Omicron Post #14
post by Zvi · 2022-01-13T18:00:01.077Z · LW · GW · 21 commentsContents
From various sources, I have become convinced that rapid tests taken from nose swabs are likely to often be several days slower at detecting infections than rapid tests that use throat swabs.
Travel
Spread
Hospitals
Severity
Outlook
China
Other and Threads
Probability Updates
China keeps daily cases under 50 per million through 2022: 40% → 30%.
Median peak cases day for United States: January 19 → January 18
Mode peak cases day for United States: January 19 → January 17
Daily cases in the the United States have peaked by February 1: 90% → 93%.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? 50% → 45%.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 55% → 45%.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 95% → 97%.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% (unchanged).
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 3% → 2%.
Generation time (serial interval) of Omicron is 3.5 days or less: 90% (unchanged).
None
22 comments
Important note on testing that I’m including at top of both posts today.
From various sources, I have become convinced that rapid tests taken from nose swabs are likely to often be several days slower at detecting infections than rapid tests that use throat swabs.
Here’s Washington Post on that, this quote should tell you what you need to know.
On one side are well-regardedexperts who argue that swabbing your throat in addition to your nose may increase the chances that a home test can detect omicron. On the other side are similarly well-regarded experts, including those at the Food and Drug Administration, who urge Americans to avoid experimenting with kits that were developed and tested using only nasal swabs.
This ‘disagreement’ over ‘experimentation’ made me that much more confident in the conclusion I’d already reached.
That is echoed by a lot of sources both personal and general, including in this heartfelt report of Bob Watcher, whose son has Covid-19 and reports back on the experience, including five days later follow-up where he’s still positive and acts confused about what to do because CDC guidelines are confusing a situation that is otherwise extremely not confusing.
Thus, if you want to know if you have infectious Covid-19, you need to use throat swabs. It’s still not 100% sensitivity or anything, but it’s a lot better, whereas nose swabs are useful but in no way all that reassuring.
If you want to satisfy a testing requirement that is of course another matter. These are very different goals.
This is a whole week’s roundup, because I got an opportunity to impact developments more directly and needed to jump on that with my non-day-job time instead for a few days. I hope to be able to talk about it soon, but can’t right now.
Travel
It’s a very good question. Why the hell are we still doing this?
The Centers for Disease Control and Prevention on Monday advised Americans to avoid travel to Canada, citing “very high” levels of the coronavirus.
Canada was placed under a Level 4 travel health notice — the highest category…“Because of the current situation in Canada, even fully vaccinated travelers may be at risk for getting and spreading Covid-19 variants,” the C.D.C. said.
The United States has higher rates of Covid-19 than Canada right now, yet we do this thing. I simply can’t take seriously, as someone who might want a physically better and healthier world, anyone who restricts travel in such ways.
The CDC resumed briefings this week. This is the kind of thing they think we need to know.
Spread
CDC Nowcast has Omicron at 98.3%, which seems reasonable to me.
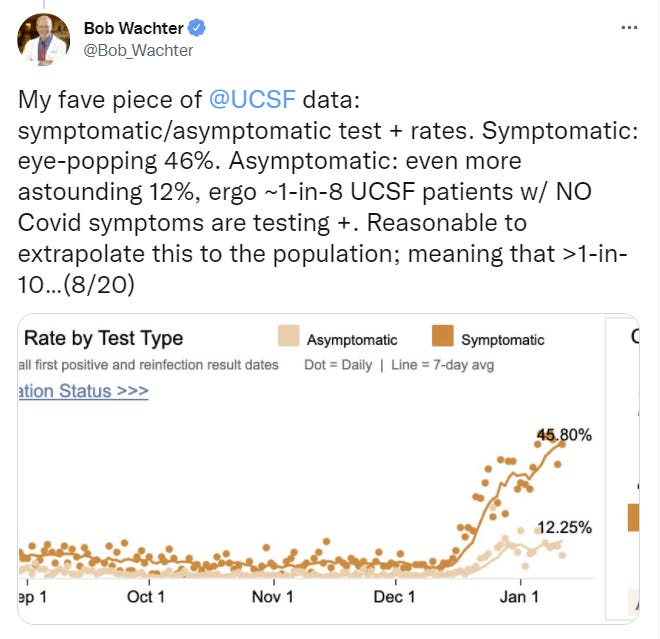
New update from Bob Wachter on San Francisco.
Two big notes are that there’s about an even mix of vaccinated and unvaccinated Covid patients outside of the ICU (this is SF, so a large majority of people are vaccinated) and then 11 of 12 in the ICU are unvaccinated. And then there’s the background rate, which is pretty astounding.
Trevor Bedford estimates that about one third of London infections are being detected. I continue to think that is low, especially given the peak already happened, but it’s not outside the range of possible answers.
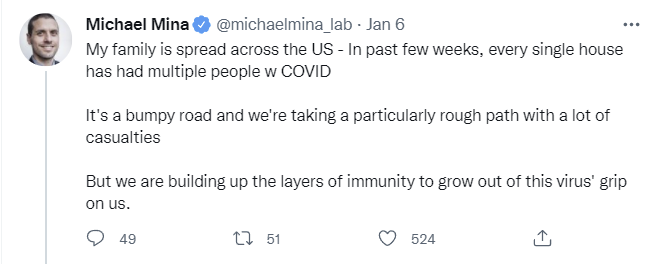
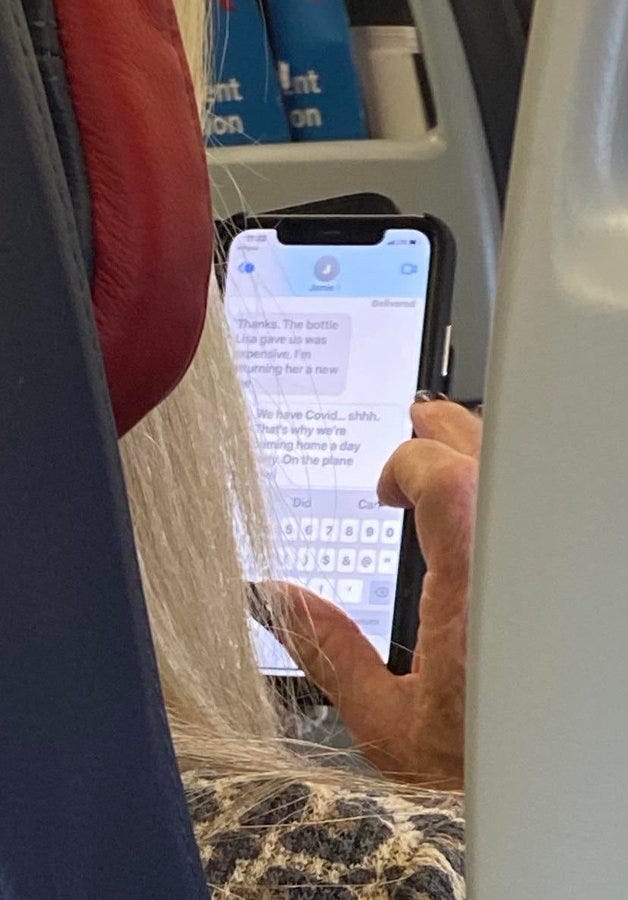
A key question for modeling how things go is whether people are modifying their behavior. Some people definitely are, but others definitely aren’t, including when they know they have Omicron. One commenter noted that their friends treated it like a cold and mostly ignored it (as opposed to what one should do with a cold, which is stay home) and then there’s this.
A thread from 9 January on progress in Scotland and rest of UK, pointing out things have peaked but don’t seem to be declining rapidly yet. Things remaining leveled off without a rapid decline is of course possible, but stabilizing this high can’t hold for long because it’s a lot of newly immune people every day. The crash is coming.
New York City is definitely at least a few days after peak.
Hospitals
Hobson’s UK hospital thread for 8 January. I interpret a lack of a more recent thread as moderately good news.
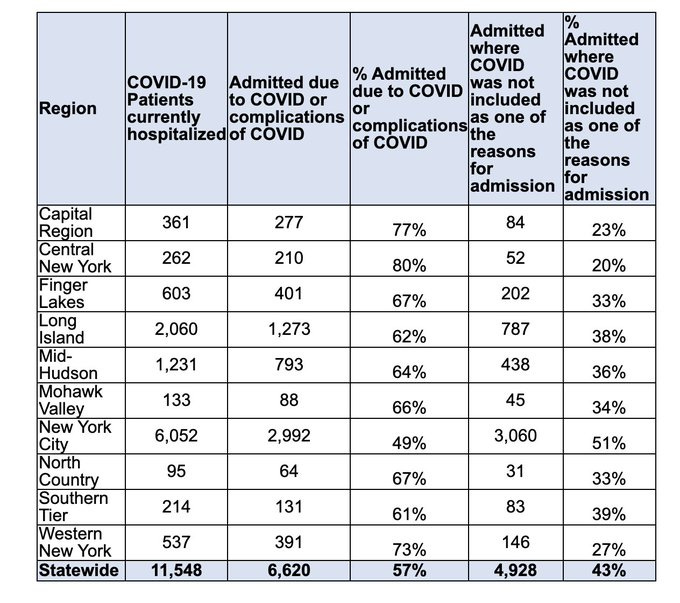
There was speculation that this was differences in definitions of ‘with Covid’ but I do not believe that is the case. I think the difference is real, and reflects population differences.
There’s also some concern this could be within-system spread and I don’t doubt that some of that is happening but I don’t think it’s primary.
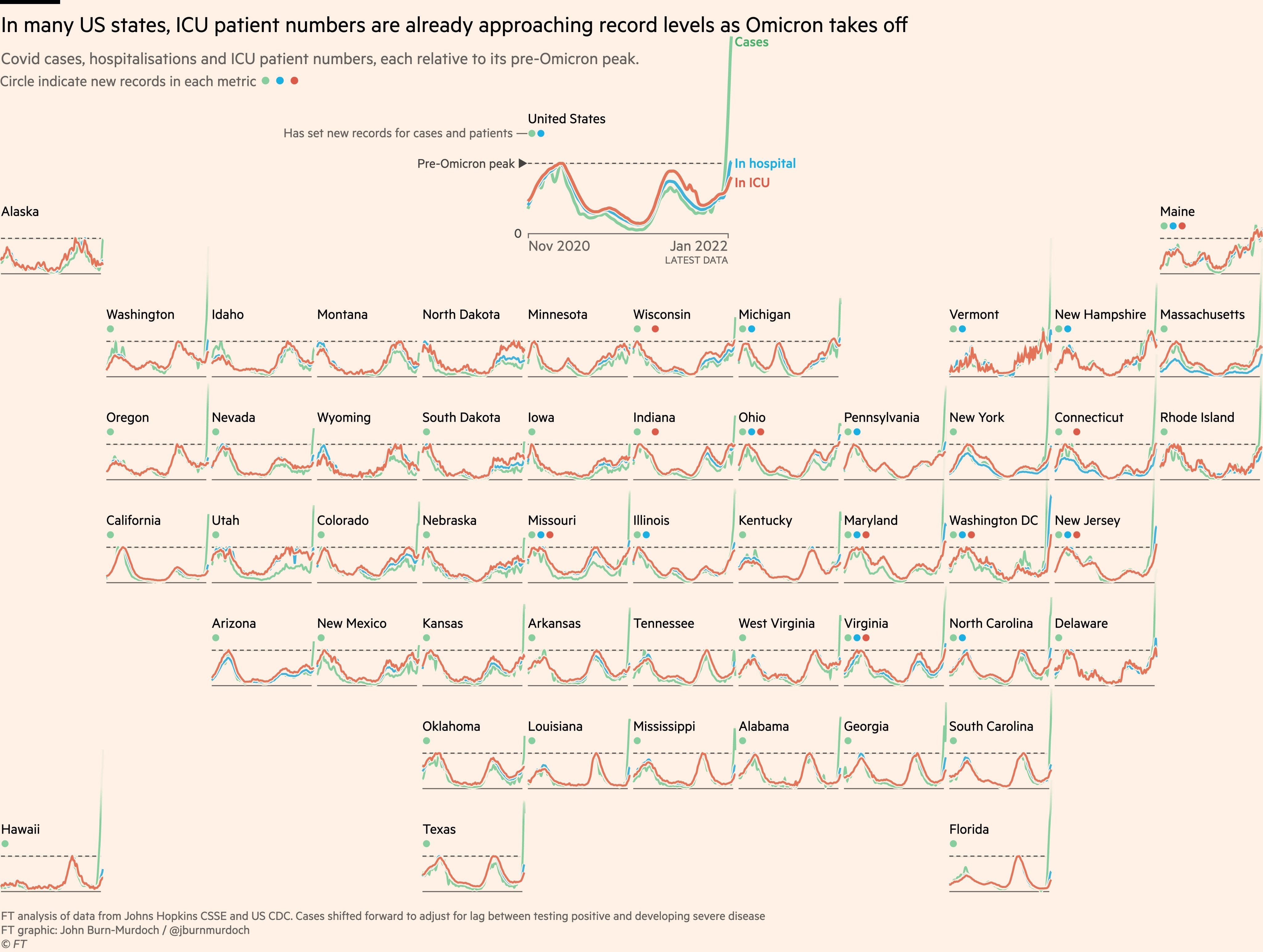
This map does not look great, but is probably selected to look scary and is also nowhere near as scary as I would have guessed a few weeks ago.
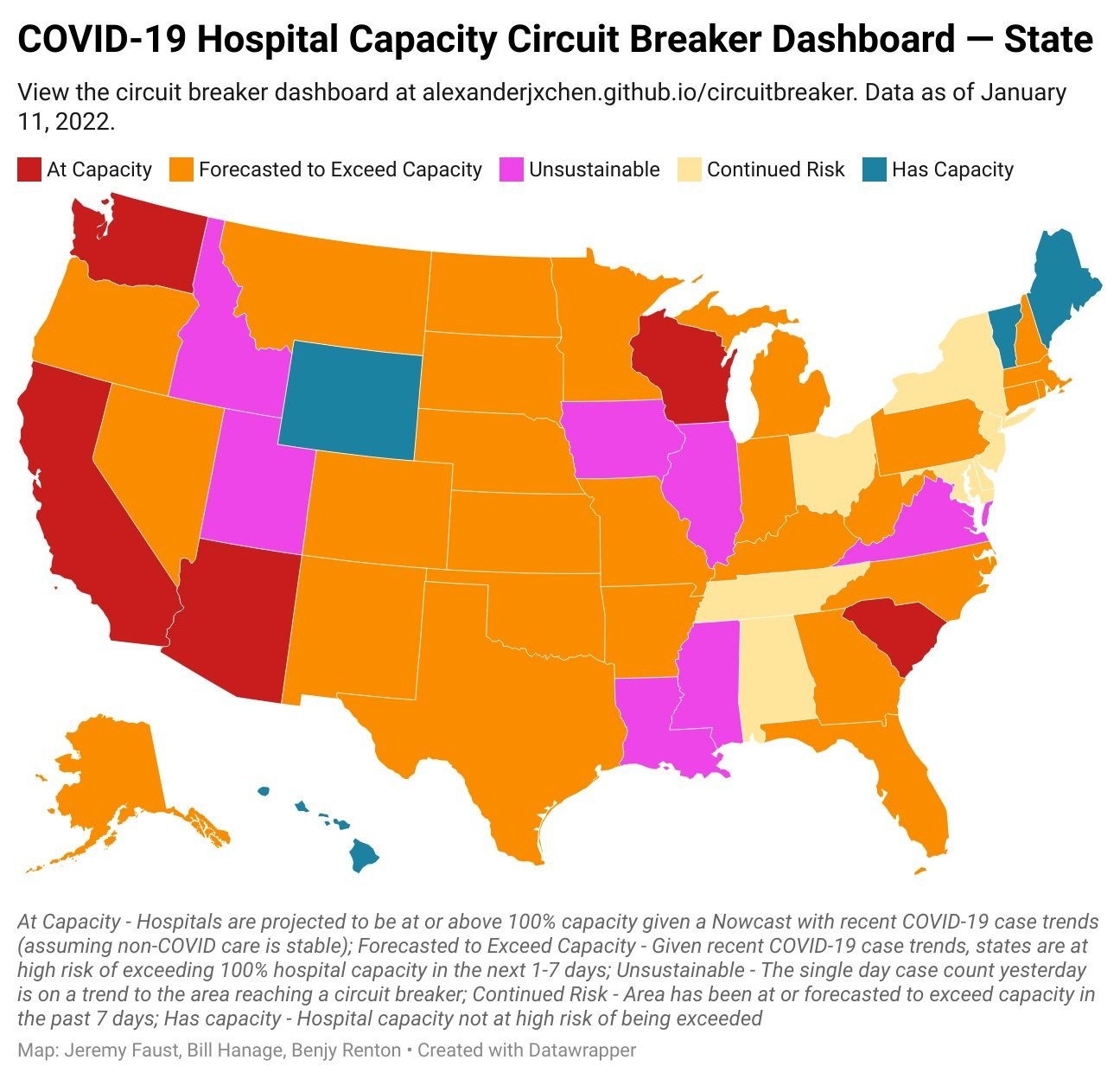
The Northeast has likely peaked in terms of cases, so the ‘continued risk’ column I think largely means things are not at risk. There isn’t that much population in the unsustainable areas here, which makes me think that it isn’t unsustainable by that much, and I expect peaks not too long from now. I am very much not making light of the situation, it’s going to suck quite a lot, but that was always the case.
Concretely here’s a report that Oregon is at 96% of capacity and that’s going up at 4%/week. Given the delay on hospitalizations after cases, will they exceed capacity? Probably, that curve would likely peak somewhere around 102%, but given the number of exponentials lying around this could have been so much worse.
Story continues to be largely about lack of staff causing the problem, rather than lack of beds.

Severity
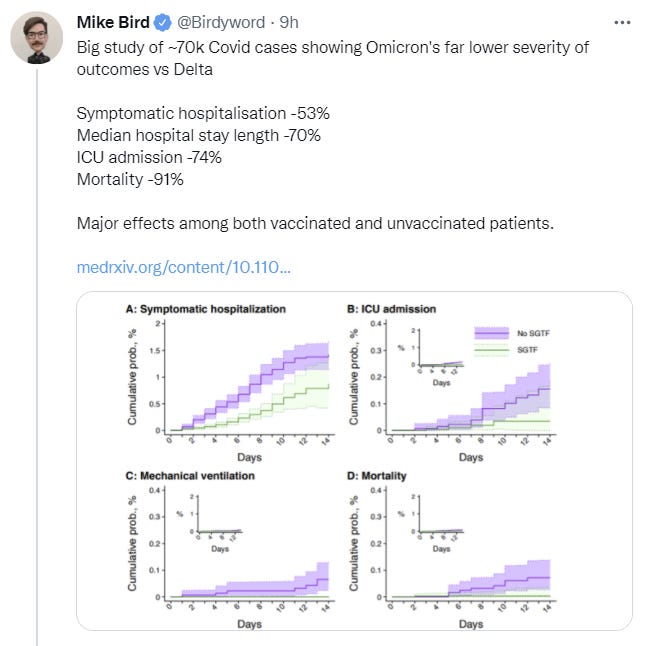
New paper finds greatly reduced severity of Omicron (direct paper link). I’m not thrilled with the controls used here but these effect sizes are so big it’s still a big game.
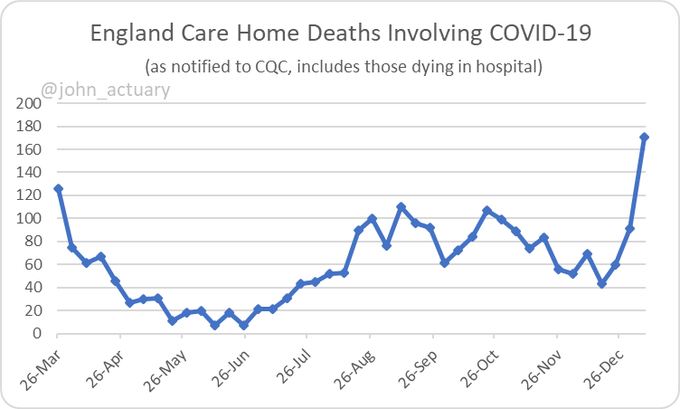
Nursing home Covid deaths up in the UK. Not good news, but once again less bad news than one might have feared, and cases are already turning around.
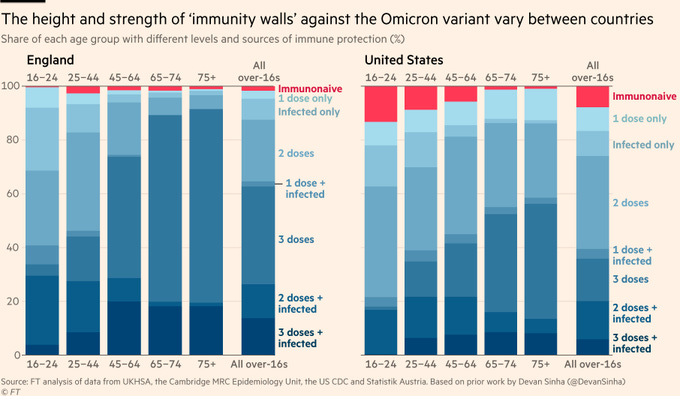
USA really does have a lot more immunologically naïve people than the UK, so we’re seeing more impact in the hospitals than other places.
Or we can look at real world data from a few other places.
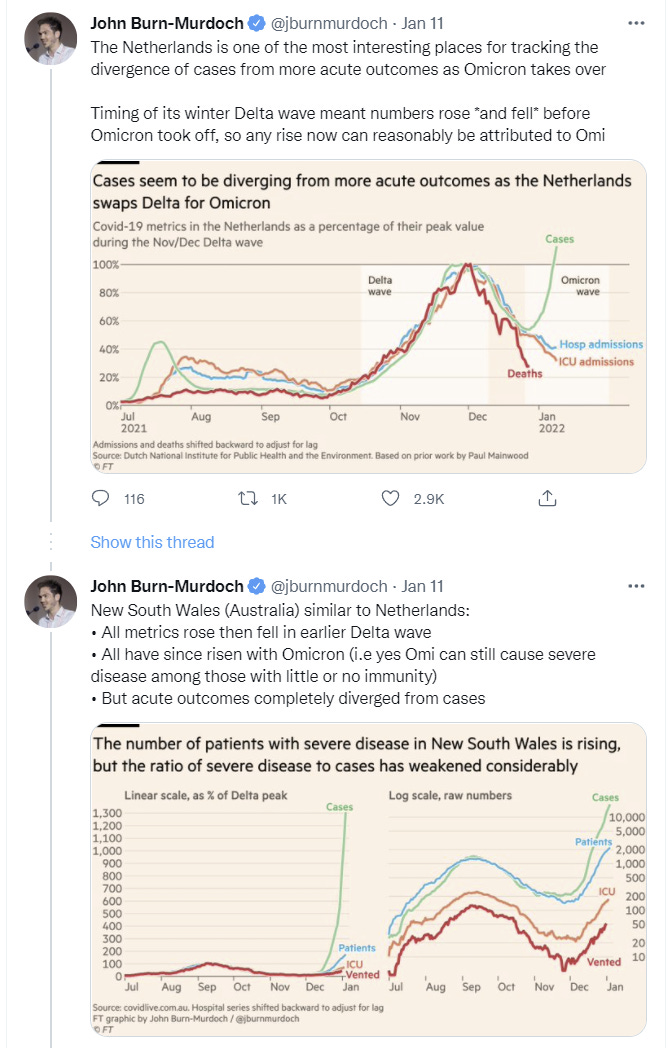
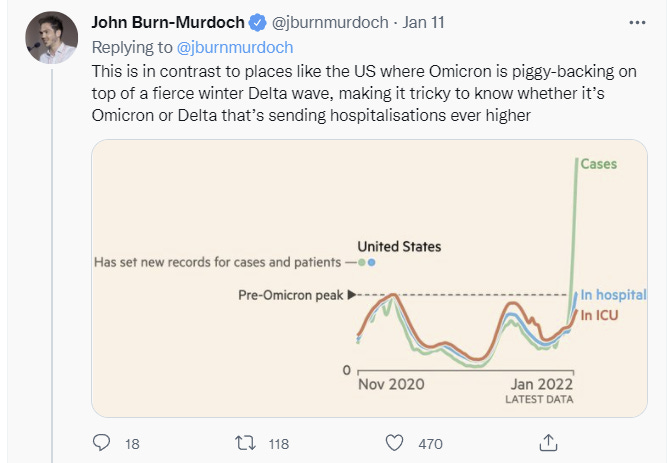
That last one is hard to read but it looks like divergence at least to me.
Outlook
Scott Gottlieb gives his prognosis on Face the Nation on 10 January. He thinks several states have already peaked, and the remaining biggest worry is in the midwest.
Current head of the FDA says most of us are going to get Covid-19, in so many words. The hospitals are going to hold, or at least mostly hold. Make risk decisions accordingly.
Would you pay a lot to have this be over, or not?
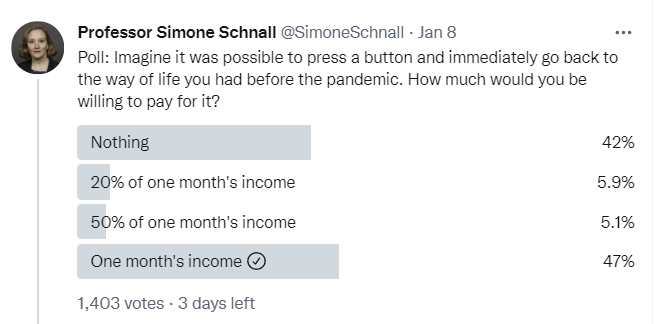
The people who answer ‘nothing’ here are either interpreting the question differently, they have very strange preferences, or they’re doing the thing where people refuse to pay for things if they don’t feel like it’s fair to be asked to pay for them. Once people acknowledge that the Before Times had their advantages, most of them are willing to pay over a month’s income, and a more interesting poll would have seen how far that goes. If answering in the spirit of the question, I would pay quite a lot, and also almost certainly not pay the full amount it was worth, if the full way of life includes everyone around me going back to the old ways and there being no Covid-19 to catch.
Thread from 8 January saying we might as well let it rip at this point, not like we have any choice.
China
Last time I asked others for opinions on the probability China could maintain its zero-Covid policy.
There are certainly signs things aren’t great. They confirmed Omicron’s presence, and they mass-tested 14 million people in Tianjin. The Olympics are still planned. But every day that passes is by default good news, so it’s not clear this is worse news than the baseline.
Here’s a roundup of takes I got.
First, an optimistic take at 70% chance that thinks China can’t fold and has the tools to win.
I would give the Chinese much better odds of keeping case counts under 50/million: 70%. China’s rulers are not lawyers and propagandists, agents of casuistry and illusion. They’re engineers and businessmen who have taken a mostly practical approach to the pandemic. And since learning to a large extent happens by doing, presumably their containment capability has incrementally improved. They are also willing to do what is necessary in accordance with their reality model, including firing deficient officials, as just happened again in Xi’an. The advent of Omicron means that they need to tighten travel restrictions further, which they’ve done for the upcoming Olympics. Another option is to acquire mRNA vaccines for those people who are most exposed to travel related risks. That would provide another defense line.
Xi has staked his reputation on this policy, and he’s also put the Party’s reputation on the line. This is crucial to them both domestically and for foreign consumption, to demonstrate the superiority of the Chinese system relative to America’s. Underlings who disappoint Xi are apt to face career destruction. The places that have seen massive Omicron outbreaks are also places that have let it rip. We haven’t really seen anyone try to contain it yet. Vaccination created what now seems like justifiable complacency. With the methods China has developed, I don’t think Omicron is that much more difficult to contain than previous variants. One reason I don’t give even higher odds is that Xi may discover that Omicron has something like a 0.1% mortality rate in China, which might at some point of national stress cause him to rethink the cost-benefit calculation. If a resumption of normality also occurs in the West while China suffers lockdowns, Xi might decide Zero Covid will not win the PR war. In other words, it’s easier for me to imagine them giving up than being defeated in battle.
Here’s a skeptical one, with a 25% chance, that thinks China can pivot and thus afford to fold.
China below 50 million: sell to 25%. My view is that most people overestimate the cost of switching to living with Omicron, e.g. “the Party has staked a lot of political capital on keeping Covid out”. That’s a severe underestimate of their propaganda/opinion guidance ability. If they want to change, they will be able to do so without paying much of a price in terms of social stability.
Here’s one that is far more optimistic than I that they can hide what is happening, I replied I would happily buy 33s and sell 80s (I’d definitely sell 80s either way, and given that I’d love to get the hedge too).
In autumn, Xi is looking to extend his term for another five years at a large party conference. Given the instability and uncertainty of what happens, if they give up on zero Covid, I can’t fathom that he would decide to give up before this important event. Afterwards, with potentially another Covid variant, and mRNA vaccines they might actually do it. However, they might just not release accurate testing numbers in that case. In fact, I don’t see why they would, it seems much more rational to just declare the pandemic to be over publicly (“we have never been at war with Covid”).
Before that, China should have enough capacity to contain the virus. Omicron has a shorter generational interval, which in some ways makes it easier to contain. Compared to Wuhan 2020, China has the capacity and the will to test everybody with PCR tests, vaccinations, and much improved digital tracking. Even if Omicron were twice more transmissible than the original strain, these improvements should offset it.China less than 50/million (officially): 80%
China less than 50/million (actual case counts, despite being unverifiable): 33%
This is another take that there’s a strong chance that Omicron comes and goes and China simply denies it. I don’t buy it. Either Omicron goes full blast or it is suppressed, and if it goes full blast I don’t see how they pretend it didn’t. Buying time is one thing, this would be very different.
A simple and skeptical take that makes sense.
Prediction responses (no strong outside view reasons to think I’m right here):
China keeps cases contained: sell to 30%. Their pulling out all the stops has been barely enough before, I expect even China to have lockdown fatigue and I generally expect Chinese government action to be less competent than e.g. Korea or Singapore.
This is a longer take that puts China’s chances even short term at 10%. Here’s one at 15%. This one says 20% if they don’t cancel the Olympics. Basically the argument is ‘it’s too hard, it can’t be done.’
None of the arguments on either side that were new seemed that strong, but overall I’m somewhat more skeptical than I was last week that China can pull this off.
Other and Threads
Wall Street Journal Editorial boldly goes somewhere, proposing it would be safer to speed up the spread due to effects on future mutations, and, well, wow, just wow, that’s a set of words they made me type, good show. Also inspired this rebuttal thread, if it isn’t obvious to you why the proposal makes no sense.
Andy Slavitt thread from 7 January. Still in the prevention mindset, but pointing out that the task is essentially hopeless.
Probability Updates
China keeps daily cases under 50 per million through 2022: 40% → 30%.
Having another mass testing round so quickly is somewhat bad news, and the ‘market’ I surveyed was generally on the lower end although with disagreement. I’m updating somewhat lower and we’ll go from here until we can get a real market up.
Median peak cases day for United States: January 19 → January 18
Mode peak cases day for United States: January 19 → January 17
Daily cases in the the United States have peaked by February 1: 90% → 93%.
My timeline has moved up on average as we see peaks, but given the lack of an overall peak yet the distribution is somewhat asymmetrical. A peak in February would at this point be very surprising, given some areas have peaked already, but strange things do happen.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? 50% → 45%.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 55% → 45%.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 95% → 97%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 30% (unchanged).
The general vibe that things get to be over makes me more optimistic about lifting restrictions in the medium term. Based on doing a bunch of modeling this week I’m finding myself putting in transmission edges slightly under 100% more than above so I should update there as well. The verdict on less virulent seems to be fully in but guarding against model error a bit, and for the 75% number I expect never to know for sure.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% (unchanged).
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 3% → 2%.
I was asked why my booster chance wasn’t updating. Basically it’s because I don’t expect much news at this time. They’re preparing the boosters as one would expect, but no idea whether they will push those boosters on the already boosted. As for the crisis scenario, it seems clear we won’t get there, things won’t justify a reaction and it would take a lot to provoke one. Again, holding back for model error, no one wants to end up in Bayes Hell.
Generation time (serial interval) of Omicron is 3.5 days or less: 90% (unchanged).
Modeling made it clear this is indeed in about this range for me right now. This is another ‘we’ll probably never know and I may never update here again’ case.
21 comments
Comments sorted by top scores.
comment by simon · 2022-01-13T20:54:06.889Z · LW(p) · GW(p)
Not sure what reasons the Wall Street Journal gave (haven't seen the article), but they're probably right. Faster spread doesn't change the total number of cases all that much v. slow spread but it does reduce the average number of sequential infections each lineage experiences before the disease burns out, thus the evolutionary distance possible for the disease to achieve.
Replies from: localdeity, yunxiang-zhu, CraigMichael↑ comment by localdeity · 2022-01-14T06:36:16.492Z · LW(p) · GW(p)
Exactly my logic. The more generations you have to work with (and apply selective pressure to), the easier it is to produce a highly-optimized virus (the thing we don't want).
Let's suppose that each person-to-person transmission adds mutations that affect the "badness" of the virus (say, immunity escape). I would assume you get a normal distribution. Now, suppose we want to make a virus that's 4 standard deviations above average.
If we have to do this in one generation... Wikipedia tells us that the rate of samples being >4 standard deviations away from the mean is roughly 1 in 16k; since that includes both below and above, we would need 32k infections on average to produce the +4sd virus.
If we have two generations, then what we can do is produce a +2sd virus in the first generation, select it (assume we can do this perfectly), and use it to produce candidates for the +4sd virus. +2sd is 1 in 44, so on average we would need 44 infections in the first generation to make the +2sd virus, then make 44 more from it, for a total of 88 infections. With 4 generations, we need 6 infections per generation to gain +1sd, totaling 24 infections.
If we wanted to make a +6sd virus: 1 generation requires 1 billion infections, 2 generations requires 740 x 2 = 1480 infections, 3 generations takes 44 x 3 = 132 infections, and 6 generations takes 6 x 6 = 36 infections. If we wanted to make Delta... I have no idea how many standard deviations it is from the original SARS-CoV-2, but I'm confident that we wouldn't get anywhere near it if COVID Patient Zero infected the entire planet by direct transmission.
For another angle: Suppose you have a budget of 1000 infections. If you have 1 generation, then you can gain about +3sd in that generation. 6 generations, you can get +2.5 per generation, totaling +15sd. 20 generations, you get about +2sd per generation, totaling +40sd. 70 generations gives you about +1.5sd per generation, yielding +105sd.
Changing the size of each generation has only a marginal effect on how many stddevs you can get from it. The probability density function for standard deviations decreases superexponentially with the distance from the mean. Much more important is the number of generations you have.
Now, this is with utterly perfect selection on every generation, if we take the best (worst) virus from each generation and delete all the rest. Luckily real selection pressures are a lot weaker than that. But I think models would essentially be "if you're infecting N people in each generation, then the next generation's virus will be, on average, +x standard deviations more infective/immune-escaping/etc. than the previous", and I'm pretty sure the fact will remain that doubling or even tripling N will have only a small effect on x. An intuition pump: Shrinking the generation size means taking people who would have been infected by virus version n (plus mutations), and instead infecting them with version n+1 (plus mutations); clearly this accelerates development.
Therefore, if, say, 4 billion people will get infected, and if we want the virus to be as little evolved as possible by the end, then we should make this happen in as few generations as possible. (This to be balanced against the risk of having so many people sick at once that (a) health care systems are overwhelmed or (b) other services have too many workers out sick. Also, there is something to be said for waiting for treatments like Paxlovid, although my impression is that's not a practical goal for most people.)
↑ comment by Yunxiang Zhu (yunxiang-zhu) · 2022-01-14T01:17:06.975Z · LW(p) · GW(p)
Delta and Omicron are not in same sequence. Serotyping separating is happening. All the pains and deaths may not worth it.
Replies from: simon↑ comment by simon · 2022-01-14T02:59:29.211Z · LW(p) · GW(p)
I'm not sure what your point is here? Omicron is, to my understanding, replacing delta, which should be benefecial.
Replies from: yunxiang-zhu, cistrane↑ comment by Yunxiang Zhu (yunxiang-zhu) · 2022-01-14T03:32:23.295Z · LW(p) · GW(p)
Omicron is Delta's "nephew"
↑ comment by CraigMichael · 2022-01-14T11:14:20.864Z · LW(p) · GW(p)
it does reduce the average number of sequential infections each lineage experiences before the disease burns out
Does it, though? As a thought experiment say we just let just let A.1 rip. No lockdowns, no nothing. It burns though the world some number of months, say 3-4.
Would we not see lineages evolve in that time? There would likely be more replications in that scenarios than in the approach we’ve taken now. So maybe I can imagine there’s reason to think we’d see more linages in that scenario than we do now.
comment by AnthonyC · 2022-01-14T00:20:49.659Z · LW(p) · GW(p)
Whenever someone asks a poll question about how much people would be willing to pay to something, I wonder how much of the answer is liquidity constrained. People who live paycheck to paycheck (a majority of Americans) who literally wouldn't be able to pay a week's income for any new expense might just not engage with the counterfactual in quite the way that it was intended.
Replies from: AspiringRationalist↑ comment by NoSignalNoNoise (AspiringRationalist) · 2022-01-15T23:54:42.969Z · LW(p) · GW(p)
There's also an asymmetry between gains and losses, partly due to prospect theory, and partly due to decreasing marginal utility. I bet a lot of people would answer differently if they were asked what they would choose if given the choice between receiving the money vs. going back to the way things were before.
comment by Adam Zerner (adamzerner) · 2022-01-13T19:00:12.623Z · LW(p) · GW(p)
From various sources, I have become convinced that rapid tests taken from nose swabs are likely to often be several days slower at detecting infections than rapid tests that use throat swabs.
I'm confused about how this works. Does the test have to be designed for throat swabs rather than nasal swabs? I see some language about adding a throat swab, which would indicate that the answer is "no", but other language feels like it points towards a "yes".
comment by ponkaloupe · 2022-01-13T20:42:12.241Z · LW(p) · GW(p)
regarding that poll:
[how much would you pay] to go back to the way of life you had before the pandemic?
i really can’t think of any previous lifestyle that i actually want to go back to living. maybe it’s because i’m young, but if my lifestyle this year is ever worse than the prior year, that’s pretty close to saying that i failed at life for that year. humans are adaptable: i’m not at all surprised if 42% of respondents have adapted over the last two years and created new habits and ways of life that they aren’t interested in giving up. i’m \it{happy} for those who wouldn’t revert their lifestyle changes for a modest amount of $, because it hints that they made very positive lifestyle changes.
Replies from: JBlack↑ comment by JBlack · 2022-01-14T00:47:09.869Z · LW(p) · GW(p)
I'm very happy to be able to work 100% from home, where previously I was 0% able to work from home. I had previously asked to work from home and was flatly refused.
I would pay quite a large amount (such as a month's income) to avoid going back to that, especially since the pandemic has not yet had any comparable negative effects on my life.
comment by jmh · 2022-01-14T05:05:54.730Z · LW(p) · GW(p)
Curious on the testing note. Should I be inferring that Omicron is not as active in the nasal passage ways but rather in the upper throat? In other words, has the mutation changed the location of entry -- might not be the correct way to say that. I thought the general understanding in the past was the the virus really replicated in the upper/nasal area before spreading in the body.
comment by rosyatrandom · 2022-01-14T10:17:17.176Z · LW(p) · GW(p)
I just wish the throat swabs didn't trigger my gag reflex.
I didn't even know I had a gag reflex until I took one, and it makes the swab pretty useless as I can't get near my tonsils without having to stop before I throw up.
Replies from: Celarix↑ comment by Celarix · 2022-01-14T16:58:44.325Z · LW(p) · GW(p)
Probably not helpful today, but I've had success in reducing my horrible gag reflex by brushing my tongue for 10 seconds each day. I've been doing it for a few years, but I think I got most of my benefit in the first few months.
For something more likely to be helpful today, I've also had success with Chloraseptic throat spray to temporarily numb my throat.
comment by wangscarpet · 2022-01-14T17:22:01.878Z · LW(p) · GW(p)
What do median and mode case peaks mean here? Is that on your ordering of day? Like, if for Jan 15-19 there's a 10,20,30,14,16 is the mode the 17, the median the 19th, and the mean whatever you'd get by averaging?
comment by CraigMichael · 2022-01-14T11:02:52.293Z · LW(p) · GW(p)
Since it’s not mentioned elsewhere, there’s a good article from the Skeptical Cardiologist on paxlovid drug interactions. A lengthy quote:
Patients with hypertension, coronary artery disease, atrial fibrillation, and hyperlipidemia should pay close attention to what follows if they are considering starting the drug as they likely will need to stop or modify their cardiac medications and monitor their blood pressure and heart rates closely while taking it.
Paxlovid contains ritonavir-boosted nirmatrelvir.
Ritonavir has long been used to increase the levels of anti-HIV medications by strongly inhibiting the cytochrome P450 (CYP) 3A system which metabolizes many cardiac (and non-cardiac) drugs including nirmatrelvir, the active anti-SARS-CoV2 antiviral.
The EUA for Paxlovid makes it clear how important it is for patients and physicians to be aware of these powerful drug interactions:
Clinicians who are not experienced in prescribing ritonavir-boosted drugs should refer to resources such as the EUA fact sheet for ritonavir-boosted nirmatrelvir (Paxlovid) and the Liverpool COVID-19 Drug Interactions website for additional guidance. Consultation with an expert (e.g., clinical pharmacist, HIV specialist, and/or the patient’s specialist provider[s], if applicable) should also be considered.
comment by Daniel V · 2022-01-13T22:00:53.742Z · LW(p) · GW(p)
My worry was that maybe an antigen throat test would need a different design/reagents/whatever (since there'd be a lot more saliva, etc.) than an antigen nasal test to be sensitive. Apparently the health authorities will not explain any of the "under the hood" issues (just that a throat swab is more difficult, and therefore more dangerous, to do to yourself), and the expert WaPo got is worried not about false negatives but false positives! First, the specificity of the tests are great so it's hard to fathom what would be introduced to drop that, and second, false positives (as long as they aren't extremely common) are fine if we're talking about spread control. Plus, a quick Googling on flu nasal/throat swabs kinda suggests there's probably not a design issue. Throat swab it is!
comment by crn · 2022-01-13T20:11:04.902Z · LW(p) · GW(p)
How should we interpret the "with covid" numbers when trying to estimate the chance of being asymptomatic? My intuition is people admitted to the hospital are generally less healthy than the rest of the population. Is it fair to assume that the 12% asymptomatic rate from UCSF should be a strict lower bound on the probability that a boostered and healthy 20 something (asking for a friend) person would be asymptomatic if they caught covid?
Any good estimates on the asymptomatic rate by demographic? Maybe workplaces or schools that test regularly, or from surveillance testing?
Replies from: tslarm, cistrane↑ comment by tslarm · 2022-01-14T02:17:34.444Z · LW(p) · GW(p)
I think 12% is the positive rate among patients without symptoms at the time of the test, so if you want to extrapolate from there to an estimate of your chance of experiencing no symptoms, you'll first need to estimate how many of those people were in fact presymptomatic.
edit: also, if I'm reading your comment right, I think you're interpreting 12% as the proportion of positive cases that had no symptoms, whereas it's actually the proportion of people without symptoms who tested positive:
~1-in-8 UCSF patients w/ NO Covid symptoms are testing +