Covid 2/9/23: Interferon λ
post by Zvi · 2023-02-09T16:50:01.022Z · LW · GW · 8 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Interferon λ Physical World Modeling In Other Covid News China Remember ADHD Medication Shortage Update Other Medical and Research News None 8 comments
There are two big pieces of pandemic news this week.
One is that there is growing alarm about the dangers of avian flu, or H5N1. Likely mammal-to-mammal transmission has been identified, a lot of wild animals are infected, and there is a real danger that this will become a pandemic. I will cover this in its own post.
The other is that there are trial results for a new Covid treatment, Interferon λ. It looks super effective. Cuts hospitalizations and deaths in half, with no major side effects.
Despite this, there is zero expectation by anyone that it will be available any time soon, and little surprise about this reaction. You see, the trial was done by academics and was in Brazil and Canada. So it doesn’t count. Sorry.
Executive Summary
- We have a new drug that cuts Covid risk of hospitalizations and deaths by about half with no major side effects.
- You can’t have it. Maybe ever.
- Because FDA. FDA Delenda Est.
Let’s run the numbers.
The Numbers
Predictions
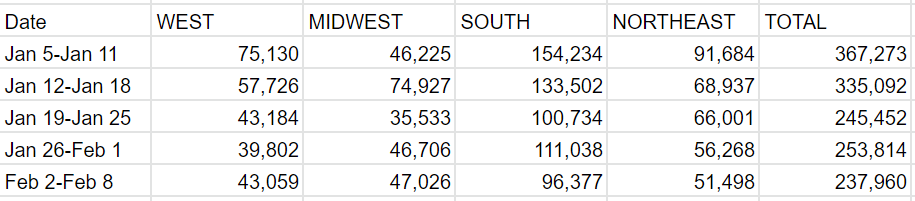
Predictions from Last Week: 210k cases (-8%) and 3,150 deaths (-8%)
Results: 238k cases (-6%) and 3,052 deaths (-11%)
Predictions for Next Week: 220k cases (-7%) and 2,750 deaths (-10%).
Last week I forgot to manually adjust Florida for cases, which I’ve fixed. That’s why the percentages above don’t match. Also means my prediction last week for cases was worse than I thought – cases were actually slightly up and I predicted a drop.
I expect deaths to continue to drop on schedule. Valentine’s Day is not a reporting-relevant holiday, although it is still a date it is important not to forget.
Deaths
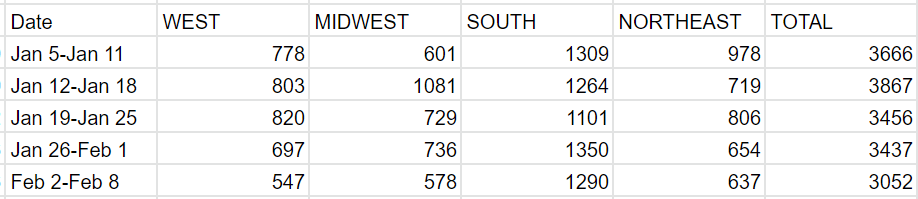

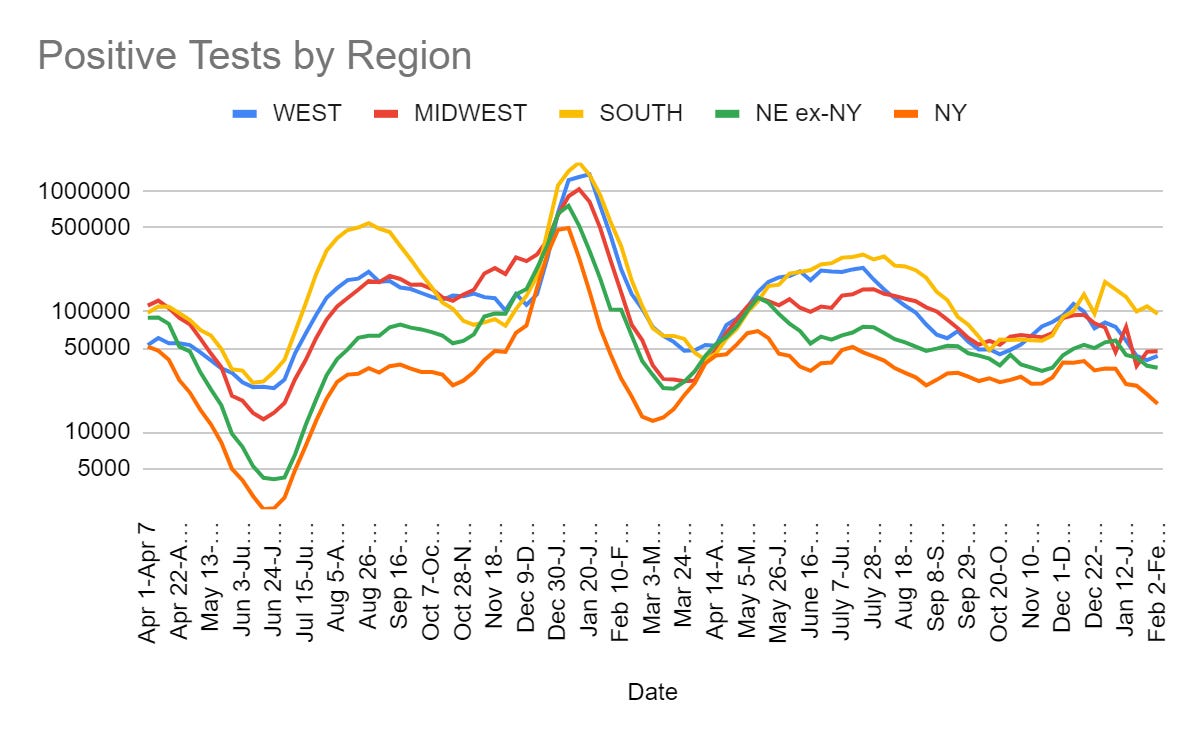
Cases
Interferon λ
As noted up top: It looks super effective. Cuts hospitalizations and deaths in half, with no major side effects. Despite this, there is zero expectation by anyone that it will be available any time soon, and little surprise about this reaction.
Here is their results summary.
A total of 933 patients were assigned to receive pegylated interferon lambda (2 were subsequently excluded owing to protocol deviations) and 1018 were assigned to receive placebo. Overall, 83% of the patients had been vaccinated, and during the trial, multiple SARS-CoV-2 variants had emerged. A total of 25 of 931 patients (2.7%) in the interferon group had a primary-outcome event, as compared with 57 of 1018 (5.6%) in the placebo group, a difference of 51% (relative risk, 0.49; 95% Bayesian credible interval, 0.30 to 0.76; posterior probability of superiority to placebo, >99.9%). Results were generally consistent in analyses of secondary outcomes, including time to hospitalization for Covid-19 (hazard ratio, 0.57; 95% Bayesian credible interval, 0.33 to 0.95) and Covid-19–related hospitalization or death (hazard ratio, 0.59; 95% Bayesian credible interval, 0.35 to 0.97). The effects were consistent across dominant variants and independent of vaccination status. Among patients with a high viral load at baseline, those who received pegylated interferon lambda had lower viral loads by day 7 than those who received placebo. The incidence of adverse events was similar in the two groups.
I am completely unsurprised both by our government denying people access to life saving medicine as a matter of course. And also completely unsurprised by the complete indifference of the public to our government indefinitely denying everyone access to life-saving medicine.
Paxlovid was the last gasp of the old ‘people are dying and we upended our lives to try and stop this, perhaps we should unnecessarily delay less than usual in deploying life saving medicine’ principle.
This is standard procedure. The FDA exists to deny people life saving medicine. For years. Instead, during that time, they die. No rush. If there isn’t enough money to justify paying to get through the process, they’ll keep dying forever. It’s fine.
The New York Times puts it this way, via MR:
A new drug quashes all coronavirus variants. But regulatory hurdles and a lack of funding make it unlikely to reach the U.S. market anytime soon.
…
a new class of variant-proof treatments could help restock the country’s armory. Scientists on Wednesday reported in The New England Journal of Medicine that a single injection of a so-called interferon drug slashed by half a Covid patient’s odds of being hospitalized.
The results, demonstrated in a clinical trial of nearly 2,000 patients, rivaled those achieved by Paxlovid. And the interferon shots hold even bigger promise, scientists said. By fortifying the body’s own mechanisms for quashing an invading virus, they can potentially help defend against not only Covid, but also the flu and other viruses with the potential to kindle future pandemics.
…
As it stands, Eiger executives said that they might seek authorization for the interferon shot outside of the United States. China, for example, has been looking for new treatment options.
…
“It doesn’t matter if the next pandemic is a coronavirus, an influenza virus, or another respiratory virus,” said Eleanor Fish, an immunologist at the University of Toronto who was not involved in the new study. “For all the viruses we’re seeing that are circulating now, there’s utility to using interferon.”
So this isn’t only about different Covid variants. It goes beyond Covid.
Except it goes nowhere, we won’t have it, unless something changes.
Eric Topol summarizes the results:




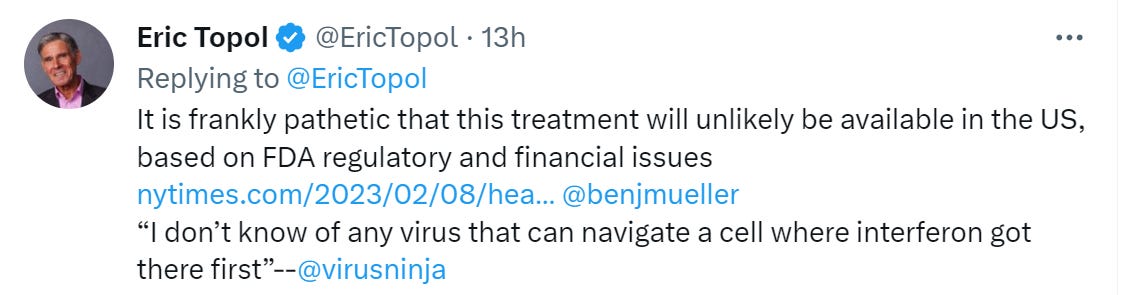
Why won’t it be approved here? Again NYT:
Eiger executives said part of the problem seemed to be that the clinical trial did not include an American site, but rather only sites in Brazil and Canada, and that it was initiated and run by academic researchers, rather than the company itself.
As reasons to deny people life-saving medicine? That is completely, utterly murderously insane. The issues here could not be clearer.
Tyler Cowen asks if we have learned nothing. To which I answer, no. We have learned something very important, which is that our institutions have no interest in reforming, or in what would cause people not to die. We have learned that we have the ability to do much better, if allowed to do so. And we have learned that those with the guns will not allow it.
Good to know.
Physical World Modeling
Dr. John Campbell (video plus links) fully buys this metastudy from 16 January claiming definitive very large impacts on Covid-19 hospitalization and mortality from Vitamin D supplementation. He goes so far as to say that not recommending Vitamin D, at this point, appears unethical. The language he uses here comes on stronger than I believe the evidence justifies.

The thing is, no, you can’t and also shouldn’t guarantee that this won’t happen again. You don’t know what the threat will look like next time. The response to ‘we did too much prevention given the costs of Covid’ can’t be ‘we can never again contain contain an outbreak of anything no matter what.’
In Other Covid News
Mask mandates are still sometimes a thing for schools, although they now tend to be conditional. Here’s Vashon High School in Washington.
What exactly did Pfizer do? Are they doing anything dangerous or worrisome here?
I was asked via PM on LessWrong this past week to look into the claim that Pfizer was engaging in ‘directed evolution’ research to prepare the vaccine for new variants in advance. I explained this seemed like Obvious Nonsense, as this in no way helps with any meaningful bottlenecks to developing a modified vaccine. At most it buys a few days.
Here is a claim being made (direct link, note source is Project Veritas so lots of salt):

Here is the framed-to-maximize-scare-level quote:
New York: Pfizer has admitted that it “engineered” treatment-resistant Covid-19 variant to test its antiviral medicine. This statement partially backs up revelation made by the US-based multinational pharmaceutical company’s director who told his date that Pfizer was deliberately “mutating” the virus to “preemptively develop new vaccines.”
Here is Pfizer’s response in full, bold is mine.
New York, N.Y., January 27, 2023 – Allegations have recently been made related to gain of function and directed evolution research at Pfizer and the company would like to set the record straight.
In the ongoing development of the Pfizer-BioNTech COVID-19 vaccine, Pfizer has not conducted gain of function or directed evolution research. Working with collaborators, we have conducted research where the original SARS-CoV-2 virus has been used to express the spike protein from new variants of concern. This work is undertaken once a new variant of concern has been identified by public health authorities. This research provides a way for us to rapidly assess the ability of an existing vaccine to induce antibodies that neutralize a newly identified variant of concern. We then make this data available through peer reviewed scientific journals and use it as one of the steps to determine whether a vaccine update is required.
In addition, to meet U.S. and global regulatory requirements for our oral treatment, PAXLOVID
, Pfizer undertakes in vitro work (e.g., in a laboratory culture dish) to identify potential resistance mutations to nirmatrelvir, one of PAXLOVID’s two components. With a naturally evolving virus, it is important to routinely assess the activity of an antiviral. Most of this work is conducted using computer simulations or mutations of the main protease–a non-infectious part of the virus. In a limited number of cases when a full virus does not contain any known gain of function mutations, such virus may be engineered to enable the assessment of antiviral activity in cells. In addition, in vitro resistance selection experiments are undertaken in cells incubated with SARS-CoV-2 and nirmatrelvir in our secure Biosafety level 3 (BSL3) laboratory to assess whether the main protease can mutate to yield resistant strains of the virus. It is important to note that these studies are required by U.S. and global regulators for all antiviral products and are carried out by many companies and academic institutions in the U.S. and around the world.
Fact-based information rooted in sound science is vitally important to overcoming the COVID-19 pandemic and Pfizer remains committed to transparency and helping alleviate the devastating burden of this disease.
I see no reason to much doubt Pfizer’s explanation. So, should we be worried about putting a new spike protein onto the original virus, within a lab, once that new spike protein is observed in the wild?
I think the answer here is clearly no. This is a good scientific practice allowing different variables to be tested on their own, and poses essentially zero additional risks. As with any generally dangerous thing, it can be difficult to draw the exact right line on what people should be doing or should be allowed to do, and one must worry about slippery slopes and development of bad habits.
I can see worlds in which we would be wise to tell Pfizer they are not allowed to do this as an unfortunate side effect necessary to stop other actions that could cause big problems. I do not however see anything here as a problem on its own.
Singapore ceases remaining Covid-19 prevention measures on Monday.
China
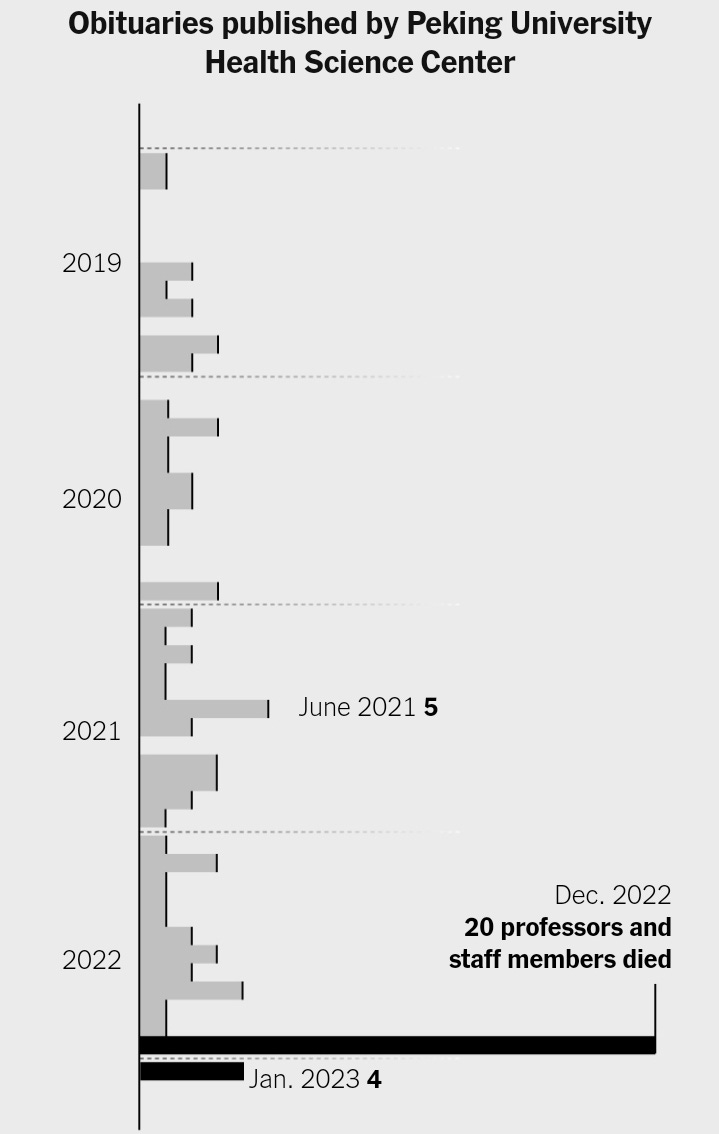
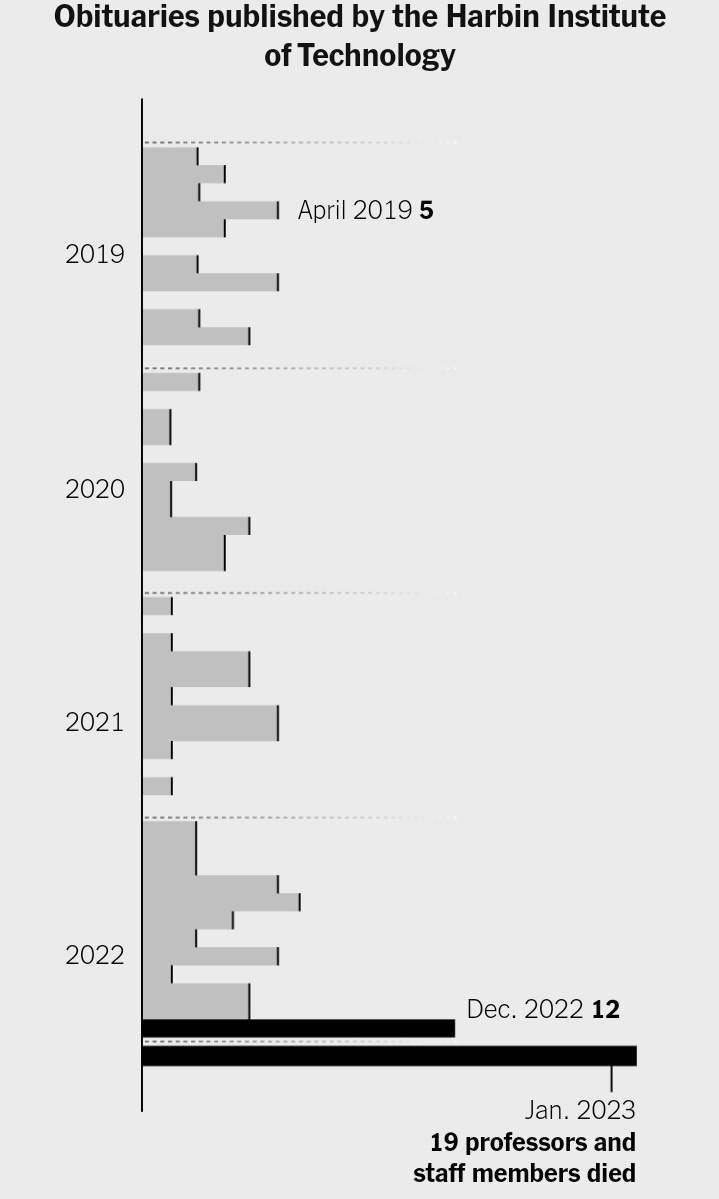
Remember
Trump and DeSantis compete to distance themselves from Operation Warp Speed and the vaccine (Bloomberg).
The Wuhan Institute for Virology had One Job, which was to help us in the case of a potential pandemic. In particular, a potential SARS-2 pandemic. Why then, asks Alina Chan, did they not share their virus sample database? If nothing else, it shows that this database was not all that useful. Either it was not worth sharing, or there was some reason they couldn’t share it.
Study on the impacts of physical distancing measures on ‘vulnerable population groups.’ Finds all the downsides you would expect, which I’d expect to find in the general population the same way. Such distancing will sometimes be necessary. It sure isn’t cheap in any sense.
ADHD Medication Shortage Update
I continue to get increasing reports of people unable to fill their meth ADHD med meth ADHD med prescriptions. This continues to be the result of an intentional cap on usage that the DEA intentionally sets (direct link) below the FDA’s estimate of usage.
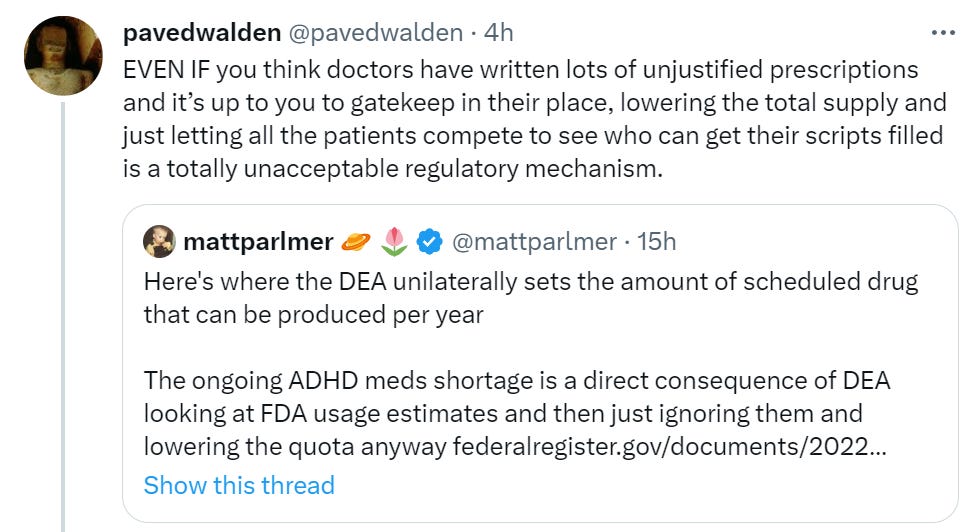
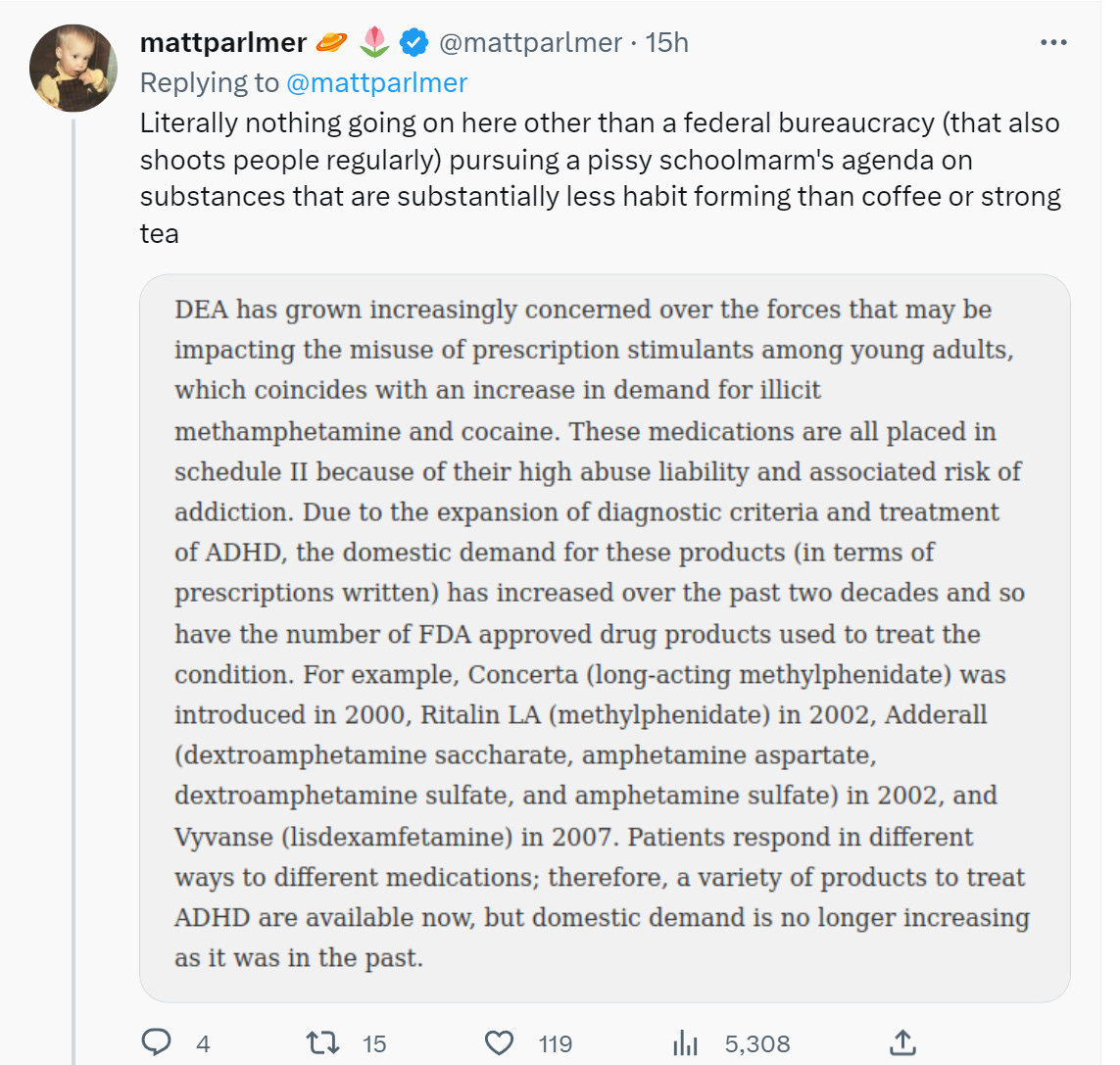
This problem by default will continue to get worse, and increasing amounts of time will be taken up, by exactly the people who need to focus and spend their time well, on securing some of the limited supply. Some will inevitably turn to black markets. We could at least have the common decency to let them bid against each other. I for one am curious how much companies would pay to ensure their workers get Adderall.
Other Medical and Research News
ACX links us to Jacob Shapiro claiming that flashing lights at the proper intervals increases learning by a factor of three (source paper). No, really, that is the claim.
“The learning rate for those locked into the right rhythm was at least three times faster than for all the other groups. When participants returned the next day to complete another round of tasks, those who learned much faster under entrainment had maintained their higher performance level.”
As Scott points out, the cost to buy the setup to try this strategy is merely hundreds of dollars, although you would still need to know how to operate the equipment. If that works, it perhaps pays for itself in one day for one student. Also if it works it would scale to everyone.
We talk about how AI or fusion power or what not would be a huge game changer. This would, if fully real, potentially be bigger, even if the effect only applied to formal learning. And there’s no reason to think this super focused state wouldn’t have tons of other uses as well. Huge if true, complete societal transformation. Can you imagine how much you would learn if you could go into triple speed at any time? How many years of schooling could be either saved or turned into actual useful knowledge and skills, dealer’s choice?
What seems to be completely missing is the proper sense of excitement. If you take this hypothesis seriously, even giving it a 1% chance it would work, you wouldn’t risk waiting around to see what happens. You wouldn’t wait for formal Proper Science to slowly study it. You’d test it, in the real world. If it works, you will know. This is not an effect size one can miss.
So I issue the challenge. Who wants to try this? I am happy to be part of this experiment. If necessary I would be happy to arrange funding.
A great illustration of how much people hate the idea of an ‘experiment.’

Oh my, without the approval of an ethics committee, some people tried to rank some other people in various criteria, including intelligence. On a spreadsheet. The horror.
You see, they were doing an experiment. And it was ‘on’ people.
Indiana lawmakers propose requiring non-profit hospitals to report the average price of every heath care service they provide. Then, if any of them exceeds 260 percent of Medicare’s price for the service, impose a fine of 10% of the hospital’s total patient-service revenue.
Given that Medicare rates cover only 53 percent of the cost of providing care, and then there are fixed costs, and some patients don’t pay their bills (can’t imagine why) there is not much margin of error, if any, left. The math seems incredibly hard.
The first twist is this price cap, as well as the price reporting, applies only to non-profits. The large for-profit hospital networks would have a large competitive advantage over non-profits. Interesting choice.
The second twist is that this is a completely insane level of fine for going over the first limit, and then essentially no further fine for going over all the limits. This presumably creates a separating equilibrium.
If you can make the ‘charge an average of exactly 259 percent more than Medicare pays, on average, for each individual service’ then maybe you can make that work. Seems extremely difficult on multiple fronts.
If you can’t, then I suppose you slap about a 20% excess charge on every bill that isn’t Medicare or Medicaid (since on the other half you’re a price taker), make sure this change is not clearly labeled as the ‘Indiana Medicare Tax Charge,’ and use the revenue to pay the tax. So the taxpayers pay the insurance companies who pay you who pays the government, who uses it to fund Medicare and pay you 53% of the cost of the treatments you provide in exchange.
Not exactly efficient, but those are the breaks, I guess.
Another fun twist is paying out tax funds to physicians in exchange for them not affiliating with hospitals? This is called ‘incentivizing independent practices.’ So the doctors who are making the most money while helping the public the least get bribed for it?
The bill also proposes giving a $1,000 tax credit for a defined amount of years to physicians who aren’t affiliated with a hospital to incentivize independent practices.
Also note the political calls to stop the ‘experiment’ social media companies are ‘running on our children.’ Same principle.
Mr. Beast paid for a thousand blind people to get surgery to help them see. Good. If your response is to attack him for this, you are a bad person.
Hospitals sometimes think three year olds are ‘too young’ to visit dying relatives? This comes from NYU Long Island, which is no slouch and certainly not cheap.
Periodic reminder that testosterone levels continue to rapidly decrease and few if any are treating this as a serious problem.
Here is a Danish study with strong echoes of the situation I encountered with colonoscopies.


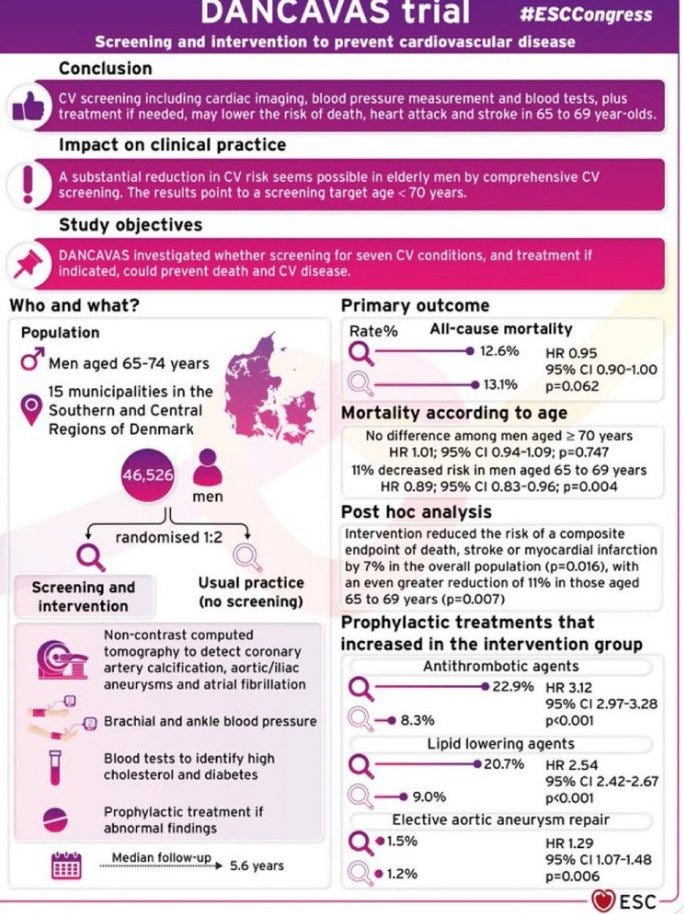

This is not a negative result so much as it is an underpowered study.
The study found a decline in mortality from 13.1% to 12.6%. That’s 4% less death, a potentially really good improvement for an invitation to a screening, depending on how much actual intervention, costs and side effects are involved. This was p=0.06, which is technically more than 0.05, so yes ‘more research is needed’ and all that but it shouldn’t be taken as evidence against treatment and diagnosis being helpful here.
ACX links to meta-analysis of CBT saying it works including as self-help unguided intervention. All the statistical evidence continues to say ‘there is this thing, it makes people better off, it’s freely available, however it’s weird and not so fun, and you’re probably not going to do it.’
ACX also links to this paper analyzing federal cancer research, which claims it is so effective it only costs $326 in federal investment cost per life-year saved. Scott Alexander suggests that if this is accurate perhaps we should be donating to this rather than anything else. That would also lead to claims of ‘for every $326 you can save a life-year!’
That makes this an excellent opportunity to explain several reasons why not.
I’ll say in advance this is based on a quick read, so it’s plausible some of these issues are my misunderstanding of what was going on, if only because it seems so stupid. If I did misunderstand one or more points here, I apologize, but the whole thing seems pretty terrible.
- The average dollar spent is going to be vastly more effective than the marginal dollar spent going forward, since the low hanging fruit will already be gone.
- Cancer treatments are neither cheap nor pleasant. The calculation here counts lives saved without counting the time and money spent on treatment. Yes, you won’t be paying that bill, but the bill is real and represents the loss of real resources that would have otherwise likely gone to other ‘life saving’ spending.
- Crowding out effects are real. At least a large portion of these findings would have happened anyway, and the Feds are taking credit for the full effect of the treatments studied.
- That’s right, this essentially counts any life saved through cancer treatment, ever.
- Study results are being translated into estimated gains at the population level, at face value. Which we all know won’t hold up in practice, it never does – they won’t work as well in the field, and also won’t be implemented where you’d want.
- Also I don’t see anything in the analysis of impact on how often the treatments actually got administered, at all? As in, maybe I’m missing something, but I can’t find the part where they check how many people actually got cancer treatments in order to estimate how many lives got saved.
- Instead, they seem to be using the formula: On the basis of a previously published method, for each trial-proven new treatment for a given type of cancer, life-years gained (LYG) at the population (Pop) level was calculated as the product of model-estimated additional life accrued to the average patient (Pt) and multiplied by the number of patients in the cancer population (NCaPop) who would benefit from the new treatment (ie, LYGPop = LYGPt × NCaPop).9.
- And then: To derive the number of patients in the cancer population to whom the new treatment would apply (NCaPop), we matched the major cancer type, stage, tumor characteristic, prior cancer, surgery, sex, and age (ie, ≥ 18 years) eligibility criteria from the clinical trial to corresponding cancer population data using the Surveillance, Epidemiology, and End Results (SEER) program.
- That’s not how many people did benefit. That’s how many people they say in theory would benefit if we gave everything to everyone.
I worry this is actually rather standard for ‘estimates of lives saved per dollar’ calculations. People get the impression ‘if you spend $326 you can save a life-year’ as if your money vanishes, the person is saved and that’s that. Whereas a lot of other people’s real resources are also being consumed that would have otherwise done good, the measurement of past effects is questionable and the forward looking marginal impacts are going to be a lot lower. And that’s in the good scenario.
8 comments
Comments sorted by top scores.
comment by DirectedEvolution (AllAmericanBreakfast) · 2023-02-09T18:00:19.833Z · LW(p) · GW(p)
So I issue the challenge. Who wants to try this? I am happy to be part of this experiment. If necessary I would be happy to arrange funding.
Edit: I spent more time reading the paper and now think this study has limited relevance for practical learning, see my reply to romeostevensit below. I'm no longer planning to invest time in this project.
I have already been considering this and would be happy to try it out. I am a biomedical engineering grad student and believe I am well positioned to get the equipment operating. I tried just setting up a strobe at 10 Hz and staring at it for a couple seconds. It's a pretty intense thing to look at. It feels "activating."
Brainstorm
I think it's probably tractable to figure out a way for people to self-test. It's self-blind compatible, since users won't know their brain frequency or phase. Potentially, a computer program could measure these outputs from the EEG, then randomly assign that day's use to be in any of the three experimental settings that show no, low, or large effects. It could put the user through one or more tasks to measure the effect, and it could be configured to report that data automatically over the long term.
I was considering the idea of creating infrastructure for users to self-test at home and then potentially report their data back to a researcher.
Logistical challenges with a distributed study like this would include:
- Sourcing EEG devices, getting users to set them up correctly, and teaching them to use the software
- We'd need to make sure the specific data necessary to obtain for this use case can reliably be obtained by a lower-end EEG headset.
- My major concern is that this study found that a 1 Hz difference between brain wave frequency and flash frequency made a huge difference to the learning rate, as did flashing at the peak vs. trough. You'd need a device capable of dealing with these frequencies and then you'd need to calibrate it, probably on a per-user basis.
- Writing software to permit measurement, display of the flash, testing of user learning and performance. If we wanted to do a distributed study in users' homes, it would need to be compatible with a range of platforms.
- If academic publishing is a desired outcome:
- Writing software to allow reporting of that data back to the researcher (or at least to the user)
- Finding an adequate number of test subjects and funding
- Writing, publishing, dealing with reviewer feedback
A more lightweight approach would be to just purchase the EEG device and figure out how to set it up to use yourself. That's probably simpler than helping a whole bunch of users figure out how to get the equipment and software working. You'd then either have to figure out how to quantify your self tests, or just stay tuned to the literature to see if this sort of approach continues to replicate and show robust effects across tests.
An even simpler approach would be to just expose yourself to 1.5 seconds of 9-11 Hz strobe daily on the presumption that sometimes, it'll happen to be sufficiently close to your actual phase and frequency that it'll create an effect, and that it's at least not hurting your learning rate. That's a big pile of assumptions and gives you no feedback, but it's very easy to do.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-02-09T19:36:33.725Z · LW(p) · GW(p)
A further thought:
Wouldn't it be neat if this light intervention could cause the phase and frequency of the person's alpha waves to change in a predictable way?
What if flashing this pattern at 11 Hz at a particular phase, for example, could cause the subject's alpha waves to change to 11 Hz and in-phase? If that in turn caused the effect on learning to improve, then you could potentially make a device like this that wouldn't require measuring the user's alpha waves. It would just synchronize the alpha waves with the flashes, enforcing the learning benefit without requiring observation. That might make this a scalable tool, since then you could have a browser app to deliver this stimulation and wouldn't require electrodes at all.
Edit: emailed the lead author to ask if this is a thing, will post a followup if I hear back
If I was interested in this line of research, that's what I'd focus on: figuring out how to control the user's alpha wave frequency and phase.
comment by romeostevensit · 2023-02-10T00:51:12.817Z · LW(p) · GW(p)
faster learning in a visual identification task (i.e. detecting targets embedded in background clutter) compared to entrainment that does not match an individual’s alpha frequency. Further, we show that learning is specific to the phase relationship between the entraining flicker and the visual target stimulus.
Doesn't sound exciting. Habituating people's attention to the right visual frequency helps them on subsequent frequency specific visual tasks.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-02-10T01:20:28.058Z · LW(p) · GW(p)
Yes, the study flickered a square at the subject's alpha wave frequency (~10 flickers/second), or about 10% out of sync. This was called "entrainment."
Then they showed one of two types of swirly dot images for 1/5th of a second, at the same pace, either synced to the peak or trough of the subjects' alpha wave.
The subjects did best at telling apart the swirly dot images if they'd gotten entrained in sync with their alpha waves AND they got shown the swirly dot images at the trough of their alpha waves.
So this isn't like "strobe yourself for 1.5 s and learn ANYTHING 3x faster!!!"
It's "there's this very specific type of visual recognition task that we can make you better at by carefully training you with brain scanners and pacing the task accordingly."
I hope it's clear this summary leaves out a ton of nuance, but I think it does a better job than other summaries I've read of representing the limitations of this study's findings for practical learning purposes.
comment by tkpwaeub (gabriel-holmes) · 2023-02-11T00:14:07.633Z · LW(p) · GW(p)
What's sorely needed is an international drug approval reciprocity treaty. A single organization, say, part of the WHO, would be tasked with periodically vetting national level food and drug approval agencies of signator countries. In exchange for this service, drugs would be instantly approved when just one country approves it.
ETA: It looks like bilateral "agreements" are a thing:
But of course that falls well short of an international treaty. And lots of bilateral agreements strikes me as o(n^2) more complicated than a hub-and-spoke framework.
And I should also add that my general vision for federalism kind of goes in both directions. Namely, I'd like it if each state could be allowed to form its own mini-FDA but the federal government's role would be to "approve the approvers"
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2023-02-11T12:39:52.853Z · LW(p) · GW(p)
Adding - does anyone else wish there was a seamless, streamlined way of recruiting more people into clinical trials so we could bring new treatments to market faster, and while we're at it at least give half the people in the trial an effective treatment?
Like, how about sn annual general consent form, directly sent to clinicaltrials.gov in exchange for a modest tax break?
comment by Alexander de Vries (alexander-de-vries) · 2023-02-10T12:00:15.852Z · LW(p) · GW(p)
ACX also links to this paper analyzing federal cancer research, which claims it is so effective it only costs $326 in federal investment cost per life saved.
They claim $326 per life-year (specifically, DALY), not per life. Huge difference!
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-02-11T03:32:56.547Z · LW(p) · GW(p)
Yes, from the results section:
The federal investment cost per life-year gained through 2020 was $326 in US dollars.
That's about $20,000 for 60 life-years.