Surgery Works Well Without The FDA
post by Maxwell Tabarrok (maxwell-tabarrok) · 2024-01-26T13:31:29.968Z · LW · GW · 28 commentsThis is a link post for https://maximumprogress.substack.com/p/surgery-works-well-without-the-fda
Contents
28 comments
Here is a conversation from the comments of my last post on the FDA with fellow progress blogger Alex Telford that follows a pattern common to many of my conversations about the FDA:
Alex: Most drugs that go into clinical trials (90%) are less effective or safe than existing options. If you release everything onto the market you'll get many times more drugs that are net toxic (biologically or financially) than the good drugs you'd get faster. You will almost surely do net harm.
Max: Companies don't want to release products that are worse than their competitors.
Companies test lots of cars or computers or ovens which are less effective or safe than existing options but they only release the ones that are competitive. This isn't because most consumers could tell whether their car was less efficient or that their computer is less secure, and it's not because making a less efficient car or less secure computer is against the law.
Pharmaceutical companies won't go and release hundreds of dud or dangerous drugs just because they can. That would ruin their brand and shut down their business. They have to sell products that people want.
Alex: Consumer products like ovens and cars aren't comparable to drugs. The former are engineered products that can be tested according to defined performance and safety standards before they are sold to the public. The characteristics of drugs are more discovered than engineered. You can't determine their performance characteristics in a lab, they can only be determined through human testing (currently).
Alex claims that without the FDA, pharmaceutical companies would release lots of bunk drugs. I respond that we don’t see this behavior in other markets. Car companies or computer manufacturers could release cheaply made, low quality products for high prices and consumers might have a tough time noticing the difference for a while. But they don’t do this, they always try to release high quality products at competitive prices.
Alex responds, fairly, that car or computer markets aren’t comparable to drug markets. Pharmaceuticals have stickier information problems. They are difficult for consumers to evaluate and, as Alex points out, usually require human testing.
This is usually where the conversation ends. I think that consumer product markets are informative for what free-market pharmaceuticals would look like, Alex (and lots of other reasonable people) don’t and it is difficult to convince each other otherwise.
But there’s a much better non-FDA counterfactual for pharmaceutical markets than consumer tech: surgery.
The FDA does not have jurisdiction over surgical practice and there is no other similar legal requirement for safety or efficacy testing of new surgical procedures. The FDA does regulate medical devices like the da Vinci surgical robot but once they are approved surgeons can use them in new ways without consulting the FDA or any other government authority.
In addition to this lack of regulation, surgery is beset with even thornier information problems than pharmaceuticals. Evaluating the quality of surgery as a customer is difficult. You’re literally unconscious as they provide the service and retrospective observation of quality is usually not possible for a layman. Assessing quality is difficult even for a regulator, however. So much of surgery hinges on the skill of a particular surgeon and varies within surgeons day to day or before and after lunch.
Running an RCT on a surgical technique is therefore difficult. Standardizing treatment as much as in pharmaceutical trials is basically impossible. It also isn’t clear what a surgical placebo should be. Do just put them under anesthetic for a few hours? Or do you cut people open and stitch them up without doing anything else? So surgical RCTs are rare and small when they happen.
Despite extreme information problems and a complete absence of federal oversight, surgery seems to work well. Compared to similar patients on the waiting list, 2.3 million life years were saved by organ transplants over 25 years. The WHO claims that “surgical interventions account for 13% of the world’s total disability-adjusted life years.” Coronary artery surgery extends lifespan by several years for $2300 a year. Cataract surgery and LASIK can massively improve quality of life for a few thousand dollars.
Surgery is also improving over time. Pancreaticoduodenectomy, the surgical treatment for pancreatic cancer, began in the late 19th century as a near death sentence, although to be fair so was pancreatic cancer. For several decades surgeons were unsure whether it was even possible to survive anything except partial versions of the procedure. They experimented on dogs, cadavers, and consenting terminal patients and improved the procedure. Today, the procedure is safe and a standard treatment for pancreatic cancer. From 2006-2012 the mortality rate halved from 2.9% to 1.5%.
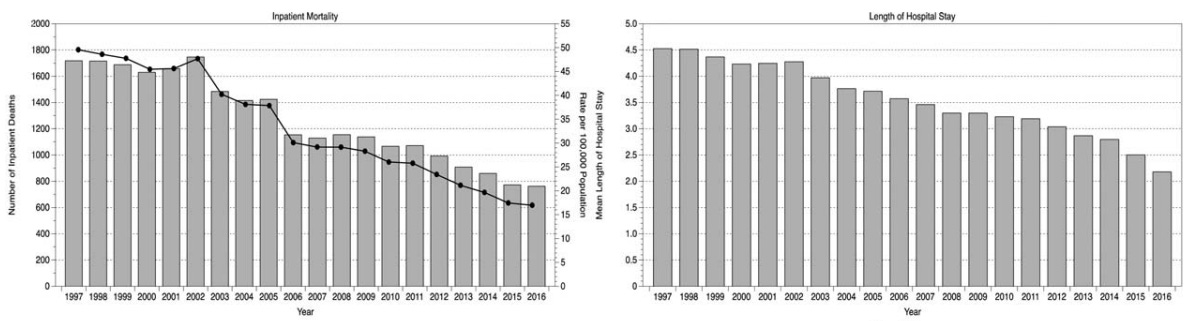
On a larger scale, among all emergency general surgery episodes in Scotland from 1997 to 2016, inpatient mortality mortality rates declined by more than three times and hospital stay lengths were cut in half, probably due to the rise of minimally invasive and robotic surgery tools.
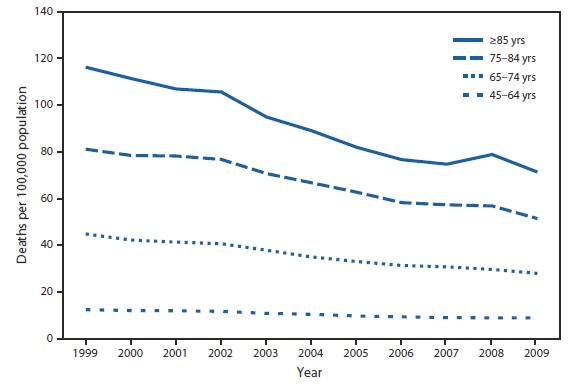
In the US, the death rate from medical and surgical care complications declined by 39% from 1999 to 2009.
Operative mortality for eight different cancer and cardiovascular operations from 1999 through 2008 declined with the lowest decline being 8% and the highest at 36%.

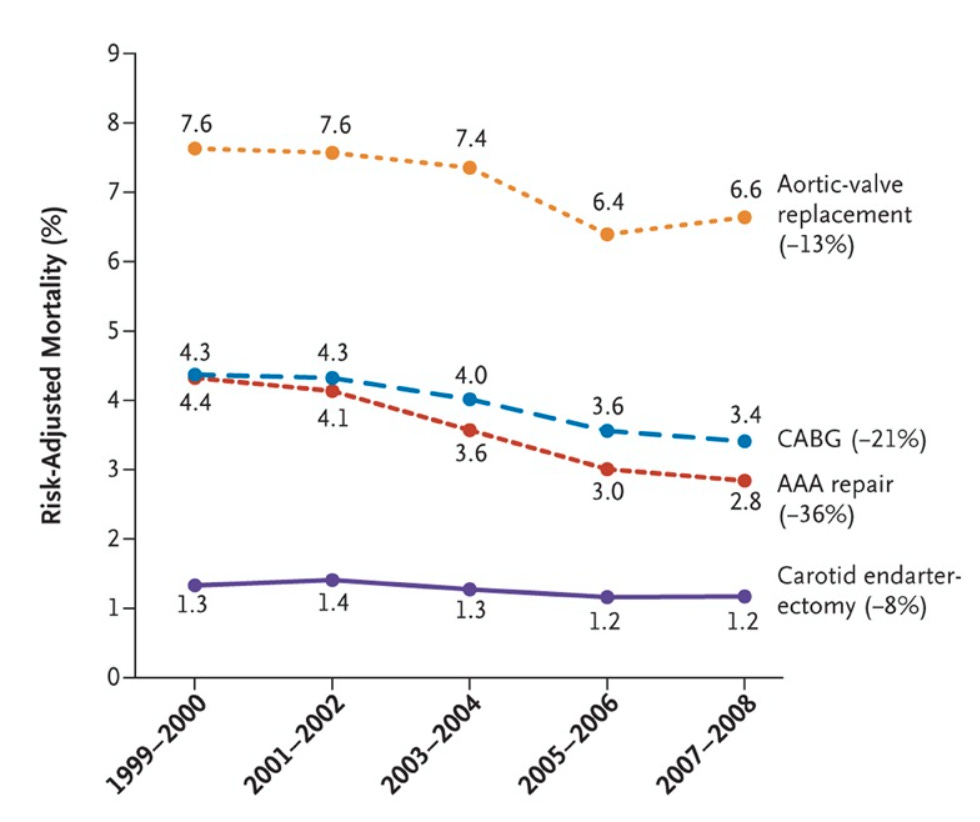
These are common surgeries with hundreds of thousands of operations each year.
There are problems with surgery. There are unnecessary deaths and ineffective procedures. There are bad actors and high prices. But surgery is not the vision of snake oil and certain death that is painted by many FDA defenders when you ask them to imagine a world without the FDA. The problems faced by surgery are matched and sometimes exceeded by problems faced by pharmaceuticals.
There are also non-governmental mechanism which constrain surgeons and protect consumers. Competition, insurance companies, hospital lawyers and ethics boards. But this strengthens the point. An FDA model is not the only way to promote consumer protection and solve the information problems presented by medicine and surgery.
So we don’t need to argue about the validity of consumer tech or cars as a non-FDA counterfactual for pharmaceuticals. Surgery has at least all of the market challenges that harry pharmaceuticals and it doesn’t have an FDA. Yet, it still muddles through. This is what we should expect pharmaceuticals to look like if we abolished the FDA. We would have a well-functioning, self-improving market for medical treatments without billion-dollar fifteen-year waits for any new drug that people want to try.
28 comments
Comments sorted by top scores.
comment by ChristianKl · 2024-01-26T21:31:27.180Z · LW(p) · GW(p)
The problems faced by surgery are matched and sometimes exceeded by problems faced by pharmaceuticals.
How do you know that?
I think it's likely that surgeries produce more undetected long-term negative side effects than most pharmaceutical interventions. Surgeries leave scars while most pharmaceutical interventions don't have an equivalent.
In the US, there's a lot more "cancer detection" and then surgical intervention than in other countries and this doesn't seem to reduce death rates by cancers. That suggests that a good chunk of those operations are essentially snake oil that doesn't prevent death but does lead to amputations.
That effect was strong enough that under the Obama administration, there was a move to reduce cancer screening because the results were just so depressing.
Spinal fusion for chronic low back pain seems to be a pretty bad surgical interventions that an FDA-like equivalent might outlaw (or severely restrict) because it often doesn't work and produces additional problems.
What do you think you would observe in a world where a good portion of surgical interventions are useless and harmful that you don't observe in our world?
comment by CronoDAS · 2024-01-26T18:44:47.685Z · LW(p) · GW(p)
Pharmaceutical companies won't go and release hundreds of dud or dangerous drugs just because they can.
At least some of them would, because there are, in fact, companies that do this in the real world. They simply use a different brand name and call them "dietary supplements" rather than drugs.
Replies from: kamil-pabis↑ comment by Kamil Pabis (kamil-pabis) · 2024-01-29T10:40:50.749Z · LW(p) · GW(p)
The supplement industry and similarly the cosmetics industry is a jarring example of what can happen with no oversight or the wrong kind of oversight. Although, to be charitable to the libertarian position, one can argue that many supplement and cosmetics companies are forced to provide inferior products since efficacious products, even when rather safe, cannot be sold on the free market for various reasons (e.g. higher doses of potassium or retinoids for photoaging).
comment by Davidmanheim · 2024-01-28T07:50:01.140Z · LW(p) · GW(p)
One problem with this analysis is that the FDA actually regulates a ton of what happens in surgeries, which sharply reduces how much this example actually proves. Specifically, they approve all of the devices that get used during surgery, from the scalpels to the monitoring equipment to the surgical sponges, all the laparoscopic instruments used in modern surgeries, and all the replacement joints and implanted or assistive devices which are being put in in many surgeries. Yes, this is different than regulating the surgery itself, but it manages to cut off a huge range of surgical interventions that could be more dangerous or less reliable, while it raises costs and slows innovation. So I'm less sure how well surgery serves as an example of working well without the FDA.
comment by Roven Skyfal · 2024-01-26T14:54:35.701Z · LW(p) · GW(p)
A really simple example of what industry doesn't care about outcomes and pumps out product despite lack of evidence of effect and even potentially adds harm is the supplement industry. They dont care about brand reputation because they just change their name or bring another product to market eventually. If you take the FDA away you will have every major pharmaceutical just releasing garbage medications that barely improve life, yet increase cost and add side effects. They already try to do this with non-inferiority studies rather than coordinating studies that show improvement. Not to mention many currently available medications barely (and statistically suspect at times) show efficacy yet rake in serious money. This argument clearly is coming from someone outside of the medical industry with a limited understanding of mechanisms at work. It seems to be coming from someone on the early side of the Dunning-Kruger Curve.
Regarding surgery there are immediate outcomes and they are treating a specific problem so it is easy to measure. These are absent or limited with medications. If a surgeon is consistently not taking the gallbladder out from patients but telling them they did, this will be discovered quickly and typically the surgeons will either be sued into not practicing or be removed from the surgeon pool. The same goes for a surgeon who isnt safely putting an aortic valve in. First off, they typically dont get to the point of being able to operate on people if they are terrible. If they do, patients die. Then the surgeon is removed from pool of operating surgeons. Thats not the same for a medication that reduces the risk of heart attack by 50% from 1% to 0.5% over a 5 year period. Have you ever seen marketing from industry? Its terrible and not aligned with the truth. It is aligned with selling a product and if thats all they need to give to a doctor then you are going to get offered medications you dont want to take.
There are also methods of self-regulation by surgery departments, residency training programs, medical boards, state licensing agencies and professional associations. So, to say that surgery is not regulated is just misinformed at best. Your argument is just really empty. I understand what you wish to be the case, its just not realistic. Its the same argument that there is no need to regulate companies from dumping pollutants into the Hudson because they will avoid it due to reputation. Thats just not how real life works.
Replies from: CronoDAS, Davidmanheim, jmh, ChristianKl, Wbrom42@gmail.com↑ comment by Davidmanheim · 2024-01-28T07:52:33.350Z · LW(p) · GW(p)
"Regarding surgery there are immediate outcomes and they are treating a specific problem so it is easy to measure"
There are longer term impacts of surgeries, though, that aren't easily measured, and surgeries tend to score far more poorly on those fronts. Fixing a (sometimes minor) problem in ways that make people need more healthcare later is at best a mixed bag.
↑ comment by jmh · 2024-01-27T14:25:35.040Z · LW(p) · GW(p)
I had not heard of the Dunning-Kruger Curve, though had heard about human tendency to over estimate our own intelligence. It's really good to have the wiki graph image in mind (being something of a jack of many trades but master of nothing -- clearly something to take a personal interest in ;-)
At the same time, it's not like the AMA or FDA or even the complex of industry controls are getting things right all the time, or even consistently weeding out the bad actors. Rather than a status quo is working or we need to change because something is not working, a better approach might be to frame the discussions in something of a Type I and Type II error context. Then we can focus on which error space represents the greatest costs/risk or greatest benefit for various settings. I'm not certain your were actually claiming the status quo is what we should want, I think more likely offering a balance to the OP's claims.
↑ comment by ChristianKl · 2024-01-27T12:26:42.753Z · LW(p) · GW(p)
If a surgeon is consistently not taking the gallbladder out from patients but telling them they did, this will be discovered quickly and typically the surgeons will either be sued into not practicing or be removed from the surgeon pool.
A surgeon saying they take out a gallbladder but don't is more equivalent to some Indian generic company like Ranbaxy saying they produce a drug that has certain active bioavailable ingredients and then they don't then it's about a ingredient having different effects.
Taking out a gallbladder might be an intervention that's positive for health or negative. Whether surgeries sold by surgeons are provide a net positive health effect is a distinct question from whether they do the surgery according to the book.
↑ comment by Wbrom (Wbrom42@gmail.com) · 2024-01-27T14:13:19.752Z · LW(p) · GW(p)
Everything you said about the myriad of ways the field of surgery regulates itself actually works to support the point you are trying to argue against.
comment by ChristianKl · 2024-01-27T00:12:33.456Z · LW(p) · GW(p)
Companies test lots of cars or computers or ovens which are less effective or safe than existing options but they only release the ones that are competitive.
You can buy nonworking fuses on Amazon if you simply buy those with good reviews and market mechanisms don't seem to prevent that.
Replies from: None, nathan-helm-burger, Wbrom42@gmail.com↑ comment by [deleted] · 2024-01-27T00:18:53.363Z · LW(p) · GW(p)
Does Siemens or GE or any company with assets and a reputation longer than 5 years sell such a fuse? That would be an example of a market mechanism that doesn't stop Amazon from selling it, but would help prevent savvy buyers from purchasing it.
An example of this working well, and better than the FDA, is the UL listing system. A UL listing is not required. So it's not blocking innovation if the UL is slow to evaluate a product, or if a company is too small and is selling some unlisted products they just developed. An improved FDA would be unable to actually block a drug from being used, but would "share information" on what it knows, if anything, on a particular drug. An improved system for building codes would not block construction of a structure that passes engineering approval, but would allow nearby residents affected to sue for the loss of their sight lines, etc, that they object to, after the fact.
The NRC would not be able to block the construction of a nuclear plant if it can't find any valid reason to deny a permit after some short period of time - same idea. Non blocking.
It's the blocking property for regulations that is destructive. This is also why "AI pauses" are so destructive, they have this same extreme negative property.
Another similar issue is governments don't have to pay the costs for their own wrong acts. For example, if a government chooses to block construction of an apartment building due to a missing environmental review, and later a judge determines that an environmental review was not required, the government shouldn't enjoy "sovereign immunity" and should have to compensate the developer for all of the costs of this action. Probably they should have to pay it in escrow before blocking anything...
Same with FDA, same with all the other examples.
Replies from: jmh, CronoDAS↑ comment by jmh · 2024-01-27T15:19:26.483Z · LW(p) · GW(p)
I think you're making claims of facts that are based on counter-factuals. While I have some sympathy to the general idea that we're in an over regulated time. I do like the idea of government and its agencies being more about reducing information and organizational costs to allow private individuals and groups to pool their resources to solve their own problems over it being the active principle in all such efforts.
I also agree that incentive structures here matter. Perhaps that type or rule requiring a set aside to escrow would make regulators more diligent in their evaluations -- but could also just produce greater delays and be a bad unintended consequence. But clearly a place to spend mental efforts.
I also agree that the margins probably do need to shift some towards private (e.g., UL) rather then public mechanisms. However, I am also reminded of the critique Hal Varian made regarding the private solutions to supposed market failures documented in Tyler Cowan's The Theory of Market Failure: they all seemed to include some government actions. The implication of your comment seems to be that we can get rid of all these agencies. I'm not sure on that point, I suspect some role remains even if we change the names for optics.
Regarding sovereign immunity, not all acts are protected and some areas the government and its agents only enjoy qualified immunity. So in your example I'm not certain that some compensation would not be supported by law. But the other twisty bit there is the government is not separate from you or me. Yes, the share we have to pay is small but in the end it is all of us who are paying. I suspect some in the local community or tax payers who see some of their money redirected to off-set the builder's cost might question that as an unjust taking. Some might think the developer failed to perform sufficient due diligence before incurring all those costs. Just a counter hypothetical for consideration on this particular point. Largely just trying to point out that your approach is not clearly a parato improving move -- or at least you're not clearly identifying the side payments that would be made to accomplish that outcome.
Replies from: None↑ comment by [deleted] · 2024-01-27T16:44:58.991Z · LW(p) · GW(p)
I think the broader scope claim is that rapid progress requires mistakes. That all of China's hastily built excess structures that have some quality issues that will cause problems for some of them, or the belching clouds of coal smoke, or all the people in the USA who were poisoned by leaded gasoline, may to some extent be a necessary sacrifice.
The eras when the most actual forward progress were made seem to have the most incidents like this. Today we have Teslas occasionally driving themselves out of control, or having component failures that legacy auto long since repaired. Or how AI models have all their faults.
It's just a vibes thing, I don't know an explicit way to prove this, but it certainly is suggestive, that the regulatory ratchet prevents negatives and also prevents the positives. And the positives can be enormous. For example if the NRC had less regulation, and a few hundred people had been exposed to radioactive releases and died, it might have prevented ~920,000 deaths over the last 40 years. https://www.hsph.harvard.edu/news/press-releases/particulate-pollution-from-coal-associated-with-double-the-risk-of-mortality-than-pm2-5-from-other-sources
I would suspect that excessively strict and arbitrary building codes/zoning are similar, that they kill more people from homelessness than are saved by a laxer system.
So that's the tradeoff. Obviously you need government, but government agencies need to be somehow responsive to the total effect of it's actions, not just it's narrow domain. The NRC has to consider the coal pollution each requirement will cause, etc. Autonomous car regulators need to consider all the crashes a flawed autonomous car software stack will prevent, not just the few it will still cause.
Sovereign immunity happens to remove one of the feedback mechanisms.
↑ comment by CronoDAS · 2024-01-30T04:41:57.549Z · LW(p) · GW(p)
Does Siemens or GE or any company with assets and a reputation longer than 5 years sell such a fuse? That would be an example of a market mechanism that doesn't stop Amazon from selling it, but would help prevent savvy buyers from purchasing it.
What happened on Amazon is that items advertised as being sold by Amazon itself wouid turn out to be Chinese counterfeits. You could order a thingamajig made by Siemens and get something with the name "Siemens" on it that wasn't actually made by Siemens.
This is what I've heard that Amazon did, and I don't know whether or not they still do:
Amazon has a "Fulfilled by Amazon" service that third party sellers can use, in which they ship products to Amazon, and when someone orders the product from that seller, Amazon will then ship them the product. However, the Amazon warehouse doesn't keep track of which seller sent in which item: if there are multiple sellers that use Fulfilled by Amazon to sell a Siemens Thingamajig, they all get marked with the same ID number and put in the same bin. If Amazon itself also sells Siemens Thingamajigs directly, its own stock gets put in the bin with the ones from third party sellers. So, if a third party seller opts to use "Fulfilled by Amazon" and ships Amazon a counterfeit Siemens Thingamajig, someone ordering a Siemens Thingamajig from Amazon directly could end up with the counterfeit that the third party seller had put up for sale.
↑ comment by Nathan Helm-Burger (nathan-helm-burger) · 2024-01-28T17:24:56.090Z · LW(p) · GW(p)
I think this example of untrustworthy brands with fake reviews shows why we don't want a completely unregulated system for safety relevant products. I do agree that the FDA is being overly cautious. I don't think that that means that no FDA at all would be better. Fortunately, I do not find it difficult to imagine a redesigned FDA which works in a much more reasonable fashion, giving us the best of both worlds. It doesn't have to be all or nothing!
↑ comment by Wbrom (Wbrom42@gmail.com) · 2024-01-27T14:14:58.147Z · LW(p) · GW(p)
Or you can buy UL listed ones that work. The UL is a private organization. Which again goes to prove his point.
Replies from: CronoDAScomment by Ponder Stibbons · 2024-01-27T08:53:58.467Z · LW(p) · GW(p)
Two things that happen in the pharmaceutical industry today despite the FDA.
- Many drug candidates (compounds with IND status sanctioned by the FDA ) are pushed into clinical investigation prematurely by venture capital funded biotech, that more established and careful pharma companies would stay away from. These have a high rate of failure in the clinic. This is not fraud, by the way, it is usually a combination of hubris, inexperience, and a response to the necessity of rapid returns.
- Marketing wins over clinical efficacy, unless the difference is large. Tagamet was the first drug for stomach ulcers released in the late ‘70s.It was rapidly overtaken by Zantac, in the ’80s, through aggressive marketing, despite minimal clinical benefit. Today there is a large industry of medical writers sponsored by the pharmaceutical industry, whose job it is to present and summarise the clinical findings on a new drug in the most favourable way possible without straying into actual falsehood.
The scientists working at the sharp end of drug discovery, who fervently believe that what they do benefits mankind (this is, I believe, a gratifyingly large proportion of them) generally respect the job the FDA do. This is despite the hoops they force us to go through. Without the FDA keeping us honest, the medicines market would be swimming with highly marketed but inadequately tested products with dubious medicinal value. Investors would be less choosy about following respected well thought-out science, when placing their money. True innovation would actually be stifled because true innovation in drug discovery only shows its value once you’ve done the hard (and expensive) yards to prove medical benefit over existing treatments. Honest and well enforced regulation forces us to do the hard yards and take no short cuts.
In 2023 55 new drugs were approved by the FDA, hardly a sign that innovation is slacking. Without regulation the figure might be ten times higher but clinicians would be left swimming in a morass of claims and counter claims without good guidance (currently generally provided by the FDA) of what treatments should be applied in which situation.
Replies from: nathan-helm-burger, Wbrom42@gmail.com↑ comment by Nathan Helm-Burger (nathan-helm-burger) · 2024-01-28T17:37:43.937Z · LW(p) · GW(p)
Yes, but the costs are sufficiently high that it discourages researchers from trying to create new medicines which would be broadly helpful but unprofitable. Such as better treatments and preventative medicine for diseases that only afflict poor people in underdeveloped regions. It doesn't have to be all or nothing. We could have a scaled back paranoia around risk, and thus allow the FDA to pass medication for vastly decreased process costs. The question then is about trade-offs. Given that there will be QUALYs lost on either side of the decision boundary, we should seek to minimize regret. Instead we are seeking to minimize Copenhagen-ethics-style culpability, and thus incurring a lot of regret. Getting rid of the FDA entirely would shift the decision boundary, but probably too far in the opposite direction. That doesn't mean the status quo is near optimal.
Replies from: Ponder Stibbons↑ comment by Ponder Stibbons · 2024-01-29T11:40:20.012Z · LW(p) · GW(p)
It is true that most pharma companies concentrate on indications that supply returns to offset the cost of development. The FDA does have a mechanism for Orphan Drug approval, for rare diseases, where the registration requirements are significantly lowered. According to this site 41 orphan drug approvals were made in 2023. Whether this mechanism is good enough allow the promototion of rare disease in the larger pharmaceutical industry is a good question. I wonder how many of these drugs, or their precursors, originated in academic labs,, and were then spun out to a start-up or sold on?
Replies from: nathan-helm-burger↑ comment by Nathan Helm-Burger (nathan-helm-burger) · 2024-01-29T16:17:27.991Z · LW(p) · GW(p)
Orphan drugs, yes. But no program for "drugs to more cheaply prevent conditions common in poor people but completely absent in rich people." That's the program I'd like to see.
↑ comment by Wbrom (Wbrom42@gmail.com) · 2024-01-27T14:20:29.384Z · LW(p) · GW(p)
The FDA does not provide good guidance on what treatments should be applied in what situations. They approve drugs for a limited set of uses and that's it. Most drugs are applied "off label" which the FDA rules that drug companies specifically cannot comment on -- so not only does the FDA not provide guidance on the most common use for most medications, they actually prevent that guidance from being provided.
Replies from: jmh, Ponder Stibbons↑ comment by jmh · 2024-01-28T15:18:31.153Z · LW(p) · GW(p)
One reason the company might not be allowed to comment on is that they lack the knowledge in that space so would only be marketing from a basis of ignorance.
However, the FDA does not prevent such guidance as a quick look at sited like WebMD or PDR will generally include information on off label use.
↑ comment by Ponder Stibbons · 2024-01-29T12:02:52.964Z · LW(p) · GW(p)
My understanding is that off-label often means that the potential patient is not within the bounds of the clique of patients included in the approved clinical trials. We don’t usually perform clinical trials on children or pregnant women, for instance. Alternatively, strong scientific evidence is found that a drug works on a related disease to the actual target. It may well make sense to use drugs off label where the clinician can be comfortable that the benefits out-way the possible harms. In other cases, of course, it would be extremely poor medicine. In any case, having statistically significant and validated evidence that a drug actual does something useful, is non-negotiable IMO.
comment by Ponder Stibbons · 2024-01-26T23:29:15.115Z · LW(p) · GW(p)
Poorly regulated health orientated companies selling products that have little or no value? Seems unlikely.. Oh wait, what about Theranos?
↑ comment by Wbrom (Wbrom42@gmail.com) · 2024-01-27T14:16:59.882Z · LW(p) · GW(p)
You mean the Theranos that is specifically regulated by CLIAA and Medicare which did nothing to stop them until they actually destroyed people's lives?