and I've been signed up with 2 other organizations that have vanished. If you can’t keep learning until old age or “death” overtakes you, you are unwilling to do so, or you are an idiot, then cryonics is not for you.
And because cryonicists are the most rabid and intense of the life extensionists, you will also soon learn that they are at the absolute edge of emerging science in this area. In other words, you stand to be the first to know about newly developed and developing technology to combat aging. That can either “kill you or cure you, “depending upon how good your judgment is.
Finally, non-cryonicists, because they have the view of cryonics as a developed product (like an automobile or a light bulb) have a similarly inaccurate and warped view of the odds. The odds of the Titanic sinking with the loss of 1517 lives were 100% on 15 April 1912. But, what if the Titanic were to have taken, say, 48 hours to sink? Depending upon how the passengers and crew behaved in that interval, the number of survivors might have gone way up, or way down.
There were a lot of smart people on board the Titanic - very clever and very inventive people. But they were panicked, they were dealing with a panicked mass of passengers, and they had very little time to react. Given 48 hours, and the willing participation of the best minds aboard that ship, how many people need have died, or would have died? Were there ways, other than the optimal loading of the inadequate number of lifeboats that would have saved lives? Would clothing those passengers consigned to the icy sea in multiple layers of clothing saturated in grease, shortening, or oil, attaching them to life-ropes, and rotating them in and out of the lifeboats, have saved additional lives? What kind of makeshift lifeboats or floating platforms could have been made on an expedient basis from materials on the ship, allowing additional passengers to remain afloat out of the freezing water?
THAT is the position of cryonics and cryonicists. The odds are not fixed to those calculated at any given point in time, because you are NOT carting off a discrete product to screw into your lamp, or to process your words, or to play your games on. YOU set the odds of success or failure to an amazing degree. [You also do this, to a tiny degree, for the success or failure of the company that you buy a light bulb or a computer from.] Cryonics is thus an ACTIVIST proposition. Customers can, of course, be customers if they insist. But in cryonics, as in any other market transaction (perfected or experimental) you get what you pay for. In the case of cryonics, the fees required for success are not even remotely reducible to cold hard cash alone. It’s going to all the composure, good judgment and raw intelligence we can muster to escape the sinking ship fate has consigned us to and make it that far shore where we can continue our journey through life, indefinitely.
I can't speak to your situation, per se. I can only tell you that in my experience (managing and marketing in both the for-profit and NPO sectors), comprehensive demographic information was very valuable. Since I don't know the agenda of LessWrong in detail, I can't say if, for instance, knowing the income distribution and the markers for charitable giving amongst LessWrongers would be of use. These typesof data help you to define the kinds of projects you can reasonably hope to fund, and thus reasonably hope to market to your demographic. Markers for giving were very reliable in my experience - today, given the economy, I don't know.
Beyond money, a well constructed survey will almost invariably reveal all kinds of insights, not just about your members, customers or readers, but about your own operation - how it is perceived, what people like but aren't getting, and sometimes, insights into your own psychology and approach that you didn't previously have. The key words here are "well designed," because it is surprisingly hard to do a comprehensive survey and get most of the questions you that you want answered, answered. And to avoid bias in the way the questions are phrased, or even in the order in which they appear in your survey. While I can't prove it, I think it likely that intelligent use of survey information, gathered in the 1980s, was in part responsible for the brief period when Alcor membership growth was nearly exponential. While such data will never do that for you absent many other things being done "right," they can, IMHO, amplify the effect of good management and marketing.
I'm not sure if this comment will stand for long here, because the questions I'm about to ask are probably mostly of interest just to me.
Christina, wen you say you'd be more interested in funding "life extension research,"(LER), I'd like to know what your vision of LER is, specifically? What kinds of technologies do you think realistically offer you a chance at indefinitely, or even moderately extending your healthy lifespan? When do you think they might be available, and with what restrictions (if any) and at what likely cost? How long do you think it is likely that advances in LER will be able to extend your lifespan - including as incremental bridges to increasingly better technologies? Finally, how much of your income are you currently contributing to LER, and if I could ask, to what kinds of LER are you contributing money?
Many thanks. I'm really quite interested in the answers to these questions.
As an aside, I'd be fascinated to conduct a comprehensive survey of lesswrong members to establish the demographics not just with respect to cryonics and LE, but across the board, and in a robust way.
Frankl didn't provide a nomenclature. His book was useful to me because it alerted me to what I was (and am), and also offered a reasonable explanation of the nature of so many of the people I found myself involved with in cryonics. Frankl observed that those people who lived independently, not just independently of the labels others put on them, but also of their roles and purpose (internal as well as external) in their social world, had in common a certainty of purpose and meaningfulness in their lives. For Frankl, those things were god and love - principally love for his wife. But this was clearly not the case for many others who survived. Their purpose might best be described as an imperative to always live and grow, and to gain knowledge and experience. A purpose that was rooted in the very nature of their being, or in their experience of reality. For whatever reason, these people understood that there is no universe without me, and that because I know from experience that life can be good, I must continue and pursue more of it. Frankl was not thrilled about this cohort, and he famously remarked, "The best of us did not survive." Frankl has little to say to me beyond the message that such people exist, that an unshakeable sense of purpose and joy in living is essential to indefinite survival, and that people who draw their purpose and identity from what they do, where they fit into their family or society, or on the basis of their rank or achievements, quickly die when these things are taken away from them. I think that's quite a lot for being so little of what he otherwise has to say in the book.
You are not wrong about "freeloading," though that term is probably (unnecessarily pejorative). The Developed world is so obscenely wasteful that it is not necessary to beg. You can get all the food you want, much of it very nice - often much nicer than you could afford to buy by simply going out and picking it up. Of course, you don't get to pick and choose exactly what you want when you want it.
Clothing, with the exception of jeans, is all freely available. The same is true of appliances, bedding and consumer electronics of many kinds. The one commodity that is is very, very difficult to get at no cost is lodging. You can get books, MP3 players, CDs, printers, scanners, and often gourmet meals, but lodging is tough. The problem with housing and why it is qualitatively different that the other things I've cited is that while it is technically illegal to dustbin dive, in practice it is easy to do and extremely low risk. It is incredibly easy in the UK, if you get a dustbin key (easy to do).
However, the authorities take a very dim view of vagrancy, and they will usually ticket or arrest the person who has either "failure to account," or is clearly living in a vehicle or on the street. This is less true in the UK than the US. However, get caught on the street as a vagrant AND as a foreigner in the UK (or in the US, or in any Developed country) and you are in a world of hurt - typically you will be deported with prejudice and be unable to renter the country either "indefinitely," or for some fixed period of time.
If you can swing lodging, then the world is your oyster (for now). I travel with very little and within 2 weeks of settling on a spot in large city, I have cookware, flatware, clothing, a CD player, a large collection of classical CDs, and just about anything else I want to go looking for. There is an art to it, but the waste is so profligate that it is not hard to master, and absolutely no begging is required (except for lodging ;-))
I have seen all the movies, most more than once. I have not yet read the books.
When you say: "I thought it was more than probable the vast majority of readers here would be familiar with me," you imply a static readership for this list serve, or at least a monotonic one. I don't think either of those things would be good for this, or most other list serves with an agenda to change minds. New people will frequently be coming into the community and their very diversity may be one of their greatest values.
LOL! You don't have to be a genius to be evil and, speaking from long, hard and repeated experience, you don't have to be a genius to a great deal of harm - just being evil is plenty sufficient. This is especially true when the person who has ill intentions also has disproportionately greater knowledge than you do, or than you can easily get access to in the required time frame. The classic example has been the used car salesman. But better examples are probably the kinds of situations we all encounter from time to time when we get taken advantage of.
I don't know much about computers, so I necessarily rely on others. In an ideal world, I could take all the time necessary to make sure that the guy who is selling me hardware or software that I urgently need is giving me good advice and giving me the product that he says he is. But we don't live in an ideal world. Many people have this kind of problem with medical treatment choices, and for the same reasons. Another, related kind of situation, is where the elapsed time between the time you contract for a service and the time you get it is very long. Insurance and pension funds are examples. Lots of mischief there, and thus lots of regulation. It doesn't take evil geniuses in such situations to cause a lot of loss and harm.
And finally, while this may seem incredible, in my experience those few people who are both geniuses and evil, usually tell you exactly what they are about. They may not say, "I intend to torture and kill you," but they very often will tell you with relish how they've tortured others, or about how they are willing to to torture and kill others. The problem for me for way too long was not taking such people seriously. Turns out, they usually are serious; deadly serious.
First, I should point out that I don't believe the choices about how to increase success for cryonics are binary, as you lay them out above. While I don't use the same language you do, my argument has been that it is not possible to get people to freely adopt cryonics in larger numbers, unless you change them, as opposed to trying to change cryonics, or how it is "marketed."
You use the words "raising people's sanity level" to describe the change you believe is necessary, before they are able to choose cryonics rationally. The dictionary definition of sanity is: "The ability to think and behave in a normal and rational manner; sound mental health." I don't know if that is the definition you are using, or not?
Depending upon how you define "rational," "normal," and "sound mental health," we may be on the same page. I would say that most people currently operate with either contra-survival values, or effectively no values. Values are the core behavioral imperatives that individuals use in furtherance of their survival and their well being. It is easy to mistake these as being all about the individual, but in fact, they necessarily involve the whole community of individuals, because it is not (currently) possible for individual humans to survive without interaction with others. Beyond these baby steps at explanation, there is a lot that must be said, but clearly, not here and not now. What I've said here isn't meant to be rigorous and complete, but rather to be exemplary of the position I hold (and that you asked me about).
It is also the case that not everyone has the biological machinery to make decisions at a very high level of thought or reasoning. And amongst those who do, arguably, few do so much of the time, especially in terms of epistemological questions (and none of us do it all of the time). That's in part what culture is for. If we considered every decision in penultimate detail, we'd never get anything done. If the culture is bankrupt, then the situation is very bad, not just for survival of the individual, but for the civilization as a whole. So, you either fix that problem, or you don't succeed with cryonics. Put another way, the failure of this culture to embrace cryonics and life extension is a symptom of the problem, rather than the primary problem itself. -- Mike Darwin
I just read over my post, and I didn't say (or imply) anything about lesswrong being a cult. I know almost nothing about lesswrong, beyond reading interesting posts here, from time to time, usually as a result of google searches. My proximate reason for posting here was that Gwern suggested I do so, and also pointed me specifically to this discussion. So I guess my question would be, "Why would anyone think that I would think lesswrong was a cult?"
My remarks about "selling cryonics as part of a cult" are long-standing ones, and go back to decisions that I and others consciously made about how we wanted to proceed back in the 1970s. Having been in a cult briefly from 1974-75, I have a good understanding of the social mechanics of breaking people down and rebuilding them in a way that is "more desirable" to whomever is doing the "human re-engineering." There was not much question in my mind then or now that many people could be "converted" to cryonics by this expedient. The questions were about "should it be done?" Ironically, I got into that cult because the founders of Alcor thought that the "guru" running the operation would make cryonics a requirement for all of his adherents. -- Mike Darwin
I'm curious as to how you know "Voldemort" is a troll?
Taken at face value, the comments above are those of a sociopath. This is so not because this individual is willing to sacrifice others in exchange for improved odds of his own survival (all of us do that every day, just by living as well as we do in the Developed World), but because he revels in it. It is even more ominous that he sees such choices as being inevitable, presumably enduring, and worst of all, desirable or just. Just as worrisome is the lack of response to this pathology on this forum, so far.
The death and destruction of other human beings is a great evil and a profound injustice. It is also extremely costly to those who survive, because in the deaths of others we lose irreplaceable experience, the opportunity to learn and grow ourselves, and not infrequently, invaluable wisdom. Even the deaths of our enemies diminishes us, if for no other reason than that they will not live long enough to see that they were wrong, and we were right.
Such a mind that wrote the words above is of a cruel and dangerous kind, because it either fails, or is incapable of grasping the value that interaction and cooperation with others offers. It is a mind that is willing to kill children or adults it doesn't know, and is unlikely to know in a short and finite lifetime, because it does not understand that much, if not almost all of the growth and pleasure we have in life is a product of interacting with people other than ourselves, most of whom, if we are still young, we have not yet met. Such a mind is a small and fearful thing, because it cannot envision that 10, 20, 30, or 500 years hence, it may be the wisdom, the comfort, the ideas, or the very touch of a Romanian orphan or of a starving sub-Saharan African “child” from whom we derive great value, and perhaps even our own survival. One of the easiest and most effective ways to drive a man mad, and to completely break his will, is to isolate him from all contact with others. Not from contact with high intellects, saintly minds, or oracles of wisdom, but from simple human contact. Even the sociopath finds that absolutely intolerable, albeit for very different reasons than the sane man.
Cryonics has a blighted history of not just attracting a disproportionate number of sociopaths (psychopaths), but of tolerating their presence and even of providing them with succor. This has arguably has been as costly to cryonics in terms of its internal health, and thus its growth and acceptance, as any external forces which have been put forward as thwarting it. Robert Nelson was the first high profile sociopath of this kind in cryonics, and his legacy was highly visible: Chatsworth and the loss of all of the Cryonics Society of California's patients. Regrettably, there have been many others since.
It is a beauty of the Internet that it allows to be seen what even the most sophisticated psychological testing can often not reveal: the face of the florid sociopath. Or perhaps, in this case I should say, the name of same, because putting a face to that name is another matter altogether.
The reason I haven’t posted here before is that I’ve had no burning reason to, and I’m busy.
While there are many discrete reasons why cryonics hasn’t been (more) successful, the single biggest reason is the most obvious one; it has not been demonstrably shown to work. If suspended animation were a demonstrated reality tomorrow, and it was affordable (i.e., not like spaceflight, which is demonstrably workable, but not yet affordable) then the tide would be turned. Even then, it is unlikely there would be any kind of flash-stampede to the freezers.
A schoolmate and friend of mine just died a few weeks ago of pulmonary fibrosis. He was an ideal candidate for a lung transplant. But, he couldn’t afford it, so he just laid there and died. Thousands of people who need transplants die each year, even though it is a proven modality of treatment that is yielding a significant number of quality years of life. But, it is costly, there aren’t enough donors, and here’s the really remarkable thing, the vast majority of people who could benefit from a transplant are never even candidates.
Consider Richard DeVos, the co-founder of Amway: http://www.rickross.com/reference/amway/amway24.html. In 1983 DeVos, suffering from coronary artery disease, had bypass surgery. In 1992 DeVos had another bypass surgery, and by 1995 it was clear he had end stage congestive heart failure (CHF). How many people have you known or heard about who fit that description, and subsequently go on to die a perfectly pedestrian death; at home or in the ICU? Such deaths are so routine no one gives them a second thought.
And it’s for damn sure that no one gives them a second thought when the patient is a 71 year old man! However, if you are absolutely fixated on staying alive, and your net worth is well in excess of 2 billion 1997 dollars, well, the rules of the game are different for you. DeVos got his heart in London, and the Amway corporate jet flew him there from Grand Rapids, MI. That was in 1997, and as far as I know, DeVos is still alive. There are countless ~71 year old men in the US, and elsewhere in the Developed World, dying of CHF right now. In those cases, the word "transplant" is neither uttered nor heard – even though it is very much a reality that if you have the money, the persistence and the luck – a heart transplant offers the prospect of another 5 years of reasonably good quality life, on average.
I worked in hospital, mostly in critical care medicine, for 7 years. The overwhelming majority of patients are passive – they do what their physicians advise and if they do have alternative ideas, they are usually easily dissuaded from pursuing them. And, truth to tell, most of the “alternative ideas” patients have are bad ones, including Steve Jobs. But, if you are smart, lucky and rich – and you come to your senses, as Jobs did, it can be whole other ball game. Jobs suffered recurrent pancreatic cancer (islet cell neuroendocrine tumor) after a Whipple procedure in 2004. That is just about as close as you can get to a death sentence, since the usual location of the met(s) is the liver. It is current medical consensus that liver transplantation in patients with recurrent pancreatic cancer that has metastasized to the liver is contraindicated. In fact, I know a couple of transplant surgeons who call such a procedure a murderous waste of a liver, and a life! However, Jobs got a liver transplant in 2009. I strongly suspect that he has very recently received additional cutting edge treatment not widely available.
Cryopreservation/cryonics is likely to creep in on little cat’s feet – with a big jump or two along the way. Cryobanking of parenchymatous organs will probably be one jump, reversible cryopreservation of the brain another, and finally, whole body suspended animation. But it behooves us to beware that lots and lots of people are “calmly” accepting their fates today, who could in fact be ‘rescued’ by already extant medical technology - but for the knowledge, the money and the will. And THAT is what is NOT likely to change. To a surprising degree, people stay alive because it has been made very easy for them to do so. Make it difficult, and you start to see people dropping away.
Cryonics demands a very high passion for and commitment to staying alive, not just because it is currently such a lousy product, but because, to be really credible, it DEMANDS ACTION to improve the odds of its success. Most people are not activists, and what's more, most people will refuse a chance at more life when you take away the superficial things that they mistake for their person-hood, or identity. And cryonics proposes to do exactly that. There is historical precedent for this. In his incredibly insightful book, MAN'S SEARCH FOR MEANING, Viktor Frankl noted that the people in the Nazi concentration camps fell into two groups. The first group consisted of the majority of those interned there, and they were people who defined themselves in terms of their social milieu: if you asked them who they were, they would say, "I am a doctor, a lawyer, a mother..." The second group consisted of a small minority of people who thought of themselves as existing completely independent of any label, any role, or any relationship they had with others, or with society.
When you entered a concentration camp, they took away you clothes, your profession, your family and even your name. For most people, that was the equivalent of taking away their very identity, and thus their will to live. As Frankel observed, it was mostly only the people in second, much smaller group, that survived.
It is from that tiny minority in the population as a whole, that cryonics draws it adherents. They are people who want to live, regardless, and who do not define their sense of self on the basis of their jobs, their social interactions, or really, on anything other than a raw, visceral passion to survive. Some find that absolutely terrifying.
Rationality Bootcamp and Advanced Sanity Techniques? The first things sane and rational people do, are to exercise due diligence in gathering the facts before they make crazy and unfounded public statements such as:
1) "I suspect that Mike Darwin wants a grand narrative of Why, Oh Why Cryonics Fails, a grand narrative that makes sense of this shocking and incomprehensible fact and gives some info on what needs to be done to relieve the frustration." and
2) "Mike Darwin thinks that if you have better preservation techniques, people will sign up in droves, because right now they're hearing about cryonics and rejecting it because the preservation techniques aren't good enough."
Really? Not only don't I believe those things to be true, I've never said that they were. Au contraire, the only grand narrative of why people haven't embraced cryonics in droves is a very complicated one which, onto 40 years later, I'm still learning about and struggling to fully understand. In 1981 I wrote an article (with Steve Bridge) entitled "The Bricks in the Wall" about the many reasons why people find it difficult to embrace cryonics: http://www.alcor.org/cryonics/cryonics8111.txt. If I recall correctly, there were at least a dozen reasons given in that essay, including things like loss of others, loss of self, lack of technical confidence, incompatible worldview, high social cost, fear of temporal displacement... Since that article was written, I've learned of many more reasons why people reject cryonics and why they don't decide to opt for it - which, as it turns out, can be two very different things.
Ironically, much of my career in cryonics has been spent arguing against "the big idea," "the grand solution," "the magic bullet," or "the single rich individual who will provide the solution to the problem of why cryonics has fared so poorly." There is no single reason, unless you want to consider the myriad individual reasons, in aggregate, as a single cause of the failure. If you insist on that approach, then the best you will do (and you could do far worse) is to note that by any normal market standards, cryonics is a shitty product. It costs a lot, it is unproven, there are many commonplace reasons to believe that existing institutional structures have a poor chance of surviving long enough for the patients to be recovered, it has been plagued by legitimate scandals and failures and the constraints imposed by the existing medico-legal infrastructure mean that, statistically, you've got a ~30% chance of being autopsied, or otherwise so badly degraded that whoever it is that is recovered from the procedure isn't very likely to be you (e.g., presumably if your DNA is intact a clone could be made). So cryonics doesn't stack up very well as a normal market product.
Having said that, if you want to 'sell' cryonics as part of brainwashing package, or a religion, I'd be the first to say that it can probably done. It has been my observation that you can get people to do almost anything if you rob them of their will, and subvert their reason. For myself, I don't think that's a good idea.
As to the issue of improved preservation techniques causing people to sign up in droves, surely you jest? Any improvement in cryopreservation techniques short of fully reversible suspended animation will 'only' have an incremental effect. So for example, if organ cryopreservation for the kidney were achieved tomorrow, and organ banks for kidneys opened their doors 6 months later, I would indeed expect to see an increase in people opting for cryonics, but not a stampede.
Historically, the same was true of the introduction into cryonics of credible ideas for repairing cryoinjury and of scientific documentation that brain ultrastructure was surviving cryopreservation (under ideal conditions) reasonably well. Both of those advances widened the appeal of cryonics to a very small group of people. Nevertheless, they were significant, because if you have 40 members, and such advances give you 240, or a 1,040 - then that's a huge benefit.
Finally, if reversible whole body suspended animation were developed tomorrow, the vast majority of people would still not opt for it. In fact, they more or less never would. What would have to happen first is that a relatively small cohort of the population who command respect, authority and power, would have to decide that it is in their interest to have suspended animation become a commonplace medical treatment. By this, I do not mean to imply some focused or intelligent cabal, or group of conspirators, but rather that all kinds of empowered people in many walks of life must be persuaded before the society at large will embrace cryonics. In other words, it will be a process and probably a complex one, before Mrs. Smith sits in her doctor's office and is either offered, or asks about, suspended animation as a possible alternative to her ending up dead from her advanced ovarian cancer.
In my opinion there are no magic bullets. Rather, there are just a lot bricks in a large wall of opposition that have to be patiently worried away, one, or a few at a time. It's all too easy to see TV coverage of the Berlin Wall coming down and say, "Jeeze, look how quick and easy that was!" Not. The back-story needs to be considered and in the case of cryonics that back-story has been unfolding for nearly fifty years - and there are still less than 2K people signed up worldwide.
Finally, it is indeed a cruel and unpleasant reality that life isn't very rewarding for many people, and that it all but completely lacks the zest, joy and wonderful sense of adventure that can be seen in the eyes of any well cared for child. The biology of maturation and aging do much to drain away that sense of wonder and appetite for life. But it is much more likely the case that the way we lead our lives is the primary culprit. I recommend watching multiple episodes of a TV program called "Undercover Boss." Just watch what people who work in factories, in offices, in laundries and in loo cleaning businesses do all day. It is horrible. It is, in fact, the exact opposite of the situation we DEMAND that children be in. Indeed, one of the most repellant things to people in the West is "child labor." Well, if the normal workaday work is so horrible for children, what makes it good for adults? And if we propose to live for millennia, and longer, then don't we, by definition, have to be as children: open, mobile, playful and exploring in our interaction with the world? I have done all kinds of jobs, from working at Mc Donald's (2 years) to cleaning loos and dirty motel rooms. Work is a good and character building thing. But it can also be a corrosive and soul destroying thing that robs people of any strong desire to fight for life. Methinks that perhaps you need to work at McDonald's dressing hamburger buns for a year or two.
I found this a fascinating and amusing exercise. The 1990 Alcor article, "The Cost of Cryonics" and the accompanying tabular breakdown of the actual marginal costs that was used, in part, to generate the scenario above, were done by me in 1989-1990. [And you will note they have not been repeated since ;-0] If you look closely at that article you’ll also note that there is a disclaimer at the start which says, “these opinions are mine and do not represent those of Alcor…” That was there because the management was not happy with my projections, and instead backed those of Ralph Whelan http://www.alcor.org/cryonics/cryonics9310.pdf. If you go to page 10 of Ralph’s article you’ll see the projected growth rate for Alcor. The article also contains projections for “post-start-up” economies of scale. If you actually take the trouble to look at where Alcor is today, versus the “anticipated” numbers in that article, you’ll see that just about every assumption made was wrong. A short while ago, Brian Wowk tersely informed me during a phone call that my projections, if adjusted for inflation, constitute the actual current rate at which Alcor charges for cryopreservation services. I’m not sure if this is true, or not, because I haven’t bothered to re-run those numbers.
What is interesting in looking over the discussion here on Less Wrong is that all these various cost estimates don’t take into account the social and political context in which they are supposed to operate. Cryonics is very expensive if it is practiced as a high technology endeavor aimed at minimizing the extent to which it is (reasonably) technologically practical, damage from ischemia and from cryopreservation. And that was in the absence of skilled professionals who are vulnerable to malpractice judgments doing the procedures. When my estimates were done in the late 1980s, reasonably skilled, but non-professional people, were available to minister to cryonics patients. Any global scale-up of cryonics would have to factor in not only professionals’ fees and associated costs (licensing, regulation, litigation, etc.), but also the complex infrastructure required to implement such a technology on a widespread basis.
If you do that by, for instance, looking at the cost to provide EMS services to people in the US or the UK, you will find it is staggeringly expensive, and that far from there being economies of scale, the costs rise, dramatically. If you posit making Universal Cryonics a reality at a high level of technology, then you can easily bound the cost by simply using the existing medical system as your model. How much does it cost to respond to and to and transport a patient in cardiac arrest to a hospital ED? Add to that say, ~ $5,000 for ischemia-reperfusion medications and for en-route cooling. Then, figure out how much a typical Coronary Artery Bypass Graft (CABG) costs today and add to that ~ $25,000 for cryoprotectants, associated IP licensing, and for extended use of the OR for CPA perfusion. From there, you can try to figure cool-down costs. If you like, you can just plug in existing numbers for cool-down. What you’ll find if you do this is that cryonics will cost about $170,000 to $250,000 for the up-front part of the procedure. And that is being very, very conservative and assuming that automation can be used to pinch hit for expensive human labor.
The only place where there is a reasonable possibility for economies of scale is in storage. Mostly, those economies of scale have already been reached by Alcor and CI for the type of storage they are using. In other words, if you want further economies of scale you have to build BIG, because the only way you get more efficient is by exploiting the reduction in heat leak that is to be had by decreasing the surface to volume ratio of your cryogenic storage system. That can most efficiently be done by building very large spherical storage vessels. Of course, practical considerations will kick in at some point and, unless you want to build gigantic storage vessels that you just pitch patients into like cord wood, you’ll need a way to access individual patients at will. This requirement greatly constrains the simplicity of the engineering it is possible to use, and thus increases the costs. Still, I would guess that you might halve existing neuro storage costs.
Finally, once you have a society that takes cryonics seriously, not only are they going to start suing for bad care, they are going to want protections to be present against sudden, undetected cardiac arrest and against myriad other contingencies that could frustrate cryopreservation andthat will also increase cost. Finally, they are going to want protection against existential risks to cryopreserved patients. Consider the situation today with nuclear power plants. These energy generating pieces of infrastructure are very dangerous if mishandled, sabotaged or subjected to fire, earthquake, flooding, or any of a number of other man-made or natural calamities. As a consequence, these plants are subject to very costly uber-engineering AND REGULATION. And even with such costly precautions, they are still sadly vulnerable, as recent experience attests.
Completely leaving aside the issue of how securely people will want to store their cryopreserved relatives, there can be little doubt about how securely they will want to store themselves once they are in a vulnerable and indeed completely helpless state. That means a level of engineering that is at least comparable to, or better than that currently employed in nuclear power installations. And there will be pragmatic limits on economies of scale because few sane people would buy off on the idea of 4 or 5 mega-regional storage facilities for the whole planet, or even for the whole of the US.
The take home message is simple. Barring absolutely “Singularity-style” improvements in technology and wealth, cryonics is going to not only remain an expensive proposition; it is going to get a lot more expensive. For a mature “universal cryonics procedure” in the framework of existing/foreseeable technology, my guess would be that the cost would be between $500,000 and $750,000 per person in the West, and perhaps half of that in the Developing World – but with a lot more risk (no hardened storage facilities, more risk of unattended death, and so on).
If you pull cryonics out of the context of a “universal, mainstream operation,” then costs could be very different. – Mike Darwin