Alcor vs. Cryonics Institute
post by prespectiveCryonaut · 2012-04-09T01:49:32.295Z · LW · GW · Legacy · 125 commentsContents
125 comments
I searched but did not find any discussion comparing the merits of the two major cryonics providers in the US, so I figured it might be productive to start such a discussion myself by posing the question to the community: which provider would you choose, all things being equal: Alcor or the Cryonics Institute?
From my research, Alcor comes across as the flasher, higher-end option, while CI seems more like a Mom-and-Pop operation, having only two full-time employees. Alcor also costs substantially more, with its neurosuspension option alone running ~$80k, compared with CI's whole-body preservation cost of ~$30k. While Alcor has received far more publicity than CI, much of it has been negative. The Ted Williams fiasco is probably the most prominent example, although the accuser in that case seems anything but trustworthy. However, Alcor remains something of a shadowy organization that many within the cryonics community are suspicious of. Mike Darwin, a former Alcor president, has written at length on both organizations at http://www.chronopause.com, and on the whole, at least based on what I've read, Alcor comes across looking less competent, less trustworthy, and less open than CI.
One issue in particular is funding. Even though Alcor costs much more, it has many more expenses, and Darwin and others have questioned the long term financial stability of the organization. Ralph Merkle, an Alcor board member and elder statesman of cryonics who has made significant contributions to other fields like nanotechnology, a field he practically invented, and encryption, with Merkle's Puzzles, has essentially admitted(1) that Alcor hasn't managed its money very well:
"Some Alcor members have wondered why rich Alcor members have not donated more money to Alcor. The major reason is that rich Alcor members are rich because they know how to manage money, and they know that Alcor traditionally has managed money poorly. Why give any significant amount of money to an organization that has no fiscal discipline? It will just spend it, and put itself right back into the same financial hole it’s already in.
As a case in point, consider Alcor’s efforts over the year to create an “endowment fund” to stabilize its operating budget. These efforts have always ended with Alcor spending the money on various useful activities. These range from research projects to subsidizing our existing members — raising dues and minimums is a painful thing to do, and the Board is always reluctant to do this even when the financial data is clear. While each such project is individually worthy and has merit, collectively the result has been to thwart the effort to create a lasting endowment and leave Alcor in a financially weak position."
Such an acknowledgement, though appreciated, is frankly disturbing, considering that members depend utterly on these organizations remaining operational and solvent for decades, perhaps even centuries, after they are deanimated.
Meanwhile, CI carries on merrily, well under the radar, seemingly without any drama or intrigue. And Ben Best seems to have very good credentials in the cryonics community, and Eliezer, one of the most prominent public advocates of cryonics, is signed up with them. Yet the tiny size of the operation still fills me with unease concerning its prospects for long-term survivability.
So with all of that said, besides cost, what factors would lead or have led you to pick one organization over the other?
1: http://www.alcor.org/Library/html/CryopreservationFundingAndInflation.html
125 comments
Comments sorted by top scores.
comment by maxmore · 2012-04-09T05:48:25.267Z · LW(p) · GW(p)
“However, Alcor remains something of a shadowy organization that many within the cryonics community are suspicious of.”
Really? That’s a remarkable statement. Alcor has a long history of open communication with its members and the cryonics community in general. Among the ways Alcor does this:
- Cryonics magazine
- Alcor News emailings
- RSS feed
- conferences
- case reports
- extremely detailed website with information on finances, governance… everything
- Facebook page
- Member Forums
See: http://www.alcor.org/newatalcor.html
“Mike Darwin, a former Alcor president, has written at length on both organizations at http://www.chronopause.com, and on the whole, at least based on what I've read, Alcor comes across looking less competent, less trustworthy, and less open than CI.”
Darwin is a member of Alcor, not CI. How do you explain that? Darwin thoroughly enjoys criticizing Alcor (rightly or not) but remains a member. In a related comment, ahartnell says “from what I have read both seem to provide basically the same service”.
This is a remarkable belief. Alcor uses the most advanced cryoprotectant, M22, to perfuse whole bodies and neuros. CI uses a less advanced (and cheaper) cryoprotectant but cryoprotects ONLY THE HEAD, allowing the rest of the body to be straight frozen with massive damage. That’s especially odd since (many of) CI members are insistent about being whole body patients rather than neuros.
Also, and VERY importantly, ischemic time matters hugely. CI members can get standby and transport services from SA by paying a fee (one that makes Alcor neuros significantly LESS expensive). Otherwise, except for CI members undergoing clinical death in the Detroit area, this means long ischemic times and tremendous damage. When I was at CI’s 2011 AGM, Aschwin and Chana de Wolf presented their research findings showing the frightening damage done by extended ischemic time. They also showed that a large majority of CI patients experienced that damage. Staggeringly, no one objected, challenged them, or seem the least concerned.
You mention Mike Darwin, yet note that in Figure 11 of a recent analysis by him, he says that 48 percent of patients in Alcor's present population experienced "minimal ischemia." Of CI, Mike writes, "While this number is discouraging, it is spectacular when compared to the Cryonics Institute, where it is somewhere in the low single digits."
As to Ralph Merkle’s comments: His frank assessment of past practices contradicts the claim that Alcor is secretive. His comments were also about past practices. Unlike CI, Alcor has created robust practices and mechanisms for long-term maintenance and growth of the Patient Care Trust Fund and the Endowment Fund. Go take a look at CI’s financial reports. See how little money is available for the indefinite care and eventual revival of each patient. Also look at the returns on investment of those funds.
For those interested in comparing Alcor and CI, plenty of basic factual information is available here:
http://www.alcor.org/FAQs/faq06.html#choose
Replies from: gwern, shminux, CharlesR, prespectiveCryonaut, benbest, elityre, mkmk↑ comment by gwern · 2012-04-09T16:33:39.477Z · LW(p) · GW(p)
Darwin has also criticized CI here:
http://chronopause.com/index.php/2011/04/14/cryonicists-teach-your-children-well/
And this situation isn’t hypothetical either, because when the Cemetery Board came down on the Cryonics Institute (CI) , CI, and thus the American Cryonics Society (ACS), decided to surrender control of their patients to the state. Now, it is the laws and jurists of the state of Michigan that determine the conditions under which a patient can be removed from a cryostat at CI, and be relocated elsewhere, not the CEO or the Board of either CI, or ACS. If you want to understand the practical implications of this, you can go to http://www.bhsj.org/forms/disinterment%20and%20reinterment.pdf and to http://law.onecle.com/michigan/333-health/mcl-333-2853.html and read what you find there. It isn’t pretty.
http://chronopause.com/index.php/2011/02/13/on-the-need-for-prosthetic-nocioception-in-cryonics/
I do not want to seem too harsh on Alcor here, because Alcor did have cameras, and does lock its patient dewars. The Cryonics Institute does not even lock their patient dewars – this is an issue I have raised with their management several times over the years, but to no avail. Any careful reading of Johnson’s book, Frozen, should eliminate any doubt as to why locking access to the patients on multiple levels is not only desirable, it is essential.
http://chronopause.com/index.php/2011/02/23/does-personal-identity-survive-cryopreservation/#comment-247 (his longest sustained criticism that I know of, too long to quote in full)
It was a snotty, and probably inappropriate remark. Basically I was commenting on the operational paradigm at CI, which is pretty much “ritual.” You sign up, you get frozen and it’s pretty much kumbaya, no matter how badly things go. And they go pretty badly. Go to: http://cryonics.org/refs.html#cases and start reading the case reports posted there. That’s pretty much my working definition of horrible. It seems apparent to me that “just getting frozen” is now all that is necessary for a ticket to tomorrow, and that anything else that is done is “just gravy,” and probably unnecessary to a happy outcome.
...Even in cases that CI perfuses, things go horribly wrong – often – and usually for to me bizarre and unfathomable (and careless) reasons. My dear friend and mentor Curtis Henderson was little more than straight frozen because CI President Ben Best had this idea that adding polyethylene glycol to the CPA solution would inhibit edema. Now the thing is, Ben had been told by his own researchers that PEG was incompatible with DMSO containing solutions, and resulted in gel formation. Nevertheless, he decided he would try this out on Curtis Henderson. He did NOT do any bench experiments, or do test mixes of solutions, let alone any animal studies to validate that this approach would in fact help reduce edema (it doesn’t). Instead, he prepared a batch of this untested mixture, and AFTER it gelled, he tried to perfuse Curtis with it. See my introduction to Thus Spake Curtis Henderson on this blog for how this affected me psychologically and emotionally. Needless to say, as soon as he tried to perfuse this goop, perfusion came to a screeching halt. They have pumped air into patient’s circulatory systems… I could go on and on, but all you need to do is really look at those patient case reports and think about everything that is going on in those cases critically.
...What is unethical is the sleight of hand CI has engaged in. They want to be able to say that, “No cryonics patient has been thawed out for lack of funding since 19XX…” So, in order to make that so, they get the mortuary industry to freeze the poor devils, and then if things “don’t work out,” it’s the morticians who get stuck thawing the person out. It’s a beautiful “moral switch and bait” in that it recasts the act of cryopreserving a person such, that: You are not a cryonics patient when you get frozen. You are not a cryonics patient if you stay frozen for years. In fact, you are only a cryonics patient when CI says you are cryonics patient. CI has become the Hane’s Underwear, Co., Inspector #12 of cryonics....
Moving on:
Go take a look at CI’s financial reports. See how little money is available for the indefinite care and eventual revival of each patient. Also look at the returns on investment of those funds.
When I posted on the Alcor grandfathering issue, I finished by asking what the situation for CI was. No one but Jason took up the question.
Replies from: ahartell, Nova_Division, advancedatheist↑ comment by Nova_Division · 2012-04-10T01:52:26.775Z · LW(p) · GW(p)
Can anyone here tell me more about Johnson's book "Frozen" mentioned in this comment? I looked it up on Amazon and read Alcor's response to legal issues here: http://www.alcor.org/press/response.html but what I want to know is, from LessWrongians who have read it, is it all a crock, or is there some truth in it?
Replies from: bgwowk↑ comment by bgwowk · 2012-04-11T01:23:19.400Z · LW(p) · GW(p)
In my role as an Alcor director, I had the painstaking and unpleasant task of investigating the veracity of Johnson's book allegations to determine which of them required legitimate corrective action or litigation for defamation. Some of the allegations published in New York Daily News and wire services in 2009 promoting the book weren't even anywhere in the book (e.g. allegations that Alcor dismembered live animals). Such lies about the book itself were apparently just invented to get international media attention two days before the book's release. Some of the allegations inside the book were so outrageous that no reasonable person knowing anything about cryonics could believe them, such as Alcor kidnapping teenagers and homeless people and burying them in the desert, or engaging in drug trafficking and wild car chases. Other allegations, such as certain cryonics cases being "botched," I knew immediately were false because I had personal knowledge of the cases, or because they were repeats of false allegations Johnson made during his previous reach for fame in 2003.
http://www.alcor.org/Library/html/sportsillustrated.htm
Many other allegations required investigation. In some cases, such as false allegations of illegal waste disposal, public sources were sufficient to refute them.
http://www.cryonet.org/cgi-bin/dsp.cgi?msg=22461
To summarize, although there was enough superficial truth in "Frozen" and enough real controversy in Alcor's history to establish a veneer of credibility to the casual reader, the vast majority of the book is deliberately crafted to depict Alcor and cryonicists in the worst possible light, and uses literally hundreds of false claims and allegations to do it. It's not just a matter of poetic license, but fabrication of entire anecdotes and conversations that never happened. In some cases there was also editing of conversations to create completely different meanings than the original conversations (editing that ABC News co-participated in, but that's another story). There were accounts of cryonicists having loathsome medical conditions that they did not have (one of the legal definitions of defamation per se), partying with human remains, animal abuse, cultism, brainwashing, deviant sex, and poor hygiene. As one commentator on Amazon.com put it, Johnson could have been more credible had he not go so completely over-the-top.
Partial book rebuttals concerning matters they have personal knowledge of have been published by well-respected cryonicists Steve Harris and Charles Platt
http://www.network54.com/Forum/291677/thread/1258263309/The+Instability+of+Larry+Johnson%27s+History
http://www.cryonet.org/cgi-bin/dsp.cgi?msg=32722
Alcor chose to litigate 32 defamation claims in the present New York lawsuit that is continuing against the publisher, Vanguard Press, and coauthor Scott Baldyga.
http://www.alcor.org/Library/pdfs/NewYorkComplaintAmendedJan2010.pdf
We could have added many more, but those are enough work as it is. Someday, once the litigation is done, I may write a 100-page tome of everything that is false in that book. But in the meantime my time and freedom to do is limited by the fact that the litigation is still ongoing.
It's unfortunate and unfair that news media keep rehashing this stuff. It's so much easier to destroy things than create them.
Replies from: ciphergoth, enoonsti, melmax↑ comment by Paul Crowley (ciphergoth) · 2012-04-11T06:39:35.584Z · LW(p) · GW(p)
coughs er, though I'm sorry that it was said about people about whom it wasn't true, it seems a little unfair on those of us who enjoy deviant sex to include it in such a list.
↑ comment by enoonsti · 2012-04-12T08:16:33.556Z · LW(p) · GW(p)
As I was reading Frozen, I kept thinking: "You know what this book needs? A randomly inserted car chase." Sure enough, OP delivered. Oh, and if I received incompetent death threats, I would have had them checked for fingerprints. But Larry didn't have them checked. Because he probably printed them out himself.
tldr; I hope someday you get around to that tome.
↑ comment by melmax · 2012-12-04T15:31:05.602Z · LW(p) · GW(p)
Partial book rebuttals concerning matters they have personal knowledge of have been published by well-respected cryonicists Steve Harris and Charles Platt<<"
Respected by whom, Dr. Wowk? Other people being funded by LEF, such as yourself? If these two "pillars of the community" are the best you can come up with, Vanguard will mop the floor with Alcor, if their case ever goes to court. Platt has been accused of being dishonest (both privately, and publicly), by an amazing number of individuals, who have had the misfortune of working with him. Harris has committed a number of blunders, such as libeling a medical professional he did not know, (in the interest of protecting a company closely related to Alcor); publishing what appears to be a policy of euthanizing Alcor and/or SA clients who show signs of life during a cryonics procedure; and endorsing laymen having access to propofol.
If your two star witnesses can be proven to have publicly lied, in the interest of protecting Alcor and/or Suspended Animation, (both those companies receive funds from LEF, as does Dr. Wowk's 21CM), how will their testimony hold up in court.?
The laymen reading this, and other forums, might believe the propaganda Dr. Wowk participates in, but things are likely to go differently, in a court of law. Judging by the published court documents, Vanguard is willing to put up a good fight and, unlike Johnson, they are probably well-funded enough to do so.
↑ comment by advancedatheist · 2012-04-09T18:22:14.151Z · LW(p) · GW(p)
CI's threadbare state after all these decades seems especially surprising considering that Robert Ettinger founded it, and apparently he couldn't do any better with it despite his status as one of the the originators of the cryonics movement
Nonetheless, Ettinger's cryosuspension made the national news last summer. By contrast, the suspension of Fred Chamberlain by Alcor a few weeks back went unnoticed in the larger world, despite Alcor's somewhat higher name recognition, because Fred never became the public face of cryonics.
Yet, as others have pointed out, CI operates as a "cemetery," and the bureaucratic mind doesn't allow for the removal of bodies in cemeteries to subject them to experimental medical procedures. A suspension with CI therefore resembles the selling point of the Roach Motel: You can check into the dewar, but you can never check out.
Replies from: gwern, mkmk↑ comment by gwern · 2012-04-09T18:33:14.370Z · LW(p) · GW(p)
Yet, as others have pointed out, CI operates as a "cemetery," and the bureaucratic mind doesn't allow for the removal of bodies in cemeteries to subject them to experimental medical procedures
I don't think that really matters: if revivification works, there will be a way around that. The important thing is getting bodies intact to that point. Subjecting them to procedures might be an interesting restriction on CI, except as far as I know, once one is cooled, there are no procedures besides topping up the tanks and every blue moon being switched from tank to tank.
I take Darwin as pointing out that CI has legal vulnerabilities to outside coercion and pressure that Alcor has apparently avoided; I haven't read his links so I don't know what, but lawsuits and activist public officials and overly broad public health laws come to mind.
Replies from: advancedatheist↑ comment by advancedatheist · 2012-04-10T00:38:34.487Z · LW(p) · GW(p)
Yet, as others have pointed out, CI operates as a "cemetery," and the bureaucratic mind doesn't allow for the removal of bodies in cemeteries to subject them to experimental medical procedures
I don't think that really matters: if revivification works, there will be a way around that.
That doesn't necessarily have to happen. Peter Thiel in his recent debate with George Gilder argues that most forms of engineering since 1970 have become effectively illegal. Some universities might still offer degrees in nuclear engineering, for example, but that field has horrible job prospects, so it might as well have become illegal. It wouldn't take much to add cryonics to the list of prohibited technologies.
Replies from: arundelo, TimS, gwern↑ comment by arundelo · 2012-04-10T02:02:58.929Z · LW(p) · GW(p)
I found the Thiel-Gilder debate.
Thiel's list of fields where "innovation in stuff was 'outlawed'":
- petroleum engineering
- nuclear engineering
- electrical engineering
- chemical engineering
- mechanical engineering
- bio-engineering
I can believe that changes in the law and the legal-political climate have hampered innovation in at least some of those fields, but by "outlawed" Thiel seems to mean "a bad career choice", judging from what he says at 42:17.
Edit: Thiel does not just mean "a bad career choice"; he gives some examples of what he does mean at about 9:50 of this July 16 2012 debate with Eric Schmidt:
I think it's because the government has outlawed technology. We're not allowed to develop new drugs with the FDA charging $1.3 billion per new drug. You're not allowed to fly supersonic jets, because they're too noisy. You're not allowed to build nuclear power plants, say nothing of fusion, or thorium, or any of these other new technologies that might really work. So, I think we've basically outlawed everything having to do with the world of stuff, and the only thing you're allowed to do is in the world of bits. And that's why we've had a lot of progress in computers and finance. Those were the two areas where there was enormous innovation in the last 40 years. It looks like finance is in the process of getting outlawed, so the only thing left at this point will be computers [...]
↑ comment by TimS · 2012-04-10T00:50:49.482Z · LW(p) · GW(p)
[nuclear engineering] has horrible job prospects, so it might as well have become illegal.
That's not a very accurate way to think about legal problems. For comparison, PhDs in English Literature have horrible job prospects, but that's not evidence that English Lit is becoming illegal.
Replies from: advancedatheist↑ comment by advancedatheist · 2012-04-10T15:05:24.059Z · LW(p) · GW(p)
If your field of engineering, despite its productive potentials, faces political moves to shut it down and throw you out of work, that has about the same effect as making it illegal.
Replies from: CarlShulman↑ comment by CarlShulman · 2012-04-12T00:07:16.095Z · LW(p) · GW(p)
Facing threats of possibly somewhat lower salaries and job prospects is quantitatively far less severe than being banned. Cutting the expected value of training for a profession by 10% is very different from cutting prospects by 50% or 90%.
↑ comment by mkmk · 2012-04-16T00:10:36.989Z · LW(p) · GW(p)
Robert Ettinger had a superior cryosuspension because he didn't rely on long distance remote standby from SA or elsewhere. He planned and had his ducks in a row so to speak. Many Alcor and SA contracted patients have rotted for many hours waiting for the very expensive far away teams. Some of these things were due to to matters out of anyone on the remote standby team's control but distance cannot be removed as a factor. Robert had set up his own local standby with family, friends etc and the results speak for them selves.
Also the only reason CI ever had to operate under the cemetary statutes is because of negative PR and generated by Alcor with the Ted Williams case. Michigan bureaucrats responded to the negative PR with the current state of affairs. The cloak of cemetery regulation does protect CI to a limited degree in the future from further Alcor PR nightmares because it can be regulated in a way that the Michigan bureacrats can understand. So in the end it worked to CI's benefit. I would hardly blame CI for making lemonaid out of Alcor generated lemons!
↑ comment by Shmi (shminux) · 2012-04-09T20:09:14.538Z · LW(p) · GW(p)
Since you are around to answer questions...
As I mentioned elsewhere, my biggest concern is the continuous operation of a cryoshop over the potential centuries or even millennia until the revival is attempted, as nearly no entities have ever survived that long. I have been unsuccessful in my search for an Alcor executive explicitly responsible for existential risk analysis and mitigation.
By existential risk to the company I mean an event that would result in the company failing to the degree that the stored patients are discarded, even though the outside world merrily hums along, and not an event that wipes out a large chunk of humanity.
The FAQ does not seem to answer the obvious hard questions like "what if Morgan Stanley goes under?", "what if the US dollar collapses?", "what other existential risks exist, and what are their probability estimates and error bars?", "what is the estimated lifetime of Alcor until it suffers a complete failure from one of the existential risks to it coming to pass?" etc. By the way, if you think that the answer to the last question is "infinite", I recommend a basic probability and statistics course.
In other words, the risk management appears to be at the level no better than that of a regular insurance company, which is completely inadequate for an organization whose long-term survival is the most critical issue. Is this perception wrong?
Replies from: advancedatheist↑ comment by advancedatheist · 2012-04-10T00:28:35.440Z · LW(p) · GW(p)
The FAQ does not seem to answer the obvious hard questions like [snip] "what if the US dollar collapses?"
I thought the value of the U.S. dollar has already "collapsed" since 1913, though the people who make this claim as part of anti-Fed crankery don't seem to understand their own propaganda.
↑ comment by CharlesR · 2012-04-09T06:55:30.526Z · LW(p) · GW(p)
maxmore, since you're here, I have a question:
How much life insurance do I need?
The cost for whole body is $200,000. So do I need $200,000 or do I need what it costs at time of death? Historical data says the cost doubles every 20 years.
Replies from: maxmore↑ comment by maxmore · 2012-04-09T08:38:34.245Z · LW(p) · GW(p)
CharlesR: First of all, let me say that I have sufficient funding for whole body, yet I have chosen the neuro option. I find it difficult to fathom why anyone would want to bring along a broken-down old body which is going to have to be replaced anyway. We can store ten neuro patients for the cost of one whole body patient (which means that we are probably underpricing WBs currently). A neuro arrangement with Alcor currently costs $80,000. Although WB prices may have to rise before long, I've heard no suggestion that neuro rates need to rise anytime soon.
However, assuming someone is determined to take along their complete body, no matter how old and infirm, to answer your question: You CURRENTLY need a MINIMUM of $200,000. At that rate, we are currently drawing between 3% and 4% of the amount going into the Patient Care Trust for indefinite care and eventual revival. That may be sustainable, but is more than our desired conservative estimates. We aim to draw no more than 2% per year. Currently, I'm driving to reduce our costs, especially for liquid nitrogen. Early next year, we should be able to revise our contract and bring these down significantly.
Even so, you should plan to have available not $200,000, but that amount compounded by something like the general rate of inflation. (Your cost doubling rate of 20 years looks close to me. I think it's maybe 22 or 23 years, given a century-long average, but very close...) Unfortunately, some cryonicists have assumed that costs would remain unchanged. Given the history of inflation, that expectation is simply either ignorant or irrational. I would urge every cryonicist to plan for costs to rise by at least the historical long-run average of about 3% annually.
How do you plan for that? You might take out considerably more life insurance initially. You might take out the current minimum or a bit more, then over time supplement that by prepaying additional amounts. We are currently figuring out various options that might help deal with the annoying but inevitable reality of inflation.
If you, or anyone else, would like to discuss this in more detail and in a more personal way, please, please, please, call me at 480.905.1906 x113
--Max
Replies from: TheOtherDave, bogdanb↑ comment by TheOtherDave · 2012-04-09T13:18:51.016Z · LW(p) · GW(p)
I find it difficult to fathom why anyone would want to bring along a broken-down old body which is going to have to be replaced anyway.
Well, the brain will have to be replaced as well. If we assume everyone who signs up for cryonics is solely motivated by the intent to maximize the expected value of their continued information-theoretical identity after their cells die, we might infer that those people suspect that some of that information-theoretical identity resides somewhere other than their brain... in their adrenal glands, perhaps, or in their fat cells, or who knows.
That said, I am skeptical about both the premise and the conclusion.
Replies from: David_Gerard, James_Miller↑ comment by David_Gerard · 2012-04-09T14:40:59.537Z · LW(p) · GW(p)
The spare brain in the gut? About a thousandth the size of the one in the head, but rather influential.
Replies from: TheOtherDave↑ comment by TheOtherDave · 2012-04-09T15:49:36.625Z · LW(p) · GW(p)
Just to be clear, what I'm skeptical about is the idea that cryonics adopters are in fact generally seeking to maximize the expected value of their continued information-theoretical identity after their cells die.
I certainly agree that there's stuff outside my brain that contributes significantly to the construct I'll label "TheOtherDave" for convenience, including but not limited to the enteric nervous system. (Indeed, much of that stuff is outside my body as well.)
Not that this makes me a skeptic about post-mortem person reconstruction, particularly. I'm perfectly prepared to believe that something could be extracted from my properly-preserved body that would be similar enough to me for it deserve the label "TheOtherDave" about as well as I do. Ditto for my properly-preserved brain; in that I'm not at all confident that the extracranial stuff is necessary when it comes to distinguishing plausible "TheOtherDave" candidates from implausible ones.
To be honest, though, I'm not convinced that my brain is necessary either. Constructing a plausible "TheOtherDave" candidate from information outside my body (e.g, my writings and relationships and demographics and so forth) probably isn't that much harder than doing so from information inside my body; given a system capable of doing the latter, it's likely less than a few centuries of progress until we have a system capable of doing the former. (Actually, I'm not entirely convinced that former is harder than the latter at all.)
↑ comment by James_Miller · 2012-04-09T18:06:29.015Z · LW(p) · GW(p)
people suspect that some of that information-theoretical identity resides somewhere other than their brain
That's why I've gone whole body with Alcor.
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-11T19:57:27.734Z · LW(p) · GW(p)
Yes, unquestionably some of the "information" that constitutes your person hood is in your gut, your glands, your immune system and your peripheral nervous system. However, your position would seem to imply that these things, and things much more central to your identity, such as your brain structure, are like unchanging books or artifacts on a museum shelf. They aren't. In fact, by the time you are 80, you will have lost roughly a third of your brain mass and your brain will be a tattered "remnant" of what it once was. You're now losing roughly 80K neurons a day. The practical consequences of this will be a massive transformation of your personality and of your functional capabilities. If that change were to be imposed on you all at once, you would not only be horrified, you likely wouldn't even recognize the resulting individual as the same person. More likely, you'd consider that individual to be a cruel and sadistic parody of yourself.
The point is that your "identity" is a dynamic thing which is badly degraded over time by aging. This is important information to keep in mind, because it provides context for what I'm going to say now. I have known a good number of people who have no stomach or intestines. They could not eat food of any kind. They stayed alive by virtue of total parenteral nutrition (TPN) which provides for all their fluid and nutritional needs intravenously. These people did not undergo any perceptible change in memory, personality or person-hood. At least three such people I've known have also had kidney transplants. That's even more interesting, because we now know that many patients with successful, long term grafts become chimeric with the donor! Donor immune and stem cells colonize the patient! Similarly, any mother is chimeric for each of her fetuses. In fact, in animals, if you injure the mother's heart or brain during pregnancy, the fetal stem cells are the ones which repair the damage - massively remodeling the damaged organs. This chimerism seems to be an evolutionary adaptation to protect the mother against injury during pregnancy.
To my knowledge, no one is upset at the idea that a significant fraction of the stem cell population in such people is ALIEN. And those stem cells are genetically and functionally different from the native ones. Maybe more than the gut, the immune system is an extension of the brain - they interact dynamically and the immune system can and does profoundly effect mood and behavior.
So what is identity? Well, that's complicated, but one thing is clear, it is NOT static and a lot of the changes in the structures which determine it happen all the time as part of life, and you have little or no control over them. Where this intersects whole body vs. neuro is that you have the need (arguably the necessity) to decide just what parts of you are truly essential to your person-hood AND at what cost in risk to survival they can be taken along during cryopreservation.
If you are smart, cool, and rational, you'll try to determine just what parts of you are really you - are really essential to your person-hood. This would be an impossible black box of a task were it not for contemporary transplant and artificial organ medicine. There are tens of thousands of people on dialysis or who get kidney transplants. There are people with no hearts, or new hearts, and people with gut, liver, pancreas and renal transplants. There are countless people with bone marrow transplants and countless others whose spinal cord and peripheral nervous system have been functionally disconnected from their brains. Do these people constitute an acceptable degree of survival for you as persons? If so, I would suggest you delve into the logistics, economics and hard practical realities of cryopreservation that must endure over a period of many decades, or far more likely, a century or two. It is NOT easy to handle, move or care for whole body patients. They are a ball and chain and cannot be moved or evacuated quickly. They are subject to a large burden of state regulation which neuros are not, and they suffer additional injury to the brain as a result of compromises necessary to achieve cryoprotection and cooling.
If you think that those components of you identity present in your body are worth those added risks, then you should go whole body. However, my question is, where is the empirical evidence to support that belief? I've known many, many transplant patients well, and neither they nor I saw any noticeable transformation in their identity. Indeed, the transformation, such as it was, was the return to fully functioning person-hood which resulted from becoming chimeric with another human being or a machine.
Replies from: James_Miller↑ comment by James_Miller · 2012-04-11T20:07:46.411Z · LW(p) · GW(p)
Thanks for the very thoughtful reply. I hadn't properly considered the "ball and chain" risks of whole body you mentioned. Is there much of a chance that technology will develop in a way so that I will be revived sooner if I go with whole body rather than neuro?
↑ comment by bogdanb · 2012-04-09T19:43:25.107Z · LW(p) · GW(p)
I find it difficult to fathom why anyone would want to bring along a broken-down old body which is going to have to be replaced anyway.
Even assuming that making a new body is better than fixing the broken one (quite likely especially if ems are included in “new body”), how would its nerves (or equivalent) be connected to the repaired brain without a template of where each of the old nerves went? I was under the impression that the neural system, like the circulatory system, is “the same” between individuals only on the large scale, and individual fibers grow more or less randomly, like arterioles, the brain learning the positions of everything during growth.
I can well imagine almost-AGI level machines able to deduce most or maybe all of these based only on watching the effects of gentle prods to the inputs on unconscious brains, but with only human-level intelligence, even with em technology and fantastic (but not AI) computers I can’t quite see how you could do it without participation from the patient, and thus subjecting them to what I imagine might be described as “hellish maelstrom of the senses” for a quite long time.
(I don’t expect definite answers, of course—like the rest of cryonics, if we knew all the details we’d be doing it right now. I just wonder if this was discussed somewhere, and perhaps there’s something I’m not aware of which makes it simple in principle given some plausible anticipated advances. Do we even know if it’s possible, looking at just a single random axon, cut at the neck, to tell whether it connected to a nociceptor or a proprioceptor, even knowing exactly where it goes and everything there is in the brain? I mean, other than prodding it and asking the patient what they felt.)
Replies from: Merkle↑ comment by Merkle · 2012-04-10T09:12:07.352Z · LW(p) · GW(p)
You might want to read Cryonics, cryptography, and maximum likelihood estimation.
Short summary: if cryptanalytic methods can recover the wiring of World War II rotor machines knowing only some input-output pairs and with only limited information about the actual wiring, then similar algorithms should be able to recover the neuronal "wiring" between different cortical areas when we already have a wealth of information about that wiring plus a good knowledge of acceptable input-output pairs.
↑ comment by prespectiveCryonaut · 2012-04-09T06:49:50.971Z · LW(p) · GW(p)
Thanks for your reply, Max. It does seem that Darwin is a bit harder on Alcor, but perhaps some of that is just because it's closer and more personal to him from having worked there and being signed up with them.
Replies from: maxmore↑ comment by maxmore · 2012-04-09T08:23:39.799Z · LW(p) · GW(p)
Yes, exactly! Darwin says very little about CI. He's enormously critical of Alcor. Why? The answer is complicated, but part of it clearly is that he was a major force in Alcor in earlier years and has perfectionist standards that ignore costs and other real constraints. He may also be envious that he isn't running things. Alas, his past relationships make that inevitable.
Despite his impulse to stick in the knife, I keep a close eye on his detailed blog posts, since he does have a remarkable depth of knowledge. That depth and his most excellent writing skills often fool people into believing that his judgment is better than it is. But, flawed as it is, his writing contains much of value, so I set my feelings aside and glean as much value as I can from his views.
If Darwin were to turn his attention to CI, the result would be truly ugly!
Please note, that I'm GLAD that CI exists. I respect Ben Best. I think he's doing the best he can with what I think is a badly flawed approach. Although I worry about CI's future, anyone who wants to be cryopreserved but genuinely cannot afford Alcor (about the cost of a venti coffee at Starbucks daily) should definitely look to CI and an alternative.
--Max
Replies from: mikedarwin, curiousepic, cath, mikedarwin↑ comment by mikedarwin · 2012-04-11T09:06:02.362Z · LW(p) · GW(p)
There's no mystery about why I have comparatively few criticisms posted about CI. My reasons for this are as follows:
1) Ci is what it is. What you see is pretty much what you get, and that this is so is evident from the discussion here. The perception of CI as a "mom and pop" outfit is but one example I could cite from this discussion. Ci does not project itself as using a medically-based model of cryonics. It's case histories are ghastly - and anyone who doesn't take the time to read them, or who can't see what the deficiencies are, well, you can't (as I've learned the hard way) fix clueless.
2) I am not a CI member. The reason I am not a CI member can be divined from my written criticisms and by looking over point #1, above. If I were a Ci member, I have no doubt that I would have posted reams of criticisms. Note that I said "posted," because, in fact, I have written reams of criticisms, suggestions, detailed technical advice and countless letters and personal communications on specific deficiencies at CI. I have also generated Power Point presentations and written many pages of material on how CI could improve its capabilities. To their credit, CI has at least listened to these suggestions and critiques; and they are responsive to same. This is not imply that they are receptive. But at least they listen and engage in dialogue. Alcor does not.
3) Since I am not a CI member, and I do not believe CI materially misrepresents itself, or its capabilities, and because they have invited private criticism in the past, I see no need to discuss their deficiencies publicly, beyond the (comparatively) brief remarks I've made from time to time. What would be the point of going further? The only exception I can think of is when CI takes actions that could, or which do materially impact the operation of cryonics as a whole. Some examples of that would be their submission to regulation by the Michigan Cemetery Board, their practice of accepting at need cases absent any defined standards for informed consent, and their practice of having morticians freeze, and if necessary, thaw cryonics "bodies," whilst claiming that cryonics "patients" haven't thawed out since the 1970s.
4) Because Alcor represents itself as a medically-scientifically based cryonics operation I believe that it is not only deserving of the criticism it has received, but of much more. While the care Alcor patients receive is, on average, much better than that available at CI, it is still, in my opinion, grossly substandard, frequently marred by inexcusable iatrogenesis, and not in keeping with the highly professional and medically sophisticated image that Alcor projects on its website, in its literature, and via the media. If anyone is truly interested, I'm wiling to discuss specifics - and in detail. In fact, shortly I will be posting a piece about research priorities in cryonics, which should give some perspective on just how Less Right Alcor has become.
5) The problem is deeper than the specifics at Alcor, it is inherent in cryonics itself. A simple introduction to the root problem can be found here: http://chronopause.com/index.php/2011/02/13/on-the-need-for-prosthetic-nocioception-in-cryonics/
A much more detailed analysis of the problems that have beset and thwarted cryonics can be found here :
http://cryoeuro.eu:8080/download/attachments/425990/Cryonics_Failure_Analysis_Part_2v5.2.pdf
http://cryoeuro.eu:8080/download/attachments/425990/Cryonics_Failure_Analysis_Part_3v5.4.pdf
[Please note that the server hosting the two files above is sometimes unavailable - please try again if you aren't successful.]
This post http://chronopause.com/index.php/2011/05/29/a-visit-to-alcor/ provoked outrage from Max More and in private correspondence, now many months ago, he told me he was working on a response that would demonstrate my criticisms were in error.. Apparently, he is still working on it.
I've posted a more detailed explanation of the problems vis a vis Alcor and cryonics as a response to this post.
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-11T09:06:45.762Z · LW(p) · GW(p)
The major problems at Alcor are truly abysmal management, for which the Alcor Board of Directors is to blame, and lack of a professional culture and staff to administer the front end of cryopreservation. The situation is almost identical to one that would exist if the board of directors of a hospital tried to deliver medical services without physicians and nurses, but rather hired "the best they could find" to do these professionals' jobs. Thus, there might be a veterinarian doing cardiac and neurosurgery, a chemist operating the heart lung machine, and so on. The absence of credentials, per se, is not the core issue here, because it is perfectly possible for such individuals to do these tasks and to do them "reasonably" well.
Because cryonics did not become a mainstream medical, industrial, or business activity, it necessarily is in the realm of very small "visionary enterprises," like the early days of flight or radio, or perhaps in the realm of the dedicated (professional) amateurs. A good example of the latter is amateur astronomy, where the people involved are fantastic - mostly level headed, focused, responsible and astonishingly capable. Amateur astronomers have made more brass tacks basic discoverers of heavenly bodies than their professional counterparts, and they have made major contributions to the fundamental science, as well. There are essentially no kooks, and their equipment and facilities are often spectacular and demonstrate fabulous innovation and engineering skill.
The barnstormers at the start of flight were "crazy," extreme personalities, but the fact that they had to fly and thus had to work with real machines which could CRASH and KILL them, kept them on track. However, a careful observer of their history will note that their mortality rate was terribly high. Those that survived barnstorming and doing air mail runs were, in effect, a "filtered product" who represented the best of practical skills, engineering ability, risk taking, and bad-ass courage. In that respect, Lindbergh and Fred Chamberlain had personalities that were extraordinarily similar.
I've had considerable contact with HAM radio clubs and amateur astronomers and there is simply no comparison to cryonicists. Ditto for the pioneering ultralight aircraft guys of 25 years ago. If you spend any time around these kinds of groups, you quickly see that they attract as many dysfunctional, narcissistic personalities, as does cryonics, but 99.9% of the time these people flake away, almost instantly. In the HAM groups it happens during the run up to getting your basic license. It doesn't matter how much physics you know, or how smart you are, most of the test is FCC regulations, proper jargon, and things that you must memorize. The loonies flee!
Having said that, it's been interesting to watch the quality of amateur radio enthusiasts plummet in recent years. This is because the equipment is now all solid state, it is much less expensive, and the days of building you own radios from parts are over. Also, the requirement for Morse code was dropped from the entry level licensing exam.
If you, or I, or anyone else looked at a TV set, or an MP3 player, or even a modern HAM radio and said, "I'm going to build one of those; I can do it just as well as Samsung and much less expensively," we'd likely all just laugh and figure the poor guy was crazy. Nobody tries to do that because it is stupid, just like no one in their right mind says, "My wife needs open heart surgery and those bastards at the Medical Center want $50K to do it! That's ridiculous, I've seen it done on TV and my brother in law is a veterinarian, so we're going to do it ourselves." The hubris required to take such an action, let alone the lack of commonsense, is just indescribable.
Now, if your wife needs surgery, you cannot possibly find a doctor to do it, and you think you can learn the craft well enough to give her fighting chance, well that's another matter - depending upon how you go at it! If you have 5-6 years to prepare, you're willing to do the work and you're willing to kill a LOT of dogs, you can indeed teach yourself the basics and perhaps have a 25% chance of pulling it off - providing it is a SIMPLE surgical procedure that she needs. You can actually do this from books, journals and lots of failed attempts in the "dog lab." When I was kid in the late 1960s, several teens a little older than me (15-16 years old) actually set up and did do cardiac surgery in their garages on dogs, and the animals survived! They built their own heart lung machines (HLMs). Today, such an action would be illegal and it is impossible to imagine teenagers building their own heart lung machines! But, in fact, this really happened.
The first practical HLM was built by the maverick surgeon C. Walton Lillehei, and a colleague, Richard Dewall . Lillihei was the archetype of the founder of almost any daring new profession (in this case, cardiac surgery): he was brilliant, courageous - just an incredible man. He started doing open heart surgery BEFORE the HLM by using another human being as the HLM in a technique called "cross circulation." He'd hook up a volunteer to the patient and use the volunteer's heart and lungs to support the patient while he operated. This was brutally controversial at the time and, of course, eventually one of the volunteers died due to a technical error in the OR! It was almost the end of Lillehei, and he barely escaped criminal prosecution. I mention Lillehei because his first HLM was built from a commercial "finger" tubing pump, with the oxygenator made from PVC beer tubing, a cheap glass frit, some stainless steel pot scratcher pads, and other odds and ends. Their total cost, excluding the pumps, was ~ $15.00: http://i293.photobucket.com/albums/mm55/mikedarwin1967/m8jpg.jpg
{kind=link}
It worked brilliantly and was the design template for every HLM up until bubble oxygenators were replaced by membranes in the late 1980s. Now, if you look at the machine in that picture, it is something that anyone with a modicum of hand-skills could build. The pumps were standard, off the shelf industrial finger-pumps used in the food processing industry. So, a kid with some bucks really could build his own HLM - in fact, he could do it today. The difference is, as I previously pointed out, is that he'd be hauled off to jail if he tried to use it. And if you can't use it, why build it?
However, if you really want to master (simple) basic cardiac surgery, it will cost you a fortune in time, equipment, animals and supplies. The only way such a situation would make sense is if you were in a world where there were lots of doctors, medical supplies, equipment and so on, but you and your wife were banned from access to them. Your money wasn't any good and you had to "operate underground," literally. That's the situation cryonics was in and still is in, to a great degree.
The critical difference is that there is today in cryonics no perceived need to "get it right" with animals, or any other feedback-driven test system. It's like the guy I describe above who just decides he and vet brother in law will show up in the garage one day with whatever their idea of what is needed is, and they'll simply operate on his wife! But wait, what happens if they do that? Well, pretty clearly it will be a HORRIBLE MESS, not only will the wife die, but it will be a gruesome fuck up - just unimaginably bad - worse than if she were murdered with an ax. Then what happens? Well, they go to jail, there will be a huge outcry, it will be front page news. In short, they will get subjected to the CONSEQUENCES of their stupid and irresponsible acts.
However, if you are "freezing" your wife, well, who knows how it turned out? Who cares? She looks great! You feel real good about it! And if she does thaw out and rot, well, she was dead anyway, right? So, no harm and no foul. Certainly there are no social or legal consequences for any errors, oversights or failures. There isn't even any way to KNOW that such things might have (or indeed did happen).
THAT IS CRYONICS.
And when good quality people do come along, or people who sincerely want to put their money into cryonics, there is always some damned fool who will tell them how easy it is, how much more quickly THEY will show them results, and on and on and on. If you were doing anything else; running a dog food company, or making women's' handbags, you couldn't get away with that, because the product wouldn't sell and you might even be in court for killing peoples' pets with tainted food. But, not so with cryonics...
Cryonics came reasonably close to crossing the threshold into professionalism with Alcor in the 1980s, but that effort imploded. Jerry Leaf was cryopreserved and I left to pursue more conventional biomedical research (a terrible mistake, in hindsight). Absent a well defined and well established culture of professionalism that included self-correcting feedback mechanisms, Alcor fell back to become something broadly similar to CI. Instead of functioning as a hospital board of directors does, Alcor's Directors became de facto managers - arbiters of the technical details of care, by default. This has been a disaster, not only for those receiving such care, but because Alcor (much more than CI) now serves as a spolier to professionalism. The high tech veneer and the appearance of biomedical competence short circuit any perception that something is seriously wrong, and that things were once, and could again be, much better.
Replies from: bgwowk↑ comment by bgwowk · 2012-04-11T20:19:04.844Z · LW(p) · GW(p)
Mike, let's be fair about this. Veterinary surgeons for thoracic surgery (after loss of Jerry Leaf) and chemists for running perfusion machines were also used during your tenure managing biomedical affairs at Alcor two decades ago. You trained and utilized lay people to do all kinds procedures that would ordinarily be done by medical or paramedical professionals, including establishing airways, mechanical circulation, and I.V. administration of fluids and medications. Manuals provided to lay students even included directions for doing femoral cutdown surgery.
http://www.alcor.org/Library/html/1990manual.html
The good cases that you were able to do with lay help (and being only a dialysis technician by credential yourself) are the stuff of cryonics legend. That was how cryonics was done back then. With the resources that were available then, and the need to provide cryonics response over vast geographic areas, using trained lay cryonicists was the most effective way to deliver cryonics care for many years. Some history of this is discussed here
http://www.alcor.org/Library/html/professionals.html
In the 2000s Alcor began to supplement trained lay cryonicist teams by deploying a staff paramedic to cases whenever possible. In the 2010s, Alcor began using Suspended Animation, Inc., more extensively. As announced here,
http://www.alcor.org/blog/?p=2174
Alcor policy is now to use Suspended Animation, Inc.., (SA) for all cases in the continental U.S. outside of Arizona which SA can reach in time. Local trained lay teams are now only used as first responders, bridging time between notification of emergencies and arrival of SA.
The significance of this is that SA now uses board certified cardiovascular surgeons and certified clinical perfusionists on almost all cases. I've met two of SA's contract cardiovascular surgeons, one of whom trained under Michael DeBakey. These are top-rank professionals who go out on cryonics standbys, and get cryonics patients on cardiopulmonary bypass faster than ever before in cryonics. They established fem-fem bypass on one patient last year in only 15 minutes.
http://www.alcor.org/blog/?p=2175
Another patient was placed on bypass only 7 minutes after arrival in SA's vehicle using emergency median sternotomy, never before done in cryonics.
http://www.alcor.org/blog/?p=2267
These are professional surgeons and perfusionists who do median sternotomies and cannulations so fast that in their day jobs they actually save patients who suffer cardiac arrest from fixable causes (e.g. "fatal" DVTs). This is now the level of care available under ideal circumstances in cryonics.
In Alcor's O.R., Alcor is presently evaluating and training two board certified general surgeons to supplement the veterinary surgeon and neurosurgeon who have been used by Alcor for the past 15 years. Alcor has transitioned toward utilization of professionals whenever possible or practical. There are now more medical professionals doing the work of cryonics than ever before in the history of cryonics; not just scientists and technicians, but actual clinicians.
You are also mistaken, at least partially, about utilization of animal models in training. Even though professional surgeons and perfusionists already have extensive and ongoing clinical experience, SA uses a porcine model to train its contract surgeons, perfusionists, and other personnel in the specific procedures of cryonics.
There are shortcomings to this model. Contract clinicians are extremely skilled at specific procedures that must be done, but they are not cryonicists. For example, they don't understand cerebral ischemic injury, its mechanisms, and significance in the context of cryonics. This can hypothetically lead to difficulties understanding and managing cases with moderate periods of warm ischemia that would ordinarily be "written off" in conventional medicine. Cryonicist involvement is still essential. However on balance, as measured by the speed and competent handling of standbys and transports in which they have been involved, participation of cardiovascular surgeons and perfusionists has been very positive. I hope we can continue to afford it.
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-12T04:51:45.493Z · LW(p) · GW(p)
Brian, when you say: "Mike, let's be fair about this. Veterinary surgeons for thoracic surgery (after loss of Jerry Leaf) and chemists for running perfusion machines were also used during your tenure managing biomedical affairs at Alcor two decades ago. You trained and utilized lay people to do all kinds procedures that would ordinarily be done by medical or paramedical professionals, including establishing airways, mechanical circulation, and I.V. administration of fluids and medications. Manuals provided to lay students even included directions for doing femoral cutdown surgery," you are either not reading what I wrote or are not being fair yourself. I not only acknowledge that this was so, I go so far as to say it is completely acceptable with the caveat that such people are instructed, vetted and mentored properly. I'll go even further (as I have repeatedly, elsewhere) and state that the most highly qualified medical personnel can be dangerous, or even worse than useless unless they have been trained and mentored in human cryopreservation as a specialty. There's nothing remarkable about this; no reasonable person would want a psychiatrist or a dermatologist doing bowel or brain surgery.
Some of the same people who performed very well in the past, and who are not medically qualified, are still at Alcor. The individual people, per se (in this instance), are not the problem. Rather, it's the absence of the paradigm of cryonics as a professional medical undertaking that's missing. The evidence for that is present in Alcor's own case histories where highly qualified medical personnel do things like discontinue cardiopulmonary support on still warm patients in order to open their chests for cannulation (http://alcor.org/Library/pdfs/casereportA2435.pdf) or drill burr holes without irrigating the drilling site with chilled fluid to prevent regional heating of the brain under the burr. We are in complete agreement on these issues, as far as I can tell. Where we apparently differ is on how to resolve them.
The most interesting thing to me about this post from Brian is information it communicates for the first time. I follow Alcor's announcements, read its magazine and track its public blog, as I necessarily must, so I am surprised to learn that "In Alcor's O.R., Alcor is presently evaluating and training two board certified general surgeons to supplement the veterinary surgeon and neurosurgeon who have been used by Alcor for the past 15 years." This is the kind of information that I would expect to see showcased in the organization's literature and on its website, not disclosed here. This is the kind of thing that happens over and over and which degrades member confidence in the transparency of the organization. The next question is, who what, where and how? What are the details of this training? What kind of model is being used? What are the results to date?
Yes, SA does use pigs for training, but they use them in a non-survival mode - they get no robust feedback about errors, and no new insights. In fact, Brian might have mentioned that Alcor has used both animals and human cadavers in this manner, but I think he understood that the point I was making was about vetting your skills in an outcome driven fashion. That is not being done.
What's even more disturbing is that there is virtually no visibility into the outcome from even these training operations. SA and Alcor are both essentially black boxes - there is no data, no performance reports, not even any reports or internal scoring of how well simulated cases proceeded. There's at least one reason for this, and that is that there is no scoring system, internal or external. When things go wrong, well, it's oops, we shouldn't do that next time. And if that isn't the case, then I'd love to hear it and I want to see the data to document it. That is an eminently reasonable request.
It's great that Alcor can sometimes mount skilled perfusionists and highly skilled emergency vascular surgeons. But that isn't the issue. The issue is the framework of knowledge, understanding and consistent performance that is absent. A surgeon or a perfusionist are, absent mentoring (internship), TOOLS to be used by and within that framework. If a man tells me he has the best glass cutting tool money can buy, but he doesn't know how to cut glass, well, I'm going to be underwhelmed.
Alcor patient case reports are disorganized, inconsistent and erratic narratives that make objective evaluation impossible. No great genius is required to consistently collect and organize the key data that define how well a case went - or didn't. The first cryonics case report was done by a 17 year old and a 22 year old graduate student:
http://www.lifepact.com/images/MTRV3N1.pdf
Examples of competently executed cases and case reports are available on Alcor's own web site and the data captured, reduced and presented in these case reports was achieved using a tiny fraction of the financial and personnel resources Alcor currently has available:
http://www.alcor.org/Library/html/casereport8511.html
http://alcor.org/Library/html/fried.html
http://alcor.org/Library/html/casereportC2150.htm
http://alcor.org/Library/html/casereport8504.html
LOOK AT THESE CARE REPORTS CAREFULLY and then look at those on the Alcor website from 1997 forward: http://www.alcor.org/Library/index.html#casereports
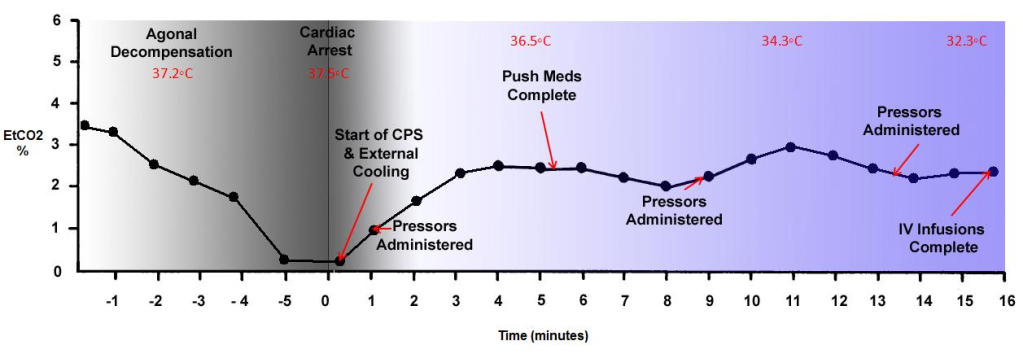
I'm not trying to be contrary, difficult, or unreasonable. What I am asking for is core competence, not perfection. There is nothing either exotic or impossible in that. For example, Alcor has a Novametrix CO2SMO capnograph and respiratory function analyzer. The device can effortlessly capture and write to disk over 60 different respiratory parameters and it measures the end-tidal expired carbon dioxide (EtCO2) in the patient's breath. The EtCO2 is the gold standard for determining how effective cardiopulmonary support (CPS) is. And if CPS is not effective, than that is both additional ischemic time the patient is experiencing and it is an opportunity to intervene and fix the situation. Or at worst, it offers the possibility of learning what caused inadequate CPS so that it might be avoided next time. The only skill required to use the device is to put the walnut sized sensor in line between the patient's airway and the ventilator on the LUCAS CPR machine: http://frankshospitalworkshop.com/equipment/documents/pulse_oximeter/user_manuals/Novametrix_8100_-_User_manual.pdf That should make it easily possible to produce graphic data like this:
http://i293.photobucket.com/albums/mm55/mikedarwin1967/EtCO2inCPSgraph.png
{kind=link}
THAT kind of data speaks definitively to how that patient was stabilized and transported, and in aggregate it provides a statistical dataset that speaks to the overall performance of the organization. It should be accompanied with graphic data for the patient's TEMPERATURE, mean arterial pressure (until the time of arrest), the SpO2 (pulse ox) and other relevant data. This was done in the past by stressed out, sleep deprived, mostly volunteer people who were trained in-house. If that kind of data collection and accountability are considered "perfectionist," or some kind of golden past no longer to be achieved, then I restate my opinion that something is terribly wrong.
Paramedics are taught that the single most important and most critical indication of the efficacy, or lack thereof, of CPR is the EtCO2 of the patient over time. Where is this data???? This is only one of countless examples I could use - but it is especially relevant because it is simple data to collect, and I know from Alcor's recent case reports that they have a CO2SMO and they are actually using it on patients during the peri-arrest hospice period. Again, where is the data? That data is the ONLY way anyone has to evaluate the quality of cryonics cases because the patients cannot speak to us.
If you want to stop my criticisms, you need only show me the data and offer me and everyone else the opportunity to be reasonably certain it is valid and representative.
Replies from: bgwowk, maxmore, grendelkhan↑ comment by bgwowk · 2012-04-12T17:10:54.900Z · LW(p) · GW(p)
Your points are mostly well-taken, Mike. Not everything is better than it used to be. While the basic cryopreservation technology (vitrification) is better, and some important aspects of service delivery are better, Alcor does not have in-house expertise comparable to the era of you and Jerry Leaf. With the benefit of hindsight, I would say that people of such caliber willing to devote their life to cryonics are a historical anomaly not amenable to formulaic replication.
With respect to communications, the two new potential O.R. surgeons I spoke of were not a public announcement being withheld because Alcor is opaque and untrustworthy. Contact was made with them only within the past few weeks, as discussed at a recent public board meeting. I mentioned them only because your message seemed to imply that Alcor was content with the status quo.
I confess that you have a knack for twisting the knife of public criticism in ways that prompt me to "announce" things that aren't ripe for announcement, and that lead to more questions and criticism. When will I learn? :)
↑ comment by maxmore · 2012-04-12T17:59:20.515Z · LW(p) · GW(p)
"I follow Alcor's announcements, read its magazine and track its public blog, as I necessarily must, so I am surprised to learn that "In Alcor's O.R., Alcor is presently evaluating and training two board certified general surgeons to supplement the veterinary surgeon and neurosurgeon who have been used by Alcor for the past 15 years." This is the kind of information that I would expect to see showcased in the organization's literature and on its website, not disclosed here. This is the kind of thing that happens over and over and which degrades member confidence in the transparency of the organization. "
In fact, I did mention the new surgeons, briefly, in an Alcor News post on April 2: http://www.alcor.org/blog/?p=2518 And similarly in the issue of Cryonics magazine now in production. Since we are just starting to work with these surgeons, it didn't yet seem appropriate to report much more. We are continually reporting on just about everything. Your attempt to cast Alcor as non-transparent should be obviously false to anyone who looks at what we communicate.
↑ comment by grendelkhan · 2013-10-17T22:27:00.032Z · LW(p) · GW(p)
I think I'm missing something here. As I understand it, you (Mike Darwin) have a great deal of experience and expertise in the actual practice of cryonics, as well as a lot of actionable recommendations. The current staff at Alcor (e.g., Max More) seem to take you seriously.
Is it a silly question to ask why you're not working for Alcor?
Replies from: None↑ comment by curiousepic · 2012-04-09T14:31:14.732Z · LW(p) · GW(p)
Could you briefly explain or point to anything about info how CI's approach is flawed?
EDIT: This comment helped: http://lesswrong.com/r/discussion/lw/bk6/alcor_vs_cryonics_institute/6a2c
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-11T09:18:02.788Z · LW(p) · GW(p)
No, and that's the trouble! Because, you see, if cryonics were like any other medical procedure, I'd simply point to the STATISTICS and to the MAIMED and DEAD patients. In fact, the errors and screw ups would be a huge public scandal, because people would have SUFFERED and DIED. Indeed, the patients themselves (who were not killed outright) would be hollering to high heaven via every available media outlet. Cryonics patients never complain because they can't.
Because no cryonics patient suffers, or dies, or experiences any other OUTCOME of any kind, your only choice, if you want to understand differences in procedures, quality of care, and so on, is to delve into the complex, technical specifics.
You don't have to learn the details of automotive engineering, metallurgy, and so on, to go pick out a good automobile. All of that huge body of technical and scientific knowledge is effectively INVISIBLE to you as a consumer (as well it should be) because you can look at PERFORMANCE as your guide to making a good buy. All that science and engineering gets reduced to miles per liter, road reliability and, of course, your comfort, convenience and safety while driving it! So "close" are the performance specs between automobiles that a significant part of what makes therm sell and out-compete each other is styling - just how the damn thing looks!
Think about that.
↑ comment by cath · 2012-04-30T05:53:12.910Z · LW(p) · GW(p)
Perhaps Alcor should do the perfusions and freezing and CI chug away at the storage which needs safety and stability. About Mike's or anyone's judgment for that matter, it is a commonplace that no one person has good judgment in all areas. Alcor's judgment in selection of personnel may be comparatively poor, but on the other hand I note few comments of a scientific or technical nature on his technical arguments, and as my own knowledge is rusty, I crave input from someone other than Mike of an exact nature, and not the dismissive "often fool people into believing that his judgment is better than it is" type of comment. I'm not fooled by any of this, but sorely lacking in the means to exercise my own intellect on the critical area of perfusion technology and I am becoming concerned that Mike's technical postings are ignored in substance and detail because of a general lack of technical and scientific know-how in both organizations. At some point in the future if research on reanimation continues to be at or near zero BOTH organizations will be storing people whose information loss is approaching an upper asymptote of 100% regardless of the technology used to get them into the capsules in the first place.
↑ comment by mikedarwin · 2012-04-11T20:43:43.928Z · LW(p) · GW(p)
This post from Max More is the kind of post that I would expect to see voted off of LessWrong. I have not had a substantive conversation with Max More about cryonics, let alone my personal position, psychology, desires or motivations in over 20 years. We did correspond recently, and I have asked Max for permission to make that complete correspondence, minus personal incidentals not material to cryonics, public. He has flatly refused. Why, I do not know, but I do know that that is the only substantive communication he and I have had in decades and that it is completely documented in writing. Prior to that, at least to my knowledge, our relationship was cordial and not marred by any disagreements or conflicts. Nor do we have any confidants or intimates in common. Thus, the question arises, how would Max know anything about whether I am "envious that I'm not running things"? As he says, he doesn't know this, he can only speculate because he has refused to speak with me on these matters.
He then goes on to say something that I find remarkable to be left unchallenged here on LessWrong:
"That depth (of knowledge) and his most excellent writing skills often fool people into believing that his judgment is better than it is"
LessWrong, as I understand it, is a forum where people are mastering the craft and science of evaluating the logic and substance of the arguments put forth by people, including thinkers and writers here and elsewhere - not based on their style, cleverness of articulation, or their speculations. If anyone has questions about the assertions I make, feel free to ask for the evidence. We may not always agree on how to weight it, but the evidence will (hopefully) always be there, and it will be credible. Where I overstep or make a mistake, you will find me quick to acknowledge and apologize.
Replies from: gwern↑ comment by gwern · 2012-04-11T20:57:17.172Z · LW(p) · GW(p)
http://chronopause.com/index.php/2011/08/09/fucked/ and sequels have cost you more than one LWer's opinion of your judgment because it matched exactly the sort of doomsaying which has cost contrarians literally billions of dollars over the past 4 years in bad bets against the dollar and US stocks (eg. Peter Thiel's Clarium fund alone, or Dr. Doom for that matter). It's not a surprise if they acknowledge your facts but question your judgment, which is the same sentiment Max is expressing.
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-12T02:39:48.366Z · LW(p) · GW(p)
My comments about economic, social and political matters don't speak to how people should invest in the market, or to who will win the coming election. They speak to the general condition of the economy and the culture over the long haul. As I've observed in print before, plenty of people will get rich, and millions of people have gotten richer, despite the fact that diversion of wealth from the people who primarily produce it is at an all time high. I am the first to acknowledge that it has been fantastic advances in productivity that have made this possible. But that doesn't make the reality go away that the system is increasingly thwarting innovation, overspending its resource base, and appropriating vast amounts of wealth which is used inefficiently, is wasted, or is actually used for contra-productive purposes.
All I have said, in addition to these fairly mundane observations, is that, sooner or later, something's got to give. To some extent this has already happened in that many trillions of dollars of wealth have disappeared, or been reallocated to cover "bad actions" of various kinds. The situation in Europe is actually much worse than it is here, and if it becomes impossible to maintain solvency of large EU nations such Greece, Italy and Spain, then the effect will, again, be felt in the US and elsewhere.
What I have no way of knowing is how much "re-assignable" wealth is present in the system - and just as importantly, if it will be reassigned to cover "bad acts." That' difficult to assess wealth covers a huge range of goods and actions, from the quality of food people eat, to whether they use paper towels or go back to using rags! I've never claimed any special insight in those matters, and for good reason; because the data to make those kinds of "forecasts" simply isn't available.
So, my position is very much like that of someone who warns that "crime doesn't pay." It doesn't - not in the long run, because it is destructive of productivity, and destructive of effective human social interaction. But the BIG question is, what exactly constitutes the "long run?" That's not a joke, and I am mindful that the Soviet Union ground on for 70 years. That's an economist's eternity, and then some. Pepsi Cola made millions betting that Soviet Russia would continue for decades. Do I think Fidelista Cuba is doomed? Absolutely. I also think it is a miserable, oppressive place. But I wouldn't care to give any odds on how long it will survive.
Finally, if all the "non-contrarians" on this matter are concerned with or about is financial gain, regardless of the system's characteristics or "meta-qualities," then I have nothing to say to them and their disappointment in my "judgment" is as understandable as it is mutual.
Replies from: gwern↑ comment by benbest · 2012-04-13T13:18:56.603Z · LW(p) · GW(p)
It is odd that Max would criticize CI for only perfusing the head in light of the fact that the great majority of Alcor patients are neuros (head-only). The head and the brain are the most important part. CI will perfuse the body with glycerol for CI Members who request it, but CI does not do this unless requested. Look at CI's Perfusion Preference document, which all CI Members have the option of completing when making cryopreservation arrangements: http://cryonics.org/documents/Perfusion_Preference.html . When the majority of Alcor Members opt for neuro, why rag on CI about the fact that the majority of CI Members opt for no body perfusion (or opt by default)?
In any case, vitrification of the body is not possible either at Alcor or CI at present. CI's vitrification solution can eliminate brain ice formation and even demonstrably results in hippocampal slice viability when cooled to -130Celsius and rewarmed, and is vastly less expensive than M22. I doubt that the extra expense of M22 is worth the difference. I do believe that it is important to make cryonics affordable, and I am pleased to be offering a lower cost alternative. Standby/Stabliization/Transport (SST) from Suspended Animation is an optional extra for CI Members, but SST is mandatory for Alcor Members. Only about a quarter of CI Members with cryopreservation arrangements have chosen to have SST from SA (I have chosen that option). I am proud that the comparisons page at CI does not involve a lot of breast-beating, but only contains objective information http://cryonics.org/comparisons.html .
Replies from: maxmore, benbest↑ comment by maxmore · 2012-05-04T05:07:30.616Z · LW(p) · GW(p)
Ben: I wasn't actually criticizing CI for not perfusing the body other than the brain, I was simply pointing it out. CI members in general seem very insistent on the importance of cryopreserving their entire body. Given THAT, it seems important to note that their body will not be cryoprotected. However, thanks for pointing out that CI will do so if requested. How often is that request made?
Why do you say that vitrification of the body is not possible "either at Alcor or CI"? It is done at Alcor for whole body members.
↑ comment by Eli Tyre (elityre) · 2019-09-12T10:02:44.910Z · LW(p) · GW(p)
CI uses a less advanced (and cheaper) cryoprotectant but cryoprotects ONLY THE HEAD, allowing the rest of the body to be straight frozen with massive damage. That’s especially odd since (many of) CI members are insistent about being whole body patients rather than neuros.
I did not know this. Thanks.
↑ comment by mkmk · 2012-04-16T00:46:08.993Z · LW(p) · GW(p)
I was at CI's AGM when Aschwin and Chana during their talk took the time to trash talk CI at its own conference and I was upset despite maxes assertion otherwise. Fortunately for the de wolfs, the audio at the meeting was substandard and for those of us who heard it there was no chance to challenge these absurd statements. No where was there any attempt to quantify or verify alleged damage. To the best of my knowledge the de wolf's have not been allowed to autopsy and remove brain tissue from CI or Alcor patients to do a scientific comparison. There was also no other attempt to separate out unrelated factors. Which CI patients were they specifically referring too? Were they referring to incomplete case reports cherry picked from both organizations for a comparison? Surely both organizations have had cryosuspensions in which factors outside their control was at play. IE patient not found dead for several hours or days. Are we comparing apples to apples here? This was is far from a scientific comparison and Max and the de wolfs as scientists should be ashamed of making such smoke and mirror un substantiated assertions. The fact remains there is no way aside from defrosting our patients to compare procedures and even then if we are to make a fair comparison then we need to look at optimal cases from both organizations and subtract out factors such as the over priced false sense of security and misrepresentation that is in long distance remote standby. The truth is simple. Speed and early cooling with vitrification supplemented by good planning is worth 100 times a delayed remote standby even if its members paid $500,000 for the process. Lets be honest to potential members. Just because someone here on Lesswrong says CI or Alcor has had better cryosuspensions does not mean it is true to be repeated over and over. I demand unbiased controlled evidence otherwise these allegations are a cheap shot nothing more.
Replies from: benbest↑ comment by benbest · 2012-04-16T15:28:48.173Z · LW(p) · GW(p)
Last October Aschwin de Wolf replied to misinterpretations of his presentation at the 2011 CI AGM with the following statement which he authorized me to reproduce at that time, and which I will reproduce again here. -- Ben Best
** Aschwin's comments below *
It has come to our attention that our recent presentation has caused some controversy on the CI members mailing list. As far as we can tell, a lot of the criticism is aimed at how other people (including Alcor Officials) have interpreted our presentation. In our presentation there is no comparison between Alcor and CI at all. As a matter of fact, we deliberately avoided framing the issue like this. Our presentation just summarized the practical implications of our research for cryonics. One of the most robust findings in our studies, and scientific papers of others researchers going back to the 1960s, is that cerebral ischemia produces perfusion impairment in the brain in a time- and temperature dependent manner. In cryonics such perfusion impairment translates itself into ice formation. The real difference is not between Alcor and CI but between people who do not receive rapid stabilization and cooling and those who do. In ourpresentation we outlined a number of things CI members can do to reduce warm and cold ischemia, including relocation and ensuring that there will be rapid cooling after pronouncement of legal death. We did not use the phrase "2/3 of CI members" in our slides but we did point out that the majority of CI members experience prolonged periods of warm and cold ischemia - this can be easily verified by checking the case reports on the CI website. Such ischemic delays produce perfusion impairment and ice formation. Most CI members can do something about the probability of this happening to them, so this can hardly be construed as an endorsement of Alcor. As a matter of fact, speaking for myself, I prefer a model where a cryonics organization leaves more flexibility to its members as to whether and how to make arrangements to prevent injury to the brain after pronouncement of legal death. We would never claim that the ischemia that many CI members experience is catastrophic because we do not know what future cell repair technologies will be capable of. Of course, this should not excuse people to limit postmortem damage as much as they can.
Having said all this, this does not mean that research cannot contribute to mitigating some of the effects of prolonged warm and cold ischemia. We made a number of recommendations during our presentation and hope to present a more comprehensive set of technical recommendations to improve CI procedures in the near future. We had constructive exchanges about this with Ben and Andy.
comment by Merkle · 2012-04-09T07:36:12.769Z · LW(p) · GW(p)
General advice: if you can afford it, sign up with Alcor. If you can't, sign up with CI.
If you want more information, I'd recommend the Alcor FAQs.
I should provide some context for my comments on Alcor's previous track record on creating endowments: we had just received a $7M bequest, had placed $3.5M into the Patient Care Trust Fund, and the Board had decided to put the other $3.5M into an Endowment and withdraw only 2% per annum, or about $70,000 per year, for Alcor's operational needs. Some members were feeling quite euphoric and were proposing that we spend some significant amount of the principal on various worthy projects, including reduced dues for said members and increased spending on certain pet projects. It seemed advisable to inject a note of sobriety into the discussion and to somewhat deflate the expanding expectations. While helpful, this bequest did not free us from the constraints of fiscal responsibility, and explaining why the Board was being so parsimonious with this windfall seemed appropriate at the time.
Given this context, I wouldn't interpret these comments as "disturbing".
Replies from: dbaupp, None↑ comment by dbaupp · 2012-04-09T12:04:07.966Z · LW(p) · GW(p)
(For anyone reading this, some context: Merkle is on Alcor's Board of Directors)
↑ comment by [deleted] · 2012-04-09T13:03:55.435Z · LW(p) · GW(p)
the Board had decided to put the other $3.5M into an Endowment and withdraw only 2% per annum, or about $70,000 per year, for Alcor's operational needs.
Have they stuck to this plan, or has the piggy bank been smashed open?
Replies from: maxmore↑ comment by maxmore · 2012-04-09T18:54:41.730Z · LW(p) · GW(p)
Alcor has stuck to this plan. The board takes it very seriously. Not only have we not taken out more than 2% per year, the board have frequently pushed to add more to the Endowment Fund even where it could legitimately be put into operations.
Replies from: wedrifid, None↑ comment by wedrifid · 2012-04-09T21:08:00.341Z · LW(p) · GW(p)
the board have frequently pushed to add more to the Endowment Fund even where it could legitimately be put into operations.
By 'pushed to add' do you mean took actions that actually resulted in adding or that they made a noble effort?
Replies from: maxmorecomment by [deleted] · 2012-04-09T04:41:07.100Z · LW(p) · GW(p)
So with all of that said, besides cost, what factors would lead or have led you to pick one organization over the other?
The cost difference isn't just large in terms of the actual cryopreservation fee. Alcor charges member $800 per year, while CI charges $120. That made the difference for me; I'm currently filling out the paperwork for CI.
comment by James_Miller · 2012-04-09T04:16:37.295Z · LW(p) · GW(p)
Peter Thiel, Ray Kurzweil (I've heard), and Robin Hanson are Alcor members.
Replies from: None↑ comment by [deleted] · 2012-04-09T04:49:24.388Z · LW(p) · GW(p)
Why is this relevant? Presumably they have access to more or less the same information that we do.
Replies from: Nisan, James_Miller, Jayson_Virissimo, army1987↑ comment by Nisan · 2012-04-09T17:13:12.288Z · LW(p) · GW(p)
Peter Thiel might be motivated to exert optimization pressure in the direction of keeping Alcor alive.
Replies from: James_Miller↑ comment by James_Miller · 2012-04-09T18:09:46.329Z · LW(p) · GW(p)
And it's always nice to align your very-long-term interests with those of a brilliant billionaire.
↑ comment by James_Miller · 2012-04-09T05:08:29.549Z · LW(p) · GW(p)
But they might be better at processing information than some of us.
Replies from: None↑ comment by [deleted] · 2012-04-09T05:44:33.515Z · LW(p) · GW(p)
There are no experts in the field of evaluating cryonics corporations, because there are, as of yet, no successful cryonics corporations.
Replies from: ciphergoth↑ comment by Paul Crowley (ciphergoth) · 2012-04-09T08:40:56.982Z · LW(p) · GW(p)
People can vary in how much time, effort, knowledge and intelligence they put into the assessment.
↑ comment by Jayson_Virissimo · 2012-04-09T06:50:59.568Z · LW(p) · GW(p)
Actually, I updated slightly towards Alcor being the best choice for cryonics because of this information, since all 3 are likely more intelligent, rational, and informed than I am.
Replies from: None↑ comment by [deleted] · 2012-04-09T08:31:41.676Z · LW(p) · GW(p)
Surely there are three famous people signed up with CI. Eliezer's one, I suppose. This evidence isn't evidence.
Replies from: Jayson_Virissimo↑ comment by Jayson_Virissimo · 2012-04-09T08:57:59.755Z · LW(p) · GW(p)
If Yudkowsky is signed up with C. I., then that is slight evidence that C. I. is superior to Alcor. This is so not because he is famous, but because he is more intelligent, rational, and informed than I am. Of course, if I actually studied cryonics in-depth, then my new knowledge would screen-off most of the evidential weight of the opinions of these "famous" people.
Replies from: CarlShulman, maxmore, mikedarwin↑ comment by CarlShulman · 2012-04-11T04:26:24.185Z · LW(p) · GW(p)
As far as I can tell, Eliezer picked C.I. to minimize the cost of signaling his views about cryonics, not because he thought it was better than Alcor. See this comment.
See the comment below: My primary reason for signing up for cryonics was because I got sick of the awkwardness, in important conversations, of trying to explain why cryonics was a good idea but I wasn't signed up for cryonics.
↑ comment by maxmore · 2012-04-09T09:14:45.253Z · LW(p) · GW(p)
Consider that it might actually be evidence for a different conclusion: Eliezer signed up for cryonics some years ago, when he had little income, bravely foregoing well-paid employment in favor of pursuing his core goals. (I can relate to that!) I would very much like to talk to E.Y. about whether it's time to reconsider his past decision based on current information and current finances. I'm just an email or a phone call away, Eli...
Replies from: gwern, army1987, Eliezer_Yudkowsky, Jayson_Virissimo↑ comment by gwern · 2012-04-09T14:10:11.762Z · LW(p) · GW(p)
Consider that it might actually be evidence for a different conclusion
I'd express it this way: by conservation of evidence, Eliezer signing up for CI is evidence for CI and against Alcor. Within the set of reasons/scenarios which lead to him signing up for CI, the observation about when Eliezer signed up is evidence for the 'economizing' explanation in which his signing up is not evidence for CI over Alcor.
(This may sound contradictory, but the important thing is that A as a set can be shrinking in total probability even as individual members of A become more likely.
An example of this would be the hope function: if you're searching drawers one at a time for a letter, each time you search a drawer, you expect more strongly that the next drawer will hold the letter, even as you also expect more strongly that the letter is not in your desk at all.)
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-11T20:46:37.671Z · LW(p) · GW(p)
Umm, here's a suggestion: WHY DON"T YOU JUST ASK ELIZER HOW AND WHY HE MADE THE DECISION? Why speculate?
Replies from: gwern↑ comment by A1987dM (army1987) · 2012-04-10T00:04:28.878Z · LW(p) · GW(p)
Someone did ask EY whether the fact that he signed up with CI whereas Hanson signed up with Alcor meant he disagreed with him about something important about the two institutes, and IIRC he answered it was just that Hanson was richer and older than him so of course he'd chosen the higher-end option. (I cannot find that comment, since even a search for Eliezer CI Hanson Alcor in the internal LW search engine turns up umpteen pages.)
↑ comment by Eliezer Yudkowsky (Eliezer_Yudkowsky) · 2012-04-18T02:46:39.938Z · LW(p) · GW(p)
Indeed, I'm young and not yet rich. If I was rich, though, given my prior state of knowledge I would've gone with SA + CI on the belief that CI seemed more long-run stable - CI seems more risk-averse and more financially prudent. I've updated somewhat on the financial prudence of Alcor as a result of reading these threads, and if the decision suddenly mattered for some reason, I would now require more investigation to figure out whether SA + CI or Alcor was the better long-run bet.
Replies from: maxmore↑ comment by maxmore · 2012-05-04T05:27:42.541Z · LW(p) · GW(p)
Depends what you mean by risk-averse. Alcor has an unquestionable history of fighting for its members' wishes, rather than giving up on them at the mere hint of a legal battle. The only way in which CI could be said to be more financially prudent (but in a way with its own costs) is in its remarkable ability to hold down operating costs. I'm working hard on reducing our costs without undesirable penalties in terms of capabilities. I think we are also now at a point where further membership growth will yield significant economies of scale.
But take a look at both organizations' financial statements. You will see that CI expects to maintain patients indefinitely -- and revive them -- on a small amount of per-patient funding. That takes some heroic and highly risky assumptions to accept. Alcor has carefully structured institutions and policies to manage sustainably for the long-term, including strict limits on what can be charged to the patient care trust fund, a 2% draw on the Endowment Fund, and an investment policy that has been giving us gains (while CI has been losing on its investments). If you continue to delve into the gory details, I think you may continue to update your views further.
↑ comment by Jayson_Virissimo · 2012-04-09T09:21:30.859Z · LW(p) · GW(p)
Yes, many (almost all) events are evidence for more than one hypothesis.
↑ comment by mikedarwin · 2012-04-11T20:25:58.069Z · LW(p) · GW(p)
The first question you need to ask Yudkowsky (and yourself) is a damned difficult one to answer "simply," and that is what are the currently well known, well understood, and well documented BIOLOGICAL differences in outcome that are likely to pertain using the two different approaches in the reasonably optimum case. Reasonably optimum means that the member is experiencing medico-legal death under controlled conditions with competent cryonics organization personnel in attendance, My bet is that only a few people on the planet can answer that question, and that Yudkowsky isn't one of them.
Of course, if you do not believe the degree of molecular, histological or gross damage to the patient matters, within broad limits, then such differences are immaterial. For instance, if you think that several hours of warm ischemic injury, followed by 12 to 24 hours of cold ischemic injury, followed by reperfusion injury, followed by grossly inadequate cryoprotective perfusion/equilibration in the brain resulting in large areas of massively ice injured brain tissue will be easily repairable with Nanotechnology, then you will be largely insensitive to the differences between Ci and Alcor, or a well done cryoprotective perfusion and a poorly done one.
My question for such people is, "Why bother with perfusion at all? The ischemic delays are very damaging. Why not just have yourself packed in dry ice as soon as you are pronounced and get shipped off to CI? It would be about $10K to $15 cheaper and you'd only be faced with Nano-repair of cryoinjury?" No need for Nano, Nano, one Nano will do.
I'm in the final stages of preparing Part 3 of THE EFFECTS OF CRYOPRESERVATION ON THE CAT for publication on Chronosophere. Part 3 is the transmission electron microscopy of the tissues under different conditions of cryopreservation (Part 2 was the histology: http://chronopause.com/index.php/2012/02/14/the-effects-of-cryopreservation-on-the-cat-part-2/). You can look at those pictures of cell and tissue structure and decide for yourself which condition you'd rather be in.
Replies from: Eliezer_Yudkowsky↑ comment by Eliezer Yudkowsky (Eliezer_Yudkowsky) · 2012-04-18T02:43:39.903Z · LW(p) · GW(p)
I realize I'm probably going to lose some points with you by stating this. But assuming the limit of perfect technology and the absolute correctness of the pattern theory of identity - if you can't accept these hypotheses, please just say so, instead of answering based on a different hypothesis - is there any definitive rejection of my admittedly naive notion that if you can literally read out every single atomic position, then "Chop off the head with a guillotine and drop it into a bucket of liquid nitrogen" should, yes, just work? I admit that my actual belief and assumption is that current cryonics efforts are massive overkill by people who don't realize that liquid nitrogen is not a secure encryption method for brains.
Replies from: Random832, MixedNuts, JulianMorrison, Mitchell_Porter, thomblake↑ comment by MixedNuts · 2012-04-20T16:22:57.535Z · LW(p) · GW(p)
Can you refine what you mean by "the limit of perfect technology"? If you expect atomic tweezers, you're probably right. If you expect superpowered but still annoying analogues of current methods for manipulating individual atoms, you're probably wrong. Nanotech is surprisingly hard - it looks less like surgery with a knife you made with a rock and more like using the rock to pound on the knife's handle during surgery. (But I'm an amateur.)
↑ comment by JulianMorrison · 2012-04-20T12:10:06.718Z · LW(p) · GW(p)
You lose whatever information is no longer in the atoms, which might be a lot because the skull is not designed to assist cooling, and the brain is a considerable thermal mass. It's going to cool slowly, be shredded to mush by crystal formation, and be warped and cracked by thermal stress, while undergoing runaway chemical reactions and cell death. Your "limit of perfect technology" is then faced with an awe inspiring task of running the reaction products backwards, modelling and reversing the thermal damage, un-killing the cells, and splicing the cracks, in 3D on tissue that does not come with alignment hints, and then inferring a mind. There's going to be some level of physically unavoidable data loss even in the perfect case, the data is entailed in thermal noise and random photons and the damage is no longer reversible without reversing the universe. Presumably the perfect technology will paper over these cracks by copying in mind structures from Mr Perfectly Average. But the end result would be that you're less you.
↑ comment by Mitchell_Porter · 2012-04-30T09:13:06.693Z · LW(p) · GW(p)
I am a cryoskeptic because I don't believe the pattern theory of identity, but in any case, it seems that this is a rather important issue for people who do, and who are seeking cryonic suspenstion. This thread (and Mike Darwin's blog) are full of detailed histories and analysis about numerous aspects of cryonics. But I don't see an analysis anywhere of how the organizations rate, when evaluated specifically from the perspective that atomic-scale mapping and reconstruction/simulation of the suspended brain will become possible, and that this is enough for personal survival. If we assume this to be true, and if we put aside considerations about the relative ability of cryonics organizations to keep their patients frozen - just focusing on the specific suspension procedures that they apply - how do they rate? Are any of them "not good enough", even by these assumptions? Or do they all get a pass?
↑ comment by thomblake · 2012-04-18T17:00:22.963Z · LW(p) · GW(p)
is there any definitive rejection of my admittedly naive notion that if you can literally read out every single atomic position, then "Chop off the head with a guillotine and drop it into a bucket of liquid nitrogen" should, yes, just work?
Logically, it's possible that there is dynamic information not conveyed by "every single atomic position" that is lost when making a static copy. One could imagine that a recording of the positions over some amount of time would do better.
Admittedly, our current understanding of physics might already rule out this possibility without my knowing.
Replies from: khafra↑ comment by khafra · 2012-04-20T17:12:32.680Z · LW(p) · GW(p)
I've wondered, before, whether there's any way to get yearly MRI, eeg, fMRI, etc. recordings on durable media for future preservation with your corpsicle. I couldn't afford it, but it seems like it could be useful.
Replies from: TheOtherDave↑ comment by TheOtherDave · 2012-04-20T17:22:59.752Z · LW(p) · GW(p)
There are also more esoteric uses for regular baselines of that sort of thing. They come in handy while recovering from brain damage, for example.
↑ comment by A1987dM (army1987) · 2012-04-09T23:56:28.692Z · LW(p) · GW(p)
And they've also got much more money, for that matter.
comment by ahartell · 2012-04-09T03:44:22.511Z · LW(p) · GW(p)
I'm thinking Cryonics Institute at the moment but I haven't done too much research yet. The main factors are that CI will be much closer to my next area of residence and that from what I have read both seem to provide basically the same service (except I think with CI you might need to get Suspended Animation to move your body).
EDIT: It looks like Alcor uses a better cryoprotectant and that many CI clients are damaged before being transferred to their facilities (I'm unsure if this is the case for those who contract with Suspended Animation).
EDIT 2: After reading this, I'm not sure how I feel about CI.
Replies from: benbest, benbest↑ comment by benbest · 2012-04-13T21:43:17.329Z · LW(p) · GW(p)
Concerning Mike Darwin's comments about the Curtis Henderson case, I suggest that you read the case report http://cryonics.org/reports/CI95.html There is no incompatibility between DMSO and PEG. The PEG make the solution hyperoncotic as the expected. My big mistake, and it was a bad one, I acknowledge, is that most of the vitrification solution was ruined because I was not aware that PEG would come out of solution when placed in a freezer. The patient was, however, perfused with the remaining solution, and was very well dehydrated as the burr holes indicated. Note particularly the paragraph
"A number of CI Directors have become concerned that I have been modifying the cryoprotectant carrier solutions without adequate testing. The components I have used have been extensively tested in animal experiments and in clinical trials, and I have an extensive collection of peer-reviewed journal articles documenting tests. But none of these articles mention putting PEG into a freezer. In response to concerns by CI Directors (and my own concerns) I will not make more modifications to the carrier solutions, and I believe we should return to using the traditional VM−1 carrier for the time being. I have paid for some research to be done on this by outside researchers. Given the excellent dehydration seen with this patient, I think it would be a mistake to return to an iso-osmotic, non-oncotic carrier solution for the EG solutions. But I am returning to ordinary m-RPS-2 carrier solution for the 70% VM−1. "
My mistake did not have the disastrous consequences implied by Mike Darwin. On the other hand, I acknowledge that it was a mistake, and I have not since made any solution modifications based on literature studies without lab verification by our researchers, Ashwin and Chana de Wolf. I do learn from my mistakes, and I admit this was a bad one that COULD have been serious, and I have resolved that it will not be repeated in the future -- or even risk being repeated. Others may prefer to say that having made such a mistake indicates my character, and will refuse to believe that I regretted my mistake and resolved to do better in the future. I will add that I have attempted to be very forthcoming about this mistake in addition to ensuring that it is not repeated.
Replies from: mikedarwin, mikedarwin↑ comment by mikedarwin · 2012-04-29T23:12:13.695Z · LW(p) · GW(p)
This is a remarkable statement from Ben Best, and one that perhaps speaks best as to why CI is not a cryonics organization being run on a rational, scientific, evidence based basis. When Ben Best writes: "There is no incompatibility between DMSO and PEG. The PEG make the solution hyperoncotic as the expected. My big mistake, and it was a bad one, I acknowledge, is that most of the vitrification solution was ruined because I was not aware that PEG would come out of solution when placed in a freezer.," he is making a statement that has the following outright errors, misunderstandings or distortions in it:
First, DMSO and PEG are incompatible in that they cannot be used either safely or effectively under the conditions required to carry out cryoprotective perfusion in a clinical (or research) setting. The first fact to consider is that DMSO-PEG solutions will often undergo gel formation when cooled to temperatures above freezing if left under refrigeration long enough. This phenomenon has a variable time course and is akin to nucleation and freezing in supercooled solutions - such mixtures may remain clear for days, or undergo precipitation/gel formation within hours of cooling.
Second, the perfusate in question, VM-1 is designed to be administered at a SUBZERO temperature in order to minimize toxicity. The final concentration of cryoprotectants in VM-1, a roughly equal mixture of DMSO and ethylene glycol (the latter is the principal ingredient in automotive antifreeze) is ~ 70%! In the brain tissue slice experiments performed by CI's researcher Dr. Yuri Pichugin who invented VM-1, this very high concentration of agent was not introduced until the temperature of the brain tissue was -20 degrees C! CI's own protocol calls for the introduction of VM-1 at the lowest possible temperature that they can achieve, given that they have no heat exchanger in their patient perfusion circuit. The way CI attempts to get the temperature of the final pass of VM-1 below 0 degrees C, and as close to to -20 degrees C as possible, is by the expedient of placing bottles containing the perfusate into a standard household-type freezer. The pre-chilled bottles of perfusate are then loaded into picnic chests and the perfusate is dispensed from there.
This Mickey Mouse operation rsults in perfusate that is at some (variable) subzero temperature when it is pumped through the perfusion circuit and delivered to the patient.
Refractive Index values only taken during CI−VM−1 perfusion
TIME (AM) TEMP (ºC) Flow rate
(liters/minute) Pressure mm Hg RJVRI LJVRI
1:11 3.2 1.13 127
1:14 3.8 1.06 131
1:20 5.5 1.36 120 1.3976
1:26 7.0 1.07 117 1.3986
1:30 5.6 1.32 103 1.4017 1.4167
1:35 4.9 1.4048
1:37 4.1 1.4258 1.4242
1:40 3.5 1.4043 1.4183
1:45 2.5 1.4137 1.4209
1:47 2.0 1.4153 1.4224
1:50 1.6 1.15 139 1.4207 1.4236
1:52 Upper Body Perfusion Halted
2:00 Lower Body Perfusion Begun
2:00 0.5 0.42 121
2:03 0.5 0.32 136
2:05 0.5 0.32 134
2:10 0.5 0.31 143
2:13 0.5 0.40 200
2:15 0.5 0.46 185
2:20 0.5 0.46 175
2:25 0.5 0.48 191
2:33 0.5 0.48 174
Lower Body Perfusion Halted
Dry Ice Slurry Added to Head
2:37 −2.0
↑ comment by mikedarwin · 2012-04-30T02:13:46.668Z · LW(p) · GW(p)
This is a remarkable statement from Ben Best, and one that perhaps speaks best as to why CI is not a cryonics organization being run on a rational, scientific,or evidence based basis. When Ben Best writes: "There is no incompatibility between DMSO and PEG. The PEG make the solution hyperoncotic as the expected. My big mistake, and it was a bad one, I acknowledge, is that most of the vitrification solution was ruined because I was not aware that PEG would come out of solution when placed in a freezer," he is making a statement that has the following outright errors, misunderstandings or distortions in it:
First, DMSO and PEG are incompatible in that they cannot be used either safely or effectively under the conditions required to carry out cryoprotective perfusion in a clinical (or research) setting AS PRACTICED BY CI. The first fact to consider is that DMSO-PEG solutions will often undergo gel formation when cooled to temperatures above freezing if left under refrigeration long enough. This phenomenon has a variable time course and is akin to nucleation and freezing in supercooled solutions - such mixtures may remain clear for days, or undergo precipitation/gel formation within hours of cooling.
Second, the perfusate in question, VM-1, is designed to be administered at a SUBZERO temperature (-7 degrees C) in order to minimize toxicity. The final concentration of cryoprotectants in VM-1, a roughly equal mixture of DMSO and ethylene glycol (the latter is the principal ingredient in automotive antifreeze) and has a total concentration of these two agents of ~ 70%!
In the brain tissue slice experiments performed by CI's researcher Dr. Yuri Pichugin who invented VM-1, this very high concentration of agent was not introduced until the temperature of the brain tissue was -20 degrees C! CI's own protocol for human cryonics patients calls for the introduction of VM-1 at the lowest possible temperature that they can achieve (~ -7 degrees C), given that they have no heat exchanger in their patient perfusion circuit. The way CI attempts to get the temperature of the final pass of VM-1 below 0 degrees C, and as close to the ideal of -20 degrees C as possible, is by the expedient of placing bottles containing the perfusate into a standard household-type freezer. The pre-chilled bottles of perfusate are then loaded into picnic chests and the perfusate is dispensed from there.
Continued....
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-30T02:16:58.312Z · LW(p) · GW(p)
This Mickey Mouse operation results in perfusate that is at some (variable) subzero temperature when it is pumped through the perfusion circuit and delivered to the patient. While CI case reports are chaotic and inconsistent - some report temperature data during perfusion (http://www.cryonics.org/reports/CI97.html), some do not (http://www.cryonics.org/reports/CI75.html) - it is clear that even with the practice of pre-cooling the VM-1 perfusate in a freezer before perfusing it, CI patients never (so far as I can determine from published case reports, see: http://www.cryonics.org/refs.html#cases) reached subzero temperatures of -7 degrees C throughout VM-1 administration and in fact rarely reach subzero temperatures at all. This despite what CI says in its own description of how its patients are to be perfused with VM-1:
http://www.cryonics.org/research/CI-VM-1.html
"The Cryonics Institute protocol for perfusing the heads (brains) of cryonics patients is a 4-stage stepped open circuit perfusion:
(1) blood washout with carrier solution (4ºC) (2) 10% Ethylene Glycol (4ºC) (3) 30% Ethylene Glycol (4ºC) (4) 70% CI−VM−1 (−7ºC)"
I would also note that in the same document, it is stated that the positive research results achieved with VM-1 in rats were achieved only under these conditions:
*"To test the toxic effects of CI−VM−1 (with or without ice blockers) hippocampal slices were saturated with increasing concentrations of ethylene glycol at 0ºC and −7ºC before cooling to −20ºC for ten minutes of saturation with CI−VM−1 (with or without ice blockers). The DMSO in CI−VM−1 is less toxic at lower temperatures, and is least toxic when introduced at −20ºC. Adding the ethylene glycol first and cooling at 0.3ºC/minute ensured that the solution would not be frozen at −20ºC when the CI−VM−1 (with or without ice blockers) is introduced. The results of the toxicity test were as follows:
86.1% viability +/- 5.8% for 55% concentration CI-VM-1 without ice blockers 89.6% viability +/- 6.2% for 52% concentration CI-VM-1 with ice blockers*
Refractive Index values only taken during CI−VM−1 perfusion
CI Patient 97: http://www.cryonics.org/reports/CI97.htm
TIME (AM) TEMP (ºC) Flow rate(liters/minute) Pressure mm Hg RJVRI LJVRI
1:11 3.2 1.13 127
1:14 3.8 1.06 131
1:20 5.5 1.36 120 1.3976
1:26 7.0 1.07 117 1.3986
1:30 5.6 1.32 103 1.4017 1.4167
1:35 4.9 1.4048
1:37 4.1 1.4258 1.4242
1:40 3.5 1.4043 1.4183
1:45 2.5 1.4137 1.4209
1:47 2.0 1.4153 1.4224
1:50 1.6 1.15 139 1.4207 1.4236
1:52 Upper Body Perfusion Halted
2:00 Lower Body Perfusion Begun
2:00 0.5 0.42 121
2:03 0.5 0.32 136
2:05 0.5 0.32 134
2:10 0.5 0.31 143
2:13 0.5 0.40 200
2:15 0.5 0.46 185
2:20 0.5 0.46 175
2:25 0.5 0.48 191
2:33 0.5 0.48 174
Lower Body Perfusion Halted
Dry Ice Slurry Added to Head
2:37 −2.0
Refractive Index values taken during CI−VM−1 perfusion CI Patient 91: http://www.cryonics.org/reports/CI91.html
TIME (am) TEMP (ºC) RJVRI RBHRI LBHRI
9:35 7.0 1.4084
9:38 5.4 1.3655
9:40 4.2 1.4169
9:42 3.7 1.4198
9:46 2.1 1.4041
9:48 1.7 1.4138
9:50 1.8 1.4194
9:53 1.5 1.3721
9:55 1.1 1.4239
9:57 0.6 1.4206
10:00 0.4 1.3809
10:02 0.4 1.3830
10:07 0.7 1.4229
10:09 0.7 1.4233
10:11 0.6 1.3959
10:15 0.6 1.3971
10:16 0.8 1.4046
Continued....
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-30T02:18:34.432Z · LW(p) · GW(p)
As you can see from the CI data above and below, patient temperatures never come anywhere near -7 degrees, let alone the -20 degrees C called out in either the original animal research, or in CI's own publicly posted protocol for how cryoprotective perfusion is to be administered. In fact, it is necessary to look a number of case reports to even document that CI is perfusing its p atients with VM-1 chilled in a mechanical freezer: "Perfusion with CI−VM−1 vitrification solution began at 3:04 A.M. The CI−VM−1 was at freezer temperature (about −20ºC) in contrast to the ethylene glycol, which was at refrigerator temperature (about 3ºC)" see: http://www.cryonics.org/reports/CI110.html In fact, this patient was one of the very few who achieved any subzero temperature during cryoprotective perfusion with VM-1:
Refractive Index values only taken during CI−VM−1 perfusion CI Patient 110: http://www.cryonics.org/reports/CI110.html
TIME (AM) Nasopharyngeal temperature (ºC) Flow rate(liters/minute) Pressure mm Hg RJVRI
3:07 8.25 1.07 102
3:08 6.9 1.06 101
3:09 5.3 1.07 100 1.3700
3:11 3.6 1.3769
3:16 4.3 1.39 101 1.3670
3:19 2.0 1.37
3:20 0.8 1.00 1.62 1.367
3:20 Perfusion Halted/Surgery
3:30 0.4 0.35 134 1.4166
3:33 −1.4 0.29 135
3:37 −2.6 0.26 120 1.42
3:40 −3.6 0.24 111 1.424
3:41 −1.4 0.29 135
3:43 −3.7 0.26 127 1.42
3:40 −3.0 0.28 126 1.454
3:45 −3.7 0.26 118
3:48 −3.9 0.28 128 1.4346
3:53 −5.3 0.28 125 1.4281
3:57 -5.6 0.27 122 1.4285
4:00 −5.8 0.26 120 1.4296
4:03 −5.8 0.26 117 1.4276
4:05 −5.8 0.26 117 1.4276
4:10 −5.7 0.26 115 1.4284
4:15 −4.6 0.26 114 1.4284
4:20 -3.8 0.26 109 1.4250
4:23 −3.0 0.27 86 1.4181
4:07 −2.3 0.34 82 1.4204
Since it is standard CI operating procedure (and a biological imperative to reduce toxicity) to pre-cool VM-1 in a freezer before use, and since PEG-VM-1 solutions invariably undergo gel formation/precipitation under such conditions, then how is it possible to say, as Ben Best does, "There is no incompatibility between DMSO and PEG"? In fact, there is, because PEG solutions with glycerol or ethylene glycol do NOT undergo this kind of transition - at least they didn't in my laboratory. Even more to the point, Aschwin & Chana deWolf, two researchers who work with CI reported this phenomenon to Best some weeks or months (as I recall) before he decided to conduct this ad hoc experiment on Curtis Henderson. I know this because i was a party to the correspondence.
Continued....
Replies from: mikedarwin↑ comment by mikedarwin · 2012-04-30T02:18:47.363Z · LW(p) · GW(p)
Next up for discussions is the issue of "hyperonconicity." Just as cells require a certain "tonicity" (electrolyte concentration) to maintain their normal volume, tissues with capillaries require a certain concentration (and type) of large (macro-) molecules (colloid) to avoid accumulating water between the cells and becoming swollen, or edematous. Hyperonconicity refers to any solution that has more ability to hold water in the circulatory system (circulating blood or perfusate) than would be the case under NORMAL conditions. The key word there is NORMAL. The macromolecules that comprise colloids can be thought of as molecular sponges that hold water in the capillaries and prevent it from accumulating in between cells as a result of the hydrostatic pressure of perfusion.
This water holding ability is quite complex and nuanced and depends upon the condition of the junctions between the cells in the capillary, the charge of the colloid, the unique chemical properties of the colloid (poorly understood), the configuration of the colloid molecule, and so on.
Onconicity and hyperonconicity are thus in actual practice, relative terms - relative to the condition of the capillary membrane. It is quite possible to have a markedly hyperoncotic perfusate and still have massive edema due to accumulation of water and of the colloid in between the cells! This is so because injured capillary membranes do not behave the same way as healthy or intact ones do - they leak! They leak colloid and with the colloid goes water. Simply cooling the organs (or bodies) of non-hibernating animals results in increased capillary permeability and the leakage of colloid and water into the spaces between cells. There is currently not a complete understanding of why this happens, or why some colloids do not leak as much in the cold as do others. In fact, only a very few species of colloid have been shown to leak less in hypothermia.
Capillary injury and consequent leakage of colloid from ischemia is vastly worse than that induced by hypothermia alone, and no colloid has been identified which is effective at inhibiting this leak, or even reducing it enough in clinical settings to meaningfully change outcome. In the setting of serious ischemic injury in the presence of high concentrations of cryoprotectant, NO COLLOID OR OTHER MOLECULAR SPECIES HAS BEEN SHOWN TO SIGNIFICANTLY REDUCE EDEMA - INCLUDING the PEGs OF VARIOUS MOLECULAR WEIGHTS. CI's own research associates had reported this to CI prior to Ben's decision to do an ad hoc experiment on a human patient with absolutely no prior laboratory animal or even bench testing of the perfusate. The only thing more unconscionable than such an uninformed and reckless action is the continued denial that it was such, and that his "mistake did not have the disastrous consequences implied by Mike Darwin."
Here is what Ben Best says about the outcome for Curtis Henderson in terms of cryoprotective concentration at the end of perfusion:
" The refractive index of the effluent was 1.366 after six liters of VM−1 had been perfused, and was 1.3586 at the end. Intermediate values were as low as 1.3586 and as high as 1.3651, but this was a small range with no trend, and is indicative of random variation. These values are well below the values of 1.416 for 60% VM−1 and 1.4275 for 70% VM−1 — and they showed no trend."
Based on the reported refractive indexes of the venous effluent, I would estimate that Curtis Henderson had approximately 20% to 20% cryoprotectant in his brain - most of which was ethylene glycol. That would (again roughly estimating) equate to about 1.5M to 2.0 M glycerol in terms of colligative cryoprotective effect. I have not yet posted the electron micrographs (EMs) of the damage incurred when 3M glycerol is used as a cryoprotectant in the cat brain, but the histology is posted here: http://wp.me/p1sGcr-lt . I can tell you that the EM's are vastly worse than are the light micrographs.
I have provided a detailed, and I believe accurate, scientific rebuttal to Ben Best's claims. For onto a decade I have privately urged CI to either stop advertising that they are perfusing human patients under conditions which yield 86.1% viability +/- 5.8% (for a 55% concentration CI-VM-1 at - 20 deg C FOR TEN MINUTES, followed by cooling to and rewarming from -130 degrees C at 0.3 degrees C/min) brain tissue viability and ultrastructure, when in reality they are treating patients with 70% VM-1 delivered at +7 (or higher) to -7 deg C (rarely) over far longer periods of time (hours) and in the presence of ischemic insults that typically run to many hours, or even days!
This isn't about elegance of writing, it's about facts, most of which are derived from CI's own website.
↑ comment by benbest · 2012-04-13T21:23:56.447Z · LW(p) · GW(p)
Any funeral director can move your body. Most CI patients are shipped in ice or dry ice by funeral directors. Contracting with Suspended Animation for SST (Standby/Stabilization/Transport) can minimize ischemic damage. Three-quarters of CI Members with contracts and funding for cryopreservation have not opted for SA. Most people do not die unexpectedly, but for those who do neither Alcor nor SA will be of much help in the ischemic damage produced in those cases. SST is not available from Alcor or SA outside of North America, at present.
Replies from: maxmore↑ comment by maxmore · 2012-05-04T05:36:10.007Z · LW(p) · GW(p)
The last statement is not accurate. Currently, with some warning, Alcor WILL deploy people outside of North America. In the near future, we expect to be able to deploy more local responders either instead of or in addition to our own personnel.
comment by the gears to ascension (lahwran) · 2019-02-12T03:49:16.252Z · LW(p) · GW(p)
Any news on this? (hey yall front page comment readers)
comment by Shmi (shminux) · 2012-04-09T02:27:50.346Z · LW(p) · GW(p)
To quote Peter Lynch, "I want to buy a company any fool can run, because eventually one will". Making a company fool-proof is essential when the main purpose of the company is to survive several hundred years (maybe even thousands), an exceedingly rare occurrence. None of the current cryo shops seem anywhere close to having the necessary structure in place.
Replies from: ciphergoth↑ comment by Paul Crowley (ciphergoth) · 2012-04-09T03:42:32.799Z · LW(p) · GW(p)
The post asks a very specific question, which your comment does not help answer.
Replies from: shminux↑ comment by Shmi (shminux) · 2012-04-09T06:58:19.732Z · LW(p) · GW(p)
"neither" is a valid answer...
Replies from: ciphergoth, wedrifid↑ comment by Paul Crowley (ciphergoth) · 2012-04-09T08:37:17.140Z · LW(p) · GW(p)
Every time I posted about cryonics on my journal, I had to put in an addendum to say "WARNING: COMMENTS NOT ABOUT THE SPECIFIC SUBJECT OF THIS POST WILL BE DELETED", otherwise I ended up having all the usual arguments about cryonics in every post I made about it. This post is not here to have all those arguments again, or even the specific argument about whether a good enough firm to sign up with exists. This post is for someone who has decided to sign up to discuss which of two EXISTING firms to sign up with.
comment by Maelin · 2012-04-12T08:35:29.883Z · LW(p) · GW(p)
A while back I decided it was time to stop cryocrastinating, and discovered that CI do not offer any collection services to where I live and seemed to be largely "you're on your own if you're outside the US" while Alcor had... some kind of international process that I couldn't really clarify despite asking.
Eventually I got sick of Alcor seeming to only check their emails once per week and abandoned the whole quest. So I got pushed away from CI because they refused to help me in Australia, and pushed away from the other org because they consistently gave the impression of being hugely uninterested.
Now I just hope I don't die until A) one of the existing organisations starts acting like they actually want me to sign up, or B) someone better opens up shop.
Replies from: enoonsti↑ comment by enoonsti · 2012-04-13T02:04:51.382Z · LW(p) · GW(p)
Did you check out Stasis Systems of Australia? They appear to be in the early stages of development, but it may be something worth keeping an eye on:
http://stasissystemsaustralia.com/
In the meantime, if you are truly interested in cryonics, then I recommend taking a more proactive approach (writing articles, joining/forming local groups, etc). Don't simply treat it as a good for consumption. Alcor and CI are confronted with a logistical nightmare and so each of us really have to contribute more than just money.
comment by Paul Crowley (ciphergoth) · 2012-04-11T06:44:00.679Z · LW(p) · GW(p)
AIUI, since I'm in the UK, the only part of my cryopreservation that my US-based provider would handle is final cooldown and storage; the rest would be done by Cryonics UK in either instance. I think that means there's currently no downside in going with the cheaper provider.
Replies from: enoonsti↑ comment by enoonsti · 2012-04-13T02:25:44.538Z · LW(p) · GW(p)
I haven't heard about Cryonics UK for a while. Are you part of their standby team?
Replies from: ciphergoth↑ comment by Paul Crowley (ciphergoth) · 2012-04-13T07:50:47.153Z · LW(p) · GW(p)
No; I've been to one training event, but I can't afford the time/costs to go repeatedly.
comment by DumbedDown · 2015-09-25T03:30:36.106Z · LW(p) · GW(p)
Old thread, but here goes... does it matter if CI clients are more "messed up" on average than Alcor clients currently? If we believe in constant scientific progress, isn't it just a matter of Alcor clients being revived in the mid 2100's vs. CI clients being revived in the mid 2200's???
Having just started researching my own cryonic future, any significant updates as to this 2012 Alcor vs. CI thread...? It scared me off $29K CI back onto $220K Alcor...
As to full body, might my full body DNA be used to recreate my specific young adult body -- I am thinking I want full body with head detached for quick infusion... Might my aged original body have monetary value in 2200 that I can sell-trade for whatever...?
comment by mkmk · 2012-04-15T23:48:26.860Z · LW(p) · GW(p)
I have chose the Cryonics Institute for several reasons. It is not only the price which makes a huge difference to me because I can potentially save my entire family (5 people for less then the cost of 1 person at Alcor) but there is other reasons as well. While I might agree that in some circumstances Alcor can do a better job at profusion they often do not and certainly to me they do not justify the costs. Alcor has huge overhead compared to CI the number one expense being personnel. It only takes 2 people at CI to do what many more take for much more in resources. The costs of such overhead are likely to grow as they are with Alcors price. This is another reason, because rather then bringing prices under control they will be forced to raise prices again and again. This chases away more and more customers until the company cannibalizes itself and collapses. I would rather grow an organization through more members rather then a few rich ones. There is also a moral lesson here as well, because if cryonics works then more people would be save because of the lower price.
I have heard the arguments that no matter what there will be damage and Darwin/ Aschwin and Chanda have claimed this to be the case. I have also heard them all say Alcor is better but at the same time they all seem to be falling back on the nanotechnology will fix things just as much as CI does. After all Alcor throws many body's away as in nueros. What could be a greater hurdle for nanotechnology then a complete neck down rebuild. So Max's argument that CI doesn't profuse the body rings hollow. As for the amount of damage to the brain, it seems to me the biggest factor is neither of the company's procedures, sterile technique, or formulas that make much of a difference but rather speed and quick ice that is all. Both companies vitrify with a good formula so thats a minor issue. Alcor claims that it has a standby service and if a CI member wants to have the same service he can contract with SA so again no difference. In fact, it is still much cheaper even with the SA standby option. I think the fact that CI lets its members have the option rather then being forced into Alcors standby is a huge reason I chose CI. I could take the thousands saved and plan and pay for local standby myself for a fraction of the costs. To me Alcors and SA's standby makes sense only if you live within 50 miles of either company. This standby to me is a huge false sense of security because the member thinks everything is taken care of. Things just don't work that way. The logistics will not allow it. Every member of any cryonics organization must have their own standby unless they have a nice planned death and then standby matters little. You just have someone drive you to CI or Alcor.
For 150+ thousand dollars I could afford a pretty good personal standby and I could share in local training. Its the difference between centralized so called professionals who are too far away and a huge network of good lay people willing to help out. Funeral directors and a few friends and family may not be as good as Alcor's or SA's centralized team but what does it matter if the special team is 8 hours away? It reminds me of the difference between having good enough CPR from a layperson moments away or a team of doctors and equipment 2 hours away! When you need CPR you need it now... not 2 hours from now. So I opt for CI and my own standby. If I was rich and I live very close to Alcor or SA , I might change my mind. For all the fancy talk about this and that, this is the common sense of the matter. I would rather use the money myself to set up a very good local standby that I can trust. All of the talk by Alcor members about superior profusions etc can not even be validated unless we take patients out of their cryostats and actually look at their brain tissues. Both companies have failed with patients in many hours of warm ischemia. The only difference is that CI's failures cost170,000$ less.
I suggest both companies do more to form layperson networks to include funeral directors and more research and development on patient early warning cardiac arrest alerts rather then fancy formulas that attempt to perfuse an already rotten corpse. Centralized standby is a fail from the get go no matter how professional the staff or shinny equipment. That's why the worlds Fire & emergency response teams consist of many lay people that bring the patients to central medical centers. The strength is in the vast network not the central standby professionals. For all the other talk about research and development or patient revival etc. I have to make my feelings clear we are simply an ambulance company to a future hospital. We aren't that future hospital nor should we pretend to be so. We don't have the time, luxury, or money to play that part. The more we drift from the basics of ambulance company to the future the more bogged down we get in irrelevant factors rather then simple fast cooling and fast vitrification! I am not saying we shouldn't strive to improve and use better techniques but there is such a thing as common sense and a point of diminishing returns. Alcor may be a little better if you live in Arizona and are rich but outside of that the costs just don't justify the returns. I will save my money and use CI and form my own standby. If I were an Alcor member outside Arizona you can bet your butt I would have some standby in place my life would depend on it despite all the money I could throw at them. The rest is smoke and mirrors or shinny cryostats.
comment by cath · 2012-04-24T04:19:43.635Z · LW(p) · GW(p)
I signed up with Bay Area Cryonics Society in 1977, and changed to Alcor in 1985, along with my husband, Thomas Donaldson, a mathematician and writer, who is now a neuropreservation patient with Alcor, as of 2006. We changed because of the dynamism and research brought to Alcor by Mike Darwin and Jerry Leaf, both of whom I first met in 1979. I switched to CI about ten years ago after moving back to Australia.
A big reason for moving back to Australia was largely because as a result of the lawsuits engaged in by Alcor, the Dora Kent case and Donaldson's lawsuit against the State of California for assisted suicide in the event of destruction of neural tissue by his brain tumour, my bipolar disorder became severe and I ran out of medical insurance. About this time, a young man in contact with Alcor committed suicide, and the response of a number of the Libertarian Alcor members was that "this must have been what he wanted" i.e. his death by suicide, and not cryonic suspension. As a person who has contemplated suicide, this was not an impressive response.
Whilst in Australia, I phoned Alcor to find out how the much-promised (over years) review of members paperwork was going, and the staff member (presumably being paid) was unable to make an international phone call, and unable to handle my anger at this ineptitude. I switched promptly to CI because Andy Zawacki made the call with grace and ease.
Subsequently on the cryonic suspension of Thomas, Alcor went against the stated wishes in his paperwork (that had a personal and potentially critically important justification), of not making public his suspension by doing so "informally", after a staff member tried to coerce me to allow them to do so, using sarcasm when I refused and was in a crisis of shock and grief. There was a poor history of returning my phone calls whilst I was administering his estate, by senior Alcorians. Hugh Hixon and Mike Perry are notable exceptions.
During this severe period of my life, Ben Best and Andy Zawacki were sensitive and supportive, and good listeners. Hugh Hixon, Mike Perry and Aschwin have also been active in contacting me in a short time frame, and Hugh was supportive in the time immediately after the suspension. As Alcor has the copyright of Thomas' published writings, and a number of people have contacted me wishing to read some of them again, the Alcor board was approached to allow me to do so. I have not heard from them in several months. Merkle was responsible for suppression some of Thomas' writings critical of nanotechnology, so I hope this is an oversight and not suppression, or the policy that once a person is suspended and paid up there is no responsibility for the intellectual continuation of patients' lives. This is hard particularly because of the personal and emotional costs of the euthanasia lawsuit. Most particularly, I wished to make his fiction more available to interested readers.
In summary, I am not surprised Alcor runs into difficulties with lawsuits. Cryonics is a "people business" as well as a technology provider, dealing with people in some of the most extreme emotional situations, and I think Alcor may do this side of the business poorly. I have the confidence that should I become irrational and suicidal, CI would have the skills to call me back to myself, so I remain with them, and try to put any spare cash into research or general running costs. At some point the immeasurably valuable quality of "the human touch" can be more important than technological accessories and certainly better than the lawsuits that its lack of possession may bring.
comment by Shmi (shminux) · 2012-04-09T20:04:23.703Z · LW(p) · GW(p)
As I mentioned elsewhere, my biggest concern is the continuous operation of a cryoshop over the potential centuries or even millennia until the revival is attempted, as nearly no entities have ever survived that long. I have been unsuccessful in my search for an Alcor executive explicitly responsible for existential risk analysis and mitigation.
By existential risk to the company I mean an event that would result in the company failing to the degree that the stored patients are discarded, even though the outside world merrily hums along, and not an event that wipes out a large chunk of humanity.
The FAQ does not seem to answer the obvious hard questions like "what if Morgan Stanley goes under?", "what if the US dollar collapses?", "what other existential risks exist, and what are their probability estimates and error bars?", "what is an estimated lifetime of Alcor until it suffers a complete failure from one of the existential risks to it coming to pass?" etc. By the way, if you think that the answer to the last question is "infinite", I recommend a basic probability and statistics course.
In other words, the risk management appears to be at the level no better than that of a regular insurance company, which is completely inadequate for an organization whose long-term survival is the most critical issue.
comment by taw · 2012-05-01T12:49:37.336Z · LW(p) · GW(p)
Such an acknowledgement, though appreciated, is frankly disturbing, considering that members depend utterly on these organizations remaining operational and solvent for decades, perhaps even centuries, after they are deanimated.
Decades? You are being ridiculous. If cryonics works it will be many centuries as an absolute minimum. And no organization in the entire history had unbroken record like that. Even the Catholic Church had breaks from time to time.
Replies from: JoshuaZ↑ comment by JoshuaZ · 2012-05-01T15:11:52.666Z · LW(p) · GW(p)
Decades? You are being ridiculous. If cryonics works it will be many centuries as an absolute minimum.
What makes you reach this conclusion?
And no organization in the entire history had unbroken record like that. Even the Catholic Church had breaks from time to time.
The last anti-Pope was in the late 1400s. Even if one includes the Reformation and Counter-Reformation that's at least three centuries of unambiguous stability. There are also still extant corporations dating from the 700s. In the case of many companies, they go out of business because the product they are selling is no longer relevant (e.g. typewriter companies) but cryonics corps will continue to remain relevant as long as they have patients.
Replies from: taw↑ comment by taw · 2012-05-01T16:10:19.624Z · LW(p) · GW(p)
What makes you reach this conclusion?
First, we need technology of living forever as a precondition before any kind of rethawing makes any sense, and this technology is so obviously centuries away. Just notice how slowly any kind of anti-aging research progresses.
I'd happily bet against any cryonics rethawing happening in the next few centuries, but there's no market for that.
The last anti-Pope was in the late 1400s. Even if one includes the Reformation and Counter-Reformation that at least three centuries of unambiguous stability.
Just to mention a few breaks I remember - pope was imprisoned and Rome sacked in 1527), Napoleon took over Rome and exiled the pope in 1798), and takeover of Rome by Kingdom Italian was at least highly disruptive if it didn't constitute a full break of continuity.
There are also still extant corporations dating from the 700s.
Their list is extremely dubious, and even cases where companies really operate since the listed date includes a lot of breaks (like Wedel's for WW2, Communist takeover etc. - only the brand really continues all that time).
I'd take no entries on their list at face value.
Replies from: JoshuaZ, AngryOnion↑ comment by JoshuaZ · 2012-05-02T00:06:21.891Z · LW(p) · GW(p)
Valid points. The continuity of the Catholic Church had a lot more interruptions after the last anti-Pope. And your point about functional interruptions of old businesses is quite relevant since cryonics patients aren't going to survive just off a surviving brand name. I think you may be overestimating the amount of time it will take for cryonics to work, but I haven't thought about the time-frame that hard.
Replies from: gwern↑ comment by gwern · 2012-05-02T00:50:26.025Z · LW(p) · GW(p)
If you had Catholic Church style cryonics orgs, interruptions wouldn't be so bad - you could build vast (dare I say cathedral-sized?) underground cryonics graves with excess volume & boil-off times measured in years or decades. You could analogize to libraries: books decay and need active protection and fires are risks, but can go a few years without (probably) being destroyed. The Church has succeeded in some very long-term libraries.
Replies from: JoshuaZ↑ comment by AngryOnion · 2013-02-05T18:38:59.329Z · LW(p) · GW(p)
I'd love to bet for cryonics happening within this century, if not within 50 years. What makes this bet even more interesting is that pretty much everyone is betting against it.
Key in my estimation is the phenomenon of exponential progress, particularly since the dawn of mass internet and the unbelievable wealth and ever increasing and improving information exchange.
The technology to living forever, as you put it, is probably just around the corner (within 30 years), but yes, the chronological order makes sense, at least for old folks.
Replies from: shiggity↑ comment by shiggity · 2013-03-28T07:02:15.658Z · LW(p) · GW(p)
Exponential progress? Nothing has changed within the last 50 years. At all. We've always had the personal computer, smartphones, buckyball quantum entanglement, the World Wide Web, the full sequence of the human genome, a deactivated Leukemia-killing HIV strain, autostereoscopy, in vitro fertilization, OCR, GPS, LHC, 3D printing, and robotic exoskeletons for paraplegics.
And nothing will change in the next 50.