Covid 10/13/22: Just the Facts
post by Zvi · 2022-10-13T14:40:01.324Z · LW · GW · 7 commentsContents
Executive Summary The Numbers Predictions Deaths Cases International Cases and Deaths Physical World Modeling Obvious Nonsense: Florida Man Commissions ‘Study’ In Other Covid News None 7 comments
As discussed last week, I am going to shift procedures a bit. From this point forward, the Covid posts themselves will only cover Covid-19 and related issues.
There will then be a second post that contains all non-Covid developments that I do not think have reason to want their own posts.
Other content will be moved into its own posts, some of which will be held longer in order to offer better logical organization – e.g. there will not be a weekly post on housing or energy, more like a monthly post, and I’ll be holding housing content until I have enough of it. Feedback on this plan is of course welcome. Alas, this post was still too long for email.
Executive Summary
- Weekly update now splitting up by topics.
- Rising cases in Germany, no alarming general pattern yet.
- More of the usual Long Covid studies fail to enlighten us.
Let’s run the numbers.
The Numbers
Predictions
Prediction from Last Week: 221k cases (-18%) and 2,300 deaths (-17%).
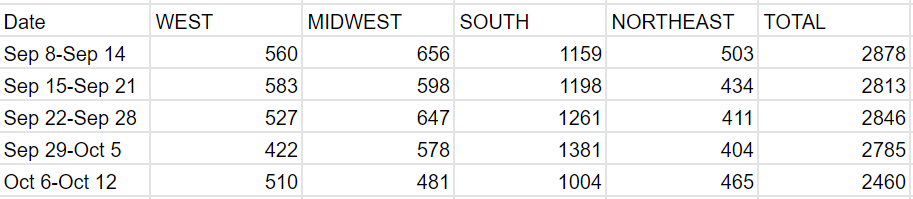
Result: 234k cases (-13%) and 2,460 deaths (-12%).
Prediction for next week: 234k cases (+0%) and 2,500 deaths (+2%).
I overshot a bit. That could be that the holiday had lower than usual impact, or that the underlying rates did not slow down much. That makes this a higher uncertainty week than the last several weeks, although not high by historical standards. Even if we are going to get a winter wave, we still likely have some more declines left first.
Deaths
Cases
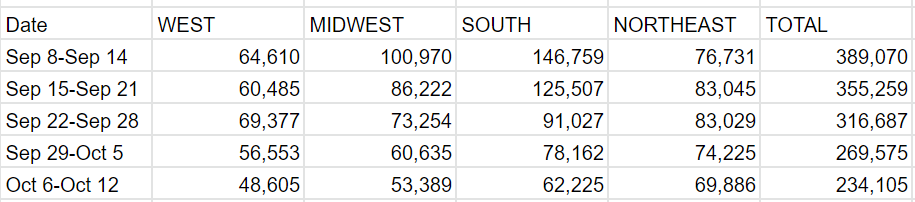
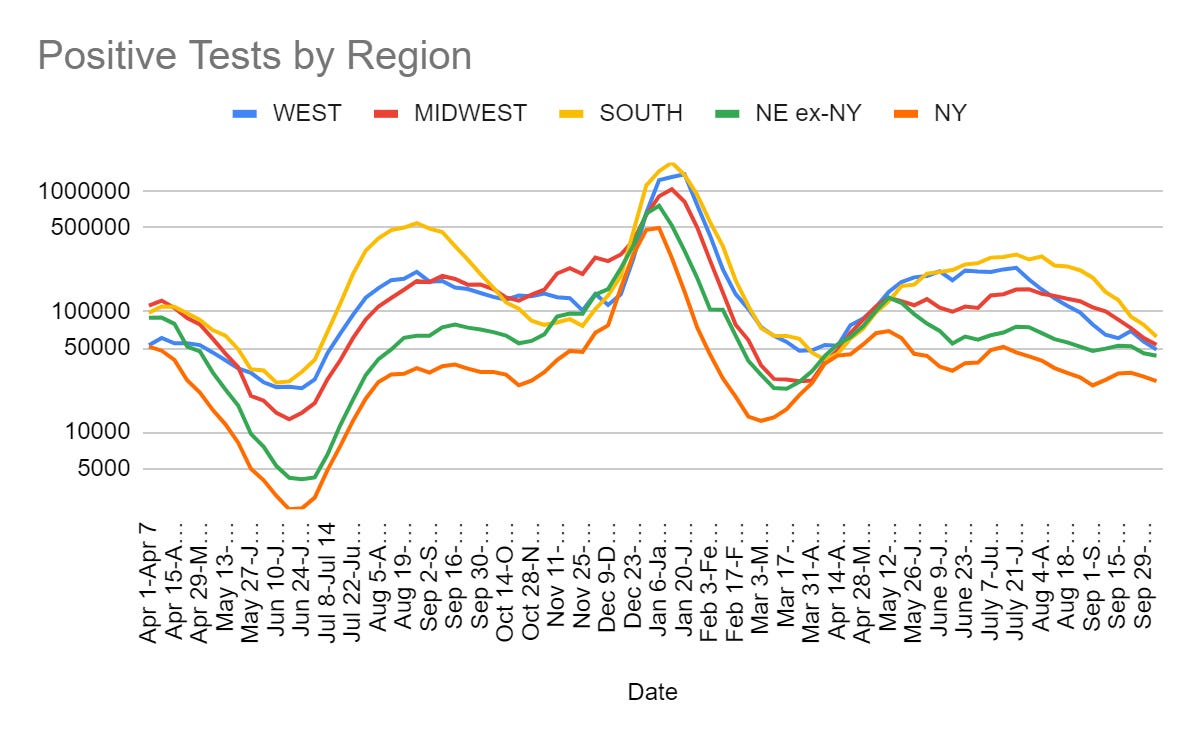
Florida’s count came in low enough this week that cutting it in half might have been a mistake. For now I’m choosing to follow procedure. Keeping an eye in case Florida does report somewhat next week.
International Cases and Deaths
I haven’t looked at these numbers in a while. Given that there were claims that waves were descending upon Europe, it seemed like time to look.
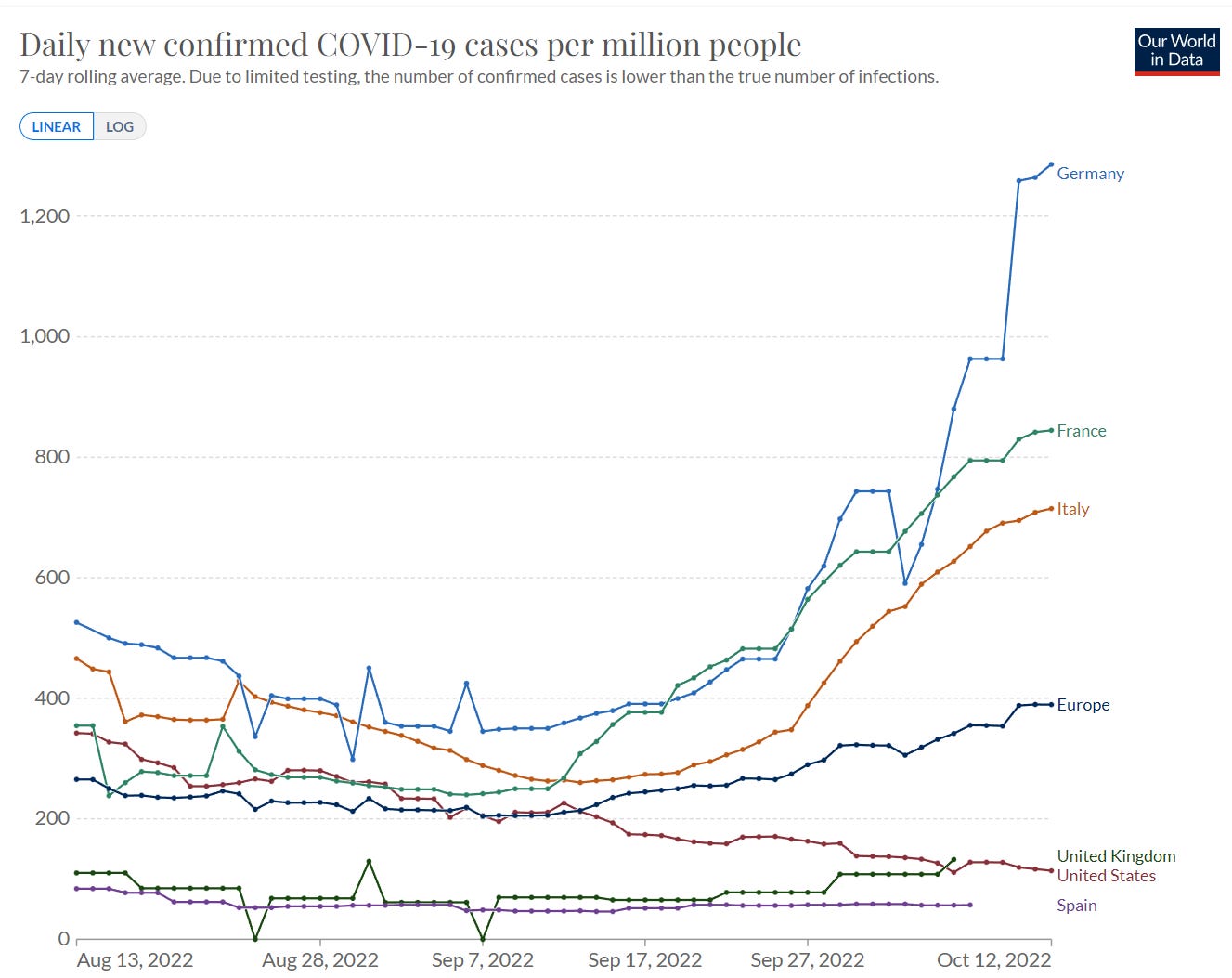
Here’s cases for major Western European countries since July 1:
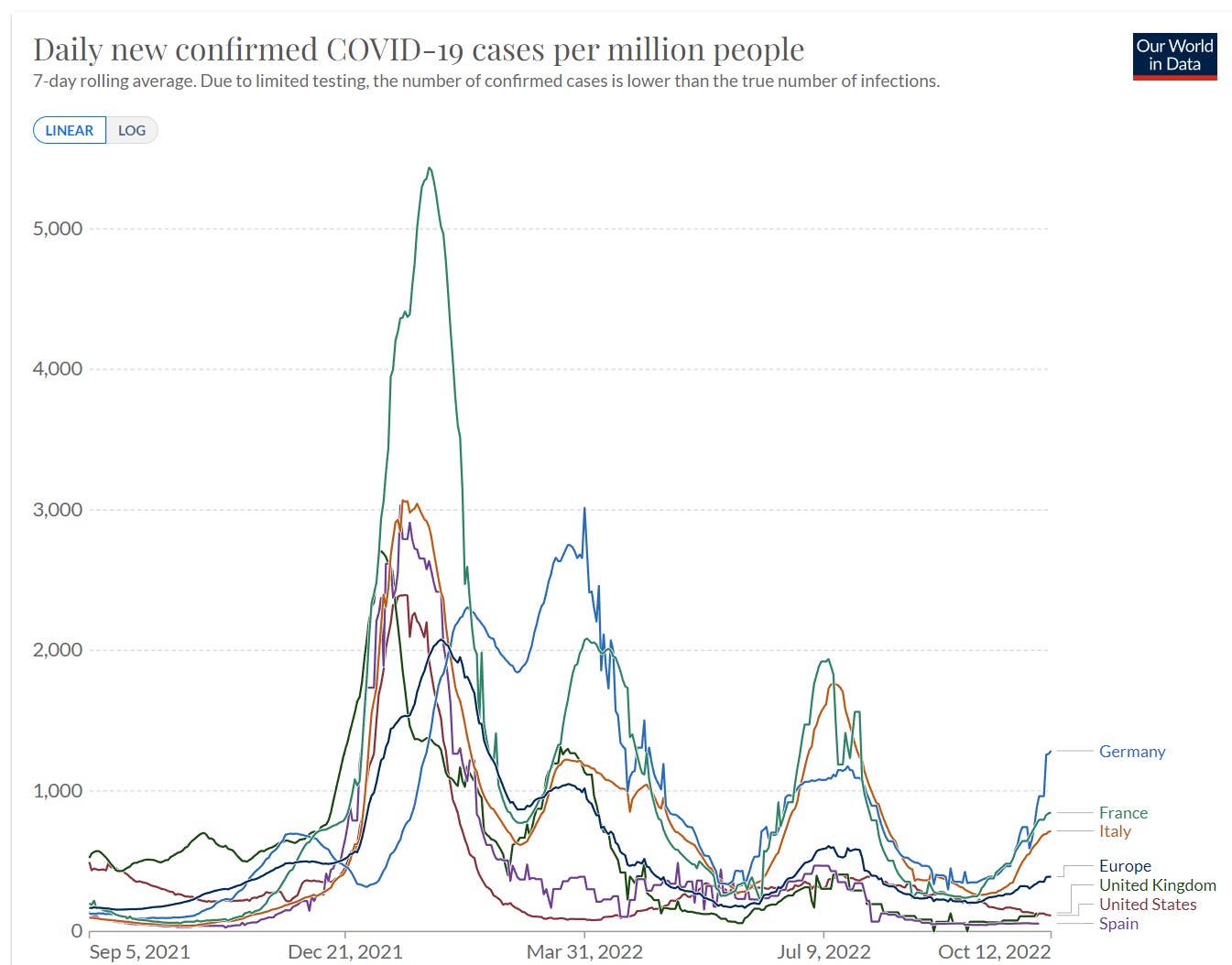
For context, same chart zooming out:
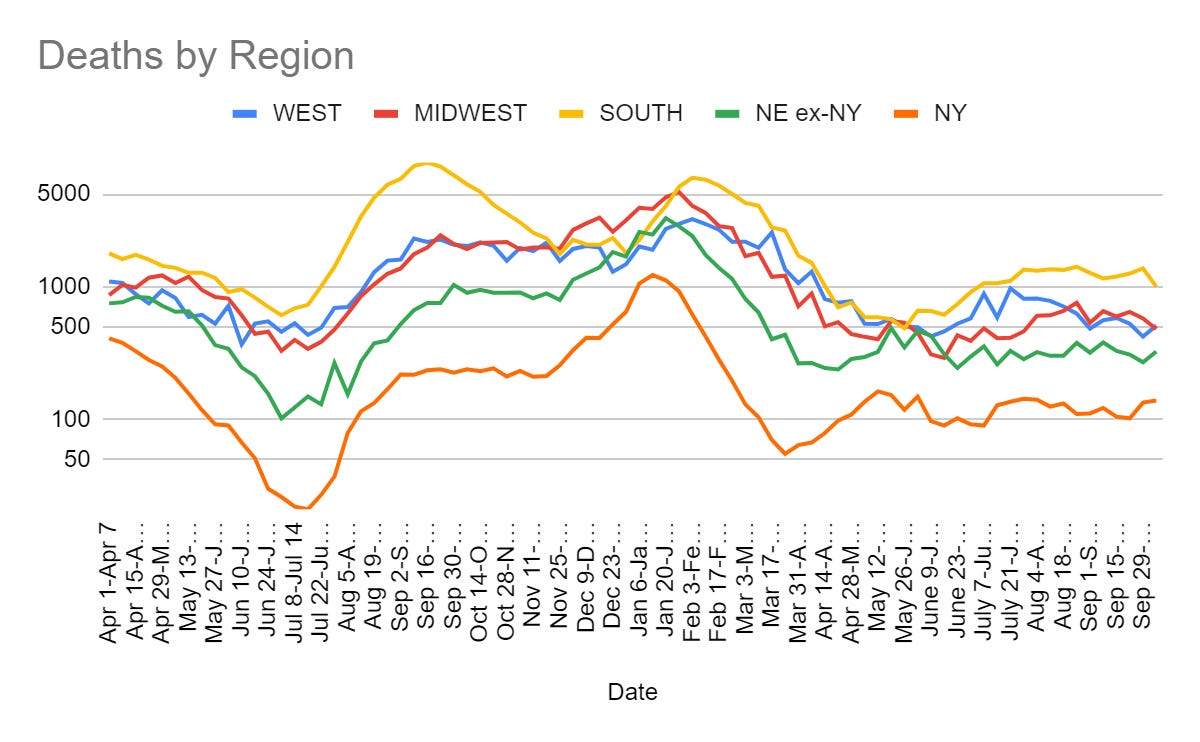
We definitely see an upswing in several countries, caused at least in part by the new variants.
What we do not see in any country other than Germany and perhaps Austria (I also checked most of the smaller European ones) experiencing the kind of scary rapid exponential growth that preceded previous major variant-based waves. Every other country is still below France and Italy’s levels and none of them show a rapid rise in cases.
We did not see a similar bump last year, so this presumably isn’t Oktoberfest.
This isn’t nothing to worry about, especially for Germany. It also isn’t something I would lose sleep over. If the new variants were about to wreck havoc, I would expect to see a different cross-country pattern than this.
Physical World Modeling
Analysis of total Covid death rates around the world, finds Iron Curtain countries did a lot of fudging as did India, America didn’t fudge, the countries that postponed Covid for a long time paid a high price but did prevent a lot of deaths by doing so. While I don’t entirely trust the methodology here, I find it useful.
Paxlovid cuts one’s risk of death from Covid-19 by a third if you’re over 50, and still most eligible people don’t use it. David Leonhardt has a thread lamenting how this happened, with Paxlovid coverage being about all the downsides while ignoring the massive overwhelming upside.
Nope, not going to do it, wouldn’t be prudent. I am not reading this one. We are not doing Medium Covid.
We will still do a bit of long Covid via a new study, though.
I guess. Once again, the cohort is almost entirely (96%!) unvaccinated.
And once again, the 6% who self-classified as ‘not recovered’ are often ‘not recovered’ from distinct other things, as we neglect long-term health conditions in general.
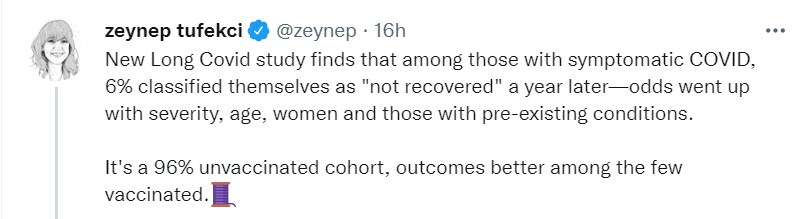
Always note that ‘group X is at higher risk than this average’ always also means ‘group ~X is at lower risk than this average.’
Those are certainly issues. To me the even bigger issue is still that the controls are never adequate. Does ‘having a control group’ here fix that?

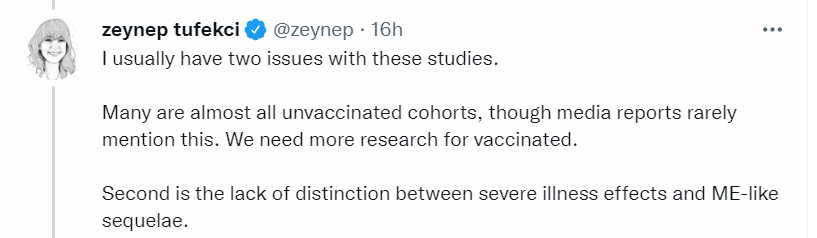
Let’s see, here is the study itself. I cannot find evidence of controls that would address the usual selection effects. So this seems to not tell us anything new.
More interesting to me is another study from the same thread.
If vaccination cut Long Covid rates by ~96% then these studies are simply not applicable to the current situation.
A call to get the “untested” bivalent boosters because they are forward looking and planned for BA.5, invoking the Wayne Gretzky Principle of skating where the puck will be. The problem is that the puck will be with newer variants within a few months. If we want to follow the WGP, we need a much much faster process.
A look at why only 4% of eligible Americans got the new boosters. A third of Americans plan to get them eventually. This is then framed as ‘who is to blame for this failure’ rather than considering that perhaps people are making reasonable decisions.
“I blame the federal health bureaucracy,” agreed Jon Favreau, a host of “Pod Save America,” a progressive podcast, and former speechwriter for President Barack Obama. “This was not the White House’s fault. This is not the top scientists in the administration’s fault. This was the agencies dragging their feet and a small, very vocal group of experts who happen to be on Twitter a lot.”
Right after Biden announced the booster plan, Favreau sought out and got a third booster dose — not waiting for the health agencies to act. “I had a baby at home that was unvaccinated, and I didn’t want to take my chances,” he recalled.
A CDC spokesperson defended the agency’s process to review and encourage the boosters last year.
“Suggesting that federal agencies’ review of the boosters had some significant impact on their uptake is bizarre and wrong,” said the CDC’s Kevin Griffis. “We know the reasons why people don’t get boosted … It’s not because experts spent a few weeks reviewing the data” but because many vaccinated Americans believe that two shots are sufficient.
That’s Favreau’s third booster, because he ‘had a baby at home that was unvaccinated.’ This does not exactly capture the epistemic or cost-benefit analysis high ground.
Others are getting other things wrong.
Sitting at a table inside the Lewisville, Tex., public library, which she made sure was wiped down, Kay Cudjoe, 65, a retired educator, said she’s already made her appointment for the new booster, which would be her fourth dose — but isn’t planning on any more.
“This is the last one I’ll have to get,” Cudjoe added. “At least that’s what I understand.”
In some sense, yes this is the last one she’ll have to get. In another sense, she didn’t have to get this one if she didn’t want. In most senses that she did have to get this one, she probably is going to ‘have to’ get another one at some point as the mutations go by.
Consider Maggie Clement, 27 years old:
“The first two shots, I missed a day of work. And with my booster, I missed two days,” she said.
You are not going to convince her to get the shot without lying to her, nor would convincing her be doing her any favors.
That doesn’t mean the campaign wasn’t botched. If everyone ‘had all the facts’ and was thinking well, my presumption is that most elderly people would get boosted, along with many in the 50-65 range and a few below that. That’s a lot higher than 4%.
Doctors who see patients decline shots will often treat them as stupid, or ‘a danger to my own family.’ This is not a new phenomenon; Arnold Kling here gives a personal anecdote about an unrelated test he knew was useless:
His response was to call my wife and warn her that I was acting strangely, and that I was citing someone he had never heard of (Bayes). I eventually went for the test. But after that experience, I switched doctors.
Yelling that there are warning signs is not going to work, either, no matter how real.
One can also note that in the UK, if you are under 50, you cannot get the new boosters at any price. What is not the only responsible thing to do, is forbidden. That’s at least a huge step up from that which is not mandatory.
It also doesn’t mean there aren’t people who are irresponsibly getting in the way, also Law of No Evidence (Drink!).
“I just don’t think we have any evidence that it’s better,” Offit said, pointing to a New England Journal of Medicine study that he said “shows underwhelming evidence” for it.
I mean, that’s so damn clean. He’s citing evidence as proof there is no evidence. Make it a double. Then it gets better:
Still, heendorses the shot for more vulnerable groups: people over age 75 or living in nursing homes; those with chronic conditions such as severe Type 1 Diabetes, lung or heart disease; and those with weakened immune systems.
What do you even say at that point?
I see two choices.
You might claim that the new scary variant will ruin everything once again.

Also always fun to claim, as Gregory does, that this means we should magically have somehow implemented Zero Covid and gotten the rest of the world to do the same, Because Variants. Here’s the tweet they quote from Cornelius Roemer.
It has since been over a week and none of the accounts I follow are sounding the alarm bells, as lots of distinct evasive variants do the standard climb up while they are new. Here’s his follow-up on the 6th and here is an analysis he links to from Tom Wenseleers.
Claim from JP Weiland a week ago that these new variants will drive a new wave, labeling them collectively (BQ.1.1, BN.1, XBB, BA.2.75.2) as ‘Pentagon’ variants. This seems to make the (very easy to make) error of assuming new variants will sustain their current growth rates once they take over.
Could there be such a wave in winter? I mean, sure, of course, there is no reason to dismiss that. The weird thing about this is so many different variants rising at once. That’s not the pattern from before. It also raises the question, did they all arise at the same time? From the same source somehow? It is confusing, and makes any given variant seem less unique and also less scary.
Or you claim a falsely high number of Americans have long Covid presumably (the misquote of the literature here is in the USNWR article being linked to).

All the usual caveats about the NCHS data of 7.2% continue to apply. Real long term health issues after Covid do not imply causation, previous long term health conditions were always under-noticed, under-treated, under-studied and under-reported, we continue not to see signs of an additional 6% of the country having important activity limitations, almost anything could count, and so forth. If I was inclined to, I could say I ‘had Long Covid’ under their definitions, and it would in practice be nonsense.
Here is a review of Long Covid pathobiology and what might causing it (direct link), which proposes mechanisms. I have not had the opportunity to read it.
Person doesn’t understand why Novavax has not been approved as a booster despite evidence suggesting this would be effective. It has not been approved as a booster because the system is designed to not approve things and once we already ‘have an updated booster’ the bar is going to be much higher than ‘probably works better than what we have.’ Even if it did work better, they’d likely want to ‘avoid confusion.’
Meanwhile, in other avoiding confusion news, are we seriously doing this again?
Yes, people will continue to get infected after vaccination. I still wonder how effective the vaccines would need to be at preventing infection before they wouldn’t have switched to ‘the primary goal is to reduce severity.’ Either way, yes, we are going to keep doing this one forever.
Obvious Nonsense: Florida Man Commissions ‘Study’
I could decide not to indulge this at all. That would normally be The Way, but I decided: Not this time. Let’s have a little fun with this one. What did he find?


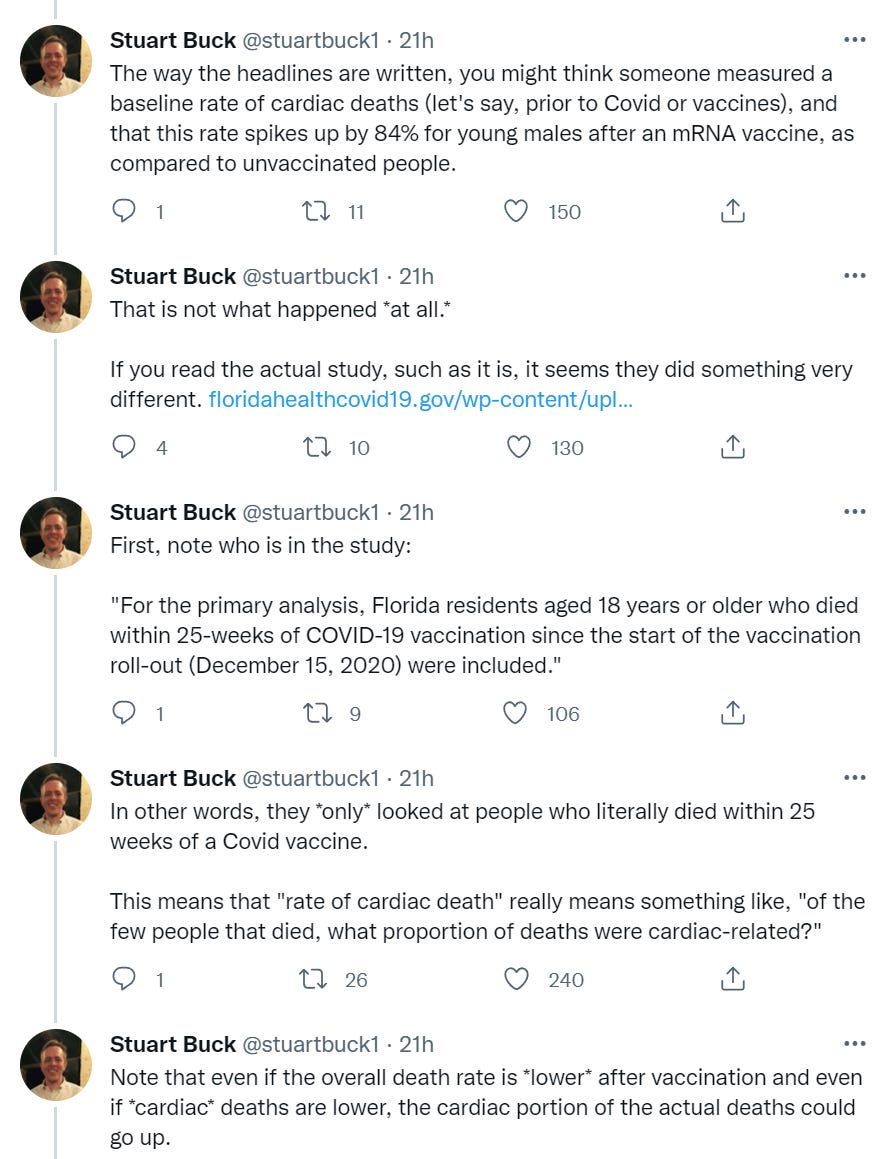
Yikes. An 84% increase! Oh no. That sounds bad, huge if true. Would still be far better than being unvaccinated, as always, outside of at most those with acute conditions.
No authors is strange. Can’t remember hearing that elsewhere.
Basic idea of this design seems fine. Compare death rate in one period to death rate in another period.
What about the details?
Here’s that JAMA article, that found no links here at all.
Those are big limitations, but it seems like if you’re robust then those limitations go the other way. If you’re taking a noisy measure and the noise is random, and you still see signal with a strong sample size, that is good signal.

Oh.
I see.
She then talks about Covid not being excluded properly , which seems like at most a secondary problem at this point.
That’s definitely asking the wrong questions. I see no reason I should care about what portion of deaths are X. I care about my chance of dying from X. Wrong denominator, sir.
Dr. Deepti Gurdasani has some other fun nitpicks:
- The study doesn’t properly exclude Covid deaths.
- The people who die in period one are still considered ‘at risk’ in period two. Which matters because of the crazy way they are doing ratios (e.g. the study doesn’t count people who don’t die).
- The study causes a reduction in all-cause deaths for the at-risk period. Huh.
Also the Tampa Bay Times contacted four experts whose work was cited and they all say the study is obvious cherry-picked nonsense. You can’t do this.
Full study is here. It’s grade-A stupid.
It can’t fully be ignored in the sense that this is coming from the Florida Surgeon General, with the support of Florida Man (aka Ron DeSantis) who could plausibly be a future President.
In Other Covid News
Cases rising again in Shanghai. Here we go again?

You can scream ‘working from home is better’ into the void all you want. Being at the office makes you harder to fire. Being at the office tells your employer you are more serious. It is an unmistakable and large advantage over those that do not come into the office. Is that worth a commute and giving up working from home? Maybe it is. Maybe it isn’t. You still must, if given the option to go in, make a choice.
I once worked from home rather than move to where my company had its offices. As what I believe was the direct result of that, (1) my life was infinitely better, (2) I produced a lot more value for the company, and (3) I lost the political fight over who would end up running the place without realizing I had lost it. I would make the same choice over again, but my eyes would be open, and I would either make a real attempt to win those fights or accept that I would inevitably lose them and do it gracefully.
Life in China continues to look bleak. This from the NYT is the latest piece.
The most obviously jarring aspects, for me, were technological. China under “zero Covid” is a web of digital codes. At the entrance to every public space — restaurants, apartment complexes, even public restrooms — is a printed-out QR code that people must scan with their phones to log their visit. Everyone also has a personal health code, which uses test results and location history to assign a color. Green is good. Yellow or red, and you may be sent to quarantine.
Venkatesh Rao, still masking after all these years, also Arnold Kling.
Biden Administration talks about need to build biosecurity capacity in their official security strategy document (48 pages). Sophie Rose calls this ‘amazing news.’ It is better to say more generic pro-biosecurity things in such documents rather than fewer such things, I suppose. I will still reserve ‘amazing news’ for actual actions taken towards actual biosecurity, especially with Congress seeming to be unwilling to fund such activities. The most concrete thing listed seems to be ‘support the WHO’ and that also is not an organization that has been inspiring confidence recently.
7 comments
Comments sorted by top scores.
comment by Wei Dai (Wei_Dai) · 2022-10-13T23:53:17.543Z · LW(p) · GW(p)
I'm finding some of the points in the post too cryptic or assuming too much background knowledge of your thinking for me to grasp. Can you please explain a bit more or link to past relevant posts?
That’s Favreau’s third booster, because he ‘had a baby at home that was unvaccinated.’ This does not exactly capture the epistemic or cost-benefit analysis high ground.
Why not? What does current epistemic or cost-benefit analysis high ground look like?
Venkatesh Rao, still masking after all these years, also Arnold Kling.
What's the significance of this?
Replies from: Viliamcomment by Aransentin · 2022-10-13T16:28:06.588Z · LW(p) · GW(p)
We did not see a similar bump last year, so this presumably isn’t Oktoberfest.
Last year Oktoberfest was cancelled, so maybe it is?
comment by ChristianKl · 2022-10-13T18:49:41.596Z · LW(p) · GW(p)
I think the key reason that there isn't more uptick in vaccination is that the FDA make it very clear that updating the booster was very unimportant to them and that it was unimportant to give everyone who's infected Paxlovid.
If you don't recommend people to use Paxlovid when they get infected to reduce their symptoms, telling them to get vaccinated to reduce their symptoms is going to be a hard sell.
That’s definitely asking the wrong questions. I see no reason I should care about what portion of deaths are X. I care about my chance of dying from X. Wrong denominator, sir.
If people die for 10 different reasons and die at twice the rate for one of those reasons, you need a smaller sample size to detect a significant effect for the specific reason than when you look at the overall death rate. That's why most drugs that are given to prevent people from dying don't focus on overall death rates but measure the effect on a specific illness in their clinical trials.
To me, it sounds like it's a study that P-hacked a result with relatively little data.
comment by tkpwaeub (gabriel-holmes) · 2022-10-15T17:04:29.633Z · LW(p) · GW(p)
One thing I don't see talked about very much is that attempting to predict who's at risk of long covid, as a function of severity of the initial infection is very much playing to an inside straight: the illness has to be severe enough to cripple you but not kill you. It's related to the reason that long term disability insurance I'd tricky for even the best actuaries and underwriters.
comment by Lao Mein (derpherpize) · 2022-10-14T04:17:33.727Z · LW(p) · GW(p)
Currently living in Shanghai. Things are... OK? I have to do a COVID test (takes under a minute to 20 minutes, depending on how long the line is; the average is under 5.) every 3 days, and the day before I go to a hospital. While a lot of places require masking and COVID passes in theory, the only places I've seen them enforced are at work and in hospitals, where security checks your pass. No one at work wears masks, even if they're sick. Public masking is pretty rare, but then again I don't take public transit. This is the new normal, and I can see it continuing indefinitely. Also, people who can't use/afford smartphones are pretty screwed, since you need like 5 different apps to get by.
The food delivery app has the vaccination status and live body temperature of the delivery driver. I'm not sure how that's done. Still no updated vaccine that I'm aware of, despite the Red Army deploying their own in June 2020.
comment by Benya Fallenstein (benya-fallenstein) · 2022-10-16T15:21:19.234Z · LW(p) · GW(p)
I mean, that’s so damn clean. He’s citing evidence as proof there is no evidence.
Not quite the same, but similar mood: since there is no evidence, we thought we'd check if we could reinterpret the evidence to not be evidence.
Although no evidence suggests that [norovirus] is transmitted via the airborne route [9], the importance of this route has been suggested by several published reports [10]. [...]
To explore in greater detail the possibility of fomite versus airborne transmission of noroviruses, we reassessed the evidence in support of airborne transmission in a norovirus outbreak at a hotel restaurant in the UK in 1998 [21] by testing whether the alternative fomite transmission route could have led to a similar pattern of secondary cases.
The reference for "no evidence" was a CDC page that stated that "[t]here is no evidence showing that people can get infected by breathing in the virus" without discussing any evidence (the archive date on this link is within a week from when the article says they accessed the page):
http://web.archive.org/web/20170902234244/https://www.cdc.gov/norovirus/hcp/clinical-overview.html
The original article:
Xiao, Shenglan, Julian W. Tang, and Yuguo Li. "Airborne or fomite transmission for norovirus? A case study revisited." International journal of environmental research and public health 14.12 (2017): 1571.