Covid 9/24: Until Morale Improves
post by Zvi · 2020-09-24T15:40:02.594Z · LW · GW · 16 commentsContents
Positive Test Counts Deaths Positive Tests by Region Test Counts For Relief That Lasts The Vaccine Protocols The Correct Vaccine Protocols CDC Accidentally Tells Truth, Profusely Apologizes CDC Announces They Have Antibody Results, Provides #Analysis Claim 3: Before having Covid-19, everyone is susceptible to Covid-19. In Other Sort-Of News: Links That Tell The Same Old Story None 16 comments
Last Two Weeks: Covid 9/17: It’s Worse, Covid 9/10: Vitamin D
There is a pandemic. It is not going anywhere.
The news, on the other hand, is ready to move on. There is a supreme court seat open. There is an election coming soon, complete with a first debate. There are protests and presumably riots flaring up once again, this time regarding there no direct charges to any police officers in the death of Breonna Taylor.
Oh, and the President of the United States said yesterday, and I quote:
“Well, we’re going to have to see what happens. You know that I’ve been complaining very strongly about the ballots and the ballots are a disaster,” Trump said, when asked if he could commit to the peaceful transition.
“(G)et rid of the ballots and you’ll have a very … there won’t be a transfer, frankly. There’ll be a continuation.”
If you are going to vote for Biden, vote in person. Make sure your vote counts and reduce the chances of chaos breaking loose before that happens.
If you’re going to vote for Trump despite everything, at least have the decency to vote by mail. That way, to count your vote, we’ll have to… count the votes.
Who cares about the pandemic? No one, it seems. That’s old news. The pandemic is now merely one more prop, albeit a big one, in the political game.
I can’t even argue. I too am more worried about the election than the pandemic, at this point.
We all grow tired of this pandemic. The damage accumulates. Economies and lives and reputations and credibility get destroyed week in and week out, and nothing good seems to come of any of it. Solutions get ignored, and the situation fails to improve. The same scolds keep saying we need to keep holding out, while scolding anyone attempting to solve the problem. Same covid time, same covid channel. If I didn’t have people thanking me every week for doing these, it would be difficult to keep going.
As usual, most of the Covid news falls into our existing patterns. When no one cares enough to do anything, but they do care enough to make sure no one else does anything, each week’s news is going to look like the previous week’s news.
And yet, if we look, there is always something worth talking about. Including one piece of genuinely great news.
Let’s run the numbers.
Positive Test Counts
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| July 30-Aug 5 | 91002 | 64462 | 212945 | 23784 |
| Aug 6-Aug 12 | 93042 | 61931 | 188486 | 21569 |
| Aug 13-Aug 19 | 80887 | 63384 | 156998 | 20857 |
| Aug 20-Aug 26 | 67545 | 66540 | 132322 | 18707 |
| Aug 7-Sep 2 | 55000 | 75401 | 127414 | 21056 |
| Sep 3-Sep 9 | 47273 | 72439 | 106408 | 21926 |
| Sep 10-Sep 16 | 45050 | 75264 | 115812 | 23755 |
| Sep 17-Sep 23 | 54025 | 85381 | 127732 | 23342 |
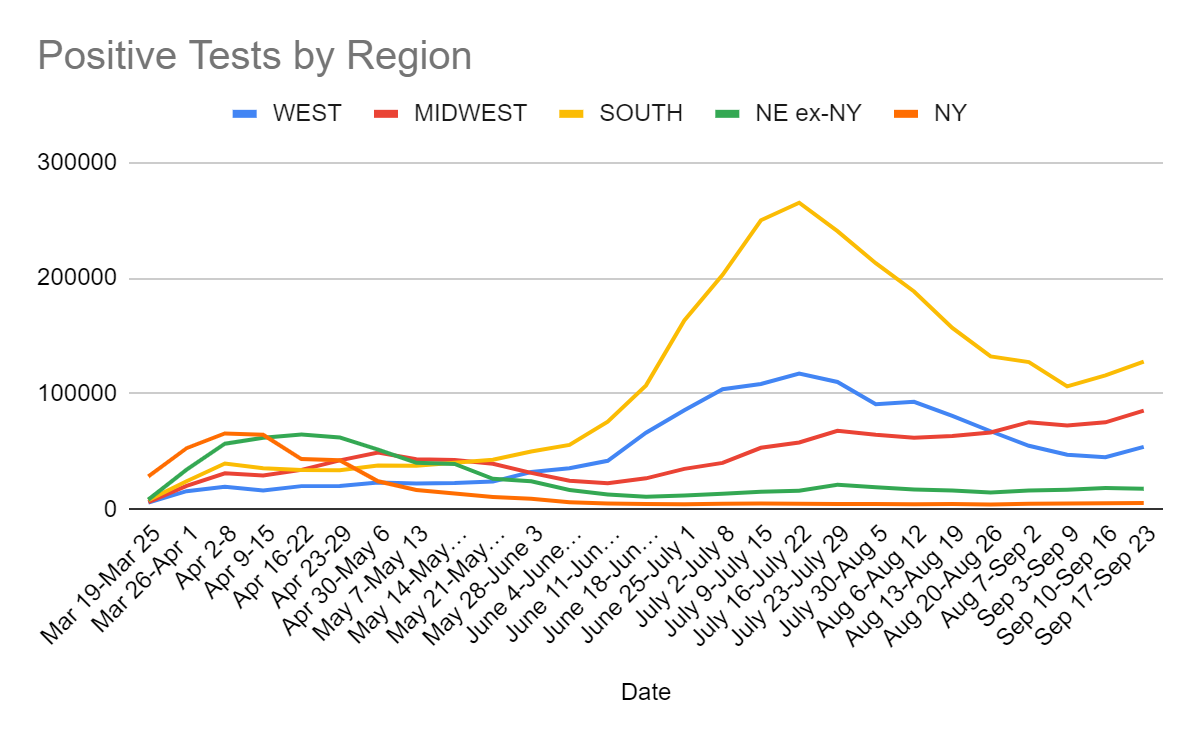
That looks bad, but the change is more than all accounted for by increased testing. It’s actually fine.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| July 16-July 22 | 1469 | 674 | 3106 | 524 |
| July 23-July 29 | 1707 | 700 | 4443 | 568 |
| July 30-Aug 5 | 1831 | 719 | 4379 | 365 |
| Aug 6-Aug 12 | 1738 | 663 | 4554 | 453 |
| Aug 13-Aug 19 | 1576 | 850 | 4264 | 422 |
| Aug 20-Aug 26 | 1503 | 745 | 3876 | 375 |
| Aug 27-Sep 2 | 1245 | 759 | 3631 | 334 |
| Sep 3-Sep 9 | 1141 | 771 | 2717 | 329 |
| Sep 10-Sep 16 | 1159 | 954 | 3199 | 373 |
| Sep 17-Sep 23 | 1016 | 893 | 2695 | 399 |
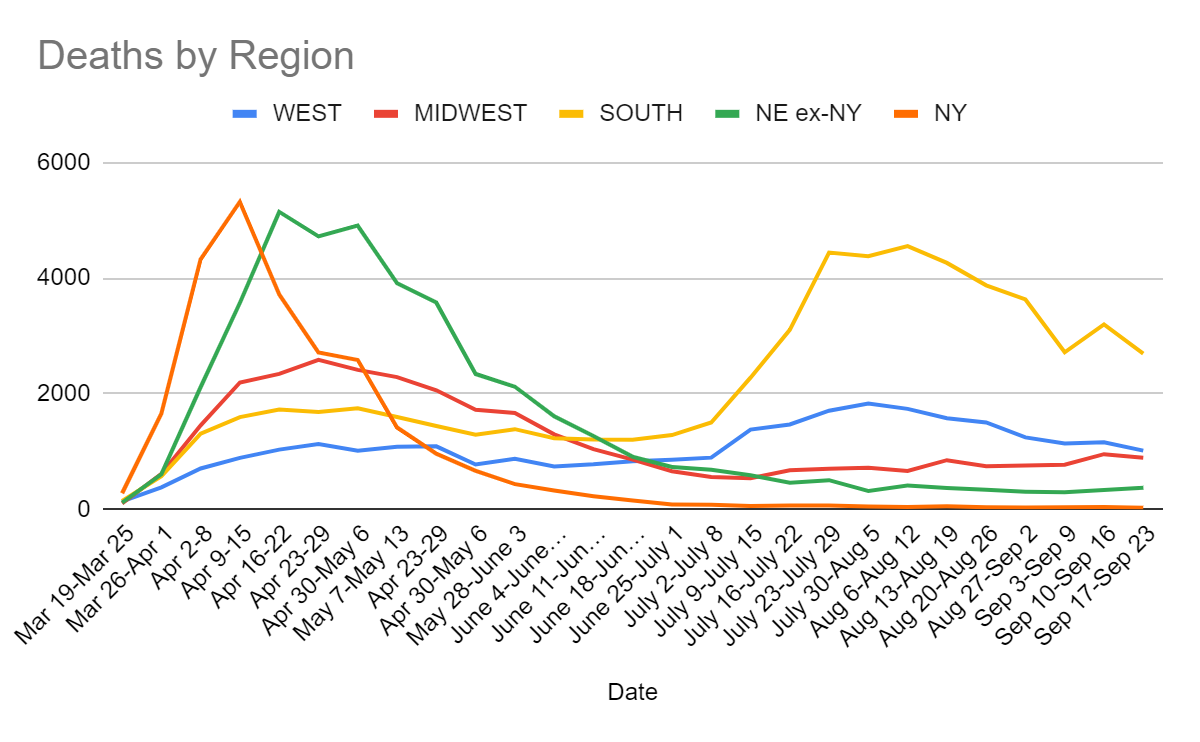
A worrisome uptick continues in the Northeast region. We see improvement in the other three. There was a large jump last week in the Midwest, so the modest pullback still isn’t great. But the South and West numbers are definitely encouraging. New York’s was as well, down to a new low of 27 deaths all week for the whole state.
Positive Tests by Region
| Percentages | Northeast | Midwest | South | West |
| 7/30 to 8/5 | 2.58% | 7.26% | 12.35% | 6.68% |
| 8/6 to 8/13 | 2.30% | 5.67% | 14.67% | 6.98% |
| 8/13 to 8/20 | 2.06% | 5.62% | 9.41% | 6.47% |
| 8/20 to 8/26 | 1.86% | 5.78% | 9.93% | 5.88% |
| 8/27 to 9/2 | 1.87% | 6.37% | 9.38% | 4.78% |
| 9/3 to 9/9 | 1.97% | 6.02% | 8.48% | 4.13% |
| 9/10 to 9/16 | 2.41% | 5.99% | 11.35% | 4.49% |
| 9/17 to 9/23 | 2.20% | 5.96% | 7.13% | 4.11% |
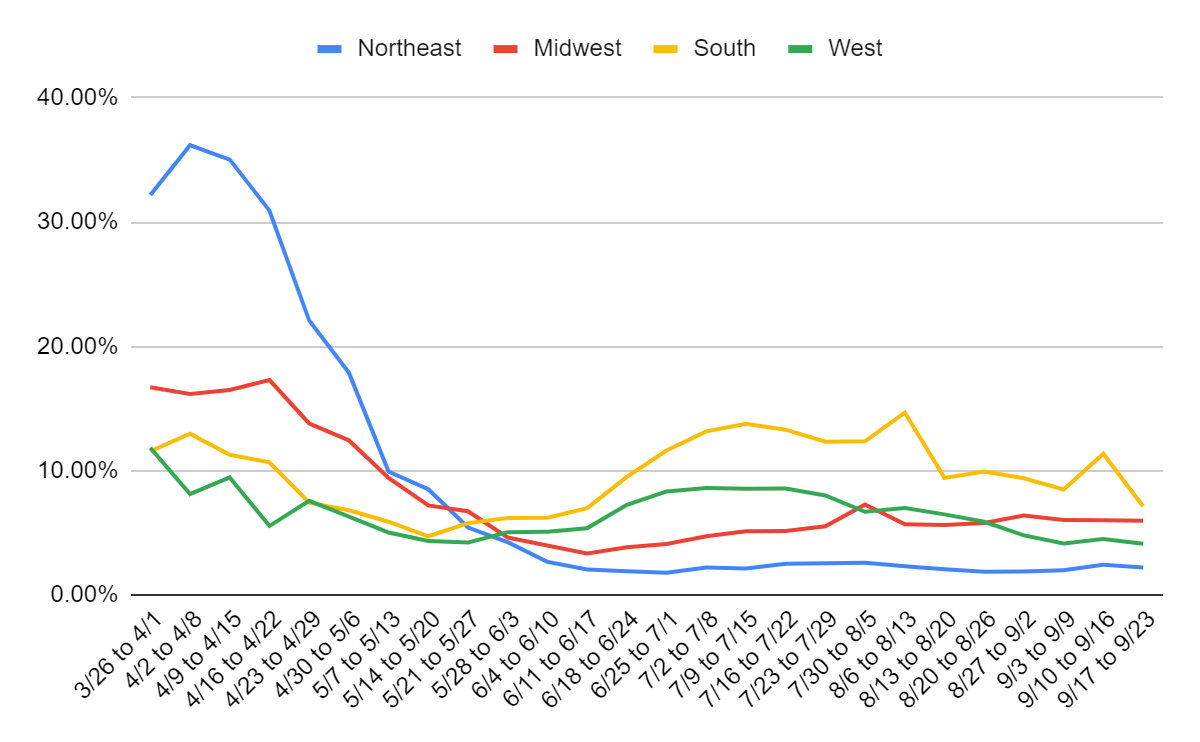
Last week looks very scary here. This week looks good. The South is now doing better than it has in some time as is the West, and the Northeast is pulling back from the dramatic rise last week. I suspect some amount of negative tests were held back last week for whatever reason, and got dumped into this week, so things should look smoother than they do.
Still this is a great relief. Last week looked like we might be about to ramp up once again, potentially quite rapidly. Now it seems much less likely that is going to happen. That assumes of course that we want less cases now rather than more cases – I actually think it’s reasonable at this point to want to get it over with, if it wouldn’t cause additional lockdowns, but I do think it would case additional lockdowns, so I’d prefer to avoid it.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| July 17-July 29 | 5,746,056 | 7.9% | 452,889 | 1.0% | 1.34% |
| July 30-Aug 5 | 5,107,739 | 7.8% | 484,245 | 1.0% | 1.46% |
| Aug 6-Aug 12 | 5,121,011 | 7.3% | 506,524 | 0.9% | 1.58% |
| Aug 13-Aug 19 | 5,293,536 | 6.2% | 548,421 | 0.8% | 1.68% |
| Aug 20-Aug 26 | 4,785,056 | 6.0% | 553,369 | 0.7% | 1.77% |
| Aug 27-Sep 2 | 5,042,113 | 5.5% | 611,721 | 0.8% | 1.85% |
| Sep 3-Sep 9 | 4,850,253 | 5.3% | 552,624 | 0.9% | 1.93% |
| Sep 10-Sep 16 | 4,632,005 | 5.8% | 559,463 | 0.9% | 2.01% |
| Sep 17-Sep 23 | 5,719,327 | 5.2% | 610,137 | 0.8% | 2.10% |
Welcome back, testing, to levels seen in mid-July. Hopefully this is the start of a trend or at least a new normal, rather than a blip. The positive rate is clearly an improvement as well, assuming the extra tests aren’t negative tests are new tests, rather than being dumped onto the system from previous weeks.
It is telling that this week we saw a bunch of headlines about the ‘rising number of cases’ when that is obviously not what this chart says at all. The previous week was a scary increase. This week’s headline numbers are obviously good news. Yet even now, in September, the whole ‘do less testing so it looks less bad’ strategy is the correct strategy if you want good media. And what we incentivize, we are likely to get. Hate the player if you wish, but first hate the game.
By the way, if you’re in New York City and need a rapid test, a friend reports this as a good source.
For Relief That Lasts
In a surprise to few who read this column, the newest potential solution to Covid-19 is essentially an attempt at regulatory arbitrage.
Nasal solution may stop spread of COVID-19, study finds.
It’s still early and the results were in a lab, so not that great a chance it works. But we’re all excited, because if it works the Very Serious People might be forced to let us use it.
Every now and then, ask what regulatory behaviors would look like if they wanted us all to lose our jobs, starve to death, get sick and die.
And be thankful they have not yet closed all their loopholes.
The Vaccine Protocols
They look good. The trials are way too small, of course. Why do 30,000 when you can do 300,000? It’s not like these vaccines are that dangerous. But given size limitations and the standards we live by, these seem… fine?
They don’t look remotely optimized, of course. The actual sensible thing would be to continuously check the results via computer and report if thresholds are ever crossed (and have higher thresholds to compensate for that). It’s also not clear to me what kind of logic is behind the thresholds involved here. The p-values necessary for a positive finding keep getting larger as the study continues. There’s no evidence of any attempt to do a Bayesian analysis. So what’s really going on here?
There’s some psychological story behind this design. I’m curious what it is, but I have at best small pieces of that puzzle.
In any case, how fast we get results will depend on the rate of infections in the trials. The better the vaccine, the slower we get the results, but only by a factor of 2-3 at most since there’s a control group, and results are expected this year. Each trial has at least 30,000 people, who they presumably are testing continuously. They need roughly 150 infections to finish, so a 1% infection rate in the control group would do it, or 0.5% from the combined group. How fast will we get there?
If you go by actual positive tests in the USA, that’s ten weeks to get 1% infected. Those who volunteer for a trial could be more or less at risk modulo the vaccine itself, and it’s not obvious to me which way that goes. Nothing we can do but wait.
The Correct Vaccine Protocols
Challenge trial! Actual first world government funded challenge trial!
Celebrate, good times, come on!
We need to do it bigger, faster, better. But something is so so much better than nothing.
CDC Accidentally Tells Truth, Profusely Apologizes
This column strongly believes in good incentives and in redemption. If the CDC or anyone else comes around way too late to the truth and/or the right strategy, we will applaud them for doing so sooner rather than later. The ‘what took you so long’ approach helps no one.
Unfortunately, that is not this story.
This week, the CDC came out with new guidelines that said the Covid-19 virus is airborne. You can be infected by breathing in air that contains the virus.
No. Shirt. Sherlock.
Let it sink in that now, in September, the CDC finally got around to admitting the most important single fact about Covid-19 – that the virus is airborne. That’s the primary mode of infection.
Then the WHO called, and asked what the CDC was doing saying the virus was airborne. Because the WHO has yet to admit this one. They are continuing to lie to all of us.
The CDC, being called out for accidentally speaking truth to the public, moved quickly to correct the situation. They declared that the new guidelines were only a draft, and rescinded them.
Without saying anything remotely like: Yes, obviously the Covid-19 virus is airborne. We’re a bureaucracy and we haven’t gotten the wording right yet, so those guidelines aren’t official yet, but
So the headlines are now that the CDC retracts guidelines saying Covid-19 is airborne.
This is like if Google Maps had people driving into a river, then changed to a new map that didn’t do that, but realized the new map misspelled the town’s name, so they restored the old version of the map until they could fix the problem. Which doesn’t seem realistic, so to fix that, let’s substitute Apple Maps.
What is the game, at this point? Why hold to this lie?
Because (if my explanations in previous columns and posts haven’t made this clear yet, if they have you can skip this) it’s the foundational lie behind the idea that there are ‘safe’ and ‘unsafe’ configurations and actions. That if you stay six feet away, and Sacrifice to the Gods with frequent ‘deep cleaning,’ you’ll be safe. So in order to protect arbitrary guidelines, to get people to latch onto simple heuristics that they think will cause the public to do what’s good for them, the science has to say that which does not correspond to physical reality. I can’t even say “to say that which is not” because that implies they know the difference. They certainly don’t much care.
So. Yeah. CDC Delenda Est.
That’s the shot. Now for the chaser.
CDC Announces They Have Antibody Results, Provides #Analysis
Here’s a news report on the latest announcement. I encourage reading it before reading my take on the new information.
The first thing to note is that the CDC director is directly conflating has not yet had the virus with susceptible, and also conflating tested positive on the serology test with has had the virus:
The head of the Centers for Disease Control told Congress on Wednesday that preliminary data from nationwide testing shows that over 90 percent of Americans have not contracted the Coronavirus, as top federal health officials continued to implore Americans to take precautions in order to slow the virus outbreak.
“More than 90 percent of the population remains susceptible,” Dr. Robert Redfield told a Senate hearing, saying serology tests have shown clear trends in the spread of the virus.
This makes three implicit claims which imply a fourth claim.
Claim 1: If and only if you have had Covid-19, your serology test will be positive. Modulo small false positive and false negative rates due to measurement error, which I agree are small enough we can mostly ignore both of them once we get to the 10% level.
Claim 2: If and only if you have a positive serology test, you are not susceptible to Covid-19. Again, modulo a false result that can mostly be ignored in both directions.
Claim 3: Before having Covid-19, everyone is susceptible to Covid-19.
Claim 4 (From Claim 1 + Claim 2): Having Covid-19 and recovering makes you permanently immune to Covid-19 reinfection. Or, at a minimum, makes you immune for a period of no less than seven months.
(There’s also the tidbit that >25% of infections are ages 18-25. That’s quite a narrow range, and one at very low risk.)
So first off, I’d like to congratulate Redfield for acknowledging that immunity is long lasting. It’s not like there was any real doubt, but scaring people with ‘who knows how long it lasts and it’s gonna end Real Soon Now’ remains a key part of the Very Serious People scare tactic policy portfolio.
Then I’d challenge the other two claims rather strongly.
There are some strong claims out there that lots of people are not susceptible to Covid-19, or are highly varying degrees of susceptible. Those claims may or may not be right. But the idea that no one is effectively immune without first gathering enough direct antibodies to test positive on the serology test seems like obvious nonsense. That’s not how the immune system works.
Second, we have lots of screaming that ‘immunity fades’ because antibody levels fall over time. So people who would have tested positive on serology, stop testing positive, yet these cases have near-zero reinfection rates. It seems obvious we both have some people who are immune without being infected and producing antibodies in the first place, because of cross-immunity or other lines of defense, and that we also have some people who no longer show antibodies but are still immune because of other lines of defense and the ability to remember and produce the antibodies again if needed.
The question is whether there are only a few such people, or there are lots of such people.
If we took the CDC’s data at face value, what would that mean? They say ‘Over 90%’ so that’s a claim that under 10% tested positive. How far under 10% should we assume? Given the incentives and other actions of the CDC, let’s assume this means something like 9%, versus a nationwide 2.1% rate for positive test results from PCR tests.
The peak of rates in the study was 24%, presumably for New York City but perhaps not. That’s higher than previous measured antibody results, but lower than plausible infection rates – my model has New York State at around 25%, and the city is far higher than the rest of the state. Our go-to outside machine learning plausible guess puts USA overall rate at 16% (which implies a measured death rate of roughly 0.4%), but has only 21% for New York State. That still is substantially higher than 24% being the highest observed local rate would imply. Note that the machine learning model has Arizona at 24.6%, substantially higher than New York, and many southern states in the 21% range.
On its own these are more data points, and they are useful parts of the puzzle. The way it is presented, however, strikes me as another attempt to have it both ways, and describe everyone as in danger as often as possible to try and get people to behave the way the CDC wants.
This week’s other interesting serology test news is this study from Japan: Dynamic Change of COVID-19 Seroprevalence among Asymptomatic Population in Tokyo during the Second Wave. Those numbers are rather boggling. I don’t know what to make of them and am curious what others think. To avoid anchoring too much, I won’t say more.
In Other Sort-Of News: Links That Tell The Same Old Story
Because we’ve decided that every test needs to be as effective as our best test, or we can’t use it, even though that is mind-bogglingly murderously dumb. I’d explain, but I’d only be repeating myself.
This keeps happening. There’s an activity that it seems plausible would have unacceptably high risk of Covid-19 infection. For example, you might want to play professional sports, or you might want to treat patients in a hospital. Safety protocols are implemented, including masks and frequent testing and hyper-awareness of the dangers.
In the case of airlines, lots of attention is also paid to air flow.
Then the tests come in, and despite more vigilance and testing, and therefore much higher probabilities of finding each case, the case rates end up lower than the general population. In this case, the positive rate for flight attendants is under 1%, whereas the confirmed positive test rate for the USA is above 2%.
The pattern is clear. Risky things are risky, but risky things done with a real dedication to safety, and a willingness to endure major costs to get that safety, are actually net safer than the background risk level.
Does this mean it is ‘safe to fly’?
No. It means that if one takes professional-level precautions, flying can be put into the ‘safe’ bucket. But that’s true of most things that aren’t about packing people into tight spaces so they can share an experience with each other.
SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels
Yet another correlational study about Vitamin D. The correlational verdict is so beyond in that, as the person who linked me to this put it, there really isn’t much point. Figured I’d throw it in, but it doesn’t change anything.
USPS Had Plan to Send Everyone Face Masks
Plan was rejected by the Trump Administration in order to ‘not cause panic.’ Also perhaps to avoid giving people the impression that the Postal Service was competent and important and could do other things like let people vote. Either way, I consider this a positive update. Our civilization did figure out a good plan to do something important. Yes, it didn’t happen because someone actively decided to stop it, but I’d rather be competent and up against malice than be incapable at all.
Our Antigens, Our Selves – Marginal REVOLUTION
Another story from Marginal Revolution about how the FDA puts insane restrictions on how people might gain information about themselves and their health, because if someone had information they might change their behavior based on that information, and information can sometimes be wrong or misinterpreted, so information should be regulated as a high-risk medical device.
I violently agree that all of that is bonkers – FDA is the original member and still captain of the Delenda Est Club. I only have one bone to pick, which is with the term ‘Unintended’ Consequences.
Unintended?
I say intended. One hundred percent intended. The intention was to prevent people from having access to the information they need to make decisions to protect their health. People dying is not an unintended consequence of that.
You stop systems from functioning, they stop working. You refuse to tell people when they’re sick or how to get better, and they die more often. This isn’t complicated or hard.
I wasn’t intending to get fat, I just wanted to eat lots of giant meals and delicious desserts every day and never exercise. Don’t look at me like that.
I mean, officer, I only intended him to stop moving so I could take his wallet. That’s why I shot him in the face. I didn’t intend to kill him.
There are frequently unintended consequences of regulation. They are usually but not always destructive. There are also frequently fully intended, and fully predictable, destructive consequences of regulation. When you regulate something and it gets more expensive, lower quality, less innovative, subject to an oligopoly or monopoly and increasingly nonsensical and maze-like, and those subject to the regulations capture the regulatory body and sculpt it to their own ends… You do not get to say these consequences are unintended.
You can say those consequences are worth it. You can say that the world with the regulations is better than the world without them, in spite of those consequences. You can’t call them unintended anymore.
See everyone next week. Now more than ever, I hope things stay quiet.
16 comments
Comments sorted by top scores.
comment by Rain · 2020-09-24T18:34:21.724Z · LW(p) · GW(p)
Thank you very much for posting these.
Replies from: Theodore Ehrenborg↑ comment by Theodore Ehrenborg · 2020-09-24T19:16:30.398Z · LW(p) · GW(p)
Seconded
comment by Dorikka · 2020-09-25T19:49:17.736Z · LW(p) · GW(p)
Thanks Zvi, these are super informative!
Use of povidone-iodine as mouthwash and nasal spray looks promising as prophylaxis (and potentially treatment, but lower confidence on that.) The study Zvi linked (https://jamanetwork.com/journals/jamaotolaryngology/fullarticle/2770785#ooi200049r25) appears to be the latest in discussions occurring in otolaryngology since April (https://www.google.com/search?q=povidone+iodine+nasal+spray&oq=pobidone&aqs=chrome.1.69i57j35i39l2j0l2.2542j0j4&client=ms-android-att-us&sourceid=chrome-mobile&ie=UTF-8). Other informative articles here (https://journals.sagepub.com/doi/full/10.1177/0145561320932318) and (https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3563092).
I plan to start using appropriately diluted povidone iodine solution as nasal spray and mouthwash when I'm in contact with (or proximity to) strangers. I'm pretty comfortable using Betadine 10% as the base for mouthwash (diluting it with water since the commercially sold mouthwash version is somewhat difficult to procure.)
I'd love any insights/thoughts on the correct product to use as the base for nasal spray (prior to mixing with saline), as the above protocol does not reference a particular product, and the additives in different povidone-iodine solutions seem to vary a fair amount.
Replies from: PeterMcCluskey↑ comment by PeterMcCluskey · 2020-09-26T02:30:35.203Z · LW(p) · GW(p)
I've got this Povidone Iodine Prep Solution USP, from a Chris Masterjohn recommendation. He suggested (back in May) diluting it 20x.
Replies from: Dorikka↑ comment by Dorikka · 2020-09-26T07:19:24.399Z · LW(p) · GW(p)
Thanks for the info! Two questions:
-
The linked article indicated that 10% solutions were widely available on Amazon, and links this one, but doesn't seem to give any indication why he picked that one in particular - just wanted to check if you might have seen this reasoning somewhere/if it exists.
-
I'm not familiar with Chris Masterjohn - his web page looks like he's a content creator trying to leverage his Nutritional Science PhD into being seen as knowledgeable about a wide variety of things - is this human known to say true and useful things?
comment by jimmy · 2020-09-24T19:43:12.034Z · LW(p) · GW(p)
Hypothetically, what would the right response be if you noticed that one of the main vaccine trials has really terrible blinding (e.g. participants are talking about how to tell whether you get the placebo in the waiting room)?
It seems like it would really mess up the data, probably resulting in the people who got the the vaccine taking extra risk and leading the study to understate the effectiveness. Ideally, "tell the researchers" would be the obvious right answer, but are there perverse incentives at play that make the best response something else?
If I didn’t have people thanking me every week for doing these, it would be difficult to keep going.
Thanks Zvi. The effort is definitely appreciated.
Replies from: Zvi, Owain_Evans, MichaelBishop↑ comment by Owain_Evans · 2020-09-25T09:33:39.894Z · LW(p) · GW(p)
I presume the blinding is imperfect because some of the vaccines cause mild reactions that the placebo wouldn't. I doubt it's a big problem. The people doing the trial are selected for being more conscientious than the average person. (For one of the two trials, the rate of Covid seropositivity was only ~1% for people starting the trial, which is lower than the general US population). They will not want to risk their household members getting Covid, and they will have been warned that that the vaccines are unlikely to work perfectly.
↑ comment by Mike Bishop (MichaelBishop) · 2020-09-28T13:42:35.193Z · LW(p) · GW(p)
Researchers should 1) survey participants regarding their possible exposure risks, and 2) ask them whether they think they got the placebo, and with what degree of confidence. Adjusting for these should reduce the problem.
comment by zby · 2020-09-24T18:42:26.679Z · LW(p) · GW(p)
The interesting tidbit is WHO calling CDC and having their statements retracted. How come? What authority has WHO over CDC? Why it needs to be everywhere the same? https://www.overcomingbias.com/2020/09/the-world-forager-elite.html
Didn't Trump withdrew US from WHO?
comment by Owain_Evans · 2020-09-24T17:40:28.601Z · LW(p) · GW(p)
Is there a scientific paper on the testing of flight staff? The airline industry is in dire straits and so it's not surprising they can produce a positive statistic on the (alleged) safety of flying.
comment by PeterMcCluskey · 2020-09-28T03:37:30.514Z · LW(p) · GW(p)
The Japanese study is pretty weird.
Here are some ideas I brainstormed fairly quickly:
I see no signs of researcher misconduct, but I don't see enough evidence to be very confident that their evidence is real.
Could people in Japan be much healthier to start with than most of the countries that have an IFR > 0.1%?
- what are Japanese vitamin D levels?
- I suspect they have high vitamin K2 levels (from natto, kimchi, etc.). What does this do?
- less obesity?
- different genes (blood type? fewer APOE4 alleles?)
Could transmission there involve a much lower initial viral load?
Could they do an unusually good job of preventing transmission to vulnerable people, while enabling plenty of transmission between others?
The only research I found time to do was to check the vitamin D content of fish. I was mildly surprised to find that it's high enough to make vitamin D deficiency fairly rare in a culture that expects virtually everyone to eat fish.
I'll give a 25% chance that vitamin D explains more than half of this puzzle. Most of the other ideas are quite unlikely to explain more than 5% each.
Replies from: Bucky↑ comment by Bucky · 2020-09-28T16:10:01.023Z · LW(p) · GW(p)
I suspect that those results don't generalise to the whole population.
Japan's testing shows 25,000 cases in Tokyo.
If that study's seropositivity rate generalises to the whole of Tokyo then there have been ~4,300,000 actual cases.
Japan's positivity rate on testing during the second peak got up to 6% so it is unlikely they are missing that many cases.
The numbers are so far apart that I wouldn't really believe that the seropositivity rate generalises at all.
(Note that Tokyo has 400 confirmed deaths and 25,000 cases giving CFR = 1.6%. Assuming some missed cases this puts the IFR in the normal range.)
Looking at it in a bit more detail the seroprevalence increased before Tokyo started seeing increases in positive tests so I really don't think these numbers will pan out in the long run.
EDIT: actually 25k is Tokyo prefecture and 4.3M refers to Tokyo city - Tokyo prefecture at 46.8% would be 6.5M.
comment by Owain_Evans · 2020-09-24T17:45:54.387Z · LW(p) · GW(p)
Re: Why not do 300k instead of 30k for vaccine trials? Clearly bigger trials would be better -- especially as the current trials aren't that representative of the general population or the most at-risk groups. But presumably the logistical cost of 10x more patients is significant. You have to be testing all these people for COVID and following up on any possible adverse reactions. I think lack the lack of challenge trials is the biggest problem. (Note that AFAICT, UK trial is likely to happen but not 100% confirmed and it only starts in January.)