Nursing doubts
post by dynomight · 2024-08-30T02:25:36.826Z · LW · GW · 23 commentsThis is a link post for https://dynomight.net/breastfeeding/
Contents
Except… The one big trial How much did breastfeeding increase? Did more breastfeeding lead to healthier babies? Did more breastfeeding lead to better long-term health? Intermission Did more breastfeeding lead to higher IQ? Did more breastfeeding lead to higher IQ later in life? Nursing doubts None 23 comments
If you ask the internet if breastfeeding is good, you will soon learn that YOU MUST BREASTFEED because BREAST MILK = OPTIMAL FOOD FOR BABY. But if you look for evidence, you’ll discover two disturbing facts.
First, there’s no consensus about why breastfeeding is good. I’ve seen experts suggest at least eight possible mechanisms:
- Formula can’t fully reproduce the complex blend of fats, proteins and sugars in breast milk.
- Formula lacks various bio-active things in breast milk, like antibodies, white blood cells, oligosaccharides, and epidermal growth factor.
- If local water is unhealthy, then the mother’s body acts as a kind of “filter”.
- Breastfeeding may have psychological/social benefits, perhaps in part by releasing oxytocin in the mother.
- Breastfeeding decreases fertility, meaning the baby may get more time before resources are redirected to a younger sibling.
- Breastfeeding may help mothers manage various post-birth health issues?
- Infants are often given formula while lying on their backs, which might lead to fluid buildup in the ears and thus temporary hearing loss during a critical development period?
- Breastfeeding is cheaper??
Second, the evidence for breastfeeding is overwhelmingly observational: It’s not based on experiments, but rather looking at the existing population and “observing” that breastfeeding is correlated with having mildly fewer infections (of many kinds) and slightly lower obesity. It may also be correlated with better outcomes in terms of allergies, diabetes, lymphoma, colitis, Crohn’s disease, or later IQ.
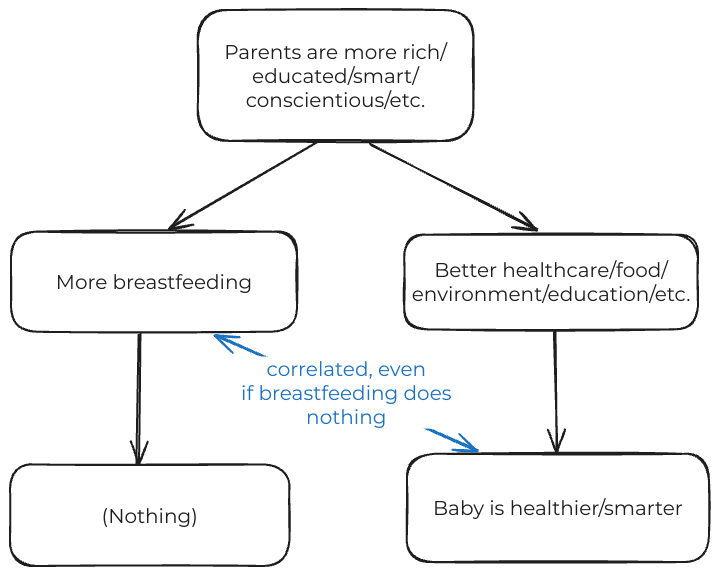
Observational evidence is disturbing because correlations are bad. Even if breastfeeding did nothing, people think it’s good, so the same parents who breastfeed more tend to have higher socioeconomic status and provide lots of other goodies too. Babies that wear baby Rolex watches are probably healthier on average. But that’s because their parents are rich, not because Rolexes are good for you. Could breastfeeding be like that?
Of course, experts are aware of this issue. They try to compensate for it by “controlling” for upstream variables. The most-cited meta-analysis on breastfeeding and IQ collected 18 papers that each controlled for different things, like parental education, social status, or how much social interaction the baby got. The control variables seemed to matter a lot:
| Among studies that… | Breastfeeding associated with a… |
|---|---|
| Did not control for maternal IQ | 4.1 IQ point increase |
| Controlled for maternal IQ | 2.6 IQ point increase |
But what about paternal IQ? Might smarter dads convince mothers to breastfeed more? What if you forgot to control for something, or your data was noisy, or the relationship is nonlinear? (What if smarter babies manipulate their mothers into breastfeeding more?) If any of that happens, then correlations will probably exaggerate the causal impact of breastfeeding.
So there’s been a small movement in recent years to push back against Big Nurse, to argue that, despite the public health messaging, there is no clear evidence that breastfeeding is beneficial. (See Stuart Richie at Science Fictions or Emily Oster at Five Thirty Eight or The Guardian for good versions of this argument.)
Naturally, I am sympathetic. Down with groupthink! Down with control variables! Down with putting so much pressure on mothers based on weak evidence!

Except…
Imagine you just gave birth on a desert island—one that for some reason has an unlimited supply of formula. You’re considering breastfeeding your baby, but you can’t read any studies. What should you do?
Well, there’s an obvious evolutionary argument. Maybe the epidermal growth factor and obscure mix of fats in breast milk are crucial. Or maybe they aren’t. But they’re probably not bad. So it seems like breastfeeding might be good or might be useless, but it probably isn’t harmful? It seems safest to breastfeed if you can, right?
Now, if you don’t trust all these correlational studies that claim positive results, throw them out. But then, you’d still want to breastfeed because of the evolutionary argument. Some skeptics seem to be not just disregarding these studies but seeing them as evidence of no effect. That seems wrong.
And we don’t only have correlational studies. We also have one large randomized trial.
The one big trial
If you decide some day to run a randomized trial on breastfeeding, you will soon notice a problem: You can’t gather a bunch of babies and then choose half to be breastfed, because (a) their mothers would ignore you, and (b) stopping kids from being breastfed is correlated with going to prison.
The best you can do is gather a big group of mothers, and then try to convince half of them to breastfeed more. And then you have to compare all the babies in the two groups, because if you pick out only those who were/weren’t breastfed, then you’re back to correlations. (We talked about this kind of “intention to treat” study design before when looking at colonoscopies.)
The PROBIT breastfeeding trial was run in Belarus between 1996 and 1998. This was a good time and place to run a trial, because Belarus at the time resembled rich countries in having access to basic medical care and sanitary water, but fairly low baseline breastfeeding rates. The trial worked with 32 hospitals across the country. At half the hospitals, researchers intervened by training staff on methods to maintain lactation and promote breastfeeding. The other half were left as controls. Researchers only tracked women who breastfed at least some. During the trial, 17,795 such women gave birth at these hospitals. (One control hospital was discovered to be faking their data and thus excluded.)
So, first question:
How much did breastfeeding increase?
That depends on what you measure:
| Breastfed at 3 months | Intervention | Control | Difference |
|---|---|---|---|
| any | 72.7% | 60% | 12.7% |
| mostly | 51.9% | 28.3% | 23.6% |
| exclusively | 43.3% | 6.4% | 36.9% |
| Breastfed at 12 months | Intervention | Control | Difference |
|---|---|---|---|
| any | 19.7% | 11.4% | 8.3% |
| mostly | 10.6% | 1.6% | 9.0% |
| exclusively | 7.9% | 0.6% | 7.4% |
Which “type” of breastfeeding matters most? Intuitively, you’d think that the first feed for a newborn matters more than one last feed before a two-year old is fully weaned. But nobody really knows.
This trial increased different “types” of breastfeeding by different amounts. This makes everything else tricky to interpret, since we don’t know what “type” is most important. But let’s not miss that all the increases are modest: All the numbers in the right-hand columns of the above tables are much smaller than 100%.
OK, second question:
Did more breastfeeding lead to healthier babies?
For gastrointestinal infections and rashes, probably. For respiratory infections and croup, maybe. And for ear infections, probably not.
| Outcome | Intervention | Control | Significant? |
|---|---|---|---|
| Gastrointestinal infection | 9.1% | 13.2% | ✓ |
| Hospitalization for gastrointestinal infection | 3.2% | 3.6% | × |
| Any rash | 12.3% | 18.3% | ✓ |
| Eczema | 3.3% | 6.3% | ✓ |
| Non-eczema rash | 9.9% | 13.5% | ✓ |
| ≥2 Respiratory tract infections | 39.2% | 39.4% | × |
| ≥2 Upper respiratory tract infections | 36.1% | 36.2% | × |
| Hospitalization for respiratory tract infection | 17.9% | 20.5% | × |
| Croup | 17.9% | 20.5% | × |
| Ear infection | 6.2% | 6.0% | × |
| Death :( | 0.25% | 0.35% | × |
Skeptics typically accept that the significant results above are probably real, but suggest that the impact is small—e.g. only a 4% decrease in the chance of the baby getting a GI infection.
I totally disagree with that.
Remember, that 4% decrease is not the result of “breastfeeding” instead of “not breastfeeding”. All babies in this trial got at least some breastfeeding! That 4% decrease is the result of a modest increase in breastfeeding intensity. If you ran a trial that compared no breastfeeding to exclusive breastfeeding for 12 months, the impact would surely have been much larger.
Note: The benefits of breastfeeding may be somewhat lower for the median reader of this blog than the median late 1990s Belarusian. You probably have access to cleaner water, more/better medical care and newer formula that includes things like DHA, ARA, and more nucleotides.
Did more breastfeeding lead to better long-term health?
The researchers checked in on the babies repeatedly as they became children and eventually teenagers. They found… essentially no effect!
- When they were 6.5 years old, asthma and allergies were very slightly worse in the intervention group.
- When they were 11.5 years old, BMI, height and blood pressure were a tiny bit higher in the intervention group.
- When they were 16, there was no benefit in terms of weight and blood pressure, and BMI was again slightly higher. The intervention group did very slightly better in eczema and asthma and slightly worse in terms of lung function.
(They also discovered in the last follow-up that another hospital was faking data.)
None of these results were significant, and all of the magnitudes are tiny. Many of the differences are probably just noise. It’s hardly conclusive, but if modest increases in breastfeeding led to massive improvements in long-term physical health, you probably wouldn’t get the above results. So this is some evidence that modest increases in breastfeeding don’t lead to gigantic improvements in long-term health.
Intermission
Here’s a woman in 1903, simultaneously breastfeeding a human infant and a bear cub.

Did more breastfeeding lead to higher IQ?
The original PROBIT study didn’t measure IQ, possibly because there are no IQ tests for 1-year olds. But a few years later, they had doctors track down most of the kids and give them an intelligence test when they were 6.5 years old.
| Outcome | Intervention | Control | Significant? |
|---|---|---|---|
| Vocabulary | 53.5 | 46.9 | ✓ |
| Similarities | 56.6 | 50.7 | ✓ |
| Block designs | 57.2 | 54.6 | × |
| Matrices | 52.8 | 50.9 | × |
| Verbal IQ | 108.7 | 98.7 | ✓ |
| Performance IQ | 108.6 | 104.8 | × |
| Full-scale IQ | 109.7 | 101.9 | × |
A 7.8 point increase in full-scale IQ? From a modest increase in breastfeeding intensity? I am very skeptical.
The above results were not blind. The doctors administering the tests knew if their hospital was in the intervention group or not. So the researchers took a random group of 190 children and sent them to an independent (blinded) psychiatrist.
| Outcome | Intervention | Control | Significant? |
|---|---|---|---|
| Vocabulary | 51.7 | 50.6 | × |
| Similarities | 54.2 | 51.2 | × |
| Block designs | 55.9 | 53.7 | × |
| Matrices | 50.2 | 48.9 | × |
| Verbal IQ | 105.2 | 102.1 | × |
| Performance IQ | 105.2 | 102.6 | × |
| Full-scale IQ | 105.7 | 102.6 | × |
These results seem more believable. None of the differences are significant, but a non-significant result doesn’t mean the true magnitude is zero. If the true difference in full-scale IQ were 3.1 points as above, there would be no chance of significance with a sample of this size. It’s uncertain, but given this data, the best guess is 3.1 points, not 0 points.
Is 3.1 points small? Well, a 100 IQ is higher than that of 50% of the population, while a 103.1 IQ is higher than 58%. Adding 3.1 IQ points to a kid ranked 13th in a 25-person class would push them up to around 11th. And, personally, if you were going to drop my IQ by 3.1 points, I would not be super stoked about it.
And remember, 3.1 points is still just the impact of a modest increase in breastfeeding intensity. If you ran a trial that compared no breastfeeding to exclusive breastfeeding for 12 months, the impact would surely have been much larger.
The researchers also had (blinded) teachers rate the academic performance of the students. Across reading, writing, math, and other subjects, the intervention group always did slightly better, to an amount corresponding to 1 or 1.5 IQ points. Which, again, is pretty small. But what do you expect from a moderate increase in breastfeeding?
If you combine those two sources of evidence and then extrapolate to a comparison of “lots of breastfeeding” vs. “no breastfeeding”, what’s your best guess? For me, I’d say 5-10 IQ points.
Of course, we don’t know that there’s a 5-10 point (or even a 1 point) increase. It might just be noise. But these results are definitely consistent with breastfeeding having a pretty substantial effect.
Did more breastfeeding lead to higher IQ later in life?
Much later, another group followed up and tested most of the cohort again, at the age of 16. This time they used a computer-administered test. Their results were that the intervention group did slightly better on average: 0.8 IQ points higher.
These results are often presented as contradicting the previous study. (“Breastfeeding doesn’t impact IQ after all!”) Of course, the 0.8 point difference might just be noise. But if it were real, would it contradict the previous 3.1 point difference? I don’t think so.
Consider teaching. It’s known that great teachers (and small classes) in kindergarten increase student test scores. But the benefits “fade out” over time. By the time those kids are in 7th or 8th grade, the benefit is gone.
Or consider a pair of identical twins, one of which is adopted into a poor family, and the other a rich family. My intuition is that the benefit of starting out rich would have an increasing impact on IQ over time. (“The rich kid gets better day-care, which leads to better performance in school, eventually a better college, a higher-paying job, a smarter spouse, etc.”) But this intuition seems to be wrong! The genetic heritability of IQ increases over a lifetime. The twins seem to converge, not diverge and the benefits of starting out rich fade out.
So a significant difference at age 6.5 that declines to much less at age 16 isn’t a weird contradiction that needs to be explained. That’s a common pattern.
Nursing doubts
Given the immense pressure our society puts on women to breastfeed, I always assumed the evidence for it was overwhelming. After all, breastfeeding is natural. And nature doesn’t care about being convenient or politically correct.
But I think the skeptics have a point. The evidence for breastfeeding is much shakier than people realize.
Why is breastfeeding sacred? Why do I feel so uncomfortable even examining the evidence? I mean, ultrasonic humidifiers might be bad for you, but you run 3 ultrasonic humidifiers in your house and no one bats an eye! I think breastfeeding is different because… public health people decided it should be, and we’ve internalized their messaging.
But just because the public health people might be over their skis doesn’t mean they’re wrong. (“Even a stopped public health person over their skis is right twice a day.”)
The priors clearly suggest that you should breastfeed if you can. And shaky evidence isn’t proof that breastfeeding is useless. We have one big RCT, which suggests breastfeeding does make babies a bit healthier, and probably boosts IQ for young children—possibly by a sizable amount.
But if you can’t breastfeed, the good news is that this RCT doesn’t suggest this dooms your child. The impact on long-term health and long-term IQ both seemed to be small. In this trial, not breastfeeding looked less like brain damage and more like a really bad kindergarten teacher. Update your prior as you see fit.
23 comments
Comments sorted by top scores.
comment by Valentine · 2024-09-03T15:18:56.484Z · LW(p) · GW(p)
I think breastfeeding is different because… public health people decided it should be, and we’ve internalized their messaging.
I haven't gone around and checked much, but my gut impression isn't that this is about public health people. I think it's more like a Chesterton's Fence backlash against previous generations' experts claiming that formula was obviously better. IIRC, mothers were warned against using breastmilk and told to go to formula instead, because it's Scientific™. So it took some cultural pushback to reclaim evolution's solution to feeding newborns.
Replies from: dynomight↑ comment by dynomight · 2024-09-08T14:15:09.532Z · LW(p) · GW(p)
My impression was that the backlash you're describing is causally downstream of efforts by public health people to promote breastfeeding (and pro-breastfeeding messages in hospitals, etc.) Certainly the correlation is there (https://www.researchgate.net/publication/14117103_The_Resurgence_of_Breastfeeding_in_the_United_States) but I guess it's pretty hard to prove a strict cause.
comment by Sandy Skelaney (sandy-skelaney) · 2024-09-03T22:03:11.361Z · LW(p) · GW(p)
I'd like to add some context to the "pressure to breastfeed" argument, especially regarding the history, which is missing from these experiments. In the 1970's Nestle launched a worldwide marketing campaign promoting formula feeding as better than breastfeeding. With big money behind the campaign and profit incentives, it was effective. This resulted in numerous bacterial illnesses and child deaths in Africa as the water being used was contaminated. Nestle had no reason or fiscal incentive to educate people in local communities or supply clean water. The controversy with formula is often not framed as one about private sector incentives and how profit margins dictate sales tactics. After this major f up in Africa, corporations were somewhat more careful. However, even today, they will inundate expecting mothers with formula samples. This is strategic. It's observational, but I'm willing to bet that most new mothers hold on to the samples, "just in case," even if they intend to breastfeed. Breastfeeding is difficult for most women in the first few weeks, causing pain and discomfort. The companies understand that during this time of vulnerability, one might reach for the samples to get a reprieve. The more often you do this, the less milk you produce, until you end up effectively nudged to make the switch. The facts and figures shared here assume that we are all acting as "rational man" weighing the pros and cons of breastfeeding and the impact of child wellbeing. There is an underlying profit motive to formula that does impact our behavior on this issue through our interactions with formula companies. Our decisions are not always made in a rational manner. It is worth understanding the context behind why some people are very passionate about the breastfeeding debate. And yes.. it is cheaper.
comment by Elizabeth (pktechgirl) · 2024-09-01T23:04:33.481Z · LW(p) · GW(p)
Curation notice: a good old fashion fact post. It's relevant, detailed, and legibly written.
comment by Mo Putera (Mo Nastri) · 2024-08-30T11:06:49.315Z · LW(p) · GW(p)
Is 3.1 points small? Well, a 100 IQ is higher than that of 50% of the population, while a 103.1 IQ is higher than 58%. Adding 3.1 IQ points to a kid ranked 13th in a 25-person class would push them up to around 11th. And, personally, if you were going to drop my IQ by 3.1 points, I would not be super stoked about it.
And remember, 3.1 points is still just the impact of a modest increase in breastfeeding intensity. If you ran a trial that compared no breastfeeding to exclusive breastfeeding for 12 months, the impact would surely have been much larger.
For context, in high-income countries lead poisoning is estimated to have lowered IQ by a comparable amount (the paper doesn't explicitly state the IQ drop, but does say that the mean blood lead level in HICs is 1.3 μg/dL and provides the chart below), and lead poisoning is taken pretty seriously.
00166-3/asset/ebfd713b-2f9e-4017-8506-aca6d1b78662/main.assets/gr1.jpg)
comment by Nathan Helm-Burger (nathan-helm-burger) · 2024-09-03T14:43:16.698Z · LW(p) · GW(p)
My background: My mother was a lactation consultant educator. As a teenager I was the tech support for her lectures, keeping the then early tech of computer projectors working properly for her. I would just read a book while she lectured, but I say through so many lectures it eventually sunk in anyway. She eventually started trying it her new tests on me, knowing that if I did poorly the test was too hard.
So here are some key points I want to make, not in favor of breastfeeding exactly (although I do think it's good, and that breastmilk is good!), but in favor of making it easier.
-
Some women just have a really hard time producing milk. That's ok! You can still get nearly all the benefits without breastfeeding, by using a breastmilk bank! Some women overproduce milk, and for their own health must pump it out. Some of them donate this excess milk to a breastmilk bank for others to use.
-
It shouldn't be painful. If it is, something is wrong and you should seek support from a lactation consultant. Don't trust doctors with this, most are clueless about breastfeeding and will give actively harmful incorrect advice. My rough estimate is that 90% of women should be able to breastfeed without pain (if given correct advice and guidance), and the remaining 10% should just give up and use a breastmilk bank. In our well-fed modern society, overproduction is quite common. As a community we produce more way more breastmilk than we can use!
-
There are a lot of technical details, and getting them right matters. If done incorrectly, things can start to go wrong. If you correct this quickly, within the first couple days, you'll be fine. The longer you let things go wrong, the worse it gets. Women who've been doing things slightly wrong and hurting themselves for many days are in for a load of trouble. The problems compound and become increasingly bad, and the recovery will be painful whether you decide to continue breastfeeding or not. Get help early and often!
-
A good quality breastpump makes a big difference. There are tons of shoddy ones, so getting advice on which ones are good is important. They can cost several thousand dollars, but are fully cleanable, so many women choose to rent (since they only need them for a year or two).
-
The first few weeks are indeed much more important. Aim to give breastmilk at least for the first couple months, ideally. Again, it doesn't need to be your breastmilk, use a bank if needed!
-
If possible, talk with a lactation consultant before giving birth. There's a lot of technical details to learn, and getting it wrong hurts! If you have had breast surgery, you definitely want to talk with a lactation consultant. A lot of plastic surgeons are clueless about mammary glands and unnecessarily mess stuff up in there. Another potential problem you might notice before giving birth is if your breasts are still smallish in the third trimester. There's a chance you will underproduce milk, and you be prepared to have that be only a portion of your babies calories. You can supplement with a breastmilk bank and/or formula. Don't use a standard bottle to supplement though if you plan to also breastfeed, instead you need to use things that won't teach the baby bad nursing habits.
↑ comment by juliawise · 2024-11-27T15:34:32.576Z · LW(p) · GW(p)
>As a community we produce more way more breastmilk than we can use!
This doesn't really seem right to me; or at least it relies on mothers' volunteer work to pump, sterilize, and store their milk. If you actually need to get rid of extra milk, pumping and dumping is way easier than keeping the milk clean and cold. And if you have an oversupply, pumping a lot is how to continue having an oversupply.
This is sort of like claims that we could produce lots of vegetables if everyone turned their front yard into a miniature farm and spent their spare time doing subsistence agriculture; technically true but not how most people want to spend their time.
↑ comment by Nathan Helm-Burger (nathan-helm-burger) · 2024-11-27T22:37:39.966Z · LW(p) · GW(p)
Does it currently rely on volunteer effort from mothers with available supply? Yes. Does it need to? No. As a society we could organize this better. For instance, by the breastmilk banks paying a fair price for the breastmilk. Where would the breastmilk banks get their money? From the government? From charging users? I don't know. I think the point is that we have a distribution problem, rather than a supply problem.
↑ comment by localdeity · 2024-09-03T22:40:20.445Z · LW(p) · GW(p)
Any specific knowledge about colostrum? (Mildly surprised it hasn't been mentioned in the thread.) Do breastmilk banks usually supply that, and is it worthwhile?
comment by Richard121 · 2024-09-08T21:01:48.769Z · LW(p) · GW(p)
The advice we were given was "Fed is best".
However, we also very much wanted to breastfeed, primarily due to convenience and cost.
Getting started was very difficult. We used a small number of premixed formula bottles, two of which were "free samples". We almost gave up.
A lactation consultant helped us find a comfortable position, and eventually ended up with the "rugby hold", which makes no intuitive sense whatsoever - the infant is held under the arm, legs almost behind the mother.
Once started, breastfeeding turned out to have several clear advantages, some of which were very surprising to us:
-
Low poo volume. Breastfed babies produce very little poo early on, as almost everything is absorbed. Formula produces a lot more poo. (This is apparently well-known among midwifes & health visitors, but not mentioned until we actively asked)
-
Low to no poo stink compared to formula. (Anecdotal) In discussion with other parents we found that the formula fed infants poo smelled a lot worse, even accounting for volume and parental preference (your own child's poo stinks less than that of all other children)
-
Reduced rate of constipation. Formula fed infants are at a much higher risk of constipation, as a side effect of the above.
-
Reduced posseting. Bottle fed infants swallow a lot more air due to the mechanics involved, which makes them need more burping and bring up more milk when they do. Obviously this is due to the bottle itself rather than what's in it, but formula fed is 100% bottle while breastfed is some lower percentage.
-
Night feeds didn't require full waking. The mother can do it half asleep and the infant is fed almost instantly, as mentioned elsewhere. However, this can only be done by the breastfeeding mother. The partner cannot assist.
-
(Anecdotal) Flying was easy. When disturbed, simply insert nipple and infant is immediately calmed. However it is possible a pacifier would work similarly well for a bottle fed infant.
comment by juliawise · 2024-11-27T15:30:11.852Z · LW(p) · GW(p)
Other health claims: breastfeeding slightly reduces risk of breast cancer in the mother and increases chance of colorectal cancer and breast cancer in the child.
comment by sandstoneviolin (Andrew) (sandstoneviolin) · 2024-09-07T01:02:32.700Z · LW(p) · GW(p)
Back when my co-parent & I were navigating these decisions 6-10 years ago, we came across a study that really shaped our thinking: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4077166/. Basically, the researchers analyzed outcomes in families where the siblings were breastfeeding-discordant. The punchline: "Once we restrict analyses to siblings and incorporate within-family fixed effects, estimates of the association between breastfeeding and all but one indicator of child health and wellbeing dramatically decrease and fail to maintain statistical significance."
It's only a single study, but it takes a fairly unique approach to addressing the issues in observational research on the topic, and as such, we weighed it pretty heavily in our decision-making. It's also worth keeping in mind that parental happiness and mental health makes a difference, and breastfeeding was very challenging to my co-parent from that standpoint (although the details are another story).
comment by jefftk (jkaufman) · 2024-09-09T10:21:14.302Z · LW(p) · GW(p)
The benefits of breastfeeding may be somewhat lower for the median reader of this blog than the median late 1990s Belarusian. You probably have access to cleaner water, more/better medical care and newer formula that includes things like DHA, ARA, and more nucleotides.
Why somewhat? It's plausible to me that even just the lack of DHA would give the overall RCT results.
On priors I'd expect formula to be worse: there are strong evolutionary reasons for breast milk to be the ideal food, while formula is limited by our capability to understand what babies need. If we were missing something important in formula to where babies were dying early we'd notice, but as the effect size gets smaller the chance we notice goes way down. But running studies and updating our practices based on them is still a factor, and DHA is mandatory (in the US) now. I'd still guess that an RCT today would show IQ impacts, but this is based on priors about how hard this problem is, our civilizational capacity, and the incentive structures for formula manufacturers, and not primarily on an RCT in quite a different environment.
Replies from: dynomight↑ comment by dynomight · 2024-09-10T18:38:40.999Z · LW(p) · GW(p)
Why somewhat? It's plausible to me that even just the lack of DHA would give the overall RCT results.
Yeah, that seems plausible to me, too. I don't think I want to claim that the benefits are "definitely slightly lower", but rather that they're likely at least a little lower but I'm uncertain how much. My best guess is that the bioactive stuff like IgA does at least something, so modern formula still isn't at 100%, but it's hard to be confident.
comment by Rvanlaer · 2024-09-04T01:50:16.299Z · LW(p) · GW(p)
The RCT doesn’t sound properly randomized if people were deciding themselves whether to listen to the advice? Perhaps people with higher IQ listen to the intervention better. And then we just see the genetic correlation.
Replies from: PoignardAzur↑ comment by PoignardAzur · 2024-09-05T09:04:56.584Z · LW(p) · GW(p)
As I understand it, the point of "intention to treat" RCTs is that there will be roughly as many people with high IQ in both groups, since they're picked at random. People who get the advice but don't listen aren't moved to the "didn't get advice" group.
So what the study measures is "On average, how much of an effect will a doctor telling you to breastfeed have on you?". The results are more noisy, but less vulnerable (or even immune?) to confounders.
comment by Review Bot · 2024-09-02T10:24:19.620Z · LW(p) · GW(p)
The LessWrong Review [? · GW] runs every year to select the posts that have most stood the test of time. This post is not yet eligible for review, but will be at the end of 2025. The top fifty or so posts are featured prominently on the site throughout the year.
Hopefully, the review is better than karma at judging enduring value. If we have accurate prediction markets on the review results, maybe we can have better incentives on LessWrong today. Will this post make the top fifty?
comment by Viliam · 2024-08-30T09:02:34.425Z · LW(p) · GW(p)
One more practical reason for breastfeeding is that it is convenient. Imagine that a baby starts crying at night.
- Start breastfeeding. The baby is calmed immediately. You can stay in the bed. 20 minutes later you can both sleep again.
- Go prepare a formula. You need to get out of the bed, prepare the formula, check the temperature. Meanwhile the baby is crying. That makes both of you more awake, so when all is done, it is not sure that both of you will fall asleep quickly.
Similarly, when you go outside your home. How convenient is it to breastfeed, vs prepare the formula?
Replies from: winstonBosan, whitakk↑ comment by winstonBosan · 2024-08-30T21:12:24.260Z · LW(p) · GW(p)
It doesn’t seem like you are arguing that breastfeeding is universally more convenient than formula. But breast feeding can be very inconvenient:
- It is often painful
- Elevated chance of inflammation
- Public spaces are not setup for mothers to breast feed; some may not value it, but a lot of people value privacy.
Formula’s convenience lays in enabling asynchronous feeding of the baby - by separating the role of the producer and the role of the feeder, the other partner can take care of the baby whilst the mother sleeps.
Another compromise to make is store breast milk and reheating it on demand!
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2024-09-01T06:14:38.985Z · LW(p) · GW(p)
Continuing the list...
- mother can't be separated from the baby for longer than it takes them to get hungry, and must handle every nighttime wakeup. In the newborn phase that can be every 1-3 hours.
- you can get around this by pumping, but this has its own costs. Pumping is uncomfortable to painful, time consuming, and then has all the inconvenience of formula feeding and then some (like maintaining a cold chain, and more steps requiring sterilization). It's also a hardcore logistical puzzle to get as much stored milk as possible without underfeeding your infant in the moment. The best solutions are the least convenient to the mother.
- and this is all pretty best case scenario. Lots of women or their babies have medical impediment or just don't produce enough milk, even on medication.
- some babies suck at breastfeeding and need a bottle. you could always pump and bottle feed, but as we covered, pumping has its own cost.
- some women need medications that are contraindicated by breastfeeding.
None of this contradicts the evidence that breastfeeding is beneficial, or easier for some people. But the frame should be "this is (usually) a sacrifice that we want to quantify the benefits of, to figure out if it's worth it" not "hey, free value!"
Replies from: sandstoneviolin↑ comment by sandstoneviolin (Andrew) (sandstoneviolin) · 2024-09-07T01:04:25.375Z · LW(p) · GW(p)
YES! These points are tremendously overlooked. Breastfeeding was a major psychological issue for my partner for these reasons, as well as some others that might have been a bit personal or idiosyncratic. Either way, it's not AT ALL a zero-cost choice.
↑ comment by whitakk · 2024-09-02T15:47:56.312Z · LW(p) · GW(p)
fully agree with the others who have pointed out the many cases where breastfeeding is less convenient, but more practically, one of the most useful baby-hacks in my experience was to put a tiny “skincare fridge” in the baby’s room and put bottles in it overnight (for prepared formula or pumped breast milk)
comment by Petr 'Margot' Andreev (petr-andreev) · 2024-09-02T05:51:35.405Z · LW(p) · GW(p)
To consider the cognitive development of a child is to delve into a deeply intricate process, one that evolves from kinesthetic experiences, through a kinesthetic-auditory phase, and eventually to a primarily visual mode in adulthood. This progression is not just a sequence of developmental stages but a roadmap to understanding the profound ways in which human perception and cognition are shaped by sensory interactions.
From conception to around the age of three, a child's brain is particularly attuned to sensory inputs, with a strong emphasis on tactile and kinesthetic experiences. The neural landscape of a child’s brain at this stage is heavily interconnected with their fingertips and mouth, areas densely packed with neurons. The importance of touch, smell, and texture cannot be overstated—they are the primary means through which infants engage with the world. It is through touching various surfaces, feeling different textures, and experiencing a range of smells that their neural pathways are actively molded and shaped.
Consider, for instance, the tragic 20th-century experiment where infants in orphanages were left in cribs without any physical interaction or emotional engagement. Despite adequate nutrition, many of these children suffered from severe developmental issues, and some even died. The absence of maternal touch and attention—a stark deprivation of kinesthetic and emotional stimuli—had devastating consequences, underscoring the critical role of sensory interaction in early development.
Thus, to understand infant cognition and development, we must strive to recreate a holistic environment that mimics the natural, nurturing surroundings of a caregiving woman. This means that researchers should design studies where the caregiver—ideally a person with a genuine emotional connection to the child, like a grandmother—provides not just sustenance but also tactile and auditory stimulation. The entire process of holding the child, feeding (even if with artificial milk), and engaging through touch, sound, and smell is likely crucial to normal development. The caregiver’s authentic, attentive presence might be just as important as the physical care itself.
Even culturally revered images, from the Madonna and Child to the Pietà, emphasize this tactile, kinesthetic connection. These iconic representations resonate deeply, especially with post-Christian societies, because they reflect an innate understanding of the primal importance of touch and physical closeness. This kinesthetic intimacy is foundational, particularly in early development, before the shift towards a more visual and abstract mode of cognition that dominates later educational stages.
By the time children enter school, their cognitive focus shifts, favoring visual and discrete information processing due to its efficiency in transmitting and analyzing data. This transition often creates a bias in researchers who, due to their own cognitive frameworks, may find it challenging to empathize with the significance of tactile and kinesthetic experiences in early childhood. However, this shift should not be allowed to overshadow the profound importance of early sensory experiences in shaping diverse cognitive pathways.
This perspective is informed by works such as Masaru Ibuka's Kindergarten is Too Late!, Dick Swaab’s We Are Our Brains, Robert Sapolsky’s insights on behavioral psychology, Allan Pease’s exploration of body language and age-related perceptual changes, and Richard Dawkins’ The Selfish Gene. These sources collectively highlight the vital role of tactile and sensory elements in early human development, suggesting a richer, more nuanced understanding of how we learn to perceive and engage with the world.