Covid 6/30/22: Vaccine Update Update
post by Zvi · 2022-06-30T14:00:01.476Z · LW · GW · 6 commentsContents
Executive Summary The Numbers Predictions Deaths Cases BA.1.2.3.4.5 FDA Considers Eventually Updating Vaccine The Long Long Covid Trek In Other News Not Covid None 6 comments
This week’s news is that the FDA advisory committee voted overwhelmingly to update the vaccine for Omicron, after a delay of only six months, which means they’ll get to deciding which way it should be updated Real Soon Now and then they can tell the pharma companies what requirements they want to place on that. There’s some chance the update will happen at a time that isn’t never, and even a tiny chance the update might not be hopelessly behind the virus when it happens. You never know.
Executive Summary
- BA.5 now the dominant strain.
- We might eventually update the vaccines. Maybe.
- Authorities are still using misinformation to justify policy.
Let’s run the numbers.
The Numbers
Note that I am increasingly forced to make adjustments to account for obviously delayed or wrong reporting. Florida reports every two weeks, and a number of states did something requiring at least some form of adjustment. These decisions are
Predictions
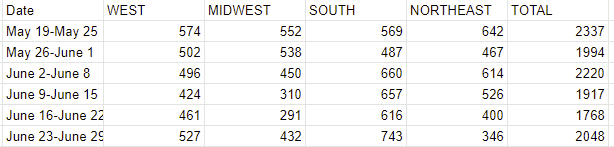
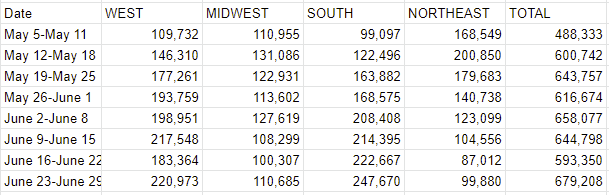
Prediction from last week: 675k cases (+14%) and 2,015 deaths (+14%).
Results: 679k cases (+14%) and 2,048 deaths (+16%).
Prediction for next week (4th of July!): 600k cases (-13%) and 1,800 deaths (-16%).
This is a holiday prediction. I expect the true situation to hold roughly steady, with drops due to the extra reporting this week going away plus the missing reporting next week.
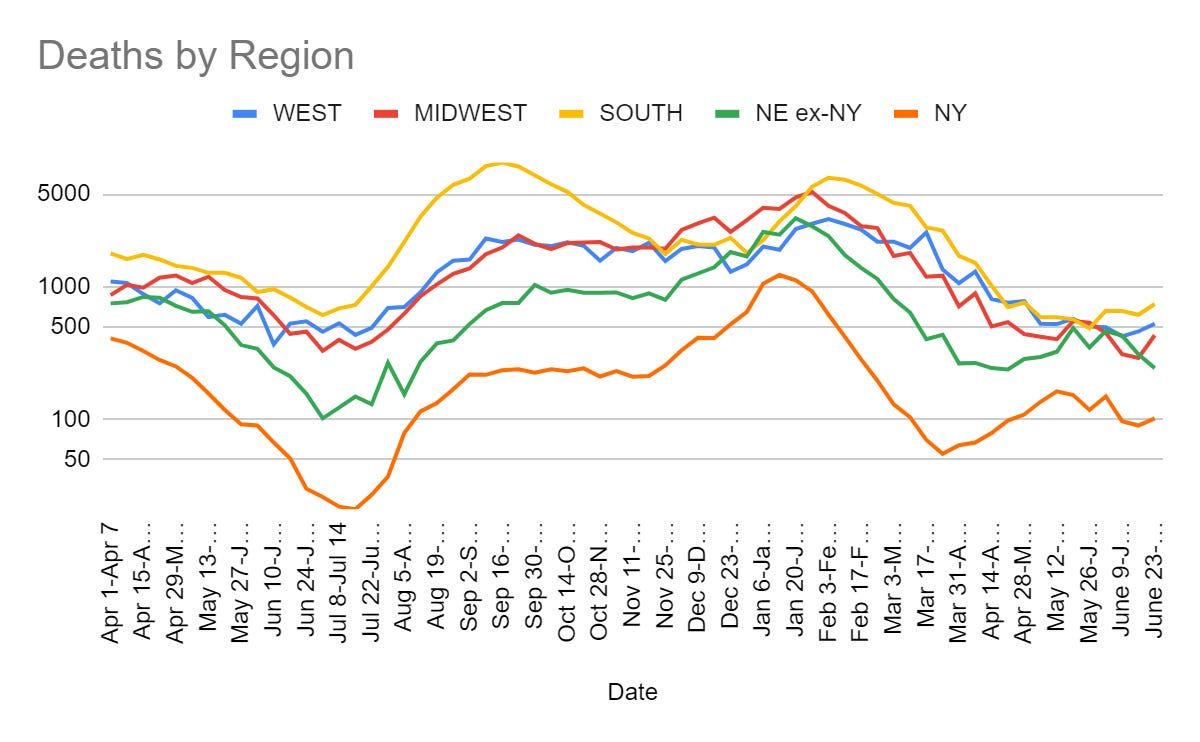
Deaths
Cases
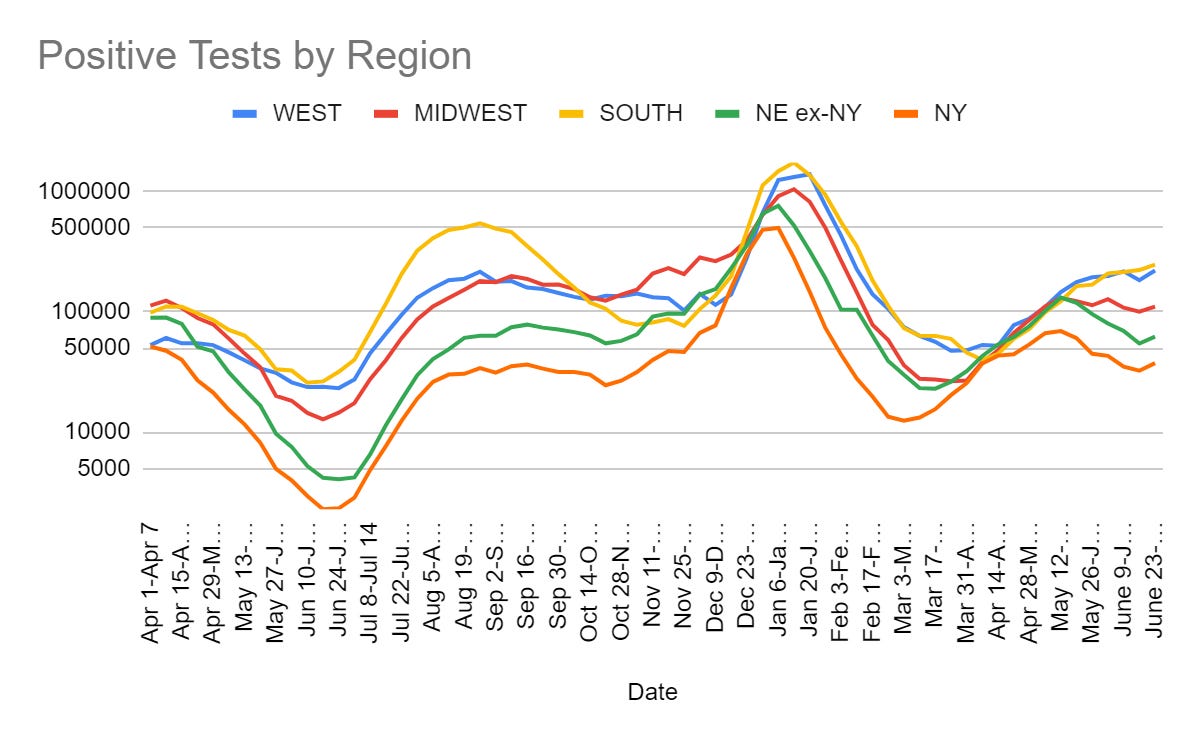
As expected this is a bounce back from the holiday weekend. Now we are headed into another holiday weekend, so I expect a drop back down again. Things are less smooth at the state level than they appear at the regional level, but nothing is that dramatic.
We are entering the period of most rapid percentage growth in BA.5 on a week-to-week basis, so if we are going to see that transition cause a lot of problems then these next two weeks are when we will see clear signs of that.
BA.1.2.3.4.5
BA.4 and BA.5 are now the dominant strains.
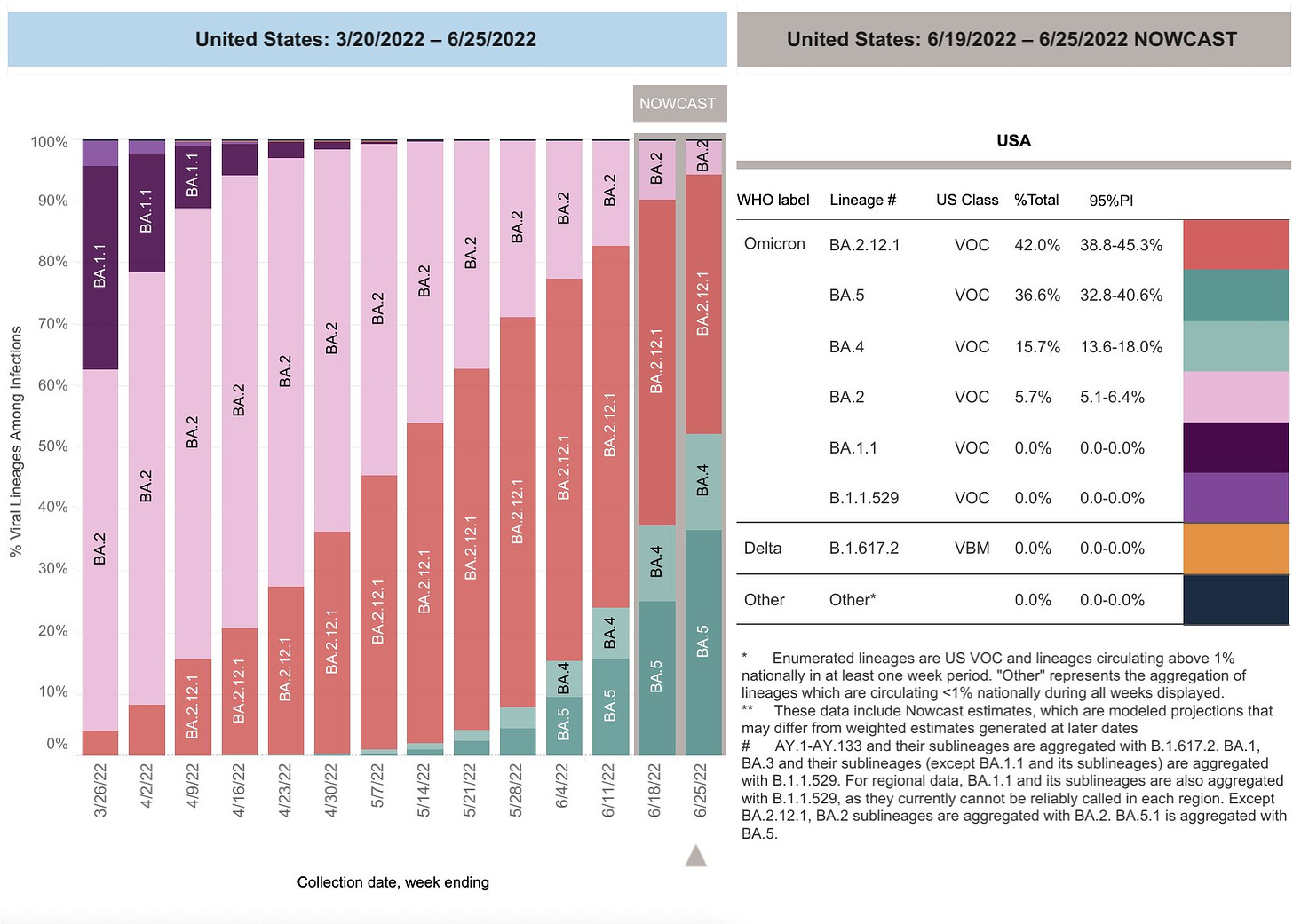
Technically BA.2.12.1 is bigger than either of them in the latest data set, but by the time the data gets reported BA.5 will have passed it. None of this was ever in doubt.
The good news is that so far there is no sign of the next variant.
Eric Topol covers our new dominant strain, BA.5.
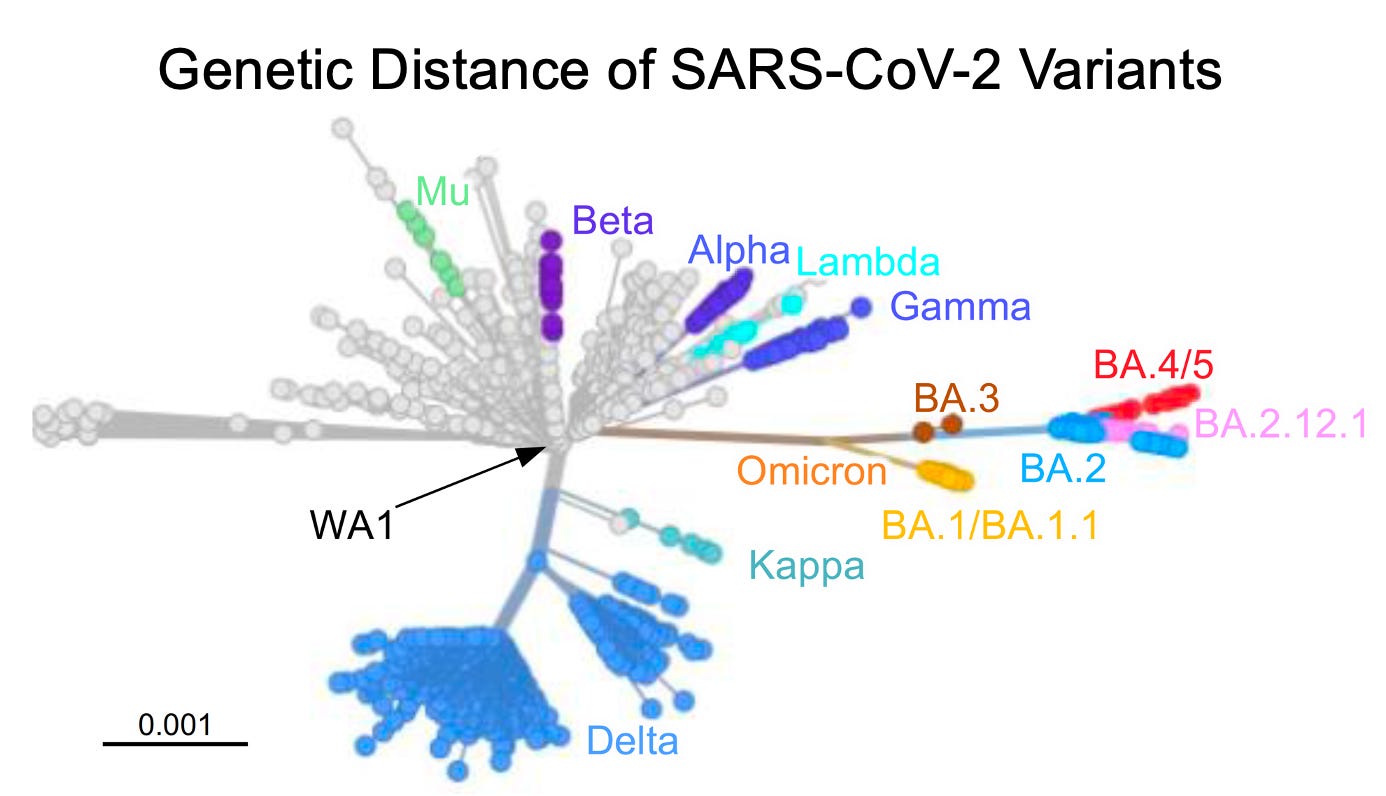
If Omicron really is off in a complete different direction than any of the previous dominant strains, then that is importantly good news. It means that Omicron did not take Alpha, Beta or Delta and then add additional changes to make things worse. Instead, it did different things.
If that’s true, then it means the virus has gotten stuck via hill climbing at various points, and there’s a chance we don’t have to worry as much about Variant A → Variant B → Variant C → Variant D.
Mostly the early section is about how much more fit BA.5 is, how it spreads so much faster and more effectively. Topol keeps saying how it’s so much faster and more effective, but the change here doesn’t seem out of line with previous changes.
Look at how terrible it is we have all these cases, he says.

And look how terrible it is that this new version makes the vaccine less effective, and is quite possibly deadlier.
But, of course, it’s not deadlier in practice, no matter how deadly it is or is not in theory. We know this because not many people are dying. You can of course say that this is because of prior infection and vaccination, and you’d be right, but that still counts in terms of how worried we should be and how we should react (although it is important for you as an individual to avoid double-counting this).
Should we wait for a BA.5 booster? That will take months, and it should be noted it took more than 7 months for the Omicron BA.1 booster to be tested, a delay that is exceedingly long and unacceptable relative to the timing of validation and production of the original vaccines in 10 months during 2020.
There is no right answer but variant chasing is a flawed approach. By the time a BA.5 vaccine booster is potentially available, who knows what will be the predominant strain?
This is flat out saying that we can’t update a booster before everyone gets infected by a given variant anyway. He simply states this as fact, rather than going into why we can’t do this faster. It’s especially unacceptable given that if it wasn’t for Topol we likely could have done better than 10 months for the initial vaccine – I’ve accepted using him as a source but I’m not going to forget about that little incident.
The overall message is right. Our capitulation is sickening, and there is no reason our science and our production lines couldn’t keep up with the situation. We simply are choosing not to do that.
Speaking of which, how are those vaccine update efforts going, FDA?
FDA Considers Eventually Updating Vaccine
They held a hearing, and they’re in favor of doing it. Eventually. In theory. As soon as they take months scheduling a meeting, and decide exactly how they want the update to work so as to invalidate any previously collected work or data. As you do.
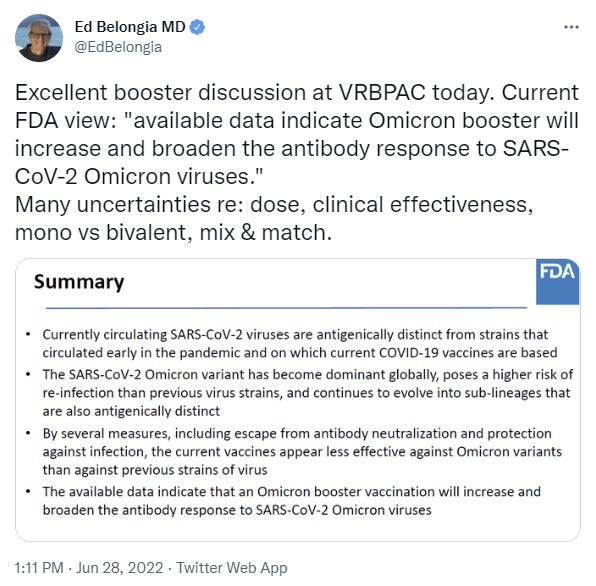
Trevor Bedford, the day before the hearing, correctly points out that at this point effectiveness against BA.4/BA.5 is most important. Clear enough.
The meeting agreed, here’s the rundown. Weekend editor also offers a summary.
Meetings of the Food and Drug Administration’s vaccines advisory committee are never dull affairs. Drenched in data, maybe, but never dull.
Why? Why are they never dull? They should usually be dull. They should be mind-bogglingly, infinitely dull, because these decisions are massively overdetermined and the whole point is to go through all the motions to ensure no one is blameworthy and to guard against any errors or deceptions. That should mostly be highly dull work. What is going on that is instead so… exciting all the time?
The confluence of factors includes waning immunity, the possibility of the emergence of a new variant, and the looming arrival of winter, with weather that keeps people indoors more, in much of the country.
“So those three things combined make us realize that we do need to think about a campaign for boosters sometime in the fall. And getting it right, thinking about what we might do differently than we’ve done now, is important,” Marks said.
I would have suggested that we should update the vaccine because of the confluence of these three factors:
- We have a vaccine for the wrong version of Covid.
- We can update the vaccine.
- The updated vaccine will work better.
Mostly I’d go with #3.
But all right, you do you FDA, and cite all the detailed reasons why it is good and important to save lives in this particular instance rather than in most instances when your job is to stand between the person trying to save lives and the lives they are trying to save and yelling ‘you shall not pass.’
Good news, they are going to change to a version that targets BA.4/BA.5, by a vote of 19-2:
8:00 p.m.: Frequently, for an FDA panel, the result cannot be fully summarized by just a vote tally. That is especially the case today.
The panel was broadly in favor of telling companies to start manufacturing an Omicron-containing booster, with only two panelists voting that the data did not yet support creating such a shot.
But there was consensus on more than that. The panelists largely agreed that the booster should contain the BA.4 or BA.5 variants of Omicron. The data for shots containing these variants largely comes from tests on animals, not humans, but the panelists believed the new vaccine would be similar enough to previously tested variant vaccines that it is worth trying to get ahead of the next viral mutation, to go, as one panelist said, where the puck is going, not where it is now.
That is how slow the FDA process is. By the time they got to this recommendation, BA.4 and BA.5 taken together had already become the most common strain. This wasn’t a case of failing to extrapolate to the inevitable situation several weeks from now being overcome by some miracle. This was acknowledging what had already happened as if it was ‘getting ahead of the next viral mutation.’ Which was actually the previous viral mutation that already not only happened but has already become dominant given delays in data collection.
Consider what is implied here. They seriously considered updating to an already obsolete version due to concerns over the data they refused to let pharma companies collect. That’s what has become of the vaccine that was designed in one or two days and that they claimed could be updated in a week. That’s what the FDA is all about.
Well, that and trying to create a new wave of organized crime around the selling of illegal cigarettes, but that’s a different issue because it’s something people care enough about to defy unreasonable restrictions.
What could the objections possibly be? Oh, no, way stupider than that.
“I’m uncomfortable with the U.S. having a vaccine that’s not accessible to the rest of the world,” Perlman said, noting there’s already a perception that the U.S. and other wealthy countries have put themselves first. “And if we’re saying that a bivalent vaccine is so much better, but it’s not accessible to much of the world, I think that’s ultimately a bad thing for getting vaccines out to the whole world.”
You have two cows. There aren’t enough cows for everyone. The FDA kill the cows.
This is completely insane. We shouldn’t ‘put ourselves first?’ We shouldn’t first make sure our own citizens get the best life-saving medicine available, then help others? Instead, we should give no one any life-saving medicine, you see, until we have enough cupcakes for the entire class. Until then, we should let our own citizens die. Great.
No, no, Perlman says, this isn’t about equity, it’s practical!
A number of countries are still relatively early in their vaccine rollouts. If there’s a perception that there is a better vaccine, they may object to using vaccines based on the original SARS-2 virus. That’s already been seen with countries holding out for mRNA vaccines, because of the view that they are the best Covid vaccines.
So you’re saying that we shouldn’t give our citizens life-saving medicine because others might see that it is so much better at saving lives they want to hold out for the superior version, and we don’t want them to make this ‘wrong’ choice? Is that it?
The good news is, it turned out fine, we can give the new life-saving medicine because it isn’t that much better at saving lives?
But the existing Covid vaccines are still doing a great job in protecting people against severe disease and death. As Kate O’Brien, technical lead on vaccines at WHO, told me recently: “There’s not a first class and a second class of vaccines, if these ones come out.”
Or is it the opposite, that we are now worried that the new one isn’t sufficiently better but people might think it was sufficiently better, so now we can’t give it out? Are better things better or worse this time? Who can say? There definitely aren’t ‘first and second class’ of things where some things are better than other things, no sir, absolutely not, that never happens and it’s never all right to go with second best. We need to ensure that everything second best is illegal, which means that if making the second best thing illegal would be a problem then we have to keep the first best thing illegal instead so that the second best thing isn’t second best.
Right. Got it.
Some fans for Novavax. Two panelists spoke out in favor of the data shown by Novavax indicating that its shot against the original strain might work well as a booster against Omicron strains. James Hildreth, CEO of Meharry Medical Colllege, said the Novavax data were “the most compelling thing I’ve seen today” and that the data seem “more impressive to me than the data for Pfizer and Moderna.” Wayne Marasco of the Dana-Farber Cancer Institute made similar comments, wondering if the Novavax data were showing the limitations of the mRNA vaccines. Hildreth encouraged the FDA to consider Novavax’s emergency use application quickly.
The Novavax vaccine remains illegal.
How do we measure vaccines? One problem here is that there aren’t enough measures, outside of clinical data, to know if a vaccine is working. Ofer Levy of Boston Children’s Hospital implored the FDA to take the lead in finding one. “If we aren’t able to identify a correlate of protection, we are fighting with one arm behind our back,” he said.
Yes, it is a real shame that we made it illegal to collect data or know things. We’re all trying to find the guy who did this.
There’s a bunch of technical discussions about which approach is right for the updated vaccine. Moderna claims it’s better to use a mix of original strain and Omicron. Pfizer claims it’s better to use only Omicron. Someone’s right, someone’s wrong, and frankly I’m totally willing to not investigate the question further and declare it somebody else’s problem.
As for what to do about that problem, the answer is to ensure there isn’t a vote so that we can do whatever we want?
6 a.m.: As I mentioned in the introduction, there’s only one voting question slated for today. It’s on whether an Omicron strain should be included in Covid boosters.
But the FDA is asking VRBPAC to consider a number of other questions; they are just not, it appears, going to be asked to vote on them. That means the agency gets to hear the views of their advisers, but doesn’t face the thorny issue of ignoring their recommendations, should the FDA decide not to follow that advice.
And the questions the FDA wants discussed but not voted on cover a lot of important ground. Like: Which version of Omicron should be included in the updated vaccine, if updates are called for? The FDA’s analysis for the meeting, found here, acknowledges there currently are no data on how well boosters based on BA. 4 and BA. 5, the subvariants that are now surging across the country, would actually work. And yet it’s clear the FDA is considering instructing manufacturers to make updated vaccines using one or the other of them.
VRBPAC will also be asked to discuss but not vote on whether updated vaccines should be monovalent — targeting only Omicron — or bivalent, retaining the original vaccine and adding an Omicron strain to it. It is being asked to opine on whether the existing primary series vaccines — the ones that have been in use since late 2020 — can still be used for people who’ve never been vaccinated before if the booster shot composition is changed.
With no votes on these questions, policy setting may be easier for the FDA.
So yes, it does seem like the strategy is to avoid having the FDA advisory panel vote on things so that when the FDA ignores them there won’t be a vote that they’re ignoring. Smart.
That would have been a state of the art finding if it had happened in, oh I don’t know, December? So six months ago?
Did they end up doing the right thing here? Mostly, yeah, does seem like it. Eventually. This has been delayed by almost a year at this point. So while there are some points for eventually probably allowing, in the future, some vaccine updating to occur, the main story is how utterly broken the entire process continues to be.
Except, some say, not so fast.Let’s not rush into anything.
I can only look on such things with the single tear of sadness and/or the fire of a thousand suns. It is a full argument for never doing anything at all. We don’t know how much it will help to update, so we shouldn’t update. We don’t want to update to the obviously correct option because we don’t have enough data, so we should wait until we have the data, at which point there will be another variant. So we never update, or we’re always a year behind.
And then there’s the kicker:
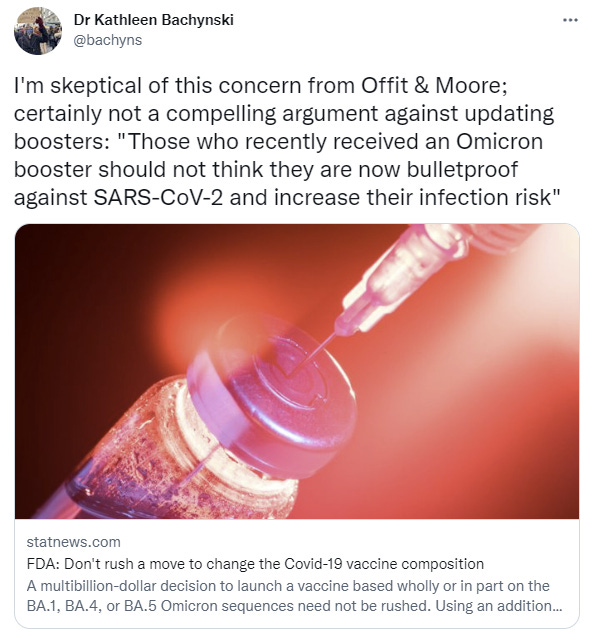
I believe you are indeed reading that correctly. We shouldn’t let people protect themselves against disease, because they might feel they were more protected than they are. So instead we should make it illegal for them to protect themselves. Because they might believe something that people don’t actually believe – public health has a long history of imagining what people might think or believe in response to things, in ways that imply a lack of contact with ordinary humans, perhaps due to social distancing.
This is public health. This is what very serious people actually believe. It is also flat out anti-vax. This is the face of the enemy.
Zeynep also finds this line of argument incoherent, but is concerned about the ability to do the rollout globally and ‘equitably.’ I continue to notice that the best way to get a rollout to the people in the back of the line is to first satisfy the people in the front of the line, then keep going, and if you instead break up the line and insist on ‘equity’ then this is reliably a way to get everyone nothing at all. The way to roll this out globally is to… roll it out, nationally. Then go from there.
The Long Long Covid Trek
There is one again a new Long Covid study. The whole thing is a big mess, with this standing out:
Third, the study reveals small but significantly higher quality-of-life scores on some scales of the Pediatric Quality of Life Inventory (PedsQL) in some age groups of children who had COVID-19. This finding seems paradoxical given that cases also reported more long-lasting symptoms, but is reassuring for children with COVID-19.
If net quality of life can be measured as going up, the problem seems highly unlikely to be so bad, even if I presume the effect is ‘not real.’ If it is real, I have snarky guesses on why but you can guess what they might be easily enough.
In Other News
Universal Covid vaccines to enter testing. America is shamefully not supporting these efforts, but they are not getting sufficiently in the way to stop them, and that’s looking to be good enough.
Elmo got the vaccine. Not cringe at all. Nor was the inevitable Ted Cruz response.
CDC continues to spread known misinformation (as in, source has admitted the error) in its official communications, claiming children die of Covid-19 far more than they actually do.
Here’s one thing that happened when this was pointed out (Jerome Adams is a former surgeon general).
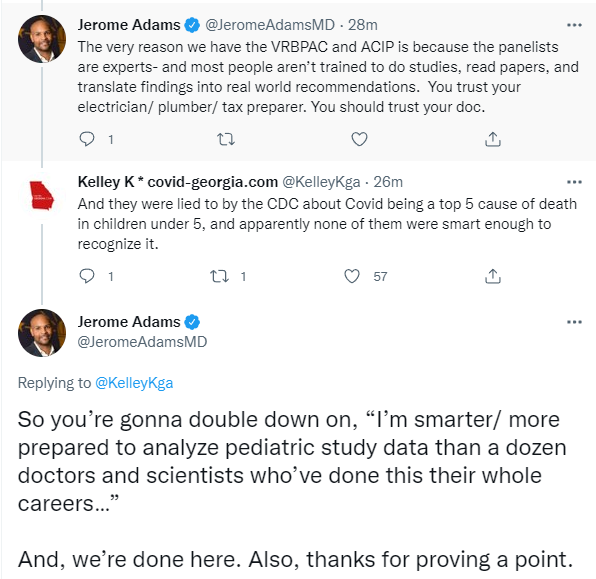
Yes, we are going to double down on being better prepared to analyze study data then a group that got it wrong, had it pointed out and admitted to by the source, then doubled down on the wrong thing and used it as justification for national policy. I happen to agree with the policy for other reasons, but yikes.
I am confused that Ethan Mollick is confused.

Seems to me he cleared up his own confusion. The system is failing and everyone wants to not notice. The point of a blue-ribbon commission is to drive the adoption of organizational reforms. No one wants to do organizational reforms, so why would they want a blue ribbon commission?
Sam Enright wraps up his excellent 4-part coverage of the Covid response in Ireland with an excellent list of things to do to prepare for next time, if anyone was interested in preparing for next time.
- Use human challenge trials.
- Subsidize superforecasters and prediction markets.
- Stop using the phrase ‘no evidence.’
- All medicines approved by the FDA (America), MHRA (UK), PMDA (Japan), TGA (Australia), Medsafe (New Zealand), HPFB (Canada), or any other trusted regulator should be approved automatically, in addition to the local EMA.
- All doctors and nurses certified in any OECD country should also be certified.
- Hospitals should be exempt from all local building codes.
- Diversify your information sources.
- Red-team your pandemic response.
- Be extremely hesitant to ban things that might help you.
- Allow “price gouging.”
- Have a diversity of vaccines, tests, and funding models.
- Spend early and often on candidate vaccines.
- Celebrate heroes.
That is an excellent list, and Ireland can be crossed out with America (or anywhere else) written in its place, flipping the roles of EMA and FDA. My only objections are where this does not go far enough in some places. We should be extremely hesitant to ban things even if they don’t help, and it’s not only hospitals that should be exempt from business codes, and so on. Those are minor quibbles. Beyond that, it’s again a question of where this did not go far enough, and sidestepped other things. There are so many worthwhile things. Again, a fine start.
Not Covid
EU, while it restarts its coal plants after shutting down nuclear ones, is reluctant to help provide fertilizer to poor nations due to climate change concerns.
This week I reported my experience with Air Conditioner Repair. The update is that the manager called me, apologized for how things were handled and gave me a full refund. Her explanation was that they are not equipped for these kinds of air conditioners so they should have turned the job down once they realized and walked away, and she’s going to call the technicians in and give them a stern talking-to. I explained that they not only didn’t turn down the job they then tried to tell me I needed to spend $28k on replacements, and she was all ‘yep, sorry about that, our bad, had no idea what we were doing and definitely shouldn’t have done that’ as if that made it better or something, rather than being an admission that they were trying to defraud me. So I still have to decide whether to spend effort being louder but I did get my refund so mostly the story ends here.
I also offered a fun little review of the charming little game This Merchant Life.
6 comments
Comments sorted by top scores.
comment by Florin (florin-clapa) · 2022-06-30T23:41:47.570Z · LW(p) · GW(p)
This is what happened:
Wrong expert opinion [EA · GW] (no airborne transmission) → respirators not recommended → multiple lockdowns until vaccines became widely available → millions of dead people, massive economic and social disruption
This could have easily happened:
Fast expert opinion change (no airborne transmission → airborne transmission) → use first lockdown to manufacture respirators for everyone → use respirators until pandemic burns out or vaccines and therapeutics become widely available → thousands of dead people, only one lockdown, minimal economic and social disruption
The ideal scenario (everyone prepped with respirators for decades) could have also happened but expert opinion seemed to have been too stubborn to have considered airborne transmission as a real possibility before this pandemic, and even when sufficient evidence was acquired, this opinion was slow to change.
For similar pandemics (or future variants of the current virus that won't respond to available vaccines or therapeutics) the solution is obvious: use respirators until the pandemic burns out or effective vaccines and therapeutics become widely available. Strangely, there still has been no big push to send respirators to areas of the world where vaccines and therapeutics like Paxlovid are less available.
Another thing that expert opinion continues to get wrong is its focus on the not-that-great disposable respirators [LW · GW] rather than the better-in-almost-every-way reusable respirators (including PAPRs [LW · GW]). If this doesn't change and another pandemic (or nasty variant) develops, the disposables will run out again, a lot of them will fail (as they probably do today) to provide adequate protection (due to poor face seals), and the results will be similar to (or worse than) the current pandemic.
comment by Aaron U (aaron-u) · 2022-06-30T15:09:49.075Z · LW(p) · GW(p)
In the meantime, at least we can still mask. If only anyone would tell us to do that.
Replies from: TrevorWiesinger↑ comment by trevor (TrevorWiesinger) · 2022-06-30T18:07:46.538Z · LW(p) · GW(p)
Make sure to wear a P100 mask instead of an N95 mask or lower, and to eat outdoors. Both of those things are cheap and well worth avoiding the risk of brain damage, which remains difficult to estimate due to vague or unreliable publications. Anyone wearing an inadequate mask will probably catch the virus again anyway, so there's not much point in worrying about the one-way valve.
comment by trevor (TrevorWiesinger) · 2022-06-30T15:12:05.459Z · LW(p) · GW(p)
- That was actually pretty close to best-case scenario with the air conditioner apology, that woman had one job and that job was to not admit to fraud by a slip of the tongue, no matter how skilled the person on the other end might be at making people slip up and admit to fraud. Admitting fault only works with medical malpractice lawsuits, maybe; and that's an apology for a clear mistake, not fraud.
- Whenever I hear someone affirm their belief that a large institution is trustworthy, this is the slogan I use in response: Large Powerful Institutions Are Never Trustworthy, Their Management Structure Fundamentally Requires Too Many Lawyers In Order To Defend Against Power-Hungry Opportunists,
- this is a slogan; in reality, listing the types of opportunists and defenses is better for conversation e.g. bribe-savvy billionaires, the military having a very short time horizon on something (e.g. a war or a brain-eating virus), and all the ambitious snakes constantly waiting for their once-in-a-lifetime chance to claw their way to the tippy-top
- Does anyone have an estimate of the probability/prioritization that the military is currently worried about an imminent foreign lab leak in the short-term, versus mainly being concerned with biodefense in the longer term?
We shouldn’t let people protect themselves against disease, because they might feel they were more protected than they are. So instead we should make it illegal for them to protect themselves.
That's actually reasonable, because the current vaccines don't protect people much in the first place. Most ordinary people I've met (generally urban areas) tend to think of vaccines and boosters as this perfect armor that make them totally fine. When in reality they're probably spreading the virus at mostly the same rate.
The authorities are not willing to dispel this misinformation because doing so might compromise mass vaccination campaigns in the future, with diseases that actually kill lots of people. Some things in public opinion last generations, like awareness of lobbyist influence, so the safest bet is to make vaccines as popular and beloved as possible. If vaccination is kept out of the headlines, then that is one less way that vaccination attitudes can be destabilized in the future (with future pandemics, vaccines not only might work, but also might prevent a deadlier virus from killing a third of the population). Especially if the virus itself doing just fine at imposing herd immunity upon the masses and nobody knows or cares about the brain damage that they are actively getting.
comment by UtilityMonster (Matt Goldwater) · 2022-07-01T04:06:47.901Z · LW(p) · GW(p)
If Omicron really is off in a complete different direction than any of the previous dominant strains, then that is importantly good news. It means that Omicron did not take Alpha, Beta or Delta and then add additional changes to make things worse. Instead, it did different things.
If that’s true, then it means the virus has gotten stuck via hill climbing at various points, and there’s a chance we don’t have to worry as much about Variant A → Variant B → Variant C → Variant D.
Why are the odds higher that a new variant that emerges from the current dominant strain would be more deadly than a new variant that emerged from something else? Especially since the current dominant strain is now Omicron rather than Delta.
comment by tkpwaeub (gabriel-holmes) · 2022-07-01T20:03:05.565Z · LW(p) · GW(p)
For #10, I'd replace it by a more agnostic "allow price gouging OR enforce nationwide rationing" - however you feel about free market vs government control, the idea that there's a conflict-free middle ground where we ban price gouging but don't go all in with rationing is pure fantasy.