The literature on aluminum adjuvants is very suspicious. Small IQ tax is plausible - can any experts help me estimate it?
post by mikes · 2023-07-04T09:33:51.849Z · LW · GW · 3 commentsThis is a question post.
Contents
Study 1 None Answers 37 Lao Mein 3 Οἰφαισλής Τύραννος 3 avturchin 1 Ben Declerck 1 DirectedEvolution -5 prepper None 3 comments
I am a PhD biostatistician who has worked on a project in this area. I am hoping to crowdsource opinions on this issue, especially from readers with knowledge of neurology, nephrology and/or toxicology.
The recent news cycle motivated me to spend some time reading up on the safety literature for aluminum vaccines. Aluminum is not in the Covid vaccine, but it is in many childhood vaccines.
I am deeply unsettled by what I found. Here is a summary. I would appreciate being corrected in the comments:
- The science on this topic is surprisingly neglected. Aluminum is a known neurotoxin in small concentrations in the brain. So, the obvious follow-up question: "Is the amount accumulated from childhood vaccines so small as to be irrelevant?" Unfortunately, aluminum has not undergone rigorous safety testing for cumulative cognitive effects. The fact that I could not find a convincing answer reflects a multi-decade policy failure.
-The evidence for safety cited by regulators and mainstream review papers appears to have gaping issues (see end of post for notes on the studies Mitkus et al (2011) and Karwowski et al (2018). They do not justify anywhere near the amount of faith being placed in them.)
-Mainstream educational sources are gaslighting readers by suggesting that the net exposure in vaccines is less than dietary exposure, e.g. here is what CHOP's Vaccine Education Research Center says
but this fails sanity checks with basic multiplication, given the oral bioavailability of aluminum is about 0.1 - 0.3% in diet and <0.01% in antacids according to the ATSDR. No wonder people are going nuts about the public health experts.
-There is a whole literature of claims on blood brain barrier mechanics, chemical state of the aluminum after injection, and transport via macrophages, which regulators are ignoring, but should probably affect the analysis of Mitkus 2011. I am entirely unqualified to judge and don't particularly trust this literature, so I'm ignoring this but looking forward to comments on the topic.
-Alternatives to aluminum exist, including mRNA and other new adjuvants. In the 2000's, regulators pushed industry to remove mercury from childhood vaccines; they should consider doing this again.
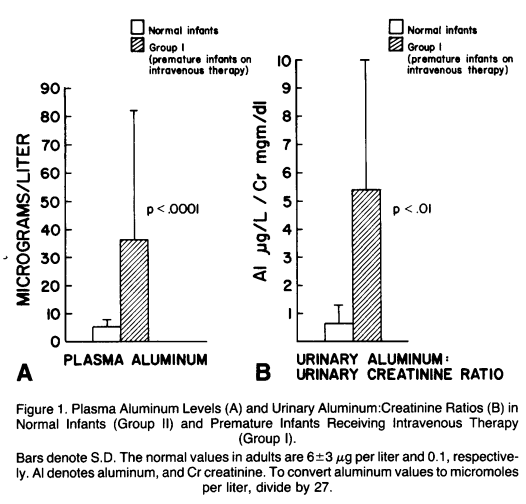
-A cognitive tax due to aluminum on the scale of ~0.1 IQ point for the first Hepatitis B shot is plausible (that's just from the first 250 micrograms of Al. There are > 4 mg in the whole schedule). That's my rough fermi estimate, based on an experiment showing developmental delay in premature infants exposed to hundreds of micrograms aluminum in IV fluids (Bishop et al 1997). This estimate is extremely sensitive to assumptions about renal clearance and sensitivity of brain development in premature infants compared to full term. Can anyone suggest a more accurate method? With this approach: does anyone know enough nephrology to pin down the length of time that intravenous aluminum in Bishop's premies would have spent circulating in blood, given their reduced renal function? Anyone know enough neuro to comment on whether impacts on cognitive development should be linear in the amount of neurotoxin? How much larger should it be in premies vs term infants?
______
Notes on failures in the literature:
Claims of safety of aluminum seem to bottom out in mainly two papers: Karwowski et al (2018) and Mitkus et al (2011). The FDA cites Mitkus 2011 to determine a tolerable risk level of aluminum exposure and argues that vaccine exposure is below it; the UK health authority and various review papers (such as this one) cite Karwowski as evidence of low accumulation of aluminum in infants.

Study 1
-Mitkus et al (2011) which the FDA commissioned on this topic, argues that exposure to aluminum due to vaccines is low compared to oral exposure limits. The trouble is that the study uses an old and unusually large dietary absorption figure (0.78%) [apparently Keith et al 2002, to which Mitkus is an update, uses the same number], and that 0.78% number is now well out of range from more recent estimates: average 0.1% bioavailability from diet according to the ATSDR.
This criticism is also made here. If this criticism is correct, vaccine exposure appears to be well above the scale of dietary aluminum exposure. Eyeballing the figures in Mitkus, reducing the MRL by a factor of 8 seems to consume more or less the entire safety margin, and should reverse the conclusion of safety. I have been unable to find an adequate regulatory response to this criticism.
_________
Study 2:
-Karwowski et al (2018) is cited in a number of review articles to argue that the body aluminum burden in infants attributable to vaccine Al content has been minimal. But based on the limited results presented, the study does not seem capable of supporting such a takeaway, due to lack of variability in the regressor variable (total vaccine aluminum dose). The analysis runs a regression and finds that aluminum contents in the blood and hair of 9-13-month-olds are not correlated with prior vaccination aluminum exposure. But the spread of the aluminum exposure range in their data is incredibly small, so this regression analysis could not have had any power to detect a signal. I can't be certain because they don't plot their data or report a coefficient table, but the paper says of their sample: "Median estimated cumulative vaccine aluminum load was 2.9 mg (range: 1.43-3.55mg, IQR = 0.11mg)." Most of their patients were following the schedule - great for the patients! But terrible for the experiment quality. The small variability they did have was probably age-correlated - so, the increased aluminum due to having had more shots would have been spread out in a larger infant's body. Not to mention, hair gets cut by the time a child reaches 13 months, blood clears rapidly, and the early exposure is probably what matters most for the brain. This study appears to be basically useless, and it is damning that a mainstream review such as Destafano, Bodenstab, and Offit (2019) would say: "The strongest evidence of the safety of aluminum in childhood vaccines is provided by [Karwowski et al 2018]."
Answers
The crux of your argument, that micro-gram level AL exposure has negative impacts, is based on the premature infant aluminum toxicity paper. It's a p-hacked piece of junk. They found no significant effect (P=0.39!!!) and then started analyzing subgroups until they got a p<0.05. Without adjusting for multiplicity, of course. Its implications would also only generalize to premature children. In addition, this study focuses on premature infants, not vaccine-age children. And blood AL levels were never taken! It's a bad paper and should be ignored.
On the other hand, this publication cites a paper noting that radio-labeled aluminum has 99.5% of injected aluminum being removed from the blood after 24 hours... but also that 50% is removed after an hour, and that it has a biological half-life of 7 years (!!??). Apparently, it mostly settles to the bones. This matches the 40-50mg total AL load figure I've seen elsewhere.
This brings us to Priest's paper, which actually explores the blood-brain barrier in regard to aluminum and it estimates... 8 micrograms of transfer from the blood to the brain per year. The brain has much lower levels of AL than the rest of the body. This implies that sudden spikes in blood aluminum levels simply won't have a major impact. Remember, aluminum can only cause brain damage if it reaches toxic levels. High blood AL only increases the speed at which brain AL levels increase. What really matters is the actual levels of brain AL, which is determined by long-term blood AL levels.
So let's look at chronic exposure. The average human consumes ~10mg of aluminum in their diet daily. Assuming 0.1% bioavailability, this is 0.01mg per day. Over a year, that's equivalent to a 4mg injection of aluminum. So more than you get from the entire vaccine schedule.
Edit: I forgot children were tiny. Whoops. So you still get more AL in your blood from the vaccines than normal food.
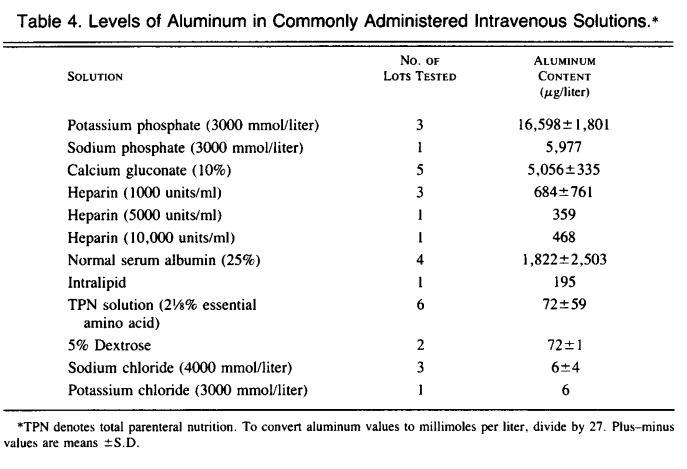
Edit2: It turns out that people actually just went and injected premature infants with massive amounts of IV aluminum until some had toxic levels of AL. Apparently, some were getting 100ug of IV AL per day, most of it from non-food IVs (16.6 mg/L for potassium, which is just nuts).
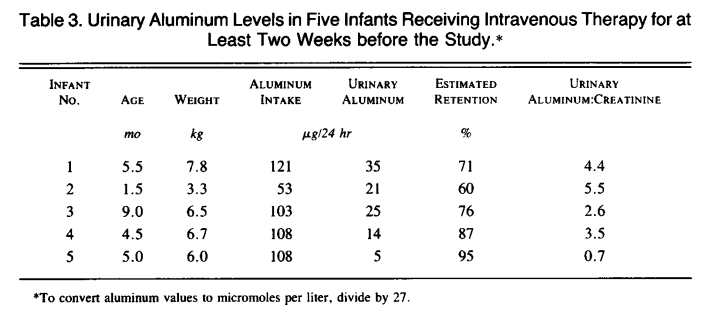
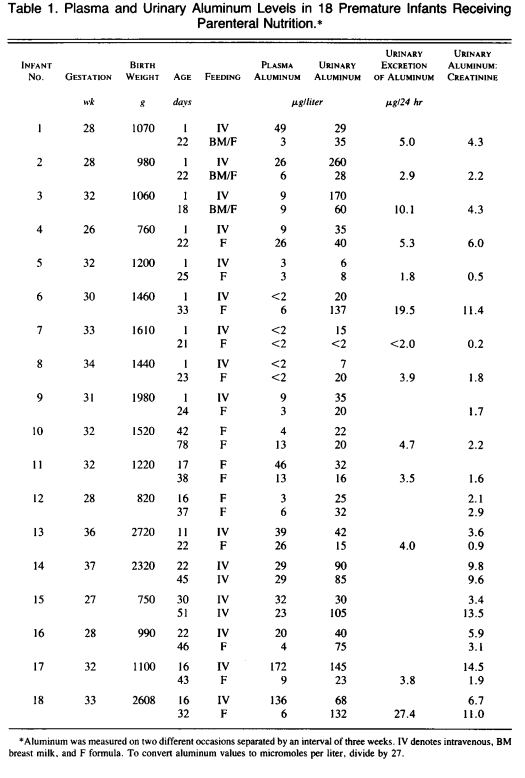
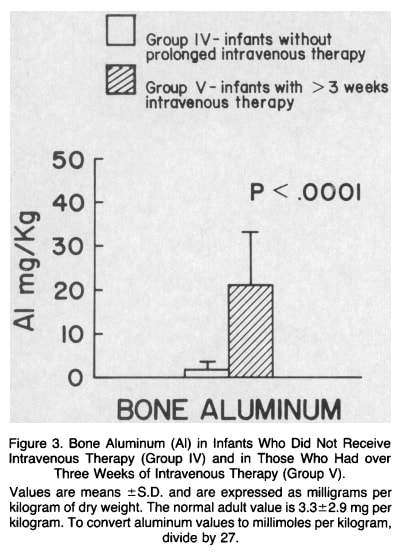
The infants in this study were injected with <3mg of IV AL over the course of a few weeks, and you see 10x levels of AL in all their tissues compared to controls. If we take ~100 ug/day, multiply that by 20 days, we get~2mg of aluminum. The highest blood AL levels detected was 172, so I guess in a worst-case scenario, for the Hep B vaccine at birth (200 ug AL), you can expect an increase of ~17 ug/L of blood AL for a few days/weeks? That seems fine? And every shot afterward is for a much bigger child, so I don't think it's too problematic. Premies also seem to have similar renal AL expulsion rates as adults most of the time. Except when they don't. I think you can maybe make a precautionary case about the at-birth Hep B vaccine specifically for renal-impaired premies, but not anything else.
And yes, it looks like the AL is sinking into the bones. A newborn has 80 g of bone on average, and 20mg/kg * 0.08kg = 1.6mg of aluminum. That's where it all went! The numbers end up working out, which is nice.
Is there maybe a way for immune cells to carry aluminum directly to the brain? Possible. If you find a paper finding evidence of that, I'll take a look at it, but my intuition is that it's unlikely.
↑ comment by bhauth · 2023-07-04T21:09:46.763Z · LW(p) · GW(p)
Replies from: ChristianKl, mikes↑ comment by ChristianKl · 2023-07-05T12:20:01.351Z · LW(p) · GW(p)
It seems that mRNA vaccines basically don't need any adjuvants because the RNA in the vaccine is already working as an adjuvant.
That suggests that any RNA/DNA would work and you don't need the specific DNA of the host. Giving some random DNA might work as an adjuvant.
DNA also has the advantage that it's a big molecule and thus won't cross the blood-brain barrier.
↑ comment by mikes · 2023-07-05T17:46:38.497Z · LW(p) · GW(p)
Great post!
One update to make is that the dietary absorption figure (.78%) used by Mitkus to map from the dietary MRL to intravenous seems to be off by a factor of 8 (the ATSDR says average dietary bioavailability is 0.1%; the .78% number is out of range from all other study estimates and doesn't even make clear sense as a takeaway from the Al-26 study that it came from); so the exposure amount from vaccines appears to be basically equal to the MRL, rather than well below.
So that would put us at exposure comparable to 1% of what's needed for "observable effects" in mice according to the study cited by the ATDSR;
A second possible update: if you look harder for those observable neurological effects, apparently you can find them in rodents at a tenth of that level?
This source says:
"there are numerous reports of neurotoxic effects in mice and rats, confirmed by coherent neurobiological alterations, for oral doses of Al much < 26 mg/kg/d: 6 mg/kg/d reported in 1993 [86], 5.6 mg/kg/ d reported in 2008 and 2009 [87,88], 10 mg/kg/d reported in 2016 [89], 3.4 mg/kg/d reported in 2016 and 2017 [90,91], and even 1.5 mg/kg/d reported in 2017 [92]."
I don't know how to assess the reliability of this literature.
Third possible issue to litigate is whether the specific form of aluminum matters, and the specific form in vaccines can pass the BBB more easily via immune cells. Comment chain for that issue here [LW(p) · GW(p)]
↑ comment by mikes · 2023-07-04T12:26:42.849Z · LW(p) · GW(p)
edit 3/4: for those coming off here the front page: on further inspection from the discussions below, and after looking into Bishop's follow-up study and lack of similar follow-ups, it seems quite possible the original Bishop paper's analysis was subject to selection effects / p-hacking. But if we ignore the Bishop paper, we are still in the position of multiplying the aluminum intake of infants by a large factor, without ever having done careful studies on long-term side effects. See other threads for discussion on animal studies and neurotoxity.
edit 1: There are neurotoxicity results in animal literature, not just in Bishop. Below I argue there is no evidence of p-hacking in the Bishop paper itself except that there are p-values of size .03 [EDIT: No longer my view]. I am not happy that this is the state of our evidence base, and it is a point against that they did not publish their dataset. But even if their effect size is overstated by a large multiplicative factor, we may still have a problem.
edit 2: I just found that there is a 2009 follow-up study with the same infants studied in Bishop 1997. There was no significance on the cognition reanalysis, which could assemble only 30%. of the original patients, although slightly fewer showed up / were eligible from the high-aluminum group (they entirely excluded recruiting patients with development < 85). "Non-significance" doesn't say much about the actual cognitive effects, given the very small sample size and a likely Berkson's paradox effect due to development thresholding and selection on "did-they-show-up." What bugs me a lot more is that they post nothing about the new cognition data, not even group means, which does support adverse inferences about their publication practices.
re: Bishop et al 1997: and p-hacking
I believe this paper was well-regarded enough that it motivated FDA to create new regulations for aluminum content in IV fluids. They even set the standard at its Al-depleted 5 microgram/kg/day level.
Bishop claimed that the subgroup analysis was pre-planned. If many of those babies were only on the drip for a day or so, as they claim, then the p=0.39 difference of means analysis was never going to be the estimator we should look at.
I thought the regression they did (p = .03) was always going to be the best estimator given the expectation of a dose-response relationship, and should have been the first thing they mentioned in the abstract. It is where I took my estimate from to start. I figured a shrinking factor of about 2 on the effect size would be sensible to account for selection.
Knowing this, would you still high-probability think e.g. they have p-hacked on the choice of outcomes, and the particular cut-point, and then claimed it was a planned subgroup analysis, and chucked in the regression after too, and there's selection on the neuromotor function, and most likely the whole thing is bunk? Maybe - the medical literature can be awful sometimes. It was apparently enough to make the FDA move before. If this is still a crux, we can probably go look at animal literature.
re: generalization from this study: A "vaccine-age child" is a 1 day old child. We give the hepatitis B vaccine, >200micrograms aluminum, at birth. Al probably enters bloodstream over the next days/weeks. Generalization from premies to newborn/1-month-old infants is probably not perfect, but does seem plausible. As I mentioned, major differences to look for are kidney filtration and brain vulnerability. Are the newborns consistently >>10x more robust, as would be needed to make this a nonissue? This I do not know, and would hope to ask an expert.
re: Priest: the pharmacokinetics literature looks complicated, and I'm not sure what to take away from it. I think animal studies have indicated that release from muscle to the rest of the body is slow, not immediate, hitting the bloodstream over the scale of days/weeks. Not sure if this is settled.
re: radio-labeled aluminum: bang me on the head again if you have a specific takeaway for this, but if it was just context, I'll add some: This resource claims that about 1% of aluminum in the blood winds up in the brain. I don't know where they get this claim from, though, or even what it technically means.
removed due to above edits: the chronic exposure calc at the end:I think you need to account for infants' lower body-weight, which means your result is off by a factor of ~20ish and puts us back into elevated-Al territory for the first year of life.
↑ comment by Lao Mein (derpherpize) · 2023-07-04T14:03:05.959Z · LW(p) · GW(p)
- Bishop et. al. is absolutely bullshit and I will die on this hill. Do I think people lie about when they make statistical decisions when the alternative is not meeting p=0.05? Yes, of course. I see it all the time. Note that there are no replications or even anything close. What do you call a study with non-adjusted p-size of 0.03 and no replications? False. This IS absolutely the crux here. Bishop is the main reason to suspect AL being dangerous to infants. If you remove it, why are we even considering the hypothesis in the first place?
- The FDA changing IV regulations based on very weak evidence is in-character, but also means that replication studies are harder, which may explain why we don't see them. But someone should still be able to analyze past data and come up with something if Bishop is right. We don't have that. And it only takes 6-12 months to go from deciding to write a data reanalysis paper to having it published, so they've had enough time.
- The really important thing is: how much do AL injections affect infant blood AL levels? Note that infants have AL in their blood without injections. Since AL can only reach the brain through the blood, the total amount of AL passing into the brain is just blood_AL_levels * time. Let's call that TAL. So our research question is: do AL injections raise blood AL levels high enough such that TAL is significantly elevated? Remember that the brain has lower AL levels than other tissues, so there's no selective uptake by the brain. Instead, it seems to mostly go to the kidneys and bones, where it's harmless.
- This is why the radio-labeled study is so important. It shows AL levels normalizing very quickly as it enters the body, even before it can be moved into urine by the kidneys. This is why I bring up the 50% in 1 hour and 99.5% in 24 hours statistics. This means that the AL from injections doesn't have much time to sit in the blood and wait to enter the brain.
- Therefore, in order for AL from injections to cause brain AL levels to rise significantly over the baseline, it has to raise AL levels long after injection. I found a rabbit study showing that a 0.85mg AL injection to ~2kg 21-day-old rabbits only resulted in their blood AL levels spiking to a peak of ~10 micrograms/kg of blood (for sanity, I'll refer to this as 10 ug/L. I won't quibble about whole blood vs. serum) before going back to <1 ug/L after <48 hours. This then increased somewhat back to 1 ug/L for some over the following days, but we don't see a massive chronic increase. 1 ug/L is much lower than human infant levels, which weirds me out and makes me a bit suspicious. I assume the rabbits were eating very low aluminum diets, so the effects would be even lower in a human. I'm unsure about this study since the rabbits started with such a low AL level, but their estimate for vaccination raising the TAL of a human infant by 1% sounds about right.
- Remember exposure in the womb. This Indian study found similar AL levels in cord blood and maternal blood, around 10-20 ug/L. By the time an infant gets their first vaccines, they've already been exposed to maternal blood AL for 10 months! So vaccines have to result in greater TAL than maternal exposure in order to have significant effects. Based on the data, I find this unlikely.
- We just don't see major changes in blood AL levels in children based on age. I'm using the data from this blood/hair study. If AL injections do chronically increase blood AL levels, we would see a sharp increase after each vaccination, which we don't. These are 9-13 month infants, who are getting a lot of vaccines, and they only have 15 ug/L average blood AL. There was no significant correlation between age and blood AL levels! Older kids with more vaccinations don't have a significantly higher AL level than younger kids. There are plenty of other studies showing similar (lower, in general) blood AL levels. If vaccination was chronically increasing blood AL, why can't we see that?
↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-07-04T18:42:56.229Z · LW(p) · GW(p)
The big question these days is about ASIA syndrome - autoimmune disorder triggered by adjuvants. Here is a review from this year, which also links to a 2019 review of Al-induced chronic fatigue syndrome. "Once the aluminum-containing vaccine is injected, instead of rapidly solubilizing in the extracellular space, it accumulates at the injection site, forming aluminum conglomerates. This delay in solubilization allows the injected aluminum particles to be quickly captured by cells of the immune system and transported to different organs, including the brain, where aluminum stimulates the inflammatory response and causes chronic neurotoxicity."
They also talk about a 2020 sheep study that showed " Animals in the vaccine and adjuvant-only groups exhibited individual and social behavioral changes. Affiliative interactions were significantly reduced and aggressive interactions and stereotypies were significantly increased. Some of these alterations observed in this experimental model are similar to those observed in the ASIA syndrome."
Some symptoms used to diagnose ASIA include "myalgia, myositis, arthralgia, arthritis, chronic fatigue, sleep disturbances, demyelination, memory loss, pyrexia, and dry mouth."
One paper points out that the immune system plays a role in mediating brain development via intercellular cross-talk. It also points out that in children, renal function and the blood-brain barrier are incomplete, and so in conjunction with the small size of children and elevated levels of Al exposure relative to adults, there's mechanistic reason to think they may be vulnerable to Al-induced ASIA-mediated neurological disorders. There is some evidence (which they cite, i.e. Gallagher and Goodman) that vaccines are linked to autism in neonates. There is also apparently substantial evidence linking ASIA to neurological disorders in adults.
Based on what I see, there are two plausible mechanistic routes by which aluminum adjuvants could directly or indirectly impair childrens' neurological development, and some modest animal experimental and human epidemiological evidence to support that this might actually be going on. It's not enough for me to be convinced that this is a widespread common issue, or that the risks posed by vaccines outbalance the risks posed by infection, but I am intrigued.
↑ comment by mikes · 2023-07-04T14:33:13.947Z · LW(p) · GW(p)
1,2. [this point edited] I do think the neurotoxicity has been shown in animal studies; not sure how to assess comparability of scales to humans though - see this comment [LW(p) · GW(p)]. I agree lack of follow up / re-analysis is kinda sketch, but the study area seems to be generally neglected? I think FDA regulations hit soon after the study, which would limit options for replications, but maybe some retrospective analysis would have been possible in the period where manufacturers were struggling to remove Al from IV fluids.
345. I think the hypothesis is, yes, the aluminum sits in muscle at first and doesn't rush directly into the blood. I can't judge it myself, but this paper has lots of thoughts about the rabbit study and ways it could be misleading, and perhaps-too-complicated-but-heck-if-I-know theories about the chemistry.
6. very interesting, this looks like a strong argument I hadn't considered. thanks for bringing this up! I'm glad they don't find a correlation in this study. Blood / cord aluminum may be a relatively variable/fleeting thing, though; if this were averaged over gestation time I'd find it quite convincing. Not sure how much it would change in these women day-to-day, and whether we should think a reasonable signal is findable?
7. The child is growing about linearly and getting more vaccines / aluminum load about linearly. blood vol is proportional to body mass. net result, everything looks kinda constant per blood unit, if we didn't add more then Al per blood unit should drop over time.
Replies from: derpherpize↑ comment by Lao Mein (derpherpize) · 2023-07-04T15:01:59.485Z · LW(p) · GW(p)
Neurotoxicity where blood levels reach 500ug/L and cause clear problems with brain function has been shown. But we don't see any effects on animals at 10-20ug/L. The window for studies, however, isn't closed! We can go back and use past records. Data like which IV nutritional formula is used and infant/adult brain function are easy to collect, even decades after. This is why I am so suspicious about the lack of replications.
I understand that aluminum may be released into the blood over time. However, the only way this can cause brain problems is by raising blood aluminum levels. We do not see an increase in blood aluminum levels. We don't even see significant differences between vaccinated and unvaccinated children in the US from the hair/blood analysis paper! That's enough for me to call it case closed until new information comes out.
It's entirely possible that 10-20 ug/L is bad for children, before and after birth. But removing AL from vaccines would barely move the needle.
Replies from: ChristianKl, AllAmericanBreakfast, mikes, mikes↑ comment by ChristianKl · 2023-07-04T21:23:24.455Z · LW(p) · GW(p)
If 10-20 ug/L would mean a loss of 1-2 points of IQ it's unlikely that the animal studies were strong enough powered to pick up such an effect.
If the aluminium goes into the brain that would mean you wouldn't see it in the blood or hair.
If you want to make a statement about it not going to the brain you either have to account where it went or look in the brain.
↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-07-04T22:17:07.960Z · LW(p) · GW(p)
I am not sure it’s accurate to say that chronically increased blood levels of aluminum is the only way to cause brain problems. The reviews I linked in my other comment suggest that aluminum can affect brain function by:
- Being carried to the brain by immune cell endocytosis.
- Disrupting immune cell cross-talk with the CNS.
- Rapidly crossing the incompletely developed neonate blood brain barrier before being cleared more slowly by incompletely developed neonate kidneys. Remember that the aluminum clearance data is from healthy adult males.
↑ comment by mikes · 2023-07-05T18:21:52.828Z · LW(p) · GW(p)
For animal studies at lower ranges of Al exposure:
This source says:
"there are numerous reports of neurotoxic effects in mice and rats, confirmed by coherent neurobiological alterations, for oral doses of Al much < 26 mg/kg/d: 6 mg/kg/d reported in 1993 [86], 5.6 mg/kg/ d reported in 2008 and 2009 [87,88], 10 mg/kg/d reported in 2016 [89], 3.4 mg/kg/d reported in 2016 and 2017 [90,91], and even 1.5 mg/kg/d reported in 2017 [92]."
What blood levels would you think this maps to?
Or do you think these studies are bunk?
↑ comment by Lao Mein (derpherpize) · 2023-07-05T23:14:40.278Z · LW(p) · GW(p)
https://sci-hub.ru/10.1007/s12640-016-9656-y
The study they were citing was a typically underpowered mouse study with p-hacked groups. Why did they choose to run 2 groups, each with their own controls, on the same tests? The only significant behavioral difference between the groups was that controls performed better on the memory test.

But 1.5 mg/kg and 8.3 mg/kg are normal human-level AL intakes! And look at those error bars! Also, they ran their analysis completely wrong. This null hypothesis you're supposed to be testing against is "there is no difference in exploration time (c-a) between each groups". Instead, they were testing against "there is no difference in exploration time between a and c". That is, their null hypothesis was that their mice had no memory, they found that their control group definitely did have memory, and concluded that AL had an effect... But then they used the wrong control group? Everything in this study is wrong and the authors and reviewers should feel bad.
Let me reiterate that. THEIR ONLY STATISTICALLY SIGNIFICANT RESULT WAS THAT CONTROL MICE HAD FUNCTIONAL MEMORY. THE ERROR BARS ON TEST GROUP MICE WERE SO HIGH YOU CAN'T TELL EITHER WAY. THEY DID THEIR ANALYSIS WRONG AND THEIR CONCLUSIONS SHOULD BE DISCARDED. So yeah, it's completely bunk.
↑ comment by mikes · 2023-07-04T21:45:50.868Z · LW(p) · GW(p)
Just noting that in the hair/blood analysis paper there were no unvaccinated children, so no useful comparison could be made from that paper alone - I complained about this in the main post body.
Also, most of these kids were probably arriving at the lowest point in their Al cycle, when they're right about to get more shots? It says "We obtained data for this cross-sectional study from a cohort of healthy infants presenting to an urban, primary care center for well child care."
They had aluminum levels median ~15 ug / L and a much higher mean with some large positive outlier samples, which the study then excluded. I don't see this study as evidence against vaccines causing increase in blood aluminum levels
↑ comment by simon · 2023-07-04T15:01:39.682Z · LW(p) · GW(p)
Remember exposure in the womb. This Indian study found similar AL levels in cord blood and maternal blood, around 10-20 ug/L. By the time an infant gets their first vaccines, they've already been exposed to maternal blood AL for 10 months! So vaccines have to result in greater TAL than maternal exposure in order to have significant effects. Based on the data, I find this unlikely.
But mikes above said:
We give the hepatitis B vaccine, >200micrograms aluminum, at birth
And that looks a heck of a lot higher. So I'm confused by the "Based on the data, I find this unlikely" statement. Edit: I see, it's because it's absorbed by the muscle and doesn't go to the blood, or if it goes to the blood it then goes to the bone?
Like, the maternal blood is being circulated so I'd expect it to lead to some equilibrium Al level (unless it's absorbed somewhere and not coming free again). Whereas, the vaccine is adding a whole lot that isn't being circulated out by the vaccine itself (though I assume there must be other mechanisms to dump it out of the body if it isn't increasing a lot after vaccines).
↑ comment by Lao Mein (derpherpize) · 2023-07-04T15:34:36.887Z · LW(p) · GW(p)
It gets excreted over time but also accumulates in the bone, where it is slowly released into the blood over time.

↑ comment by simon · 2023-07-04T15:44:39.603Z · LW(p) · GW(p)
OK, thanks. On the other hand, if Aluminum is excreted that fast, doesn't that suggest that the blood level is pretty heavily increased for a short time (since I assume it must be in the blood to get excreted and I also assume that the timescale of such excretion, given that it's in the blood, should probably be at least a day or so?)
Replies from: derpherpize↑ comment by Lao Mein (derpherpize) · 2023-07-04T16:37:36.960Z · LW(p) · GW(p)
You're right - it's what we would expect. And yet the actual blood aluminum levels we measure aren't that high! So where is all the aluminum? Well, biopsies show that kidneys have something like 10x the AL levels of other soft tissues in rabbits, so I suspect that's where a lot of the aluminum goes during the first hour. This is then excreted in urine, explaining why urine AL levels are sometimes higher than blood AL levels. After that, tissues slowly release their aluminum into the bloodstream, where they get absorbed by the kidneys before blood AL levels can rise too much. Sounds nice in theory, but probably more complicated/downright wrong in practice.
Will do more research tomorrow.
↑ comment by ChristianKl · 2023-07-04T13:47:52.376Z · LW(p) · GW(p)
Remember, aluminum can only cause brain damage if it reaches toxic levels.
What evidence do we have for the claim? Why wouldn't there be a linear relationship between the amount of aluminum in the brain and the amount of damage?
Replies from: Markvy↑ comment by Markvy · 2023-07-04T15:23:55.003Z · LW(p) · GW(p)
I think that that’s what he meant: more aluminum in the brain is worse than less. What he was trying to say in that sentence is this: high levels in the blood may not mean high levels in the brain unless the blood level stays high for a long time.
Replies from: ChristianKl↑ comment by ChristianKl · 2023-07-04T20:54:57.584Z · LW(p) · GW(p)
That would suggests ignorance of basics of toxicology.
There are substances for which it's literally true that the are only cause damage when they reach a certain level. Water for example is toxic at high levels but causes no damage at normal levels.
That's because the body can process a certain amount at water at one time. You only cause damage is you consume more water than the body can handle.
On the other hand the establishment opinion on radiation is "there's no safe level of radiation". There are some people who think the establishment position on radiation is wrong here and radiation is only a problem when it's so strong that it overwhelms self repair processes.
Damage due to aluminium could be in either class. It could be that a certain level is required to cause damage or it could be a linear relationship.
Claiming that the damage is small and claiming that there's no damage are two different claims.
↑ comment by mikes · 2023-07-05T17:05:35.342Z · LW(p) · GW(p)
Starting a new comment chain here for the debate on immune cell transport of aluminum:
A pretty succinct argument with citations is given here, claiming that injected aluminum hydroxide is in an insoluble state above ph7.35, so immune cells capture it.
I guess after that, it's assumed they'll take it through the blood brain barrier, and drop it when / where they die? For the ones that die in the brain, and they don't need to drop very much to cause a problem, because brain Al levels are usually very low and are retained with extremely long half life.
I don't know whether to trust the argument. It doesn't seem obviously crazy?
Vaccine advocate literature tries to contradict the claim by stating "all of the aluminum present in vaccines enters the bloodstream" but is ignoring rather than countering the argument.
The theory seems possible to straightforwardly confirm or refute with animal studies. E.g. just give a soluble aluminum iv to group A and a vaccine injection to group B, and then compare the amounts that get loaded into bone tissue vs brain tissue after a while. Kinda weird that this has never been done; is it really that hard to set up such a study?
↑ comment by Lao Mein (derpherpize) · 2023-07-06T00:06:36.473Z · LW(p) · GW(p)
https://sci-hub.ru/10.1186/1741-7015-11-99

They did this and it was fine. Reference levels are around 1 mg/kg for humans. Yes, immune cells gobbled up the aluminum and spread it around the body. Some of it went to the brain, raising the local AL levels. No control group is a bit sus. And this is with an 18 ug injection into ~35g mice. That's like a 500 ug injection into a 1kg baby. C57 are the wild-type mice, btw.
Replies from: mikes↑ comment by mikes · 2023-07-06T07:30:03.230Z · LW(p) · GW(p)
Nice! Shame the error bars on this are super large - in this figure I think that's not even a confidence interval, it's a single standard error.
Not sure if this is useful for anything yet, especially give the large uncertainty, but I think we have the tools now to make two different kinds of rough estimates about brain loading of Al from vaccines.
Estimate 1: Assume immune transport. Resulting load of between 1 - 2 mg / kg of Al in dry brain, since this study suggests about 0 - 1 mg/kg increase in Al. [I'm using a liberal upper confidence here and assuming it's natural to generalize using the absolute amount that got added to the mouse brain, rather than % added from baseline. If we used %'s it'd be somewhat less.]
reasoning:
If we take a 18ug injection into 35g mouse, that's like 1.5mg into 3kg baby at birth, or like 5mg into a 10kg one-year-old child. So, this comparison maps pretty reasonably to the load of the vaccine schedule. Eyeballing from that figure, it suggests the vaccine schedule yields a 0 - 1 mg/kg increase of Al content in dry brain, using a liberal interpretation of the standard errors for the upper end.
Estimate 2: Assume accumulation is linear with respect to Al blood levels. Comparing blood reference levels to estimate a multiple on the relevant rate of gain in Al, the end result is 1.67 - 2.33 mg/kg level of Al / g dry brain weight at age 1.
reasoning:
Some studies are of the opinion that healthy people have about 5ug/L of Al concentration in blood. Source: this review says:
1. Elshamaa et al. (2010) compared serum Al in 43 children on chronic renal dialysis (where dialysate Al was less than 10 mg/L) to serum Al in 43 healthy children. The dialysis patients used Ca acetate or carbonate to control circulating phosphate, and none of these children received Al-containing phosphate binders. Serum Al was significantly higher (18.4 +- 4.3 mcg/L) in renal patients than in healthy referents (6.5 +-1.6 mcg/L). The source of the elevated serum Al in these cases appeared to be erythropoietin (EPO).
2. By way of comparison, plasma and serum Al concentrations in healthy humans range from less than 1.6 to 6 mg/L (median = 3.2 mg/L or 0.12 mM)
Maybe we should assume that the healthy aluminum reference level is slightly but not hugely higher in 0-1 age children, due to their reduced glomerular filtration rate - at worst, doubled?
Karwowski et al 2018 shows a median blood level of about 15 ug/L in their sample of vaccinated children, and the mean is presumably much higher.
Interpreting this as doubling or tripling of the blood level, that would double or triple the rate of accumulation.
If we are to assume that the reference level of 1 mg/kg would be maintained in the "control" child over time, and the child triples in size from age 0 - 1 year, then tripling the rate of total aluminum addition over that year would result a total... 2.33 mg / kg dry brain in the healthy 1 year old child's brain. Doubling, results in 1. 67 mg/ kg
edited to fix units!
↑ comment by Lao Mein (derpherpize) · 2023-07-06T08:17:19.968Z · LW(p) · GW(p)
A couple of things:
The 15 ug/L figure was just the first one I found - the study actually noted that most others have found lower (5-10 ug/L) levels in children.
Instead of working backwards, why not just compare blood AL levels in matched vaccinated and unvaccinated children? Different countries have different vaccination schedules and so on. I'm not digging further because I should be doing other stuff, but it's a good lead.
I couldn't find any reference Al levels for childrens' brains.
1.67mg/g of Aluminum in a one-year-old's brain doesn't pass the sanity check. I think the above chart has a typo - that should be ug/g, not mg/g. Otherwise the mice would be very dead! Also, normal Al levels in the brain are around 1 ug/g, a mouse has a brain mass massing 0.4g (dry mass ~0.3g), and 1mg/g would imply ~0.3 mg of Al, far more than injected in the first place.
Replies from: mikes↑ comment by mikes · 2023-07-06T09:08:26.664Z · LW(p) · GW(p)
whoops, fixed my units. got too used to seeing it written in mcg/g!
some findings of blood levels
Paper from 2011 titled:
Wide variation in reference values for aluminum levels in children

This paper is from 1992:
cites two studies:
in premature infants fed orally,
mean AL level is 5 mcg/L, SD of 3
another study of very young infants
4 - 5 mcg/L, SD of <1
It seems sensible to estimate that if 5 mcg/L is normal for newborns, and normal for older children, that it should be normal at age 1 as well.
I also found another study in China, which cited a geometric mean of >50 mcg/L. I guess either pollution or poor measurement equipment can totally wreck things.
I'm amazed both by the substantial lack of key evidence regarding the effectivity and safety of at least some vaccines, and by the radicalization of the discourse everywhere, even here, where you can rarely express an opinion without being heavily censored or criticised.
An example:
https://www.lesswrong.com/posts/Ccv8PinXRgRTKpGaj/what-we-ve-learned-so-far-from-our-technological-temptations?commentId=P9SMrtmmznTxF8q3Q [LW(p) · GW(p)]
I gain nothing by doubting the effectivity and safety of any treatment. I don't work in the industry, I don't monetize my opinions, I don't even get social points. If I express my doubts is because I'm worried and want to know the truth. For some reason, this is politically incorrect in most circumstances.
Why and how this topic became taboo? Even if I'm stupid, and ignorant, I act in good faith, I truly want to know and, in case I'm right, to help people. Why am I censored for asking questions and showing some weak points in the narrative?
↑ comment by ChristianKl · 2023-07-05T12:16:41.169Z · LW(p) · GW(p)
There's a difference between asking questions and making arguments where you expect other people to watch Youtube videos, especially in the comments of another thread that's not centrally about vaccination.
If you want to make a point about common beliefs about the deaths prevented by vaccines being wrong, it would make more sense to do that as a top-level post and lay out the full argument so that it's not necessary to watch any external websites to judge the argument.
Replies from: o-faislis-tyrannos↑ comment by Οἰφαισλής Τύραννος (o-faislis-tyrannos) · 2023-07-05T13:13:13.956Z · LW(p) · GW(p)
That's a good argument, thank you. I see how expecting people to watch videos about one little assumption made in the original message instead of carefully laying out the core of the arguments and presenting them in a way that more precisely answered to my concerns about what was written in the thread was a bad approach and could be interpreted as too general or derailing even. I will try to do better next time.
This reminds me of when I found an error in a popular asteroid impact effects calculator. The calculator suggested that an impact would generate only very minor earthquakes. For instance, if the Moon were to collide with the Earth, it would barely be noticeable on the other side of the planet.
I reached out to the creator of this model. They responded by explaining that their data is derived from a study on the effects of minor impacts on the Moon, as measured by a certain Apollo scientific instrument.
The study concluded that minor impactors contribute less than 0.0001% of their energy to seismic waves. However, I believe there is a significant difference between minor impactors on the Moon and larger impactors on Earth. Minor impactors hit a solid surface, and most of their kinetic energy is directed into ricocheting debris, with only a tiny fraction becoming sound waves.
In contrast, larger (kilometer-sized) impactors on Earth would penetrate deep underground, and the Earth's surface around them would behave more like a liquid. This liquid-like surface would create a large 'splash', and a significant portion of the impact energy would be converted into waves—I estimate this to be between 1 and 10 percent.
Consequently, I believe that the seismic effects of potential impactors are underestimated when compared to more widely-recognized effects such as global tsunamis and climate change.
If you want to read more about the science behind aluminium adjuvants, http://vaccinepapers.org/ is a goldmine of info mainly about aluminium in vaccines.
http://vaccinepapers.org/the-foundation-for-al-adjuvant-safety-is-false/ is also worth a read.
TLDR: the science behind the safety of aluminium adjuvants is sorely lacking.
Here is another study that seems relevant:
https://pubmed.ncbi.nlm.nih.gov/22001122/
Aluminum is a ubiquitous element that is released naturally into the environment via volcanic activity and the breakdown of rocks on the earth's surface. Exposure of the general population to aluminum occurs primarily through the consumption of food, antacids, and buffered analgesics. Exposure to aluminum in the general population can also occur through vaccination, since vaccines often contain aluminum salts (frequently aluminum hydroxide or aluminum phosphate) as adjuvants. Because concerns have been expressed by the public that aluminum in vaccines may pose a risk to infants, we developed an up-to-date analysis of the safety of aluminum adjuvants. Keith et al. [1] previously analyzed the pharmacokinetics of aluminum for infant dietary and vaccine exposures and compared the resulting body burdens to those based on the minimal risk levels (MRLs) established by the Agency for Toxic Substances and Disease Registry. We updated the analysis of Keith et al. [1] with a current pediatric vaccination schedule [2]; baseline aluminum levels at birth; an aluminum retention function that reflects changing glomerular filtration rates in infants; an adjustment for the kinetics of aluminum efflux at the site of injection; contemporaneous MRLs; and the most recent infant body weight data for children 0-60 months of age [3]. Using these updated parameters we found that the body burden of aluminum from vaccines and diet throughout an infant's first year of life is significantly less than the corresponding safe body burden of aluminum modeled using the regulatory MRL. We conclude that episodic exposures to vaccines that contain aluminum adjuvant continue to be extremely low risk to infants and that the benefits of using vaccines containing aluminum adjuvant outweigh any theoretical concerns.
↑ comment by mikes · 2023-07-05T01:42:21.809Z · LW(p) · GW(p)
This is one of the studies mentioned above in the post, Mitkus et al. 2011
Replies from: AllAmericanBreakfast↑ comment by DirectedEvolution (AllAmericanBreakfast) · 2023-07-05T03:32:32.565Z · LW(p) · GW(p)
Oops, retracted
-Alternatives to aluminum exist, including mRNA and other new adjuvants.
This is not really true. Despite aluminium being a neurotoxin that is detrimental at any dose just like mercury, with identical neurotoxic effects as mercury, no viable alternatives exist that were as extensively tested, and most alternatives are in fact much more dangerous. I'm not an expert on mRNA, but we have all seen with the covid shots that the side-effects were much more extreme. And for all we know it didn't need adjuvants because the spike protein itself is cytotoxic.
This is not to say that we can't develop better adjuvants, for example by using natural chemokines, which are of course not licensable hence not researched. However, this would only really address the small subset of the population, who are sensitive to heavy metals and somehow can't detoxify from them as effectively as others. Autoimmune reactions, anaphylaxis and other side-effects of vaccines, some of them also resulting in encephalitis and subsequently autism, will still persist even with healthier adjuvants, due to the nature of artificially provoking the immune system, which sometimes just leads to unpredictable immune reactions, no matter what you do.
Conceivably you could work out some extended-release nanoparticle coating to mitigate this problem. But who cares about that, if manufacturers are exempt from liability anyway?
Of course with such a lunatic vaccine schedule as found in the US that has close to 100 shots, the toxic metal poison with longest half-life estimated around 7 years, accumulates so much that it is predestined to cause all sorts of neurological dysfunction. In a sane vaccine schedule, you have just 10 shots and the ability for people to opt out. Aluminium then isn't really a major priority to improve vaccine safety. There is even limited research and reason to believe that aluminium hydroxide does not cross the blood-brain barrier that much in most people. But of course the overall toxocology of aluminium is not that simple. Especially if you inject doses that are between 10 - 100 times higher than what you would naturally absorb through food.
Bottom line is we don't really know about adjuvant safety, because really no one cares, and no one does the studies. With a little bit more censorship and vaccine Lysenkoism, the profits are just rolling and keep on rolling. Anti-vaxxer science is fascist science that undermines society and harms the greater good. That's all you really need to know about.
3 comments
Comments sorted by top scores.
comment by ChristianKl · 2023-07-04T10:35:39.368Z · LW(p) · GW(p)
Alternatives to aluminum exist, including mRNA and other new adjuvants.
That leaves the question of whether the other alternatives are really safer. Adjuvants are by their nature substances that produce an inflammatory response, and inflammatory responses in the brain are also the way that harm gets produced.
The COVID mRNA vaccine we saw had relatively high side effects the next day after taking the vaccine relative to the average vaccine that's prescribed.
What do we know about the other new adjuvants?
For vaccines that are not based on mRNA, which unfortunately are coated with LNP which crosses the blood-brain barrier, we might have a standard "You are not allowed to use adjuvants that cross the blood-brain barrier". Do we know whether such a standard would rule out the other adjuvants as well or would it let them pass?
Replies from: mikes↑ comment by mikes · 2023-07-04T10:41:35.159Z · LW(p) · GW(p)
Great questions. I am not knowledgeable about new adjuvants. Here is Derek Lowe on the topic of new adjuvants:
https://www.science.org/content/blog-post/enhancing-enhancers-vaccines
Also,
Many vaccines do not have adjuvants
I would expect it is usually possible to reduce or remove the adjuvant in exchange for more repeated doses. But immune systems are weird, and I can't say that confidently
↑ comment by prepper · 2023-07-04T15:00:33.759Z · LW(p) · GW(p)
Only live-attenuated vaccines may (sometimes) not need adjuvants. Plus you sometimes have other ingredients acting as adjuvants that are not declared as such. For example mercury is declared as a preservative, not adjuvant, but it performs the same function. Also as of recent they started removing constituents from the ingredient list, that were part of the manufacturing process (e.g. culture media), but are not "intended" part of the final product. If a food manufacturer washes potatoes with iodine for example in order to clean them, he is not required to list that as an ingredient, regardless of whether or not quantities in the final product are relevant.
To put simply without a live virus, the immune system recognizes the would-be antigens as simply garbage molecules, and not as a threat. In order for immunization to work, you need to inject something dangerous like a live virus, aluminium, some kind of toxic protein or cytokine alongside the antigen.