Covid 9/17: Done Biden His Time
post by Zvi · 2021-09-17T12:00:01.580Z · LW · GW · 14 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Vaccinations Vaccine Effectiveness Vaccine Mandates NPIs Including Mask and Testing Mandates Think of the Children Ivermectin In Other News Not Covid None 14 comments
No more mister nice guy. The dude will not a-Biden. All this vaccine hesitancy is a bunch of malarkey. If you’re not vaccinated, the President is mad as hell and he’s not going to take it anymore.
The question then becomes, what is he gonna do about it, under what authority, and what will happen when he does it?
There’s also the question of booster shots. They clearly work. The CDC is doing what it can to prevent or stall any expansion of them anyway, and we’ll see if the FDA manages to finish that job.
Today the FDA will be debating booster shots, with such logic as ‘if vaccines still provide protection then we don’t need boosters’ and arguments over there not being 16-17 year olds in test samples because 18 is a magic number, and what the difference is between 50-59 and 60+ age bands, and arguments over exact dosages that might cause ‘confusion’ or ‘waste’ if they’re too low, as opposed to looking to see whether boosters work. I’d go into more detail here but I basically can’t even at this point. Even the pro-booster case is relying on the Israeli data which wouldn’t exist if the FDA had any say in the matter (and which has all the flaws of all the other Israeli data, probably, but no one ever seems to much care). The FDA is looking for any excuse to screw this up, partly in order to punish Biden for trying to do things because they would help people instead of ‘following the science,’ but also partly because they’d do that anyway, they hate giving people legal access to medicine. It’s both their one job and their least favorite thing.
If they pull it off, a lot of people are going to be checking a box claiming to be immunocompromised. Which is mostly fine with the FDA, so what if everyone is forced to be dishonest all the time in order to get medicine, that’s good actually since it means nothing that goes wrong is the FDA’s fault. Someone else will get blamed and sued.
[Note: This week’s post is on Friday due to Yom Kippur. Predictions made based on Thursday’s data.]
Executive Summary
- Vaccine mandates for everyone.
- Acts of congress for no one.
- Vaccine mandates for some, somewhat dishonestly acquired booster shots for many of the same people.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 940k cases (+0%) and 10,800 deaths (+5%)
Results: 950k cases (+1%) and 13,111 deaths (+27%).
Prediction for next week: 900k cases (-5%) and 13,000 deaths (-1%).
There were a lot of extra deaths with many states seeing very large increases. If cases had gone up a lot as well I would conclude that I was underestimating the holiday effect. That’s still possible, since perhaps the true case level could be declining faster than I expected to compensate for it, but it seems unlikely. I looked for a large dump of prior cases, but there’s nothing big enough to account for the bulk of this. I’m going to moderately increase my estimate of the lag between cases and deaths, and assume a bunch of this increase is likely a data artifact of some kind unless it gets sustained. That makes next week’s death number hard to predict.
The case number has less uncertainty. If cases do go up a lot this week, I’ll suspect that it’s due to schools engaging in absurd amounts of testing resulting in us finding a lot of extra asymptomatic cases. They’re testing weekly in my son’s preschool so the chance of officially counting my son’s case if he gets one went from very low to reasonably high, and false positive rates aren’t zero. Many others could be in a similar spot.
Deaths
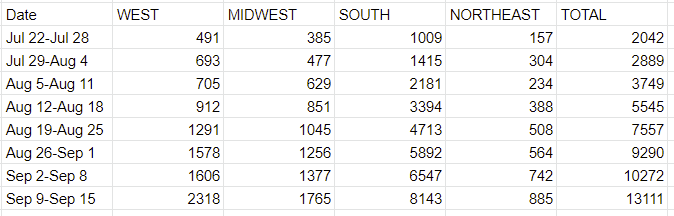
That’s a large jump across the board, which I didn’t expect given the lagged case counts, so as usual the question is to what extent this is a data artifact. I checked for anomalies and didn’t find any, so the error would have to be something nationwide. There was a return from a holiday, although the effect seems bigger than that could explain alone. If this rise is real, we need to worry that this represents the hospitals in many places becoming overloaded.
Cases
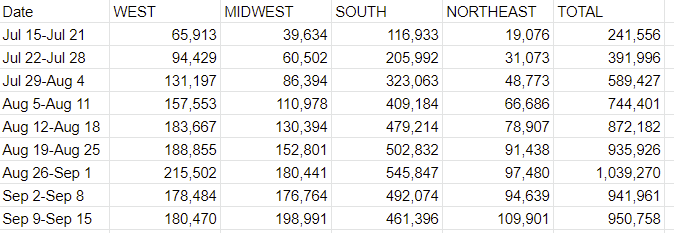
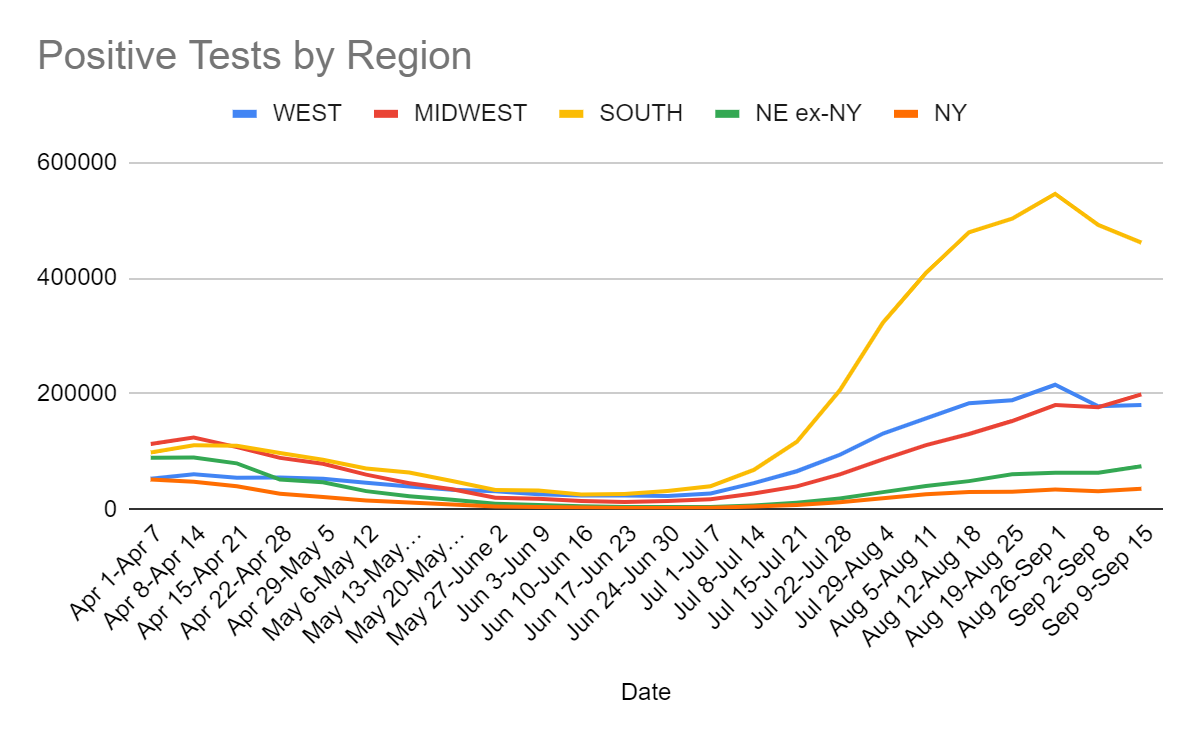
We seem to have clearly peaked in the South. It’s less clear we are at or beyond peak in other regions. We’re definitely at least close unless something unexpected happens.
Vaccinations
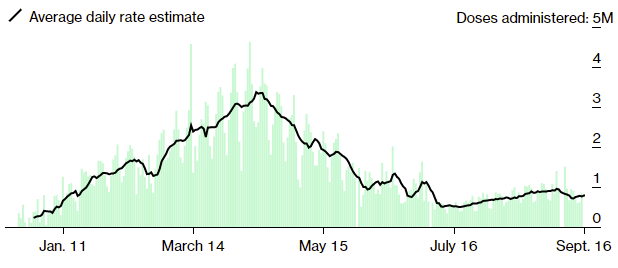
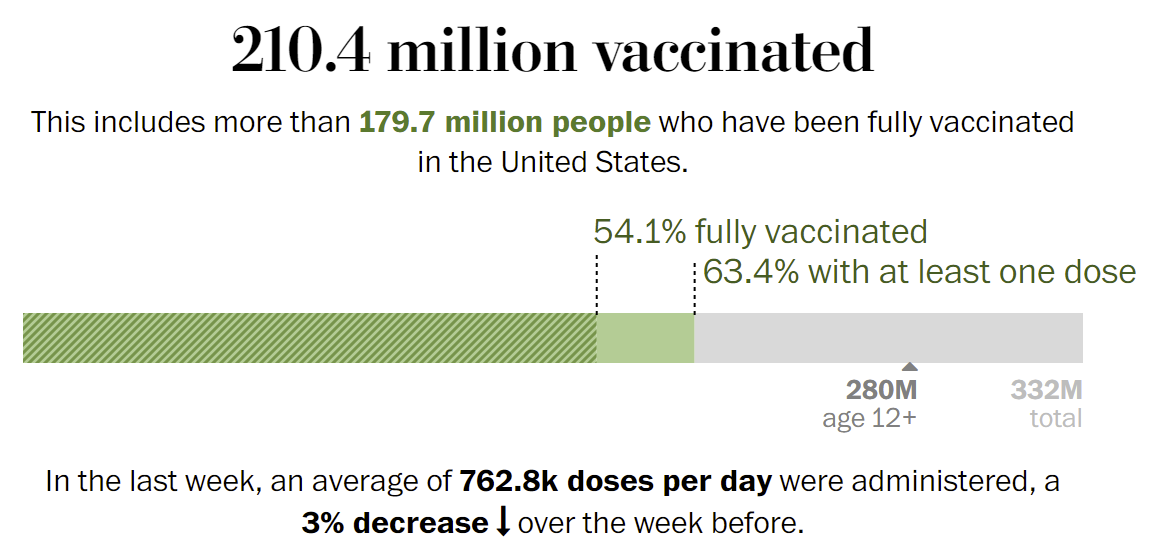
Biden’s push has not yet resulted in a surge of vaccinations. We don’t know the counterfactual, so we don’t know to what extent various mandates and potential future mandates are the only thing stopping vaccinations from slowing further. There’s also the impact of Delta, as the case and death rates are likely a lot of what’s motivating people to finally get vaccinated (as well as motivating them to impose new mandates).
If there was a graph that charted vaccinations over time as a percentage of the eligible unvaccinated population, that would look interestingly different. If you looked at the percentage of the population that isn’t saying they’ll never get the vaccine no matter what, it would look more different still.
What we can definitively conclude is that the skeptics were correct regarding full FDA approval. It was not (almost) anyone’s true rejection. The impact is going to be in enabling mandates, especially the big push this week by Biden, which would not have been practical without full approval.
Vaccine Effectiveness
Randall Monroe is on the case.
Did you know that the CDC is so slow that the FDA thinks it’s a problem? That they regularly slow walk giving out their data? That what they call ‘political pressure’ is someone pointing out that being slow means people die so maybe time is of the essence or something? Read the whole thing.
Well, finally, what do you know, the CDC says vaccines still work (paper).
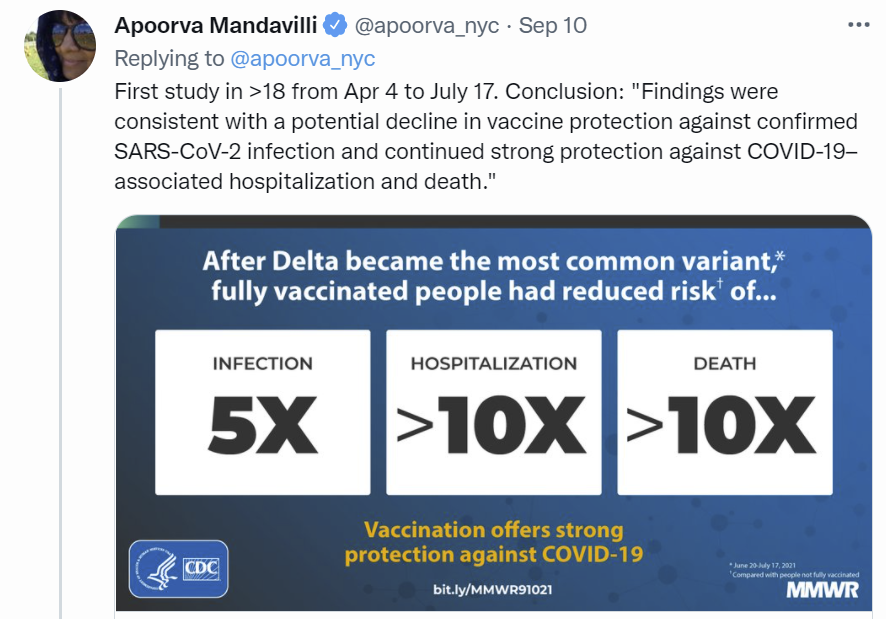
This led to a certain amount of gloating, as in maybe they should have waited for this ‘study’ ‘data’ to come in before the whole scare over Provincetown and worrying vaccines might not still work. My initial reaction was that this was bad news, since my model previously thought that vaccines are even better than that.
Instead, I rapidly discovered this seems to be actual zero news of any kind. Here’s what passes for their new findings:
During April 4–June 19, fully vaccinated persons accounted for 5% of cases, 7% of hospitalizations, and 8% of deaths overall; these percentages were higher during June 20–July 17 (18%, 14%, and 16%, respectively). Using the reported 37% vaccination coverage for the 13 jurisdictions during April 4–June 19 and an assumption of 90% VE, vaccinated persons would have been expected to account for 6% of cases (close to the 5% observed). With 53% coverage reported during June 20–July 17, vaccinated persons were expected to account for 10% of cases at a constant VE of 90%; the observed 18% would have been expected at a lower VE of 80%.
Within each age group, the percentage of vaccinated persons among cases, hospitalizations, and deaths increased with increasing vaccination coverage (Figure 1). As the prevalence of SARS-CoV-2 Delta variant surpassed 50%, the percentage of vaccinated persons among cases in each age group increased at rates corresponding to benchmarks for lower VE (i.e., from approximately 90% to <80%). Increases in the percentages of vaccinated persons aged ≥65 years among COVID-19–associated hospitalizations and deaths also appeared higher than expected. During June 20–July 17, age-standardized rates of cases, hospitalizations, and deaths among persons not fully vaccinated increased weekly; among fully vaccinated persons, case rates increased, but rates of hospitalizations and deaths remained largely unchanged (Figure 2).
So they multiplied the same basic data we’ve been looking at every week, that everyone essentially already knew, and somehow this became a headline. The 80% seems very much like a round number that was vaguely close to making the basic arithmetic work out if you literally adjusted for nothing whatsoever in either direction. Good work getting published, I guess?
Turns out that was only the first of three studies. Here’s the second one. It’s not more enlightening, and doesn’t show any signs of controlling for anything or of, once again, being anything more than ‘do what we’ve already done, but lower the sample size to cover a smaller geographical area.’ It finds Moderna more effective than Pfizer once again, which I continue to assume is because Moderna uses larger doses, and always will because that which is submitted to the FDA cannot be altered. Third study seems like it’s the second study again, except now with veterans, so the sample is non-representative.
Here’s some data from the UK (hat tip: Ben Hoffman), with all the caveats that this is raw data rather than being corrected for anything. Also some good graphs on various variants, as well.
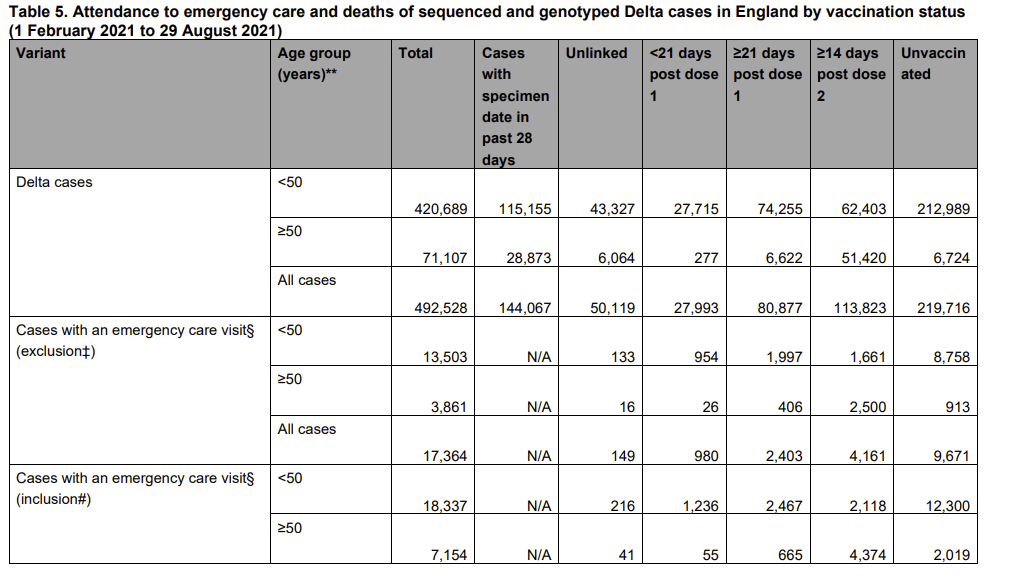
About 90% of all people vaccinated in the United Kingdom have had two doses. Yet those with only one dose account for about 50% of all Delta cases. That implies the effectiveness of the second dose over and above the first dose in terms of observed cases is something like 90%, although again lots of corrections in various directions are missing.
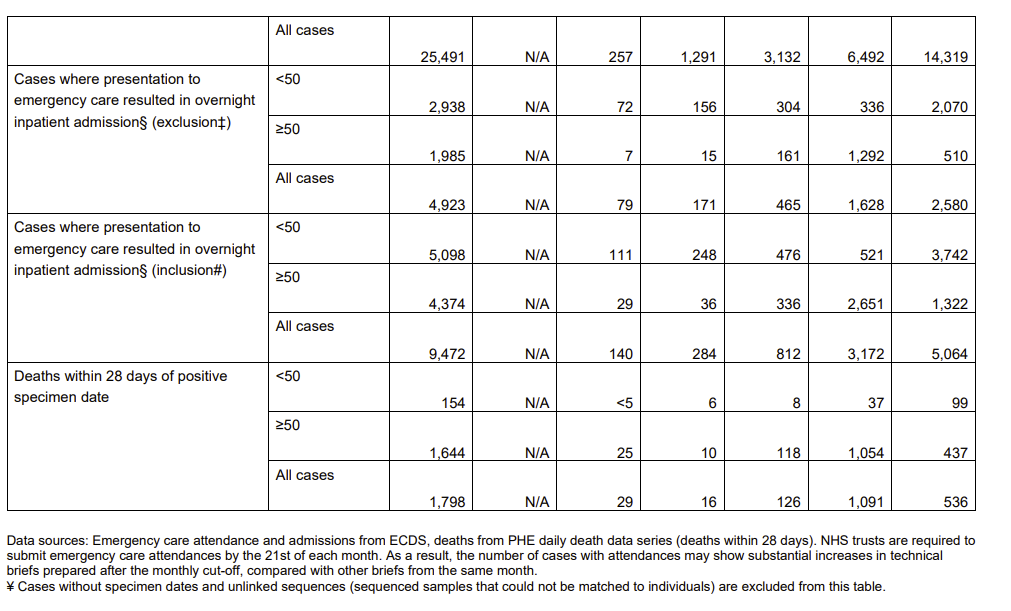
The emergency visits are less lopsided, but that’s clearly due to age, with less of the elderly stopping after one dose. If you look at the Under 50 group, you see similar ratios of emergency care visits to the ratio of cases.
When we look at deaths, we see a strange shortage of deaths in the partially vaccinated population. Even the unvaccinated population seems to do better within the age bounds. I thought about this for a bit, and concluded that this is likely to mostly be age, as dividing into two groups is insufficient, and in the Over 50 group the death numbers go the other way. We have tons of data saying that vaccines offer better protection against death than against infection, so the extra deaths are a proxy for how much older the vaccinated population was than the other two groups.
We also have this other data from the UK, from a preprint. Here’s their numbers against symptomatic disease.
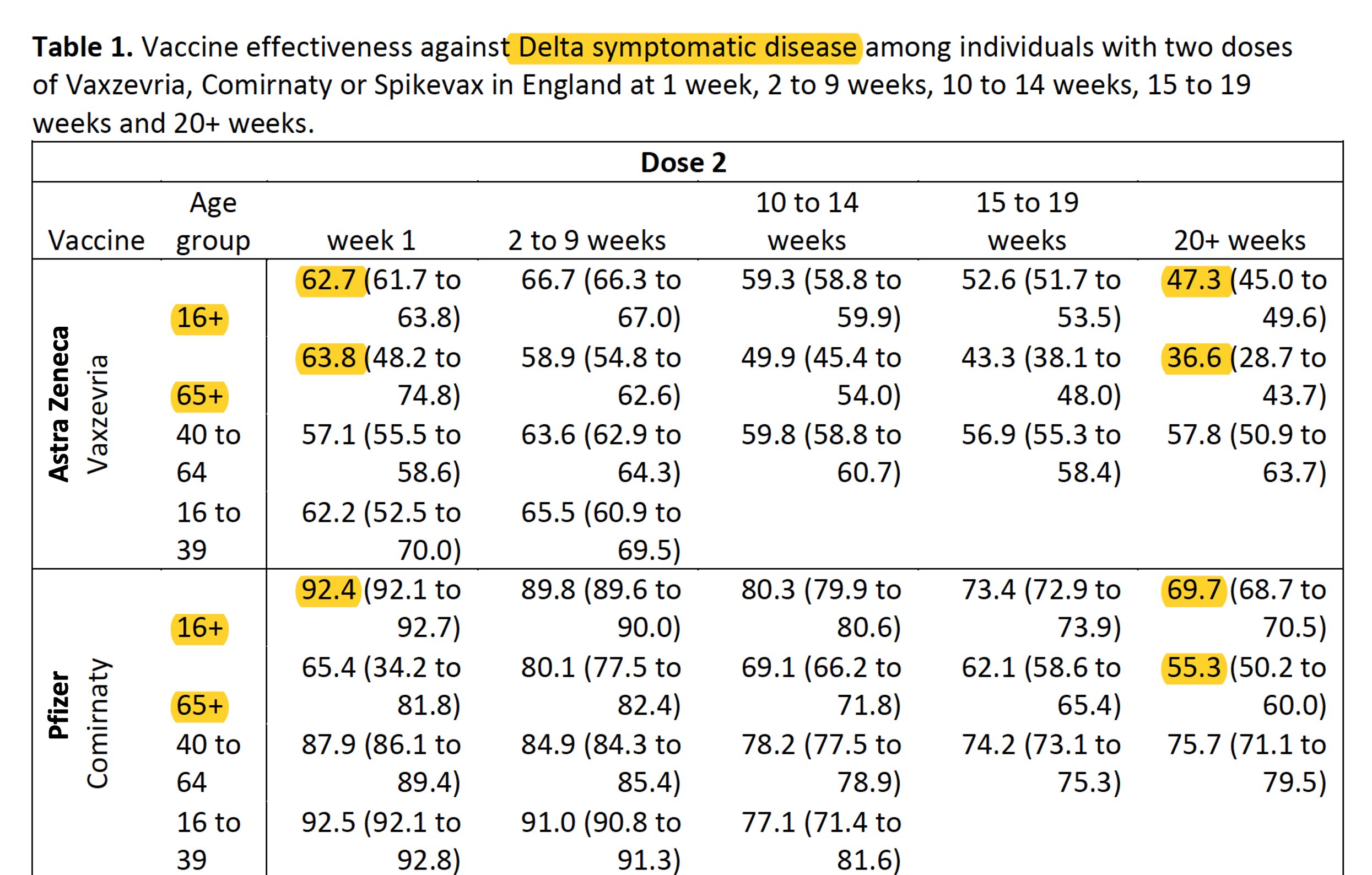
There’s a bunch of comparisons between groups here where the confidence intervals don’t make sense. For example, note that for AstraZeneca the 40 to 64 age group effectiveness at 20+ weeks has a confidence interval that is higher than and doesn’t intersect with the interval for the 16+ age group, where the opposite (and more plausible scenario) is true during weeks one through nine. We strangely see a similar pattern for Pfizer, once again with non-overlapping intervals.
I suppose it’s possible that this is a real effect, and older immune systems get more advantage out of the vaccines longer term while younger people have a stronger short term response, but sufficiently older people are worse on all fronts, but mostly I don’t buy this story. And especially when you combine this with the claim that longer-interval dosing regimens are more effective, this is not giving much room for vaccines in the United States to be that effective at this point. Then once again, you have to explain the basic data.
Here’s their numbers against hospitalization.
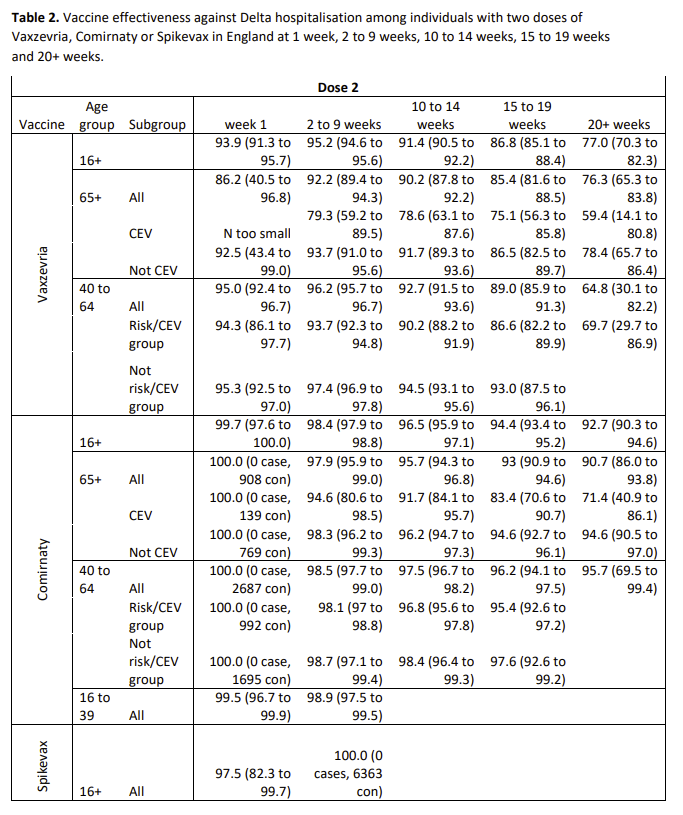
CEV means clinically extremely vulnerable. So this is saying that the worse off you are, the less vaccines can help you.
At least one study has found that the vast majority of those in the UK have antibodies. My best guess as to what’s going on here is pretty simple. Over time, more and more of the unvaccinated population got Covid-19, and became protected. Thus, the measured protection offered by vaccination went down. That and selection effects.
You should totally worry that I’m looking to dismiss such findings of waning vaccine effectiveness, rather than fully going where the evidence takes me. You should also worry that having found reasons why the first few such alarm bells were wrong and dumb, I’m going in assuming the new ones are too. I’m doing my best not to do any of that, but I may not have fully succeeded.
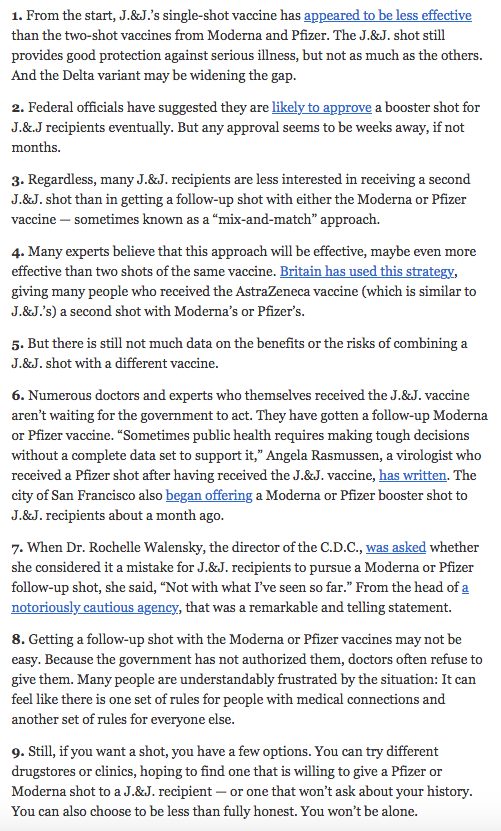
Booster shots improve vaccine effectiveness, especially if you have J&J and then get a shot of an mRNA vaccine. So The New York Times is now pointing out not only that this is a good idea, but that all you have to do to get your shot is to lie. Interesting.
Vaccine Mandates
It’s the big one this week. Biden is done playing, and it’s time to pull out the big guns.
What can he actually do though? In theory we have a constitution and a republic, and the President has limited authority, and Biden is at least firmly committed to maintaining the illusion of the illusion of limited Presidential authority – e.g. when his lawyers all said his eviction moratorium was unconstitutional, he kept calling until he at least found one lawyer somewhere willing to say it might be constitutional, and when the court does throw it out, he’ll at least try again in a slightly different fashion once again backed by a legal opinion. Sadly, it’s an upgrade.
And of course, there’s a strong correlation between not wanting to get vaccinated and muttering various things of variable accuracy about ‘the constitution’ so it’s not surprising that I learned about Biden’s new mandates through a post like this:
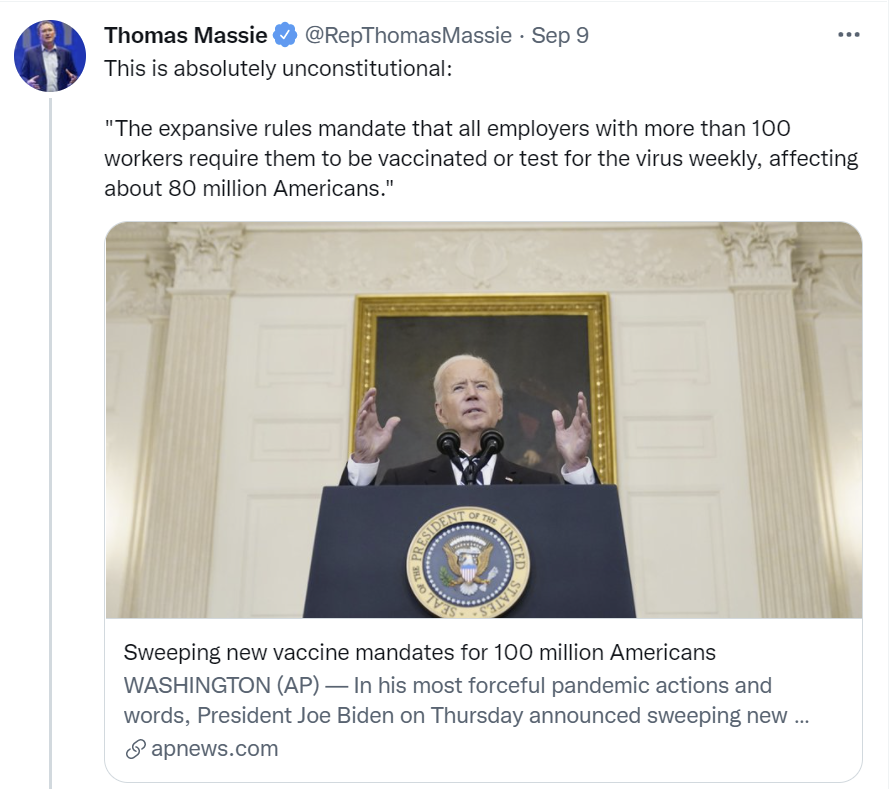
Here’s a summary of the full six point plan.
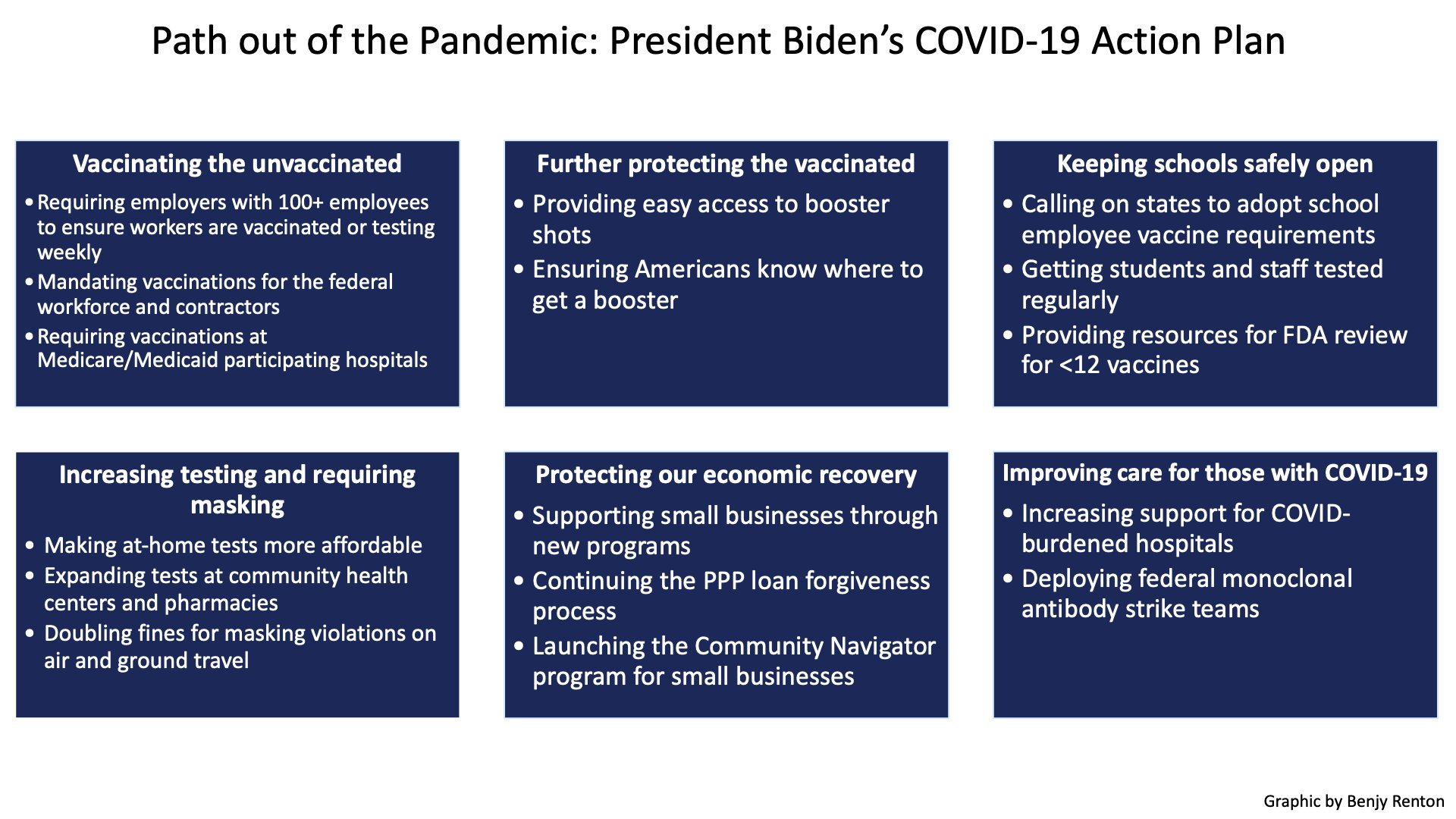
My subcategories are slightly different, but similar.
Some of this is basic, ‘and you’re doing this now? What changed and why didn’t this happen on January 20th?’ stuff like making at-home tests more affordable, and expanding tests at community health centers and pharmacies, increasing support for hospitals and deploying monoclonal antibody ‘strike teams.’ Also ‘providing resources for FDA review’ for the vaccines does seem like a good second-best idea. It’s a little strange that we finally worked all that stuff out in the same week, almost like it was held back, but hey. Five almost purely positive bullet points here.
We have the ‘doubling fines for masking violations’ line which is the standard ‘we’re super duper mad now so to show how bad we are we’ll increase fines’ thing. I find it tiresome but it doesn’t matter.
We have the economic section, which isn’t necessary, the economy is doing fine, but sounds like it’s not incinerating enough money to worry about relative to the other money incinerations we’re doing (while noting that if we were literally incinerating money that would be far better, cause then you can print more, it doesn’t actually cost much.)
Next up we have the booster shots, under ‘further protecting the vaccinated.’ I’m happy to see Biden going ahead with this and ignoring the FDA’s foot dragging. I would have been happier if I’d seen an explicit ‘including people who got Moderna or J&J’ here, especially J&J. Offering boosters to those who got J&J (if they want them) is the next ‘if you cared at all you would do this’ task.
We have the demand that students at schools be regularly tested (along with the staff) despite the staff being vaccinated as per the previous bullet point and the children being children. I continue to be confused how many people see such demands as reasonable but I’ve accepted that they do and it no longer surprises me.
Finally we have the actual mandates, for any company with 100+ employees (with a testing option), for all federal workforce and contractors (except the USPS, whose employees are so empowered they are sometimes easier to convict of federal crimes rather than to fire), for any Medicare or Medicaid participating hospital (the most explicit of all I-needed-a-reason qualification out of several), and for all school employees (which he admits he can’t do but is encouraging the states to do).
It’s clear that Biden wanted to do, which was to impose a full vaccine mandate on all Americans, with or without an intentionally overburdensome testing alternative. If he felt able to issue a full mandate here, I presume he would have.
Italy is doing something very close to full mandatory vaccination.. The article in question predicts a huge wave of opposition as a result. I don’t.
Here Biden is doing a strange mix of both. He’s exercising his authority in a way that attempts to look as broad and strong as possible, but which is technically forced to hide behind OSHA and end up as a convoluted mess that doesn’t hit all the places it would like to. The strangest part of the new rules is that they didn’t include requirements for interstate travel, which he has clearer authority to issue than the rules he did issue, and I’m expecting those to probably follow unless conditions improve quickly. If we are going to go this far (and presumably then keep going if conditions don’t improve), I do think it would be better to be clear on what we’re doing, and outright mandate the vaccine, and be done with it. Mason has similar thoughts.
The federal employee mandate seems fine and good. As I’ve said before, employers should get to impose such mandates, so this seems like a very reasonable use of authority. I’m glad this one happened.
The requirement on hospitals also seems like a good place to impose a mandate. If you work at a hospital, yes, you absolutely need to be vaccinated. You’re around sick people a lot, who aren’t there by choice, and your entire job is to help those sick people get well and not die. If you refuse vaccination, there’s multiple good reasons you shouldn’t keep working at that hospital. Alas, many nurses in particular are refusing the vaccine, they’re willing to protest and be loud, and there’s a shortage of nurses, so it’s hard/expensive for a given hospital to do the correct thing. Imposing the requirement from above lets the hospital point out it’s not their decision, and the nurses can’t threaten to go to a different hospital.
I do despise the mechanism of authority here, which is where the fact that the Federal government has already stepped up and royally messed up the health care system by hijacking its payments structure is then used to hold any and all participants hostage to the whims of the Feds. Also, the idea that such moves don’t fit the definition of ‘coercive,’ as the court rather ludicrously ruled regarding Medicare funding, defies common sense. It’s coercion, it’s an end run, it’s a mockery and all that, and this should be noted whenever it is invoked as such, but those are the rules in practice.
But is the mandate on employers here constitutional? It certainly isn’t obviously constitutional, and the tie to OSHA and large employers is a clear indication that this wouldn’t be constitutional without OSHA.
When first asked about the mandate soon after this, my reply was that I noticed I was confused how it was constitutional.
David French breaks it down for us. I’m not taking his word for it, since there’s (as one would expect) broad disagreement, but this seems broadly right to me as a matter of law.



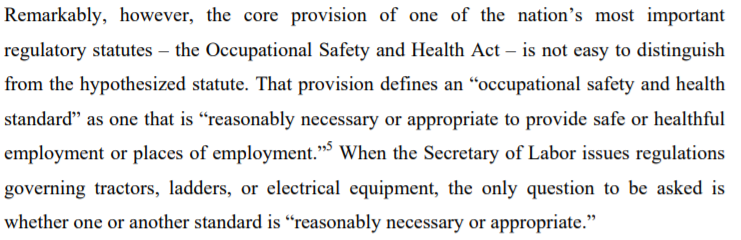


This post in Reason by a legal expert lays out another perspective, gets into the Exact Words this is likely to come down to, and is also not sure what the outcome will be. It makes a convincing (to me) case that allowing this move would likely represent a de facto large expansion of OSHA’s powers, and hence of effective presidential power, to impose arbitrary rules because they feel like it. I saw a warning asking people not to challenge the mandate for exactly this reason, as it may force the court to set a bad precedent it would prefer to avoid.
Worth noting that OSHA definitely has a blood pathogens policy already, which some people think makes this clearer cut than all that. Others disagree.
This is my current view of the situation.
- Vaccine mandates are legal if done under act of Congress.
- But that’s if Congress passed a law, which they didn’t, and won’t, because good luck with that.
- Luckily for Biden, a long time ago, Congress kind of told OSHA ‘do whatever you want in the name of safety to companies with 100 workers.’
- Using the commerce clause like this is pretty much bullshit.
- But, says SCOTUS, mostly legal.
- Congress delegating this way is terrible.
- But, says SCOTUS, mostly legal.
- In practice, SCOTUS will probably (but not definitely, I asked Polymarket to get us some real odds!) uphold this mandate.
- Which, again, is pretty much bullshit.
- But their call.
Whether or not it is upheld, the fig leaf of a fig leaf has been upheld and reinforced. One can even say the fig leaf here is genuine, which is even better. I do believe that Biden thinks this is constitutional, that he made compromises to make that true, and that this combination of beliefs is reasonable.
Meanwhile, employers will put this into practice before there is even a formal rule let alone enforcement or a court challenge, and employees will have to deal with that reality.
Private employers get to benefit from the same dynamics that benefit the hospitals. If two thirds of jobs have to mandate vaccination, including you, the employees can’t reasonably blame you and have far fewer prospects and places to go. Many of them will no doubt blame you anyway, and there’s no shortage of bad legal takes, but it will help. It will also help with worries about protests and boycotts.
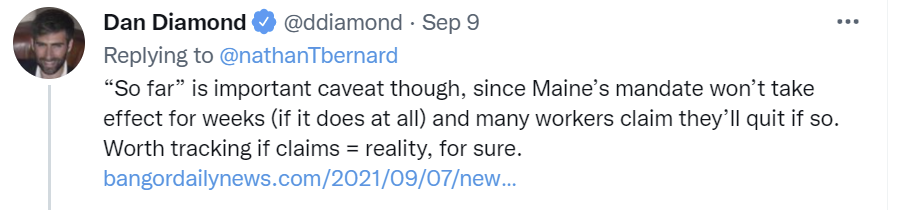
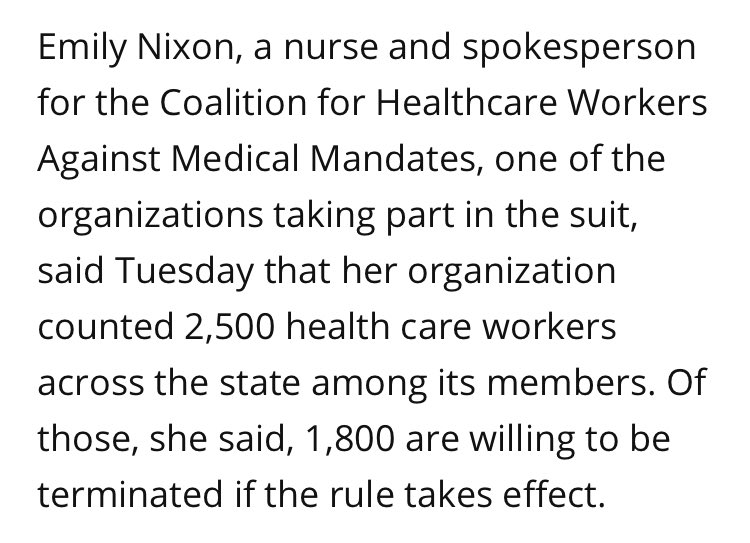
Surveys are saying that if you told the unvaccinated they had to either get vaccinated or they were fired, that most of them would choose to be fired.
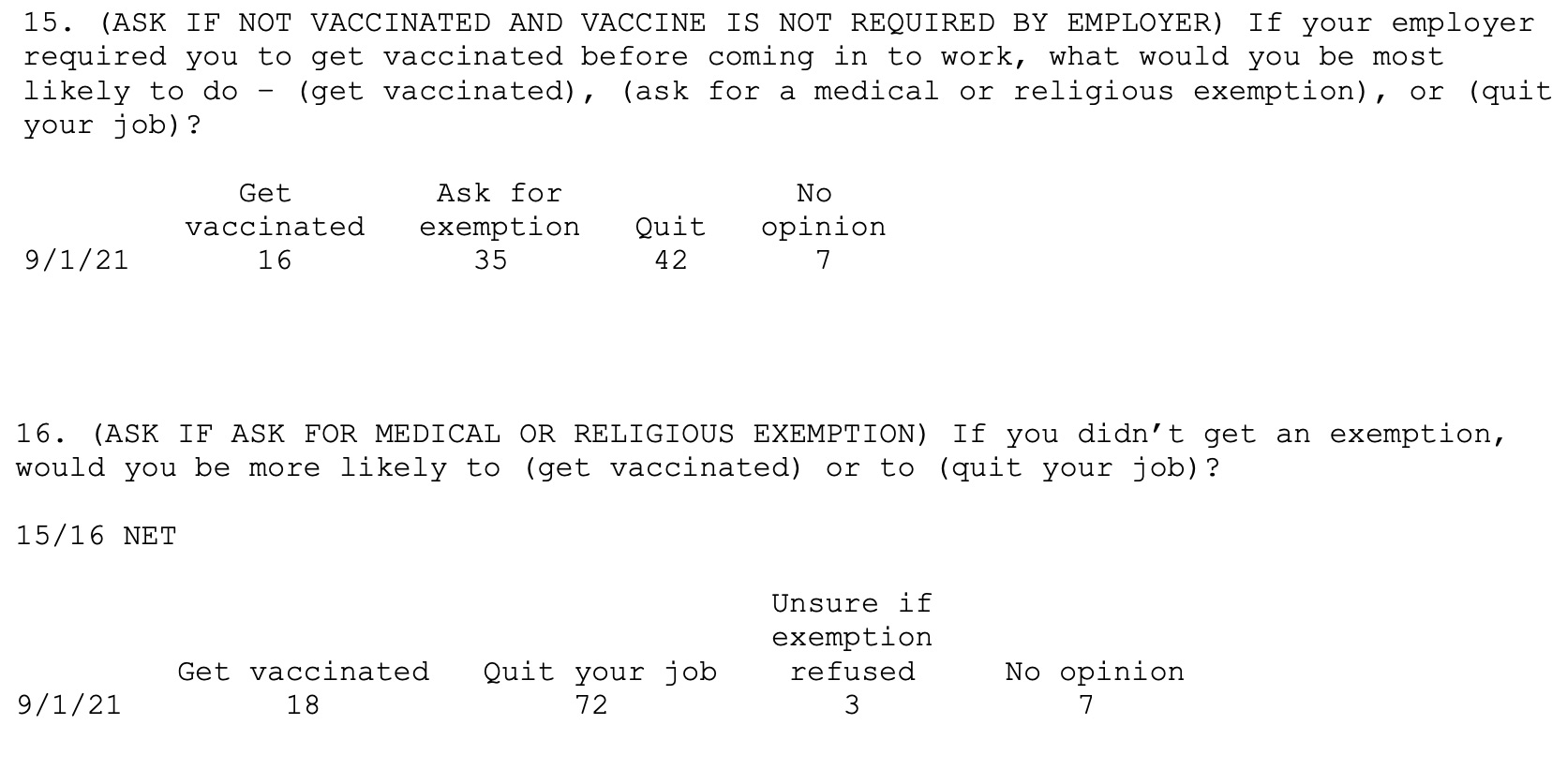
I flat out do not believe these people. At all. Zeynep explains, but with less willingness to endorse as strong an effect size as I have.
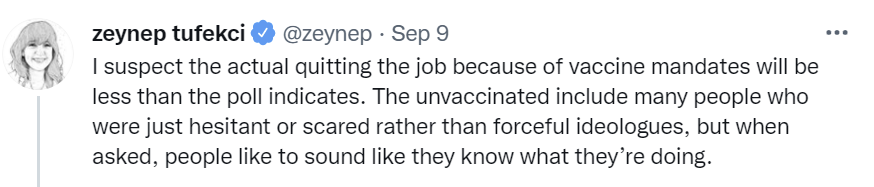
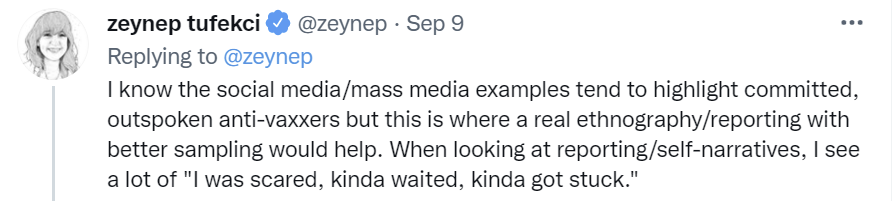
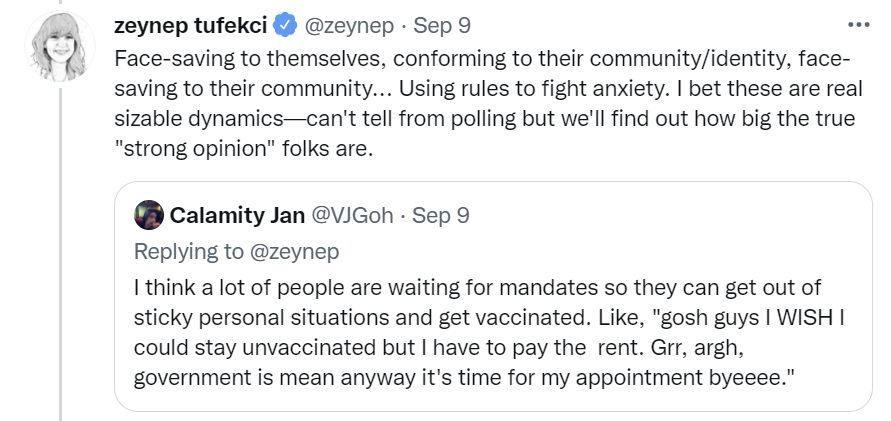
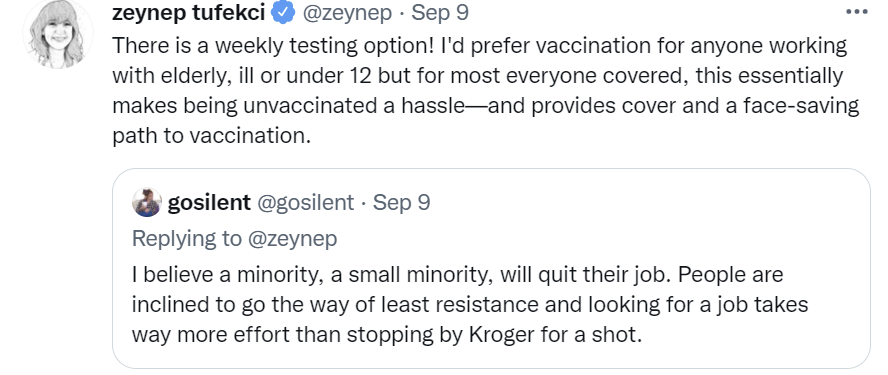
The testing option is annoying, but how many people would actually even quit their job over the weekly test if there was no vaccination option? Are anything remotely like two thirds or more of those who are currently on the hill of not being vaccinated prepared to die on it? I’d be shocked if one in ten pulls that trigger. Especially because we’ve already run this experiment a few times, to varying degrees.
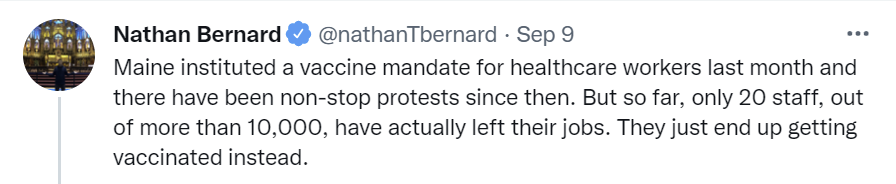
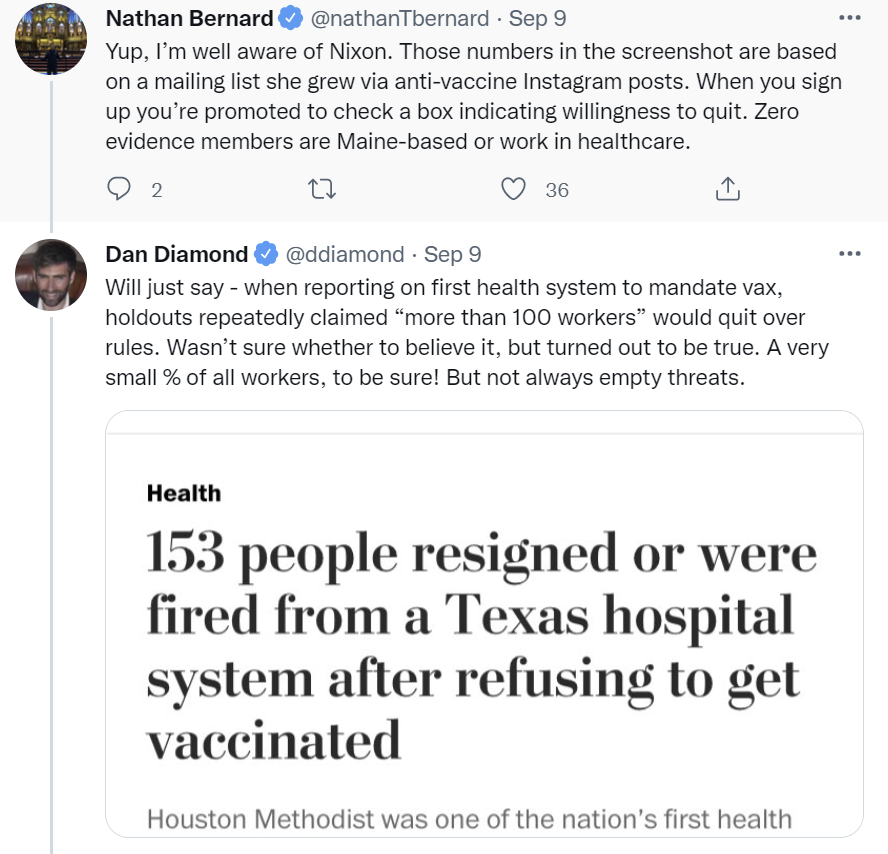

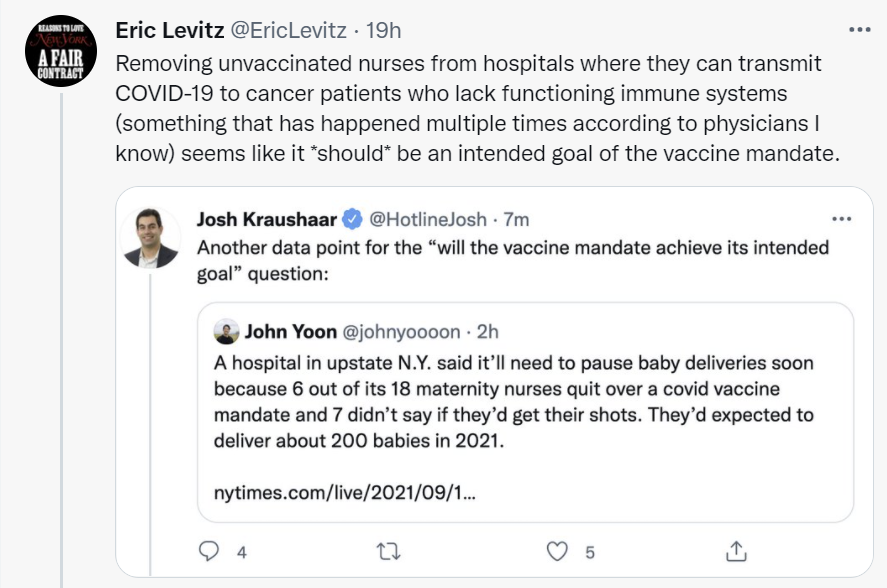
(We also have the hospital in New York that had to stop delivering babies noted above, but this seems like a Not Necessarily the News case, in the sense that we have the one example of this happening that’s Big News, rural hospitals likely don’t have much short term slack here, and we haven’t heard of other examples of similar situations.)
So under 1% of employees, or about 2% of unvaccinated employees, ended up quitting over this, and that was with other places to go. That sounds right to me.
That doesn’t mean this isn’t potentially a big deal.
Let’s say that 0.5% of all workers covered by the mandate quit. Biden’s mandate covers (very roughly) 100 million workers, so that’s still five hundred thousand people who would lose their jobs. That’s a lot, and it’s potentially a big deal. If you’re willing to hire unvaccinated workers, and can keep your work force small enough to allow that, you suddenly will have a much easier time finding otherwise good help. For those covered by the mandate the opposite will happen, there will be lots of jobs to fill and less people who can fill them. It’s a potentially substantial subsidy for small business. On the other hand vaccinated workers will mostly prefer to work with other vaccinated workers, so this could also offset or go the other way.
Others will doubtless decide to start new businesses to show them who is boss and get their revenge, which is presumably great. More people should start new businesses, and I truly wish them all the best of luck. Except the ones whose businesses are about fighting against vaccinations. Everyone else, let’s do this.
Note that some of the opposition to all this might not be as principled as it is made out to be.


My position isn’t fully static but mostly hasn’t changed, and I’m not looking to have the same discussions again, but for clarity I currently believe:
- Employers, both public and private, should be free and encouraged to mandate vaccination, and those that forcibly interact with the vulnerable especially.
- Indoor venues should be free and encouraged to mandate vaccination for entry.
- Non-essential (to a given person’s life) indoor public spaces should require vaccination, as should medical facilities, nursing homes and other such places.
- Vindictive rules that destroy value rather than protect it are not good. A rule makes sense if and only if it creates sufficient value by creating safer spaces and controlling spread. Justifying a rule by saying that the threat to destroy value will cause vaccinations should be out of bounds.
- No travel bans. They’re deeply stupid, even when they’re not things like banning European travelers for less than no reason, which we are somehow still doing.
- If we are go past the above policies, we would be better off instead acknowledging what we’re doing and outright mandating vaccinations. We’ve done it in the past, it’s not some scary new escalation.
- If we did decide to do that, I’d support it as part of a package where we otherwise chilled the f*** out and lifted other rules, the way Denmark recently declared Covid not a societal threat and lifted all restrictions, but not otherwise.
- In general, I believe the most important crux with those who oppose mandates is that I believe vaccine mandates are primarily substitutes for destructive alternative restrictions that are worse for freedom, and those who oppose mostly think they are mostly complements that ramp up restrictions of all kinds. If I was convinced I was wrong about this, I’d be forced to reconsider.
- I have another crux with many who oppose mandates, which is that I think it’s freedom-enhancing to give people choice in association, such as not wanting to employ the unvaccinated, so I’d still support private mandates unless I was convinced I was wrong about that as well, the same way that whether you’re vaccinated influences my decision of whether to sit down with you to have lunch and banning that seems rather terrible. I draw a sharp distinction between ‘you are allowed to mandate vaccination’ and ‘you must mandate vaccination’ whereas very few people in surveys seem to notice the difference.
- Some others have the crux that they don’t think vaccinations much matter, or they think vaccinations are unsafe (or not sufficiently proven to be safe), or that if you’re vaccinated that’s sufficient protection that you shouldn’t care who else around you is unvaccinated. It would be very hard to change my mind on any of those, but changing my mind on any of those would indeed change my conclusion.
- There are additional cruxes in various other places, this list is not complete.
- You’re still free to make comments and I’m still free to do my best not to engage further, and I intend to do my best.
A court has ordered that New York’s vaccine mandate for hospital workers is temporarily suspended for those seeking religious exemptions.
Having trouble getting the necessary paperwork? No problem, our church will take care of that as long as you become a paying online member. Markets in everything, solve for the equilibrium, blatant lies are the best kind and all that.
At least for now, the NBA will not mandate vaccinations for its players. They’re going to do a bunch of social shaming instead, like having them travel on a different bus. The league has an 85% vaccination rate, which is good, but far from 100%. The Knicks, Nets and Warriors will be exceptions due to state law, which should give them a small but meaningful edge this season. I wonder if it’s priced into the gambling lines.
In other vaccine mandate news, the employees don’t always oppose mandates, and also sometimes it’s time to take a bold stand against an overbearing union and overly demanding workers, but I’m guessing this wasn’t one of those times.

NPIs Including Mask and Testing Mandates
A case that the Bangladesh mask study didn’t tell us much of anything. I don’t think this is quite fair, they did have other stuff going on as well, but I do think it’s mostly right.
Meanwhile, the mask mandates might in practice have missed a spot?
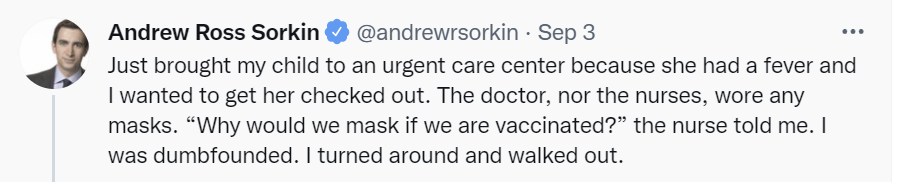
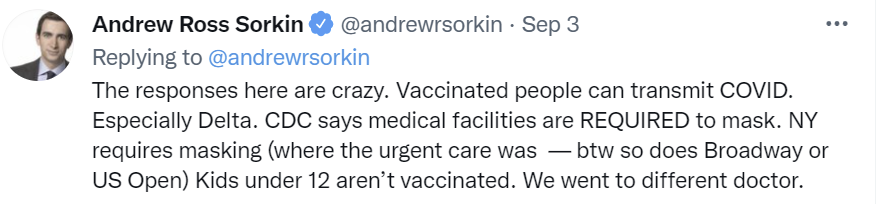
The craziest part about this is that if you’re treating a bunch of sick people, you kind of should wear a mask even if Covid-19 didn’t exist, because it also helps prevent a lot of other things that could be causing this child’s fever. Yet it also shows the logic of authoritarianism. Sorkin’s arguments about why the masks were necessary, and why he (quite sensibly) walked out have nothing to do with a physical world model, and everything to do with the rules and regulations.
Mostly news was quiet on this front this week.
Think of the Children
Our child’s preschool, like many such places, required a Covid test be taken in the few days before school. My wife’s understanding was that buying a rapid test and administering it herself would not suffice. She called a service that was supposed to come to us and provide the test, but they failed to show up with no explanation, then we called them, they said they’d call us back, and they didn’t call back either. She then took our son to six urgent care centers to try and get a test, but all of them turned us away because they already had lines out the door and no space, presumably because everyone else was doing the same thing. So the next day, I showed up at 7:30am with him to ensure we’d be first on line to get an appointment, they opened at 8, they declined our insurance at 8:15 and charged $180 so we’d have a signed official document that a thing had been needlessly stuck up our son’s nose while I forcibly held his head in place and his arms back, yeah that’s fun times, we were let in around 8:35 and someone did in fact stick the thing up his nose while I held him forcibly in place, around 8:55 the doctor came in and handed us a piece of paper that affirmed they’d stuck it up his nose so now everyone could be happy they’d generated enough extra Covid-19 exposure from hanging around inside an urgent care center that school could begin.
Yeah, great system, no trouble at all, keeps everyone safe, doesn’t waste valuable health care system resources, it’s all very reasonable and I have no idea what anyone is complaining about.
They’re also going to do it again, every week, forever, but at least in the future they’ll be arranging the logistics and bringing someone into the classroom to do it.
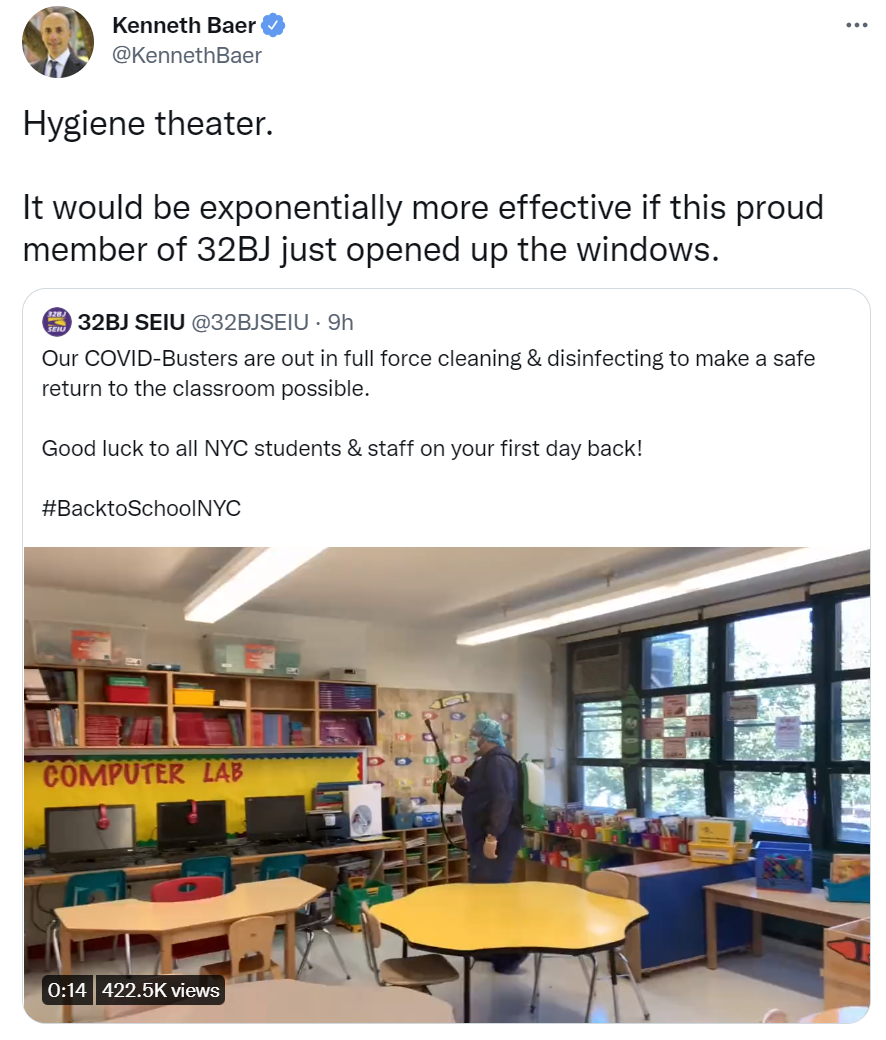
What do you want us to do, open a window? That wouldn’t be safe.
I complain about the weekly tests, because mumble mumble something about the children being four years old and fully masked at all times, but the testing is the least crazy part of the whole Covid protocol. It’s much less crazy than the part where parents are kept out of the building, or when kids are forced to eat on the sidewalks or given all-liquid lunches so they can keep their masks on. It’s even way less crazy than forcing them to wear masks, because do the math:
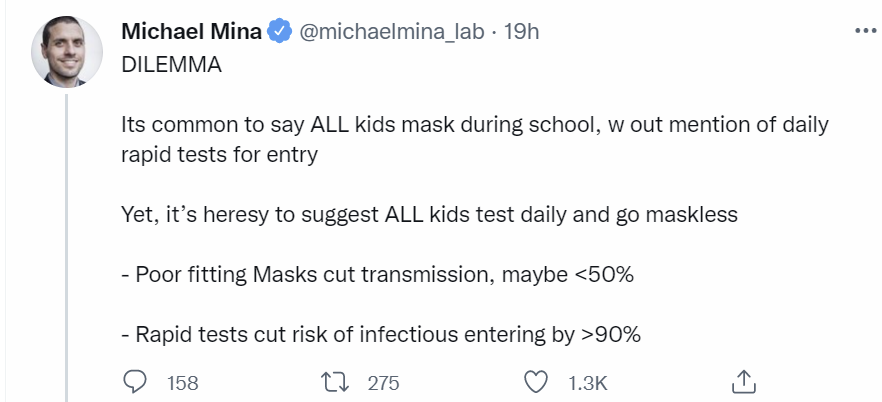
Assuming the masks are poorly fitting isn’t fair, but 50% still seems like a fair practical estimate here. As does 90% for daily rapid testing. I’m not going to go over that logic again, but when someone is highly infectious, the tests will almost always be positive, so the tests are doing the job they need to be doing. If anything, the extra sensitivity from PCR would actively be harmful here, since it would force stupid reactions.
The true cost, if we were to use reasonable rules, of rapid tests ae a small amount of time and a few bucks. That seems way better than all-day mandatory mask usage while trying to learn, and you get a much bigger payoff.
Alas:
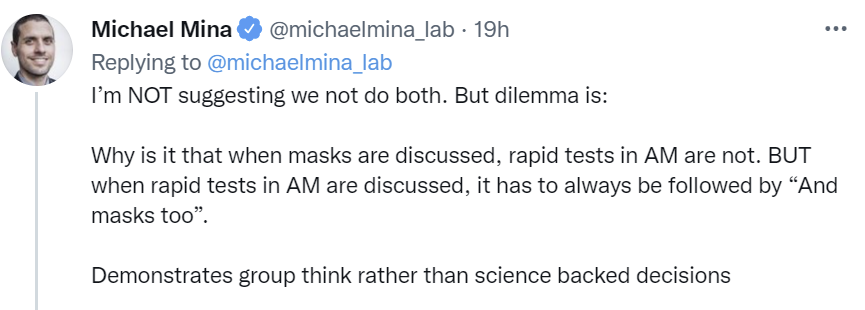
In practice, that’s right. The point of rapid testing in context is that it can be a substitute for other prevention and can make people less crazy, but if it’s a complement that doesn’t otherwise make anyone change anything except when it’s positive they panic, then it’s only making things crazier. Which makes it unclear if Mina is even helping, since as he points out it seems implausible that anyone will actually take his substitution solution, rather than Following The Science.
Last week there were good questions about whether the crazy college restrictions were one outlier college or if they were typical, with the presumption that they were a Not Necessarily the News extreme example. We now have an Ivy, Brown, doing something similar at least for a while:
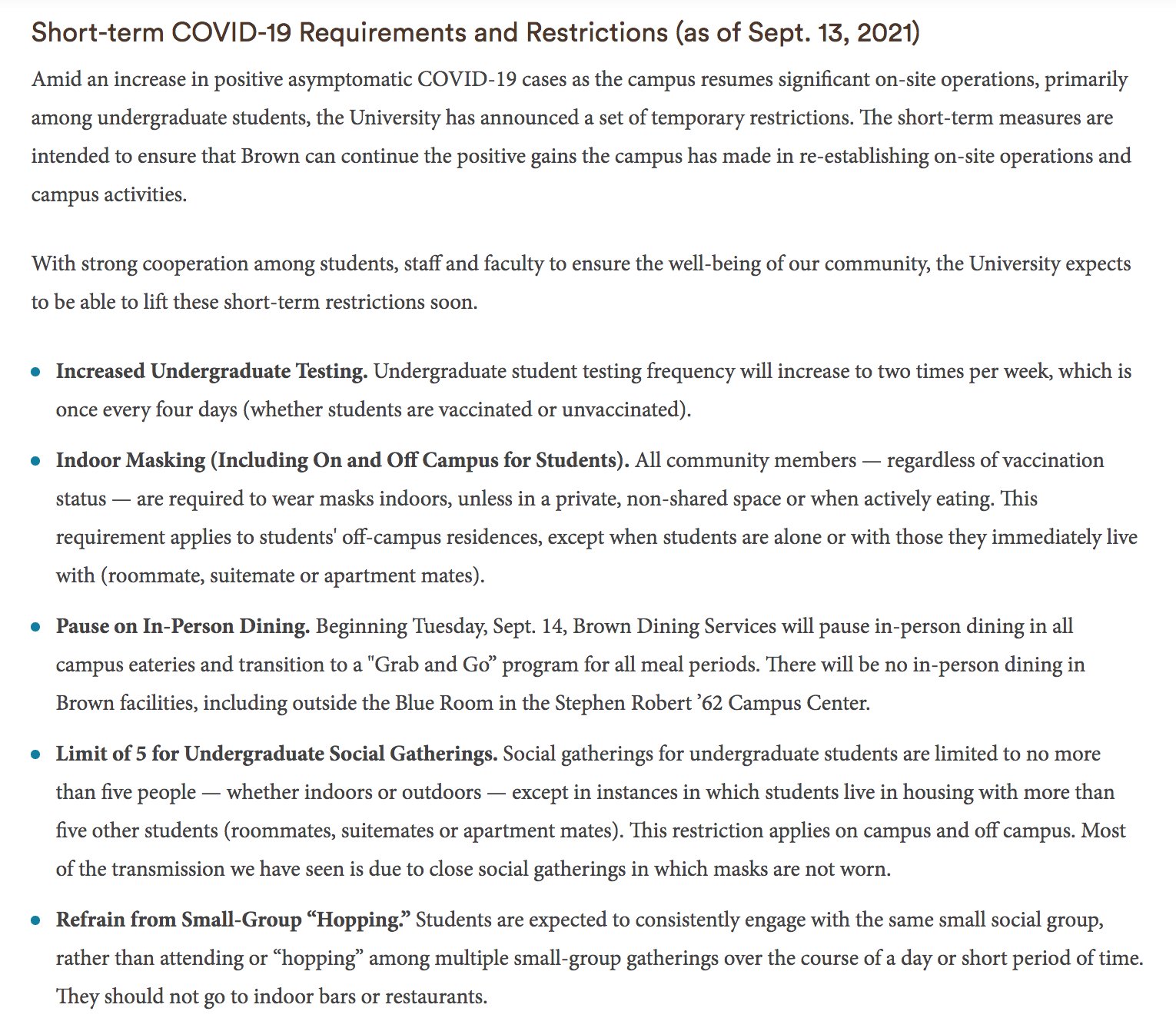
Note the first line, amid an increase in positive asymptomatic Covid-19 cases. This implies there likely was not even a single symptomatic Covid case.

This seems right. Given current conditions, if you test everyone weekly, eventually you’ll find some cases, then you can blame that on whatever you want to blame it on, and offer your Sacrifices to the Gods. As Tracey points out, the last bullet point, ‘Refrain from Small-Group “Hopping,” is especially chilling, essentially telling people they should only have one isolated friend group. You know, like they had in Columbine. And didn’t massively overreact to in a way that pointlessly traumatized an entire generation.
Whereas this Washington Post article’s true title is Parents Acting Crazy. If you think like this:

Then whatever happens to be top of mind will drive you crazy. If you take one small probability among dozens or hundreds or more, and label it ‘the salient risk’ then a large fraction of parents (and other people) go insane. This describes parents who are letting the risk of their young children getting Covid taking over their heads. ‘It’s like a fire alarm every day.’ If you have a fire alarm every day, eventually one considers the possibility that they’re not all that related to fires, whether or not you realize that in context your child is a dragon.
No matter how crazy the behaviors are, all of these stressed out, ruined lives are mostly over nothing, but that noting is still living rent free in a lot of heads, and every bit of that suffering and loss is on the FDA and its pointless demands and delays, and on the CDC and everyone else who sends the message to behave in exactly this way.
When people anticipate vaccines are immanent, they decrease how much social distancing they do. That’s the opposite of rational, but it’s a known pattern, and in this case it means we should see things improve for kids a bit earlier. The paper’s response of course is to suggest that ‘stricter measures will be required’ due to this decreased distancing, on the assumption that the policy goal is always more distancing.
A new Long Covid study on children is available from Israel.

I highlight this both because it’s how I first found the study, and also because of the mindset it indicates. Paul would have been skeptical, but the right person amplified the Twitter link, so that’s that.

Wow, that sounds scary. Can we have some details?
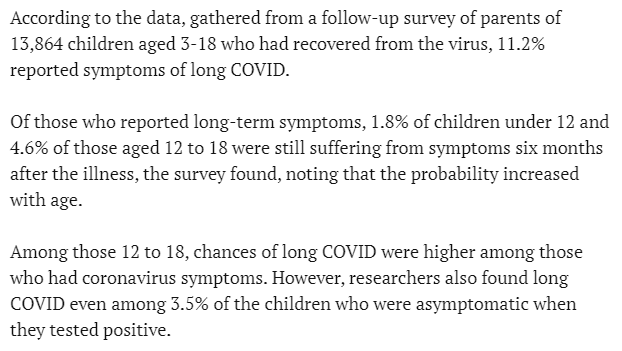
So what they’re calling ‘Long Covid’ is mostly things that last less than six months, with a large majority of children reporting all symptoms vanishing by then. I consider this a misleading headline.
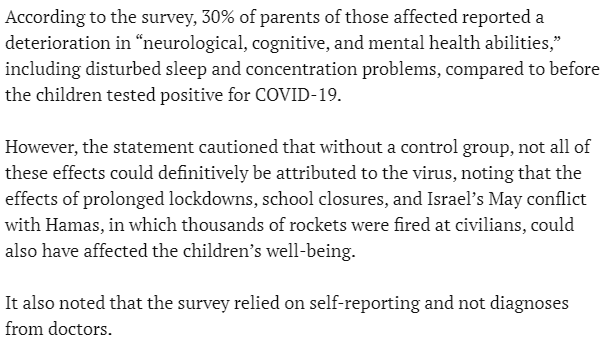
No control group at all doesn’t mean the results are totally useless, but it’s kind of close given how much Covid prevention messes up mental health. I don’t see the link to the actual paper, so I can’t easily dig in further, and given what I’ve seen I’m going to stop there.
My proposal is to survey kids who never tested positive for Covid to see if they’re reporting such symptoms, then do antibody tests on those kids, and check to see how much correlation is found between having Covid antibodies and the survey results. My prediction is that the effect size will be very small. This vaguely sounds like it would be considered “ethical” so someone please make this happen.
Perhaps the true pandemics among children lie elsewhere.
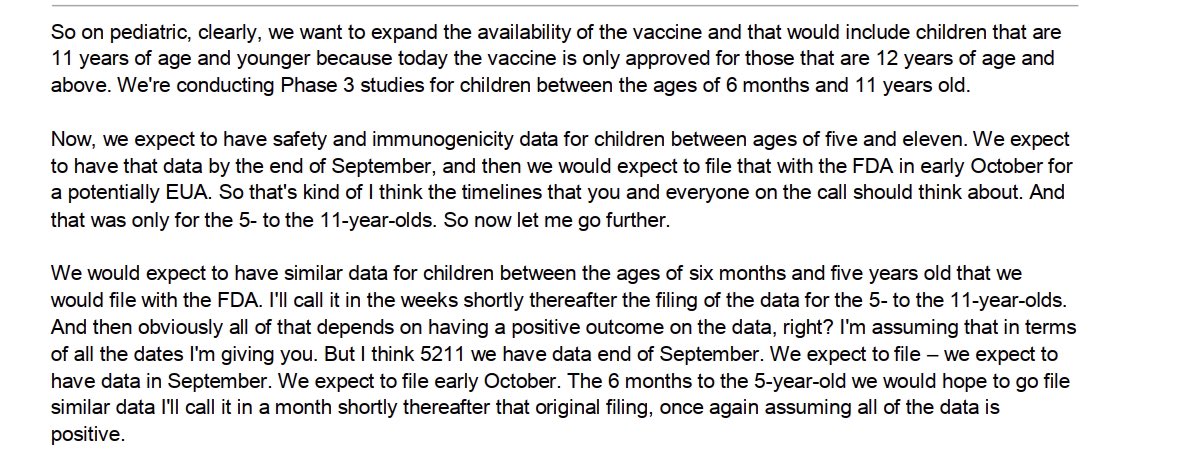
At least some good news, the phase where we can more fully blame the FDA for the lack of approval for child vaccinations is fast approaching.
Here’s data on exactly what we were forcing kids to do in various places, at various times during the pandemic.
Ivermectin
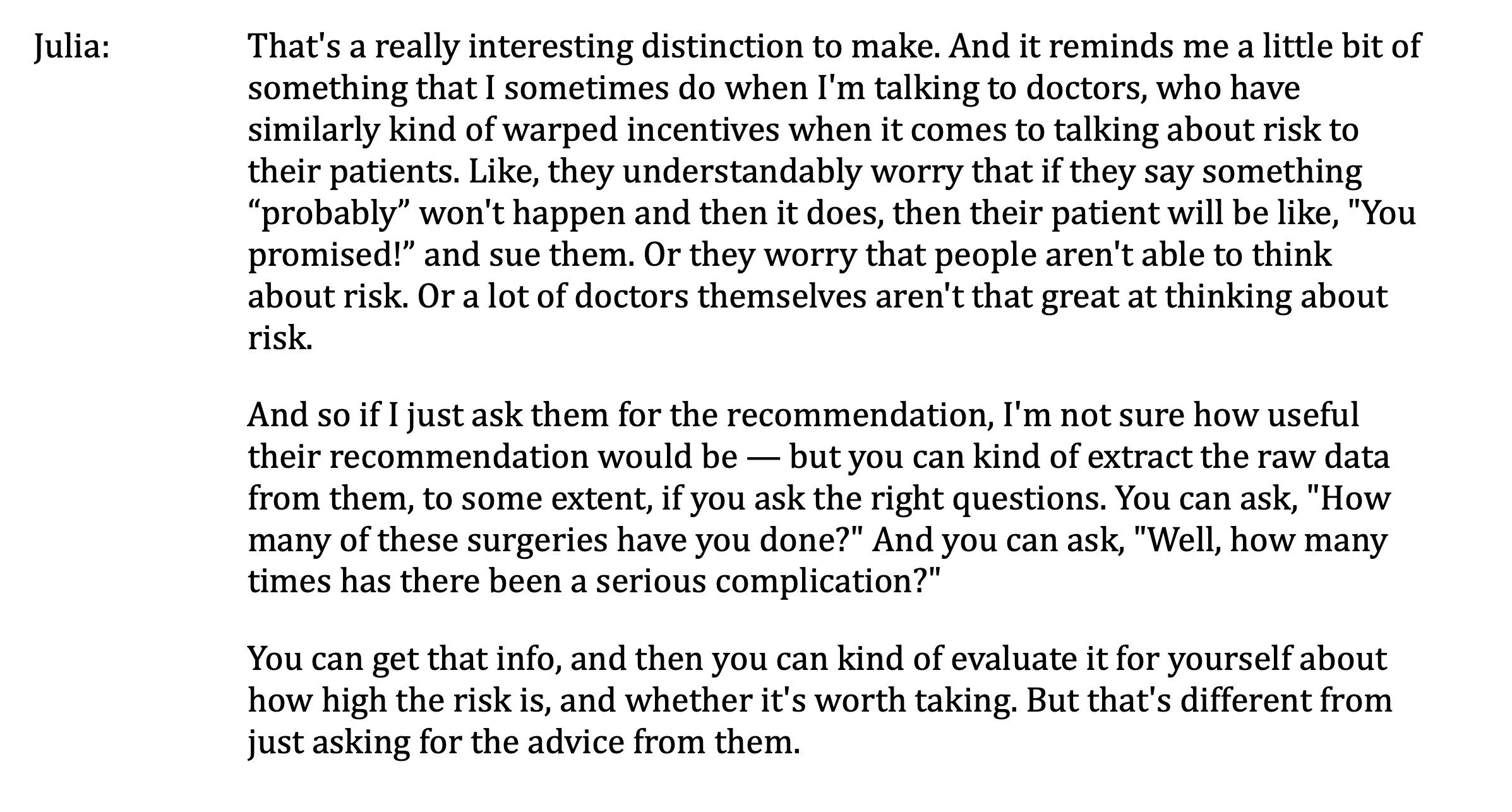
Kelsey Piper, after her recent self-recommending appearance on the podcast Rationally Speaking, wrote to host Julia Galef with this rather strong update:
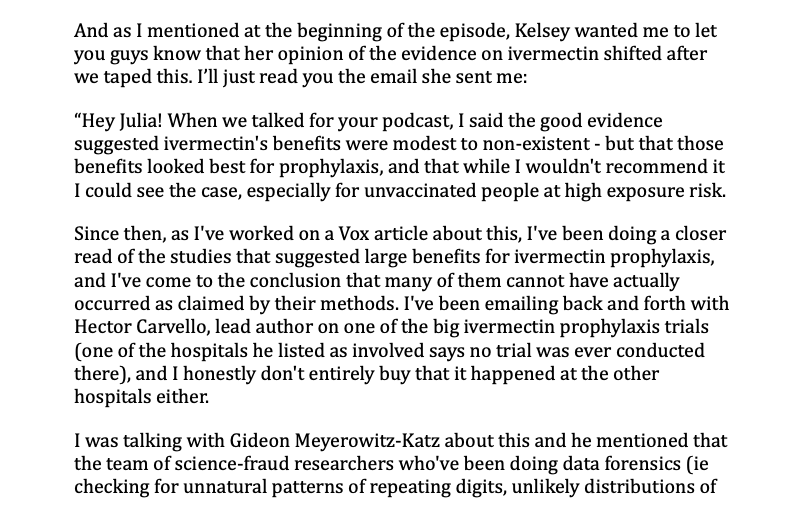
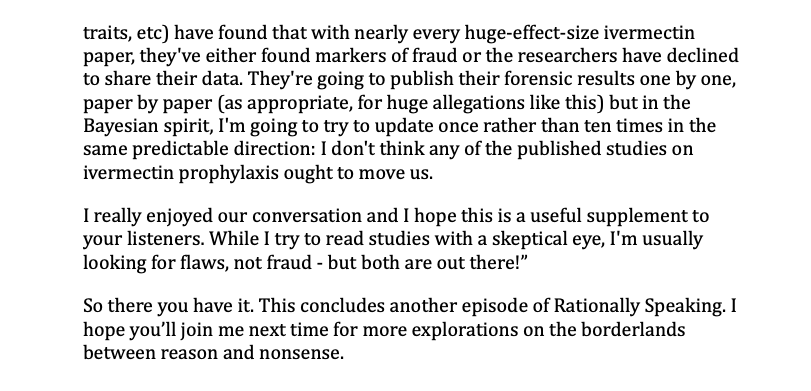
Kelsey isn’t always right but I trust her to be making an intellectually honest effort here, and ‘the hospital the trial says it was conducted at says the trial never happened’ is a pretty big deal, and if someone commits that level of fraud once at a minimum I would assume everything else they’ve done isn’t real until proven otherwise. How much to downgrade the not-proven-fraudulent evidence in the face of increasingly frequent findings of fraud is a hard question, but the answer sure isn’t zero, and I don’t think our prior on all this should have been great to begin with.
If you dig into the thread there’s also some interesting discussion about secondary attack rates, which is a relevant question on its own in addition to its bearing on the plausibility of the Ivermectin studies, I haven’t had time to dig into that question yet.
In Other News
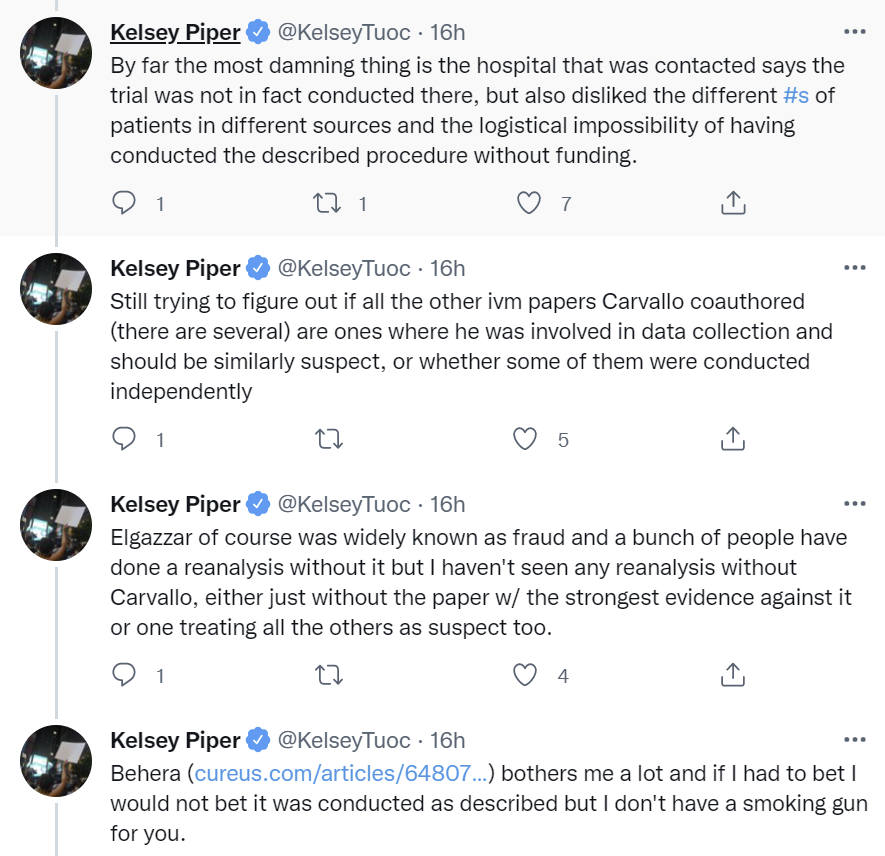
Also from Julia’s podcast with Kelsey, here’s Kelsey on the FDA and CDC.
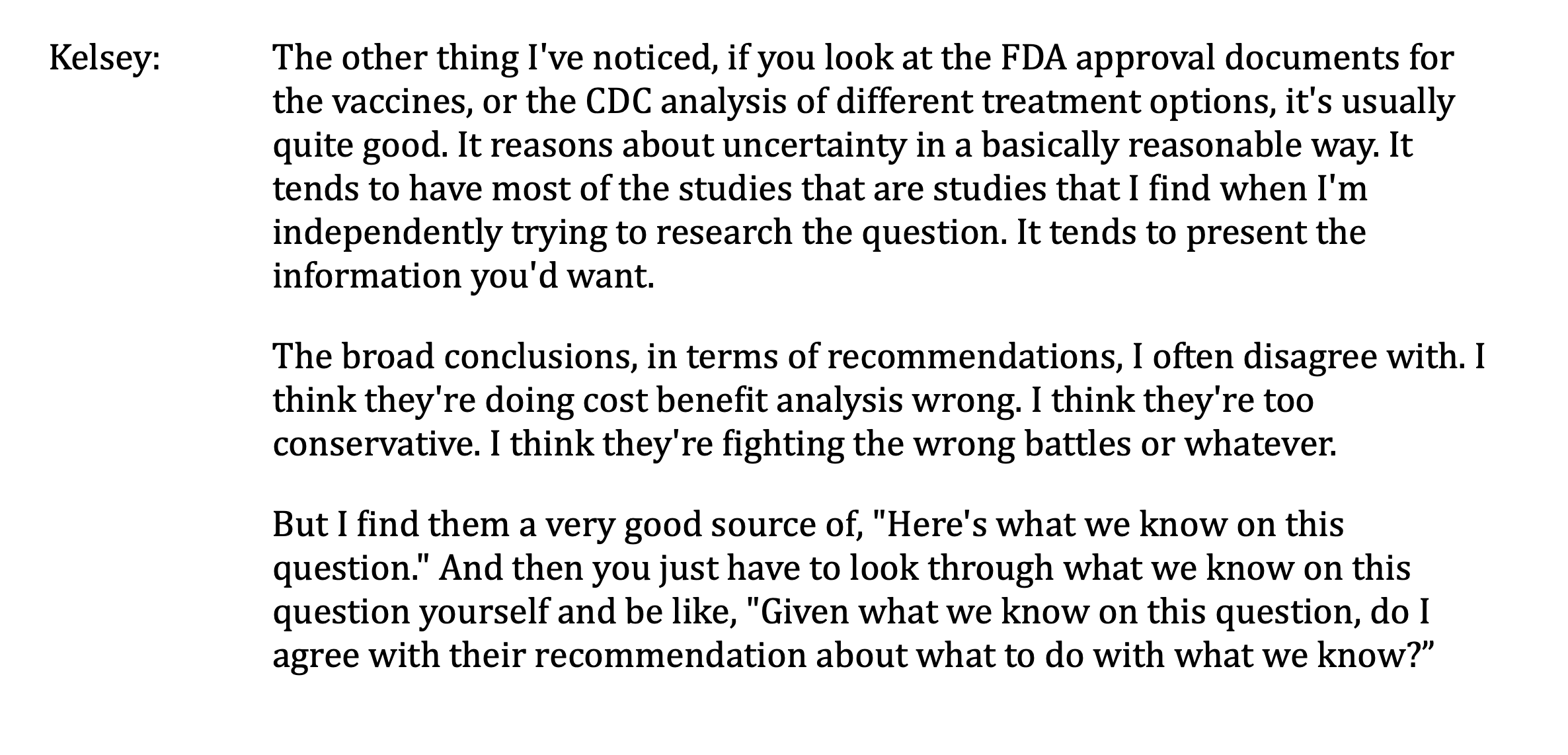
This has been my experience with the FDA. At least they get their facts right. They don’t do the right things with those facts, and they’re way too slow in gathering them, but to the extent that they offer you facts it’s fine to run with them. The CDC I am less confident in on these fronts, especially after Provincetown and the studies listed in an earlier section. It’s the whole thing where they kind of said vaccinated people couldn’t transmit Covid when that didn’t make any sense and then got everyone to panic by saying that maybe it didn’t prevent transmission at all which also didn’t make any sense, and now are making a big deal out of widely available basic statistics, on top of everything that came before, and the reports that the CDC withholds data.
A detailed look at exactly how how the FDA messed things up.
A review of Scott Gottlieb’s book Uncontrolled Spread. I’ll requote the part Alex Tabarrok quoted.
If there’s one overarching theme of “Uncontrolled Spread,” it’s that the Centers for Disease Control and Prevention failed utterly. It’s now well known that the CDC didn’t follow standard operating procedures in its own labs, resulting in contamination and a complete botch of its original SARS-CoV-2 test. The agency’s failure put us weeks behind and took the South Korea option of suppressing the virus off the table. But the blunder was much deeper and more systematic than a botched test. The CDC never had a plan for widespread testing, which in any scenario could only be achieved by bringing in the big, private labs.
Instead of working with the commercial labs, the CDC went out of its way to impede them from developing and deploying their own tests. The CDC wouldn’t share its virus samples with commercial labs, slowing down test development. “The agency didn’t view it as a part of its mission to assist these labs.” Dr. Gottlieb writes. As a result, “It would be weeks before commercial manufacturers could get access to the samples they needed, and they’d mostly have to go around the CDC. One large commercial lab would obtain samples from a subsidiary in South Korea.”
At times the CDC seemed more interested in its own “intellectual property” than in saving lives. In a jaw-dropping section, Dr. Gottlieb writes that “companies seeking to make the test kits described extended negotiations with the CDC that stretched for weeks as the agency made sure that the contracts protected its inventions.” When every day of delay could mean thousands of lives lost down the line, the CDC was dickering over test royalties.
In the early months of the pandemic the CDC impeded private firms from developing their own tests and demanded that all testing be run through its labs even as its own test failed miserably and its own labs had no hope of scaling up to deal with the levels of testing needed. Moreover, the author notes, because its own labs couldn’t scale, the CDC played down the necessity of widespread testing and took “deliberate steps to enforce guidelines that would make sure it didn’t receive more samples than its single lab could handle.”
This mostly isn’t new information. Still, some new details, and a healthy reminder. Listen all ya’ll, it’s a sabotage. This is more than ‘failed utterly.’ Failed utterly implies the goal was success. How would you differentiate what is described here from enemy action?
Imagine a private corporation had done this. What would have happened next?
An analysis of how long tests can offer you confidence that you are not infectious, and thus can safely interact with others, if you believe yourself to be at risk of having been infected. He uses physical world reasoning that seems at least reasonable, and reaches these conclusions:
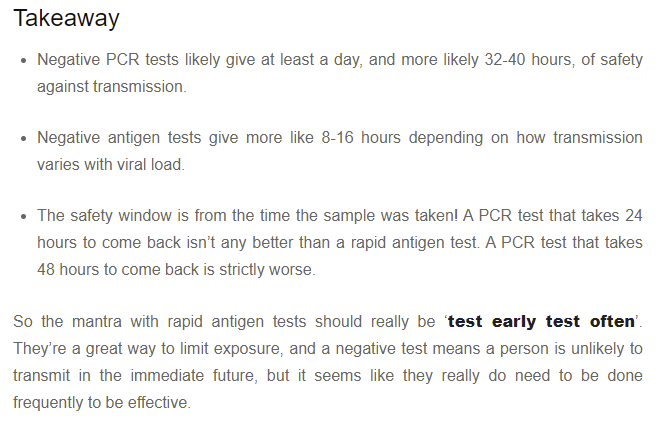
This treats Safety (with a capital ‘S’) as a Boolean state, which of course is a highly crude approximation, but the idea is that this is about how long you have (again, after the sample is collected) in which your risk is super duper low. And it emphasizes that speed matters a lot, and PCR is only good anti-transmission tech if its turnarounds are good.
Also worth emphasizing is that, as Mina keeps tirelessly pointing out, that PCR has a lot of true positives in the sense that the person is infected, but where the person isn’t infectious to others – the test is ‘too sensitive’ for this purpose, especially during recovery. Whereas the rapid tests aren’t quite sensitive enough compared to what would be ideal, but they’re still pretty damn good in terms of practical benefits.
NYU hospital in New York City gives excellent care, as long as you are very very certain you will not be the one who has to pay for it. And they sent me an email with this subject line, which buys so much goodwill I might bother completing the attached survey:

I got pushback on the Australia section last week, saying things weren’t that bad. This week, we learned both that a lot of Australians are in a place where they want more than six drinks a day, and the government is not letting them have them. Draw your own conclusions.
Meanwhile, here’s how their vaccinations are going. It’s worth noting, if you can’t leave your house until everyone is vaccinated, what’s your incentive to accept a second-best vaccine rather than wait?
From last week, Scott Alexander presents Too Good To Check: A Play in Three Acts. Recommended if you haven’t already seen it. I claim victory, since I’m able to feel smug about the conclusion rather than any of the previous things that were too good to check. It conveniently confirms all of my priors.
Good news though, at least one life was saved.

A thread on whatever happened to Novavax. I don’t know which of those explanations are right and which of the right ones are doing the work, but it’s hard to look at this and think ‘yep, we did everything we could, there was no way to spend more money or lower barriers and produce more vaccine doses.’
A thread reminding us that all the details of how we give out vaccines were basically guesses as to what would quickly satisfy the FDA, they make no sense and we’ll likely never know the right answers.
Alaska state senator says she is unable to reach the capital for votes because she is banned from Alaska Airlines after she refused to comply with the federal mask mandate, a move she calls ‘unconstitutional’ because words do not have meaning to such folks. It’s also clear she damn well can reach the capital anyway, it’s just expensive and annoying to go back and forth given where she’s chosen to live. Ah well. We all make choices in life.
Speculation that differences between states with different vaccination rates might have a lot to do with different rates of obesity, since the two happen to be correlated. Being obese makes Covid much more dangerous, yet we have established such strong norms against pointing out that it’s better to not be obese that we’ve made actual zero effort to use Covid as an opportunity to help people stop being obese. So I’d like to take this opportunity to encourage everyone out there to do what it takes to get down to a healthy weight, and to get yourself to a place where you feel good every day instead of feeling bad. I continue to put large effort into maintaining this, but yes it can be done, and yes even before Covid it was totally, totally worth it. Also, there’s a new drug that sounds promising, see the Not Covid section.
Also, while we’re at it, reminder to make sure to take Vitamin D.
This the latest effort to quantify Long Covid, which I found a link to via LessWrong, with the author thinking of it as similar to chronic fatigue syndrome. There’s enough thoughtful effort here that it needs to be included, but what sticks out at me is the continued reference point shifts in what constitutes Long Covid. Surveys ask people if they have any symptoms at all, that’s considered Long Covid, then that’s comapred to CFS because the most typical symptoms are most typical of CFS. Therefore create association of Long Covid as equivalent to lifelong crippling fatigue. And as usual, I have zero faith in what passes for controls in such measurements. There are then some calculations I’d argue with even given the premise. And if things really were this bad, and a good fraction of a percent of people who got Covid ended up permanently crippled, many of them unable to work normal jobs, I’d point out how many people already did have Covid by this point, it’s at least a large minority of the population. So this seems like the kind of thing that would be impossible to miss on a population level.
This chart still throws me for a loop when I see it:
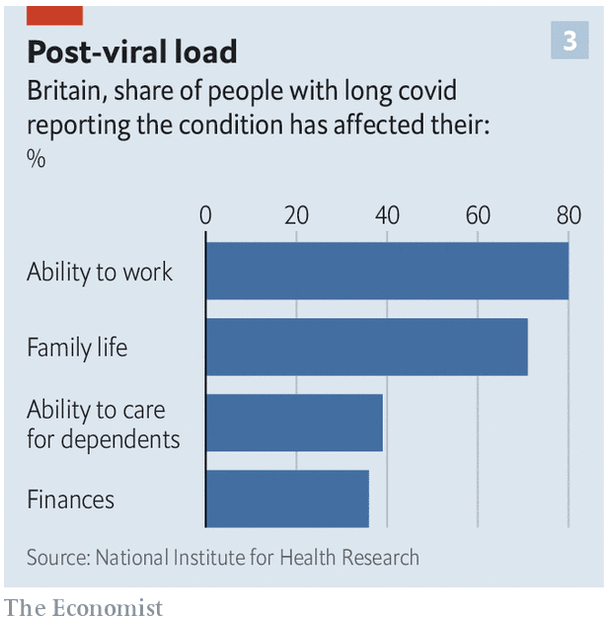
Any one of these would be possible, but thinking about them relative to each other is rather strange. I would think that something that ‘affected your ability to work’ as well as family life and ability to provide care would impact one’s finances more often than that.
One interesting thing about the post is the framing of the takeaways. The author identifies this primarily as a strong argument for vaccination. His analysis suggests that vaccination cuts risk of Long Covid by an order of magnitude:
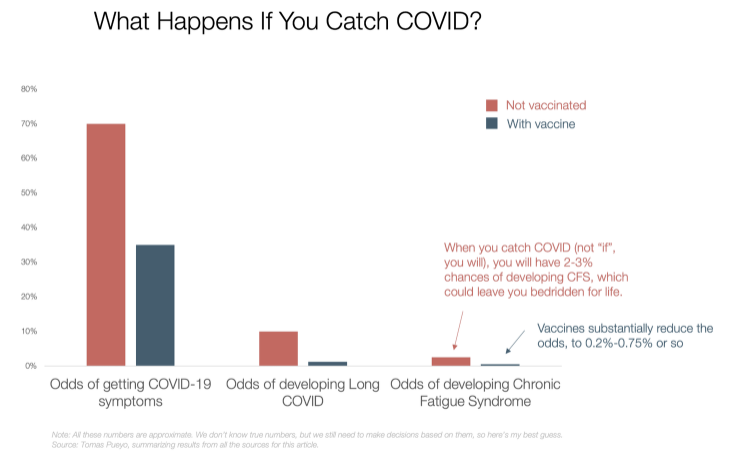
Note that this is despite him thinking vaccines are only 50% effective against infection by Delta, which is well outside my reasonable bounds for mRNA.
He also notes that it seems like many Long Covid victims improve when given the Covid vaccine, long after their infections:
It’s not the only benefit from vaccines. They can also help relieve some CFS.
Apparently, about 30-40% of Long Haulers report an improvement in their symptoms after being vaccinated. It doesn’t cure the symptoms, and we’re not sure how long that relief lasts, but at least it looks like it helps some of them. How can that be?
To answer that question, we need to understand what might cause CFS in Long Haulers.
What Might Cause CFS in Long COVID?
There are three main hypotheses on why these symptoms last so long:
The COVID-19 virus (or other equivalent viruses for other CFS) survives inside the body forever, pushing the immune system to chronic alert level.
The immune system becomes dysregulated, and stops fighting another set of viruses, which now are more free to roam and affect the body, which the immune system then needs to fight in a chronic war.
A dysregulated immune system attacks the body itself. In this case, it would be an auto-immune disease.
There is evidence for all 3, across both Long Haulers and patients with other types of CFS. Tests have found in the blood remains of viruses and high levels of antibodies.
I started going down this rabbit hole, but I stopped when I saw the complexity of the disease and how little we still know about it.
It seems like this data point isn’t being followed up on sufficiently. Either this is some sort of placebo effect, in which case that’s a huge deal and we should ride that placebo train for all its worth, or it’s not, which is an even bigger deal. It also, under this model, has strong implications for CFS that’s caused by other diseases, since the story is that CFS is often caused by the aftereffects of some infection. Have we tried giving people vaccines in those cases? Failing that, have we tried re-infecting them with whatever they had before as a next best option? CFS is really, really bad, so it seems worth trying?
Along similar lines, if you got vaccinated, got Covid and then got Long Covid anyway, this model suggests getting a booster shot might still help you some of the time, and it’s a low risk thing to try, based on my understanding of the plausible mechanisms here.
It also emphasizes once again that Covid suggests we don’t pay enough attention to fighting the spread of other infectious diseases, as they may be far more destructive than we realize, and thus far more worth fighting.
Not Covid
At the movies: I saw Shang-Chi and the Legend of the Ten Rings, another Marvel origin story movie. It exceeded expectations and lived its best life. Then I saw Free Guy, which is better and definitely underrated, although I am very much in the target audience here. I have a model of why critics didn’t respect it properly, but no spoilers.
Biden partners with Australia to build nuclear submarines. Insert what you think I almost said next here.
Saw this and I think it may explain quite a lot. I preliminarily endorse OpenPhil or another sufficiently large EA donor fully funding this.


I saw this, in an interesting discussion on the future of weight loss (hat tip: MR):

Way to bury the lead. I briefly got theoretically super excited, because can you imagine how amazing it would be to be able to take negative amounts of marijuana, as if it were something coming out of Wonka’s factory? Appetite suppression is nice at times, but imagine being smarter and faster and more motivated to get things done when the situation calls for it. Then, you could pull a reverse and feast. Alas, I’m pretty sure that’s not how any of this works, and also the drug in question has some issues regarding mental health and was never approved – although if it did what my imaginary version did I wouldn’t care, cause with those benefits I’d hold things together just fine, and like Eliezer I’d be immune to the Gods of Irony.
The real lead in weight loss of course lies elsewhere, in that they seem to have finally found a drug that works.
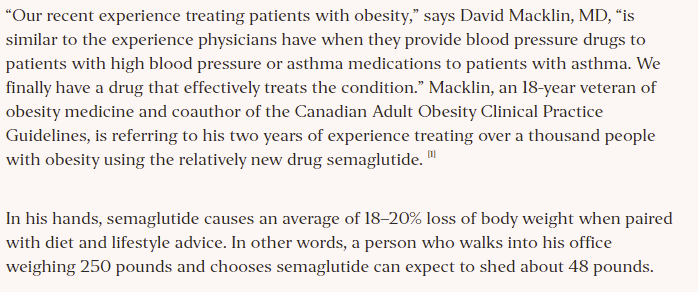
Alas, such a thing is of no help to me. My twin problems are a love of calorically rich foods and an impossibly slow metabolism. I lost the weight the hard way [LW · GW], and the majority of days, decades later, I continue to fight the good fight and optimize my meals with more care than anyone else thinks is reasonable, a policy for which I have no regrets. As I wrote above, it’s all been totally, totally Worth It.
The problem is that this new would-be-miracle drug (I haven’t looked into it in detail) works via appetite suppression. That doesn’t help me at all, and if anything takes joy away from my life. Le sigh. It also suggests a very clear model of why weight loss attempts almost always fail, and what causes the few successful ones to succeed.
Even more interestingly, the effects aren’t limited to food:
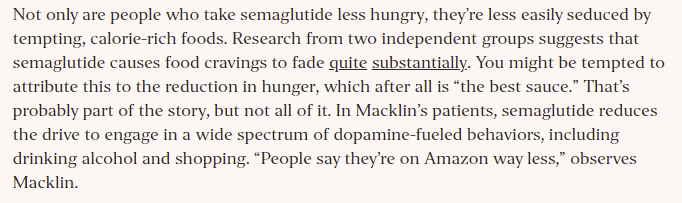
If you could turn that knob down in other areas, would you want to?
14 comments
Comments sorted by top scores.
comment by PatrickDFarley · 2021-09-17T16:16:33.872Z · LW(p) · GW(p)
I believe vaccine mandates are primarily substitutes for destructive alternative restrictions that are worse for freedom, and those who oppose mostly think they are mostly complements that ramp up restrictions of all kinds.
That is definitely a crux, thank you for pointing that out.
or that if you’re vaccinated that’s sufficient protection that you shouldn’t care who else around you is unvaccinated.
This is 100% me. My view is: if your solution requires absolutely everyone to buy in to it - that is, it requires successful coordination across all cultures within the US, or in the world - then you don't have a solution, you have a wish. The wish is for human nature to be fundamentally different from what it is.
Forcing coordination through federal mandates is different, in that it's actually possible. But I see a similar kind of wish here. Re the substitute/complement question above, I believe the hypothetical version of the US government that successfully exercises such control over its citizens' physical bodies and then promptly relinquishes that degree of control, is a US government not run by humans.
I happen to think the vaccine is an actual solution under the strict definition above. As in, I got it, so the pandemic is over for me. The reductions in infection and long-term risk are well documented here, and in my view they're enough to justify taking the (underrated) benefit of no longer worrying about my covid risk (including caring about the vax status of those around me) (obviously I'm still worried about the second-order effects). I've had a really enjoyable summer that was full of social interaction, travel, dating, etc.
Tldr: "Real life" has enough utility that I count my individual vaccination as sufficient risk mitigation to justify it.
comment by CraigMichael · 2021-09-18T07:05:49.739Z · LW(p) · GW(p)
Vindictive rules that destroy value rather than protect it are not good. A rule makes sense if and only if it creates sufficient value by creating safer spaces and controlling spread. Justifying a rule by saying that the threat to destroy value will cause vaccinations should be out of bounds.
This template is a good heuristic for rules in general.
Zvi, you are loved like a milkshake… not in like a reckless obesogenic way, but a like a thoughtful anabolic consumption of milkshake way.
Replies from: PatrickDFarley, alex-c↑ comment by PatrickDFarley · 2021-09-18T17:45:14.995Z · LW(p) · GW(p)
Yeah, I was pretty bothered a couple years ago when we were doing the "kids in cages" news cycle, and the red tribe people kept saying stuff along the lines of, "it's good that our policy is unpleasant, because it's a deterrent against future infractions".
Any degree of cruelty can be (correctly!) framed as a deterrent. So in general we should be really wary of those kinds of policies.
↑ comment by Alex C (alex-c) · 2021-09-22T20:21:27.484Z · LW(p) · GW(p)
The problem with the principle is there are often pre-commitments to not make the sensible rules, so they have to find workarounds.
comment by Stephen Bennett (GWS) · 2021-09-20T22:03:36.781Z · LW(p) · GW(p)
I noticed that this post isn’t in the covid 19 sequence I can find from your profile(nor are the other September posts). Was that an intentional change? I found it useful to be able to link people to that sequence as a stable location to find your posts who would probably not be interested in lesswrong more broadly.
Replies from: Zvicomment by MondSemmel · 2021-09-17T21:19:40.128Z · LW(p) · GW(p)
Somehow for me lots of images in this post don't load and can't be reloaded in-page, but do load if I load the individual images in a new tab. How is it even possible that the web works like this?_? (If it matters, I'm on Firefox.)
Replies from: gwillen↑ comment by gwillen · 2021-09-20T06:38:54.731Z · LW(p) · GW(p)
If it's like last time, and if I recall correctly what I found then, it's all the images hotlinked from Twitter, because Twitter has set a browser security header on their images that blocks hotlinking.
Replies from: Zvi↑ comment by Zvi · 2021-09-22T13:10:42.277Z · LW(p) · GW(p)
Does this mean I need to always use snipping tool rather than copy image, or will that somehow also not work?
Replies from: gwillen↑ comment by gwillen · 2021-09-27T03:45:53.836Z · LW(p) · GW(p)
I don't know, sorry -- I am not that familiar with the tools for composing LW posts. But hopefully this information will help someone from LW tell you the right thing to do? All I know is, if you can get the image hosted by LW and not by Twitter, it will fix the problem.
comment by tkpwaeub (gabriel-holmes) · 2021-09-20T12:36:11.946Z · LW(p) · GW(p)
Point of order on the "expansion" of OSHA's powers. OSHA is an agency, and the working definition of agency is that it contains miniature versions of all three branches. The executive functions are inherited, obviously. The legislative functions take the form of proposed regulations with public comment periods, and administrative hearings are judicial.
comment by GreatHornedOwl · 2021-09-19T23:35:59.709Z · LW(p) · GW(p)
Firstly, praise. These regular posts are very informative.
Secondly, an enquiry. Recently (within the week) the UK Government pulled back on ordering doses on (what would have been) one of only two available inactivated vaccines. I have a sneaking suspicion that this is due to geopolitics (the company, Valneva, is French). Do you have any specific information on this?
Replies from: Zvicomment by tkpwaeub (gabriel-holmes) · 2021-09-19T09:22:46.704Z · LW(p) · GW(p)
I can't even begin to express how much I appreciate your inclusion of 6 and 7 in the above points.