We desperately need to talk more about human challenge trials.
post by DirectedEvolution (AllAmericanBreakfast) · 2020-12-19T10:00:42.109Z · LW · GW · 25 commentsContents
25 comments
Note: Thanks to Peter McCluskey, whose comment below helped me develop my thoughts further and which is worth reading in addition to this post.
On March 11, 4,611 people had died of COVID-19, and the WHO declared the disease a pandemic. To date, COVID-19 has killed over 1.6 million people. It may cause lasting injury to many more. The COVID-19 vaccine was designed in two days, and finished on January 13th, 2020. We have waited almost a year to test the now two approved vaccines for safety and efficacy. One idea that could have allowed us to complete testing much more quickly, potentially saving an enormous number of lives, was human challenge trials.
On May 6, 2020, the WHO published Key criteria for the ethical acceptability of COVID-19 human challenge studies.
1DaySooner is a nonprofit advocating for human challenge trials, and estimates that "thousands or millions" of lives could be spared by a human challenge trial. In an HCT, informed volunteers are willingly infected with the virus in order to speedily test the efficacy of a vaccine. This gives results faster than waiting for enough conventional study participants to get accidentally infected by COVID-19 to test whether the vaccine works.
Given that millions of lives were potentially at stake, have we talked about it much?
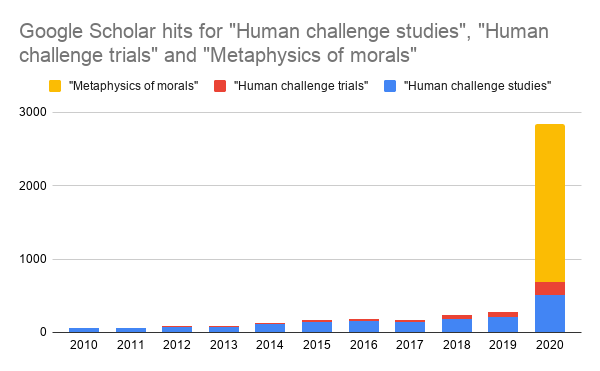
Let's first consider the scientific discussion. In 2020, the number of articles referencing "human challenge trials" or "human challenge studies" more than doubled over the previous year, as measured by Google Scholar hits, to 171 and 512 articles, respectively. There is an all-time total of 493 and 2,200 articles containing these two terms.
This is a pressing moral issue. Yet, for perspective, there were almost 2,200 papers in English this year alone on the major 18th century philosopher Immanuel Kant's "Metaphysics of Morals."

There were also well over 10,000 scholarly articles this year referencing Zika virus, a disease which, though terrible in its own right, is dwarfed by the magnitude of COVID-19. We had plenty of moral philosophers and infectious disease experts on hand. It seems conceivable that much more scholarly discussion of this important topic was possible both prior to and during the pandemic.
To those who have treated this issue, I offer my sincerest thanks.
What about major media news outlets? The New York Times alone has had 2,299 opinion pieces on COVID-19 as of Dec. 19, 2020, so they haven't exactly been neglecting the pandemic.
Yet the list of links below appears to approximately represent all the combined coverage of human challenge trials in the New York Times, Wall Street Journal, Huffington Post, Vox, and the Los Angeles Times. I found 9 10 articles, though I probably missed a few.
For an idea that could have saved at least several hundred thousands lives, not to mention allowing a speedier economic recovery, we need more.
Though few in number, each of the following articles is in itself a success. No matter their position or focus, they help to address a severe shortage of public debate about human challenge trials:
- April 9, 2020: “Human challenge trials,” where healthy volunteers would be exposed to Covid-19, explained (Vox)
- April 29, 2020: Why It Takes So Long To Make A Coronavirus Vaccine (Huffington Post)
- April 30, 2020: There May Be a Dangerous Shortcut to a Coronavirus Vaccine (NY Times)
- May 11, 2020: One Idea for Speeding a Coronavirus Vaccine: Deliberately Infecting People (Wall Street Journal)
- June 9, 2020: Can a Vaccine for Covid-19 Be Developed in Record Time? (NY Times)
- July 1 2020: Researchers Debate Infecting People on Purpose to Test Coronavirus Vaccines (NY Times)
- October 20, 2020: Dozens to be deliberately infected with coronavirus in UK ‘human challenge’ trials (Covered in several outlets)
- November 17, 2020: The ethics of deliberately infecting volunteers with Covid-19 to test vaccines (Vox)
- December 3, 2020: Confused about COVID-19 vaccines? Here’s your guide to vaccine vocabulary (LA Times)
- December 20, 2020: When You Can’t Just ‘Trust the Science’ (NY Times)
For writing them, I congratulate their authors: Dylan Matthews and Sigal Samuel (VOX); Jenna Birch (Huffington Post); Spencer Bokatt-Lindell, Denise Grady, Siddhartha Mukherjee, Dan Barouch, Margaret (Peggy) Hamburg, Susan R. Weiss, George Yancopoulos, and Ross Douthat (New York Times); Sumathi Reddy (Wall Street Journal); Karen Kaplan (Los Angeles Times); and all the authors who have occasionally managed to find space for this issue in other outlets.
While there are academic books on the topic, search for "human challenge trials" or "human challenge studies" on Google Books and you'll not find any popular books specifically focusing on human challenge trials. There are, however, plenty of popular books already dealing with the course of the pandemic so far. Perhaps they touch on this issue, but human challenge trials are well worth at least a few focused books on the subject.
Popular discussion of human challenge trials was barely on the radar during this pandemic. Yet HCTs need our sustained attention - if not to expand their use during this pandemic, then to consider how we'll deal with the next one.
Before the COVID-19 pandemic, the ins and outs of pandemic preparation were far from most people's minds. Prior to March, some might have said it was irresponsible to advocate such an ethical edge case for a disease that hadn't even been declared a pandemic. As the pandemic rolled along, it was perhaps more important to gain public acceptance of the response we did make, rather than to critique it. Now, the vaccines are approved, and it's almost a moot point. In six months, the pandemic will be winding down, and we'll all be ready to move on and think about other things.
Then we'll have a year. Five years. Ten. Twenty. But at some point, we may very well be threatened by another global pandemic.
So when will we have a serious discussion about human challenge trials? Doesn't the public deserve to be brought into a debate about the methods its own government and taxpayer-funded scientists (and ethicists) use to address such a crisis?
Billions of people could be having debates around kitchen tables, on Facebook, and the pages of newspapers about their thoughts and feelings about human challenge trials. They need leadership and activism to guide their attention to this issue. They need thoughtful writers to frame the issues clearly.
The history of deliberately infecting people with a disease, or allowing them to remain infected, contains smallpox blankets, used as a bioweapon as part of the genocide of Indigenous tribes in North America; Benjamin Jesty's inoculation of his family with cowpox to prevent smallpox; the Tuskeegee "Study" in which Black Americans were allowed to succumb to syphilis by white scientists; Nazi medical experimentation on Jews; Barry Marshall's self-experimentation with H. pylori; and sensible modern medical trials. The stories are deep, and range from the horrific to the heroic. The ethical issues are complex, and touch on matters of race, class, politics, and science.
We need a rich, long-term public discussion to make sense of all this. It needs more editorials, blog posts, books, and formal debates; the topic is profoundly neglected. The discussion should be intersectional and it should also strive for something like scientific objectivity. Nobody, layperson or expert, should be too confident that their first intuitions on the subject are correct. Our approach to medical ethics has ancient roots. Rather than allowing it to fossilize, we should encourage it to grow.
For those of us who survive, Coronavirus has cost us a year and counting.
Remember, this is about helping ourselves to live and thrive, in alignment with our values. What approach best contributes to that goal? Let's make sure that the next time a deadly virus manifests a global pattern of exponential growth, we've given serious and sustained thought to the ethics of human challenge trials.
25 comments
Comments sorted by top scores.
comment by PeterMcCluskey · 2020-12-19T20:59:22.378Z · LW(p) · GW(p)
Let me suggest that human challenge trials are a bad idea in a pandemic such as this, because they're too slow.
We can see, from RADVAC use that competent experts who were focused on minimizing their personal risk, that at least some untested vaccines look safer than a lack of vaccines.
So the only ethical strategy was to approve emergency use of at least some vaccines back around February. Possibly there were some vaccines were too novel for this to be safe. Do any of the people who are saying untested vaccines are risky quantify the risks that they believe support their position?
Why might the experts with the most media attention be wrong about this?
- the FDA is scared of anything which would suggest that their normal process hurts people by delaying good medicine.
- pharma companies are worried that competitors will be able to sell new medicines more easily.
- both expect to be blamed much more for harm caused by medicine than for harm due to lack of medicine.
↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-19T22:11:11.655Z · LW(p) · GW(p)
Hi Peter! That line of argument should be an important part of this discussion as well.
For an individual person, it's unquestionably better to give them an untested vaccine and no disease (as in administering an untested vaccine in the context of a conventional trial), rather than an untested vaccine and a disease (as in a human challenge trial). The tradeoffs between conventional trials, HCTs, and untested emergency voluntary mass vaccination campaigns, are less clear at a population level, which is why I think it needs more study and debate.
I focused this post around HCTs because they seem more conventional than emergency untested vaccination campaigns. It seemed to me that anyone hesitant about changing the status quo would be more likely to support HCTs than a mass untested vaccination campaign.
Now, I'm not so sure. The ethical qualm with HCTs is rooted in a medical ethic that prioritizes the wellbeing of the individual.
Imagine we face a another pandemic. We know the disease is deadly and that we have no treatment for it. We have reason to think the vaccine is relatively safe and at least somewhat helpful. Under those conditions, it seems like the best way to prioritize the wellbeing of individual patients is to allow them to take an untested vaccine.
So the key unquestioned assumption is not the ethics of HCTs. That at least has been examined, if insufficiently. It's not even the ethics of administering an under- or untested medical treatment, which we already do all the time.
Instead, it's the ethics of requiring that phase III trials have the minimum power/study size to gather adequate safety and efficacy data.
Why can't we instead say that in emergency circumstances, it's unethical to limit the study size? Instead, when a disease becomes a deadly pandemic to the extent that we're considering lockdowns, the entire population should have the opportunity to voluntarily participate in a vaccine trial. We already allow Phase I and Phase II to be combined. Why not also allow Phase III to be expanded?
I'm going to start exploring that angle; I wonder if that will be a more tractable approach to rethinking our pandemic response.
↑ comment by brianwang712 · 2020-12-26T16:24:31.813Z · LW(p) · GW(p)
So I think that you're right to point out the bias that many experts have in overprioritizing wanting to avoid harm from a vaccine at the cost of ongoing deaths from the pandemic. That's likely a very strong consideration playing into their judgments here, and one that should be fought against.
That being said, I think another concern that is underappreciated in these debates is lack of efficacy, rather than lack of safety. What if—and this is probably more likely—a vaccine doesn't result in any harm, but also just doesn't do anything to prevent disease? How much time have you spent getting pharma to invest time and resources into developing a manufacturing process for a particular vaccine, and getting the vaccine distributed to people, only to find out it doesn't work? How many people will have lost trust in the vaccine development process such that they won't take a subsequent vaccine, even if it works much better? Do you really have the option to "start over"? Maybe moreso now than ever the answer is "yes" given the relative agility with which you can move from design to manufacturing process with mRNA vaccines, but with anything cell culture-based you've probably lost months, at which point you might be in a worse situation than if you'd started with trials. This scenario doesn't have to play out with literally zero efficacy, the same considerations apply if you have, say, 30% efficacy. You could blow your shot at developing a 90% efficacy vaccine b/c you've spent down all your resources on the 30% efficacy one.
The implicit theory behind this concern is that you have a limited bank of public trust + resources to work with, such that if you spend it all on the first try and it doesn't work out, then there's no going back. So best to make sure your one try definitely goes well, e.g. by setting up trials first.
I think it's unclear exactly to what extent this theory holds up, but I think it warrants serious consideration. Too often I think these debates stop at "well the expected risk of harm to any given individual from even an untested vaccine is much less than the expected risk of harm from being unvaccinated, so we should give untested vaccines as early as possible" rather than considering the true counterfactual at a society-wide level.
Replies from: brianwang712↑ comment by brianwang712 · 2020-12-26T16:39:07.964Z · LW(p) · GW(p)
Potential counterargument against the above: Well, yes, any individual pharma company might only have one shot, but as a society we could have many different untested vaccine candidates going out to people all at once. We already have a risk diversification mechanism by having many different vaccine candidate options, so we don't need to further avoid risk by doing trials on all of them. And we also don't have to give untested vaccines to literally everybody, just small populations at first.
Response to the counterargument: If the proposal is to give a bunch of untested vaccine candidates to people early on in the pandemic before knowing for sure how they work, haven't you just reinvented clinical trials? Maybe a conception of them that is faster and to a larger population, but still fundamentally the same thing?
comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-20T01:45:10.841Z · LW(p) · GW(p)
Here's a linguistic issue. "Ethics of human challenge trials/studies" is easy to Google. But if I wanted to look up papers on the ethics of allowing hundreds of millions of people to participate in phase III vaccine trials during a pandemic, rather than the bare minimum needed to generate adequate power, what term would I search for?
Replies from: PeterMcCluskey↑ comment by PeterMcCluskey · 2020-12-20T19:05:45.282Z · LW(p) · GW(p)
I'll guess that there's no literature on the subject.
FDA rules require a lot more work per patient for trials. I'm guessing something like $10k per patient, so you're likely proposing more than a trillion dollars in spending. And that assumes there are no problems with hiring and training enough people to run the trials.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-23T00:51:33.185Z · LW(p) · GW(p)
Given that the US government typically values the life of an individual at around $10 million, you only need to save 100,000 US lives to make that worthwhile. We've lost triple that number in this pandemic. Certainly it would be logistically complex, but we have to compare the logistical complexity of running that kind of trial with the current complexities we face.
comment by Mitchell_Porter · 2020-12-19T15:02:49.275Z · LW(p) · GW(p)
"Billions of people could be having debates ... about human challenge trials."
There's something peculiar about this way of promoting the idea. Either human challenge trials are worth it, or they are not worth it, or "it depends" (on context, on opinion). It shouldn't require billions of people to figure out something that basic. And if the answer is "it depends", then it's going to depend on medical technicalities or simply on local culture, and again, having billions debate it isn't helpful.
Whether to have human challenge trials is ultimately a question about something that very few people are involved with, namely vaccine development methodology. To seriously address it requires knowledge of that process that few of us possess. If debates need to occur, quality matters more than quantity.
Replies from: remizidae, Ericf, AllAmericanBreakfast↑ comment by remizidae · 2020-12-19T21:55:51.862Z · LW(p) · GW(p)
I strongly disagree with this idea that only a few vaccine experts should be debating the topic. Aside from a few basic technical concepts, the basic question here is ethical. Everyone can judge ethical questions. And if the past year has taught us anything, it’s that medical ethics questions are too important to be left to the experts.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-19T22:19:52.455Z · LW(p) · GW(p)
I agree; it seems like the contrary argument assumes that experts make better decisions and take a more flexible approach on issues where there's less direct public pressure, awareness, and debate. Instead, it seems to me they're like to say "that seems weird, I'm busy, so why bother listening to your weird proposal." Reminds me of Big Block of Cheese Day from the West Wing.
↑ comment by Ericf · 2020-12-19T17:53:08.240Z · LW(p) · GW(p)
Having everyone talk about it builds awareness and familiarity in the population, basically ensuring that it becomes politicized, and either guaranteeing it happens next time, or ensures it does not happen, depending on which faction happens to be in power at that time. I mean, Measles Vaccine is already "controversial" and Measles is worse than covid (in both transmissibility and cfr)
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-19T21:08:53.393Z · LW(p) · GW(p)
Hi Ericf, thanks for responding! Do you think that it's possible to run a human challenge trial in the early stage of a deadly pandemic, without any known treatment for the disease, without provoking a major public debate?
If not - if debate and politicization of early-pandemic HCTs is guaranteed - then it seems to me that the right question isn't whether to debate it, but how to debate it. And that's only a relevant question if we have accepted the need to debate it.
Replies from: Ericf↑ comment by Ericf · 2020-12-20T01:07:01.448Z · LW(p) · GW(p)
I haven't kept up on the state of debate of the trolley problem, but there should be a discussion among bio-ethisists and regulators about the ethics of infecting N people to prevent N x X infections among other people. The current state seems to be "it is unethical to switch tracks, no matter who is on each track." Which, for all I know, is the correct answer.
↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-19T18:20:03.561Z · LW(p) · GW(p)
I appreciate you commenting!
My intuition is that experts need to see public opinion change, as well as that of their colleagues, before they’ll feel comfortable running more HCTs. Without some amount of pressure, our tendency to see inaction as less blameworthy than action will prevent a serious reconsideration of how we do things.
Also, even quality expert debate is lacking, as the OP I hope makes clear.
Finally, I think that ethics are for everybody. People should have a say in the ethics of the society in which they live.
Overall, it’s not clear to me if you just disagree with the one line you picked out, or the substance of the post overall.
Replies from: Mitchell_Porter↑ comment by Mitchell_Porter · 2020-12-20T10:28:22.205Z · LW(p) · GW(p)
I disagree with that one line, mostly - the idea that having "billions" of people "debating" an issue is a meaningful or constructive goal.
Human challenge trials seem like a useful thing. Although maybe there's some inconvenience because the infected people need to remain quarantined throughout the trial. And maybe there are other considerations that I don't know about, intrinsic to vaccine development, that make it less useful or practical than it seems.
Those are about the extent of my thoughts on the issue. They are not especially deep.
I'm just saying that this vision of having everyone on Earth "debating" your favorite issue doesn't make sense. I see two things to be accomplished here: clarity about whether and how human challenge trials are appropriate, and having policy and practice reflect this.
If there is actually still something to be discovered regarding the desirability and efficacy of HCTs, having "billions" debate it is not the way to do it. The vast majority of people on Earth know almost nothing about how the immune system works or the process of developing vaccines. They are not in a position to know any technical considerations that may affect the utility of HCTs.
remizidae said, "I strongly disagree with this idea that only a few vaccine experts should be debating the topic. Aside from a few basic technical concepts, the basic question here is ethical. Everyone can judge ethical questions."
I am not saying that only vaccine experts should have a say. But I am saying that you can't have this discussion without them! There may always be some detail, regarding how the real world works, that impacts the viability of HCTs, and which only experts know about.
But OK, let's suppose that HCTs make technical sense in certain contexts. Then perhaps "the basic question here is ethical", and "everyone can judge" it. If everyone can judge this appropriately, surely it doesn't take billions of people to arrive at one of (1) yes (2) no (3) it depends?
On the other hand, if you think you already know that HCTs are useful and important and neglected, but are held back by institutional resistance, then maybe it would help to convince a lot of other people that things should change. But in that case, I would find the language of "debate" to be disingenuous.
I mean, suppose you stirred things up enough that billions of people were debating HCTs, and it turned out that for some reason, they're no good. You would have wasted the time of the entire human race, as well as probably permanently misleading millions of people on the issue.
So you need to make a choice. Are you basically certain that HCTs urgently need to become acceptable? Then openly advocate them. Are you still unsure whether HCTs would actually make for a better world? Then try to figure out whether they would, before you set out to "guide the attention" of billions to this issue.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-20T21:53:10.167Z · LW(p) · GW(p)
Let's imagine that "billions" is two billion people, and that it takes the reading of one book for each to feel they have an adequate depth of understanding to have an informed opinion on pandemic vaccine testing alternatives. That might be 5 hours per person.
Ten billion person-hours is a little over one million person-years.
COVID-19 has killed over 1.6 million people so far. If a better approach to vaccine testing could have prevented 2/3 of those deaths, and each person who died lost just one QALY (which I suspect is an unrealistically conservative estimate), then that balances out with the time investment of having two billion people read a book.
Consider that over two billion people are certainly spending more than a total of five hours talking and thinking about the pandemic. Having a large part of the time they were going to spend thinking and talking about it anyway devoted to HCTs and other alternative vaccine testing approaches would be a good use of that time.
It's also possible that humanity would make the considered decision not to enact an alternative approach because they value conventional medical ethics to that degree. I don't have the hubris to be certain they're wrong. But I am confident that they should consider it.
As Peter McCluskey illustrated, although I've thought about this issue way more than anybody else I personally know in real life, I still am nowhere close to adequately educated on the subject. So I feel confident in advocating for mass conversation on the subject, but not for mass adoption of HCTs.
Replies from: Mitchell_Porter, ChristianKl↑ comment by Mitchell_Porter · 2020-12-21T13:00:28.126Z · LW(p) · GW(p)
I did some google-research... From wikipedia, I learned that HCTs have already been performed many times, for a variety of pathogens (I didn't know that). So it seems like they are already part of accepted practice.
I found a reddit thread with comments from a few people who work in the medical industry, remarking e.g. that HCTs would only have come in at Phase 3 and would only have saved a little time. And a PNAS opinion piece giving what I guess is the common opinion among the bioethics establishment, that HCTs are not appropriate for Covid, and their reasons for this opinion (I have not studied their arguments; but they mention 1DaySooner).
Whatever their merit, I note that these counterarguments do not involve pure ethical reasoning about the bare idea of HCTs, they involve technological and epidemiological details that outsiders do not know.
This is why I'm against this call for "mass conversation". So far all I'm hearing is "if we had vaccines sooner, lives would have been saved, what if HCTs would have done this?" But it turns out that HCTs have been used in the past, and that there are alleged reasons why they wouldn't help in the specific case of Covid.
At the very least, an HCT advocate using our recent global experience as motivation, ought to now address the specifics of how the Covid vaccines were developed, and provide some plausible detailed reasons as to why and how HCTs could have accelerated that process.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-21T18:13:51.483Z · LW(p) · GW(p)
I can actually expand on this a little bit for you.
HCTs have been run in the past, but only for diseases where we had an efficacious treatment. The reason COVID HCTs would only have been run in the Phase 3 stage is because early in the pandemic, we had no proven-effective treatment.
This is a choice based on ethical and political reasoning, rather than science.
As Peter McCluskey points out, the choice not to begin an immediate mass-vaccination campaign with the untested mRNA vaccines we had on January 13th is likewise based on political and ethical reasoning, rather than a scientific choice. We now know, of course, that those vaccines were extremely effective. We'd have saved a colossal number of lives if we had. If we'd paused to run HCTs early on and then distributed the vaccines, we'd have still saved the vast bulk of lives that have been lost.
It's only because our institutional leaders have made the ethical and political choices they have on our behalf that HCTs appear to be ineffective. We could have made different choices that were equally scientific, but based on different political and ethical reasoning. Continuing with our conventional ethical/political choice cost us over a million lives. Is it worth it? Medical ethicists disagree, none of the experts are talking about it enough, and it's time for them to step it up and for The People to have a say.
Replies from: Mitchell_Porter↑ comment by Mitchell_Porter · 2020-12-22T10:34:17.590Z · LW(p) · GW(p)
OK, let's talk about some of the issues that would arise in this scenario.
Taking an mRNA vaccine means becoming temporarily transgenic. mRNA for Covid spike protein is injected into your muscle cells, they produce it, and this stimulates antibody production.
In having trials, one is not only testing that the Covid mRNA vaccine is effective against Covid; one is also testing whether the vaccine itself has side effects.
Are you proposing to move straight to mass vaccination, without testing for vaccine side effects? But if not, how will making the trials HCTs, save time? HCTs are only different in the way that they test efficacy against the pathogen. When it comes to testing for side effects of the vaccine itself, don't you have to wait just as long as you do, in a non-challenge trial?
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-22T17:11:33.116Z · LW(p) · GW(p)
Yes, I think there are basically three options:
- Vaccinate with safety and efficacy data (conventional trials)
- Vaccinate only with efficacy data (early HCTs)
- Vaccinate with no data (immediate vaccination campaign on development of a vaccine)
I'm advocating that option 2 and option 3 be considered as realistic scientific, ethical, and political possibilities during the early stage of a deadly future pandemic akin to the one we face now.
Two of the questions I still have are:
- What are the worst side effects of any vaccine that's ever been tested?
- How frequently do vaccines fail in conventional trials due to safety concerns?
This paper finds that 33% of tested vaccines have made it through all 3 trial phases. One of the worst consequences of a historically approved vaccine, used as an example by the AAMC of why we can't rush a COVID-19 vaccine, was the polio vaccine where 120,000 doses contained live virus.
This caused ten deaths. Stack that up against over 1.6 million and counting.
Once again, I'm not strictly saying the AAMC is wrong. But they are begging the question. Comparing the historical base rate of deaths due to unsafe vaccines vs. the base rate of expected deaths due to COVID-19 is, on its face, a pretty reasonable and obvious approach to evaluating what we should do.
The AAMC glosses right over this issue. They must know it's why many of their readers are looking up the article in the first place. So they're choosing to ignore this line of thinking. I'm asking them to stop ignoring it.
Replies from: Joe_Collman, Mitchell_Porter↑ comment by Joe Collman (Joe_Collman) · 2020-12-23T00:14:13.145Z · LW(p) · GW(p)
If (2) and (3) were seriously considered, then I'd think you'd particularly want to avoid using only a single vaccine. From a civilizational point of view, the largest issue isn't the expectation of the direct outcome - it's that there's a small chance you may have a bad outcome with very little variance across the population.
I'd be much less concerned about doing (2) or (3) with twenty different vaccines than with one.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-23T00:48:22.061Z · LW(p) · GW(p)
Black Swan considerations definitely apply here. Although as far as I know, we haven't had a vaccine that outright killed the majority of the people taking it, it's not impossible. Maybe it's just rare enough that we haven't established a meaningful base rate. You'd also want to be concerned about the possibility of interactions from giving multiple vaccines to one person.
It might make sense to do something like vaccinating populations in the hardest-hit areas first, trying new vaccines as they become available, prioritizing the safest and most effective vaccines as data emerges.
↑ comment by Mitchell_Porter · 2020-12-28T10:43:10.762Z · LW(p) · GW(p)
If you want to make the case that with a different ethos, Covid-19 mortality might have been dramatically lower, it would help to exhibit a scenario in which this happens.
Much is being made of the fact that mRNA vaccines were first synthesized, very soon after the virus's genetic sequence became available. But this just means that a particular molecular construct (a carrier for spike protein mRNA, I guess) could quickly be synthesized.
To go from that to mass vaccination, even if we skip trials for efficacy and safety, requires that you know enough about how the virus and the vaccine behave within the body, to have some idea of where and how to administer the vaccine to a patient. Also, there needs to be infrastructure to mass-produce the vaccine, and a way to distribute it.
Complications known to me, in the case of Covid mRNA vaccines, are that Covid's interaction with the body and the immune system is intricate and was not immediately understood (this matters in deciding how to introduce a vaccine into the body), and that mRNA vaccines currently require ultracold refrigeration for their distribution, an infrastructure that doesn't even exist in some countries.
Let's see a concrete counterfactual scenario for rapid deployment of a Covid mRNA vaccine in 2020, that takes into account these two factors; and then we can start to estimate how many extra lives the HCT ethos might have saved.
↑ comment by ChristianKl · 2020-12-21T15:06:35.849Z · LW(p) · GW(p)
Let's imagine that "billions" is two billion people, and that it takes the reading of one book for each to feel they have an adequate depth of understanding to have an informed opinion on pandemic vaccine testing alternatives. That might be 5 hours per person.
I don't think there's a policy issue on which one billion people let alone two billion people read a book.
Even for an issue like climate change most people don't read a book about it.
When it comes to the usefulness of a public debate it's worth looking at two important enviromental issues. Mercury pollution is bad. CO2 pollution is bad.
Obama's EPA managed to be very effective in fighting mercury pollution but unable to do anything about fighting CO2 pollution. A key difference between the two is that CO2 pollution was a heavily politized issue while nobody spoke about mercury pollution.
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2020-12-21T18:15:28.113Z · LW(p) · GW(p)
How do those thoughts influence your response to the broader argument?