Covid 2/24/22: The Next War
post by Zvi · 2022-02-24T14:30:01.434Z · LW · GW · 4 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Physical World Modeling Prevention and Prevention Prevention Prevention Think of the Children Announcing Alvea – An Effective Altruist Covid-19 Vaccine Project In Other News Not Covid None 6 comments
Russia has invaded Ukraine with the stated goal of 'demilitarization and denazification.'
On its face, this has nothing to do with Covid. The invasion may reflect a perception, either on the part of Putin or otherwise, from our Covid-19 response or otherwise, that the West has shown itself incapable of dealing with real world physical problems, and therefore feeling he has a free hand. It also may have shown Putin and/or others that one can use justifications that are obvious and blatant nonsense lies with impunity. Those facts also may have little or nothing to do with it. We do not know.
I do not feel qualified at this time to comment further beyond an urgent call to build as many state of the art nuclear power plants as we can as quickly as possible, so I’ll be looking at other sources and watching the BBC News like everyone else to try and get a handle on the war. At least for now I’d only be adding noise.
Under such conditions, and with Omicron in decline and relatively mild, it may seem foolish to focus on Covid-19. Ignoring other events would be a mistake, but ignoring Covid-19 would also be a mistake. Covid-19 prevention efforts continue to disrupt our lives, and as events in Canada have shown us such events can pose long term existential threats to our freedom. Justin Trudeau has ended his emergency decree, but the groundwork remains laid for next time. There is danger that a variety of pandemic measures might not only continue for far too long but even become permanent.
As for the actual case and death counts? Sure, worth tracking those too.
Executive Summary
- Russia invades Ukraine.
- Canada freezes bank accounts of those they dislike without due process.
- Covid cases continue to decline.
Let’s run the numbers.
The Numbers
Predictions
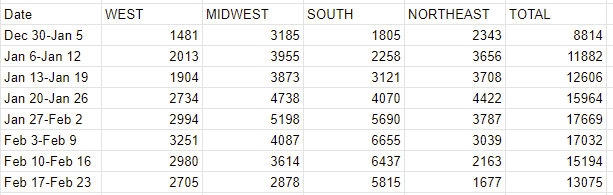
Prediction from last week: 555k cases (-35%) and 11,400 deaths (-25%).
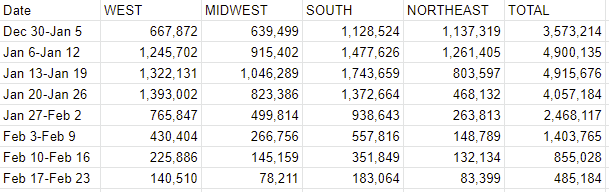
Results: 485k cases (-40%) and 13,075 deaths (-14%).
Prediction for next week: 340k cases (-30%) and 10,460 deaths (-20%).
I forgot about Presidents Day, which explains cases dropping somewhat more than I expected, so I presume true case counts were closer to the path that I expected.
That only makes the small decline in deaths more puzzling. There are echoes of this in the past, where death counts declined less rapidly than expected at the tail end of a wave, presumably because of a long tail of how long it takes some patients to die and/or officials to register some of the deaths. It is not plausible that death rates are suddenly much higher, so such lags are the only remaining explanation. I do still expect the decline to accelerate from here, but I will temper such expectations.
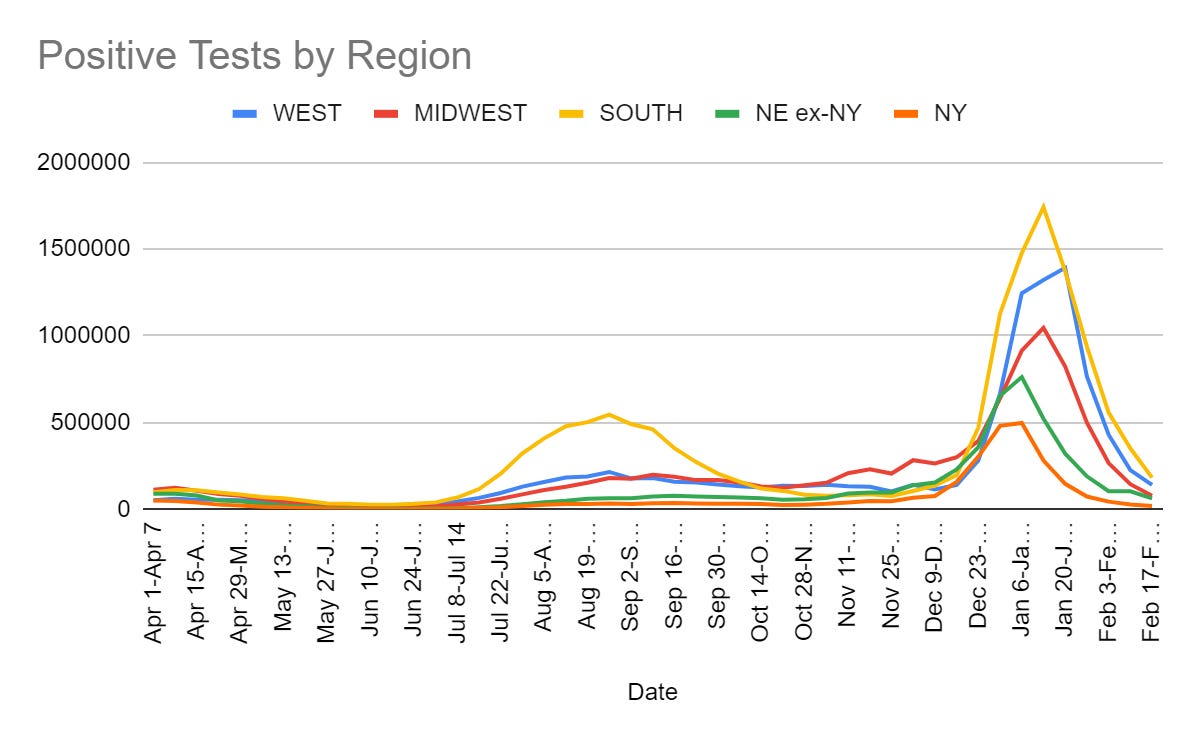
Given the declines continue to be broad-based across all regions, I don’t expect them to slow much – the smaller decline here mostly represents me adjusting for the holiday.
Deaths
Cases
Physical World Modeling
The BA.2 variant of Omicron is going to take over from the BA.1 variant. Should we be worried?
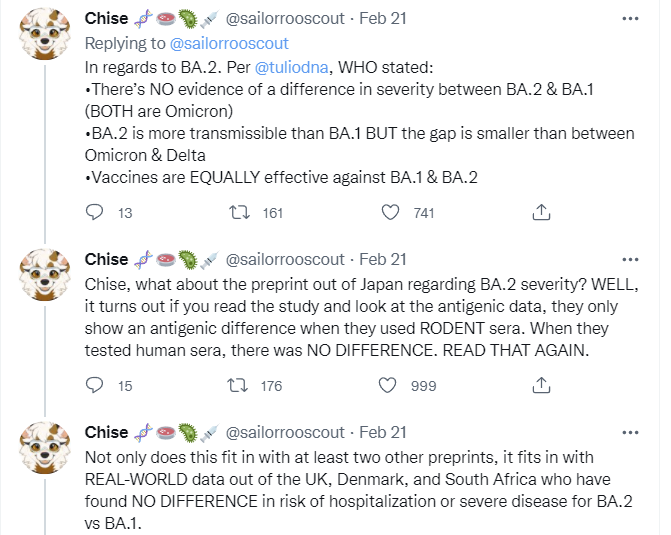

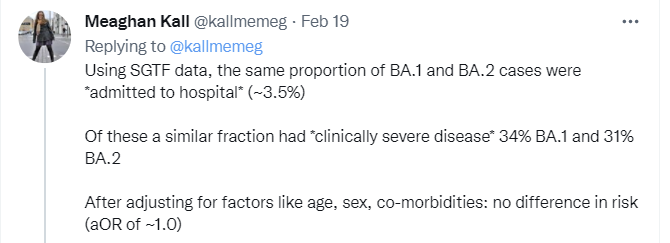
It does mean rate of spread will rise somewhat, but if it was enough to put us back into a nightmare it would not have taken this long.
Study puts the India death toll in the 3.2mm-3.7mm range.
Sanofi vaccine tests at 100% effective against severe disease. FDA approval will be tricky and it is not clear another vaccine matters at this stage, but still good news.
CDC data seems to contradict itself. The difference does not much matter for what we should do, but it is still rather a large mistake to be making and risks leading to a lot of confusion.
Zeynep thread on Long Flu cases from the 1919 pandemic. Such problems are nothing new and have been underplayed for a long time. Disease is not good for humans.
Prevention and Prevention Prevention Prevention
New York City Mayor Eric Adams keeps getting better, reveals plans to perhaps let my people go right here where I live.
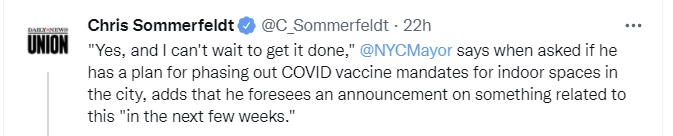
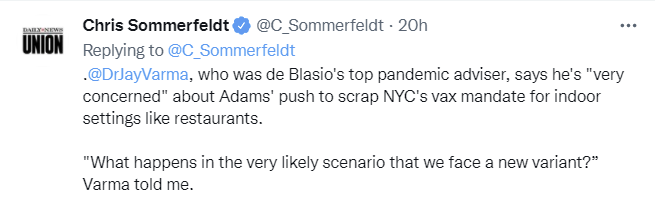
If and when there is another variant that changes the situation sufficiently that we need to rethink the situation, it seems easy enough to temporarily reinstate the mandate. It is high time, and ‘can’t wait to get it done’ shows exactly the right attitude. We are very close to the traditional 10 cases per 100k people per day threshold (I think we’re at 12 right now). When we get to 10 is when I start pushing on things like the guidelines in my own building.
Who counts as ‘we’ is always tricky.
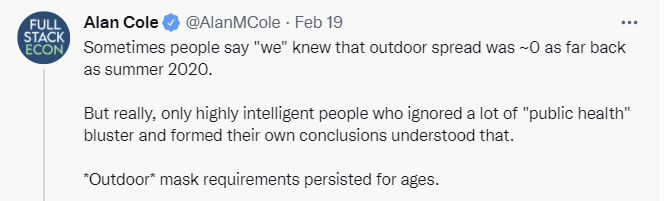
What counts as ‘we’ knowing a thing? If those who are ‘forming their own conclusions’ know it but public health officials refuse to acknowledge it and the rules do not reflect it, do we know it?
Yes. I think that counts. The statement “We knew X but officials kept saying ~X” seems to me to be meaningful and not a contradiction. Consider the top reply to above.
What “we” know and what is official policy are, to me, different magisteria.
Here is an interesting argument that what matters most is not when to end restrictions, but what it would take to start them up again.
There is also a basic obviously correct point here, which is that our public health apparatus failed us and we need to fix it so that does not happen again, and in particular we need to get ahead of the situation and project forward (as I have attempted to do) rather than react only when things are already bad.
There is also the point that the key problem with lifting restrictions, both in terms of consequences and in getting people to be all right with it, is specifying what would make us reverse course. It’s also a discussion that’s better to have now, rather than later. We can agree to end restrictions now, and then resume them if and only if the agreed upon conditions surface, which can include ‘new pandemic threat that isn’t Covid’ without exact details on that front.
What would be a good rule? The temptation is to say ‘never’ and I would endorse that in the absence of a new variant but new variants that are sufficiently dangerous remain possible. We would want a principle for what to do if that happened. I would say that in order to re-impose restrictions we would need to either see a new variant that had (1) was clearly going to take over and spread rapidly enough to have a peak approaching or exceeding January 2022, (2) had large additional immune escape and (3) was expected to be substantially more dangerous than Omicron despite the availability of new treatments. Or alternatively, if (4) the hospitals were clearly about to be overwhelmed, by some definition of that, maybe just use the hospital criteria since reacting too soon only burns up the public’s willingness to endure restrictions anyway.
That would be my suggestion. If someone wants to reimpose rules simply on modestly higher case levels, they should say that now so we can all know what we are dealing with – but also so we can perhaps reach an understanding.
While 70% of Americans think ‘Covid is here to stay and we should get on with our lives’ opinions about whether to actually decrease prevention are all over the map. About half of people still seem to want to keep current measures in place or even strengthen them, despite no practical hope that this would ever end.
Here are some poll results about indoor mask mandates in particular.
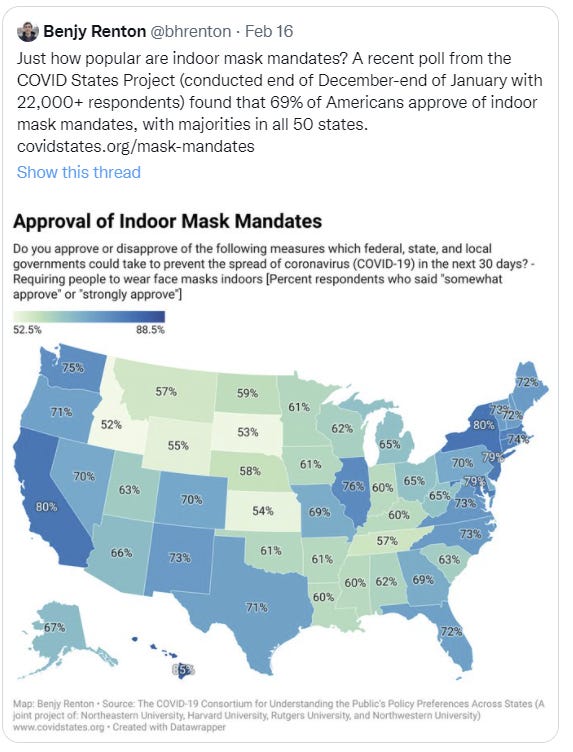
Note however that this poll, although shared this week, referred to indoor mask mandates for the next thirty days as of the end of December. At that time the argument for a temporary indoor mask mandate was maximally strong. Cases are dramatically down since then.
It is widely believed that speaking helps to spread Covid, including in public places. Yet if you try to book a ticket on the Acela (a term also used sarcastically to describe a particular brand of Eastern elites), you can get tickets only in the Quiet Car. The rest of the train is already sold out, because people prefer to be able to talk.
You may not think that is how things should be, but that is how they are. And no, the Acela does not run from Alabama to West Virginia.
Not only is the quiet car otherwise underrated, this shows how much people actually care about physical Covid prevention for its own sake. The answer is very little.
When the account DefiantLs got suspended from Twitter I started following it for a bit, until this one made me realize I’d had more than enough.

Not only is it impossible for people to tell the difference between public mandate and private choice, they are being mocked as hypocrites and liars for daring to notice that there is a distinction.
The fifth circuit court ruled that United’s employees might suffer irreparable harm if its vaccine mandate was implemented. A conservative judge dissenting from the decision brings what can only be described as The Fire, and calls for en banc consideration even though decision wasn’t published. Thread is wild, if you dig that sort of thing you should check it out.
UK now lets you order free lateral flow tests every 72 hours instead of every 24. It is odd that stricter limits need to be imposed now after demand has peaked. Perhaps too many people were using this to hard tests.
Think of the Children
CDC has lowered its requirement for how fast kids learn speech. [LW(p) · GW(p)]

They didn’t say why they did this, but perhaps could masks be hurting children’s ability to learn language, and they’re trying to pretend it is fine?
Mostly I’m all for lowering ‘milestones’ because my experience as a parent says that the primary purpose of milestones is to find the place in which your child is below average and then freak you the hell out about it for no good reason.
Washington Post has an article about mask battles in Virginia public schools where students now are free to choose.
Youngkin issued his mask-optional order, which aims to give Virginia parents choice over masking in both public and private schools, on his first day in office. A fierce fight ensued: Seventy of 131 Virginia school districts refused to comply and kept their mask requirements, according to a Washington Post analysis, and parents and school officials filed a flurry of lawsuits for and against the order. This week, the Virginia General Assembly narrowly passed — along largely partisan lines — a law that requires all schools to go mask-optional on March 1, ensuring every one of Virginia’s more than 1.8 million public and private schoolchildren will face masking decisions and tensions at school in days to come.
Lawsuits in all directions is our fate these days in such situations. There is little freedom of action, even over the question of whether those forced to attend will have this little bit of freedom of action.
As one might expect, school officials often did their best to enforce the now-disallowed mask mandate by other means.
Some Virginia students were thrilled to remove their masks — but their elation quickly souredwhen administrators in districts that still required masking sent unmasked children into isolated rooms or back to their homes.
Later in the post is the story of two students who tried to not wear masks, and were imprisoned and denied their educations as punishment by the school until they gave in. As a consequence, they are being socially ostracized.
The term is ‘can’t let it go’:
School now feels, Swan said, “like a war zone”: a raging partisan battle that no one can opt out of, because every single student arrives with evidence of their politics — those without masks typically lean right, she said — written across their faces. Swan said she has stopped speaking with students who go maskless because they are dismissive of the decision to mask and unwilling to hear a different opinion.
Yes, you can opt out of this ‘partisan battle,’ but we’ve drilled in such toxic messaging that the kids can often no longer see that.
Notice the framing. If you make the anti-Narrative decision, you are ‘unwilling to hear a different opinion.’ So she stops speaking with them. Which, I believe, is the literal definition of being unwilling to hear a different opinion – if you do not agree with her, she will not speak to you.
The entire article, in the Washington Post, paints a strangely one-sided picture.
Students who want to go maskless are doing so because they not only see little risk but also because they systematically find it difficult to learn while wearing masks. One has given up wearing glasses because they kept fogging up, and is learning semi-blind. Others found it difficult to focus, talk and listen.
Students and parents who insist on mask mandates ignore (and presumably when challenged, deny the existence) of such problems, impose mandates via isolation and ostracism and treat any disagreement as evidence of unreasonableness. Two students raised actual concerns. One has severe lung damage and sounds like he has no business being in school regardless of who wears what masks given the level of health concerns. Remember that masks only offer modest protection. The other is physically concerned is concerned because her getting Covid might force a family member to quarantine, and then be unable to take another family member to the hospital for an unrelated condition. Quite telling.
The ACLU is suing to force schools to force students to wear masks, on the theory that not requiring masks is ‘excluding, denying access or segregating.’ I remember when the ACLU did not actively fight against civil liberties.
Announcing Alvea – An Effective Altruist Covid-19 Vaccine Project [EA · GW]
I find this project super exciting, and I consulted for them briefly on modeling cases to help plan their clinical trials. I’ll be happy to help them again if they once again need my expertise or advice.
We’ve had effective COVID vaccines for more than a year, but there are still countries where less than 10% of people have received a dose. Omicron has been spreading for almost three months, but pharma companies have only just started testing variant-specific shots. mRNA vaccines are highly effective, but they’re hard to manufacture and nearly impossible to distribute in parts of the developing world.
We won’t be ready for the next variant, or the next pandemic, until these problems are solved.
…
We’ve initially structured Alvea as a three-month sprint to test the hypothesis that an exceptionally bright, dedicated group of people can quickly accomplish remarkable things in this space. In the past eight weeks, we’ve built a team of 35 drug developers, logistics experts, physicians, operators, and scientists to bring the project to fruition. We’re supported by a network of consultants and partners with deep experience in every aspect of vaccine development and infectious disease response.
This is exactly what we should be doing, for both the ‘EA’ and ‘everyone’ values of we.
In the 60 days since our inception, we’ve designed twelve versions of our Omicron vaccine, responded to the emergence of the BA.2 subvariant, produced hundreds of doses of our lead candidate, run preclinical experiments in mice and sheep, kicked off scalable manufacturing processes, planned Phase I and II clinical studies, and identified potential partner countries for accelerated trials. There’s an enormous amount of work still to be done, but we are well on our way.
They are hiring, and if you’re thinking about it I’d encourage you to reach out to them.
Alvea is led by Ethan Alley and Grigory Khimulya (Co-CEOs), Cate Hall, and Kyle Fish. Our team is growing rapidly, and we’re particularly keen to expand in the following areas:
- Wet laboratory (molecular biology, in vitro and in vivo development)
- Clinical trial operations and logistics
- General company operations
- cGMP manufacturing and quality
- Technical/scientific management
We’d love to hear from anyone who’s interested in dropping everything to get involved! Reach us at info@alveavax.com.
Here’s a post that lists some other ideas for potentially big EA biosafety projects. [EA · GW] It’s good to think big, and to actually go attempt to Do the big Thing.
In Other News
Bloomberg reports that Paxlovid supply is catching up to newly reduced demand. This is a huge deal. If Paxlovid is available to whoever wants it the risks from Covid-19 drop dramatically, and any decision on a personal level to be afraid of Covid-19 at all while vaccinated simply does not make any sense.


Latest Ivermectin study finds a (probably coincidental) small negative effect on disease progression. My model is that people are either convinced it doesn’t work or convinced it does in ways that won’t be moved by such studies, so more such studies won’t make the question more over than it already was, but including anyway.
Some info on China’s ‘wet markets.’
Thread where WHO is its usual unhelpful self, in a low-key internal conference way.
Report from the NYC Anime Convention where Omicron spread amongst a group of friends. A positivity rate of 2.5% is judged to be evidence that ‘masks and other countermeasures worked’ but the associates of the local patient zero largely still got infected with Omicron, so this is an odd use of the word ‘worked.’
UK Covid testing company sells customer genetic information to third parties. If this surprises or alarms you, what can I say, always read your contract.
Following up on the ‘CDC is insanely cautious’ principle from last week, one should point out it goes that much deeper. They recommend not only well done burgers but well done steak, requests for which rightfully get one actively thrown out of fine restaurants. Treat CDC requirements as being similar to requiring steak be cooked well done.
This thread attempts to give an answer to ‘should we mask?’ now that we have the option not to, and attempts to offer various logic and considerations, from someone who has offered various useful physical modeling during Omicron, but the core thinking is truly bizarre to me if taken at face value.
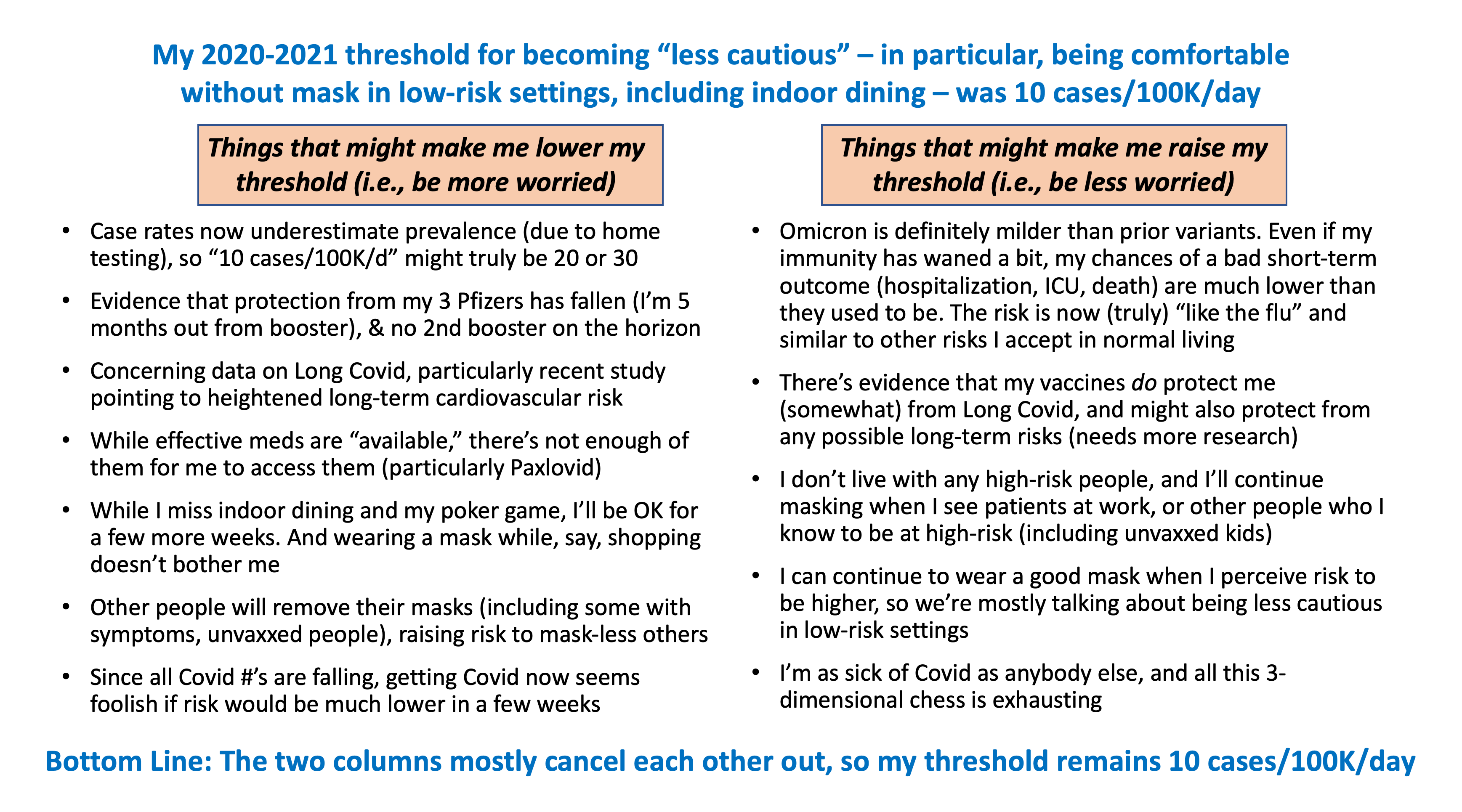
My guess on the actual logic here is that an arbitrary threshold was picked, and disposing of it would require more justification than sticking with it, so there are strong internal pressures to find a way to say everything cancels out and stick with the same threshold even though the threshold should clearly have gone up. That then combines with morality-based pandemic models, where what determines risk is largely whether people’s prevention sacrifices are worthy.
Case rates are underestimated? Yes, but no reason to think they are now more underestimated than they were before Omicron, so this isn’t a change, except to extent that many cases are so mild they are literally going unnoticed. Which might be true but doesn’t sound like a reason to on net increase worry.
Protection has fallen? Maybe somewhat, but the original threshold predates the boosters entirely, as well as Omicron, and the booster isn’t listed in the righthand benefits column to begin with.
The data on Long Covid I’ve analyzed in detail and at this point and I do not believe such considerations look worse than they did previously, whatever one’s view on them overall.
Others ditching masks increasing your risk and thus encouraging you to wear a mask can be true or false depending on what you are controlling for. If we know how many cases there are, and that cases are declining at a given rate, then noticing lack of masks does not increase our estimate of risk, because whatever is happening was already priced in. If anything, everyone else going maskless decreases your estimate of risk, because it means that going maskless would keep your relative risk the same as theirs, and we already know the average risk level. Similarly, seeing everyone around you indoor dine and take other risks should make you more worried if you don’t know the number of cases or rate of case growth. But it should make you less worried if you do know the number of cases and rate of case growth already.
Paxlovid being partially available is a reason to be less cautious on net, not more cautious, yet somehow Paxlovid ends up in the ‘more worried’ column.
Being able to ‘live with it for a few more weeks’ was always true, and when will that stop? A better way of putting this is ‘cases are declining rapidly’ and all right, I guess, but it’s still marginal costs versus marginal benefits. The real objection here is the last one, that it ‘seems foolish’ to risk now if risk is lower later, rather than doing an EV calculation where lower risk in future sufficiently raises the value of prevention now.
Overall, I can’t see a plausible case that the ‘more worried’ considerations could come close to cancelling out the booster and the transition to Omicron. Especially since we are still talking about doing the especially high-value prevention efforts even below whatever threshold we pick. If the risk is truly ‘like the flu’ as he states why are we even having these conversations at this point?
Not Covid
Before the war started I was working on clearing out my backlog of non-Covid things, so I have a draft of a lot of those that I hope to go live with later today once I finish organizing it. Then I need to think about what makes sense given the war that started overnight.
4 comments
Comments sorted by top scores.
comment by maia · 2022-02-24T19:02:58.288Z · LW(p) · GW(p)
Emily Oster has commentary on the CDC milestone update that I find very compelling:
The last round of developmental milestones from the CDC focused more on what we would expect from the average child. This update is intended to capture something like: at least 75% of children at this age would meet this milestone. This means, then, that if a child is not meeting it, they are in the lower 25% in terms of that area. And this is the group we want to flag for possible early intervention. Prior to the update, the guidelines were closer to identifying the average — the 50th percentile. But, of course, moving from a milestone that identifies the 50th percentile of the distribution to one that identifies the 25th percentile will change the expectation.
Makes way more sense for the milestones to be 25th percentile if the goal is "have the milestones set that you SHOULD freak out if your child doesn't meet them", i.e. most children will meet them rather than only 50%.
comment by Dirichlet-to-Neumann · 2022-02-25T13:05:19.419Z · LW(p) · GW(p)
I'd be very interested if you were trying something similar to your Covid chronicle for Putin's invasion war. I learned a lot reading you on Covid, and I think understanding wars (in general) requires a fair bit of the same capacity you needed for the pandemic crisis.
Replies from: Zvicomment by Pattern · 2022-02-24T21:17:25.595Z · LW(p) · GW(p)
Washington Post has an article about mask battles in Virginia public schools where students now are free to choose.
Youngkin issued his mask-optional order, which aims to give Virginia parents choice over masking in both public and private schools,
Students are free to choose? Or parents?
As a consequence, they are being socially ostracized.
Huh. From the link:
Seconds after they walked into the school building, Sam and Andrew said, administrators directed them into an empty auditorium with about a dozen other students who had also come to school without masks. The boys remained there for the rest of the day, supposedly learning asynchronously — meaning they completed assignments without live instruction — although both said they didn’t learn at all.
That persisted for a week. Eventually the boys were moved from the auditorium into an empty classroom “that didn’t have any lights on,” because staffers never bothered to turn them on, Sam said. But they were determined to prevail. When the two teens kept showing up maskless for a second week, officials allowed them back into their classrooms but erected plexiglass bubbles around their desks, making them feel like social pariahs, the boys said.
...
Both teens said they noticed a change in how some people at school treated them. Other students who support masking have stopped speaking to the boys: “They kind of treat us like we’re an embarrassment,” Sam said.
Even when both boys again started going to school masked, the social ostracizing has persisted, they said.
...
On Thursday, Henrico schools began allowing students to attend class maskless in early obedience to the new Virginia law — and, after their first day of breathing unencumbered, both boys said they were, finally, feeling better.
Not clear if persisted after that, but, perhaps that remained to be seen. (Assumption: yes, it persisted, at least for a time.)
The entire article, in the Washington Post, paints a strangely one-sided picture.
A very particular picture:
“I wanted to speak from a student perspective, because you don’t hear much of that on the news,” Angela, 18, who wants to pursue a career in social work, said in an interview. “You hear ‘Parents are fighting for this.’ ‘Adults are fighting for this.’ I wanted to make sure a student voice was heard.”
In comparison to the Washington Post itself earlier in the article:
The Washington Post asked parents across the state to share how their children are feeling about school masking policies, garnering nearly 200 submissions from families living in at least 25 school districts.
They don't seem to care about that perspective, and they're not subtle about it.
One has given up wearing glasses because they kept fogging up, and is learning semi-blind.
How cold is that classroom?
One has severe lung damage and sounds like he has no business being in school regardless of who wears what masks given the level of health concerns.
Is that legal? (Not being in school?)
The other is physically concerned is concerned because...
The other is physically concerned because...?
The ACLU is suing to force schools to force students to wear masks, on the theory that not requiring masks is ‘excluding, denying access or segregating.’ I remember when the ACLU did not actively fight against civil liberties.
That oversimplifies a tad: See footnote 1.
Notice the framing. If you make the anti-Narrative decision, you are ‘unwilling to hear a different opinion.’ So she stops speaking with them. Which, I believe, is the literal definition of being unwilling to hear a different opinion – if you do not agree with her, she will not speak to you.
This is also the WP's framing though. It chose to say it that way instead of
- 'persuading students not wearing masks to do so is risky because it involves a greater degree of exposure'
Finding an individual who does what they want for the reasons they want may be possible, out of hundreds.
Students and parents who insist on mask mandates ignore (and presumably when challenged, deny the existence) of such problems,
Top down systems systematically prove inflexible, and unhelpful. Also see footnote 1.
If Paxlovid is available to whoever wants it the risks from Covid-19 drop dramatically, and any decision on a personal level to be afraid of Covid-19 at all while vaccinated simply does not make any sense.
and any decision
or
then any decision?
Following up on the ‘CDC is insanely cautious’ principle from last week, one should point out it goes that much deeper. They recommend not only well done burgers but well done steak, requests for which rightfully get one actively thrown out of fine restaurants. Treat CDC requirements as being similar to requiring steak be cooked well done.
Hm. Are there options here involving a su vide that are safer (and tastier)?
Paxlovid
Availability seems like (at some point) it might be worth a post. Googling turned up:
https://www.drugs.com/price-guide/paxlovid
The cost for Paxlovid oral tablet (150 mg-100 mg) is around $10 for a supply of 30 tablets, depending on the pharmacy you visit. Prices are for cash paying customers only and are not valid with insurance plans.
Interesting.
https://www.goodrx.com/conditions/covid-19/covid-pill-cost-availability
The COVID-19 pills are in short supply in some areas, while other areas may have plenty in stock. More courses of molnupiravir have been delivered to states than Paxlovid so far. Eligible patients can receive the treatment free of charge during the public health emergency.
Hm. Who is eligible?
In late December 2021, the FDA granted emergency use authorization (EUA) to Pfizer’s Paxlovid (nirmatrelvir and ritonavir) after clinical trials showed it cut the risk of hospitalization and death for people at high risk of severe COVID-19 by nearly 90%.
Paxlovid is authorized for eligible adults and children age 12 and older who weigh at least 88 pounds. You would take 3 pills (2 nirmatrelvir pills and 1 ritonavir pill) by mouth twice a day for 5 days. You should start taking the pills within the first 5 days of feeling COVID-19 symptoms.
In studies, Paxlovid interacted with many common medications.
Paxlovid is the first-choice recommendation for patients with mild to moderate COVID-19 who are at high risk of hospitalization or death, according to the National Institutes of Health treatment guidelines.
The NIH order of preference is:
- Paxlovid
- Sotrivimab (a single IV infusion)
- Remdesivir (an IV infusion)
- Molnupiravir
(the quotes conflicted with the bullet points, I added the bullet points back in)
I wonder what those medications it interacts with are.
Unlike Paxlovid, molnupiravir is only authorized for adults age 18 and older. It’s not known to interact with any medications, but further studies are needed to confirm this.
...
States with larger populations have received more treatment courses from the federal government than those with fewer residents. States also have different ways of distributingthe antiviral pills among hospitals, clinics, local health departments, and pharmacies.
More treatment courses of molnupiravir than Paxlovid have been delivered to states and territories for distribution so far.
...
How much do Paxlovid and molnupiravir cost?
COVID-19 antivirals to be free to patients during public health emergency
January 13, 2022
Paxlovid cost the U.S. government about $530 per course. Molnupiravir cost the U.S. about $700 per course. Both antiviral drugs are “available to the applicable patient population free of charge during the COVID-19 public health emergency,” a spokesperson from the Centers for Medicare & Medicaid Services (CMS) said in an email. It’s unclear how long coverage will last.
Are there any COVID-19 preventive options for people who can’t get vaccinated?
New option for people who can’t get the COVID-19 vaccine
January 13, 2022
Evusheld is a combination of two monoclonal antibody medications: tixagevimab and cilgavimab. The FDA granted EUA for Evusheld for COVID-19 pre-exposure prophylaxis — to prevent an infection if you’re exposed to the virus in the future — for certain people age 12 and older who weigh at least 88 pounds. It’s an alternative option for people who can’t get a COVID-19 vaccine because of a serious allergy or likely won’t respond well to the vaccine because of a weakened immune system. A healthcare provider would give you 2 injections of Evusheld as a single dose.
The U.S. government ordered another 500,000 doses of Evusheld, White House officials said. In addition to the 700,000 doses already ordered, that’s a total of 1.2 million doses soon to be available through the end of March. Eligible patients can receive Evusheld at no cost. You may need to ask your healthcare provider how to get it, as it may not be available at your local pharmacy.
...
There is one other monoclonal antibody, sotrovimab, authorized for early treatment of high-risk patients with mild to moderate COVID-19 that is effective against the Omicron variant. Sotrovimab is in short supply, according to NBC and other news outlets. Its manufacturers, GlaxoSmithKline and Vir Biotechnology, recently announced that the U.S. government is buying 600,000 more doses. The doses are scheduled for distribution during the first quarter of 2022.
Paxlovid Interactions
Drug classes of particular concern are those that include drugs that are prone to concentration-dependent toxicities, including (but not limited to) certain antiarrhythmics, oral anticoagulants, immunosuppressants, anticonvulsants, antineoplastics, and neuropsychiatric drugs.
...
Medications That Are Contraindicated or Should Not Be Coadministered With Ritonavir-Boosted Nirmatrelvir (Paxlovid)
This table is a guide and not a comprehensive list of all possible drugs that may interact or should not be coadministered with ritonavir-boosted nirmatrelvir (Paxlovid).
...
There's 50 drugs in the left side of the table* (don't use Paxlovid with this) and 5 less on the right side**.
*Prescribe an alternative COVID-19 therapy for patients who are receiving any of the medications listed.
**If the patient is receiving any of these medications, withhold the medication if clinically appropriate.
- If withholding is not clinically appropriate, use an alternative concomitant medication or COVID-19 therapy.a
That's a long enough list I'm not going to try and copy it here. (Also not sure about tables in comments. With bullet points.)
There was also a note in there about how patients with certain conditions* are going to need different doses.
*I spotted a note about kidney function.
Footnote 1.
Other students, especially those with health conditions, were horrified to find themselves seated next to maskless peers, unable to do anything except ask to change seats. All too often, students said, their teachers denied that request, citing instructions from higher-ups not to segregate students by mask status.