UPDATE 7/21/2021: As you doubtless know at this point, it was not over. Given the visibility of this post, I'm going to note here at the top that the prediction of a potential large wave of infections between March and May did not happen, no matter what ultimately happens with Delta (and the prediction was not made with Delta in mind anyway, only Alpha). Some more reflections on that at the bottom of this post here [LW · GW].
A year ago, there were reports coming out of China about a new coronavirus. Various people were saying things about exponential growth and the inevitability of a new pandemic, and urging action be taken. The media told us it was nothing to worry about, right up until hospitals got overwhelmed and enough people started dying.
This past week, it likely happened again.
A new strain of Covid-19 has emerged from southern England, along with a similar one in South Africa. The new strain has rapidly taken over the region, and all signs point to it being about 65% more infectious than the old one, albeit with large uncertainty and error bars around that.
I give it a 70% chance that these reports are largely correct.
There is no plausible way that a Western country can sustain restrictions that can overcome that via anything other than widespread immunity. This would be the level required to previously cut new infections in half every week. And all that would do is stabilize the rate of new infections.
Like last time, the media is mostly assuring us that there is nothing to worry about, and not extrapolating exponential growth into the future.
Like last time, there are attempts to slow down travel, that are both not tight enough to plausibly work even if they were implemented soon enough, and also clearly not implemented soon enough.
Like last time, no one is responding with a rush to get us prepared for what is about to happen. There are no additional pushes to improve our ability to test, or our supplies of equipment, or to speed our vaccine efforts or distribute the vaccine more efficiently (in any sense), or to lift restrictions on useful private action.
Like last time, the actions urged upon us to contain spread clearly have little or no chance of actually doing that.
The first time, I made the mistake of not thinking hard enough early enough, or taking enough action. I also didn’t think through the implications, and didn’t do things like buying put options, even though it was obvious. This time, I want to not make those same mistakes. Let’s figure out what actually happens, then act upon it.
We can’t be sure yet. I only give the new strain a 70% chance of being sufficiently more infectious than the old one that the scenario fully plays out here in America before we have a chance to vaccinate enough people. I am very willing to revise that probability as new data comes in, or based on changes in methods of projection, including projections of what people will decide to do in various scenarios.
What I do know is we can’t hide our heads in the sand again. Never again. When we have strong Bayesian evidence that something is happening, we need to work through that and act accordingly. Not say “there’s no proof” or “we don’t know anything yet.” This isn’t about proof via experiment, or ruling out all possible alternative explanations. This is about likelihood ratios and probabilities. And on that front, as far as I can tell, it doesn’t look good. Change my mind.
The short term outlook in America has clearly stabilized, with R0 close to 1, as the control system once again sets in. Cases and deaths (and test counts) aren’t moving much. We have a double whammy of holidays about to hit us in Christmas and New Year’s, but after that I expect the tide to turn until such time as we get whammied by a new more infectious strain.
Instead of that being the final peak and things only improving after that, we now face a potential fourth wave, likely cresting between March and May, that could be sufficiently powerful to substantially overshoot herd immunity.
Let’s run the numbers.
The Numbers
Predictions
Last week’s prediction: 13.1% positive rate on 11.5 million tests, and an average of 2,850 deaths per day.
Results: 13.7% positive rate on 10.7 million tests, with an average of 2,677 deaths.
We didn’t test substantially more people than last week, and the positive test percentage didn’t fall much, and the death rate didn’t rise much. Everything in a holding pattern. Some of that could be pending Christmas issues. Fool me twice, and all that.
This next week is Christmas plus New Year’s, so reporting issues are inevitable. Another week for wide error bars.
Prediction: 13.6% positive rate on 10.1 million tests, and an average of 2,500 deaths per day.
Note that I expect the deaths decline, at least, to be about reporting rather than about actual numbers, which I don’t think will start to decline much for a bit longer.
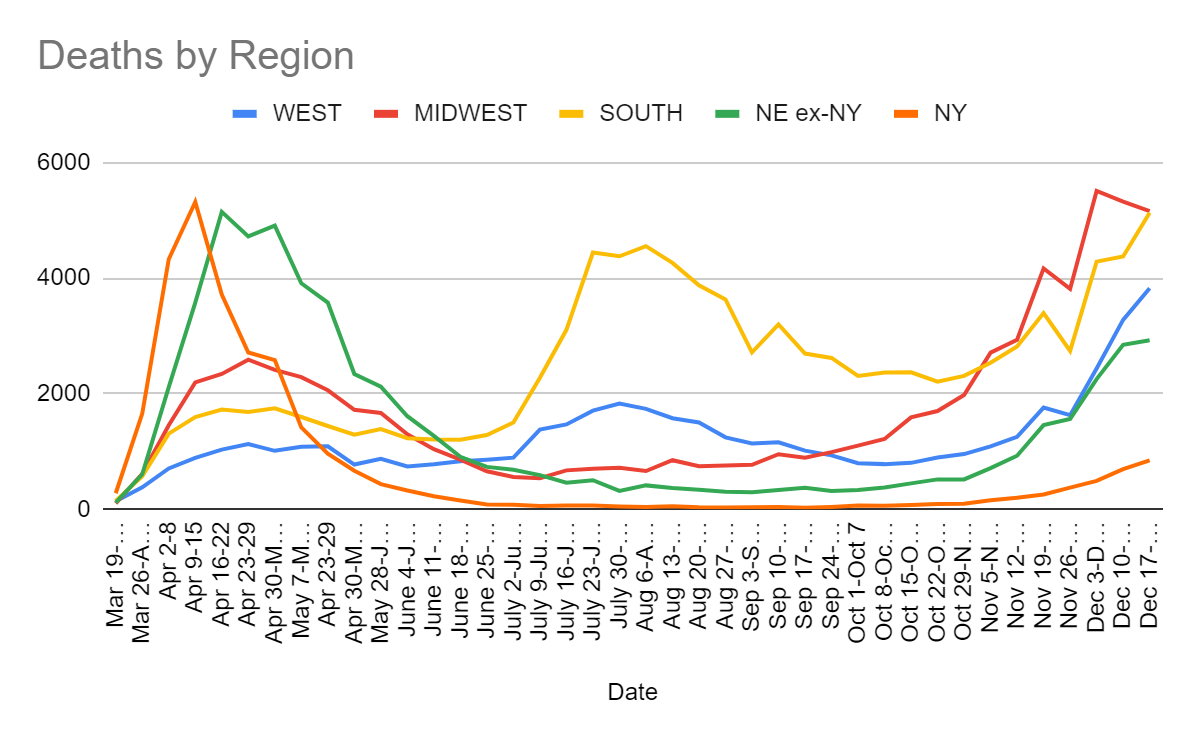
Deaths
Date
WEST
MIDWEST
SOUTH
NORTHEAST
Oct 22-Oct 28
895
1701
2208
612
Oct 29-Nov 4
956
1977
2309
613
Nov 5-Nov 11
1089
2712
2535
870
Nov 12-Nov 18
1255
2934
2818
1127
Nov 19-Nov 25
1761
4169
3396
1714
Nov 26-Dec 2
1628
3814
2742
1939
Dec 3-Dec 9
2437
5508
4286
2744
Dec 10-Dec 16
3278
5324
4376
3541
Dec 17-Dec 23
3826
5158
5131
3772
Death rates didn’t rise all that much due partly to the decline in the Midwest, but they are still up in the other three regions and substantially in the West and South. It seems clearly a few weeks too early to hit peak deaths based on when we had peak infections.
Going forward, the vaccine will start to be effective for those who get infected next week, so to the extent we are protecting residents of nursing homes, we’ll see that effect in the death rate start to be noticable in late January. I expect deaths to be in decline by then.
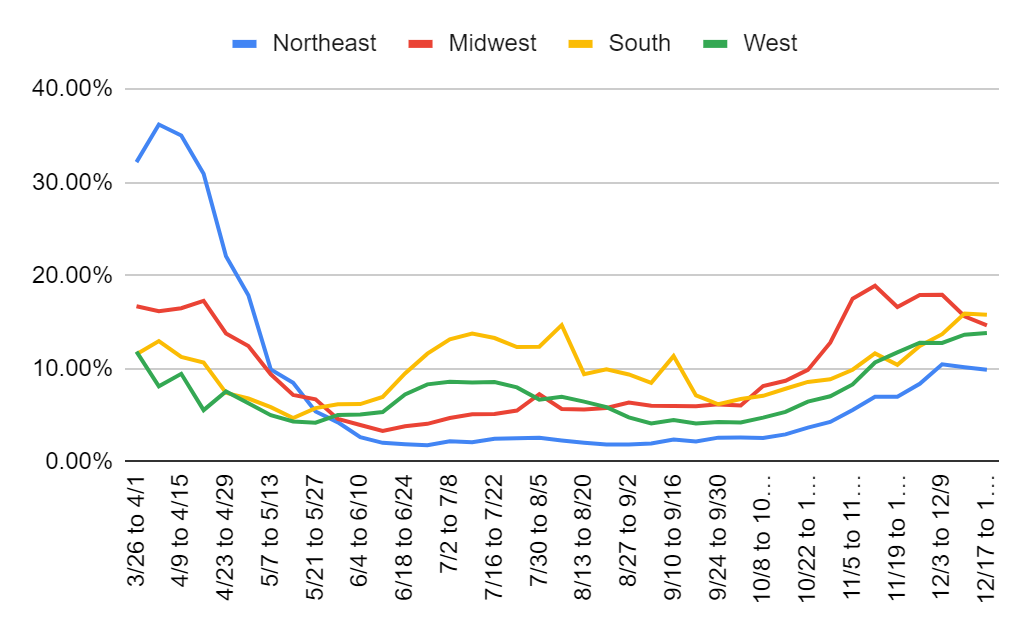
Positive Test Percentages
Percentages
Northeast
Midwest
South
West
10/22 to 10/28
3.68%
9.87%
8.58%
6.46%
10/29 to 11/4
4.28%
12.79%
8.86%
7.04%
11/5 to 11/11
5.56%
17.51%
9.89%
8.31%
11/12 to 11/18
6.99%
18.90%
11.64%
10.66%
11/19 to 11/25
7.00%
16.62%
10.41%
11.75%
11/26 to 12/2
8.38%
17.90%
12.45%
12.79%
12/3 to 12/9
10.47%
17.94%
13.70%
12.76%
12/10 to 12/16
10.15%
15.63%
15.91%
13.65%
12/17 to 12/23
9.88%
14.65%
15.78%
13.82%
Quiet on all fronts. Midwest clearly in slow decline, looks like other regions also ready to follow, as soon as we get past the holidays. There’s also an overall one-time bump coming of unknown size, but after that we should be clear until the new English or South African strain becomes a problem.
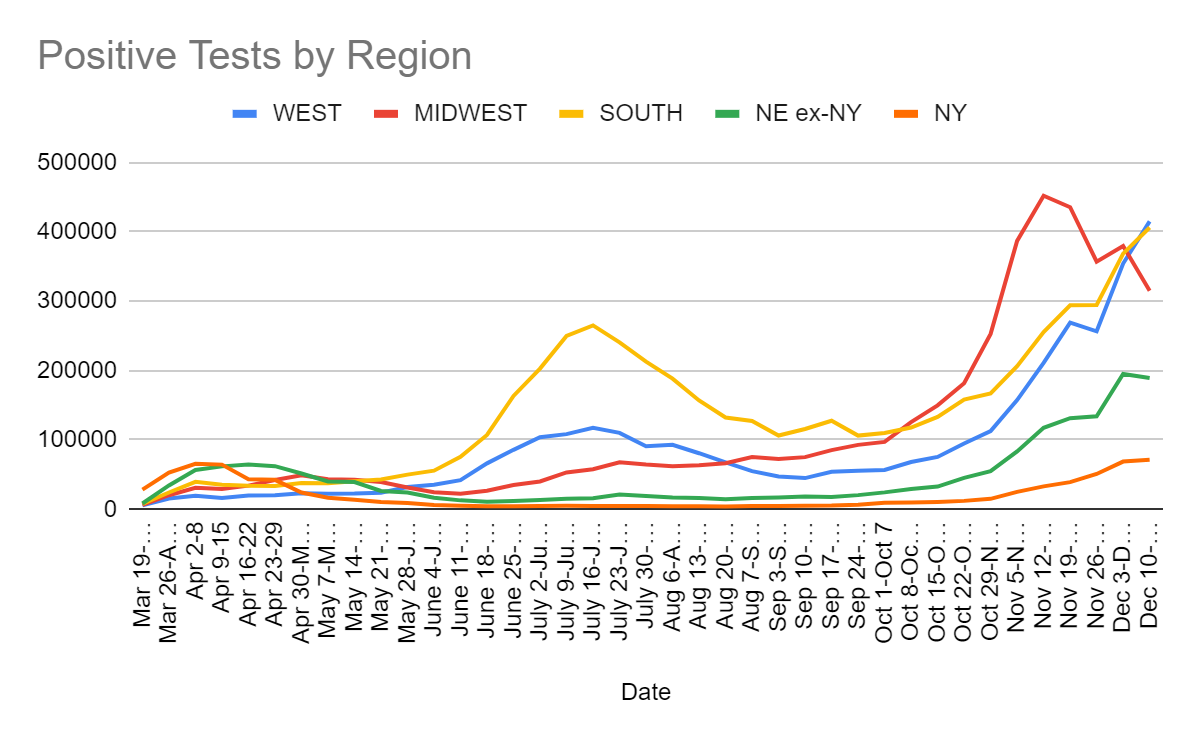
Positive Tests
Date
WEST
MIDWEST
SOUTH
NORTHEAST
Oct 22-Oct 28
94983
181881
158123
57420
Oct 29-Nov 4
112684
252917
167098
70166
Nov 5-Nov 11
157495
387071
206380
108581
Nov 12-Nov 18
211222
452265
255637
150724
Nov 19-Nov 25
269230
435688
294230
170595
Nov 26-Dec 2
256629
357102
294734
185087
Dec 3-Dec 9
354397
379823
368596
263886
Dec 10-Dec 16
415220
315304
406353
260863
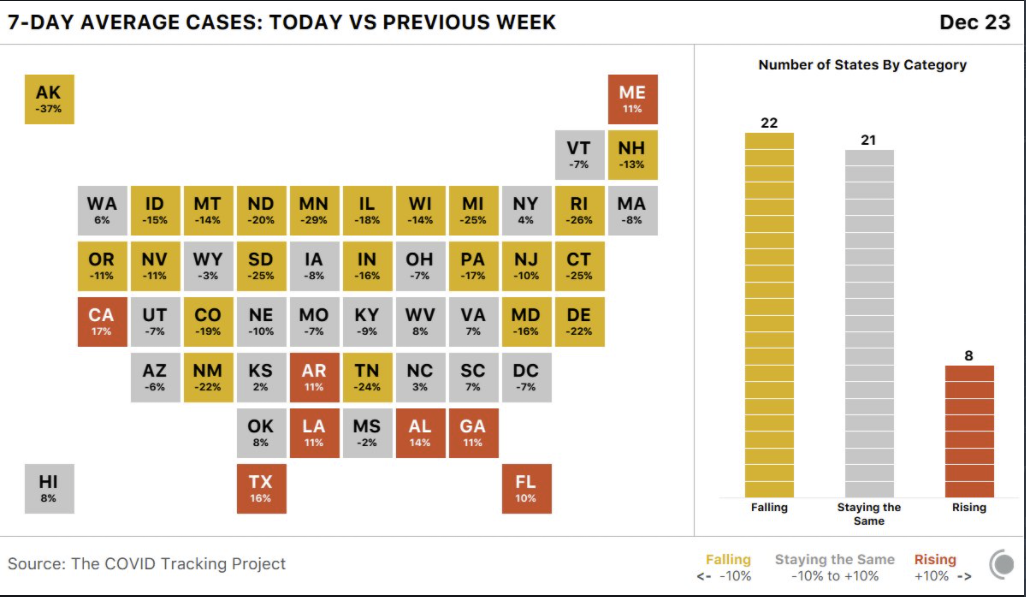
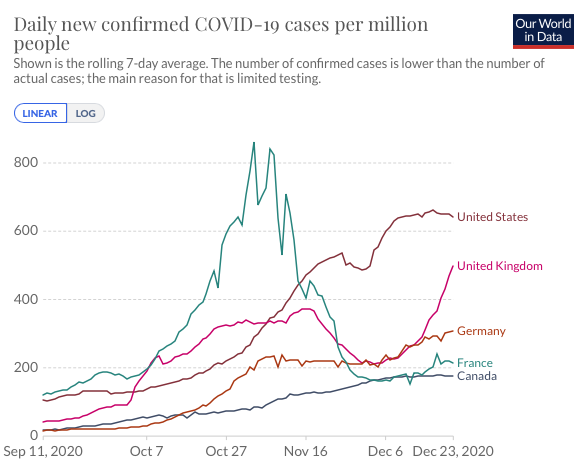
Also, this seems like a nice graphic:
But it’s also potentially misleading, because the increased cases in the deep South are mostly increased testing. The California increase is largely real. It would make sense that California would be the place that has stalled its crisis for the longest, between not having cold weather and imposing draconian restrictions all year, and so perhaps it’s finally time for them to face the music.
Test Counts
Date
USA tests
Positive %
NY tests
Positive %
Cumulative Positives
Oct 15-Oct 21
6,461,028
6.4%
865,890
1.2%
2.52%
Oct 22-Oct 28
6,943,470
7.5%
890,185
1.4%
2.67%
Oct 29-Nov 4
7,349,648
9.5%
973,777
1.6%
2.89%
Nov 5-Nov 11
8,285,878
10.7%
1,059,559
2.4%
3.16%
Nov 12-Nov 18
9,033,621
12.4%
1,155,670
2.9%
3.50%
Nov 19-Nov 25
10,415,393
11.8%
1,373,751
2.9%
3.87%
Nov 26-Dec 2
9,741,057
11.7%
1,287,010
4.0%
4.22%
Dec 3-Dec 9
10,458,644
13.9%
1,411,142
4.9%
4.66%
Dec 10-Dec 16
10,694,845
13.8%
1,444,725
4.9%
5.11%
Dec 17-Dec 23
10,710,356
13.7%
1,440,770
5.1%
5.56%
This is the silent scandal no one is talking about. Why are we no longer expanding testing? It seems clear now that our capacity hasn’t been expanding in December. It’s clear that demand greatly exceeds supply, and that more testing would be a huge help. When things were improving slowly, at least they were improving. Now it looks like we are stalled out, well short of where we need to be. Vaccinations are important, but until we get a lot farther along on those, so are tests.
Covid Machine Learning Projections
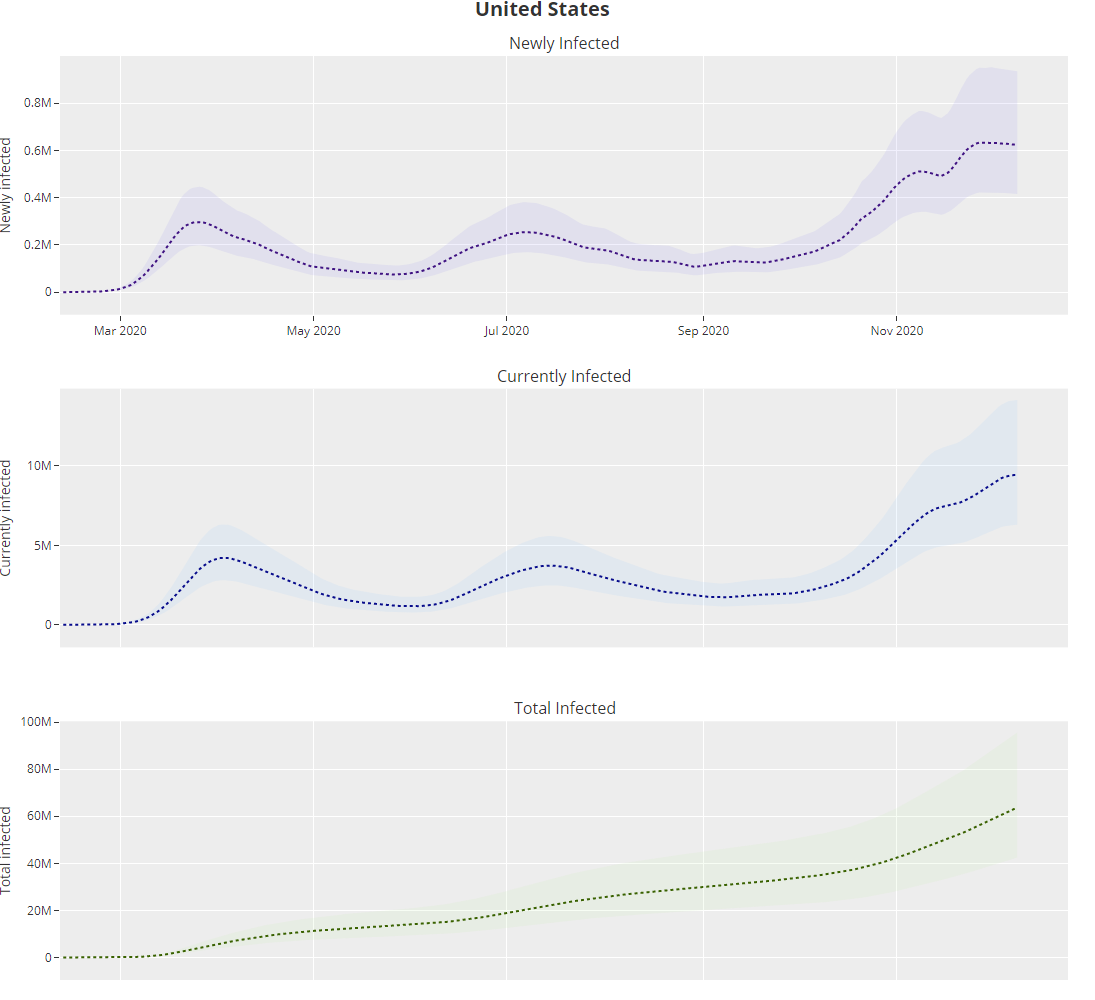
Machine learning projections say infections have been static since about November 25, which mostly matches the testing data. We can assume that the projections will keep saying similar things for the next two weeks.
Their predicted total infected is up to 19.2% on December 9, stabilized at 623k new infections per day. The total is up from 17.9% on December 2. As a reminder, I consider these lower bound estimates.
The immunity effects here compound fast. Even if you assume people get infected completely at random, going from 17.9% to 19.2% immune reduces R0 by 1.6%, which reduces infection levels by that much every five days or so, or 9% per month, and we’re introducing that effect permanently each week. After a month of this level of effect, you’ll see a 16% decline from newly immune people alone. After two months, infection levels would be cut in half.
Selection of who gets infected makes the effect bigger, and also we get to add vaccinations.
Of course, the control systems ensure it does not work that way, as people will notice things improving and take more risks, but it’s worth noting that things will start rapidly getting better if we can only hold onto our current levels of prevention, and let immunity from all sources do the job from there.
Europe
Going to use short-dated graphs to improve readability. If you want the longer view you can get it at OurWorldInData, or previous weekly Covid posts.
Sh
The positive test percentages chart is so incomplete and all over the place that I’m going to stop posting it, but you can go to the source if you still want it.
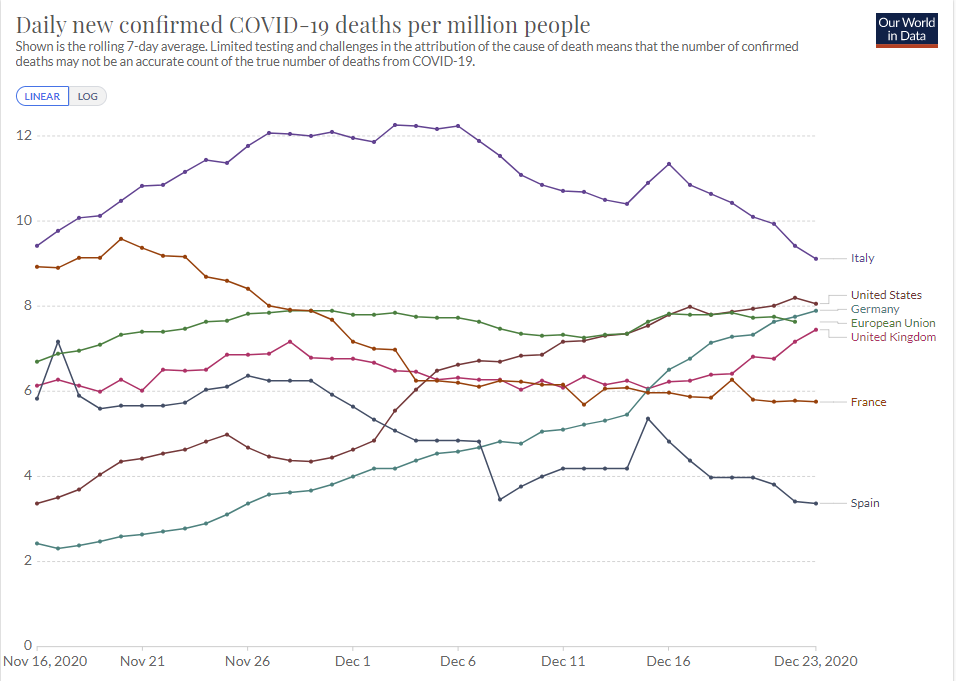
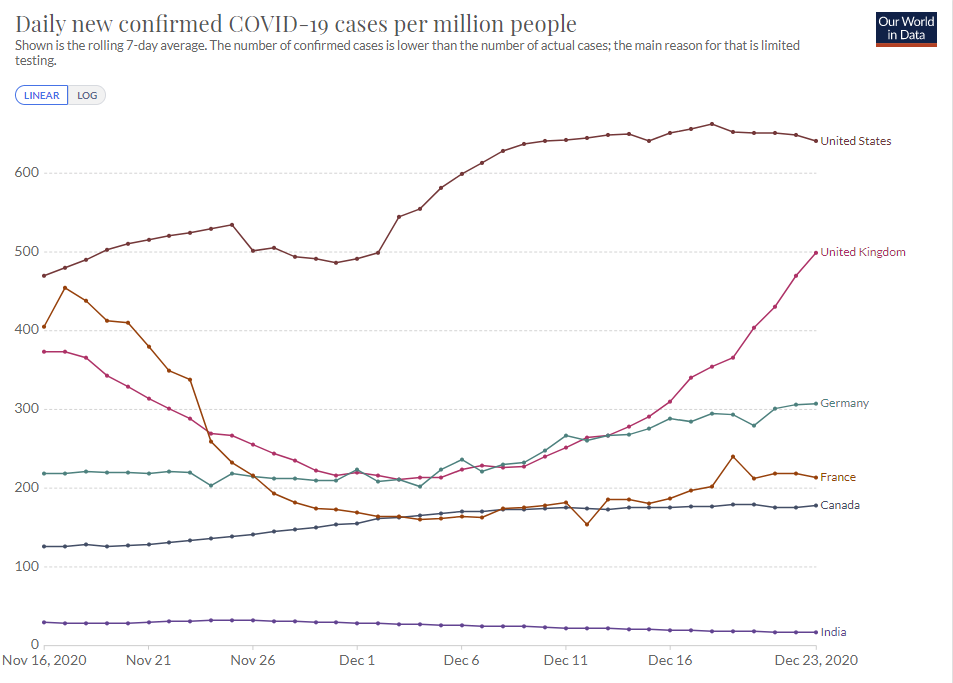
Deaths in Europe continue to run close to those in the United States, suggesting the Europeans are finding cases less often than we are, or have worse medical care or are worse at protecting vulnerable populations.
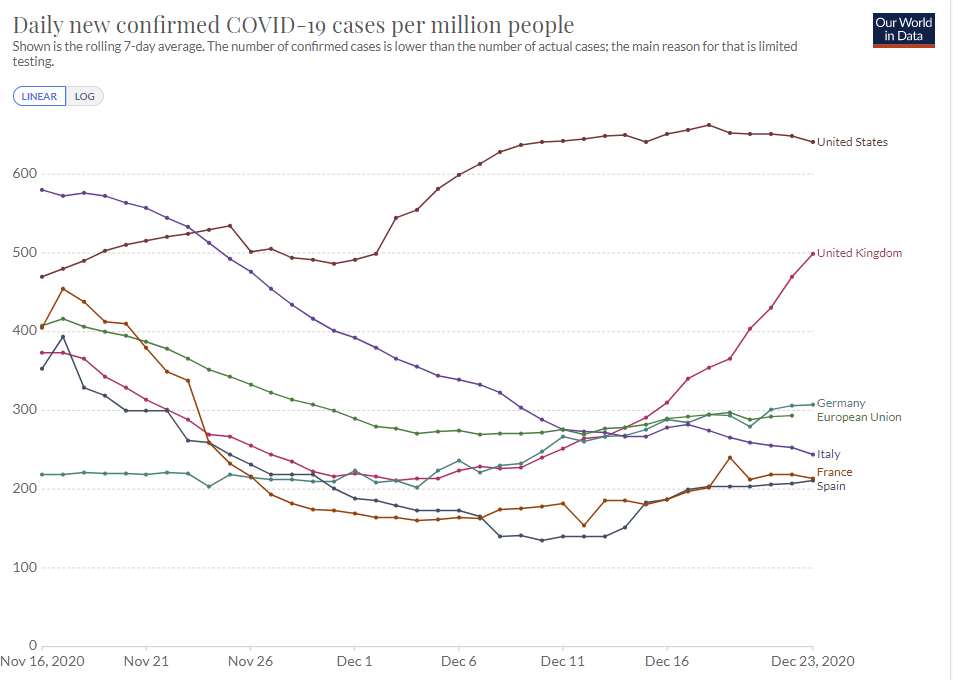
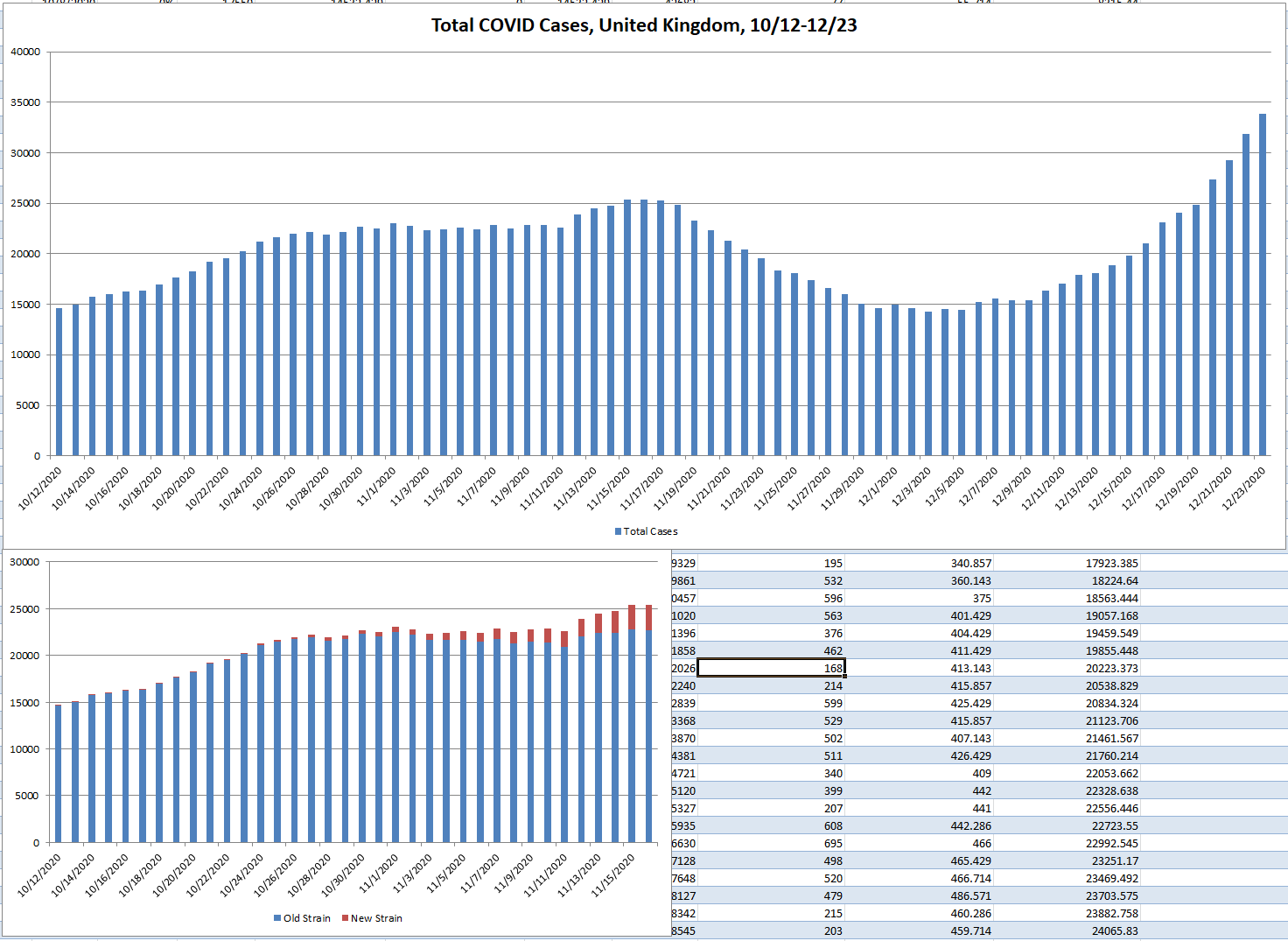
Then there’s that United Kingdom graph going rapidly vertical in infections. Turns out, there’s a reason, and it’s not that they lifted their restrictions…
The English Strain
The big newsthis week is that England has identified a new strain of Covid-19 that is ‘up to 70% more infectious’. The new strain dominates in southern England, including London, and the graphs tell a rather clear story.
Oh no.
You’re probably wondering the same question I was when I read that, which is that we know that ‘up to’ means we’re not willing to commit to anything at all (did you know I am up to 15 feet tall? It’s true!), but what the hell does ‘70% more infectious’ mean?
It could mean a lot of different things.
To me, there are two natural hypotheses for what it means.
One sensible definition of this is that 70% more people get infected each day, so it raises R0 by that percentage. If previously things were stable, 70% more infectious would cause infections to rise 70% each serial interval, which I’ve been approximating at about five days. So if it was this, things would about double each week.
Alternatively, it could mean that any given physical interaction was 70% more likely to infect you. This seems unlikely to be it, because how would anyone know what this value was, but it still makes at least some intuitive sense and has some practical value. So if before, if you went home for Christmas and someone was infected, you’d have a 10% chance of getting Covid-19, now that number is 17%.
The difference between those two is that if you get exposed multiple times, you can only get infected once, so the first scenario is a bigger jump in cases than the second one. Depending on how much ‘overkill’ you think takes place when people get infected, the difference could be big or it could be small.
As a third option, it could mean any given exposure is effectively as if you were exposed to 70% more virus. Chance of catching the virus is non-linear with viral load, so in some ways this is a more than 70% increased risk (if previously load was below threshold to get infected, and now it isn’t), and in other ways it could be less once you get to the other end of the curve. This also changes the distribution of initial viral loads, in ways that might be good or bad for outcomes and death rates. If you are reliably getting higher initial loads, that’s bad. If you are getting infected despite low loads then, given that we know you’re infected, that’s good, perhaps quite good.
What I definitely didn’t consider was the possibility that this was measuring the length of the doubling time because that’s not remotely a fixed number and using this doesn’t make any sense and arrrrrgh and then I saw this [LW(p) · GW(p)] on this post [LW · GW]:
What is still driving me crazy is that CellBioGuy presumed that this was what they meant. I mean, I certainly hope it is what they meant in terms of ‘that physical property of the world would kill less people’ but I can’t help but notice it would be completely insane in a way that even my model of predicted general insanity isn’t handling well. The model isn’t even handling the presumption by CellBioGuy very well here.
(Do check out the rest of that comment by CellBioGuy [LW(p) · GW(p)] anyway – even though the presumption in question turned out to be wrong, the rest of the comment has a lot of good gears-level details on various issues, but it’s too long to put here in full. I’d like to know how well the rest holds up.)
So on the plus side, statistics are being reported in a way that is relative sane.
On the minus side, this seems rather like it can be summed up as: We’re fucked, it’s over.
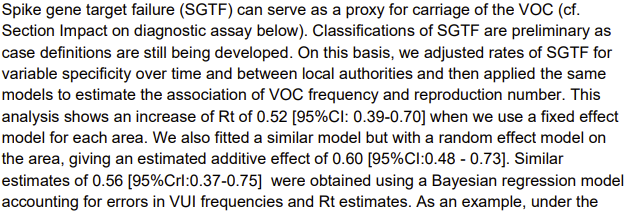
This is estimated as a 65% increase in infectiousness. If we want to stabilize infections in an area that was previously stable we’d need what would previously have been an R0 of about 0.6. If you have an R0 of 0.6 that means you would have previously been cutting infections in half each week or so.
Does that sound like something any Western country could possibly accomplish from here? What would even trying to do that even look like? Is there any chance people would stand for what was necessary to do that?
And that’s only what it takes to get a holding pattern.
Under such dire circumstances, a phase 4 lockdown has been invoked. What does that mean? Glad you asked, here are the guidelines.
The missing restrictions that stick out are not shutting down houses of worship, and allowing people to move house. Also funerals can go up to 30 people, whereas weddings are capped at 6. Also ‘support groups’ can meet up to 15 people and I don’t see anything saying it needs to be outdoors.
Whereas essentially any social contact of any kind is forbidden (e.g.: “You cannot meet people in a private garden, unless you live with them or have formed a support bubble with them”), your ‘bubble’ is highly restricted in its sizing, and you’re not allowed to be outside without a ‘reasonable excuse’ although those include groceries, going to the bank or exercising.
So basically, if you’re outside where it’s safe, they’ll harass you and maybe worse. Whereas if you stay inside, technically it’s not allowed but in practice it’s a lot less likely anything happens to you, unless the anything in question is ‘you catch Covid-19.’ The rules are porous enough that they aren’t enforceable against the things that are risky but enforceable enough to shut down the relatively safe actions that keep people sane. And with weird exceptions for remarkably large indoor gatherings for certain events that are textbook superspreaders.
All of which is what our model expects to see, and none of which seems likely to be remotely sufficient if the new strain is as infectious as they estimate.
The strain has already been seen in several other countries. Flights between the United States and the United Kingdom have not been shut down. Many European countries are shutting down some travel, which will slow things down a bit, but headlines like this one…
…illustrate that slowing things down is all that’s being aimed at. Which is good, because it’s too late anyway. There would not be any drivers to test if this was a real attempt at containment.
If the estimate of 65% more infectious is correct: The strain doubles every week under conditions where other strains are stable.
My father sent me this video (24 min) that makes the case for all of this being mostly a nothingburger. Or, to be more precise, he says he has only low confidence instead of moderate confidence that the new strain is substantially more infectious, which therefore means don’t be concerned. Which is odd, since even low confidence in something this impactful should be a big deal! It points to the whole ‘nothing’s real until it is proven or at least until it is the default outcome’ philosophy that many people effectively use.
Note that he also suggests the new strain is likely to be less virulent, and make us less sick, which could also be part of why it’s more infectious. If so, that’s great news (I can think of a scenario where it is actually bad news, but it’s an unlikely corner case).
He also points out correctly that a lot of nations don’t do much sequencing, so we should assume the new variant can’t be contained to England at this point. Doesn’t mean we shouldn’t try in order to slow it down, but such efforts will still fail.
The video seems strong on the scientific details, and the speaker strikes me as an excellent explainer/teacher, which is why I’m willing to link to it.
Alas, as is often the case with academics that are good at learning and explaining scientific things, the epistemology is bonkers. His core argument is: “You cannot use epidemiological data to prove a biological property.” With a side of Covid-19 being spread mostly by super-spreaders (true) and thus the new variant could be winning at random.
All of which is not how knowledge or Bayes’ rule works. It’s not how any of this works.
There is a valid point here, of course. Relying solely on the numerical growth of the strain or of infections in England generally, without looking at the context, doesn’t provide that much evidence. There are often other explanations. And his points about mutation in and of itself being commonplace and mostly harmless are well taken.
That doesn’t change that evidence is evidence, and a likelihood ratio a likelihood ratio. Experiments are not some special class of thing that are the only way one can make predictions or assign probabilities, and it’s weird that people can be so good at academic scientific thinking while not understanding this, and in fact it seems that when we train people to do academic science we also train them to not think about other information and to be careful not to use Bayes’ rule and to ridicule anyone who tries to use non-academic information in order to know things.
With that in mind, we look at the evidence and think about possible explanations, and mostly I find that there aren’t other plausible ones worth assigning much weight to.
Let’s start with those charts above. They aren’t quite this:
But then again, when you consider the context of England being under lockdown conditions that had previously turned the tide, and that have stabilized the situation elsewhere in Europe…
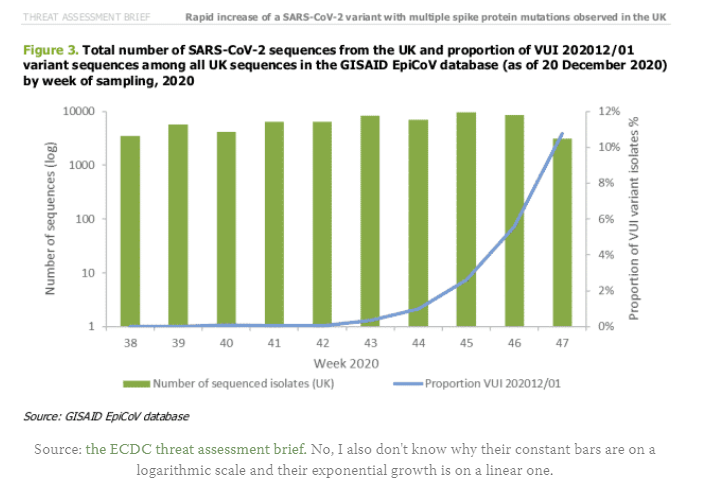
And combine it with the share of infections from the new strain from the earlier chart, and work out what those combine to imply…
This definitely does qualify under “hot damn, look at this chart.” This is a huge, dramatic increase in infections happening very quickly. A doubling in one week.
Note also that the warnings went out to the public on December 19. The out-of-sample data from the next few days strongly reinforce the hypothesis that we’re screwed.
The other plausible causes of such a rapid rise are not present. England didn’t suddenly relax its conditions this much. The law of large numbers is more than sufficient to make me very dismissive of ‘random chance via superspreader events’ as an explanation. How big are these superspreader events?
If my understanding of the situation is correct, there is only one conclusion:
This variant cannot be stopped short of mass vaccinations. It is not going to be stopped short of mass vaccinations.
All that is left is a holding action. Realistically, we can’t make enough of a dent to turn the tide of cases of the new strain until at least May. That’s about twenty weeks from now. That’s twenty doublings. So for every case that’s escaped to the United States so far, we can expect (does quick math) a million cases. Then another few doublings in June and July.
I do think we can do better than that, because it appears the tide is starting to turn now on the old strain, we’ll get a bunch of incremental help from increased immunity along the way, and control systems will set in.
But mostly, it seems like if you have vaccines and people who don’t want to die, you might want to hurry. I’ll get back to gaming the scenario out in the conclusion section.
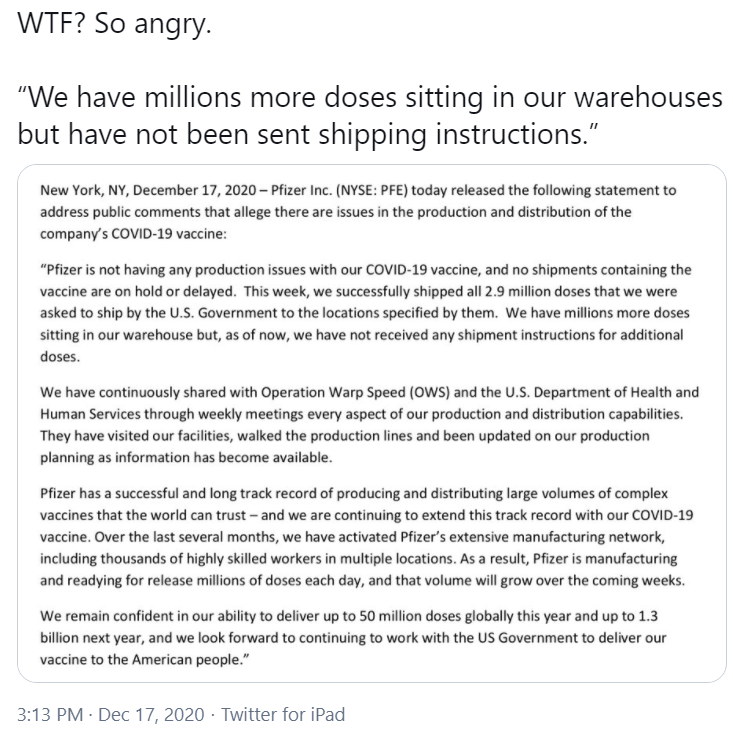
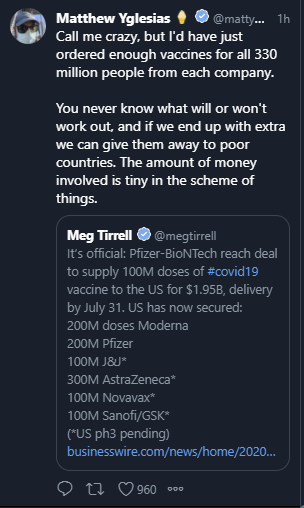
It seems that Pfizer executives are sitting around baffled that they have millions of additional doses of vaccine, and those doses are sitting on shelves unused, with continuous risk of spoilage, while they help no one. We have confirmation that this is explicitly not holding back second doses, and is coming as a complete surprise to Pfizer.
As a reminder, using a few million additional doses will cut infections by about 1% compounding each week, if distributed at random. If used selectively, an extra few million can cause a double digit drop in the death rate a month out, due to how concentrated deaths are among the elderly.
Distinctly from the issue of vaccine going to waste, the estimates given to states were too high, for which (Twitter video link) the head of Operation Warp Speed has taken responsibility. Such admissions are so virtuous and unexpected that they are clear signs of competence and trustworthiness. I agree strongly with Alex Tabarrok here, and my esteem for those involved went way up rather than down.
Oh, and also:
Versus:
So there’s that. While regular folk are told to cancel the holidays. Merry Christmas, suckers.
Still, CNN again:
If true, that would be two weeks behind schedule, but assuming all of this is on a different track than manufacturing, so long as the process doesn’t keep falling further behind, I guess it’s not actually so bad? That’s a big ‘so long as.’ But it’s a plausible one, as initial difficulties don’t have to translate into difficulties once things are running and it’s not Christmas.
Then there’s the issue of that second dose. The science behind why you need two doses is strong and makes sense, except for the little matter of the data. It’s clear that the first dose alone is much more than half as effective as two, and we don’t have enough doses. And the first thing I asked when I saw that result was something that is once again being pointed out. Booster shots do not have to be given two weeks after the first shot. The measles booster comes a year later. Multiple sources confirm that there is no reason to expect a six-months-later second dose to be any less effective a booster.
We are mostly wasting an entire half of our vaccine supply by dosing exactly the worst people with it – the people who got the first dose. I can see double dosing those in nursing homes anyway, because they’re 1% of the population and over a third of deaths, so even a small additional boost is still worthwhile, and their immune systems are weak so it’s reasonable to worry the first dose alone won’t get the job done there. But beyond that, there’s no excuse I can see beyond saying the rules are the rules.
Here’s where we are, it seems:
Doses that arrive on July 31 are not doses I expect to prevent many infections. And this total does not leave much margin for error, we barely have enough doses if we don’t use AstraZeneca and insist on everyone getting two shots.
A real case can be made that, given our inability to do suppression properly, a Western government’s policy ends up mostly coming down to their effect on the vaccination schedule. Did they advance vaccine research?
On those fronts, we come out well ahead of the European Union. Does anything else matter by comparison? And how did we manage to do that?
Casey Mulligan reminds us that one of the things Trump has been doing for a while is getting the FDA to kill less people by speeding up and streamlining its processes. So when the time came for Operation Warp Speed, the concept was shovel ready. The “experts” all said eighteen months minimum and the “experts” got ignored. We certainly could have pushed much harder much faster, even given initial conditions. I’m not going to stop pointing that out. The decision to balk at buying extra doses might be the worst single decision of the last four years, of any kind. But when I model alternative administrations, from either tribe, I model a much slower vaccine effort. When we reach the end, it’s not clear that won’t matter more than every other decision combined.
In England, it seems they are going to be testing a vaccine grown using tobacco plants? Approval to begin trials is in. This seems like a great illustration of our regulatory state, because you can’t take the life-saving vaccine they grow with the tobacco plants, but you can take the tobacco in your pipe and smoke it even though we know it kills you. Okay, then.
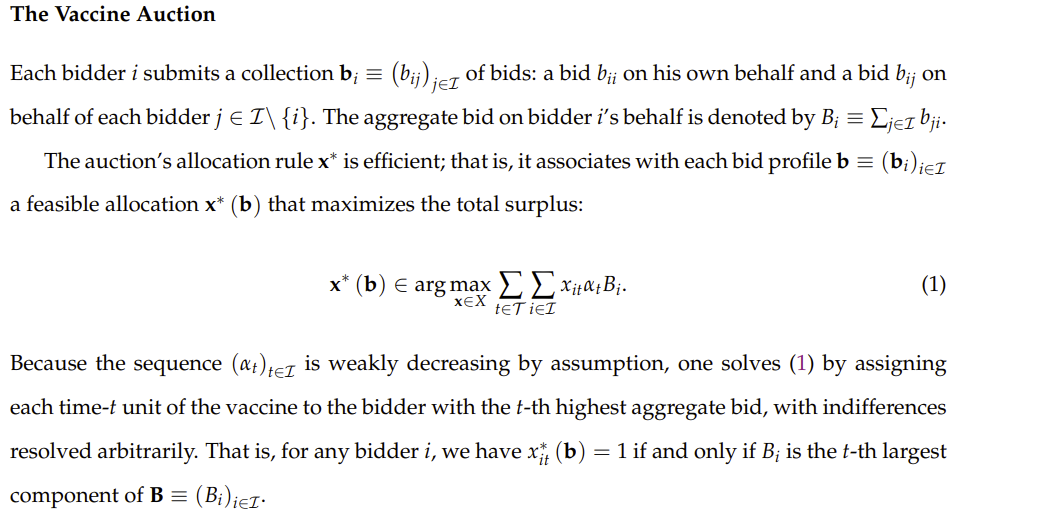
Theoretical Vaccine Auction
If you want to properly allocate a scarce resource like a vaccine, obviously you use an auction. I said it last week, people righteously said that things are not worth to the customer what the customer will pay for them because poor people have less money than rich people, and no, sorry, that’s not how this works, that’s not how any of this works.
The good news for those who disagree is that there is not the slightest danger of any attempt at an efficient allocation of the vaccine.
Externalities, on the other hand, are definitely real. To the extent that they are different for different people, we should take that into account. In theory, an auction can do that because others can subsidize the bids of those whose vaccination is beneficial to them. In a first best situation lots of people would subsidize lots of others near them and the government at various levels would also supplement bids, but presumably people mostly won’t get such acts together and it won’t happen except highly locally, inside families and corporations.
My guess is that for all the talk of externalities, they’re not that different for different people other than those who were previously being irresponsible, and subsidizing them for that seems like it has some large moral hazard issues plus the worst offenders probably already had it. The exception would be those that provide a lot of value if they can expose themselves to the virus that they couldn’t otherwise, but are not being paid for that service enough to place the bids themselves. Health care workers in hospitals likely quality, but you can fix that if you subsidize the hospital to bid for them, and generally that class of solution seems like it should work.
Thus, the obvious solution of “N-lot, pay N+1th-highest-bid auction that repeats every so often” seems like it’s just correct on first principles, and then once you run the first one likely you can slowly reduce price to keep supply and demand balanced without having to go through all the trouble of more auctions?
So that’s not that interesting a paper and also it’s about four lines long, so it was odd when I followed a Marginal Revolution link to this paper about how to auction off the vaccine only to find a much longer paper.
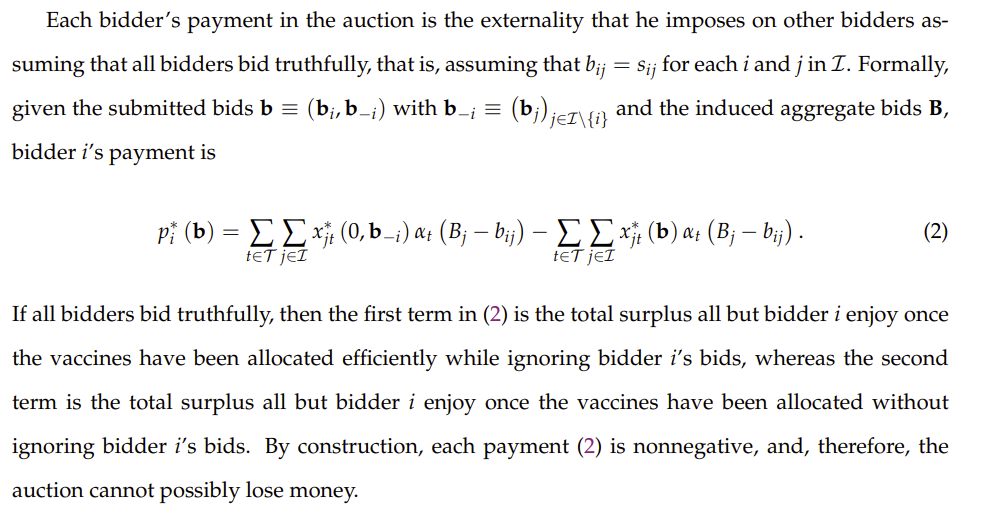
Which goes on to suggest this:
Which is exactly why no one wants to participate in auctions or read economics papers. I believe that the paper’s approach boils down to “everyone writes down how much they value each person getting the vaccine at each possible point in time, drawing that curve for everyone” and then the auctioneer solves for the best possible solution that maximizes surplus, and everyone pays the marginal cost imposed on others behind them, as measured by how much they don’t want to wait one more slot to get their vaccine.
Which, I mean sure, that’s technically correct of course, the best kind of correct, but it’s also making my brain hurt reading it and that’s despite intuitively knowing the answer the moment the question was asked. No one is going to want to think about let alone write down full utility curves, the practical cost would be enormous.
And getting people in the wrong spot in line by a little bit is at worst a small mistake, and also not that meaningful given the logistics of vaccine administration. The vaccine is not exactly being teleported around.
Thus, I’m pretty sure in practice this reduces to ‘find the price that mostly clears the market and charge that price, then adjust it to keep clearing the market.’ The whole thing where others can bid on your behalf is how ‘people can buy things with dollars’ works already.
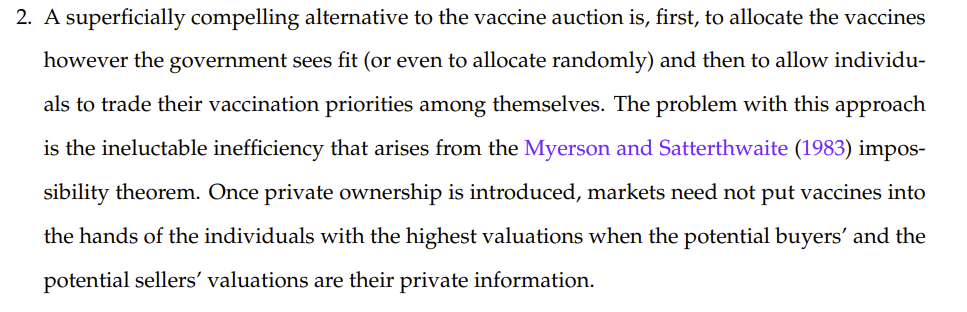
In response to the people saying ‘but poor people are poor and rich people are rich, you bastards’ they say the following:
This is, essentially, distribute a valuable asset according to politics, then allow trade. Which is a worse version of full free trade, since it involves political reallocation of wealth and (as noted by Myerson) results in a lot of profitable trades not happening because of various frictions, and also makes people feel bad about not selling their vaccine dose and also about selling their vaccine dose, because choices are bad. It seems obviously better than allocating via politics alone, since most of the trades that happen will be hugely profitable to both sides – the person selling will get a payment much, much bigger than they’d have found necessary, and the person buying will pay much, much less than the amount they value the vaccine. The ZOPA (zone of possible agreement) here is mostly huge. I have a hard time imagining that choices being bad overcomes that.
What I personally would love is a form of abstract that is “the paper that we would have written if we were only trying to get the central point across and didn’t care about formal anything at all.” Not quite You Have About Five Words [LW · GW] (I keep thinking the ‘have’ is ‘get’ and having to correct myself, maybe the title should change) but mostly not that much more than that. A one-page Econ 101 cheat sheet can cover actual everything the class teaches, and most economics papers have at most one paragraph of actual information.
Here, it sure seems like the whole paper boils down to “Standard auction theory applies here.”
It usually does.
This, for example, is a great use case. Not Covid-19 related or in any way essential, but pretty great.
Another modest proposal is to fix the prices and then let people pay them, skipping over the auction as such, so we know we can raise $50 billion dollars for vaccine production and distribution (and motivation, shall we say) by letting a few people skip the line. That makes it easy to see it’s an absurdly good deal, but also either wouldn’t get enough takers or is leaving a lot of money on the table, in exchange for being easy to think about.
Also, that post points out something that seems important. What could be a better way to motivate people wanting the vaccine, than to show our richest, most famous and most powerful people paying really big bucks to get the shot a few months sooner?
If I am interpreting this correctly, those with power used politics to get vaccinated first, ahead of nurses and residents. Residents, of course, are indentured servants giving four years of work under terrible conditions with hugely below market pay in exchange for the right to join a monopolistic guild that enforces scarcity of health care provision via government restrictions on supply of residences and slots in medical school.
This is exactly how political distributions of goods always go, except that this time it was a really bad look to give administrators in offices the vaccine before doctors who were actually treating Covid-19 patients. That’s what “The list created by the algorithm was supposed to be vetted” means here, that they were supposed to do a check to make sure their naked appropriation of vaccine had some plausible deniability attached at some level, whereas it turned out it didn’t.
But of course, as the thread points out, blaming ‘the algorithm’ or saying ‘there are problems with the algorithm’ is the obvious nonsense. Yes, there was a ‘problem with the algorithm’ and the ‘problem’ was ‘the people with power over the contents of the algorithm gave themselves top priority.’ This wasn’t some complex calculation. It didn’t involve machine learning. The result wasn’t surprising to anyone who came up with the criteria. The criteria was giving resources to the powerful rather than the powerless, via deeming them more ‘important’ or ‘vital’ or something.
This time, thankfully, they got caught. Yet they still got their vaccine shots.
Thus, this apology is the height of hypocrisy:
Did not anticipate, you say. Equitable distribution, you say. In case you ever wonder what equitable distribution means when those with power say it, now you know.
You gotta love the line “Though our intent was to ensure the development of an ethical process, we recognize that the plan has significant gaps.”
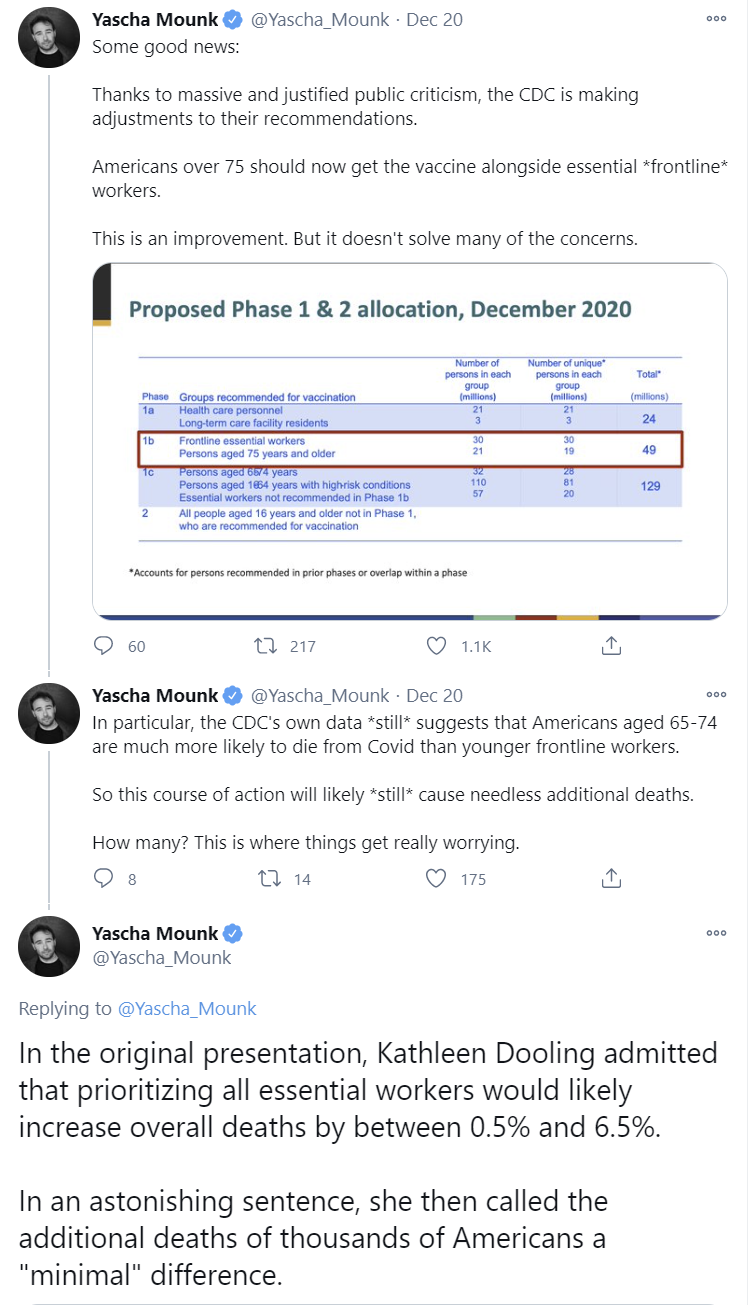
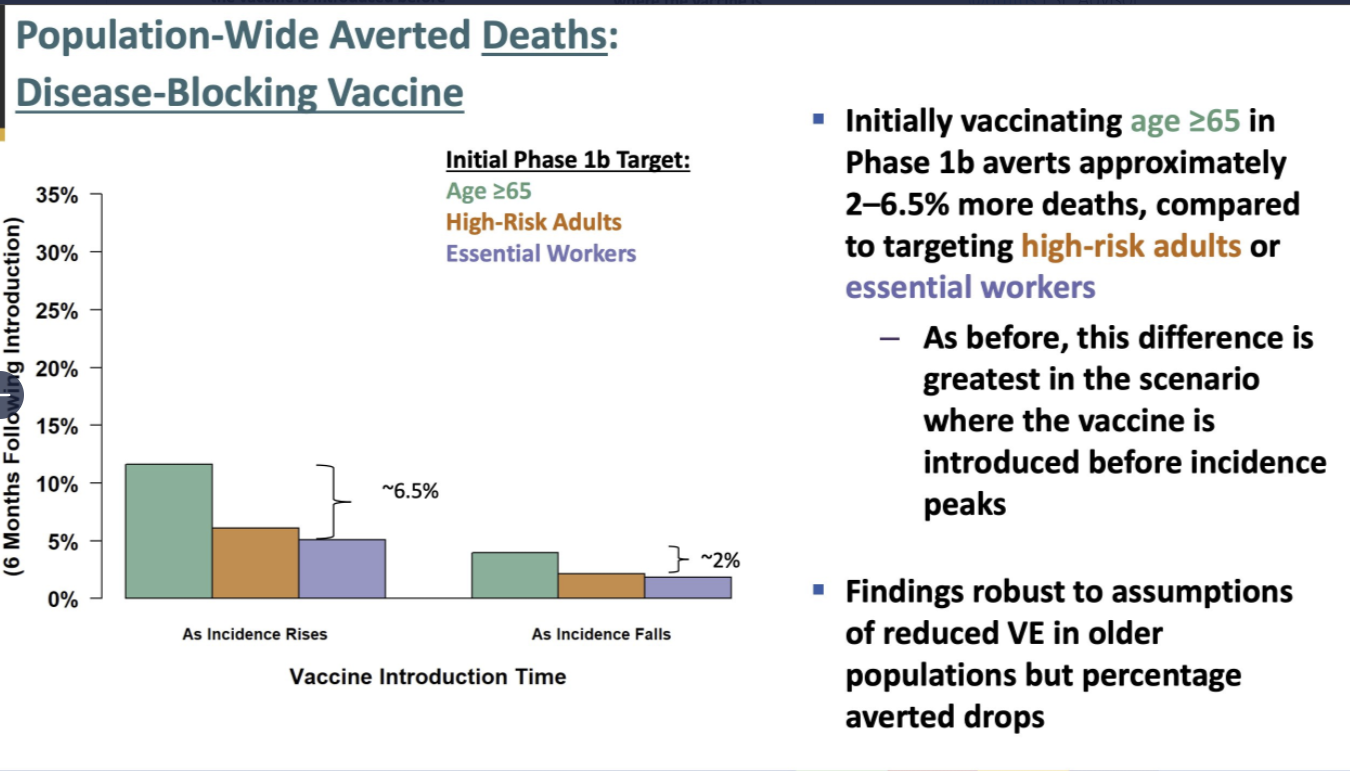
It is unclear to me to what extent this is driving policy decisions, but it seems like it came close to happening, with the CDC only reversing after a public outcry. The mayor of New York has endorsed this perspective explicitly.
So. Yeah.
But congratulations to Texas, among others (via CNBC):
The government anticipates that people will not Act Responsibly on Christmas, and thus is pre-emptively punishing them in order to send a message.
What’s interesting is her proposal that we can understand such acts by the Very Serious People as being primarily about face.
This reaches many of the same conclusions and makes many of the same predictions as many of the models and gears I’ve been using, but seems importantly different in ways that require more attention. These dynamics have been mostly left out of my models, and that seems like it might have been a mistake.
I am going to think more about whether it makes sense to incorporate such dynamics more centrally.
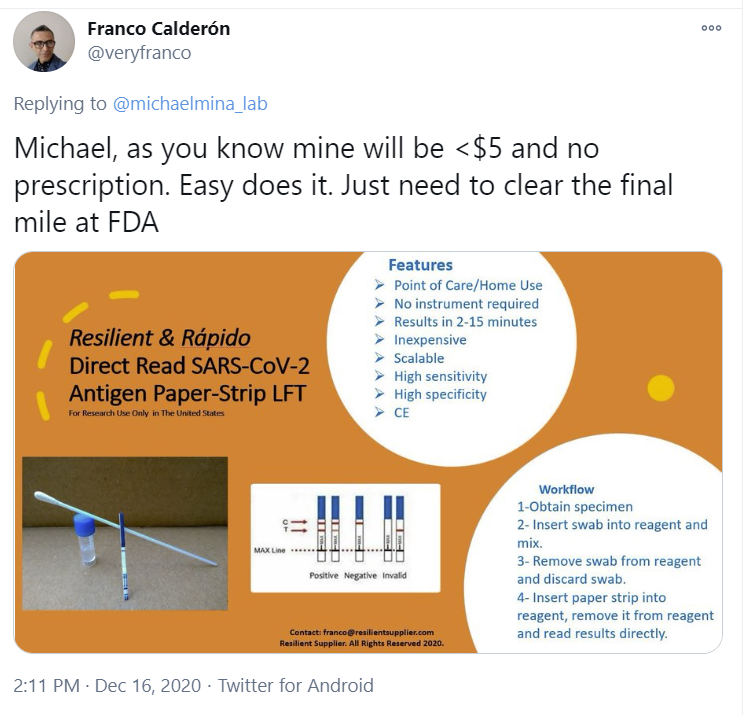
Quest for the Test
The good news is a $5 paper test strip has been approved by the FDA for home use. Of course, doing so legally will require an additional $25 so a digital MD service can watch you do it, which also means all sorts of coordination problems and activation energy and having to be observed by medical people silently judging you. Because of the need to beware trivial inconveniences [LW · GW] it seems like the additional costs will be hugely destructive of the potential value here, although massive value should still remain.
Perhaps the next one will do better? As usual there’s claims it is coming Real Soon Now:
Alas I expect that last mile to find a way to at least inflict a lot of damage, even if cleared.
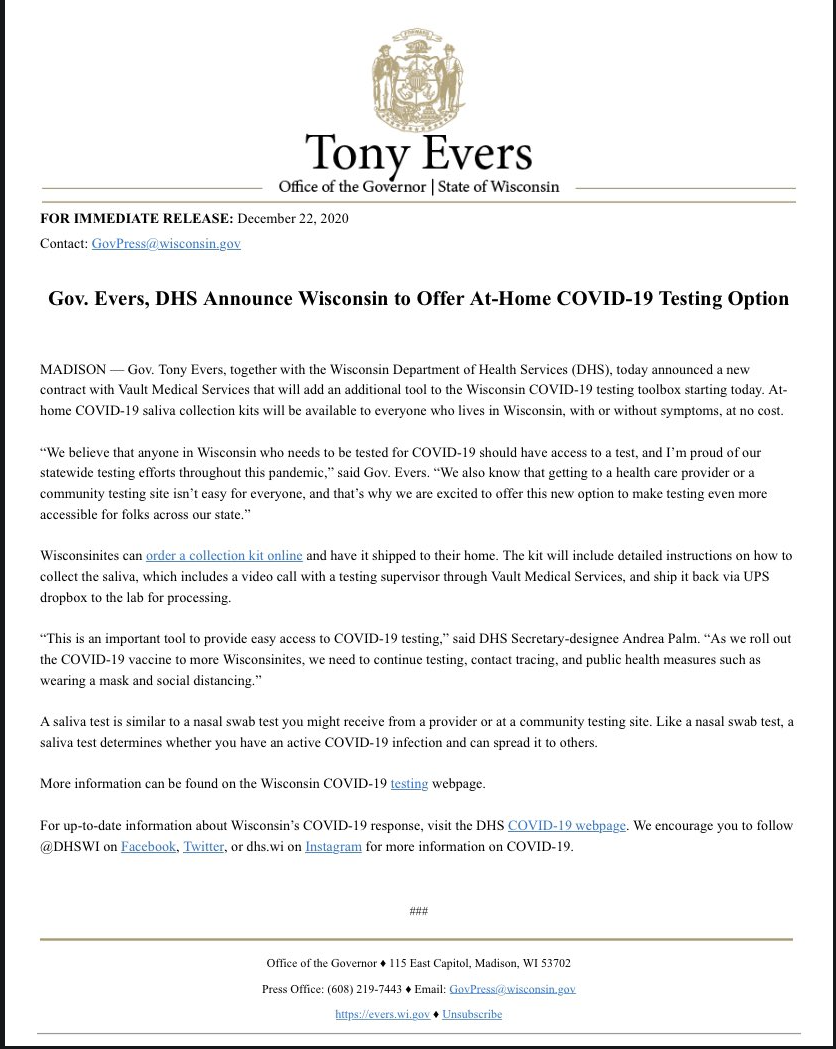
Whereas this plan from Canada seems awesome, taking the methods of continuous rapid testing that worked in some universities and applying them more generally to businesses that value being open.
Free testing on demand, sample collection at home, even if it isn’t rapid, and even if they require a zoom call during the sample collection. And you need an email for each of your children, even if they’re two weeks old. Still. That’s not bad!
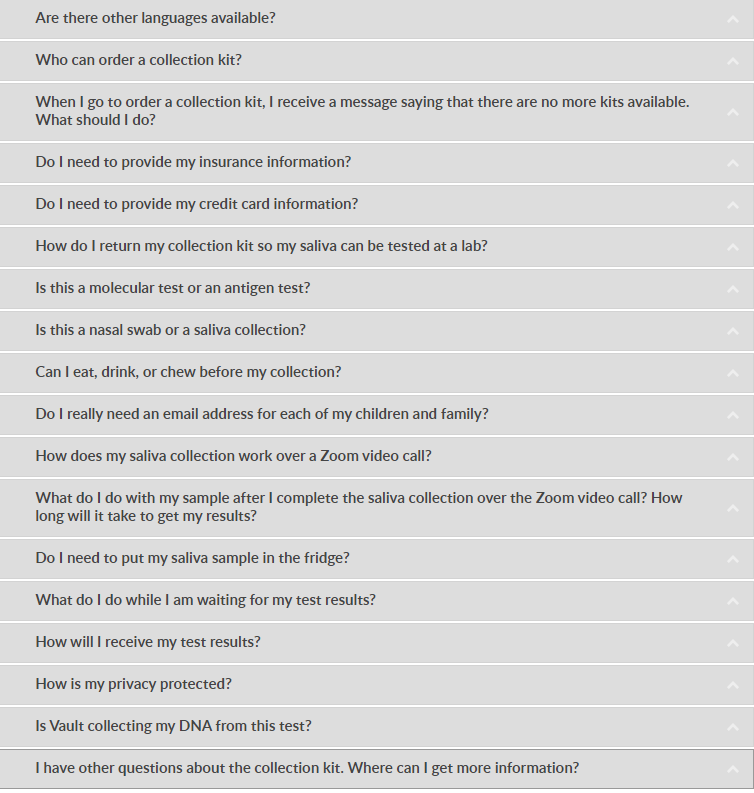
A sign they do not understand the proper goal of testing is that they don’t grok that people might want to do this periodically without any particular reasons to worry:
Another sign is, look for the mysteriously missing question on this FAQ list:
Oh yeah, that question. How long until I get my test results?
Good question!
In Other News
This analysis of how Covid-19 spreads seems excellent as far as I can tell, making a strong case that it’s mostly or entirely aerosol transmission, and that this fits the observed data fine, thanks. People I respect led me to it and also had the same take. If there’s anything wrong here, please speak up.
CDC issues the following guidelines and it only took until (checks calendar) December 21:
If you’re looking for treatments, this Quora response seems to be a real attempt at providing guidelines one could use. As usual I’m going to tread lightly on the treatment side and not take a stand.
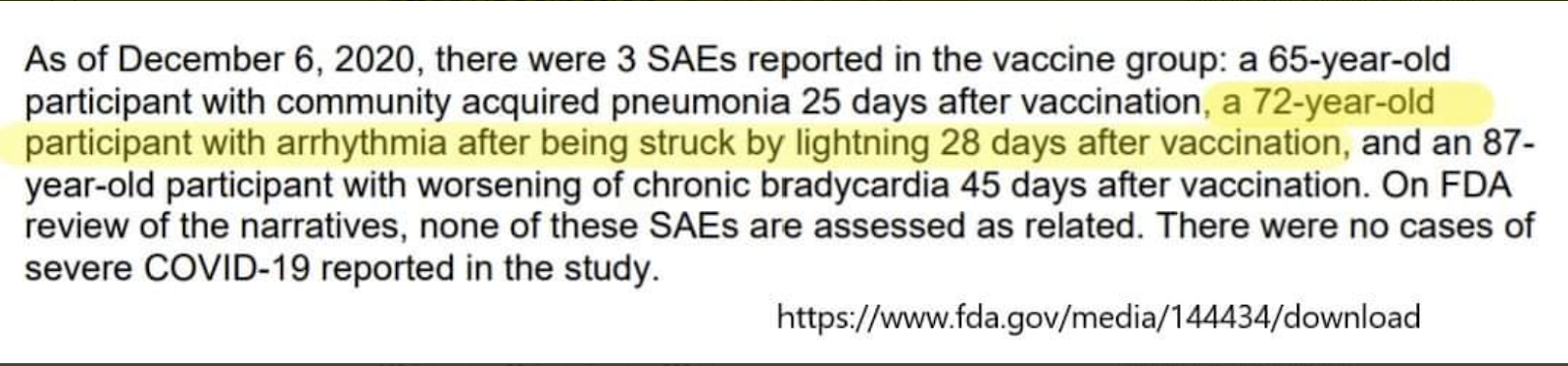
Not a metaphor: Yes, you literally have to report as a ‘severe adverse event’ requiring investigation when someone in your vaccine trial is struck by lightning:
Official in Buffalo gives press conference announcing 60 people died, reporters only ask questions about the division champion Buffalo Bills. Official then tells them to ‘get their priorities straight’ but their priorities are already quite straight. The reporters know there’s a lot of deaths, and a lot of Covid-19, but what is the actionable information about that, that the official could tell them, that they don’t already know? What impacts people’s lives? The team could be in an unknown amount of trouble, and that matters to people in Buffalo. Whereas barring a change in policy that would have already been announced, they know exactly how screwed they are personally, and what they have to do. The true objection here is that when people are dying it’s wrong to not waste one’s time showing one’s concern about that and instead care about “trivial” things like the thing most or at least many people in Buffalo have cared most about the last few months. Or years.
Is using the bathroom essential? Second worst person Mayor De Blasio’s administration decided that it was not:
When a predictable uproar followed, he laid the blame on actual worst person Governor Andrew Cuomo, and requested that they gracefully allow New Yorkers to use indoor plumbing, a request that it seems has been granted:
Also, among other rules, employees cannot drink alcohol under any circumstances, which seems rather cruel except for the part where they never enforce it. Right now I bet a lot of them could use a drink.
This seems to be what you get when you shut everything down for months and months on end:
Why It Took So Long for the Army to Make Masks. The army masks are cloth masks with the right color scheme and symbols. That’s it. They are now getting around to being able to make them. The money quote for me is this:
According to the Army:
The CCFC was designed, developed, and produced along an expedited timeline. It normally takes 18–24 months for DLA (Defense Logistics Agency) to have the item available for order once the technical description, design, and components are approved and submitted. The CCFC, from inception to issuance, is slated to take less than one year.
The army is bragging that they figured out how to make masks this fast.
If there is a war, perhaps someone should tell the army. Seems like information they would want to know.
Would I accept the Chinese vaccine? I mean, yes, I still think it’s better than nothing, but wow do they continue to be bad at science in a way that seems almost intentional:
I know you think you’re helping but maybe just send paid time off?:
Not Covid, rather about hearing aids, once more with feeling: FDA Delenda Est.
Not Covid: MIRI gives its yearly research update. Disappointing to learn that research they couldn’t talk about didn’t pan out, and also disappointing that they still can’t talk about what it was, especially given hopes that the ideas might still have merit. Good to know they are willing to pivot to other different things and aren’t going to either keep going down a known blind alley or joining the gradient descent crowd. Also great to hear they are considering fleeing Berkeley, which I strongly endorse doing almost no matter the destination. Would love to do some coordination on that, but I’d definitely settle for the New Hampshire scenario, which I think would greatly enhance their ability to think.
Also not Covid, Other LessWrong news: The 2018 review is ongoing, but not many reviews are being written [? · GW]. I’d encourage those who qualify to help change that. I’m especially curious to hear people’s takes on my nominated posts.
Universal, the cult of the expert as explained by the Washington Post freelancer system:
There are many unknowns that have a dramatic effect on the path forward, and how the endgame plays out.
A few big ones dominate.
I do not see it as plausible that the new strain is confined to England. It has already been seen in several other nations, and the numbers in England are not compatible with it not being essentially everywhere already. It’s still right to cut off flights and travel now to slow things down, but the barn door is already wide open.
The biggest question is, instead, is the new English strain (or another similar strain like the one found in South Africa) really 65% more infectious as measured by infections per infected individual?
If that number is greatly exaggerated, then the strain will take a lot longer to get to where it matters, and even when it does the control systems and vaccinations can keep things mostly in check, and we are still on something not too different from the previous track. My guess is that aside from England itself, we could mostly deal with about a 33% more infectious strain given our timetable before it does that much damage.
If the 65% number is accurate, however, we are talking about the strain doubling each week. A dramatic fourth wave is on its way. Right now it is the final week of December. We have to assume the strain is already here. Each infection now is about a million by mid-May, six million by end of May, full herd immunity overshoot and game over by mid-July, minus whatever progress we make in reducing spread between now and then, including through acquired immunity. Which will help somewhat, but likely only buy a few weeks at most.
One worry I have is that the control system could actively make things worse between now and then, and accelerate the timeline. By the end of January, we should see up to a one third drop in the death rate purely from protecting nursing home residents, and then it will drop further as we protect other elderly people. If as I suspect the control system mostly acts on the death rate, they will use this as a reason to loosen and take more risk, and infection numbers will rise, or not fall the way we would have otherwise expected.
Then once the new strain arrives, it will be like March and April 2020, where by the time the deaths start spiking it is very late in the game, and there have already been three or more additional doublings.
The good news is that when this happens, most of our most vulnerable will have had the opportunity for vaccination. Assuming most of them take it, the (need for) hospitalization rate should be dramatically lower, and the IFR should also be dramatically lower if the hospitals don’t collapse. The hope is that with enough of the vulnerable protected, even a gigantic surge in cases might not collapse the system.
That’s the hope. It is basically the best (realistic) case scenario. It seems to be too late to speed up vaccine production much, although I see some reports Joe Biden is considering using the Defense Production Act to do so, in which case why the hell aren’t we doing whatever it takes to get that happening already? Have we considered throwing relatively tiny amounts of money at the problem? Maybe not quite that relatively tiny? No? Oh well. But I digress.
On the good news front, our tests still mostly seem to work fine for the new strain, although there is some small worry.
There is the concern that the vaccine might not be effective against the new strain, but based on my looking into this, the prior on there being much effect here should not be so high, except insofar as the new strain is more infectious so everything will be somewhat less effective at preventing spread. But if the virus has escaped from the vaccine already while also becoming more infectious, the timeline does not allow us to adjust even if we acted correctly, let alone acting realistically, the best we can hope for is maybe to protect some of the most vulnerable but I do not expect a Biden administration to allow movement fast enough to do that in this scenario. Instead, we’d see completely overwhelmed medical systems across the country, and that would be that.
On the potentially very good news front is the other big question. Is the new strain less virulent (dangerous) than the old one, and if so by how much?
I don’t think this is a favorite to be true, but I do think there’s a substantial chance (30%?) that it is, and we should investigate. All the news reports say that there’s no reason to expect that the mutation is more dangerous, which is true, but also not the change one would expect to often happen. The real question is whether it is now less dangerous, and for now the answer is we don’t know. If the effect size is big we will presumably figure this out by the end of January. Keeping an eye on England’s IFR will be important.
There are plausible physical mechanisms that suggest that some of these mutations may have led to less virulence. One piece of evidence that the strain is less virulent is that it is more infectious! Being less virulent causes it to be more infectious, so if the strain is more infectious, there’s a decent chance part of that was caused by less virulence.
Note that if we do face that scenario in the fourth wave, unless virulence has gone down quite a bit, you now face an even more stark version of what you did preparing for the third wave.
If we are in this scenario, it is inevitable that there will be a several week period, at a minimum, in which it is super easy to catch Covid-19, with a super infectious strain everywhere, and at a time when there will be no hospitals to help you, and no vaccine that works.
In that scenario, actually protecting yourself becomes vital if you haven’t been infected by the time the climax is approaching. As in essentially not being anywhere near a human outside your bubble, for weeks on end, at least until the hospitals stabilize.
It also becomes realistic again to worry about our supply chains or civil disorder. I expect everything to hold, but that can’t be assumed.
Then there’s the other nightmare. When this starts to happen, how will the authorities react?
Benevolent authorities would be responding now by making every attempt to speed up our vaccine efforts, and to prioritize the most vulnerable while we can. But if we had such benevolent authorities, they would have already been doing that. When something goes from super overdetermined to super duper overdetermined, it’s not generally the time to expect people to suddenly come up with the right answer when they didn’t before. Still, there’s some hope that this would happen, as the ‘don’t let it get so bad they sell out of pitchforks’ mechanics kick in. The other problem, as I’ve noted, is that there is not that much room to move faster without much more aggressive disregarding of barriers put in to prevent action, which would cause a ton of cognitive dissonance, and is not Biden’s style.
The question is what our actual, present authorities will do.
Like England, they might go for a full ‘lockdown.’ My assumption is that if they do this, people will end up largely ignoring it, and it won’t be enforced. There’s no will to make real restrictions stick even in blue tribe areas, and red tribe areas would be in open revolt, especially when it comes from a Biden administration. People have had enough, and they’ll have been told the story of how things were supposed to be returning to normal.
And even when they do that, they’ll still provide enough loopholes that it presumably wouldn’t work even if people didn’t go into open defiance of the rules.
Still, will they try anyway, doing epic additional economic damage and potentially causing open conflict? I worry about this a lot.
Thus, I don’t know if one should buy stocks or sell stocks on this, or even if one should buy volatility on this or not. If things crest once more and then burn out, that is not bad for stocks. It’s only bad if we get a dramatic response, which wouldn’t help the problem much but also give us a whole additional set of problems. We need to get ready, now, to do what we can to stop this from happening when the moment arrives, if the moment arrives. Sure, if it worked one could argue in favor, but the math seems rather clear that it won’t do any good. When politicians start trying to make it to next week without taking blame, and attempt to destroy everyone’s lives to do it, we need to find a way to stop them.
Or we could figure out how to make our efforts actually work. It’s not impossible. Is there still time to get our house in order and deal with this head on, if we want to? Hell yeah. But we can’t do it by Sacrificing to the Gods and taking sledgehammers to everything people like doing. We can’t even do it via doing that and being willing to shut down economically important activity, not for long enough to work. I’d be pleasantly surprised if we could even stabilize growth rates that way, and it’s completely unsustainable.
What we could do is prepare a testing regime now. Have that in place a few months from now, for real, and do the kind of testing on everyone that some universities do with their students. If we took all the regulatory gloves off, my guess is we wouldn’t even have to subsidize to get there on time. Add in proper focus on Vitamin D, airflow, outdoor activity and so on. We could still make it, and it would be an essentially free action.
We could probably start this on January 20 and still make it.
To be clear: We won’t attempt to do this, and it won’t happen. But it’s important to note that we still could, in at least some sense, still win, while also noting that we will lose. You never know. Maybe someone, somewhere, is actually listening.
In summary, I am attempting here to do now what I failed to do in December or January, which is to actually model what happens next based on exponential growth and realistic reactions by authorities.
My guess is that the English strain is probably sufficiently infectious to get there before enough vaccinations can happen to let realistic measures contain the pandemic. Right now I’m giving the strain something like a 70% chance to be sufficiently infectious, and if it is, I don’t see a way around this outcome.
This has counterintuitive implications, both for public policy and for individuals. As always, one’s approach to the pandemic must be to either succeed if one can do so at a cost worth paying, or fail gracefully if one cannot succeed. Thus, one could plausibly either make the case for being even more careful in response, or to folding one’s hand entirely. You can raise, or you can fold, but you can’t play passive and call all bets and hope to go to showdown.
It’s also important to figure out whether the new strain is less virulent than the old one, and if so to what extent, since that could change the math on sensible courses of action quite a bit. I haven’t fully wrapped my head around the implications, and I doubt many others have either. Simply saying it is “good news” does not begin to cover how this changes correct actions.
Let’s actually engage with the physical situation and model out what happens, and learn from last time out’s mistakes.
UPDATE 7/21/2021:
As you doubtless know at this point, it was not over. Given the visibility of this post, I'm going to note here at the top that the prediction of a potential large wave of infections between March and May did not happen, no matter what ultimately happens with Delta (and the prediction was not made with Delta in mind anyway, only Alpha).
I've talked extensively about the situation across many other posts, but for visibility I'm going to summarize my view of what happened here.
First, the early reports said that Alpha (this post calls it the English Strain, which is now called Alpha) was 65% more infectious than baseline. Instead, it looks like Alpha was about 40% more infectious. I noted that on our timetable, we could deal with about a 33% more infectious strain under the predicted-at-the-time vaccine timetable before major damage was done.
Second, when I was writing this post, I expected vaccine deployment to be substantially slower in its first few months than it ultimately was. I made a clear mistake not making this assumption explicit, but we got a lot more shots into arms that I expected during this period - I was thinking 100 million shots in 100 days (e.g. Biden's stated goal) and we did substantially better than that.
Together, these two incorrect assumptions explain why the wave did not occur, although they alone are insufficient to explain why things continued to improve so rapidly. My guess is that I was also somewhat underestimating seasonality, and that Alpha scared people sufficiently that the control systems acted differently than they otherwise would have, which also should have been considered more.
I gave the headline scenario about a 70% chance of playing out. It didn't play out, and the above reasons are why (in my current model) it failed to play out, and how I put a 70% probability on something that didn't happen.
Looking at what did happen, if we had indeed been facing a 65% more infectious strain at that time rather than 40%, we would have faced a wave of some size even with the other factors being better than I anticipated, but not the size of wave I was predicting; it would have taken a number more like 75% to cause a crisis before vaccinations could kick in. On reflection, given what I knew at the time, if we take the distribution of possible properties of the Alpha strain as a given, I think I should then have been predicting more like 40%-50% chance of the scenario rather than 70%.
Contrasting the situation with Alpha, where I thought it was at 65% more infectious than baseline and that it would cause a large wave before we could sufficiently vaccinate with Delta, where it's perhaps 120% more infectious than baseline but we've already done a lot of vaccinations, and now we are seeing rises in cases, is interesting, and will be an interesting test of whether the other assumptions I was making were accurate.
I said it last week, people righteously said that things are not worth to the customer what the customer will pay for them because poor people have less money than rich people, and no, sorry, that’s not how this works, that’s not how any of this works.
It seems easy to construct a scenario where this is untrue, or at least conflicts with an intuitive definition of "value". If I'm trying to auction off a rare food item in a room with Jeff Bezos and a starving person with no money, Bezos can easily win the auction if he has the slightest desire for the food. A tiny rounding error on his fortune is more than the starving person's entire life is worth (in a monetary sense). Bezos clearly puts a higher monetary value on the food, but it seems absurd to suggest that this is an example of the food being allocated to the person who values it the most. To use a more realistic example, it's hard for me to agree that a billionaire values their tenth vacation home more than a homeless person who is in danger of freezing in the winter.
I'm generally in favor of free markets, and maybe allowing Jeff Bezos to do whatever he wants produces an overall better world than the alternative. However, it seems disingenuous to say that his vast fortune means that he can value an item of trivial importance more than other people value anything at all.
At the moment, the poor person and the rich person are both buying things. If the rich person buys more vaccine, that means they will buy less of the other things, so the poor person will be able to have more of them. So the question is about the ratios of how much the two guys care about the vaccine and how much they care about the other thing... and the answer is the rich guy will pay up for the vaccine when his vaccine:other ratio is higher than the other guys. This is the efficient allocation.
It might be the case that it is separately desirable to redistribute wealth from the rich guy to the poor guy. This would indeed allow the poor guy to buy more things. But, conditional on a certain wealth distribution, it is best to allow market forces to allocate goods within that distribution.
(For simplicity I have ignored macroeconomics in this post, but the same argument broadly goes through if you don't.)
At the moment, the poor person and the rich person are both buying things. If the rich person buys more vaccine, that means they will buy less of the other things, so the poor person will be able to have more of them. So the question is about the ratios of how much the two guys care about the vaccine and how much they care about the other thing... and the answer is the rich guy will pay up for the vaccine when his vaccine:other ratio is higher than the other guys.
This is only true if the rich person is already spending as much money as possible, so an increase in spending on Item A must cause a decrease in spending on Item B. For someone like Jeff Bezos, an increase in spending on Item A probably just results in slightly less money spent by his great-grandchildren in 100 years.
It might be the case that it is separately desirable to redistribute wealth from the rich guy to the poor guy. This would indeed allow the poor guy to buy more things. But, conditional on a certain wealth distribution, it is best to allow market forces to allocate goods within that distribution.
I don't see why this has to be true in all scenarios. If we want to make sure that the starving guy gets some of the food, can't we just allocate the food to him directly, rather than having to give him enough money to win a bidding war with Jeff Bezos? Perhaps we desire a system where, in general, Jeff Bezos can use his money to do whatever he wants, but we have safeguards in place to prevent him from outbidding a starving guy on the food he needs to survive. I recognize that this may not be efficient in monetary terms, but it could be efficient in terms of overall human utility.
I think I disagree a bit with both (but what do I know).
For someone like Jeff Bezos, an increase in spending on Item A probably just results in slightly less money spent by his great-grandchildren in 100 years.
This doens't seem to me to be the right way to think about it. Short term, the more he spends on Item A will result in lower spending on Item B, or lower investment in his companies, a lower transfer of money from him to someone else (like through lower savings). Or more money being spent overall if he just uses up cash he had hidden in his pillow; which increases prices for everyone (but this will be made up for in some future).
If we want to make sure that the starving guy gets some of the food, can't we just allocate the food to him directly, rather than having to give him enough money to win a bidding war with Jeff Bezos?
Who produces the food and can set the prices? If it's private companies, then they wouldn't sell it to the state for cheaper than to Bezos, so it would be as expensive to the state as giving that same money to the poor and let them outbid Bezos. If the state owns the stuff, then [insert standard anti-socialism arguments]. If the prices are fixed by the state, then its inefficient and there may not enough production for all. If the prices fixed by the state but depend on the person -- or on how many of X you have bought this month or stuff like that -- then that introduces whole new types of messes.
I agree that in a very strict sense money spent on X definitionally cannot be spent on something else (you already spent it so don't have it). But does that type of tautological view matter here? (And if that is not the basis of your point and I'm misunderstanding, sorry.)
This kind of reminds me of the old Richard Pryor movie Bruster's Millions.
I suspect the numbers have change but at one point I recall Bezos had a new worth of 90 billion. Even with a paltry 1% return on total assets that's like 900 million a year. Could you spend all that? I'm not sure I could really keep tracking of an income stream like that -- I suspect I would often be doing the equivalent of dropping a million on the floor now and then and forgetting to pick it up for a week or so.
So the rich buying more vaccines doesn't really equate to not buying enough of other things that prices for those other things drop enough to make more available to the poor (who are budget constrained much more realistically than are the rich).
I am under the impression that you are thinking something like: "Bezos has ~100 billion to spend. If he spends 1 million in X, then he has 1 million less to spend on the rest. But he won't even get to spend it in his lifetime, so that extra million in X doesn't change how much he would spend in Y. Therefore, it's wrong to say that Y will become more available because Bezos spent in X.".
I don't think that's the right way to think about all this. (Warning: oversimplification coming):
Bezos earns some income, say, in a year. Almost all of it will be spent. Most will be invested and not consumed, so it will still increase his net worth, but that demand for stuff is still there, affecting the economy. Bezos is already probably spending about as much as he can, and what he is not spending he is saving which probably means transferring it to someone else who will spend it. So, if he spends USD 10 in X, it's reasonable imho to "expect" the economy to get USD 10 less spending in non-X stuff (on avg)
I said it last week, people righteously said that things are not worth to the customer what the customer will pay for them because poor people have less money than rich people, and no, sorry, that’s not how this works, that’s not how any of this works
I pointed out the error last week, too. I'm disappointed to see it doubled down on.
Agreed. To be fair to Zvi, he did make clear the sense in which he's talking about "value" (those who value them most, as measured by their willingness to pay) [ETA: "their willingness and ability to pay" may have been better], but I fully agree that it's not what most people mean intuitively by value.
I think what people intuitively mean is closer to: I value X more than you if: 1) I'd pay more for X in my situation than you'd pay for X in my situation. 2) I'd pay more for X in your situation than you'd pay for X in your situation.
(more generally, you could do some kind of summation over all situations in some domain)
The trouble, of course, is that definitions along these lines don't particularly help in constructing efficient systems. (but I don't think anyone was suggesting that they do)
Agreed on all points, except for about how clear the author was being about the use of the word "value". Although he does make the reference to willingness to pay, his rhetorical point largely depends on people interpreting value in the colloquial sense. He writes, in the previous post:
If we’re not careful, next thing you know we’ll have an entire economy full of producing useful things and allocating them where they are valued most and can produce the most value. That would be the worst.
Imagine if you alter the phrasing to this, which is roughly equivalent under the "value = willingness + ability to pay" paradigm:
If we’re not careful, next thing you know we’ll have an entire economy full of producing useful things and allocating them to people who can pay the most money for them and where they can generate the mostwealth for those people. That would be the worst.
Many people might reasonably object to that scenario, even though it sounds silly when we phrase their objection as "I think we should allocate resources to people who value them less". My own feelings are probably closer to the author's than those of the hypothetical objectors, but I'd prefer it if we could avoid these kind of rhetorical techniques.
The market cares for individuals about as much as evolution does.
Yes. Bezos can bid more for the meal than the hungry drifter. Why is that the case? It's because Bezos is instrumental to offering a useful service to literally billions of people and the drifter... isn't.
It seems cruel. It is cruel. But it's a cruel world we live in. It is perfectly possible for preventing Bezos from being mildly "hangry" at an inopportune time to alleviate more suffering worldwide than preventing one shiftless vagrant from starving to death.
And that's not intuitively obvious because your social instincts are programmed for a world where you know everyone in your entire community personally and can see exactly what they're contributing with your own eyes.
Set the situation in a small tribe where you're choosing between feeding the shaman who knows where the watering holes are and what food is safe to eat and is obviously critical to the survival of everyone, or feeding the aged cripple who can barely walk unassisted and your social instincts will likely choose correctly. You'll still be sad, but finite resources often means hard choices.
We use markets to decide things like this because they're the most efficient way we know of to deal with the scope of the calculation being far too big for our puny brains to handle all at once. But that cuts us off from always being able to understand the why of the calculation result. And so when the market hands down a result that is painful to look at we reflexively want to call it a "market failure" and "correct" it.
But there are consequences for doing that. The fact that the immediate consequences of the market's choice are obvious and the long-term consequences of overriding that choice are invisible (except with great effort) doesn't mean that there are no costs. There is no free lunch. Every choice must be paid for. While you might sometimes "beat the market" and spot the more-optimal solution just the sheer difference in data-crunching capability means that, most of the time, you're going to be wrong. Even if the consequences don't hit for years. Even if you've stopped paying attention by the time the piper comes around to collect his due.
At the end of the day what keeps the system running is that 98% of us are decent people who care about others, even strangers. Jeff Bezos certainly could outbid the starving vagrant. But, unless this were the last meal in the world, would he? Likely not.
And if he did I expect he could be easily persuaded to purchase a more normal meal for the fellow -- it's a trivial cost to him and most normal people would get a good feeling from doing it.
And even if he didn't, in a full economy that high bid lowers the cost of another meal and encourages an increase in meal production, so that 2% of selfish people are still at least pulling their own weight.
It's not that a market always makes things perfect for everyone. It's that, in the long run, it screws up less often that the other systems we currently know of.
To use a more realistic example, it's hard for me to agree that a billionaire values their tenth vacation home more than a homeless person who is in danger of freezing in the winter.
I don't see "value" as a feeling. A freezing person might desire a warm fire, but their value of it is limited by what can be expressed.
That said, a person is a complex asset, and so the starving person might trade in their "apparent plight" (e.g. begging).
For example, the caring seller of the last sandwich might value alleviating "apparent plight" more than millions of shares of AMZN. Whether they do or don't exactly determines the value of an individuals suffering against some other asset, in terms of the last sandwich.
Four months later, the US is seeing a steady 7-day average of 50k to 60k new cases per day. This is a factor of 4 or 5 less than the number of daily new cases that were observed over the December-January third wave period. It seems therefore that one (the?) core prediction of this post, namely, that we'd see a fourth wave sometime between March and May that would be as bad or worse than the third wave, turned out to be badly wrong.
Zvi's post is long, so let me quote the sections where he makes this prediction:
Instead of that being the final peak and things only improving after that, we now face a potential fourth wave, likely cresting between March and May, that could be sufficiently powerful to substantially overshoot herd immunity.
and,
If the 65% number is accurate, however, we are talking about the strain doubling each week. A dramatic fourth wave is on its way. Right now it is the final week of December. We have to assume the strain is already here. Each infection now is about a million by mid-May, six million by end of May, full herd immunity overshoot and game over by mid-July, minus whatever progress we make in reducing spread between now and then, including through acquired immunity.
It seems troubling that one of the most upvoted COVID-19 post on LessWrong is one that argued for a prediction that I think we should score really poorly. This might be an important counterpoint to the narrative that rationalists "basically got everything about COVID-19 right"*.
It seems troubling that one of the most upvoted COVID-19 post on LessWrong is one that argued for a prediction that I think we should score really poorly.
I agree. FWIW, I strong-downvoted this post in December. I think this is the first LW post that I have strong-downvoted before.
Additionally, I commented on it (and on threads where this post was shared elsewhere, e.g. on Facebook) to explain my disagreement with it, and recorded ~the lowest forecast of anyone who submitted their forecast here that there'd be a 4th wave in the US in 2021.
What I failed to do was offer to bet here on the 4th wave question. I think the only time that I tried to make a bet on this topic was in a discussion on Facebook (set to friends-only) that began with "Well, it's time to pull the fire alarm on the UK mutation." I commented on the post on 12/26/20 with the following:
Would you be interested in operationalizing a bet on this? (If you don't think its good practice to bet money on COVID infections/cases/deaths or otherwise aren't interested in betting money, we can just make it a reputational bet.)
I get the sense that like Zvi you are being too pessimistic about how bad the new strain will be for the US relative to how bad thing would have been even without the new strain.
Zvi, I agree with you that the CDC's reasoning was pretty sketchy, but I think their actual recommendation is correct while everyone else (e.g. the UK) is wrong. I think the order should be something like:
Notably, both papers don't even consider vaccinating essential workers as a potential intervention. The only option categories are by age, comorbidities, and whether you're a healthcare worker. The first paper only considers age and concludes unsurprisingly that if your only option is to order by age, you should start with the oldest. In the second paper, which includes HCWs as a category (modeling them as having higher susceptibility but not higher risk of transmitting to others), HCWs jump up on the queue to right after the 80+ age group (!!!). Since the only factor being considered is susceptibility, presumably many types of essential workers would also have a higher susceptibility and fall into the same group.
If we apply the Zvi cynical lens here, we can ask why these papers perform an analysis that suggests prioritizing healthcare workers but don't bother to point out that the same analysis applies to 10% of the population (hint: there is less than 10% available vaccines and the authors are in the healthcare profession).
The actual problem with the original CDC recommendations was that essential workers is so broad a category that it encompasses lots of people who aren't actually at increased risk (because their jobs don't require much contact). The new recommendations revised this to focus on frontline essential workers, a more-focused category that is about half of all essential workers. This is a huge improvement but I think even the original recommendations are better than the UK approach of prioritizing only based on age.
Remember, we should focus on results. If the CDC is right while everyone else is wrong, even if the stated reasoning is bad, pressuring them to conform to everyone else's worse approach is even worse.
Many people on this website are hardcore social distancers, interacting only with essential workers. To them it seems natural that essential workers are the majority of the transmission and do not have immunity yet. But most people aren't social distancing very hard at all. In Nashville, were I currently am, the bars and restaurants are often full. My immune brother when to house parties and indoor concerts on New Years Eve. I doubt that essential workers constitute even a majority of current transmission.
So we vaccinate 80 million people and reduce transmission by 50%, maybe. That would take months. Meanwhile, there are only 50 million Americans over 65, doing >90% of the dying, and we could vaccinate them in just two months.
TLDR; The transmission argument for essential workers assumes people comply with social distancing. People aren't doing that anymore, so vaccinate the vulnerable.
That seems plausible right now, in January, at our current level of social distancing compliance. But why would the degree of distancing stay constant over vaccination? It hasn't even stayed constant the last 8 months when nobody has been vaccinated.
So far we have a clear pattern. People voluntarily comply when the issue seems important because there are lots of infections, hospitalizations and deaths. During lulls the issue becomes less available and compliance drops. In the best case for essential worker vaccination, it produces a lull in February-March. But if you actually drop the reproduction rate then that 3x factor goes away immediately. Unless you have a reliable plan to get people to keep social distancing even when things seem over, vaccinating the vulnerable saves lives in expectation.
Don't forget there's another factor: Coming down with COVID can easily take someone out of the workforce for a couple of weeks.
The essential workers may be at less risk of dying, but depending on how you define "essential" having a large portion of them down for the count could put quite a crimp in your ability to hand out vaccines.
Even if this is right, it still seems incredibly dysfunctional for CDC (and other governing bodies) to not use age categories among healthcare workers, and other essential worker categories.
One point not noted anywhere as far as I can see is that, by allowing the pandemic to spread to millions of people, the risk of a more dangerous or virulent strain appearing increased enormously.
If the pandemic had been kept to relatively small numbers, as in Taiwan, New Zealand, Australia, Vietnam, Thailand, (China if you believe their statistics on this, unlike all their other statistics are correct) etc. this new more infective strain would likely never have appeared.
What is the underlying argument here. I don't understand viral mutations sufficiently to know but have assumed they are largely random events. If so, isn't this claim a bit like a fair coin landing heads for the past 10 flips and claiming the odds of tails has not increase?
I think Zvi is (still) overly confident in pessimism (or, at least, headline-Zvi, as opposed to actual-content-Zvi, which is somewhat more hedged). The new variant is probably pretty bad and the distribution of predictions should look worse compared to what it did a week ago - but there is a ton of uncertainty still, and the headline is unjustified.
Sidenote on predictions: Zvi previously predicted that social distancing would be a thing of the past by the time summer ended, that COVID-19 would cease to be the dominant news story (which would remain the case indefinitely), and that we would have given up to the point of approaching herd immunity by now. Social distancing, though weaker than it once was, is still very much in effect, COVID-19 continues to be the dominate our collective attention, and we have limited the pandemic to the point where we can still potentially save millions of lives with the vaccines.
Zvi and many others on LW (including myself in this) totally failed to predict how people in the US would react to this virus. From this, I've updated that we're bad at predicting how politics and humans will respond to novel unexpected events, and probably a bit overly pessimistic about other humans' ability to be persuaded by rational argument and Real Bad Stuff happening.
I think that predicting the course of the disease or predicting whether a certain variant is more infectious is mostly a different kind of prediction from predicting people's behavior.
Unfortunately, people's behavior in response to the new strain is also really important for how bad it will get, so ¯\_(ツ)_/¯
a bit overly pessimistic about other humans' ability to be persuaded by rational argument and Real Bad Stuff happening.
I am surprised that you say "overly pessimistic"? It seems that the outcome we got of hovering around R=1 with the economy being shut down in large parts for almost a full year was basically the worst-case outcome, with nobody I know being pessimistic enough about how bad it went (it appears to me that the costs of runaway heard immunity would have been drastically less, especially given that we are likely to reach something like 40% prevalence anyways before the vaccine).
Depends on what you mean by "pessimistic," I guess. I think my model back in March was that basically everyone would dismiss COVID as being "like the flu"; tons of people would die; but no one would really pay much attention to it.
Instead, people actually freaked out about it and lots of people actually got overly into enforcing quarantine restrictions on each other. I was expecting that people would fail to even parse the small chance of death by COVID as sufficiently important to be worth worrying about, and that didn't turn out to be true.
I agree that the real outcome is much worse than we could have done overall, with e.g. mass testing or challenge trials -- though I don't agree that this is clearly worse than runaway herd immunity. Back-of-the-envelope calculation: if 1% of the US population died of COVID, that's around 3 million deaths, which in VSL terms is around $30T. The US's GDP for one year is around $20T. My error bars on the validity of VSL at that scale are pretty large, as is my uncertainty about comparing GDP to VSL, and other non-GDP considerations of lockdown... but the two certainly seem comparable in magnitude, and I weakly think that lockdown is better in terms of total social utility.
(edit: of course we're at ~300k deaths now, which changes the analysis by 10% or so; still seems like the calculation comes out about the same as of right now. The effect of another huge wave could change this calculation substantially.)
It is very unlikely that we would have gotten to 100% prevalence in any world, which would be necessary for 1% of the U.S. to die. With all the superspreader dynamics, you would likely reach heard immunity at something like 50% prevalence, maybe even less than that, and we are about 40% of the way there. This also completely ignores age-related effects. The average life-years lost per covid death is ~10-15, since the average person who dies of COVID is much older.
This all results in a VSL closer to 1/10th of the value you cited (~2 for only getting to 50% prevalence and a factor of 5 for age-related effects). Then, if you take into account that we aren't actually on track to prevent most of the relevant deaths (we are already at 20% historical prevalence and are likely to reach 30%-40% before widespread vaccine adoption, suggesting that we are likely to end up with 60-70% of the relevant deaths, compared to the world with zero lockdowns), the numbers really aren't looking good.
This makes the total calculation come out to more something like a counterfactual $1T in VSL terms. I think with that, it's looking pretty unlikely to me that the lockdowns we had were worth it, even just taking into account the economic effect of this year (not to mention that the total impact and length of lockdowns is likely to extend substantially into 2021). I also think this year will have a large number of highly negative long-run effects on institutions, political tension and long-term health for lots of people that will make the overall cost of the lockdown greatly exceed the deaths that were prevented.
Back in March, there was a lot of concern that uncontrolled spread would overwhelm the medical system and some hope that delay would improve the standard of care. Do we have good estimates now of those two effects? They could influence IFR estimates by a fair amount.
Also, my understanding is that the number of infections could've shot way past herd immunity levels. Herd immunity is just the point at which the number of active infections starts declining rather than increasing, and if there are lots of active infections at that time then they can spread to much of the remaining people before dwindling.
Habryka's point is that roughly the same number of people would've died either way, because in both situations the same number of people will get it – something like 40%. But in one of them we *also* shut down the economy for over a year. That's why it's the worst of both worlds – worst of deaths, worst of economy.
You can consider it, but you cannot get it in most Western countries. Either way, it doesn't change Habryka's point that we're currently in the worst possible world.
Have a look at the state of Victoria in Australia, which went from close to 700 cases a day in early August to zero in about 8 weeks. https://www.covid19data.com.au/victoria
For me an important factor is that we have three different pints of data that suggest the new strain is more infectious. First, it's rapidly replacing the existing strain in areas where it is preset. Second, those areas are seeing surges of infections that don't occur in other areas. Third, it seems like individuals infected with the new strain have 3 or 4 times the viral load of individuals with the previous strain - which would neatly explain higher transmissiblility. I'm going with an 85% chance that this is genuinely more transmissible.
I'm not at all sure our current wave will fade before the new strain starts making an impact so I'm 50% on two waves.
Higher peak viral load does correlate with more severe symptoms but not that strongly. I think it's unlikely that this strain is less virulent than the previous one because most transmission happens before symptom onset and there isn't as much selective pressure for that as their would be for a virus with more normal kinematics. Post herd immunity there'll probably be selective pressure for longer incubation periods and that might lead to less virulence, but that's further down the road. Because most severe disease happens when viral load has gone down I figure it's most likely that how well the virus is able to fool the host's immune system causes both peak viral load and severe disease but I'm very unsure about this. Still, this is only a half order of magnitude in max viral load and that varies by many orders of magnitude between individuals and is still only weakly correlated with disease severity so even if it has an effect I don't expect it will be large.
Other sources of evidence (albeit weaker): the nature of the mutations (some of which have been studied prior to emergence of the new strain), the related evidence from South Africa.
Does that [cutting cases by 50% per week] sound like something any Western country could possibly accomplish from here?
Yes. Have a look at the state of Victoria in Australia, which went from close to 700 cases a day in early August to zero in about 8 weeks. https://www.covid19data.com.au/victoria
I sympathise with people in countries run by incompetent buffoons (i.e. most of Europe and the Americas) but it is not inevitable.
Overall a terrific post - your point about the need to act before there is certainty is solid gold.
Also New Zealand, which has a handful of new cases trickling in from arrivals, but approximately zero community transmission due to the managed quarantine at the border. Even if this new strain has the increased transmissibility I expect NZ to not be anywhere near overwhelmed.
One of the differences is that transmission is, for obvious reasons, much, much easier to control on an island. Hawaii isn't doing nearly as badly as the rest of the United States, for example.
The forecasting community is very concerned. The community prediction for a new Metaculus question on whether a single variant that is at least 30% more transmissible than preexisting variants infects 10M worldwide before mid-2021 is currently 87%:
For what it's worth, I personally have a fairly solid forecasting track record and my own predictions are as follows, see more here:
-80% chance this specific new strain is >30% more transmissible
-90% chance *any* new strain before mid-2021 is >30% more transmissible
-65% chance this specific new strain is >50% more transmissible
-71% chance *any* new strain before mid-2021 is >50% more transmissible
29 Dec update:
-85% chance this specific new strain is >30% more transmissible
-93% chance any new strain before mid-2021 is >30% more transmissible
-70% chance this specific new strain is >50% more transmissible
-75% chance any new strain before mid-2021 is >50% more transmissible
FWIW I don't foresee any of these estimates surpassing 95% confidence until we get some virological data to confirm the epidemiological data we're seeing
There is a lot of good information here, but unfortunately a lot of hyperbole, and a lack of sources to allow us to check your numbers.
First, the headline, which conveys emphatic certainty. Contrast that with the body, which says
"all signs point to it being about 65% more infectious than the old one, albeit with large uncertainty and error bars around that. "
"I give it a 70% chance that these reports are largely correct."
(Bolding mine)
Next:
The media told us it was nothing to worry about, right up until hospitals got overwhelmed and enough people started dying.
This is a gross generalization, similar to those made by people set out to demonize the media regardless of the facts. A quick google shows dozens of warnings from CNN from January to late March.
The first US death was mid February. We reached 1000 deaths ("enough" is a very broad term) around March 26.
Back to the first quote above - it mentions "all signs" pointing to something. Best I can tell, it was one study. Please correct me if I am wrong.
What evidence went into the 70% chance estimate?
Under "The Numbers/Predictions" heading- where did the predictions come from? What assumptions were made in creating the predictions? We have no idea.
Under "Deaths" through "Test Counts" - where did the tabular data come from? There is a source for one chart, but that is it. Your comment on the chart seems dubious.
the increased cases in the deep South are mostly [due to] increased testing.
but you only show testing data for NY and USA. Furthermore, if the increased cases are only due to increased testing, positivity should be flat. Your data show it is rising in the South, which supports the premise that the cases are increasing independent of testing.
More hyperbole here:
This definitely does qualify under “hot damn, look at this chart.” This is a huge, dramatic increase in infections happening very quickly. A doubling in one week.
Here is the graph as presented.
Here is the same data in a larger context.
The new variation was detected first in the UK in September. Cases went from about 20 on September 1 to 370 in mid November. Then they *dropped* to 213 before jumping up to 500.
This does not seem to be caused by something in September. If it were, the exponential growth rate we see in December would have started back then.
France had a higher rate of increase, probably not due to this new strain, and nonetheless brought it under some control.
The rate of increase in the UK since Dec 6 is about the same as the US in November.
So while it is possible the new strain is causing the recent surge, it is quite likely that other things have a larger influence.
And finally
Multiple sources confirm that there is no reason to expect a six-months-later second dose to be any less effective a booster.
So why not link to those multiple sources? The nearby link to the margilanrevolution.com does mention the possibility of a 6 month later dose being an option, but provides no data to back that up, other than a single example of a vaccine for a completely different disease.
But ln(370/20)/ln(2) = 4.2. This means that the new strain doubled 4 times between September and mid-November, suggesting a typical doubling time of just over two weeks.
This is approximately what is observed at the end of December.
But indeed, I don't understand why the number of infected people suddenly decreases at the end of November. An explanation would be helpful.
Where can we find the source saying that there were about 20 cases of new strains in September?
But indeed, I don't understand why the number of infected people suddenly decreases at the end of November. An explanation would be helpful.
As henryaj says above, the UK was in a national lockdown Nov 5 - Dec 2. Accounting for a lag in catching it -> positive test, that matches the graph reasonably well
I looked into things a bit and think it's 85% likely that the new variants in the UK and SA are significantly more transmissible, and that this will lead to more severe restrictions globally in the next few months because no way they aren't already in lots of places. I also think there's a 40% chance the SA variant is significantly more deadly than previous variants, but not sure if that means 50% higher IFR or 150% higher (I have no idea what prior to use for this).
Update December 26th: The longer we hear no concerning news about the lethality of the SA variant, the more likely it is that it's indeed benign and that initial anecdotal reports of it being surprisingly aggressive in young-ish people without comorbidities were just rumours. Right now I'm at 20% for it being significantly more deadly, and it's falling continuously.
To be clear, I don't mean to take a stance on how much more transmissible it is exactly, 33% or 65% or whatever. I think it's 85% likely that it's a difference that's significant enough to affect things, but it's less clear whether it's significant enough that previous containment strategies become vastly more costly or even unworkable.
Why are we seeing new variants emerge in several locations independently in a short time window? Is it that people are looking more closely now? Or does virus evolution have a kind of "molecular clock" based on law of large numbers? Or is the "clock" here mostly the time it takes a more infectious variant to become dominant enough to get noticed, and the count started whenever plasma therapy was used or whatever else happened with immunocompromised patients? Should we expect new more infectious variants to spring up all over the world in high-prevalence locations in the next couple of weeks anyway, regardless of whether the UK/SA/Nigeria variants made it there via plane?
AFAICT the reason immunocompromised patients are important is they can stay infected for several months. I read a paper recently where such a patient held on for about 5 months, and by my count, samples averaged 3 mutations per month (although I'm sure there's a better way to adjust the numbers than what I did). So there's time to infect enough IC'd patients, plus n months to evolve in them. If antibodies are a necessary ingredient that would delay these steps more. Then there's time for the highly fit strain to outcompete other strains, which is proportional to 1ln(Rfit/Rother). And finally, time to establish the strain is growing and time to check for evidence of causality.
IIRC the UK strain became a major issue later, but the UK has nearly the best genome surveillance which is why the announcements happened so close to each other. Fuzzy on the timelines, but I think SA announced theirs later. Maybe SA decided to call the press due to the UK announcement instead of waiting for better proof? And/or sped up the search for evidence.
Regardless, assuming both are legit, the close announcement times seem to be mostly coincidence. But I think we should expect other strains with large jumps in R to start being an issue soon, even if most won't be recognized as quickly.
I notice I'm confused- SA's variant, if legitimately due to a huge jump in R, doesn't have huge numbers of mutations.
If the UK variant had a 45% jump in R, and SA's has a 20%, and >20% is much more commonly due to IC'd patients, then it seems reasonable that the super-fit, highly mutated strains show up alongside the more mundanely fit, moderately mutated ones. The super-fit's take longer to bake but they take off faster. But then again I'm trying to make a theory to explain 2 data points that I'm not 100% are both correct, so as much as this feels correct it probably isn't.
So the emerging wisdom is that the SA variant is less contagious, or are you just using 20% as an example? The fact that SA is currently at the height of summer, and that they went from "things largely under control" to "more hospitalizations and deaths than the 1st wave in their winter" in a short amount of time, makes me suspect that the SA variant is at least as contagious as the UK variant. (I'm largely ignoring politicians bickering at each other over this, and of course if there's already been research on this question then I'll immediately quit speculating!)
Oops, missed this. I don't check LW messages much.
20% was not an exact value. At the time I wasn't aware of any estimates. Since then I've heard that the standard curve fit returns a ~50% growth per 6.5 days, some or all of which may be due to immune escape.)
I had a couple assumptions that made me think the SA strain was less contagious in expectation:
High contagiousness is more likely when high mutation numbers were seen, and correspondingly emergence would tend to be later. The SA variant gained local dominance earlier than the UK.
There was (and is) much less data on the SA variant. Due to the high variation in number of infectees per sick person, my prior is that on average, a variant that seems to be gaining ground is not as infectious as a curve fit implies, because luck could be a big factor and is more common than extreme fitness.
I'm confused by your pessimism about England's Tier 4 restrictions:
So basically, if you’re outside where it’s safe, they’ll harass you and maybe worse. Whereas if you stay inside, technically it’s not allowed but in practice it’s a lot less likely anything happens to you, unless the anything in question is ‘you catch Covid-19.’ The rules are porous enough that they aren’t enforceable against the things that are risky but enforceable enough to shut down the relatively safe actions that keep people sane. And with weird exceptions for remarkably large indoor gatherings for certain events that are textbook superspreaders.
All of which is what our model expects to see, and none of which seems likely to be remotely sufficient if the new strain is as infectious as they estimate.
Tier 4's bundle of restrictions is almost identical to those from England's "second lockdown" in November. (See e.g. here.) But you write as though you believe the "second lockdown" was impactful:
[...] the context of England being under lockdown conditions that had previously turned the tide [...]
How effective are these kind of measures at controlling things (a) before the new strain and (b) with the new strain?
This heavily discussed paper from Dec 23 addresses question (b), using the same model the authors previously applied to question (a) in this paper. These papers are worth reading and I won't attempt to summarize them, but some relevant points:
The authors argued for the "second lockdown" in the 2nd linked paper on the basis of its projected impacts on mobility, thus R, thus etc.
The 2nd linked paper was later updated with data from November, showing that their model did quite well at predicting the effect on mobility, R, etc.
The 1st linked paper (on new strain) approximates Tier 4 as being equivalent to "second lockdown" in its effects
The 1st linked paper (on new strain) is worth reading in its entirety as it provides some (provisional) quantitative backing to intuitions about the impact of various measures (Tier 4 / Tier 4 + school closures / Tier 4 + school closures + XYZ amount of vaccination)
Not the OP so can't answer for him, but qualitatively the second (November) lockdown was quite different from the first (March) lockdown - much more leeway given on exercising outdoors, workplaces largely stayed open (even if people were working from home). In March, police officers would move people along if they were sitting on a park bench (as that's not exercise); the second time round things were much less strictly enforced. Rules around forming 'bubbles' with other households also didn't exist in March.
Tier 4 is essentially the same as the November lockdown but you can meet one other person outdoors.
A really key difference between March and November is that schools were open in November but not March. Though the UK is now in a third lockdown, and it looks like schools won't be re-opening
Also, that post points out something that seems important. What could be a better way to motivate people wanting the vaccine, than to show our richest, most famous and most powerful people paying really big bucks to get the shot a few months sooner?
I did not think of this at all until you pointed it out.
IMO The title is overly dramatic and seems to claim that the news about the new strain is more significant than I actually think it is in terms of how much it should cause us to update our views of what infection risk and US COVID-19 deaths will be in 2021.
In this post Zvi doesn't try to forecast how many infections/cases/deaths there would be in the US without this new strain (unless I missed it... it is a long post). Yet he really should, because doing so will lead one to realize that the US is likely going to be at or close to herd immunity by ~May-June anyway, so a new transmissible strain that becomes dominant in the US around that same period can't plausibly make as huge of a difference as Zvi seems to be saying in this post.
Good Judgment's median estimate for "How many total cases of COVID-19 in the U.S. will be estimated as of 31 March 2021?" is ~130M currently. And Good Judgment's median estimate for "When will enough doses of FDA-approved COVID-19 vaccine(s) to inoculate 100 million people be distributed in the United States?" is ~May 1st currently. https://goodjudgment.io/covid/dashboard/
Assuming that 20% of vaccines go to people who had already been infected, this would mean that by May, approximately ~220M people (220M = ~140M + 0.8*100M) the US will be immune, or about 66% of the population. This could easily be higher or lower, but the point is that we're going to be at or close to herd immunity by the time Zvi says this new viral strain would start becoming dominant in the US.
In short, the news would be much worse if this new viral strain had spread to the degree that it has now several months ago. But in reality, I think we'll be at or close to herd immunity already by the time it becomes prominent, so it won't make that much of a difference.
EDIT: I misread Zvi's piece initially and mistakenly thought he wrote that that the new strain wouldn't become dominant in the US until May. I now see that he says "Instead of that being the final peak and things only improving after that, we now face a potential fourth wave, likely cresting between March and May, that could be sufficiently powerful to substantially overshoot herd immunity." Taking this view as true instead makes me see the new strain as significantly worse news: specifically, this two-month shift might be sufficient to make an additional ~10-15% of the population get infected/sick before herd immunity is reached. (I still think the post title is overblown, but still this is a significant update for me.)
My 8-months-ago self would be surprised to learn that the US average COVID-19 deaths/day has risen again to 1,300 deaths/day. I don't understand why this happened. Does anyone know? Is it a combination of vaccine and/or natural immunity not lasting? Or is it that there are still a lot of unvaccinated people? Or were my estimates of how many Americans had been infected so far too high?
What can countries/states do? Impose hard lockdowns, focus test/trace/isolate resources on the new strain, stop travel, get people wearing N95s, create extra hospitals, vaccinate (using less effective vaccines as well as Pfizer/Moderna), run challenge trials to see how vaccines protect against new strain and against transmission, and ... hope for the best. One source of uncertainty is how much news of a complete collapse of hospitals in some region will impact behavior in regions that haven't collapsed yet. (I fear a "boy who cried wolf" scenario, where people think, "We never needed those temporary hospitals last time").
What can individuals do? If the new strain is not more severe, then the risk for young and healthy people remains low. Presumably staying at home and receiving deliveries still has very low risk of infection. People who might need hospital care for non-Covid reasons should make plans. (If health care collapses, how much bigger is the risk from Covid for young people? You'll probably get priority but standard of care will drop substantially.)
EDIT: Added some important points about vaccination I left out.
then the risk for young and healthy people remains low
Don't confuse risk of death with risk overall. I personally know several young people who suffered months of debilitation, in some cases still feeling sick months later. From some limited studies this appears to be common, and permanent damage appears to be not uncommon including damage to testes, brain/memory etc.
At best we do not know the long term effects. Tell someone suffering from shingles (which was eventually found to be a result of prior chicken pox infection) that chicken pox is a "mild" condition.
I stand by my claim. We know the effects 10 months out. If some studies have convinced you otherwise, it would be useful to cite the evidence (maybe in a separate post).
Yeah, I was thinking something similar. It seems the bottom line is we'll have to stay at home and receive deliveries for most of the next 4-8 months, while vaccines and infections bring the world toward herd immunity. So as individuals, we should make sure we're suitably located and supplied for that scenario.
Isn't it weird that the new more infectious Covid strain that will take over the world just so happens to originate in the only place where we are checking for Covid strains?
Some possibilities: - It didn't originate in the UK. It's already widespread in many countries, and the UK just happened to detect it. - There's actually a bunch of more infectious strains all over the place, but they just haven't been detected. The higher infectiousness has already been impacting the covid case numbers for a while.
Some possibilities: - It didn't originate in the UK. It's already widespread in many countries, and the UK just happened to detect it. - There's actually a bunch of more infectious strains all over the place, but they just haven't been detected. The higher infectiousness has already been impacting the covid case numbers for a while.
Looking at daily infections in Western countries, they came down significantly after restrictions were reimposed starting in September. Why is it that only in the UK (and Netherlands + a handful others) are daily infections rising at an alarming rate despite restrictions still in place?
It's a great point. So is your guess that the fact that the new strain originated on the exact country where we do most of the checking for new strains just a coincidence? And not some form of survivorship bias?
There's a possibility that it didn't originate in the UK, but it likely originated either in the UK or one of the other handful of countries that have seen significant spikes in infections despite no loosening of restrictions.
I wonder if the sudden increase is not just the result of some holiday or cold weather some time before. What are the chances that a new strain would dramatically increase daily cases in two countries within a few days of each other. Notably it started to increase in the Netherlands a few days before the UK. If anything this would point to it coming from a third country, yet it would still be odd that the outbreaks progress roughly in the same manner.
Note to mods: I would like to modify this version to add a prediction widget for the proposition "The new English Strain is at least 50% more infectious than the currently dominant American strain of Covid-19" and one for "There will be an additional distinct large wave of Covid-19 infections in the United States 2021". But I forgot where the post is that explains how to create such things I couldn't find it.
Comments from an anonymous source (who I vouch for as a careful thinker) on Dec. 22 and 24:
Hmmm, if Trevor [Bedford] is taking this seriously then I’m updating towards this one maybe mattering
The April mutation scare I found totally unconvincing
I’m still not totally convinced fwiw
[...] There’s some evidence [the new strain] increases viral load, so same vectors, just more likely to get a big enough dose
[...] The last bit hubbub about new strains turned out to be a nothing burger. And unlike Zvi I think super spreader dynamics are totally fine to explain things
If you look across the whole history of each country over time, there are tons of random unexplained massive rise in cases
Is every one of those a new mutation? Absolutely not
[...] How many random unexplained huge rises have we seen across how many countries?
Most countries have had 1-3 big waves, and they’re only sometimes concurrent with each other, across dozens of major tracked countries
So at least several dozen quasi-independent observations[...] even more so if we use sub-regions within countries
Anonymous (Dec. 24): [links to Zvi's post above, arguing the link above isn't wrong but understates the real-world consequences]
David (Dec. 25): I can't say I came away from that post believing that "we're fucked, it's over" (like, beyond what someone might have thought two weeks ago, at least) was a well-argued or reasonable conclusion. The view I held/hold is: "we should be concerned — perhaps very much so — and we might be fucked, but also there's a strong chance not". The "maybe not" doesn't mean "don't be concerned", and he seems to be conflating the two, even while criticizing others for doing exactly that.
There's just a huge amount of uncertainty right now about exactly how contagious this strain is, and he's taking the dead center of the confidence or credible intervals from some very, very early modeling, and possibly not properly accounting for the founder effect along with many other sources of variance over time in number of cases that aren't due to changes in the virus itself. And you can't just say "law of large numbers" (for a complex, dynamic, nonlinear process in which LLN may not apply) or "evidence is evidence" (when there's a ton of noise in our epidemiological data which can make it very difficult to interpret) as a way to dismiss these possibilities.
(Everything else aside, he also made at least one numerically substantial mistake in the extrapolation process: from a chart of daily new cases in the UK, going from ~305/M on Dec 16 to ~500/M on Dec 23, he called that "doubling in one week". Then he extrapolates that, for every arrival of the new strain in the US today, that amounts to 1M infections in 20 weeks. But that's actually a ratio of 1.64x, which extrapolates out to 20k infections in 20 weeks. (Of course the reality is much more complicated than either simplistic extrapolation.))
This is all to say that I think we should be concerned about the new strain, but he's treating some very preliminary analysis as if it's analogous to our state of knowledge about Covid in, say, early February 2020, as opposed to, like, late December 2019.
(Perhaps a tangent, but then again maybe not since this seems to undergird his thinking on this subject: I really don't think it's accurate to say that non-Bayesians are "bonkers". In fact I find it kind of bonkers to say that. One reason is that any attempt to be a Bayesian in the real world runs into huge problems identifying prior probability distributions in any meaningful way which is also inter-subjectively useful. Another, more significant problem with his take on it is that likelihood ratios for "non-academic information", as he puts it, are almost impossible to meaningfully pin down, so it makes them rather thin gruel for an objective discussion, as opposed to confirming pre-existing biases. Not saying such information should be ignored entirely, but nor can they just be plugged into Bayes' Rule in some mechanistic ritual.)
"It’s clear that [testing] demand greatly exceeds supply."
Is this true? Are people that want tests unable to get them? Or do people just not want to get tested? Or did we tell people early in the pandemic that testing capacity was limited and that they shouldn't get tested unless they've been exposed and people still believe that now? I suspect it's the last.
I've had three tests, all paid for 100% by insurance (I think it would be $64 w/o insurance, IIRC). Turn around time on the first (early June) was three days, second (Nov) was three days, and the third (a few days ago) was a day and a half. The only thing I had to do each time was tell them that I was exposed at work, which was varyingly true. My brother gets tested every other week through work. Fiancée got tested at CVS and they didn't even ask her that screening question. I haven't had a single experience leading me to believe tests are in short supply.
Don't tell my employer that. The guy in the office next to me got it (from a meeting at work) and gave it to the girl across from me. There are a total of four offices in my building. I was deemed "not to be a close contact".
The money question to me WRT the UK strain is what it's doing in other countries. Are other countries where the strain has been detected seeing the same rise in cases? Are they doing enough sequencing to know it even if they are?
Anecdotal, but I've lived in a few cities in the United States over the past few months, and testing still varies wildly:
In Los Angeles, during July and August, testing was great. I could get tested whenever I wanted, in a drive through test that never took more than 20 minutes. There were a ton of people getting tested, but the overall operation was efficient, so they were able to process a huge volume of cars (6 lanes, probably around 4 minutes per car) per day. I got tested > 5, < 15 times here.
In New York (Manhattan) things were not as easy. I've been able to do walk in testing at a lab, but it was a 2 hour wait. I've done this twice, and once left due to the wait. This is what is available to the general public. Note that I also get tested through work, and thats self service and reports are within 24 hours, but this is not available to the public. I've been tested >20 times for work, and only twice on my own.
In Montana, we could only get a COVID test if we were 1) prescribed one by the doctor and 2) scheduled an appointment before hand and 3) had an exposure or "reason" we were being tested.
Anecdotally I'd agree that testing demand greatly exceeds supply. A few key locations have matched their testing availability supply with the demand, but by and large the demand still exceeds it across the majority of the United States. I don't think the public conscious still thinks of testing as in the early days (dont get tested unless you show symptoms) - most large metropolitan areas is now used to relatively frequent tests when available, and more rural places simply don't have the same access to testing, so they don't get tested unless they know they've been exposed.
Again, this is anecdotal and not grounded in facts or figures from objective sources. These are just my observations over >20 tests in the past 150 days.
Amazing how it differs by region. Here in the UK, anecdotally tests are pretty easy to come by and turned around rapidly - but are still restricted only to those with canonical COVID symptoms (fever/cough/change in sense of smell or taste).
Although Zvi's overall output is fantastic, I don't know which specific posts of his should be called timeless, and this is particularly tricky for these valuable but fast-moving weekly Covid posts. When it comes to judging intellectual progress, however, things are maybe a bit easier?
After skimming the post, a few points I noticed were: Besides the headline prediction which did not come to pass, this post also includes lots of themes which have stood the test of time or remained relevant since its publication: e.g. the FDA dragging its feet wrt allowing Covid tests, which is somehow still the case a year later; governments worldwide utterly failing at buying capacity or otherwise incentivizing more production of vaccines or tests; endorsing an analysis that Covid spreads via aerosol transmission; etc.
I do have one outsized nitpick with this essay, however. The headline "We’re F***ed, It’s Over" is alarmist, which is in principle fine given its dire prediction, and might make sense to regular readers of Zvi's blog. But once such a post is shared more widely, sometimes the only thing a reader sees is the headline, and it seems to me like this headline cannot, and will not, be properly understood by those who do not know who Zvi is, and how he reasons. Even on LW, many people will not read the entirety of such a long essay, and might lack the context to understand the headline.
Regarding that context:
full herd immunity overshoot and game over by mid-July
...
This has counterintuitive implications, both for public policy and for individuals. As always, one’s approach to the pandemic must be to either succeed if one can do so at a cost worth paying, or fail gracefully if one cannot succeed. Thus, one could plausibly either make the case for being even more careful in response, or to folding one’s hand entirely. You can raise, or you can fold, but you can’t play passive and call all bets and hope to go to showdown.
This perspective makes sense. In these terms, the original prediction suggests shifting one's strategy towards folding or losing gracefully, rather than fighting a losing battle. But that's because this pandemic was never an x-risk. We could afford to play this game of containing the disease (possibly unfortunately so, as argued in this comment chain [LW · GW]), whether we had a realistic shot at victory or not. But game over, in this context, is indeed merely meant as a game loss, by someone who professionally played card games with plenty of variance, and who knows that folding is an entirely valid strategy in such a situation.
But that's not how I expect most people to interpret that headline? Even now, part of me interprets it as claiming "we're all going to die". And if, for example, a sufficient number of x-risk researchers wrote the same headline, that interpretation might be entirely accurate.
In this perspective, there's only one real game we play, and that game must be won. As one fictional character put it:
There can only be one king upon the chessboard.
There can only be one piece whose value is beyond price.
That piece is not the world, it is the world's peoples...
While survives any remnant of our kind, that piece is yet in play...
And if that piece be lost, the game ends.
To conclude, I understand that these posts are written at a speed premium, and would not complain about a random sentence like this; but as a headline of a >270-karma post, this is rather suboptimal.
Your post inspired me to research the mutations of SARS-COV-2 a bit myself, so I would have context before coming back to properly engage with your post. I still am very overwhelmed, but thank you for writing it.
Deaths in Europe continue to run close to those in the United States, suggesting the Europeans are finding cases less often than we are, or have worse medical care or are worse at protecting vulnerable populations.
Note that Europe & the EU both have significantly higher median ages than does the U.S. (~42 & 42.6 versus 38.1).
It should be possible to make rough estimates of chance the UK strain has reached country X by looking at the spread within the UK (where there's some coverage) and extrapolating based on volume of travel within UK and between UK and country X. If the UK data is too sparse now, it should be possible to do this in a week or two.
Focusing on the Alpha (here 'English Strain') parts only and looking back, I'm happy with my reasoning and conclusions here. While the 70% prediction did not come to pass and in hindsight my estimate of 70% was overconfident, the reasons it didn't happen were that some of the inputs in my projection were wrong, in ways I reasoned out at the time would (if they were wrong in these ways) prevent the projection from becoming true. And at the time, people weren't making the leap to 'Alpha will take over, and might be a huge issue in some worlds depending on its edge spreading and how fast we vaccinate' at all.
We also saw with Omicron how, when the variables turn out differently, we do see the thing I was pointing towards, and how people are slow to recognize that it might happen or is going to happen. I do think this had the virtue of advancing the understanding of what was plausibly going to happen. If it overshot a bit in terms of how likely it had its core predictions coming true, that's something to improve going forward, but very much a 'man in the arena' situation, and much better than my 'not be confident so say little or nothing' approach that I shared with most others in Jan/Feb 2020.
To what extent this justifies inclusion in a timeless list is up for grabs, but I think it's important that the next time we notice something like this, we speak up fast and loud (while also striving for good calibration on the chance it happens, and its magnitude)
"Under this model we estimated a growth rate of 71.5 per year, corresponding toa doubling time of 3.7 days (95% CrI: 2.4 – 4.9) and a reproduction number of 2.27 (1.84 – 2.73)"
I dunno, it's not so clear to me that we should expect "fourth wave in the US" as opposed to "fourth wave in one or two cities of the US". Think of how it took 12 months to get from Wuhan to where we are today ... I don't think that's all isolation fatigue, I think it's partly that region-to-region spread takes a while. Trevor Bedford offered the mental picture: Wuhan was a spark in November, and 10 weeks later it was a big enough fire to throw off sparks that started fires in Italy, NYC, etc., then 10 weeks later those fires were big enough to throw off sparks to other cities etc., and many rural areas were finally getting their first outbreaks in the most recent couple months. Maybe something like, "R0>1 only because of a small number of unusually infectious people (either due to quirks of biology or behavior / situation), so it's likelier than you would think for a contageon to never start in a particular place, or to fizzle out immediately by chance". Then maybe it takes until late summer for the new strain to really get going in most places, by which time you have vaccines and weather / sunlight mitigating it.
...But maybe NYC and Boston are first in line again. Strong travel connections to England...? :-/
I dunno, I could see it going either way, behaviors (especially travel levels) are different now than last year, as are immunity levels.
Low confidence, I haven't thought too hard about it.
This article says it's worth watching but doesn't want to ring the alarm yet. It notes that the prior on mutations being bad is low, as there's been a lot of them with this virus. (H/T Alyssa Vance.)
I did a series of podcasts on COVID with Greg Cochran and Greg was right early on. Greg has said from the beginning that the risk of a harmful mutation is reasonably high because the virus is new meaning there are likely lots of potential beneficial mutations (from the virus's viewpoint) that have not yet been found.
There was a huge number of cases before September around the world. Why didn't we see the new more transmissive variants earlier? (One source could be cross-over from some animals, another is the rare cases of extremely long-lasting Covid infection. Curious if people are doing Bayesian calculations for this.)
It could be the time lag from when antibody-based plasma therapy (if that makes sense, I'm not even sure that's how it works) started to be used somewhat widely, plus the time it takes for a new variant to spread enough to get noticed.
There is also quick growth in Czech republic and Netherlands. It looks like new strains are already there. Also, what worry me, is what happen when these new strains from different places recombines.
Also, what worry me, is what happen when these new strains from different places recombines.
As far as we know, we don't have evidence that indicates that recombination is likely. It's a virus and not a bacteria that can simply exchange plasmids.
Correct me if I'm wrong, but I was under the impression that recombination is not a thing for RNA-based lifeforms? That, and it would require at least some form of 'pollination', I believe?
In response to "What does 70% more infectious mean?", I found this slide deck, with the relevant part on slide 17, which I will reproduce below (N501Y is the name of the relevant mutation):
For example, under the additive assumption, an area with an Rt of 0.8 without the new variant would have an Rt of 1.19 [1.04-1.35] if only N501Y was present
...
For example, under the multiplicative assumption assumption, an area with an Rt of 0.8 without the new variant would have an Rt of 1.18 [1.02-1.40] if only N501Y was present
TL;DR: it appears "up to 70% more infectious" is based on observed data, so that if you previously observed an Rt of 0.8, you should expect to observe a new Rt of somewhere between 1.0 and 1.4 with the new strain, ceteris paribus.
EDIT: I previously included this bottom section, which MichaelLowe points out doesn't make sense and I also realized is wrong; see comment thread below.
I found the Wikipedia article on the new strain to have the most clear explanation of the calculation, that this is the result of the observed doubling time being reduced from 6.5 days to 6.4 days; I'll quote the relevant bit:
Data seen by NERVTAG included a genomic analysis showed that the relative prevalence odds of this variant doubled every 6.4 days. With a presumed generational interval of 6.5 days, this resulted in a selection coefficient of
ln(2)⋅6.5/6.4=+0.70(+70%)
They also found a correlation between higher reproduction rate and detection of lineage B.1.1.7. While there may be other explanations, it is likely that this variant is more transmissible; laboratory studies will clarify this.
Thanks for the explanation. I do not understand the formula however. As I read your explanation, if both strains had the exact same doubling time of 6.5 days, one strain would still be ln(2) *6.5/6.5 = 0.69 more infectious than the other one, so I must be misunderstanding.
We are trying to solve for the selection coefficient, which I interpret as "how much of an advantage does this strain have over the previous strain".
It is here that I realize I don't know how the Wikipedia editor found the 6.4 number, I couldn't find it anywhere in the citation. The calculation they perform with the log odds comes from the YouTube video, which in the cited segment is actually talking about a different lineage, B.1.177 (this is different from B.1.1.7 ! Did the editor confuse these two?)
Logistic growth model indicates VUI grows +71% (95%CI: 67%-75%) faster per generation (6.5 days)
Limitations: Sample frequency is noisy & overdispersed in ways not captured by this model
So it turns out that this log odds calculation is not relevant to how we get this "70%" number, it was actually simply interpolated from the data by performing a logistic regression.
EDIT: I have now edited Wikipedia to remove the original calculation using the log odds.
Operationalizing "There will be an additional distinct large wave of Covid-19 infections in the United States 2021" as "The 7-day average of new cases according to Worldometers will decrease by at least 33% from a previous value in 2021 and then later increase to at least 150% of the previous high", I'm forecasting 38%.
(EDIT: Update 12/28: I updated my forecast to 48% after realizing that I had my timing wrong on when the new strain might become dominant in the US. Previously I thought Zvi said something like 'not until May, or maybe June or July', but I now see he actually said "Instead of that being the final peak and things only improving after that, we now face a potential fourth wave, likely cresting between March and May, that could be sufficiently powerful to substantially overshoot herd immunity." If the new wave actually becomes dominant in March (or early April) (instead of May or later, as I mistakenly thought Zvi was saying before) and is as transmissible as it seems, that will probably be soon enough that there will still be enough not-immune people for there to be a significant surge in cases to cause the above forecasting question to resolve positively.)
This operationalization isn't that great because changes in numbers of tests could affect it a lot, but at least it's concrete.
Alternatively we could operationalize it in terms of the midpoint newly infected estimate at https://covid19-projections.com/ . Doing this and using the same 33% and 150% as above, I'd forecast 32%.
(For the Elicit question in the post, I went with the first operationalization and said 38% (EDIT 12/28: Now 48%.))
My operationalization of this question that I defined above on 12/26/20:
There will be an additional distinct large wave of Covid-19 infections in the United States 2021" as "The 7-day average of new cases according to Worldometers will decrease by at least 33% from a previous value in 2021 and then later increase to at least 150% of the previous high.
The peak 7-day average of US cases on Worldometers was [256,191 cases/day](https://www.worldometers.info/coronavirus/country/us/) on January 11, 2021.
For this question to resolve positively per my operationalization, the 7-day average of US cases on Worldometers would need to exceed 150% of that number, i.e. 384,286.5 cases/day.
That in fact happened: On 12/31/2021, Worldometers reports 397.409 cases/day, so the question resolves positively.
Had 2021 ended one day sooner, the question would have resolved negatively, as the 7-day average of cases on 12/30/2021 was 353,932 cases/day, still below the necessary 384,286.5 cases/day threshold. Wow!
My final forecast was 25%, so I get the worst Brier Score of anyone. I also clearly failed to anticipate new variants. The fact that Omicron came so close to the end of 2021 doesn't save my forecast from from the fact that it negligently ignored the possibility of variants.
And to be fair to everyone else, they probably didn't have my specific operationalization in mind, which clearly could matter a lot to the resolution of the question, so I'll let others judge their own forecasts.
In regard to priorities between young frontline workers and the at-risk elderly. I hope they're optimizing for saving life-years, and not lives (ie. if a healthy 20yo has 60yrs ahead of them, and a healthy 70yo has 10yrs ahead of them, saving the 20yo saves 6x as many life-years)
Other than that interesting post, I'll be keeping an eye on that new strain.
I downloaded the dataset from OurWorldinData and estimated the % of cases coming from the UK strain based on the GSAID chart (Note: It's unclear what exactly they mean by "Week 47", so the percentages might be off by up to 7 days, but I did my best.) If there is better data on this, (In particular, an updated GSAID dataset) please let me know, I couldn't find any. I would be happy to redo the below analysis with data past 11/16.
On the below charts, the top chart is total Covid cases. The bottom chart is total Covid cases broken down by strain. I started this by saying I thought you were overreacting, but then I deleted that sentence, because now I'm not sure. One thing you will notice that is lost in the above is that the emergence of the new strain was immediately followed by a large reduction in total cases. It was already at 10% of sequenced strains by ~11/16. This gives me some hope that things are not as dire as maybe they appear. Without the data from 11/17 onward, it seems really hard to say what's happening in the UK with respect to the new strain. But I'm finding several sources now that are saying current infections in the UK are ~50% new strain. So that would be consistent with the possibility that lockdowns leveled out the old strain infections at ~15000 per day and the rise over the last few weeks is all attributable to the new strain. But I think ultimately the data I have is inconclusive.
Can you explain what you mean by this in regards to Los Angeles?
"This seems to be what you get when you shut everything down for months and months on end"
Restrictions are pretty strong at the moment, but as far as I can tell from looking at LA county data, the restrictions that went into effect as the end of November approached followed a trend of rising hospitalizations consistently rising from the end of October. And given the day-to-day essential freedom of activity I enjoyed from May through then, I'm not sure how I'd justify characterizing the county as everything-shut-down unless I shrank the definition of "everything." I didn't actually go to the pool or beach parties, but I got the invites.
I appreciate a good deal of the rest of the analysis, just puzzled by this bit. Is it a statement of how civil direction feels, or is it about specific limitations (perhaps including some I don't much notice)?
FYI, I'm not actually forecasting 50% on the two Elicit questions at the end of the post. Tapping on the distributions caused me to unintentionally make forecasts on them. I was able to modify the forecasts, but saw no way to remove them, so just set them to 50% so as to hopefully mislead others as little as possible. (While I'd like to actually make forecasts on these questions, I think how they are operationalized matters a lot and yet I did not see any operationalization provided for them.)
The first time, I made the mistake of not thinking hard enough early enough, or taking enough action. I also didn’t think through the implications, and didn’t do things like buying put options, even though it was obvious. This time, I want to not make those same mistakes. Let’s figure out what actually happens, then act upon it.
I acted in March, and I want to act again. As a former money manager, I know exactly how I would hedge this risk. My current issue is that I am not fully convinced that this issue will lead to weakness in capital markets.
Let's say we use the US stock market as the hedging tool (an S&P 500 ETF like SPY or VOO). What would need to happen for it to fall a considerable amount (10%+)?
Additional restrictions across the board for a considerable amount of time without appropriate stimulus.
I don't have the confidence to believe that the statement above will happen. We are about to enter an era of a democratic president, democratic majority in the house of representatives, and a potential tied senate. I am confident that more stimulus will pass if needed.
I am not sure how politically viable it is to enact additional restrictions in Europe / North America. I am sure some majors, governors, heads of state will enact additional restrictions, but I doubt it will be a coordinated effort. Furthermore, I am also not confident the populace will follow said restrictions.
So at the moment, I am convinced that this is serious, that it will probably cause significantly more loss of life in the next 6 months, but it won't affect capital markets they way COVID-19 did back in March.
On a personal level, we are increasing our protections towards our elders. Here's to hoping they get vaccinated by the end of February.
Ok, that took me 20 minutes, but they should now all be on a better CDN. Please let me know if anyone still runs into problems with the images not loading!
Huh, very weird. If you have a screenshot of broken images you can copy-paste here, would be useful. I tried to fix all of them, so would be surprised if they are broken for anyone.
The measles booster comes a year later. Multiple sources confirm that there is no reason to expect a six-months-later second dose to be any less effective a booster.
About this, strange stuff seems to be happening in Lithuania (that's Europe). After around 6 months, you get an invitation for a booster. Previously, you could just test for antibodies and if there were high enough, postpone your booster. This seemed reasonable.
Now they are simply canceling green passes (this thing lets you in malls and other non-essential amenities etc etc) for those who are due to get their third shot. This leads many people to justly question their intentions. The trust is at an all-time low here.
There's also a very curious document which supposedly states that EU is promising to buy enough vaccines to jab everyone around 8 times (disclaimer: I have not read the document deeply enough, so I'm looking for anybody adept at legal language).
The big problem I see is that so many of the sources of information about what's going on have their own preferred solutions, and their own side-agendas that they're taking advantage of the crisis to push.
And that wouldn't be an inherent problem except that a lot of them have built up quite a history of telling any lie that seems convenient for getting people to do as they're told.
And then they wonder why even their more reasonable demands are met with skepticism and pushback.
Here where I live the lockdown rules are obviously nonsensical and arbitrary and designed to hurt certain demographics that have annoyed the governor in the past. Meanwhile they just as obviously won't add much to stopping the spread beyond what people are already doing on their own. Restaurants are only allowed to do takeout orders. Stores have to limit themselves to a small portion of capacity. But we're keeping the schools open... Attendance is mandatory per the truancy laws. And the teachers at the school aren't allowed to ask or talk about potential covid cases because that would be a HIPPA violation...
Even if you assume the people in charge aren't malicious, in a lot of ways they're totally incompetent. And on top of that they're dishonest, so even if what they suggest sounds like a good idea it takes a lot of effort to determine if they're actually basing it on the truth or not.
Yup. We're doomed. Either the virus will get us, or the panicking masses will submit to totalitarianism out of fear. Doesn't matter which. We're doomed.
I think at least some of the reason for the UK's vertical line is increased testing capacity (up by about 60% since 1 Dec). If you look at cases per test comparing 1 December to nowish the number is up about 40% (I picked a couple of points on the 7 day average). Which is quite different to the doubling being presented raw.
My father sent me this video (24 min) that makes the case for all of this being mostly a nothingburger. Or, to be more precise, he says he has only low confidence instead of moderate confidence that the new strain is substantially more infectious, which therefore means don’t be concerned. Which is odd, since even low confidence in something this impactful should be a big deal! It points to the whole ‘nothing’s real until it is proven or at least until it is the default outcome’ philosophy that many people effectively use.
I think this is a great video, it explained a lot of things very clearly. I'm not a biologist/epidemologist/etc., and this video was very clear and helpful. In particular the strong prior "a handful of mutations typically does not lead to massive changes in reproduction rate" is a valuable insight that makes a lot of sense.
That being said, the main arguments against this new strain variant being a large risk seem to be:
The prior mentioned above.
The fact that current estimates of increased transmission rates are based on PCR testing, which does not identify variants.
The possibility of alternative explanations for the increase in nationwide infections in the UK, which have not been sufficiently ruled out (in particular superspreaders).
I think he is claiming that the NERVTAG meeting minutes are drawing a causal link between the lower ct value of this variant on PCR tests and its increased transmissibility, and that this is an uncertain inference to draw.
However, personally I think the strongest case for the increased transmissibility of this new variant comes not from indirect evidence as presented above, but from the direct observation of exponential growth in the relative number of cases over multiple weeks/months. See for example the ECDC threat assesment brief or the PHE technical briefing. These seem to strongly imply that, while being agnostic about the mechanism, this new variant is spreading very rapidly. So all things considered the linked video makes me update only very weakly towards a lower probability of this new variant being massively transmissible - a good explanation for growth shown in both reports is still missing if it is not inherently more transmissible.
I don't see much confusion about why cases are growing in England despite being under lockdown. I think it's the same reason why cases are growing in Southern California despite being under lockdown. People are tired of restrictions, enforcement and public messaging is a total joke, etc. and all of this is happening during Christmas time.
…illustrate that slowing things down is all that’s being aimed at. Which is good, because it’s too late anyway. There would not be any drivers to test if this was a real attempt at containment.
If the estimate of 65% more infectious is correct: The strain doubles every week under conditions where other strains are stable.
I disagree. It's popular to say "mass testing isn't as good as shutting down the economy". But there are three problems with that argument.
We don't have a policy levers (state capacity or political will) to shut down the economy more than currently.
Shutting down the economy further would cause more costs than gains.
For the vaccine part, the amino acids sequence of the new variation does not change too much for the vaccine to be ineffective (according to the professional), so it's not over "yet".
Not sure why the down votes on this one. One of the arguments made at the outset was that a possible vaccine would, for technical reasons specific to coronaviruses generally, cover likely mutants. I don't think the new strain changes anything, but it might politically justify continuing restrictions