Omicron Post #3
post by Zvi · 2021-12-02T15:10:00.632Z · LW · GW · 15 commentsContents
Biden on Omicron Vaccine Approval Travel Restrictions Omicron Everywhere New EU Assessment New Summary Thread The Timeline Other Omicron Links Probability Updates Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 35% → 40%. Chance that Omicron will displace Delta: 80% → 85%. Chance that Omicron is importantly more virulent than Delta: 10% → 8%. Chance that Omicron is importantly less virulent than Delta: 40% → 35% Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 80% → 80% (no change). Will the CDC label Omicron a variant of high concern before 2022? ?% → 15% Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 4% → 3%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30% (unchanged). Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 3%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 15% → 12%. Will Omicron be >1% of all cases by the end of the year? ?% → 70%. None 15 comments
I have split off the Omicron post from the weekly post, which covers other aspects of Covid. I made judgment calls on where to put a few things.
Omicron continues to spread quickly, but the news surrounding Omicron is clearly slowing down, so these updates can hopefully space out a bit more.
Post on Polymarket’s Covid prediction markets, and potential future markets discussion. Direct link to market on whether Omicron will be >1% of cases by the end of the year, which is currently a moderate favorite.
Biden on Omicron
A few hours after my second Omicron update, Biden went on TV to talk about the new variant.
Here are some highlights:
(1:00) He says that he told us he would always be honest with us, so he’s going to talk about the new Omnicron (which I do admit sounds cooler) variant. Damn that campaign promise, guess we’re going to have to be honest.
(1:00) He says that South Africa’s transparency in telling us about Omnicron is to be applauded, for it allows us to take action, so he took action right away to cut off travel to South Africa. What even are incentives, how do they work, not a metaphor for entire legislative agenda?
(1:30) We can’t stop Omnicron, we can only slow it down, giving us time to take other actions. Therefore get vaccinated. ‘Cause for concern, not cause for panic.’ Because we’re the best, you see, and also science.
(2:30) ‘We have more tools than ever to fight the variant. From vaccines to boosters, to vaccines for children.’ So… vaccines? We have vaccines? ‘And much more.’
(3:00) Did you know ‘deaths from Delta are coming down’? Checks notes.
(3:30) Booster. Vaccinated. Vaccinated. Booster.
(4:30) Mask.
(4:45) This, which I wish I fully believed:
We will now find out what counts as ‘every available tool.’ Also, why aren’t we using ‘every available tool’ with regard to, let’s say, Paxlovid?
(5:30) I will tell the CDC and FDA to use ‘the fastest process available without cutting any corners.’
Wait, if there’s a faster process available that doesn’t cut any corners, then… then…
(5:45) Same thing for ‘modifications to current treatments for those who get ill with the Covid virus.’
(5:50) “Look, I’m removing all roadblocks to keeping the American people safe.”
Paxlovid remains illegal.
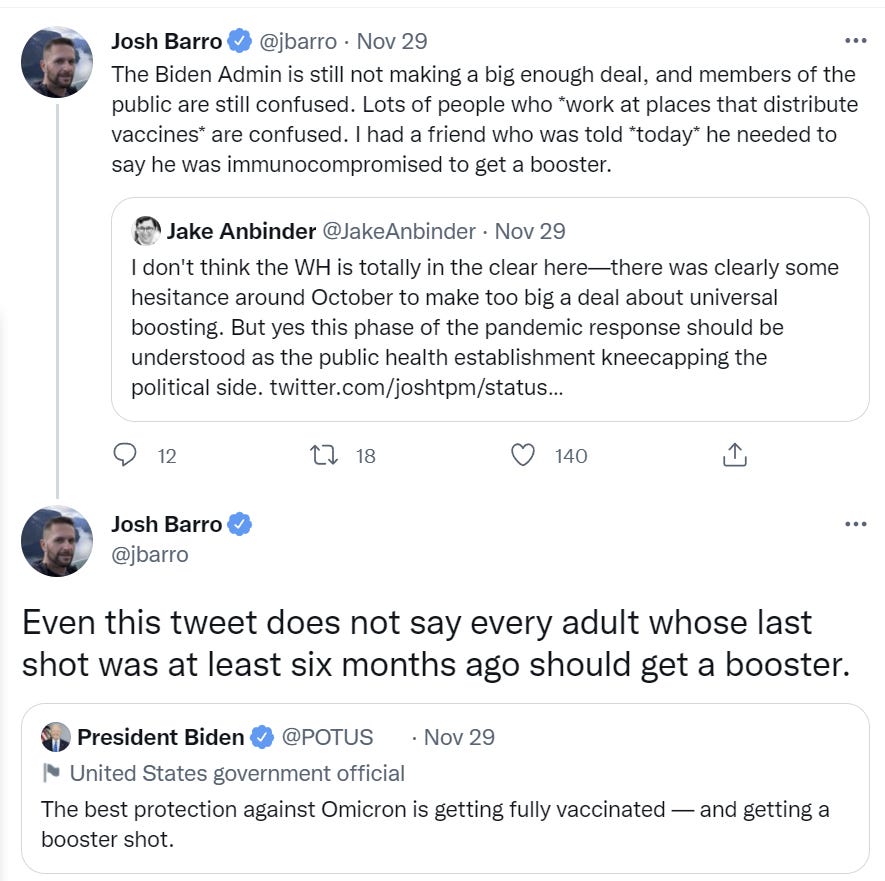
(6:05) “If you are vaccinated and worried about this virus, go get your booster.”
Logically this implies that if you have gotten your booster, you should not be worried about this virus. Interesting.
(6:25) Promises a plan for the winter on Thursday that will not use lockdowns, but will use ‘widespread vaccinations, boosters, testing and more.’
(7:00) This statement, the last line of which is pretty rich:
It’s time for the ‘rest of the world’ to ‘step up?’ This is a competition and we’ve set the high score so never mind all the extra doses we could have manufactured, or the ones we’re letting expire, or sit for months in warehouses despite our unwillingness to approve them? It doesn’t matter whether we’ve done our ‘fair share’ or some such nonsense, or who is ‘leading’ it matters what we can do and whether we’re doing it.
He then assures us that no shot given overseas will ever ‘come at the expense of any American’ and he will ensure we are protected first. So get your booster now, to make it easier to send doses overseas?
(9:00) “We’re throwing everything we can at this virus. That’s how we reopen our [various].”
Thing is I think he actually believes that we are throwing everything we can at this virus? And that doing so is ‘how we reopen’ as opposed to deciding to reopen or stay open?
Questions start.
(10:00) Q: Do you think that there will be a future reluctance to report variants due to the reaction this time?
A: No, nor am I going to address the incentive problem at all.
Once again, it is vital that we actively reward South Africa for having good records, seeking accurate information and sharing that information. Otherwise, you get what you pay for, and you’ll deserve it. We need to be louder about this.
At far less than the bare minimum, we need to ensure that we don’t let them run out of vital reagents for their work.
Q: What are we doing to detect Omicron here?
A (from Fauci): First, we required testing and proof of vaccination for travelers even before Omnicron. Our PCR tests, fortunately, do pick it up.

Q: Are you considering additional travel restrictions? Are you calling upon state and local officials to reinstate mask mandates?
A: I’m encouraging wearing masks indoors except for eating or speaking at a microphone. I might do more travel restrictions if things get bad enough, but I don’t anticipate it.
Those restrictions would be put into effect when they’d do less than no good.
Q: Will things like intermittent travel restrictions be the new normal? Why are you taking lockdowns off the table?
A: I expect this not to be the new normal, because the new normal will be that everyone gets vaccinated and boosters so we don’t see the spread of these viruses. And yes, lockdowns are off the table because ‘if people are vaccinated and wear masks there is no need for lockdown.’
Vaccines are magic. Masks are talismans.
Q: Are you considering requiring Covid tests for domestic flights?
A: At this point that’s not been recommended. I would wait for the scientific community to give me a recommendation on that.
Because, you see, Biden is Following the Science rather than making decisions.
What would it mean to be doing all we can? Even purely on vaccinations, including booster shots?
Presumably it would start with getting rid of any and all barriers to vaccinations or booster shots. Instead we have things like this, where we continue to force people to lie or otherwise do unpleasant things.
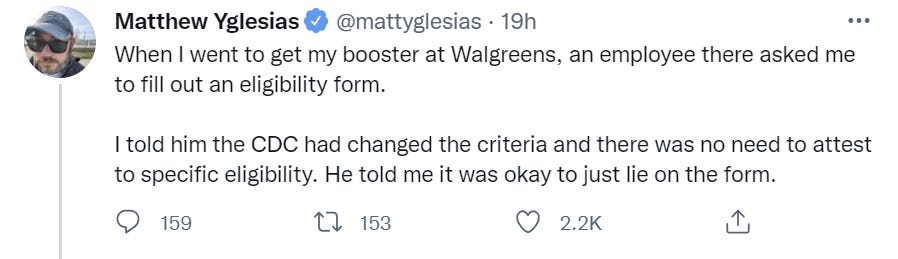
A large percentage of people considering a booster, that I know about, at least delayed getting boosted over such concerns, and almost all of them had stress about them.
Yet the messaging on this somehow remains less clear than it could be. The policy is right, but one still needs to ensure that everyone knows what the policy is.
Even if you don’t think that ‘normalize lying on official forms’ is inherently a problem, or punishing the scrupulous is a problem: Beware trivial inconveniences. [LW · GW] If we can’t even make people not lie on forms (or, much better, have them skip as many forms as possible outright, people hate forms) and such issues barely get noticed at all, that doesn’t speak well to how serious our other efforts are going.
Vaccine Approval
Biden promises explicitly to approve a new vaccine variant with all possible speed.
The European Union is saying they can do it in 3-4 months.
“Companies adapting their formulations to include the new sequencing (…) will then have to show that the production system works, they will then have to do some clinical trials to determine that this actually works in practice.”
Total civilizational failure. If we do need such an update, we probably do not have 3-4 months. By the time those months elapse, and the new shots are distributed and given, the game will mostly already be over. It’s still worth bothering, but in terms of most of the lives you could have saved, you lose. Good day, sir, and good night.
Travel Restrictions
The Biden administration and CDC (it’s not clear who is really in charge) considering additional requirements for all travelers coming from anywhere, including Americans (WaPo).
The Biden administration is preparing stricter testing requirements for all travelers entering the United States, including returning Americans, to curb the spread of the potentially dangerous omicron variant, according to three federal health officials.
As part ofan enhanced winter covid strategy Biden is expected to announceThursday, U.S. officials would require everyone entering the country to be tested one day before boarding flights, regardless of their vaccination status or country of departure. Administration officials are also considering a requirement that all travelers get retested within three to five days of arrival.
In addition, they are debating a controversial proposal to require all travelers, including U.S. citizens, toself-quarantine for seven days, even if their test results are negative. Those who flout the requirements might be subject to fines and penalties, the first time such penalties would be linked to testing and quarantine measures for travelers in the United States.
This only makes sense if you think that Omicron is in many other places in quantity but isn’t in the United States in similar quantities. Otherwise, this will have only a nominal effect on Omicron but a large effect on travel. The differential is why a restriction on Southern Africa plausibly makes sense, once it’s gone such restrictions need to be lifted.
Normally, I’d laugh at what such folks consider speed.
Other key details were still being ironed out Tuesday. It’s not clear when the new policy would take effect. But given the urgency of limiting the spread of what might be a highly transmissible variant, speed is considered essential. It’s possible the policy could take effect in a week or two, according to one official.
In this case I won’t, because if it’s flights from arbitrary locations then there’s no longer a speed premium. There’s not an anything premium, but there’s especially not a speed premium.
Here is how we think about ‘requirements’ these days, and how much we both don’t do cost-benefit calculations at all and use performative rules to punish the scrupulous.
As a practical matter, stateand local health departments are unlikely to be able to enforce requirements for additional testing and anyself-quarantines once travelers arrive in the United States. More than 200,000 people arrived by plane daily in November, a figure that does not include travel over the Thanksgiving holiday, federal authorities said.
Even if only a quarter of those travelers comply with the requirements,however, it would make a difference by allowing for more prompt detection and isolation of at least some infected people who might be able to spread the virus, said public health experts.
“If you consider over 200,000 people a day [arriving in the United States], even 50,000 would help” determine the extent of spread, one of the three federal health officials said in a text message.
Janet Hamilton, executive director of the Council of State and Territorial Epidemiologists, said that such measures are “a critical step for reducing transmission of SARSCoV-2, whether we are dealing with a newly emerging variant like Omicron or working to reduce transmission of already circulating strains.”
If you want to ask people to voluntarily do such testing, sure, that’s great, ask them. Pretending these are requirements with no ability to enforce or expectation of adherence is rather awful.
I do agree that such policies, if they were able to differentiate who had Omicron versus Delta, would be highly useful information, which is the main reason to ask nicely, as other methods of getting the same information are likely harder to implement right now. Otherwise, there’s no point, unless I’m misunderstanding the math involved.
As a personal data point: My wife and I had booked a vacation trip to Cancun in January. If it was a matter of a few extra Covid-19 tests, I doubt that would make any difference. If we were suddenly on the hook for a weeklong quarantine, and it was enforceable, we would be forced to cancel the trip because with kids involved there’s no way to quarantine at a ‘reasonable price.’
Omicron Everywhere
This seems rather alarming in terms of the timeline and spread, the full thread seems worth reading:
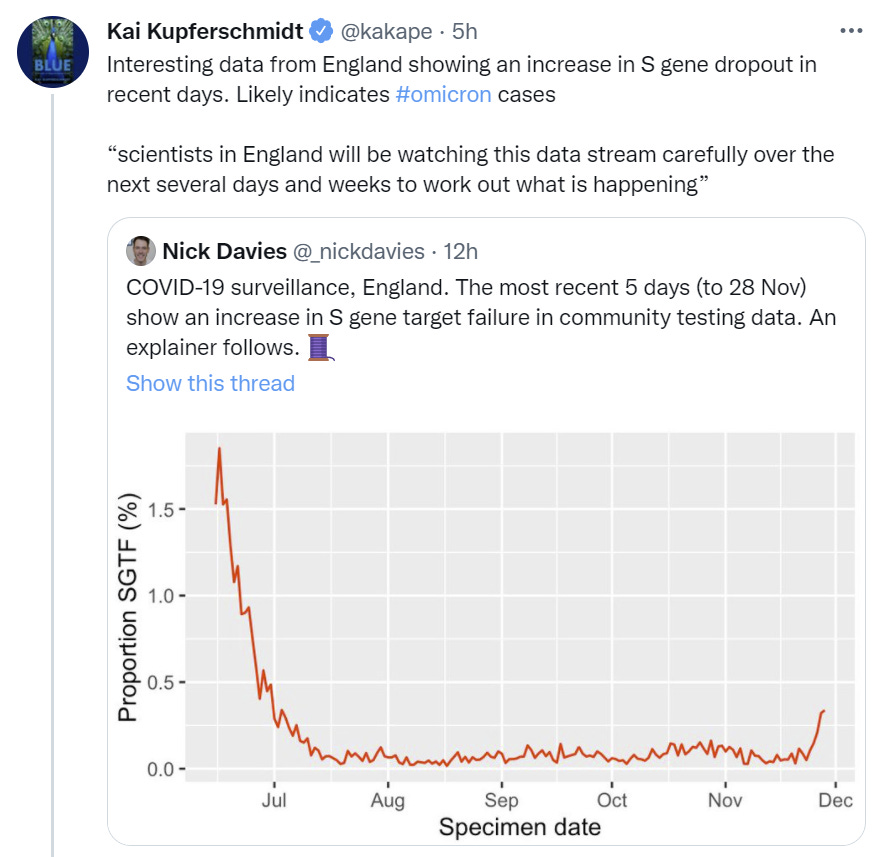
The thread warns this is an imperfect proxy but I do not believe in this level of coincidence.
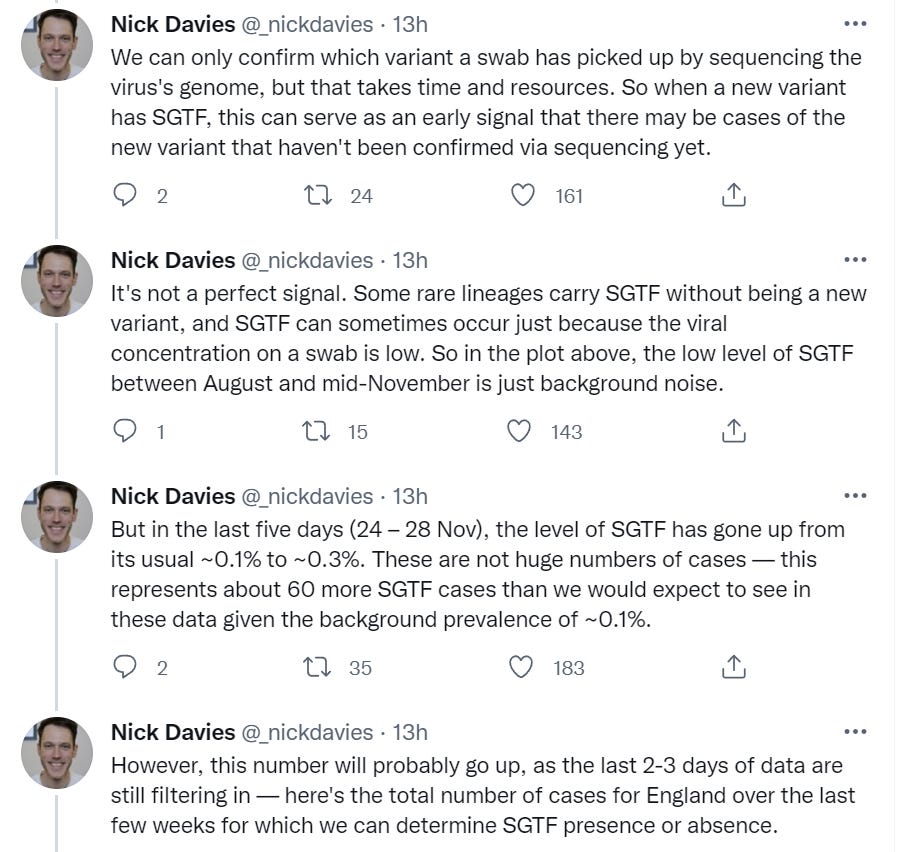
The lag on this is several days:

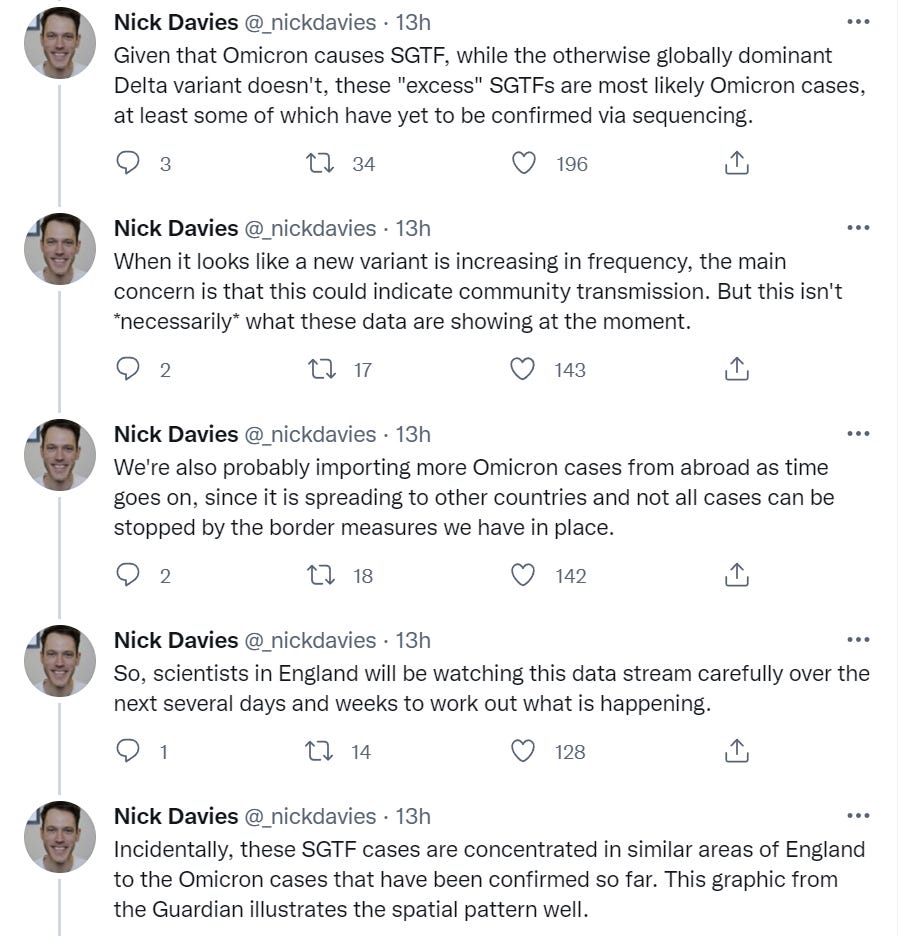

This seems like there’s an extra ~0.2% incidence of SGTF above the old baseline, and it happened over the course of about a week. If we are already at 0.2%, and growth rate mirrors what happened in South Africa, the situation is about to escalate very quickly. We’ll know in a few days if that happens, but if this hits 0.4% extra (0.5% total) within 2-3 more days, then it’s time to buy the ‘1% of cases by end of year’ futures very aggressively and open markets with a much higher target percentage.
The Dutch and others are reporting the presence of Omicron up to 11 days before South Africa announced the presence of the new variant, and they don’t know that the cases involve contact with South Africa.
Dutch health authorities announced on Tuesday that they found the new Omicron variant of the coronavirus in cases dating back as long as 11 days, indicating that it was already spreading in western Europe before the first cases were identified in southern Africa. The RIVM health institute said it found Omicron in samples dating from November 19 and 23.
…
Belgium and Germany have also said that sample tests confirm the variant was in those countries before South African health officials alerted the world on November 24 to its existence.
…
“It is not yet clear whether the people concerned [in the earlier cases] have also been to southern Africa,” the RIVM said, adding that the individuals had been informed of their Omicron infections and that local health services had started contact tracing.
If tests looked at people who were in South Africa earlier, and found Omicron, that’s unsurprising but moves up the timeline a bit. If tests looked at random people with no link to Southern Africa and they found Omicron, that means it’s already a non-trivial presence, the game is going to end that much faster, and the travel bans probably shouldn’t last too much longer because they’re not going to make much of a difference.
New EU Assessment
This came out Thursday morning New York time. Here’s the direct link to the report.




This was new to me as well:

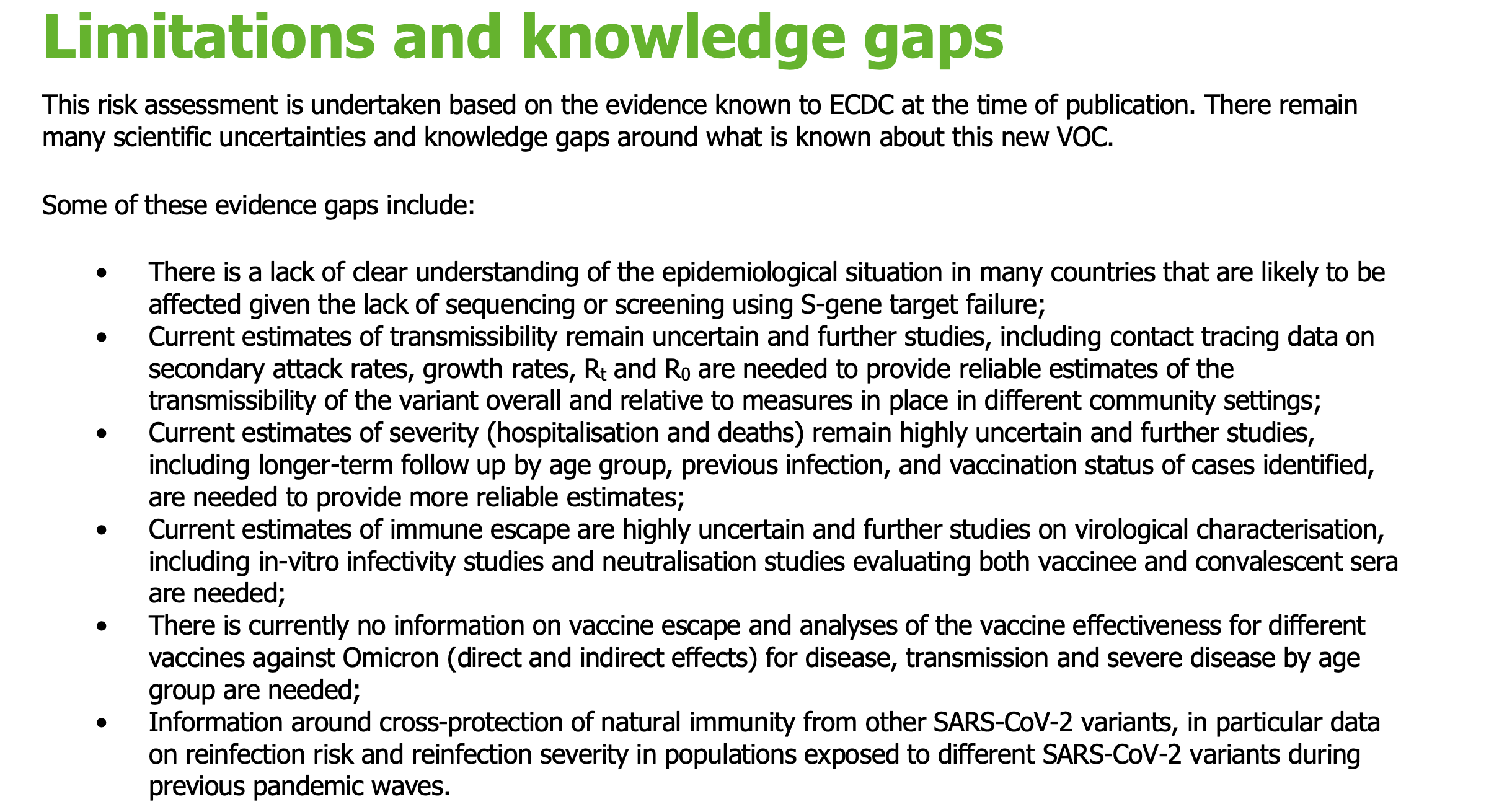
Based on what we’re seeing in England, two weeks is starting to look generous at this point. That’s still a valuable two weeks, but keeping the bans around much longer than that seems not very useful. I’d like to see announcements that all travel bans will be lifted at the end of the year for anyone not attempting a full closure (e.g. not trying to actually win the game but only lose slower.) And again, to accompany it with concrete thanks to those we have been cutting off to make them whole again.
I noticed this:
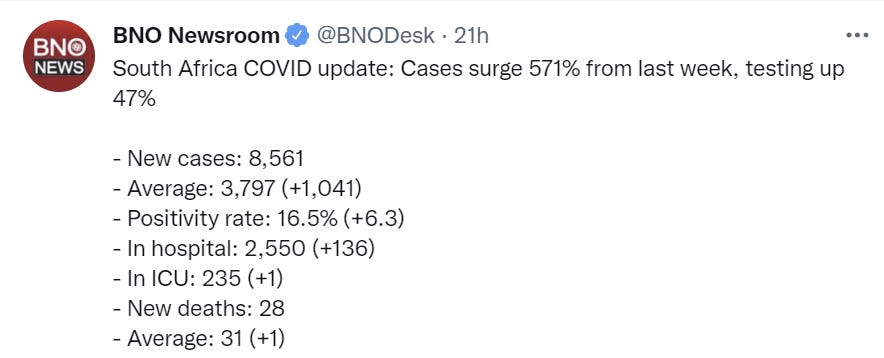
Data from South Africa indicate an increase of hospital admissions of COVID-19 cases in the Gauteng province from 136 on week 45, to 279 in week 46, and to 647 on week 47, concomitantly with the increasing predominance of the Omicron VOC among the reported COVID-19 cases [40]. While case rates are increasing faster than in previous waves in the Gauteng province, hospitalization rates are in line with previous increases [41]. The age structure of affected cases in South Africa is not known to ECDC, so it is unclear how this may impact on the risk of hospitalization and/or ICU admission among affected cases.
This is strong evidence that either Omicron is less severe and/or Omicron is infecting less vulnerable people, which would likely be due to immune erosion properties but could perhaps also be due to coincidental infection patterns, although that gets rapidly less plausible over time as this scales higher.
If Omicron doesn’t have immune erosion properties, that would not only be great news, it would mean that Omicron itself is also great news.
They’re still trying to prioritize over booster shots, which is odd since it’s hard to believe there’s a supply shortage:
As has been highlighted previously, countries should consider a booster dose for those aged 40 years and above, first targeting the most vulnerable and the elderly and then expanding to all adults aged 18 years and above at least six months after completion of the primary series.
They support using the S-gene deletion as a proxy for Omicron:
S-gene target failure (SGTF) using the Thermo Fischer TaqPath assay or other similar assays that fail to detect the S-gene when it carries the deletion Δ69-70 can be used to screen for the Omicron VOC. From currently in GISAID deposited sequences in Europe reported during week 44-47 2021 (GISAID data as of 2021-11-30) it can be concluded that no non-Omicron variants with Δ69-70 are circulating and therefore the SGTF can be reliably used as a screening method for the identification of the Omicron VOC. Extremely low number of non-Omicron sequences with Δ69-70 have been submitted to GISAID worldwide. However, it cannot be excluded that other variants with this genetic profile emerge in the future or are already circulating in very low levels. It is therefore recommended that a subset of samples with SGTF should be selected for confirmation by sequencing (at least 10% or according to available resources).
I note that they are recommending a percentage of cases be sequenced as opposed to a fixed number of cases, which seems wrong? What matters is the number of sequences you do rather than the percentage, unless I’m missing something.
Overall this seems like about as good a document as we could have hoped for from the European Union at this point. It isn’t dense with new information and doesn’t attempt synthesis under uncertainty, but those would be unreasonable expectations. They’re epistemically, politically and otherwise restricted. Within those restrictions they mostly acquit themselves well.
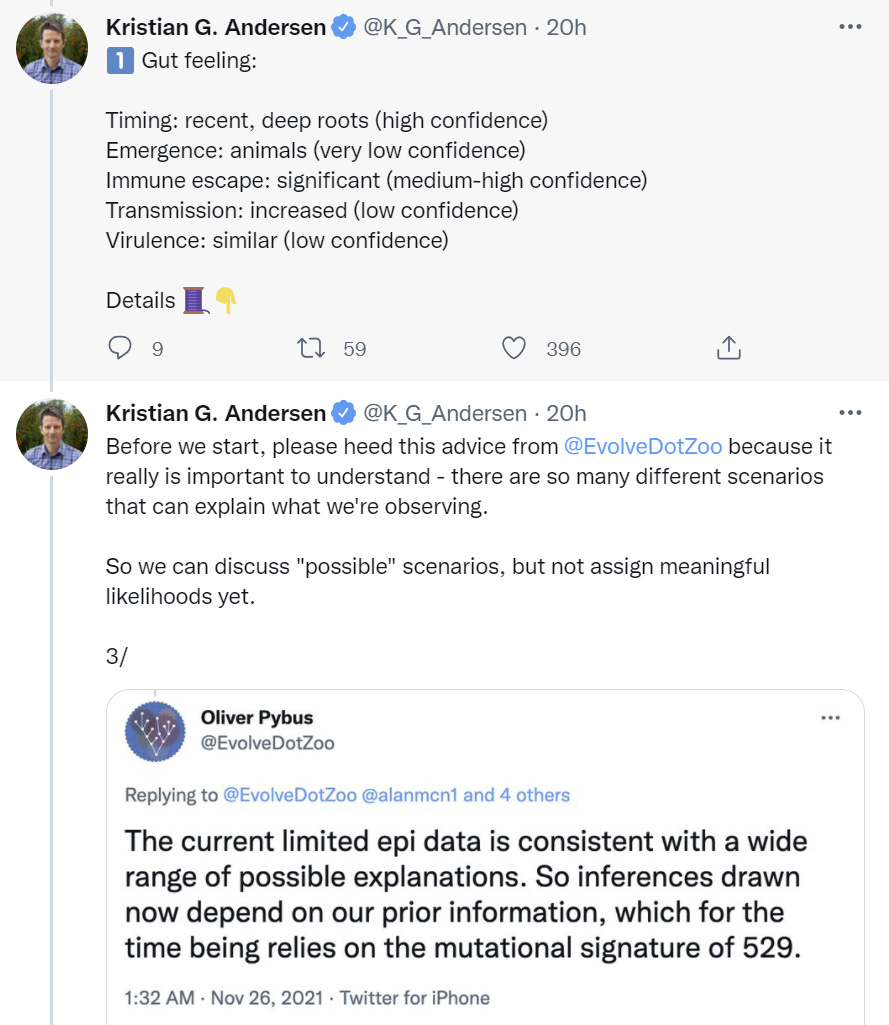
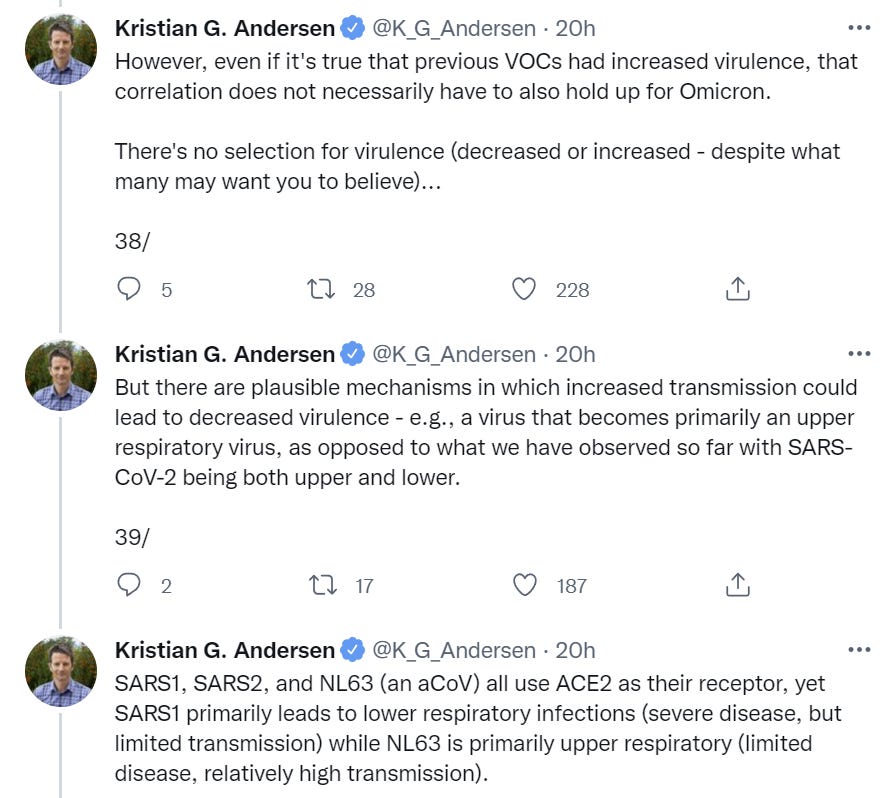
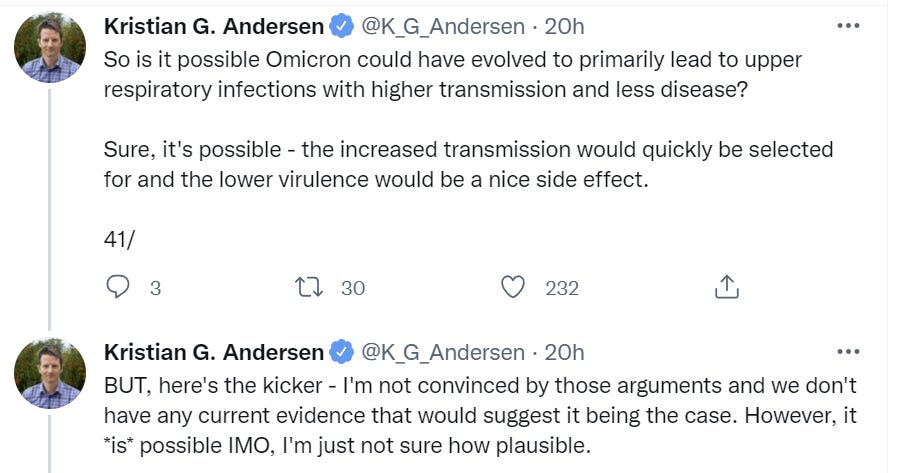
New Summary Thread
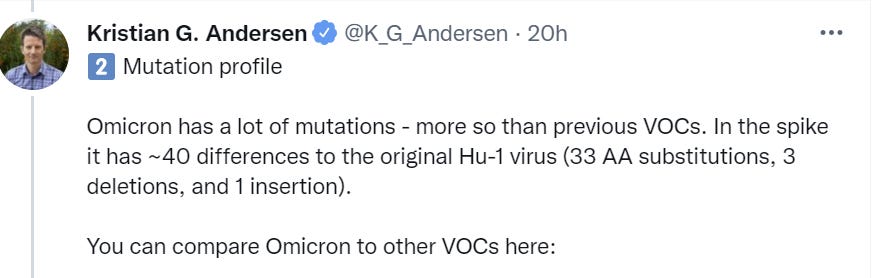
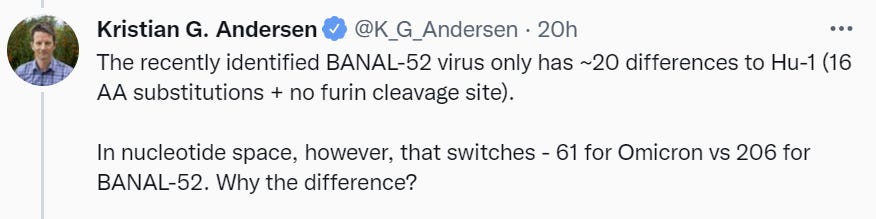
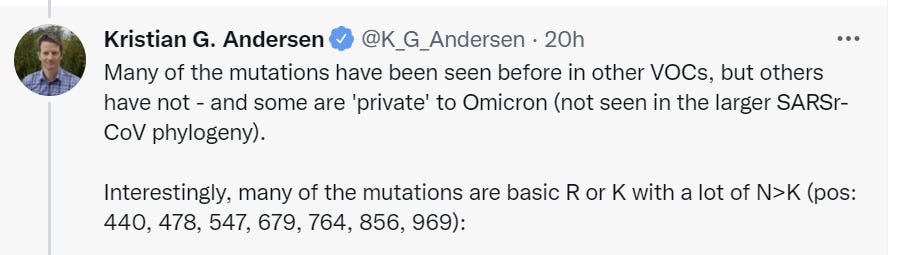
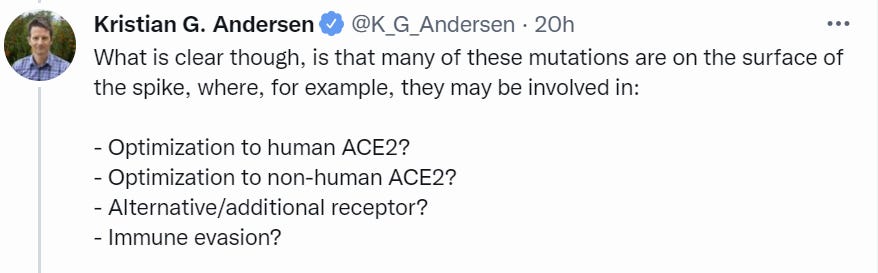
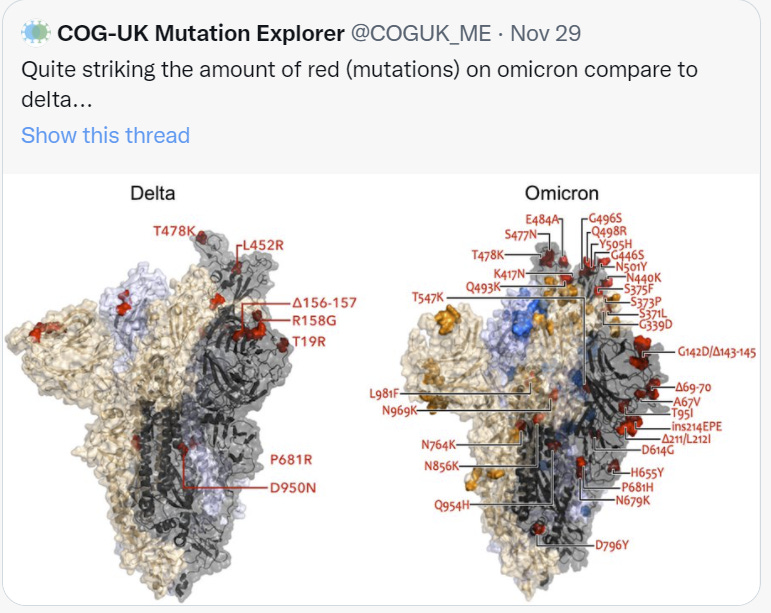
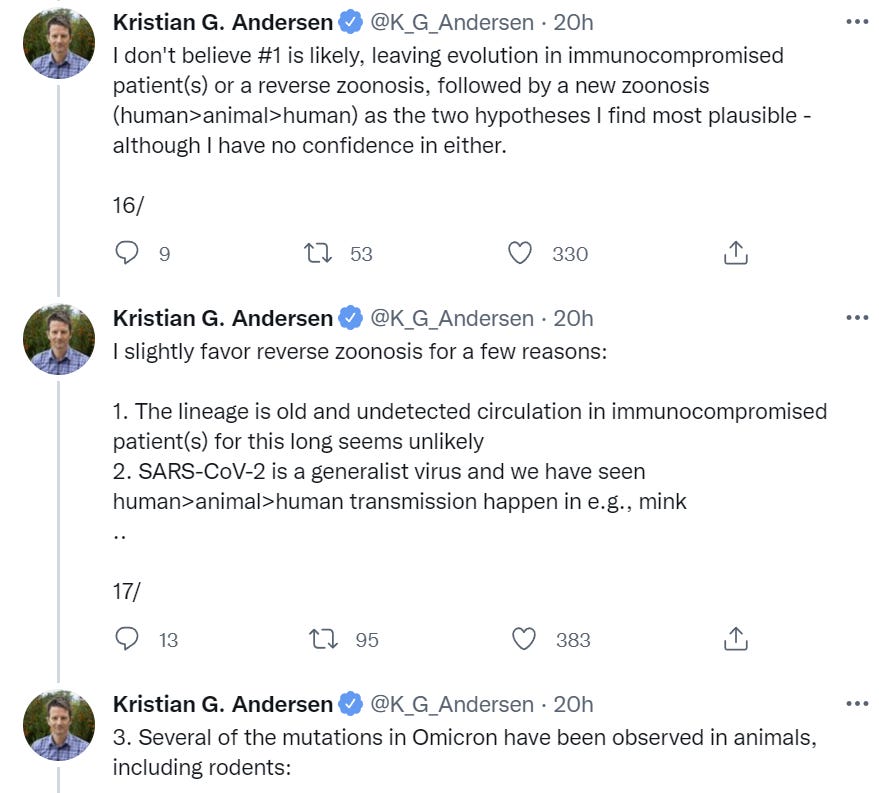
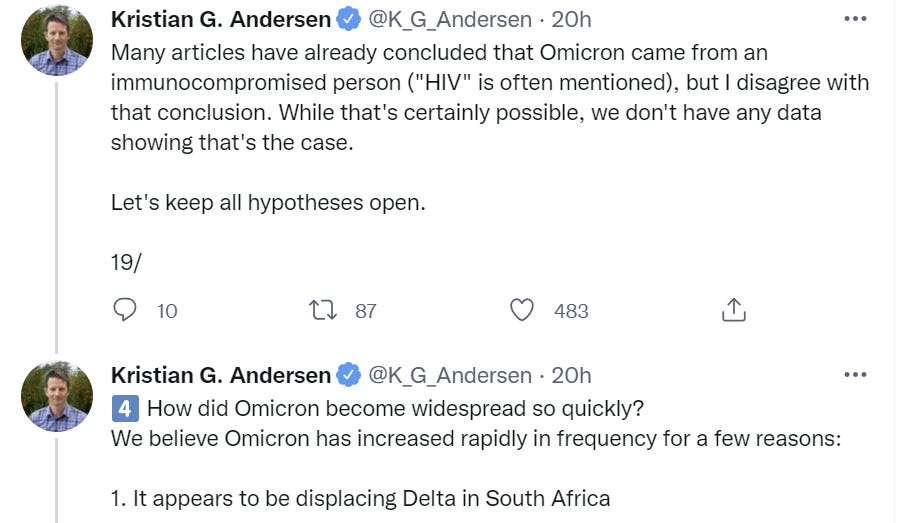
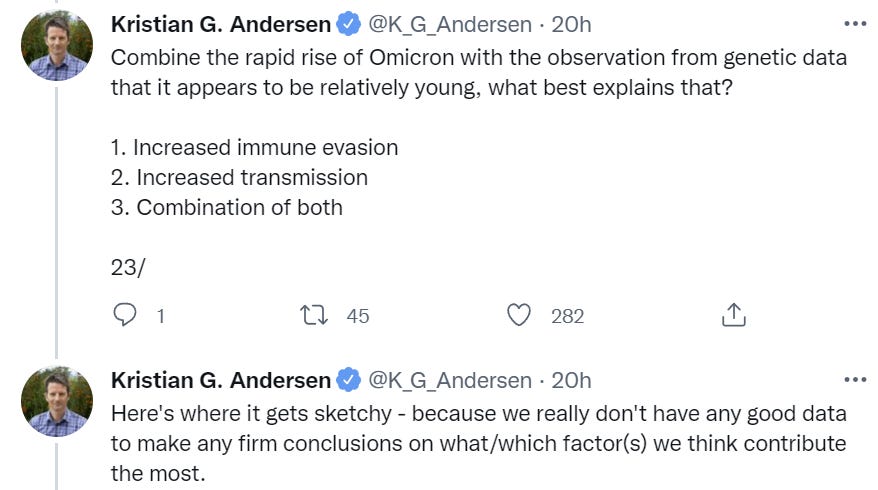
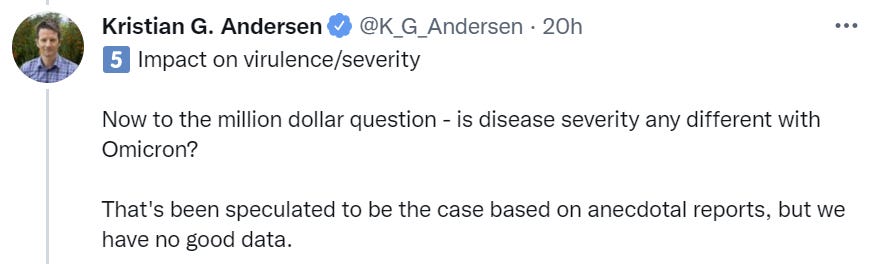
Here’s Kristian Anderson on what we know so far, which went up on Tuesday. He favors zoological origin for Omicron, points out it’s impossible yet to differentiate higher transmissibility versus immune erosion but expects to find both, and thinks it emerged recently and is rising rapidly. Nothing inconsistent with previous understanding, but lots of good details.


Link is here. We mentioned it last time, it’s one of those accurate and helpful as first steps but not that useful beyond that types of write-ups.
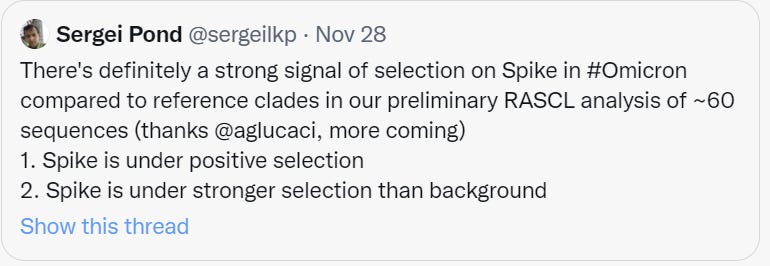



He then links to this study.


He then links to this Trevor Bradford thread.









There’s a bit more but I’m stopping here for length.
The Timeline
As usual, this is in chronological order, and thanks again to BNO Newsroom (Ko-Fi / Patreon if you want to help them out). This begins on Monday right after the last timeline stopped.



I’ll stop including ‘first confirmed case’ reports here except for the USA.



Despite not being worried about being infected, I think I am an underdog to take my Cancun vacation in January.

We’re not looking all that hard. Meet the new boss and all that.


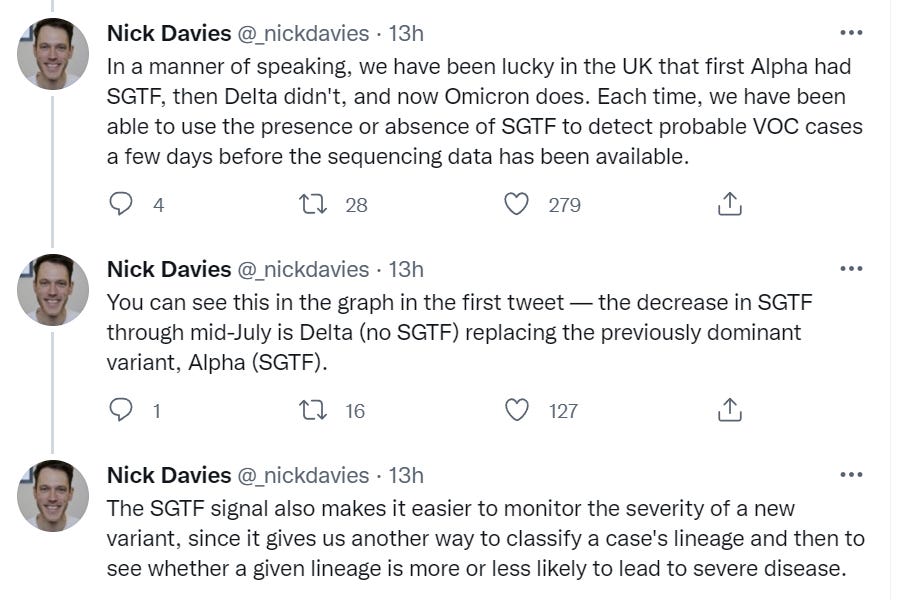
This looks like what we would see if Omicron had a large transmission advantage, and it clearly has a very large advantage in Africa, but isn’t quite yet unmistakably that outside of Africa. Note that England’s S-deletion data didn’t appear on the timeline, but is an important data point.
Other Omicron Links
This is the official CDC variant tracker.
Zeynep thread that points out we don’t know much yet.
Trevor Bradford thread on how transmissible and immune erosive Omicron might be.
Israel’s health minister claims initial signs are promising that vaccine protection will remain robust, without indicating how they have sufficient information to make even that preliminary statement. I’m all for synthesis of everything we know and being a Bayesian, but I doubt that’s what’s happening here and a lot of this was oddly specific.
That explains where these ‘memes’ start.

We don’t know that Omicron is mild, but we also don’t have ‘absolutely no evidence’ that is mild. Once again this is not how evidence works.
South African wastewater data.
Paxlovid expected to be effective against Omicron.
Mina explains why some vaccines stop transmission and some don’t, for those who don’t know.
Probability Updates
In general, everything seems broadly on track with previous observations, so I was able to mostly get more confident.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 35% → 40%.
More data from South Africa and the deletion data from the UK are suggestive that the edge in practice is very high, but it’s still too early to know much. Updating this little feels somewhat unprincipled, but the South African data wasn’t all that surprising. Prediction market data is also suggestive.
Chance that Omicron will displace Delta: 80% → 85%.
Displace here means ‘Omicron has a large percentage of all USA cases and a lot more USA cases than Delta at some point in 2022.’
Prediction markets are favoring rapid spread of Omicron in ways that imply this is very likely, and sooner rather than later, but we still don’t have the smoking gun that this is happening in the developed world, and I worry people don’t realize how hard it is to get to 1%. If I saw people looking to bet directly on the yes side here at these kinds of odds or higher, I’d likely increase my fair value quickly.
Chance that Omicron is importantly more virulent than Delta: 10% → 8%.
Chance that Omicron is importantly less virulent than Delta: 40% → 35%
The decline from 40% to 35% is mostly me having time to reflect on our evidence, rather than me updating on new evidence. Note that the comparison here is ‘in the same individual’ rather than the average case, since the average case is more likely to be a breakthrough and thus milder. The decline from 10% to 8% is a case of new news being good news.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 80% → 80% (no change).
Will the CDC label Omicron a variant of high concern before 2022? ?% → 15%
We are still waiting to know for sure. I do expect this but I don’t think we have reason to be more confident than we were before.
The VOHC question is far less clear, and the new prediction market on that has it at 10% which is why I’m adding this question. That’s about the decision process as much as it is about the properties of the Covid, and someone bet some real money on the No side, so it’s hard not to mostly believe that they’re right about the speed at which such things move, but it does seem like 10% must be a little low, so for now I’m going with 15% but assume that I’m at least as high as the prediction market so long as it’s not above 30% or so, at which point I’d have to think more.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 4% → 3%.
We got additional assurances, and additional revealed preferences not to be too hurried about new versions of boosters, and no news is good news.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30% (unchanged).
I don’t see that much urgency and the vaccines seem more confidently to still be effective against severe disease, but I do see things headed towards modifications of the vaccines, so sticking where I was for now.
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 3%.
There’s no reason to suspect this and I see more assurances not to worry, but there’s always some chance until there’s an encounter with the enemy, and given this says ‘less’ rather than ‘substantially less’ I probably got a little overconfident earlier.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 15% → 12%.
Biden’s assurances about lockdowns were politically the clearly correct thing to say unless you expect to have to do lockdowns, but they also make it that much harder to go back on those assurances, and it is increasingly clear that even if Omicron isn’t less virulent in any given case it will be less virulent in general plus we’ll probably have access to Paxlovid in time. I’m somewhat less worried about this.
Will Omicron be >1% of all cases by the end of the year? ?% → 70%.
The data in the United Kingdom suggests that we are on a rather fast schedule, but I notice that this implies that Omicron will rapidly displace Delta, and there are a lot of ways for that to happen despite things going slower than this, so it’s hard to get this number too high yet. There’s a prediction market available if you’re interested.
15 comments
Comments sorted by top scores.
comment by Rafael Harth (sil-ver) · 2021-12-02T16:19:12.381Z · LW(p) · GW(p)
(6:05) “If you are vaccinated and worried about this virus, go get your booster.”
Logically this implies that if you have gotten your booster, you should not be worried about this virus. Interesting.
It does not. "go get your booster" is clearly short for "you should get your booster assuming you don't already have one". The negation of that isn't "you already have a booster", it's "you should not get your booster even if you don't already have one". So the contrapositive of this statement is "if you shouldn't get your booster even though you don't already have one, then you shouldn't be worried about the virus".
(You can also see that something went wrong with the implication you've drawn, seeing as you've derived an unreasonable statement from a reasonable one. The contrapositve is logically equivalent, it can't be less reasonable.)
Replies from: Zvi, J Mann↑ comment by Zvi · 2021-12-02T19:39:15.330Z · LW(p) · GW(p)
I disagree that the derived statement is unreasonable. I also disagree that it's obviously saying something other than what it literally says.
Replies from: oumuamua↑ comment by oumuamua · 2021-12-03T09:12:19.823Z · LW(p) · GW(p)
Saying "if you are worried, you should get your booster" is not at all equivalent to "if you have gotten your booster, you should not be worried about this virus".
The first statement permits that one can still be worried after having gotten one's booster (just a little less), which the second statement does not permit. Therefore, those two statements cannot be logically equivalent.
If you had written "if you have gotten your booster, you should not be as worried about this virus [as before]", that would have been fine.
Replies from: TurnTrout↑ comment by TurnTrout · 2021-12-03T16:48:17.719Z · LW(p) · GW(p)
Flag: even being less worried is an additional inference not demanded by the form of the contrapositive of "if you're worried, you should get your booster" . But that's just a nitpick over how literally we're meaning logical equivalence.
↑ comment by J Mann · 2021-12-02T17:27:09.985Z · LW(p) · GW(p)
Presumably, a more complete statement would be "If you are vaccinated and worried about this virus, go get your booster. If (or once) you have your booster, if you're still worried, increase ventilation and limit social contact, particularly in poorly ventilated spaces. Also, lose some weight, fatty."
comment by ZachWeems · 2021-12-02T20:32:54.565Z · LW(p) · GW(p)
Retracting a comment on a previous post:
Previously said Helix had PCR tests that would "flag" this variant & predicted they'd give us handy graphs from this data. The company says they changed their PCR's a couple months ago, and the new ones won't flag the variant.
comment by jmh · 2021-12-02T19:32:45.362Z · LW(p) · GW(p)
An entirely lighthearted comment, perhaps in keeping with some humor in your recap of Biden's speech.
Omicron Everywhere
so it's actually omnicron?
On a more serious note, are there any good, and known, models related to mid-pandemic travel restriction value? Perhaps particularly for mutation cases given the time lag to identify the new mutations. If one is sure the mutation is not yet present (and that it has a very, very low probability of emerging in its own) then restricting travel will absolutely slow down the rate it will eventually arrive. But that seems like a dream case.
comment by demost · 2021-12-03T16:48:38.466Z · LW(p) · GW(p)
Researcher Alex Sigal has followed the mutations of the coronavirus in an HIV patient over months [1], and he believes that the pattern of mutation in the Omicron variant is similar to what they had observed in that patient. So he favors the HIV scenario for the development of Omicron.
And he speculates that, given this scenario, this would increase the chances of Omicron being milder than other variants, because, as he puts it, a virus that persists for months in an immunodeficient patient is probably not particularly deadly.
It doesn't quite match my own intuition, since the major damage of a corona infection seems to come from your own immune response, rather than directly from the virus. But my expertise is quite limited, so I trust Sigal's gut feeling on this question much more than my own. However, I think that "gut feeling" and "speculation" does describe the level of confidence.
[1] https://www.eurekalert.org/news-releases/609570 (edit: corrected link)
(All infos from German magazine SPIEGEL, which is unfortunately paywalled and in German.)
Replies from: ChristianKl↑ comment by ChristianKl · 2021-12-04T12:27:25.226Z · LW(p) · GW(p)
Researcher Alex Sigal has followed the mutations of the coronavirus in an HIV patient over months [1], and he believes that the pattern of mutation in the Omicron variant is similar to what they had observed in that patient. So he favors the HIV scenario for the development of Omicron.
One of the aspects of Omicron is that over half of the mutations are focused on the spike protein. It would be very interesting to know whether that pattern is also true for Sigal's patient or whether the mutations in that patient are more distributed.
comment by Julian Schrittwieser (julian-schrittwieser) · 2021-12-03T09:35:16.452Z · LW(p) · GW(p)
Does Omicron already having spread through community transmission in the Netherlands (and other European countries) before the reports from South Africa, yet still not being as widespread in Europe, suggest that it's not that transmissive after all?
comment by Yunxiang Zhu (yunxiang-zhu) · 2021-12-03T02:39:35.460Z · LW(p) · GW(p)
According to the data of SA, Omicron is either importantly immune erosive, or R0>=30. I hope it's immune erosive.