Prescriptions, Paradoxes, and Perversities
post by Scott Alexander (Yvain) · 2015-04-30T04:52:19.000Z · LW · GW · 4 commentsContents
I. II. III. IV. V. VI. VII. Footnotes None 4 comments
[WARNING: I am not a pharmacologist. I am not a researcher. I am not a statistician. This is not medical advice. This is really weird and you should not take it too seriously until it has been confirmed]
I.
I’ve been playing around with data from Internet databases that aggregate patient reviews of medications.
Are these any good? I looked at four of the largest such databases – Drugs.com, WebMD, AskAPatient, and DrugLib – as well as psychiatry-specific site CrazyMeds – and took their data on twenty-three major antidepressants. Then I correlated them with one another to see if the five sites mostly agreed.
Correlations between Drugs.com, AskAPatient, and WebMD were generally large and positive (around 0.7). Correlations between CrazyMeds and DrugLib were generally small or negative. In retrospect this makes sense, because these two sites didn’t allow separation of ratings by condition, so for example Seroquel-for-depression was being mixed with Seroquel-for-schizophrenia.
So I threw out the two offending sites and kept Drugs.com, AskAPatient, and WebMD. I normalized all the data, then took the weighted average of all three sites. From this huge sample (the least-reviewed drug had 35 ratings, the most-reviewed drug 4,797) I obtained a unified opinion of patients’ favorite and least favorite antidepressants.
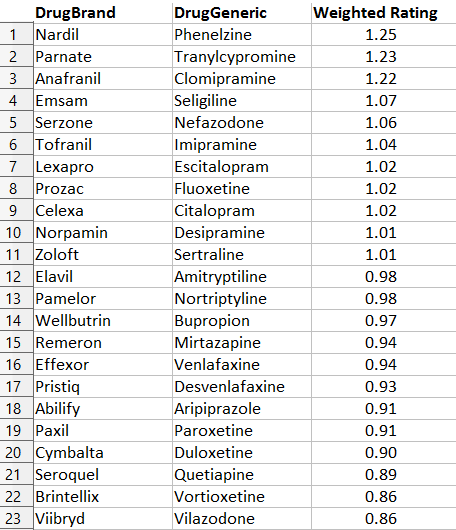
This doesn’t surprise me at all. Everyone secretly knows Nardil and Parnate (the two commonly-used drugs in the MAOI class) are excellent antidepressants1. Oh, nobody will prescribe them, because of the dynamic discussed here, but in their hearts they know it’s true.
Likewise, I feel pretty good to see that Serzone, which I recently defended, is number five. I’ve had terrible luck with Viibryd, and it just seems to make people taking it more annoying, which is not a listed side effect but which I swear has happened.
The table also matches the evidence from chemistry – drugs with similar molecular structure get similar ratings, as do drugs with similar function. This is, I think, a good list.
Which is too bad, because it makes the next part that much more terrifying.
II.
There is a sixth major Internet database of drug ratings. It is called RateRx, and it differs from the other five in an important way: it solicits ratings from doctors, not patients. It’s a great idea – if you trust your doctor to tell you which drug is best, why not take advantage of wisdom-of-crowds and trust all the doctors?

The RateRX logo. Spoiler: this is going to seem really ironic in about thirty seconds.
RateRx has a modest but respectable sample size – the drugs on my list got between 32 and 70 doctor reviews. There’s only one problem.
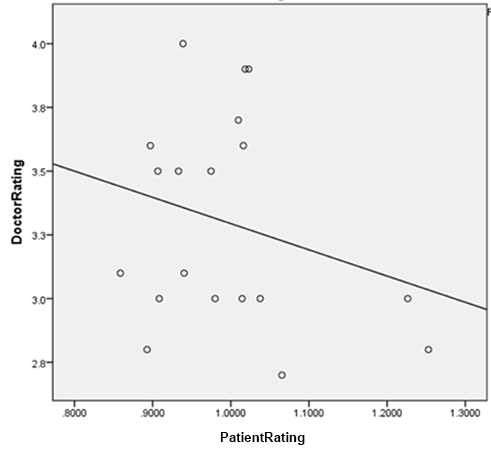
You remember patient reviews on the big three sites correlated about +0.7 with each other, right? So patients pretty much agree on which drugs are good and which are bad?
Doctor reviews on RateRx correlated at -0.21 with patient reviews. The negative relationship is nonsignificant, but that just means that at best, doctor reviews are totally uncorrelated with patient consensus.
This has an obvious but very disturbing corollary. I couldn’t get good numbers on how times each of the antidepressants on my list were prescribed, because the information I’ve seen only gives prescription numbers for a few top-selling drugs, plus we’ve got the same problem of not being able to distinguish depression prescriptions from anxiety prescriptions from psychosis prescriptions. But total number of online reviews makes a pretty good proxy. After all, the more patients are using a drug, the more are likely to review it.
Quick sanity check: the most reviewed drug on my list was Cymbalta. Cymbalta was also the best selling antidepressant of 2014. Although my list doesn’t exactly track the best-sellers, that seems to be a function of how long a drug has been out – a best-seller that came out last year might have only 1/10th the number of reviews as a best-seller that came out ten years ago. So number of reviews seems to be a decent correlate for amount a drug is used.
In that case, amount a drug is used correlates highly (+0.67, p = 0.005) with doctors’ opinion of the drug, which makes perfect sense since doctors are the ones prescribing it. But amount the drug gets used correlates negatively with patient rating of the drug (-0.34, p = ns), which of course is to be expected given the negative correlation between doctor opinion and patient opinion.
So the more patients like a drug, the less likely it is to be prescribed2.
III.
There’s one more act in this horror show.
Anyone familiar with these medications reading the table above has probably already noticed this one, but I figured I might as well make it official.
I correlated the average rating of each drug with the year it came on the market. The correlation was -0.71 (p < .001). That is, the newer a drug was, the less patients liked it3.
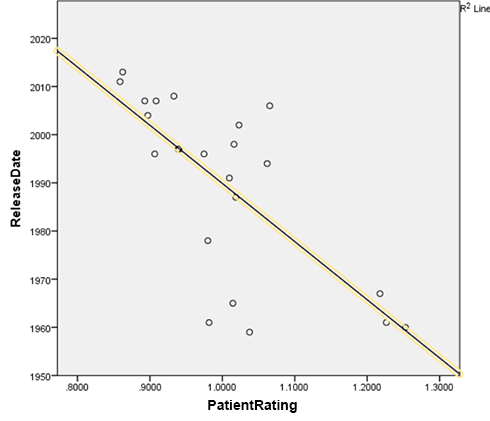
This pattern absolutely jumps out of the data. First- and second- place winners Nardil and Parnate came out in 1960 and 1961, respectively; I can’t find the exact year third-place winner Anafranil came out, but the first reference to its trade name I can find in the literature is from 1967, so I used that. In contrast, last-place winner Viibryd came out in 2011, second-to-last place winner Abilify got its depression indication in 2007, and third-to-last place winner Brintellix is as recent as 2013.
This result is robust to various different methods of analysis, including declaring MAOIs to be an unfair advantage for Team Old and removing all of them, changing which minor tricylics I do and don’t include in the data, and altering whether Deprenyl, a drug that technically came out in 1970 but received a gritty reboot under the name Emsam in 2006, is counted as older or newer.
So if you want to know what medication will make you happiest, at least according to this analysis your best bet isn’t to ask your doctor, check what’s most popular, or even check any individual online rating database. It’s to look at the approval date on the label and choose the one that came out first.
IV.
What the hell is going on with these data?
I would like to dismiss this as confounded, but I have to admit that any reasonable person would expect the confounders to go the opposite way.
That is: older, less popular drugs are usually brought out only when newer, more popular drugs have failed. MAOIs, the clear winner of this analysis, are very clearly reserved in the guidelines for “treatment-resistant depression”, ie depression you’ve already thrown everything you’ve got at. But these are precisely the depressions that are hardest to treat.
Imagine you are testing the fighting ability of three people via ten boxing matches. You ask Alice to fight a Chihuahua, Bob to fight a Doberman, and Carol to fight Cthulhu. You would expect this test to be biased in favor of Alice and against Carol. But MAOIs and all these other older rarer drugs are practically never brought out except against Cthulhu. Yet they still have the best win-loss record.
Here are the only things I can think of that might be confounding these results.
Perhaps because these drugs are so rare and unpopular, psychiatrists only use them when they have really really good reason. That is, the most popular drug of the year they pretty much cluster-bomb everybody with. But every so often, they see some patient who seems absolutely 100% perfect for clomipramine, a patient who practically screams “clomipramine!” at them, and then they give this patient clomipramine, and she does really well on it.
(but psychiatrists aren’t actually that good at personalizing antidepressant treatments. The only thing even sort of like that is that MAOIs are extra-good for a subtype called atypical depression. But that’s like a third of the depressed population, which doesn’t leave much room for this super-precise-targeting hypothesis.)
Or perhaps once drugs have been on the market longer, patients figure out what they like. Brintellix is so new that the Brintellix patients are the ones whose doctors said “Hey, let’s try you on Brintellix” and they said “Whatever”. MAOIs have been on the market so long that presumably MAOI patients are ones who tried a dozen antidepressants before and stayed on MAOIs because they were the only ones that worked.
(but Prozac has been on the market 25 years now. This should only apply to a couple of very new drugs, not the whole list.)
Or perhaps the older drugs have so many side effects that no one would stay on them unless they’re absolutely perfect, whereas people are happy to stay on the newer drugs even if they’re not doing much because whatever, it’s not like they’re causing any trouble.
(but Seroquel and Abilify, two very new drugs, have awful side effects, yet are down at the bottom along with all the other new drugs)
Or perhaps patients on very rare weird drugs get a special placebo effect, because they feel that their psychiatrist cares enough about them to personalize treatment. Perhaps they identify with the drug – “I am special, I’m one of the only people in the world who’s on nefazodone!” and they become attached to it and want to preach its greatness to the world.
(but drugs that are rare because they are especially new don’t get that benefit. I would expect people to also get excited about being given the latest, flashiest thing. But only drugs that are rare because they are old get the benefit, not drugs that are rare because they are new.)
Or perhaps psychiatrists tend to prescribe the drugs they “imprinted on” in medical school and residency, so older psychiatrists prescribe older drugs and the newest psychiatrists prescribe the newest drugs. But older psychiatrists are probably much more experienced and better at what they do, which could affect patients in other ways – the placebo effect of being with a doctor who radiates competence, or maybe the more experienced psychiatrists are really good at psychotherapy, and that makes the patient better, and they attribute it to the drug.
(but read on…)
V.
Or perhaps we should take this data at face value and assume our antidepressants have been getting worse and worse over the past fifty years.
This is not entirely as outlandish as it sounds. The history of the past fifty years has been a history of moving from drugs with more side effects to drugs with fewer side effects, with what I consider somewhat less than due diligence in making sure the drugs were quite as effective in the applicable population. This is a very complicated and controversial statement which I will be happy to defend in the comments if someone asks.
The big problem is: drugs go off-patent after twenty years. Drug companies want to push new, on-patent medications, and most research is funded by drug companies. So lots and lots of research is aimed at proving that newer medications invented in the past twenty years (which make drug companies money) are better than older medications (which don’t).
I’ll give one example. There is only a single study in the entire literature directly comparing the MAOIs – the very old antidepressants that did best on the patient ratings – to SSRIs, the antidepressants of the modern day4. This study found that phenelzine, a typical MAOI, was no better than Prozac, a typical SSRI. Since Prozac had fewer side effects, that made the choice in favor of Prozac easy.
Did you know you can look up the authors of scientific studies on LinkedIn and sometimes get very relevant information? For example, the lead author of this study has a resume that clearly lists him as working for Eli Lilly at the time the study was conducted (spoiler: Eli Lilly is the company that makes Prozac). The second author’s LinkedIn profile shows he is also an operations manager for Eli Lilly. Googling the fifth author’s name links to a news article about Eli Lilly making a $750,000 donation to his clinic. Also there’s a little blurb at the bottom of the paper saying “Supported by a research grant by Eli Lilly and company”, then thanking several Eli Lilly executives by name for their assistance.
This is the sort of study which I kind of wish had gotten replicated before we decided to throw away an entire generation of antidepressants based on the result.
But who will come to phenelzine’s defense? Not Parke-Davis , the company that made it: their patent expired sometime in the seventies, and then they were bought out by Pfizer5. And not Pfizer – without a patent they can’t make any money off Nardil, and besides, Nardil is competing with their own on-patent SSRI drug Zoloft, so Pfizer has as much incentive as everyone else to push the “SSRIs are best, better than all the rest” line.
Every twenty years, pharmaceutical companies have an incentive to suddenly declare that all their old antidepressants were awful and you should never use them, but whatever new antidepressant they managed to dredge up is super awesome and you should use it all the time. This sort of does seem like the sort of situation that might lead to older medications being better than newer ones. A couple of people have been pushing this line for years – I was introduced to it by Dr. Ken Gillman from Psychotropical Research, whose recommendation of MAOIs and Anafranil as most effective match the patient data very well, and whose essay Why Most New Antidepressants Are Ineffective is worth a read.
I’m not sure I go as far as he does – even if new antidepressants aren’t worse outright, they might still trade less efficacy for better safety. Even if they handled the tradeoff well, it would look like a net loss on patient rating data. After all, assume Drug A is 10% more effective than Drug B, but also kills 1% of its users per year, while Drug B kills nobody. Here there’s a good case that Drug B is much better and a true advance. But Drug A’s ratings would look better, since dead men tell no tales and don’t get to put their objections into online drug rating sites. Even if victims’ families did give the drug the lowest possible rating, 1% of people giving a very low rating might still not counteract 99% of people giving it a higher rating.
And once again, I’m not sure the tradeoff is handled very well at all.6.
VI.
In order to distinguish between all these hypotheses, I decided to get a lot more data.
I grabbed all the popular antipsychotics, antihypertensives, antidiabetics, and anticonvulsants from the three databases, for a total of 55,498 ratings of 74 different drugs. I ran the same analysis on the whole set.
The three databases still correlate with each other at respectable levels of +0.46, +0.54, and +0.53. All of these correlations are highly significant, p < 0.01. The negative correlation between patient rating and doctor rating remains and is now a highly significant -0.344, p < 0.01. This is robust even if antidepressants are removed from the analysis, and is notable in both psychiatric and nonpsychiatric drugs.
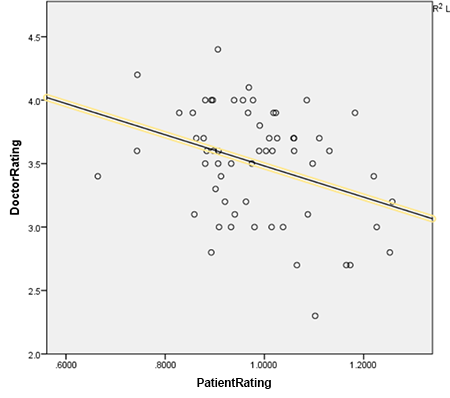
The correlation between patient rating and year of release is a no-longer-significant -0.191. This is heterogenous; antidepressants and antipsychotics show a strong bias in favor of older medications, and antidiabetics, antihypertensives, and anticonvulsants show a slight nonsignificant bias in favor of newer medications. So it would seem like the older-is-better effect is purely psychiatric.
I conclude that for some reason, there really is a highly significant effect across all classes of drugs that makes doctors love the drugs patients hate, and vice versa.
I also conclude that older psychiatric drugs seem to be liked much better by patients, and that this is not some kind of simple artifact or bias, since if such an artifact or bias existed we would expect it to repeat in other kinds of drugs, which it doesn’t.
VII.
Please feel free to check my results. Here is a spreadsheet (.xls) containing all of the data I used for this analysis. Drugs are marked by class: 1 is antidepressants, 2 is antidiabetics, 3 is antipsychotics, 4 is antihypertensives, and 5 is anticonvulsants. You should be able to navigate the rest of it pretty easily.
One analysis that needs doing is to separate out drug effectiveness versus side effects. The numbers I used were combined satisfaction ratings, but a few databases – most notably WebMD – give you both separately. Looking more closely at those numbers might help confirm or disconfirm some of the theories above.
If anyone with the necessary credentials is interested in doing the hard work to publish this as a scientific paper, drop me an email and we can talk.
Footnotes
1. Technically, MAOI superiority has only been proven for atypical depression, the type of depression where you can still have changing moods but you are unhappy on net. But I’d speculate that right now most patients diagnosed with depression have atypical depression, far more than the studies would indicate, simply because we’re diagnosing less and less severe cases these days, and less severe cases seem more atypical.
2. First-place winner Nardil has only 16% as many reviews as last-place winner Viibryd, even though Nardil has been on the market fifty years and Viibryd for four. Despite its observed superiority, Nardil may very possibly be prescribed less than 1% as often as Viibryd.
3. Pretty much the same thing is true if, instead of looking at the year they came out, you just rank them in order from earliest to latest.
4. On the other hand, what we do have is a lot of studies comparing MAOIs to imipramine, and a lot of other studies comparing modern antidepressants to imipramine. For atypical depression and dysthymia, MAOIs beat imipramine handily, but the modern antidepressants are about equal to imipramine. This strongly implies the MAOIs beat the modern antidepressants in these categories.
5. Interesting Parke-Davis facts: Parke-Davis got rich by being the people to market cocaine back in the old days when people treated it as a pharmaceutical, which must have been kind of like a license to print money. They also worked on hallucinogens with no less a figure than Aleister Crowley, who got a nice tour of their facilities in Detroit.
6. Consider: Seminars In General Psychiatry estimates that MAOIs kill one person per 100,000 patient years. A third of all depressions are atypical. MAOIs are 25 percentage points more likely to treat atypical depression than other antidepressants. So for every 100,000 patients you give a MAOI instead of a normal antidepressant, you kill one and cure 8,250 who wouldn’t otherwise be cured. The QALY database says that a year of moderate depression is worth about 0.6 QALYs. So for every 100,000 patients you give MAOIs, you’re losing about 30 QALYs and gaining about 3,300.
4 comments
Comments sorted by top scores.
comment by glorius_lasagne · 2019-10-27T17:05:02.148Z · LW(p) · GW(p)
This is such an incredibly well researched and well thought out post, it's a surprise and a disappointment that there has been no comments even four years later (I had been looking forward to reading the discussion section). I really have to thank you for the effort you put into compiling the data. It had helped me decide what to try first.
Also, all the top 5 rated antidepressants significantly affect either the dopaminergic system or the norepinephrine system or both, while most antidepressants primarily affect the serotonin system. The treatment of atypical depression is known to improve with the supplementation of psychostimulants like modafinil, buproprion and occasionally ritalin to typical antidepressant therapy. These drugs increases the amount of dopamine and norepinephrine (only dopamine in the case of modafinil) in the synapses. So that could just be the shared thread for why certain antidepressants are more effective than others - by not just increasing serotonin.
By the way could you reupload the excel file? I cannot seem to download it but would really like to look through the data in more detail.
Replies from: habryka4, eigen↑ comment by habryka (habryka4) · 2019-10-27T19:32:02.990Z · LW(p) · GW(p)
(This post was originally posted here, where it got over 250 comments: https://slatestarcodex.com/2015/04/30/prescriptions-paradoxes-and-perversities/)
↑ comment by eigen · 2019-10-27T18:38:31.157Z · LW(p) · GW(p)
You can find discussion of this post on Scott's Blog.
comment by Ben (ben-lang) · 2024-04-19T16:01:55.349Z · LW(p) · GW(p)
I don't think the negative correlation between doctors and patients opinion of the drugs is surpassing.
Rat poison would probably get a low score from both doctors and patients. However, nobody is being prescribed rat poison as an anti-depressant so it doesn't appear in your data. Why is nobody being prescribed rat poison? Well, doctors don't prescribe it because they think its a bad idea, and patients don't want it anyway.
In order for any drug to appear in your dataset somebody has to think it is good. So every drug should have net-approval from at least one out of the doctors and patients. Given this backdrop a negative correlation is not surprising.