New SARS-CoV-2 variant
post by TheMajor · 2020-12-20T21:22:54.711Z · LW · GW · 16 commentsContents
16 comments
tl; dr: there is a mutated strain of COVID that seems to spread a lot more quickly. Here is its Wikipedia page.
Last Monday (Dec 14) the UK MP's were informed of a new strain of COVID-19, named "VUI – 202012/01". This strain seems to spread more quickly than other forms of COVID-19, and wikipedia claims that this might be related to the mutated spike protein.
Two days ago (Dec 18) the NERVTAG (an expert panel advising the Chief Medical Officer of the UK, who in turn advises the UK Department of Health and Social Care) meet and release their meeting minutes, stating that:
- "Growth rate from genomic data: which suggest a growth rate of VUI-202012/01 that that is 71% (95%CI: 67%-75%) higher than other variants." [sic]
- "Studies of correlation between R-values and detection of the variant: which suggest an absolute increase in the R-value of between 0.39 to 0.93."
amongst other information on this new strain (the meeting minutes are 3 pages only so I encourage people to check them if interested).
Yesterday (Dec 19) Prime Minister Boris Johnson announced a lockdown for London, South East and East of England starting the day after (so today, Sunday), to combat the spread of this new strain.
Today (Dec 20) the European Centre for Disease prevention and Control (ECDC) released a threat assessment brief. The same day multiple countries in Europe (a quick search reveals Germany, France, Belgium, the Netherlands, Italy and Austria, but I possibly have missed others) issue travel restrictions from the United Kingdom and South Africa.
To the best of my ability to interpret the above documents it is too early to make conclusive statements about the impact this strain will have on the COVID-19 pandemic. The threat assessment brief states that "To date, there is no indication of increased infection severity observed related to the variant, but the assessment is challenged by the fact that the majority of cases were reported in people under 60 years old, who are less likely to develop severe symptoms [29].". This seems like relatively good news - so far the health impact is not noticeably worse. However, the strain is spreading like a wildfire:
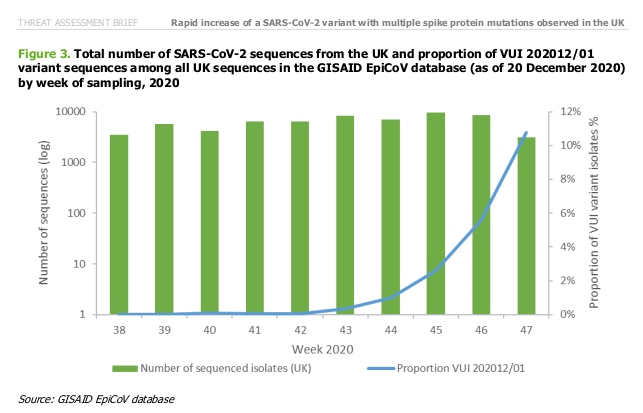
The blue line is the fraction of all reported COVID-19 cases in the UK that are VUI – 202012/01 cases. It appears to be growing exponentially, indicating that it spreads more easily than other strains (it is outcompeting them).
As stated above it is not clear what the impact of this strain will be on public health. Some questions that I would love to see discussion on include
- How likely is it that the spread of this new strain was caused by a few superspreaders, and that most of the above is blown out of proportion?
- What, uh, does the "71% higher growth rate" mean? Is this different from the R in that is also incorporates the length of the incubation period/infectious period? Can we infer the reproduction rate R from the growth rate or vice versa?
- Is there any reason to suspect this new strain might have an impact on vaccination plans? Are the currently approved vaccines (pick a country of choice to decide what this means) possibly better/worse/other against this strain?
16 comments
Comments sorted by top scores.
comment by [deleted] · 2020-12-21T05:21:15.556Z · LW(p) · GW(p)
I've become enough of an arrogant SOB evolutionary biologist poking his nose where it doesn't belong over the last year that I believe I have answers to all of these, and a few other important things to say. WHILE MAKING IT CLEAR I AM NOT A VIROLOGIST OR IMMUNOLOGIST OR EPIDEMIOLOGIST AND THAT I COULD EAT MY WORDS IN THE FUTURE, though I have been pretty good so far.
How likely is it that the spread of this new strain was caused by a few superspreaders, and that most of the above is blown out of proportion
That would make sense if the frequency was rising in early introductions or when spread was thin on the ground. Increasing fraction of the total infections while spread is already thick makes me think that there is more likely to actually be an actual effect on contagiousness. They report a decent detectable increase in genome copy number as measured by PCR and sequencing in upper respiratory samples which makes me think this is likely. More on the virology later.
What, uh, does the "71% higher growth rate" mean
TLDR: I think that it's probably barely 15% more infectious and the math of spread near equilibrium amplifies things.
I admit that I have not read all available documents in detail, but I presume that what they said means something like "if ancestor has a doubling time of X, then variant is estimated as having a doubling time of X/(1+0.71) = 0.58X"
This can only be related to a parameter like R0 in relation to how much R0 has already been reduced by behavior changes to its effective actual R since the math gets really nonlinear and I presume I am either missing their math or there will be more detailed documentation in the future. In the mean time let's run through an example.
I have seen estimates of 'generation times' for SARS-2 clustering around 5 days in the presence of all the stacked up behavior changes. Doubling time is related to the generation time and the effective replication number Re, by the equation:
doubling time = ln(2) * generation time / (Re-1)
If you have reduced the Re to 1.1 with a 5 day generation time then you get a doubling time of 35 days. If you have reduced it to 1.2 then you get a doubling time of 17 days. In the former case, if you take 35 days to 0.58*35 = 20.1 days, you get Re going from 1.1 to 1.172, only 7% higher infectiousness. In the latter case, if you take 17 days to 10 days, you get Re going from 1.2 to 1.34, a 12% increase. Presumably the base R0 increases by a similar factor.
In short, the closer you are to equilibrium when measuring the effect the larger the effect a small change in contagiousness will have. Given that compared to unmitigated situations we are pretty close to Re=1 and I never see cases doubling recently in Britain in less than two weeks, I doubt that the total factor of increase of infectiousness is actually all that large. You get a huge nonlinear effect as you move the numbers around near one, even when the total factor of increase is not huge, but mitigation increasing by only a small factor can counteract it.
Prepared to eat this, hard, if I am misinterpreting what has been said.
Is there any reason to suspect this new strain might have an impact on vaccination plans? Are the currently approved vaccines (pick a country of choice to decide what this means) possibly better/worse/other against this strain?
It is almost certain that the vaccines (all of which present exactly the same piece of the virus to the immune system) work a bit less well on this variant, but at the same time I think it changes absolutely nothing important of substance for the near future.
For now, ignore EVERYTHING except the spike protein. This lineage bears several mutations in this gene, responsible for fusing the virus to target cells and the main target of antibody responses (and a good fraction but not all of the T cell response). They are, separated thematically:
deletion 69–70
deletion 144
N501Y
A570D
D614G
P681H
T716I
S982A
D1118H
Deletion 69-70 and deletion 144 are in what's called the N-terminal domain. This is not quite the business end of the spike but is near to it and is involved in invasion to some degree via mechanisms that are not well understood. The double deletion has appeared independently several times, and seems to be helpful in becoming more invasive to human cells to some degree and also may help escape a subset of antibodies possibly as a side effect. Bit of a loooong story there I won't quite get into here. Anyway, these are in a domain that constitutes about 20% of human neutralizing antibodies and are quite possibly somewhat immunologically relevant.
N501Y& and A570D are particularly interesting because they are in the receptor binding domain that actually sticks to ACE2. In particular, N501Y has already been identified as a mutation that increases the strength of binding to the ACE2 receptor. It also functions as a known escape mutation, and the other one could as well.
An escape mutation is a mutation that causes a subset of antibodies functional against the ancestor to become inert. However, vertebrate immune systems generate a small quantity of a large number of antibodies against their targets, so generally speaking when an escape mutant comes along there are other antibodies around to take up the slack.
I have seen papers exposing large numbers of recovered human serum samples against various escape mutations. When one at a time was presented, only the weakest ~7% of responses (presumably consisting of the fewest antibody types) were affected at all and only a subset of those dropped below likely having an effect. When two escape mutations were added, it went up to about 20%, still biased strongly towards the weaker responses. But again, not all those responses dropped to zero, some just got weaker. Of note, natural responses to the virus vary in strength by a factor of TWO HUNDRED, and a weak response is very different from a strong response.
I would expect that each escape mutation you add makes the fraction of responses that have a problem go up, and the size of the problem to go up. We are talking 2-4 escape mutations here, so there is likely some immunological impact.
D614G is one of the first mutations in the history of this virus from January and is likely associated with a mild increase in contagiousness to humans, via a slight change in the geometry of the trimer that is completely immunologically irrelevant.
The rest of the mutations are in parts of the spike that are a lot less likely to be immunologically relevant, even if maybe one or two of them changes something about the arrangement of the three spike monomers in the trimer that could theoreticaly affect binding or synergize with others to affect binding efficacy or shedding of the S1 domain from the protein or any number of other things, but dont necessarily and a bunch of them are probably just silent.
Given the sheer strength of responses created by immunization so far, as strong or even stronger than the very strongest natural responses, I find myself doubting that even multiple escape mutations will be able to break through the response to the vaccines. I would presume they would make the speed with which immunization immunity decays increase, and mean that fewer additional mutations on top of this base would be needed to properly evade it.
But we will have do deal with this anyway! It is now known that the human coronaviruses do evolve on a timescale of circa a decade to be able to escape previous antibody responses, we just constantly get exposed to these new changes as they barely break through into us. Over a timescale of somewhere in the single digit years, I would presume that this virus would evolve to escape immunity be it natural or vaccinated. And there is a hell of a difference between getting infected when you are completely naive and have never seen anything like it, and when you just barely can be broken through into and you are still generating antibodies and T cells that both are still reactive, even if it can slip past well enough. A vaccination rolled out to prevent this first burn through a naive population is vital, and we will see if we can keep ahead of eventual evolution with later boosters or if we just live in equilibrium with another respiratory virus which will not be like the current situation.
*****
This is where I nerd out randomly on something else. Almost nobody is commenting on the fact that this lineage also contains a nonsense mutation in ORF8!
ORF8, the 8th identifiable reading frame in the genome, is one of the several tricksy accessory proteins that the virus uses to subvert and confuse the adaptive and innate immune system both - in particular, it gums up the MHC complex that body cells use to present viral protein fragments to the adaptive immune system, both to train it upon first exposure and to tag a cell for destruction by eventual trained T cells. This and other accessory proteins are almost certainly a large fraction of why this disease is so immunologically weird and causing such messed up immune responses in severe cases.
A nonsense mutation is a mutation that turns one of the codons that codes for an amino acid into a STOP sign, preventing the production of everything downstream of that position in the protein. This nonsense mutation is practically right at the beginning of the protein, so functionally speaking it is obliterated.
This protein has, in the various lineages around the world, accumulated less impactful mutations at a faster rate than almost any other position in the genome, indicating that it is not under a lot of selective pressure to be maintained. The accessory proteins are probably needed to replicate in bats, whose immune systems are tuned differently than ours - their antiviral interferon responses are on a freaking hair trigger and their inflammatory responses are damped incredibly low. They are probably a lot less necessary in other mammals. A similar protein literally fell to pieces over the course of the first SARS outbreak twenty years ago, and multiple lineages have been seen with big deletions in this gene over the course of the SARS-2 outbreak but none of them became particularly common, and indeed several are basically confirmed to have died out entirely.
If NOTHING else, this lineage proves that the loss of the tricky accessory proteins is not a death sentence for the virus and the possibility of them being lost over time in the future remains. This may be a mechanism of eventual self-attenuation, if previous research in Singapore indicating that the ORF8-deleted lineages were significantly less likely to send people to hospitals pans out (there was not enough research for me to be confident of this buty there were some reports that really need to be followed up on). It is possible that this utterly broken ORF8 basically 'hitchhiked' alongside the spike protein changes that are likely responsible for increased transmissibilty, even if it is mildly harmful to the virus. This virus does not seem to be doing recombination in the human population, so such evolutionary hitchhiking can become an important force.
Replies from: SDM, billmei, avturchin, brianwang712↑ comment by Sammy Martin (SDM) · 2020-12-21T20:22:49.908Z · LW(p) · GW(p)
EDIT: PHE has seemingly confirmed the higher estimate for change in R, ~65%. https://t.co/r6GOyXFDjh?amp=1
What, uh, does the "71% higher growth rate" mean
TLDR: I think that it's probably barely 15% more infectious and the math of spread near equilibrium amplifies things.
I admit that I have not read all available documents in detail, but I presume that what they said means something like "if ancestor has a doubling time of X, then variant is estimated as having a doubling time of X/(1+0.71) = 0.58X"
In the meeting minutes, the R-value (Rt) was estimated to have increased by 0.39 to 0.93, the central estimate being +0.66 - 'an absolute increase in the R-value of between 0.39 to 0.93'. Then we see 'the growth rate is 71% higher than other variants'. You're right that this is referring to the case growth rate - they're saying the daily increase is 1.71 times higher, possibly?
I'm going to estimate the relative difference in Rt of the 2 strains from the absolute difference they provided - the relative difference in Rt (Rt(new covid now)/Rt(old covid now)) in the same region, should, I think, be the factor that tells us how more infectious the new strain is.
We need to know what the pre-existing, current, Rt of just the old strain of covid-19 is. Current central estimate for covid in the UK overall is 1.15. This guess was that the 'old covid' Rt was 1.13.
(0.66+1.13)/1.13 = 1.79 (Rt of new covid now)/1.13(Rt of old covid now) = 1.58, which implies that the Rt of the new covid is currently 58% higher than the old, which should be a constant factor, unless I'm missing something fundamental. (For what it's worth, the Rt in london where the new strain makes up the majority of cases is close to that 1.79) value). So, the Rt and the R0 of the new covid is 58% higher - that would make the R0 somewhere around 4.5-5.
Something like that rough conclusion was also reached e.g. here or here or here or here or here, with discussion of 'what if the R0 was over 5' or '70% more infectious' or 'Western-style lockdown will not suppress' (though may be confusing the daily growth rate with the R0). This estimate from different data said the Rt was 1.66/1.13 = 47% higher which is close-ish to the 58% estimate.
{kind=link}
I may have made a mistake somewhere here, and those sources have made the same mistake, but this seems inconsistent with your estimate that the new covid is 15% more infectious, i.e. the Rt and R0 is 15% higher not 58% higher.
This seems like a hugely consequential question. If the Rt of the new strain is more than ~66% larger than the Rt of the old strain, then March-style lockdowns which reduced Rt to 0.6 will not work, and the covid endgame will turn into a bloody managed retreat, to delay the spread and flatten the curve for as long as possible while we try to vaccinate as many people as possible. Of course, we should just go faster regardless:
Second, we do have vaccines and so in any plausible model faster viral spread implies a faster timetable for vaccine approval and distribution. And it implies we should have been faster to begin with. If you used to say “we were just slow enough,” you now have to revise that opinion and believe that greater speed is called for, both prospectively and looking backwards. In any plausible model.
If you are right then this is just a minor step up in difficulty.
Tom Chivers agrees with you, that this is an 'amber light', metaculus seems undecided (probability of UK 2nd wave worse than 1st; increased by 20% to 42% when this news appeared), some of the forecasters seem to agree with you or be uncertain.
Replies from: None↑ comment by [deleted] · 2020-12-21T20:41:54.977Z · LW(p) · GW(p)
Taking an effective R value from ~1.2 to ~1.8 would WAY more than double the growth rate. I really don't think that this makes sense, and that number for an increased R value seems like it should be referring to the unmitigated R0 value that is then reduced by behavioral interventions.
EDIT: doubling time would go from 17 days to 4 days (!) with the above change of numbers. This doesn't fit given what is currently observed.
An R0 going up by ~0.4-0.9 also fits well with my imputation of a ~15% increase in infectiousness, as estimates of an unmitigated R0 range from circa 3 to 5.
I think this is what happens when people don't show their work.
Replies from: SDM↑ comment by Sammy Martin (SDM) · 2020-12-21T20:54:51.473Z · LW(p) · GW(p)
EDIT: doubling time would go from 17 days to 4 days (!) with the above change of numbers. This doesn't fit given what is currently observed.
The doubling time for the new strain does appear to be around 6-7 days. And the doubling time for London overall is currently 6 days.
If the mitigated Rt is +0.66 and the growth rate is +71% figures are inconsistent with each other as you say, then perhaps the second is mistaken and +71% means that the Rt is 71% higher, not the case growth rate, which is vaguely consistent with the Rt is +58% higher estimate from the absolute increase. Or "71% higher daily growth rate" could be right and the +0.66 could be referring to the R0, as you say.
This does appear to have been summarized as 'the new strain is 71% more infectious' in many places, and many people have apparently inferred the R0 is >50% higher - hopefully we're wrong.
Computer modelling of the viral spread suggests the new variant could be 70 per cent more transmissible. The modelling shows it may raise the R value of the virus — the average number of people to whom someone with Covid-19 passes the infection — by at least 0.4,
I think this is what happens when people don't show their work.
So either 'R number' is actually referring to R0 and not Rt, or 'growth rate' isn't referring to the daily growth rate but to the Rt/R0. I agree that the first is more plausible. All I'll say is that a lot of people are assuming the 70% figure or something close to it is a direct multiplier to the Rt, including major news organizations like the Times and Ft. But I think you're probably right and the R0 is more like 15% larger not 58/70% higher.
EDIT: New info from PHE seems to contradict this, https://t.co/r6GOyXFDjh?amp=1
Replies from: None↑ comment by [deleted] · 2020-12-21T20:57:33.569Z · LW(p) · GW(p)
Yeah I was going with my quick and dirty numbers from earlier. Way I see it what's probably happening is that doubling time for Britain as a whole has been ~2 weeks both about a month ago and recently (eyeballing graph from worldometer), and you are probably talking about a new doubling time of ~1 week for this variant under identical conditions.
Redoing math for a two week starting doubling time and the stated change in doubling time you get a R value going from ~1.25 to just under or circa 1.5, so basically similar order.
News sources do not use precise language, and precise language matters here.
Replies from: SDM↑ comment by Sammy Martin (SDM) · 2020-12-22T00:00:04.400Z · LW(p) · GW(p)
Update: this from public health England explicitly says Rt increases by 0.57, https://twitter.com/DevanSinha/status/1341132723105230848?s=20
"We find that Rt increases by 0.57 [95%CI: 0.25-1.25] when we use a fixed effect model for each area. Using a random effect model for each area gives an estimated additive effect of 0.74 [95%CI: 0.44- 1.29].
an area with an Rt of 0.8 without the new variant would have an Rt of 1.32 [95%CI:1.19-1.50] if only the VOC was present."
But for R, if it's 0.6 not 0.8 and the ratio is fixed then another march style lockdown in the UK would give R = 0.6 *(1.32/0.8)= 0.99
Replies from: TheMajor↑ comment by TheMajor · 2020-12-22T11:07:11.225Z · LW(p) · GW(p)
I've been trying to understand this discussion (and I agree that this is one of the central questions for the model of how things will progress from here, in particular if March-style lockdowns will be sufficient or not to halt the spread of this strain). But now I'm mainly confused - isn't such a dramatic increase in Rt incompatible with the slower increase in the graph, as pointed out by CellBioGuy?
Edit: I've read yesterday's PHE investigation report, and they do explicitly confirm it is an increase of over +0.5 to the Rt under the conditions in England in weeks 44-49 of this year. So this seems like the bad possible interpretation, where it really does spread significantly more.
↑ comment by billmei · 2020-12-30T20:40:37.264Z · LW(p) · GW(p)
In response to "What does 71% higher growth rate mean?", I made a comment in this thread [LW(p) · GW(p)] going through the calculations in more detail.
TL;DR: it appears "up to 70% more infectious" is based on observed data, so that if you previously observed an of 0.8, you should expect to observe a new of somewhere between 1.0 and 1.4 with the new strain, ceteris paribus.
Edit: Not sure what is the etiquette around cross-posting comments, mods feel free to delete this duplicated comment if necessary.
↑ comment by avturchin · 2020-12-21T11:50:30.824Z · LW(p) · GW(p)
It looks like that not only the share of infections by new virus, but the total number of infection is also rising. UK had record 35k infections yesterday. Netherlands has a spike of infections from 5k to 14k during December. Thus even if this virus is not deadly per se, it will put more pressure on the medical system and will turn deadlier at the end.
↑ comment by brianwang712 · 2020-12-22T23:13:37.518Z · LW(p) · GW(p)
Anyway, these are in a domain that constitutes about 20% of human neutralizing antibodies and are quite possibly somewhat immunologically relevant.
Can you point to where I can find more about this estimate? I'm starting to think of the NTD as more immunodominant than that. E.g., out of 19 potently nAbs isolated here, about half were RBD-targeted and half were NTD-targeted. Here you see similar or more NTD-targeted antibodies in the convalescent plasma of 2 patients than RBD-targeted antibodies (both are outnumbered by anti-S2 antibodies, but I'm—perhaps naively—assuming those are mostly non-neutralizing). Deletions in the NTD also seem to be selected for in response to immune pressure (e.g., in response to convalescent plasma therapy, in persistently infected patients).
In particular, N501Y has already been identified as a mutation that increases the strength of binding to the ACE2 receptor. It also functions as a known escape mutation
Good news — maybe N501Y doesn't confer escape from neutralization.
I have seen papers exposing large numbers of recovered human serum samples against various escape mutations. When one at a time was presented, only the weakest ~7% of responses (presumably consisting of the fewest antibody types) were affected at all and only a subset of those dropped below likely having an effect. When two escape mutations were added, it went up to about 20%, still biased strongly towards the weaker responses. But again, not all those responses dropped to zero, some just got weaker.
I feel like I've seen the paper you're referencing but can't seem to find it now. In any case, I've also been surprised by other papers showing large impacts of single mutations against polyclonal sera. For example, the 69/70 deletions (in combination with the maybe-irrelevant D796H) drop neutralization activity against 3 high titer convalescent plasma samples by >50% (table 1, figure 4C here). Also, several variants—of note, especially E484K, found in the South African variant—seem to drop neutralization activity of convalescent sera, including some that are higher titer, several-fold (Fig 5A here). I used to have more faith in the polyclonal response but I'm starting to question it a bit.
comment by Douglas_Knight · 2020-12-28T03:35:22.357Z · LW(p) · GW(p)
How likely is it that the spread of this new strain was caused by a few superspreaders, and that most of the above is blown out of proportion?
The probability is basically zero. But the question is whether the obvious hypothesis is false, not whether a particular alternate hypothesis is true. There are many alternate hypotheses more likely than that, and most important the final bucket of "other," hypotheses that I have not thought of. Here are a few suggestions I have heard: (1) It is biologically different and spreads easily in children, but if they closed the schools, it would be negligibly different. (2) Measurement error. 2a: All sars2 produces RNA after infectiousness is over, effectively false positives and maybe this produces lots of RNA for much longer, effectively higher false positives and more lagging signal. 2b: It is mainly detected by applying the usual 3 tests for sars2 and failing a particular one. So it is inherently a noisier test, although it is not at all clear how this could produce the observed pattern.
Replies from: TheMajor↑ comment by TheMajor · 2020-12-28T08:36:19.766Z · LW(p) · GW(p)
Your point on alternative hypotheses is well taken, I only mentioned the superspreader one since that was considered the main possibility for strong relative growth of one variant over another without increased infectiousness. Could you expand on the likelihood of any of these being true/link to discussion on them?
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2020-12-28T15:52:08.795Z · LW(p) · GW(p)
If you make any of these hypotheses precise enough to calculate, then I don't think that they are likely enough to be worth calculating. The point was just to give suggest how big the space of unknown unknowns is. I think you need an outside view to estimate it. You might hope to get that from the virologists, but they are dismissing it as a "founder effect" which is even more specific, rather than accepting the ignorance of an outside view.
I think I got them all from Francois Balloux, though I'm not sure what he was saying and I may have interpolated a lot of detail. I got 2a and maybe 1 from here. 2b is from here, a response to the first thread. Added: actually, I think I got 2a from the "Does it matter" video, which was generally hostile to reason and knowledge epidemiology, but did suggest something like this at the end.
comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-21T00:58:44.192Z · LW(p) · GW(p)
From Ewan Birney, deputy director general of the European Molecular Biology Laboratory and joint director of its European Bioinformatics Institute in Cambridge:
Birney said the vaccines have been tested with many variants of the virus circulating. “So there is every reason to think that the vaccines will still work against this new strain, though obviously that needs to be tested thoroughly.”
comment by SoerenMind · 2020-12-21T19:12:54.793Z · LW(p) · GW(p)
Some expert commentary here: https://www.sciencemag.org/news/2020/12/mutant-coronavirus-united-kingdom-sets-alarms-its-importance-remains-unclear
Noteworthy:
- We previously thought a strain from Spain was spreading faster than the rest but it was just because og people returning from holiday in Spain.
- Chance events can help a strain spread faster.
- The UK (and Denmark) do more gene sequencing than other countries - that may explain why they picked up the new variant first.
- The strain has acquired 17 mutations at once which is very high. Not clear what that means.
↑ comment by [deleted] · 2020-12-21T19:18:26.501Z · LW(p) · GW(p)
The spectrum and rate of excess mutations (assuming they all came in one step) is similar to what has been recorded elsewhere in immunocompromised people chronically infected for a month or two straight, in which there's more time for multiple lineages to coexist in the same body and compete with selection against each other and a longer time with high viral numbers without transmission bottlenecks.