Rob Bensinger's COVID-19 overview
post by habryka (habryka4) · 2020-03-28T21:47:31.684Z · LW · GW · 11 commentsThis is a link post for https://docs.google.com/document/d/10MFFoUMYHqGB3cLCxuqhsM2kahtOQVybPhLG-YNZdaI/
Contents
1. Why I think you should self-quarantine 2. Ways to reduce risk now: A. Avoid people, especially indoors. B. If you do need to be around people, face away from them, minimize talking, etc. C. If you do need to be around people, wear something over your mouth and nose. D. Don’t put coronavirus in your face. E. Have emergency supplies. F. Print out copies of your health records. G. Disinfect surfaces. H. Use copper tape or UVC light on commonly touched surfaces. I. Consume 2,000-6,000 IU of Vitamin D daily, in the morning. J. Run an air filter. K. Stay healthy: eat well, sleep well, get exercise. 3. Things to do if you get sick: A. Prepare in advance. B. Understand how COVID-19 usually presents and progresses, so you can make an informed guess about how likely you are to have it. C. Take zinc immediately if you start feeling any cold-, flu-, or COVID-19-like symptoms. D. Start monitoring your oxygen more often at the smallest warning sign. E. Take care of yourself. F. Lie on your front. G. Monitor for clotting problems. H. Consider taking more extreme measures if you're experiencing serious COVID-19 symptoms, or if you have the resources to take bonus precautions. None 11 comments
Robby posted this to Facebook on March 15th, and just updated section 2 and 3 with new information, making this I think currently one of the best guides to how to respond to this whole situation.
(Added Jun. 4: List of changes to this document. [LW(p) · GW(p)])
(Added Nov. 9: This document evolved from some recommendations I put together for friends, colleagues, and family on Feb. 27, when much less was known about COVID-19. At the time, it made sense to prepare for the worst and emphasize quick, dramatic action.
Over time, this document evolved into more conditional advice: rather than "lock down immediately," I assumed that different individuals would have different risk tolerances, and I try to give advice for how to mitigate risk without building in the assumption that everyone should be maximally cautious. Still, it's worth emphasizing these points explicitly:
- Pay attention to what's going on around you (e.g., COVID-19 rates in your area) and pick the risk level that makes sense for you, given your circumstances, your preferences, and the preferences of people you might expose.
- Being over-cautious has real costs, just as being under-cautious does.
For more COVID-19 information and recommendations, try microcovid.org or Zvi Mowshowitz's updates [? · GW].)
If you live in the US, I recommend that you self-quarantine immediately (to the extent that's possible for you) to avoid exposure to COVID-19, the new coronavirus disease. I'll explain why below, then give tips on how to reduce exposure and what to do if you get sick.
Quarantine isn't all-or-nothing, and every little bit helps. Even if you expect to catch COVID-19, you're likely to get sicker if you're exposed to more viral load early on.
(Paul Bohm says "pretty much any viral/bacterial dose study shows that result". Divia Eden: "As I understand it, the virus replicating is an exponential process, and antibody production is an exponential process too. So an early difference in load should make it easier for the latter to outpace the former.")
So even if you can't (e.g.) work from home right now, I would still recommend taking large measures to reduce your exposure.
Disclaimer: I put this document together in my free time to collect tips and background information I’d seen on COVID-19 from a variety of sources. I am not a doctor or an epidemiologist. In writing this, I prioritized breadth, clearness/useability, and getting information out quickly. I didn't put a lot of my own time into vetting each claim (though I plan to continue correcting errors as they’re pointed out to me), and I’d expect some of the information below to turn out later to be incorrect.
1. Why I think you should self-quarantine
[Section omitted from the crosspost, since most people appear to understand the importance of self-quarantine by now. The section can still be found here.]
2. Ways to reduce risk now:
A. Avoid people, especially indoors.
The CDC believes that COVID-19 is mainly spread person-to-person, "through respiratory droplets produced when an infected person coughs or sneezes. These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs."
COVID-19 has a long incubation period and high transmission rate, including significant asymptomatic transmission [LW · GW]. This means that talking [LW · GW] is also probably a common vector — you'd be surprised how much spit flies when people talk.
(Added Apr. 26: evidence continues to accumulate that talking is an important vector. COVID-19 superspreader events have typically involved large groups of people talking, singing, or shouting indoors. From Scott Gottlieb: “Study of 318 outbreaks in China found transmission occurred out-of-doors in only one, involving just 2 cases. Most occurred in home or public transport. Raises key chance for states to move services outdoors (religious, gym classes, restaurants, etc). https://www.medrxiv.org/content/10.1101/2020.04.04.20053058v1”)
So my top recommendation is to avoid being near other people (unless you're self-quarantining together), especially in crowded or indoor spaces.
(Added Mar. 16, from Michael Keenan: "Starting at midnight, all non-essential work and movement outside homes is banned in Alameda county and most other bay area counties. Grocery stores and pharmacies will remain open, and restaurants may still do takeout food (and presumably delivery), for those who are still using that." Similar measures may be taken elsewhere in the US soon; be prepared for the possibility.
(Added Apr. 26: cf. quick thoughts about the COVID-19 endgame.))
Added May 8: I recommend reading immunologist Erin Bromage’s The Risks — Know Them — Avoid Them in full. Some key claims:
- To get infected, you plausibly need to be exposed to ~1000+ SARS-CoV2 viral particles (source) — either all at once, or over minutes or hours. The more viral particles are present, and the more time you spend exposed to them, the greater your infection risk.
- “[T]he droplets in a single cough or sneeze may contain as many as 200,000,000 virus particles.” A single cough releases ~3000 (mostly large) droplets traveling at 50 mph (source). A single sneeze releases ~30,000 (mostly small) droplets traveling up to 200 mph (source). Smaller particles hang in the air longer. If someone sneezes or coughs, "even if that cough or sneeze was not directed at you, some infected droplets — the smallest of small — can hang in the air for a few minutes, filling every corner of a modest sized room with infectious viral particles. All you have to do is enter that room within a few minutes of the cough/sneeze and take a few breaths and you have potentially received enough virus to establish an infection."
- In contrast, "a single breath releases 50 - 5000 droplets", most of which fall to the ground quickly; nose-breathing releases even fewer droplets (source). "We don't have a number for SARS-CoV2 yet, but we [...] know that a person infected with influenza releases about 3-20 virus RNA copies per minute of breathing" (source). This suggests that if your only exposure to an infected person is via them silently breathing on the other side of a room, it will probably take an hour or longer for them to infect you.
- Speaking releases “~200 copies of virus per minute. Again, [pessimistically] assuming every virus is inhaled, it would take ~5 minutes of speaking face-to-face to receive the required dose” (source).
- A toilet flush aerosolizes droplets (which might contain viable virus), so “treat public bathrooms with extra caution (surface and air)” (source).
- “[P]lease don't forget surfaces. Those infected respiratory droplets land somewhere. Wash your hands often and stop touching your face!”
- “We know that at least 44% of all infections — and the majority of community-acquired transmissions — occur from people without any symptoms (asymptomatic or pre-symptomatic people) (source). You can be shedding the virus into the environment for up to 5 days before symptoms begin. [...] Viral load generally builds up to the point where the person becomes symptomatic. So just prior to symptoms showing, you are releasing the most virus into the environment.”
- “The main sources for infection are home, workplace, public transport, social gatherings, and restaurants. This accounts for 90% of all transmission events. In contrast, outbreaks spread from shopping appear to be responsible for a small percentage of traced infections.” (source). “The biggest outbreaks are in [nursing homes,] prisons, religious ceremonies, and workplaces, such [as] meat packing facilities and call centers.” Outbreaks seem to happen disproportionately often in colder indoor environments, and at larger and more social gatherings like weddings, funerals, birthdays, and networking events.
- “Indoor spaces, with limited air exchange or recycled air and lots of people, are concerning from a transmission standpoint. We know that 60 people in a volleyball court-sized room (choir) results in massive infections. Same situation with the restaurant and the call center. Social distancing guidelines don't hold in indoor spaces where you spend a lot of time, as people on the opposite side of the room were infected.
“The principle is viral exposure over an extended period of time. In all these cases, people were exposed to the virus in the air for a prolonged period (hours). Even if they were 50 feet away (choir or call center), even a low dose of the virus in the air reaching them, over a sustained period, was enough to cause infection and in some cases, death.
“Social distancing rules are really to protect you with brief exposures or outdoor exposures. In these situations there is not enough time to achieve the infectious viral load when you are standing 6 feet apart or where wind and the infinite outdoor space for viral dilution reduces viral load. The effects of sunlight, heat, and humidity on viral survival, all serve to minimize the risk to everyone when outside.” - You shouldn’t worry especially about “[brief visits to] grocery stores, bike rides, inconsiderate runners who are not wearing masks”. “[F]or a person shopping: the low density, high air volume of the store, along with the restricted time you spend in the store, means that the opportunity to receive an infectious dose is low.” If you have to work in a grocery store, or spend lots of time in an office or classroom — especially one with more people sharing the same space and/or air, or one that requires "face-to-face talking or even worse, yelling" — you should be much more worried.
Bromage says grocery stores aren't "places of concern", but I gather he means they’re relatively safe if you’re keeping a good distance from everyone, going when the store is pretty empty, etc. If a single cough from someone a few feet away who isn’t facing in my direction can give me COVID-19 within a few seconds, that still seems “concerning” to me!
Additionally, Jim Babcock comments on “infections while shopping appear to be responsible for 3-5% of infections”:
The source for this covers Ningbo from January 21 to March 6. My main worry, when looking at this number, is that Ningbo's mitigations may have been more effective for stores than they were for other places, in ways that don't generalize to the US. For example, I'm pretty sure they would have been screening people for fever on entry, and enforcing mask usage. I haven't been hearing of fever-screens in Berkeley (though I haven't really been out of the house), and while we do now have a mask ordinance, it's mostly cloth masks (which are less effective) and compliance doesn't seem to be very good.
And:
The specific number for the ~1000 virus-particle claim is cited to a pretty sketchy source; it leads to a couple epidemiologists speculating with no data, and what they actually say is:
> "The actual minimum number varies between different viruses and we don’t yet know what that ‘minimum infectious dose’ is for COVID-19, but we might presume it’s around a hundred virus particles."
and
> "For many bacterial and viral pathogens we have a general idea of the minimal infective dose but because SARS-CoV-2 is a new pathogen we lack data. For SARS, the infective dose in mouse models was only a few hundred viral particles. It thus seems likely that we need to breathe in something like a few hundred or thousands of SARS-CoV-2 particles to develop symptoms. This would be a relatively low infective dose and could explain why the virus is spreading relatively efficiently."
So there's uncertainty of about an order of magnitude, here. On the other hand, the broader claim--that exposure size matters--is almost certainly true, and the implications of the specific number 1000 are mostly screened off by more-specific observations of which places people are getting it.
Bromage has softened the grocery store claim to “In contrast, outbreaks spread from shopping appear to be responsible for a small percentage of traced infections.”, and now cites an additional two studies for the 1000-particle claim: 1, 2.
B. If you do need to be around people, face away from them, minimize talking, etc.
Added Jun. 2: Jonathan Kay writes on Apr. 23,
According to the binary model established in the 1930s, droplets typically are classified as either (1) large globules of the Flüggian variety—arcing through the air like a tennis ball until gravity brings them down to Earth; or (2) smaller particles, less than five to 10 micrometers in diameter (roughly a 10th the width of a human hair), which drift lazily through the air as fine aerosols.
[...] Despite the passage of four months since the first known human cases of COVID-19, our public-health officials remain committed to policies that reflect no clear understanding as to whether it is one-off ballistic droplet payloads or clouds of fine aerosols that pose the greatest risk—or even how these two modes compare to the possibility of indirect infection through contaminated surfaces (known as “fomites”).
Gaining such an understanding is absolutely critical to the task of tailoring emerging public-health measures and workplace policies, because the process of policy optimization depends entirely on which mechanism (if any) is dominant:
1. If large droplets are found to be a dominant mode of transmission, then the expanded use of masks and social distancing is critical, because the threat will be understood as emerging from the ballistic droplet flight connected to sneezing, coughing, and laboured breathing. We would also be urged to speak softly, avoid “coughing, blowing and sneezing,” or exhibiting any kind of agitated respiratory state in public, and angle their mouths downward when speaking.
2. If lingering clouds of tiny aerosol droplets are found to be a dominant mode of transmission, on the other hand, then the focus on sneeze ballistics and the precise geometric delineation of social distancing protocols become somewhat less important—since particles that remain indefinitely suspended in an airborne state can travel over large distances through the normal processes of natural convection and gas diffusion. In this case, we would need to prioritize the use of outdoor spaces (where aerosols are more quickly swept away) and improve the ventilation of indoor spaces.
3. If contaminated surfaces are found to be a dominant mode of transmission, then we would need to continue, and even expand, our current practice of fastidiously washing hands following contact with store-bought items and other outside surfaces; as well as wiping down delivered items with bleach solution or other disinfectants.
Zvi Mowshowitz comments [LW · GW]:
Identified Super Spreader Events are Primarily Large Droplet Transmission
The article makes a strong case that in identified super spreader events [SSEs] the primary mode of transmission is large droplets. And that large droplets are spread in close proximity, by people talking (basically everything) or singing (several choir/singing practices) frequently or loudly, or laughing (many parties) and crying (funerals), or otherwise exhaling rapidly (e.g. the curling match) and so on.
There is a highly noticeable absence of SSEs that would suggest other transmission mechanisms. Subways and other public transit aren’t present, airplanes mostly aren’t present. Performances and showings of all kinds also aren’t present. Quiet work spaces aren’t present, loud ones (where you have to yell in people’s faces) do show up. University SSEs are not linked to classes (where essentially only the professor talks, mostly) but rather to socializing. [...]
Zvi argues that surfaces and small aerosolized droplets are unlikely to be major infection vectors for COVID-19. He discusses methods for avoiding large droplet transmission:
Large Droplets: Six Foot Rule is Understandable, But Also Obvious Nonsense
For large droplets, there is essentially zero messaging about angling downwards or avoiding physical actions that would expel more droplets, or avoiding being in the direct path of other people’s potential droplets.
Instead, we have been told to keep a distance of six feet from other people. We’ve told them that six feet apart is safe, and five feet apart is unsafe. Because the virus can only travel six feet.
That’s obvious nonsense. It is very clear that droplets can go much farther than six feet. Even more than that, the concept of a boolean risk function [i.e., one that sharply divides everything into either "risky" or "risk-free", with no shades of grey] is insane. People expel virus at different velocities, from different heights, under different wind conditions and so on. The physics of each situation will differ. The closer you are, the more risk.
Intuitively it makes sense to think about something like an inverse square law until proven otherwise, so six feet away is about 3% of the risk of one foot away. That’s definitely not right, but it’s the guess I feel comfortable operating with.
Alas, that’s not the message. The message is 72 inches safe, 71 inches unsafe.
Unlike the previous case of obvious nonsense, there is a reasonable justification for this one. I am sympathetic. You get about five words. “Always stay six feet apart” is a pretty good five words. There might not be a better one. Six feet is a distance that you can plausibly mandate and still allow conversations and lines that are moderately sane, so it’s a reasonable compromise.
It’s a lie. It’s not real. As a pragmatic choice, it’s not bad.
The problem is it is being treated as literally real.
Joe Biden and Bernie Sanders met on a debate stage. The diagram plans had them exactly six feet apart.
In an article, someone invites the author, a reporter, to their house to chat. Says he’s prepared two chairs, six feet apart. “I measured them myself,” he says. [...]
And so on. People really are trying to make the distance exactly six feet as often as possible.
[...] This is society sacrificing bandwidth to get a message across. Again, I get it. The problem is we are also sacrificing any ability to convey nuance. We are incapable, after making this sacrifice, of telling people there is a physical world they might want to think about how to optimize. There is only a rule from on high, The Rule of Six Feet.
Thus, we may never be able to get people to talk softly into the ground rather than directly looking at each other and loudly and forcefully to ‘make up for’ the exact six foot distance, which happens to be the worst possible orientation that isn’t closer than six feet.
In theory, we can go beyond this. You get infected because droplets from an infected person travel out of their face and touch your face.
Thus, a line is remarkably safe if everyone faces the same way, modulo any strong winds. The person behind you has no vector to get to your face. And we can extend that. We can have one sidewalk where people walk north, and another on the other side of the street where people walk south. If you see someone approaching from the other direction, turn around and walk backwards while they ensure the two of you don’t collide. If necessary, stand in place for that reason. Either way, it should help – if this is the mechanism we are worried about.
[...] Yes, it’s annoying to not face other people, but you absolutely can have a conversation while facing away from each other. It’s a small price to pay.
In similar fashion, it seems a small price to pay to shut the hell up whenever possible, while out in public. Talking at all, when around those outside your household, can be considered harmful and kept to a bare minimum outright (and also it should be done while facing no one).
Zvi emphasizes that there’s much more benefit to slightly reducing the risk from the largest infection sources (including large droplets as a category), than from hugely reducing the risk from fairly unlikely infection sources:
Focus Only On What Matters
[...] Within those big risks, small changes matter. They matter more than avoiding small risks entirely.
A single social event, like a funeral, birthday party or wedding, might well by default give any given person a 30%+ rate to infect any given other person at that event if the event is small, and a reasonably big one even if large. You only need one. Keeping slightly more distance, speaking slightly less loudly, and so on, at one such event, is a big risk reduction. [...]
Whereas a ‘close contact’ that doesn’t involve talking or close interaction probably gives more like (spitballing a guess, but based on various things) an 0.03% rate of infection if the other person is positive, and likely with a lower resulting viral load. Certainly those contacts add up, but not that fast. Thus, a subway car full of “close contact” might give you 10 of them per day, most of whom are not, at any given time, infectious. If this model is correct.
In another post, Zvi writes [LW · GW]:
Risks Follow Power Laws
[...] Slight reductions in the frequency and severity of your very risky actions is much more important than reducing the frequency of nominally risky actions.
The few times you end up talking directly with someone in the course of business, the one social gathering you attend, the one overly crowded store you had to walk through, will dominate your risk profile. Be paranoid about that, and think how to make it less risky, or ideally avoid it. Don’t sweat the small stuff.
And think about the physical world and what’s actually happening around you!
And:
My best guess is there is something like 5-10 times as much risk indoors versus the same activity outdoors. [...]
The combination of quick and outdoors and not-in-your-face probably effectively adds up to safe, especially if you add in masks. During the peak epidemic in New York things were so intense that it would have been reasonable to worry about miasma. Now, I would do my best to keep my distance and avoid talking at each other, but mostly not worry about incidental interactions.
I do expect there to be a spike in cases as the result of protests and civil unrest.. To not see one would be surprising, and would update me in favor of outdoor activities being almost entirely harmless.
C. If you do need to be around people, wear something over your mouth and nose.
Be sure not to touch/adjust the mask/covering (or your face) while wearing it, except to take it off (and throw it away or sanitize it) when you're done using it.
I've heard some people claim masks aren't useful, but this is wrong, provided you're careful to wear them correctly.
- https://jamanetwork.com/journ…/jama/article-abstract/2749214
- https://jamanetwork.com/journals/jama/fullarticle/184819
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2662779/
- https://academic.oup.com/cid/article/65/11/1934/4068747
If you don't have surgical masks, home-made masks or scarves can also be effective. This study shows that home-made masks (made from tea cloth) were less effective than surgical masks, but still useful.
Added Mar. 28: Scott Alexander reviews the literature and concludes, "If the shortage ends, and wearing a mask is cost-free, I agree with the guidelines from China, Hong Kong, and Japan – consider wearing a mask in high-risk situations like subways or crowded buildings. Wearing masks will not make you invincible, and if you risk compensate even a little it might do more harm than good. Realistically you should be avoiding high-risk situations like subways and crowded buildings as much as you possibly can. But if you have to go in them, yes, most likely a mask will help."
Added Apr. 26: For homemade masks, Hrothgar says:
[...] I'd choose the thickest, most finely woven materials available and layer them as much as possible without making it difficult to breathe. Then I'd wear those outside, taking all other precautions (distance, goggles, etc), and breathe SLOWLY through my nose. Slowly because lower air velocity reduces penetration, nose because it acts as a filter as well. Then I'd wash everything immediately & thoroughly upon arriving home.
Source: Combine these studies about the effectiveness of cloth/DIY masks
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2440799/
https://academic.oup.com/annweh/article/54/7/789/202744
with this tweet (by a virologist) about the importance of initial viral load
https://twitter.com/PeterKolchinsky/status/1239560638239838215
and then the missing piece is about droplet size + filter grain, which will vary based on what you put over your face.
Thicker materials are better, as you might expect. Towels & Hanes sweatshirts performed best in this study:
Added Jun. 2: Zvi Mowshowitz writes [LW · GW], “[E]ven cloth masks on both ends of an interaction are almost certainly good for a 25% reduction in risk and probably 50%-75%.”
D. Don’t put coronavirus in your face.
From Patrick LaVictoire:
Like most respiratory diseases, coronavirus is transmitted in water droplets coughed or sneezed out by sick people. If the droplets dry out completely, the virus is destroyed.
They dry out in air pretty quickly- if you’re more than ten feet away, you’re unlikely to inhale them. But on surfaces including metal, glass, and plastic, they can persist for hours or even days. (That’s where the bleach wipes come in; clean your sink handles, especially, in case someone comes in with the virus and washes it off.)
The biggest danger, then [if you're avoiding social contact with others], is that you will touch a surface with coronaviruses on it, and then (before washing your hands thoroughly) touch your mouth, nose, or eyes. Once the virus is in one of those, you’re likely to get sick.
So the number one tip is to learn, now, to stop touching your face with your hands.
PBS says (added Mar. 30):
What’s the best surface for killing viruses? Our skin. In the cases of both flu and cold-causing viruses, infectious particles on our hands are usually gone after 20 minutes.
Between its pH and its porous nature, our body’s natural barrier to the word does a great job at killing viruses, Greatorex explained. “Our hands are quite antimicrobial themselves,” she said. “They have their own bacteria that live on them — no matter how clean you are — and they don’t actually harbour viruses that well.”
So I could imagine it being quite helpful to switch from touching your mucous membranes once every few minutes to doing so once every few hours.
I hear that surface transmission wasn't the primary way SARS spread, so I'm not sure how worth worrying about surfaces are. A lot of people have noted that coronavirus can survive on surfaces up to 9 days in certain conditions (or even longer if it's cold), but Will Eden says: "This paper is the source of the 9 day figure. However that’s the maximum length on any surface under ideal conditions. In some cases it only lasts hours. And it doesn’t establish whether any of that is infectious!"
Regardless, my other three main recommendations are: spend less time touching surfaces that a large number of other people touch (added: or talk near); try to minimize how much you touch your eyes, nose, or mouth; and wash your hands more often, using full medical hand-washing protocol (image; mnemonic; animated version). Note that for COVID-19, hand sanitizer isn't a good replacement for hand-washing.
{kind=link}
{kind=link}
Added Jun. 2: Zvi Mowshowitz argues [LW · GW]:
It’s been months. We don’t have concrete examples of infection via surfaces. At all. It increasingly seems like while such a route is possible, and must occasionally happen, getting enough virus to cause an infection, in a live state, via this route, is very hard. When you wash your hands and don’t touch your face, it’s even harder than that.
Meanwhile, those who refuse to touch surfaces like a pizza delivery box end up in more crowded locations like grocery stores, resulting in orders of magnitude more overall risk.
[...] Until I get very unexpected evidence, surfaces are mostly not a thing anymore. If lots of people touch stuff and then you touch it, sure, wash your hands after and be extra careful to not touch your face in the interim. Otherwise, stop worrying about it.
[... Food] is at most minimally risky, even if it doesn’t get heated enough to reliably and fully kill the virus. You don’t have to ruin all your food. People are often avoiding foods that seem risky. Once again, it makes sense that it could be risky, but in practice it’s been months and it does not seem to work that way. The precautions people are taking will incidentally be more than good enough to guard against contamination of food at sufficient levels to be worth worrying about. I mean, sure, don’t eat at a buffet, but it’s not like any of them are going to be open, and even then the (also mostly safe) surfaces are likely scarier than the food.
[...] Your risk is from the waiter, or from the other diners, being in that room with you for a while. Thus, takeout, delivery and/or eating outdoors.
I agree with Zvi that it seems increasingly likely that surface transmission is rare, though he seems to be wrong that there are no examples (see comments [LW · GW]), and I haven’t seen a clear argument for whether the number of COVID-19 cases caused by surface transmission is closer to 1/10 of all cases versus, say, 1/10,000. Given my own circumstances, I’m likely to do things like “order delivery pizza” more often in the weeks to come, but I’ll also likely make use of Yao Lu’s tips while infections are still commonplace in my part of the US:
I’m a chemo nurse, this is what I tell my high-risk patients:
I personally don’t trust takeout that much because I think a lot of restaurant workers don’t have sick leave, so it’s more likely your food was prepared by someone symptomatic. But you can cut the risk to near zero by doing this:
1. Wash your hands well
2. Put your own bowl on your kitchen counter
3. Pick up the restaurant container, and pour the food into your own bowl
4. Throw away the restaurant container
5. Wash your hands well
6. Thoroughly heat up the food. (at least 70C for a minute, or whatever the best current guideline says)
If you do this, in this order, you are extremely safe even if someone coughed viruses all over the food and the container. Heat would kill the virus, and handwashing would prevent indirect transmission from the bag/container.
E. Have emergency supplies.
I would recommend stockpiling at least a month of non-perishable food. 2-3 months is even better. Err on the side of buying food that you like; idiosyncratic favorite foods are less likely to be sold out on Amazon right now, and it's important to make your self-quarantine pleasant so you're less likely to want to take unnecessary risks later.
From residents of the Event Horizon house (https://docs.google.com/…/1Rn6WrTat0Cb6gfatWv-TcSBToh3…/edit): "Most dedicated disaster prep food is already sold out, but you could get a bunch of canned foods (e.g. beans, fish, vegetables, fruits) and dry foods (e.g. rice, pasta, dried fruit, peanut butter) that you like and can eat."
I would similarly stock up on other essential items, especially medications you need.
Added Apr. 26: The CDC recommends having a two-week backup supply of clean drinkable water. I would recommend stockpiling 1+ months of water (i.e., 30+ gallons per person) if you have room. The Guardian reports Apr. 20 that there’s an emerging shortage of CO2, and The Prepared notes that “CO2 is an essential input for the municipal water treatment process. (It’s also vital to many critical industrial processes–from agriculture to meat processing to food preservation).” The Prepared also notes other chemicals used in water treatment whose supply could be disrupted in various scenarios.
F. Print out copies of your health records.
From Event Horizon: "If hospital infrastructure is overwhelmed, you may not be able to access this information. The most important information to have on hand is your history of major health problems and surgeries, immunization records, and medications you are currently taking. Here is a template for such a health record: https://docs.google.com/…/1fCCTcwrULo5w4vnymhziCVdctM…/edit…"
G. Disinfect surfaces.
(Especially commonly touched surfaces like door handles and light switches.)
The WHO notes, "In China, human-to-human transmission of the COVID-19 virus is largely occurring in families [...] most clusters (78%-85%) have occurred in families." Divia Eden comments: "One of my takeaways was that delivery of packages was unlikely to be a major vector, in China anyway."
That said, packages may still be the main risk source for you if relying on packages for food; and the risk may rise in contexts where containment measures have failed and the virus is more widespread globally. So if it's not too much trouble for you, or if you're unusually at risk, it probably makes sense to sanitize packages too.
The easy version of this is letting packages sit in direct sunlight for a while before opening them. Heat and UV radiation are good for killing coronavirus. (Added Mar. 28: https://www.nejm.org/doi/full/10.1056/NEJMc2004973 reports, "SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard, and viable virus was detected up to 72 hours after application to these surfaces (Figure 1A), although the virus titer was greatly reduced[....] On copper, no viable SARS-CoV-2 was measured after 4 hours[....] On cardboard, no viable SARS-CoV-2 was measured after 24 hours[.]")
Fortunately, the hard version is only slightly harder, since coronaviruses are easy to kill with a wide variety of cleaning agents. From https://en.wikipedia.org/wiki/Viral_envelope, discussing enveloped viruses in general: "The lipid bilayer envelope of these viruses is relatively sensitive to desiccation, heat, and detergents, therefore these viruses are easier to sterilize than non-enveloped viruses, have limited survival outside host environments, and typically transfer directly from host to host."
Good options for cleaning agents include 70% isopropyl alcohol (note: higher or lower percentages may be less effective; see also Sarah Constantin’s review) or the items on this (CDC-referenced) list: https://www.americanchemistry.com/Novel-Coronavirus-Fightin….
Important update from Duncan Sabien (added Apr. 29): “PSA: if (e.g.) getting ice cream delivered by a third party, or doing disinfection that involves wiping or dunking the ice cream such that it melts a good bit before you finally get it into the freezer ... Haagen Dasz is like 3x better at refreezing back to ice cream texture and consistency than Ben and Jerry's. Don't know why; just know the brute fact.”
Added Jun. 2: See also Zvi Mowshowitz’s recommendations to worry less about surfaces [LW · GW], quoted above.
H. Use copper tape or UVC light on commonly touched surfaces.
(Updated Apr. 1)
From Sarah Constantin:
Frequently touched items, especially in public places, should probably just be irradiated with UVC light and/or coated with copper as a routine prevention measure.
(Regular UV light is an effective disinfectant but can also blind people and burn skin; UVC is a shorter wavelength, equally effective against microbes but not harmful to eyes or skin.)
UVC is used in germicidal lamps and germicidal irradiation. Far-UVC light (207-222 nm) seems safest for human skin.
Solid copper doesn't kill viruses on contact, but it makes it hard for viruses to survive on a timescale of minutes or hours (https://www.lesswrong.com/…/coronavirus-justified-practical… [LW(p) · GW(p)]). Putting copper tape (Amazon link) on things like cell phones, door handles, and light switches can therefore reduce risk.
Try to minimize wrinkles in applied copper tape, so that taped surfaces remain easy to disinfect as needed. Robert Miles suggests: "Tape should be cut to the right size, and you need a tool which is finger shaped, harder than a finger but softer than copper - wood or plastic is good, I use the rounded end of a swiss army knife. Running that along seams and small creases makes them mostly disappear". Be careful of papercuts.
I. Consume 2,000-6,000 IU of Vitamin D daily, in the morning.
"Since COVID usually kills via pneumonia, and insufficient vitamin D appears to be a surprisingly large risk factor in respiratory infection, it’s probably pretty important to keep vitamin D levels sufficient (which in most people means supplementing it specifically, esp if there’s any quarantine that affects food)." (https://www.lesswrong.com/…/coronavirus-justified-practical… [LW(p) · GW(p)])
Added May 8, from Jim Babcock:
Wikipedia summarizes https://pubmed.ncbi.nlm.nih.gov/21419266/ as "vitamin D functions to activate the innate and dampen the adaptive immune systems". Assuming that's true (I haven't verified it, and vitamin D is a subject known for attracting sketchy claims), then deficiency would lower the minimum infectious dose. On a population scale, this would be a better explanation for the infections-latitude correlation than temperature is, and would suggest that mass-distributing vitamin D supplements would be a good R-lowering strategy.
J. Run an air filter.
Sarah Constantin: "In a retrospective study in Utah hospitals, high concentrations of particulate matter in the air were associated with slightly but significantly higher (OR = 1.004) rates of admission to the emergency room for pneumonia, and slightly (OR = 1.02) but significantly higher rates of pneumonia mortality.[12] Having air filters in the home may be slightly protective."
K. Stay healthy: eat well, sleep well, get exercise.
(Added Apr. 27: And consider avoiding things that might put you in a hospital, like motorcycle races or getting pregnant; hospitals are risky during pandemics.)
3. Things to do if you get sick:
(Mar. 28 update: I largely rewrote this section today. This section remains relatively speculative and subject to change. COVID-19 is a new disease that we're still in the early stages of understanding, and as Sarah Constantin notes, there aren't many good studies on how best to treat flu- or pneumonia-like illnesses from home. Still, phlegm and flu wait for no man, and we're forced to make the best guesses we can with the available evidence.)
A. Prepare in advance.
Things to buy right now for if you get sick: Pedialyte or gatorade powder, over-the-counter inhalers, a humidifier, acetaminophen, mucinex/guaifenesin, pseudoephedrine, zinc lozenges, oral thermometers, and a finger pulse oximeter. Maybe hydroxychloroquine or chloroquine and/or a home oxygen concentrator, if you can find it online or get it prescribed by your doctor. See below for details.
While still healthy, take your temperature (orally) and use your finger pulse oximeter. Do this multiple times per day over several days, to make sure the devices are working and to get a sense of your baseline numbers.
(Added Apr. 26: given the “silent hypoxia” update at the bottom of 3D below, and the blood clot update in 3G below, you should probably use the pulse oximeter regularly even if you’re showing no symptoms, and should stay alert for signs of stroke, heart attack, or pulmonary embolism even if you’re showing no other symptoms.)
Figure out who can help take care of you if you get sick.
Added Jun. 2: Plan in advance what hospital you’ll go to if necessary, and be ready to call a doctor if you have troubling symptoms. Zvi Mowshowitz writes [LW · GW]:
Medical care matters [for fatality rates]. Total breakdown of medical care in practice leads to several times the fatality rate under regular circumstances. High quality treatment at current knowledge levels can probably drive death rates down further, so the ratio between full success and complete breakdown can be rather large – something like an order-of-magnitude difference between 0.2% and 2%.
I don’t have a strong opinion at this point about particular medical treatments beyond the above.
B. Understand how COVID-19 usually presents and progresses, so you can make an informed guess about how likely you are to have it.
Direct testing can obviously help, but depending on where you are and what symptoms you have, it may be very difficult to get tested in the US, and the test results may come back too late to be useful. It's still worth getting tested if circumstances allow, e.g., to clarify treatment priorities, aid in containment, or check for other infections. Per Sarah Constantin:
It’s important to get tested by a doctor if you have a respiratory illness you think is COVID-19. Even if you can’t get access to a COVID-19 test, you might also have a different bacterial or viral infection (either instead of or in addition to COVID-19) which is treatable by antivirals or antibiotics. It’s very common for viral pneumonia to be complicated by an opportunistic bacterial infection, and killing the bacteria can help improve outcomes.
As of Feb. 24, the WHO listed COVID-19 as causing these symptoms with the following frequencies:
fever (87.9%), dry cough (67.7%), fatigue (38.1%), sputum production (33.4%), shortness of breath (18.6%), sore throat (13.9%), headache (13.6%), myalgia [muscle pain] or arthralgia [joint pain] (14.8%), chills (11.4%), nausea or vomiting (5.0%), nasal congestion (4.8%), diarrhea (3.7%), and hemoptysis [coughing up blood] (0.9%), and conjunctival congestion [inflammation in the white of the eye] (0.8%).
(Also, up to 50% of infections might be asymptomatic, while still being contagious [LW(p) · GW(p)].)
The WHO report continues:
People with COVID-19 generally develop signs and symptoms, including mild respiratory symptoms and fever, on an average of 5-6 days after infection. [...] Using available preliminary data, the median time from onset to clinical recovery for mild cases is approximately 2 weeks and is 3-6 weeks for patients with severe or critical disease. Preliminary data suggests that the time period from onset to the development of severe disease, including hypoxia [serious lack of oxygen], is 1 week.
(For adults, you’re generally considered to have a fever if you have an orally measured body temperature of 100.4°F / 38 °C.)
(Added Apr. 5: Anna Salamon says, “Median incubation period is probably 7 days, not 5 days; early studies that resulted in the 5-day estimate were done only on people who end up hospitalized, and those who don't (and who have somewhat milder infections) turn out to have somewhat longer incubation periods. Source: https://www.medrxiv.org/content/10.1101/2020.03.15.20036533v1”)
From Vox:
'Covid-19 disease usually begins with mild fever, dry cough, sore throat and malaise,' writes Megan Murray, a professor of epidemiology at Harvard Medical School, in an FAQ for the Abundance Foundation. 'Unlike the coronavirus infections that cause the common cold, it is not usually associated with a runny nose.' These symptoms emerge five or six days after infection on average, but can show up in as little as a day or as much as two weeks after exposure.
From Business Insider, a day-by-day progression of typical cases:
Day 1: Patients run a fever. They may also experience fatigue, muscle pain, and a dry cough. A small minority may have had diarrhea or nausea one to two days before.
Day 5: Patients may have difficulty breathing — especially if they are older or have a preexisting health condition.
Day 7: This is how long it takes, on average, before patients are admitted to a hospital, according to the Wuhan University study.
Day 8: At this point, patients with severe cases (15%, according to the Chinese CDC) develop acute respiratory distress syndrome, an illness that occurs when fluid builds up the lungs. ARDS is often fatal.
Day 10: If patients have worsening symptoms, this is the time in the disease's progression when they're most likely to be admitted to the ICU. These patients probably have more abdominal pain and appetite loss than patients with milder cases. Only a small fraction die: The current fatality rate hovers at about 2%.
Day 17: On average, people who recover from the virus are discharged from the hospital after 2 1/2 weeks.
Elizabeth van Nostrand has been looking into what the earliest symptoms of COVID-19 infection tend to be. She writes [LW(p) · GW(p)]:
Most academic/medical papers start with the person’s first contact with the medical system, which is too late, so I looked at social media and news reports. These are obviously going to be biased towards people with symptoms severe enough to be interesting, but not so severe as to die. I also restricted myself to test-confirmed cases, which because I was also looking at mostly American sources biases things towards severe cases. And I’m counting on people to represent themselves honestly. So there’s a lot going against this sample.
In total I found 11 cases, plus two notes from doctors doing front line work. [...] From this very small and biased sample:
- 36% of people started with a cough on their first day (55% if you count two people who had very mild symptoms on day 1 and developed a cough on day 2)
- 64% started with a fever.
- 18% of people started with both on the same day.
- 18% started with neither symptom (but developed a cough on day 2)
- 78% eventually developed a cough
- 91% eventually developed a fever. The only person who didn’t eventually develop a fever I think might be a false positive, because his symptoms were very weird.
- 27% had digestive symptoms (mostly nausea)
- 1/3 of recovered people had been hospitalized. [...]
You may have heard that 80% of cases are mild. Keep in mind that that paper defined mild to include mild pneumonia, which I would classify as at least moderately severe.
From Sky News:
The British Association of Otorhinolaryngology (ENT UK) say asymptomatic patients - ones who do not have a fever or a cough - could show a loss of smell or taste as symptoms after contracting coronavirus. [...] 'In [many] young patients, they do not have any significant symptoms such as the cough and fever, but they may have just the loss of sense of smell and taste, which suggests that these viruses are lodging in the nose.' [...] Dr Nathalie MacDermott, clinical lecturer at King's College London said infections that normally occur through the 'nose or the back of the throat" often lead to a loss in sense of smell and taste, but cautioned that research around the new symptoms for COVID-19 isn't yet widespread in the medical community.'
Stat reports that anywhere from 30% to 67% of COVID-19 patients temporarily lose their sense of smell.
One study found higher rates of digestive issues (103 out of 204 cases), broadly construed. 40% of patients experienced lack of appetite, 17% diarrhea, 2% vomiting, 1% abdominal pain. "Moreover, the digestive symptoms among the larger group grew more severe as the severity of COVID-19 increased[.]"
COVID-19 can also present with rashes on the limbs. And the virus can apparently infiltrate cerebrospinal fluid and can cause neurological symptoms.
So... apparently COVID-19 symptoms include "approximately everything".
COVID-19's presentation seems to vary a lot. Typically, if you see symptoms at all, you'll see respiratory symptoms such as coughing, chest tightness, or shortness of breath; and these are the symptoms to keep the closest eye on, since COVID-19 deaths are usually via respiratory failure. But I've also heard accounts of pretty debilitating-sounding fatigue or intense/long-lasting fever. E.g. (from an unconfirmed case):
[...] IT CAN LAST FOR AGES: Onto what I didn’t expect (or hadn’t been prepared for) symptoms wise. The main thing was the sheer length of it – though again, in my own case it was over very rapidly. Isabel wasn’t so lucky. Fevers are nasty, but this was a fever that ground on for days without really breaking or spiking. The duration of C19 seems to be one of the unusual things about it – in Isabel’s case it peaked around day 8 (the worst of the fever), then again on day 10 (the worst of the breathing issues, which luckily were still mild). Apparently for hospitalised survivors in Wuhan the median release day was Day 24. Be prepared for a long haul.
IT EBBS AND FLOWS: This is something I really wish I’d been expecting – for Isabel, C19 didn’t follow a predictable pattern of worsening, peaking and recovery. There was a period of initial but manageable illness, then a rapid decline into being entirely bedridden, then two separate peaks of illness with improvements in between, and only now a sustained recovery. It took her until Day 11 to say “I’m feeling a bit better”, and as an observer there were clear rallies and declines along the way, which made everything particularly nerve-racking: you never quite know if things have improved, and declines are especially frightening.
THE BEST-KNOWN SYMPTOMS MIGHT NOT BE THE WORST: If you’re like me, when you think of Coronavirus you think fever, dry cough and changes in breathing, which are the signature symptoms. Isabel had all of those, but for her the worst effects were exhaustion, nausea, aches and dehydration. She was weakened by it to a degree I’ve never seen outside very old and ailing relatives, well beyond any flu either of us have had. She needed a constant supply of painkillers and water (which she was often too weak to actually lift to her lips) and had zero appetite. In a non-pandemic – or if she was on her own – she would definitely have been in hospital. As it was, fortunately her breathing was never bad enough to need that.
The "ebbs and flows" aspect of COVID-19 seems very common in anecdotal reports. E.g., from another unconfirmed case:
3/7 - I attended a party with at least one known person that tested positive, and >5 others that reported similar symptoms on an almost identical timeline
3/9 - Day 1 - Mild fever (99.5) for a few hours. Chills. Headache. It was gone by the evening
3/10-11 - Days 2-3 - Muscle pain, fatigue - both pretty mild
3/12-14 - Days 4-6 - I felt better, no symptoms at all. This led me to believe it was just a head cold
3/15-16 - Days 7-8 - I had a tightness in my chest and some difficulty breathing. This is when I started suspecting it might not be a cold
3/17 - Day 9 - Cough started. Mild, but dry. Throat is irritated.
3/18 - Day 10 - No more cough, no more chest tightness, no trouble breathing. Throat is slightly irritated but feels like I’m getting better
3/19-20 - Days 11-12 - Uh oh. Fever comes and goes throughout the day, much harder to breath, cough is back and is worse. The shortness of breath was sudden and very unpleasant.
3/21 - Day 13 - Today. Right now I feel better than I did all week. No fever, no difficulty breathing, and no cough. But I’ve been tricked before so I’m being patient and giving it a few more days to be sure. I don’t think I’m quite out of the woods yet. [...]
Well, it definitely wasn't over when I wrote this post on day 13. That night had another wave of chest pain and shortness of breath and days 14 and 15 felt like a low grade asthma attack that wouldn't go away.
Days 16 and 17 - The dry cough turned into a productive cough and the combination of mucinex and hot tea gave me some relief.
Today, day 18, I finally feel mostly ok. I'm not coughing and I can breathe!
Unfortunately, the lab I got tested with was shut down by the FDA so I won't be getting my test result: https://www.nytimes.com/…/coronavirus-home-testing-swab-kit… [...]
Some notes:
1. Don’t trust the 'lull'. This progression seems to be pretty common - one slightly feverish day, then back to normal, and then the second wave. Or third [and fourth], in my case. I wish I had been more aware of this - I exposed some people on days 4-6. So far none of them are showing symptoms, but I would have acted differently if I had known this was a typical covid pattern.
2. It is really useful to have a pulse oximeter. Get one on amazon for <20$. This let me check my vitals even in the middle of the worst part of not being able to breathe and see that my oxygen levels were normal (97-99). I would've made my way to a hospital if it had dropped <90[.]
Symptoms like runny noses are useful to track because their presence provides some evidence that you don't have COVID-19. Colds tend to cause sneezing, whereas COVID-19 and flu don't cause sneezing. Colds also cause runny or stuffy nose, which are rare in COVID-19 (and somewhat uncommon in the flu). And the flu has a sudden onset, whereas COVID-19 and colds usually have gradual onsets.
That said, since COVID-19 is especially dangerous and can present in a variety of ways (and it's always possible you have COVID-19 and another illness), you should be careful not to prematurely rule out the possibility that you have COVID-19.
C. Take zinc immediately if you start feeling any cold-, flu-, or COVID-19-like symptoms.
Zinc lozenges "have been proven to be effective in blocking coronavirus (and most other viruses) from multiplying in your throat and nasopharynx. Use as directed several times each day when you begin to feel any "cold-like" symptoms beginning. It is best to lie down and let the lozenge dissolve in the back of your throat and nasopharynx. Cold-Eeze lozenges is one brand available, but there are other brands available." (Sources: this + this)
The discussion on LessWrong [LW · GW] suggests that ordinary zinc lozenges may be ineffective for various reasons, and that one of the only products that seems likely to be effective is 'Life Extension Enhanced Zinc Lozenges' (which are currently sold out on Amazon).
One option that maybe makes intuitive sense is mixing liquid ionic zinc with water and using it like mouthwash when you start feeling ill? I'm not sure. Be warned, however, that zinc nasal sprays have been found to permanently remove people's sense of smell, and regular use of zinc in other forms may also damage your sense of taste or smell over time.
From Elizabeth van Nostrand [LW(p) · GW(p)]:
Take zinc at the first symptom. [...] The method of action is zinc ions attaching to your throat. So pills are useless. It has to be a lozenge. [...] Chris Masterjohn claims only zinc-gluconate and -acetate work. I don't know if this is true, but the only studies I found used gluconate and acetate, so it seems wise to prefer them. [...] The terrible taste and loss of sense of smell says it’s working, unless you already lost your sense of smell to COVID.
D. Start monitoring your oxygen more often at the smallest warning sign.
(Added Apr. 26: ... including if you’re asymptomatic but have exposed yourself to possible infection vectors in the last two weeks. If you develop a fever or experience significant chest tightness or difficulty breathing, definitely start monitoring your oxygen; but don’t wait that long if you can avoid it.)
From residents of the Event Horizon house:
Since COVID-19 is a disease with significant respiratory involvement, and that's the pathway by which it usually kills, you'll want to go to the hospital if you’re having trouble breathing, and your blood oxygen levels are consistently below ~90-94% (for people at sea level), while you are using the pulse ox as directed. (Brief dips should generally not worry you, due to normal fluctuations and the imperfection of the measurement.)
Eli Morningstar adds:
Advice to avoid freaking yourself out with a home pulse oximeter (avoid user error):
- Keep your hand below your heart when measuring
- Don't wear nail polish on the finger you're using
- Hold something warm first, ie don't have cold hands
I now think “respiratory involvement... is the pathway by which it kills” is wrong, or at least very incomplete. I’m moving toward thinking of COVID-19 as a vascular or clotting disease at least as much as a respiratory one. Asthma isn’t a major risk factor for COVID-19 death; age, obesity, diabetes, heart disease, and hypertension are.
From the Washington Post May 10:
In the initial days of the outbreak, most efforts focused on the lungs. SARS-CoV-2 infects both the upper and lower respiratory tracts, eventually working its way deep into the lungs, filling tiny air sacs with cells and fluid that choke off the flow of oxygen.
But many scientists have come to believe that much of the disease’s devastation comes from two intertwined causes. The first is the harm the virus wreaks on blood vessels, leading to clots that can range from microscopic to sizable. [...] The second is an exaggerated response from the body’s own immune system, a storm of killer “cytokines” that attack the body’s own cells along with the virus as it seeks to defend the body from an invader.
[...] “What this virus does is it starts as a viral infection and becomes a more global disturbance to the immune system and blood vessels — and what kills is exactly that,” Mehra said. “Our hypothesis is that covid-19 begins as a respiratory virus and kills as a cardiovascular virus.”
[...] ACE2 receptors, which help regulate blood pressure, are plentiful in the lungs, kidneys and intestines — organs hit hard by the pathogen in many patients. That also may be why high blood pressure has emerged as one of the most common preexisting conditions in people who become severely ill with covid-19.
Oncologist Tatiana Prowell describes (on May 5) a Swiss autopsy series on Twitter:
[...] pathologists who did autopsies on these 21 people who died of #COVID19 think lung damage & blood clots in the smallest blood vessels (capillaries) of the lungs were the major cause of death. They found clots even in [patients] on blood thinners, which should’ve prevented them.
And quoting CellBioGuy [LW · GW] (Apr. 13, Apr. 22):
ACE2 is expressed on endothelial cells lining blood vessels. If you get bad viremia the inner sheath of blood vessels, especially in heavily infected organs, probably just gets all messed up.
[...] The virus may be causing abnormal inflammation and a whole-body, but especially concentrated in the lungs, hyper-coagulable state that is triggering microscopic blood clots in the lungs that are one of the main contributors to morbidity and mortality and ineffectiveness of ventilation.
[...] This hyper-coagulable state might explain the reports of anomalously low oxygen measurements in people that would ordinarily indicate death or [unconsciousness]. They might have small clots in the finger the sensor is on triggering temporary sporadic low blood flow. It also could explain more of the fact that ventilators are less useful than they thought - some people going on them probably didn't actually need them.
[...] Additionally, there are two bits of immunology that explain parts of this virus's behavior and suggest ways of hurting it. First, the virus evolved in bats in which the interferon response is on an absolute hair trigger, and accordingly in human cells it almost completely escapes the interferon response. This allows it to replicate to absurd viral loads before the immune system notices it, explaining the extreme infectiousness shortly before symptoms develop. Then when the immune system notices it, it goes all out on a huge viral infection, triggering an inflammatory response that is all out of whack and can do a lot of damage. This means that it is vulnerable to inhaled interferon pretreatment (https://www.biorxiv.org/content/10.1101/2020.03.07.982264v1). On top of this, it may be that anything that reduces the replication of the virus in this period before the adaptive immune system mounts a robust response could reduce the probability of progression to severe disease. If antivirals work out or if chloroquine is effective (given the biochemistry I am very hopeful!), they will probably be most effective early via reducing the fraction of patients that progress to severe disease.
Second, there is evidence that the virus is able to enter and destroy (but not replicate within) T-cells using the same receptor it uses everywhere else, triggering immune suppression and altering the inflammatory profile (https://www.nature.com/articles/s41423-020-0424-9). It lacks HIV's obscene dirty tricks and isn't actually replicating within them, so this would be a temporary thing until recovery.
I want to emphasize that you may need to go to the hospital on very short notice. Serious COVID-19 cases appear to not-infrequently progress from 'little or no care needed' to 'serious care needed immediately' on very short timescales. E.g., from ProPublica:
I have patients in their early 40s and, yeah, I was kind of shocked. I’m seeing people who look relatively healthy with a minimal health history, and they are completely wiped out, like they’ve been hit by a truck. This is knocking out what should be perfectly fit, healthy people. Patients will be on minimal support, on a little bit of oxygen, and then all of a sudden, they go into complete respiratory arrest, shut down and can’t breathe at all.
The second week of symptom presentation seems like it may be particularly dangerous. Please monitor symptoms carefully, even if your symptoms were relatively mild in the first week. From the CDC:
Some reports suggest the potential for clinical deterioration during the second week of illness. In one report, among patients with confirmed COVID-19 and pneumonia, just over half of patients developed dyspnea [labored breathing] a median of 8 days after illness onset (range: 5–13 days). In another report, the mean time from illness onset to hospital admission with pneumonia was 9 days. Acute respiratory distress syndrome (ARDS) developed in 17–29% of hospitalized patients, and secondary infection developed in 10%. In one report, the median time from symptom onset to ARDS was 8 days.
Depending on how serious your symptoms are, and on how crowded nearby hospitals are at the time, you may want to go to the hospital even if your breathing is OK. If possible, talk to a doctor over the phone/video to get their recommendations. The above is meant to be advice about when you definitely should receive hospital-level care; but it's not necessarily smart to wait until the last moment.
All that said, for several reasons, it's often a bad idea to go to a hospital during a pandemic when it isn't absolutely necessary:
- You might not have COVID-19. Going to a hospital may then expose you to COVID-19, on top of your other illness. (Catching COVID-19 is much more dangerous for people who have another illness.)
- You might have COVID-19 and end up exposed to much greater viral load early in your disease progression, which is likely to seriously worsen your symptoms. Discussion of the importance of viral load here: https://www.facebook.com/robert.wiblin/posts/887350766835. But Nick Tarleton says: "[I] would naively imagine that once someone is solidly {infected + mounting an immune response}, more external viral load would be a pretty small factor."
Similar advice from Elizabeth van Nostrand: https://www.lesswrong.com/…/what-should-we-do-once-infected… [LW(p) · GW(p)]
Added Apr. 26: streawkceur writes [LW(p) · GW(p)], “According to this article, it seems clear by now that low oxygen is in fact dangerous even when you feel fine, so buying a pulse oximeter is useful. https://www.nytimes.com/2020/04/20/opinion/sunday/coronavirus-testing-pneumonia.html” Quoting the article:
[...] These patients did not report any sensation of breathing problems, even though their chest X-rays showed diffuse pneumonia and their oxygen was below normal. How could this be?
We are just beginning to recognize that Covid pneumonia initially causes a form of oxygen deprivation we call “silent hypoxia” — “silent” because of its insidious, hard-to-detect nature.
Pneumonia is an infection of the lungs in which the air sacs fill with fluid or pus. Normally, patients develop chest discomfort, pain with breathing and other breathing problems. But when Covid pneumonia first strikes, patients don’t feel short of breath, even as their oxygen levels fall. And by the time they do, they have alarmingly low oxygen levels and moderate-to-severe pneumonia (as seen on chest X-rays). Normal oxygen saturation for most persons at sea level is 94 to 100 percent; Covid pneumonia patients I saw had oxygen saturations as low as 50 percent.
To my amazement, most patients I saw said they had been sick for a week or so with fever, cough, upset stomach and fatigue, but they only became short of breath the day they came to the hospital. Their pneumonia had clearly been going on for days, but by the time they felt they had to go to the hospital, they were often already in critical condition. [...]
We are only just beginning to understand why this is so. The coronavirus attacks lung cells that make surfactant. This substance helps the air sacs in the lungs stay open between breaths and is critical to normal lung function. As the inflammation from Covid pneumonia starts, it causes the air sacs to collapse, and oxygen levels fall. Yet the lungs initially remain “compliant,” not yet stiff or heavy with fluid. This means patients can still expel carbon dioxide — and without a buildup of carbon dioxide, patients do not feel short of breath.
Patients compensate for the low oxygen in their blood by breathing faster and deeper — and this happens without their realizing it. This silent hypoxia, and the patient’s physiological response to it, causes even more inflammation and more air sacs to collapse, and the pneumonia worsens until oxygen levels plummet. In effect, patients are injuring their own lungs by breathing harder and harder. Twenty percent of Covid pneumonia patients then go on to a second and deadlier phase of lung injury. Fluid builds up and the lungs become stiff, carbon dioxide rises, and patients develop acute respiratory failure.
By the time patients have noticeable trouble breathing and present to the hospital with dangerously low oxygen levels, many will ultimately require a ventilator.
Silent hypoxia progressing rapidly to respiratory failure explains cases of Covid-19 patients dying suddenly after not feeling short of breath. [...]
There is a way we could identify more patients who have Covid pneumonia sooner and treat them more effectively — and it would not require waiting for a coronavirus test at a hospital or doctor’s office. It requires detecting silent hypoxia early through a common medical device that can be purchased without a prescription at most pharmacies: a pulse oximeter.
Relatedly, Paul Bohm notes, “54% of asymptomatic cases and 79% of COVID-19 symptomatic cases on the Diamond Princess had ground-glass abnormalities in their CT scans.”
This suggests that even if you seem completely asymptomatic (or have very mild symptoms), you should periodically use a home pulse oximeter if there’s a nontrivial risk you recently caught the virus. Additionally, unusually fast and deep breathing is a thing to watch out for, even in otherwise asymptomatic or mildly symptomatic people.
Added May 12: Stat reports Apr. 21:
[...] The new analysis [... suggests that] unusual features of the disease can make mechanical ventilation harmful to the lungs.
[...] “In our personal experience, hypoxemia … is often remarkably well tolerated by Covid-19 patients,” the researchers wrote, in particular by those under 60. “The trigger for intubation should, within certain limits, probably not be based on hypoxemia but more on respiratory distress and fatigue.”
Absent clear distress, they say, blood oxygen levels of coronavirus patients don’t need to be raised above 88%, a much lower goal than in other causes of pneumonia.
[...] Covid-19 affects the lungs differently than other causes of severe pneumonia or acute respiratory distress syndrome, the researchers point out, confirming what physicians around the world are starting to realize.
For one thing, the thick mucus-like coating on the lungs developed by many Covid-19 patients impedes the lungs from taking up the delivered oxygen.
For another, unlike in other pneumonias the areas of lung damage in Covid-19 can sit right next to healthy tissue, which is elastic. Forcing oxygen-enriched air (in some cases, 100% oxygen) into elastic tissue at high pressure and in large volumes can cause leaks, pulmonary edema (swelling), and inflammation, among other damage, contributing to “ventilator-induced injury and increased mortality” in Covid-19, the researchers wrote.
[...] There is a growing recognition that some Covid-19 patients, even those with severe disease as shown by the extent of lung infection, can be safely treated with simple nose prongs or face masks that deliver oxygen.The latter include CPAP (continuous positive airway pressure) masks used for sleep apnea, or BiPAP (bi-phasic positive airway pressure) masks used for congestive heart failure and other serious conditions. CPAP can also be delivered via hoods or helmets, reducing the risk that patients will expel large quantities of virus into the air and endanger health care workers.
[...] “We use CPAP a lot, and it works well, especially in combination with having patients lie prone,” Schultz said.
E. Take care of yourself.
From Duncan Sabien:
Symptom mitigation seems extremely likely to be extremely important, especially those related to the respiratory tract. Early prophylactic measures (zinc lozenges, things to soothe throat and prevent coughing), Tylenol (NOT NSAIDs). Lots of fluids with lots of electrolytes (Pedialyte if you can get it, Gatorade if you can't). Temperature regulation.
The biggest thing I'm worried about is permanent post-recovery respiratory problems, and it seems to me that most of those are caused by symptomatic damage rather than by the direct actions of the virus itself.
I believe that most (though not all!) sources these days think fevers are good by default, and you shouldn't try to lower your fever unless it gets dangerously high. Regarding what counts as "dangerously high", Elizabeth van Nostrand says: "I was taught 103ºF, some people say 104ºF, that’s probably the range."
From Event Horizon:
[If] your fever is dangerously high (103°F / 39.4°C or higher) [then you may need to] lower your body temperature manually. Ways to treat fever safely: acetaminophen/paracetamol (do not exceed recommended dose; do NOT use NSAIDs); Drinking more fluids; Take a bath (but NOT an ice bath or a cold bath); Place cool washcloths (NOT icepacks) under the armpits and in the groin area.
[...] Have something to help you rehydrate if you are sick and losing fluids. Gatorade Powder (https://smile.amazon.com/Gatorade-Thirst-Quencher-Powder…/…/) is a good option because you can buy it in bulk, unlike Pedialyte. Also, liking the things that you drink might ensure you keep doing it. Here (https://med.virginia.edu/…/Homemade-Oral-Rehydration-Soluti…) is a guide to creating oral rehydration solution (used to treat fatal diarrhea, also useful for vomiting and general dehydration) from a variety of bases and household ingredients."
(As noted here [LW(p) · GW(p)], the warnings against NSAIDs above are plausibly overstated.)
From Divia Eden: "I would get mucinex and a humidifier if possible." See the nurse recommendations here. Elizabeth van Nostrand says: "Take pseudoephedrine if you have unpleasant sinus pressure." (Note: not phenylephrine / Sudafed PE, which is apparently useless.)
Stay warm, take it easy, and get lots of rest.
F. Lie on your front.
(Added Mar. 31.)
Leora Horwitz, a New York doctor working in a non-ICU COVID-19 unit, says:
Proning [i.e., having patients lay on their stomach] is now standard in our ICU and I tried hard to get my sicker patients to do it too to head off intubation. [...]
In response to the question "Is proning something we can do at home to help with milder symptoms? My brother is short of breath but not at ICU level, should he try this?", Horwitz says:
Yes, can’t hurt, likely help
Koulouras et al. and Pan et al. also suggest that ARDS patients may see better outcomes from lying on their chest.
If you’re showing COVID-19 symptoms, you may want to start lying on your chest instead of your back or side (using pillows for support as needed), at least if you can sleep and rest well in that position.
Relatedly, postural drainage strikes me as something that might help ameliorate symptoms in people with relatively serious symptoms, and can be done at home.
G. Monitor for clotting problems.
(Added Apr. 27.)
Evan Hubinger says:
There have been a lot of reports recently of young people (30s and 40s) developing blood clotting complications due to covid19 infection, resulting in strokes, heart attacks, and pulmonary embolisms. Apparently this can happen even for people who are otherwise asymptomatic. Actionable items:
1. Monitor yourself for stroke, heart attack, etc. symptoms and get to the hospital ASAP if you have any—one of the major reasons these cases are so bad right now is that young, otherwise asymptomatic people aren't used to looking for stroke symptoms and aren't rushing to the hospital.
2. If you think there's a high risk you might have covid19, consider taking a blood thinner such as aspirin.
From Live Science on Apr. 23:
[...] The link between COVID-19 and clots has led some hospitals to put all COVID-19 patients on low doses of blood thinners to prevent clots, according to CNN.
[...] A recent study from the Netherlands, published in the journal Thrombosis Research, found that out of 184 COVID-19 patients in the ICU, more than 30% experienced some type of clotting issue. [...]
From CNN on Apr. 23:
[...] The new coronavirus appears to be causing sudden strokes in adults in their 30s and 40s who are not otherwise terribly ill, doctors reported Wednesday.
[...] Dr. Thomas Oxley, a neurosurgeon at Mount Sinai Health System in New York, and colleagues gave details of five people they treated. All were under the age of 50, and all had either mild symptoms of Covid-19 infection or no symptoms at all.
"The virus seems to be causing increased clotting in the large arteries, leading to severe stroke," Oxley told CNN.
"Our report shows a seven-fold increase in incidence of sudden stroke in young patients during the past two weeks. Most of these patients have no past medical history and were at home with either mild symptoms (or in two cases, no symptoms) of Covid," he added.
[...] "For comparison, our service, over the previous 12 months, has treated on average 0.73 patients every 2 weeks under the age of 50 years with large vessel stroke," the team wrote in a letter to be published in the New England Journal of Medicine. [...]
From the Washington Post on Apr. 25:
[... At Mount Sinai there have been] several recent [large-vessel] stroke patients in their 30s to 40s who were all infected with the coronavirus. The median age for that type of severe stroke is 74.
[...] Many researchers suspect strokes in covid-19 patients may be a direct consequence of blood problems that are producing clots all over some people’s bodies.
[...] At Mount Sinai, the largest medical system in New York City, physician-researcher J Mocco said the number of patients coming in with large blood blockages in their brains doubled during the three weeks of the covid-19 surge to more than 32, even as the number of other emergencies fell. More than half of [them] were covid-19 positive.
[...] The covid-19 patients treated for stroke at Mount Sinai were younger and mostly without risk factors.
On average, the covid-19 stroke patients were 15 years younger than stroke patients without the virus. [...]
Symptoms to watch out for:
- For stroke, the FAST mnemonic summarizes the main symptoms: if one side of your face starts drooping or goes numb, one arm suddenly goes weak or numb, or your speech becomes slurred or garbled, it's time to call 911. Other symptoms can include: sudden leg weakness or numbness, especially on one side of the body; sudden confusion, trouble understanding speech; sudden trouble seeing in one or both eyes; sudden trouble walking, dizziness, loss of balance or coordination; sudden severe headache with no known cause.
- For heart attack in cis women, the Heart Foundation lists these signs: "(1) As with men, women’s most common heart attack symptom is chest pain or an uncomfortable pressure, squeezing, fullness or pain in the center of your chest. It lasts more than a few minutes, or goes away and comes back. (2) Pain or discomfort in one or both arms, the back, neck, jaw or stomach. (3) Shortness of breath with or without chest discomfort. (4) Other common symptoms in women include breaking out in a cold sweat, nausea/vomiting, or feeling lightheaded, palpitations; sleep disturbances and unexplained fatigue."
For heart attack in cis men: "(1) Chest discomfort. Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain. (2) It used to be thought that only chest pain was a sign of heart attack, but it’s possible to have discomfort that doesn’t register as painful. Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach. (3) Shortness of breath with or without chest discomfort. (4) Other signs may include breaking out in a cold sweat, nausea or feeling lightheaded."
I don’t know of research on heart attack signs in people undergoing transgender hormone therapy; data may be scarce because this is a relatively young population.
The Heart Foundation adds: "Don’t wait to get help if you experience any of these heart attack warning signs. Although some heart attacks are sudden and intense, most start slowly, with mild pain or discomfort." - For pulmonary embolism, Cedars Sinai says, "The most common symptoms include: sudden shortness of breath (most common); chest pain (usually worse with breathing); a feeling of anxiety; a feeling of dizziness, lightheadedness, or fainting; irregular heartbeat; palpitations (heart racing); coughing or coughing up blood; sweating; low blood pressure. You may also have symptoms of deep vein thrombosis (DVT), such as: pain in the affected leg (may happen only when standing or walking); swelling in the leg; soreness, redness, or warmth in the leg(s); redness and/or discolored skin."
Added May 3: I previously echoed Evan’s recommendation of taking aspirin prophylactically. Based on a comment [LW(p) · GW(p)] from John Maxwell, I’m no longer recommending that:
I just finished a video appointment with a cardiologist where we discussed the clotting thing. Even though he seemed to think I had COVID, and I recently had an abnormal EKG and some mild chest tightness, he thought it was better to avoid blood thinners. Apparently he has been receiving Cochrane reports on COVID before they are publicly available. He said that the increased clotting is usually in patients w/ some kinda predisposition and tends to be worse with more severe symptoms. Even for low-dose aspirin, he thinks the risk of bleeding is larger than the potential benefits. "I've seen all these complications from blood thinners." (I'm 28 FYI.)
Note that despite previous speculation [LW · GW] on LW regarding prophylactic use of low-dose aspirin for longevity, a large clinical trial found it wasn't useful in older folks (age 65+). Note this bit:
"Significant bleeding—a known risk of regular aspirin use—was also measured. The investigators noted that aspirin was associated with a significantly increased risk of bleeding, primarily in the gastrointestinal tract and brain. Clinically significant bleeding—hemorrhagic stroke, bleeding in the brain, gastrointestinal hemorrhages or hemorrhages at other sites that required transfusion or hospitalization—occurred in 361 people (3.8 percent) on aspirin and in 265 (2.7 percent) taking the placebo."
At the very least, I suggest you change your recommendation from "aspirin" to "low-dose aspirin". Overall, I'm more inclined to trust secondhand accounts of Cochrane preprints than collections of anecdotes in the media.
Added Jun. 2: Jim Babcock said on Apr. 28,
My first-pass literature review turned up some claimed mechanisms by which platelets and clotting may serve an immune purpose. I don't know if that's what happening here, but there's a possibility that this works like fever reduction: helpful in extreme cases, bad in minor cases and early in the progression.
Low-dose heparin seems to be common hospital protocol now, so data should be forthcoming for that scenario. I don't know what recommendation to give to minor cases self-treating at home, though.
H. Consider taking more extreme measures if you're experiencing serious COVID-19 symptoms, or if you have the resources to take bonus precautions.
Moderate-to-severe cases might benefit from a home oxygen concentrator. Sarah Constantin discusses oxygen supplementation topics: Oxygen Supplementation 101 + Non-Invasive Ventilation Outcomes + How Effective is Non-Invasive Ventilation in COVID-19? (Mar. 19-22), CPAP for COVID-19 (Apr. 5); and Avoiding Intubation in COVID-19 Silent Hypoxemia (May 4). Connor Flexman adds some thoughts [LW(p) · GW(p)] (Mar. 17).
Speculative and risky, but: If you can, you may want to acquire chloroquine or hydroxychloroquine. Be sure to read the entire write-up at https://docs.google.com/…/160RKDODAa-MTORfAqbuc25V8WDkLjqj…/.
Specifically for people in high-risk groups, Anjali Gopal suggests: "can you sign [...] up for clinical trials for antiviral drugs in nearby research hospitals? Some research coming out around this has started to show efficacy of remdesivir, chloroquine, and hydroxychloroquine wrt covid, though of course, this is still all very speculative and needs to be verified by RCTs. (A lot of these trials are often only open for people in high risk groups[.)]" Elizabeth van Nostrand: "One place I have found to find RCTs is https://clinicaltrials.gov/ . Normally I would verify the details of how to join but I assume they are busy right now."
Added Apr. 27: If you’re worried about blood clot risks from COVID-19 (discussed in 3G), you may want to use home coagulation tests.
11 comments
Comments sorted by top scores.
comment by Rob Bensinger (RobbBB) · 2020-05-12T17:55:33.989Z · LW(p) · GW(p)
Updates, May 8-12:
___
2A. Avoid people.
I recommend reading immunologist Erin Bromage’s The Risks — Know Them — Avoid Them in full. Some key claims:
- To get infected, you plausibly need to be exposed to ~1000+ SARS-CoV2 viral particles (source) — either all at once, or over minutes or hours. The more viral particles are present, and the more time you spend exposed to them, the greater your infection risk.
- “[T]he droplets in a single cough or sneeze may contain as many as 200,000,000 virus particles.” A single cough releases ~3000 (mostly large) droplets traveling at 50 mph (source). A single sneeze releases ~30,000 (mostly small) droplets traveling up to 200 mph (source). Smaller particles hang in the air longer. If someone sneezes or coughs, "even if that cough or sneeze was not directed at you, some infected droplets — the smallest of small — can hang in the air for a few minutes, filling every corner of a modest sized room with infectious viral particles. All you have to do is enter that room within a few minutes of the cough/sneeze and take a few breaths and you have potentially received enough virus to establish an infection."
- In contrast, "a single breath releases 50 - 5000 droplets", most of which fall to the ground quickly; nose-breathing releases even fewer droplets (source). "We don't have a number for SARS-CoV2 yet, but we [...] know that a person infected with influenza releases about 3-20 virus RNA copies per minute of breathing" (source). This suggests that if your only exposure to an infected person is via them silently breathing on the other side of a room, it will probably take an hour or longer for them to infect you.
- Speaking releases “~200 copies of virus per minute. Again, [pessimistically] assuming every virus is inhaled, it would take ~5 minutes of speaking face-to-face to receive the required dose” (source).
- A toilet flush aerosolizes droplets (which might contain viable virus), so “treat public bathrooms with extra caution (surface and air)” (source).
- “[P]lease don't forget surfaces. Those infected respiratory droplets land somewhere. Wash your hands often and stop touching your face!”
- “We know that at least 44% of all infections — and the majority of community-acquired transmissions — occur from people without any symptoms (asymptomatic or pre-symptomatic people) (source). You can be shedding the virus into the environment for up to 5 days before symptoms begin. [...] Viral load generally builds up to the point where the person becomes symptomatic. So just prior to symptoms showing, you are releasing the most virus into the environment.”
- “The main sources for infection are home, workplace, public transport, social gatherings, and restaurants. This accounts for 90% of all transmission events. In contrast, outbreaks spread from shopping appear to be responsible for a small percentage of traced infections.” (source). “The biggest outbreaks are in [nursing homes,] prisons, religious ceremonies, and workplaces, such [as] meat packing facilities and call centers.” Outbreaks seem to happen disproportionately often in colder indoor environments, and at larger and more social gatherings like weddings, funerals, birthdays, and networking events.
- “Indoor spaces, with limited air exchange or recycled air and lots of people, are concerning from a transmission standpoint. We know that 60 people in a volleyball court-sized room (choir) results in massive infections. Same situation with the restaurant and the call center. Social distancing guidelines don't hold in indoor spaces where you spend a lot of time, as people on the opposite side of the room were infected.
“The principle is viral exposure over an extended period of time. In all these cases, people were exposed to the virus in the air for a prolonged period (hours). Even if they were 50 feet away (choir or call center), even a low dose of the virus in the air reaching them, over a sustained period, was enough to cause infection and in some cases, death.
“Social distancing rules are really to protect you with brief exposures or outdoor exposures. In these situations there is not enough time to achieve the infectious viral load when you are standing 6 feet apart or where wind and the infinite outdoor space for viral dilution reduces viral load. The effects of sunlight, heat, and humidity on viral survival, all serve to minimize the risk to everyone when outside.” - You shouldn’t worry especially about “[brief visits to] grocery stores, bike rides, inconsiderate runners who are not wearing masks”. “[F]or a person shopping: the low density, high air volume of the store, along with the restricted time you spend in the store, means that the opportunity to receive an infectious dose is low.” If you have to work in a grocery store, or spend lots of time in an office or classroom — especially one with more people sharing the same space and/or air, or one that requires "face-to-face talking or even worse, yelling" — you should be much more worried.
Bromage says grocery stores aren't "places of concern", but I gather he means they’re relatively safe if you’re keeping a good distance from everyone, going when the store is pretty empty, etc. If a single cough from someone a few feet away who isn’t facing in my direction can give me COVID-19 within a few seconds, that still seems “concerning” to me!
Additionally, Jim Babcock comments on “infections while shopping appear to be responsible for 3-5% of infections”:
The source for this covers Ningbo from January 21 to March 6. My main worry, when looking at this number, is that Ningbo's mitigations may have been more effective for stores than they were for other places, in ways that don't generalize to the US. For example, I'm pretty sure they would have been screening people for fever on entry, and enforcing mask usage. I haven't been hearing of fever-screens in Berkeley (though I haven't really been out of the house), and while we do now have a mask ordinance, it's mostly cloth masks (which are less effective) and compliance doesn't seem to be very good.
And:
The specific number for the ~1000 virus-particle claim is cited to a pretty sketchy source; it leads to a couple epidemiologists speculating with no data, and what they actually say is:
> "The actual minimum number varies between different viruses and we don’t yet know what that ‘minimum infectious dose’ is for COVID-19, but we might presume it’s around a hundred virus particles."
and
> "For many bacterial and viral pathogens we have a general idea of the minimal infective dose but because SARS-CoV-2 is a new pathogen we lack data. For SARS, the infective dose in mouse models was only a few hundred viral particles. It thus seems likely that we need to breathe in something like a few hundred or thousands of SARS-CoV-2 particles to develop symptoms. This would be a relatively low infective dose and could explain why the virus is spreading relatively efficiently."
So there's uncertainty of about an order of magnitude, here. On the other hand, the broader claim--that exposure size matters--is almost certainly true, and the implications of the specific number 1000 are mostly screened off by more-specific observations of which places people are getting it.
Bromage has softened the grocery store claim to “In contrast, outbreaks spread from shopping appear to be responsible for a small percentage of traced infections.”, and now cites an additional two studies for the 1000-particle claim: 1, 2.
___
2I. Consume 2,000-6,000 IU of Vitamin D daily, in the morning.
From Jim Babcock:
Wikipedia summarizes https://pubmed.ncbi.nlm.nih.gov/21419266/ as "vitamin D functions to activate the innate and dampen the adaptive immune systems". Assuming that's true (I haven't verified it, and vitamin D is a subject known for attracting sketchy claims), then deficiency would lower the minimum infectious dose. On a population scale, this would be a better explanation for the infections-latitude correlation than temperature is, and would suggest that mass-distributing vitamin D supplements would be a good R-lowering strategy.
___
3D. Start monitoring your oxygen more often at the smallest warning sign.
[Removed or de-emphasized information suggesting hospitals will be overrun, which never really happened in the US and probably never will. This includes cutting the long Connor Flexman comment [LW(p) · GW(p)], though I still link it in the context of home oxygen concentrators.]
I now think “respiratory involvement... is the pathway by which it kills” is wrong, or at least very incomplete. I’m updating toward thinking of COVID-19 as a vascular or clotting disease at least as much as a respiratory one. Asthma isn’t a major risk factor for COVID-19 death; age, obesity, diabetes, heart disease, and hypertension are.
From the Washington Post May 10:
In the initial days of the outbreak, most efforts focused on the lungs. SARS-CoV-2 infects both the upper and lower respiratory tracts, eventually working its way deep into the lungs, filling tiny air sacs with cells and fluid that choke off the flow of oxygen.
But many scientists have come to believe that much of the disease’s devastation comes from two intertwined causes. The first is the harm the virus wreaks on blood vessels, leading to clots that can range from microscopic to sizable. [...] The second is an exaggerated response from the body’s own immune system, a storm of killer “cytokines” that attack the body’s own cells along with the virus as it seeks to defend the body from an invader.
[...] “What this virus does is it starts as a viral infection and becomes a more global disturbance to the immune system and blood vessels — and what kills is exactly that,” Mehra said. “Our hypothesis is that covid-19 begins as a respiratory virus and kills as a cardiovascular virus.”
[...] ACE2 receptors, which help regulate blood pressure, are plentiful in the lungs, kidneys and intestines — organs hit hard by the pathogen in many patients. That also may be why high blood pressure has emerged as one of the most common preexisting conditions in people who become severely ill with covid-19.
Oncologist Tatiana Prowell describes (on May 5) a Swiss autopsy series on Twitter:
[...] pathologists who did autopsies on these 21 people who died of #COVID19 think lung damage & blood clots in the smallest blood vessels (capillaries) of the lungs were the major cause of death. They found clots even in [patients] on blood thinners, which should’ve prevented them.
And quoting CellBioGuy [LW · GW] (Apr. 13, Apr. 22):
ACE2 is expressed on endothelial cells lining blood vessels. If you get bad viremia the inner sheath of blood vessels, especially in heavily infected organs, probably just gets all messed up.
[...] The virus may be causing abnormal inflammation and a whole-body, but especially concentrated in the lungs, hyper-coagulable state that is triggering microscopic blood clots in the lungs that are one of the main contributors to morbidity and mortality and ineffectiveness of ventilation.
[...] This hyper-coagulable state might explain the reports of anomalously low oxygen measurements in people that would ordinarily indicate death or [unconsciousness]. They might have small clots in the finger the sensor is on triggering temporary sporadic low blood flow. It also could explain more of the fact that ventilators are less useful than they thought - some people going on them probably didn't actually need them.
[...] Additionally, there are two bits of immunology that explain parts of this virus's behavior and suggest ways of hurting it. First, the virus evolved in bats in which the interferon response is on an absolute hair trigger, and accordingly in human cells it almost completely escapes the interferon response. This allows it to replicate to absurd viral loads before the immune system notices it, explaining the extreme infectiousness shortly before symptoms develop. Then when the immune system notices it, it goes all out on a huge viral infection, triggering an inflammatory response that is all out of whack and can do a lot of damage. This means that it is vulnerable to inhaled interferon pretreatment (https://www.biorxiv.org/content/10.1101/2020.03.07.982264v1). On top of this, it may be that anything that reduces the replication of the virus in this period before the adaptive immune system mounts a robust response could reduce the probability of progression to severe disease. If antivirals work out or if chloroquine is effective (given the biochemistry I am very hopeful!), they will probably be most effective early via reducing the fraction of patients that progress to severe disease.
Second, there is evidence that the virus is able to enter and destroy (but not replicate within) T-cells using the same receptor it uses everywhere else, triggering immune suppression and altering the inflammatory profile (https://www.nature.com/articles/s41423-020-0424-9). It lacks HIV's obscene dirty tricks and isn't actually replicating within them, so this would be a temporary thing until recovery.
[...]
Replies from: RobbBB[...] The new analysis [... suggests that] unusual features of the disease can make mechanical ventilation harmful to the lungs.
[...] “In our personal experience, hypoxemia … is often remarkably well tolerated by Covid-19 patients,” the researchers wrote, in particular by those under 60. “The trigger for intubation should, within certain limits, probably not be based on hypoxemia but more on respiratory distress and fatigue.”
Absent clear distress, they say, blood oxygen levels of coronavirus patients don’t need to be raised above 88%, a much lower goal than in other causes of pneumonia.
[...] Covid-19 affects the lungs differently than other causes of severe pneumonia or acute respiratory distress syndrome, the researchers point out, confirming what physicians around the world are starting to realize.
For one thing, the thick mucus-like coating on the lungs developed by many Covid-19 patients impedes the lungs from taking up the delivered oxygen.
For another, unlike in other pneumonias the areas of lung damage in Covid-19 can sit right next to healthy tissue, which is elastic. Forcing oxygen-enriched air (in some cases, 100% oxygen) into elastic tissue at high pressure and in large volumes can cause leaks, pulmonary edema (swelling), and inflammation, among other damage, contributing to “ventilator-induced injury and increased mortality” in Covid-19, the researchers wrote.
[...] There is a growing recognition that some Covid-19 patients, even those with severe disease as shown by the extent of lung infection, can be safely treated with simple nose prongs or face masks that deliver oxygen.The latter include CPAP (continuous positive airway pressure) masks used for sleep apnea, or BiPAP (bi-phasic positive airway pressure) masks used for congestive heart failure and other serious conditions. CPAP can also be delivered via hoods or helmets, reducing the risk that patients will expel large quantities of virus into the air and endanger health care workers.
[...] “We use CPAP a lot, and it works well, especially in combination with having patients lie prone,” Schultz said.
↑ comment by Rob Bensinger (RobbBB) · 2020-06-04T00:22:24.973Z · LW(p) · GW(p)
Updates, June 2:
___
2A. Avoid people, especially indoors.
[Section renamed from "Avoid people."]
[Deleted the CDC quote that COVID-19 is mainly spread "between people who are in close contact with one another (within about 6 feet)", per Zvi's criticism of the meme.]
___
2B. If you do need to be around people, face away from them, minimize talking, etc.
[New section.]
Jonathan Kay writes on Apr. 23,
According to the binary model established in the 1930s, droplets typically are classified as either (1) large globules of the Flüggian variety—arcing through the air like a tennis ball until gravity brings them down to Earth; or (2) smaller particles, less than five to 10 micrometers in diameter (roughly a 10th the width of a human hair), which drift lazily through the air as fine aerosols.
[...] Despite the passage of four months since the first known human cases of COVID-19, our public-health officials remain committed to policies that reflect no clear understanding as to whether it is one-off ballistic droplet payloads or clouds of fine aerosols that pose the greatest risk—or even how these two modes compare to the possibility of indirect infection through contaminated surfaces (known as “fomites”).
Gaining such an understanding is absolutely critical to the task of tailoring emerging public-health measures and workplace policies, because the process of policy optimization depends entirely on which mechanism (if any) is dominant:
1. If large droplets are found to be a dominant mode of transmission, then the expanded use of masks and social distancing is critical, because the threat will be understood as emerging from the ballistic droplet flight connected to sneezing, coughing, and laboured breathing. We would also be urged to speak softly, avoid “coughing, blowing and sneezing,” or exhibiting any kind of agitated respiratory state in public, and angle their mouths downward when speaking.
2. If lingering clouds of tiny aerosol droplets are found to be a dominant mode of transmission, on the other hand, then the focus on sneeze ballistics and the precise geometric delineation of social distancing protocols become somewhat less important—since particles that remain indefinitely suspended in an airborne state can travel over large distances through the normal processes of natural convection and gas diffusion. In this case, we would need to prioritize the use of outdoor spaces (where aerosols are more quickly swept away) and improve the ventilation of indoor spaces.
3. If contaminated surfaces are found to be a dominant mode of transmission, then we would need to continue, and even expand, our current practice of fastidiously washing hands following contact with store-bought items and other outside surfaces; as well as wiping down delivered items with bleach solution or other disinfectants.
Zvi Mowshowitz comments [LW · GW]:
Identified Super Spreader Events are Primarily Large Droplet Transmission
The article makes a strong case that in identified super spreader events [SSEs] the primary mode of transmission is large droplets. And that large droplets are spread in close proximity, by people talking (basically everything) or singing (several choir/singing practices) frequently or loudly, or laughing (many parties) and crying (funerals), or otherwise exhaling rapidly (e.g. the curling match) and so on.
There is a highly noticeable absence of SSEs that would suggest other transmission mechanisms. Subways and other public transit aren’t present, airplanes mostly aren’t present. Performances and showings of all kinds also aren’t present. Quiet work spaces aren’t present, loud ones (where you have to yell in people’s faces) do show up. University SSEs are not linked to classes (where essentially only the professor talks, mostly) but rather to socializing. [...]
Zvi argues that surfaces and small aerosolized droplets are unlikely to be major infection vectors for COVID-19. He discusses methods for avoiding large droplet transmission:
Large Droplets: Six Foot Rule is Understandable, But Also Obvious Nonsense
For large droplets, there is essentially zero messaging about angling downwards or avoiding physical actions that would expel more droplets, or avoiding being in the direct path of other people’s potential droplets.
Instead, we have been told to keep a distance of six feet from other people. We’ve told them that six feet apart is safe, and five feet apart is unsafe. Because the virus can only travel six feet.
That’s obvious nonsense. It is very clear that droplets can go much farther than six feet. Even more than that, the concept of a boolean risk function [i.e., one that sharply divides everything into either "risky" or "risk-free", with no shades of grey] is insane. People expel virus at different velocities, from different heights, under different wind conditions and so on. The physics of each situation will differ. The closer you are, the more risk.
Intuitively it makes sense to think about something like an inverse square law until proven otherwise, so six feet away is about 3% of the risk of one foot away. That’s definitely not right, but it’s the guess I feel comfortable operating with.
Alas, that’s not the message. The message is 72 inches safe, 71 inches unsafe.
Unlike the previous case of obvious nonsense, there is a reasonable justification for this one. I am sympathetic. You get about five words. “Always stay six feet apart” is a pretty good five words. There might not be a better one. Six feet is a distance that you can plausibly mandate and still allow conversations and lines that are moderately sane, so it’s a reasonable compromise.
It’s a lie. It’s not real. As a pragmatic choice, it’s not bad.
The problem is it is being treated as literally real.
Joe Biden and Bernie Sanders met on a debate stage. The diagram plans had them exactly six feet apart.
In an article, someone invites the author, a reporter, to their house to chat. Says he’s prepared two chairs, six feet apart. “I measured them myself,” he says. [...]
And so on. People really are trying to make the distance exactly six feet as often as possible.
[...] This is society sacrificing bandwidth to get a message across. Again, I get it. The problem is we are also sacrificing any ability to convey nuance. We are incapable, after making this sacrifice, of telling people there is a physical world they might want to think about how to optimize. There is only a rule from on high, The Rule of Six Feet.
Thus, we may never be able to get people to talk softly into the ground rather than directly looking at each other and loudly and forcefully to ‘make up for’ the exact six foot distance, which happens to be the worst possible orientation that isn’t closer than six feet.
In theory, we can go beyond this. You get infected because droplets from an infected person travel out of their face and touch your face.
Thus, a line is remarkably safe if everyone faces the same way, modulo any strong winds. The person behind you has no vector to get to your face. And we can extend that. We can have one sidewalk where people walk north, and another on the other side of the street where people walk south. If you see someone approaching from the other direction, turn around and walk backwards while they ensure the two of you don’t collide. If necessary, stand in place for that reason. Either way, it should help – if this is the mechanism we are worried about.
[...] Yes, it’s annoying to not face other people, but you absolutely can have a conversation while facing away from each other. It’s a small price to pay.
In similar fashion, it seems a small price to pay to shut the hell up whenever possible, while out in public. Talking at all, when around those outside your household, can be considered harmful and kept to a bare minimum outright (and also it should be done while facing no one).
Zvi emphasizes that there’s much more benefit to slightly reducing the risk from the largest infection sources (including large droplets as a category), than from hugely reducing the risk from fairly unlikely infection sources:
Focus Only On What Matters
[...] Within those big risks, small changes matter. They matter more than avoiding small risks entirely.
A single social event, like a funeral, birthday party or wedding, might well by default give any given person a 30%+ rate to infect any given other person at that event if the event is small, and a reasonably big one even if large. You only need one. Keeping slightly more distance, speaking slightly less loudly, and so on, at one such event, is a big risk reduction. [...]
Whereas a ‘close contact’ that doesn’t involve talking or close interaction probably gives more like (spitballing a guess, but based on various things) an 0.03% rate of infection if the other person is positive, and likely with a lower resulting viral load. Certainly those contacts add up, but not that fast. Thus, a subway car full of “close contact” might give you 10 of them per day, most of whom are not, at any given time, infectious. If this model is correct.
In another post, Zvi writes [LW · GW]:
Risks Follow Power Laws
[...] Slight reductions in the frequency and severity of your very risky actions is much more important than reducing the frequency of nominally risky actions.
The few times you end up talking directly with someone in the course of business, the one social gathering you attend, the one overly crowded store you had to walk through, will dominate your risk profile. Be paranoid about that, and think how to make it less risky, or ideally avoid it. Don’t sweat the small stuff.
And think about the physical world and what’s actually happening around you!
And:
My best guess is there is something like 5-10 times as much risk indoors versus the same activity outdoors. [...]
The combination of quick and outdoors and not-in-your-face probably effectively adds up to safe, especially if you add in masks. During the peak epidemic in New York things were so intense that it would have been reasonable to worry about miasma. Now, I would do my best to keep my distance and avoid talking at each other, but mostly not worry about incidental interactions.
I do expect there to be a spike in cases as the result of protests and civil unrest.. To not see one would be surprising, and would update me in favor of outdoor activities being almost entirely harmless.
___
2C. If you do need to be around people, wear something over your mouth and nose.
[Deleted the advice for individuals not to buy medical-grade masks because it doesn't currently seem like good advice (and I'm not particularly convinced it was ever good advice).]
Zvi Mowshowitz writes [LW · GW], “[E]ven cloth masks on both ends of an interaction are almost certainly good for a 25% reduction in risk and probably 50%-75%.”
___
2D. Don’t put coronavirus in your face.
Zvi Mowshowitz argues [LW · GW]:
It’s been months. We don’t have concrete examples of infection via surfaces. At all. It increasingly seems like while such a route is possible, and must occasionally happen, getting enough virus to cause an infection, in a live state, via this route, is very hard. When you wash your hands and don’t touch your face, it’s even harder than that.
Meanwhile, those who refuse to touch surfaces like a pizza delivery box end up in more crowded locations like grocery stores, resulting in orders of magnitude more overall risk.
[...] Until I get very unexpected evidence, surfaces are mostly not a thing anymore. If lots of people touch stuff and then you touch it, sure, wash your hands after and be extra careful to not touch your face in the interim. Otherwise, stop worrying about it.
[... Food] is at most minimally risky, even if it doesn’t get heated enough to reliably and fully kill the virus. You don’t have to ruin all your food. People are often avoiding foods that seem risky. Once again, it makes sense that it could be risky, but in practice it’s been months and it does not seem to work that way. The precautions people are taking will incidentally be more than good enough to guard against contamination of food at sufficient levels to be worth worrying about. I mean, sure, don’t eat at a buffet, but it’s not like any of them are going to be open, and even then the (also mostly safe) surfaces are likely scarier than the food.
[...] Your risk is from the waiter, or from the other diners, being in that room with you for a while. Thus, takeout, delivery and/or eating outdoors.
I agree with Zvi that it seems increasingly likely that surface transmission is rare, though he seems to be wrong that there are no examples (see comments [LW · GW]), and I haven’t seen a clear argument for whether the number of COVID-19 cases caused by surface transmission is closer to 1/10 of all cases versus, say, 1/10,000. Given my own circumstances, I’m likely to do things like “order delivery pizza” more often in the weeks to come, but I’ll also likely make use of Yao Lu’s tips while infections are still commonplace in my part of the US:
I’m a chemo nurse, this is what I tell my high-risk patients:
I personally don’t trust takeout that much because I think a lot of restaurant workers don’t have sick leave, so it’s more likely your food was prepared by someone symptomatic. But you can cut the risk to near zero by doing this:
1. Wash your hands well
2. Put your own bowl on your kitchen counter
3. Pick up the restaurant container, and pour the food into your own bowl
4. Throw away the restaurant container
5. Wash your hands well
6. Thoroughly heat up the food. (at least 70C for a minute, or whatever the best current guideline says)
If you do this, in this order, you are extremely safe even if someone coughed viruses all over the food and the container. Heat would kill the virus, and handwashing would prevent indirect transmission from the bag/container.
___
2G. Disinfect surfaces.
See also Zvi Mowshowitz’s recommendations to worry less about surfaces [LW · GW], quoted above.
___
2H. Maybe stop taking ibuprofen/advil?
[Deleted this section because the post is getting long and this seems messy and uncertain. I'll reproduce the Apr. 26 version of the section in a reply to this comment for when I want to link directly to it.]
___
2J. Run an air filter.
[Provisionally deleted "Also, quit smoking." because I haven't been keeping up with the debate about cigarettes or nicotine.]
___
3A. Prepare in advance.
Plan in advance what hospital you’ll go to if necessary, and be ready to call a doctor if you have troubling symptoms. Zvi Mowshowitz writes [LW · GW]:
Medical care matters [for fatality rates]. Total breakdown of medical care in practice leads to several times the fatality rate under regular circumstances. High quality treatment at current knowledge levels can probably drive death rates down further, so the ratio between full success and complete breakdown can be rather large – something like an order-of-magnitude difference between 0.2% and 2%.
I don’t have a strong opinion at this point about particular medical treatments beyond the above.
___
3G. Monitor for clotting problems.
Jim Babcock said on Apr. 28,
My first-pass literature review turned up some claimed mechanisms by which platelets and clotting may serve an immune purpose. I don't know if that's what happening here, but there's a possibility that this works like fever reduction: helpful in extreme cases, bad in minor cases and early in the progression.
Low-dose heparin seems to be common hospital protocol now, so data should be forthcoming for that scenario. I don't know what recommendation to give to minor cases self-treating at home, though.
[I meant to add the above before, but forgot about it. This is part of why I withdrew the recommendation that people take aspirin at home whenever they start showing COVID-19 symptoms.]
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2020-06-04T00:23:58.277Z · LW(p) · GW(p)
[Copy of the Apr. 26 section "Maybe stop taking ibuprofen/advil?", deleted from the main text Jun. 2. A still earlier version just said that some sources were warning about NSAIDs and to therefore avoid them out of an abundance of caution.]
Fang et al. write in The Lancet:
Human pathogenic coronaviruses (severe acute respiratory syndrome coronavirus [SARS-CoV] and SARSCoV-2) bind to their target cells through angiotensin-converting enzyme 2 (ACE2), which is expressed by epithelial cells of the lung, intestine, kidney, and blood vessels.[4] The expression of ACE2 is substantially increased in patients with type 1 or type 2 diabetes, who are treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs).[4] Hypertension is also treated with ACE inhibitors and ARBs, which results in an upregulation of ACE2.[5] ACE2 can also be increased by thiazolidinediones and ibuprofen. These data suggest that ACE2 expression is increased in diabetes and treatment with ACE inhibitors and ARBs increases ACE2 expression. Consequently, the increased expression of ACE2 would facilitate infection with COVID-19. We therefore hypothesise that diabetes and hypertension treatment with ACE2-stimulating drugs increases the risk of developing severe and fatal COVID-19.
Qiao et al. conclude that ibuprofen enhances ACE2 in diabetic rats. Qiao et al. is the only study I've seen on 'ibuprofen increases ACE2', and this claim is uncited in Fang et al. The ibuprofen-ACE2-COVID link doesn't seem to be widely known / accepted / cared about, based on the discussion on Science Translational Medicine (which argues increased ACE2 might reduce COVID-19 severity; see also the comment section) and Snopes. I also don't know whether I should expect other NSAIDs to interact with ACE2 in the same way as ibuprofen.
On Mar. 14, Samira Jeimy wrote: "In Germany and France, ICU physicians have noticed that the common thread amongst young patients needing #COVIDー19 related ICU admission is that they had been using NSAIDS (Advil, Motrin, Aleve, Aspirin)." She cites the Lancet paper and Day:
Scientists and senior doctors have backed claims by France’s health minister that people showing symptoms of covid-19 should use paracetamol (acetaminophen) rather than ibuprofen, a drug they said might exacerbate the condition.
The minister, Oliver Veran, tweeted on Saturday 14 March that people with suspected covid-19 should avoid anti-inflammatory drugs. “Taking anti-inflammatory drugs (ibuprofen, cortisone . . .) could be an aggravating factor for the infection. If you have a fever, take paracetamol,” he said.
His comments seem to have stemmed in part from remarks attributed to an infectious diseases doctor in south west France. She was reported to have cited four cases of young patients with covid-19 and no underlying health problems who went on to develop serious symptoms after using non-steroidal anti-inflammatory drugs (NSAIDs) in the early stage of their symptoms. The hospital posted a comment saying that public discussion of individual cases was inappropriate.
But Jean-Louis Montastruc, a professor of medical and clinical pharmacology at the Central University Hospital in Toulouse, said that such deleterious effects from NSAIDS would not be a surprise given that since 2019, on the advice of the National Agency for the Safety of Medicines and Health Products, French health workers have been told not to treat fever or infections with ibuprofen.
Experts in the UK backed this sentiment. Paul Little, a professor of primary care research at the University of Southampton, said that there was good evidence “that prolonged illness or the complications of respiratory infections may be more common when NSAIDs are used—both respiratory or septic complications and cardiovascular complications.”
He added, “The finding in two randomised trials that advice to use ibuprofen results in more severe illness or complications helps confirm that the association seen in observational studies is indeed likely to be causal. Advice to use paracetamol is also less likely to result in complications.”
Ian Jones, a professor of virology at the University of Reading, said that ibuprofen’s anti-inflammatory properties could “dampen down” the immune system, which could slow the recovery process. He added that it was likely, based on similarities between the new virus (SARS-CoV-2) and SARS I, that covid-19 reduces a key enzyme that part regulates the water and salt concentration in the blood and could contribute to the pneumonia seen in extreme cases. “Ibuprofen aggravates this, while paracetamol does not,” he said.
Charlotte Warren-Gash, associate professor of epidemiology at the London School of Hygiene and Tropical Medicine, said: “For covid-19, research is needed into the effects of specific NSAIDs among people with different underlying health conditions. In the meantime, for treating symptoms such as fever and sore throat, it seems sensible to stick to paracetamol as first choice.” [...]
The Snopes page above cites Tom Wingfield saying:
In the UK, paracetamol would generally be preferred over non-steroidal anti-inflammatory drugs (“NSAIDS”) such as ibuprofen to relieve symptoms caused by infection such as fever. This is because, when taken according to the manufacturer’s and/or a health professional’s instructions in terms of timing and maximum dosage, it is less likely to cause side effects. Side effects associated with NSAIDs such as ibuprofen, especially if taken regularly for a prolonged period, are stomach irritation and stress on the kidneys, which can be more severe in people who already have stomach or kidney issues. It is not clear from the French Minister’s comments whether the advice given is generic ‘good practice’ guidance or specifically related to data emerging from cases of Covid-19 but this might become clear in due course.
So most sources seem to agree that acetaminophen is at least a bit better than ibuprofen for treating fever-causing illnesses in general; but there's confusion and disagreement about whether ibuprofen is unusually good or bad for COVID-19 in particular, and I don't get the sense using ibuprofen is widely seen as a terrible idea. Elizabeth van Nostrand writes, "France is recommending against NSAIDs and against ibuprofen in particular. I will be very surprised if that ends up being born out (and WHO agrees with me)".
Overall, the evidence is such that I'm avoiding ibuprofen right now, but I wouldn't recommend going to huge lengths to avoid ibuprofen.
See 3E below on whether and when it's a good idea to manually reduce fevers at all.
comment by Rob Bensinger (RobbBB) · 2020-06-04T19:07:46.705Z · LW(p) · GW(p)
Summary of changes, focusing on sections 2-3.
Mainly I want to make it easier to track when I retracted or modified something potentially decision-relevant. If something was deleted, I both note when that happened and (so people don't miss it) italicize all mentions below and put the original addition in angle brackets < >.
Feb. 27 — First deprecated post. Added: stocking up on supplies like 2+ weeks of food and water, surgical masks, and personal medications; printing out health records; washing hands more often, <for 20 seconds>, using medical protocol; avoiding touching eyes, nose, or mouth; not adjusting mask while wearing it; <never re-using masks>; going to the hospital only if really necessary; <signing up for cryonics> [but I do recommend this for many people]; <informing friends and family and making sure everyone can contact someone if they need help> [but I do recommend this]; minimizing exposure to crowded places and places like offices and grocery stores; using pedialyte powder, acetaminophen, <aspirin>, over-the-counter inhalers if you get sick; using finger pulse oximeter and going to hospital <if it gives a number below 92% at sea level>; using thermometer <as an earlier warning sign than the oximeter>; <worrying a lot about overwhelmed hospitals in the US>
- Deleted: washing hands for 20 seconds
Mar. 15 — Second deprecated post. Added: Americans who haven't self-quarantined doing so ASAP; trying to minimize initial viral load if exposed; being wary of transmission even from people who aren't showing symptoms; being wary of people coughing, sneezing, talking<, or breathing>; <being wary of people ≤ 6 feet away> [but I do recommend this]; being wary of indoor interactions; wearing home-made masks or scarves if you don't have surgical masks; <using sleeve instead of hand if your eye itches>; <carrying a handkerchief for touching your nose or mouth without using your hands>; minimizing exposure to surfaces lots of people touch; not using hand sanitizer as a substitute for hand-washing; stocking up on 1+ months of non-perishable food; probably sanitizing package (with sunlight, 70% isopropyl alcohol, or many household cleaners) if it's easy or if you're unusually at risk; copper-taping commonly touched surfaces; <not using NSAIDs [LW(p) · GW(p)]>; supplementing Vitamin D; eating well, sleeping well, exercising; using zinc if you may be getting sick; maybe aquiring chloroquine, though this is more speculative and risky and you should be sure to read https://docs.google.com/document/d/160RKDODAa-MTORfAqbuc25V8WDkLjqj4itMDyzBTpcc/edit; <noting average time from infection to symptom onset is 5 days>; short symptom overview; treating fever with fluids, baths (but not ice bath or cold bath), cool washcloths under armpits and in the groin area (not icepacks); going to hospital if finger pulse oximeter repeatedly gives numbers below ~90-94% at sea level
- Deleted: using aspirin if you get sick; going to hospital if finger pulse oximeter gives a number below 92% at sea level; signing up for cryonics [but I do recommend this for many people]; informing friends and family and making sure everyone can contact someone if they need help [but I do recommend this]
- Deleted but then re-added later: stocking up on water
Mar. 16 — Added: <not buying medical-grade masks since health care providers need as many as possible>
- Deleted but then re-added later: buying medical-grade masks
Mar. 20 — Added: using mucinex and humidifier if you get sick
Mar. 28 — Google Doc and partial LessWrong mirror [LW · GW]. Added: wearing face coverings in general; sanitizing face coverings as an alternative to throwing them away; disinfecting surfaces you touch a lot; running an air filter; <running an air purifier>; <quitting smoking> [but I do recommend this]; taking pseudoephedrine for sinus pressure; using oral thermometers (rather than skin-surface thermometers); maybe considering hydroxychloroquine as an alternative to chloroquine (but read https://docs.google.com/document/d/160RKDODAa-MTORfAqbuc25V8WDkLjqj4itMDyzBTpcc/edit first); maybe getting a home oxygen concentrator; testing thermometer and oximeter while healthy to get baseline numbers; figuring out who can help take care of you if you get sick; detailed symptom overviews; <using trouble breathing as an early warning sign for hypoxia>; <targeting ~94-96% PaO2 if using home oxygen concentrator>; being ready to go to hospital on very short notice, even if first-week symptoms seem mild; talking to a doctor over phone/video first; taking things to soothe throat and prevent coughing if sick; not trying to lower your fever unless it gets to 103°F or higher; considering postural drainage for severe symptoms; if sick and in an at-risk group, considering signing up for nearby clinical trials
- Deleted: being wary of people breathing; never re-using masks
Mar. 31 — Added: lying on your front if you get sick
- Deleted: using sleeve instead of hand if your eye itches; carrying a handkerchief for touching your nose or mouth without using your hands
Apr. 1 — Added: using UVC light to disinfect surfaces
- Deleted: running an air purifier
Apr. 5 — Added: noting average time from infection to symptom onset is 7 days
- Deleted: noting average time from infection to symptom onset is 5 days
Apr. 26 — Added [LW(p) · GW(p)]: tips for homemade masks; stocking up on 1+ months of water; watching out for (possibly unconscious) unusually fast and deep breathing as an extremely serious warning COVID-19 sign, even if not accompanied by discomfort or other symptoms; using oximeter every few days even if you feel fine; using oximeter a lot and otherwise monitoring symptoms carefully if might have recently been exposed, or if you start showing lower oximeter readings, other "silent hypoxia" signs, or cold/flu symptoms, rather than relying on fever as the first warning sign
- Deleted: using thermometer as an earlier warning sign than the oximeter; using trouble breathing as an early warning sign for hypoxia
Apr. 27 — Added [LW(p) · GW(p)]: <keeping Vitamin K intake low/moderate [LW(p) · GW(p)]>; avoiding motorcycle races and reproduction; watching for signs of heart attack, stroke, or pulmonary embolism even if you have no other symptoms and no known risk factors; <taking aspirin prophylactically if you get sick or may get sick soon>; maybe using home coagulation tests if sick
Apr. 29 — Added: noting Haagen Dasz refreezes better than other ice cream brands
May 3 —
- Deleted: taking aspirin prophylactically if you get sick or may get sick soon
May 8 — Added [LW(p) · GW(p)]: noting Erin Bromage's "Successful Infection = Exposure to Virus x Time" guidelines; avoiding public restrooms; avoiding rooms where someone might have recently coughed, sneezed, or yelled
May 10 —
May 12 — Added [LW(p) · GW(p)]: noting other forms of oxygen supplementation may be much better than invasive mechanical ventilation
Jun. 2 — Added [LW(p) · GW(p)]: focusing more on large-droplet transmission, less on aerosol or surface transmission; avoiding talking in public; being quiet and aiming down if forced to talk in public; avoiding facing nearby people in public; relying on physical models rather than the "6-Foot Rule"; prioritizing small reductions to larger risks over large reductions to very small risks; meal delivery being much safer than going grocery shopping; disinfecting delivered meals
- Deleted [LW(p) · GW(p)]: being wary of people ≤ 6 feet away [but I do recommend this]; not buying medical-grade masks since health care providers need as many as possible; not using NSAIDs [LW(p) · GW(p)]; quitting smoking [but I do recommend this]
Jun. 4 — Added: this very comment
- Deleted: keeping Vitamin K intake low/moderate [LW(p) · GW(p)]
Nov. 9 — Added: preamble discouraging hyper-caution and encouraging adjusting to circumstances.
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2020-06-04T19:15:24.115Z · LW(p) · GW(p)
Tobias Dänzer says in a Google Doc comment:
FYI, you're simultaneously proposing very high doses of Vitamin D, and keeping vitamin K intake low (section 2L). I've mostly read recommendations to take both together.
Random non-authoritative source: https://www.healthline.com/nutrition/vitamin-d-and-vitamin-k#section3
> Put simply, vitamin D toxicity may cause blood vessel calcification, while vitamin K may help prevent this from happening.
> SUMMARY: Scientists don't know whether high vitamin D intake is harmful when vitamin K intake is inadequate. Evidence suggests it might be a concern, but a definite conclusion cannot be reached at this point.
Of course, Covid may not care about this, and I don't know how to quantify the relative risks, but they should probably be acknowledged.
In response to this, I've deleted the section on Vitamin K, which was already really speculative. The deleted section is copied below:
__________________________________________________
Per 3G below, COVID-19 seems to be causing blood clots in many people. Vitamin K apparently has a large pro-clotting effect, so I recommend reducing intake of foods rich in vitamin K now, and cutting them out altogether for a few weeks if you think you may have recently contracted COVID-19. Cleveland Clinic says high-vitamin-K foods include:
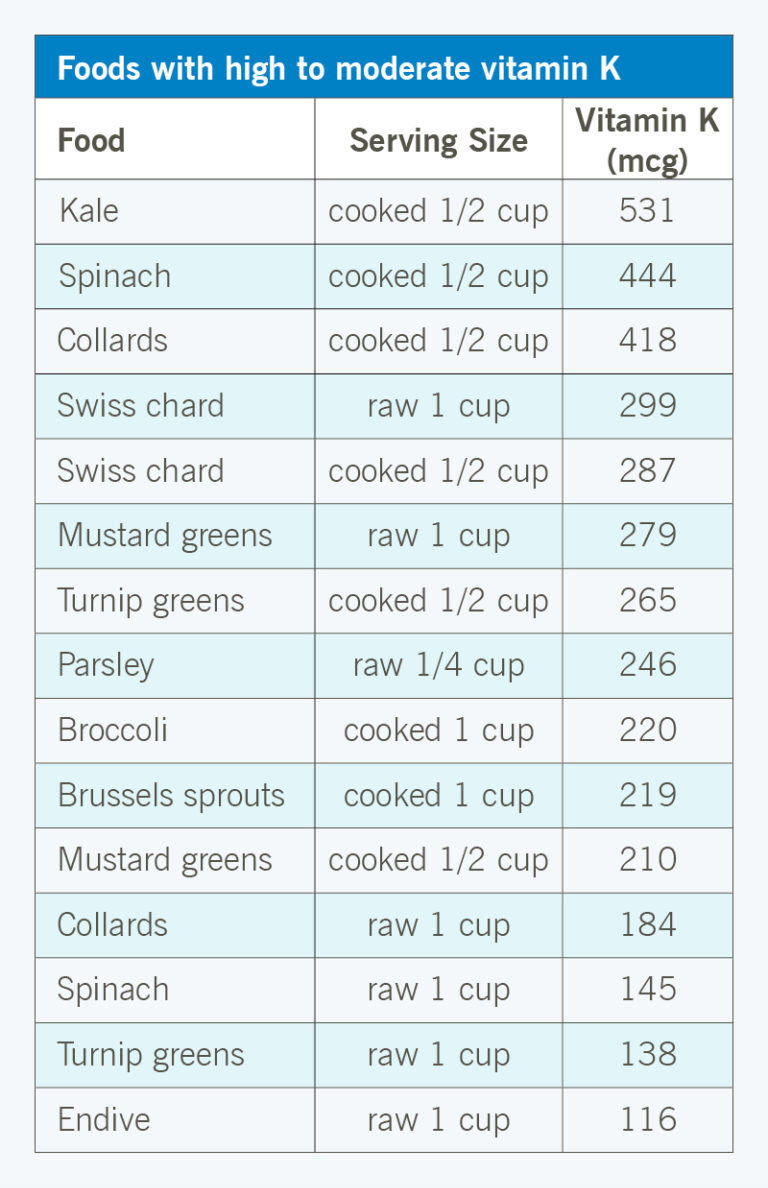
Other vegetables are generally fine and great.
Eating healthy, exercising regularly, avoiding smoking, etc. also normally reduces clotting risk. (But excessive clotting caused by COVID-19 may not work like normal: the Washington Post says COVID-19 is causing strokes in young people "mostly without risk factors", and CNN suggests they often have "no past medical history" and have mild or otherwise-asymptomatic cases of COVID-19, all of which suggest the clotting issues may be disproportionately affecting healthy people, even as COVID-19's more typical symptoms disproportionately affect less healthy people.)
comment by John_Maxwell (John_Maxwell_IV) · 2020-04-04T07:20:30.591Z · LW(p) · GW(p)
I'm confused why people aren't talking about guaifenesin more for COVID. It seems like COVID kills by clogging your lungs up with mucus that's hard/impossible to cough out, and guaifenesin is a drug that loosens congestion. (Probably best to get the stuff without DXM, because you want to be coughing!)
comment by K B (k-b) · 2020-04-23T19:37:52.013Z · LW(p) · GW(p)
Hello, thanks for the useful tips. Any chance of an update? There seems to b a lot of new info around , eg on:
chloroquine
remdesivir, other antivirals
smoking
thrombosis/cardiac problems
ventilator deaths
symptoms (eg lack of fever)
etc etc
↑ comment by Rob Bensinger (RobbBB) · 2020-04-27T18:51:23.066Z · LW(p) · GW(p)
I've now made updates, here and on the Google Doc version. They can be found by searching with ctrl-f for 'Added Apr. 26' and 'Added Apr. 27'. Additions made:
___
2A. Avoid people
Evidence continues to accumulate that talking is an important vector. COVID-19 superspreader events have typically involved large groups of people talking, singing, or shouting indoors.
From Scott Gottlieb: “Study of 318 outbreaks in China found transmission occurred out-of-doors in only one, involving just 2 cases. Most occurred in home or public transport. Raises key chance for states to move services outdoors (religious, gym classes, restaurants, etc). https://www.medrxiv.org/content/10.1101/2020.04.04.20053058v1”
[...]
Cf. quick thoughts about the COVID-19 endgame.
___
2B. If you do need to be around people, wear something over your mouth and nose.
For homemade masks, Hrothgar says:
[...] I'd choose the thickest, most finely woven materials available and layer them as much as possible without making it difficult to breathe. Then I'd wear those outside, taking all other precautions (distance, goggles, etc), and breathe SLOWLY through my nose. Slowly because lower air velocity reduces penetration, nose because it acts as a filter as well. Then I'd wash everything immediately & thoroughly upon arriving home.
Source: Combine these studies about the effectiveness of cloth/DIY masks
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2440799/
https://academic.oup.com/annweh/article/54/7/789/202744
with this tweet (by a virologist) about the importance of initial viral load
https://twitter.com/PeterKolchinsky/status/1239560638239838215
and then the missing piece is about droplet size + filter grain, which will vary based on what you put over your face.
Thicker materials are better, as you might expect. Towels & Hanes sweatshirts performed best in this study:
___
2D. Have emergency supplies.
The CDC recommends having a two-week backup supply of clean drinkable water. I would recommend stockpiling 1+ months of water (i.e., 30+ gallons per person) if you have room. The Guardian reports Apr. 20 that there’s an emerging shortage of CO2, and The Prepared notes that “CO2 is an essential input for the municipal water treatment process. (It’s also vital to many critical industrial processes–from agriculture to meat processing to food preservation).” The Prepared also notes other chemicals used in water treatment whose supply could be disrupted in various scenarios.
___
2H. Maybe stop taking ibuprofen/advil?
[Section renamed from "Probably stop taking NSAIDs like ibuprofen."]
[Section rewritten. Summary: I now put less probability on NSAIDs being bad, and for reasons noted below, I specifically suggest taking the NSAID aspirin if you think you have COVID-19. I've added quotes to this section so it's easier to see the complicated mess of claims that people are making.]
___
2K. Stay healthy: eat well, sleep well, get exercise.
And consider avoiding things that might put you in a hospital, like motorcycle races or getting pregnant; hospitals are risky during pandemics.
___
2L. Keep Vitamin K intake low/moderate.
[New section. Summary: on priors, vitamin -K-rich foods may increase clotting risk from COVID-19.]
___
3A. Prepare in advance.
Given the “silent hypoxia” update at the bottom of 3D below, and the blood clot update in 3G below, you should probably use the pulse oximeter regularly even if you’re showing no symptoms, and should stay alert for signs of stroke, heart attack, or pulmonary embolism even if you’re showing no other symptoms.
___
3D. Start monitoring your oxygen more often at the smallest warning sign.
... including if you’re asymptomatic but have exposed yourself to possible infection vectors in the last two weeks. If you develop a fever or experience significant chest tightness or difficulty breathing, definitely start monitoring your oxygen; but don’t wait that long if you can avoid it.
[Section renamed from "Start monitoring your oxygen immediately if you develop a fever or experience significant chest tightness or difficulty breathing."]
[...]
streawkceur writes [LW(p) · GW(p)], “According to this article, it seems clear by now that low oxygen is in fact dangerous even when you feel fine, so buying a pulse oximeter is useful. https://www.nytimes.com/2020/04/20/opinion/sunday/coronavirus-testing-pneumonia.html” Quoting the article:
[...] These patients did not report any sensation of breathing problems, even though their chest X-rays showed diffuse pneumonia and their oxygen was below normal. How could this be?
We are just beginning to recognize that Covid pneumonia initially causes a form of oxygen deprivation we call “silent hypoxia” — “silent” because of its insidious, hard-to-detect nature.
Pneumonia is an infection of the lungs in which the air sacs fill with fluid or pus. Normally, patients develop chest discomfort, pain with breathing and other breathing problems. But when Covid pneumonia first strikes, patients don’t feel short of breath, even as their oxygen levels fall. And by the time they do, they have alarmingly low oxygen levels and moderate-to-severe pneumonia (as seen on chest X-rays). Normal oxygen saturation for most persons at sea level is 94 to 100 percent; Covid pneumonia patients I saw had oxygen saturations as low as 50 percent.
To my amazement, most patients I saw said they had been sick for a week or so with fever, cough, upset stomach and fatigue, but they only became short of breath the day they came to the hospital. Their pneumonia had clearly been going on for days, but by the time they felt they had to go to the hospital, they were often already in critical condition. [...]
We are only just beginning to understand why this is so. The coronavirus attacks lung cells that make surfactant. This substance helps the air sacs in the lungs stay open between breaths and is critical to normal lung function. As the inflammation from Covid pneumonia starts, it causes the air sacs to collapse, and oxygen levels fall. Yet the lungs initially remain “compliant,” not yet stiff or heavy with fluid. This means patients can still expel carbon dioxide — and without a buildup of carbon dioxide, patients do not feel short of breath.
Patients compensate for the low oxygen in their blood by breathing faster and deeper — and this happens without their realizing it. This silent hypoxia, and the patient’s physiological response to it, causes even more inflammation and more air sacs to collapse, and the pneumonia worsens until oxygen levels plummet. In effect, patients are injuring their own lungs by breathing harder and harder. Twenty percent of Covid pneumonia patients then go on to a second and deadlier phase of lung injury. Fluid builds up and the lungs become stiff, carbon dioxide rises, and patients develop acute respiratory failure.
By the time patients have noticeable trouble breathing and present to the hospital with dangerously low oxygen levels, many will ultimately require a ventilator.
Silent hypoxia progressing rapidly to respiratory failure explains cases of Covid-19 patients dying suddenly after not feeling short of breath. [...]
There is a way we could identify more patients who have Covid pneumonia sooner and treat them more effectively — and it would not require waiting for a coronavirus test at a hospital or doctor’s office. It requires detecting silent hypoxia early through a common medical device that can be purchased without a prescription at most pharmacies: a pulse oximeter.
Relatedly, Paul Bohm notes, “54% of asymptomatic cases and 79% of COVID-19 symptomatic cases on the Diamond Princess had ground-glass abnormalities in their CT scans.”
This suggests that even if you seem completely asymptomatic (or have very mild symptoms), you should periodically use a home pulse oximeter if there’s a nontrivial risk you recently caught the virus. Additionally, unusually fast and deep breathing is a thing to watch out for, even in otherwise asymptomatic or mildly symptomatic people.
___
3G. Take aspirin prophylactically, and monitor for clotting problems.
[New section.]
Evan Hubinger says:
There have been a lot of reports recently of young people (30s and 40s) developing blood clotting complications due to covid19 infection, resulting in strokes, heart attacks, and pulmonary embolisms. Apparently this can happen even for people who are otherwise asymptomatic. Actionable items:
1. Monitor yourself for stroke, heart attack, etc. symptoms and get to the hospital ASAP if you have any—one of the major reasons these cases are so bad right now is that young, otherwise asymptomatic people aren't used to looking for stroke symptoms and aren't rushing to the hospital.
2. If you think there's a high risk you might have covid19, consider taking a blood thinner such as aspirin.
From Live Science on Apr. 23:
[...] The link between COVID-19 and clots has led some hospitals to put all COVID-19 patients on low doses of blood thinners to prevent clots, according to CNN.
[...] A recent study from the Netherlands, published in the journal Thrombosis Research, found that out of 184 COVID-19 patients in the ICU, more than 30% experienced some type of clotting issue. [...]
From CNN on Apr. 23:
[...] The new coronavirus appears to be causing sudden strokes in adults in their 30s and 40s who are not otherwise terribly ill, doctors reported Wednesday.
[...] Dr. Thomas Oxley, a neurosurgeon at Mount Sinai Health System in New York, and colleagues gave details of five people they treated. All were under the age of 50, and all had either mild symptoms of Covid-19 infection or no symptoms at all.
"The virus seems to be causing increased clotting in the large arteries, leading to severe stroke," Oxley told CNN.
"Our report shows a seven-fold increase in incidence of sudden stroke in young patients during the past two weeks. Most of these patients have no past medical history and were at home with either mild symptoms (or in two cases, no symptoms) of Covid," he added.
[...] "For comparison, our service, over the previous 12 months, has treated on average 0.73 patients every 2 weeks under the age of 50 years with large vessel stroke," the team wrote in a letter to be published in the New England Journal of Medicine. [...]
From the Washington Post on Apr. 25:
[... At Mount Sinai there have been] several recent [large-vessel] stroke patients in their 30s to 40s who were all infected with the coronavirus. The median age for that type of severe stroke is 74.
[...] Many researchers suspect strokes in covid-19 patients may be a direct consequence of blood problems that are producing clots all over some people’s bodies.
[...] At Mount Sinai, the largest medical system in New York City, physician-researcher J Mocco said the number of patients coming in with large blood blockages in their brains doubled during the three weeks of the covid-19 surge to more than 32, even as the number of other emergencies fell. More than half of [them] were covid-19 positive.
[...] The covid-19 patients treated for stroke at Mount Sinai were younger and mostly without risk factors.
On average, the covid-19 stroke patients were 15 years younger than stroke patients without the virus. [...]
If you start showing COVID-19 symptoms or you think there's a good chance you were recently infected, then especially if you're young, I suggest that you start taking aspirin prophylactically, to reduce the risk of blood clots. (Don't take aspirin if you have low blood pressure; do take it if you have normal or elevated blood pressure.)
Symptoms to watch out for:
- For stroke, the FAST mnemonic summarizes the main symptoms: if one side of your face starts drooping or goes numb, one arm suddenly goes weak or numb, or your speech becomes slurred or garbled, it's time to call 911. Other symptoms can include: sudden leg weakness or numbness, especially on one side of the body; sudden confusion, trouble understanding speech; sudden trouble seeing in one or both eyes; sudden trouble walking, dizziness, loss of balance or coordination; sudden severe headache with no known cause.
- For heart attack in cis women, the Heart Foundation lists these signs: "(1) As with men, women’s most common heart attack symptom is chest pain or an uncomfortable pressure, squeezing, fullness or pain in the center of your chest. It lasts more than a few minutes, or goes away and comes back. (2) Pain or discomfort in one or both arms, the back, neck, jaw or stomach. (3) Shortness of breath with or without chest discomfort. (4) Other common symptoms in women include breaking out in a cold sweat, nausea/vomiting, or feeling lightheaded, palpitations; sleep disturbances and unexplained fatigue."
For heart attack in cis men: "(1) Chest discomfort. Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain. (2) It used to be thought that only chest pain was a sign of heart attack, but it’s possible to have discomfort that doesn’t register as painful. Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach. (3) Shortness of breath with or without chest discomfort. (4) Other signs may include breaking out in a cold sweat, nausea or feeling lightheaded."
I don’t know of research on heart attack signs in people undergoing transgender hormone therapy; data may be scarce because this is a relatively young population.
The Heart Foundation adds: "Don’t wait to get help if you experience any of these heart attack warning signs. Although some heart attacks are sudden and intense, most start slowly, with mild pain or discomfort." - For pulmonary embolism, Cedars Sinai says, "The most common symptoms include: sudden shortness of breath (most common); chest pain (usually worse with breathing); a feeling of anxiety; a feeling of dizziness, lightheadedness, or fainting; irregular heartbeat; palpitations (heart racing); coughing or coughing up blood; sweating; low blood pressure. You may also have symptoms of deep vein thrombosis (DVT), such as: pain in the affected leg (may happen only when standing or walking); swelling in the leg; soreness, redness, or warmth in the leg(s); redness and/or discolored skin."
___
3H. Consider taking more extreme measures if you're experiencing serious COVID-19 symptoms, or if you have the resources to take bonus precautions.
[Section renamed from "Consider taking more extreme measures if you're experiencing serious COVID-19 symptoms, or if you're at-risk (i.e., you're older or have other health issues) or have the resources to take bonus precautions."]
If you’re worried about blood clot risks from COVID-19 (discussed in 3G), you may want to use home coagulation tests.
Replies from: John_Maxwell_IV↑ comment by John_Maxwell (John_Maxwell_IV) · 2020-05-01T20:55:45.357Z · LW(p) · GW(p)
I just finished a video appointment with a cardiologist where we discussed the clotting thing. Even though he seemed to think I had COVID, and I recently had an abnormal EKG and some mild chest tightness, he thought it was better to avoid blood thinners. Apparently he has been receiving Cochrane reports on COVID before they are publicly available. He said that the increased clotting is usually in patients w/ some kinda predisposition and tends to be worse with more severe symptoms. Even for low-dose aspirin, he thinks the risk of bleeding is larger than the potential benefits. "I've seen all these complications from blood thinners." (I'm 28 FYI.)
Note that despite previous speculation [LW · GW] on LW regarding prophylactic use of low-dose aspirin for longevity, a large clinical trial found it wasn't useful in older folks (age 65+). Note this bit:
Significant bleeding—a known risk of regular aspirin use—was also measured. The investigators noted that aspirin was associated with a significantly increased risk of bleeding, primarily in the gastrointestinal tract and brain. Clinically significant bleeding—hemorrhagic stroke, bleeding in the brain, gastrointestinal hemorrhages or hemorrhages at other sites that required transfusion or hospitalization—occurred in 361 people (3.8 percent) on aspirin and in 265 (2.7 percent) taking the placebo.
At the very least, I suggest you change your recommendation from "aspirin" to "low-dose aspirin". Overall, I'm more inclined to trust secondhand accounts of Cochrane preprints than collections of anecdotes in the media.
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2020-05-03T15:26:55.535Z · LW(p) · GW(p)
Thanks, John. Based on this, I've removed my recommendation that people take aspirin, and I've added your full comment to that part of the post.
↑ comment by Rob Bensinger (RobbBB) · 2020-04-23T18:25:25.116Z · LW(p) · GW(p)
I'm not immediately planning any changes. If folks make things easy on me by saying specific sentences they want added, references they want linked, etc., that increases the probability I'll make updates. :)