What are good resources for gears models of joint health?
post by Randomized, Controlled (BossSleepy) · 2021-06-06T17:39:50.303Z · LW · GW · 36 commentsThis is a question post.
Contents
Answers 7 ChristianKl 1 George None 36 comments
Painscience.com and Hargrove's "A Guide To Better Movement" are pretty good for a model of predictive processing and the roll of the nervous system in chronic pain and movement. I still don't feel like I have a good model of bone and joint health in general, however. Eg, I'm currently nursing a flare up of patelo-femoral pain in my left knee. I've done a number of things over the past few months to deal with it, with some success, including buying and reading Painscience's book length patelo-femoral tutorial. Recently I've had a bit of pain in my foot, possibly in the tibiocalcaneal or tibionavicular tendons. I find that even though I now know a fair amount about PFS and the way the nervous system processes pain, these models don't generalize well to sporadic, idiopathic pain in another joint.
Possibly the answer is: "lol that model doesn't exist", or "lol wanna get a phd?" but if there are good resources, I'd be an eager consumer.
A sub-question that I'm particularly interested in is: what, if anything, is know about the relationship between base line muscle tone and joint issues? I have good reason to think my baseline muscle tone is higher than average.
Answers
A lot of my related knowledge comes from in person teaching and not from reading books, so I unfortunately can't point you to specific sources for everything.
The best related research does come these days from the people that gather around the Fascia Research Congress. A few Rolfers like Robert Schleip and Thomas Myers decided to give academic science a go and across bodywork discipline and related academia the Fascia Research Congress is the central venue for going beyond the methologies of individual disciplines.
Tense fascia leads to high muscle tone and that can then make individual body parts tense enough to hurt. When the problem travels between different parts of the body that's often what's happening
From that point it frequently also happens that you get inflammation in that body part which produces additional issues.
As humans age, bones in various joints grow which results in a loss of flexibility. It might be that this isn't true for a hunter gatherer who uses his joints a lot more then the average Westerner but bone growth does reduce flexbility of joints as people grow older.
Cartilage like the meniscus for the knee often gets thinner over time which produces joint problems. The old fashioned belief is that such cartilage doesn't grow back. These days we have research at the leading edge that suggest that sometimes some cartilage grows back but we don't have good models about it.
Various other illnesses also lead to joint problems. Lymn disease for example can produce joint pain.
↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-07T00:14:58.458Z · LW(p) · GW(p)
Fascia Research Congress. A few Rolfers like Robert Schleip and Thomas Myers
I'll look into the Fascia Research Congress and these two!
Tense fascia leads to high muscle tone and that can then make individual body parts tense enough to hurt. When the problem travels between different parts of the body that's often what's happening
Does that suggest that trigger-point release, various forms of massage and something like Paul Ingraham's mobalization prescription are good starting places?
From that point it frequently also happens that you get inflammation in that body part which produces additional issues.
Any suggestions how to tell if you have inflammation and what to do if you do? Ingraham's Patella Femoral Syndrome tutorial is basically a book disquisition about low-level systemic inflammation in the knee cap, and his prescription is: lots and lots of gentle rest. He suggests the knee cap may be an unusual joint in that it it's under a lot of pressure even if just sitting still with a knee bent at 90 degrees, so recovery can be hard, but I'm guessing "lots of rest + standard PRICE treatment" is the typical prescription for other inflamed joints?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-06-07T01:11:09.417Z · LW(p) · GW(p)
I'll look into the Fascia Research Congress and these two!
Thomas Myers wrote Anatomy Trains two decades ago which is a text book that was important for giving the field form. At that time it was state of the art. The general concept of myofascial meridians is a very useful gearmodel. On the other hand it's two decades old and I have been told that a lot of the book is outdated and Myers himself is not a person who's good at updating.
Robert Schleip is these days seen more as an authority.
Any suggestions how to tell if you have inflammation and what to do if you do?
Inflammation generally means that the knee starts hurting when you use it and it starts hurting more when you use it more. It's worth noting here that a torn muscle can also hurt if you put pressure on it. Infortunately, I can't tell you much more here.
Inflammation does mean that the joint needs rest but it's important to move enough to not get more stiff. Ibuprophen can also reduce inflammation. In December after just being inside for a few weeks I went walking and put too much stress on my new. A week of Ibuprophen was what my aunt who's a normal doctor recommended.
But that wasn't "low level inflammation". When it comes to "low level inflammation" I think it's hard to know what's going on. When it comes to fascia or muscles you have osteopaths you have good feedback loops to understand the effects of their actions by feeling with their hands what happens. When it comes to "low level inflammation" that's a model that you can't directly feel with your hands and thus while bodyworkers might have a theory about it being a cause, they don't have feedback processes to validate that theory.
While the theory of "low level inflammation" is plausible it's from my perspective problematic that the people talking about it don't have good ways to know whether they are right or wrong.
It's similar to how Todd R. Hargrove is someone who gathered the knowledge he has primarily through feedback loops involves movement and is therefore more trustworthy when he says "I you do these movements, that happens" then when he speculates about what the involved neurons are doing.
It's always good to ask yourself in a field like this where a lot of knowledge doesn't come out of traditional academia how people know things and whether they are exposed to feedback loops that allow them to know what they are talking about.
Does that suggest that trigger-point release, various forms of massage and something like Paul Ingraham's mobalization prescription are good starting places?
My personal experience with messages by people trained in physiotherapy is that they often don't produce latesting effects, but it depends a lot on the skill level of the person and message is a fairly broad term.
A lot of people who do have skill trained in some particular methology that's not globally available. What's globally available is osteopaths who are generally well trained.
I don't have much experience with trigger-point release myself nor talked about it with someone who understands how things work. If you do observe that it's a way you can reduce your body tension over periods that are more then a few hours then it's something in favor of it but it seems very indirect to me.
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-07T15:00:43.166Z · LW(p) · GW(p)
It's similar to how Todd R. Hargrove is someone who gathered the knowledge he has primarily through feedback loops involves movement and is therefore more trustworthy when he says "I you do these movements, that happens" then when he speculates about what the involved neurons are doing.
Are you skeptical of the central nervous system sensitization pain mechanism?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-06-07T15:29:06.163Z · LW(p) · GW(p)
My general prior is to be skeptical of most neuro-based explanations for phenomena outside of neuroscience. Hypothesis might be true, but it's very hard to check whether they are true. I generally prefer knowledge that's backed by empirics over knowledge that rests on assumptions about understanding of how a black box works internally.
If your problem is personal, i.e you're dealing with joint issues, unless you're suffering from a muscle-wasting disease or are over the age of 50, reading about stuff will be low yield.
Long term joint pain is solved by:
- strengthening muscles in order to not put a strain on "weak" joints [evidence: solid]
- Hormetic effects joint usage [evidence: weak clinical, but look at e.g. people doing yoga, I'd say this is an issue of people not studying the correct demographics]
- Zone 2 training, aka cardio, allowing you to more efficiently partition fuel to muscles and thus do more movement without suboptimal muscle usage [evidence: I'd assume moderate but unsure]
- Stability training [evidence: not good because everyone disagrees what exactly this involves, but basically all physiotherapists are doing some form of stability training so it's obviously useful | overall you can pick a specific older technique and you will get solid evidence, but newer stuff might actually be better, but less tested]
Now, can you optimize past that? Sure you can.
But unless you are already doing, say, 2 hours of zone 2 4-5 times a week, 30 minutes of resistance training 2-3 times a week (the kind where you are in excruciating pain by the end, i.e. proper resistance training not aerobics masquerading as resistance training), 20-40 minutes of daily stability training (could be morning yoga, could be stretching recommend by a therapist, could be whatever).
Then reading up on joint pain will be useless.
It may be that you are an athlete, in which case discount the above, if you're doing 4-6 hours of effort per day on average then a better model of movement is probably the key. But even then it might make more sense to take a scientific approach and just try different things and be quick to quantify (e.g. don't look for joint pain after trying a new style of movement, look for proxies in your blood).
But again, if you're not an athlete, by reading up on this stuff you are simply running away from the real solution, which involves the hard work of building a pattern of 1-2 hours of varied exercise every day.
↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-19T22:54:37.114Z · LW(p) · GW(p)
Stability training [evidence: not good because everyone disagrees what exactly this involves, but basically all physiotherapists are doing some form of stability training so it's obviously useful | overall you can pick a specific older technique and you will get solid evidence, but newer stuff might actually be better, but less tested]
I did a little quick searching for "knee stability training protocol" and.. found a few things that looked pretty obvious. Quads, hams, calves, etc. More or less what I'd expect. I don't suppose you have any secret sauce beyond that?
resistance training 2-3 times a week (the kind where you are in excruciating pain by the end, i.e. proper resistance training not aerobics masquerading as resistance training),
Ie, "train to failure"? If so, I was under the impression that training to failure is now considered less effective/useful.
(e.g. don't look for joint pain after trying a new style of movement, look for proxies in your blood).
I'm not an athlete, but what would the proxies be?
Replies from: George3d6↑ comment by George3d6 · 2021-06-21T09:06:42.644Z · LW(p) · GW(p)
I did a little quick searching for "knee stability training protocol" and.. found a few things that looked pretty obvious. Quads, hams, calves, etc. More or less what I'd expect. I don't suppose you have any secret sauce beyond that?
No, it's really very much about your individual body and where you have lacks, you need an in-person trainer to be able to see this and over time as you move more you'll become more aware of your body and be able to say "Ah, it's x area that's too stiff, or activating too much, or that should be working but isn't or whatever"
Ie, "train to failure"? If so, I was under the impression that training to failure is now considered less effective/useful.
No, training to failure is a bad idea in that it's both unhealthy (muscle injury, joint issues) and unideal for muscle growth. But from the perspective of most people "training to failure" is actually "training to a few reps close to failure" because outside of people that are fairly advanced it's close to impossible to push yourself to the gun-to-the-head limit. If you want you can try "train until your form fails and you pinky-promise are unable to keep it no matter what", and realistically that should suffice.
I'm not an athlete, but what would the proxies be?
standard markers of inflammation, ESR, CRP, etc. Or you could even look for the curve of cortisol response and clotting factors with a venous catheter, I guess. But again, not at all relevant outside of an academic curiosity unless you are training to be an athlet (which is unhealthy and should be avoided).
Replies from: BossSleepy, BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-22T17:53:13.625Z · LW(p) · GW(p)
standard markers of inflammation, ESR, CRP, etc. Or you could even look for the curve of cortisol response and clotting factors with a venous catheter, I guess. But again, not at all relevant outside of an academic curiosity unless you are training to be an athlet (which is unhealthy and should be avoided).
Are you implying I shouldn't [overly] worry about chronic inflammation? I'm pretty confident there is an inflammatory component here -- icing and voltaran do seem to help. It's been long enough (3 months) that I've started to think about trying a curcumin supplement and/or just cooking with tumeric+black pepper a bunch.
Replies from: George3d6↑ comment by George3d6 · 2021-06-24T22:15:56.713Z · LW(p) · GW(p)
Oh, not at all, chronic inflammation could be a thing.
I'm just saying that tracking how your exercise routine affects chronic inflammation is a very min-maxy type of things.
Chronic inflammation could very much be a macro problem that leads to joint pain.
Did you already test basic stuff? Like immune cell counts, homocysteine, uric acid, CRP, fibrinogen, ASLO blah. Basically, a standard blood panel an obsessed GP would give you? If not I'd certainly start with that.
I mean, for all you know this thing could be caused by eating too much meat, or gluten intolerance, or whatever (not saying those reasons are especially likely, just examples of "dietary problem that is easily caught on tests and can be easily resolved)
↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-22T00:42:45.340Z · LW(p) · GW(p)
No, it's really very much about your individual body and where you have lacks, you need an in-person trainer to be able to see this and over time as you move more you'll become more aware of your body and be able to say "Ah, it's x area that's too stiff, or activating too much, or that should be working but isn't or whatever"
Thank you for the info! Do you have any thoughts on how to evaluate a trainer's ability to discern this sort of thing? I'm happy to work with trainers and pay for expertise, but my general sense is that standards of research in sports medicine aren't great.
36 comments
Comments sorted by top scores.
comment by leggi · 2021-06-13T05:45:57.662Z · LW(p) · GW(p)
sporadic, idiopathic pain in another joint.
Can I clarify before I spend time writing a long answer - You are looking for a model that explains why you've now got pain in your foot (with a history of knee pain)?
If that's what you want to know, it's not complicated - pain spreads over time.
How I'd briefly explain things:
We alter position to avoid pain.
Positional changes alter the stresses throughout the body (we are connected from head to fingers to toes).
Stresses are unevenly distributed when the body is not in an ideal posture.
Alterations due to pain = not good for posture.
Poor posture = Pain.
One problem area spreads to another as the body keeps adjusting to avoid pain.
https://www.lesswrong.com/posts/gfYdtiJXFXxGeLd9X/a-good-posture-muscles-and-self-awareness [LW · GW]
I've written a fair bit about muscles, connective tissues and pain in this post [LW · GW].
I could write specifics about knee pain if want.
Otherwise, some good resources:
Basic bone physiology, pathology:
http://www.cldavis.org/woodard_bone/text/1_1.htm (veterinary - think "mammalian")
http://www.cldavis.org/woodard_bone/text/4_1.htm
https://www.patellofemoral.org/pfoe/index.html
https://www.anatomyumftm.com/knee
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295692/
↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-13T17:27:55.726Z · LW(p) · GW(p)
Can I clarify before I spend time writing a long answer - You are looking for a model that explains why you've now got pain in your foot (with a history of knee pain)?
Yup.
I'm also looking to better understand my PF pain.
Poor posture = Pain.
I'd say I'm somewhat confused about this model, based on a reasonable amount of reading. Paul Ingraham, Todd Hargrove and Greg Lehman all point at a lot of clinical evidence that postural and structual models of pain aren't very explanatory, which I think can be 80% pithy sumerized by "there are lots of cases where people have pain in tissues that appear healthy and no pain in tissues that show visible, gross lesions and other damage." I've been working a health coach for the past few months who seems smart and well meaning -- they recommended I make some (reasonably subtle) gait adjustments to help externally rotate the femur while walking. I was quite skeptical of this theory, but I've come across the cue before (ie, to try to emphasize the outer edge of the foot more than the inner), and I've been good-faith trying it to see what happens. I'm about 60% confident that this gait alteration may be involved in the ideopathic footpain -- I've had PF pain flairups before, but never ran into this foot tendon/ligament issue.
Thank you for the resources, I'll definitely spend time with those.
Replies from: leggi↑ comment by leggi · 2021-06-14T11:45:02.844Z · LW(p) · GW(p)
I hesitate to use the word "posture" due to the various models it conjures in people's minds (slouching, pictures of the spine etc.) Put these images aside for a moment.
Posture = Position of the body.
All the body, at any time.
Good posture = good positioning - the body works well.
Poor posture = bad positioning.
(Bad positioning could be structural or due to inappropriate usage)
Bad positioning is bad for moving parts. Inappropriate tensions, misalignments, friction, stress.
Bad things in the body - detected by sensors, information transmitted by nerves, brain says PAIN!
The body adapts over time. Pain progresses if bad positioning is not corrected.
(One adaptation I propose - physical restrictions in connective tissues form in a response to inflammation, which can be triggered by a multitude of things. Over time these restrict range of movement, apply tension, generate pain. The body is very adaptable. It can take a lot of stress and abuse. The mind can ignore a lot of pain signals. An individual's awareness levels and tolerance affects when issues are noted/treatment is sought i.e. become clinically significant.
I'm about 60% confident that this gait alteration may be involved in the idiopathic foot pain
This is a good example of what I mean by "poor posture" causing pain. Gait alteration = changing how you move = altering posture/position. If these alterations have resulted in pain, I'd classify it as postural pain i.e. pain due to poor positioning.
Consciously changing your gait involves the activation of different muscle fibres to what you have been using. Either this is "corrective" (improving positioning with activation of the 'right' muscle areas) or it's detrimental to positioning with increased use of the 'wrong' areas of muscle (causing stress on muscles and a progression of issues. Myalgia, spasms, fatigue, trigger points → tensions in tissue, pulling on periosteum "joint pain" which stimulates bone remodelling/osteophyte formation ... )
If you are at 60% in thinking a gait change and your foot pain are connected, then I hope you'll give real consideration to my model for otherwise unexplained pain. (I've taken a very sudden active dislike to the word idiopathic, it's not idiopathic pain - anymore.)
My model fits with all the information I've seen over the years - quote and link to any studies you find relevant and I'll explain how. I joined LW with a "please rip to shreds" about my Base-Line theory of health and movement so please do! I am p>99.999 confident that what I propose is right. I'd like that rigorously tested. Break me, crush me. Release me from the frustration of knowing (with every fibre in my body) that I'm right ; )
I'm also looking to better understand my PF pain.
Keep studying the anatomy.
Focus on where the pain is coming from. Deep breathing, explore with your mind.
Bear in mind, dissection photos of pre-prepared specimens are usually designed to demonstrate components rather than showing the natural state of a joint. Schematic diagrams are just that, ligaments look like strings or ribbons crossing joint spaces at specific points, they don't show that most connective tissues aren't discrete parts, they blend from one named structure into another. Ligaments being thickened bands within a web of connective tissues around a joint, closely associated with fascia, joint capsule and periosteum, which then blends to tendons and aponeuroses to connective tissues containing myocytes ("muscles").
Have a look at dissection videos of the knee joint. (preferably fresh rather than pickled tissues). After removal of the skin it's obvious how much of everything is encased in connective tissues - a bright white 'bandage' of fibrous tissue (mostly collagen). The ligaments of the knee are thickenings in this web of connective tissue. A bit of tension somewhere pulls on surrounding areas.
The experience of handling a (skinned) knee brings another level of understanding. Seeing the layers. Feeling where bits attach tightly to bone. Feeling the bits that glide as the knee flexes and extends. The change in tension of various thickenings in the tissues around the bones. The trochlear groove for the patella. There is much to experience. Goat or sheep knees (known as the stifle) are a reasonable approximation if you do want to really get to know the knee.
The joints of the leg - hip, knee, ankle, foot offer a lot of potential for movement. The knee joint is mostly extension/flexion, it has very little medial/lateral movement - there is almost no slack. Any issues above or below the knee (rotations, tensions etc. from the hip/ankle/foot which put the leg in a less than ideal position) will show first in the knee. (The hip and ankle/foot have much more slack so can cope for longer with mal-positioning/misusage but it will appear with poor positioning).
This has good rather long and I'm out of time, but if you are interested - I could run through a diagnostic process for knee pain.
Replies from: ChristianKl, BossSleepy↑ comment by ChristianKl · 2021-06-21T23:05:37.185Z · LW(p) · GW(p)
I am p>99.999 confident that what I propose is right.
Stating that you are 9999,9% confident that a theory is right, isn't a signal that you know what you are talking about. Even if you would say p>0.99999 (which equals 99,999%) that's still a signal for not being well calibrated because having that kind of certainty for that class of statements is incredibly hard to achieve.
Replies from: leggi↑ comment by leggi · 2021-06-22T13:41:07.966Z · LW(p) · GW(p)
Well blushing a lot at my typo. I went from % to <p> and apparently forgot about the decimal point.
I'm not one to put numbers on things but it's popular on LW and my fingers spat it out as I was typing.
I am certain.
I've never been so certain of anything in my life.
What confidence level would be acceptable?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-06-22T13:46:29.113Z · LW(p) · GW(p)
I've never been so certain of anything in my life.
You are more certain of that then the sun going up tomorrow?
Replies from: leggi↑ comment by leggi · 2021-07-03T09:58:54.409Z · LW(p) · GW(p)
I expect the sun to come up tomorrow, I am confident it will, but I am not certain of any future event. There's plenty of time between now and then for things (however improbable) to occur that mean the sun doesn't come up.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-07-03T11:39:21.548Z · LW(p) · GW(p)
That doesn't answer the question of how the certainty of the two events relate to each other.
Replies from: leggi↑ comment by leggi · 2021-07-03T12:32:03.495Z · LW(p) · GW(p)
There's not much in it but - based on my experiences and the anatomical facts - I am more certain about Base-Line Theory of Health and Movement that I am about the sun coming up tomorrow. There I've said it. It's what I believe. That strongly. Even so, I would be willing to change my mind and that's why I persevere with looking for feedback.
Have you ever found the 5 main muscles on your body and given some thought about how they are functioning?
Replies from: BossSleepy, ChristianKl↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-05T21:30:44.955Z · LW(p) · GW(p)
There's not much in it but - based on my experiences and the anatomical facts - I am more certain about Base-Line Theory of Health and Movement that I am about the sun coming up tomorrow. There I've said it. It's what I believe. That strongly. Even so, I would be willing to change my mind and that's why I persevere with looking for feedback.
I'd also say that, just on a basic level, this is poor calibration. I would put "sun doesn't rise tomorrow" at... 1 in 10 million? 1 in 100 million? Maybe those are even too high, 1 in 10 million events do happen with some frequency, but maybe I'm just fundamentally deluded about the nature of reality right now. If my understanding of history and physics isn't completely borked, I'd be comfortable pushing that probability down to below 1 in a billion or lower.
I'm also comfortable predicting at 90% certainty that a majority of other LWers would also have probabilities for sun-doesn't-rise tomorrow below 1 in 1 million.
These are.. like.. real brute facts about reality kinds of things. General relativity. Newtonian mechanics. QM. Nuclear physics. That's the kind of foundation you can build 1 in 100 million-ish certainty on. Stuff with biology is in an entirely different realm of (un)certainties.
Replies from: leggi↑ comment by leggi · 2021-07-06T09:00:54.623Z · LW(p) · GW(p)
I agree, biology is a realm of uncertainties. The wonder of how living organisms function blows my mind. The level of complexity phenomenal.
However, anatomy is much more fixed. Grossly examinable and recordable. Studied in detail for hundreds of years. We have accurate atlases of how the body is put together, what attaches where....
Anatomy can be complicated (I've very much skipped over a lot of details about the pelvic floor muscles and connective tissue structures) and individual variations are seen, but there is much more certainty about how we are put together than biology as a whole.
I know I am right. It has taken a lot for me to get to the point of saying that out loud. Question everything has been a motto of mine for a very long time - and it will always be with me. But I feel how I feel, and accepting that feels right - especially having facts and logic on my side (IMO at least - please someone look at the anatomy!).
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-06T16:09:05.299Z · LW(p) · GW(p)
However, anatomy is much more fixed. Grossly examinable and recordable. Studied in detail for hundreds of years. We have accurate atlases of how the body is put together, what attaches where....
Anatomy may be more or less fixed, but our understanding of it is definitely much more fluid, and it seems possibly still pretty incomplete: apparently we've recently discovered enough new gross anatomical facts that an overview article was published on them in 2019.
I know I am right. It has taken a lot for me to get to the point of saying that out loud.
Putting aside the issue of levels of certainty here, I'd agree with ChristianKl that I'm a bit unclear what the implications of your model are, except perhaps, "pay attention to your posture and movement" which I already do a fair amount.
Replies from: leggi↑ comment by leggi · 2021-07-07T10:36:26.084Z · LW(p) · GW(p)
From the link you provided:
"A very recently reported third discovery demonstrated a previously unknown tissue component-'interstitium'-a networked collagen bound fluid-filled space existent in a number of human organs."
I read that and thought:
"What? The interstitium? I learned about that 30 odd years ago. Wasn't that one of the things I had to label when sketching from a histology slide, wow that was so long ago .... "
What has been recently noted and publicised is the interstitium in its form in living tissues. From this article:
The researchers said these fluid-filled spaces had been missed for decades because they don't show up on the standard microscopic slides that researchers use to peer into the cellular world. When scientists prepare tissue samples for these slides, they treat the samples with chemicals, cut them into thin slices and dye them to highlight key features. But this fixing process drains away fluid and causes the newfound fluid-filled spaces to collapse.
Histology 101. Tissues are distorted when prepped for slides. I was taught that at vet school (if not before). I'd assumed / never thought about it, that it was common knowledge amongst medical folks.
I've handled a lot of 'fresh' mammalian tissues (canine, feline, bovine, equine, ovine, caprine and various others). I'll go out on a limb and say it's all the same stuff - bone and muscle fibres all wrapped and blended in a web of connective tissues ... in humans too. (This could be a major error. I've not handled enough human flesh to really know....)
Seeing live/freshly dead tissues, feeling them in your hands, is a very different experience from learning from a textbook, histology slides or studying bodies prepared for dissection. They can't compare in giving understanding of how a body is put together, of what it really consists of. These experiences give me lot of confidence in what I say about the role of connective tissues, also the knowledge that defining and delineating is very difficult so I'm sticking to the covering term of 'connective tissue' which I wrote a bit about here [LW · GW]. I don't know the precise pathology of 'physical restrictions in connective tissues'. (Is it collagen fibres cross-linking? Is it interstitial components hardening from fluid to gel to the palpable lumps I can feel subcutaneously? Is it a combination of many factors?!) A good question is how to sample and examine these tissues without distortion.
Putting aside the issue of levels of certainty here,
Phew, much appreciated. : )
I'd agree with ChristianKl that I'm a bit unclear what the implications of your model are, except perhaps, "pay attention to your posture and movement" which I already do a fair amount.
I've been side-tracked by "posture".
My model is about learning to use your body better. I believe the 5 main muscles of movement are key to this, leading to:
- Better physical health.
- Better mental health.
- Less pain and tension in the world.
The level of knowledge about the structure and location of the anatomy I share is at a sufficient level for me to use the word "fact" ( grinding my teeth as I type this, I don't like to use "fact" for anything).
Muscle tissue blending with connective tissues is very hard to describe in full detail but, ignoring the pelvic floor for a minute, the other 4 main muscles are big and easy to palpate. We know their attachment points to bone and connective tissue structures (minor variations in individuals have been noted and no doubt there are more that have not).
The is enough information for someone to find the muscles on their own body, to touch them and increase conscious awareness of them.
There is much still to learn, to put together, to figure out. I believe Base-Line Theory increases understanding of how we could better use our bodies, of why there is so much unexplained pain -and how to fix it.
As a simple experiment if you are willing, find the 5 midline markers [LW · GW]and feel for their relative positioning. As you move through your day, pause to take a few deep breaths and try to be more aware of your midline anatomy. Use it as a reference for the positioning of the rest of your body. See how it feels, what you experience.
Thank you for the interaction! It's very useful.
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-19T02:31:38.490Z · LW(p) · GW(p)
Hi. Apologies for not following up sooner -- my dad's been in the hospital.
Muscle tissue blending with connective tissues is very hard to describe in full detail but, ignoring the pelvic floor for a minute, the other 4 main muscles are big and easy to palpate. We know their attachment points to bone and connective tissue structures (minor variations in individuals have been noted and no doubt there are more that have not).
The is enough information for someone to find the muscles on their own body, to touch them and increase conscious awareness of them.
Okay. Abs, butt, quads, traps. I'll try being more mindful of those, and see if anything suggestive appears. But I also feel like Dr Scott Dye's failure-of-homeostatis model is more specific to what I'm going through ATM, and gears-y and prescriptive.
Seeing live/freshly dead tissues, feeling them in your hands, is a very different experience from learning from a textbook, histology slides or studying bodies prepared for dissection. They can't compare in giving understanding of how a body is put together, of what it really consists of. These experiences give me lot of confidence in what I say about the role of connective tissues, also the knowledge that defining and delineating is very difficult so I'm stic
This honestly sounds amazing. Is there a way for a civilian to get access to large mammal [human?] dissections? I'm assuming med schools don't just let you enroll in a single course or audit the anatomy offerings?
Thank you for the interaction! It's very useful.
Thank you for your engagement : )
Replies from: leggi, leggi↑ comment by leggi · 2021-07-21T11:23:15.244Z · LW(p) · GW(p)
Some comments on Dr Scott Dye's failure-of-homeostatis model:
I read the abstract "Patellofemoral Pain: An Enigma Explained by Homeostasis and Common Sense" and found myself nodding along...
overload and/or injury produces pain. Bone overload and synovial inflammation are common sources of such pain.
Patience and persistence in nonoperative care results in consistent success. Surgery should be rare"
I agree with all that. I'd classify it as common sense as they say in the title.
But after reading the article a couple of times I don't feel the authors were saying anything new.
Our Hypothesis: Loss of Homeostasis Causes Pain
We hypothesize that pain is the result when load applied to musculoskeletal tissues exceeds the ability to maintain homeostasis. Loss of tissue homeostasis from overload and/or injury produces pain.
Overload/injury = stresses beyond tolerable levels --> damaged tissues & inflammatory processes,
which the authors are describing as "loss of homeostasis". The use of "homeostasis" feels unnecessary.
Injury/overload = damage. simples.
However, the inflammatory processes are anything but simple. Inflammation is a rabbit hole I avoid looking to deeply into, I'd be lost for a very long time!
Pain anterior knee. —a consistent set of symptoms, signs, and test results—that does not exist.
I agree with this, and it happens to fit with my 'individual trauma imprint' explanation for pain-related symptoms. What our bodies have been subjected to, the damage sustained. With innumerable positions the body has a massive capacity for adaptation. As damage builds up, patterns of symptoms will emerge throughout the body but we're all a bit different.
Emotions play a role in pain as well, and somatization resulting in knee pain is a well-known phenomenon, particularly in adolescent women related to stress or even abuse.
I checked the article's references for more details about somatization but found nothing listed. (I also noted the references are mostly to other articles by the authors.) Whilst I do believe emotions and the physical body are intertwined, this statement feels more like a dismissal of knee pain when reported by the young and female. Adolescent women being told "it's all in your mind" when nothing shows on exam or standard imaging. I wonder how often adolescent men with knee pain are told it's due to their emotions too, or do they get a "diagnosis" of patellofemoral something or other? I didn't find anything to back up this as a "well-known phenomenon".
I say: The knees are joints that are under a lot of stress with little slack so problems appear here first when the body is not aligned and fully balanced. Stress/abuse affects positioning of the body.
Poor positioning can be subtle but it takes its toll. Knee pain - slight adjustments in the joints above and below i.e. hip and ankle to avoid the pain. It affects the whole leg, which then affects the body-whole over time. The body is very adaptable, able to cope with a lot of misusage and abuse but the imbalance and misalignments are cumulative.
The treatments listed: activity modification, cold therapy, anti-inflammatories, physical therapy. are (or at least should be) standard protocols. I'm cringing at the thought that surgery might be pushed in some parts of the world (without good reason), and thankful I wasn't prescribed opiates as a teenager.
I was going to comment more on cold therapy but I thought I'd check some things I'd always been told, turns out it's an another rabbit-hole to go down.
https://www.physio-pedia.com/Cryotherapy
https://thesportjournal.org/article/the-r-i-c-e-protocol-is-a-myth-a-review-and-recommendations/
Cold - good or bad? It does numb the area for a while but what's the deeper effects on the tissues...
↑ comment by leggi · 2021-07-19T13:44:24.002Z · LW(p) · GW(p)
I hope your Dad is doing OK. No worries with timeframes - less than immediate responses are one of LW's strengths IMO.
Abs, butt, quads, traps. I'll try being more mindful of those,
Fricking awesome! Feel for positioning, freedom to move, and balance in left and right. Just to expand a little ...
abs. All good. Imaging extending the linea alba between the rectus abdominis every in-breath. Pubic symphysis to sternum.
butt. fair enough. Big ass muscles - gluteus maximus.
quads. What makes you say "quads" here? It would be very useful for the insight. Focus on the rectus femoris, shin to hip bone. The quadriceps share a distal insertion (common ligament of quads.-patella-patellar ligament-tibial tuberosity) but the rectus femoris is only one of the quads to cross both hip and knee joints. image here. or in the post main muscles made easy [LW · GW]. I think of the rectus femoris as the guide muscle of the quadriceps, positioning the leg so the 3 vasti muscles 'fall into line' (I don't like that phrase - but have nothing better).
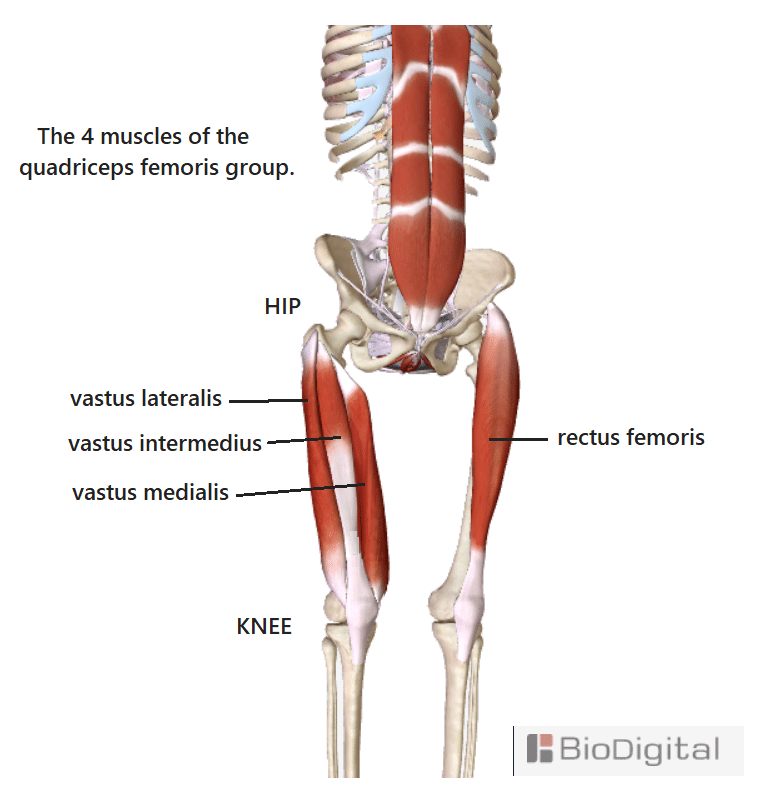{kind=link}
traps. Excellent. The trapezius muscles should free to support the head and arms through a full range of movement. Movement starting from lower trapezius.
(coughs) Pelvic floor. The base foundation of the body.
It would be useful to me to know how much is "the pelvic floor muscles being important" common knowledge here?
This honestly sounds amazing. Is there a way for a civilian to get access to large mammal [human?] dissections?
Commenting here got me thinking about who has the opportunity to handle really really fresh tissues like I've had. It's not a long list: Anyone who turns animals into meat. Anyone performing autopsies on the freshly dead. Euthanasia and immediate post-mortem is possible in the veterinary world but human corpses are likely to be older when examined and it doesn't take long (1-2 hours) for connective and adipose tissues to change consistency - temperature and humidity dependant. A certain class of serial killer (skip over that one). Anyone who turns animals into meat. Surgeons, especially those dealing with mass trauma injuries. Removing dirt out of fuzzy connective tissues is a bitch...
I imagine most human dissections aren't fresh enough to really appreciate "live" tissues. So, how to get in on the action? If you can find a farmer/small-holder type willing to let you watch a butchering, a hunter that processes the carcass, a fresh meat butcher. Or a friendly large animal/equine vet that's willing to call you when the chance to do a fresh post mortem arises.
I've been fortunate with the opportunities I've had to increase knowledge and understanding of mammals 'in the flesh', something I appreciate a lot more now that I've stopped to think about it.
I have quite a lot to say about the link you provided, so will be back with a separate comment. Have you worked through "DAMN-IT" (from one of my previous comments) and seen where that gets you?
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-19T16:09:35.664Z · LW(p) · GW(p)
I hope your Dad is doing OK.
He's dying. Likely going into palliative soon.
I have quite a lot to say about the link you provided, so will be back with a separate comment. Have you worked through "DAMN-IT" (from one of my previous comments) and seen where that gets you?
Yeah, informally. I don't really have a lot. I saw a physiatrist a few weeks ago, she felt there may be a little arthritis in the joint, but it wasn't the main problem.
I've got an order from my GP for blood work, including looking for markers of systemic inflammation, but haven't had a chance to fill it yet. In general I don't feel like I'm very inflamed -- my other joints don't really have a lot of issues (well.. a bit of tendency to rotator cuff soreness from climbing, but it generally seems well managed).
I lost a lot of leg strength with lockdown, bec I lost access to bit barbells, which has been shown to be a risk factor for knee pain. I've been working on rebuilding hip flexor and abductor strength, altho more in the high-reps/body-weight range.
There was no major mechanical incident or change; I'm pretty careful with my diet (like, careful enough to worry about omega-6/3 ratios, and to eat sardines a couple of times a week. I don't really eat industrially processed or produced foods, except for tofu, which is a staple and canned beans).
They seem to respond well to icing and voltarine, which makes me slightly more confident in the "low grade inflammation" theory.
↑ comment by ChristianKl · 2021-07-05T20:45:54.567Z · LW(p) · GW(p)
Have you ever found the 5 main muscles on your body and given some thought about how they are functioning?
I think I'll have to say a bit more about my background. I went through the professional training for Danis Bois perceptive pedagogy. Part of it is anatomy and getting in relationship with various anatomical features.
Besides that general training I had for a while 1-on-1 anatomical teaching with someone that went through classic osteopathy training and then also entered the perceptive pedagogy field and who has three decades of working on people and fixing their issues. He has a good local reputation and a bunch of Yoga and pilates teachers go to him when they are old and their body has issues from being overextended in Yoga positions.
Those are the kind of people I'm asking when I want to know something about how the body works.
One story that Danis Bois likes to tell is that he once had a meeting with the teacher who brought Yoga to France and asked them: "How do you deal with the doubt?" Then the Yoga teacher replied something like: "I have no doubt because Yoga has 4000 years of tradition".
Part of what makes the community around Danis Bois a good spiritual community for me is that the people actually doubt whether they get things right and are constantly open to updating their models. It makes it a community that's very compatible with being a rationalist. You seem to me like the Yoga people who are overconfident and not aware of the tradeoffs that they are making.
When it comes to the particular question of posture, I had a conversation with another person who's also in the perceptive pedagogy field a few months ago. The person also has three decades of treating people a separate professional training in a more mainstream modality in which she teaches. She goes to workshop of different people to know what's out there. She just wrote her first academic paper. I said something about posture being a mix of fascia and muscle and she said: "No, it's just fascia" and I think told me in that context a story of a Alexander Method teacher who was very tense as a result of overcontrolling his body.
Those are the kind of people I ask when I want to know something about how human anatomy works.
In constrast to that you have a few years of personal experience, to the extend that you do have had positive effects in that time for what you are doing you have no idea what the effect 30 years down the line will be as you are not exposed to such data yet you present certainty while the people I listen to frequently say they are uncertain.
The aestethic of accepting uncertainty is something that both exists in the rationality community and in the perceptive pedagogy community. Part of that accepting uncertainty does lead to not just completely ignoring you based on reference class concerns and lack of both training and regularly working on helping other people deal with issues.
With my background written out, let's get back to your theory. The way scientific paradigm work is that a paradigm doesn't have any probability attached to it. It's a way of seeing a field.
Only empiric events have probabilities. To do science you actually need theories that make predictions. This requires making claims more specific. I think if you would start making your claims more specific and start making claims that would actually be testable it's likely that you get into contact with more uncertainty about your model.
Replies from: leggi↑ comment by leggi · 2021-07-06T08:45:50.590Z · LW(p) · GW(p)
Thank you for providing some background. I found it very insightful into your methods of thought and what you consider evidence. (I had to google pedagogy, I don't know what to make of "perceptive pedagogy".)
You've studied anatomy, I think great! Most people (in my experience) find anatomy intimidating but I would hope someone who has studied it would feel more comfortable giving some consideration some, fairly basic, anatomical facts.
I said something about posture being a mix of fascia and muscle and she said: “No, it’s just fascia”
And you are happy to accept that statement? That muscles, the bodily tissues that change the relative positioning of different parts of the body, don't affect the position of the body (i.e. posture)?
The state of the connective tissue system (including the ill-defined fascia) is important. The way muscles are functioning, moving the parts and repositioning, is also important. Humans have the capacity to send motor commands to "voluntary muscles". Muscles can be used to consciously alter positioning, to change posture. Anyone who says body position is just about fascia loses a lot of credibility in one swoop IMO.
Those are the kind of people I ask when I want to know something about how human anatomy works.
Have you done any independent research? Fact checking? Thought about it for yourself? Or are you relying on the opinions of others (however great you feel their experience/knowledge/credentials are)?
I don't want anyone to just believe me, I want the anatomy to be given some thought. I am constantly open to updating my model, but without feedback I can only work with my experiences. And the facts.
You didn't answer the question I asked:
Have you ever found the 5 main muscles on your body and given some thought about how they are functioning?
A simple yes or no will do at this point.
↑ comment by ChristianKl · 2021-07-06T14:30:07.653Z · LW(p) · GW(p)
Thank you for providing some background. I found it very insightful into your methods of thought and what you consider evidence. (I had to google pedagogy, I don't know what to make of "perceptive pedagogy".)
It's not a term where you will learn that much online.
In the beginning Danis Bois started out teaching Fasciatherapy. After a while he came to the conclusion that the New Agey people are too closemined and he wanted to try the scientific community. He got a Phd in pedagogy and became professor in somatic-psychoeducation and perceptual psycho-education at the Universidade Moderna in Lisbon, Portugal. As a result he added a new aspect to his teachings. More recently, as his knowledge progressed he used the new term of perceptive pedagogy.
English isn't the main language but French and the French base term is pédagogie. The scope of the term in French and in German is a bit different then the scope of the English word pedagogy and in the university time the translation was education as in somatic-psychoeducation.
http://fasciatherapie.org/international/index.php/fasciatherapy-dbm/danis-bois is one public biography of him that gives a bit of an overview over a part of the work and the part that interfaces directly with anatomy.
And you are happy to accept that statement? That muscles, the bodily tissues that change the relative positioning of different parts of the body, don't affect the position of the body (i.e. posture)?
Posture it's where the body naturaly without effort. For a muscle to hold something in a specific position it has to fire constantly which costs energy. It makes sense for the body to save that energy by using fascia to hold the posture.
It's also worth noting here that I did pay a serious price for receiving physiotherapy after Schrott for my scolioses (e.g. the goal is posture correction). It trained into my body reflexes that when the muscle tonus falls below a certain point my body tenses up. The cost of that was an inability to fully relax.
It was quite an effort and required an ability to intervene in quite basic processes to get rid of most of that stuff.
You haven't noticed the skulls around the idea of muscles driving posture.
Have you done any independent research? Fact checking? Thought about it for yourself? Or are you relying on the opinions of others (however great you feel their experience/knowledge/credentials are)?
The same somatic-psychoeducation comes about from it being a paradigm about how to learn from the experience out of the moment. Valuing embodied knowledge instead of abstract knowledge in generally true accross different somatic paradigms and that's why it's hard to acquire state of the art knowledge in the field by reading. It's also why a lot of knowledge isn't written down as a lot of people don't value abstract knowledge.
This isn't physiotherapy where people have a textbook that tells them what to do and then do it. Coincidently that's also the reason why the physiotherapy textbooks are rubbish. It's how you can find something that's for you interesting that you haven't read in any textbook about physiotherapy.
The 1-on-1 anatomy thing wasn't about transfering intellectual knowledge it was about feeling the entities in the body of another person (so in some sense it was 1-on-1-on-1)
A simple yes or no will do at this point.
The point I was making is that I thought about all the main muscles and how they work multiple times in the last five years.
Thinking through how muscles work is nothing really new. The physiotherapy might not really do it regularly and rather learn abstract knowledge and that's why you didn't find the ideas when you looked there but that work has been done elsewhere.
The issue is that the body is very complex and different processes interplay with another.
Replies from: leggi↑ comment by leggi · 2021-07-07T09:58:48.312Z · LW(p) · GW(p)
Posture it's where the body naturaly without effort. For a muscle to hold something in a specific position it has to fire constantly which costs energy. It makes sense for the body to save that energy by using fascia to hold the posture.
This is an issue of definitions then. I agree that it is the connective tissue system that provides passive support for the body, minimising muscular effort. I also believe it is the location of 'physical restrictions' that cause tension, alter positioning and restrict range of movement.
My definition of posture: The position of the body - all of it, at any time.
(I checked a few sources for a definition of posture. Lots of options out there, pretty much saying what I am calling posture and several mentioning the role of muscles.)
I'm not advocating attempts to get muscles to hold a specific position - in any shape or form. Think gentle movement and relaxation ...
Working with the '5 main muscles of movement' and consciously connecting with them provides a lot of sensory feedback about the relative positioning of the torso, head and limbs. Whether it be using 5 midline markers, the linea alba or Base-Line muscles (pelvic floor + rectus abdominis) as the starting reference for positioning (whatever works for an individual). This sensory feedback provides the information needed to work towards a full range of natural movement and a body that is balanced and aligned - where all the parts of the body in the correct relative positioning and free to move, including the myofascial meridians.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-07-07T10:26:32.527Z · LW(p) · GW(p)
Working with the '5 main muscles of movement' and consciously connecting with them provides a lot of sensory feedback about the relative positioning of the torso, head and limbs.
While that claim is true, it's also not useful as there are a lot of different ways to get sensory feedback.
Take a posture idea like "A simple way to adjust your body into a better posture is to imagine a string attached to the top of your head, towards the back. "
It seems reasonable for a lot of people. We are at a point where Alexander Technique teachers say "You have inaccurate stereotypes of us if you think we would advocate a bad idea like that."
Given your idea of how posture works, would you also argue it's a bad idea and that your idea is very different. If so how do you think your idea is different?
Replies from: leggi↑ comment by leggi · 2021-07-07T10:47:13.351Z · LW(p) · GW(p)
Yes, there are a lot of ways to get sensory feedback. I listed some to increase awareness of the relative positioning of the midline anatomy here. [LW · GW]
imagine a string attached to the top of your head, towards the back. "
The "imagine a string" example is great - if it works for an individual and they engage the 'right' muscles to improve posture. It didn't for me, my body was too restricted and misaligned, my 'myalgia of imbalance' too advanced for imagining a string to be of any help.
To take the string idea further, think of the linea alba and nuchal & supraspinous ligaments as part of this string. To straighten the string the main muscles are the rectus abdominis and trapezius muscles. The "attached to the top of your head, towards the back" I'd replace with the external occipital protuberance.
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-21T01:37:04.946Z · LW(p) · GW(p)
Also, for FWIW, while I don't have ChristianKI's level of education in movement, I am an experienced mediator, have done a reasonable amount of work with body scans and some work with tuning the motor cortex and three years of pretty serious contact improv dancing prior to lockdown. I think my proprioception is likely better than average, altho I'm not super confident in that, nor do I have a good sense if it's 60th or 90th percentile.
Replies from: leggi↑ comment by leggi · 2021-07-21T12:11:15.162Z · LW(p) · GW(p)
I watched a few videos and contact improv looks great. (Full disclosure I watched the videos x2 speed I've little patience watching most stuff). For people in a good enough physical condition, and relaxed enough to go with it, I can see it being beneficial and a lot of fun. (5 years ago I would have hated the idea because back then movement = pain, pain, pain and I couldn't have let go to move) It looks like free-flowing movement, guided instinctively by the body rather than the brain trying to control and direct. Support is being provided which allows increased movement (I achieve similar things by legs hanging off the bed, leaning over arm of chair, using the kitchen worktop as a bar, swinging from posts...) Working towards a full range of natural movement means moving through all the positions possible, the "more awkward" is easier when support is available and the 'support' is also moving which adds more randomness and further increase range of movement. I find a similar, gentle, effect moving around in water and letting my limbs float around but if I get the opportunity I will try contact improv.
Now seems a good time to have a minor rant about our modern flat earth..... Walking (especially barefoot) over uneven terrain flexes and stretches the whole of the body in a way that shoes and flat ground just don't allow.
I will take some time to have a good read of bewelltuned. Are there particular bits that resonate with you? For now, pulling this quotation:
By repeating certain movements and positions over and over again (e.g. during sitting work), we involuntarily strengthen connections between movements and muscles that don't make much sense lumped together.
This fits with my distorted 'body map in the mind' that sends motor commands to the 'wrong muscles', adding to imbalance and misalignment.
What do you experience when you are focused on your body?
(body scanning? I don't know much about the methods involved)
How would you describe your sense of proprioception?
My 'conscious proprioception' skills were pretty much at zero when I started and it's been a revelation actively experiencing the sensory feedback from by body. Starting with focus on my pelvic floor and rectus abdominis 'Base-Line' muscles from where movement originates and using my midline anatomy as the reference for positioning of the rest of my body.
Active engagement of the Base-Line muscles creates a positive feedback loop, increasing awareness of :
- Voluntary activation of muscles.
- The body map in the mind
- Proprioceptive feedback that is compared to the map. Seeing the sparkles. The basis of chakras and Qi?
Now I'm aware of my body in a way I never was before. I was always very clumsy...
↑ comment by Randomized, Controlled (BossSleepy) · 2021-06-16T19:00:33.665Z · LW(p) · GW(p)
This has good rather long and I'm out of time, but if you are interested - I could run through a diagnostic process for knee pain.
I haven't had a chance to digest this all, but I'd certainly be interested.
Replies from: leggi↑ comment by leggi · 2021-06-18T12:55:20.087Z · LW(p) · GW(p)
A diagnosis should focus on finding the aetiology. i.e. knowing why there is an issue (not just naming the problem. Anything idiopathic isn't a diagnosis, it's a label IMO).
{IRL I'd want a:
- Full history including details of all other ache and pains you experience - location, duration, severity, type, frequency, initiating actions etc. The good reason for you suspecting increased muscle tone? Do you physically feel tense? Spasms? Restricted movements? Other health issues, history of injuries etc.
- Thorough clinical exam. Of the primary problem areas checking for heat, swellings, areas that are painful/tender in palpation. Bruising, scarring etc. Testing range of motion and response to movement in various positions.
}
This "DAMN-IT" mnemonic can used to work through possible aetiologies of any body issue. There is some cross-over between categories ("inflammatory" is a common response to something wrong) and it may not be a totally inclusive list (but I can't think of anything that doesn't fit somewhere). It's very a useful tool:
D = Developmental, Degenerative.
A = Autoimmune, Atrophic, Allergic, Anomalous.
M = Metabolic, Mechanical, Mental.
N = Nutritional, Neoplastic.
I = Inflammatory, Infectious, Ischemic, Immune-mediated, Inherited, Iatrogenic, Idiopathic.
T = Traumatic, Toxic.
- - -- ---
So first steps are history & exam. Depending on what shows up:
Possible imaging - radiographs, MRI, ultrasound
Possible other tests - blood work, joint tap (if indicated).
If a clinician finds nothing remarkable on exam, a kind of "you say there's pain but I can't find anything specific" the usual process is prescribe rest, anti-inflammatories. +/- ice, physical therapy (some exercises to do) and come back in 3-6 weeks if not better. If you do go back, imaging would be the next step (gotta do something if they come back....)
- - -- ---
Think about the anatomy and were your pain is coming from.
Run though the aetiology list - what categories would you consider possible sources of your symptoms? I know which ones I'd pick out without other clinical signs, but I don't know your situation so it's over to you!
Replies from: supposedlyfun↑ comment by supposedlyfun · 2021-06-19T23:58:43.014Z · LW(p) · GW(p)
I am p>99.999 confident that what I propose is right. I'd like that rigorously tested. Break me, crush me. Release me from the frustration of knowing (with every fibre in my body) that I'm right ; )
If you're that confident in your position=pain theory, why would you need DAMN-IT? Why would your assessment of a patient do anything other than figure out which of your Big 5 muscles are involved in the pain? If the answer is, "Strengthen the glutes and your pain will stop," then how is any pain ever properly characterized as degenerative?
Alternatively, if your theory is actually "position=pain/Big 5 unless some other pathology is involved," then doesn't your theory only say, "I'm 99.999 percent confident that pain properly diagnosed as idiopathic by someone who doesn't subscribe to my theory is explained by my theory"?
At what point are you describing an invisible dragon [LW · GW]?
Here's the thing. You say you came to LW to get your theory disproven. Fine. But you are so confident in it that you expect to be wrong about one in one hundred thousand beliefs that you hold with that level of confidence. Beliefs I hold to that level of confidence include 9 * 7 = 63, because it's possible I am misremembering my multiplication tables.
Now. Imagine trying to convince me that 9 * 7 = something else, just you and me in an empty room with no calculators.
This is why your entire sequence went by with minimal engagement and mild upvoting. The amount of work involved in "breaking you" is tremendous, especially over the Internet, especially when your model takes eight disorganized posts and has many irrelevant images in it, and you seemingly haven't absorbed some basic lessons of The Sequences (TM). If I'm going to spend a bunch of time engaging with your theory and finding cruxes, I want to know in advance that you'll play by the rules of good reasoning.
I'm not unwilling, but can you first provide three substantive answers to the following question:
What evidence would falsify your theory?
Replies from: leggi, leggi↑ comment by leggi · 2021-07-03T09:53:20.813Z · LW(p) · GW(p)
My theory is based on anatomical facts, logic (feels like I'm stating the obvious) and my subjective experience. It's not complicated but there are multiple parts (split over several posts). I find myself using a lot of words in an attempt to explain clearly and simply (unsuccessfully it seems) so attempting to use as few words as possible and clarify my theory:
Base-Line Theory of Health and Movement:
Use the right muscles. Balance and align body and mind.
Anatomy of alignment
- Linear structures: Linea alba, supraspinous & nuchal ligaments.
- 5 midline markers: Pubic symphysis, navel, xiphoid process, jugular notch, external occipital protuberance.
The body is balanced and aligned when midline anatomy can be positioned to create the median plane.
5 main muscles of movement, dynamic balance and alignment
The position of the rest of the body is relative to Base-Line. The body's core pillar of strength.
- Pelvic floor - the Base foundation of the body.
- Rectus abdominis - central Line. Supporting all movement. Alignment of the linea alba.
Base-Line to legs:
- Gluteus maximus. Strength and stability of posterior pelvis.
- Rectus femoris. Align hip and knee joints.
Base-Line to upper body:
- Trapezius - to guide the head and arms through a full range of natural movement. Alignment of nuchal & supraspinous ligaments.
Conscious Proprioception
Increased awareness of the sensory feedback regarding position, motion and balance. Feel how to move to increase alignment and balance, starting from Base-Line.
Pains & weird sensations
- Using the wrong muscles results in myalgia of imbalance.
- Restrictions in connective tissues = stiffness, physical tensions = pain and weird sensations.
Restrictions result from tissue trauma (inflammation, injury, infection, surgery, stress etc.) and as long-term adaptation to poor posture. Individual trauma imprints. - Misalignment increases with cumulative damage. Pain spreads.
Mental
Chronic pain negatively affects sleep quality, mental well-being, quality of life. Physical tensions = mental tensions.
- - -- --- -----
So, with "what is Base-Line theory?" cleared up...
What evidence would falsify your theory?
1) Anything that offers an alternative explanation for my decades of pain and subsequent recovery over the past 4 years. I've researched my pain for decades. I've not come across anything that would invalidate Base-Line theory health and movement. No inconsistencies with what is "known" as far as I can see. (please anyone, tell me different.)
2) Any evidence that what I have experienced is some existential mindfek rather than what I think of as reality. Open to suggestions (very much a joke....)
3) No supporting evidence when 'use the right muscles to balance and align the body' is tested.
Two parts to examine:
- Test validity of "the right muscles".
- Test "body balanced and aligned" is a good thing.
Many methods to test come to mind both those parts.
- Looking for the presence/absence of physical misalignment in chronic pain patients. (Chronic pain patients that can align their midline anatomy to create the median plane would disprove me).
- Assessing levels of pain in those who's body is balanced and aligned. (Full range of natural movement with high pain levels would disprove me).
- Studying those with no pain and their state of physical alignment. (Finding grossly physically misaligned people with no/little pain would be evidence to disprove me).
- Biomechanical studies as the body as it goes through a full range of natural movement looking at the condition and positioning of the 5 main muscles. The trapezii have the most potential movement and are responsible for the alignment of the upper body, so if I had to pick one muscle pair to study I'd start with them.
For the assessment of chronic pain there is a lot to consider. Technology will bring better recording methods of aches and pains. More specific location, duration, intensity, frequency, type of pain. I've plenty of feedback to give on how to record pain more accurately.
One easy assessment for clinicians is to examine the condition of the nuchal ligament. Minimally invasively accessed and should be easily palpated. (I'd like clinicians to have examined a "free neck" to appreciate how much movement there should be and how the nuchal ligament aligns when the head is dropped forward).
Clinical trials.
I'm drooling at the thought of access to motion capture and digital analysis. How many dots would I get? I'd start with the 5 midline markers, hip bones, tibial tuberosities, C7, spine of scapulae ... Precise placement of markers is crucial.
Computer analysis allows detailed, blind assessment of movement and state of alignment of participants compared to the calculated potential range of movement for each individual. Assessment at 0, 3, 8 and 16 weeks as rough figures.
Or simpler testing, subjects stand with their back to column/wall. How does it feel/measurements. Then take a few deep breaths and think of aligning your midline to the column. Relax and allow the rest of the body to move as feels natural. Note what moves where. body parts, pain... Use a long, straight stick ...
Potential early testing participant groups that spring to mind:
- Medical students from several schools. Broadly similar age range. Should have no trouble understanding the anatomy. 1/2 the schools told to focus on the 5 main muscles and how they move. 1/2 no instructions. Attendance of movement classes for all participants?
- A group who do regular exercise classes together to minimise variables to what exercises are used. Take half a class, provide resources (intro. session, videos, pictures) to the relevant anatomy. Encourage focusing on using the main muscles as they move and feeling for the alignment of their midline anatomy. Ask them not to tell the other half of the group acting as the control.
- Chronic pain suffers. 1/3 told about the 5 main muscles, 1/3 told to increase movement, 1/3 nothing.
That'll have to do for now.
Replies from: BossSleepy↑ comment by Randomized, Controlled (BossSleepy) · 2021-07-04T12:55:26.568Z · LW(p) · GW(p)
Replies from: leggi↑ comment by leggi · 2021-07-06T08:37:02.850Z · LW(p) · GW(p)
I've read Painscience over the years. It's one of the few places that attempts to cut through the BS of "pain medicine" and I agree with Paul on many things.
However, I am looking at "posture" from a new perspective. (Kind of wish I had another word for body-position - pose? A lot of bad thinking is currently applied to "posture".)
Posture = the pose you are in = the positioning of all the bits of your body, at any time.
- Good posture = good positioning. Enabled by an unrestricted range of movement, normal tensions within the connective tissue system and the appropriate use of muscles.
- Bad posture = bad positioning = misalignment of moving parts = increased biomechanical stress. At some point the body will start to generation warning signals - pain.
The body is an incredible machine with a massive capacity to tolerate misusage, adapting its positioning to avoid pain and spread the burden of misplaced forces. Every adaption however, reduces alignment and increases imbalance, a progression of worsening positioning overtime. The more strain/exertion/trauma the body is expose to the more misalignment develops. For the body to function at/near optimal, it much have all potential position possibilities open to it - a full range of movement - allowing whatever posture/position that is most appropriate to be used for the task at hand.
Paul Ingraham says in the article you linked to:
Poor posture is any habitual, self-imposed positioning that causes physical stress, especially coping poorly with postural challenges.
There is a big difference between “poor posture” and “postural stress,” but the distinction seems to be absent from most discussions of posture and ergonomics.
I say poor posture is when there is postural stress. Also posture can be active or passive (conscious engagement of muscles or subconscious brain to body commands to muscles - habits).
If there isn't stress, it's not a bad position to be in so it's not a poor posture. Examples Paul uses:
The most stereotypical poor posture of them all — a hunched upper back, with the shoulders rolled forward
Is this really an example of "poor posture"? If the shoulders can be "unhunched", if the subject has a full range of movement, hunched is just another pose. Being in a position that is classically labelled "poor posture" isn't an issue if stress is minimal, and no pain is generated (RSI in wrists much more likely with "texting hunches"). However if movement of the neck and shoulders are restricted, if "hunched" is a fixed feature, the body is less able to adjust when it needs to, so it becomes a bad posture, generating postural stresses.
“Squatting like a baby” ...... hopelessly unrealistic for most people.
I understand Paul's view on this, a few years ago I would have laughed at the thought of getting into a squatting pose and cried out loud twisting and rotating to get into an approximation of the position. I would have battled a lot of pain to stay there, fidgeting and adjusting looking for the least painful option. But I can squat comfortably now. It wasn't an aim, or something I intentionally did. It's just another position to move into and out of as I work with the whole of my body, using my Base-Line as starting reference for relative positioning of the rest of my body - to sense my posture for myself and feel how to move to improve my range of motion.
Read though my take on posture [LW · GW]. Question the validity of each statement.
Read though Paul's take on posture. Question the validity of each statement. (I still agree with a fair bit in the article.) Check the references and consider what, who, how was studied. I'm not impressed with the quality of any studies listed. It'd be more efficient if you link to any ones you find that have some validity rather than me trying to comment on them all.
On a personal note, my patellofemoral pain started (bilaterally) when I was about 7 yrs old. I got a diagnosis of chondromalacia patellae, a label that sounded special but did nothing to reduce the pain in my knees. Walking was always painful, occasionally to the point of almost non-weightbearing. The pains shifted around and around in my knee (and the rest of my body) as my posture altered to avoid pain and keep on going. Now that use the right muscles to position my legs to torso (rectus femoris to align hip and knee joints, gluteus maximus to stabilise the posterior pelvis) my knee pains have finally gone.
↑ comment by leggi · 2021-06-21T10:33:40.349Z · LW(p) · GW(p)
Thank you for the comment, there's a lot of questions in there to deal with.
My theory is not not just "position = pain" as you put it. There's a bit more to what I am saying, but at its shortest:
Chronic malpositioning causes pain. (This pain is currently either labelled as idiopathic, or may have a label/syndrome but it's cause is still not understood - i.e. still technically idiopathic.)
To break it down:
(As I see it) there are two options with "pain". Either:
- Signals are generated somewhere in the body and we end up experiencing "pain" . (Pathway which involves various stimuli activating 'tissue sensors', electro-chemical transmission of information via peripheral nerves to central nervous system (spinal cord to brain) .
Or
- Something occurs in the brain that makes us think "pain".
Malpositioning = increases stress on body. (Misalignment, imbalance. Basic biomechanics.) (Inappropriate/excess) stress is bad. "Pain signals" occur where something bad is occurring.
Why would your assessment of a patient do anything other than figure out which of your Big 5 muscles are involved in the pain? If the answer is, "Strengthen the glutes and your pain will stop," then how is any pain ever properly characterized as degenerative?
It's not a matter of "figuring out which of .... 5 muscles are involved in the pain" or of "strengthen" a muscle and stop the pain. I would like to know what I've written that led you to these thoughts so I can edit and clarify so others don't make the same mistake.
As I stated full history and clinical exam are important for a full assessment. Gather all the information/evidence, consider all the possibilities. Lots of things can go wrong in the body.
I was sharing a diagnostic process so the OP can work through the possibilities and rule things in/out. If nothing else shows up indicating other issues, then mechanical/postural/positional/usage issues are the options left - i.e. the "idiopathic pain" my Base-Line theory deals with.
When is "degenerative" a primary aetiology? It is a pathology. Specifically, for joint pain - "degenerative joint changes" may be post-traumatic, post-infection, mechanical 'wear and tear', nutritional issues .... Degeneration may or may not be detectable on clinical exam but is something that can be often be seen on imaging. Something for the clinician to show the patient "There, there's the source or your pain" clinician has made a "diagnosis", but patient is still in pain and the primary cause hasn't been found.
There is a lot of cross-over with the DAMNIT list. It is diagnostic tool to run though aetiologies - for any health issue, not just pain. It's not perfect but it is useful.
How many things induce inflammation?!
.You say you came to LW to get your theory disproven.
What I actually said was "please tear to shreds". I meant think about what I say, pick apart bit by bit. There's several threads to pick at. Some real consideration of the anatomical facts I present and how the body is put together. Pointing out any errors.
especially when your model takes eight disorganized posts and has many irrelevant images in it
I'm disappointed that you consider my posts disorganised, but good to know. Thank you. I was hoping they were a progression from facts, definitions and logic to my experiences and updated thoughts. Seems like I failed there.
Feedback is what i want. Some consideration of what I am saying. Pointing out any errors. Some examples of issues with my posts would be great. How much did you read? Where did I lose you? I'll freely admit that presentation isn't my strong point and it's hard to know what level to pitch at. I want to provide accurate anatomy, without it being overwhelmingly wordy. And to provide enough background information for anyone who isn't familiar with human physiology. When I realised I wouldn't be publishing a couple of drafts I was working on I did slip some bits into other posts, which might account for a disorganised feel. There is a fair bit of repetition because it does all come down to the anatomy of alignment (midline structures able to align, the body balanced either side) and the 5 main muscles: pelvic floor, rectus abdominis (either side of linea alba), gluteus maximus, rectus femoris. trapezius (either side of nuchal and supraspinous ligaments) that are key to achieving dynamic alignment and balance and having a body that is well-positioned.
I find anatomy easier to understand in pictures rather than words hence many images. And it is all about the anatomy. Which images do you consider irrelevant?
I would really appreciate your thoughts in more detail.
I will be back with a response to what evidence would falsify my theory, it's more than I can just rattle off.
If you are genuinely willing to give some thought to Base-Line theory then spend some time thinking about the anatomy, finding the muscles on your body and breathing with your Base-Line. [LW · GW]
Lie on the floor and take a few deep breaths. Touch your pubic symphysis, navel and xiphoid process in turn. Imagine the line (the linea alba) that joins them extending as you breathe. Close your eyes and focus on the sensory information your body is providing. Give that a go. More than once.
Replies from: ChristianKl, supposedlyfun↑ comment by ChristianKl · 2021-06-21T23:14:34.754Z · LW(p) · GW(p)
What I actually said was "please tear to shreds". I meant think about what I say, pick apart bit by bit. There's several threads to pick at. Some real consideration of the anatomical facts I present and how the body is put together. Pointing out any errors.
Generally, muscles don't determine posture but fascia do. Using muscles to hold posture is unnecessary waste of energy and adds tension to the body. When bad posture gets fascia to stick together via fibrin the factors that are involved in getting it unstuck in more complex then "you have to have strong muscles" or even acting from those muscles.
That doesn't mean that muscles aren't important but "I have a theory that explains everything while completely ignoring the state of the art" just doesn't give you a complete picture.
Replies from: leggi↑ comment by leggi · 2021-06-22T13:54:11.287Z · LW(p) · GW(p)
Muscles move bones. Muscles do determine posture, along with connective tissues. I did edit my "posture post" after you'd read it. Originally I'd not mentioned the condition of connective tissues affecting posture (a glaring omission!). I find "fascia" too restricting as a term, I'm sticking with connective tissues.
- Muscles alter positioning/posture in an active manner.
- The condition of connective tissues affects posture in a more passive manner.
factors that are involved in getting it unstuck in more complex
Could you provide details about these factors? This is the stuff I'm looking for.
The anatomy is as near to "fact" as it gets but "restrictions in connective tissues" is my weak spot. I don't have any specific histological results or evidence past my experience and reasoning based on available knowledge. (What I've seen incidentally in various studies over the years does fit with "sticky connective tissues" - inflammation's a bitch)
I've felt the restrictions, heard them, seen them as I've moved and released tissues, regaining a little more movement each time. Something is giving, releasing. Connective tissues/ECM is the only tissue it could be (other suggestions welcome). Body wide releases. I can feel my myofascial meridians, where the lines of tension are. I can 'see' them when I close my eyes and focus on how my body is moving - proprioceptive feedback from my body giving me a visual representation of the state of my body in lights and colours, flashes and streams.
I'm not saying you have to have strong muscles, I'm saying you have to use the right muscles.
↑ comment by supposedlyfun · 2021-06-21T22:11:36.334Z · LW(p) · GW(p)
I'm going to wait for your thoughts on what would falsify your theory, because if it's a real effort, I'll be more inclined to put in the work you are requesting.
"Irrelevant" was the wrong word re images; sorry to have sent you down a rabbit hole--I should have said, "not obviously necessary to the point being made and/or unaccompanied by some explanation of why I should learn about what's in the image". I'd look at an image, read your text on either side of it, and have no idea why you were including it.
If you are genuinely willing to give some thought to Base-Line theory then spend some time thinking about the anatomy, finding the muscles on your body and breathing with your Base-Line. [LW · GW]
Lie on the floor and take a few deep breaths. Touch your pubic symphysis, navel and xiphoid process in turn. Imagine the line (the linea alba) that joins them extending as you breathe. Close your eyes and focus on the sensory information your body is providing. Give that a go. More than once.
Why? How many times, for how long? What evidence do you expect this practice to give me in support of your theory? If I don't feel anything, will you count that as evidence against your theory, or will you explain it as somehow supporting your theory, like Freud would claim that a patient was in denial if they claimed not to have some desire that his theory predicted that they would have?
Replies from: leggi↑ comment by leggi · 2021-06-22T13:34:24.507Z · LW(p) · GW(p)
Why? How many times, for how long? What evidence do you expect this practice to give me in support of your theory? If I don't feel anything, will you count that as evidence against your theory, or will you explain it as somehow supporting your theory, like Freud would claim that a patient was in denial if they claimed not to have some desire that his theory predicted that they would have?
I can answer each of those questions if you want me to. I am willing to spend the time if you ask but what value are my words to you?
I am offering you a map.
If you want to explore your territory it is up to you.
I will still be back with the big question of anti-theory evidence.
I would be very interested in your prior regarding me passing this test. Even if you don't want to share, pick a number now. ; )
I'm finding it a valuable exercise, so thank you for the interaction.