Covid 8/5: Much Ado About Nothing
post by Zvi · 2021-08-05T14:00:00.700Z · LW · GW · 34 commentsContents
The Numbers Predictions Deaths Cases Vaccinations Vaccine Approval Vaccine Mandates Mask and Testing Mandates Vaccine Hesitancy Delta Variant The CDC Reinstates Its Mask Mandates The Provincetown Study The Leaked CDC Slides Thinking of the Children Apply for the Survival and Flourishing Fund In Other News Not Covid None 34 comments
Getting into the weeds on the CDC’s new guidance and scaremongering, and the study they cited as justifications, caused this week’s post to get rather long. That was necessary, but if you don’t need the details, by all means skip the sections in question in favor of this summary: The CDC’s failure to apply Bayes’ rule, correct for base rates or locate sufficiently large or remotely representative samples knows few if any bounds, and their conclusions are still mostly the same conclusions my model had reached weeks ago. Very little has changed. Our new model of Delta is almost entirely the same as our old model of Delta.
The other big development is the continuing fights over the growing number of mask mandates and vaccine mandates, and the potential descent of our children into a potentially permanent ever present young adult dystopia. It seems the same kids that aren’t allowed to get vaccinated are at so much risk that parents are being told by health officials on CNN to mask up in their own homes.
Not Covid, but worth mentioning up top: The latest set of grant applications to the Survival and Flourishing Fund are due on August 23. If you have a long term future oriented organization, I’d urge you to consider applying, more details at the link or later in this post.
In other news, there’s a good righteous FDA Delenda Est rant from Scott Alexander, if you’d like one.
Cases followed their expected path, and deaths followed.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 610,000 cases (+55%) and 2,450 deaths (+20%).
Result: 589k cases (+50%) and 2,889 deaths (+41%).
Deaths still went up slower than cases or lagged cases, but it seems we can’t continuously get giant additional weekly declines in the CFR. Only predicting a 20% rise there seems overly optimistic in hindsight and I’m considering it a bad prediction on my part. From here it seems right to predict rises in death that are only slightly lower than the rise in cases lagged several weeks.
Prediction for next week: 855,000 cases (+45%) and 4,100 deaths (+40%).
I still do expect deaths to go up slightly less than cases, partly because there’s lag everywhere in the system, but I no longer expect the underlying ratios to change much going forward. Case growth should slow down as behaviors adjust, and there’s some chance at any time we hit the peak although I expect that to still be at least a few weeks away.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Jun 24-Jun 30 | 550 | 459 | 706 | 186 | 1901 |
| Jul 1-Jul 7 | 459 | 329 | 612 | 128 | 1528 |
| Jul 8-Jul 14 | 532 | 398 | 689 | 145 | 1764 |
| Jul 15-Jul 21 | 434 | 341 | 732 | 170 | 1677 |
| Jul 22-Jul 28 | 491 | 385 | 1009 | 157 | 2042 |
| Jul 29-Aug 4 | 693 | 477 | 1415 | 304 | 2889 |
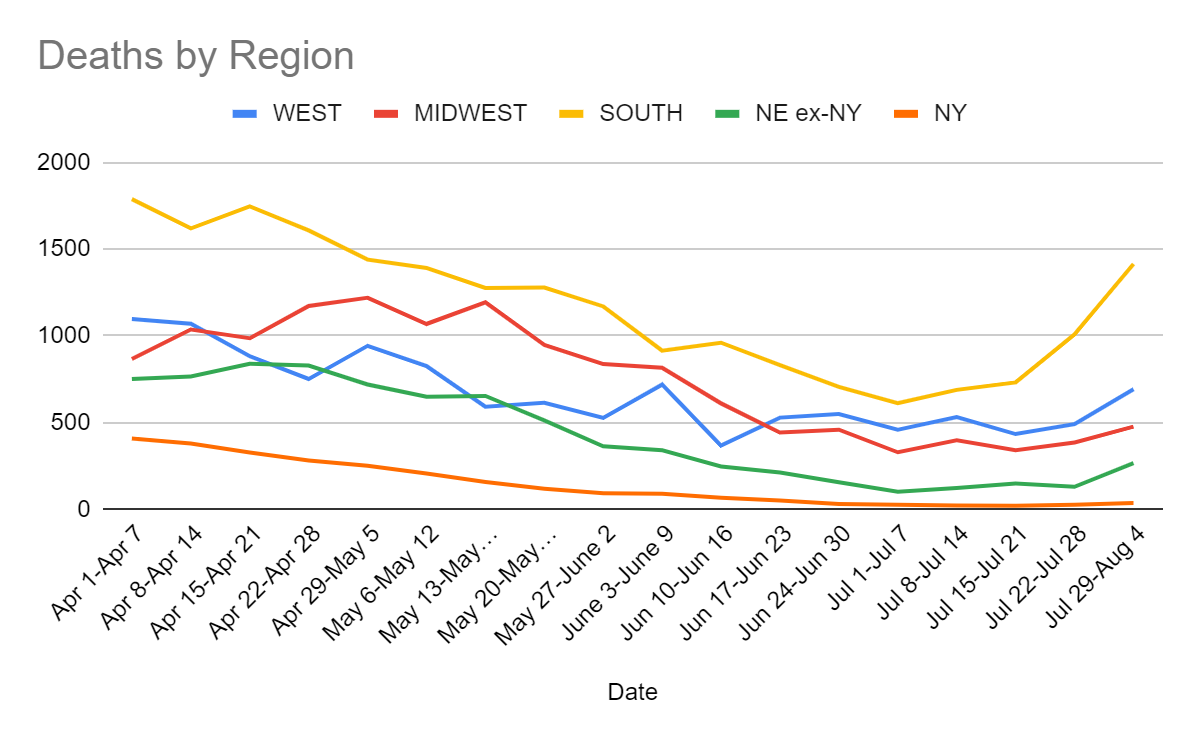
Death rates are far lower than they were in previous waves, and are still rising slower than cases, but the hope that we’d see only +20% this week was fully dashed.
Cases
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Jun 10-Jun 16 | 23,700 | 14,472 | 25,752 | 8,177 | 72,101 |
| Jun 17-Jun 23 | 23,854 | 12,801 | 26,456 | 6,464 | 69,575 |
| Jun 24-Jun 30 | 23,246 | 14,521 | 31,773 | 6,388 | 75,928 |
| Jul 1-Jul 7 | 27,413 | 17,460 | 40,031 | 7,065 | 91,969 |
| Jul 8-Jul 14 | 45,338 | 27,544 | 68,129 | 11,368 | 152,379 |
| Jul 15-Jul 21 | 65,913 | 39,634 | 116,933 | 19,076 | 241,556 |
| Jul 22-Jul 28 | 94,429 | 60,502 | 205,992 | 31,073 | 391,996 |
| Jul 29-Aug 4 | 131,197 | 86,394 | 323,063 | 48,773 | 589,427 |
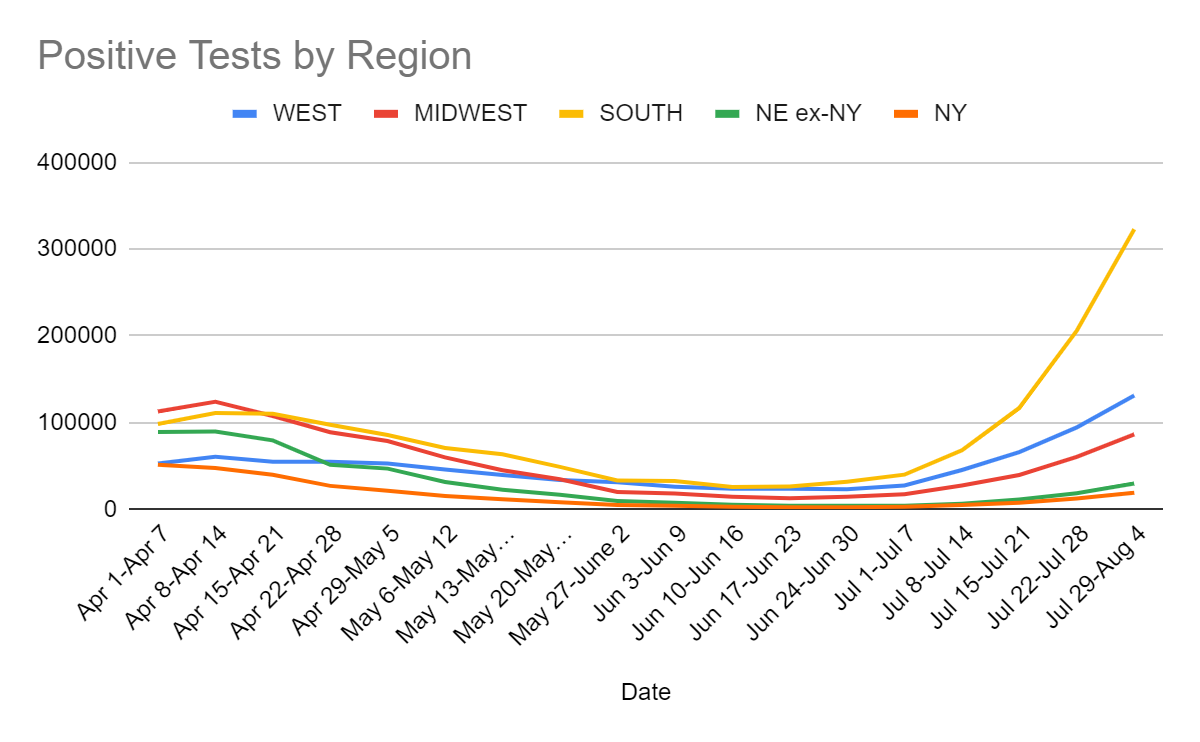
Similar growth in all regions. Vaccination levels matter, but also people adjust to their current situations in various other ways.
Vaccinations
I am slightly worried that the rise in vaccinations largely represents booster shots – I don’t know if that would mess up the statistics or not. If the numbers represent only first and second doses, they are very good news. Third doses aren’t useless (again, I’d happily accept one), but they’re less valuable than first or second doses by a lot, and counting them would give the wrong impression of the situation.



(This map is a few days old but seemed enlightening anyway.) There’s clearly state effects here, with Florida, Arkansas, Louisiana and Missouri doing better than similar areas slightly across the border. The map mostly corresponds closely to where there are the most cases, so people are responding to what is going on around them.


I don’t know the answer to either half of this question. The first half is whether they actually do go out and get someone vaccinated – I’m guessing they probably do, since no one piped up to say they didn’t and I don’t see why not, but that’s a very weak guess. The question is whether this increases supply or only redirects supply (and if it redirects, whether it does so from where it would be wasted entirely, or not).
I’ve tried at various points to figure out what the true supply constraints are, and to what extent ‘pay more money’ causes there to be more vaccine doses. There have been a lot of claims about various bottlenecks. I continue to believe that money is indeed a medium-term constraint on supply of Covid-19 vaccines, and I strongly believe that expectations of payment for such vaccines are a strong long-term constraint both on this vaccine and on other similar creations in the future.
So at a minimum, the general action of doing things such as this, which at least do bid up the price, seems like a good use of funds. Not as good as ‘fund manufacturing capacity when it matters most’ but still better than most uses of funds.
I’d also note my continued frustration with calculations on whether interventions, including vaccine efforts, are worthwhile that frame it entirely in terms of dollars per life saved. Then count only the directly saved lives. That is one good metric to track, but it is far from the whole story of the benefits of such efforts, which in such cases I believe point almost entirely in one direction. In our haste to quantify effects and rely on multiplication, it is important not to count only that which we can explicitly measure and directly observe.
It looks like we have even more support for vaccine mix and matching being not only effective, but more effective than the best vaccine on its own (paper).
What some of us are curious about is what happens if you go in the other order, and do AZ last, especially AZ as the third shot, because many of us are in the position of having had two mRNA shots. If we can take a cheap second or third shot with less short term side effects and get better protection that way, we’d like to know. But I anticipate we may never know about this, because once mRNA shots get thought of as ‘better’ it’s impossible to run the experiment ‘ethically.’
A theme this week, as we’ll see with the CDC’s new data, is that when you ban good data collection, you end up obsessing over what little data collection you happened to be able to do instead.
Also, it would be nice if we didn’t let mRNA vaccines expire unused, which it seems we are about to do in some states. Likely worth being louder about this but don’t know how to do so productively. Oh, and the way this was presented implies that the only reason they’re ‘expiring’ is that they technically have a ‘shelf life’ that’s running out and all we have to do is change that number, the shots themselves are totally fine.
Vaccine Approval
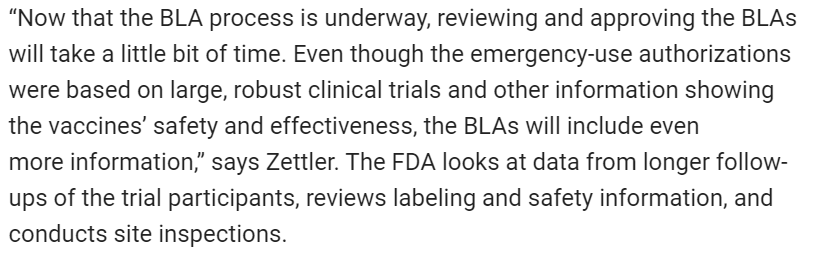
The FDA still has not fully approved the Covid-19 vaccines. Why?
They required a ton of data and paperwork, which they need to carefully work through despite knowing all the conclusions already, and they didn’t feel like putting ‘all hands on deck’ to do this busywork until a few days ago.
As Alex Tabarrok puts it, Welcome to the Club. This is what the FDA always does. It doesn’t consider the evidence in front of its face, imposes requirements that lead to applications too heavy to lift, then takes its sweet time evaluating those applications, while it continues to not give permission and thus while people needlessly die. That’s standard operating procedure.
For Covid vaccines, we have had the biggest Phase IV trial in the history of the world. The vaccines are clearly safe and effective. They are sufficiently safe and effective that we are mandating the vaccines wherever we can, there are huge public campaigns to increase vaccination rates, and those who refuse the vaccine are being painted by all Responsible Sources and Very Serious People as some mix of irresponsible, stupid, selfish and victims of a con, among other similar things.
So in this particular case, things grew sufficiently egregious that increasing numbers of people, including increasingly some of the Very Serious People (e.g. Eric Topol), pointed out the situation.
This is good.
Ideally it causes people to recognize that the problem is the standard operating procedure in the general case, rather than the particular issue in this specific case, but at a minimum this does seem to be speeding up the process.
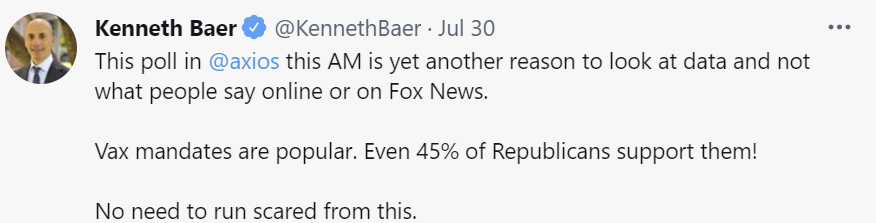
You see, the FDA finally got on the case (WaPo)!


Note the future tense on that, dated June 30.
Previously, at most some hands were on deck, but soon all hands will be on deck, or at least more hands will be on deck than one would otherwise expect. Regardless of where all those hands were previously and how light they make the work, this is excellent news. So, given all hands on deck and overwhelming evidence of both safety and efficacy, how long is this going to take?
Don’t worry, it’s much faster than normal. Here’s when it started:

The application process was sufficiently onerous, and/or required sufficiently robust data, slash didn’t feel sufficiently urgent to Pfizer, such that Pfizer didn’t submit until May 7. It can be debated how much of that part of the delay is on the FDA, versus how much is on Pfizer, or on Moderna who waited until June 1.
It has now been two months since Moderna submitted, and three months since Pfizer submitted. All hands are on deck, we are going ‘much faster than normal’ yet we are still not done. Think about what this means for normal.
It is good to see acknowledgement that the FDA’s job is risk management, and that they should consider the potential upside of speeding up their actions, which is the same as considering the downsides of slowing down their actions, versus a reasonable baseline of ‘approve this yesterday because obviously.’ This then is, presumably, the best they can do. And Biden won’t interfere to speed things up, presumably because that would not be ‘following the science’ or what not.
The FDA also still hasn’t given its approval for mRNA booster shot follow ups to the J&J shot, despite it being quite overdetermined that this is a good idea, forcing this to go ahead without them and without proper record keeping, likely resulting in a bunch of bad record keeping and also slowing this down quite a lot.
There also are not any officially approved tests for Covid-19, either, although that does not seem to bother people in the same way so it is not an urgent matter. The failure to authorize much better and cheaper testing is urgent, but that’s been true for over a year, and I’ve given up on that.
Bloomberg breaks it down like this in their newsletter, which reiterates the basic facts but is even more skeptical of the outcome and is somehow trying to justify the delays:
There were reports of the hope that this will happen in the Fall, which means some time before December.

Getting the approval in December would be almost completely too late. At that point, if we were going to have another Delta wave, it would be far too late for new vaccinations to have much impact on it, and either the extra vaccinations won’t be necessary, or else essentially everyone would already have antibodies.
The good news is that after this happened, the timeline seems to have moved up:
It turns out that putting all hands on deck actually matters, and concluding things you already knew isn’t all that hard after all.
What about fears that this will ‘further undermine confidence’ or look ‘rushed?’ I estimate those costs at exactly zero, versus the benefits of getting rid of the quite valid and successful ‘the vaccines are not approved’ argument. If you tell a regular person ‘no, the FDA needed six months to review the application properly and they rushed it and finished in three’ I do not expect such arguments to get much traction.
Regardless of how many more weeks or months we must wait, these delays are unacceptable, and entirely unnecessary. Authorize these vaccines today, and demand resignations as needed to make that happen.
Vaccine Mandates
Last week, I got a surprising (to me, anyway) amount of very forceful pushback from commentators on how authoritarian it was to make association with people dependent on them not being likely to become sick and to make those around them sick, or to require those who choose to not reduce that risk to mitigate the resulting risk to others at their own expense. I disagree with this assessment, and have said my peace on the matter. Others are welcome to continue talking about it, if desired.
This is a pretty big new mandate, and the most coercive since you’re not allowed to quit the military, but also the kind of thing you sign up for when you join:

Previously, there was a survey asking vaccine hesitant troops why they were refusing the vaccine. In addition to the usual responses, one of them was ‘I never get to tell the army no, and now I can.’ That highlighted how weird it was that there wasn’t a mandate in place already, which was due mostly to the vaccine still being on emergency use authorization. Which is not the way I model a military capable of winning wars responding to this situation.
We also picked up Disney and to some extent Walmart (WaPo).

Importantly, we also picked up Tyson Foods. Meat packing is an important bottleneck that caused supply chain problems back in early 2020, and is also an environment almost built to spread Covid-19.
New York City has mandated vaccinations for indoor dining and gyms.
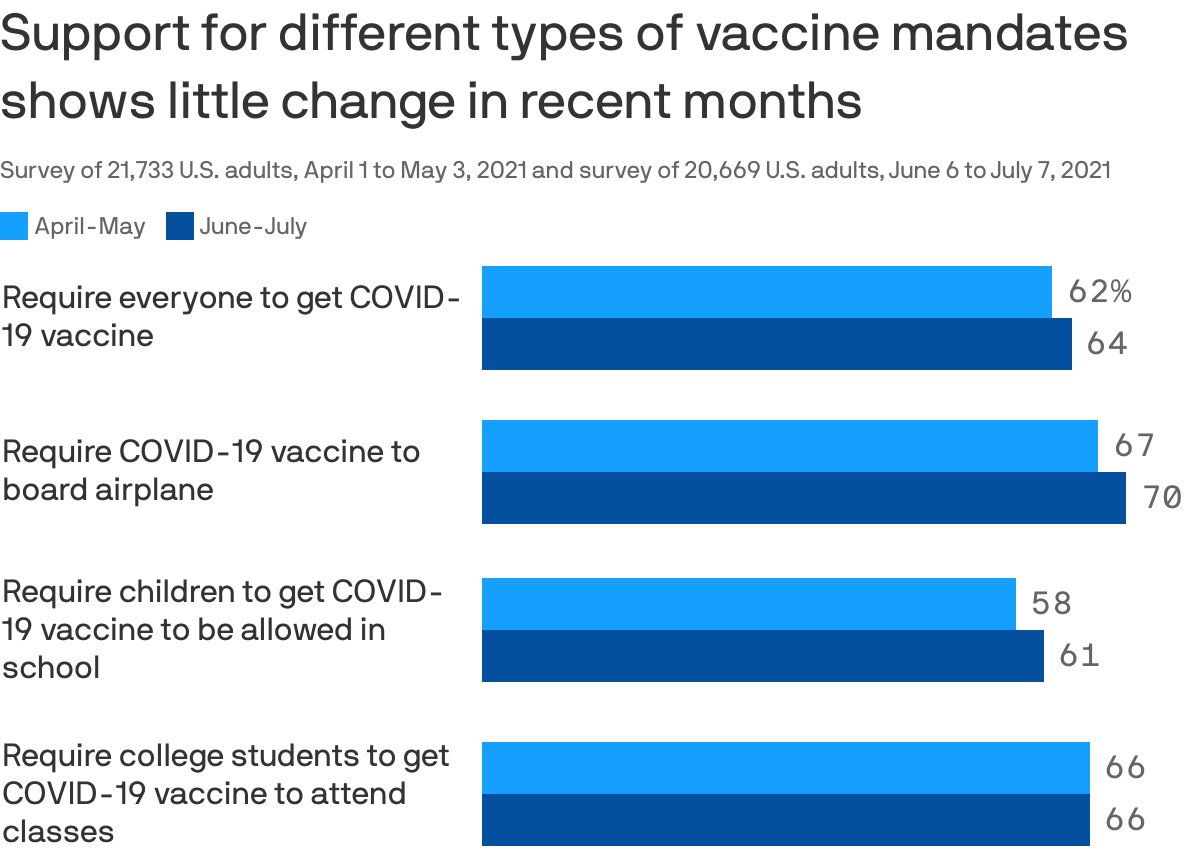
It turns out that much more coercive vaccine mandates are widely popular (original post, survey):
Here are some crosstabs:

And by region, note that only the Dakotas and Wyoming are under 50% (and even they are over 50% for the airplane question):

The mandates we are actually discussing and implementing are ‘if you want this job where you interact with people in person you need to be vaccinated’ which I’d put at somewhat less coercive than even requiring vaccination to board an airplane, which now has 70% support.
One thing I find most interesting about this survey are the relative support numbers. Requiring everyone to be vaccinated is more popular than requiring vaccinations for school, where children are already required to get vaccinated for any number of other things. It makes sense that college student requirements would be more popular than either of those, and that the airplane requirement is more popular still since it puts people into close quarters with random other people, and also because people don’t understand how good ventilation is on airplanes.
What is more striking than the order is the small size of the gaps here. It doesn’t matter much what the scope or target of the mandate is, something like 90% of people are either for all the mandates or against all the mandates.
One can also compare these numbers to the adult vaccination rates. 64% of respondents favored requiring everyone to get vaccinated. Approximately 68% of adults are at least partially vaccinated. And 70% favor requiring vaccinations for air travel, a higher percentage than are vaccinated themselves.
The crosstab they didn’t list, but I very much want to see, is how much those groups correspond. How many people are unvaccinated but think it should be mandatory? How many are vaccinated, but think it shouldn’t be? To me this seems like the most important crosstab, and also the thing most important to control for here. I want to see if their percent vaccinated matches the population’s number, including by region.
Regardless of that, it sure looks like Americans don’t only not draw much distinction between types of mandate. They don’t even draw much of a distinction between their personal choice to get vaccinated, and a full vaccination mandate!
This is a general problem, where people fail in practice to draw much of a distinction between “Yay X” and “X is mandatory.” If X is a yay, send in the men with guns and ensure X happens. Or more commonly, “Boo X” and “X is forbidden.”
There are some people who are very, very against vaccination mandates of all kinds, but they are very much in the minority.
Noticing and caring (correctly) that mandates have a much higher burden of proof than ‘the thing is typically a good idea’ puts one in a much smaller minority even than that.
Also from the survey:

I hate the ambiguity in the wording here but I presume it means about 20-30% of respondents are in those hard-to-get categories, which leaves 70-80% who aren’t.
In other news, let’s ask what everyone really cares about. Covid-19. Who to blame?
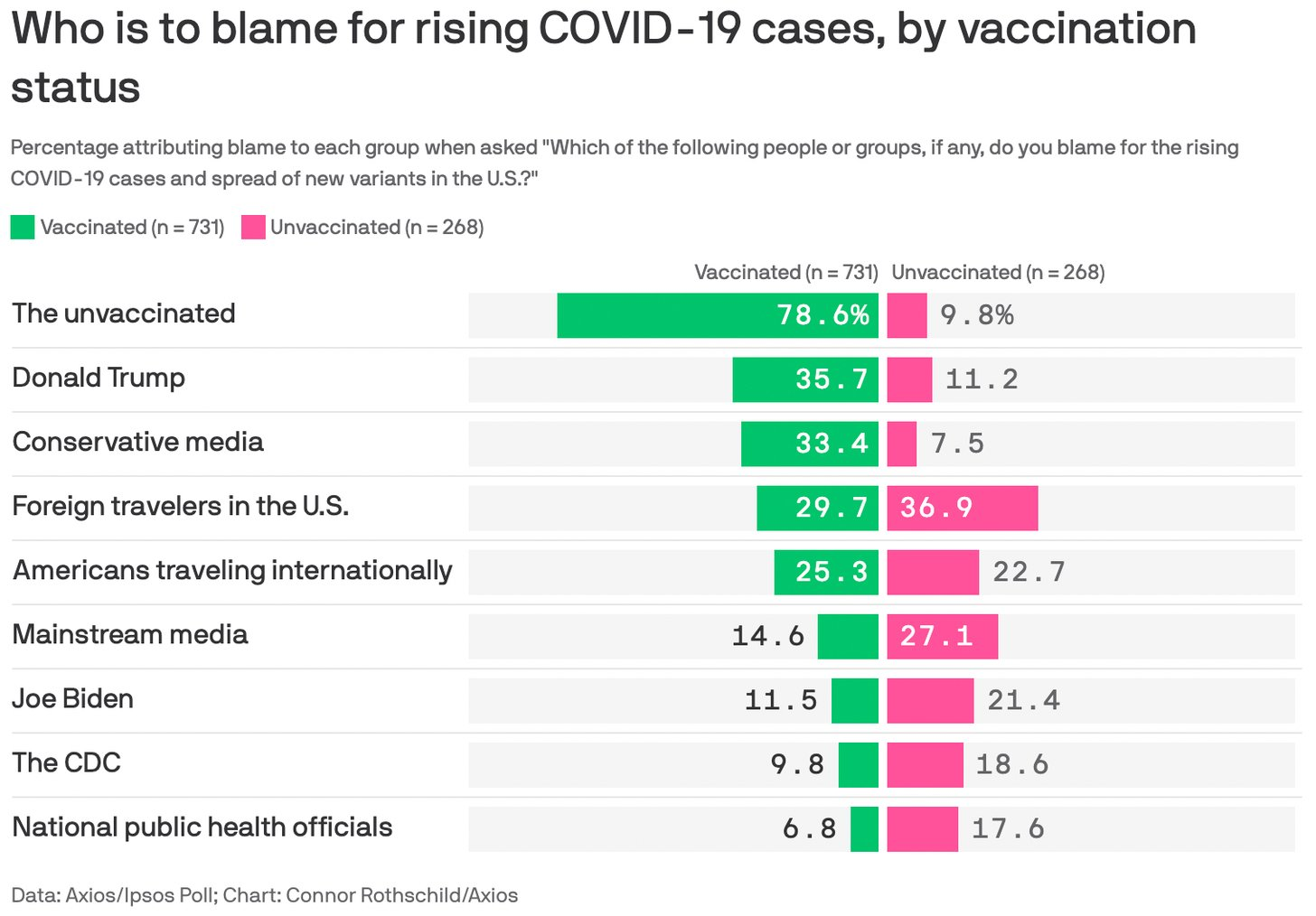
A hidden point of data here is that 73.1% of people responding are vaccinated, which (given an adult vaccination rate at the time of just under 70%) gives us an estimate of how biased survey responses are likely to be.
Mask and Testing Mandates
LA’s positive test rate will be going down soon. Every child (and teacher) in an LA United school will need to get tested weekly, even if vaccinated.
In New York, and in many other places, the teachers’ union is strongly opposed to this, with any testing of the unvaccinated to be covered fully at taxpayer expense, while they previously insisted on keeping schools closed until teachers could get vaccinated no matter the case level, which is a hint as to what game they are playing to win.
It’s not like it’s a handful of holdouts, either…
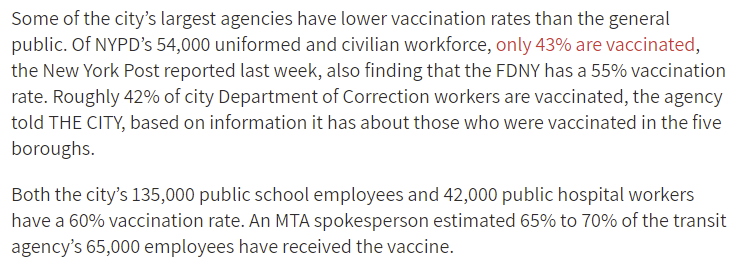
These numbers are much lower than the adult population’s vaccination rate in the area. It’s mind boggling that 40% of teachers in NYC schools remain unvaccinated. This is the group charged with ‘educating’ our children? Union can’t allow teachers in classrooms until they’ve been vaccinated, then almost half of them refuse to get vaccinated. We’ve made a huge mistake.
I realize it’s impossible for multiple reasons, but my preferred scheme would be not only to mandate vaccinations going forward, but take this opportunity to start over and fire every teacher not currently vaccinated as not qualified to teach anything to children, and go from there.
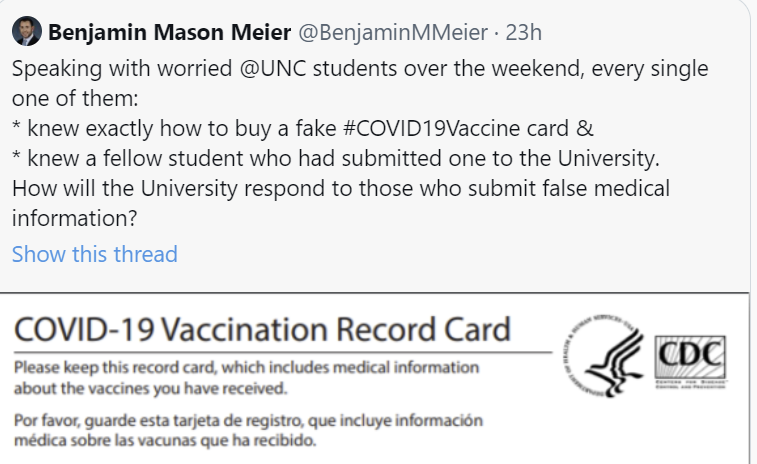

So our current standard is that we don’t require the vaccination, lots of students lie about it anyway in case that changes, and if we don’t explicitly get them to affirm that their statements are true then we can’t hold them accountable even if we find out they were lying? Sounds about right. Academic standards are not what they used to be.
Vaccine Hesitancy
Who is vaccine hesitant? Some data.
I find it interesting (for non-Covid reasons) that everything here lists both the positive and negative effects, except when females are less likely to be vaccinated, and then it’s only the positive effect. The argument that the two are mirrors of each other is not one the source would likely be happy to be quoted on in this day and age, given its implications.
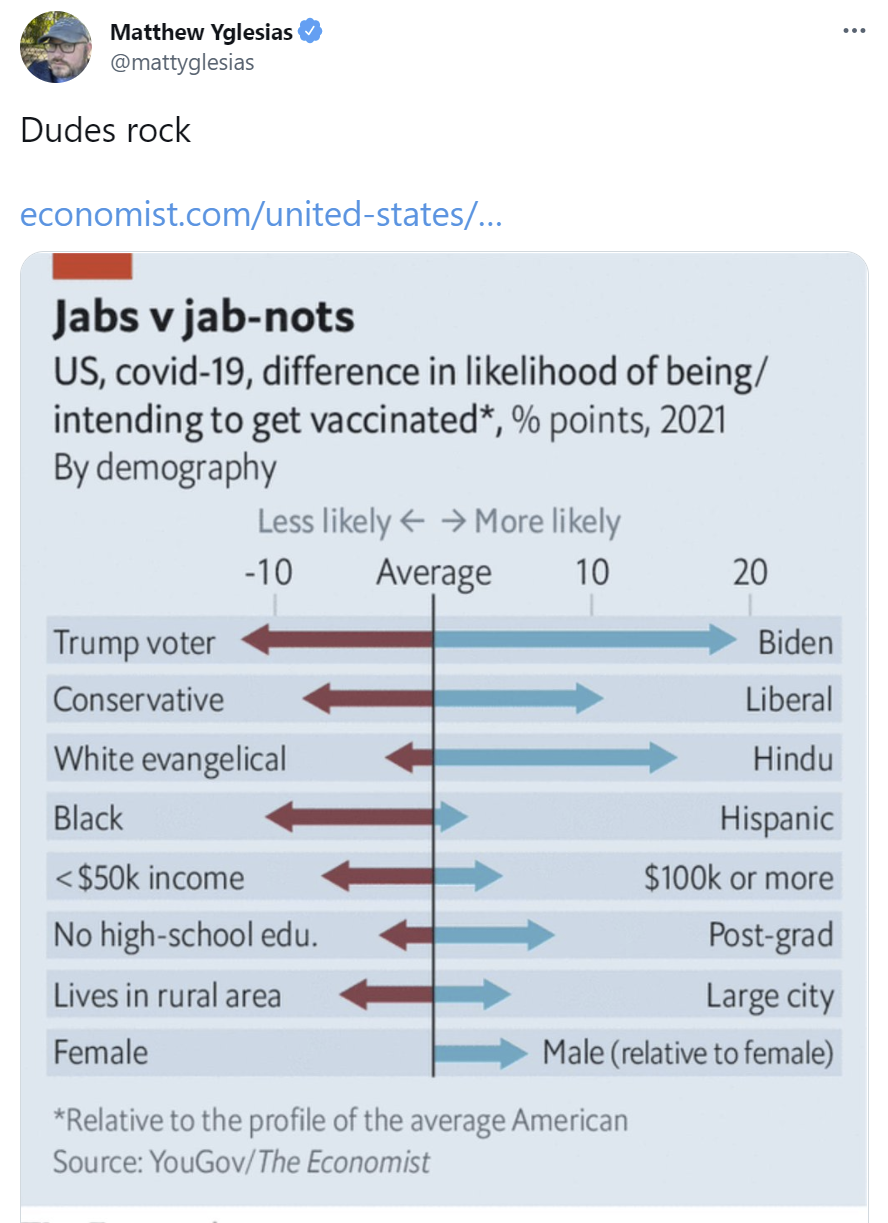
Especially since it seems like dudes intend to rock but in fact keep putting off their rocking until a future date (link to data):

(Reminds me a little of this graph about which animals people think they can beat in a fight, which was covered as ‘men think crazy things’ but that’s not how I read the actual numbers).
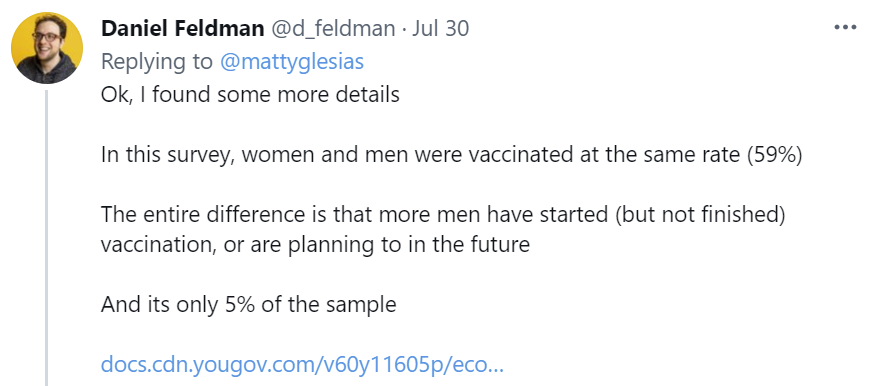
From the replies, another chart:
There are some contradictions between the data sets, but mostly they tell similar stories. I also like the ‘only if required’ category because it puts a reasonable estimate slash lower bound on the benefits of a requirement, which would be the vaccination of 6% of adults or 18% of non-vaccinated adults.
Samo Burja argues that one side was always going to be anti-vax while the other was pro, so we should be thankful it’s blue America that was pro rather than the other way around. If one has to choose, giving whoever controls the media the right position does seem better, so the question is whether he’s right that we had to choose. I don’t think this is obvious – one side may be coming out against motherhood but we can draw hope from the fact that we still have broad support for apple pie.
Andrew Yang may not be a successful candidate, but he will forever live on in our hearts both for wearing a ‘math’ pin and as the ‘pay people money’ guy:

How about vaccine lotteries, do those work? Yep, those work.
New York’s combination of new requirements and new incentives? Yep, those work.
How about requiring the vaccine in order to fly? Yep, incentives matter again. We don’t have magnitude here, so unfortunately this doesn’t provide that good a natural experiment on how much people value the ability to fly. But I don’t think that’s even the second most interesting thing here, despite being what I noticed being called out…
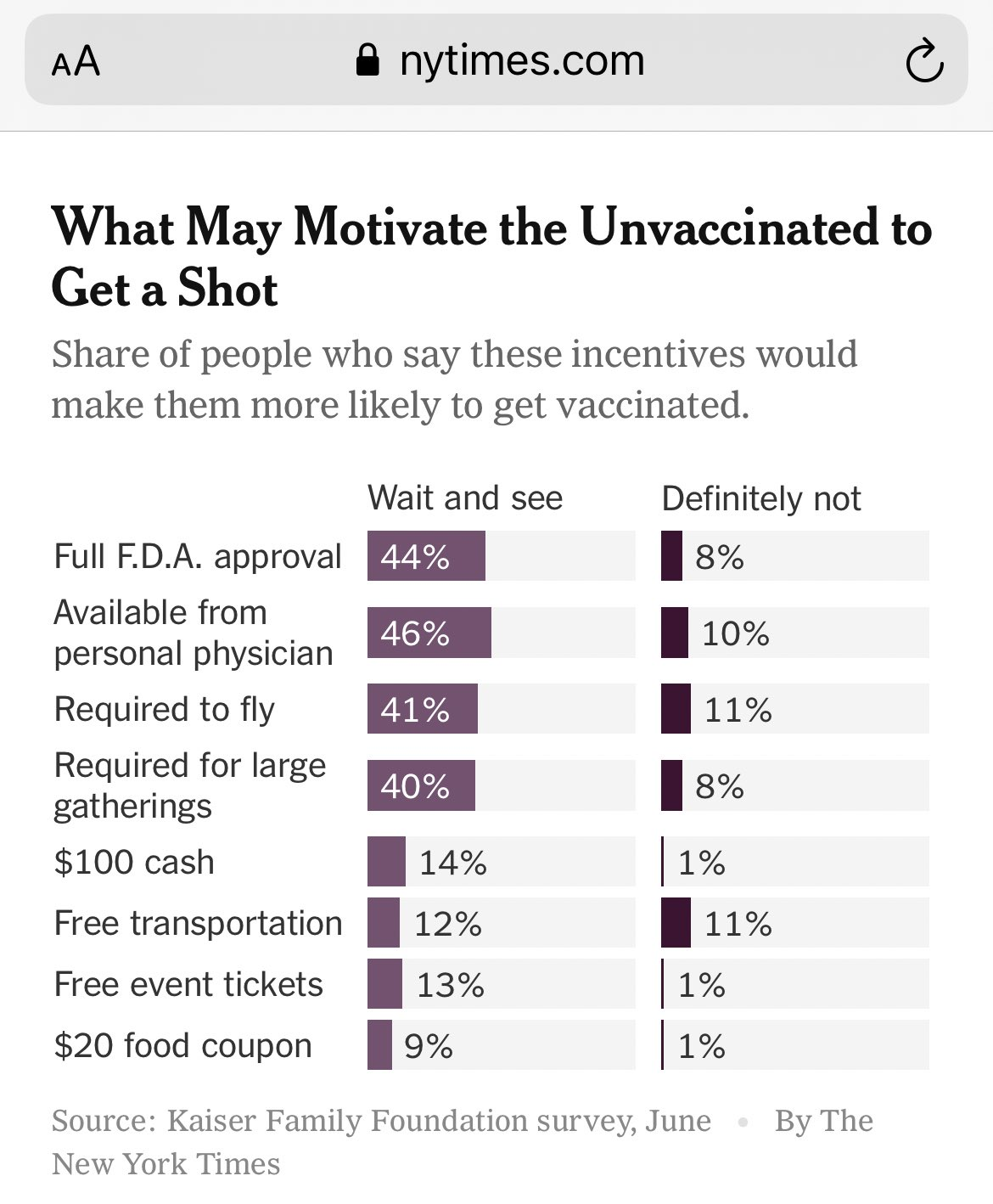
There’s the top four all which are big, and the bottom four which are small but meaningful, although ‘more likely’ is a far cry from ‘turns a no into a yes.’
The big two are the first two, because they’re both not coercive and they’re free. Full F.D.A. approval would be helpful for fully half the remaining people. Getting the vaccine to personal physicians, which also should have happened a long time ago many times over, also helps with half of people.
Combine those two, and my guess is you pick up a large percentage of the remaining ‘gettable’ people, no coercion required. That doesn’t mean the $100 cash wouldn’t help, I’d throw that in too, but notice that the $20 food coupon (worth less than $20!) gets you more than halfway there at a fifth of the price. That makes sense, the marginal demand curve should slope downward here, and I’m still happy to pay the marginal costs to bump the payment to $100, especially since it would mostly go to poorer people anyway.
One concern is that all these ‘rewards’ might make people hold out next time to try and get the rewards. Again, people respond to incentives. The good news here is my model does not think this much matters. Yes, some people would move from taking the early free option to holding out for the bribe, but mostly that delays people during the period when demand exceeds supply, and hence no bribes are on offer. So it’s good, actually. If in March, everyone knew that anyone would get $100 for being vaccinated starting in April then that’s a way of allocating scarce resources by price without everyone losing their heads over it. Sounds good to me. So what if you end up having to bribe some people who would have gotten it for free?
Also, a gentle reminder that incentives matter in all directions, and sometimes mistakes get made…

If you think lying to say you’re vaccinated is easy, lying to say you’re not vaccinated is even easier, as long as you’re willing to endure the things people say to those who aren’t vaccinated.
Delta Variant
There are three core messages here.
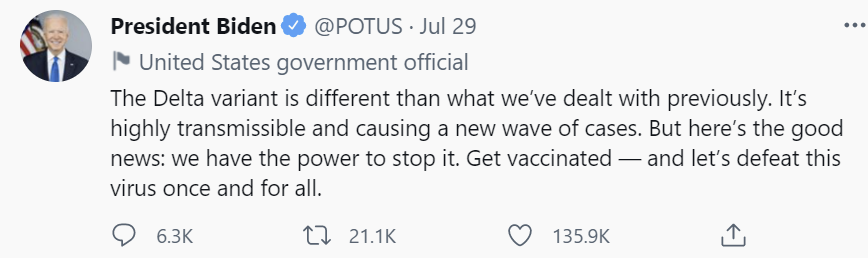
Two of them are that Delta is more transmissible and causing a new wave, and that vaccinations work. Those are true and important.
The third is that we have the power to stop it, and defeat the virus once and for all.
That one seems to me to be false, at least for meaningful definitions of ‘we’ and ‘have the power to stop it,’ and especially ‘once and for all.’
Yes, at some point, likely not that long from now, things will turn around the way they did in India, the UK and the Netherlands, once we’ve had enough time for the control system to adjust and for enough people to be infected and/or vaccinated. That won’t be the end of Covid, and it won’t count as having stopped it, so much as having gotten through it.
The important thing is that the ship has almost entirely sailed. We’d prefer to get more vaccinations and otherwise improve things on the margin, but over the range of mask mandates and other new countermeasures, are we going to change what happens much from here? If we did, are we going to be willing to keep those countermeasures online indefinitely? Are we going to be willing to mandate vaccinations and if necessary booster shots sufficiently effectively to get paid off for buying all that time?
It seems like the answer is clearly no. That doesn’t mean it’s senseless to take reasonable precautions on the margin, but this is mostly only a battle worth fighting if one can win. If failure is inevitable, and we’ve mostly gotten as many vulnerable people vaccinated as we’re going to get, it would be better to fail fast.
That is a central fact to keep in mind when looking at the new mask mandates and other updates coming out of the CDC and elsewhere. Preventive measures make sense when they are necessary to control spread, and also sufficient to have worthwhile benefits. The window available is not impossibly narrow, but it is not infinitely wide either. And in the possible (or at least theoretically possible) worlds in which vaccinated individuals are at great risk of infecting others, I don’t see how we could hit the window.
Also, before we discuss the CDC’s new mask mandate and its justifications, a reminder that if you institute a mask mandate, it’s important to follow that exact mandate yourself.
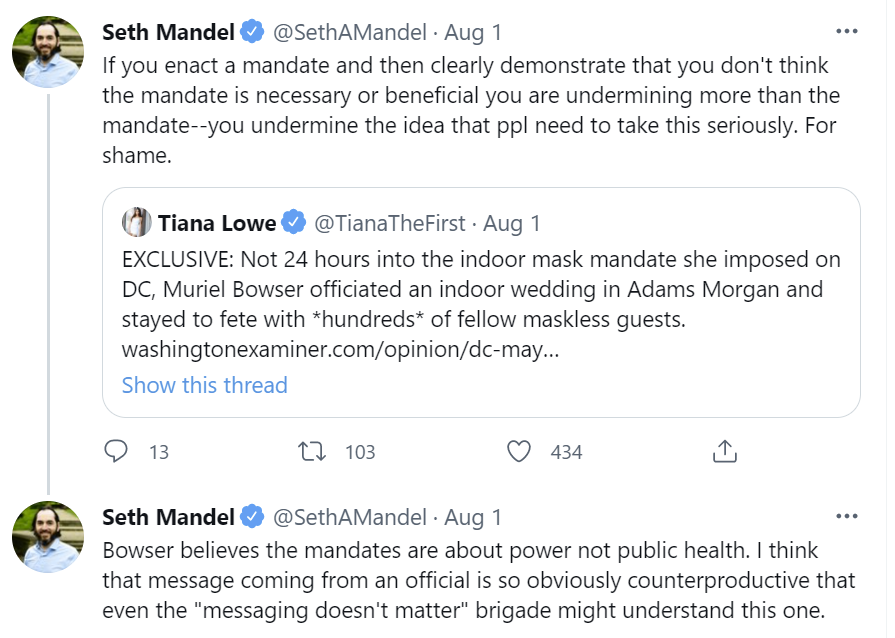
And even if you do sometimes violate the rules you’re telling everyone else to follow, you definitely shouldn’t be explicitly exempting yourself from those rules.
Similarly, there are also reports that Pelosi has violated the house mask mandate on at least three occasions, in addition to all the Republicans who are violating it to own the libs.
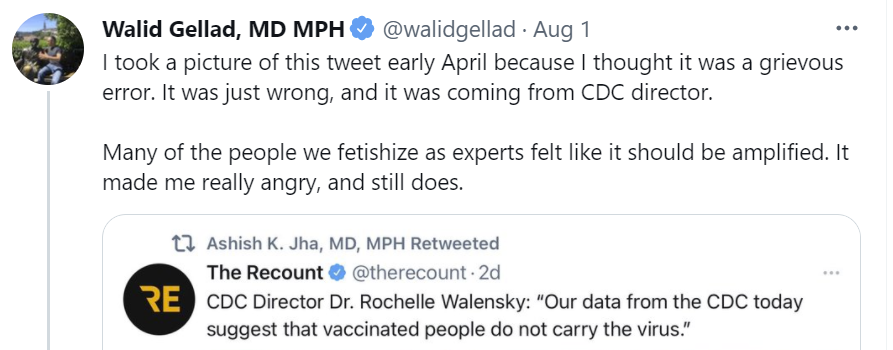
The CDC Reinstates Its Mask Mandates
Point: When the facts change, I change my mind. What do you do, sir?
The political strategy of ‘flat out deny saying the thing you said when the video cameras were rolling’ has its disadvantages, such as the media usually having easy access to what was being filmed by those video cameras. I understand it when your brand is going to be ‘I lie all the time, what are you going to do about it?’ but that’s very much a pro-malarkey stance.
One refinement is where you don’t quite say the thing explicitly, and can sort of claim that you only said it implicitly, as is the case here. Fooling people on such things tends to be infrequent, but it does enforce that you have the power to decide what you did and did not say retroactively, and thus your alignment with the destruction of the public record. So I suppose there are some strategic advantages.
In any case, the term ‘forever’ and the term ‘at the time’ are not close friends, and Delta has been known since well before the statements about taking off one’s mask forever. Did the situation change? Yes. Is the situation worse than would have been reasonably anticipated? I think yes, the developments of the past two months have been worse than expected. But, well, yeah. Imagine it flipped.
That’s distinct from the question of whether reinstating these mask requirements makes physical sense. If it turns out the messaging earlier was a mistake, I’d prefer owning the mistake to pretending a mistake wasn’t made, but it’s still better not to keep the mistake running – if it was indeed a mistake.
So, what facts changed that perhaps should change minds? Why are they suddenly saying things like this?

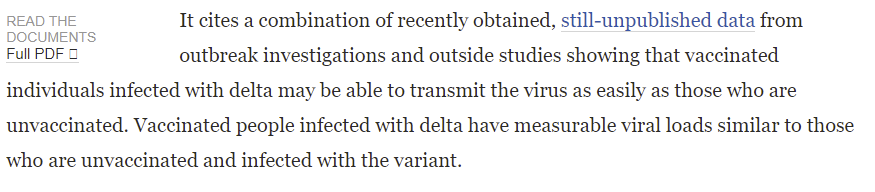

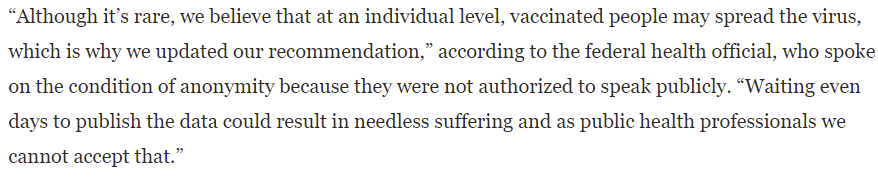
They waited days to publish the data. The CDC initially did the infuriating thing of refusing to release their data, which even the mainstream media like WaPo pointed out was terrible but they did then release the data, and we have it now.
One theory on what might be causing this.
Which results in completely false things like this:

And also various news reports like this, which seem like the point – get people scared before they can analyze the data.

To go with the general trend of, well, this:
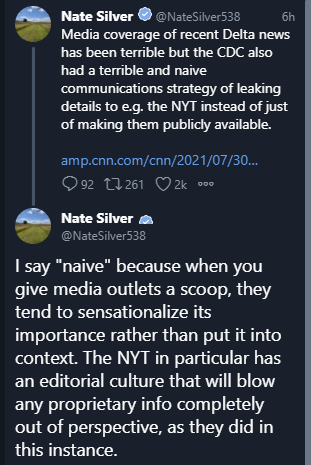
The first half of this isn’t fully true, but it’s way too true

Another communications problem:

It’s tricky when you both want to tell people how great the vaccine is and promise how people can return to their normal lives with no worries whatsoever, to get them to take the vaccine, and then also turn around and lie about how ineffective the vaccine is in order to scare them into not changing their behavior afterwards. It’s even harder doing both simultaneously. Everyone involved gets whiplash. I almost sympathize.
The CDC’s new mask mandate is in areas with sufficient spread, which means it’s constantly expanding in scope each day in ways that are completely inevitable, so it would have been better to bite the bullet for everyone at the same time:

To make it easy to find, analysis of the study itself gets its own section.
The Provincetown Study
For those not looking to get into the weeds, this was an outlier situation, there were tons of base rate errors that the study makes no attempt to correct for, we learned very little, and mostly the CDC is making a big deal over all this for no good reason.
For those who want to dive into the weeds here, let’s get to it.

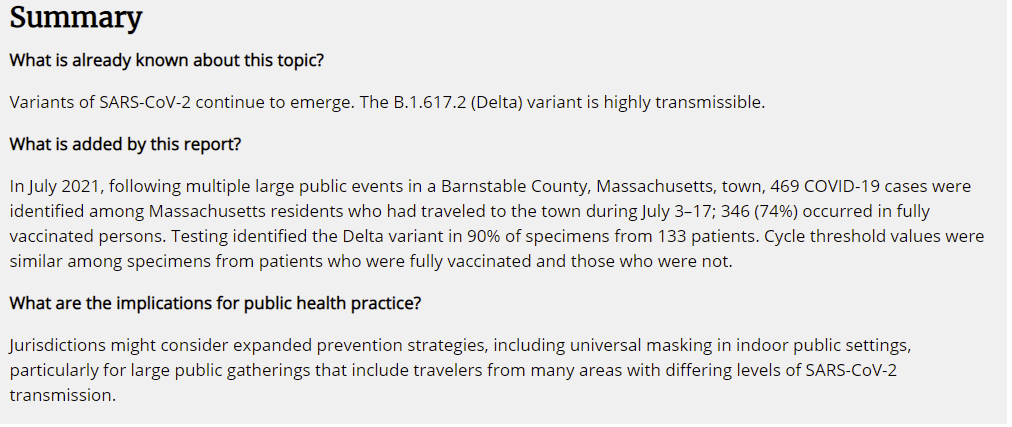
So the headline findings are claimed to be (1) among cases that could be identified, vaccinated and unvaccinated people had similar cycle threshold values (and by implication, perhaps had similar ability to spread the virus) and (2) 74% of cases occurred in fully vaccinated persons, versus 69% vaccination coverage for the area.
The suggestion to reimplement restrictions is standard issue, but I note here that if vaccines were sufficiently ineffective in practice against Delta, there would be no reasonable way to stop the pandemic, and I’d want to do the opposite of the implications listed here and stop trying.
Most vaccinated patients were symptomatic:

Four of five hospitalized patients were fully vaccinated. None of them died.
“A cluster-associated case was defined as receipt of a positive SARS-CoV-2 test (nucleic acid amplification or antigen) result ≤14 days after travel to or residence in the town in Barnstable County since July 3.”

So it’s all Delta, and 74% of identified cases were symptomatic, including 79% of vaccinated cases, with the usual mix of symptoms.
…and that’s pretty much it.
Here is the bulk of their #analysis:
“The findings in this report are subject to at least four limitations. First, data from this report are insufficient to draw conclusions about the effectiveness of COVID-19 vaccines against SARS-CoV-2, including the Delta variant, during this outbreak. As population-level vaccination coverage increases, vaccinated persons are likely to represent a larger proportion of COVID-19 cases. Second, asymptomatic breakthrough infections might be underrepresented because of detection bias. Third, demographics of cases likely reflect those of attendees at the public gatherings, as events were marketed to adult male participants; further study is underway to identify other population characteristics among cases, such as additional demographic characteristics and underlying health conditions including immunocompromising conditions.*** MA DPH, CDC, and affected jurisdictions are collaborating in this response; MA DPH is conducting additional case investigations, obtaining samples for genomic sequencing, and linking case information with laboratory data and vaccination history. Finally, Ct values obtained with SARS-CoV-2 qualitative RT-PCR diagnostic tests might provide a crude correlation to the amount of virus present in a sample and can also be affected by factors other than viral load.††† Although the assay used in this investigation was not validated to provide quantitative results, there was no significant difference between the Ct values of samples collected from breakthrough cases and the other cases. This might mean that the viral load of vaccinated and unvaccinated persons infected with SARS-CoV-2 is also similar. However, microbiological studies are required to confirm these findings.”
That’s what the CDC updated on? This is what’s causing a chorus of “Vaccinated people may spread Covid as much as unvaccinated people”? That’s it?
All right, so what’s actually going on here in this study?
I’m not going to go full Not Necessarily the News, but it’s remarkably tempting, because the sample is clearly nothing like a normal one.
The first big hint is that this took place during a series of gatherings, mostly of men, and that most of the infections were of men so it’s clear that this happened mostly among those attending the gatherings rather than the background population.
The second even bigger hint is that the numbers look absolutely nothing like the numbers we observe in the general population, on several measures.
The infected population is mostly male, and of course it was mostly travelling and engaging in unusually high risk activities and almost certainly stuck in a superspreader event.
Most cases (74%) were symptomatic, which isn’t normal when looking carefully for cases.
Most cases (74% again) were in vaccinated people, which was higher than the population percentage that was vaccinated in the surrounding area. We know vaccines are effective at preventing Covid-19 and at preventing symptomatic Covid-19, and even if they’re not as effective as we think, less than zero is not on the table here, ‘cmon.
Vaccinated cases were more likely to be symptomatic than non-vaccinated cases, which we also know isn’t normal, on top of there being more such cases than the population baseline.
The Ct values in vaccinated patients were as high as those in unvaccinated patients, which was one of the banner headlines in the scare tactic articles, but viral loads themselves were not measured, and again we know that infections in the vaccinated are less severe.
So there are essentially two ways to interpret this data.
Method number one is to become The Man of One Study, think that vaccines suddenly have entirely stopped working, ignore all the other overwhelming evidence to the contrary that’s actually everywhere – even the anti-vax crowd mostly admits the vaccines work – and then reason from there. You could argue that it magically permits full infection and transmission and hospitalization but still prevents death since there were no deaths in this sample, but that doesn’t actually make any physical sense.
Of course, none of the rest of that scenario makes any physical sense either. Wrong Conclusions Are Wrong, and taking the results of this study at face value flies in the face of the whole vaccinated people not getting Covid, not getting sick from Covid and not dying from Covid phenomenon that has very much persisted under Delta.
I didn’t quite explicitly Defy the Data [LW · GW] on the Israeli vaccine effectiveness measurements, but I did point out the data didn’t make any sense even internally and that they really, really didn’t make sense versus observed population data elsewhere, and that the ‘these vaccinations were older’ explanation wasn’t actually going to fly. Whereas the 88% effectiveness number out of the UK made me sad, but was also plausible, made sense and could live in the same physical world we observe, so I took it far more seriously.
That’s a roundabout way of saying that taking the study’s data is, when taken at face value, Obvious Nonsense, and thus we will be using method number two.
Method number two is to ask what could have caused the study to get these answers that on their face are Obvious Nonsense, realize that this has everything to do with base rate fallacy and the failure to apply Bayes’ theorem, with mostly vaccinated people attending the gatherings, and the pattern whereby infections are identified and tracked missing asymptomatic infections en masse which are concentrated among the vaccinated, and vaccinated people being more likely to get tested, and so on, in some combination.
This thread looks at the basics under method two, points out how much worse things would have been in Provincetown without vaccines, and concludes the study doesn’t tell us much.
Twitter was in general top form, here is a small sample.








Oh, and what kind of event was it that had this many men and so many infections? Well, as it turns out…



The cohort being 85% male makes it clear that the virus did not spread to the area’s general population much, and stayed focused on the people who travelled there largely in order to have sex. Which is a reasonably good way to get very exposed to Covid-19. So. Yeah.
The Leaked CDC Slides
The Washington Post got hold of the CDC’s slides. If you can, I encourage you to click through and look at the slides yourself, it’s much easier to read them there, they’re all worth seeing and I can’t be copying over all of them.
The first slide gets off to a great start, with a worthy cause:

Slide two notes that breakthrough cases may reduce public confidence in the vaccines, which is true enough, and I noticed I was pleasantly surprised it didn’t say that news of those breakthroughs was what was reducing confidence.
Then comes slide three, which is a very good data visualization and tells where their heads are actually at with regard to the vaccines.
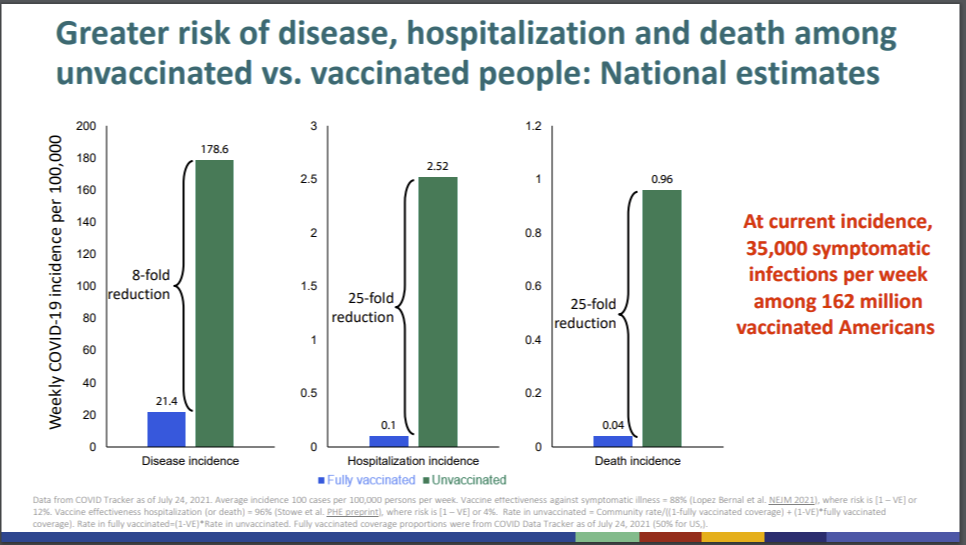
An 8-fold (87%) reduction in incidence, and a 25-fold (96%) reduction in hospitalization and death. That’s exactly in line with all the other estimates. I agree with those numbers, good job. But how has ‘the war changed’?
Slide four shows that a rising percentage of hospitalizations and deaths are among the vaccinated, and explicitly notes this is because of the increase in vaccinations, and the tendency for the most vulnerable to get vaccinated more often. Again, good, but that’s the old war.
Slide 7 shows early vaccine effectiveness, which was quite good:
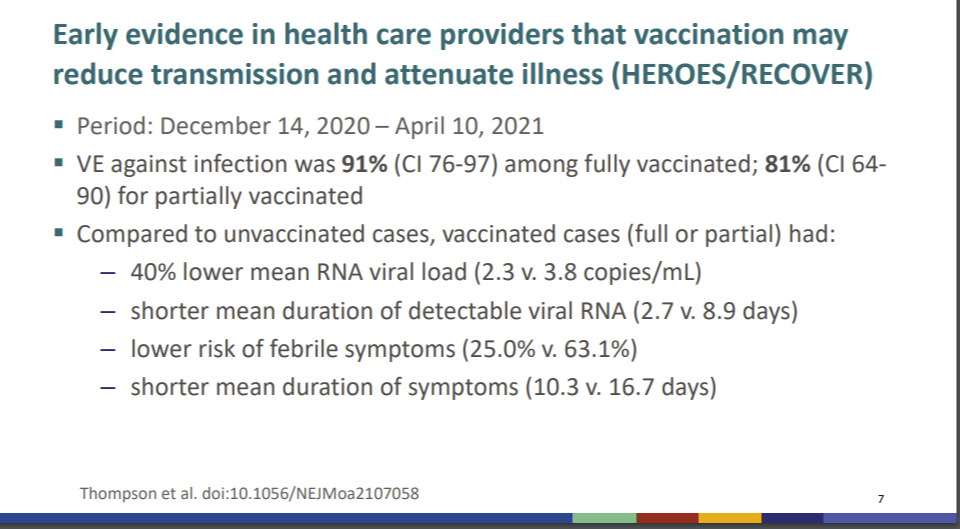
The rest of the pre-Delta section goes into a bunch of other numbers, which all tell similar stories, all of which matches up with what we knew previously. Nothing to report here other than that we’re all on the same page.
This is their big picture understanding of Delta absent vaccinations:

This again is exactly in line with previous estimates, although it has reasonably large error bars. If anything here is different, it’s that this is saying Delta is not much deadlier than the ancestral strain.
Bunch of other as-excepted stuff, then this is the first mention of the new study:
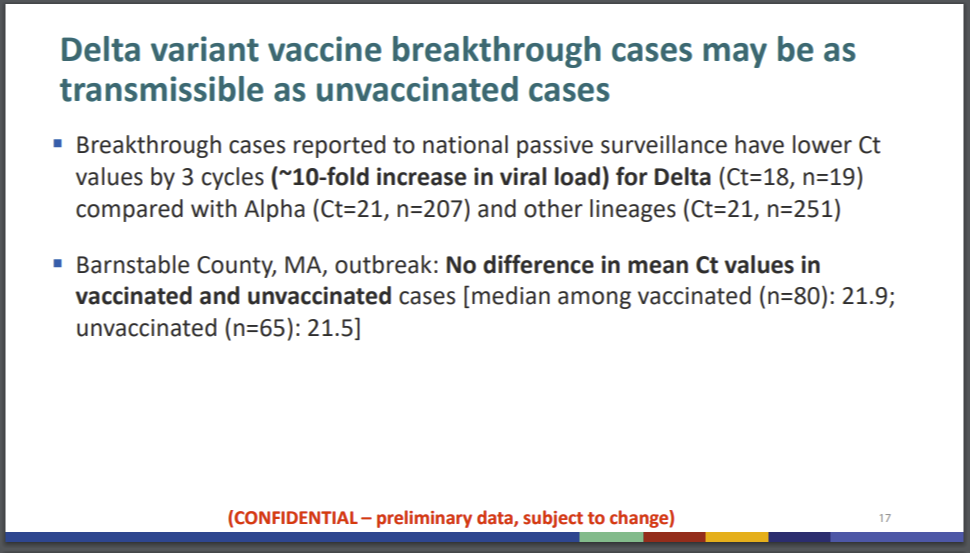
Interestingly not present in the slides are the Ct values for non-breakthrough infections outside of Barnstable County, MA’s outbreak. I find this absence quite odd.
In slide 19 they uncritically report the Israeli data that has been shown to come from faulty statistical methodology (and which never made sense in the first place).
In slide 20 they assume 50% of infections are reported, which seems crazy high, and also model assuming no distancing of any kind which seems like a pure counterfactual. Then, they use the results of that model to conclude the need for ‘universal masking.’ The need for containment without benefit of immunity from infections is left as an unstated assumption.
Slide 22 is their summary:
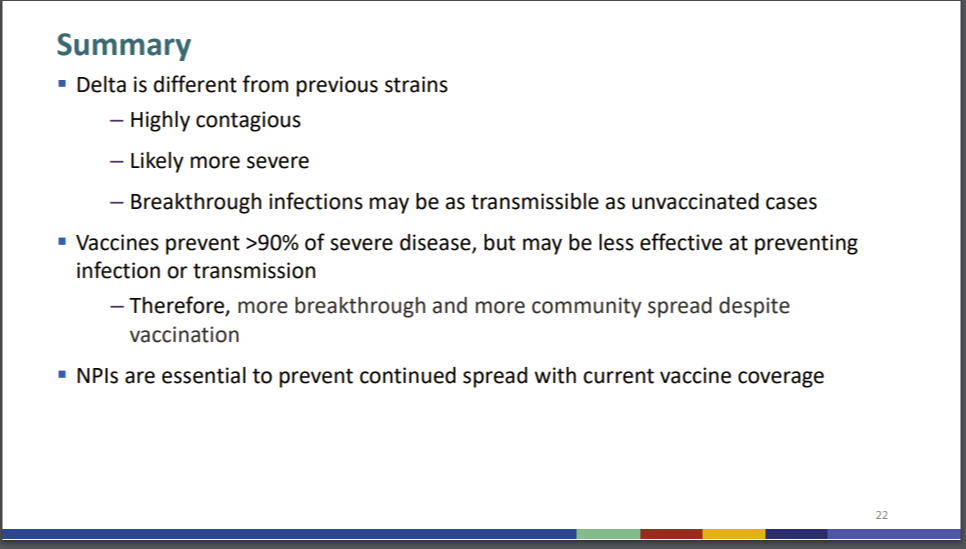
I mean, all right, sure, all of that is true as far as it goes. If you want to prevent continued spread with current vaccine coverage, and no distancing, without waiting for the resulting infections to do the job for you, yes you will at a minimum need a lot of masks.
Finally, recommendations:
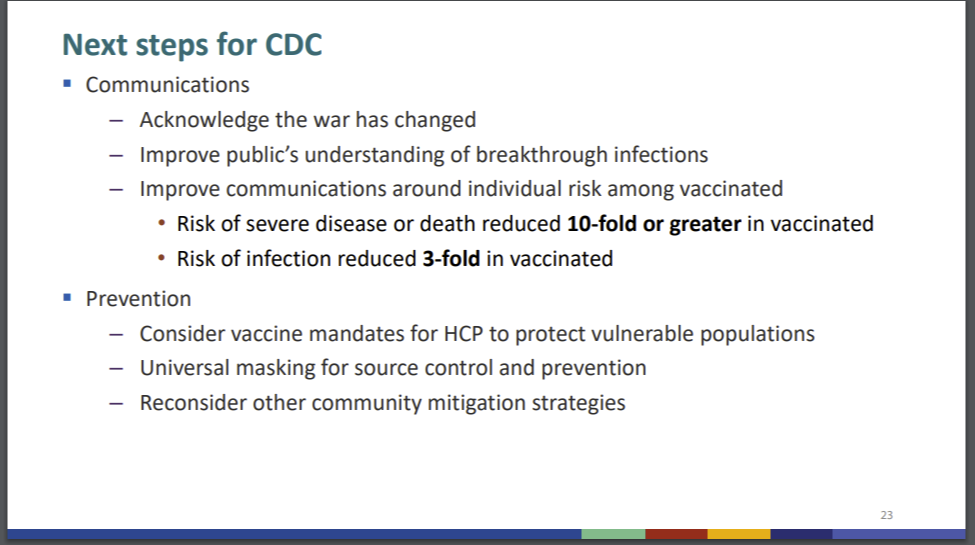
Suddenly they’re going down on this last slide to 75% effectiveness (with a conspicuously missing ‘or greater’ given that it’s there in the previous line), which is not what you’d conclude from their previous slides, but that almost feels like a quibble.
It seems that ‘the war has changed’ here doesn’t mean anything new, it simply means that Delta spreads easier than Alpha at exactly the ratio we previously believed, with exactly the vaccine effectiveness levels we previously believed, except it’s being compared to a hypothetical situation without Delta rather than what should have been fully recognized weeks ago if not earlier. Whoops.
This Chise thread on Twitter makes it clear things are worse than I realized upon first reading. Among other things you’ll find there:



That seems generous, as these are at best kind of evidence of viral loads. Plus even then, the amount of failure to control for any of the things is very much not small.
In case you’re wondering what study Chise is referring to there, here’s a link, it’s the Singapore study (thread / study):
I mean, we mostly knew this already, and the sample sizes here are low, but now Studies Show. So even if the Ct ranges are similar at one point (with the huge error bars, it’s impossible to know), that doesn’t mean what it’s being taken to mean.
About that issue of sample size. In all these studies that show ‘no difference’ the sample sizes are tiny, and the confidence intervals quite large. Here’s the graph from the Provincetown study:

As discussed above, Ct value is not exactly what we want to measure, but even if it was, and even if we ignore all the other problems here, these are very wide error bars. The Wisconsin study has the same problem and also concluded that Ct scores were similar after throwing out any results with sufficiently low Ct scores.
The war has changed thanks to Delta. The war has not changed in the past two weeks. Except insofar as the CDC has decided to change its approach to fighting, taking a maximally dark interpretation of the data rather than offering anything importantly new, in ways that don’t hold up to scrutiny or checks for base rates, and how much that’s going to mess various things up.
The only explanation I can come up with is that previously the CDC had and/or was painting a very wrong picture that vaccinated people were fully immune…
I don’t know to what extent this was what was happening, either intentionally to encourage vaccination and/or unintentionally via misunderstanding the science, and it’s not always possible to make those two distinct. What I do know is that if previously you had the false impression that vaccinated people were completely safe, and then changed your story to vaccinated people being only mostly safe, perhaps that would explain what happened this past week?
Thinking of the Children
There’s a video at the link, he definitely said this, and I’d hope this would illustrate how completely and utterly insane the whole thing is and that we should maybe not listen to the other insane recommendations either.

Even within your own household, children too young to be vaccinated are too vulnerable to allow you to show them your face. Ever.
With that, we get to the post going around this week explaining (for those who don’t know this already) exactly what we may be doing to our kids forever, even if only for the opening picture that should now haunt your dreams:
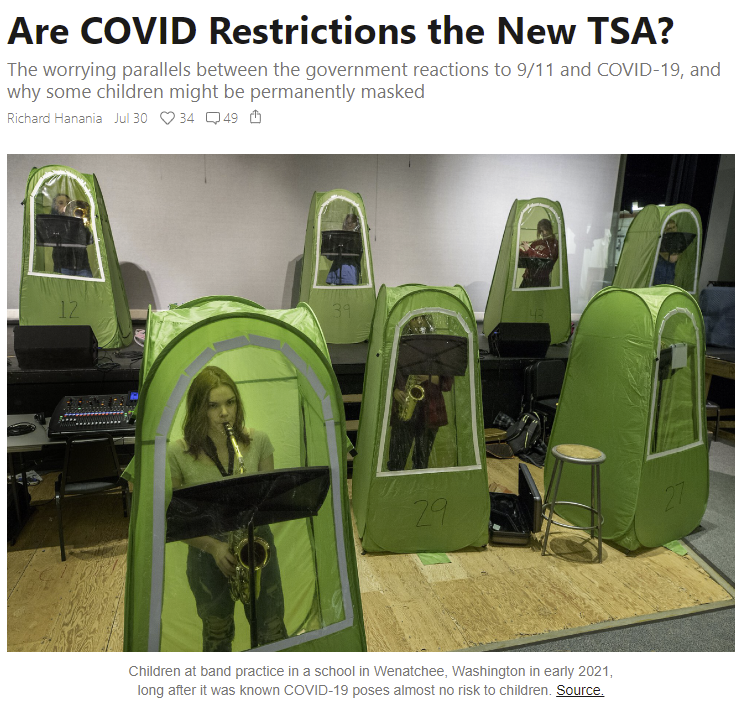
You can decide for yourself how to think about the photo above, combined with an official request for masking at home with one’s own children.
The difference between official school policies and young adult dystopian novels is that no one would buy this in a young adult dystopian novel, because it’s fiction and therefore has to make at least some sense.
Meanwhile, as noted earlier, many teachers remain unvaccinated (40% in NY), and in most places the teachers’ unions have put a stop to any talk of a mandate.
It’s one thing to say that people make individual choices, but does this look like freedom or individual choice to you? Or does it look like a Geneva Convention violation for our young prison population, potentially doomed for years to come to never see a face, based on something that is not at all a threat to them and never was? Do we hate our children that much?
Apply for the Survival and Flourishing Fund
They’re giving away a bunch of money. I’m helping figure out where to send it, and I encourage anyone with a worthy cause helping with our long term future to apply. Here’s the announcement, with more details at the link:
The Survival and Flourishing Fund, a virtual fund backed by philanthropists Jaan Tallinn and Jed McCaleb, is organizing the distribution of est. $8MM-$12MM in grants this November, with applications from orgs due on August 23. Applications are essential to enabling the grant recommendation team to learn about and debate the pros and cons of each organization under consideration, both old and new. So, please encourage applications from any awesome charitable projects you know about that are trying to support humanity’s long-term survival and flourishing!
In Other News
I’ve been accused recently of ‘carrying water’ for the government because of my stance on vaccination policy. Unsurprisingly, I don’t see it that way. Despite admiring those who do get paid for this, I’m not one of them, and on Tuesday I learned that such people exist.
I have between 5k and 100k followers! Presumably I qualify. Check, please. Every little bit helps.
Scott Sumner’s thoughts on what we should do now.
Your periodic reminder from Scott Alexander: FDA Delenda Est. He’s in full righteous fury form, which is reliably top quality. I will quote the concluding section:
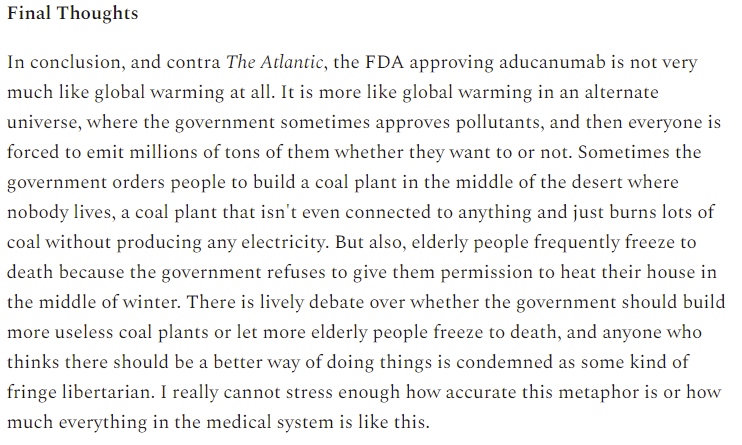
Mostly I am in violent agreement with the post, with the one exception being where Scott essentially shrugs and says ‘incentives, what are you gonna do?’ and refuses to hold anyone accountable for the whole thing or hold out any hope we could do better without raising the general sanity waterline. In order to understand what’s going on, it is vital to understand that many important actions in the system are actively perverse, and are chosen because they are worse rather than better, hurting people rather than helping them, and that people are rewarded for having an actively reversed morality and punished for having a normal one. Costs are benefits, and benefits are costs, not that anyone would then dare be seen doing a calculation. And it’s also important to note that the blame dynamics and other incentives involved, to the extent they are real and contraining, are not inevitable consequences of the sanity waterline’s current level, they are the dynamics that happen to exist, have lots of path dependence and could be changed.
Scott’s proposal for unbundling the FDA seems like an excellent second-best alternative to my preference for burning the building to the ground and salting the Earth. His first proposal, with five approval tiers, is more complex than I believe to be necessary – counting fully unapproved things, there are 6 tiers. Then again, the entire American health care system is far more complex than necessary, a lot of which is engineered for blame avoidance combined with fraudulent extraction of money, so it can’t be quite as simple as it sounds.
Your periodic reminder that Emergency Use Authorization didn’t exist at all until 2004. So things could have been so, so much worse.
Not that things are great now, we are told to follow a particular regime whether or not it makes any physical sense.
Although it can in some cases be done, presumably via lying:
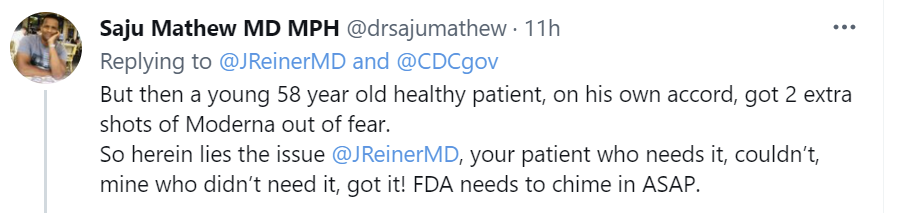
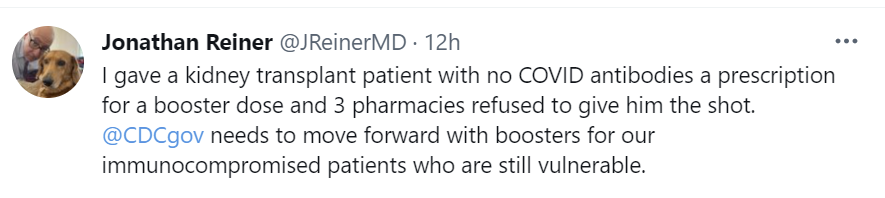
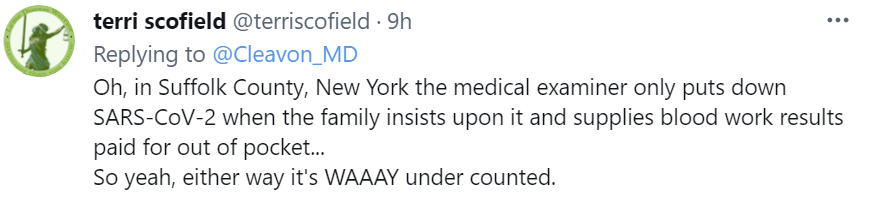
Death counts might be a little low after all?
AI fails to help with Covid. It is noteworthy that AI provided no assistance, and this offers some explanations. Data sets are terrible, and combining them often meant overlap where data in the training set got into the test set. Labeling relied on humans and incorporated their ‘biases.’ Fonts from hospitals and other contextual clues were used to cheat. The same techniques got used over and over again by everyone, so the failure of one attempt was highly correlated with the failure of other attempts. The results were not clinically ready.
I believe that these are real and important problems, but as a complete explanation I am not buying it. Several times, we heard stories of promising AI diagnostic techniques. In each case, the story was that there was this thing that would work, but the regulatory burden of being allowed to use it meant nothing would ever happen. Then we never heard about the situation again, the same way we never got rapid testing without AI or any number of other low hanging fruit improvements.
Also, if we didn’t have good data sets on which to train the AI, maybe don’t consider that purely a fatal flaw in AI, and rather consider that also a fatal failure to collect data. In general, it sounds like we tried ‘throw off-the-shelf existing techniques at the problem using what data is around’ and that was about it.
The WHO has called for a ban on booster shots, in the belief that somehow this will direct vaccine doses to those who don’t have them, rather than resulting in there being less vaccine doses available. I will still happily accept a booster if offered one.
Lamda variant said to show vaccine resistance in the lab in a preprint. I can’t find any way to distinguish the things said here from a harmless situation or from signs of the next big thing, but it’s not a good sign. Need to keep an eye on it in any case.
Nature’s write-up of Fast Grants. It’s super effective, or at least has a lot less wasted time.
For those who need it or are curious: Nature post on how Covid infects cells.
China is finally running into trouble with the Delta variant. Their efforts at containment so far have been valiant, but if their vaccine is as ineffective as it looks and they continue to be unable to admit this, the task is not going to be getting any easier. Containing the original variant for the past year had big advantages, but it also means no immunity other than from vaccinations. And if and when containment fails, it’s going to be prohibitively expensive to try and put it back in place.
Financial Times article explaining the breakthrough infections has this excellent visualization:
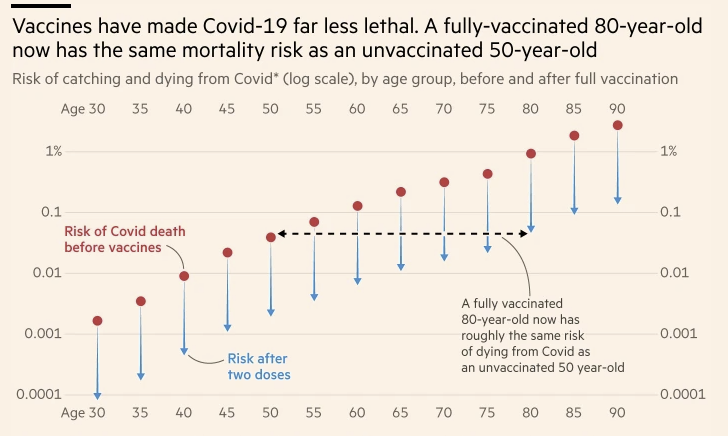
I think this is pessimistic, and that vaccine protection against death is several times lower than this, but the representation here is excellent.
This is not a great sign or a great look.


The government wishes to remind you that you should wait to protest the lockdown until after the lockdown has been lifted.
Scott Aaronson introduces us to his term blankface, for a perspective on one of the causes of our problems responding reasonably to situations.
A lot of people say they’ll quit if forced to go back to the office, with almost 20% saying either definitely or probably, and another 20% being unsure, and a lot of people being eager to go independent.
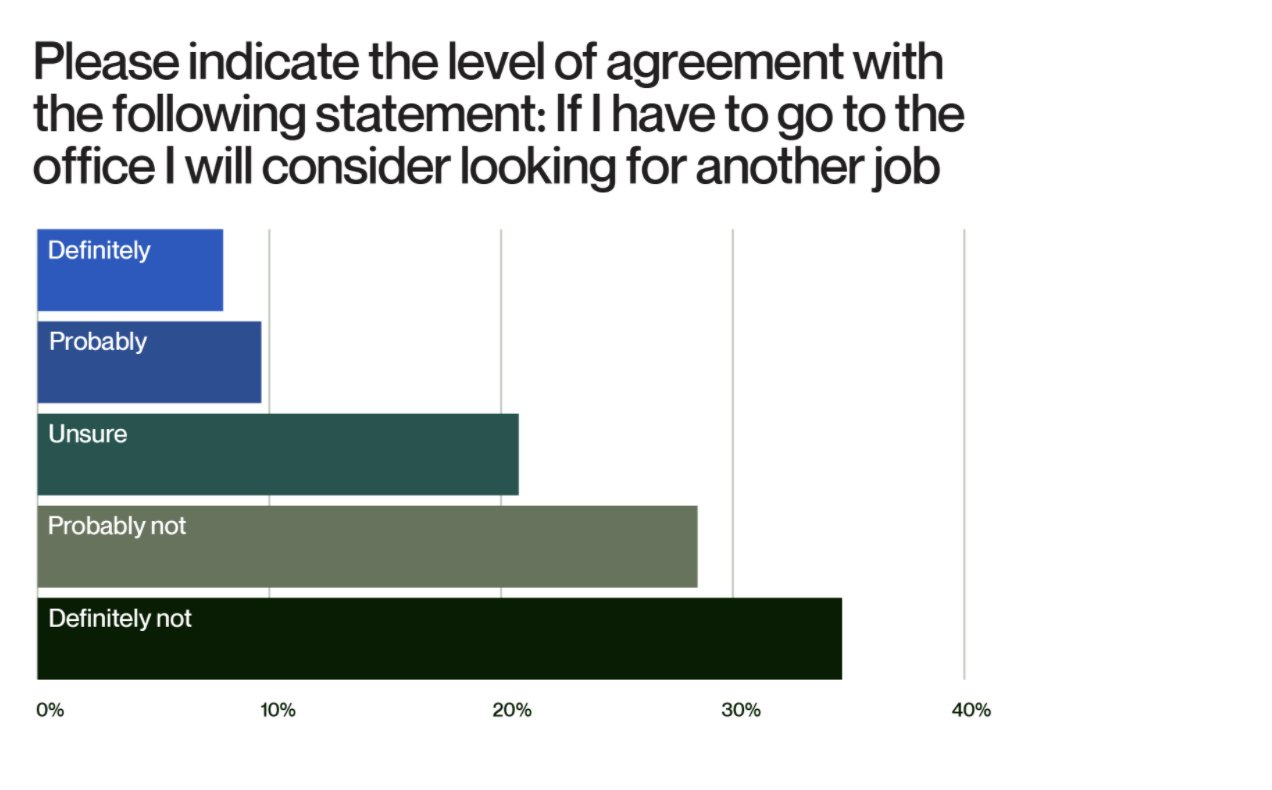
I would be surprised if most of this were not cheap talk, but even a small amount of it not being cheap talk would be expensive. Also, good for the people involved, cause they’re right, offices are mostly terrible, even if I’m excited to sometimes go into an office once it becomes possible. The last time I had to go to an office and be ‘on’ all day five days a week, even at an unusually good place to work with great people, it made me completely miserable until I figured it out and left.
Alex Tabarrok points out that the exact same ‘first doses first’ logic is now being applied to ‘second doses first’ as opposed to third doses, and attributes this to status quo bias. I think that’s mostly right but imprecise and would frame it more as action vs. inaction, falling in line behind authority and the avoidance of potential blame, but it’s mostly the same thing. And yes, the arguments about third doses are the same as the ones about second doses. This is similar to the shift in the UK to where second doses that are insufficiently delayed (e.g. are on the original schedule) are considered super risky because the immunity resulting isn’t as good.
Not Covid
In existential risk news, Scott Alexander brings us an updated look at long term AI risks. Assessments of these risks by those working in this field are super high compared to what one should be comfortable with given the stakes, but are remarkably low compared to what one might expect from people in the field. They’re also remarkably spread out, in a way that doesn’t feel like an attempt to model the future so much as an attempt to give answers that seem reasonable. Make of that observation what you will.
Biden intentionally violates the constitution, but feels bad enough about it to admit it explicitly.
This WaPo article has more details. It seems that all his lawyers told him no, this is blatantly illegal and forbidden and that which is forbidden is not allowed, including what is described as ‘quadruple checking the tires’ but when this was found to be an unacceptable conclusion, a search was on to find a new lawyer, somewhere, who would present a legal theory that could be presented as having a non-zero chance of standing up in court, and that’s about the level of legal argument they found, but Biden takes too much pride in his understanding of government and straight talking attitude to hide what was going on.
He did all this in order to extend the eviction moratorium, which has now gone on over a year, and is essentially the taking of private property without compensation. If we are extending this now, when does it end? What happens to the rental market?
Not directly Covid, but words of wisdom on how to tell whether someone breached a contract:

And now for something completely off-topic:
I’d say ‘I hope you’re happy about it’ to all the people I know who voted for it, except for the fact that they are definitely happy about it.

My model, based on what was motivating them, says: They’re mildly disappointed that eggs and veal will remain available for purchase but happy about the improved conditions and higher prices. And they’re downright giddy about the prospect of pork potentially being unavailable.
Want everything to grind to a halt? Propositions!

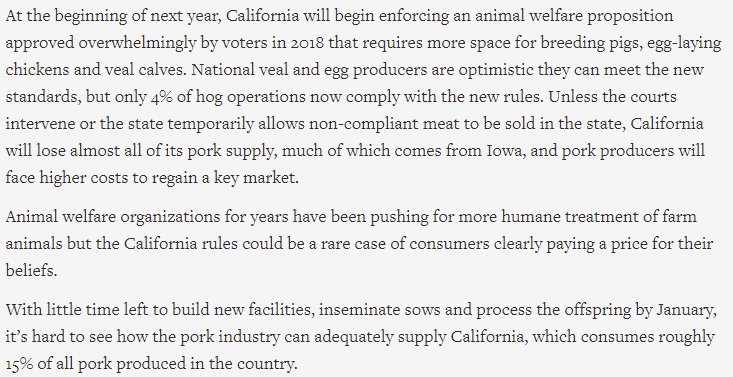
Alas for them, supply and demand don’t work the way the headline writers think…

Adding an extra 15% cost effectively forces such farms to choose to either supply California or supply others, which creates two distinct pork supply chains, which adds further to costs. The thing is, that’s the costs to adhere to the requirements, not the costs to demonstrate compliance. As with all such things, by the time all the paperwork is done, the costs might be considerably higher for that reason as well. The lack of any guidance on exact requirements or enforcement mechanisms is a lot of why almost no one is prepared to meet the new requirements – you can’t comply until you know what compliance means. Plus even if you did know, what will tomorrow bring?

But to me that’s not the interesting part. The interesting part, to me, is that last line, which is an estimate of the elasticity of demand for pork, and it’s shockingly high.
This is saying that if the pork supply was cut in half, all it would take would be a 60% increase in prices to clear the market. Wait, what? We’re that sensitive to prices on something this cheap? Because pork prices at the local supermarket are stupidly cheap, in a ‘can you believe civilization lets us eat meat for almost no money’ kind of way.
As in these are the Instacart prices:



You can pay a lot more to get higher quality stuff, if you so desire, but the prices really are super low. Bacon is more expensive by the pound, but I hope those involved are using smaller portions. Choose life.
So you’re telling me, you raise these prices by 60%, and half the time people say ‘nah, let’s get something else instead.’? I definitely would not have expected that. It seems more like what would happen if a particular source increased prices, rather than all sources of pork together.
And then we come to a very strange statement:

Increasing prices by 60% is estimated in California to cut demand in half. If 15% of the nation’s pork goes to California now and half of it can’t in the future, then that’s 8% more for the rest of us, which in a perfect world might cut prices a few percent.
I don’t see much danger in these standards becoming nationwide, unless other states are persuaded to pass similar laws. If California eats 15% of the pork at current prices, and compliance with their rules raises prices 15%, and raising prices 60% cuts demand in half, then it stands to reason that raising prices 15% would cut demand by 12%, so even if everyone made the move at once it’s barely worth it, and you’re going to get eaten alive by whoever didn’t make the move. This seems like it’s above the threshold of cost that California can impose.
But then again: You never know. Incentives matter.
34 comments
Comments sorted by top scores.
comment by Dave Orr (dave-orr) · 2021-08-05T20:37:05.658Z · LW(p) · GW(p)
For a fascinating, borderline nsfw look at bear week during COVID, and why infections might be atypical, this reddit thread is worth a gander.
"My point is... To everyone worried about the P-Town data: I wouldn't get too nervous going to the grocery store just yet -- unless you tend to have orgies at Market Basket."
Replies from: Zvi↑ comment by Zvi · 2021-08-06T09:55:20.118Z · LW(p) · GW(p)
I wonder how much of what happened is because people are afraid to point such things out.
Replies from: supposedlyfun↑ comment by supposedlyfun · 2021-08-08T00:46:06.369Z · LW(p) · GW(p)
It didn't feel momentous, but the fact that the study and coverage thereof simply...didn't say it was Bear Week...seems to have updated the baseline probability of my prior that "A given outlier study being used to advocate for counterintuitively high restrictions is explained by some bullshit" to like 90%. Given how much data we already had that said something else, maybe my prior was too low.
It seems like the media could have said, "although this was during Bear Week, which may have led to increased social contact..." without getting much blowback.
I guess it's a metagame where you can't say certain things about people IFF they're a subgroup (gay men) that tends to be a victim of prejudice for unrelated reasons. Unlike, say, the coverage of Sturgis last year, where no one expected pogroms against motorcycle gangs. Some rule like, "If your factual statement will be used to 'justify' hatred, you shall not make it."
I'm really missing the updates from UWash's Alliance for Pandemic Preparedness on the latest studies. Having a ton of study/data points was really nice. They stopped updating in June with no explanation I could find.
comment by Will Sorenson (will-sorenson) · 2021-08-05T17:31:48.596Z · LW(p) · GW(p)
.
Replies from: Measure, Zvi↑ comment by Measure · 2021-08-05T21:18:36.633Z · LW(p) · GW(p)
This, at least, from the wiki page:
Mirror life presents potential dangers. For example, a chiral-mirror version of cyanobacteria, which only needs achiral nutrients and light for photosynthesis, could take over Earth's ecosystem due to lack of natural enemies, disturbing the bottom of the food chain by producing mirror versions of the required sugars.
↑ comment by Zvi · 2021-08-06T09:48:04.545Z · LW(p) · GW(p)
Section deleted because someone credibly raised the case it is an infohazard, which I assume carries over to a request to delete these comments as well but the visibility level is very different and I leave that to others to decide.
My basic decision was 'well, if the person who knows who said anything said to not talk, and my other feedback (at main blog) was that this wasn't a big deal so don't worry about it, then I guess I'm not doing net good here and should stop.'
comment by Craig Fratrik (craig-fratrik) · 2021-08-05T16:11:20.316Z · LW(p) · GW(p)
NIH Director Francis Collins claimed he misspoke, and tweeted to clarify.
Let me clarify the masking message that I garbled on @NewDay this morning. Vaccinated parents who live in communities with high COVID transmission rates should mask when out in public indoor settings to minimize risks to their unvaccinated kids. No need to mask at home.
https://twitter.com/NIHDirector/status/1422654529087189000
Not sure how to feel about the poor communication, but propagating the followup, I think.
Replies from: Zvicomment by Radford Neal · 2021-08-05T16:16:31.724Z · LW(p) · GW(p)
You say "these are very wide error bars", in reference to the plot of Ct value versus vaccination status, hence casting doubt on the idea that the vaccinated and unvaccinated have similar Ct values.
But I think the boxplots shown represent the distribution of values, NOT the uncertainty in the estimated mean. With n=84 and n=127 for the two groups, the standard error in the difference in the two means should be around 0.5 (an exact figure isn't obtainable from the displayed data, which shows quantiles, not standard deviations). Whether that's "small" or not is of course a subjective judgement, but it's a lot smaller than the size of the boxes.
However, a serious problem with this plot is that the unvaccinated are lumped together with "unknown" and "not fully vaccinated". Since unknowns may well be vaccinated, and the partially-vaccinated have a large part of the immunity of the fully-vaccinated, the plot is basically useless.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-11T09:12:33.354Z · LW(p) · GW(p)
Another problem is that Ct values are a logarithmic function of viral load. Increasing the Ct value by 1 corresponds to halving the viral load.
comment by ejacob · 2021-08-05T21:48:25.640Z · LW(p) · GW(p)
The medical examiner thing seems totally fine - in this county they only see bodies that are sent for autopsies; i.e. something is fishy about their death. If you die in an ICU because of low oxygenation you don't get sent to the medical examiner. If you die from a knife to the back and your family wants to argue that you died from COVID-19 then it makes sense for the medical examiner to want them to pay for it.
- My mom, a Suffolk county based doctor who used to do autopsies
comment by Florin (florin-clapa) · 2021-08-05T21:23:24.072Z · LW(p) · GW(p)
...I note here that if vaccines were sufficiently ineffective in practice against Delta, there would be no reasonable way to stop the pandemic, and I’d want to do the opposite of the implications listed here and stop trying.
I don't see how this can be correct. Effective PPE exists in the form of elastomeric respirators and PAPRs that should be able to stop any pandemic.
↑ comment by Zvi · 2021-08-05T21:36:11.420Z · LW(p) · GW(p)
Yes, there are More Dakka options available for individuals but at the population level these are non-starters - and if I had to choose between wearing one of those all the time indefinitely and getting Covid, I'd take my chances with Covid.
Replies from: florin-clapa, florin-clapa↑ comment by Florin (florin-clapa) · 2021-08-05T23:49:01.790Z · LW(p) · GW(p)
The same reasoning was deployed against wearing masks and doing most of the restrictions and I suspect also against switching from masks to respirators before and even during the winter wave. Millions died as a direct result of this poor reasoning. The same mistake is being repeated in countries that have little access to vaccines. Millions more will die there, if they haven't already. And what if it will become clear that vaccines won't be able to prevent (due to some variant worse than Delta) another massive wave of infections that leads to lots of long covid and death? Should the arbitrary personal preferences about face coverings of a handful of policy makers determine the fate of millions or even billions of people? No, the lesson should be that how you feel about personally using an option shouldn't shape general recommendations or public policy; all reasonable options should be presented and the public should be allowed to choose which option to use, if any.
Replies from: Zvi↑ comment by Zvi · 2021-08-06T09:52:54.611Z · LW(p) · GW(p)
If the argument here is that we should tell the public the option exists for individuals, I agree - is that link the best one or does anyone have a better one, so I can do so next week?
If the argument here is that policy makers should be trying to get this to become a new norm until things get better, I strongly think that would (1) make life worse and (2) be a complete nonstarter for 90%+ of the population.
Replies from: florin-clapa, Pattern↑ comment by Florin (florin-clapa) · 2021-08-06T23:14:24.224Z · LW(p) · GW(p)
The argument depends on the population. If people have access to effective vaccines, then effective PPE like elastomeric respirators are probably not needed except perhaps by the most risk-averse individuals. I say "probably" because there still seems to be a bit of uncertainty about long covid even for the vaccinated. At any rate, elastomerics should still be recommended as a replacement of masks in case a variant comes along and makes vaccines significantly less effective or as an option for people that still don't trust vaccines. This would also encourage the public to get used to the idea of using respirators for future pandemics and give a larger part of the public motivation and more time to prepare. For the rest of the world where vaccines are scarce or of poor effectiveness (and given the fact that masks don't seem to work all that well against variants), respirators could be used as a bridge to vaccination or other effective medical interventions.
Calls for more effective PPE for the public is nothing new but has mostly fallen on deaf ears. Elastomerics were mentioned on this site [LW · GW] and in a few other places near the start of the pandemic but were mostly were ignored. There was a push during the winter wave for better PPE, but instead of switching to respirators, multi-layered masks were recommended in the US for poor personal preference reasons. Germany started to recommend everything from surgical masks all the way up to disposable (and often leaky) respirators but elastomerics were not mentioned as far as I know. I haven't bothered looking for more recent face covering recommendations of other countries, but I highly doubt that any are recommending elastomerics, and the WHO (like the CDC) certainly doesn't mention respirators at all. The situation is a lot worse for PAPRs. Very few people know that these things exist and even fewer know that cheap (and seemingly effective) PAPRs are possible; even I wasn't aware of the things until a few months ago. This persistent and widespread avoidance of recommending effective PPE for no good reason seems bizarre and quite insane.
↑ comment by Pattern · 2021-08-08T20:05:15.231Z · LW(p) · GW(p)
are probably not needed except perhaps by the most risk-averse individuals.
a) That seems interesting for economic reasons.
b) Or those who are in more risk.
c) There is something to using the Intermediate Value Theorem here. Just because going way more Dakka seems like a bad idea, doesn't mean something less extreme wouldn't be an improvement. (Although comfort might be a big factor here - something which doesn't change effects much, but is more comfortable (or looks cooler) might be much more easily accepted.)
↑ comment by Florin (florin-clapa) · 2021-08-09T00:10:11.901Z · LW(p) · GW(p)
Another point that should be emphasized is that the longer people don't have access to effective vaccines and also don't have adequate protection (respirators and PAPRs), the more likely it will be for more dangerous variants to evolve. This situation is a repeat of what happened during the start of the pandemic when mask wearing was discouraged: it allowed the virus to spread like wildfire and accelerated the emergence of dangerous variants.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-09T10:38:57.241Z · LW(p) · GW(p)
Not to dismiss your concerns, but I'm not sweating variants. I do make a point to mask up when I'm in an enclosed public space.
- Convergent evolution. The variants aren't very variable from one another (and they've had a lot of time to diversify):
- New variants seem to arise in people who are severely immunocompromised. ("supermutators" if you will)
- It is unlikely that we will ever eradicate covid, unless we:
a) start putting salt licks in our backyards and declare open season on does and fawns:
https://www.nytimes.com/2021/07/30/science/white-tailed-deer-coronavirus.html
and
b) start treating our wastewater with rat poison:
https://www.thecity.nyc/2021/7/29/22600656/covid-mutations-in-new-york-city-sewage-possible-dog-rat
- If it's true that the Russian flu was actually a coronavirus that evolved into OC43 (now endemic), then I'm not too worried about covid becoming "just another endemic coronavirus". The vaccines are simply a way of speeding up the process in a way that minimizes deaths.
↑ comment by Pattern · 2021-08-08T20:02:29.642Z · LW(p) · GW(p)
There was a time when it would have seemed reasonable for say, grocery stores (as opposed to beaches). (Although I might be overestimating traffic around the time of the panic buys of toilet paper, I don't know whether it was higher or if people just bought way more.)
I wonder why it seems more unthinkable for schools to be outside than to shutdown or be online. (I've never thought about this before, but why are roofs rarely designed to be used? Is it cost* or custom?)
*Obviously that tradeoff looks slightly different now.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-09T16:51:54.576Z · LW(p) · GW(p)
Classes were, in fact, held outside during the 1918 pandemic.
Replies from: Pattern↑ comment by Pattern · 2021-08-10T18:37:50.960Z · LW(p) · GW(p)
And yet today (and throughout 2020) they are either 'at home', 'open' or 'closed', instead of being held outside.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-10T19:03:44.751Z · LW(p) · GW(p)
The failure to pick off low hanging fruit is inexcusable .
↑ comment by Florin (florin-clapa) · 2021-08-09T04:56:54.856Z · LW(p) · GW(p)
Another potential problem with giving up is that you may get reinfected multiple times if enough dangerous variants emerge and your risk of death and long covid may dramatically increase.
comment by tkpwaeub (gabriel-holmes) · 2021-08-06T10:57:40.971Z · LW(p) · GW(p)
I wonder what others think about the possible link between severe Covid and latent CMV:
https://immunityageing.biomedcentral.com/articles/10.1186/s12979-021-00218-z
comment by tkpwaeub (gabriel-holmes) · 2021-08-06T00:04:06.403Z · LW(p) · GW(p)
I think the FDA is terrified of the possible repercussions of approving just one of the vaccines, because
-
People might flock, or even stampede, to one particular vaccine. The vaccines will no longer be seen as "fungible" This could potentially slow down the pace of vaccinations - drastically
-
It may be harder to justify, legally, keeping the other two under an EUA when there's at least one that's been fully approved.
-
Appearance of conflict of interest, insider trading, etc. Exhibit A, Martha Stewart Exhibit B, Scott Gottlieb (on the board of Pfizer)
So they're dragging it out so they can at least shorten the gap to days instead of weeks.
comment by magfrump · 2021-08-07T18:48:24.317Z · LW(p) · GW(p)
Your model of supporters of farm animal welfare seems super wrong to me.
I would predict that actually supporters of the law will be more unhappy the more effect it has on the actual market, because that reveals info about how bad conditions are for farm animals. In particular if it means shifting pork distribution elsewhere, that means less reduction in pig torture and also fewer options to shift consumption patterns toward more humanely raised meat on the margins.
Those costs can be worth paying, if you still expect some reduction in pig torture, but obviously writing laws to be better defined and easier to measure would be a further improvement.
comment by tkpwaeub (gabriel-holmes) · 2021-08-13T14:33:45.819Z · LW(p) · GW(p)
For the statistics you cite on Wyoming and the Dakotas, I'm curious to know what would happen if you separate out the Indian reservations.
comment by tkpwaeub (gabriel-holmes) · 2021-08-09T16:50:23.788Z · LW(p) · GW(p)
Perhaps one way to demystify the percentages that you're seeing with absolute mandates versus various types of "conditional" mandates is the burden that the latter place on underpaid, overworked gatekeepers. The more things you add to the list of "things that should require vaccination" the closer you'll get to flat out mandates, the kind that are typically backed up by large fines.
comment by tkpwaeub (gabriel-holmes) · 2021-08-09T09:26:10.139Z · LW(p) · GW(p)
This is a really interesting approach to estimating actual prevalence:
https://www.medrxiv.org/content/10.1101/2020.10.07.20208504v1.full
comment by malteskarupke@web.de · 2021-08-07T11:47:14.846Z · LW(p) · GW(p)
I think a lot of the public communication confuses 'catching the virus' with 'catching the disease', especially for vaccinated people. If somebody tests positive for coronavirus, but doesn't get covid, that's great. But the press makes it sound scary. They call it a breakthrough infection that happened to be asymptomatic.
And I have had people tell me to wear a mask (to an apartment showing) because even if you're vaccinated, you can still catch the virus. To which my response should have been "of course, do you understand how vaccines work? They protect you after you catch the virus, they don't stop you from getting it, and they aren't supposed to." But instead I said nothing and wore the damn mask.
Fwiw that 8x reduction number from the CDC slides is the first time that I have seen a number put on this difference. Which is very good to know, because I have now heard of several people who got sick despite being fully vaccinated, and I never knew how to adjust my thinking based on that. 8x reduction for getting sick (and 25x reduction for getting seriously sick) sounds about right for how often I have heard of this, while at the same time it won't make me update my behavior.
comment by AnthonyC · 2021-08-05T21:43:29.704Z · LW(p) · GW(p)
RE: That example of a company requiring only the vaccinated to go into the office: It could be worse. I know of at least one company where they are letting anyone who declares themselves to be afraid of getting covid stay home, but are having everyone else come back. As you might imagine, the former group has a much higher vaccination rate than the latter.