Covid 3/17/22: The Rise of BA.2
post by Zvi · 2022-03-17T16:20:00.906Z · LW · GW · 23 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Europe, South Korea and Hong Kong China Great News, Everyone Physical World Modeling BA.1 vs. BA.2 The Federal Funding Prevention and Prevention Prevention Prevention Think of the Children In Other News Prediction Markets Not Covid None 23 comments
Omicron has made its way through every major country except one – China. Its time seems to have come. As I noted on Monday, China had already locked down 60 million people amid rapidly rising case counts. Unlike previous rounds where China was able to fully take extreme measures only it could take but that held the promise of physically working, this round’s efforts seem like the exact kind of hope that is not a strategy. They’ll help to slow things down, sure, absolutely, but I can’t find a physical model where they are enough. Things will get out to the rest of China, and locking down over a billion people Chinese-style is simply not an option for any length of time. The resources are not there.
Meanwhile, Europe and the United States are dealing with the rise of BA.2, which is overtaking BA.1. My estimate is it is 25% more infectious than BA.1, which means its raw numbers should indeed be increasing for now, putting as at risk for an additional wave. I do not expect anything that needs to be disruptive, and I expect little appetite for renewed restrictions, but we have indeed done stupider things many times.
So it’s not the best time to notice that it looks like the administration really is out of money for Covid-related things. The standalone bill to provide the funding seems unlikely to pass the Senate. We might actually soon be in a situation where the federal government can spend no money on either vaccine research, other pandemic preparedness or even things like testing and treating the uninsured. Alas, the restrictions that do harm are not the interventions the government will find itself unable to fund.
Executive Summary
- BA.2 is taking over for BA.1, perhaps resulting in a small new wave.
- China is probably about to be forced out of its Zero Covid policy.
- A new highly promising therapeutic has been announced.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 170k cases (-25%) and 7,050 deaths (-22%).
Results: 190k cases (-16%) and 8,609 deaths (-6%).
Prediction for next week: 180k cases (-5%) and 6,300 deaths (-10%).
Note: Deaths excludes a -4,096 count in MA, and excludes 2,300 backlog deaths from SC.
After predicting too many cases for a few weeks running now I predicted too few. Part of that is the rise of BA.2, but the other half is adjustments from previous results causing me to doubt that our behaviors were adjusting as much as I expected to new conditions. It seems that has finally turned around. I expect both trends to continue, and we are probably near the local bottom.
The lack of a further decline in deaths is getting increasingly weird. The implied CFR keeps going up, no matter what pattern of time lag one uses. I do not understand it, but at some point one’s predictions have to fold even if there’s no explanation of why. The number of reported tests is declining but not enough to make us be missing that many more cases.
My new theory is that these are mainly ‘with Covid’ deaths rather than ‘from Covid’ deaths and the definition somehow includes anyone with recent Covid, so people who have actually fully recovered, who then died of something else, are being counted as Covid deaths. I haven’t heard that expressed elsewhere, but if that’s not true, then I got nothing. This number is too high and it does not make sense.
Deaths
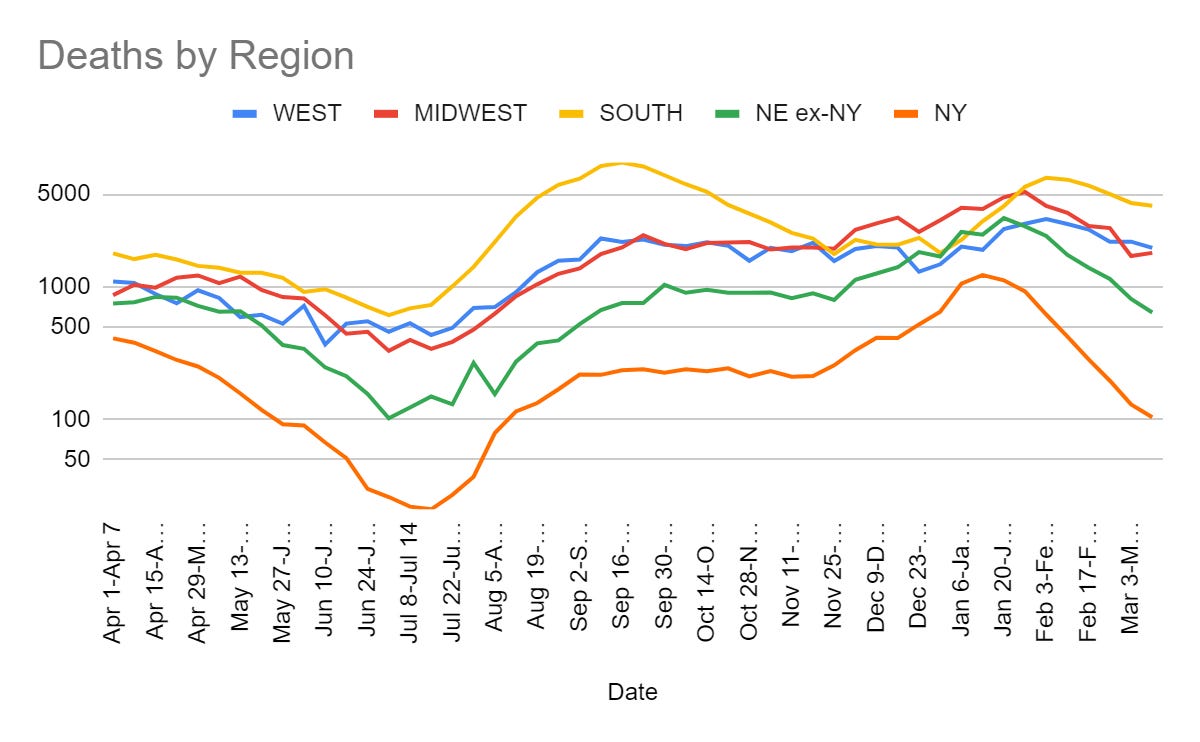
This isn’t going to make more sense if I keep looking at it more. Something in the way this data is being tabulated is super fishy.
Cases
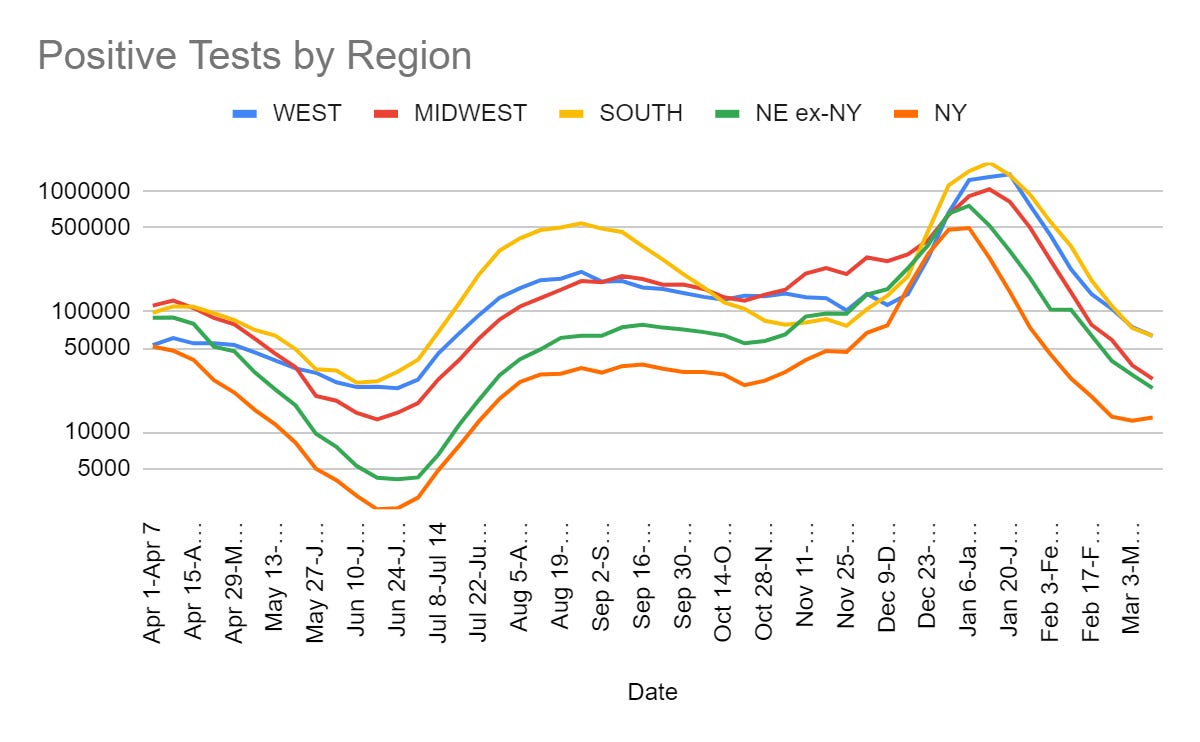
Things are still declining in most places, although they have begun creeping up here in New York, which makes sense given that we had our peak slightly earlier as well. Otherwise, the uniformity of timing is remarkable.
Europe, South Korea and Hong Kong
Cases in Europe are up, and a common line is that Europe is ‘ahead’ of us by a few weeks and represents America’s pandemic future.
Here is the situation now, with the USA on to show the contrast.
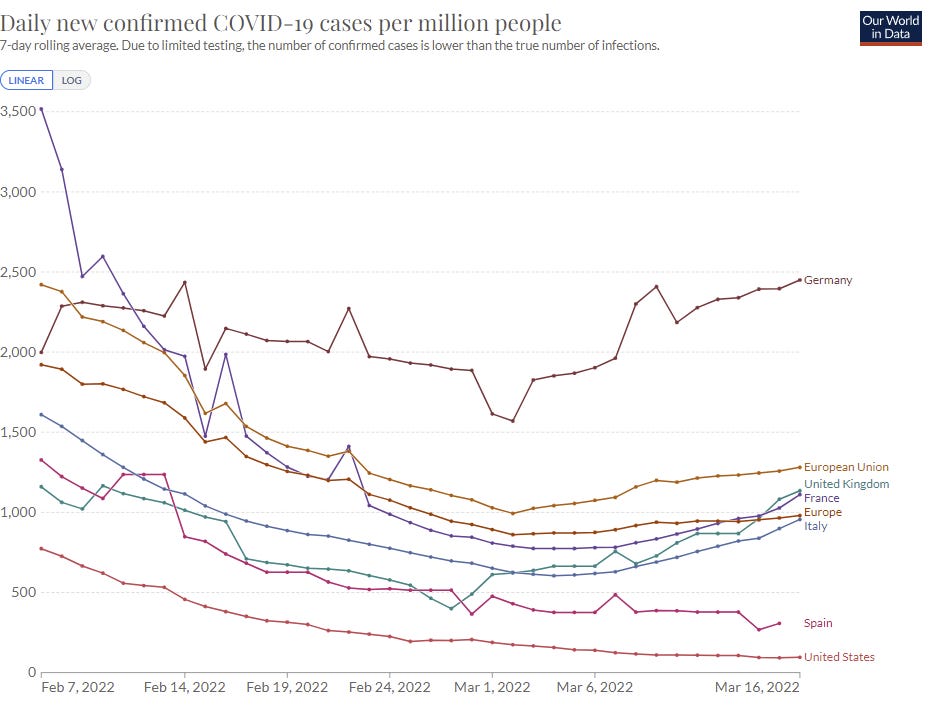
For context, zooming out and adding Denmark, Hong Kong and South Korea.
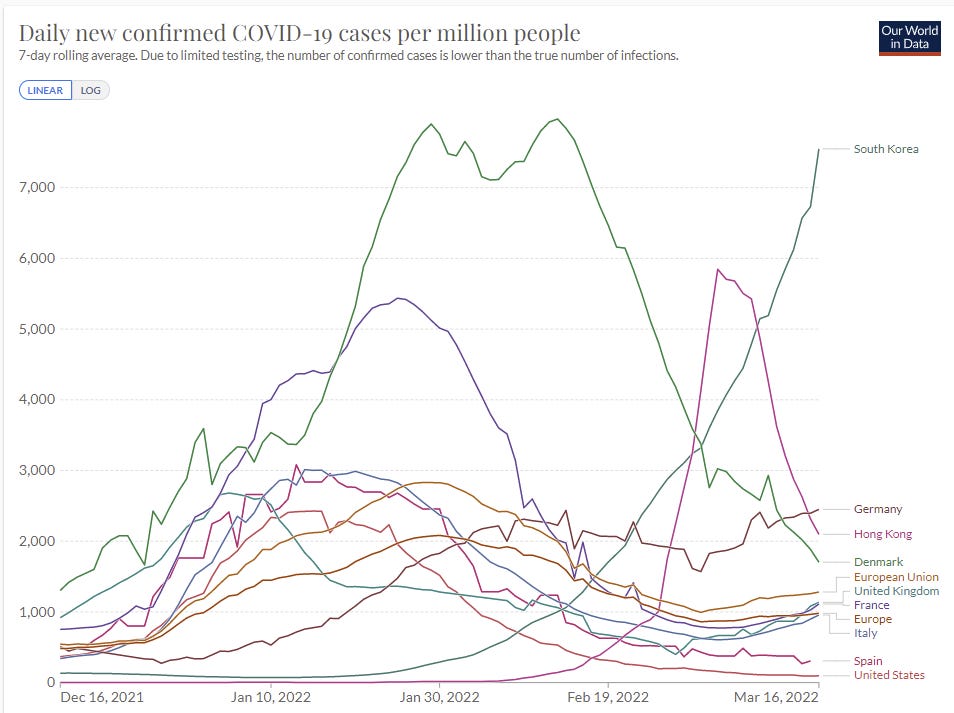
There is real concern here. Cases in many places are going up again, including the average for all of Europe or the European Union.
Notice that the United States peaked in a similar place to Europe overall, but is now dramatically lower – even at its trough Europe had 860 cases/million/day and America is currently under 100, much less than every major Western European nation.
For comparison, here’s deaths, especially to note that American deaths are relatively high even now, although that will change.
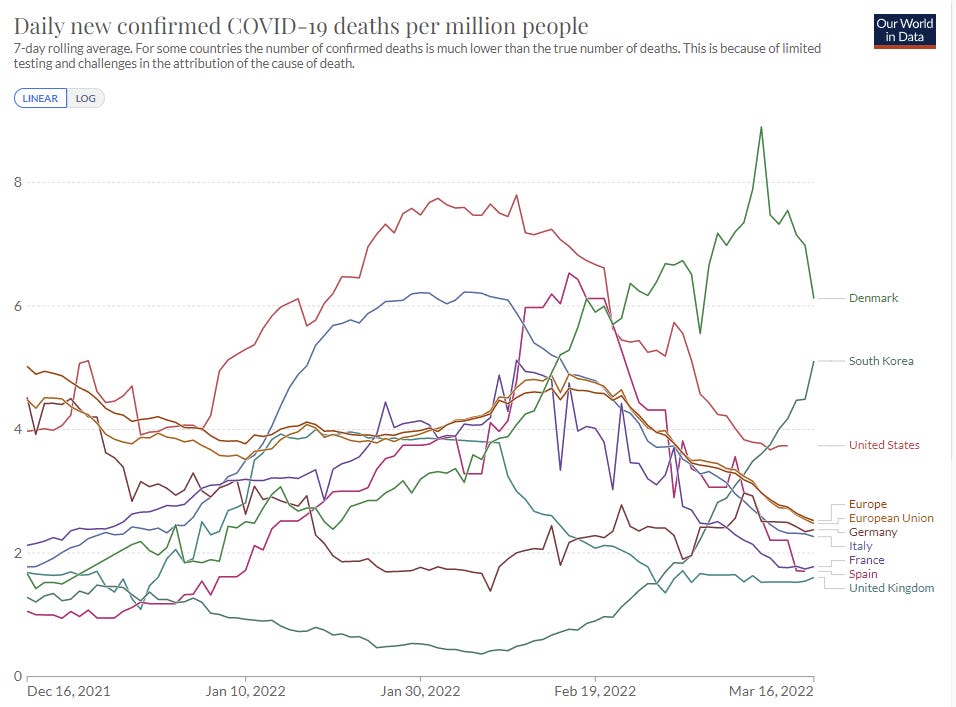
For whatever reason, current conditions in the United States are far more favorable in terms of spread than conditions in Europe. It seems highly plausible that BA.2 could be enough to make things in Europe importantly bad but not do so in the United States. Everyone talking about this will say the opposite, it seems, citing our vaccination rate, because Covid-19 is supposed to be a morality play, despite its stubborn refusal to adhere to the script.
See the sections below on BA.1 vs. BA.2 for more discussion but I believe BA.2 to be ~25% more infectious than BA.1. This is indeed enough to turn things back around and make cases rise again in Europe for a while, but the chances of things peaking substantially higher than the BA.1 wave seem quite low, and that wave was highly survivable.
Thus, in Europe this looks like mainly a political battle. There will doubtless be calls to return to doing marginally effective but highly annoying prevention efforts, including many (like vaccine requirements) that have no practical effect on the relevant timelines. It will be important to push back hard against this.
One additional note there is that I expect the war to help redirect people’s need to Do Something in a more useful direction. It is a lot easier to avoid needless panic about Covid-19 when events have given something that, no matter your perspective on it, is very much worth panicking about, and also a very practical, very real humanitarian refugee crisis. If you want to do something good, there’s something very good to do.
Things in South Korea are mind-bogglingly out of hand.
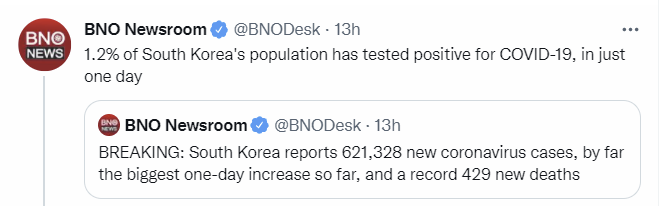
South Korea does test more than the West does, but still, my lord that is a lot. The good news is this cannot continue for long, since there are only 100% of the people around to get infected. A peak this high means a rapid peak and a rapid decline.
I have not seen any stories about rushing medical assistance in during their time of need, but this is likely in the short term an even more pressing humanitarian crisis than Ukraine, given the extra deaths that would result from medical system collapse.
Hong Kong is on the way back down in its official case counts and the descent is super rapid, but I have seen claims that this is an illusion caused by a phase change in testing procedures – I don’t know either way. I hope this is incorrect.
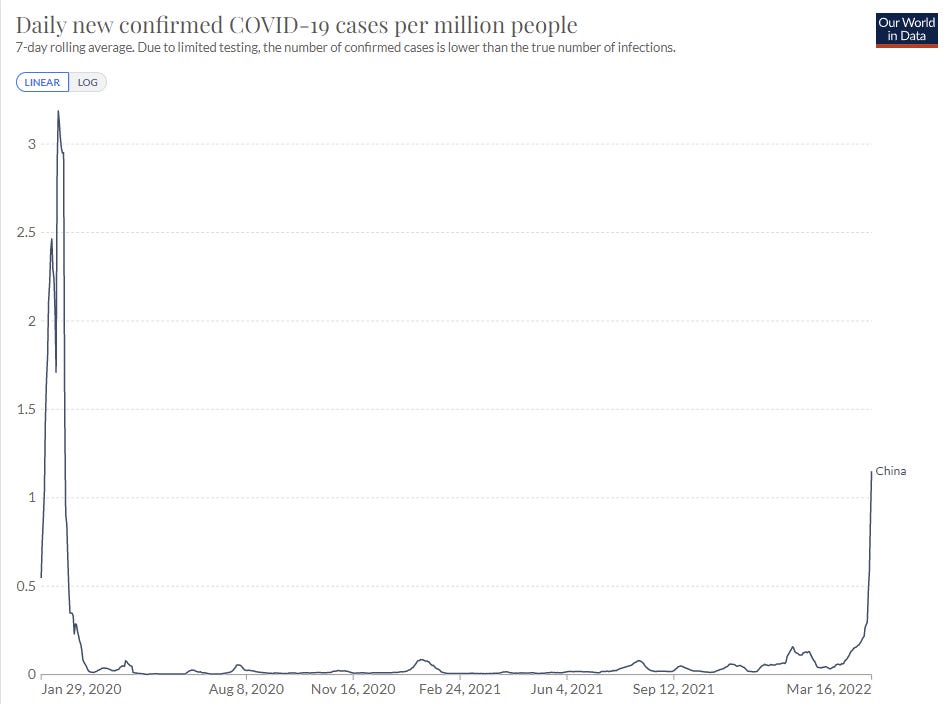
China
It seems increasingly clear that China has lost. The will to do what it would actually take to stop Omicron simply is not there.
That’s not to say that is a mistake. What it would take would have been dramatic, and how dramatic it would have to be rises each day that such actions are not taken, if it was even possible at all.
This is all mostly a reiteration of the situation from Monday, except that there is now that much less hope that things could be otherwise.
Here’s the Washington Post on the situation.
On Tuesday, the country’s economic czar Liu He cautioned that under the “complex situation,” pandemic measures must be balanced with economic and social development to “keep the economy operating within a reasonable range” and maintaining stable capital markets — a possible reference to how the draconian lockdown measures used previously could affect the economy.
You don’t get to do that. Balance means failure. There is no ‘keep the economy operating within a reasonable range’ other than winning, and then resuming the work. If the economics minister is talking like this, it seems like this is over.
The citizen complaints are also telling, I want to highlight this one in particular.
“Three years. I don’t dare get sick, and don’t even talk about having children. You don’t know what they might face,” one Internet user wrote under a hashtag for the issue that had been viewed more than 40 million times in two hours.
The madness of Covid, that it would drive one to not have children for fear of it. There are so many things like this that people let talk them into giving up having a family. Do not let this happen to you.
The ‘don’t dare get sick’ is also telling. Having a population in fear of what will happen to them if they are known to be sick is not a healthy long term situation.
As always, this could simply be an outlier anecdote, so take it in with caution.
The core problem is, as noted in the last Omicron post, they’re using half measures, and those measures cannot possibly work in the sense of keeping an outbreak fully contained.
Many more areas have implemented less stringent restrictions on movement between provinces. Flights going into Shanghai will be diverted to other cities from March 21 until May 1. All those entering Beijing must undergo a nucleic acid (PCR) test 72 hours after arrival, on top of having a negative coronavirus test within the past 48 hours.
In Tianjin, like in many cities, residents have been ordered not to leave for nonessential travel. In Shanghai, those who must leave the city, as well as those entering the city, must show a negative nucleic acid test taken in the past 48 hours.
This Reuters analysis echoes this seeking of ‘balance’ by Chinese officials. I agree that the next two weeks will be telling for their ability to contain, the difference is I have a strong expectation of what will be told.
I do still think it is possible that China achieves containment and retains its zero Covid policy in reality but the chances are in the single digits and fading fast.
So what happens now? What will it take for China to abandon the zero Covid policy when cases have already been observed in 28 of its 31 regions?
My presumption is it will take time. Logically speaking, we can see that the zero Covid policy is doomed to failure. In terms of saving face and who wants to tell Xi that the policy is done, it is not yet time. China’s levels of cases are still extraordinarily low, and perhaps things will all work out.
That is, of course, exactly the same kind of thinking of many in the West who tried such hopes and half-measures. It stands in contrast to China’s previous efforts, which were both very serious and surprisingly (to me at least) successful.
What I don’t know is how much time. What makes it sufficiently clear that China will pivot to doing its best to handle the inevitable? To implementing policies to flatten the curve and hopefully minimize how many people die, while keeping their economy from taking too much damage? That is indeed ‘balance’ but it needs to be balance that accepts that containment has failed.
Then the next question is, once China gives up zero Covid, what happens next?
The optimistic picture is that things work out like they did in Japan (or like Omicron in India). A rapid rise, but then a peak well before the situation turns critical and everyone is overwhelmed, somehow managing to turn things around while most remain uninfected. Taiwan is also a hopeful model here, and in some ways is the closest parallel.
Hong Kong and South Korea suggest the other path. A very steep climb up fueled by an immunologically naïve population, leading to a peak that no hospital system could handle, and a lot of deaths. I’ve seen reports that Hong Kong’s peak in positive tests comes from a change in testing procedures as things were overwhelmed, and we won’t know for sure until deaths start to decline again. Things look very bad.
China’s prevention policies under non-zero Covid will help determine which world they will live in, both official policies and private decisions. If they are in the bad worlds, then once things start to take off there will be urgent need to slow things down to give the medical system more time. China should hopefully be able to make unusually good use of time once they admit to the situation, being able to do things like construct hospitals within days.
The key is not to jump the gun. Once it is clear you cannot maintain zero Covid, unless you’re racing to secure medical supplies and other urgent matters and can get a big dividend from that,locking things down now, before the crisis arrives in earnest, is exactly the wrong thing to do. China, like everyone else, has a limited amount of capacity to impose restrictions on its people. Such moves are economically and socially costly, and require many resources that are in limited supply. This is very much a limited ammunition, ‘don’t fire until you see the whites of their eyes’ type of scenario. You’d want to wait until things were about to get rather desperate, then lock down hard to try and contain the peak while limiting the downsides, and hope to maintain that until the peak was over.
Starting that process now for over 50 million people is burning up those precious resources. If China extends that more in vain attempts at early containment, it had better fully work in ways I don’t expect to be possible at this point. Otherwise, things will only end up being worse. Potentially much worse.
If we get the optimistic scenario, China will be adapting to using Covid prevention procedures in widespread fashion indefinitely, but ordinary prevention procedures will combine with cultural factors favoring prevention and conforming to authority and with sensible deployment of resources to allow China to reach equilibrium without having to first infect a ton of people. There will be a modest hit to economic activity and supply chains, but not a widespread human tragedy and not too many serious lockdowns either. Factories that are important would use lots of testing and high quality masks, isolation and ventilation to stay operational.
I think this is the less likely way for things to go, but it’s definitely plausible, so I’d give it a maybe 25% chance once full containment fails.
If that’s not enough, there is little middle ground between that and a situation not as bad as (due to lower density) but centrally similar to South Korea or Hong Kong, which has the other 75%.
Also note that the peak won’t look as high as it does in Hong Kong or South Korea because China is very big and far less interconnected, so its peaks will be more local and diffused in time. Depending on ability to shift medical resources this could be a big advantage in minimizing human costs, with different cities and regions peaking at different times over several months.
This strangely suggests things like ‘let the virus rip inside Jinin now while quarantining the city from the outside and rushing in treatments’ if you fully know that’s the path things will take, but I presume this is simply impossible even if it was correct.
I wish China all the best and all the luck in getting through this. There may be a mid-week update if there is a substantial change in the situation.
Great News, Everyone
New therapeutic just dropped. From the people who brought you repurposed Fluvoxamine, this morning we give you… Peginterferon Lambda (original article).
The Phase 3 TOGETHER study of Lambda is the second largest study to date of a COVID-19 therapeutic. Final analyses evaluated data from 1,936 patients, with 84% of patients having received at least a single dose of any COVID-19 vaccine.
Final analyses using a Bayesian analytic framework showed:
- Lambda highly superior compared to placebo on the primary endpoint, with a probability of superiority of 99.91%, surpassing the prespecified superiority threshold of 97.6%
- 50% risk reduction was observed [95% Bayesian credible interval (95% BCI): 23–69%] of COVID-19-related hospitalizations or emergency room visits compared to placebo in patients treated ≤7 days of symptom onset
- 2.7% of patients (25 / 916) who received Lambda were hospitalized or had ER visits through Day 28, compared to 5.6% of patients (57 / 1020) who received placebo
- Risk reduction of COVID-19-related hospitalizations was observed:
- 42% (95% BCI: 5–66%) risk reduction when treated ≤7 days of symptom onset
- 60% (95% BCI: 18–82%) risk reduction when treated ≤3 days of symptom onset
- One COVID-19-related death in Lambda group; four in placebo group
- Incidence of any treatment emergent adverse events was similar between Lambda and placebo groups, which were primarily injection site reactions
- ABOUT PEGINTERFERON LAMBDA
Lambda is a late-stage, first-in-class, type III interferon (IFN) that stimulates immune responses that are critical for the development of host protection during viral infections and has been well-tolerated in clinical studies.Lambda is to be administered as a single subcutaneous injection so that it can be prescribed and administered at the first sign of infection or at first awareness of an exposure, potentially helping patients avoid severe illness that can lead to hospitalization and death.
The biological frameworks appear distinct, so chances are this will be cumulative with the effects of Paxlovid, and the treatment appears well-tolerated.
If this indeed cuts risk in half again, once we have sufficient supply it seems even more clear that we can shrug off additional waves.
That’s the catch. We have not yet heard anything about supply, so it might be quite a while before this has a major impact.
Physical World Modeling
New Omicron severity paper dropped (paper).
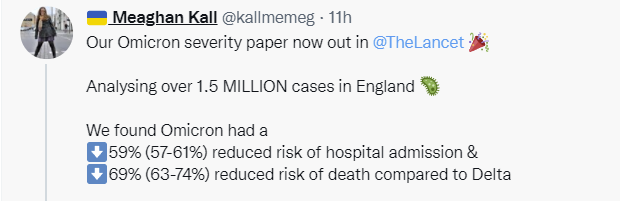

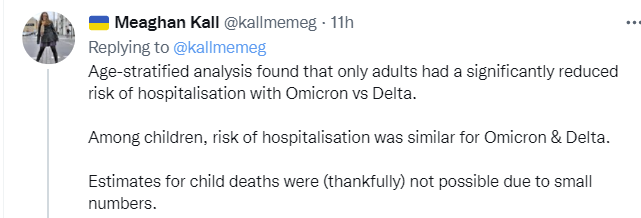
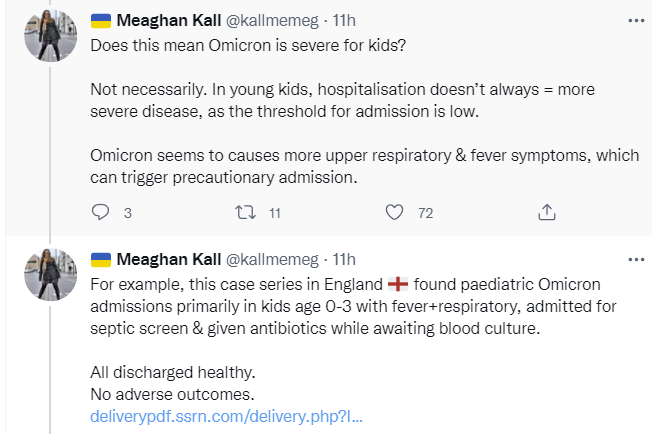
Lots of charts in the thread and in the paper, for the curious. All of this seems consistent with previous model. For kids, I’m ready to accept that relative risk to kids is higher because risk in adults is lower and risk in kids mostly didn’t change, meaning they’re somewhat less additionally protected in relative terms but still absurdly well protected.
Mask study purporting to show that masks stop Covid spread in schools is bad. Really, really bad. Shows the opposite of what it claims kind of bad. Criminal levels of bad. Seriously, this is super bad only not as good. They had a response rate of under 1%. They looked only at secondary infections, when primary infections very much told the opposite tale. They therefore looked only at contact tracing claims, which in many places automatically excluded anyone masked assuming they could not spread Covid. Seriously, wow, if not updating in the opposite direction you are making a mistake.
An argument that future variants will have unknown/random severity. I don’t fully agree, as severity does play a big role in our reaction, but mostly true as far as it goes assuming all such variants are naturally evolving. We did indeed ‘get lucky’ with Omicron, again assuming it was luck.
Thread about recombinants that might combine Delta and Omicron. Mostly seems like no need to be concerned with what we are seeing. If something happens here it would be soon since Delta seems to be going away.
Severity for Omicron continues to look very good (as in, smaller, less than, reduced) in mRNA-vaccinated, previously-exposed areas. This thread looks at Denmark. It’s full on ‘with Covid’ territory.




The thread points out correctly that this is largely due to there being a lot of testing in Denmark, so lots of mild cases are caught. But the physical implication is that if you get Covid, within the next 30 days your chance of death only rises 150%.
Long Covid remains a concern, but if we assume ‘short Covid’ deaths happen within 30 days, this direct effect only raises this-year mortality by 12%. I do not exactly want to say that is an ‘acceptable risk’ but it puts it in perspective.
In unprepared places, things can look considerably different. Thread on situation in South Korea, where they (along with Hong Kong) now have far more cases than the United States has ever had at one time on a per capita basis. As usual, the thread contains the claim that Omicron is ‘not mild’ and deadly, especially in an immunologically relatively naïve place like South Korea that did not previously have many cases.
As of Tuesday, South Korea had a 7-day average death count of 4.47 people per million. The 21-day-prior case rate was 2,161 cases per million, for an implied case fatality rate of 0.21%. South Korean tests more than we do, so we can expect the discount for missed cases to be smaller than ours, but still. As a comparison, the USA peaked in the recent wave on February 10 at 7.79 deaths per million, with a 21-day-lagged case count of 2,236 cases per million, for an implied CFR of 0.34%, or if we use the end of the rapid rise of USA cases on January 10, we get an implied CFR of 0.33%.
This is a lot of cases at once and that’s terrible, but in terms of risk of death from infections South Korea seems to be holding up fine under the circumstances.
Observations that masks are indeed a big deal in practice, and get in the way of human interactions quite a lot. Interesting throughout. Three themes:
- Lookism is a real problem and mostly unconscious.
- Non-verbal cues are super important.
- Small frictions are a big deal (aka beware trivial inconveniences [LW · GW]).
I can vouch for all three points being importantly true. Masks are a much bigger deal than many want to pretend they are when people have to have meaningful or rich interactions, in addition to the basic problem of it being hard to hear people and them being annoying and uncomfortable.
Masks were still very much the right move early in the pandemic, even with these higher costs, but this is yet another reminder that we’re being continuously gaslit about the costs involved.
Spanish study of mask mandates in schools finds them ineffective (paper). I do not put too much stock in this because the decision on where to impose a mandate was not random, but if there had been a very large effect this would likely have picked it up.
Zeynep Tufekci speculates on what would have happened if the whole world had reacted like South Korea and Taiwan, and China had been honest. What if the world had indeed, in Sam Bankman-Fried’s term from his excellent Conversation with Tyler, had its s*** together? Could Covid-19 have been suppressed? If not, what would happen?
For sufficiently strong but still possible counterfactuals, I think yes. This wasn’t that close to happening, but it also wasn’t that far from happening either. The moves to be able to beat something on this level of difficulty next time are not hard to find nor expensive to implement – multiple countries got it right. Once it got out of control anywhere, however, it was over even in such a scenario. We either all win very quickly, we have a much more rough counterfactual in terms of our abilities, or we all lose. That still would have bought us substantial time. We would have avoided March 2020, but after that if Covid isn’t fully suppressed I’m not sure what the alternative world gets to look like. The will simply wouldn’t have been there, and the best ‘adjacent but more adequate civilization’ play is to rush the vaccines.
Bob Wachter thread noting things are good now but things might not be good later.
A prediction of DOOM as European cases head back up.
Another prediction of DOOM, in this case with a map of NYC attached.
A call that BA.2 means another wave for NYC, and if it doesn’t another one will come along anyway, so in a lull now is the time to impose additional mandates and generally get ready for doomy doom doom doom. A lack of a problem means we must Do More.
Doom. Doom, like war, never changes.
There will always be More to Do, we will always be Vulnerable. If it does not come, we were still Vulnerable, and should have Done More. If it does come, even more so, no matter how little impact it has, or how much of that impact falls on those who made the choice to not Do More.
A claim that wastewater concentrations are surging in many places.
Ah yes, more of the calling for Doing More. No link back to the source but here’s the chart.
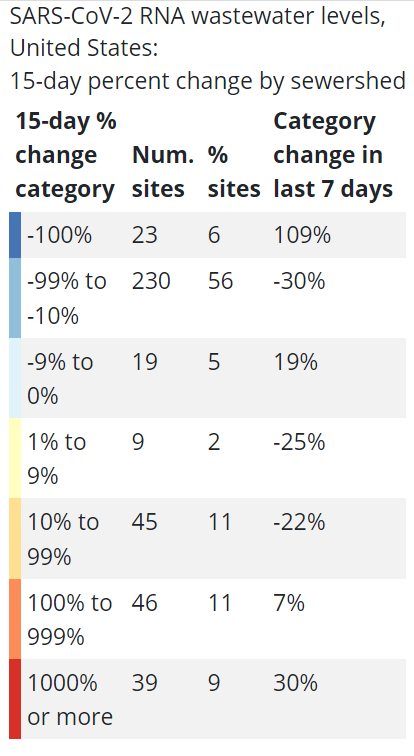
This is what one might call ‘ludicrously noisy.’ This is a problem for wastewater efforts when there are not a ton of cases. Nine percent of monitoring had a tenfold increase in those fifteen days with national cases crashing? Twenty percent doubled or more? I can’t take that seriously, any more than I take seriously that 6% of sites found actual nothing. And 67% of cites still had decreases. When you look at state data, you see uniform declines. Wastewater is great data but we can’t take it too seriously as individual data points. Instead we must aggregate.
So is that wave actually coming?
BA.1 vs. BA.2
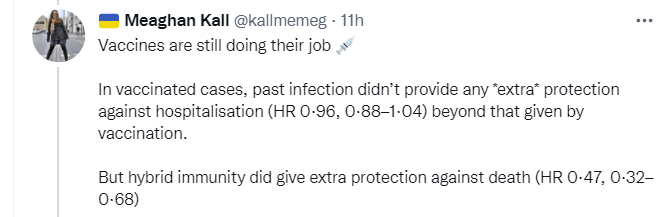
Thread on vaccine effectiveness and waning vs. both BA.1 and BA.2, based on a new study from Qatar. Bottom line is that vaccines sustainably are highly effective versus severe disease and death (90%+ for the booster) but protection against infection declines with time and was never that great. Which mostly matches previous understandings, although there are signs that vaccine might be slightly less effective against infection by BA.2 even though protection against death seems the same.
If anything, BA.2 might be slightly less severe than BA.1.
That’s not the concern, though. The concern is whether it will cause a wave of cases.
It seems clear that BA.2 is outcompeting BA.1.

The CDC estimate in question has been proven to be (let’s be polite) somewhat unreliable.
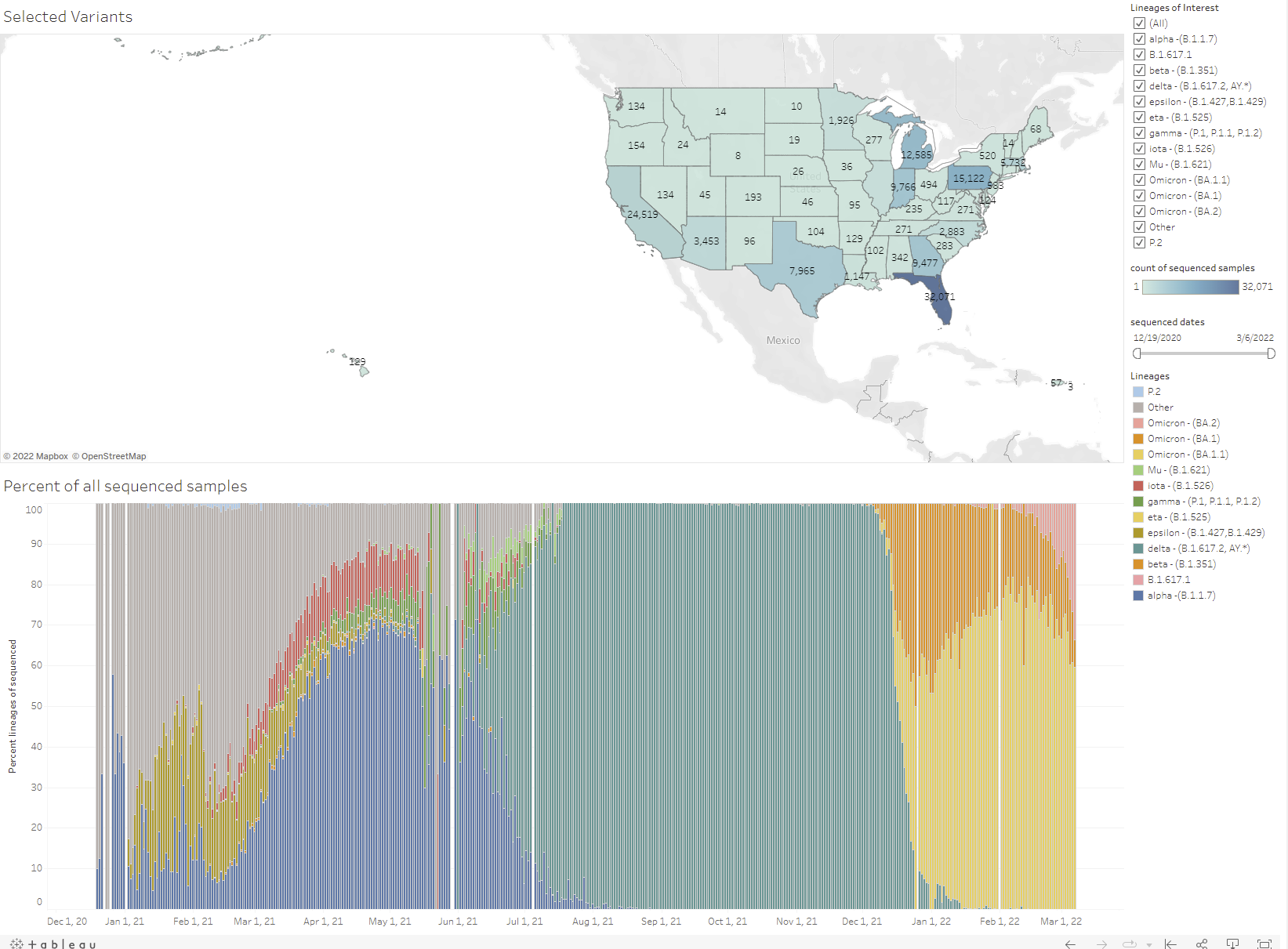
The pink is BA.2, and these are raw numbers, it’s easier to see at the site.
An interesting note is that the most BA.2 sequences are in Pennsylvania, Florida, Texas, Michigan and California. Obviously there’s some size bias there, but there seems to be zero correlation between BA.2 sequences found and amount of decline in cases in the past week. If BA.2 was going to be a huge issue, you’d have expected to see this.
The CDC projection is representing about a 15%-25% more infectious strain. The other option is noisier and harder to pin down, but suggesting higher if you look at the very recent events.
If you squint, you can see a BA.2 sample recorded on January 6, and there were a number of reports about it earlier than that. If we go backwards from 23% now with a 25% reproduction advantage every three days (which seems generous), then that would imply something like 0.2% of Omicron cases were B.2 on January 6. That I suppose is possible, and the rest of the graph looks vaguely consistent with that. So it’s likely something in that range.
Cases are declining by ~30%/week during the last few weeks, but that still means cases of BA.2 are rising.
The good news is, it doesn’t mean they’re rising all that much. I get R0 ~ 1.03 for BA.2, with cases down by 36% for BA.1, and up by 7% for BA.2 over the week, to average out to -30%.
That’s still a little scary, since it adds up over time and we could reasonably worry that prevention efforts will decrease or that weather or other cyclical conditions will worsen, and one way or another we’ve got another wave and the need to bring back a bunch of prevention.
The new variant typically has an early advantage, and the margins here are small, so it could easily go any number of ways. There’s still reason to think the resulting wave if it happens will not get that large, and also strong reason to think it will not be very lethal.
From all accounts, BA.2 and BA.1 give full cross-immunity, so the weird part of all this is why didn’t BA.2 dominate from the start? Or, if it didn’t do that, why was there enough of it early on for us to know about it from the start? For now I am assuming it started out well after BA.1 and thus there was very little of it, and we heard about it so early because it’s the kind of thing people like to talk about.
My bottom line here would be that BA.2 might cause something of a bump or even a wave, but it is unlikely to be sufficient to justify a general reversal of restrictions.
The Federal Funding
Both are rather terrible, but on different levels.
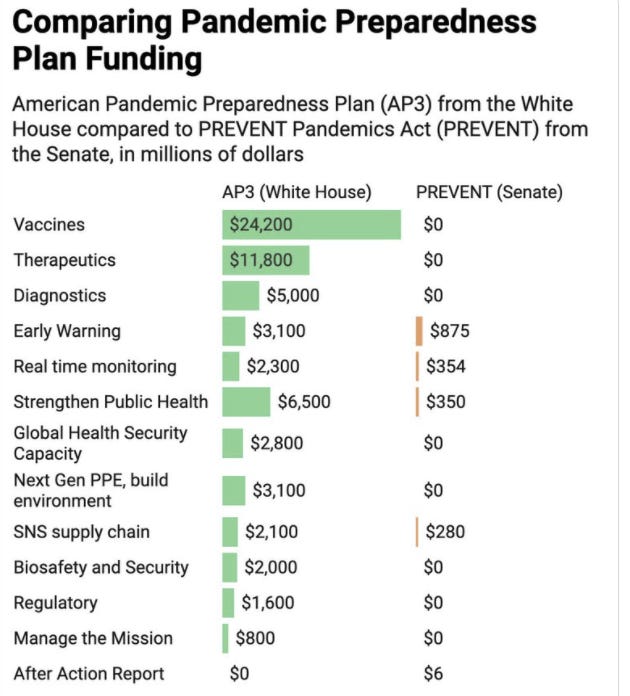
The future pandemic request was asking a lot of Congress, but still: White House asks for $65 billion for pandemic prevention, gets less than $2 billion, but at least gets funding for an ‘after action report’? Something is better than nothing, so thread reporting this still wants the PREVENT bill to pass.
In theory, one can always also increase funding in addition to the various actions in the bill.
In practice, this is another sign that congress has zero intention of allocating serious money to things that won’t have an impact before the next election and does not expect pandemic preparedness to backchain in the minds of many voters.
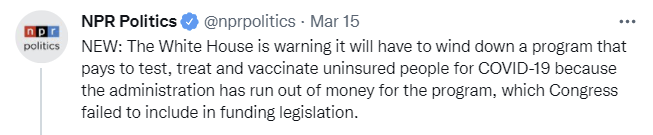
Then there’s the bigger practical problem that we have zero current pandemic funding.

I continue to presume that if there was another surge that this would be largely fixed, but in a world in which one side is determined to spend whatever is given to them then use that to ask for more, and the other side wants to limit spending, there is no easy way to get things to line up.
The UK also is dropping the ball on pandemic funding, although not on the same level.

There’s a lot of that going around including in areas that have nothing to do with Covid, this idea that once things are gone we cannot get them back. That what was once built cannot again be built, what was once assembled cannot be again assembled. There’s a fixed supply of a wide variety of Nice Things that is grandfathered in, but now any such things are not permitted. One of the central challenges we face is reversing this dynamic. I wish I had a better line on how.
Prevention and Prevention Prevention Prevention
Some hospitals continue to tell people to remove their N95s and replace them with inferior surgical masks, luckily when my wife gave birth we did not have this issue. If a hospital tells you to use an actively worse mask, would you trust them to treat you?
A suggestion that Biden should mask because he is old and therefore vulnerable (which is a good reason, it is important that he stay healthy especially now) and also ‘because we are likely to see a new surge in the next week or two’ which would indicate that masks work at preventing future infections.
Biden administration extends transportation mask mandate for another month before it was set to expire on March 18. It would have been better if it had expired, but the length of the extension being so short is encouraging. There’s a good chance this will be allowed to die in April if conditions continue to improve.
One unfortunate side effect of this requirement is to discourage use of trains and buses, which then get substituted with cars, which in turn increases our reliance on and drives up the price of oil and gas. Given the Democratic love (that I share) of public transportation, this seems like an excellent time to move to increase ridership and even push for additional (electrified!) buses and trains. Instead, we are implying they are unsafe and also making them unpleasant. Never waste a crisis.
As for masks on airplanes, that requirement remains deeply silly, but fully in line with many other silly safety theater related to airplanes.
It is good news is that the Senate voted 57-40 to override the transportation mandate. All Republicans except Romney voted in favor. Romney’s justification is that public health officials should make such decisions. Which is odd, since he’s met public health officials, but I guess I understand how he got there. Alas, it takes a two-thirds majority to override a presidential veto, and I can’t see Biden signing this.
Scotland re-imposes mask mandate due to rise in cases. We may see a lot more of this in Europe. I’m hopeful we won’t see it in that much of the United States unless we see a very large rise, and perhaps not even if then.
Thread on some attempts to ease the logistics of vaccination.
Think of the Children
CDC Data Tracker had some very serious issues in need of fixing. Which were then (at least partially) fixed this week, substantially reducing pediatric deaths. This was blamed on a ‘coding error.’ So let it be known – pediatric deaths are substantially lower than previously reported.
MIT lifts its mask mandate, flips to a mandate against masking requests.
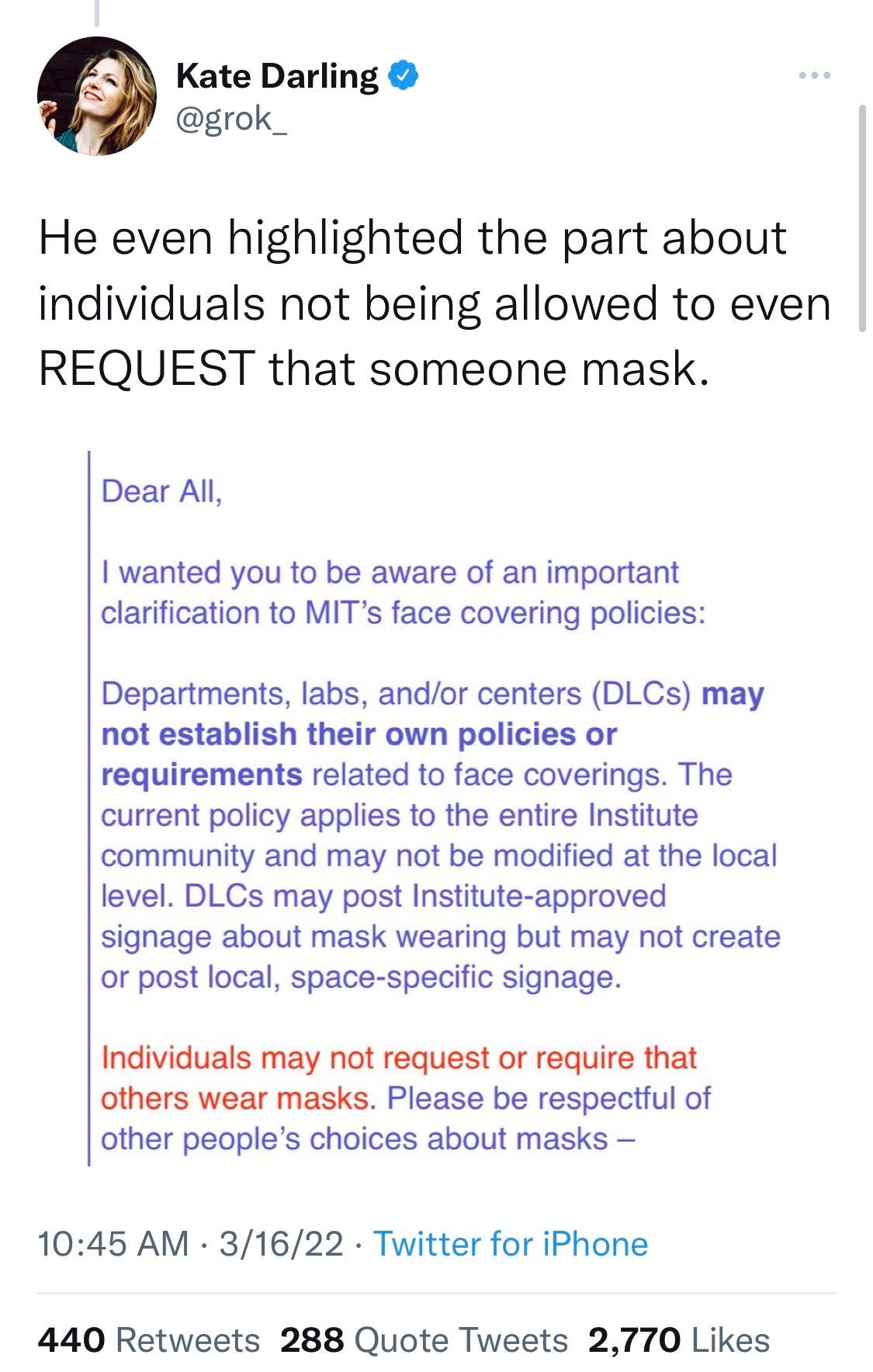
I can certainly see why one might do that – if you allow requests then refusing a request is going to be quite socially awkward at best.
Scary headline requiring explanation: A third of all USA child Covid deaths came during the Omicron wave. True as far as it goes. That was 550 deaths. Each death is a tragedy, but then the post goes on to claim that it is clear that ‘something different’ was happening.
“Omicron really did something different than Delta, and I don’t think it was just because more kids were infected,” Kane said. He saw younger patients with illnesses similar to croup and bronchiolitis, which can be dangerous in young children with “a pediatric airway the diameter of a pencil”, he said.
“It’s no longer fair even to insinuate that Covid doesn’t affect children, that Covid deaths are only in unhealthy children or kids with risk factors. That’s just not true, by the data.”
Was it?
Here’s cumulative American cases:
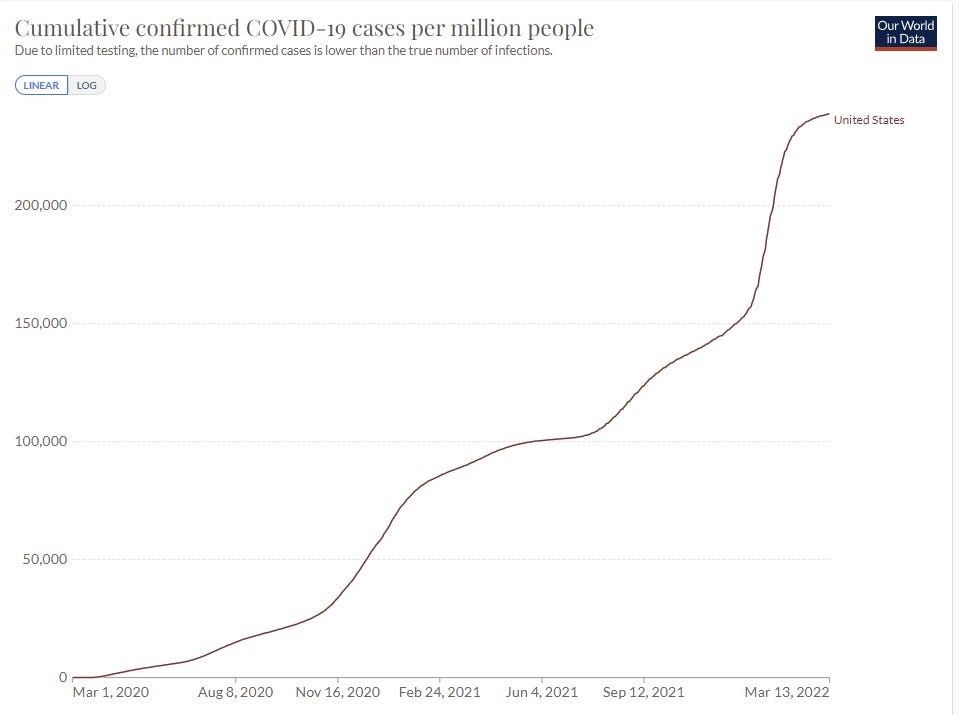
So that’s 150,000 cases per million before Omicron, and 100,000 cases of Omicron per million. Omicron was 40% of cases and caused 33% of child deaths.
That does not sound to me like things were suddenly worse, especially since a larger portion of Omicron cases were missed. Yes, kids were partially vaccinated, and this does show that Omicron was perhaps not as much relatively mild in children because of how much more mild it was in adults. But in children it’s still even more mostly harmless than previous variants, by the article’s own stats.
Varying school mask mandate lifting timelines in Canada’s provinces.

In Other News
More Dakka, taking something that is working and doing more of it, does not always work, and lockdowns were a prime example of that (short video). In order for More Dakka to be worthwhile, you need one of two things. Either you need all marginal additions to be worthwhile in and of themselves (e.g. gratitude is good and more gratitude on sane margins is better, so use more) or you need there to be a clear threshold where it would work and a mechanistic reason why and reason to expect to be able to hit that threshold. In the video’s example of trench warfare there simply was not threshold that would work. For Covid-19, there in theory was of course a threshold that would have worked if sustained sufficiently long but this was well outside the realm of serious possibility.
Note that the video this is part of was removed from YouTube for ‘violations of community guidelines’ before I could watch it, presumably for saying true things in violation of the Narrative. If anyone has a full link, please share. This guy seems great.
Dick Nixon of Twitter, an excellent account, gets stuck in UK without the funds to return home after getting Covid, forced to ask for help.
Situation in Hong Kong is quite grim, as elderly were mostly unvaccinated.
If you see one complete failure to shut up and multiply [? · GW], you should expect additional complete failures both of shutting up and also of multiplying. I would expect these two positions to correlate rather than anti-correlate, even controlling for other political stances, despite the contradiction Jeremy is pointing towards.
There may not be a cure for this (it’s a 45 second video of a very paranoid and deluded woman) but I have to say, pretty creative, very Scott Alexander, I like it.
Washington Post algorithms may need updating, they are still linking in their Coronavirus page to this article about what you need to know about Delta.
Prediction Markets
I was reminded recently that I haven’t checked prediction markets for a while in the context of Covid, so seems like a good time to do that for Polymarket – for Covid I am still skeptical that Metaculus and other sources are all that useful.
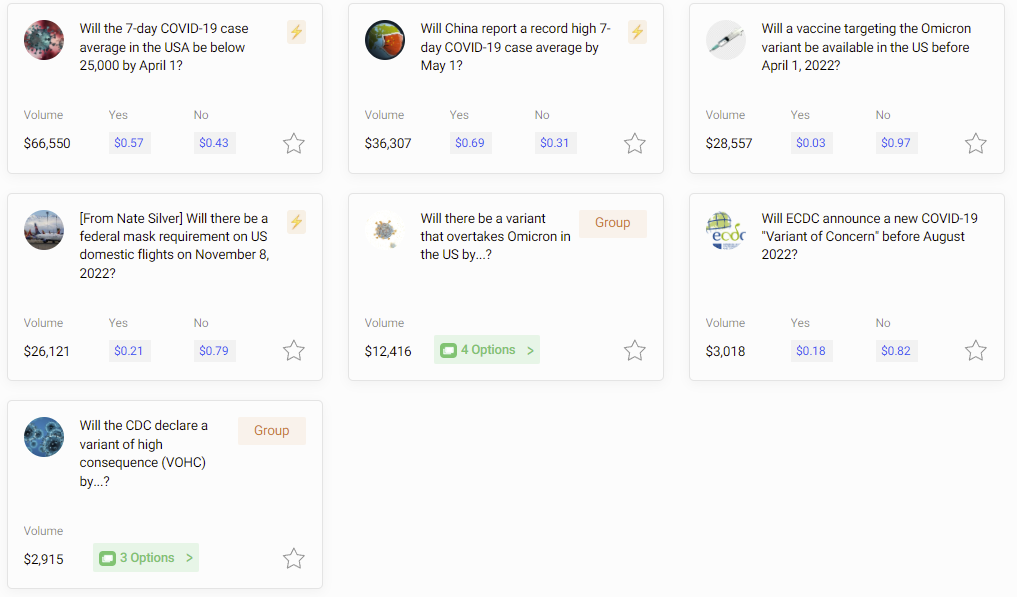
China hitting a record high was a buy before someone took the other side. It’s a screaming buy at 69%. There is not that much farther to go here.
Will we hit a 25k case average or lower by April 1? We are remarkably close to hitting it now, but BA.2 is likely to start creeping things back up. My default scenario has us barely missing this, so I think 57% is somewhat high and I’d have this more like 40%, but very sensitive to the next few days of measurements – even one surprisingly high day should probably crash this quite a bit.
The vaccine targeting Omicron by April 1 is trading at 3%. I consider this mostly an opportunity to collect interest at low risk. I suppose if your money is doing nothing else and is already in the right place collecting the interest is better than doing nothing.
Will there be a mask mandate in place on election day 2022? Currently this is at 21%, and the Senate has signaled strongly it wants this gone, but the vote would not have happened if there was any risk it would lead to a bill becoming law. This is up to a bunch of health experts and Biden, so I suspect that 21% is low here, although not enough to tie up money this long. I’d have this at more like 30%.
Will Omicron be overtaken? For some reason the April market is at 6%, that’s basically Free Money, a new variant that was detected now likely wouldn’t take over until after the deadline.
The Variant of High Consequence markets seem high, but not sufficiently obnoxiously high given time discounting.
Not Covid
Friends are great, so be friendly and make some friends.
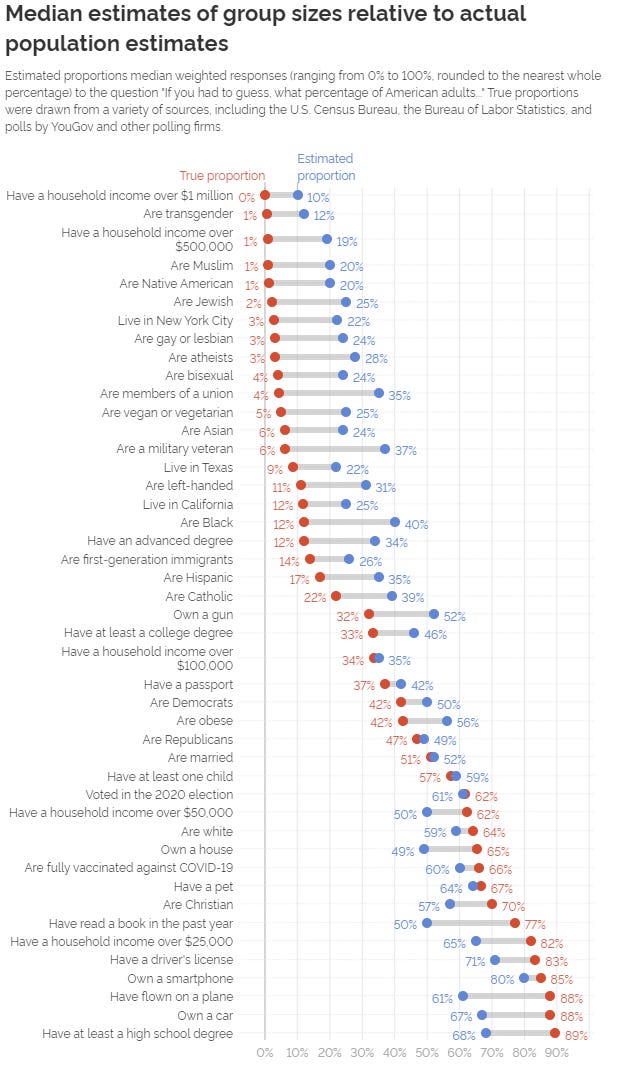
These predictions are remarkably well-ordered. There are only a small number of ‘surprising’ answers once you draw a basic regression line. Smartphone being at 80% makes sense as an outlier. The 40% guess for black population is strange but I’m guessing that’s because people are thinking about all minorities combined. Household income over $100k is interesting in that it is correct, would have expected a number in the 40s there, not sure the story, especially given the 50% for over $50k.
I am curious what would happen if you pointed out contradictions. For example, if people think 40% of Americans are black and 59% are white and 24% are Asian, and that’s 133%. Which is a lot.
What would be the sum of the guesses for all 50 states, I wonder.
Mostly though this seems like an excellent way to tell what people really think.
If some (ordinary person or an aggregate group) guesses that less than 30% of people have an attribute, it’s super rare. And if they think it’s more than 50%, they’re underestimating. So small differences near 50% are a big deal.
This also mirrors prediction market bias, although of course it’s bigger since the average prediction market user is more numerical.
Another possibility is simply that it doesn’t take many stupid guesses to get the answer very wrong when the right answer is 2%. Which is also an issue for prediction markets.
It’s also a reminder that those one talks to are weird. There are a lot of these where my bubble is off by a factor of ten or more.
Another note is that if it’s true that only 1% of Americans are transgender, 3% are gay and 4% are bisexual then that’s definitely not reflected in the broader culture and no adjustment of what numbers means is going to fix that. I’m actually highly suspicious that those numbers are that low.
And of course, there are some obvious errors on this chart. If you think only 3% of Americans are atheists I’m pretty sure you’re wrong. If you tell me 47% are Republicans, I know you’re wrong, Democrats outnumber them and there are a lot of independents as well.

Permanent Daylight Savings Time Ho?
It’s called the “Sunshine Protection Act” rather than the “Stop Making Us Fix All Our Clocks Twice A Year Act,” the “On Time Act” or the “Time Stops Flying Act,” which makes me sad, but it was sponsored by Rubio so that makes sense.
Then again, could be dumber.
Secretly and Suddenly Do The Right (or at least Better) Thing Unanimously Senate is indeed the best Senate. There is some threshold where things stop being played for politics and the necessary thing simply happens.
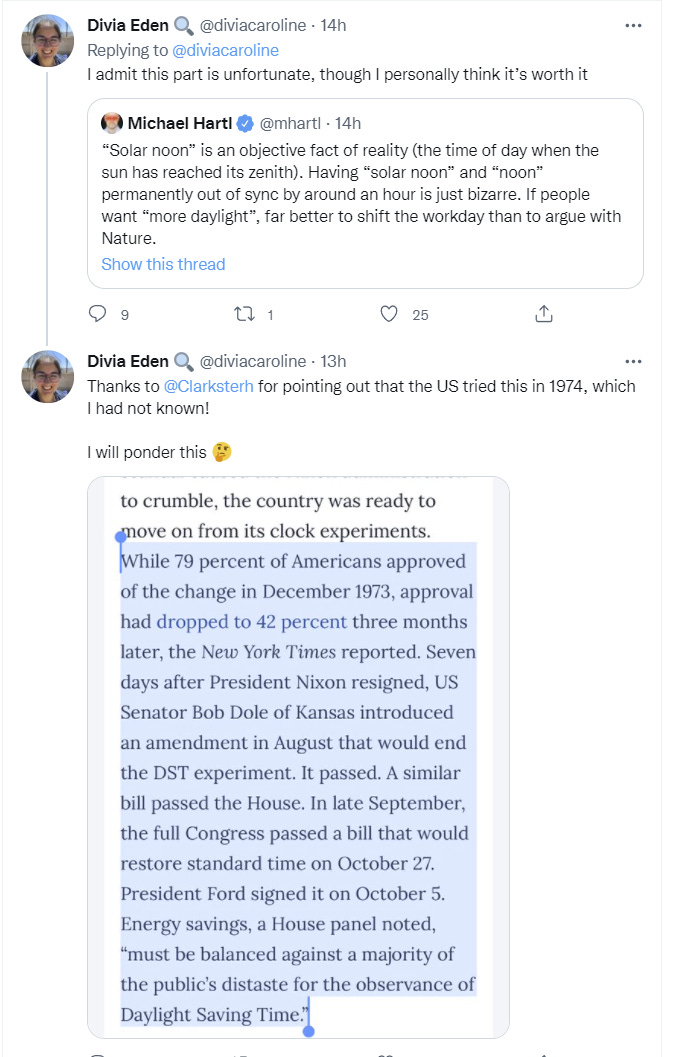
I do think that Standard Time was the correct answer, of course. It being dark at 8am for weeks on end is not good, we should have gone the other way. But switching between them is obviously worse.
In other words: The best time is an hour ago. The second best time is right now.
23 comments
Comments sorted by top scores.
comment by JenniferRM · 2022-03-17T19:41:15.523Z · LW(p) · GW(p)
Thank you for writing these Zvi. I read them, and I appreciate them.
You sort of "threw up your hands in confusion" at one point, and so I thought it might be worthwhile to respond with a note about how I've been purposefully trying to avoid having detailed models on the domain where the confusion might exist.
Specifically, I have long held off on worrying too much about the details of the medical biology of covid, out of humility or whatever.
Like: there are a zillion possible treatments, and different covid cases might evolve differently, and I'd tend to defer to an experienced clinician in their own clinic, if that clinic has good outcome numbers.
My model of local reactive skill and knowledge development predicts that two different clinics with two different genius clinicians in them could both learn to treat covid very effectively... and yet also in wildly different ways over the course of 6-18 months of a high volume of patients on which to "do their best, with variations, while observing carefully, and updating thoughtfully". So: universality properties are helpful for noticing good and bad reasoning, and universality expectations are sparse here.
Not only do I expect "valid local practical empirical knowledge" to have heterogeneity, but also it just seems like covid has heterogeneous effects on humans.
(Also, I think maybe early studies shows that if you sample different compartments of a covid infected human, you find different genomes, so there might be some within-patient evolutionary effects? I haven't heard much about this since like February of 2020 when only virology geeks and weirdo preppers were talking much about what I then tended to call "wuflu" in text messages, in private, to save on typing.)
Some people get anosmia, some don't? Wat!?
It seems sorta weird to me how variable things are, and the thing I'd hope for is like: mechanistic variety to explain outcome variety.
It would be useful, perhaps, to do a GWAS on covid outcomes, and with the large N that has accumulated this might be possible?
So DESPITE all these predictable epistemic barriers to knowing about "covid x human interactions"...
...I'm coming around to thinking that it would be useful to have a new clean mechanistic model of "how a typical fatal covid case progresses, day by day, with milestones, and typical inter-milestone amounts of time".
This seems to not yet be something that exists as part of common knowledge within the anglophone internet.
For example when I google [covid progression wikipedia] I have to click around to get to a not-very-good page about Symptoms of COVID-19 (which (right now) is more like a list of words than a mechanistic story about the handful of paths along which metaphorical "causal dominoes" can fall over in the way that dominoes could predictably fall over in general).
I'm not the first person to think "hey maybe detailed study of covid in the body of humans is useful to model" obviously.
Doctors have to think about this because this is their main job now. Hence... they've already DONE GWAS studies, and even started doing meta-analyses of covid GWAS studies.
All of this is to say that it might now, in 2022 (heading into 2023) be "too-wordcel-esque" at this point to fall back to mere "with/from" mortality distinctions?
My new theory is that these are mainly ‘with Covid’ deaths rather than ‘from Covid’ deaths and the definition somehow includes anyone with recent Covid, so people who have actually fully recovered, who then died of something else, are being counted as Covid deaths. I haven’t heard that expressed elsewhere, but if that’s not true, then I got nothing.
Like: at this point... I kind of expect to get covid several times over the rest of my life, and I think that I'll probably have lowered life expectancy even if just from from the boring normal scar tissue that forms in quite a few human bodies from from such infections, sometimes with the loss of an IQ point or 5, maybe some pulmonary fibrosis towards the end?
(A separate question I have genuine empirical uncertainty about: maybe some people have versions of covid that linger in reservoirs, as with herpes, HIV, and hepatitis that does damage over time? I don't know.)
If I get covid a couple times, and my body is damaged, and then my body gives up earlier than otherwise, and someone tries to placate me by saying "Jennifer, you're not dying from covid, you're just dying with or after covid" then I might uh.. spit at them? ...and call them idiots? ...and hope there's an afterlife so I can "go all Karen" on The Demiurge, and ask why it is has this macabre fetish for imposing body horror on embodied souls.
As a practical upshot, I would love it if there was some body-system by body-system explanation of the progression of the virus.
What do the autopsies look like?
Does covid work its way down throats into lungs slowly and creepingly, or does viral shedding from the upper respiratory area fall to the bottom of the lungs, eventually "take", and then climb back up and out, eating lung tissue as it goes? (Probably neither, but I don't know. Does anyone know? If so can you please edit wikipedia with the knowledge?)
In a world with a competently benevolent health system, I think every death would come with a little Pearlian Causal Graph that includes some body systems, some medical choices, and some larger humanistic context.
Here are some possible things that one could read off of a (hypothetical (utopian?)) single person's Official Causal Death Analysis in light of a larger graph theoretic causal reasoning framework (translated into english, with some trimming of the fuzzy leaf nodes):
(A) "ALICE was killed by lack of superfast medical care plus bleeding out, caused by lack of a real-time always-on heart monitor that can call EMH, plus a rare unskilled knife attack, whose wielding was caused by murderous intent, which was caused by discovery of marital infidelity",
(B) "BOB was killed by congestive heart failure, caused by catching flu and having complications, during 'normal' flu season (caused by lack of communicable disease filtering at various borders), while deep into 'early' senescence, possibly due to a rare allele of CUX1 (...AKA a way to 'die of old age' while relatively young)",
(C) and "CAROL was killed by traumatic brain damage, caused by a gun, caused by suicidal intent, maybe caused by bullying at a school, caused by teenagers in an authoritarian institution with low character, low morale, and inadequate leadership",
(D) and so on... (they are kind of fun to write, if you subtract out the sadness intrinsic to the writing exercise, with each one sort of like the premise of a tiny little murder mystery story).
In a framework like this, in 2022, covid would show up. If covid doesn't show up, you're doing it wrong. Not as the first step, and not as the last step, but "in the story".
Maybe, empirically, it would turn out that the data would show that people are mostly only causally "dying from covid" and never causally "dying with covid"... but I currently doubt that this is how the numbers would turn out, if such numbers were collected in a way that made it possible to tell these hypotheses apart, and then tabulated over large N, so that humans could simply know the answer.
I guess: it could be possible that someone on Earth already knows the answer to the practical empirical question here (even if they wouldn't necessarily mention causal graphs)? But I haven't found a good writeup yet that makes the knowledge easy to spread.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2022-03-18T10:13:42.669Z · LW(p) · GW(p)
Thanks for this thoughtful analysis. Concrete example: there have been house fires in which loss of smell from Covid was a contributing factor.
Also people who are "hard of smelling" often develop cardiac issues because they tend to over-salt their food. My aunt has struggled with this for several decades now after a chemical accident, and recently had a heart attack.
Replies from: JenniferRM↑ comment by JenniferRM · 2022-03-23T18:36:49.389Z · LW(p) · GW(p)
Fascinating. There's a whole literature on sense/nutrition interactions.
comment by ChristianKl · 2022-03-18T12:13:33.207Z · LW(p) · GW(p)
The future pandemic request was asking a lot of Congress, but still: White House asks for $65 billion for pandemic prevention, gets less than $2 billion, but at least gets funding for an ‘after action report’? Something is better than nothing, so thread reporting this still wants the PREVENT bill to pass.
As long as the White House believes "future pandemic prevention" means giving more money to people like Fauci who then distribute it among the virologists who started the current pandemic, not giving the White House the money it asks for might be very wise.
comment by Kenoubi · 2022-03-19T16:18:28.632Z · LW(p) · GW(p)
I can certainly see why one might do that – if you allow requests then refusing a request is going to be quite socially awkward at be evest.
Can't tell whether you're being sarcastic, but I actually think this is true. I feel like there might have been a time when these things weren't weaponised and even if it were okay to ask, no one would do it unless they were immunocompromised or something. But these days, as an employer who wants employees spending as little time and attention on masking (or lack thereof) as possible, the only maybe-stable equilibrium I can see between "masks required" and "masks forbidden" is "masks are a personal choice which you can make for yourself and yourself only". Like politics or religion, which now that I think of it masking is more or less a symbol of, nowadays (even though it does obviously also have other effects).
comment by trevor (TrevorWiesinger) · 2022-03-17T18:48:23.943Z · LW(p) · GW(p)
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2022-03-17T20:32:24.128Z · LW(p) · GW(p)
I'd counter with the theory that there's been a marked shift in why people are testing. If you're mostly testing for the purpose of controlling the spread (e.g. contact tracing) then the CFR will be lower than if you're focused on treating people who are acutely ill (with the goal of getting antivirals ASAP)
I do broadly agree with you that there are perverse incentives for people to avoid going on record as having Covid, especially with what we're finding out about possible long term cardiovascular issues (if you ever want to buy life insurance, don't get a PCR test). That could have the effect you're describing.
Replies from: TrevorWiesinger↑ comment by trevor (TrevorWiesinger) · 2022-03-20T04:28:02.696Z · LW(p) · GW(p)
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2022-03-20T13:21:33.967Z · LW(p) · GW(p)
Right. There's definitely some sort of bias in the testing.
One area in which I've run out of patience is the "Home tests are keeping case counts down" trope. In order for that to be true, you need to make a lot of assumptions about what those home-testers would be doing if there weren't any home tests available. Would they be running out to get PCR tests? Somehow I doubt it.
comment by Ruby · 2022-03-17T18:13:19.122Z · LW(p) · GW(p)
Quick mod note that we're no longer Frontpaging Zvi's Covid posts since Covid no longer appears to be a topic that most people need to follow for personal practical purposes. If you want to continue to see Zvi's posts, do either of:
- Ensure "personal blogposts" is not set to 'hidden' in your Frontpage Tag Filters (right above Latest Posts), or
- Subscribe to Zvi
↑ comment by JenniferRM · 2022-03-17T20:11:22.721Z · LW(p) · GW(p)
Could you link to the essay on "why covid doesn't matter any more for one's personal life and personal risk taking choices"?
I don't think covid stopped being important, I just think it just stopped being the #1 thing that people were officially freaking out about as part of The Zeitgeist (because Ukraine took its place as something even worse, like with nuclear fallout possibilities, and a more vivid Villain for a new style of Three Minute Hate).
Replies from: Benito↑ comment by Ben Pace (Benito) · 2022-03-17T23:53:11.329Z · LW(p) · GW(p)
For my money, the key times it was important to have covid info was:
- When we didn't know how it spread or how to compare different precautions
- When new variants were being a big deal (delta a little, omicron a lot)
At this point I think everyone is very well oriented to the first one. I think if a new variant came out we'd frontpage all posts sharing data and orienting to it.
Perhaps I'm missing some important other category because I've not been thinking about Covid recently, but I don't personally follow Zvi's Covid posts so much any more, and I have all personal practical considerations down pat.
(Actually, there's a post I might want to write about how awful antigen and NAAT testing, is after my experience running multiple 40+ people events and office spaces during Omicron and seeing how spotty and unreliable they were. This would mostly be useful for people if there's another variant.)
Replies from: JenniferRM↑ comment by JenniferRM · 2022-03-23T18:33:23.885Z · LW(p) · GW(p)
Thank you for the response. Maybe we have different definitions of "everyone" and maybe also different definitions of "new variant"?
(Perhaps the difference just loads on the indexical phrase "my money"? <3)
It seems like BA.2 is the new variant, but it hasn't been conveniently named yet because... maybe because the rein holders are trying to calm the horses right now?
(I've heard from my people who watch TV that in TV land people think the SCOTUS nomination is important, and this reminds me about how in Feb 2020 people in TV land thought that Trump's impeachment was important, even though it seemed to me like it was not at all where a sane person would keep their eyes [LW · GW].)
And in the last ~2 months I've had more "people I trade text with regularly" test positive than in the entire previous 2 years.
It seems like the smart people who test positive dither on whether to take Paxlovid or not. I think I would try to, in their situation, and even in my situation, but I haven't done a thorough review.
As several more people tested positive, wanting to know the actual truth about what might help them, I just now searched for [site:lesswrong.com zvi paxlovid]...
...and ended up back here, writing this comment in defense of "maybe covid isn't over and cogent thinking about it is still quite valuable?"
(The other big hit was Paxlovid Remains Illegal: 11/24 Update [LW · GW].)
Some Questions:
IF Paxlovid (or other anti-virals) are a net positive for <categories of people NOT chosen to get it by default for reasons related to triaging and/or politics, and rather than single-patient-centric net benefit calculations>...
...THEN it might be hard for such people to get personal-health-advancing behavioral compliance from a doctor who might grant them access to such anti-virals.
I think the antecedent is basically true, but I might be wrong.
Thus I think the consequent is also likely to be true... but again I might be wrong.
If I'm right, it means that techniques for making doctors behave like "actual good drug vendors who give the drugs they have a legal monopoly on giving" might be useful know.
Also, inventory of anti-virals can complicate matters, but I think it might regionally vary?
I guess another possibility is that everyone smart is just routing around the broken medical system, and getting real medicine from Mexico and/or Canada and/or the Internet?
Also, all this stuff tends to arise as the person is... well... "feeling sick" and might have "fewer spoons".
If there is a way to buy "the best actually helpful anti-viral" pre-emptively (in violation of evil US laws), then I'd personally and selfishly like to do this, I think? Then if I catch this new variant or the next, when I'm low on spoons and need some medicine in order to minimize my symptoms and scarring, I can just take it, without having to fight bureaucracies? Perhaps such honesty is not permitted in a top level post though?
The only sane public benefit I can see to not letting people buy anti-bacterials and anti-virals over the counter is to manage the evolution of the parasite ecosystem, but like: maybe people didn't notice that that cat is entirely out of the bag now? Like... the same logic says that you have to close the borders and gate entry based on communicable disease status, right?
So maybe the US should use diplomacy and violence to impose our anti-germicidal-drug-freedom policies globally? Or make anti-germicidals OTC? Or make the borders medically functional?
Basically: the laws here are either incoherent by accident, or incoherent on purpose because the legal system de facto hates humans and is de facto as happy for us to die as live, so long as rich people stay rich, and powerful people stay powerful, right? So good smart people should probably be writing up posts on how to break the law or else be in favor of rewriting the law, right?
On the bigger picture: China might be losing its de facto covid zero status, and so the global supply chain disruptions I feared greatly in Feb 2020 might now finally be "in the mail"?
(Or not? The CCP's "slicing and gridding" approach sounds remarkably similar to the only thing I can visualize as "actually working" to eradicate covid using reasonably small amounts of physical resources, but which I have tended to call "the green zone approach" in conversations with people, because I'm in favor of it, and "green zones" sound nice. So maybe China will keep its overall green zone status by "slicing and gridding" its little orange zones, and then making them turn locally green again? And maybe the Chinese Communist Party is telling the truth about how small and insignificant its orange zones are? But it seems like a parameter someone who cared about the world economy would focus on? Then again, maybe "caring about global prosperity is not about caring about global prosperity"</hanson>?)
I often missing things.
However, my current model is that people want it to be the case that "covid is over" and so that's how they are acting and talking.
In this model: precisely such aggregate opinions predict that we're going to have another wave... because the mass adoption of this opinion will cause a widespread decrease in all the little personal safety copes that people have been doing in their own life as a response to the general lack of a functioning public health system during this plague which will cause an increase in spread. This is consistent with so many people I personally know becoming covid positive lately.
However, I'm modeling people here as "making the kind of stupid mistake that humans make", not modeling people as "knowing something important that I don't know".
In my experience it is productive to try to find out what they someone else might have seen (as if they were smart and informed) if they are observed acting in ways that don't make sense to me.
Maybe "most people" are not engaged in some kind of motivated cognition about covid this February and March?
Maybe there are facts that are commonly known that I'm ignorant about?
If so,"for my money" I'd love to hear about these facts because I think it will help me plan in useful ways :-)
Not just for investing... also I think it is nice to help people by knowing and saying what is true, so they can also plan in useful ways, and in this regard I find myself mostly interested in understanding anti-virals, and when and how people should get them during the current(?) "covid is over" covid wave.
Replies from: Benito↑ comment by Ben Pace (Benito) · 2022-03-24T19:52:41.723Z · LW(p) · GW(p)
FWIW since writing your comment I found out about the UK Covid Case spike, and had the call with my mother where I recommended she move back to wearing her P3 in crowded spaces, like we did during Omicron. So I think I was a bit out of the loop about the new variant thing.
Regarding drugs, my model has been that if you're experiencing severe symptoms you want to take paxlovid and fluvoxamine and also a steroid like inhaled budesonide if you're having respiratory symptoms. (I took budesonide when I thought I had Covid during the omicron spike, and had the other two on-hand.)
I am in a spate of avoiding news on current events, and I just (internally) reminded the LW team that I'm not really tracking this stuff right now, so I am not fully connected to current decisions.
So good smart people should probably be writing up posts on how to break the law
I encourage pseudonymous accounts to write things they think will help others, and this idea sounds pretty good to me :)
Replies from: JenniferRM↑ comment by JenniferRM · 2022-03-25T03:52:10.484Z · LW(p) · GW(p)
Valid. I hope your mom is safe <3
It sounds like you're set with good medicine, at hand. just in case. Well played!
(Thinking about the side audience... Not that I actually know those 3 drugs are the best stack (with low side effects etc). Yet if you're informedly confident, Ben, then I take it as useful indirect evidence of things for me to research maybe, and I appreciate the info.)
Replies from: Benito↑ comment by Ben Pace (Benito) · 2022-03-25T04:34:01.376Z · LW(p) · GW(p)
Thx :)
↑ comment by Zvi · 2022-03-17T23:38:51.658Z · LW(p) · GW(p)
Noting that I think this decision is reasonable - people who want these updates have several ways to find them (they can also subscribe to the Substack at thezvi.substack.com, or use thezvi.wordpress.com in addition to subscribing here).
While I agree with JenniferRM there is still much to explore and figure out that matters, that doesn't mean most people need to follow things week-to-week - the things she's talking about are work for a select minority that reports back.
↑ comment by MondSemmel · 2022-03-18T11:41:11.088Z · LW(p) · GW(p)
It seems a bit unwise to post this comment after not frontpaging this post, as people won't be able to follow your advice if they don't see it in the first place :p.
comment by nim · 2022-03-18T04:59:09.615Z · LW(p) · GW(p)
Regarding death count not making sense: I remember way back before testing was available, people were guessing at the covid death rate from numbers that included excess all-cause mortality. Is that a statistic which could be available and useful here, or have the past couple years been so unpredictable that we have inadequate recent+normal data to compare against?
comment by localdeity · 2022-03-18T00:08:18.402Z · LW(p) · GW(p)
If the federal government loses the will to find the cash to buy Paxlovid, at what point does it make sense for a private charity to step in? (Will Pfizer sell to such an organization?)
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2022-03-18T10:10:48.334Z · LW(p) · GW(p)
I'm assuming insurance companies will pay for it. The government will still be paying indirectly to the extent that insurance premiums are pre-tax.
I'm also predicting that Paxlovid will probably end up being used for way more viruses than just Covid. If that happens, it could obviate the need for testing.
comment by Nanda Ale · 2022-03-17T21:12:18.988Z · LW(p) · GW(p)
Are there any arguments against opting into a fourth booster, for folks like myself who only had mild shoulder soreness as a side effect? I have some risk factors but would consider not myself high risk. (My parents on the other hand, very much high risk.) I see 'immune fatigue' brought up. As far as I can tell this is more of a theoretical thing that could happen with too many repeated boosters, but there's no reason to think it's a plausible risk at 4.
I don't mind if the benefits are quite small, as long as they aren't negative.
Replies from: Zvi