Covid: The Question of Immunity From Infection
post by Zvi · 2021-01-20T15:50:01.101Z · LW · GW · 9 commentsContents
9 comments
Over and over and over again, I’ve been told we should expect immunity from infection to fade Real Soon Now, or that immunity isn’t that strong.
With several recent papers and the inevitable media misinterpretations of them, it’s time to take a close look at the findings.
This was originally part of the 1/21 update, but I’ve split it off so that it can be linked back to as needed, and to avoid cluttering up the weekly update.
Note that this post is not looking at any new strains that might provide immune escape. It’s studying infections during a period when such strains were not a substantial issue. This is distinct from concerns about strains with immune escape characteristics.

From this, of course, media headlines were things like “immunity only lasts five months,” but let’s ignore that and keep looking at the data, and see what the study actually says.
RESULTS SECTION:

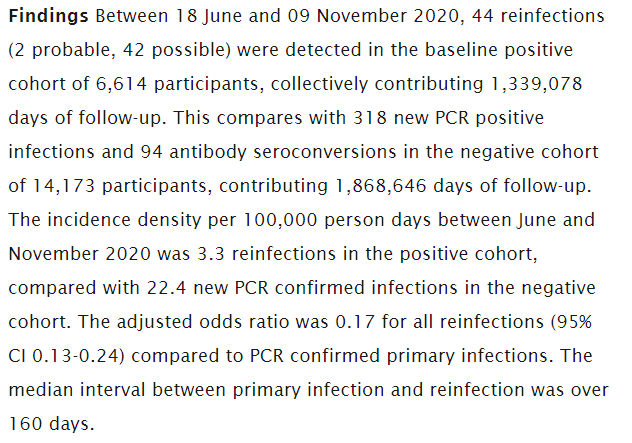
Bottom line infection rates:

Finally:
I’ll pause here before I read the discussion section.
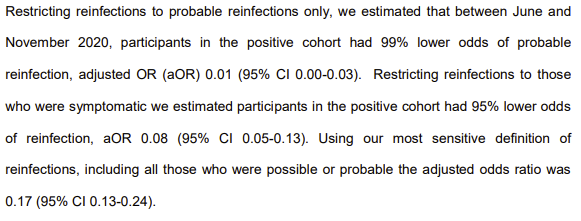
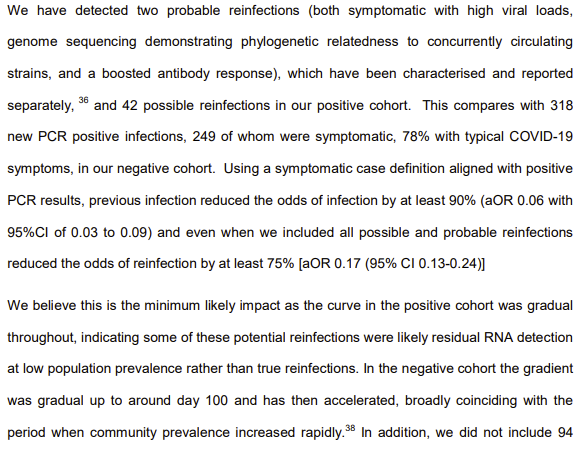
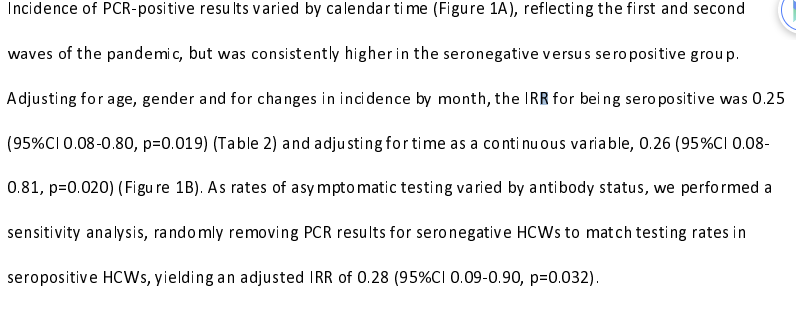
What I am seeing is that in probable infections, meaning infections that were serious enough and real enough to get confirmed, we see a 99% reduction, a large enough reduction that error in the original antibody/PCR tests might well account for either or both of the remaining two (2) cases.
Even looking at only symptomatic infections, we still get a 95% reduction.
Whereas if we only look at ‘there was a test that came back positive on people getting periodically tested, but without requiring any symptoms or verification’ we only get an 83% reduction.
Naturally, the public-facing articles all seem to quote the 83%, and ignore the 95% and 99%.
I’d also note that they nowhere attempt to control for the two most obvious differences between the two samples, which are:
- The antibody positive sample knows they are antibody positive, and thus likely took fewer precautions across the board than they would have otherwise.
- The antibody positive sample are the people who got infected the first time.
If immunity conferred zero protection, what do you think the risk ratio would have been? Three?
(And again, they also take something presented after five months of follow-up, and report it as ‘immunity lasts five months’ because journalism.)
They start off with this in the discussion, which seems maximally skeptical (e.g. ‘at least 75%’ means the 95% CI starts at 76%) and they seem to know it:
Primary conclusion here seems very clear. Past infection is highly effective protection against future infections that matter.
Secondary conclusion is that our tests are not perfect, and when you loosen your criteria, you get a bunch of false positives.
Also that it is perfectly fine not to consider that there might be a difference between the behaviors, past and present, or the prior health or immunology, of those who are known to previously have had Covid-19, in a scientific paper, with a straight face.
Mostly, this paper confirms that dogs bite men, and it is much rarer for men to meaningfully bite dogs.
On to the second paper, also oh my eyes, ouch this typeface my eyes.
First thing I note is that they used “Poisson regression” which might be technically correct but is a deeply, deeply silly way to say that you’re counting the number of days of exposure.
How scientific papers say something is “so overwhelmingly obvious we didn’t actually need to do this study but we did anyway” these days:
Their data:
Their bottom line:
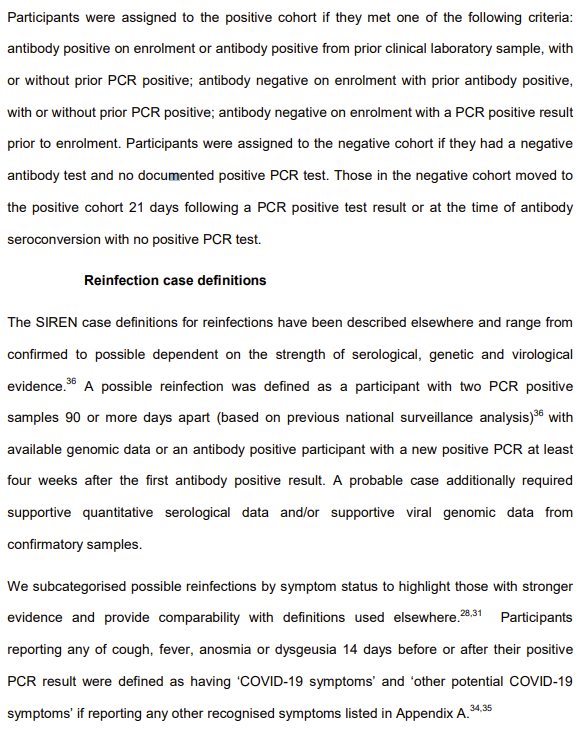
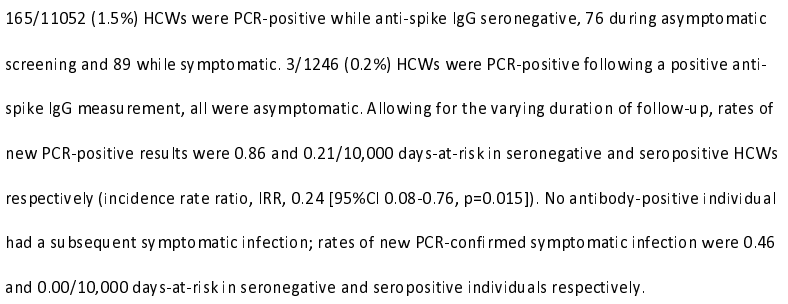
The study assumes that people are protected a minimum of 60 days following infection, and only considers exposure days after that, then measured relative frequency of positive testing of various types.
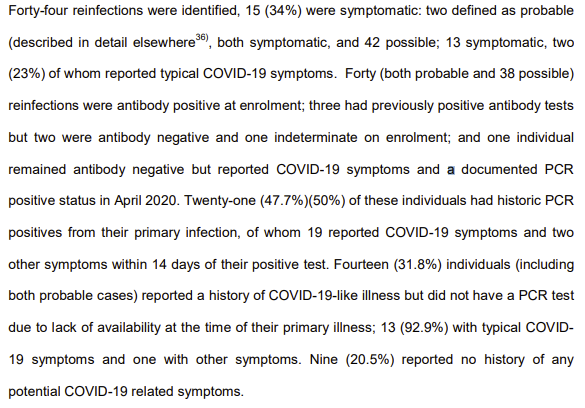
There were zero symptomatic reinfections, while roughly half of all positive tests in the non-infected group had symptoms. Various tricks get them all the way to only a 72% reduction in infections for the previously infected group, while once again not at all taking into account any way the group differs, or the rate of false positives.
These two studies, taken together, seem to tell a clear story. You are not fully protected against getting a positive PCR test, and thus there is some chance you could at future points be somewhat infectious, but for the duration of the studies you are at essentially zero meaningful health risk, or even risk of showing symptoms, from Covid-19 if you were previously infected.
9 comments
Comments sorted by top scores.
comment by Gunnar_Zarncke · 2021-01-20T18:19:31.080Z · LW(p) · GW(p)
I saw this headline on Slashdot:
Almost a Third of Recovered COVID-19 Patients Return To Hospital In Five Months, One In Eight Die
I tried to find the original study and it seems to be PHOSP and there is this on Medarxiv:
Epidemiology of post-COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study
Results Mean follow-up time was 140 days for COVID-19 cases and 153 days for controls. 766 (95% confidence interval: 753 to 779) readmissions and 320 (312 to 328) deaths per 1,000 person-years were observed in COVID-19 cases, 3.5 (3.4 to 3.6) and 7.7 (7.2 to 8.3) times greater, respectively, than in controls. Rates of respiratory, diabetes and cardiovascular events were also significantly elevated in COVID-19 cases, at 770 (758 to 783), 127 (122 to 132) and 126 (121 to 131) events per 1,000 person-years, respectively. RRs were greater for individuals aged <70 than ≥ 70 years, and in ethnic minority groups than the White population, with the biggest differences observed for respiratory disease: 10.5 [9.7 to 11.4] for <70 years versus 4.6 [4.3 to 4.8] for ≥ 70 years, and 11.4 (9.8 to 13.3) for Non-White versus 5.2 (5.0 to 5.5) for White.
Conclusions Individuals discharged from hospital following COVID-19 face elevated rates of multi-organ dysfunction compared with background levels, and the increase in risk is neither confined to the elderly nor uniform across ethnicities.
https://www.medrxiv.org/content/10.1101/2021.01.15.21249885v1.full
↑ comment by arunto · 2021-01-20T21:37:18.665Z · LW(p) · GW(p)
That doesn't look good. However, it could be less bad than it looks because of their matching criteria (Supplementary Table 1) not really assessing the severity of different types of prior health issues but their existence only (probably because that is what they had access to for such a large sample), e.g. "history of diabetes: Yes/No".
I think that a latent health status with a high probability of having complications (leading to a hospital stay) if contracting COVID-19 is also linked to a higher probability of a hospital stay or death in the following months even without contracting COVID-19. Hard to tell how much one should correct down the results of the study for deaths and hospital admissions based on that (but I believe there still remains a substantial negative long term impact by the infection with COVID-19).
comment by Sherrinford · 2021-01-21T11:24:12.063Z · LW(p) · GW(p)
"Over and over and over again, I’ve been told we should expect immunity from infection to fade Real Soon Now, or that immunity isn’t that strong. ... the inevitable media misinterpretations ... Naturally, the public-facing articles all seem to quote the 83%, and ignore the 95% and 99%. ... (And again, they also take something presented after five months of follow-up, and report it as ‘immunity lasts five months’ because journalism.)"
While this may be true (who knows), can we maybe make it a norm to back up major empirical claims and generalizations with evidence?
comment by TheMajor · 2021-01-21T10:53:00.798Z · LW(p) · GW(p)
To what extent does 'positive PCR test' equate to 'infectious'? Or is there some other good indicator? I know most health authorities say something like "if you have been contact with a person who tested positive, then from the point they are no longer symptomatic/first negative test after you have to be careful for X days', so I assumed they are (somewhat) related.
comment by kjz · 2021-01-21T01:50:09.581Z · LW(p) · GW(p)
Thanks for following up last week's discussion about the first paper. It's pretty sad that it falls on internet sleuths to debunk claims that should be obviously questionable after thinking for two seconds about the underlying scientific principles, but so it goes. This study should have been flagged immediately by a competent peer review process.
On a personal level though, I'm thankful I've been able to improve at noticing such claims myself, thanks in large part to things I've learned here.
comment by Annapurna (jorge-velez) · 2021-01-21T13:47:50.120Z · LW(p) · GW(p)
While I concur with your conclusion, I fear that if mainstream media presents the results like you did in this post, it will create a perverse incentive.
I posted the UK press release in my social media and immediately folks started saying that they should try to catch it in order to get immunity.