Josh Jacobson's Shortform
post by Josh Jacobson (joshjacobson) · 2021-08-01T04:54:38.855Z · LW · GW · 23 commentsContents
23 comments
23 comments
Comments sorted by top scores.
comment by Josh Jacobson (joshjacobson) · 2021-08-10T06:01:44.861Z · LW(p) · GW(p)
An article published today on Reuters and elsewhere reads, "Israeli survey finds 3rd Pfizer vaccine dose has similar side effects to 2nd." Buried within this article is the following:
About 0.4% said they suffered from difficulty breathing, and 1% said they sought medical treatment due to one or more side effect.
This seemed quite bad to me and like a worrisome result. I sought information on how many sought medical treatment after the second shot. I could not find this information, but I did find:
only 51 of some 650,000 people to have received the Pfizer shot sought medical attention for symptoms suffered
from a December 2020 article on Israeli vaccination. Comparing the 1% to 51/650000 = 0.008% I found that the current frequency of side effects requiring medical attention was 128x the level found after dose 1. This seemed like a bad sign.
I then sought out more information about side effects post dose 2 in Israel, which I did not find. But instead I looked at the CDC's Advisory Committee on Immunization Practices’ Interim Recommendation for Moderna, and found the following:
The frequency of serious adverse events** observed was low in both the vaccine (1.0%) and placebo (1.0%) recipients
** Serious adverse events are defined as any untoward medical occurrence that results in death, is life-threatening, requires inpatient hospitalization or prolongation of existing hospitalization, or results in persistent disability/incapacity.
- I can't believe that this was 1%! That seems surprisingly high (for either group). I expect the outside-of-trial data has not been nearly that magnitude.
- This 1% matches the current Israeli data, and with a more restrictive definition, so the Israeli data no longer seems particularly worrisome in comparison, though I may dig in to this further. In general, I feel somewhat confused by the situation.
Sources: Reuter's article from today - https://www.reuters.com/business/healthcare-pharmaceuticals/israeli-survey-finds-3rd-pfizer-vaccine-dose-has-similar-side-effects-2nd-2021-08-08/
Article from December 2020 - https://www.timesofisrael.com/1-in-1000-israelis-report-mild-side-effects-from-vaccine/
CDC's Advisory Committee on Immunization Practices’ Interim Recommendation for Moderna: https://www.cdc.gov/mmwr/volumes/69/wr/mm695152e1.htm
EDIT: This article's statistics contrast with those of Reuter's, and show data very similar to the 1st shot: https://www.timesofisrael.com/of-600000-israelis-who-received-3rd-dose-fewer-than-50-reported-side-effects/
Replies from: kamil-pabis↑ comment by Kamil Pabis (kamil-pabis) · 2021-08-10T10:07:04.336Z · LW(p) · GW(p)
With such highly subjective soft outcomes a lot depends on the way the question is phrased and interpreted (if self-reporting). Thus comparing different populations and studies is almost impossible without really carefully digging into the original publications and even then it is fraught with problems.
If I have a rash post-vaccine and I go to see my GP or pharamcist, am I seeking medical help and is this worrisome? If I get up and later realize that I need to lie down or else I will faint (vasovagal syncope, around one in ten people have some form of needle phobia), am I seeking medical help for a side-effect? Technically yes, but a saline injection would cause the same. If I have asthma or hayfever, issues with breathing, and later misattribute this to the vaccine, is this a side-effect? (around 1 in 10 people or so have asthma)
Finally, you cannot compare the serious side-effects in a trial (if this CDC figure really comes from a trial) with mild self-reported side-effects from Israel or American postmarketing surveillance. Trial participants will be monitored closely and will include a large number of at risk indiviudals (>60yo) so it is again a statistical artifact of data collection.
IMHO all the data is worthless without a very well-matched control group.
comment by Josh Jacobson (joshjacobson) · 2022-01-12T23:54:22.556Z · LW(p) · GW(p)
Bringing over the outcome of a lot of recent discussion I've had on Facebook and some research I've done regarding the Narwall Mask:
-
I believe there's currently a lot of uncertainty as to the effectiveness of the Narwall, with multiple meaningful reasons for there to be uncertainty. A lot of effectiveness outcomes would not surprise me. I do not believe it has been well-tested nor well-analyzed, at least compared to those that meet NIOSH standards.
-
I think there's enough information out there to statistically estimate its effectiveness with some reasonable degree of confidence, but it would take me another 3-8 hours (on top of my existing research) to do so. Considering a P100 is just ~$30 for me, I've just switched to that + glasses when relevant for now instead. I think others should do the same if they can achieve good fit with a P100 (the Microcovid authors seem to think this can often be achieved.) https://www.microcovid.org/paper/14-research-sources#masks
-
I think theres a 75% chance that after estimating its effectiveness, I'd find it to be meaningfully less than a P100 (e.g. less than 98.5% on the relevant filtration). I think there's a 50% chance I'd find it to be approximately equal to an N95 mask or worse.
Sharing this here because some LWers wear it and I think there's some value in sounding a warning about the mask potentially not being as effective as most likely anticipate.
comment by Josh Jacobson (joshjacobson) · 2021-08-20T00:13:57.407Z · LW(p) · GW(p)
I recently had what I thought was an inspired idea: a Google Maps for safety. This hypothetical product would allow you to:
- Route you in such a way that maximizes safety, and/or
- Route you in such a way that maximizes your safety & time-efficiency trade-off, according to your own input of the valuation of your time and orientation toward safety
First, I wanted to validate that such a tradeoff between safety and efficiency exists. Initial results seemed to validate my prior:
- The WHO says crashes increase 2.5% for every 1 km/h increase in speed.
- The Insurance Institute for Highway Safety (IIHS) reports fatalities increase by 8.5% when there is a 5mph increase in speed limit on highways, and 2.8% for the same speed limit increase on other roads.
- The National Safety Council (NSC) cites speed as a factor in 26% of crashes.
Despite these figures, I felt none of these, on their own, provided sufficient information to analyze the scale of safety gains to be had. The WHO source was outdated and without context (although there was a link to follow for more information that I didn’t see at that time), the IIHS merely talked about increases in speed limits for two types of roads, rather than actual changes in speed that results nor relative safety of the two types of roads, and the NSC provided a merely binary result.
So I went searching for more data.
And I discovered that the US National Highway Traffic Safety Administration (NHTSA) releases a shocking amount of data on every fatal car crash. There’s useful data, such as what type of road the crash happened at, what the nature of the collision was, information on injuries and fatalities, whether alcohol was involved, etc.
(There’s also a surprising amount of information that I expect might make some people uncomfortable. For every crash this data includes VIN number of vehicles involved, driver's height, weight, age, gender, whether they owned the vehicle, driving and criminal history. It also includes the exact time, date, and location of the crash.)
I used the former (useful) information for analysis on this question. Given the initial data found, I figured that one way to approximate the available gains and tradeoffs was to analyze safety-gained from turning on the “Avoid Highways” setting on Google Maps.
After some experimentation and reading others’ thoughts, it became clear that this setting avoids interstates (I-5, I-10, I-15, etc.) but not other types of highways. I used NHTSA data to calculate the number of deaths occurring on interstates vs. on other roads, and found that the Federal High Administration provides data on the number of miles driven in the US per year by type of road. Using these two sources of data, I calculated the number of miles driven per fatality on interstates vs on all other roads (for 2019):
Interstates: ~180 million miles / fatality
All Other Roads: ~104 million miles / fatality
It turns out that interstates appear to be (at least on this metric) safer than non-interstates! This was surprising to me, given the earlier cited results that pointed to speed being dangerous.
I decided that I’d do more validation of this result if this was surprising to most people, but wouldn’t perform more validation if this wasn’t. Asking around, it looks like this result is not surprising to most:
From Effective Altruism Polls:

From EA Corner Discord:

And from the LessWrong Slack:

So first of all, good job community, on seemingly being calibrated. Second, I followed my earlier plan and did not look further into this result given that it was aligned with most people's priors. And finally, I do think this makes the expected value of a Google Maps for safety significantly lower than my prior.
Assuming this result would hold through further validation, there are still ways that a Google Maps for safety could be beneficial. A few examples of this:
- Seeing if there are other road-type routing rules that would provide safer outcomes.
- Using more specific data, such as crash reports by road, to identify particularly dangerous roads / intersections and avoid them.
- There seem to be some behavioral economics-like results with road safety that could be leveraged during route design. For example, apparently roads with narrower lanes are safer than roads with wide lanes, presumably because narrower lanes have the effect of people driving more slowly, while having a lower effect on increased accident rate.
- Digging further into data on factors that contribute to crashes (alcohol, weather, distraction, evening, etc.) could reveal patterns that provide clues as to the safer route by situation.
I think this could be a really cool app to have, and I’d support its development if someone were to take it on, but it seems like a big project. I was sad and surprised to find that the potential quick win of turning on the “avoid highways” option is seemingly not a win at all (although there exist confounders and further validation would be beneficial).
Replies from: romeostevensit, WilliamKiely↑ comment by romeostevensit · 2021-08-20T00:20:41.067Z · LW(p) · GW(p)
Intersections are what kill mostly. The energy delta between two fast moving cars going the same direction is low. The energy delta between even moderatly moving cars at orthogonal or directly head to head is huge.
Replies from: joshjacobson↑ comment by Josh Jacobson (joshjacobson) · 2021-08-20T00:48:54.210Z · LW(p) · GW(p)
Intersections are what kill mostly.
This doesn't appear to be true. Using the same data I used above I get:

↑ comment by WilliamKiely · 2021-08-20T01:14:45.806Z · LW(p) · GW(p)
Perhaps the accurate way to say Romeo's point is that time spent driving through intersections is (much) more dangerous than time spent driving on roads, highways, etc.
↑ comment by WilliamKiely · 2021-08-20T01:16:17.735Z · LW(p) · GW(p)
A related question I've never seen the data on: How much more dangerous is driving at night than driving during the day? (per mile driven)
comment by Josh Jacobson (joshjacobson) · 2023-10-07T19:29:40.305Z · LW(p) · GW(p)
Would anyone like the domain alignai.org ? Otherwise I'll probably let it expire (bought for a previous org, which doesn't want it).
Replies from: johannes-c-mayer↑ comment by Johannes C. Mayer (johannes-c-mayer) · 2023-10-12T05:38:46.858Z · LW(p) · GW(p)
Replies from: ete↑ comment by plex (ete) · 2023-10-12T09:34:33.204Z · LW(p) · GW(p)
Yeah, that could well be listed on https://ea.domains/, would you be up for transferring it?
comment by Josh Jacobson (joshjacobson) · 2021-08-20T19:41:46.293Z · LW(p) · GW(p)
EDIT (7/27/23) After very preliminary research, I now think "telling people to ride in SUVs or vans instead of sedans" may turn out to be worthwhile.
As I’m working on derisking research, I’m particularly aware of what I think of as “whales”... risks or opportunities that are much larger in scale than most other things I’ll likely investigate.
There are some things that I consider to be widely-known whales, such as diet and exercise.
There are others that I consider to be more neglected, and also less certain to be large scale (based on my priors). Air quality is the best example of this sort of whale, though 3-8 other potential risks or interventions are on my mind as candidates for this, and I won’t be surprised to discover a couple whales that did not seem to be so prior to investigation.
I thought that road safety and driving was a widely-known whale. Based on a preliminary investigation (more on what this means), I now tentatively think it is not.
This preliminary analysis yielded an expected ~17 days of lost life as a result of driving for an average 30 year old in the US over the next 10 years.
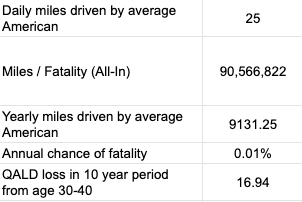
I’m not sure how many of these 17 days an intervention could capture. I suspect most likely readers of what I’d write already grab the low-hanging fruit of e.g. not driving while impaired and wearing a seatbelt. So it does not seem probable that I would discover an intervention that alleviated even 30% (~5 days) of risk. Furthermore, I suspect most interventions in this space could have large inconvenience or time costs, causing greater reduction in the expected gain of my research in this space.
While this analysis does neglect loss of QALDs due to injury, which I don’t know the scale of, I predict they are unlikely to greatly affect this conclusion.
The 10 year timeframe may seem odd to some. But if we assume that self-driving cars of a certain ability level will greatly increase the safety of vehicle travel, which I personally believe, then 10 years may be even longer than the relevant window for investigation. Metaculus predicts L3 autonomous vehicles by the end of 2022, L4 autonomous vehicles by the end of 2024, and L5 autonomous vehicles by mid 2031. It’s not entirely clear to me at which of these stages most of the safety benefits are likely to occur, nor how long widespread use will take after these are first available, but it does seem to me as though the dangers of car travel, at least for most people who are likely to read my content, will not persist long into the future.
I have some context for effect sizes I think I’m likely to find with various interventions. I have preliminary estimates for interventions affecting air quality & nuclear risk, and more certain estimates for interventions on smoke detectors and HPV vaccination. With that context, road safety does not seem to particularly differentiate itself from much else I expect to investigate. With this discovery that road safety does not seem to be a ‘whale’, I tentatively think I will not further investigate it in the near future.
Replies from: adamzerner, ChristianKl↑ comment by Adam Zerner (adamzerner) · 2021-09-01T07:52:43.467Z · LW(p) · GW(p)
If you're interested in a perspective from left field, I wrote a post [LW · GW] about how we should perhaps be valuing life wildly more than we currently are, and that if so, driving becomes a terrible idea.
↑ comment by ChristianKl · 2021-08-21T05:43:14.684Z · LW(p) · GW(p)
Furthermore, I suspect most interventions in this space could have large inconvenience or time costs, causing greater reduction in the expected gain of my research in this space.
Wearing a helmet when driving in a car would be one intervention that isn't that inconvient but I don't know the impact.
Replies from: joshjacobson↑ comment by Josh Jacobson (joshjacobson) · 2021-08-25T18:58:40.818Z · LW(p) · GW(p)
Thanks for sharing the idea. I think I'd find this inconvenient, but I do expect the inconvenience of various changes will vary significantly between people.
comment by Josh Jacobson (joshjacobson) · 2021-08-18T00:31:02.130Z · LW(p) · GW(p)
This is a follow-up to https://www.lesswrong.com/posts/RRoCQGNLrz5vuGQYW/josh-jacobson-s-shortform?commentId=pZN32PZQuBMHtM8aS [LW(p) · GW(p)] , where I noted that I found the following sentence in an article about an Israeli study on 3rd shot boosters:
About 0.4% said they suffered from difficulty breathing, and 1% said they sought medical treatment due to one or more side effect.
worrisome, and how I reconciled it.
When I posted that, I reached out to Maayan Hoffman, one of the authors of the original Israeli article, with these observations. She found these interesting enough that she reached out to Ran Balicer, the head of the study (Head of Research at Clalit Health), with my observations, and then she forwarded his response to me:
We used ACTIVE screening for AE - we surveyed 22% of the vaccinees. [The other report cited] (https://www.timesofisrael.com/of-600000-israelis-who-received-3rd-dose-fewer-than-50-reported-side-effects/) [includes] PASSIVE reports of AE that the vaccinees choose to share with the reporting system. These are complementary systems. Just like in the US and other countries. Both are important. ... What we did is quite unprecedented. In terms of timing (same day - proactive calls - data gathering - analysis - informing the public). On 4500! People - 22% of all those with 7d experience after the 3rd shot. Even in Covid - I don’t think anyone has achieved anything like this. A clear message for the public to get vaccinated.
My thoughts:
-
There's still something uncomfortable about the 0.4% having difficulty breathing to me. Based of what I cited previously from the Moderna study, and this additional context of active monitoring, the 1% seeking medical attention seems notable but not a big deal (after all, it matches placebo in the Moderna trial). It was still an update vs. my expectations when originally seeing it.
-
I think this makes me mildly more hesitant than before about the booster shot, but I definitely strongly believe the booster shot is worthwhile (in isolation, e.g. not considering global fungibility). Also, it's not at all clear that this result is unique to booster-recipients vs. earlier vaccine reactions.
comment by Josh Jacobson (joshjacobson) · 2023-07-27T22:44:02.284Z · LW(p) · GW(p)
Very quick, likely highly flawed and inaccurate Fermi on the worthwhileness of riding in SUVs or vans instead of sedans:
~50% safer per mile maybe
~20% more expensive to buy / rent / rideshare
~1 day per year gained in expectation for a 35 yo
~$10k spent on vehicle travel per year per person
Cost: ~$2k / day of life gained
Worthwhile if valuing a year at: ~$600k or greater
Replies from: pktechgirl, rhollerith_dot_com↑ comment by Elizabeth (pktechgirl) · 2023-07-29T00:52:40.548Z · LW(p) · GW(p)
what's this based on? At one point SUVs had a higher death rate due to risk of rollover, in addition to the negative externalities.
↑ comment by RHollerith (rhollerith_dot_com) · 2023-07-28T18:02:45.568Z · LW(p) · GW(p)
It's only safer for the occupants of the SUV. For everyone else, an SUV is more dangerous.
Replies from: MakoYass↑ comment by mako yass (MakoYass) · 2023-07-28T22:40:08.105Z · LW(p) · GW(p)
So factor in the cost of the other members of your decision theoretic agent-class with respect to driving SUVs for safety reasons also driving SUVs
comment by Josh Jacobson (joshjacobson) · 2021-08-01T04:54:39.096Z · LW(p) · GW(p)
~2 weeks ago, the FDA added a warning to the J&J Covid shot regarding increased risk of developing Guillain-Barré Syndrome.
Perhaps unsurprisingly, given the history with blood clots, my quick check of prevalence finds that reports of developing GBS following J&J vaccination are actually less than would be expected otherwise.
My very basic analysis: https://docs.google.com/spreadsheets/d/1wDFrDq0E6Q096E97XzU7ndP53mYC0Paf9Wyun-XxmWA/edit?usp=sharing
Numbers from: https://www.yalemedicine.org/news/covid-vaccine-guillain-barre-syndrome
EDIT: Analyzed another way, GBS cases may be 3-4x more common in J&J vaccine recipients than base rates (still highly uncommon, but I see the potential association).
comment by Josh Jacobson (joshjacobson) · 2023-09-20T21:34:05.821Z · LW(p) · GW(p)
Some lawyers claim that there may be significant (though not at all ideal) whistleblowing protection for individuals at AI companies that don't fully comply with the Voluntary Commitments: https://katzbanks.com/wp-content/uploads/KBK-Law360-Despite-Regulation-Lag-AI-Whistleblowers-Have-Protections.pdf
comment by Josh Jacobson (joshjacobson) · 2022-06-26T02:14:23.681Z · LW(p) · GW(p)
There’s a lot of COVID going on my family right now, and my father’s birthday that three of us flew in for is tomorrow. I’m trying to figure out who (if anyone) is safe to spend time with him, and to what degree.
My father: 77 years old and in very good health for his age. Four Moderna shots, has never caught COVID. He’s the one we’re trying to protect from our infections.
Me (mid-30s): Triple vaxed (Moderna). Symptoms started Sunday June 19th and had a rapid test positive Sunday. Started Paxlovid Monday. Negative rapid test w/ throat swab yesterday and today. Negative NAAT test today. Symptoms were generally mild and seem to have ended late yesterday. Been in total isolation from others since positive test.
The following four people are all living together and not distancing from one another:
My sister (early 30s): Triple vaxed. Symptoms started Tuesday June 14th. Had significant symptoms and visited ER as a precaution but didn’t need to be admitted. Received bebtelovimab monoclonal antibodies. Pregnant. Started feeling better this past Thursday, but still symptomatic. Negative rapid tests with throat swabs 2 days ago, yesterday and today, negative NAAT rapid test today.
Her husband (early 30s): Triple vaxed, symptoms also started Tuesday June 14th. Took Paxlovid starting June 16th. Mild symptoms and has felt recovered for ~6 days now. Negative rapid tests with throat swab 2 days ago, yesterday and today and negative NAAT today.
Sister’s Husband’s Mother (60s): 4x vaxed, symptoms started Saturday June 11th. Took Paxlovid starting June 13th. Symptoms ended June 15th. Negative NAAT test June 20th, negative NAAT test today, but a positive rapid test with throat swab today, then a negative rapid with a different brand.
Sister’s Husband’s Father (60s): 4x vaxed, symptoms started Saturday June 11th. Took Paxlovid starting June 13th. Had had some breathing difficulty and lethargy since June 13th, which got better for a while and now is somewhat worse. Generally continues to feel affected by COVID. Negative NAAT on June 20th, positive NAAT today, negative rapid test with throat swab today.
Different scenarios all make sense to me, but I haven’t researched much:
-
We should listen to the rapid tests, and all are safe to spend time with my Dad as much as we want, except my Sister’s Husband’s Mother, who shouldn’t spend time with my Dad.
-
Same as above, except that given my sister’s husband’s mother has been living with the others, they might be able to pass on the virus as well. So only I am safe to be around my Dad.
-
That for everyone except me, enough time has passed that they’re very, very unlikely to be contagious (plus everyone has had a preponderance of negative tests). I’m very unlikely to be contagious due to my negative tests, although Paxlovid rebound is real and at least somewhat significant. Therefore everyone else is safe to be around my Dad, but I’m a couple percent risk of being contagious.
-
We all have a couple percentage point possibility of being contagious, and that an all day affair involving all of us may result in something like a 10% chance my Dad gets covid, which may be above our acceptable thresholds. In that case, we wouldn’t get together potentially, or would only gather e.g. outside and masked.
I’m interested in and would very much appreciate others thoughts! I don’t have at all a good understanding of to what extent each of us might be contagious, and would really like the thoughts of those who may have looked into this sort of question much more than I have.