Wrinkles
post by johnswentworth · 2019-11-19T22:59:30.989Z · LW · GW · 14 commentsContents
Why do Materials Wrinkle? Skin Layers Age-Related Physiological Changes None 14 comments
Why does our skin form wrinkles as we age?
This post will outline the answer in a few steps:
- Under what conditions do materials form wrinkles, in general?
- How does the general theory of wrinkles apply to aging human skin?
- What underlying factors drive the physiological changes which result in wrinkles?
In the process, we’ll draw on sources from three different fields: mechanical engineering, animation, and physiology.
Why do Materials Wrinkle?
Imagine we have a material with two layers:
- A thin, stiff top layer
- A thick, elastic bottom layer
We squeeze this material from the sides, so the whole thing compresses.
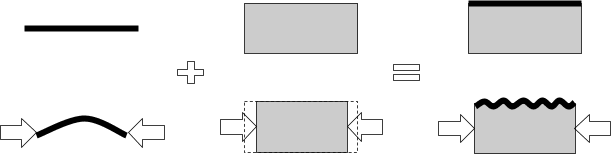
The two layers want to do different things under compression:
- The thin top layer maintains its length but wants to minimize bending, so it wants to bow outward and form an arc
- The elastic bottom layer wants to minimize vertical displacement, so it wants to just compress horizontally without any vertical change at all.
Because the two layers are attached, these two objectives trade off, and the end result is waves - aka wrinkles. Longer waves allow the top layer to bend less, so a stiffer top layer yields longer waves. Shorter waves allow the bottom layer to expand/compress less vertically, so a stiffer bottom layer yields shorter waves. The “objectives” can be quantified via the energy associated with bending the top layer or displacing the bottom layer, leading to quantitative predictions of the wavelength - see this great review paper for the math.
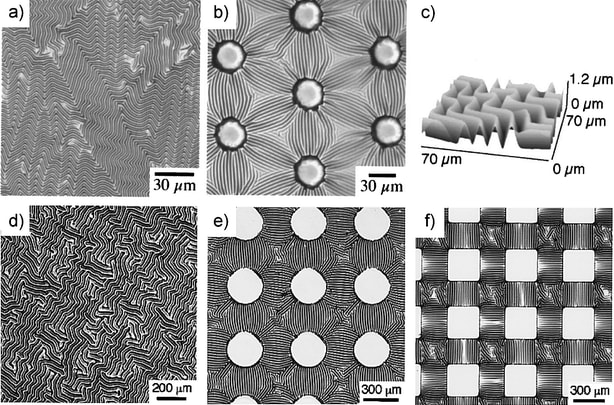
Engineers do this with a thin metal coating on soft plastic. The two are bound together at high temperature, and then the whole system compresses as it cools. The end result is cool wrinkle patterns:
Other interesting applications include predicting mountain spacing (with crust and mantle as the two layers) and surface texture of dried fruit - see the review paper for more info and cool pictures.
The same thing happens in skin.
Skin Layers
For our purposes, skin has three main layers:
- The epidermis is a thin, relatively stiff top layer
- The SENEB (subepidermal non-echogenic band, also sometimes called subepidermal low-echogenic band, SLEB) is a mysterious age-related layer, mostly absent in youth and growing with age, between the epidermis and dermis - more on this later
- The dermis is the thick base layer, containing all the support structure - blood vessels, connective tissue, etc
Both the SENEB and the dermis are relatively thick, elastic layers, while the epidermis is thin and stiff. So, based on the model from the previous section, we’d expect this system to form wrinkles.
But wait, if our skin has a thin stiff top layer and thick elastic bottom layer even in youth, then why do wrinkles only form when we get old?
Turns out, young people have wrinkles too. In youth, the wrinkles have short wavelength - we have lots of tiny wrinkles, so they’re not very visible. As we age, our wrinkle-wavelength grows, so we have fewer, larger wrinkles - which are more visible. The real question is not “why do wrinkles form as we age?” but rather “why does the wavelength of wrinkles grow as we age?”.
Based on the simple two-layer model, we’d expect that either the epidermis becomes more stiff with age, or the lower layers become less stiff.
This the right basic idea, but of course it’s a bit more complicated in practice. These guys use a three-layer model, cross-reference parameters from the literature with what actually reproduces realistic age-related wrinkling (specifically for SENEB modulus), and find realistic age-related wrinkles with these numbers:
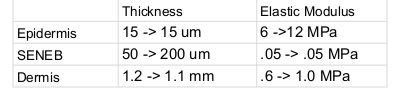
(arrows indicate change from young to old). Other than the SENEB elastic modulus, all of these numbers are derived from empirically measured parameters - see the paper for details.
Age-Related Physiological Changes
We have two main questions left:
- Why do the dermis and epidermis stiffen with age?
- What exactly is the SENEB, and why does it grow with age?
I haven’t looked too much into stiffening of the dermis, but the obvious hypothesis is that it stiffens for the same reason lots of other tissues stiffen with age. At some point I’ll have a post on stiffening of the vasculature which will talk about that in more depth, but for now I’m going to punt.
The paper from the previous section notes that the epidermis stiffens mainly due to dehydration; rehydrating the epidermis reverses the stiffening (this is the basis of many cosmetics). A dehydrated epidermis makes sense, since both the SENEB and age-related problems in the vasculature will isolate the epidermis more from the bloodstream (although I haven’t seen direct experimental evidence of that causal link).
That leaves the mysterious SENEB. What is it, and why does it grow with age?
The name “subepidermal non-echogenic band” is a fancy way of saying that there’s a layer under the epidermis which is transparent to ultrasound imaging. That’s the main way the SENEB is detected: it shows up as a space between the epidermis and dermis on ultrasound images of the skin.
As far as I can tell, little is known about the SENEB. The main things we do know:
- SENEB grows with age; see numbers above
- SENEB is found in aged skin typically exposed to sunlight (“photoaged”, e.g. hands and face) but not in hidden skin (e.g. butt).
Most authors claim that the SENEB consists of elastin deposits. That matches what we know of solar elastosis, the build-up of elastin deposits in photoaged skin. But I haven’t seen anyone systemically line up the ultrasonic and histologic images and chemically analyze the SENEB layer to check that it really is made of elastin. (This may just be a case of different researchers with different tools using different names for things which are the same.)
Assuming that the SENEB does consist of accumulated elastin, why is elastin accumulating? Well, it turns out that elastin is never broken down in humans. It does not turn over. On the other hand, the skin presumably needs to produce new elastin sometimes to heal wounds. Indeed, many authors note that the skin’s response to UV exposure is basically a wound-healing response. Again, I haven’t seen really convincing data, but I haven’t dug too thoroughly. It’s certainly plausible that elastin is produced in response to UV as part of a wound-healing response, and then accumulates with age. That would explain why the SENEB grows in photoaged skin, but not in hidden skin.
14 comments
Comments sorted by top scores.
comment by ChristianKl · 2019-11-20T12:24:34.278Z · LW(p) · GW(p)
If this would be an effective model of wrinkles, why does giving a people botox seem to remove wrinkles?
Replies from: johnswentworth↑ comment by johnswentworth · 2019-11-20T16:52:53.291Z · LW(p) · GW(p)
The wrinkle model requires compression - there has to be some squeezing from the sides. Botox kills the facial muscles which do the squeezing. (I haven't actually researched this, just an educated guess, but one reason gears-level models are important is that they let us make pretty darn good educated guesses.)
Replies from: leggi, ChristianKl↑ comment by leggi · 2019-11-20T18:48:20.128Z · LW(p) · GW(p)
Botox kills the facial muscles
No, botox doesn't "kill muscles". It paralyses muscles by disrupting nerve signals to that muscle.
"botox" uses the neurotoxin produced by the bacterium Clostridium botulinum (which also causes botulism).
I haven't actually researched this, just an educated guess, but one reason gears-level models are important is that they let us make pretty darn good educated guesses
Research is easy to do.
Guesses could be deadly when talking about neurotoxins, and definitely not appearing 'educated' in this case.
Replies from: AprilSR↑ comment by AprilSR · 2019-11-22T02:00:33.177Z · LW(p) · GW(p)
Are you sure they weren't using kill metaphorically?
Replies from: leggi↑ comment by leggi · 2019-11-22T08:19:55.296Z · LW(p) · GW(p)
I can only go on the words that are used so I'm not sure, but I didn't consider "kill" might be being used metaphorically on a rationality website.
Especially when the poster then describes it as an educated guess based on a model that lets us make "darn good educated guesses" and admits they did not even type 'how does botox work' into a search engine.
Kudos to the OP for the post but we're moving into bio-medical sciences (my background) so there are "facts" out there. Is it not better to use the knowledge that is available than making guesses?
Replies from: FireStormOOO↑ comment by FireStormOOO · 2020-03-15T22:55:28.950Z · LW(p) · GW(p)
Our model of rationalists does have to account for them being normal-ish humans who speak the language in common use around them. "Kill" is in common usage for disabling something, temporarily or permanently, without specifying mechanism; e.g. one can kill the lights or the music or wasteful spending or careless use of lanuguage on internet forums. Granted, it'd be quite prudent to avoid such use in Biology contexts. Given this is a rationality forum, what do you think is reasonable likelyhood for misunderstanding caused by sloppy use of language vs major oversights in subject matter research like you're suggesting above? I'd be very surprised if it was less than 10:1. How much does that differ from your estimate elsewhere?
[Genuinely interested in peoples' thought process during an exchange like above from a "how do we manage to talk past eachother even in a good faith rational discourse?" angle]
↑ comment by ChristianKl · 2019-11-20T23:20:00.135Z · LW(p) · GW(p)
If I understand your model, then you would predict that the facial muscle activity of older people is similar to that of younger people?
Replies from: johnswentworth↑ comment by johnswentworth · 2019-11-21T00:54:55.802Z · LW(p) · GW(p)
I would not predict that in general - loss of muscle is a major hallmark of aging, and I would expect that to have some impact. But I doubt that any age-related difference in muscle activity matters much for wrinkles.
Also, this isn't just about facial wrinkles. The same model applies to wrinkles on the hands, elbows, etc.
Replies from: leggi↑ comment by leggi · 2019-11-22T08:25:51.824Z · LW(p) · GW(p)
loss of muscle is a major hallmark of aging,
Interesting. Have you anything to back that statement up?
I don't think describing muscle loss as a major hallmark of ageing is accurate.
Muscle loss does occur as we age - likely due to lack of use, poor diet (and lower testosterone in men) since the effect can be reversed.
Replies from: johnswentworth↑ comment by johnswentworth · 2019-11-22T17:48:23.056Z · LW(p) · GW(p)
The best source I've seen on the topic is this Physiological Reviews article (I've read other sources as well, but didn't keep around links for most of them).
Reversibility is specifically addressed - age-related muscle loss (aka sarcopenia) is not really reversible. There are things people can do at any age to add muscle (e.g. exercise), but muscle is lost if exercise/diet/etc is held constant. Masters athletes are a visible example of this.
Also, it's not just skeletal muscle. For example, the pupil muscle squeezes the lens of the eye to adjust focus. In old age, that muscle loses mass, resulting in slower focusing speed. (Source: Physiological Basis of Aging and Geriatrics; the chapter on the eye is one of the best in the book). And of course there's loss of muscle mass in various sphincters, resulting in e.g. incontinence and other digestive problems. None of those muscles are suffering from lack of use.
Replies from: ChristianKl, leggi↑ comment by ChristianKl · 2019-11-22T23:05:07.645Z · LW(p) · GW(p)
Exercise increases the size of individual muscle cells but not their number. When muscle cells die it doesn't replenish them.
↑ comment by leggi · 2019-11-23T08:52:03.242Z · LW(p) · GW(p)
Looking into the term sarcopenia (I avoided it earlier as it seemed inconsistently used and I was getting confused mass +/- function loss) here's some snippets and thoughts.
Article In his closing comments to a scientific congress in 1989, Dr. Irwin Rosenberg suggested that one way to bring greater attention to the issue of the decline in muscle mass with ageing was to give it a Greek name. Although two terms were suggested (“sarcomalacia” being the other one), “sarcopenia” was the term adopted by the field ...
unfortunately in recent years the term has increasingly come to be synonymous with its operational definitions ... the term sarcopenia is appearing in other clinical literature in which muscle atrophy is present but ageing per se is not the cause.
Among the most widely observed histological features of ageing muscle is its remarkable fiber size heterogeneity.
... the available evidence strongly implicates sporadic and repeating cycles of denervation-re-innervation in the histopathology of ageing muscle
Primary loss of muscle mass versus secondary loss of muscle mass after loss of innervation - paresis/paralysis - loss of function - atrophy. From what I've read sarcopenia is a secondary loss of muscle, and I'd classify sphincter incompetence as an innervation issue rather than a primary loss of muscle mass issue. No idea if/what the significance of distinguishing between primary and secondary is but something to be aware of.
Fascinating subject, my initial comment was poorly worded/wrong depending on what age "ageing" begins - I was thinking 30+ where loss of muscle may be noted but reversed (quickly found article) but by 60+ sarcopenia with strict definition occurs. Another article I found: sarcopenia v. non-sarcopenia.
(Just enjoying being able to interact on LW as so much stuff goes straight over my head!)
Replies from: johnswentworth↑ comment by johnswentworth · 2019-11-23T17:02:57.329Z · LW(p) · GW(p)
One of the main questions I haven't found a satisfying answer to yet is whether denervation/renervation is causal for sarcopenia. Apparently a huge amount of resources went into imaging neuromuscular junctions for a while - the physiological reviews article I linked spends half the article on the topic - but that seems to be driven by historical accident more than anything. After wading through a ton of it I still haven't seen any decisive evidence on whether denervation is the main cause of muscle atrophy, or muscle atrophy causes nerve atrophy. It sounds like either is sufficient to cause the other experimentally, but it's not clear which actually comes first in aging. (And of course research is made difficult by authors sometimes making statements about causality which their data/experimental procedure doesn't actually establish.)
comment by Vaniver · 2019-11-20T22:43:12.175Z · LW(p) · GW(p)
So, if elastin buildup is causing wrinkles, then do treatments that reduce wrinkles (like salicyclic acid) reduce elastin?
It seems no, they probably increase elastin production, and are thought to reduce wrinkles because they increase production of other things (like collagen) as well. [I note this is a pretty big inference from that one study, and I'm trusting more in the fact that I first came across that claim when trying to discover the link between the two.]