Omicron Post #8
post by Zvi · 2021-12-20T23:10:01.630Z · LW · GW · 33 commentsContents
South Africa United Kingdom Denmark Around the World The English Study Severity and Its Discontents Law of No Evidence: Any claim that there is “no evidence” of something is evidence of bullshit. Spread Policy Response Threads and Articles Retrospective Outlook Probability Updates and Predictions Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 90% → 85%. Chance that Omicron is importantly more virulent than Delta: 3% → 3%. Chance that Omicron is importantly less virulent than Delta: 60% → 50%. Will the CDC label Omicron a variant of high consequence before 2022? 11% → 9%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 35% → 30%. None 33 comments
I have fallen mildly ill, as have my wife and son. So far we don’t have a positive Covid-19 test, and everyone is maximally vaccinated, but given the timing the obvious conclusions do seem likely. Wish me well, and hopefully Christmas will not be cancelled and I can keep the posts mostly going. I do have winter break to help me out.
Omicron continues to take over. Official reactions have been relatively mild, with only the Netherlands entering a lockdown that I have seen. Private reaction has been more robust, which is the best way to do it, and there are some early signs it could be having a substantial effect in the UK, although I’m guessing that is probably a mirage. As usual, we’ll know one way or another in a few days, only to have a new set of mysteries on our hands.
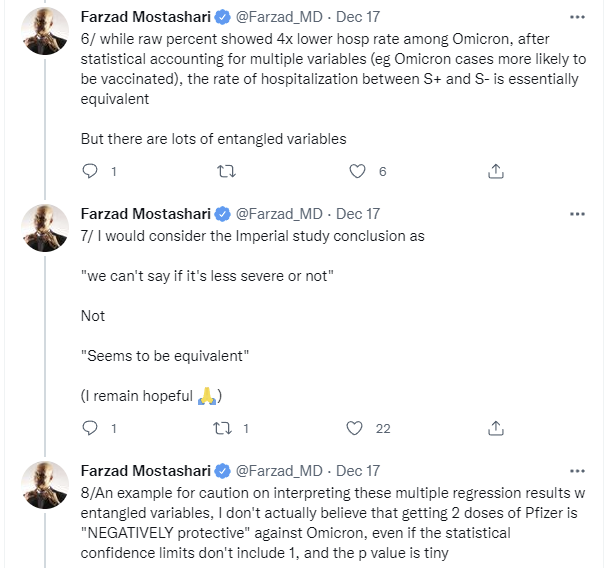
The big argument in the last few days was over severity. A new study on infectiousness in the UK was essentially misappropriated, and its 24 (!) hospitalized Omicron patients (0.15% of all cases, versus 0.7% of other cases, before controlling for things, then when controlling for things they mostly evened out) were cited as strong evidence that Omicron is not less severe than Delta. Whereas what the study actually said on the topic was mostly nothing, because there wasn’t enough data yet.
Thus the big row over the idea of there being ‘no evidence’ for things, and how that turns into those things being known to be wrong (or right!) at the whim of those who control the narrative, Scott Alexander writing how The Phrase ‘No Evidence’ Is a Red Flag for Bad Science Communication, and me writing up my previous harsher but fairer proposal for the Law of No Evidence that the claim that there is ‘no evidence’ for something is evidence of bullshit.
As usual, we’ll look at South Africa, the UK, Denmark and select other places, then survey other aspects, then update our probabilities.
South Africa
Here’s a news dashboard with good charts for South Africa. Looks like things may have somehow peaked there, at least in the most hard-hit areas, and that there will be far fewer ventilated patients than in previous waves.
This is one of the many ways we have more data. That doesn’t mean we’re closer to understanding it.
This new wave is milder per case but we already knew that. That’s not the question. Ventilator use or deaths seem better than hospitalizations since hospitalizations are partly about capacity, so 16% is encouraging, but the lag is also a thing, so the ‘could get to 20%+’ is the even more encouraging bit.
The most exciting and confusing thing is that the outbreak seems to be peaking already, at least at its point of origin in Gauteng, as usual not for any obvious reason?
Here’s an excellent interview with Trevor Bedford looking into that question. He lists five potential causes: Lack of testing, underreporting due to mildness, faster generation time, network patterns and differential vulnerability. Faster generation times are the most interesting one here. It’s worth noting that Trevor’s methods of modeling that are failing now worked for Delta in the same region, so factors that would also apply to Delta seem less plausible as explanations here.

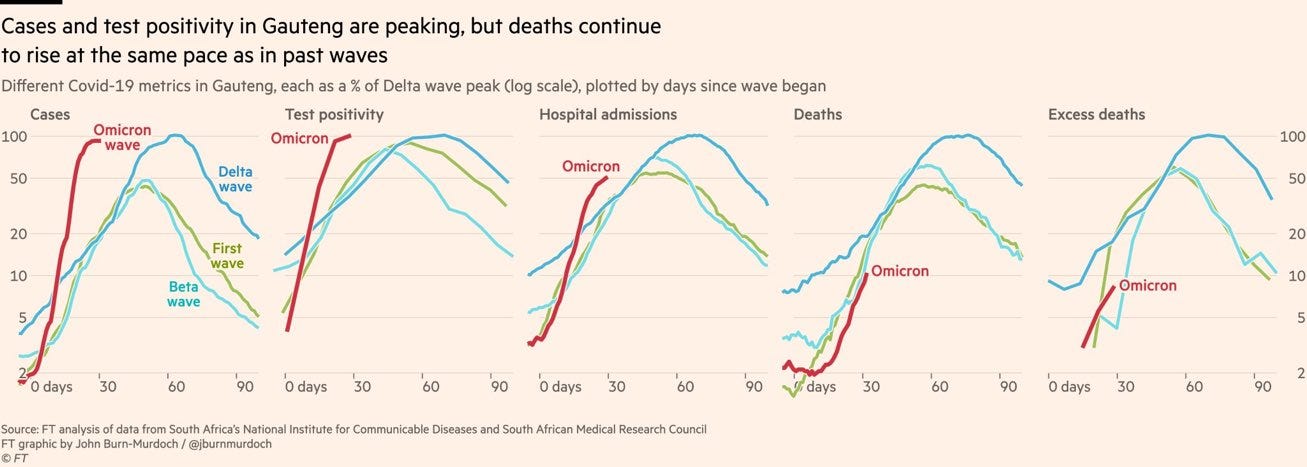
Here’s a Twitter thread with an optimistic perspective on the South African data on severity. One note is that it’s important to properly understand what this chart means:

As I understand it, in South Africa they test everyone admitted to the hospital for Covid-19 and those cases will count as admissions here. So the initial thought is that this spike could be explained by that, but maybe not?
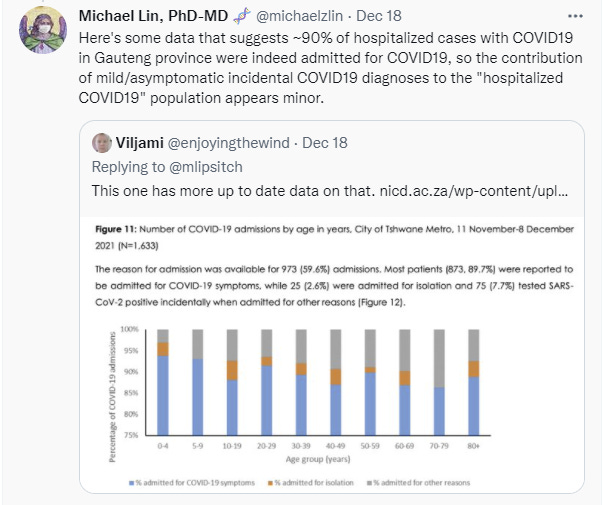
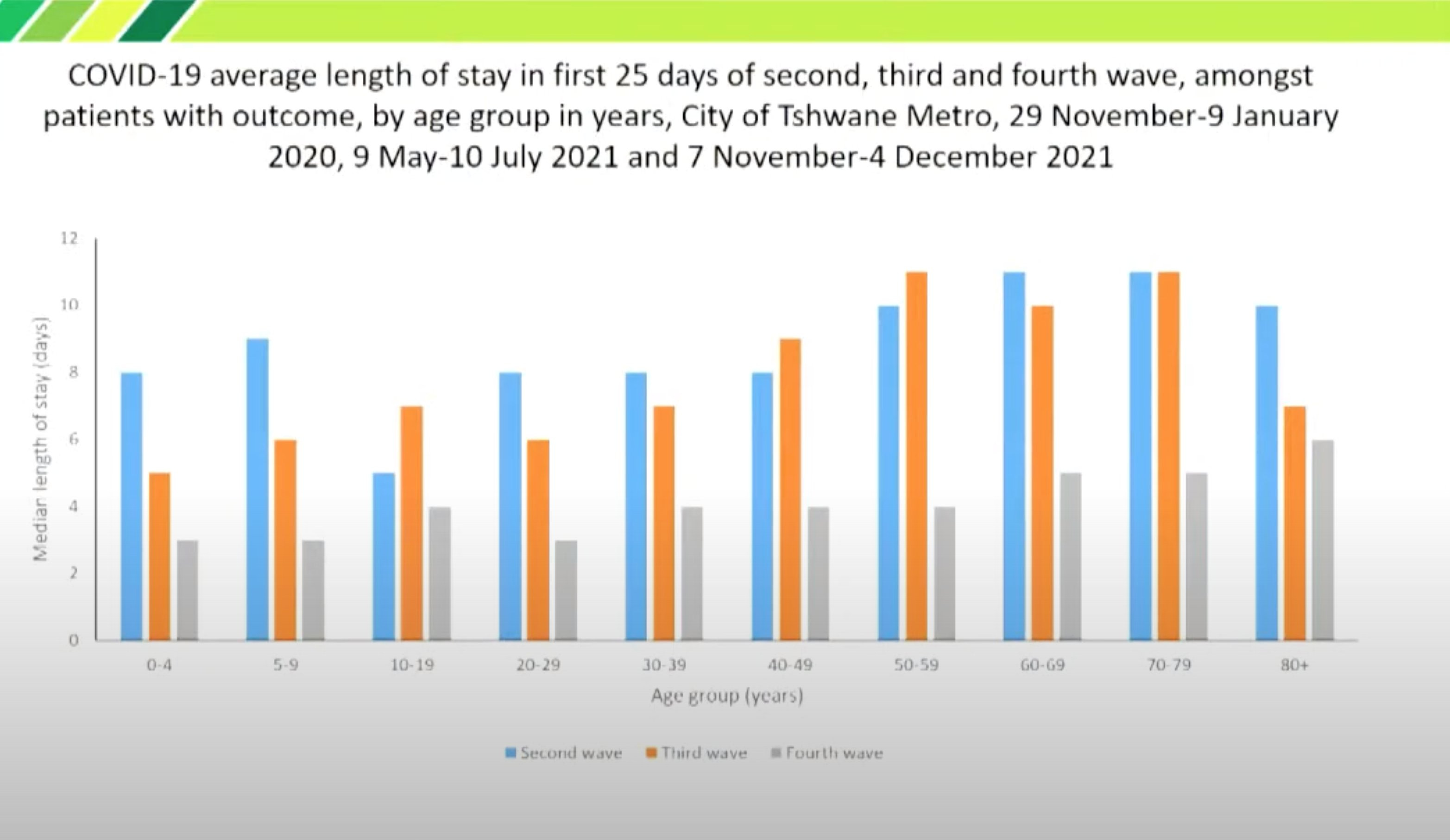
And of course there’s this, which corrects for age although not prior immunity, which does seem likely to be promising:
United Kingdom
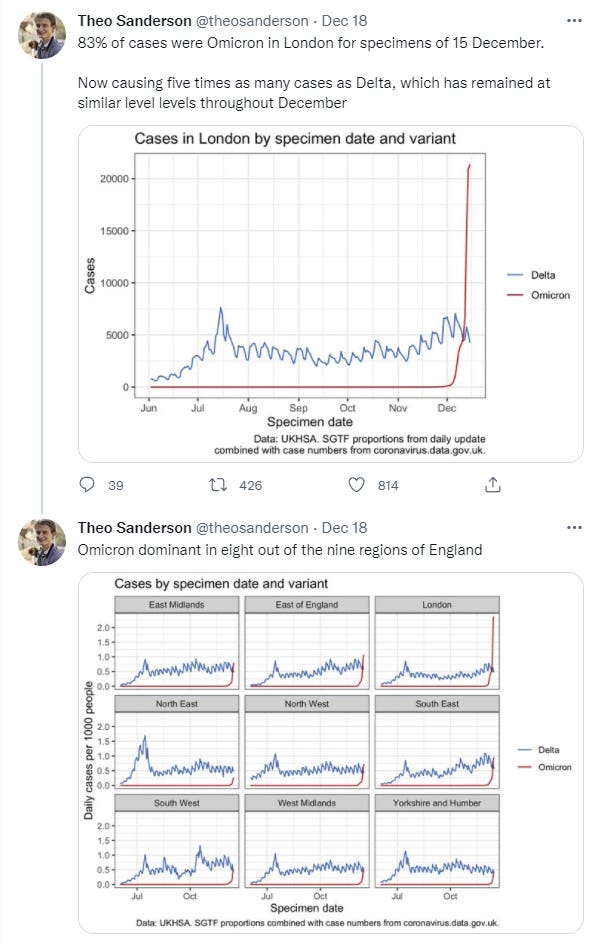
The UK files daily reports, which can be found here. Makes it very clear Omicron has taken over, and that big adjustments in behavior have happened that are rapidly taking care of Delta. This link will take you to the UK technical briefings.
There are some signs of hope, perhaps, but I don’t buy it.
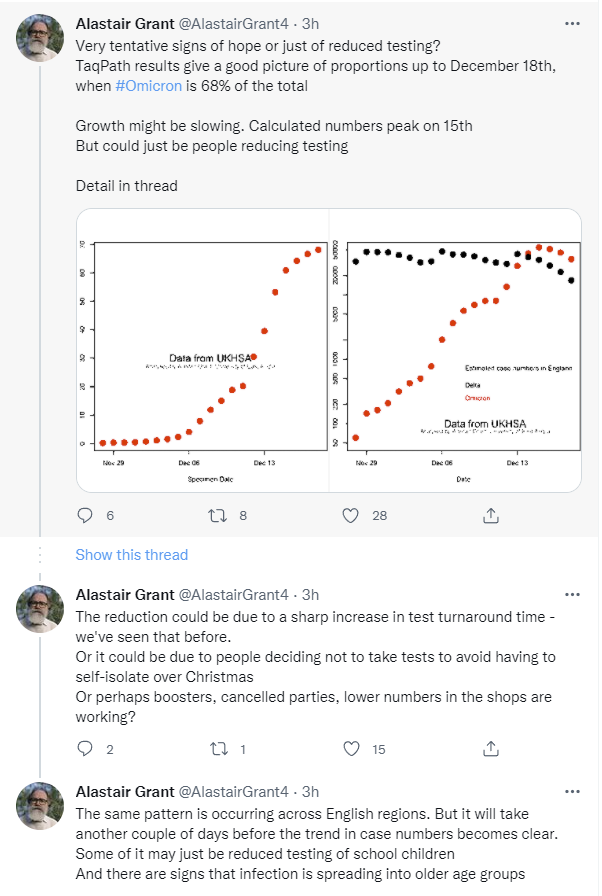
All this right after the big takeover:
For this to be turning this fast there would need to be dramatic shifts in behavior, without implementation of a government plan. I have a ton of UK readers now, wiping out the large majority of exposures, so have we seen those kinds of shifts? To what extent?
Grant notes that we are seeing this shift across regions. That shows it isn’t random, but London’s situation is dramatically different from areas that are well behind it. So why is everything hitting a plateau at the same time? And why does Omicron’s edge over Delta seem to have shrunk so much so quickly?
This could also be the data source being quirky for some reason, as I didn’t see the same thing reflected at OurWorldInData or in any obvious way by the numbers at BNONews.
Denmark
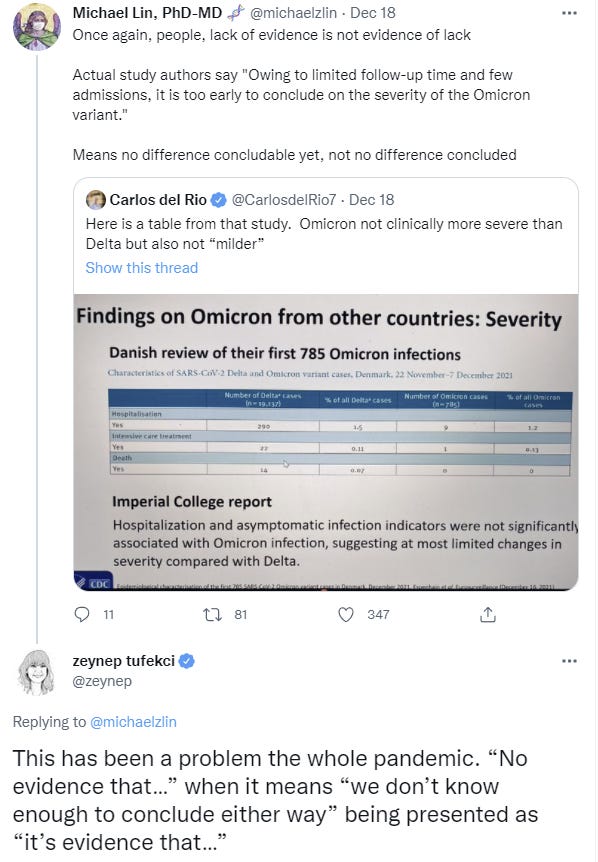
Data on severity in Denmark initially looked rather grim, and was jumped on by all the usual suspects. New data is less grim.
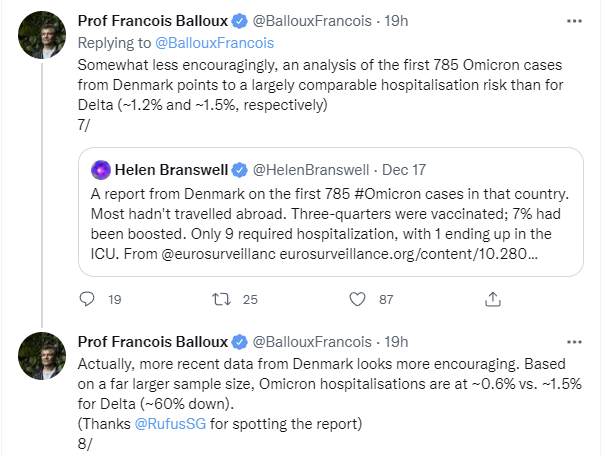
The new difference could easily disappear once we factor in reinfections and breakthroughs and age, but it’s hard to know, as opposed to the early data which would have indicated an importantly more severe strain and also would have contradicted other sources.
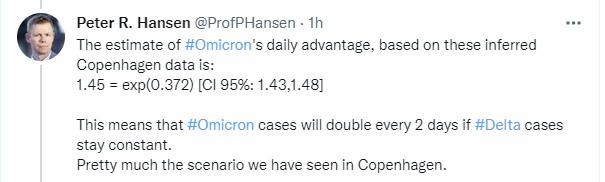
Copenhagen is by now mostly Omicron:

Around the World
New York Governor intends not to respond to Omicron with any shutdowns.
I do think such talk is meaningful but also expect it to come under extreme pressure when things get bad, if they get as bad as I expect. Meanwhile in NYC, protesters against vaccine requirements gathered at The Cheesecake Factory because people are who they are and it was a way to ensure no harm was done, and an increasing number of restaurants have been forced to temporarily shut their doors.
In Washington state, looks like Omicron has taken over.
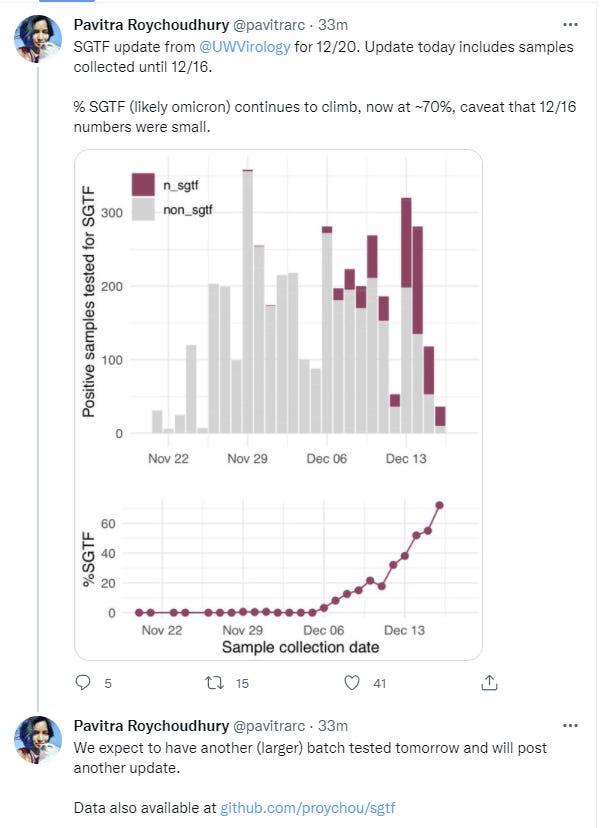
Again it does look like a big behavioral shift is driving down Delta, even though the last few days are presumably due to data lag.
In Australia, here’s one man’s story of what happened when he tried to go to a store one day and ended up in quarantine, with lots of confused officials scrambling to figure out the situation, first telling him to quarantine at home then telling him he has to go to a medi-hotel. The story definitely has that isn’t-it-Ironic feel to it, but the important thing is that they’re still trying to contain Omicron rather than giving up. I don’t see how that’s going to work, and the numbers do not look good.
At least they’re attempting to step up their game a bit and do things that could possibly work if they get massive model uncertainty in their favor, but it does not look like they are succeeding.
The English Study
Here’s the study everyone’s talking about that didn’t find evidence of reduced severity, but did find strong evidence of much more rapid spread and frequent reinfection. Let’s dig in.
Here’s their summary.
To estimate the growth of the Omicron variant of concern (1) and its immune escape (2–9) characteristics, we analysed data from all PCR-confirmed SARS-CoV-2 cases in England excluding those with a history of recent international travel. We undertook separate analyses according to two case definitions. For the first definition, we included all cases with a definitive negative S-gene Target Failure (SGTF) result and specimen dates between 29/11/2021 and 11/12/2021 inclusive. For the second definition, we included cases with a positive genotype result and specimen date between 23/11/2021 and 11/12/2021 inclusive. We chose a later start date for the SGTF definition to ensure greater specificity of SGTF for Omicron.
We used logistic and Poisson regression to identify factors associated with testing positive for Omicron compared to non-Omicron (mostly Delta) cases. We explored the following predictors: day, region, symptomatic status, sex, ethnicity, age band and vaccination status. Our results suggest rapid growth of the frequency of the Omicron variant relative to Delta, with the exponential growth rate of its frequency estimated to be 0.34/day (95% CI: 0.33-0.35) [2.0 day doubling time] over the study period from both SGTF and genotype data. The distribution of Omicron by age, region and ethnicity currently differs markedly from Delta, with 18–29-year-olds, residents in the London region, and those of African ethnicity having significantly higher rates of infection with Omicron relative to Delta.
Hospitalisation and asymptomatic infection indicators were not significantly associated with Omicron infection, suggesting at most limited changes in severity compared with Delta.
To estimate the impact of Omicron on vaccine effectiveness (VE) for symptomatic infection we used conditional Poisson regression to estimate the hazard ratio of being an Omicron case (using SGTF definition) compared with Delta, restricting our analysis to symptomatic cases and matching by day, region, 10-year age band, sex and ethnicity. We found a significant increased risk of an Omicron case compared to Delta for those with vaccine status AZ 2+weeks post-dose 2 (PD2) , Pfizer 2+w PD2, AZ 2+w post-dose 3 (PD3) and PF 2+w PD3 vaccine states with hazard ratios of 1.86 (95%CI: 1.67-2.08), 2.68 (95%CI: 2.54-2.83), 4.32 (95%CI: 3.84-4.85) and 4.07 (95%CI: 3.66-4.51), respectively, where PD3 states are categorised by the dose 1/2 vaccine used. Depending on the Delta VE estimates used (10), these estimates translate into Omicron VE estimates of between 0% and 20% PD2 and between 55% and 80% PD3 against Omicron, consistent with other estimates (11). Similar estimates were obtained using genotype data, albeit with greater uncertainty.
To assess the impact of Omicron on reinfection rates we relied on genotype data, since SGTF is associated with a higher observed rate of reinfection, likely due to reinfections typically having higher Ct values than primary infections and therefore being subject to a higher rate of random PCR target failure. Controlling for vaccine status, age, sex, ethnicity, asymptomatic status, region and specimen date and using conditional Poisson regression to predict reinfection status, Omicron was associated with a 5.41 (95% CI: 4.87-6.00) fold higher risk of reinfection compared with Delta. This suggests relatively low remaining levels of immunity from prior infection.
The headline takeaway is a doubling time of two days or less, with a 5.41-fold higher risk of reinfection, and declining vaccine effectiveness. Severity isn’t even mentioned here.
Which makes sense, because think about the timing. The study came out on December 16. There simply has not been enough time to know which cases were and were not severe, because it’s doubling every two days so >75% of the cases in the study are going to be from the previous four days, >87% from the last six.
What do they say about severity? This seems to be it.
The distribution of Omicron by age, region and ethnicity currently differs markedly from Delta, with 18-29 year-olds, the London region, and those of African ethnicity having significantly higher rates of infection with Omicron relative to Delta. Hence the crude ratios of hospitalisations to cases shown give no information on severity on their own since risk of hospitalisation increases markedly with age. Hospitalisation and asymptomatic infection indicators were not significantly associated with Omicron infection, suggesting at most limited changes in severity compared with Delta.
…
We find no evidence (for both risk of hospitalisation attendance and symptom status) of Omicron having different severity from Delta, though data on hospitalisations are still very limited.
That all seems sensible. Without controlling for things you get a result that is meaningless. After controlling for various things as best they could, what little data we have didn’t show a difference in severity, so this is some evidence against a strong difference in severity, but data is still very limited so it’s too early to draw conclusions.
Good work, everyone. So how’s it going to get covered?
Severity and Its Discontents
A common theme of many claims about the severity of Omicron is that there is ‘no evidence’ of reduced severity. This is obvious nonsense, and a prime example of the Law of No Evidence (for which I have now written a reference post), which is:
Law of No Evidence: Any claim that there is “no evidence” of something is evidence of bullshit.
Keep an eye out for this as we examine the evidence and how it is presented.
Here’s Reuters on 17 December, talking about the English study above:
Is that what even the post thinks the study said? Let’s check the opening paragraph.
The risk of reinfection with the Omicron coronavirus variant is more than five times higher and it has shown no sign of being milder than Delta, a study showed, as cases soar across Europe and threaten year-end festivities.
It doesn’t use the words explicitly, but this is the basic ‘no evidence’ move. The study didn’t show that Omicron is milder than Delta, so the study showed that Omicron is not milder than Delta.
Except that it did not do this. It did provide some evidence against such a hypothesis, especially stronger versions of it, by not finding an effect, but the study lacked sufficient power to draw much of a conclusion even on its own terms.
Infection gives you a lot more data, and thus a lot more power to learn something, such as the much higher risk of reinfection.
“Controlling for vaccine status, age, sex, ethnicity, asymptomatic status, region and specimen date, Omicron was associated with a 5.4-fold higher risk of reinfection compared with Delta,” the study, which was dated Dec. 16, added.
The protection afforded by past infection against reinfection with Omicron may be as low as 19%
…
Depending on the estimates used for vaccine effectiveness against symptomatic infection from the Delta variant, this translates into vaccine effectiveness of between 0% and 20% after two doses, and between 55% and 80% after a booster dose.
I am going to express deep skepticism that two doses provides 20% or less protection against infection by Omicron, but I can’t rule it out.
It is very clear from the body of the article, without having to look at the paper, that the paper was designed to measure likelihood of infection, and lacks the power to know about severity.
That is not about to stop headline writers. It is also not going to stop others who should know better, and are going to do this harder. For a central example, based on that same study, apologies for the source but in context seems right to use it:
Notice the alchemy here. Study finds Omicron could be just as severe, therefore implicitly it is just as severe. The attack on those who have said otherwise as having ‘endangered’ people is used to make this leap without committing a direct logical fallacy, while also enforcing the norm that no one is allowed to make guesses that could possibly understate a somber and to be taken seriously Public Health Threat, the same way one can’t be allowed to overestimate one when it’s not yet an official threat and might Cause Panic.
This is his quoted passage and his highlighting, not mine, here’s the original FT article although you have to scroll down a bit and the link might stop working after a while:

The could be is even underlined.
Here he is later on the same thread:
So not only is it endangering people to say ‘mild,’ even if it’s milder, it would still be terrible to say that, because it wouldn’t be milder than some other third thing? Wait, why are we still discussing this?
Maybe it’s because Omicron did not evolve from Delta, which is by itself strong evidence for the prior that it’s probably milder. Why should Omicron’s baseline assumed severity be that of Delta rather than that of the strain it evolved from?
Then he says the quiet part out loud.

You’re off message, you need to stop being off message, and we’re going to cast out anyone seen being off message.
And is that off message? Because ‘mild’ implies not taking things seriously, but exponential growth means even a mild version could get really, really bad, which is totally true.
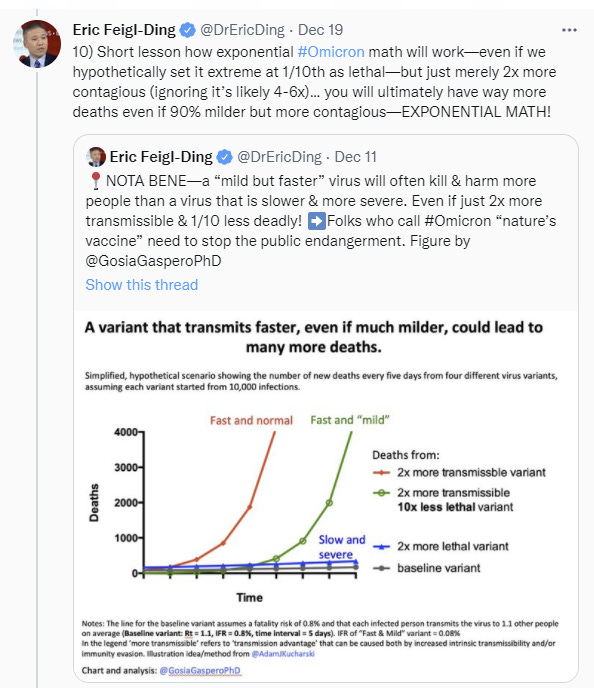
So yes. If you have ten or a hundred times as many cases, being milder only goes so far, and exponential growth still kills a lot of people. That doesn’t mean the right thing to do is start lying about the situation. Lying keeps backfiring, and we keep noticing this yet thinking it might work for us.
Nate Silver’s quote tweet response is simply (link):

Here’s another similar thread, with the same air of certainty and superiority, rubbing the failure in the face of anyone who doubted this obvious result.

That was the default assumption by everyone, despite Omicron not having come from Delta, until we saw evidence that suggested otherwise, and that is indeed how the Bayesian prior works. We see once again this pattern of someone saying ‘how dare you have considered the possibility of milder Omicron,’ despite that of course being in the prior, and accusing people of asserting it was milder when almost everyone instead merely said it might be milder, or that we’d seen some evidence of milder.
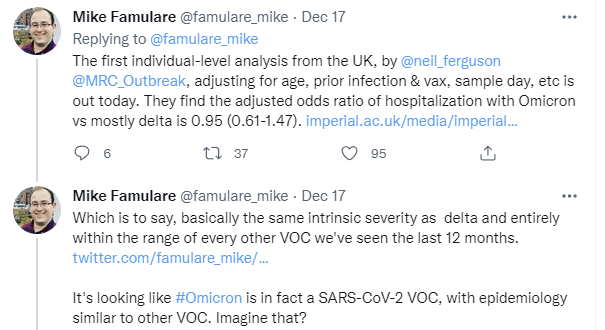
The thread improves then, because it cites other data sources.
And then the goalpost moving, once again.
Suddenly, when the issue is the term ‘milder’ Delta and 2019-nCoV are grouped together and treated as the same. Whereas the ‘at best’ language makes it clear that they are not the same and he agrees with this. The difference is substantial and important. If Omicron is about as severe as 2019-nCoV, both that seems like it should have had a substantial amount of weight in our prior, and it’s also meaningfully good news.
It seems, once again, like such Very Serious People think that the word ‘mild’ will give the wrong idea of magnitude and/or cause behaviors they don’t like, and thus the concept must be blocked out and destroyed and those promoting it shamed.
Here’s the transformation in one easy step.
Here’s an analysis of what was actually found that seems more appropriate.
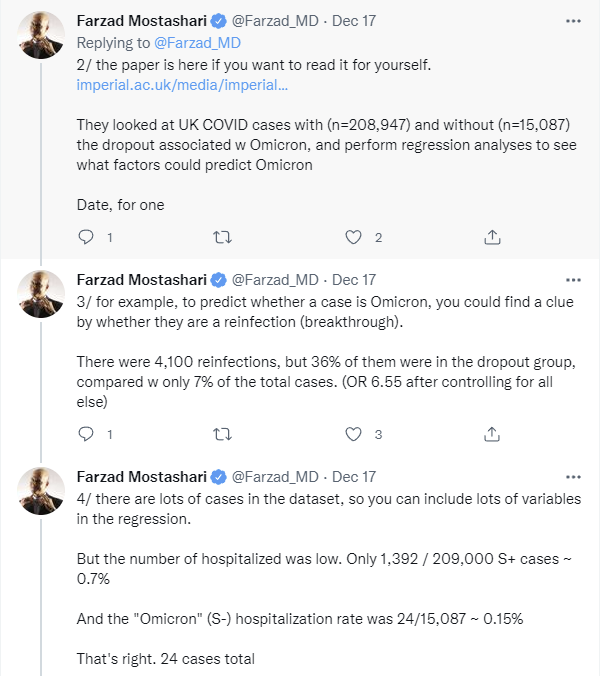
So, yes, to let you get this straight, there are only 24 hospitalizations from Omicron in this sample. That’s it. It was 0.15% of cases instead of 0.7%. After various adjustments that came out about even, which is plausible, there are a bunch of big adjustments to make, but this is nothing like big enough to rule much out that we hadn’t already ruled out. It is very little useful evidence on severity, although again it was useful evidence on spread.
My take based on current evidence is that we can rule out dramatically milder versions, we can rule out substantially more severe versions, and the question is whether this represents something like original strain or is similar to Delta, and we still don’t have that answer.
Spread
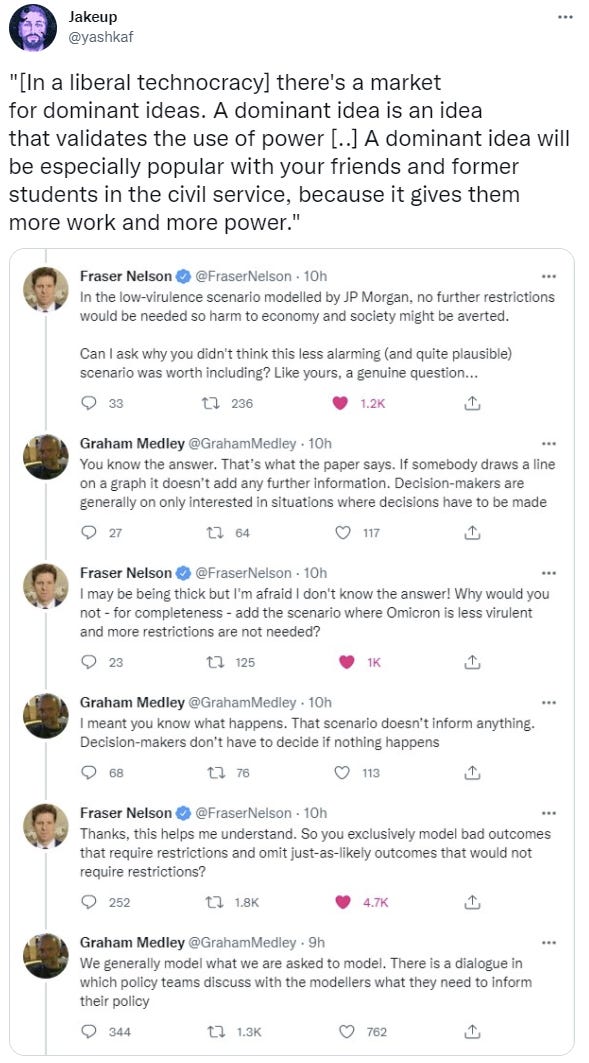
Policy Response
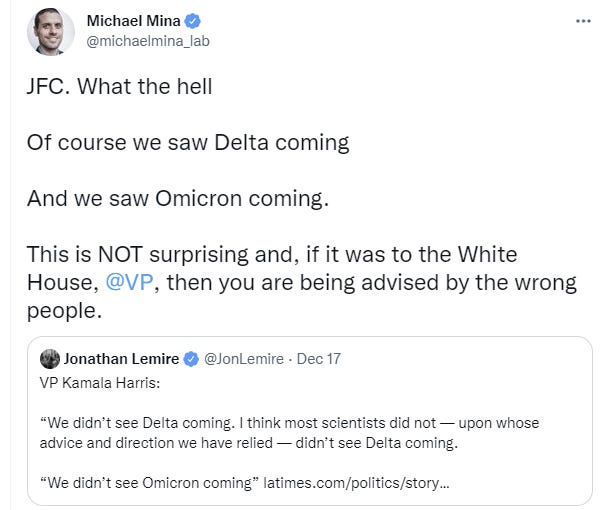
The Biden Administration is scrambling to respond to Omicron.
You see, they didn’t see it coming, just like they didn’t see Delta coming.
That seems very much like a their failure to see things problem.
Seriously, Madam Vice President, if it’s this bad, have your people call me.
You can look over the track records to see exactly who did and did not ‘see this coming’ to what extent. I didn’t put that high a probability on an Omicron-like variant two months ago, this is true, but this kind of pleading is at best unbecoming.
They did finally come out with a statement, and oh boy is it a statement.
That’s a truly impressive amount of contempt and condemnation for a large percentage of the population. Good luck with that lack of disruption thing, and also at the midterms.
Other than that, their response is to ignore what is about to happen, not do anything to substantially increase testing capacity or to facilitate treatment, downplay case counts and tell people to focus on severe disease and death.
“We’re getting to the point now where … it’s about severity,” said Xavier Becerra, the secretary of the Department of Health and Human Services, in a meeting with reporters this week. “It’s not about cases. It’s about severity.”
…
“There’s a degree of difficulty that now comes in trying to decide what means it’s severe and what you have to do to stay out of that threshold of severity,” Becerra said. “But I think that’s where we’re heading, is to try to be able to tell the public that.”
They will keep the emphasis on vaccination and boosters, which like love are all you need.
“For the unvaccinated, we are looking at a winter of severe illness and death for the unvaccinated — for themselves, their families and the hospitals they’ll soon overwhelm. But there’s good news: If you’re vaccinated and you have your booster shot, you’re protected from severe illness and death,” the President said.
Always emphasize that ‘we have tools.’
“We have the tools to fight this virus, including Omicron, and we’re in a very different and stronger place than we were a year ago and there is no need to lock down,” Zients said this week.
There are two classes of tools, the Good Tools and the Bad Tools.
Vaccines, boosters, masks, social distancing and isolating when sick are The Good Tools. Those are indeed good tools.
Paxlovid, other treatments, rapid tests and any additional restrictions that people associate with ‘lockdowns’and updated boosters for Omicron are the Bad Tools, which must never be mentioned. If we mentioned them, people might be less inclined to vaccinate, so Very Serious People are acting as if they represent an infohazard. I would like to say this wouldn’t mean we’re going to actively deny people medicine, but Paxlovid remains illegal, and testing is backing up to the point of uselessness in large part because the FDA refuses to approve many tests that are in widespread use in Europe.
I continue to be happy that few are reckoning with the implications of exponential growth, despite the resulting large quantity of obvious nonsense, because the reactions I would otherwise expect would cause far more harm than good.
I continue to be highly frustrated by the refusal to take testing or treatments seriously, especially given this (in my opinion wise) decision to mostly give up on containing Omicron. There’s always time to make things somewhat better, but mostly we have already missed our window.
Meanwhile, man are these people thinking small.
Becerra said during the meeting with reporters that the administration may need to ask Congress for more funding to combat the pandemic, citing the unknowns of the new variant.
“Are we going to have more than $10 billion worth of needs and costs on Covid, especially in regards to testing?” Becerra said. “There’s a strong chance we will, depending on where Omicron takes us.”
Ten billion dollars is nothing. We had a stimulus for six trillion. It’s crazy that we’re even blinking at ten billion in real costs.
There’s also a variety of the usual two-steps-behind speculations and talk about what ‘may’ happen in January that we are reasonably confident is going to happen next week.
A reminder that the Biden administration wanted everyone boosted, and the FDA said no. The invisible graveyard is once again visible, and once again about to get larger.
Threads and Articles
Not quite this, but I had a volunteer to help as a research assistant. Too early to know if it will work out, but one of the first assignments was to chart R0 in various places using the data available, and you can check out the results here. This could be the start of something big. You never know.
NPR interview with Dr. Ashish Jha. General optimistic attitude from Jha, including flat dismissal of the possibility of lockdown, and despite skepticism from the interviewer. Doesn’t seem to grapple with the way exponential growth works, and his optimism on tests doesn’t appreciate how backed up the system already is let alone how bad it’s about to get.
Science general summary from 17 December. Optimistic on severity, points out that at sufficient scale things still get ugly. Frustratingly still refusing to admit Omicron is more infectious in addition to having escape properties, both of which seem like settled issues by now.
Trevor Bradford thread analyzing vaccine and booster effectiveness. It is looking more and more like the booster shot makes you dramatically better at fighting Omicron than the initial shots, probably because the two-shot method was never right to begin with. If you haven’t gotten your booster, strongly consider doing so, and definitely do not attempt to wait for an updated vaccine.
Trevor Bradford thread on doubling times.
Ewan Birney thread from 18 December on general state of play from UK perspective.
Kai Kupferschmidt thread from 17 December, giving an overview of what is to come. Broadly endorsed.
Christina Pagel thread from 17 December on the situation in the UK and Ireland.
Thread predicting the whole wave won’t be a big deal, as a contrasting viewpoint. Claims highly reduced severity. I am deeply skeptical but want to offer all points of view.
Reminder that displacement of Delta will not be quick, we’ll have both around at once. It is possible it will not be complete either.
Atlantic points out the obvious, which is that We Are Not Ready for Omicron.
Retrospective
Lot of the people who gave out warnings and/or were complaining about ‘vaccine equity’ are taking victory laps like this, or others are granting the laps on their behalf.
It continues to be a huge scandal that we did not scale up vaccine production faster, and that we did not distribute our surplus faster and better. In the future we must do better. That does not mean that those who effectively said ‘you should stop giving out shots or boosters because equity’ should be taking victory laps. Additional paid-for demand increases supply, and those boosters are looking more efficient per person than initial shots at this point, and the idea that we should let our lives be seriously disrupted on this basis never made sense.
There’s also the continuing question of the origins of Omicron. If Omicron had evolved from Delta, then it would be reasonable to mutter something about ‘vaccine equity’ to the extent that we could have reduced global cases farther and faster. But Omicron didn’t come from Delta, and there are major hints that it came from Covid-19 jumping into mice and then back somehow and we can combine that with its huge number of mutations and, well, you tell me what exactly we should be worried about here.
Outlook
Probability Updates and Predictions
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 90% → 85%.
The various ways in which Omicron looks potentially to have been halted imply the potential for a much reduced generation time (aka serial interval) for Omicron, which would allow what we’ve witnessed without the need for a super large transmission advantage. Thus, it seems somewhat more plausible we won’t fully hit 100% after the initial wave.
Chance that Omicron is importantly more virulent than Delta: 3% → 3%.
Chance that Omicron is importantly less virulent than Delta: 60% → 50%.
I do think that the evidence this past few days was modestly in favor of similar virulence to Delta, but I did not find it conclusive or especially strong.
Will the CDC label Omicron a variant of high consequence before 2022? 11% → 9%.
This number hasn’t adjusted for the time that has passed, and it should have. Slightly rich market.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30%.
The Europeans did order the shots, but the ‘we’ here was intended to be Americans, and it seems like we’re not interested for now. That could easily change, though.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 35% → 30%.
The hospitals are at capacity now, but the early promising signs (or more exactly, the lack of signs of either panic or truly horizontal lines) makes me somewhat less concerned that we’ll be unable to handle things. So I’m mildly more optimistic that we’ll ‘get away with it.’
I would like to add new probabilities to the list as better intuition pumps, but I’m not fully well at the moment, so I’m going to hold off on that at least for now.
33 comments
Comments sorted by top scores.
comment by Pattern · 2021-12-21T04:38:20.227Z · LW(p) · GW(p)
I continue to be happy that few are reckoning with the implications of exponential growth, despite the resulting large quantity of obvious nonsense, because the reactions I would otherwise expect would cause far more harm than good.
I continue to be highly frustrated by the refusal to take testing or treatments seriously, especially given this (in my opinion wise) decision to mostly give up on containing Omicron. There’s always time to make things somewhat better, but mostly we have already missed our window.
Pretty sure you can't have your cake and eat it too.
comment by Adam Zerner (adamzerner) · 2021-12-20T23:46:11.865Z · LW(p) · GW(p)
I have fallen mildly ill, as have my wife and son. So far we don’t have a positive Covid-19 test, and everyone is maximally vaccinated, but given the timing the obvious conclusions do seem likely.
Sorry to hear that. Good luck. Would you mind sharing what if anything you are doing to prepare, given the symptoms? Vitamins/supplements? Drugs?
Replies from: Zvi↑ comment by Zvi · 2021-12-21T00:14:13.573Z · LW(p) · GW(p)
As noted earlier, so far D and Zinc. If I do test positive I'll add Fluvoxamine. Otherwise, taking it easy, staying hydrated and all that, and probably that's the end of it. Don't actually have a test yet. Could easily be a normal cold.
Replies from: Benito, adamzerner, CraigMichael↑ comment by Ben Pace (Benito) · 2021-12-21T01:04:13.453Z · LW(p) · GW(p)
In case this is not common knowledge: PSA that you can just buy a bunch of antigen tests on Instacart from local stores like walgreens and CVS, they come in a couple of hours, they take 15 mins to get results.
I have used many hundred such tests at this point from managing a large office in the last year, it should never be hard for you to get yourself tested, we always have them around the office and people can just use them whenever they need. I guess households have less need for them than offices and events and so don't keep like 40 in stock, but seriously the world is easy enough that it should take like <4 hours to get tested when you want to get tested.
Replies from: Zvi↑ comment by Zvi · 2021-12-21T01:23:55.473Z · LW(p) · GW(p)
Not as true as it was two weeks ago. Binex tests are sold out everywhere and the others are not on local store shelves.
Replies from: Benito↑ comment by Ben Pace (Benito) · 2021-12-21T02:05:06.623Z · LW(p) · GW(p)
Maybe I’m out of touch, and it’s spiking atm. For the last six months every time I’ve tried it’s been available for me (like 10 times).
Replies from: Zvi↑ comment by Adam Zerner (adamzerner) · 2021-12-21T05:20:02.289Z · LW(p) · GW(p)
Thanks!
↑ comment by CraigMichael · 2021-12-21T00:55:11.472Z · LW(p) · GW(p)
Do you have any specific thoughts on inhaled budesonide?
Wishing you and your loved ones a speedy recovery!
comment by ardavei · 2021-12-21T08:07:04.374Z · LW(p) · GW(p)
I don't think the Danish numbers are comforting at all, and I believe that the tweeter is comparing apple to oranges. The latter numbers cited, which are now at 91/18941 (0.48%) versus 1794/127060 (1.41%), are the total number of admissions in patients testing positive between 22. November and 15. December. Since the 14. And 15. of December have most of the positive Omicron cases, but the Delta cases are more spread out, we should expect the number of hospitalized Omicron cases relative to Delta in this cohort to rise as the disease runs its course.
Second, the characteristics of the Omicron patients bias the data. As expected, the proportion of unvaccinated cases is much higher for Delta (23.8%) versus Omicron (8.6%). But additionally, the age distributions of cases are different, with more than double the proportion of Omicron cases in the 20-29 cohort and consequently fewer in the very young and very old cohorts.
Considering these factors, I think it's unlikely that Omicron will turn out to be more than 20-25% less severe than Delta, which is what was found in the initial analysis.
The current data from Denmark can be found here: https://www.ssi.dk/-/media/cdn/files/covid19/omikron/statusrapport/rapport-omikronvarianten-20122021-9j51.pdf The Danish CDC releases these reports daily, and they can be found at their website ssi.dk (in Danish, but it should be manageable to navigate).
I hope that you get better soon.
comment by Omer · 2021-12-21T06:55:35.512Z · LW(p) · GW(p)
The meme "Omicron is milder than Delta" was rapidly spreading to the point of being regarded as a common-knowledge fact. Countering it with "there is not evidence that Omicron is milder than Delta" was (and still is) a valid refutation.
And not just in the technical/statistical sense, but also in a principled sense, meaning "this is nothing but a wild guess and wishful thinking, and there's simply no reason to think that".
This will change in the next 2 weeks (or sooner). But currently, the idea that it's milder is just a baseless hypothesis, not an educated guess.
Replies from: GWS↑ comment by Stephen Bennett (GWS) · 2021-12-21T15:08:44.366Z · LW(p) · GW(p)
That simply isn’t true:
-
omicron likely mutated from the wuhan variant instead of the delta variant, which was slightly less severe (and so our new prior should be centered on the wuhan variant)
-
the hospitalization data that is available lends modest evidence of it causing slightly less severe disease.
As far as I know, that’s most of the evidence we have, and from it my educated guess is that it tends to cause slightly less severe disease than delta. It could be about as bad or much less severe, but both of those scenarios seem unlikely. That’s an educated guess! It’s very similar to the educated guess Zvi gives at the end of this very post.
You may well be right that some people were jumping the gun, but the people I heard talking about it being milder were expressing an educated guess with appropriately flagged uncertainty.
Replies from: Omer↑ comment by Omer · 2021-12-21T15:44:07.493Z · LW(p) · GW(p)
First, the variant is still new relative to the time we've observed for the transition from "cases" to "hospitalizations" and "deaths". Additionally, the data we do have seems to indicate that the prognosis could be slightly different (symptoms appear earlier, replication is slower in the lungs...). And on top of this, high proportion of cases is of vaccinated, boosted and reinfected.
The signals that point towards the "milder virulence" hypothesis are drowning in noise. It could be that it is indeed milder, and I hope as much as anyone for this outcome. Still I stand by my above statement: currently, it's wishful thinking.
comment by ChristianKl · 2021-12-21T13:47:04.153Z · LW(p) · GW(p)
With EU approval of Novavaxx, I think we can add it to the list of bad FDA decisions not to approve it and thus provide no vaccine for people who want to vaccinate but don't want vector or mRNA vaccines.
comment by Nanda Ale · 2021-12-21T19:13:30.065Z · LW(p) · GW(p)
There are two classes of tools, the Good Tools and the Bad Tools. Vaccines, boosters, masks, social distancing and isolating when sick are The Good Tools. Those are indeed good tools.
Paxlovid, other treatments, rapid tests and any additional restrictions that people associate with ‘lockdowns’and updated boosters for Omicron are the Bad Tools, which must never be mentioned. If we mentioned them, people might be less inclined to vaccinate, so Very Serious People are acting as if they represent an infohazard.
Paxlovid:
"SCOOP: The FDA is set to authorize the Covid-19 treatment pills from *both* Pfizer and Merck. An announcement is expected this week. It would open up two significant treatment options for severe cases. A big milestone."
https://twitter.com/josh_wingrove/status/1473318224204910593?s=20
Some testing movement:
"The White House is also purchasing 500 million at-home Covid tests that Americans can order for free through a website starting in January."
https://www.cnbc.com/2021/12/21/omicron-us-to-deploy-troops-to-hospitals-purchase-500-million-covid-tests.html
comment by Pattern · 2021-12-21T04:57:41.477Z · LW(p) · GW(p)
There’s also the continuing question of the origins of Omicron. If Omicron had evolved from Delta, then it would be reasonable to mutter something about ‘vaccine equity’ to the extent that we could have reduced global cases farther and faster. But Omicron didn’t come from Delta, and there are major hints that it came from Covid-19 jumping into mice and then back somehow and we can combine that with its huge number of mutations and, well, you tell me what exactly we should be worried about here.
Lot of ifs. Sure we aint gonna vaccinate mice. (Yet.)
Before reading the links: You can be worried about both. More ways variants can happen means more variants. And more variants means more things that can kill you.
After reading the first link: I'm starting to wonder why we didn't have more pandemics (that were worse). And if maybe it's because we didn't have more pandemics (that were worse). If jumping back and forth changes things a lot, then the more that happens, it seems like the worse it gets.
After reading the second link: How many labs are we going to find out about before this is all over?
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-21T07:24:03.589Z · LW(p) · GW(p)
I think culling is more likely. If you have a pet snake, God help you
comment by Pattern · 2021-12-21T04:40:43.630Z · LW(p) · GW(p)
A reminder that the Biden administration wanted everyone boosted, and the FDA said no.The invisible graveyard is once again visible, and once again about to get larger.
We should do a thread (or a thing where people write posts instead of comments) where people share stories about the past re: graveyards that did and didn't happen.
comment by Pattern · 2021-12-21T04:37:18.040Z · LW(p) · GW(p)
Serious People are acting as if they represent an infohazard.
Maybe it's time someone wrote "“Infohazard” is a predominantly mistake-theoretic concept". Perhaps, "I know better than those foolish mortals, and they must not know the truth or they might make mistakes (like not doing what I want/worship me)."
(No offense to Bostrom, but usage isn't controlled by him because...he isn't the only person using it anymore.)
comment by Pattern · 2021-12-21T04:30:59.086Z · LW(p) · GW(p)
Seriously, Madam Vice President, if it’s this bad, have your people call me.
It looks like an indirect quote. And wasn't there something about indirect quotes not being accurate? (I haven't checked if it's 'the same group', in either sense.)
comment by Pattern · 2021-12-21T03:42:59.692Z · LW(p) · GW(p)
A common theme of many claims about the severity of Omicron is that there is ‘no evidence’ of reduced severity. This is obvious nonsense, and a prime example of the Law of No Evidence (for which I have now written a reference post), which is:
Law of No Evidence: Any claim that there is “no evidence” of something is evidence of bullshit.
When I initially read that in the reference post, I disagreed with it - due to the wording. In this context, I have the same view:
Law of No Evidence: Any one who claim that there is “no evidence” is bullshitting.
This is a rather strong statement.
"No Evidence" Heuristic: Any one who claim that there is “no evidence” is out of time out of touch.
comment by tkpwaeub (gabriel-holmes) · 2021-12-22T17:32:47.479Z · LW(p) · GW(p)
Looks like you're gonna have to tweak your "Paxlovid still illegal" evergreen! It's legal for me because I'm fat
comment by wangscarpet · 2021-12-22T03:00:40.208Z · LW(p) · GW(p)
How would you go about getting a high-risk person close to the front of the line for pavloxid treatment? I was really heartened to see the news about imminent approval because a very high-risk family member was recently exposed, but I think without hustle he would definitely not get it in time. I plan to call hospitals in his area tomorrow -- anything else?
comment by Pattern · 2021-12-21T04:33:44.372Z · LW(p) · GW(p)
That’s a truly impressive amount of contempt and condemnation for a large percentage of the population. Good luck with that lack of disruption thing, and also at the midterms.
What about people who are vaccinated and whose immune systems aren't as good? (What about people who are vaccinated and their immune systems are fine?)
comment by Pattern · 2021-12-21T03:30:46.635Z · LW(p) · GW(p)
I have fallen mildly ill, as have my wife and son. So far we don’t have a positive Covid-19 test, and everyone is maximally vaccinated, but given the timing the obvious conclusions do seem likely. Wish me well, and hopefully Christmas will not be cancelled and I can keep the posts mostly going. I do have winter break to help me out.
(This question is for everyone.)
Suppose you, the reader, get sick. And you get a fast, negative, covid test.
- What are the odds you have covid?
- How do you find out if you do?*
*If the rapid test had some probability of success, like 70%, then if you took two test you might figure 1-(1-.7)^2 = 1-.3^2 = 1-.09 = 01% you have covid. But are the rapid tests independent?**
**Even if they were, how does probability a test comes back positive vary over time if you have covid?
- How much/what evidence do you need to figure you have covid even if a test comes back negative?
- VOI, another test still makes sense (even if only to ease your nerves). However, suppose you knew in advance you wouldn't be symptomatic. How often/when should you take a test for other's sake when you have nothing at stake yourself?
↑ comment by tslarm · 2021-12-22T10:01:59.281Z · LW(p) · GW(p)
But are the rapid tests independent?
Definitely not fully independent. This paper has some data on the correlation between false-negative % and viral load:
in all groups, CareStart sensitivity followed Ct value distribution, with 96.3% sensitivity observed in all participants with Ct ≤25 and 79.6% in those with Ct ≤30. Although false-negative CareStart results were largely confined to those perhaps least likely to transmit SARS-CoV-2, the sensitivity of the CareStart test by Ct threshold cutoff was lower than observed in our recent study of the Abbott BinaxNOW in the same testing site [6] (99.3% with Ct ≤25, 95.8% with ≤30, and 81.2% with ≤35).
(Higher Ct values indicate lower viral loads.)
↑ comment by denkenberger · 2021-12-22T05:55:14.065Z · LW(p) · GW(p)
*If the rapid test had some probability of success, like 70%, then if you took two test you might figure 1-(1-.7)^2 = 1-.3^2 = 1-.09 = 01% you have covid. But are the rapid tests independent?**
You need to start with a prior for this calculation. This paper also discusses independence of tests. And I think you meant to write 91%.
Replies from: Pattern↑ comment by Pattern · 2021-12-22T16:19:40.322Z · LW(p) · GW(p)
Why would there be a 91% change you have covid if two (statistically) independent tests say you DON'T have it?
Replies from: denkenberger↑ comment by denkenberger · 2021-12-23T23:33:41.406Z · LW(p) · GW(p)
I believe your calculation was 70% chance of not having it given a negative test, so if you have two independent negative tests, that would be 91% chance of not having it (1 - 0.09), or 9% chance of having it. But in reality, false negatives are very common. And you need to start with a prior probability to update from. From the paper I referenced, if you have some symptoms and were exposed, the prior probability of having COVID might be 91%, but after one negative result, you are still at 77-80% probability of having COVID. However, if your symptoms don’t match the common ones for COVID or if you don’t know you were exposed, then the prior probability of having COVID is much lower to start with. Then a negative test result would update downward slightly from that prior.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-21T13:50:30.949Z · LW(p) · GW(p)
I wonder if they're more independent when you alternate brands
comment by Yunxiang Zhu (yunxiang-zhu) · 2021-12-21T01:36:35.839Z · LW(p) · GW(p)
More public-health measures should be taken, since boosters modified for Omicron may not.