Covid 7/15: Rates of Change
post by Zvi · 2021-07-15T17:10:01.985Z · LW · GW · 63 commentsContents
The Numbers Predictions Deaths Cases Vaccinations Delta Variant Israeli Data UK Data Transmissibility American Data In Other News None 64 comments
Cases rose by over 60% in America this week, and we’re seeing large jumps in cases around the world. I am highly suspicious about the jump in the rate of increase, but Delta certainly seems to be the real deal, and this was well above my expectations.
I worry that recently I’ve lacked sufficient skin in the game. Everyone I personally care about is vaccinated or young enough that they don’t need vaccination, so the real sense of danger is largely gone. The worry is about the reaction to Covid, rather than about Covid itself. But that’s a very real danger, and I have back that sense of ‘oh no, things could go very wrong’ because there’s the danger that we really will blow up our way of life over all this, and go into a permanent dystopia of sorts. That’s what we need to ensure does not happen.
Thus, the bulk of this post is a numbers analysis trying to figure out what we know about Delta’s transmissibility and the effectiveness of vaccines in reducing that transmissibility, using data from a variety of sources. Others are encouraged to continue this analysis and try to get to the bottom of this.
So let’s run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 3.3% (up 0.4%) and deaths increase by 7%.
Result: Positivity rate of 4.8% (!) and deaths increase by 15%.
Prediction for next week: Positivity rate of 4.7% (down 0.1%) and deaths unchanged.
The null prediction is always an option, here two distinct null predictions with distinct reasoning. For deaths it’s clear that there was a reporting gap as predicted, so I do not think the death rate last week represents things getting worse, but they likely should start to get worse given Delta is deadlier and cases have stopped dropping within the required time window, and it doesn’t seem like last week’s number was too artificially high.
The case number is trickier, as there’s good reasons to think the data is distorted, either by July 4 or otherwise:
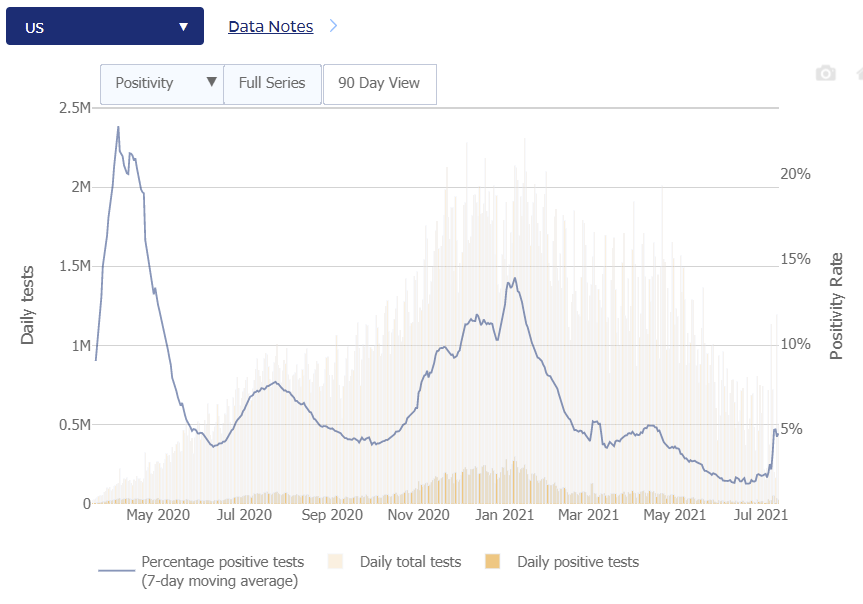
That giant spike represents going from an average of 2.6% to an average of 5.0% over two days. That’s not a thing that should happen to seven day averages. If it does, then the next five days things should continue to rise as old data cycles out for new, but that didn’t happen so far.
Perhaps July 4 was truly a superspreader event in the way that previous holidays were almost always underwhelming, as much as the previous holidays make that seem unlikely. Perhaps it’s a giant delayed data dump that didn’t include negative tests. It is hard to say. What I do know is that either things were worse than this before the jump and the low number wasn’t fully real, or the jump and new number are not fully real – one of these two numbers is misleading.
Thus, we have the standard question when a number seems to clearly overshoot, where it’s unclear where the ‘real’ number is and how fast it’s moving, so it’s unclear where it will end up. In this case, substantial real growth seems almost certain, and I definitely feel like the null prediction here is ‘chickening out’ but I’m not sure which direction to go, although I notice I’m more comfortable predicting a small reversion than an increase, while noting that such a decrease wouldn’t be ‘real.’ Thus I’m choosing a very small decline, with discussion continuing in the cases section and the Delta section, but this data doesn’t make sense.
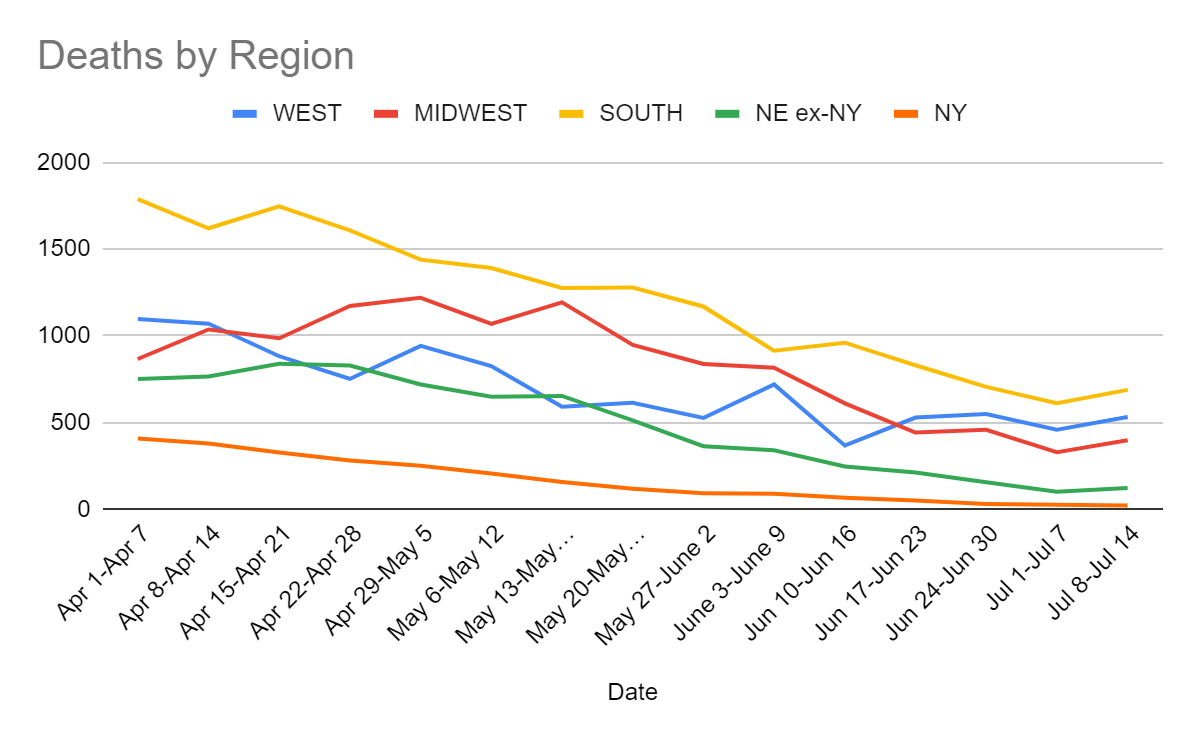
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| May 27-June 2 | 527 | 838 | 1170 | 456 | 2991 |
| June 3-June 9 | 720 | 817 | 915 | 431 | 2883 |
| Jun 10-Jun 16 | 368 | 611 | 961 | 314 | 2254 |
| Jun 17-Jun 23 | 529 | 443 | 831 | 263 | 2066 |
| Jun 24-Jun 30 | 550 | 459 | 706 | 186 | 1901 |
| Jul 1-Jul 7 | 459 | 329 | 612 | 128 | 1528 |
| Jul 8-Jul 14 | 532 | 398 | 689 | 145 | 1764 |
Cases
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| May 20-May 26 | 33,890 | 34,694 | 48,973 | 24,849 | 142,406 |
| May 27-June 2 | 31,172 | 20,044 | 33,293 | 14,660 | 99,169 |
| Jun 3-Jun 9 | 25,987 | 18,267 | 32,545 | 11,540 | 88,339 |
| Jun 10-Jun 16 | 23,700 | 14,472 | 25,752 | 8,177 | 72,101 |
| Jun 17-Jun 23 | 23,854 | 12,801 | 26,456 | 6,464 | 69,575 |
| Jun 24-Jun 30 | 23,246 | 14,521 | 31,773 | 6,388 | 75,928 |
| Jul 1-Jul 7 | 27,413 | 17,460 | 40,031 | 7,065 | 91,969 |
| Jul 8-Jul 14 | 45,338 | 27,544 | 68,129 | 11,368 | 152,379 |
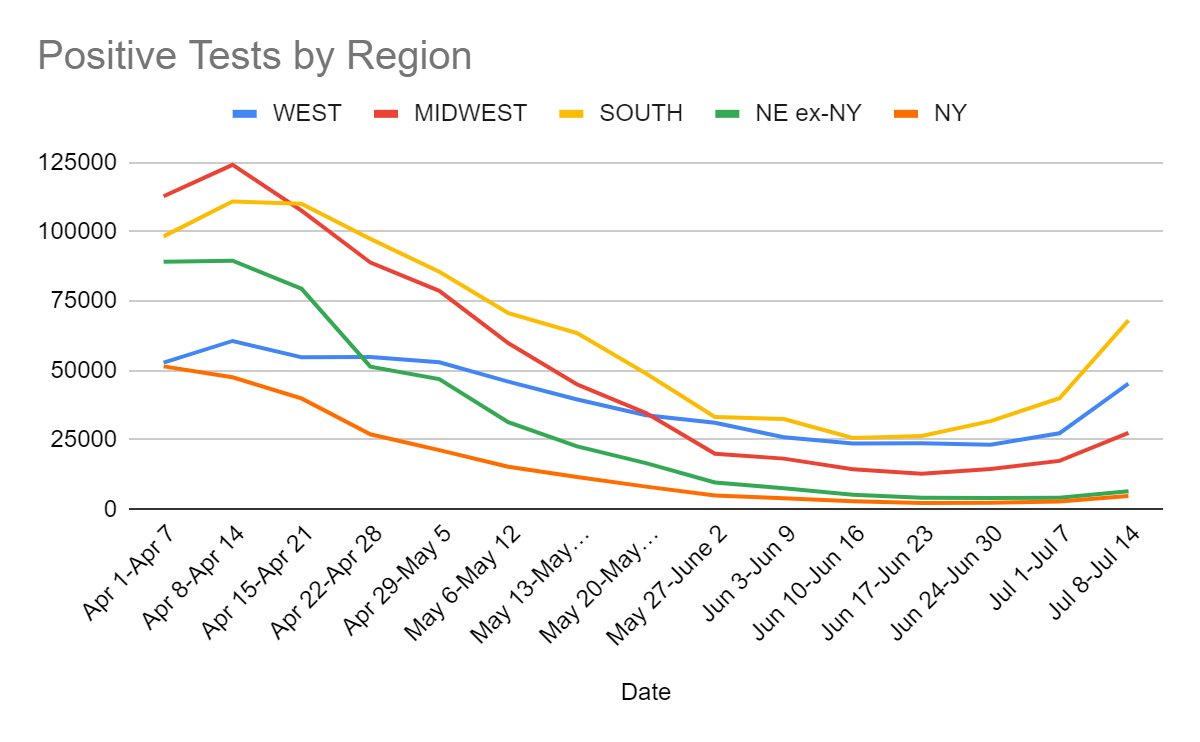
Cases are up by 66%, and the positive test rate is up by 65%, which implies the number of tests was constant.
The more I think about this, the less sense it makes.
If cases were up by anything like 66%, why aren’t we running more tests? Aren’t people testing in large part based on whether they suspect they have Covid, and whether they have symptoms or known exposures, which both should be up a lot? Are we somehow supply constrained on this, despite no observations of difficulty in getting testing done on demand? How do these numbers make any sense?
Thus, I come to the conclusion that the numbers don’t make sense, and don’t belong in the same universe. If cases double test counts should rise a lot, and that not happening is super weird.
For now, I’m going to mostly ignore the test percentages and act as if the raw positive test counts are more accurate, because if there’s one thing I definitely don’t believe, it’s the reported number of negative tests. That doesn’t make any sense no matter how bad things are.
One possible way for this to kinda sorta work is that perhaps there are people who get tested in order to show a negative test, whose tests get reported every time, and people who get tested because they want to actually know if they have Covid, who mostly only report when they’re positive. Then, doubling the size of the second group doesn’t change reported test counts much? That’s the best I can come up with.
What should we make of the 66% rise in cases? How much of it might be timeshifted and in what ways? Is this a fully real rise, and should we expect it to continue? If so, what happened?
Discussion of all that will continue in the Delta section, where I attempt to reconcile all the various different data points.
Vaccinations
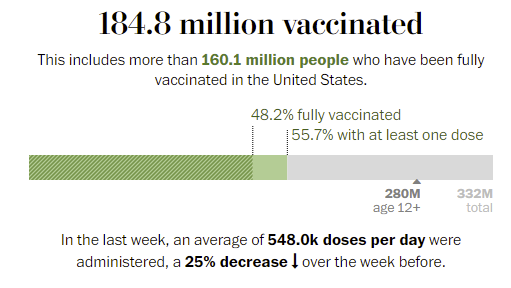
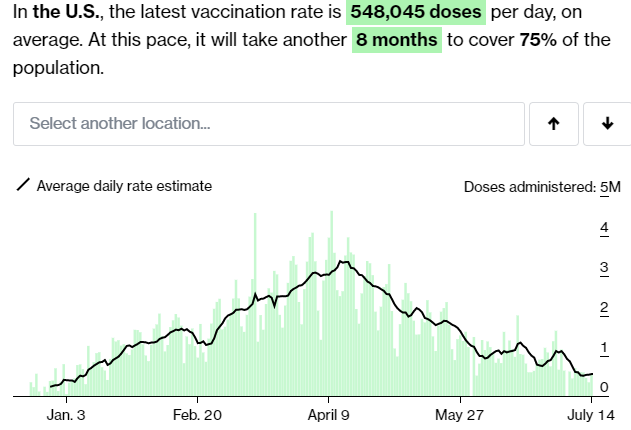
Given no attempts to halt the course of events, this is a strong result.
There’s a new warning on J&J shots (WaPo), because there were about 100 detected cases of an autoimmune disorder out of 12.8 million shots. There was one (1) death involved, again out of 12.8 million shots. It will be an interesting control group for the previous experiment where J&J got suspended. If we take a side effect that doesn’t matter, and treat it like it exists but doesn’t matter, does that have an impact? Versus treating it as a huge freaking deal and freaking out everyone and suspending the vaccine, which we are pretty sure had a fairly large impact the last time there was a side effect of magnitude epsilon.
New paper says that neither ‘give people fact box’ nor ‘explain how mRNA vaccine was developed and that it wasn’t too fast’ impacted vaccine hesitancy. Kudos for publishing the negative result. Why aren’t we seeing a lot more studies like this of various things one might do?
Then there’s the question of what is happening in Tennessee (news article).

The explanation I found was that in Tennessee teenagers can get vaccinated without ‘parental consent’ and this was creating problems. Which does not seem like much of an explanation, as there’s no reason why such consent should be required or even relevant. And certainly does not explain why this applies not only to Covid-19, but to all vaccinations period. Or why they think it makes sense to strip teenagers out of lists for reminder postcards if they’re scheduled for their second shots, but focus on the other vaccines part of this, if you’re considering that this all might have a perfectly logical explanation.
Perhaps we can at least partially salvage this by taking advantage of the ‘natural experiment,’ and observing what happens to vaccination rates. Do the reminder postcards do anything? What about the other things that got suspended? What happens to the vaccine rates for other diseases? If you can’t go with ‘prevent people from getting sick and dying’ you can at least upgrade your world models.
Genius in France: Incentives Matter!
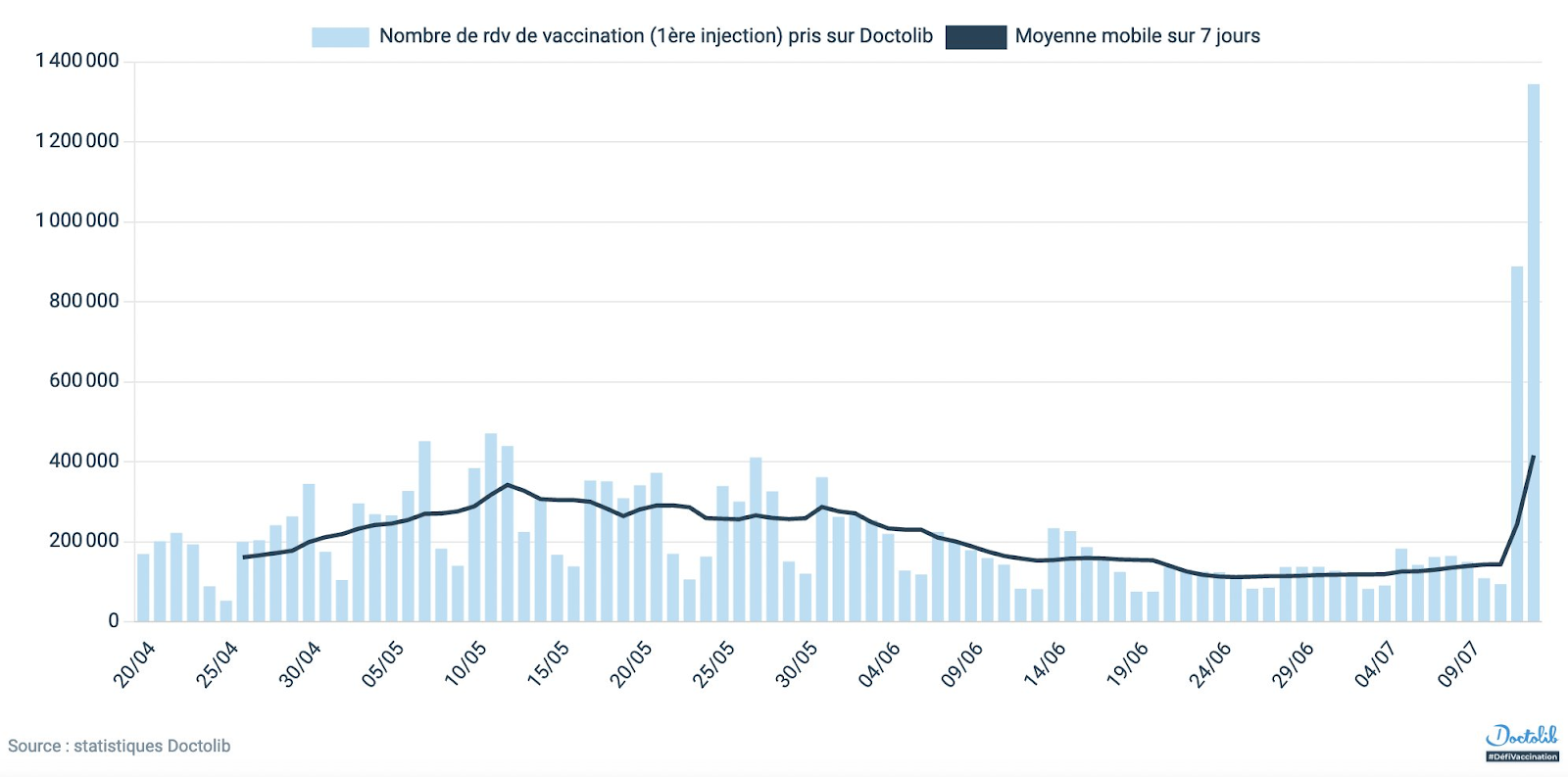
The second day exceeds the first, so those 2.2 million appointments are likely only the beginning. It’s one thing to pass up a vaccine, it’s another to pass up the ability to participate in many aspects of life. Make no mistake. If implemented, this will work.
If America’s Delta problem gets sufficiently worse that they start bringing restrictions back, and they don’t start requiring proof of vaccination in such situations but instead once again halt life for the rest of us, I call upon all of us to find this completely unacceptable, the same way I find permanent child masking unacceptable.
In such a scenario, there are two sane choices. You can either let people do what they want, or severely restrict what the unvaccinated can do. Ending life as we know it, presumably indefinitely, shouldn’t be even potentially on the table, nor should we have any tolerance for such proposals.
Delta Variant
A post entitled Delta Variant: Everything You Wanted to Know does make a real attempt to be exactly what it says on the tin. The graphs are rather cherry-picked to make things look as bad as possible, as are a number of other discussions, but the data is all legitimate. The question of the day is now exactly how bad Delta is and making sure our models of it are right to figure out what is to come. There’s a bunch of superficially contradictory data that must be reconciled, as there usually is.
Taking stock of those data points is the logical first step.
Israeli Data
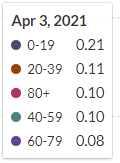
Israel offers the scariest data point, suggesting greatly reduced vaccine effectiveness.
I’ve seen the Israeli data presented in slightly different ways but this is basically what they’re reporting there. I’d like to note that the story doesn’t make sense, even on its own.
For previous strains, this is saying that vaccination wasn’t protective against hospitalization, and mostly wasn’t protective against death, once someone was infected (93% reduction vs. 93% reduction), or at least once someone tested positive. We knew even then this wasn’t remotely the case.
Then with Delta we get this gigantic drop to 64% protection against infection, but then protection against hospitalization stays at 93% and protection against death rises? So conditional on infection, this is saying hospitalization protection went from ~0% to 80%? Really?
Even the 79% number seems very very strange when looked at this way alone.
You could tell a story that justifies it. In that story, vaccine protection works 96% of the time (and there’s measurement errors), and if that happens you’re protected against severe outcomes no matter which variant you face because that wasn’t a close call, but being infected at all is a lower threshold. Before, if you were successfully vaccinated you basically never got infected (in this model), whereas now if you are vaccinated you sometimes do still get infected, but it’s never serious whereas before it never got that far in the first place. Then there’s the 4% of people for whom the vaccine doesn’t work properly, who are still at real risk. Or something like that.
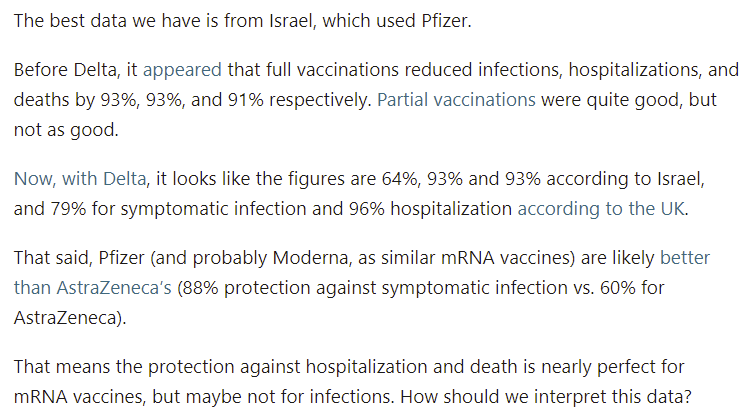
As a sanity check, what happens if we ignore the reports and attempt to back out the answer from the raw data on infection numbers?
That’s not a picture one can easily read, so click the link if you want to examine it.
Reminder:

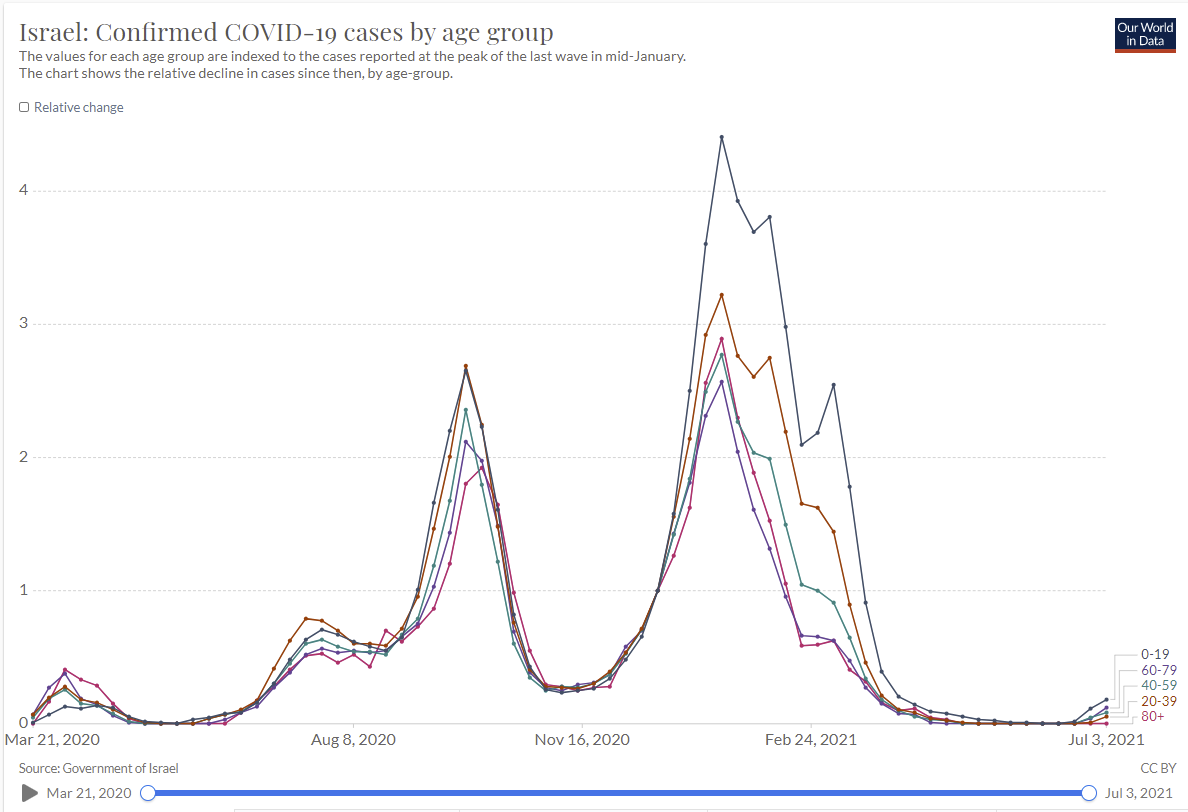
There are a lot of confounders, but let’s start with the pre-vaccine comparison.
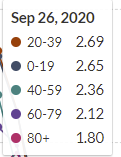
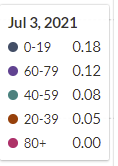
Next, let’s do a pre-Delta comparison, from when the numbers were very low, but people were mostly vaccinated:
Consider this a ‘post-vaccination’ equilibrium. Many of the young aren’t vaccinated, whereas most of the old are, so the ratios change, but almost entirely for the youngest group. Things were mostly level before otherwise, and remain mostly level now, in roughly the same order.
Now let’s look at the last day they have data for here:
It’s unfortunate we don’t have the July 10 data, but we go with what we have. This still has to represent almost all Delta cases, and gives us apples-to-apples comparisons. What can we infer from these numbers?
Also, how does this reconcile with this graph?
Israel is young, but it’s not that young, and my response to the above graph is more like ‘those sample sizes are all absurdly small because Israel didn’t have Covid that month.’ Still seems difficult to reconcile in the details, but easy in the bigger picture.
My conclusion is mostly that this is muddled enough that I can’t draw a fixed conclusion. Especially weird is the 60-79 range. One possibility is that the vaccine needs a threshold of effectiveness to prevent infection, and it’s still mostly good enough to hold off Delta, but those with weakened immune systems are in a different situation and they are mostly very old? But the share of vaccinations in such groups is still super high compared to younger groups, and the order of these groups still seems really odd. It would, however, explain how 20-39 could be the lowest major group while 0-19 is the highest, perhaps – The kids in their 20s can still largely get vaccinated, and their immune systems are still strong, so it’s highly effective? Whereas with the 40-59s it’s less effective especially on the high end, and so on.
We should also look at case counts in Israel. On June 18 they had 1.92 cases per million, right before things started rising, on June 14 it was 65.09, for R0 = 1.97. From previous data, we can presume that when Delta was a very small portion of Israeli cases, the control system adjusted things to something like R0 = 1, so we’ll keep that number in mind.
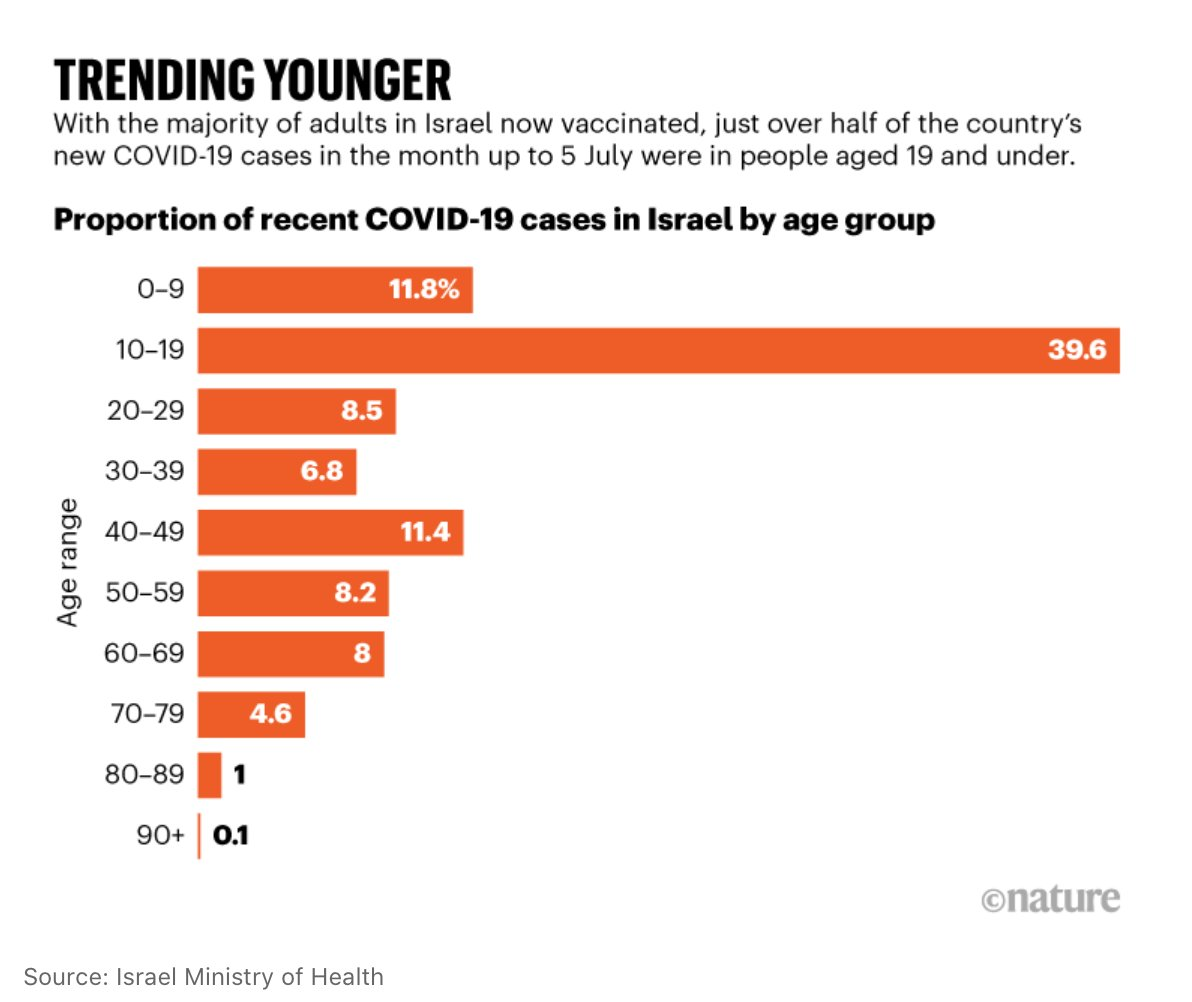
UK Data
We can presume that Alpha hasn’t increased its absolute numbers, so at this point UK is almost all Delta. On May 25 there were 35.7 cases per million. On July 14 there were 512.9, On July 4 there were 361, so the two-week R0 = 1.19. From May 25 to July 4 we get R0 = 1.32, despite a bunch of Alpha early on, so the control system has been adjusting, but also we never see a period with an extreme R0 in the UK. In April, they had Alpha and things were stable (R0 ~ 1). For an extreme situation, let’s look at relatively early lift-off of Delta and assume a base of about 30 Alpha that doesn’t count for growth rate, and start when total cases are at double that, or 60, which is June 4. Over the next 10 days things went to 107, so let’s say that this represents Delta going from 30 to 77, before much adjustment has been made, over two cycles. That would give an estimate of R0 ~ 1.60, on the high end of the range for increased base transmissibility. It doesn’t leave that much additional room. One more cycle gets us to 131, which would be R0 ~ 1.31 for Delta alone, so presumably there were adjustments being made already then.
Transmissibility
There’s the question of how much more deadly Delta is than older strains, but I’m mostly going to ignore it because it doesn’t impact the path of the pandemic much. The question is containment versus lack of containment. If Delta is twice as deadly, that’s quite bad, but it’s an isolated question. As commentators have pointed out, the data supporting the increased deadliness is not that solidly grounded. The extra viral loads are suggestive, and the early data does look like it’s more deadly for a given unvaccinated person, but our data remains not great.
The much more key variable is transmissibility of Delta versus Alpha or the original strain. I’ve been using a 120% increase, or 2.2x (220% of original infectiousness) for Delta, and a 1.4x (140% of original) for Alpha, which continues to match estimates I’ve seen. Those all presumably refer to transmissibility among the unvaccinated and ignore the vaccinated population, and I’ve been treating the numbers accordingly. I see no reason to change that methodology, but that means that we need to reconcile our numbers with the case counts that we see.
An open question is how tight the bounds are on such numbers. If we have a model where things were previously going fine and then you ‘multiply by Delta’ then the bounds are reasonably tight. However, if you think that behaviors are adjusting in real time and seasonality causes ‘random looking’ ebbs and flows naturally, then there’s room for the data to look highly misleading, and my position at this point is if anything is closer to that second view.
Either way, your model has to make predictions whose math checks out, and that’s a good place to start.
Let’s say we accept that Delta’s ‘multiplier’ is 2.2, versus the old baseline, and Alpha’s is 1.4. Now let’s suppose vaccine effectiveness is reduced from 95% to 65%. What happens? Given current vaccination rates, with an adjustment for children, that’s about another 50% increase in the rate of infections.
That would mean that Alpha to Delta is a full effective +120% increase in the rate of infection, on top of the increase from original to Alpha, or a final factor of around 3.3. Or, alternatively, it would have a ‘base’ R0 of something like 6, with a vaccine that only reduced that for the vaccinated to 2, which would mean that even in fully vaccinated populations this would double every five days under pre-pandemic behaviors.
Set aside for the moment the question of what we would want to do about that. How does it line up with the data?
In the UK, where the Delta problem is currently largest and we are confident Delta is essentially the whole pandemic (using Our World In Data as my source), we had 36 cases/100k on May 25, and 494 on July 14, 52 days later, or just over 10 cycles, and R0 ~ 1.28. During April and the first half of May, we saw the number of cases stay roughly constant within a factor of 2, so R0 > 0.9. We could factor in some increase in vaccinations, but if Delta taking over sent R0 from 0.9 to 1.28, that’s only a 42% increase, similar to what we’d expect from Delta taking over from Alpha, minus some existing more infectious strains and some extra vaccinations, give or take behavioral adjustments and seasonality.
None of this matches the greatly reduced effectiveness hypothesis, unless you presume that behaviors are substantially adjusting during this period, but the shape of the curve isn’t suggestive of that either.
American Data
In the last week, America has seen a 66% increase in cases. As discussed above, going +10% then +20% then +66% is extreme, and can’t be explained by Delta alone. The share of Delta cases can only rise by about 30% in one week, even under extreme assumptions (e.g. from 35% to 65% or something like that, would be the theoretical limit) so a +46% effect in seven days off a 30% rise would mean Delta was at least twice as transmissible as Alpha. It also means the numbers in previous weeks would have shown a bigger problem, since the displacement of Alpha by Delta has to be gradual – there’s no way there was three times the growth in Delta this week that there was last week, because math.
Overall, though, the number isn’t crazy – if we presume that the control system had already adjusted for our vaccinations and for Alpha. If we take the +66% number seriously, and compare it to the pre-Delta situation, it’s safe to presume that we had previously stabilized under a full-Alpha situation, then +66% in a week represents a 43% rise in transmissibility from Delta versus Alpha minus any extra vaccinations, so 50-60% total, which doesn’t even leave room for the vaccines to lose effectiveness since that’s our estimate range for Delta already among the unvaccinated.
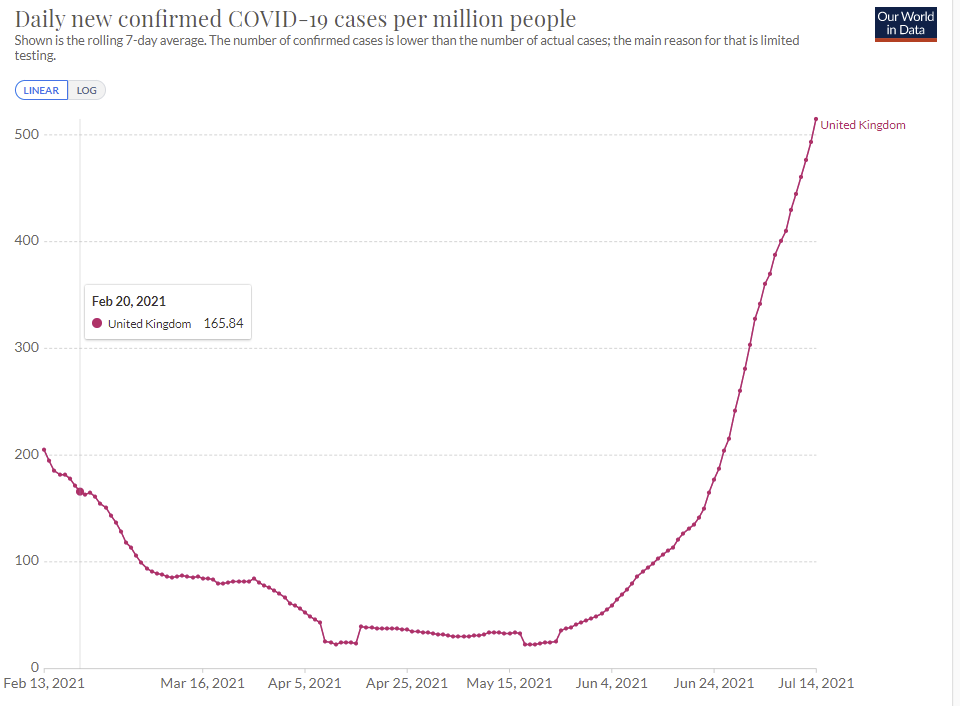
Under such assumptions, we can backchain, and it matches up with the sample data claiming that by percentage there wasn’t much Delta running around in early June, despite Delta now having taken over and now being 85%+:
An alternative calculation would be to look only at Alpha, or to compare Alpha to Delta. We have a percentage for it, so we can back out its growth in absolute numbers. It was something like 60% of cases on June 15 by this graph, and is now down to 5%. Whereas Delta went from roughly 4% to 85%.
From June 15 to July 15 is thirty days. Thirty days allows for six serial intervals. So if all of that is accurate, we get a ratio of 2.5:1, or +150% increased infectiousness, which is even higher than the +120% estimate for the full effects previously measured. We then look at absolute numbers, and see Alpha having an R0 = 0.75 over this period, versus R0 = 2.25 for Delta. Which would mean that both we’ve taken a lot more precautions recently than we did before to get things that low, and also that Delta should be doubling every four days, yet cases over the last week only rose by 66% despite starting off with the majority being Delta.
Thus I don’t believe the chart above is a representative sample – the math doesn’t add up.
One can have a hypothesis that strains crowd each other out in some sense but I don’t think the base rates are high enough for that effect to be big right now.
Then again, as I’ve been noting, if you take the numbers too seriously (as in, you don’t think there are big hidden factors and random distortions) then none of this adds up.
So where does that leave us? Can we put bounds on things?
Our lower bound should presumably be that Delta is 50% more infectious than Alpha, but that vaccine effectiveness is mostly unchanged.
Under Israeli conditions, it seems mostly safe to say that Delta is at most twice as infectious as Alpha, but that about twice is possible. This is the scariest data set.
Under UK conditions, it seems mostly safe to say that Delta is at most 75% more infectious than Alpha, and it would be difficult to get to a doubling.
Under American conditions, it seems mostly safe to say that Delta is going to be less than twice as infectious, given everything we know – the math starts to fold in on itself if we get above 75% or so, in the sense that things need to look much worse than they do. I’d put a soft bound around 75%.
We could also look at any number of other places. Israel and UK are especially picked because they’re well-vaccinated and having trouble.
Now let’s look at vaccination rates. Using Bloomberg’s ‘enough for X people’ metric, Israel is around 60%, the UK is also around 60%, and the USA is at 52.4%. That’s out of the full population, which includes children, so effective vaccination rates are somewhat higher especially for Israel (which has a younger population), and one dose is more than half of two doses, so the USA is effectively closer to 60%, and we can put Israel and the UK closer to 67% in terms of our effective percentage.
Let’s presume that in the base case, vaccinated people are 96% protected in terms of transmission. If we presume that the unvaccinated transmit at a 50% higher rate, but that the effective increase is 100% in Israel, that would give a vaccine effectiveness versus transmission of 67%. If we take the UK and presume 75% increased transmission, that implies vaccine effectiveness versus transmission of 80%. For the USA, a 75% increase in transmission would imply 76% vaccine effectiveness versus transmission.
It is possible, in theory, that this difference could be that vaccine effectiveness against transmission fades somewhat over time, and the difference here would be that Israel vaccinated earlier than other countries did.
If things were instead at our lower bound, by assumption, vaccines would remain at 96% effective.
It’s really hard to put bounds on things given all the factors we can’t account for, including control system adjustments in both directions, seasonality, and so on and so forth.
These are likely not tight bounds. There are likely a lot of behavioral adjustments involved in all of this. But it’s all very noisy, and I haven’t seen other serious attempts to figure this out. I’m encouraging everyone to take a stab at this from various angles and see what you find. There’s tons of data to work with.
If this reduced effectiveness is near those upper bounds, there is a very large problem. Even fully vaccinated populations wouldn’t be able to fully return to normal if you wanted to avoid Covid outbreaks. You’d either accept that vaccinated people and children often get Covid, and it would be fine, or you’d need to impose restrictions forever, or you’d need to get a new more effective vaccine distributed in the form of booster shots. And that’s if you got close to 100% coverage, which is not going to be happening.
Thus, the question would become, if Covid is not done with us, can we decide to be done with Covid and that life beckons, or are we actually going to kill our civilization and way of life over this despite having a vaccine that renders Covid mostly harmless?
In Other News
Fox News has generally not been as anti-vaccine as its customer base likely would have preferred, but some evidence that this may no longer be true. If I have any regular viewers reading this, can you update us?
Reasonable thread laying out different questions surrounding booster shots, which oddly still leaves out the question of whether shots can be modified to work better versus Delta. I’m confused why there isn’t more discussion about that. My presumption is that modifications wouldn’t help, which is interesting in and of itself and seems worthy of mention if true.
Deal between Israel and South Korea where Israel gives Pfizer shots now that it couldn’t use and were going to expire, gets future shots in exchange because selling things for money is evil. Post (from MR) points out that Covax’s quest to allocate vaccines equally is going to end up wasting a lot of vaccine, as many places don’t have the means to distribute the shots they’ll get.
Moderna begins a trial for yearly mRNA shot that would combine vaccines for flu, COVID-19, respiratory viruses RSV and HMPV. It turns out that not only does mRNA allow us to cure a wide variety of diseases, it lets us cure all of them at the same time, because the technology allows the payloads to be delivered together. I’d be a little concerned about short term side-effects similar to the ones with the current Covid vaccine, but my hope is that the problem can mostly be solved by proper dosing.
This is also an excellent way to give people Covid booster shots without everyone freaking out. If one shot, once a year, can deal with a wide variety of problems, that should work great, so long as the misinformation from anti-vaxxers doesn’t cause too many problems.
New Zealand didn’t secure enough vaccine shots, which is unfortunate, but is taking the AZ -> Pfizer booster path seriously, which is great.
You don’t often get to pick your allies, such as in the war on school. Or is it the war on children?

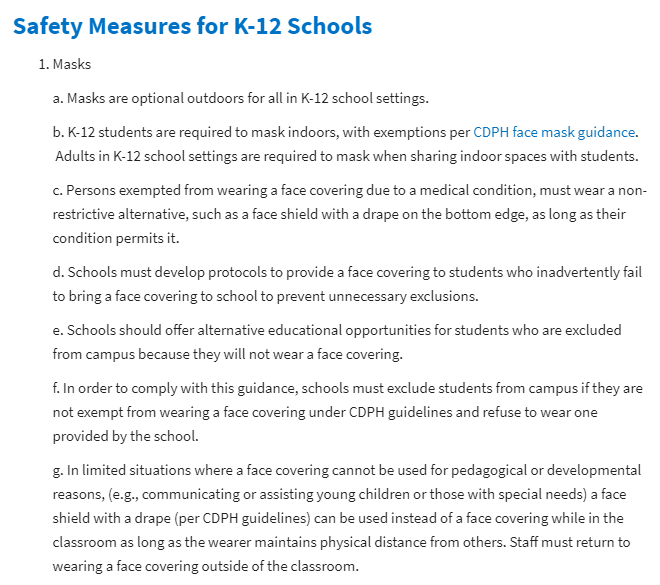
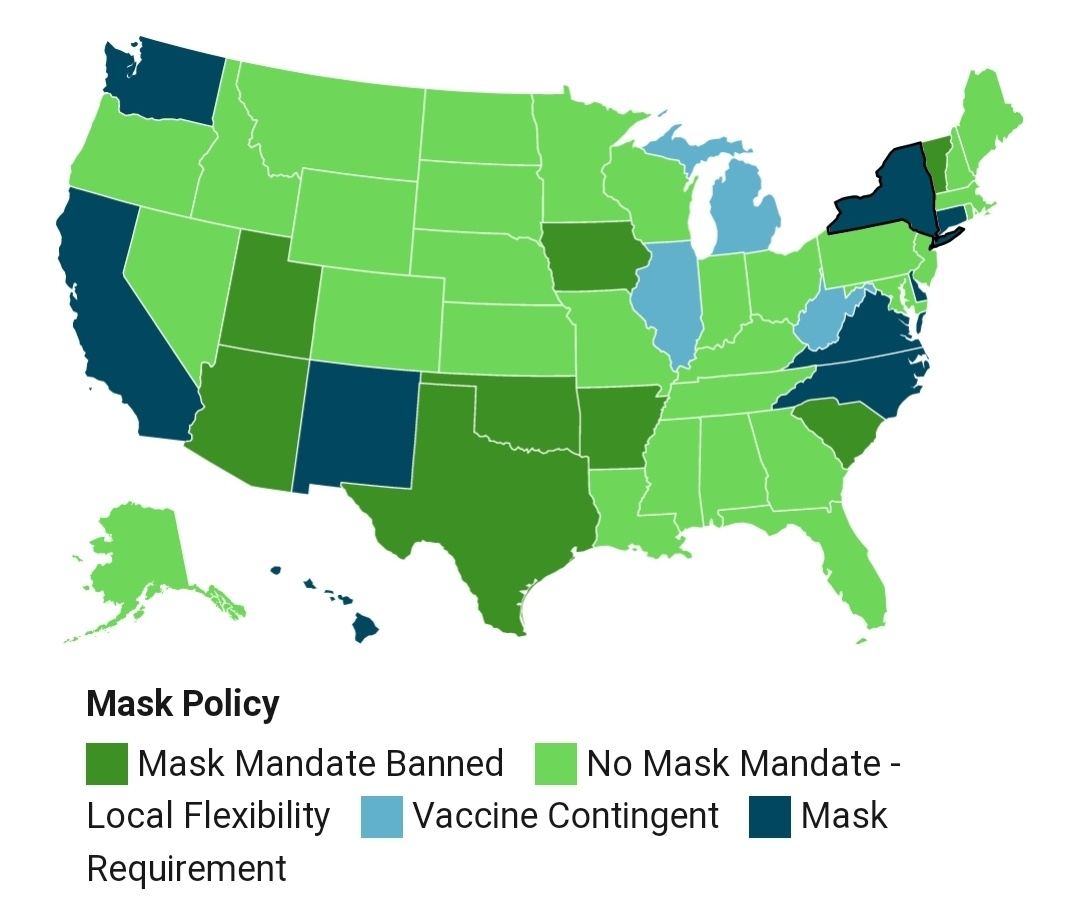
My understanding is this applies even to private schools, although good luck enforcing that. If they’re going to mandate this now, when will it end? Are they planning on keeping things like this forever? Or even going back to the torturous ‘remote learning’ at the drop of a hat?
What would it take to free our children? How bad would it have to get? Shall we run the experiment and find out?
A rant on the quest to establish that the lockdowns were always painless and super effective and that Everybody Knows this.
And some really are pushing to make the pandemic restrictions permanent. Who would want such a dystopia? (post)

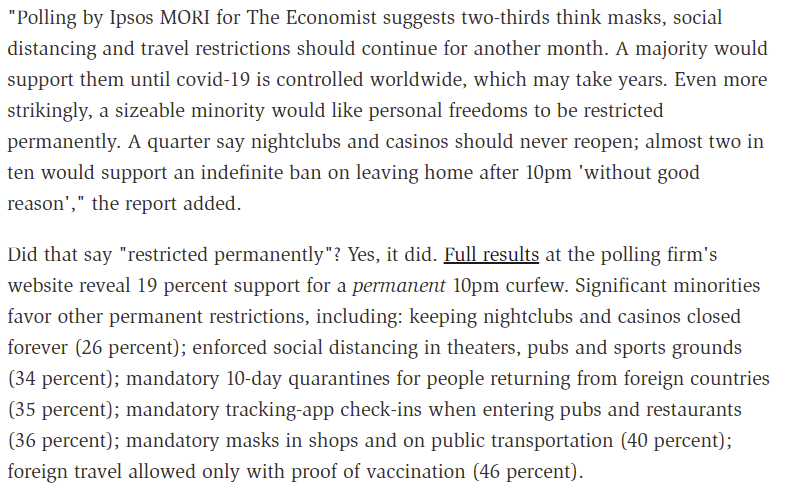
People permanently not being able to leave home after 10pm ‘without good reason’ is the kind of thing hack writers put into young adult novels. Or at least, it used to be. Then again, perhaps there’s always been a 10% share of people who shake their fists at ‘kids these days’ and actually want to be the villains in such novels. How much of this is new?
A quarter of people wanting to close casinos and nightclubs permanently (but again, how much of that has anything to do with Covid?)? A third of people favoring permanent quarantines for international travel? Tracking everyone who enters a restaurant, again, permanently? This is still less than half of people, but a third is a lot of people.
This is the fight that is coming, even if conditions are good. They hate us for our freedom. You gotta fight for your right to party.
One can still party a little too hard, even outdoors. Outdoors is much safer than indoors, but that doesn’t mean one can’t push the envelope too far:
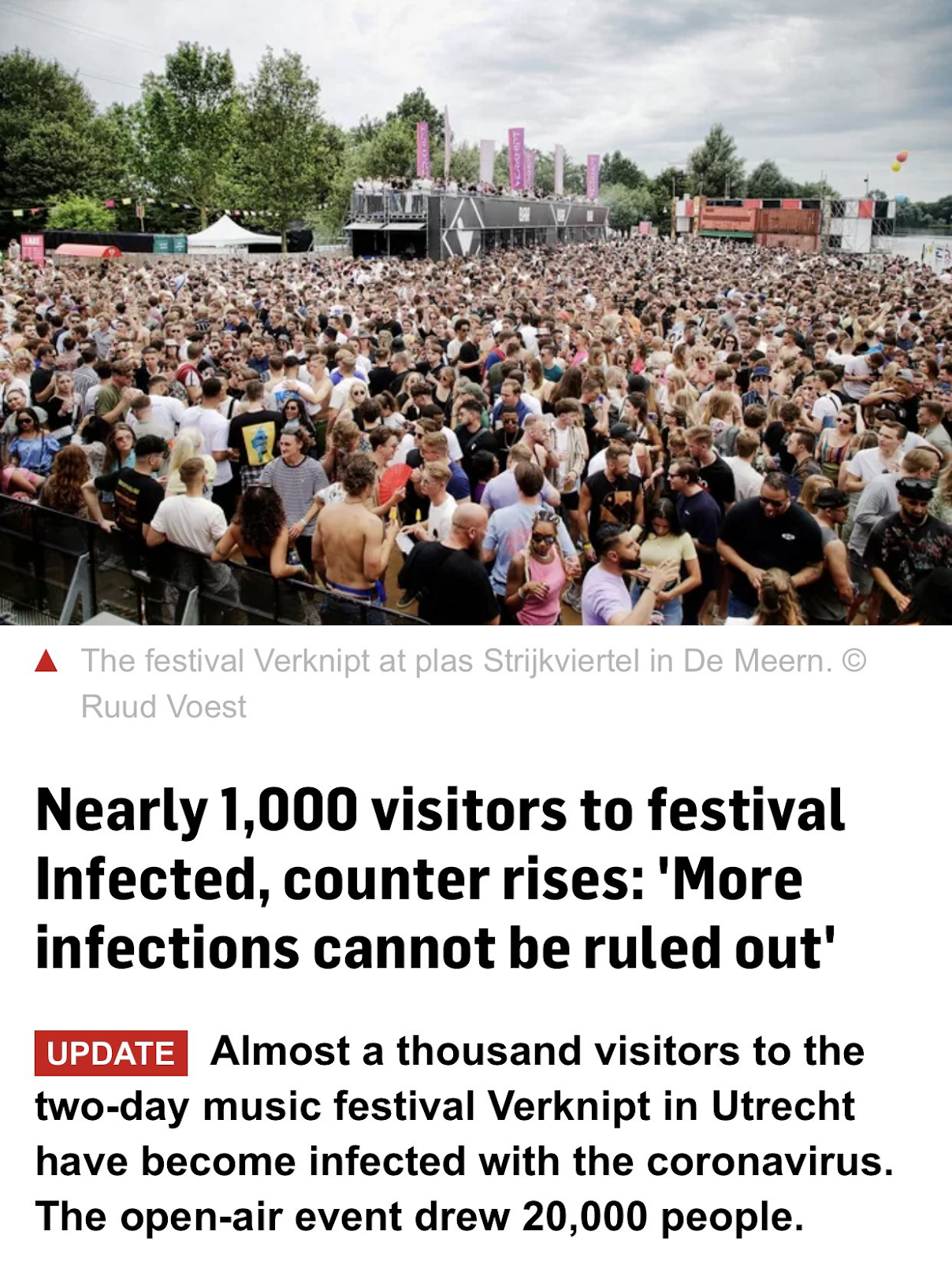
So yes, there’s mass gathering and then there’s mass gathering, might want to not do that second one. Also, ‘cannot be ruled out’ is technically true but I think we could have gone with something a little stronger. A thousand identified cases is not a thousand cases.
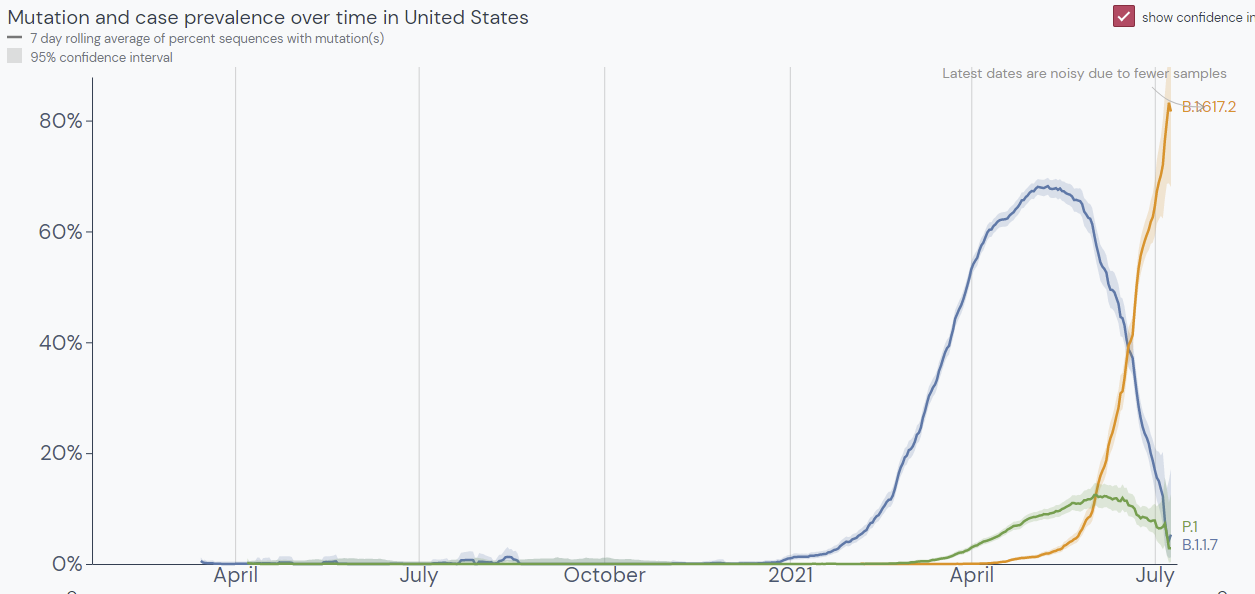
Or, alternatively, instead of protesting for left-wing causes, one can protest against a Communist regime, in which case your protest is dangerous:


Remember, whether or not something spreads Covid depends on whether it is approved of by the proper cultural authorities and Very Serious People. And this is what they think about protesting against authoritarian Communism.
63 comments
Comments sorted by top scores.
comment by Josh Jacobson (joshjacobson) · 2021-07-16T16:14:10.430Z · LW(p) · GW(p)
It seems valuable to LOUDLY NOTE that Microcovid.org has not been updated for the Delta variant https://github.com/microcovid/microcovid/issues/869 and that the adjustment should be quite significant.
I'd be interested in perspectives on what adjustment should be implemented.
comment by [deleted] · 2021-07-15T18:57:34.510Z · LW(p) · GW(p)
There have been some reports that it's not necessarily just the R value that is changing for the delta lineage, but also maybe a faster serial interval. Both of these would result in faster spread, but only the R change would affect the immunity you need to damp spread, the interval just means everything happens faster.
Replies from: Zvi, Lukas_Gloor↑ comment by Zvi · 2021-07-16T00:05:09.448Z · LW(p) · GW(p)
Thanks! Somehow I missed that, and I'll look for next week. Would make all the math much more forgiving, obviously, and make things much less scary. Also makes what happened in India make a lot more sense.
Replies from: johnlawrenceaspden↑ comment by johnlawrenceaspden · 2021-07-19T12:11:27.028Z · LW(p) · GW(p)
The first thing about this pandemic that's really confused me is: India is going full hockey-stick -> the death rate is suddenly falling in India. Do you know why that was?
↑ comment by Lukas_Gloor · 2021-07-15T20:14:07.248Z · LW(p) · GW(p)
Interesting! Do you (or anyone else) have info on what this means about the incubation period? It would be useful to know if it got shorter! Not only for meeting friends or relatives, but also because it means contact tracing becomes easier and lockdowns more effective.
Replies from: brp↑ comment by brp · 2021-07-16T05:57:42.687Z · LW(p) · GW(p)
it means contact tracing becomes easier and lockdowns more effective.
I read that oppositely. If the serial interval is shorter, contact tracers need to work faster to inform those exposed, lest those exposed become infected and transmitting. Likewise, lockdowns would only become more effective if the time each person is contagious is reduced. IIRC the delta variant, according to Indian accounts, is significantly contagious for three weeks from the date of infection as opposed to the usual two.
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2021-07-16T06:13:34.996Z · LW(p) · GW(p)
IIRC the delta variant, according to Indian accounts, is significantly contagious for three weeks from the date of infection as opposed to the usual two.
That would clearly make it harder, yeah. And good point about contact tracing. I guess the only thing that would be easier with a shorter incubation period is isolation after flights and getting down case numbers with a very tight lockdown. Everything else gets harder.
comment by jimmy · 2021-07-15T22:52:48.484Z · LW(p) · GW(p)
My wife and I went to a wedding last week, and 6 of the 14 girls who went to the bachelorette party (all vaccinated) have since tested positive for covid. I and another one of the guys (also vaccinated) got it a few days later, most likely from one of those girls (and not our partners, who both tested negative).
It's just a few cases, but nonetheless seems hard to square with the lower bound of vaccines still working super well to prevent symptomatic infection.
Replies from: dawangy, Zvi↑ comment by dawangy · 2021-07-16T15:49:27.327Z · LW(p) · GW(p)
What kinds of vaccines did you guys have? Also how long ago? I hypothesize a lot of the difference in efficacy reported by the UK (88%) and Israel (64%, kind of close to the efficacy in your situation if we make the generous assumption that all 14 would have been infected without the vaccine) has to do with the fact that Israel started vaccinating earlier.
Replies from: thjread, jimmy↑ comment by Thomas Read (thjread) · 2021-07-17T09:29:13.431Z · LW(p) · GW(p)
Also remember most people in the UK had the second dose at 8-12 weeks after the first.
↑ comment by jimmy · 2021-07-18T06:25:16.004Z · LW(p) · GW(p)
I got my first shot of Pfizer in September and the second in February. I don't know the exact answer for everyone else, but at least one J&J and I think mostly mRNA, probably at about the time it became available to 30 year olds in the states.
↑ comment by Zvi · 2021-07-15T23:57:39.670Z · LW(p) · GW(p)
Any given observation can of course but squared with any given level of effectiveness, because randomness, and also because superspreaders are a thing - so the outcomes can be highly correlated.
Hope no one got seriously ill. From the lack of mention of any adverse effects, I am guessing everyone involved is fine?
Replies from: jimmy↑ comment by jimmy · 2021-07-16T02:34:32.497Z · LW(p) · GW(p)
Any given observation can of course but squared with any given level of effectiveness, because randomness, and also because superspreaders are a thing - so the outcomes can be highly correlated.
Yeah, depends on what you mean by "hard" exactly, and what your hypotheses are. If the idea is that the vaccine makes 93% of people completely immune and leaves 7% effectively unvaccinated, then getting at least 6 of 14 should be pretty rare -- especially if you expect those 7% to be disproportionately old and unhealthy people and the 14 are all fairly young and healthy. Not impossible, but I'm squinting my eyes and double checking the methodology on anything that implies it was "just a fluke".
Explanations that assume some correlation are easier to buy, but I'm not sure what it could be correlated with that wouldn't have also shown up enough pre-delta that we'd have heard of some superspreader event where vaccinated people were passing covid to other vaccinated people.
Hope no one got seriously ill. From the lack of mention of any adverse effects, I am guessing everyone involved is fine?
Too early to tell, but I think everyone will be fine. So far no one high risk has gotten sick.
EDIT: I have some more anecdotal evidence. My cousin just told me that his friend has nearly the exact same story with his wife's bachelorette party. 6/15 so far with symptoms and positive tests, all vaccinated. There's some selection bias there since I likely wouldn't have heard about it if it were only 1/15, but not enough to make it expected under a "just a fluke" model.
Replies from: None, gabriel-holmes↑ comment by [deleted] · 2021-07-16T15:01:25.858Z · LW(p) · GW(p)
Could the fact that both anecdotes involve large groups simultaneously support the model of correlation and clustering presumably from single extremely infectious sources?
Combined with observations of significantly decreased contagiousness from vaccinated people I would expect such events to become much rarer when completely naive people are rare. Consider the dynamics here, ~6 apparently infected in one event and then only two of those continuing to pass it on at all, a sub-replacement chain in that different context.
Replies from: jimmy↑ comment by jimmy · 2021-07-18T06:55:18.250Z · LW(p) · GW(p)
and then only two of those continuing to pass it on at all
I'm not sure this is the case. I think there was significant stagger between when the girls started showing symptoms, and I don't know how many have gotten sick since then or who will get sick soon. My wife just started showing symptoms today, for example (though that's not evidence of vaccinated->vaccinated transfer because kid).
If I had to bet, I'd guess that it was sub-replacement among vaccinated, I just don't have all the data in front of me yet
↑ comment by tkpwaeub (gabriel-holmes) · 2021-07-28T18:28:17.576Z · LW(p) · GW(p)
I think the point Zvi is trying to make is that overdispersion is still a thing, even with people being vaccinated.
comment by DirectedEvolution (AllAmericanBreakfast) · 2021-07-15T17:42:47.074Z · LW(p) · GW(p)
I know you've banned the NY Times, but they did run an article back in June titled "Are Protests Dangerous? What Experts Say May Depend on Who’s Protesting What."
The Washington Post opinion page offered a justification from a public health worker for the discrepancy in September 2020: "But there is one key difference between social justice protests and Trump rallies: Those attending BLM protests by and large grasp the danger and are motivated to reduce their risk, while a large share of those attending Trump rallies deny that there is a danger at all."
It does seem, then, that there was at least some explicit reckoning with this discrepancy. We might not buy their justification.
When I look at this picture, I see that it is taking place outside, with some distance between participants, that there is widespread mask usage, and that they are not apparently protesting against anti-pandemic measures. So it seems to me that a "COVID risk" framing is inappropriate, even under the justifications offered for supporting the BLM protests and not the anti-lockdown protests.
comment by ZachWeems · 2021-07-18T22:16:49.854Z · LW(p) · GW(p)
I dug into the Israel vaccine data some. Full data is lacking and I strongly suspected the true VE is significantly higher, based on the UK's 78.2-93.2% estimate for Pfizer 2 dose. Below is my thought process.
TL;DR I thought I would find a clear reason the Israeli data was wrong. I tried to see if the interval was so large that the Israeli estimate was meaningless or if there was a huge bias, but nothing solid came up, so I've gone from "confident" to "somewhat nervous".
Here's the announcement: https://www.gov.il/en/departments/news/06072021-04
And a more quantitative version (fortunately Google Translate was pretty good at Modern Hebrew, at least in this context): https://www.gov.il/BlobFolder/news/06072021-04/en/NEWS_Corona_vaccine-eficacy.pdf
They say they used the same methodology for Delta effectiveness as what's in this older paper: https://www.gov.il/BlobFolder/news/06052021-02/ru/NEWS_Corona_lancet-article.pdf
It looks like for the recent numbers they took each age group and did a VE estimate, and combined the result. They do an example point estimate of VE for age 35-44 and get 55.7% efficacy, based on 47 vaccinated and 15 unvaccinated infections in a population that was 7.08:1 [2nd dose 7+ days ago]:[No vaccine]. Population is in units of person*days.
That's not many cases (for this age bin). What are the bounds on the example efficacy? Turns out there's a Bayesian way to calculate this, which I won't write out. Assuming I did it right, the 95% credibility interval is 16.5-74.3% for this age group.
So could the 64% expected value of VE be similarly low-confidence? There's no obvious way to guess the brackets on the 64% for the full population without knowing the relative population sizes for all groups. But it looks like the total population count is 257:1271, which is something like 25x the data points. I expect a tighter interval, but not necessarily 5x tighter because of complicated statistics.
My other thought is that there is a bias. Something that seems pretty funky is the usage of person-days. During the interval June 6-July 3, the first two weeks had <10% as many cases as the last two weeks. https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2021-06-06..2021-07-03&pickerSort=asc&pickerMetric=location&Metric=Confirmed+cases&Interval=New+per+day&Relative+to+Population=false&Align+outbreaks=false&country=~ISR Since people strictly leave the unvaccinated group and strictly enter the fully vaccinated group, the average fully vaccinated person-day was on a more case-heavy day than the average unvaccinated person-day. Combined with 1 week being too short to account for the actual effect of dose 2 on positives, maybe this introduces a heavy bias? The paper referenced for methodology includes numbers adjusted for week, but it's not clear if that means week-of-vaccination or weekly cases, and it's not clear if the Delta numbers were adjusted this way. So seems reasonable.
But only 1.97% of the population was vaccinated in this interval, and only 0.29% got Dose 2 in [interval - 1 week]. https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2021-06-06..2021-07-03&pickerSort=asc&pickerMetric=location&Metric=People+vaccinated&Interval=New+per+day&Relative+to+Population=true&Align+outbreaks=false&country=~ISR and https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2021-05-30..2021-06-26&pickerSort=asc&pickerMetric=location&Metric=People+fully+vaccinated&Interval=7-day+rolling+average&Relative+to+Population=true&Align+outbreaks=false&country=~ISR Compared to the June 6 numbers, the unvaccinated population count only had a ~5.3% decrease by the end, and the fully vaccinated had a 0.5% relative increase by the end. The only way I could see this making a big difference is if most cases and new vaccinations were in the same age bin (since the bin would have > 5.3%/.5% relative changes, and more cases mean more weight). It would not be surprising if this was a big enough factor to account for differences with UK data, given the age distribution of cases.
So long story short, I'm leaning towards the UK data being correct. But my expectations were that the Israeli data would be confidently falsified with a couple hours of thought, but this didn't happen, so I'm no longer as highly confident.
comment by [deleted] · 2021-07-15T18:37:31.728Z · LW(p) · GW(p)
It should be noted, for your contagion calculations, that people infected through immune memory are almost certainly not NEARLY as infectious to others on average as completely naive people who are infected.
https://pubmed.ncbi.nlm.nih.gov/34250518/
Israeli healthcare workers who are vaccinated who test positive have a much decreased viral RNA level in their samples, circa a factor of thirty, with the difference increasing as time from vaccination increases. There is a wide range but the whole range moves down so way fewer people will have the obscene viral levels that can do things like infecting sixty people in a room all at once. They also go from 80% showing up positive on an antigen test to 30% showing up positive on an antigen test - which has been a reasonable binary proxy for infectiousness in the past.
This makes sense. You never hear about 60 people all getting the flu at once in one place except in very special circumstances (things like an airplane sealed for two hours without air circulation and filtration), presumably because everyone has at least some anti-flu memory even if it isn't good enough to completely stop everything in its tracks. The disease dynamics when there are lots of totally naive people running around is going to be completely different from the dynamics when everyone has memory, be it from vaccines or infection.
comment by Douglas_Knight · 2021-07-17T04:00:44.057Z · LW(p) · GW(p)
One problem with positivity numbers is that positive tests are reported ahead of negative tests, so if there is a spike in testing, there will be a spike in reported positivity.
comment by Dorikka · 2021-07-15T19:51:38.402Z · LW(p) · GW(p)
Thanks for this as always! Any thoughts on the variant effectiveness estimates in this paper?
https://www.medrxiv.org/content/10.1101/2021.05.22.21257658v1.full-text
Replies from: Zvicomment by Lukas_Gloor · 2021-07-15T18:46:01.759Z · LW(p) · GW(p)
According to this German article, the Robert Koch institute estimates that 85% of the population needs to be doubly vaccinated to guarantee herd immunity to the Delta variant. This is borderline unachievable. (Edit: I think they actually mean 12+ year olds, instead of the full population. Even so.)
Without that level of vaccination, you cannot open up too much, or you'll have a slowly growing surge of cases that won't go away until herd immunity is reached naturally. This means case counts being >1% (and >>1%) for many weeks or even months, as is happening now in the UK.
Deaths may not reach the levels of previous waves if vaccination uptake among the elderly is excellent (which isn't the case in many areas in the US, though), but a lot of young people will get long covid.
It looks unclear whether vaccines even reduce the chances of catching long covid conditional on developing symptomatic covid. Or even conditional on developing asymptomatic covid, since there are some anecdotes about people developing long covid after asymptomatic infection. It's possible that vaccines give a 30% reduction to the risk, but probably not more, and the 30% itself is uncertain. Long covid seems to be more likely to happen than I initially thought. I'm unsure whether it's more like 1% or 4%, but it definitely seems significant. (Probably it's possible to figure out with certainty what the odds are – I just haven't looked into it in a while.)
comment by danohu · 2021-07-16T09:17:06.987Z · LW(p) · GW(p)
Cases in Germany have also been spiking the last 2 weeks. I don't see any explanation other than Delta being very, very infectious. Case numbers were halving week-on-week in mid-June (minimal Delta); now (most cases Delta) they are almost doubling each week. You can throw in a few other factors (control system lag, school vacations, a big football tournament), but Delta still must be doing something extreme.
One ray of light is that the increase is largely limited to people in their 20s, who are mostly not yet fully vaccinated. The vaccination rate in that age group should shoot up in the next month, so Delta might get damped more than you would expect from the overall vaccination rate in the population.
comment by waveman · 2021-07-16T02:31:11.492Z · LW(p) · GW(p)
"I worry that recently I’ve lacked sufficient skin in the game. Everyone I personally care about is vaccinated or young enough that they don’t need vaccination, so the real sense of danger is largely gone."
[Quotes because editing after using ">" for quotes is totally broken here.]
The strategies being employed at the moment in countries partially but not sufficiently vaccinated are to a close approximation the optimum for evolving viruses that are more transmissible to vaccinated people. We have a huge number of infected and a huge number vaccinated in the same population thus the maximal evolutionary pressure and opportunity.
So it is somewhat likely - hard to tell how likely - that variants that are resistant to the vaccines will appear.
When a disease is only slowly transmissible there is an evolutionary incentive for it to become less ( and less quickly) fatal. However diseases that are easily transmitted have far less incentive to become less quickly fatal e.g. cholera in some parts of the world.
My conclusion is that given the risk that a more transmissible, more vaccine resistant and more deadly variant will appear, everyone has skin in the game.
Not to mention the "long covid" syndrome which is very nasty and fairly prevalent in young people. And that we really have little idea of the long term consequences of non-fatal infections in young people.
I remember when Chicken Pox was considered a mild and harmless illness. Tell that to people who have suffered years of excruciating pain from shingles as a result of Chicken Pox later in life.
↑ comment by Lukas_Gloor · 2021-07-16T04:28:25.651Z · LW(p) · GW(p)
I tried estimating the chance that a new variant would arise in the UK in the next couple of months:
I think the risk of a new superbad variant arising in the UK is 6%. We've seen two game-changing variants so far (Alpha and Delta) out of roughly a billion Covid cases (extremely crude estimate). The UK will have roughly 10 million cases in the coming three months (extremely crude estimate). That would be 1% of the total so far, so a 2% prior for a new game-changing variant (since this happened twice already). Conditions for evolving vaccine evasion have never been better, which adds at least a factor 2, I would think. It's more in expectation, so maybe 3.5. (Also, the Alpha variant happened in the UK, so maybe conditions are particularly favorable for virus evolution here for reasons I don't understand.) OTOH, I may be ignoring that the virus has run out of low-hanging mutations. Overall, I'm going with a 6% chance.
Note that I don't necessarily predict a new variant to be more deadly by itself. (But it would be more deadly given better resistance to vaccines.)
It's indeed scary that the same experiment will be run across many countries, so in absolute terms, the odds are much larger than what's correct for the UK for the next couple of months.
But the risks per country are heavily correlated (are there low-hanging mutations that increase transmissibility?), and overall I'm not sure I'd go above 40% for a new superbad variant in 2021. I think this is partly also influenced by having read some experts express a lot of confidence that the antibodies to the spike protein, especially from the Pfizer and Moderna vaccines, are fairly hard to circumnavigate when you're the virus, because probably all Covid viruses need some kind of similar-looking spike protein. Even so, you could get a variant where infection is reduced by 50-70% after two shots of Pfizer, instead of the 15-30% we see currently. That would basically guarantee that nearly everyone gets exposed to long Covid risks of having to go through one illness.
↑ comment by [deleted] · 2021-07-20T01:38:23.876Z · LW(p) · GW(p)
Honestly I think it's quite the opposite. There is no particular reason that lineages that escape immune reactions would be more likely to be driven into existence in a population largely vaccinated or largely infected, and you don't talk about this in the context of people who have been naturally infected.
We are pulling the inevitable, the time that everyone has immune memory, closer in time to the present and ensuring that we get there with fewer rounds of viral replication in the mean time.
comment by Lukas_Gloor · 2021-07-15T18:35:05.546Z · LW(p) · GW(p)
Rapid spikes of case numbers are not unheard of. The Netherlands government opened up all restrictions, which led to a 500% increase in case numbers in a single week. They decided to close down again. (Netherlands has 40% of people fully/doubly vaccinated.)
comment by Lukas_Gloor · 2021-07-15T19:27:55.243Z · LW(p) · GW(p)
[...] which oddly still leaves out the question of whether shots can be modified to work better versus Delta. I’m confused why there isn’t more discussion about that. My presumption is that modifications wouldn’t help, which is interesting in and of itself and seems worthy of mention if true.
I'm also very confused by this! I don't immediately see why modifications couldn't be made, but yeah, the alternative (that people simply don't discuss this option) seems completely insane.
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2021-07-22T07:46:21.671Z · LW(p) · GW(p)
Actually there was some talk at least 9 days before I made the above comment: npr.org/2021/07/09/1014744345/pfizer-is-pursuing-a-booster-shot-and-new-vaccine-targeting-the-delta-variant
comment by ZachWeems · 2021-07-19T03:00:21.445Z · LW(p) · GW(p)
Various points on Delta & vaccination:
-On the UK vaccination data, the 79% number is for Pfizer and AZ combined. Since the vast majority of US vaccinations are Pfizer or Moderna, the Pfizer number should be much closer to the truth. Their EV is 87.9%, with a confidence interval from 78.2 to 93.2%.
-Looking at Israel's Delta/vaccination document linked to in my other comment, they don't have many hospitalizations or severe disease cases for either vaccinated or unvaccinated. So I don't expect their expected value number to be very meaningful, due to huge confidence intervals.
-When you compare predictions to reality in "Transmissibility", you seem to assume vaccine efficacy (VE) from cases should equal VE from R. Vaccinations seem to reduce peak viral load by a lot, regardless of conditioning on symptoms. So we should not expect the R to be very predictive of VE.
Various points on Delta and R:
-When I dig into R estimates for new variants, I find lots of disagreement comes from the serial interval estimate. Personally I convert everything to weekly growth now so I don't have to hold that information in my head.
-Regarding the calculation you did in "Transmissibility", there's pretty good data from the UK. While Delta was taking over, they estimated that the natural log of the Delta/Alpha ratio increased by 0.91/week to 0.93/week (a factor of ~2.5). I trust this value more because it is less biased by the control system. See for example Table 7 on pg 25 of https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/993879/Variants_of_Concern_VOC_Technical_Briefing_15.pdf
-I've been doing a similar estimate for the US based on weekly proportions of delta and it's descendants, albeit with a shoddier method because time constraints & heterogeneous data. The best fit is usually a relative growth rate of ~1.85 per week (although it can vary by +/- 0.1 depending on the day). I've been surprised because the US overall growth rate has been faster than 1.85 times the pre-delta rates. It might be that the highest-transmission states are now contributing much more than before? Data from https://outbreak.info/situation-reports?pango=B.1.617.2&loc=USA&selected=USA and equivalents for the AY's.
comment by tkpwaeub (gabriel-holmes) · 2021-07-28T18:25:29.362Z · LW(p) · GW(p)
It's time to fall back on the thing that governments do best: levying fines. Cities and states need to start issuing civil penalties - say $10,000 - to anyone who doesn't get vaccinated without a valid medical excuse. And criminal penalties to people who spew anti-vaxx rubbish over public airwaves.
comment by goose000 · 2021-07-20T15:52:16.227Z · LW(p) · GW(p)
A few observations.
First, it seems likely that the increase in positivity can be explained by fewer precautionary tests: fewer people are getting tested "just to be sure", fewer people are being required by work/travel/etc. to get tested. Therefore fewer negative tests.
Second, it seems likely to me that the "93%, 93%, 91%" numbers are calculated independently from each other. I.e. 93% less likely to contract than unvaccinated, 93% less likely to hospitalize than unvaccinated, and the vaccinated group was 91% less likely to die than the unvaccinated group. So with alpha, all probabilities were reduced ~uniformly. Now consider a variant (delta) where the vaccine is not as effective at reducing symptoms of any level, but is still ~as effective at preventing hospitalizations and deaths. This would decrease the likelihood of the vaccine preventing a positive test or symptoms, while not changing the hospitalization/deaths numbers much. This makes sense in my head, but perhaps there's something I'm missing?
Finally, a typo that tripped me up a bit:
We should also look at case counts in Israel. On June 18 they had 1.92 cases per million, right before things started rising, on June 14 it was 65.09, for R0 = 1.97. From previous data, we can presume that when Delta was a very small portion of Israeli cases, the control system adjusted things to something like R0 = 1, so we’ll keep that number in mind.
The second "June" should be "July", as in "July 14". (Small nitpick, I know, but it took me a minute to work out, so I figured I'd share.)
comment by tkpwaeub (gabriel-holmes) · 2021-07-18T08:25:36.303Z · LW(p) · GW(p)
The prospect of a flu/covid/hMPV/RSV combo vaccine is amazing. I suspect it could be tailored to specific zip codes depending on whatever is going around.
comment by TheSimplestExplanation · 2021-07-17T13:32:12.188Z · LW(p) · GW(p)
On June 18 they had 1.92 cases per million, right before things started rising, on June 14 it was 65.09, for R0 = 1.97.
Those dates seem wrong.
comment by tkpwaeub (gabriel-holmes) · 2021-07-17T11:56:04.103Z · LW(p) · GW(p)
I have this fantasy about making all the QAnon fever dreams come true, by putting ads on pizza boxes targeted at teenagers in Tennessee to get vaccinated.
comment by simon · 2021-07-16T02:17:51.289Z · LW(p) · GW(p)
One possible way for this to kinda sorta work is that perhaps there are people who get tested in order to show a negative test, whose tests get reported every time, and people who get tested because they want to actually know if they have Covid, who mostly only report when they’re positive. Then, doubling the size of the second group doesn’t change reported test counts much? That’s the best I can come up with.
My mental model (backed by nothing) is that a lot of people get tested due to symptoms that often aren't due to covid, so this provides a relatively constant level of negative tests even though they do actually want to know if they have Covid. (In addition to any who simply want a negative test, of course).
It's possible that perceived prevalence would affect the tendency to get tested for a given level of symptoms, but if so I wouldn't be surprised if this perceived prevalence lags the positive tests. (There's a lot of potential for weirdness here though).
People getting tested due to an interaction with a positive case would provide negative tests correlated with positive tests, but I expect this would lag the positive tests.
Just speculating - I haven't been paying attention to the negative test patterns in the past, so this might for all I know be totally at odds with the actual data.
Replies from: daniel-tilkin↑ comment by Daniel Tilkin (daniel-tilkin) · 2021-07-16T19:21:26.294Z · LW(p) · GW(p)
Also, people who get tested because they need to show proof of a negative test for some purpose would be part of this background rate as well.
Replies from: simoncomment by Annapurna (jorge-velez) · 2021-07-15T19:28:36.210Z · LW(p) · GW(p)
Any reason why not use your reasoning and expertise to put skin in the game? Polymarket has a couple of markets such as this one:
Replies from: Zvi↑ comment by Zvi · 2021-07-16T00:03:52.600Z · LW(p) · GW(p)
It's certainly not the most efficient market (e.g. there's been no update in the past few days which is clearly wrong), but I think it would be more a distraction than it's worth. Maybe after my apartment closes I can look into such things more seriously.
comment by time.less.ness · 2021-07-16T15:56:32.361Z · LW(p) · GW(p)
I note your typical disdain for the anti-vaxxers. You probably have your reasons. I struggle to discount them as quickly. If I were a betting man, I would bet there are some pretty bright and well-reasoned ones in the mix. I don't think I can predict the future well, but I wouldn't be entirely surprised to find out in 10 years the anti-vaxxers were right, for the right reasons, and that we should have given their reservations far more careful consideration[0].
If you care about being fair to that class of people[1], you need to put more thought into the position of anti-vaxxers.
I note zero comment, analysis, or consideration for people who got Covid and recovered. How do they fit into this whole mess? Ctrl-F "recover." No hits.
You applaud France's rules that would require recovered Covidees to get vaccinated. Is this your disdain for those who trust immune systems to do their jobs? Or did you and France just forget about their existence entirely? Maybe some third option I can't fathom[2]?
You seem well-intentioned to me, and I read your posts thoroughly because I feel there's signal here. But don't be surprised if certain people, many of them, even very bright and well-reasoned ones, write you off as a political pro-vax hack.
Everything I've seen so far says vaccination is a political issue, not a health concern. The evidence we choose to consider, the experts we cite, and the science we believe seem to depend on the agenda we're pushing.
____________
[0] Is "Fox News agrees with them" good enough to just write them off entirely, and ban them from the internet? Sure. Why not? Censorship has a long and illustrious historical record, full of good intentions and great results.
[1] If I'm being honest, my experience shows fairness in a political fight yields near zero benefit to anyone on either side of the political debate and costs a massive amount of stress. Hence, you probably shouldn't bother being fair. Continue to be a pro-vaxxer, wear the badge proudly, and embrace the biases it gifts you.
[2] If I'm being honest, I'm not actually a terribly bright person. I consistently fail to be able to fathom the third option in the dichotomy.
Replies from: andrew-vlahos, alexey-lapitsky, GuySrinivasan, Vanilla_cabs↑ comment by Andrew Vlahos (andrew-vlahos) · 2021-07-17T06:38:19.301Z · LW(p) · GW(p)
Decisions about covid policy have been mostly political, but vaccines weren't political before that. Consider smallpox. Smallpox was all over the world and apparently unbeatable. It was described in China in 340. George Washington and Abraham Lincoln got it, and if they died history could have gone way differently. https://rootsofprogress.org/smallpox-and-vaccines. It was just a thing that sometimes happened to people, and nothing could be done about it. Suddenly, as soon as vaccines were applied to a region. Smallpox was completely eliminated there.
A similar thing happened with Polio, Tetanus, Hepatitis A and B, Rubella, Measles, Hib, Whooping Cough, Pneumococcal Disease, Mumps, Diptheria... They are almost gone, and the only people who get them now are in places that haven't gotten consistent and almost complete vaccination.
In fact, there's one that most people alive remember. Chicken pox used to be seen as an inevitable childhood disease, to the point that people used to throw "pox parties" to get it over with. but when the vaccine was invented in 1995 it rapidly decreased, and I don't know anyone my age who has gotten it (born in 1996). It's pretty much gone now.
Zvi isn't trying to have "fairness in a political fight", as if the sides were equal. The "vaccines are effective" side is totally crushing the "vaccines are bad" side. And plague doesn't care about your politics.
↑ comment by Alexey Lapitsky (alexey-lapitsky) · 2021-07-17T10:34:37.458Z · LW(p) · GW(p)
Strongly upvoted as well, and I agree with Vanilla_cabs - I don't think it helps classifying everybody concerned about covid vaccines as anti-vaxers. Maybe we need a better term.
Here is an analysis taking into account recovered people with natural immunity in the US:
https://youtu.be/vJy8jdunpFw?t=520
Personally, I'm wondering if antibody dependent enhancement could explain some weird patterns we are starting seeing now in highly-vaccinated places.
Replies from: Kenny↑ comment by Kenny · 2021-07-29T18:41:47.040Z · LW(p) · GW(p)
I don't think it helps classifying everybody concerned about covid vaccines as anti-vaxers. Maybe we need a better term.
The better phrase would be 'people with concerns about COVID vaccines'. (Hopefully these people would also have specific, and reasonable, concerns too.)
'Anti-vax' seems to reasonably cover people skeptical of, or hostile to, vaccination generally.
↑ comment by SarahNibs (GuySrinivasan) · 2021-07-18T15:55:34.691Z · LW(p) · GW(p)
Do you have a tldr on why we might think anti-vaxxers were right for the right reasons? Seems like the default positions are "vaccines have obviously worked in the past and we're pretty sure they're gonna work in very similar ways today", and I haven't seen anything that changes my opinion much about either of those defaults.
Replies from: Vanilla_cabs↑ comment by Vanilla_cabs · 2021-07-20T08:32:03.561Z · LW(p) · GW(p)
Regardless of the general point, I think you're making a noncentral fallacy here. This vaccine differs from the vaccine archetype for multiple reasons: it uses a new, different technology, it was rushed and we have no hindsight on its long-term side effects, it does not offer as strong a protection as expected from a typical vaccine (in particular, not strong enough to eradicate the virus even if it had maximum coverage), it's used at the height of a pandemic with the risk of creating variants through recombination, the potential market has never been this huge, thus increasing the incentive for foul play. This is not a typical get-1-shot-go-carefree-for-10-years vaccine.
Replies from: Kenny↑ comment by Kenny · 2021-07-29T18:36:33.664Z · LW(p) · GW(p)
we have no hindsight on its long-term side effects
That's going to be true of any new vaccine too, which isn't helpful for deciding whether to create or use any new vaccine. (But we do have "hindsight" on every other vaccine.)
it does not offer as strong a protection as expected from a typical vaccine
We could play some reference class tennis with this one as I don't think we've ever had a vaccine for a virus similar to this one. And it seems arguably reasonable to consider the 'flu vaccine' as 'typical' and that (those) seem to offer even less protection than these.
the potential market has never been this huge, thus increasing the incentive for foul play.
What do you mean by this exactly? That the "potential market" possibly includes everyone? That doesn't seem to be that different than for other vaccinations, tho maybe you do have a point given that we're all in the middle of a global pandemic, whereas more 'typical vaccinations' only have a 'market' for some narrow age cohort.
This is not a typical get-1-shot-go-carefree-for-10-years vaccine.
Yes, this, sadly, seems to be very much the case.
Replies from: Vanilla_cabs↑ comment by Vanilla_cabs · 2021-07-29T21:59:37.939Z · LW(p) · GW(p)
And it seems arguably reasonable to consider the 'flu vaccine' as 'typical' and that (those) seem to offer even less protection than these.
Which is why when someone wants to impress you with the historical track record of vaccines, the flu vaccine conspicuously remains out of the picture.
What do you mean by this exactly? That the "potential market" possibly includes everyone? That doesn't seem to be that different than for other vaccinations
I guess maybe some other vaccines have a near-worldwide cover. Note that since world population and GDP has always been going up, every new global pandemic creates de facto an unprecedented huge potential market. Though not by much. So, I don't know?
Ok, so at this point maybe we can agree that:
1/ The COVID vaccine is less efficacious than touted last year, when the population was convinced to wait and expect salvation from it.
But:
2/ Strangely, 1) does not seem to have led policy/opinion makers to shift their bets on other horses or mellow their speech. Actually, pro-vaccination speakers have greatly radicalized this year, now advocating more and more openly shaming and punishment of unvaccinated people.
That looks something like Evaporative Cooling of Group Beliefs [LW · GW] if the cult was so powerful it could punish dissenders. And I'm honestly frightened by that.
Replies from: Kenny↑ comment by Kenny · 2021-07-30T17:37:04.046Z · LW(p) · GW(p)
2/ Strangely, 1) does not seem to have led policy/opinion makers to shift their bets on other horses or mellow their speech. Actually, pro-vaccination speakers have greatly radicalized this year, now advocating more and more openly shaming and punishment of unvaccinated people.
That looks something like Evaporative Cooling of Group Beliefs [LW · GW] if the cult was so powerful it could punish dissenders. And I'm honestly frightened by that.
I agree that this is a Sad own-goal – politicizing the vaccination efforts – but that's because I'm convinced that the vaccines are pretty effective.
But I don't think it's actually 'strange' that this happened; Sad, yes, but not strange (or thus unexpected).
↑ comment by Vanilla_cabs · 2021-07-17T06:32:45.539Z · LW(p) · GW(p)
FWIW, strongly upvoted, despite thinking that the term 'anti-vax' perpetuates a false dichitomy that poisons the well.
I am French and the "incentive" OP talks about is blackmail by a president who just got disavowed in elections (https://fr.wikipedia.org/wiki/%C3%89lections_r%C3%A9gionales_fran%C3%A7aises_de_2021#Synth%C3%A8se_des_r%C3%A9sultats LREM, the governing party, gets 0,52% of voter's votes on the first round).
I've been writing a piece explaining the background of these "incentives" but since it's a political issue, I don't think it can find a place on LW (see the recent debate on https://www.lesswrong.com/posts/BY5f7iEzHtEDJLXS7/prediction-what-war-between-the-usa-and-china-would-look [LW · GW]). [LW · GW]
One takeaway should already be obvious to anyone who's concerned with AI alignment or read Superintelligence: don't applaud when a growing potential tyrant does what you want.
Replies from: Kenny, gabriel-holmes↑ comment by Kenny · 2021-07-29T18:46:34.094Z · LW(p) · GW(p)
don't applaud when a growing potential tyrant does what you want
So, don't "applaud" anything a "growing potential tyrant does", beyond maybe something demonstrating that they're not (or no longer) interested in 'growing their tyranny'?
Replies from: aphyer, Vanilla_cabs↑ comment by aphyer · 2021-08-02T15:50:37.604Z · LW(p) · GW(p)
A better way of phrasing it might be "don't applaud a growing potential tyrant who seizes additional power just because they happen to do something you want with it." I do think the message is clear even without that change.
Replies from: Kenny↑ comment by Vanilla_cabs · 2021-07-29T21:00:45.551Z · LW(p) · GW(p)
If a potential tyrant did something like relinquishing power, then by definition they wouldn't be growing.
Edit: Oh, you mean the rule can be generalized, and after doing so seems too general for you? But it is the same rule. If you should applaud a single thing, that'd be something you want. So the implication goes both ways.
Replies from: Kenny↑ comment by Kenny · 2021-07-30T17:55:39.238Z · LW(p) · GW(p)
Meh – there seems to me to be a lot of ambiguity about what 'applauding' is, or what purposes it serves (or is intended to serve), but still, I'm confused why you wrote:
don't applaud when a growing potential tyrant does what you want
instead of just:
never applaud a growing potential tyrant
Certainly the rule isn't:
only applaud when a growing potential tyrant does what you do NOT want
As for your reply:
If a potential tyrant did something like relinquishing power, then by definition they wouldn't be growing.
Okay – but a "potential tyrant" could be growing at some point and then, after relinquishing (some) power, either no longer growing, or growing slower, or even shrinking. I don't understand why a 'by definition' argument clarifies this.
But still – why even bother to posit a rule about 'applauding' the actions of a potential tyrant at all? What's your theory about the efficacy of such a rule? What's the point? And why qualify such a rule to only those occasions when the potential tyrant "does what you want"?
Replies from: Vanilla_cabs↑ comment by Vanilla_cabs · 2021-08-02T10:41:47.948Z · LW(p) · GW(p)
And why qualify such a rule to only those occasions when the potential tyrant "does what you want"?
Because nobody needs to be warned not to applaud a potential tyrant who does not do what they want.
The idea is derived both from Superintelligence main metaphor, where sparrows try to raise an owl to solve all their problems, representing AGI without care for alignment, and past human history. In order to solve a problem, one feeds a monster that (quickly) ends up becoming much worse than the initial problem. I remember reading that in conquering the Aztec empire, Cortés took advantage of the resentment that existed between local tribes and the central government ; so did Caesar when he took over the Gaules. In fiction, the novel Brown Morning describes a slippery slope towards tyranny where some fail to react early because they're not concerned or have something to gain. The novel is very naive and simplistic, but short, universal and to the point.
Here I'm reminding that the political actor that OP notes for their efficiency, reaches such 'efficiency' through oppressive measures, lacks the solid legitimacy required to impose such extreme measures, and has an history of playing fast and loose with the tenets of democracy that predates this crisis. That's not a move in isolation, and if you look at the big picture, it's clear that 'public health' or 'saving lives' is not the endgame of these measures. Therefore, supporting those measures would be short-sighted.
Replies from: Kenny, gabriel-holmes↑ comment by Kenny · 2021-08-04T21:58:00.049Z · LW(p) · GW(p)
I'm pretty skeptical that this analysis applies to the specific example you mentioned – or not particularly strongly anyways.
But I didn't interpret your original comment as, or even notice the possibility of it, directly linking the 'doing something you want' with 'seizing more power'. aphyer's comment [LW(p) · GW(p)] helpfully clarified that.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-02T15:12:57.296Z · LW(p) · GW(p)
Would you be more comfortable with a more traditional measure like imposing a hefty fine on people who don't get vaccinated?
Replies from: Vanilla_cabs↑ comment by Vanilla_cabs · 2021-08-02T18:51:46.386Z · LW(p) · GW(p)
Depends on the amount of the fine. But even if it was reasonable, the government of my country would need to produce at least 2 other components to make a credible good will attempt at saving lives:
- They should be increasing the number of hospital beds available and hire health professionnals, instead of closing beds as they've been doing throughout the pandemic
- They should set boundaries to the duration of the fine, promise not to raise it or lenghten it, and have a credible way of showing they'll keep that promise, or, barring that, a track record of keeping their word. Instead, they have emergency powers, can pass decrees without parliament approval, and have consistently broken their words arguing that "the circumstances have changed"
↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-04T07:33:42.177Z · LW(p) · GW(p)
I guess what I like about fines is that they have a well defined endpoint. They end when people have either complied with whatever they need to comply with OR they've paid the fine.
As for hospital beds - absolutely. In fact another reason I lean toward fines is that the money can be earmarked for very specific things, like treatment.
I'm not sold on the idea of everybody needing a booster shot forever, if that's one of your concerns.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-08-03T09:15:37.493Z · LW(p) · GW(p)
Ok, it seems we have something to work with, then. Amounts and validity periods can be negotiated.