Covid 12/22/22: Reevaluating Past Options
post by Zvi · 2022-12-22T16:50:01.236Z · LW · GW · 2 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Physical World Modeling In Other Covid News Remember Reevaluating Focused Protection Other Medical and Research News None 2 comments
This is the non-China section of this week’s update. Despite there being essentially zero good statistical data about the real situation in China, things are clearly moving fast, and I have assembled what useful information I have been able to find. If cases are rising as quickly as some reports suggest, their wave could crest within a matter of weeks and life be back to normal within a few months.
Back here in America, things are quiet. It seems like it was a good week to look back, as MR did, upon our options regarding focused protection, and what we can take away from that.
Executive Summary
- China fully lets it rip, see post on that for more information.
- Protecting the vulnerable mostly is about doing generally correct things.
- Numbers rise modestly less than expected, limiting worst case risk a bit.
Let’s run the numbers.
The Numbers
Predictions
Note that last week had some case count glitches in Florida and Georgia that I didn’t catch; I’ve adjusted both in opposite directions retroactively.
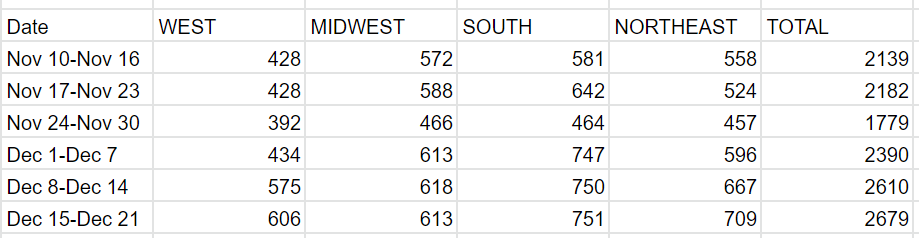
Predictions from Last Week: 435k cases (+10%) and 2,900 deaths (+10%)
Results: 427k cases (+9%) and 2,679 deaths (+3%).
Predictions for Next Week (Christmas): 410k cases (-4%) and 2,500 deaths (-7%).
Deaths number was a pleasant surprise that limits the worst case scenarios a bit. The case number was in line with expectations, especially after the FL/GA error fixes. Note that the prediction for next week is based on it being a holiday, I still expect a modest rise in actual case numbers for another few weeks.
Deaths

Cases
Physical World Modeling
CDC recommendations have always been the ultimate motte and bailey. Now a judge has made this fact text, allowing any public health department to mandate any recommendation of the CDC without the ability to challenge it.
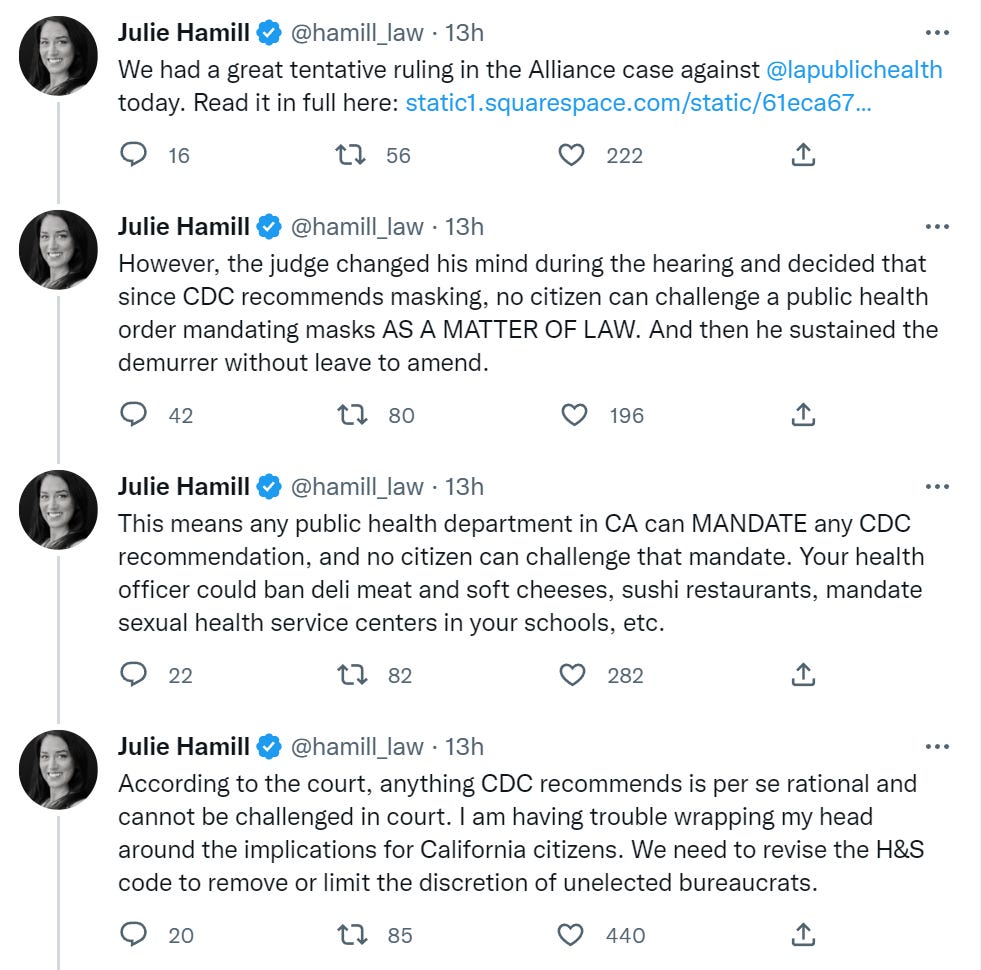
Given the tendencies of people in public health, if they have the ability to mandate something without being challenged, there is a very good chance they are going to do exactly that.
The problem is we have no category or word for the thing that we want to exist here, which is ‘CDC says this is what it thinks would be good for an individual to do, while noticing that mandating this would be deeply foolish.’ The word we use in English has been taken and now means something else, and I would expect this to happen to any chosen future words as well.
Bob Wachter thread attempts to explain the nuances of the effectiveness of masks, vaccinations, boosters and home tests. In all three cases, the issue he’s trying to fix seems to have been made worse due to authorities talking often in terms of things ‘working’ versus ‘not working’ and oversold benefits, which leads to people thinking that if the benefits are lesser or conditional, than they ‘don’t work.’ Also that regular people don’t have much ability to understand ‘works somewhat’ to begin with, so we weren’t starting from a great spot, either.
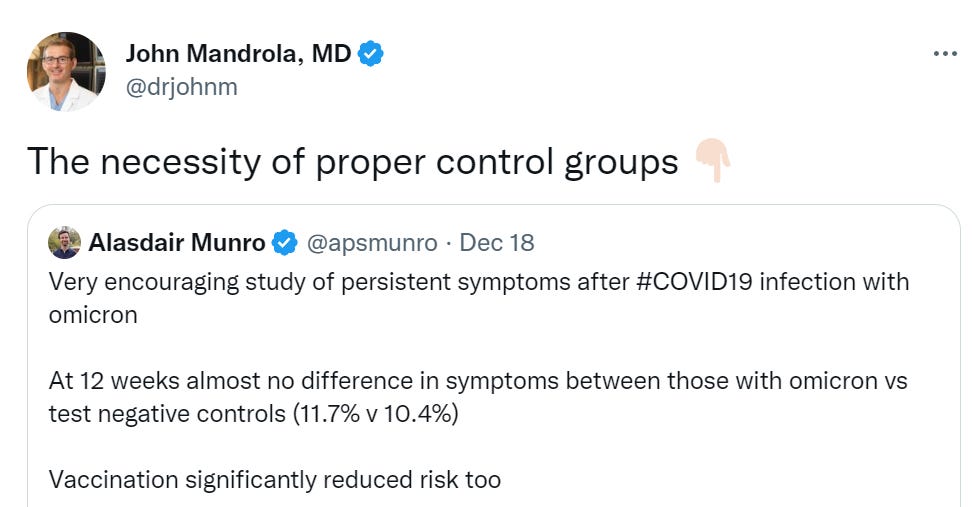
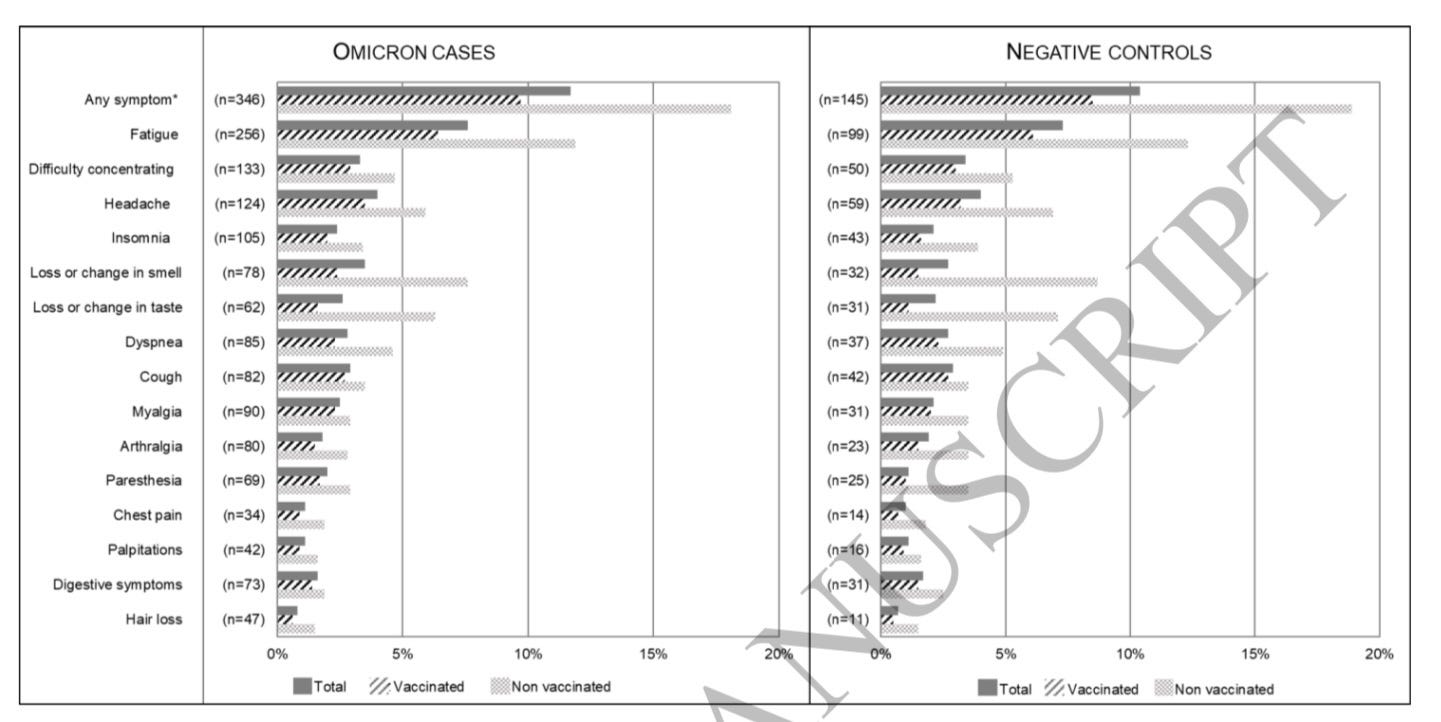
Latest example of what happens to Long Covid frequencies with proper controls (direct link).
In Other Covid News
The Biden administration has a new Covid Winter Preparedness Plan. All right, sure. They lead off with providing a bunch of free tests. Then there’s making vaccinations and treatments readily available to all Americans. It goes on to have supplies ready, monitor variants, and to ‘focus on protecting the highest-risk Americans’ which I don’t think has any practical effect. Mostly seems like handing out free tests and doing some things I am sad needed to be written in a plan to the extent they have meaning, but given that this was necessary I suppose that to the extent they have meaning it is good that they were written down.
What should the Biden administration have spent their money on? Did it make sense to spend what little was left on free tests? Jerome Adams suggests spending it on free masks.
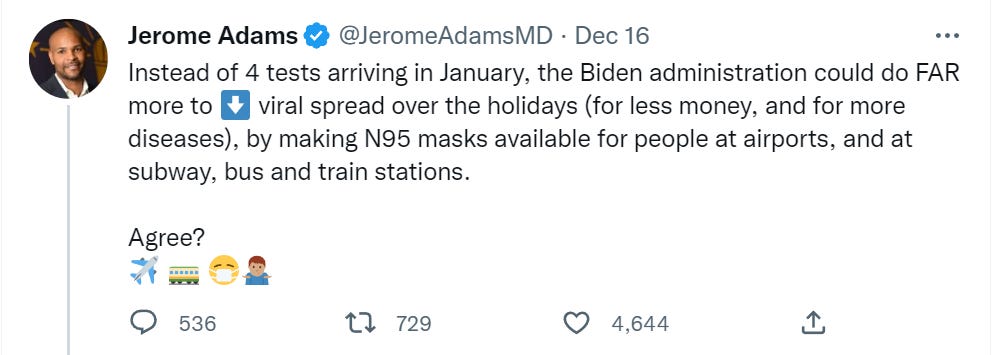
I would focus on longer term interventions and on vaccinations. Given near term actions, I do think it is very true that people often don’t wear masks because of trivial inconveniences or lack of foresight, rather than a preference not to wear one. It makes sense, from a public health perspective, to give them an easier and cheaper (both in money and cognitive effort) option, so long as this all stays voluntary. My worry is that this is an exceedingly difficult middle ground for those involved to be walking.
Especially given headlines like this: Philadelphia schools to reinstate mask mandate after winter break. Hopefully this will indeed only last ten days.
Nate Silver has the hard hitting news.


Remember
A three-minute news video reminding us what the official perspective on life was in Australia a year ago, with those who secretly ‘go see friends’ or ‘hang out by the river’ being the worst of the worst. This happened. Remember.
Stanford tried to withhold a completed degree until the student got a booster? There is always a new thing one didn’t know about.
Reevaluating Focused Protection
Alex Tabarrok asks whether focused protection along the lines of the Great Barrington Plan would have worked. His method is to ask, did better nursing homes do better?
The Centers for Medicare and Medicaid Services (CMS) has a Five-Star Rating system for nursing homes. The rating system is based on comprehensive data from annual health inspections, staff payrolls, and clinical quality measures from quarterly Minimum Data Set assessments. The rating system has been validated against other measures of quality, such as mortality and hospital readmissions. The ratings are pre-pandemic ratings. Thus, the question to ask is whether higher-quality homes had better Covid-19 outcomes? The answer? No.
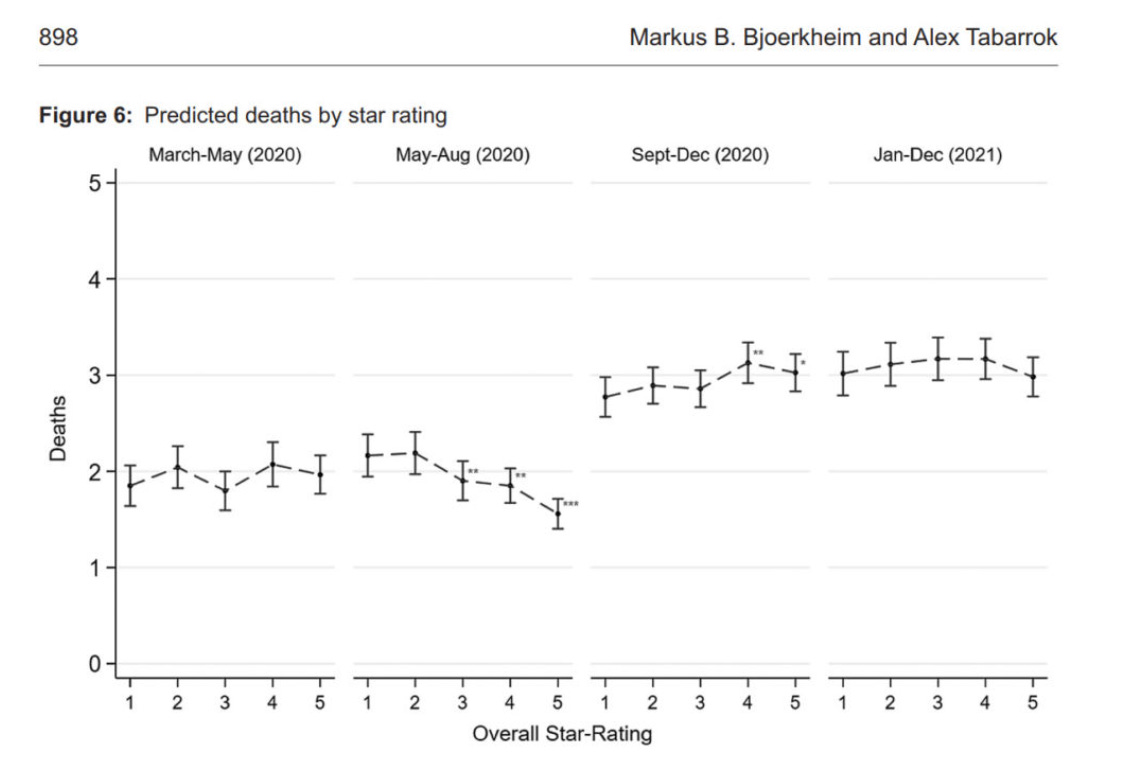
That does look an awful lot like no effect.
Finally, keep in mind that the United States did focused protection. Visits to nursing homes were stopped and residents and staff were tested to a high degree. What the US did was focused protection and lockdowns and masking and we still we had a tremendous death toll in the nursing homes. Focused protection without community controls would have led to more deaths, both in the nursing homes and in the larger community. Whether that would have been a reasonable tradeoff is another question but there is no evidence that we could have lifted community controls and also better protected the nursing homes. Indeed, as I pointed out at the time, lifting community controls would have made it much more difficult to protect the nursing homes.
I file ‘nursing home quality had no impact on Covid deaths’ in the same bucket as ‘parents have no impact on their children other than genetics.’ It doesn’t actually make any sense. If nothing else, we can all point to really bad nursing home practices that definitely got more elderly people infected or killed, the same way we can point out some really bad parents that definitely screw up their kids. You can argue that one can reasonably expect to be in the parental subset that doesn’t do that, and the point is debatable. Given what we’ve seen from nursing homes? Not so much.
Thus, I interpret this partly as saying ‘the things that worked for Covid are orthogonal to the things that worked to get high overall ratings pre-Covid.’ Why could that be? One plausible theory is that highly rated nursing homes facilitate more interactions that are more often closer, both between different residents and with the staff, which for Covid backfires. Another is that the highly rated nursing homes don’t otherwise kill their residents early, or otherwise had sicker or older residents. A third is that highly rated places didn’t try as often to disguise Covid deaths as something else. A fourth is that perhaps the users of highly rated facilities were in better social position to demand the kind of access that got people infected, whereas low rated facilities faced less such pressure. Or perhaps ratings of nursing homes are about doing snow jobs on relatives rather than being a good place for the residents. I don’t know.
I do think the core assertion here, that focused protection of those in nursing homes was not in practice a realistic option, is still mostly correct. We were not sufficiently capable of understanding what such protection would look like physically, or of implementing what we did know in the face of social and commercial pressures. There was no way to get everything we would have wanted. There were still plenty of ways to do better or more right by our most vulnerable, and one of those would have been to open up more other things sooner to larger degrees.
What about strategies of the form ‘let more healthy people get sick sooner so we shrink the window where we need to lock down nursing homes?’ That implies that we would have been capable of some combination of locking down harder during the crucial period in an effective way despite the strain on personnel, and that we would then have been able to loosen back up again despite not having vaccines, and there still being a decent amount of Covid out there even after an intentionally engineered peak. I am skeptical.
Of course, as Alex also points out, earlier vaccinations would have definitely worked. We clearly had odds to vaccinate nursing home residents months earlier, even if we couldn’t have speeded things along in general.
Tyler also gets into the act by asking: Who was really for ‘forced protection of the vulnerable?’ which I’m reproducing in full here.
Yes I do mean during the Covid-19 epidemic. As a follow-up post to Alex’s, and his follow-up, here are some of the effective measures in protecting the vulnerable, or they would have been more effective, had we done them better:
1. Vaccines, including speedy approval of same.
2. Prepping hospitals in January, once it became clear we should be doing so. That also would have limited lockdowns! And yet we did basically nothing.
3. Speeding up and improving the research process for anti-Covid remedies and protections.
4. First Doses First, when that policy was appropriate, among other policy ideas (NYT).
5. Effective and rapid testing equipment, readily available on the market.
If you were out promoting those ideas, you were acting in favor of protecting the vulnerable. If you were not out promoting those ideas, but instead talked about “protecting the vulnerable” in a highly abstract manner, you were not doing much to protect the vulnerable.
This seems right. You protect the vulnerable by doing things that improve our response overall, and having the benefits largely flow to those who are vulnerable. I would add those who advocated early for masks when authorities were telling us they didn’t work, and all the other ‘usual suspects.’
Trying to shift relative attention in various ways was mostly a side show. The only thing that seems like a plausible exception is advocating allocating vaccinations by age or real vulnerability rather than by proximity to power and ability to navigate the system.
(Original has two 5s so I incremented the numbers below by 1).
And here are three actions that endangered the vulnerable rather than protecting them:
6. Publishing papers suggesting a very, very low Covid-19 mortality rate, and then sticking with those results in media appearances after said results appeared extremely unlikely to be true.
7. Maintaining vague (or in some cases not so vague) affiliations with anti-vax groups.
8. Not having thought through how “herd immunity” doctrines might be modified by ongoing mutations.
Keep all that in mind the next time you hear the phrase “protecting the vulnerable.”
That does not mean that we could not have reallocated our Covid prevention in ways that increased the number of cases and especially early cases in the young relative to the old, and benefited thereby. Which we could have largely implemented by giving people more individual choices sooner, and letting them decide how to adjust. Such outcomes, however, fall more into the ‘we do less damage to our lives without also becoming net sicker, or at least not substantially sicker’ rather than ‘the elderly actively do better.’
Also, if you were so big on protecting the vulnerable now, they are still vulnerable to a wide variety of non-Covid problems as well as Covid. We do a lot of horrible things to our elderly nursing home residents and I see very little in the way of caring about it.
Other Medical and Research News
White House to include a permanent position in charge of pandemic response. That is a thing we did not previously have, somehow.
Preprint suggests (preprint) that herd immunity threshold for monkeypox was super duper low, like 0.5% of MSM community low, due to off the charts heterogeneity combined with not being that far over the threshold at the start. This makes sense.
Flu season still rather not great, but it is starting to improve as per Rivers’ outlook.
Flu vaccination rates were similar to last year. Makes sense that people are mostly doing what they usually do rather than responding to changing conditions, both in terms of that being expected and also logical behavior. The case for the flu shot is for many people highly overdetermined, for others (that I disagree with) the case against won’t change if you double the risks.
Reminder of how The New York Times and similar media cover things, and very good news on our emergency departments, who are doing a great job.
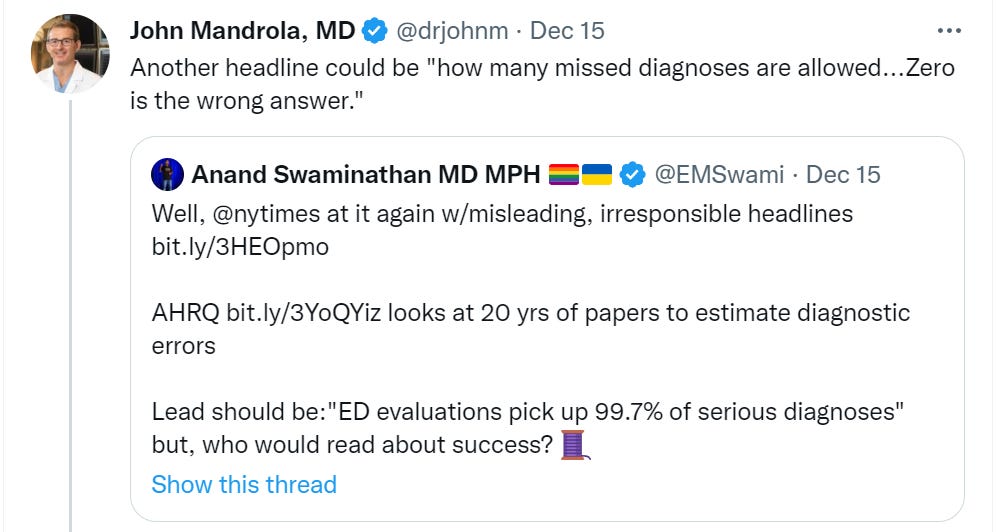
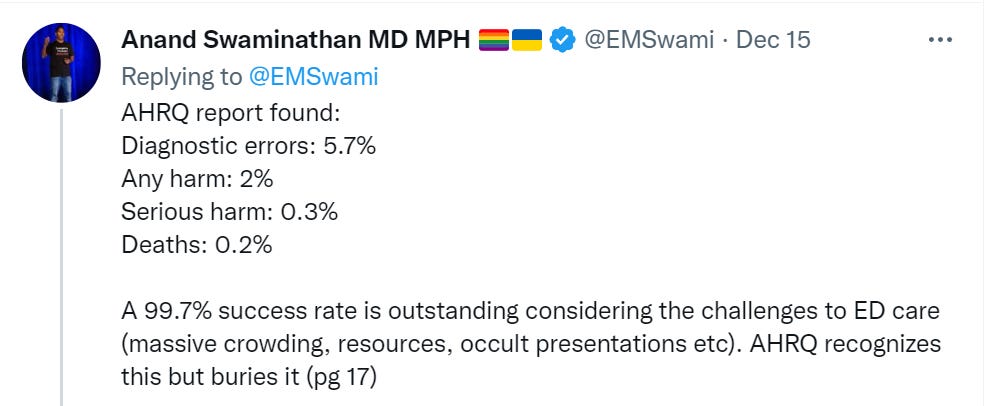
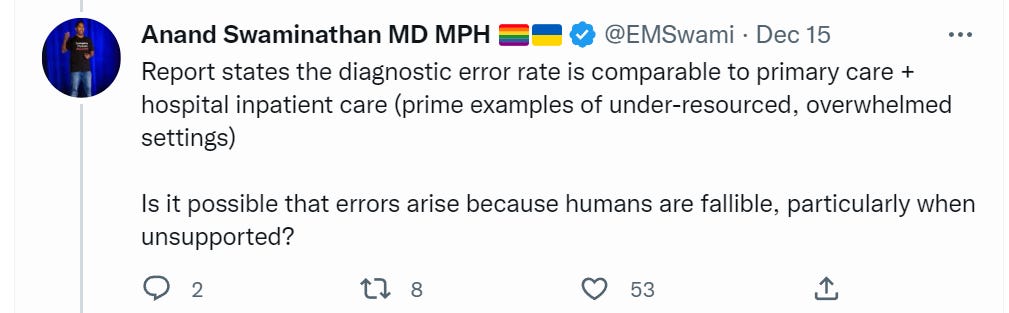
Seriously, given the conditions I’m making a note here, huge success. It’s hard to overstate my satisfaction.
That wasn’t their worst one this week. Seriously, NYT, huh (OP)? A 3% Covid-19 fatality rate got past your editors and fact checkers, even now?
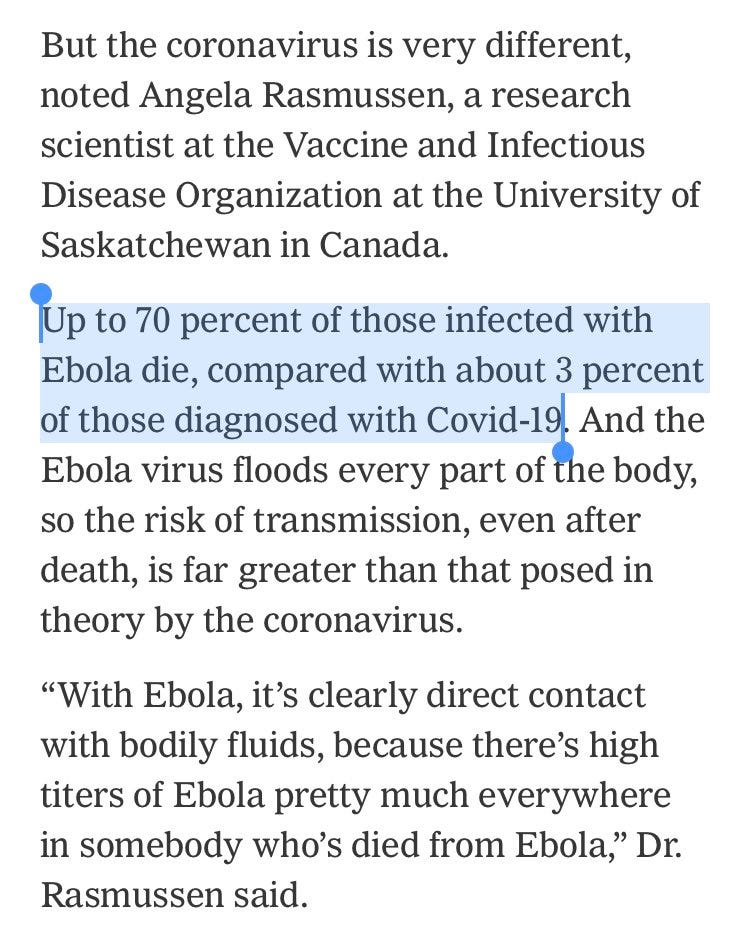
Also confused how the instinct in response can be not ‘whoops’ but rather ‘well, sort of, if you squint at it right?’
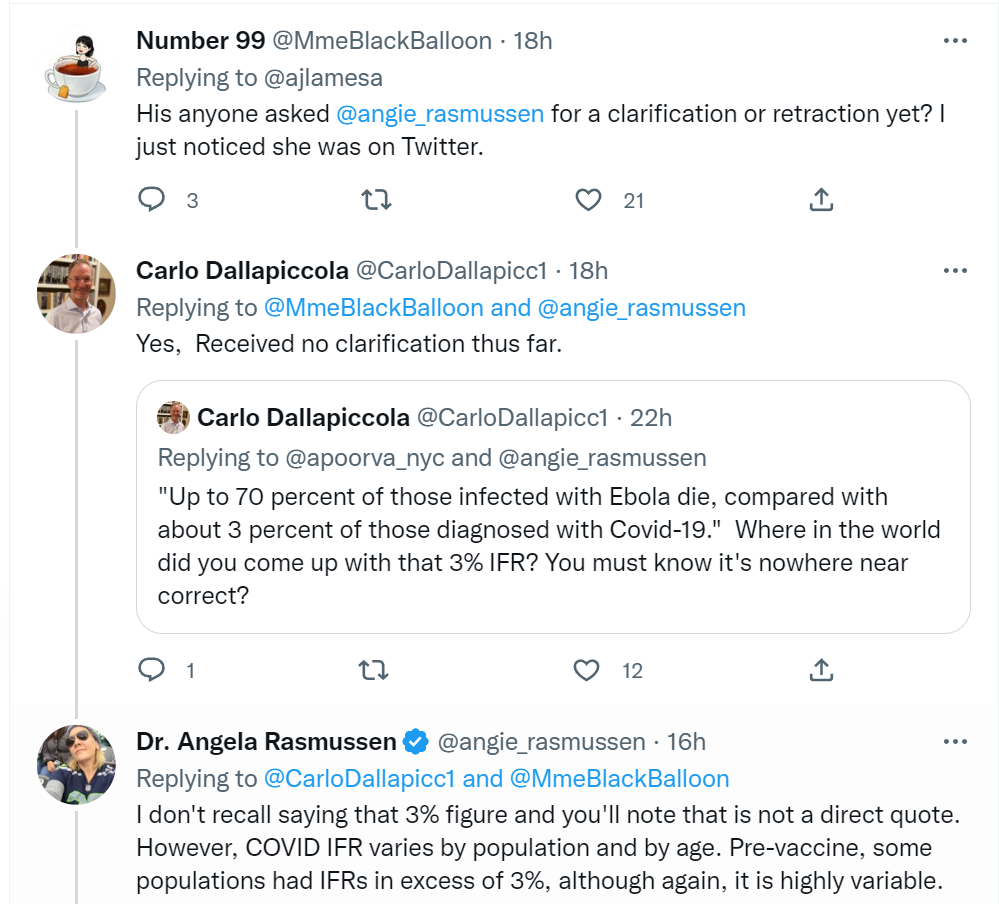
No. You don’t get to do that. Or that. Or that. Certainly not all three.
They did correct it, although in a highly misleading way.
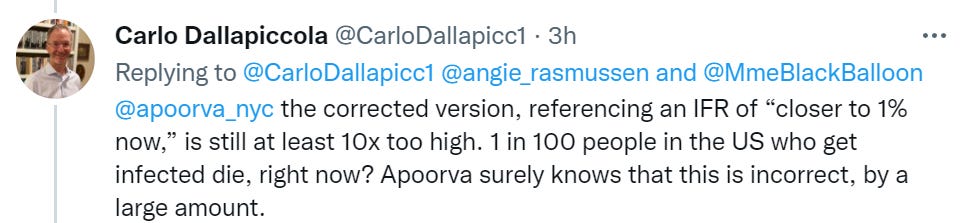
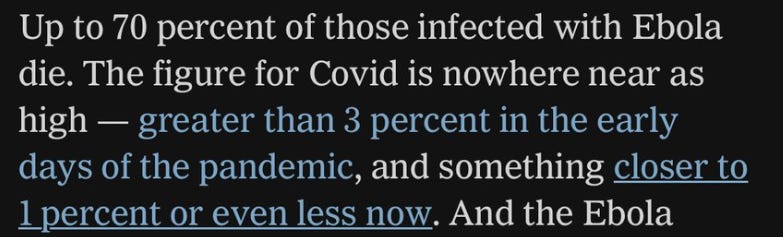
‘Closer to 1 percent’ than 3 percent implies to me somewhat more than 1 percent, which is then balanced by the ‘even less now,’ giving the impression that it’s probably around 1 percent. Which it very much isn’t.
Ventilation is a big deal. Good ventilation prevents infections, improves health and saves lives. Yet I notice my window remains closed.


We already have a lot of space that is effectively unusable due to various regulatory requirements, and lots of reasons building new things is cumbersome and expensive. I would hate to add another reason, even if you were already meeting the requirements this is one more thing you then have to continuously document and prove. That stuff adds up. Still, this one is a big game. I can see it if it was restricted to commercial and industrial zones. Ideally, of course, this happens because people demand it and are willing to pay for it.
Is the health care cost curve bending? MR links to a new paper saying that post-2009 there was a reduction of 0.8 points in health care spending growth, calling it ‘a sizeable decline in the context of the 2.0 percentage point differential in growth between health care spending and GDP in the 1970 to 2019 period.’
They imply this is due to the slowing of technological growth, which would make this very bad news on two fronts – that over time we should continue to expect growth in share of health care spending, which continues not to buy us better health, and also the bad news of slow technological growth and the further bad news that if we fixed tech growth we would undo the partial fix to the growth in health spending. Also, another (related) cause of health care spending growth is when we get wealthier, and we have not been getting as much wealthier lately.
It is better to have a huge waste of money get worse at 1.2% per year than 2.0% per year, given those are your choices. It does not mean you are in a good situation, or that the situation is improving or not doomed, even if you label it ‘bending the curve.’ My guess is this merely illustrates that yearly is not the most relevant x-axis for the curve.
2 comments
Comments sorted by top scores.
comment by hairyfigment · 2022-12-23T02:52:45.809Z · LW(p) · GW(p)
Stop lying about observed risk of death by ethnicity.
Replies from: T3t↑ comment by RobertM (T3t) · 2022-12-23T07:40:47.399Z · LW(p) · GW(p)
I see no mention of risk of death by ethnicity in the post. Do you want to clarify your accusation?