Taking Charity Seriously: Toby Ord talk on charity effectivess
post by jefftk (jkaufman) · 2013-04-10T00:59:48.204Z · LW · GW · Legacy · 15 commentsContents
15 comments
Video: (youtube)
Transcript:
I'm Toby Ord. I'm here today from Oxford University where I'm a Research Fellow in Philosophy, and also I'm the president of an organization called Giving What We Can.I should say as well that I haven't always been a philosopher. I used to be a computer scientist beforehand, but I decided I was interested in logic and things like these, which at my university, the Philosophy Department was mainly in charge of. I spent more and more time over there and I was also very interested in a whole lot of ethical questions and ended up being sucked away from Computer Science to the world of Philosophy. But, hopefully, you'll see that I've got an approach to some of these philosophical or ethical questions which is perhaps more quantitative than you are used to seeing from people who looked at these things. So, let's start.
I have always been interested in charity and helping other people and in particular, when I was an undergraduate, I used to get into conversations through the night with my friends. And they would say to me, you know, in some heated political debates, say something, like, "if you think that, why don't you send all your money to help people starving in Africa?", or some other cliche like this. This was meant to be a reduction of my position, that you can't possibly think that because you'd have to spend a lot of your time and effort helping these other people. But I started to treat it more like, "maybe I should be doing this". Maybe I should be thinking about what I'm doing with my income and maybe actually that is a logical conclusion. If you think all people are equal and so that you can help people in poor counties for less, maybe I should be doing something like that. Maybe I should investigate it.
I noticed a couple of philosophers have written on this. Peter Singer has very good papers on this: Famine, Affluence, and Morality, for anyone who wants to look that up. There are some very strong arguments so I took this seriously and started to think about what I could do in my life if I really wanted to help people who are less fortunate than myself.
When I was thinking about this, I divided the different ways I could think of helping up into these four categories. One is voluntary work, one was my career, so what good could come through my career. Another one is the personal relationships that I have. And another one was donations. I thought that [donations are] something that a lot of people neglect as a way that they can have a lot of impact in the world. It was also the thing that was most amendable to analysis. So, I decided I wanted to work out what, in terms of donations, could I do? If I really wanted to, what could I achieve? And that's the topic of this talk really.
I worked out that over my career, I'd be able to earn about one and a half million pounds, and I encourage all of you to try to work out what you'll earn of your career. I think this is an informative thing to do. Particularly as you can work out then what you could achieve if you really wanted to. And it's nice to know that through donations. It might be that you can achieve even more through your career.
I worked out that I only really needed about 500,000 pounds over my life if I can kind of kept on my current lifestyle which was (and is) very good. At that point, I was a graduate student and I had pretty much all the things I really needed in my life. I have a lovely wife and great friends, wonderful conversations, get to see beautiful places and travel to Europe once or twice a year on that—living in the UK is a nice advantage though [laughter].
But, you know, I can take some travel and listen to some, you know, the best music ever recorded and the things that I can do would rival a lot of things that a king could do a century ago; we've got it pretty good in the world today. And so I thought "actually I have a lot of these things which are a lot of value and if I spent this extra million pounds on myself, it wouldn't actually make my life much better" because the things which are of highest value in your life you get first and then you get less and less effective things added on later. And so I thought actually, you know, I could probably do that if I really wanted and carry on living at alightly above that kind of grad student lifestyle and donate about a million pounds.
So I thought, well, what can I do with that? Once you start to get a big number like this, it's worth putting in more effort. What can I do with the million pounds as opposed to, is this 10 pounds I'm donating for this fun run, is that effective, or is this other thing effective. If it's on that kind of level. (I should use dollars; I'll try. A pound is one and a half dollars.) So, try to think about these things and if it is just these very small sums, it's not really worth doing the analysis as to what's going on. But if you realize that over your life, you can do a lot with a million pounds, I mean, if you are spending a million pounds on house or something, you'd put in some time doing some research on that because you might be able to get, say a house that's, you know, 10% better, you know, it's a good deal. You know, you spend 900,000 pounds for house that would be worth a million pounds or something like that.
So, I want to think about that kind of thing when it comes to charity and trying to get a good deal. There's many ways that I could help people with my money. For example, education, empowerment of disempowered groups such as women in all countries or promoting peace. I mean, the list is very long. I'm going to focus on health in this talk because there's some really good evidence about health and so you can get quantitative and get into the nitty-gritty. And I also think that it's plausible that health in poor countries is one of the best ways that we can help people without money. If you think that actually one of these other things is even better than health, that's great because it means this is a lower bound for how much you can achieve in your life.
The first question here is, what metric should you use to try to work out what you can achieve with a certain amount of money? One common thing that's talked about is the percentage spent on overhead and administration. You often hear something where they say that only 10% of this origination's budget is spent on administration. I don't think that that's a very useful metric because what a charity does is much more important than how much it spends on these. There's a lot of variety between charities in terms of what they fund, and I think the key question instead is for a given donation how much benefit do people receive?
It could be, for example, that if an organization spends its money on program evaluation which is checking to see after they try something how well it worked. Suppose they build some wells in Kenya. If they spend some money to go back and find out whether those wells are being used or whether they're still working 10 years later, try to find out the lifespan of the well to work out how good a project it was to compare it with other projects, that counts as overhead. It also the exact type of thing that organizations should be doing, so the issue is that overhead money is not 'wasted'. Even if it were wasted, the difference of 10% or 20% or something like that between charities, as you'll see later in this talk, is actually very small. The differences get much bigger than that and so this would be relatively bad way of assessing things. There's a lot of research that can help us answer this question of "for a given donation how much benefit the people receive?" Most people aren't aware of it and the greatest difference here comes from the talk of intervention performed.
For example, you could distribute malaria nets to help prevent children getting malaria, distribute some medication to limit the effect of HIV on your system, distribute condoms to try to avoid new people getting this, build wells, or provide sanitation systems such as toilets and sewers: there's a whole lot of these different things you could be doing with money and some of them are much more effective than others, as we'll see.
Just as an example to motivate this, it's quite easy to understand. If you're providing someone with a guide dog to try to combat the bad effects of blindness, this costs about $40,000. In contrast, it costs about $20 to completely cure someone with blindness caused by trachoma. If for example, if you wanted to donate $40,000 in order to fight blindness, you could either provide a single guide dog or you could completely cure 3,000 people. There's a very big difference there. Presumably also, having a guide dog is less good than—well, being blind is less good than having your blindness cured as well. It seems like in that case, there's something of a factor of 2,000 or so between these different types of interventions. And this type of thing does come up quite a lot; this is not just an aberrant case.
But you might wonder, how can we take this idea further? This is very much an apples to apples comparison, but in many cases, you won't be able to do that. It will be, say, curing blindness as opposed to saving someone from dying of AIDS. They're quite different; it's hard to compare them. We want some way to broaden the universe of interventions which can be compared with each other in order to work out what's most effective within that universal possibilities. How can we compare apples and oranges?
Here are a couple of ways you might try to do that. The first one you might think of as: "how many lives can we save?" And that was the subtitle, I think, of this talk. That's the type of question which is interesting because I think most people don't ask that. They might hear something like, "it only costs a thousand dollars to save a life with charity," and they might respond to that by saying "well, okay, here's a thousand dollars." But they don't tend to say, "well, hang on a second, if you'd actually save someone's life literally for a thousand dollars, maybe, I should give you another thousand and another thousand!" I mean, if there was someone on the streets who you met who was dying you would take this more seriously in a certain way. What I'm trying to think of is you try and take these ideas about what we can do more seriously, to look at the hard figures for it and then to try to take them seriously.
Now, a big problem with using "how many lives can we save" as a metric, is that there's this truism public health that "no one's ever saved a life" because the person tends to die later, right? We don't—unless, you would have become immortal, that would be really be saving someone's life in that sense. And that'd be pretty good. Actually, I would recommend funding that if that was an option.—But what you're more talking about is helping someone who'll still die, it's just they die at a different time. And it's not just at a different time, right? Because it means that you have more life, right? The distance between your birth and your death is longer and you get more years of life in which to do things that are good for you. So that's the first issue, is that we can extend lives and that's what we're really talking about. So you might replace that with a question and say, "how many life years can we save?", and I think that's a much better question.
But there still is this bit about "what's the quality of that life?" And you might imagine a case where, say, you're in hospital, and you've been diagnosed with a form of cancer, and you are given an option of a treatment for that cancer which would mean that you will live longer. But that the quality of life will be much lower; maybe it's a very invasive chemotherapy. It's not obvious that you should take that. I mean, if you had ten years of life at low quality versus nine years at high quality. Quite possibly, nine years would be better. So there's cases where you want to trade off between quality and quantity, and it would be foolish to just use the quantity here.
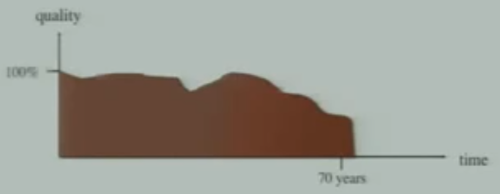
There are also cases where you want to compare non life-extending treatments. For example, if you cure someone of blindness, actually that does have a bit of an impact in how long they live, they live a bit longer if they're cured the blindness. But if we abstract that away, you can see there's also a lot of the benefit comes from turning normal years with where you're blind into years where you're sighted, and that's a lot of a benefit. So, you want to be able to capture both of those things. The way that people in public health, health economics, and practical ethics tend to think about this is in terms of quality-adjusted life years. This takes into account both the quality and the quantity, and it's also known as QALYs. So, I'm going to use that term a bit, quality-adjusted life years or QALYs. Now, to explain exactly what that is, I've got a slide here:
This is a schematic of the health-related components of someone's life. And you can see here that it starts at a hundred percent quality of life. It could start lower than that; it's just sketching something. You can see that their life goes down in quality that they perhaps become sick during the early part, and then they recover, and then there's sickness in middle age which is also recovered from, and then various stages of gradual decline towards death at about 75 years old. And you could imagine a curve like this for someone, maybe actually it would saturate a lot more. You know, you get up in the morning, you stub your toe while you get into the shower, and you drop, you know, to zero quality of life or something, or maybe negative. And then you bounce back up again and various things. You can think about your overall quality of life.
This is just meant to be health-related quality of life, but you get the basic idea. It's a measure of how well you're doing and maybe, a hundred percent, maybe, you could get about that. But in terms of health-related quality of life, we tend to think a hundred percent of someone who's perfectly healthy at that time. And zero is someone who's health-related quality is equivalent to being dead. So maybe they'd be indifferent between being at that quality or being dead. Maybe being in a coma is a good example of zero or maybe being in a level of pain which is so intense. Maybe there's levels of pain so intense that below zero, and there's some levels such that a bit above that and they're at zero. That's the basic idea.
And then you can see that to apply it in practice, you could imagine kind of stylized version of this question. Well, we have two lives here, which are, I think, both lived until 60 years at 70 percent quality:
Here's two different ways you could improve that life, maybe two different health interventions:
The first one improves the quality of that life to 90 percent, the second one improves the length of the life to 70 years. Then what you do to compare which one is the greater benefit is you just look at the area of them. So, it's just taking the integral. This, you'll be perhaps happy to know, is the standard approach used in public health that's reasonably quantitative. They allow us to compare apples and oranges within health, which is the key benefit of using this approach.
It's important to say they're only a rough measure, so, you might've been thinking, "how you'd measure this quantity of life"? You can measure when someone is born and you can measure which day they die, but I don't really understand how you could measure the quality of the life. It seems very hard.
There are surveys which are designed to elicit responses to this. For example, you ask questions such as "if you could either live for ten years in this health stage (perhaps being blind) or live seven years in full health, which would you prefer?" And then you start moving those numbers around and you keep asking the question; you can use that to elicit a quality. That's called a time-trade-off.
There's other ways as well where you imagine there is a chance you'll die. You can either be perfectly healthy with a chance to die or you can have this health state, how much chance to die would you prepare to put up with to avoid that health state? So, there are different ways like that and they have slightly different methodologies and so on, and they elicit answers to these questions.
But even then, they're probably still often going to be out by up to a factor of two. You might think that's a pretty bad metric; if I had like a yard ruler which is so inaccurate that it often got off by a factor of two, you might think that was a very bad measure, but it turns out that in the universe of interventions that we're considering a factor of two is enough to make quite a lot of progress. And I think it would often be less than a factor of two, but I just wanted to flag that. It is an inherently rough measure. And what, in some ways, is just surprising is that with such a rough measure, you can make so much progress.
So the first question here is, what is the QALY worth? A quality-adjusted life year, you know, what's one of them worth? Well, here is something. In Britain we have the National Health Service and they're prepared to spend 20,000 pounds for a quality-adjusted life year. If a new drug comes on the market, which costs less than 20,000 pounds ($30,000) for each QALY they will fund it. If it costs more than 30,000 pounds ($45,000), they won't fund it. If it's in between, they'll look at extra considerations, but they have an approach like this. There are 8,760 hours in a year, so this comes to about two pounds thirty ($3.50) for an hour of healthy life.
I don't know what you think an hour of healthy life is worth for yourself, but for me, I would definitely think that this is a pretty good deal. If someone came into this room and was selling hours of healthy life and was reputable, trustworthy distributor of quality-adjusted health hours, I would be using all the money that I have available, buy them, and also get some more money from the bank and say, well--I think that's a pretty good deal. We often go to the cinema, for example, and much more than three dollars fifty to upgrade a normal, perfectly healthy hour of our life into an hour where you're also at the cinema. It seems this a lot less good than creating in time new hours of your life in which you could do other activities and so on, so I would think actually we should be out willing to spend quite a lot more than that after per hour of our life. So maybe the NHS should try to get more funding so that they can increase that limit. If actually all the individuals in the society would be prepared to pay more out of their own pocket for it, then maybe the government should as well, that's separate question. This is trying to get an idea of what you think it's worth.
Another question is, would you spend 20,000 pounds to get a whole year? That's a bit harder because it's very large lump of life. You know it's not this fine grained. I think if you're just prepared to spend two pounds thirty for an hour then you should be probably prepared to spend 20,000 pounds per year. It's just like buying a lot of hours. But maybe you don't have that amount of money in the bank so it's hard to thinking those terms. But here's another way to think about it, is would you prefer to have a salary of 20,000 pounds per annum or a salary of 30,000 pounds per annum but be blind, one of those for the rest of your life? Or you could bump those numbers up, you could say a hundred and twenty thousand pounds versus a hundred and thirty pounds but be blind, or something like that. And for me, I would definitely think that this money is just not worth that much to me compared to my health and I would definitely choose the one in the left-hand side unless it got really, really low. So I think that I would also be prepared to spend 20,000 pounds per year. So let's move on then. So that's what it's worth. Right? It's worth at least that amount of money to us.
And what does it cost? Which is a different question. Often things cost less than they're worth, which is why we buy them. If they cost more than they're worth, you should not buy them. So spending 20,000 pounds in a QALY is a pretty good deal. Can we get one to less than that? Well, let's look at a question of preventing or curing HIV/AIDS. HIV being the virus, AIDS being the syndrome which you'd get if your viral load gets high enough in this kind of late stage where you're immunocompromised. We all now it's a major cause of death and disability in developing countries. And there are many different approaches to dealing with it. And so let's look at a few at the meantime. So here's a comparison between two different health interventions:
The first of treatment Kaposi's sarcoma which is a particular AIDS defining illness, it's a skin condition, which you only get if you're really immunocompromised. So it's one of the ways that people decide whether to say that HIV has progressed to be AIDS. And the second one is Antiretroviral Therapy which is paying for drugs which fight the viral load and help prevent HIV turning into AIDS. As you can see, the second one is much more effective than the first one. This is a longer bars are better type graph, and they're better in proportion to the length.
What we have measured in here is how many quality-adjusted life years per a thousand pounds compared to one and a half thousand dollars. And what I've drawn on there is a line which is the level it would need to be, it needs to be at least as long as that to be as effective as we thought, you know, the NHS use, which was just a yardstick that we had beforehand. And the NHS actually fund treatment of Kaposi's sarcoma and it's funded in the US as well. It's considered to be kind of on the line but to be effective enough in rich world's context. But you can say there's a very large discrepancy there in how much benefit you can produce for a given amount of donation but it's even more interesting if we zoom out and then consider another intervention, prevention of transmission during pregnancies:
So this is giving drugs to the mother--well to the would-be mother during the stages of pregnancy so that the new child doesn't get HIV. And that's a very targeted intervention because you can target that pregnant women who have HIV and so that reduces the cost and avoids an entire lifetime of HIV which is really good. And so the effectiveness of this is "quite a lot more effective".
I should say that these figures come from a report called Disease Control Priorities, second edition which is a big aggregation of the whole lot of the cost-effectiveness figures. There is a literature on this stuff where people try to estimate how cost-effective these different things are. They do different types of trials including randomized control trials. And some of it they have less information. They have to do more modeling and it becomes a bit more tentative but this is the estimate for this. But we can zoom out again and see more interventions:
We can compare it to distribution of condoms is a lot more effective again. As it's very cheap, you distribute them and you can avoid a lot of cases of HIV. And you can only just see this NHS cost-effectiveness threshold. Actually, we've moved it a little bit so you can actually see it. It would just be invisible at this point. And these things are just extremely cost-effective. And if we zoom out one more time, we can look at something—this case is not an AIDS-related intervention but distribution of bed nets to prevent malaria—that is even more cost-effective again:
At this point if we hadn't slightly enlarged it you wouldn't be able to see the bar for treatment of Kaposi's sarcoma. This new option is about a thousand times more effective. So you can do a thousand times more health gain for a given size of donation. To look at the actual number, you can see it's nearing 60 years of healthy life for every thousand pounds, which is very effective.
Let's just pause for a moment and say, you know, what can we learn from this? One thing is that health programs in developing countries can be amazingly cost-effective, about a thousand times more so than we're willing to spend in our own countries on health. And about a thousand times more effective than it's needed to be a good deal according to what we judged earlier when we said how much health do you need to get for a thousand pounds to be good deal and so on. And another thing is that our money is worth much more than we might have thought. Five pounds ($7) to thirty pounds ($45): that's the kind of estimate range for that most effective one; it's enough to buy a year of healthy life. So, it's quite interesting because you might not have thought that you're carrying around enough money in your pocket today is like a whole year of healthy life for someone else.
But you can only get these types of benefits with your money if it's used on the best programs and also, only if it's used on other people. So your money is worth a lot more than what you might thought if it's used for others. What's the catch? Otherwise, it would be great, because I'd be telling you how to get a thousand times more value for your money, for yourselves which would be a, you know, a roaring success of talk. But the point of the talk is to how get a thousand times much value for your money for other people which is a bit less of a roaring success. But I hope it's still at least interesting.
These things I talked about are mainly focused on by policy makers and [the DCP2] was aimed by policy makers, people who are administers of health in poor countries and also people who run aid programs and so forth. But they're also of interest to all of us when it comes to charity and trying to work out how we can help people most with the money that we decide to give to charity. It maybe would also make us think more about how much we should be giving once we realize it can be so effective. So, when we try to donate money, we're trying to help people and to help them as much as we can. If we had some option, and said look at two programs and the second program helps people less, you know, we wouldn't do that, right? It seems like we are trying to help people a lot.
Suppose we wanted to donate money to help fight AIDS, it really matters actually, whether that money is used to fund treatment of Kaposi's sarcoma or to fund condom distribution for example. It's a huge difference in effectiveness between these different options. And it's not actually enough to just know that the organization is trying to fight AIDS. You'd actually want to know more because some of the ways of doing that are, you know, not as effective as other ways.
You might think that actually the organizations would be the experts on this and would know and would be the most effective one. But often they're not, and one of the reasons for that is because they don't do as much program evaluation as we would like because they're trying to keep the overheads ratio really good, so that people will donate to them who've been kind of sucked in by the idea of the overhead ratio, which is a sad fact. But also, they're just generally aren't aware of these figures. There's been not enough movement to really make people aware of these figures and to be aware of how good these things can be.
Often if you talk to someone, who's say, funding a less effective treatment, I'll say that they're a efficient organization because there's no way that they could fund that treatment more effectively than what they are doing. And--but that's a different question too. Hang on. If we're really actually just trying to fight AIDS, maybe they are other ways to fight AIDS which would be more effective for those people. We don't have to always use the same intervention. And so it is relatively rare that people think of stepping to a different intervention. It's even rarer that they think of stepping to a different course, maybe they would think what we're really trying to do is make people healthier and avoid--let's say premature death or disability. In which case, maybe we should be focusing on malaria instead of AIDS and close down our AIDS, you know, start up malaria net distribution charity. I've never heard of any charity doing that.
There's a kind of mindset you can get into and if you're not familiar with these numbers, you think, well, this is where our expertise is and so on. We must be really good of doing of this. But it turns out, some of the things if you are expert at them and 20% better at doing them than anyone else, there's something else you could be doing but if you're average at, it would be ten times more effective. You're a thousand percent better. Which I think is really interesting. It's kind of the main point of this talk.
So here's a few more summaries about, you know, what does this all mean. I think one headline figure is that, where to give can be even more important than whether to give. So, suppose you had three options. One is that you don't donate anything. The second option is that you donate enough to save a hundred quality-adjusted life years by funding HIV transmission prevention which we saw was one of the middle level effectiveness. Or alternatively, you save seven hundred quality-adjusted life years by funding malaria net distribution. Well, it's interesting that the difference in absolute terms between two and three is much bigger than the difference between one and two. That's what I mean by saying "where to give". That second question can be even more important than the first question about whether to give at all.
Also, we can see that we can do pretty amazing things that we might not have thought of. So, well, you might have thought that in order to really help people, you have to go another country, away from your friends and family, do a different career not the thing that you're passionate about and that you wouldn't able to live the kind of affluent lifestyle that you are used to. But it's interesting to see that if you are to stay in your home country, do whatever job you wanted to do with your friends and family and donate 10% of your future income which would still leave you very affluent by world standards. That you could save at least 3,000 quality-adjusted life years during your career which is three millennia of life at perfect health or thirty millennia of life, you know, improving the health by 10% or something, you know, equivalent. I think that's pretty interesting that these options are there for all of us if we want to take them. It's not just a radical choice with huge amount of sacrifice. There are options with very little sacrifice which would actually help a lot.
So, you can consider this question, how much can we achieve if we really wanted to? I mean, I consider these options, spend the one and a half million pounds on myself, have my great kind of grad-student-plus life with also some extra, you know, a better car or something and bigger house and whatever. Or I could have my grad-student-plus life, you know, and also donate a million pounds to others. And my choice would be the second thing because getting extra "plus" there, just wouldn't actually improve my life much. So, I chose the second path and I still have a great quality of life and I can save at least 30,000 QALYs which is equivalent to saving 300 centuries of perfectly healthy life, which is is pretty cool, right? You know. It's a pretty exciting thing to be able to do I think.
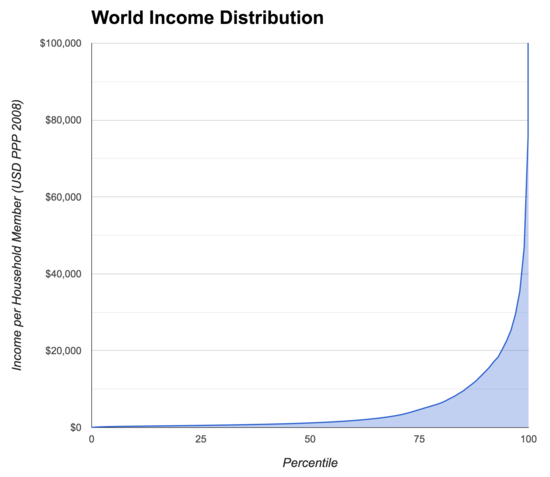
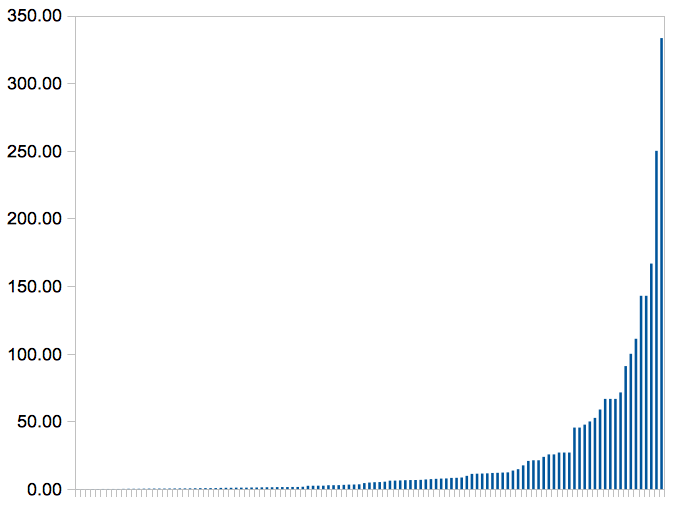
So I wanted to stop for a moment because you might be thinking, how can this be right? These numbers must be wrong. How can people in, you know, our shoes do that much to help people. And I think that this helps to make it clear and this graph is the world income distribution. And I think of it is the most important chart in economics because it's the best kind of summary of the state of the world today:
What we have here is slightly complicated. On the Y axis is income per household member. So that's a measure which if you look at how big the household is, you look at the household income, you divide by the number of people in the household. So that children count on this as well. And a child in a poor family counts different to a child in a rich family. Of course, if you're using a more naive measure, that doesn't work properly because it turns out they've got no income because they don't work a job and so it doesn't really come out right.
So it is household income per member and it's measured in US dollars adjusted for purchasing power parity. PPP means that you take into account the fact that money goes further in poorer in countries. For example, it goes about four times further in India than it does in Main Street, USA. So, what they do is, they effectively, you know, multiply someone's actual income in India by four in this graph. If you didn't do that, this effect would be even more extreme. So, but they are taking that into account already. And then what we've done is we've lined everyone in the world of up, all seven billion people from the poorest to the richest and we've looked at how much income they have.
You can see that there's this extreme spike at the right-hand side and if you're looking at this on a large projection screen, then on that screen, which is only itself about a yard and a half tall, on that scale, you can see that there is a ellipses there that I haven't been able to fit it the entirety of this curve. This is something where if you had fit in this entire curve, it would be taller than Mt. Everest at this scale. It's a pretty extreme skewed distribution. I think it's a fascinating chart for people who are into that kind of stuff.
What's particularly interesting about it, is if you actually look at it, you might do what I did, which is to look at this and think, oh, yeah, I'm somewhere in that bit where it curves around. You know, I'm rich but I'm not like really wealthy. Okay. And I won't be. You know, there's these annoying people who earn this millions of dollars per annum and isn't that unfair? And I'm quite wealthy compared to these other people. But then if you actually look at these numbers, you realize that at the moment, particularly if you're a young person without children or later on in your life when children leave home, you're going to be probably pretty wealthy on this and probably a lot of people watching this are in the richest one percent of the world's population or will soon be in the richest one percent of the world's population. So, they're in this area here. This is the richest two percent.
There's been a lot of interest recently in America, Britain, and other rich countries about the 1% and the 99% on a national scale. But it's interesting that in the global scale, we are the 1% and we often don't pay enough attention to that. But that's what's going on here. That's why the stuff that's in your pocket can buy years of healthy life, is because the stuff that's in your pocket is worth a crazy amount of money because we're all really rich. It's just that we tend to compare ourselves to our peers and so we don't notice that as much.
I'll just talk a little bit, before questions, about the organization that I've set up, which tries to take these ideas and put them into practice, and it's called Giving What We Can. It's a community of people who feel strongly about improving the lives of those people in developing countries. And it's a group where each member of the group has made a pledge to donate at least 10% of their income to wherever it is that they think can do the most to help to people in poor countries.
We also run a website that collects and shares information on the most cost-effective charities to help out members and to also help the general public. So even if one thinks 10%, maybe that's it a bit much for me, but I'd really love to find out more about this, how do I do more effective giving, which charities are they that actually implement some of these most effective interventions, and--that have done extra diligence on and so forth. Well, you know, you can go to our website and check that out.
There's two aims that we have in this organization and they fit in with what I've been talking about in this talk. So the first aim is getting people to give more. So this square represents something like what people were giving previously, on average in the US:
Firstly, I want to try to convince people that they could give a lot more than they do. It's actually not that much of a sacrifice because most of the things that are really important in our lives are actually very cheap. People say this all the time, turns out they're right. It's true. And you can get a lot of the value of your life on, you know, not much of the money of it:
So getting people to give 10% in this case. And the second aim is getting people to give to more effective organizations, which works out something like this:
So together, we massively increase the total impact. And it's very plausible that anyone who's hearing this talk could actually improve the impact they're going to have through charitable donations over their life by a factor of a hundred. Quite possibly by more than that, actually. But because you've got these two different dimensions and it's not additive, but it's multiplicative, it leads to a really big benefit if you're doing both of these things right.
Now, we have 292 members, I think, or maybe slightly more now, who've pledged to donate at least at 10% of their income. This comes to more than a hundred millions dollars of income that's pledged over their lives, which was enough to fund between two and eleven million quality adjusted life year. To put that into some kind of context, 5 million years is the period of time since humans and chimpanzees diverged evolutionarily. Or 200,000 years is the amount of time Homo sapiens has been around. So this is quite like a large amount of life. And we've got local chapters to try to discuss these ideas and get people interested in various places including Oxford, Cambridge, London, Princeton, Harvard, Rutgers, San Diego, Canberra. Some of them are universities, some of them are towns. And we try to get people involved and talking about these ideas.
To conclude, we're exceptionally wealthy living in rich countries in comparison to people in the poor countries, and our money can do hundreds of times more for them than it can for us. In fact, I gave a pretty good argument, I think, it could do a thousand times as much good. Because we think that if we spent the money on some of these health interventions where I had that barrier, that that would be better than how we spend our money. And then we realize that that would produce an amount of health which is 1,000 as much as we could produce for other people. So it's a good pretty argument that therefore we can do at least a thousand times as much to help other people. But maybe you think some of these numbers are a bit uncertain and let's, you know, be safe and say just a hundred times as much, okay?
However, it can only achieve this if it's given wisely. So we really want to spend a lot of time thinking about where to give or at least just spend a very small amount of time checking website of people who do spend a large amount of time spending probably more than hundreds of hours, maybe thousands of hours now thinking about where that is and looking at the research on this and trying to work out the best approaches. This idea, that where to give is even more important than whether to give.
Finally, the world is an unfair place with a great deal of suffering, as I'm sure you all knew before you came into the room. But we can each do a tremendous amount to help make it better and let's do so. Thank you.
Question: your example of blindness in particular, got me thinking about all these cognitive biases that people have and how they rigidly overestimate what they think is only an impact of disabilities in their life and now we're much more on a hedonic treadmill and we adapt really quickly after even losing a limb or becoming blind or something like that. How do you think we should adjust these, you know, quality figures for that, sort of, cognitive bias?
Ord: That's a great question, actually. People in public health, including here at Harvard, are looking at these types of questions and it turns out if you elicit these quality ratings by a group of healthy people—let's say in the case of blindness—they say that a year of blindness is at about half quality. It's like they'd be indifferent between two years of blind life versus one year perfectly healthy life. However, if you ask people who've been blind—particularly not just in the first six months or so, the first six months or so probably is really bad, adjusting to that—they tend to say it's less bad than that. Although interestingly, it turns out that if they regain sight, they then say, it was actually worse than they were saying when they were blind.
So there's an extra effect to this cognitive biases thing. That there is this extra aspect where it partly depends on the state they're in. And I think we often like to think the state we're in is particularly good compared to other states, so we can feel happy about our lives. But it's difficult to know exactly how to take that as your account because it seems to keep fluctuating. But I would think that maybe just taking the average of a group of sighted people and a group of blind people would at least be a good first step on that. If you did that then maybe, you know, it would say that instead of being half as good and having quality weight of .5, the quality weight should actually be .6 or .7 or something. That won't change the numbers that we're using very much though. But it is the type of thing that if we could more fine grained than this and tried to work out some more nitty gritty questions, that it'd be an improvement of the accuracy of an estimate by 20% is certainly worth having.
Question: I have two questions to this, one is could you address the next hurdle that people have to giving. So, the first hurdle is, will it make a difference, and this talk addresses that. The next question is, is this the difference that I want to make? Let's pretend that the most effective way was to give food to people who are starving in some location. And you could feed them, and let's say this was the cheapest thing that could be done and, you know, it would give the most quality adjusted life years. But then the thing is that some people might feel that doing this just means that there's going to be extra millions of people who are going to starve the next year. So many people won't give because this maybe the most effective way is to, you know, prevent people from dying by giving them mosquito nets and so on but it's just a bigger problem for another day, so that's my first question.
The second question is, if we really take this argument all the way to its extreme, let's just say the US government within the US borders, then we don't have to deal with the issue of helping and other countries. But everything that's done could be a, you know, in some sense, put on this utilitarian scale, if I build a new bridge, we can talk about how that helps people. Anyways, I mean, it's actually is not a good example but there are other kind of things like this where you can say that, well, there's other things that we do that improve people lives. And if we just determine that there are two things, let's say, that are the most effective at improving people lives, why doesn't government do only those two things and stop doing almost anything else that's not necessary, right? So, like, cut all the welfare programs, cut everything else, cut anything, you know, for special needs children whatever because this is the one, you know, these two programs that we've determine are the only ones that are, you know, going to give us the most effective results. So could you address those two concerns?
Ord: They're both big questions. I'll take the second one first. So one thing to say is the government in the US actually does do this but they use a different methodology. The one I'm talking about is called cost-effectiveness analysis, the one the US government uses is called cost benefit analysis. And that's an approach where you measure the benefits in terms of dollars and you measure the cost in terms of dollars. They try kind of pull together benefits based on how much people will be willing to pay in order to get those benefits. So they do think about this in the US and measure things like this. Although that methodology, I think has quite a lot more flaws in it. It's got a lot of more room for ethical problems to arise than from the one I'm talking about. But anyway, the thing is that if you really did want to help people as much as possible then going with a sophisticated version of this approach is the way to do that. It's just defined to be the way that helps people as much as possible. Therefore, I think that's a pretty good idea to go with.
As in your particular case, it will turn out that if there are just a couple of interventions that they will end up with diminishing marginal returns. So what we've tried to get here is estimates as to how effective it is the margin. So if you're going to save one more life from malaria and with the current amount of malaria's mosquito net distribution, how much would that cost? But if you roll that out to say 80% of the population then you're trying to get the last 20% covered, then that can be much more costly.
So sometimes there are issues where that will change and so what you want to think of is, for each of these interventions, you want to think of its cost curve, would be the most sophisticated way to do it. But also even then, you'll saturate these things. So for example mosquito net distribution, there are--the number of people dying from malaria per year is uncertain. It's somewhere between about 700,000 per annum and 2 million per annum. Let's say its one and a half million per annum and the amount it costs to save a life due to malaria on average by distributing nets is about $3,300. So, and now I've set up a multiplication problem for me. But there's something around about $3 billion worth of money that would be needed to totally cover that which is actually very small compared, to say, the US budget.
And so with some cases like this that there are very effective it turns out that you can actually completely saturate them and it won't be the case that there's just two things that end up getting done. The really effective things will get done and then they'll get to move on to the next most effective and the next most effective and they'll get quite far down the list. So, it's pretty valuable. In fact, in terms of these interventions I've got a nice chart which I didn't present but if you look at all of the interventions that the DCP2 looked at, and you do a chart of all of them, you can find that their log normally distributed that the most effective 20%, if you were to fund them all equally, 80% of the benefits would come for the most effective 20%. So, if you do work your way down from the top you actually cover a huge amount of benefit.
The first question was about additional issues. I definitely think that QALY's and the cost-effective analysis at this kind of level is not the be all and end all about this. I'm trying to just get these ideas onto the table in terms of how you can think about this with a kind of simple examples and obviously you could have, you know, more and more hours making it more sophisticated and trying to get better data and so on. But in the particular case of overpopulation, that's another thing that you'd want to think about as to the effects of that. Ideally, you want to take that into account.
Now, I can say that it turns out that there's a couple of big points you can make there. One of them is that it turns out that saving infant lives probably actually helps with overpopulation. It actually reduces the expected number of people on the planet because it turns out that there's a process called the demographic transition where once people get wealthier, they and their children start surviving better and have fewer children. And it's more than proportional, so it compensates and this is what has happened in rich countries and it seems to be happening in some of the poor countries. So, it looks like if you get actually child survival to be improved, it actually would fight overpopulation rather than exacerbate it.
The other thing I can say is even if you didn't believe that you could try to find some organizations and we recommend a couple on our website which don't save lives but just improve quality of life. So, that would be a way to do it that where that other argument wouldn't come up.
Then a third thing to say is that if you really thought that overpopulation was so bad that you're willing to just the let a whole lot of people die in order to decrease the overpopulation, the badness of helping was going to be bigger than the goodness of helping those people, then you must think that overpopulation is really, really bad. It's so bad that that even if we could spend, you know, 15 Pounds to save a year of life, that the overpopulation effect is even bigger, in which case you should just donate money to fight overpopulation. That would be the logical conclusion. The conclusion wouldn't be, there's this absolutely terrible thing that's so horrific that it overwhelms these amazingly big benefits therefore I won't do anything. But therefore I'll donate money to a group that, let's say, distributes condoms or, you know, educates people about family planning and so on, there's plenty of those groups as well. So, I think that style of response ends up, you know, not quite blocking the pulse of this argument. I hope I've answered your questions.
Follow-up question: Thank you. I think that I'm in the same way that a year of life extended can be adjusted to be a quality adjusted of a year of life extended. I'd like to see this analysis, I'd be really, really happy to see if this analysis could be further extended one more thing about whether it is also generating or getting rid of a problem. In another words one more adjustment that would be more convincing to people I think then that yes, if I donate to this I'm not only giving extra quality adjusted life years, but I'm also diminishing and not increasing the problem for tomorrow.
Ord: I agree. There's definitely potential additional considerations before taking it into account. I'm totally on board with that.
Question: You showed how giving effectively is much, much better than giving ineffectively. Have you considered the other ways of giving, volunteering, personal relationships, et cetera, work was the other one. Maybe they can be even more effective for some of us than giving money.
Ord: That's a great question. And it's plausible. I think personal relationships is one that occurs to a lot of people when they're thinking about this is. Like, you know, how can I be a good person in terms of my family and friends? But it seems that once you get to these scales, it's hard to see that really the best things that you can achieve overall in some kind of neutral, impartial sense are going to be through that.
But the other areas of volunteering is potentially very valuable, as is work, depending on what you do. So for example it could be the case that—I mean I have, in my spare time, set up this organization which has done a lot of good. And so probably I've done more good through my volunteering than I will achieve actually through all of my donations over my life, which is pretty cool. And similarly if you can find some really high impact volunteering approaches then you could do a lot of good.
It is definitely harder through volunteering or like of things in rich countries to have as much impact as we've seen. Often in fact one could have even more impact if one worked a few extra hours and then donated the money. That might seems surprising but if you remember that, using economics, that's we have a comparative advantage in some kind of field and that's the field where we get the most money. And so if go into that field and earn money and then it's very effective. Because then we can pay someone who does the thing that were interested in. So we get, for example, an expert in computing to, instead of donating their computing services to a poor person, to use that to get money to pay the person, for personal needs and to pay someone who is actually an expert in those things. As opposed to someone who's more of a dilettante. It does depend, but volunteering could be potentially even more important if you get really high leverage on it.
Work could be really important as well. It's hard to know in terms of improving technology. Obviously there's been a lot of technologies which have been very useful for poor countries. For example allowing them to leapfrog landlines and to go to cell phones in order to get connected. I think a lot of people would have thought it would take a lot longer before that would be useful. So there are potentially a lot of approaches there. And also maybe doing your job has various other effects. So obviously it depends on what it is, but I don't know exactly how to asses these things. They're quite a lot harder to asses. So I'm not claiming that they're less valuable really. So much as, there's at least quite a high bar to beat. But maybe they can be even more valuable than that. And I think that people should think about those things quite seriously.
Question: It seems that core to the high quality cost effectiveness is the fact that the donated dollars are used in developing countries. What are the implications for those who want to give locally for example in developed countries?
Ord: That's a good question. So there are various implications. So one implication is that you might think within your local area whether that's your country or your community, that you also want to take these ideas in light and to try to give effectively within those areas. I don't have particularly good data on that, but you'd probably want to start thinking about it a bit because once you see that there are several orders of magnitude separating the best and worst interventions in poor country settings, you might think that there actually could be quite a lot of discrepancy between the interventions in rich country settings. And in fact there are in term of health at least. Similar kind of curve for health interventions in rich countries.
So that's something where maybe also in other forms of volunteering or donation you could see that happening. And you'd start to see this lesson, that choosing where to give, it could be worth maybe spending half the time you'd spent earning to donate the money, just doing research on this problem, and then donating half the money to something that's more than twice as effective. That's quite plausible. So at least to spend, say 10% of the time or whatever on the question about where.
Another question though, I think would be to really think about why it is that you want to help locally instead of globally. I've had a nice advantage on this which is that I was born in Australia. And so my local thing would have been to help Australians, and wouldn't care about helping British people over, say Kenyan people because I didn't know any British people or Kenyan people. And so, it seemed fairly obvious that if I could help more people in Kenya than I could in Britain that that would be the better thing to do. Otherwise I'd be kind of unduly privileging British people for some reason.
Now, that I moved to Britain I still kind of am in the situation and I also kind of feel, why would I help Australians rather than helping more people somewhere else or helping them in better ways. So it's helped to kind of break some of that partiality for me in terms of this type of donation. But I think that I can kind of help the world more in these ways. And so one would also want to think that it's very difficult to help in such a extreme ways and to spend some time thinking about the ratios that you would end up with. Is it the case that for the most effective way you can help people locally, you could help a hundred times as many people globally? If you, then you might think, you know, can I really justify a hundred to one ratio in terms of that. Maybe if I had a chocolate cake I would give to my friend rather than to a stranger, other things being equal or something. But if there was a case I had to stop a hundred strangers having their chocolate cakes in order to give one to my friend, maybe I wouldn't do that. So it could be interesting thinking quantitatively about some of those things as well. But there's a lot of people who think that they're not swayed by these reasons and so on, if so that's fine. I'm just trying to give arguments.
Question: What is your opinion of GiveWell's recommendations? Why don't you just outsource all of your donations to them, because they seem to be looking for very similar things?
Ord: They're great. So for those people who aren't aware, GiveWell is a charity evaluator, formerly operating from New York, I think now from San Francisco. And they are doing this kind of thing, trying to look at different charities and find where you can help people the most for your donations. I think that they're great and have done good research on this. When they started up, they managed to launch a couple of years before Giving What We Can as I had to finish my PhD, but we kind of were thinking about these things in a similar time and were in contact with each other.
We're both really frustrated about the fact that there's a lot of really good research being done that's not being shared with the public. And so foundations, say the Gates Foundation, I'm sure they do a lot of realty fantastic research on where to give, and they use up those opportunities as well and they don't kind of share this information more broadly. And I think that it was great to share it. And that was GiveWell's approach to share that really publicly. I think that's they're real big advantage.
And so we at Give What We Can, take their advice very seriously. It's one of the several inputs that we take. We also talk to people at the World Health Organization, the World Bank, Oxfam, lots of places. And try to find out what going on and what we think about different interventions. And some of those we come up with different conclusions to GiveWell, but of all those kind of inputs to our decision making process, they're probably the largest and we take them very seriously. So definitely do search for GiveWell as well and have a look of what they say.
Thank you.






{kind=link}
15 comments
Comments sorted by top scores.
comment by [deleted] · 2013-04-10T19:00:06.672Z · LW(p) · GW(p)
These kinds of talks are one of the primary ways people are introduced to Effective Altruism - it seems very useful to spend some time crafting them to produce the most effective talk we can. So it would be great if people could critique this talk. I'm sure Toby wouldn't mind. To get the ball rolling, here are some of my thoughts:
- Beginning with a personal story is good
- The answers to some of the questions aren't very good: especially the responses on E2G vs other work, and local vs LEDC giving. A bit waffly. They get asked so often that we could presumably come up with a standard answer.
- Is explaining QALYs going to turn people off? Perhaps its appropriate to this audience
- The presentation could be more engaging - less on each slide, more colorful
- The conclusion is strong
ps. Thank you for transcribing this!
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2013-04-11T12:14:50.748Z · LW(p) · GW(p)
"Is explaining QALYs going to turn people off?"
QALYs are a major component of this talk. You could make another talk without QALYs, but a lot of pieces of this one, like demonstrating the huge range of effectiveness in health interventions, depend on them.
"The presentation could be more engaging - less on each slide, more colorful"
I didn't get the sense that people in the room were tuning out or would have paid more attention with flashier slides. But this probably varies based on where you are.
"Thank you for transcribing this!"
I actually only cleaned up the transcription. The initial transcription was made by someone else because one of the people who wanted to watch the talk is deaf.
comment by Raemon · 2013-04-12T15:51:26.839Z · LW(p) · GW(p)
Jeff, did you do the transcription yourself? If so, massive kudos. (I really prefer reading to watching videos when it comes to this sort of thing, although I seem to be in the minority)
I think this talk does a surprisingly good job of walking through a lot of important (and potentially cold, dry) concepts in a way that makes sense.
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2013-04-12T17:08:00.017Z · LW(p) · GW(p)
Someone else did a transcription at google, I think because a deaf employee wanted to watch the talk. I cleaned it up, fixed typos, added links, screenshots, and paragraph breaks.
comment by RomeoStevens · 2013-04-10T02:40:29.318Z · LW(p) · GW(p)
So If I donate 2 million USD over the course of my life and I expect to save around 2000 lives this clearly loses out to causing human uploading to come even 1 hour earlier.
Two problems:
I expect the cost of saving a life to go up in the future. So traditional charity will probably result in fewer lives saved. At what rate should I expect the cost of saving a life to change? Does Givewell attempt to graph this?
I have to figure out whether 2 million donated over the next several decades can plausibly cause uploading to happen sooner.
Replies from: ModusPonies, evand↑ comment by ModusPonies · 2013-04-11T19:28:40.749Z · LW(p) · GW(p)
I have to figure out whether 2 million donated over the next several decades can plausibly cause uploading to happen sooner.
This is a problem I am extremely interested in. Please PM me and/or write a post if you come up with anything.
↑ comment by evand · 2013-04-10T03:00:27.823Z · LW(p) · GW(p)
When uploading is first available, I expect it to be expensive, and for the available hardware to be limited in capacity. I assume $2M would make a noticeable impact on the uploading rate available. (Even if capacity grows rapidly due to singularity effects, I suspect this would be slow on the time scale of hours, unless some sort of manufacturing magic happens before uploading does.)
So you should trivially be able to bring about faster uploading if you're willing to set up a charity with long term planning skills to do so. How much uploading bandwidth do you expect $2M to buy?
Replies from: CarlShulman↑ comment by CarlShulman · 2013-04-10T03:32:51.668Z · LW(p) · GW(p)
When uploading is first available, I expect it to be expensive, and for the available hardware to be limited in capacity.
So do you expect uploading in the next several decades, or big slowdowns in the improvement of computation per dollar?
Replies from: evand↑ comment by evand · 2013-04-10T03:57:46.483Z · LW(p) · GW(p)
I expect most new things to first be available in small quantity at expensive prices and low quality, especially if you're literally talking about putting them to use in the first hours or days after they become possible. In fact, no non-trivial examples that involve any specialized hardware at all come to mind. Am I missing any major ones? Are there major reasons uploading would be different?
Replies from: CarlShulman↑ comment by CarlShulman · 2013-04-10T05:16:53.407Z · LW(p) · GW(p)
Why expect specialized hardware to be a bottleneck? Most software programs don't require very specialized hardware.
If computation per dollar continues on trend to far surpass minima for brain emulation, then I would expect final bottlenecks to be in brain-scanning or (more likely) understanding the neuroscience, not shaving cycles off the computation of Hodgkin-Huxley.
Replies from: gjmcomment by Jiro · 2013-04-12T22:13:59.753Z · LW(p) · GW(p)
I can think of a whole lot of unlikely ways by which keeping your money and not donating it, or doing even worse things, increases the welfare of people around the world. For instance, maybe a society where people like myself are richer encourages people in other societies to improve their societies because they see how rich they could be, to a greater degree than if people in my own society are not as rich.
Or maybe when I keep my money rather than donating to charity, the average person in my society is incrementally richer, that incrementally reduces the population in my society (because of the demographic transition), and makes people in my society better off by an incremental amount that may still be quite a lot when summed over the whole society.
Maybe me being richer, and thus the United States being richer, incrementally increases the prestige of the US on an international level, incrementally discouraging North Korea from starting a war that kills millions of people.
Alternatively, maybe a war with North Korea is inevitable but if it starts sooner rather than later fewer people will be killed (since populations will be larger in the future) and the surviving descendants will have more man years of freedom. It is conceivable that I should prefer starting a war with North Korea to stopping malaria.
Maybe I could promote ideas and policies that make Bill Gates richer, on the grounds that making him richer also increases the amount he'll donate through the Bill Gates foundation. It is even conceivable that doing this is more efficient than just giving money to the Bill Gates foundation directly, or convincing other people to do so.
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2013-04-14T05:19:58.394Z · LW(p) · GW(p)
Have you tried to make rough order-of-magnitude estimates for the effectiveness of these approaches?
Replies from: Jiro↑ comment by Jiro · 2013-04-15T15:45:28.529Z · LW(p) · GW(p)
Small effects multiplied by large populations, or small probabilities multiplied by large benefits, are very difficult to estimate and any estimates I can come up with have such large error bars that they are useless.
I should add that I think some of the ideas in the original post have this problem too. For instance, how would you calculate the magnitude of the effect by which saving infant lives encourages the demographic transition and thus reduces overpopulation?