Covid 11/24/22: Thanks for Good Health
post by Zvi · 2022-11-24T13:00:01.750Z · LW · GW · 4 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Booster Boosting Variants Physical World Modeling China In Other Covid News Other Medical and Research News Mr. Mastodon Farm None 4 comments
This Thanksgiving, I am thankful that I am once again back at full health. Covid comes and Covid goes. It was like I had a bad cold… for three days. That actually about sums it up, with some residual coughing. After a week, I was able to do a full session on the elliptical machine, so I consider everything back to normal.
I am not yet ready to wind down the Covid posts, but I am getting close to that point. If we get through the next two months without anything major happening, it will probably be time. For now, things will continue as normal.
Executive Summary
- I’m feeling much better now.
- China looks to be headed for more lockdowns, here we go again.
- Person leaving WHO apologizes for denying Covid is airborne.
Let’s run the numbers.
The Numbers
Predictions
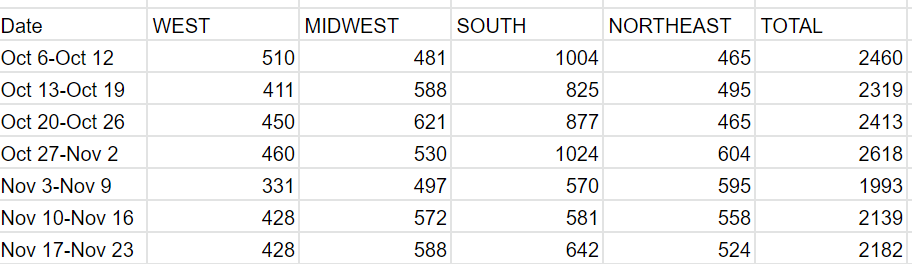
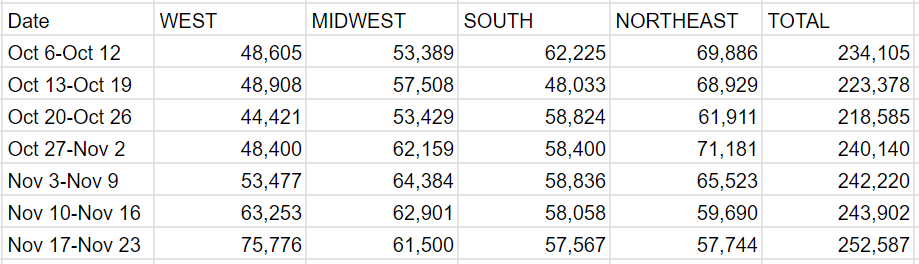
Predictions from Last Week: 250k cases (+4%) and 2,400 deaths (+12%).
Results: 253k cases (+3%) and 2,182 deaths (+2%).
Predictions for Next Week (Thanksgiving): 223k cases (-12%) and 1,850 deaths (-15%).
Standard holiday drop-off.
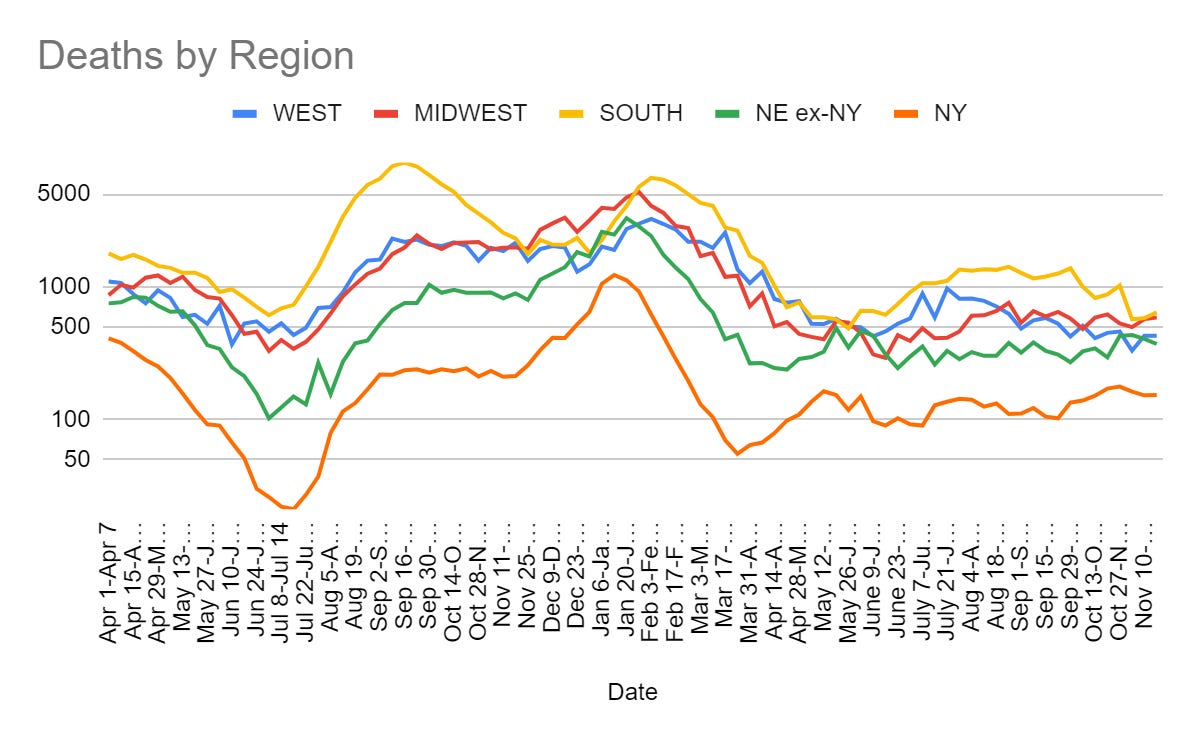
Deaths
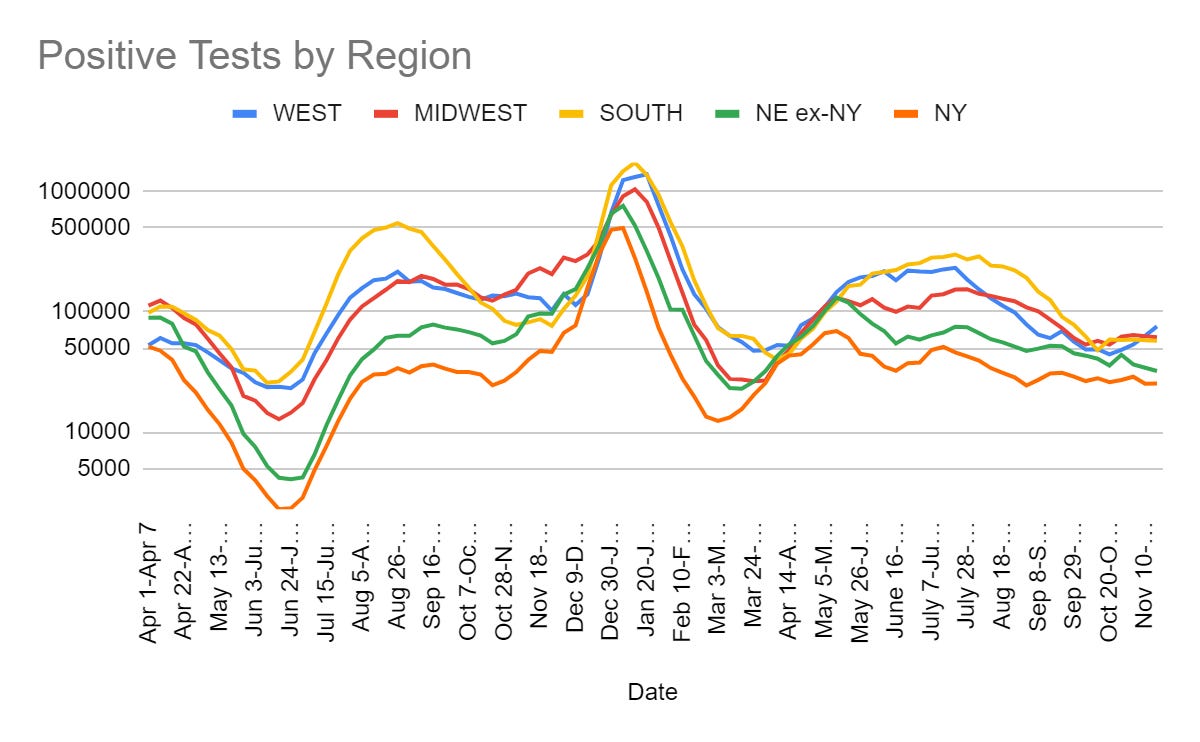
Cases
Booster Boosting
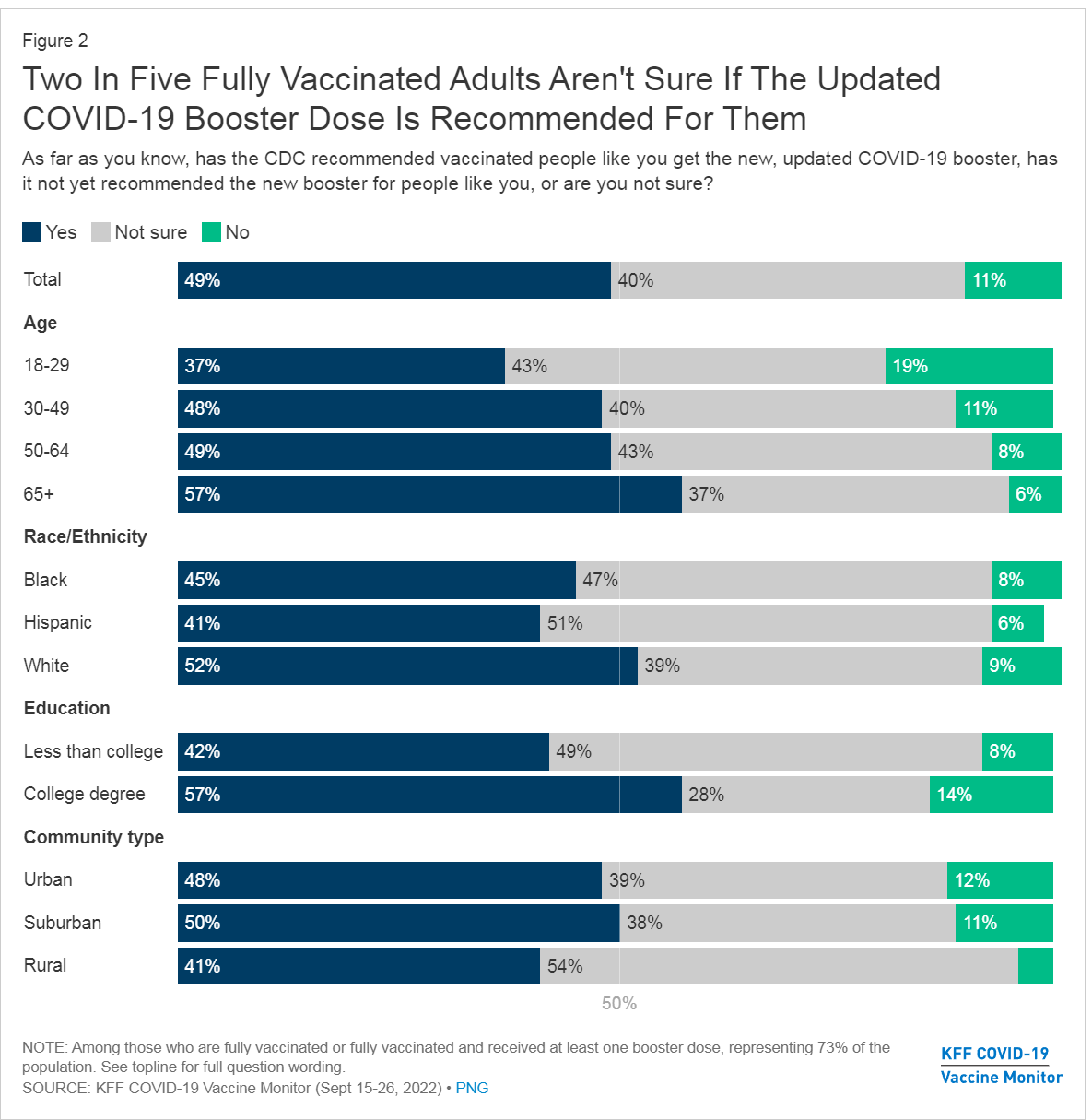
Our booster strategy is a disaster. Monovalent Omicron boosters would be superior. A 4-to-6 month interval would have been superior. Our supplies are split between initial doses that can only be used initially and that are fully obsolete, and booster doses that are something like 60%-75% obsolete (although both are still far better than nothing, to be clear.) Many don’t know the updated boosters even exist.
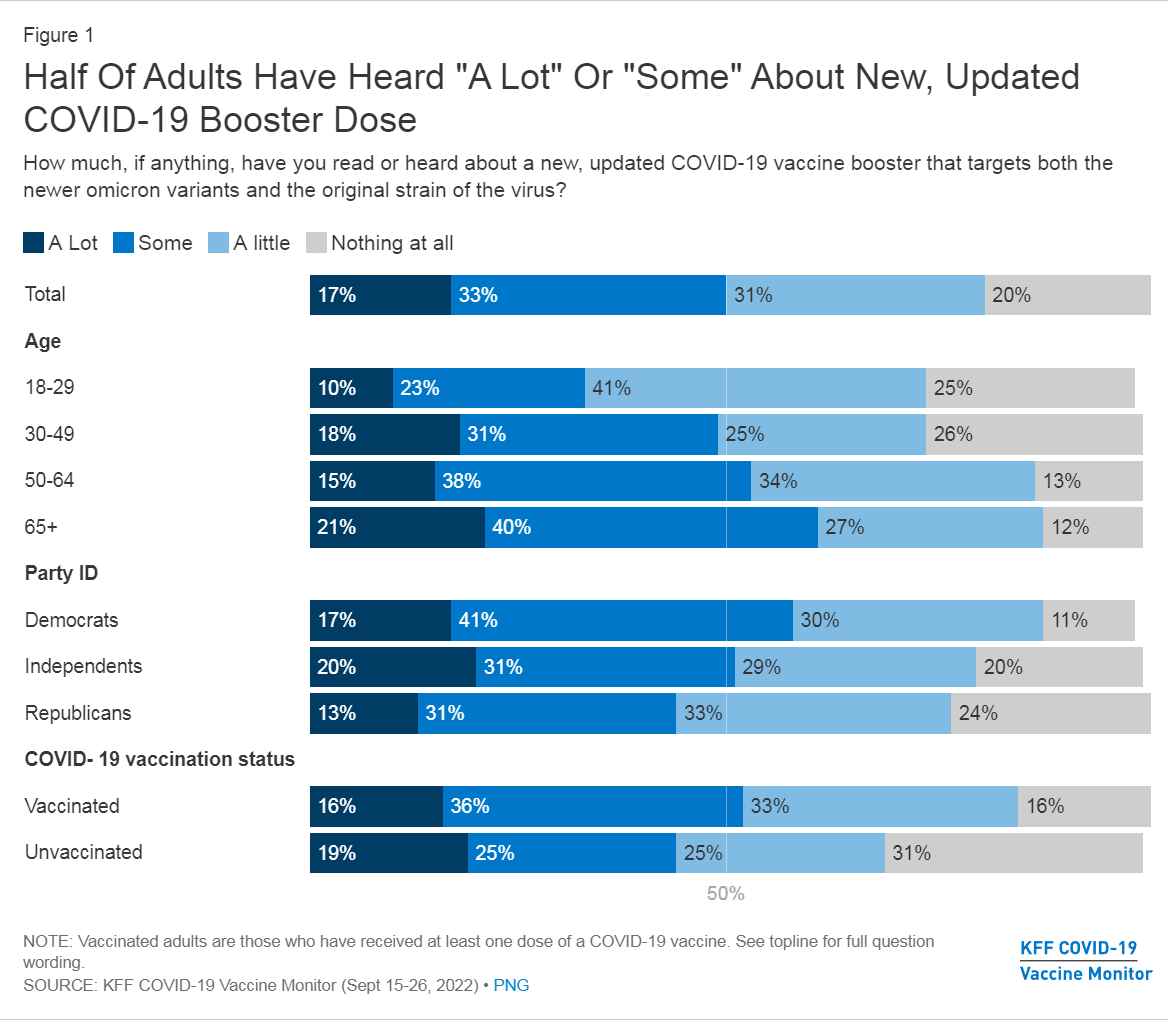
Survey says 1/5 got the bivalent booster, while another 3/5 ‘definitely’ or ‘probably’ will get it in the future. Which tells me that people are lying in the survey. We are not going to get that kind of uptake, and most people who have not gotten the booster yet are not going to go do it later.
Here is what passes for public health messaging: ‘Because I said so.’
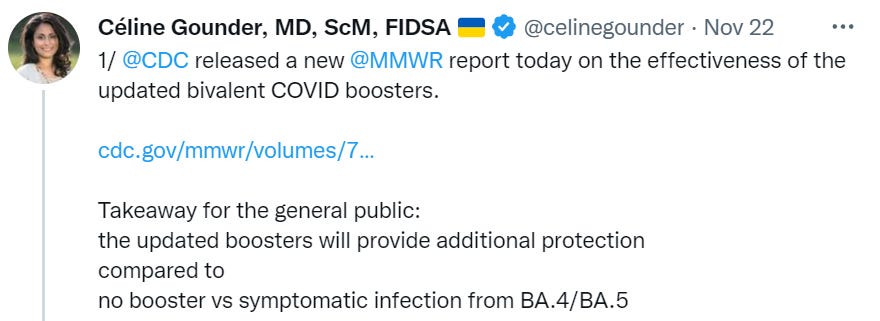

They are ‘better.’ So get them. How much better? You don’t need to know. Not your department. Cost-benefit analysis is not a thing. We are the jump department and we said jump, damn it.
To be fair, the rest of the the thread does give some numbers.

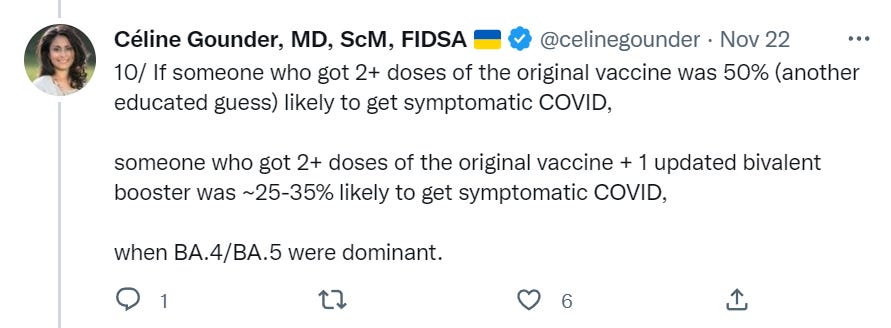
This is not nothing, if one is concerned and at high risk then boosting does seem worthwhile, yet I notice that none of this is especially encouraging with regard to boosters. If a booster alone was a 30% cut in symptomatic Covid permanently that would be one thing. Instead, this is a comparison versus completely unvaccinated and the boost is at least partly temporary, and there is no attempt to compare to older boosters.
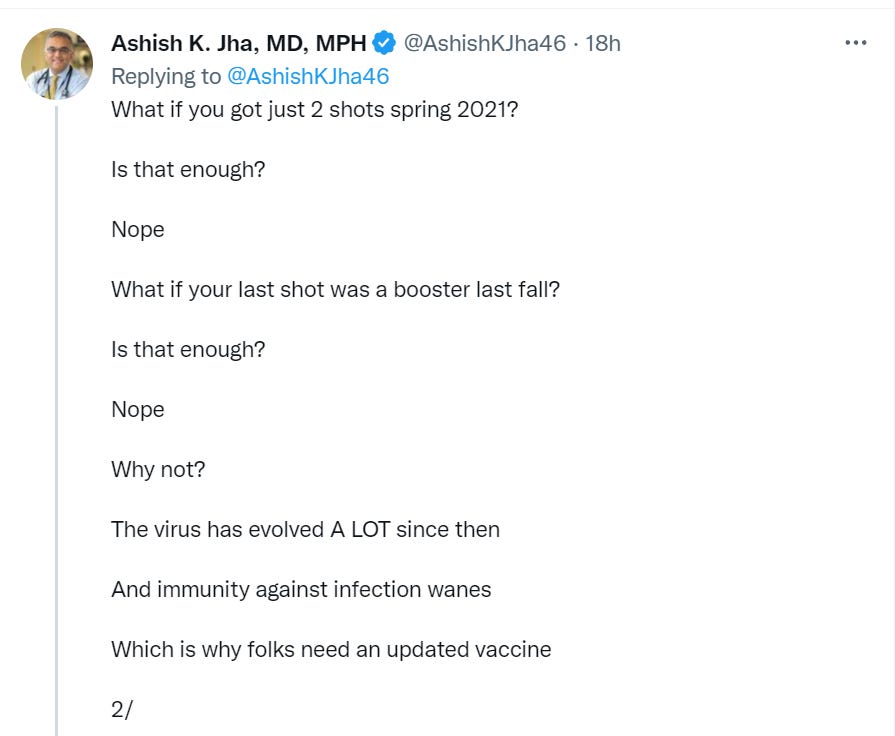
Here is another attempted message, that seems like it might be more effective, also imagine hearing this previously and the reaction from Public Health.
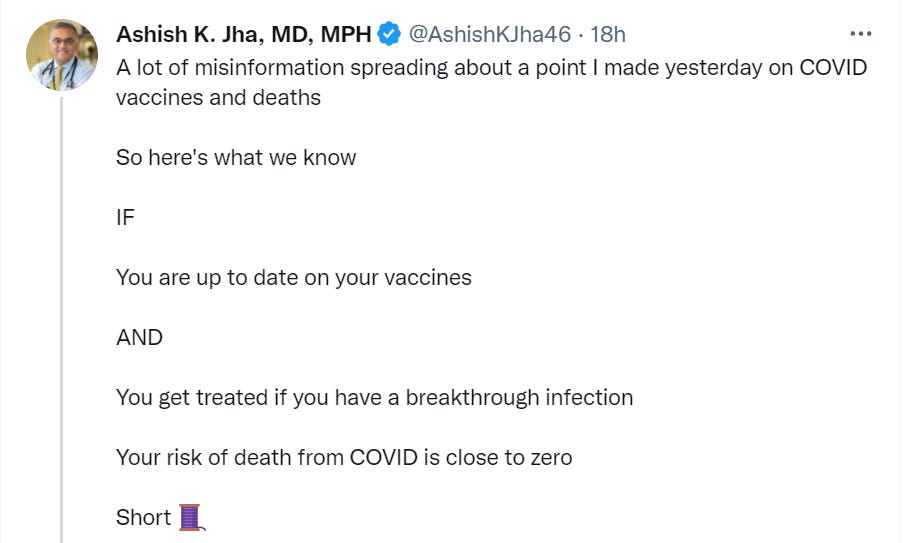
‘Close to zero’ here means, presumably, as close as public health wants it to be and no closer, since one can interpret that kind of threshold any number of ways. Also, one could point out that age and other risk factors are a much bigger impact on risk of death than whether you got a properly updated booster, even under the most generous possible interpretations of booster effectiveness, so this seems like clear misinformation as stated – and misinformation directly intended to change someone’s behavior.
Variants
Physical World Modeling
We continue not to know things.
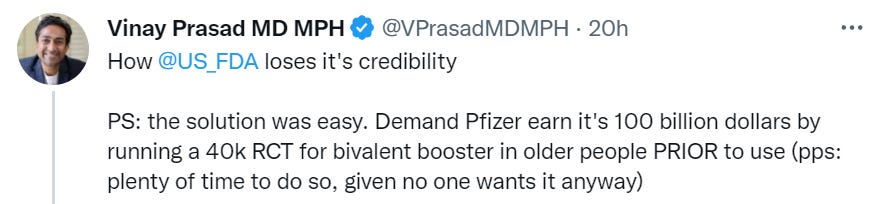
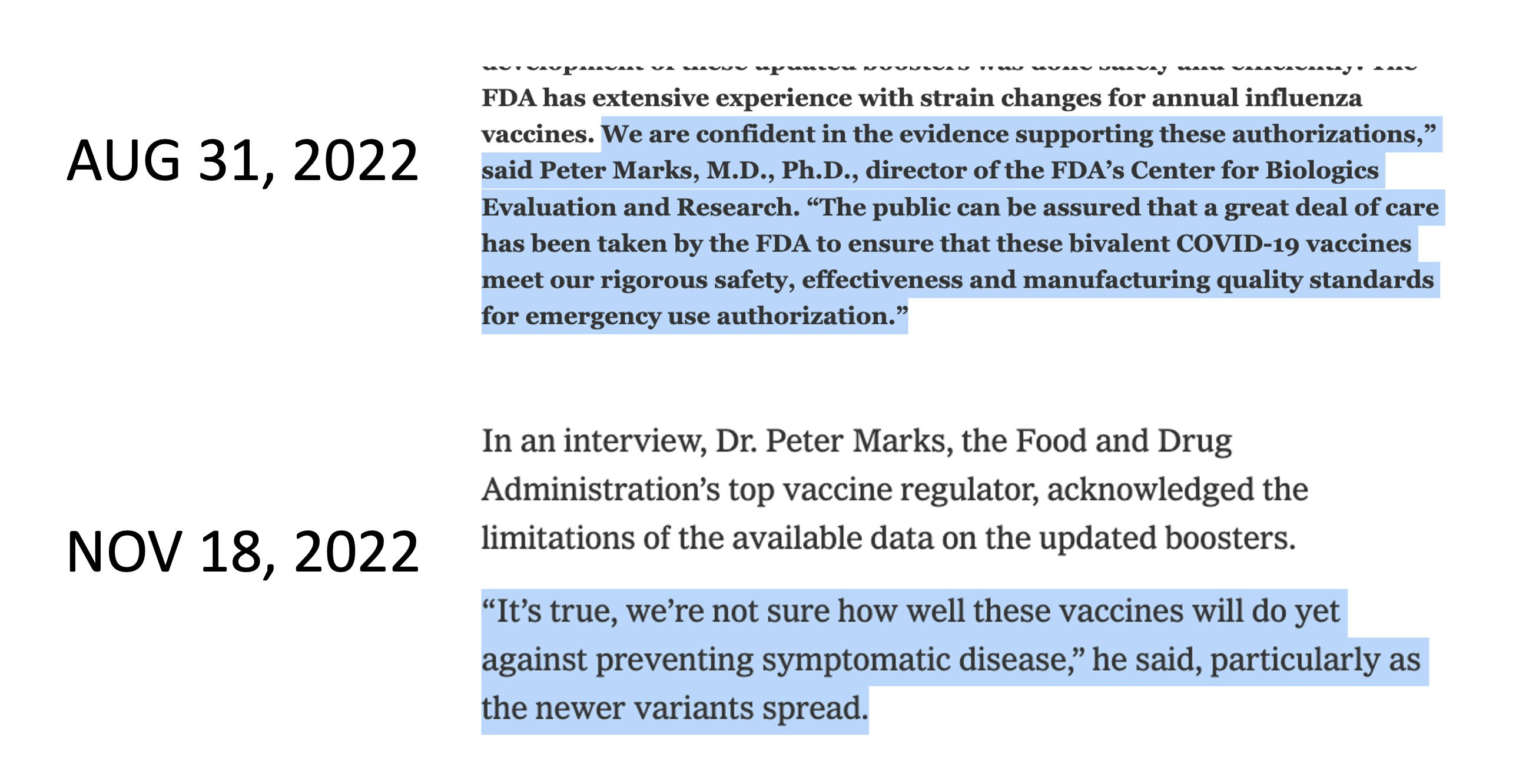
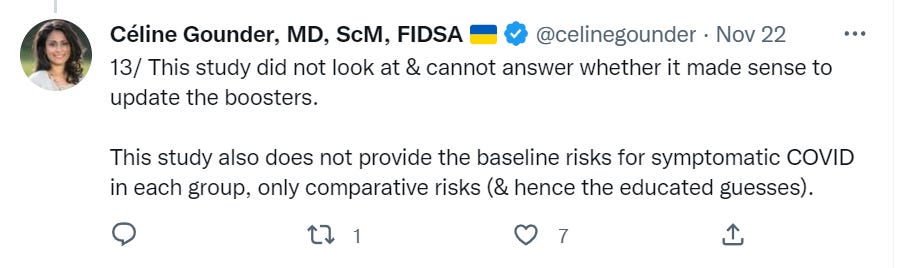
There is no contradiction here. One can have more than enough evidence to say that you are better off with option Y than option X, without knowing the effectiveness level of option Y. That is how responsible people make decisions.
Demanding a 40k person RCT of the new booster implies at minimum months of additional delay on top of delays that were already so long as to ensure we will never have a properly updated vaccine or booster.
The right solution would be to make Pfizer do the trial, while also approving the update months earlier, and also running a trial with a fully updated booster as a third option, and seeing what happens. Instead, we once again run into the problem that once we decide to act as if something is a good idea, confirming that fact becomes impossible. Not only is it an expense no one wants, it would be ‘unethical.’
Thus, we will never know the effectiveness of the bivalent booster.
We do have a new study on the evolution of the Covid mutation spectrum.
CDC’s new system for communicating Covid risk fails to communicate risks it is not communicating, says new CDC survey. Does this do a disservice to those trying to measure their risk? In some ways yes. In other ways, it prevents people from not only making mistakes but from socially imposing those mistakes on others. Low and high do not have objective thresholds, after all.
Paxlovid cuts hospitalizations by 51%, similar results by age groups and vaccination status.
China
China has been Lucy successfully pulling the football away from us for years now. A new more infectious variant comes along. It seems as if China’s zero Covid policy cannot possibly hold up. It is touch and go for a while, and there is a bunch of economic disruption that may or may not be worthwhile. Yet China’s zero Covid policy holds once again.
This latest time, China loosened its grip, going from insane paranoia levels to slightly less insane paranoia levels. Some of the loosening was getting rid of Covid prevention theater. Some of it wasn’t.
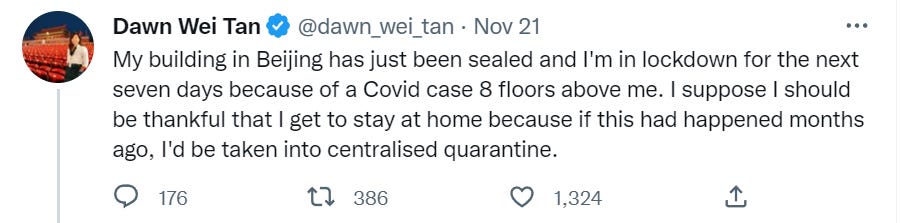
This is indeed a much less awful thing to happen than the awful thing that used to happen. It also is, presumably, somewhat less effective at the goal of containment.
Thus, once again, it seemed like the smart money would be on the system failing. Either the system is powerful enough to contain Covid or it is not. Exponential growth means that if containment is lost, China will have to deal with the same types of Covid problems as everyone else. That will be painful for a bit, face will be lost, and then life will return to normal. In the long run, it is inevitable.
Is it finally happening? It does seem like it is finally happening.
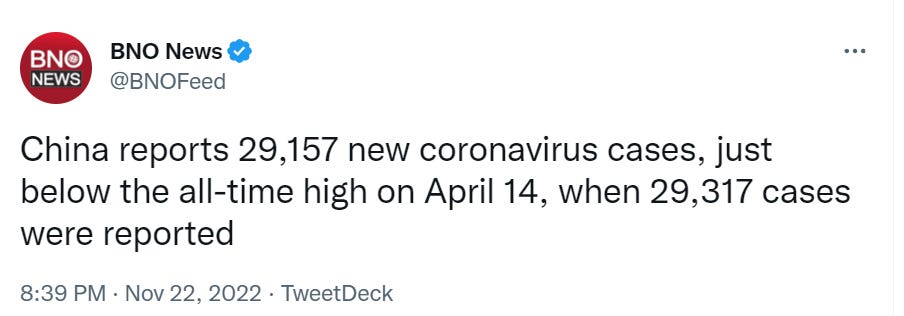
Certainly the epidemic is growing rapidly.
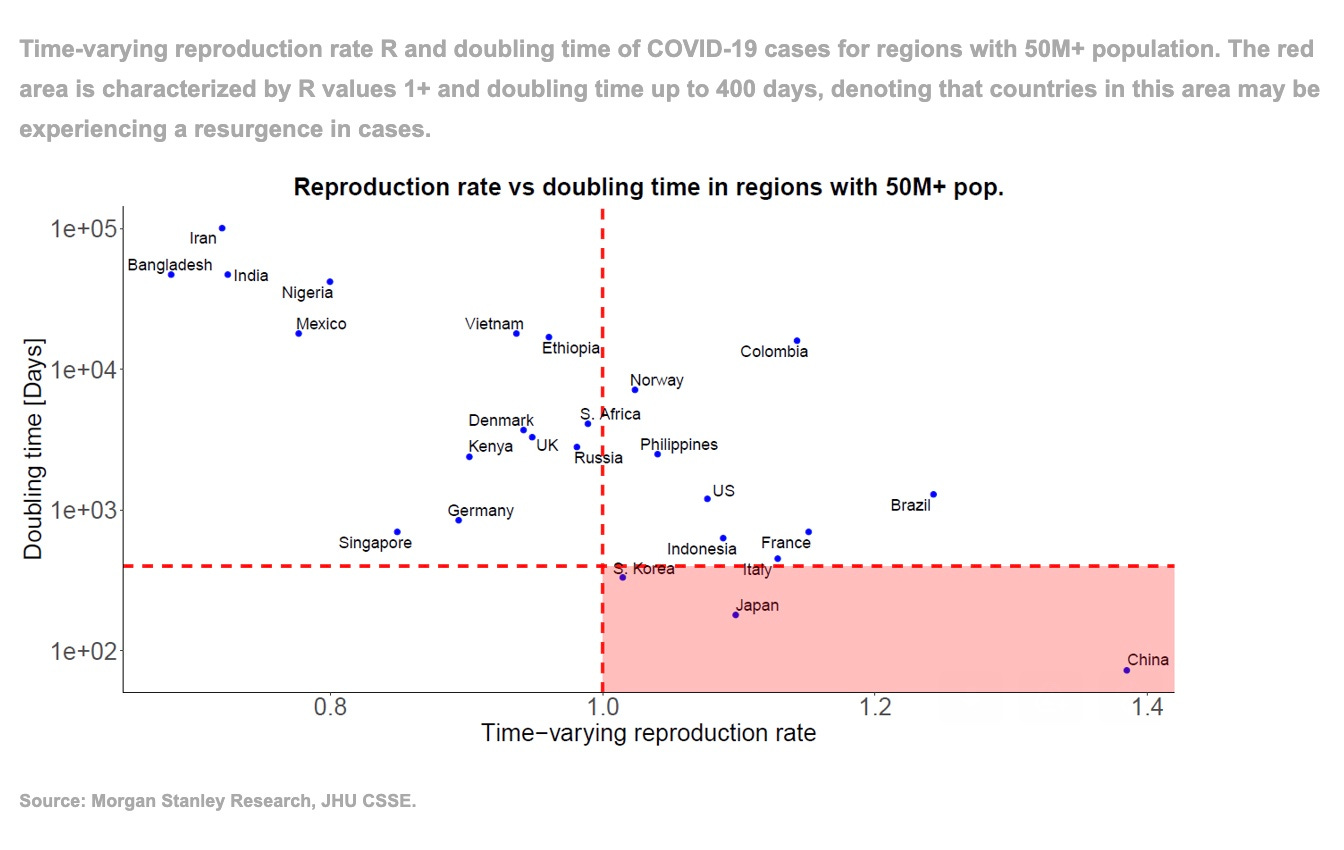
China’s system is based on cracking down hard on local flare-ups when they happen. This is expensive, and there is a limited capacity of such response.
Thus, once again, the natural expectation is that China’s system entirely fails within a few months. I am not predicting this with high confidence due to it having not happened so many times already, plus the possibility of a further crackdown to return to previous methods, so it seems more like a 30% chance this time around.
Here is Petersen-Clausen talking about how to prepare for a lockdown. Recommends lots of bottled water, long lasting milk, condiments, oversized trash bags, medication and sanitary items, and of course to stock up early.
People continue to die from the lockdowns, as people are unable to access emergency care.
Also China seems to be using checks, at least in Shenzen and Guangzhou, that require Chinese ID and thus make it impossible for those with a passport to pass local health checks, de facto banning visitors.
In Other Covid News
WHO’s departing chief, now that they are leaving, ‘regrets errors in debate over whether SARS-CoV-2 spreads through air.’ Thank you. Yes, you should have done it, and apologized for not doing it, and been loud about it, much earlier, and this was very bad and did a ton of damage. Her explanation for why this did not happen is ‘it was not my role and neither did anyone ask me to get involved in that stage.’ Which is absolutely not how any functional organization or responsible person runs. If you are the Chief Scientist at the WHO, you know Covid is airborne and you know that the WHO keeps yelling at everyone that it is NOT airborne, then it is on you to fix this, because people are dying. It is also on everyone else there. Kai has additional coverage.
Debunking of paper attempting to re-write history on the early choir-based superspreader events. What it does not explain is why this attempt is happening.
Zeynep describes battling intentionally altered screenshots of her previous statements, intended to reverse their meaning, and the general confluence of such actions with those who repeated the series of alarmist predictions like ‘monkeypox is airborne’ and ‘Omicron will infect everyone every two weeks.’ She is frustrated that her fellow scientists won’t do that much to help correct the record, basically saying liars gonna lie.
New study shows high frequency of virus co-infection and species spillover among bats.
Other Medical and Research News
It sure would be convenient to have an at-home flu test. One guess why we do not have them. That’s right. FDA Delenda Est, paranoia about people maybe learning things about themselves, pure and simple.
Excellent opportunity that those with the proper credentials should utilize: White House calls for information about how to better conduct clinical trials during public health emergencies, direct application instructions here. We desperately need a procedure for doing emergency clinical trials, ideally challenge trials of all kinds combined with other ways of getting speed when it matters most. I do not think submitting directly myself would be helpful, but if any stakeholders want to consult me on their submissions I will be happy to help (pro bono of course).

On the margin this seems right. Knowing who is at more or less risk, in ways that we cannot alter, is usually not very useful. Whereas knowing what we can usefully alter might lead us to alter it usefully, or to not waste effort altering other things.
Risk knowledge is still useful, as revealed both by people’s willingness to pay for and spend time on it, and by people changing their actions based on it. In some cases, yes, too much, where relative risk dominates absolute risk in people’s minds. In other cases, not enough.
With Covid-19, if anything, we didn’t pay enough attention to who was at what relative risk level. It was indeed actionable information, as there was a continuous infection risk versus life activities tradeoff.
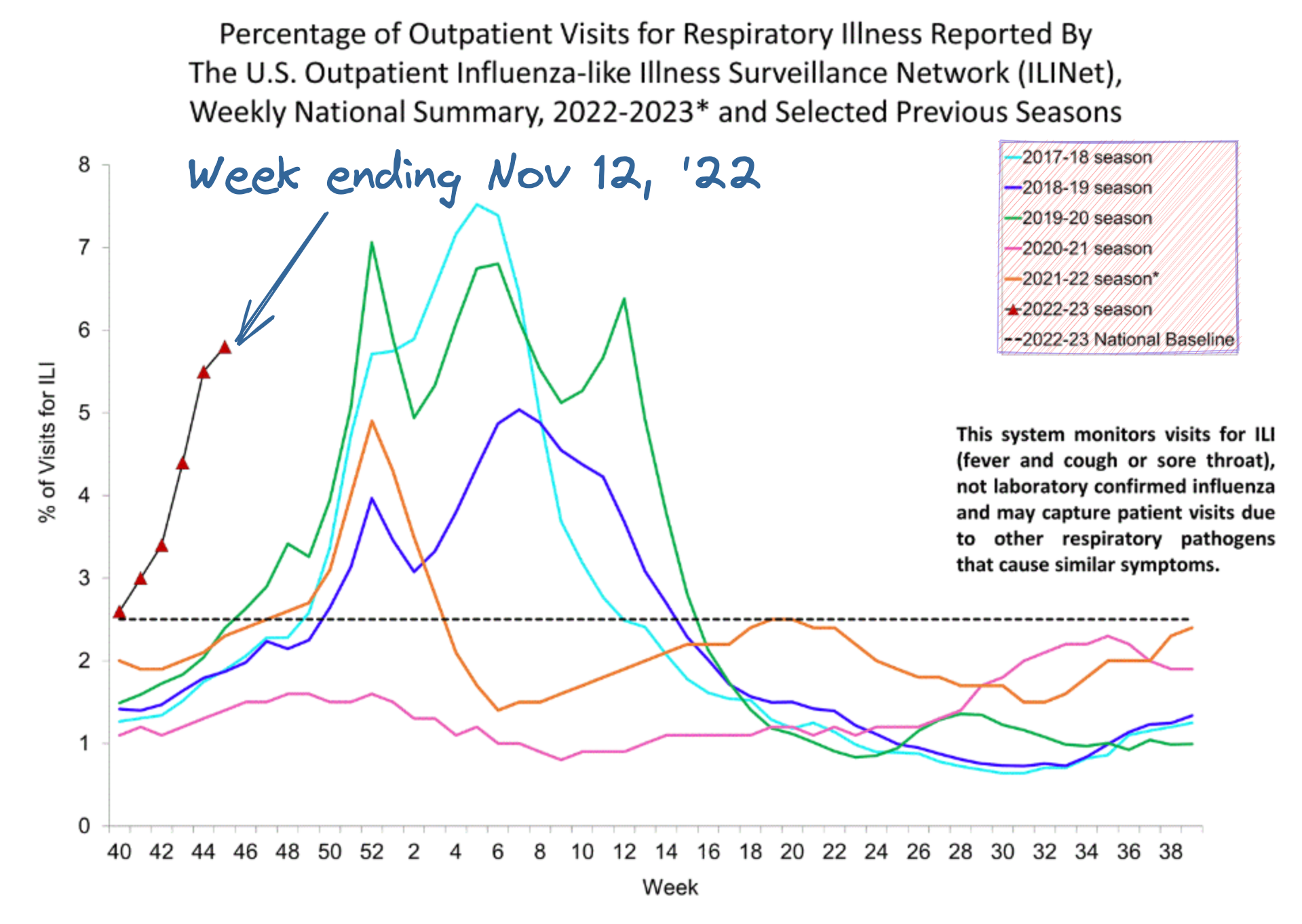
Hospitals face overload due to combination of RSV, Covid and Flu during this season.
Influenza like illness is rising earlier than usual, and hopefully will peak earlier as well.
We don’t vaccinate turkeys and chickens against bird flu, slaughtering them instead, because other countries are paranoid about bird flu and wouldn’t allow exports if we relied on the vaccine. The blame framing on this seems absurd to me, if the world says ‘do X or we won’t let you export’ then you are going to do X.
Mr. Mastodon Farm
Medical Twitter is talking a big talk about moving over to Mastodon.
It makes sense. Medical Twitter is all about ‘this particular thing that we are in a panic about is completely unacceptable and we should completely change everything to stop it no matter how high the cost and no matter what the consequences.’ It is also the home of ‘this new problem is going to overwhelm everything and become a crisis’ where often the new problem is not new, or not real.
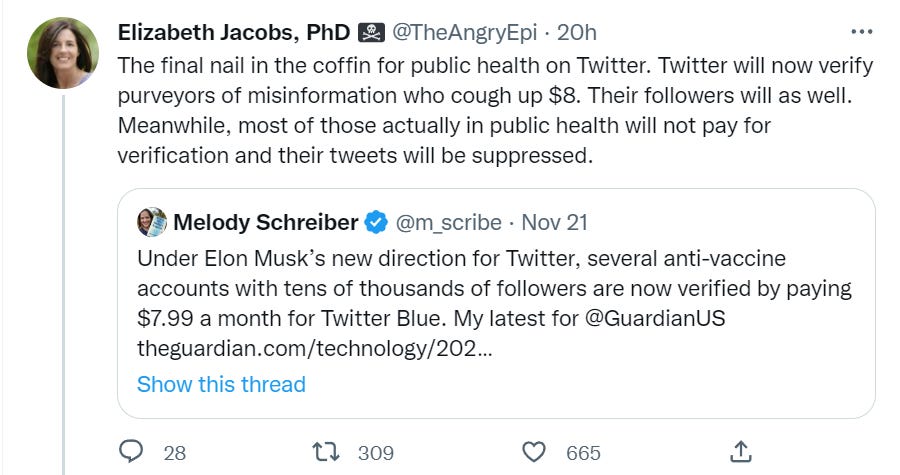
Medical Twitter is also a place where people would think that anyone with the Proper Authority Stamp of Approval (for example, a blue check) would suddenly be able to get everyone to listen to them, and be very upset about the wrong monkeys getting such symbols. In this case, anti-vax account gets blue check. Oh no.
A blue check does not mean ‘this person is smart, or knowledgeable, or trustworthy, or you should listen to them.’ Jenny McCarthy would have a blue check under the old system. A blue check means at most ‘this is who you think this is, not fake, not a bot and not an imitation.’ If an anti-vax account has a blue check then it is the real version of that anti-vax account. Accept no substitutes or imitations. Why would them having a ‘blue check’ suddenly turn their operation into overdrive? Why should it matter?
If ‘those in public health will not pay for verification’ and this will ruin the public’s access to good information, a conclusion for which I am deeply skeptical at every step, that sounds like a decision by those in public health. I know times are tough. Are they that tough? Eight dollars tough? Or is something else going on?

I see a lot of this, which again matches a lot of what we saw with Covid and medical Twitter: Morality-based outcome predictions. Outcomes are seen as driven primarily by whether visible, symbolic decisions are made ‘correctly.’ Those who stray from the path and commit sin must inevitably be struck down. Except no, this is all a side show, the game is being played elsewhere. Unless. Unless we can inflict such punishment on those acting in such ways, that acting in such ways is forced.
They also think that those who disagree with them, and are wrong, must all be automatically sought out and censored, rather than the answer to speech being more speech.
Here is Carl Bergstrom, talking about how he has gone from 5% to 10% of his Twitter follower count over on Mastodon over the last two weeks. He also notes the issues with ‘members of marginalized communities.’


The entire idea behind Mastodon is federation, that you join an instance and each instance governs itself. People are joining this because they are upset with Twitter over every little thing, and then expect Mastodon to be the solution that magically addresses their every concern. Which Mastodon, by design, cannot possibly do. If you demand a walled garden that is strictly policed by a central authority, a plan without a central authority might not be for you.
Mastodon feels like Crypto, or like how many describe Elon’s takeover of Twitter, as another instance of Discovering Why You Need Everything Over Again, and also a ‘this tech is not so hard, what do you mean not inclusive, why are you running away screaming, come back here.’
In other places I’m hearing a little discussion of ‘Hive’ which seems to have quite a few security and privacy concerns among other things. I continue not to take the Twitter ‘alternatives’ seriously.
Is it possible that three years from now we are all using some other service that looks exactly like Twitter, or (far worse outcome) some set of five different ones? Yes, if things go badly enough that outcome is possible, although I’d consider it an underdog (~25% maybe) even with all the absurd social pressure trying to make Twitter die out of spite. Is it going to be Mastodon? No.
Also see Scott Alexander on the Twitter chaos. I do not currently plan on another full post on it, but indeed do many things come to pass.
4 comments
Comments sorted by top scores.
comment by Radford Neal · 2022-11-24T15:09:52.938Z · LW(p) · GW(p)
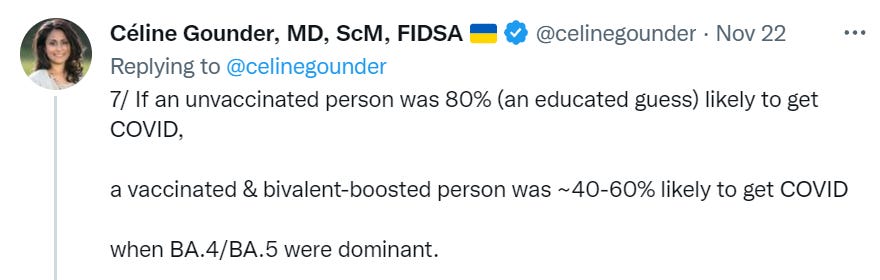
You quote the following tweets by Celine Gounder:
6/ Absolute vaccine effectiveness
= (risk of infection among unvaccinated) - (risk of infection among vaccinated
= ~20-40%
7/ If an unvaccinated person was 80% (an educated guess) likely to get COVID,
a vaccinated & bivalent-boosted person was ~40-60% likely to get COVID when BA.4/BA.5 were dominant.
These are nonsensical, and to the extent they have any sense, are probably wrong, and if they are not wrong, they do not support her recommendation to get the booster.
First, the nonsense: It's meaningless to talk about someone's chance of getting COVID without specifying over what time period - an 80% chance of getting COVID in the next day? I don't think so. But then what does it mean? And it is also completely ridiculous to talk about absolute reduction in risk of infection (over whatever time period), when this risk obviously depends on other factors, such as how isolated the person is. You can tell it's nonsense from the fact that the risk for a person who has little contact with others might be only 10% (over a month, say), and after subtracting 20-40%, you get a negative number. No, that can't be right.
Second, it's probably wrong: At least, I certainly hope that the vaccine is more effective than that.
Finally, if it's really that ineffective (and also not effective at preventing serious illness, an issue not mentioned in the tweets quoted), then getting the booster seems ill-advised. There's little benefit, and nobody actually knows whether getting repeated doses of an mRNA vaccine might have long-term side effects. (The cells of your body that the mRNA vaccine prompts your immune system to kill are not necessarily the same ones as for more traditional vaccines, for which there is better long-term safety data.)
comment by Lao Mein (derpherpize) · 2022-11-24T15:46:57.889Z · LW(p) · GW(p)
I can see zero-covid holding indefinitely. People here are fundamentally OK with daily COVID tests and 1, 2, maybe even 3 months of lockdown a year forever. There are limits to the infectiousness of diseases, and I don't see any disease spreading in a condition of permanent lockdown.
Replies from: derpherpize↑ comment by Lao Mein (derpherpize) · 2022-11-24T15:58:55.925Z · LW(p) · GW(p)
Actually, now that I think about it, the most likely scenario is that China shuts down all incoming international travel permanently, even for Chinese citizens. Speaking of which, do we know how new cases are popping up in China? Surely it's from international travel, right?
comment by ROM (scipio ) · 2022-12-14T13:23:06.119Z · LW(p) · GW(p)
Thus, once again, it seemed like the smart money would be on the system failing. Either the system is powerful enough to contain Covid or it is not. Exponential growth means that if containment is lost, China will have to deal with the same types of Covid problems as everyone else. That will be painful for a bit, face will be lost, and then life will return to normal. In the long run, it is inevitable.
Given the CCPs backtracking from its zero covid policy (at least for the moment), this looks like it was a pretty good prediction.