Covid 11/10/22: Into the Background
post by Zvi · 2022-11-10T13:40:00.991Z · LW · GW · 5 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Booster Boosting and Variants Physical World Modeling China And Now An Important Message Long Covid Other Medical and Research News None 5 comments
There was a lot of news this week.
Elon Musk continued to Do Things at Twitter.
America had midterm elections. The polls were roughly accurate, with ‘candidate quality’ mattering more than expected especially on the Republican side.
FTX imploded. For now I am letting Matt Levine handle coverage of what happened.
None of it had anything directly to do with Covid. So this will be short.
Executive Summary
- I hear there were midterms.
- And that FTX imploded.
- Covid death number down a lot, presumably not a real effect.
Let’s run the numbers.
The Numbers
Predictions
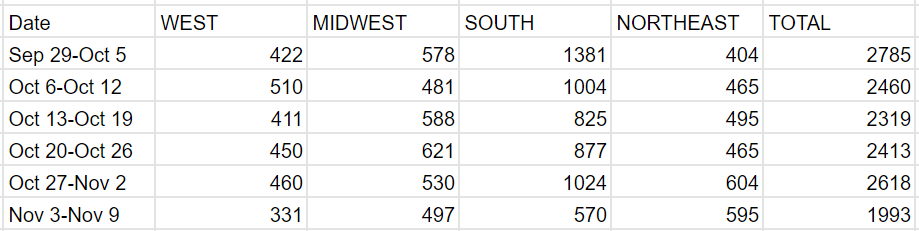
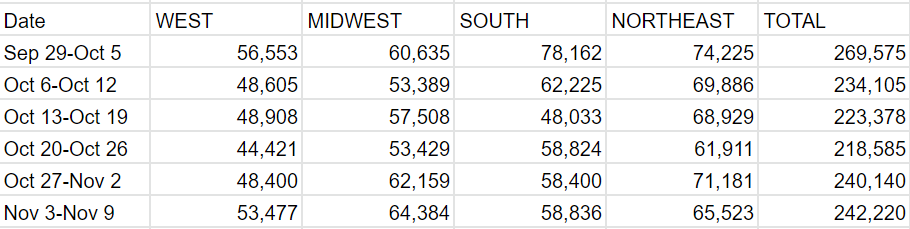
Predictions from Last Week: 255k cases (+7%) and 2,600 deaths (-1%)
Results: 242k cases (+1%) and 1,993 deaths (-24%!).
Predictions for Next Week: 250k cases (+4%) and 2,400 deaths (+20%).
That death number is super weird. At first I thought ‘what, they can count votes or they can count deaths but not both at the same time?’ or ‘election day isn’t actually a holiday is it?’ Then the case number came in flat even in the South, although Alabama didn’t report any cases at all (which wasn’t a big enough effect for me to adjust).
Some of the drop is that last week had a spike of about 250 deaths in North Carolina. Still leaves the majority of the gap unexplained. I don’t know. I don’t see how there could have been a large real drop in deaths, and if it was a reporting issue we would have seen a decline in cases. Also, in the regions where we see a decline in deaths, West and South, we don’t see relatively few cases. So the reporting explanations don’t make that much sense here, and it seems unlikely cases actually rose a lot while being underreported or anything like that.
It does raise uncertainty in deaths a lot for next week, and to some extent also for cases, in the usual ‘was this real or was it both fake and in need of reversal’ dilemma. We shall see.
The good news is that there is not much practical impact on decision making, unless this is all hiding a tidal wave of new infections. That is possible. I would still not expect anything like last year’s wave, and for things not go on too long before stabilizing, but the timing between weather and sub-variants would make some sense.
Deaths

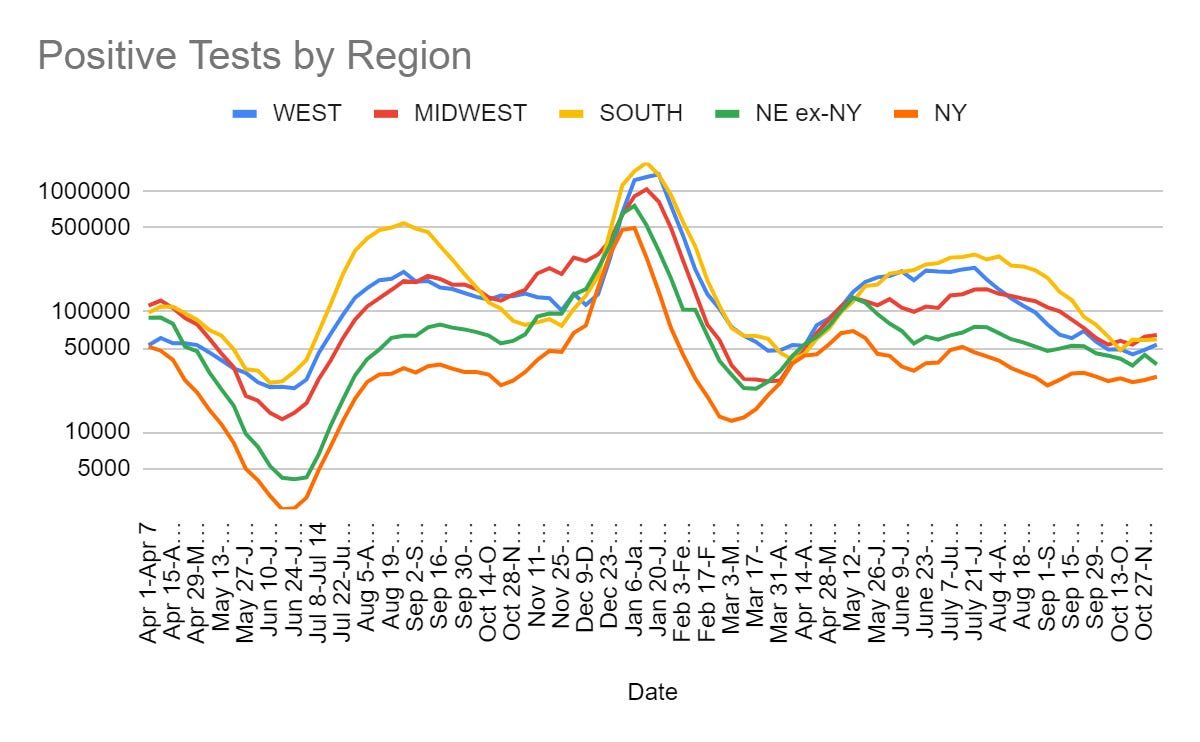
Cases
Booster Boosting and Variants
Nothing.
Physical World Modeling
Babies born during lockdown more often miss developmental milestones (study).
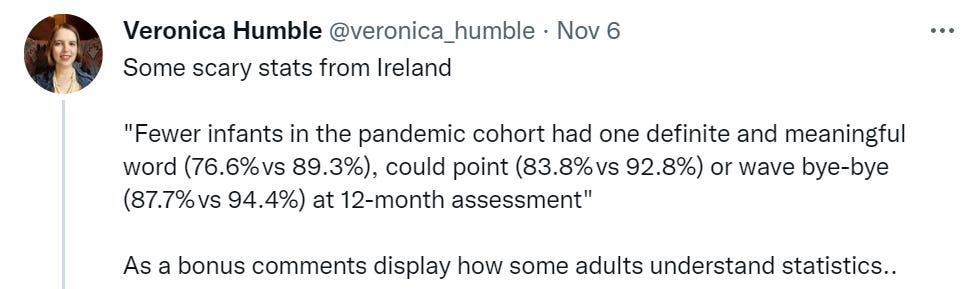
I doubt this leads to that much in the way of permanent impacts. It still seems rather not good, the effect sizes here are quite large.
Study finds that Paxlovid reduces risk of Long Covid. Would be weird if it didn’t.
China
Via MR, Nucleic Acid Testing ‘now accounts for 1.3% of China’s GDP.’ Zero Covid is a rather large drag on China’s economy that will be cumulative over time. From the comments, which also interestingly feature massive negative votes everywhere:
I’m a teacher in China and EVERYONE gets tested at least THREE times per week. It is such a waste of time and money.
Meanwhile full surface paranoia continues. The Zero Covid principle and the constant testing would not be my approach, but I understand. The surfaces obsession is something different. Everyone has to know at this point that it doesn’t do anything.
China reiterates Covid Zero Policy (Bloomberg), calls for more targeted and also ‘more decisive’ measures. No signs they will abandon surface paranoia. This seems like it likely gets worse before it gets better.
And Now An Important Message
An SNL sketch, best of the season by far. If you haven’t yet, watch it.
Long Covid
Article from Yale on chronic disease in general and how Long Covid may help us get a better understanding of what it is and how to deal with it. Does not provide much new. Mostly it is the same old ‘now that we have an Official Recognition for a chronic disease maybe we can actually study one of them and that could help us with the others’ story.
Other Medical and Research News
From MR, more on the study on what happens when the FDA loosens its regulations on medical devices. What happens is that the devices get more innovative, effective and cheaper without being substantially less safe. Paper is more robust and compelling than I was originally giving it credit for, and I am moving up ‘lower thresholds for changing devices from Class III to II to I’ in Balsa’s list of candidate interventions.
Saloni offers a bunch of links and takes, for those interested.
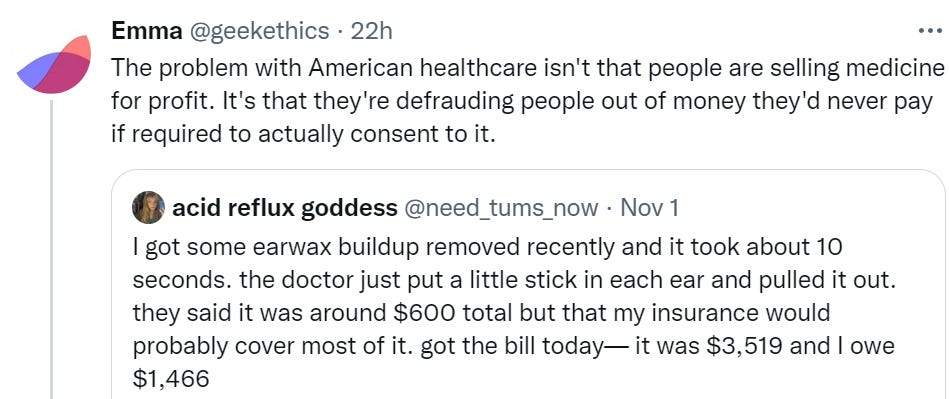
This is common. I have experienced very close versions of this.
From an ethical standpoint, this bill is illegitimate and should not be paid. This case is not even close.
What details would have to change before a $1,466 bill for a 10 second procedure the patient could have done herself (and a generic doctor visit) would carry an ethical obligation to pay? Purely on ethical grounds, I am going to go ahead and say it requires something like ‘you were warned explicitly that this could cost that kind of money and that you might have to pay for it, and you agreed to go ahead anyway.’
From a practical standpoint (not legal advice! not financial advice!) based on experiences I know about, when hospitals bill you like this it is mostly aspirational. They would love it if you paid this absurd bill. They also know it is an absurd bill. They could, in theory, if they wanted to, harass you, send your debt to a collection agency, report you to credit agencies or even sue you and attempt to seize your assets. In practice, that seems highly unlikely. The likely consequence is… nothing.
Another tale of the medical system lying to us.
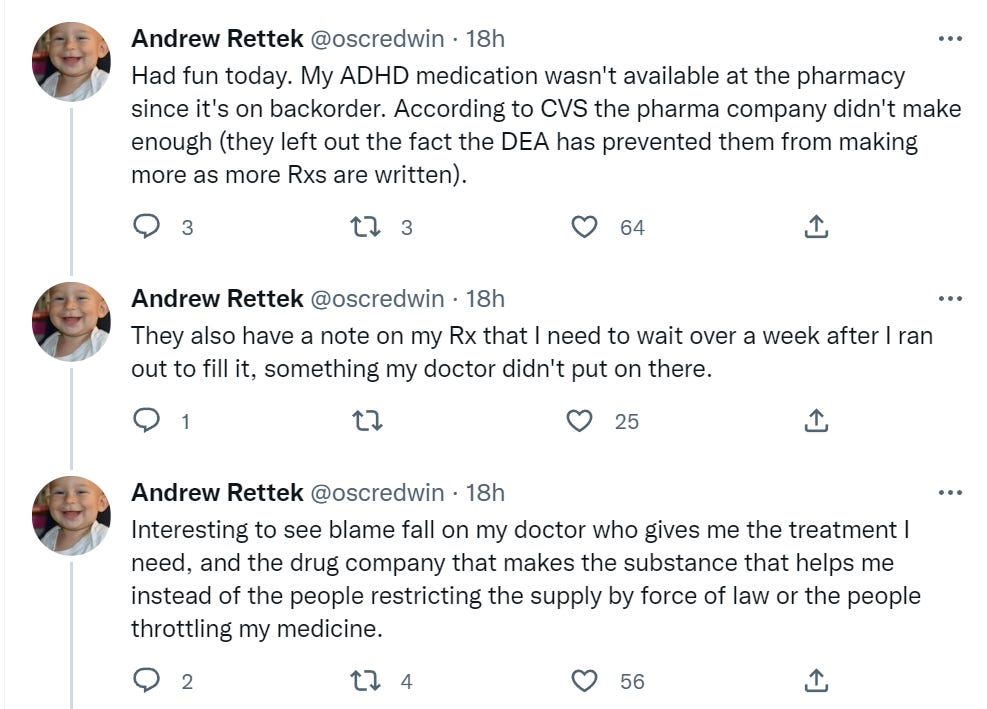
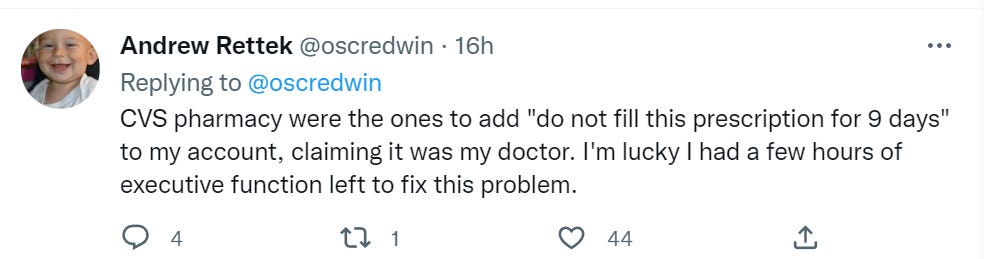
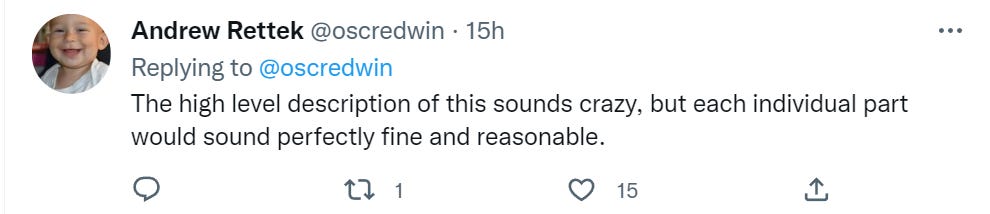
Hedges are often the most amusing part of such stories. None of this seems reasonable to me, including most of the individual steps. Also, ‘luckily I was able to spend several hours of executive function to fix this’ is not a happy ending. It is a very expensive ending.
Meanwhile, they are taking aggressive steps to ensure that drugs we all know work but who no one can afford to get FDA approval for never end up being taken by humans. It used to be you could get something approved cheaper in dogs or horses or cats, and then humans could get it and de facto make their own decisions. Now they are tightening the rules to prevent this, and there isn’t enough money on in animal medicine to pay for human approval, so the patent expires and the drug is never approved. The obvious stopgap solution to this is to make the first FDA approval of the drug a patent-extending event with respect to the FDA-approved uses it got approved for, for some reasonable period. The logic is the same as with normal patents, someone has to do the work and you need to be sure they are rewarded.
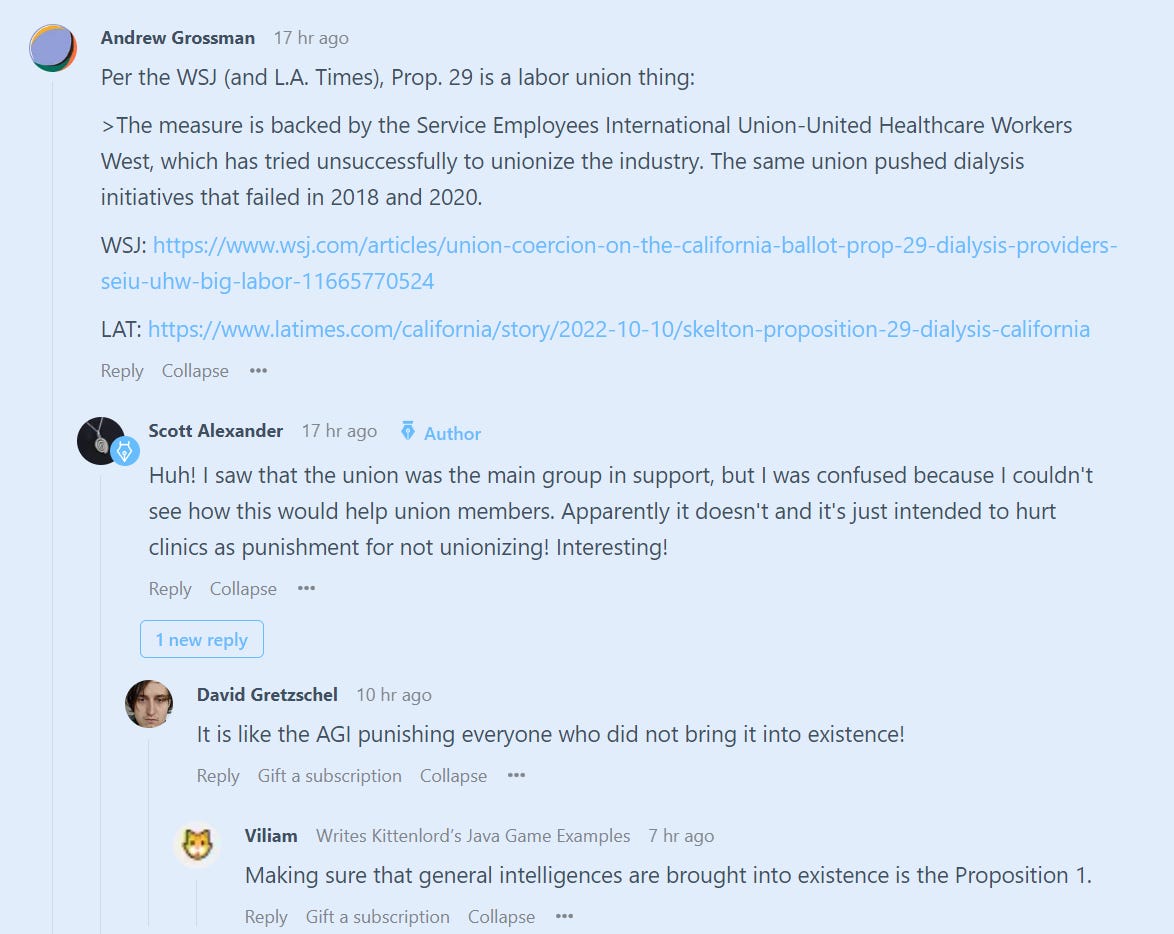
Scott Alexander wonders where the hell Prop 29 (aka The Kidney Thing That Keeps Getting Proposed Every Year) comes from and who is backing it and a comment answers it. Turns out it’s proposed… out of spite? (WSJ / LAT)
Explanation of the Alexander Technique as noticing and pausing when you are about to execute functions within yourself. Made the whole thing make sense to me, although I have no way of knowing if my new understanding is right or not.
In case you missed it, Zeynep’s Law.
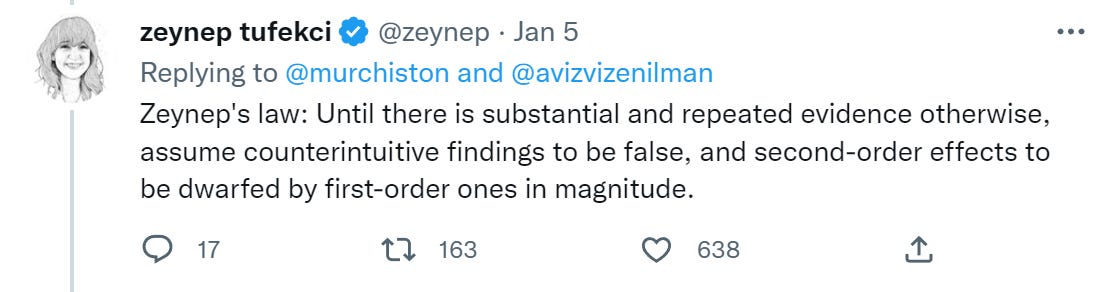
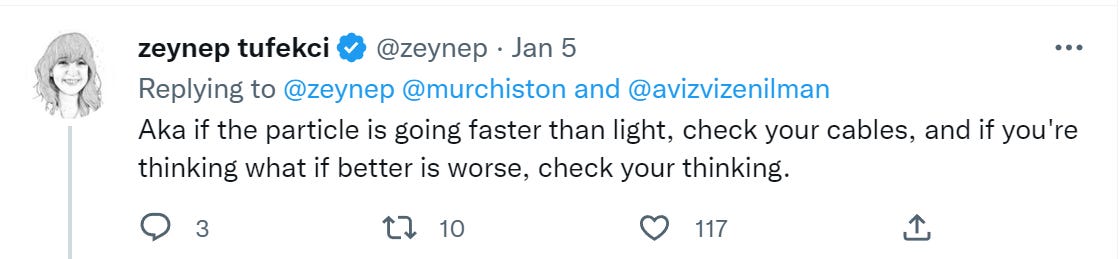
I am not entirely here for this. Mostly, though, yes, and I am totally here for the second formulation.
5 comments
Comments sorted by top scores.
comment by gabrielrecc (pseudobison) · 2022-11-10T15:52:01.400Z · LW(p) · GW(p)
Had a similar medical bill story from when I was a poor student: Medical center told me that insurance would cover an operation. They failed to mention that they were only talking about the surgeon's fee; the hospital at which they arranged the operation was out-of-network and I was stuck with 50% of the facility's costs. I explained my story to the facility. They said I still had to pay but that a payment plan would be possible, and that I could start by paying a small amount each month. I took that literally and just started paying a (very) small amount monthly. At some point they called back to tell me to formally arrange a payment plan through their online portal, which gave me options with such high interest rates that there was no way my future earnings would increase at a fast enough rate to make a payment plan make any sense whatsoever. I called back and explained this, and said that if those were the only options I guess I would just have to try to scrape the money together now, and that I was prepared to try to do this. The administrator, bless her heart, asked me to hold for awhile, and eventually came back to say "I've spoken with my colleagues, and your current balance owed to us is now zero dollars".
This (along with a few other experiences in my life) has underscored how sometimes an apparently immovable constraint can evaporate if you can manage to talk to the right person. That said, I felt very lucky to have been taken pity on in this way -- I feel like having one's balance explicitly zeroed out in this way is rare! But it's interesting to hear that Zvi knows of cases where someone just didn't pay, with no consequences. I would have assumed that they'd normally report nonpayers to credit agencies and crater their credit scores after long enough, as it costs them nothing or almost nothing to do so. Would be interested either to hear other people's anecdotes of what happened after nonpayment of a large hospital bill (positive or negative), or to see data on this if anyone knows of any.
comment by Gordon Seidoh Worley (gworley) · 2022-11-11T02:24:01.557Z · LW(p) · GW(p)
So I take an Alexander lesson nearly every week and have for something like 4 years now. I can say that the linked tweet about AT is basically right, although I think it overplays the level of conscious access you can get to what's going on. I generally describe it to people as behaviorist retraining of posture and movement: the methods of AT are nothing more than just getting you to develop new habits via dressed up clicker training, and they work really well because clicker training works really well. Your teacher stands and moves naturally, uses their hands to inform your body about what their body is doing, and your body slowly learns to copy what they're doing, all while your teacher says phrases that you come to associate with what's happening so you can just say something to yourself like "forward and up" and then your body does it.
Replies from: ChristianKl↑ comment by ChristianKl · 2022-11-11T10:54:06.182Z · LW(p) · GW(p)
The Alexander Technique is old. One of the implications of that is that over time different teachers evolved different ideas and there are significant differences between teachers. The one teacher with whom I had a 5-day course said that in her teacher training they practice sitting up and sitting down for hundreds of hours. I was talking with another Alexander technique teacher and they said that didn't do the "sitting up and down"-thing that intensely.
The level of conscious access you can get with one lesson per week and the level that you can get with very intensive training are different.
If you approach it as a behaviorist exercise as you describe that's not a practice of increasing conscious access. If you want to train conscious access then it would make sense to add more of a Feldenkrais-like approach of playful discovery. In that, the teacher's job is to point your attention to what's outside of your attention.
comment by tkpwaeub (gabriel-holmes) · 2022-11-16T11:53:37.405Z · LW(p) · GW(p)
Re medical bills (or any bills, for that matter):
A major change from the TCJA in 2017 was allowing more businesses, including some health care providers and third party debt collectors, to use cash accounting rather than accrual accounting for the purpose of computing taxable income. The upshot is that treatment plus a printed and mailed bill no longer counts as revenue for a lot more businesses. That's precisely what allows for the "aspirational" bills you're describing. Repealing this provision would go a long way to taming this particular aspect, I believe.
comment by Lao Mein (derpherpize) · 2022-11-11T01:21:13.314Z · LW(p) · GW(p)
Maybe obscuration of medical costs is a social thing? Here in China, there is a giant LED board in hospitals that lists the exact costs of various medical procedures (e.g. "Hip replacement: $1000"). But I imagine seeing hyper-expensive medical costs at every visit might be upsetting to a lot of people in the US.