Covid 11/11: Winter and Effective Treatments Are Coming
post by Zvi · 2021-11-11T14:50:02.374Z · LW · GW · 19 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Vaccinations Vaccine Effectiveness Vaccine Mandates It’s Over Think of the Children Ministry of Truth In Other News None 20 comments
I was considering splitting off my analysis of the effectiveness of Pfizer’s Paxlovid, a new Covid-19 treatment pill, but it’s so straightforward there’s no reason to do that. It works, with our best guess being it is 89% effective at preventing hospitalization and death, and that’s that. Trial was halted because medical ‘ethics’ is crazy and decided we couldn’t study the pill because it was too effective. Paxlovid still needs to be approved and production needs to be scaled up, but both of these seem like near certainties.
In the meantime, it looks like cases are heading back upwards again. There was high uncertainty (I said I’d be more surprised by no change than by some change, but it wasn’t obvious which direction was more likely) so this was definitely in the possibility space, but it’s near the top end and rather disheartening.
There’s the usual kinds of developments on other fronts, but none of it should come as a meaningful surprise.
Executive Summary
- Pfizer’s new Covid-19 treatment pill Paxlovid is ~89% effective at preventing hospitalization and death, but it will take several months to ramp up production and gain official approvals before it is widely available. Effective treatment is coming.
- Cases are starting to increase again outside of the South. Winter is coming.
- Everything else about as you’d expect.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 442k cases (no change) and 7500 deaths (-11%)
Results: 470k cases (+7%) and 8092 deaths (-4%).
Prediction for next week:
The miss on deaths is due to a large increase in the West. On reflection I likely should have baked some of that in, -11% was a lousy prediction and -7% or so would have been a better prediction. I do think that this is still a disappointing number despite that. For cases the miss is the same size, but this seems more like uncertainty rather than mostly being a mistake in prediction. Cases rising this much this quickly was definitely surprising, and a large update on what’s likely to happen this winter.
Deaths
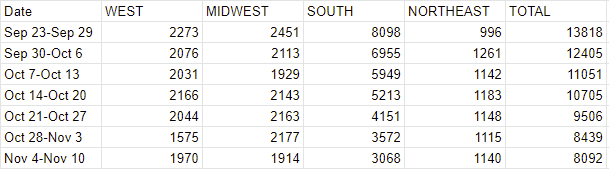
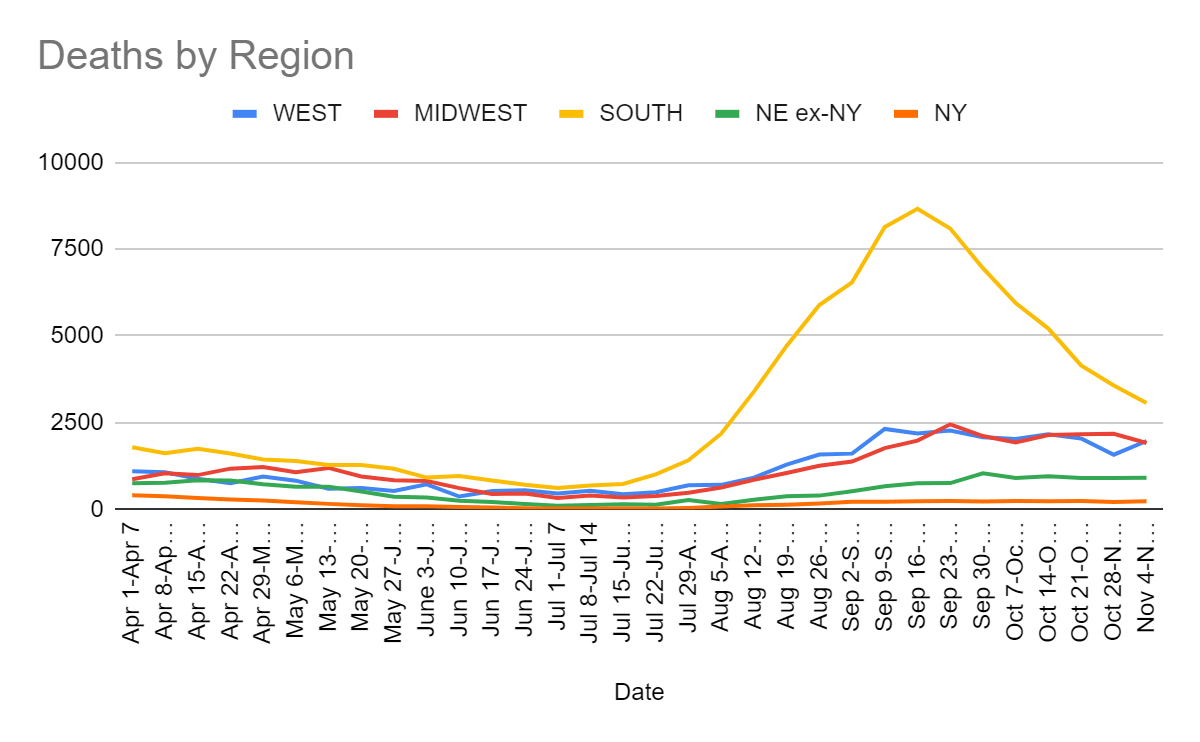
The jump in the West is not centered on one particular state, with several reporting the highest levels in a while. I’d like to say it is a systematic reporting pattern somehow, and I presume that some deaths from last week out West got shifted into this week. I don’t have any gears for that explanation and given it’s not focused in one state I don’t feel great about not having any gears to explain it. Still, it seems a lot more likely than this being a real decline followed by a real increase.
Cases

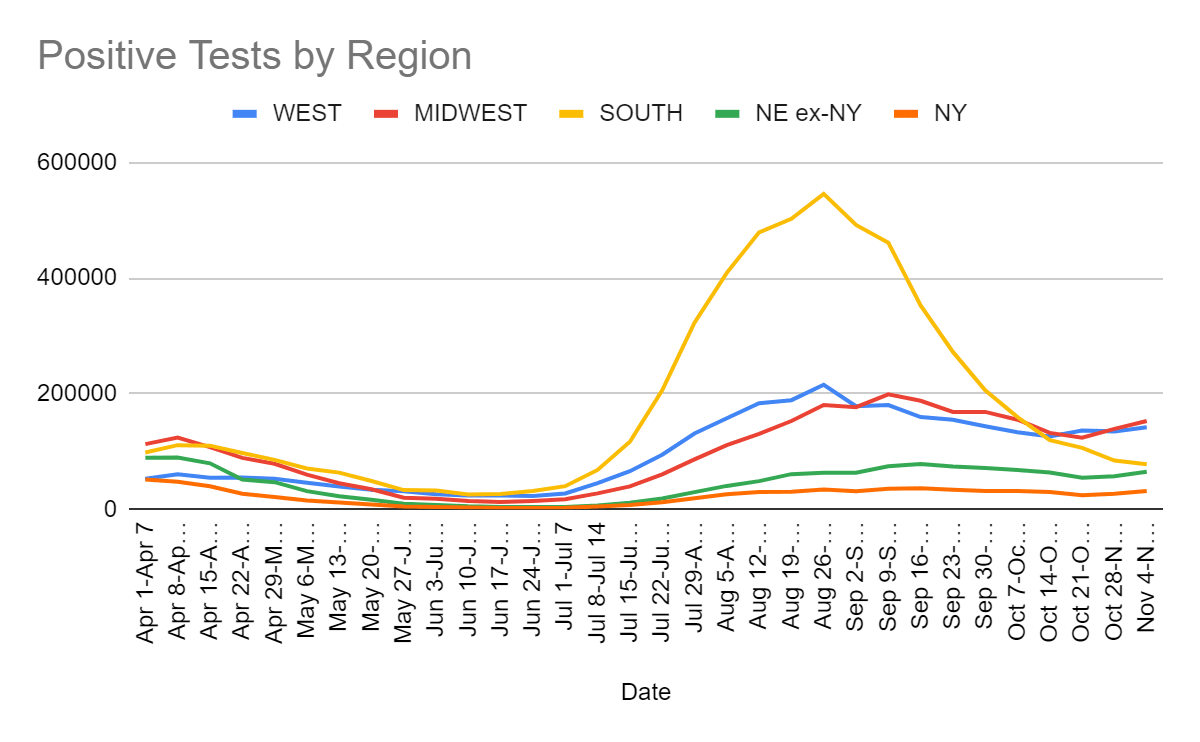
The increase looks fully real. The question is not whether cases will continue increasing, but rather whether the increase will accelerate and by how much. Child vaccinations will help a bit once they come online, but that will take a while and the total size is likely small, so we are probably looking at another winter wave.
Vaccinations
This section intentionally skipped this week.
Vaccine Effectiveness
Half doses of Pfizer produce strong immune response (MR), presumably with fewer short term side effects, and conserving supply. We could have vaccinated far more people far quicker, here and around the world, with smaller doses. Oh well. At least kids are already going to get lower doses. This will almost certainly have exactly zero impact on the doses given out in the United States, and at this point it’s too late for most of the gains from this anyway.
Did you know the vaccines are super effective against all-cause mortality? I mean, no, that’s crazy and any such finding is super duper suspicious and presumed hopelessly confounded but it would be remiss not to holy **** check out this chart from this video:
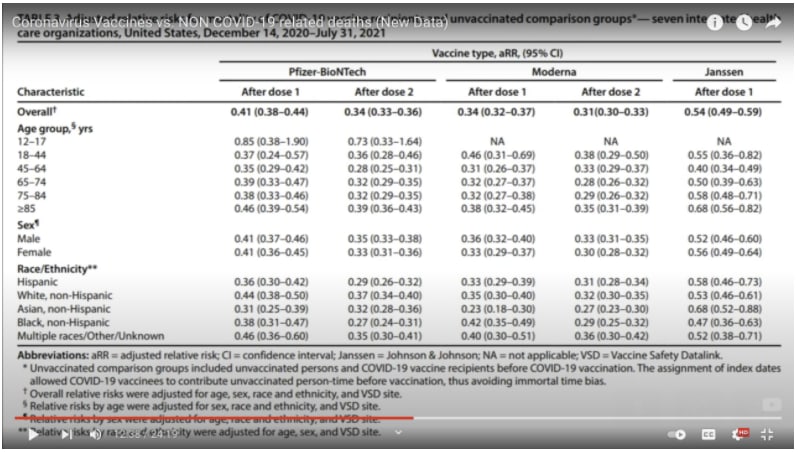
The effect is even stronger for Moderna than Pfizer which is stronger than J&J, and second doses are stronger than the first dose alone, and it survives segmentation by age, with the control group being people who got the flu vaccine within the last two years (but not the Covid-19 vaccines). Sample size is 11 million.
Can you imagine what people would say if these statistics were reversed with even 10% of this magnitude? With 1% of this magnitude? If people were somehow dropping dead far more after being vaccinated than those who didn’t get vaccinated? The vaccines most definitely would not remain legal, and no amount of figuring out and correcting for the confounders would make any difference. That would be the end.
I want to be super clear that I don’t buy this as a ‘real’ reduction. This has to be some sort of confounder effect somewhere, or an outright error, and the more interesting question is what that is all about. Maybe the control groups here are super weird somehow. I don’t have an explanation, and assume I’m missing something. Yet this is part of a very clear unmistakable pattern that no, the Covid-19 vaccinations aren’t causing major other problems in quantity.
Vaccine Mandates
I’ve repeatedly noted that when vaccine mandates come into effect the number of people who actually quit rather than get vaccinated isn’t always zero, but it is always quite low. Would that change if the job is more fungible, more replicable and less appealing? For example, a truck driver?
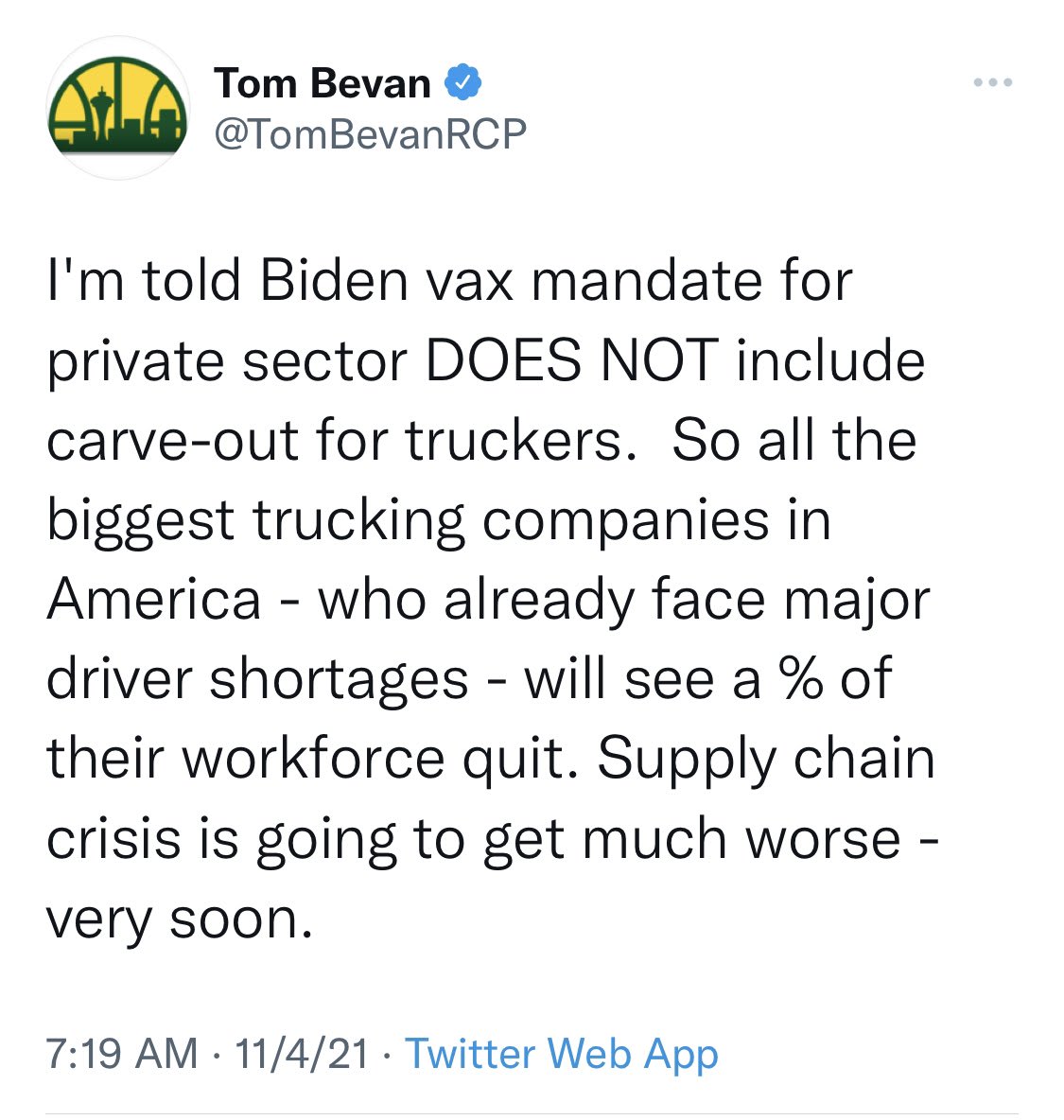
This is a rather terrible place to put a mandate, since truck drivers mostly spend their time alone driving trucks and we can’t afford to lose them at the moment. That doesn’t automatically mean this calls for a carve-out, since rules need to be simple and once the exceptions start things escalate quickly. It does introduce a potential serious issue, since trucking is a potential bottleneck on much of the economy.
By default I don’t expect much impact here, for several reasons, yet there are still reasons to worry. First, here’s the case for not worrying, as I see it.
- I don’t expect the rules to be enforced here in a meaningful way. Carve outs don’t need to be official to work, and I’m skeptical we’ll see much enforcement at all outside of the especially juicy targets.
- The baseline that almost no one actually cares enough to lose a job over vaccination. We might see somewhat more but it’s still not that many.
- If someone does quit, they have the option to walk over to a smaller truck company and get a job with them instead. Truck driving is mostly small businesses that are constantly forming and changing (source: listening to the Odd Lots podcast), with lots of turnover and highly fungible tasks. If someone needs to get in under the mandate’s employee limit to keep working, they’ll do that, and who does what job driving which truck is presumably mostly fungible in the end. That definitely works out on the road. What’s less clear to me is whether there’s the same flexibility at the ports to transfer staff to sufficiently small companies, if those jobs are sufficiently distinct, which in some ways they might be.
- This has echoes of a few years ago, when everyone thought truckers would quit over monitoring devices, and basically none of them did. We actually ended up with a capacity overhang because everyone was ready for a bunch of drivers to quit and then they didn’t quit.
- Thus there’s an either/or dynamic to this. If This Time Is Different it’s largely because it won’t much impact the supply chain, and if it would impact the chain, it won’t be different.
I’ve seen two counterarguments to all this that give me pause.
The first is that when someone leaves a particular trucking job, they often exit the trucking industry entirely. This is weird to me given that trucking jobs seem mostly fungible and there’s high demand for truckers, but it seems there’s other good options and the labor markets in those other options are very hot, so given the impetus of job switching some people will leave entirely. Which in turn implies that their cost of leaving the job is low, and it’s more realistic that they might quit a job over the vaccine issue.
The second is that while the effect will be small, this is a market where marginal throughput and capacity changes can have oversize effects. So if only let’s say 2% of truckers change jobs, even if that would long term return to equilibrium, that could have a very large impact on freight costs or cause bottlenecks. And for various reasons, especially stickiness in the future, it’s hard to quickly adjust wages sufficiently to compensate, so there might be considerable short term additional friction where we can least afford it.
In other mandate news, as a friend asked in a locked account, what exactly is the word “responsible” doing in this sentence?
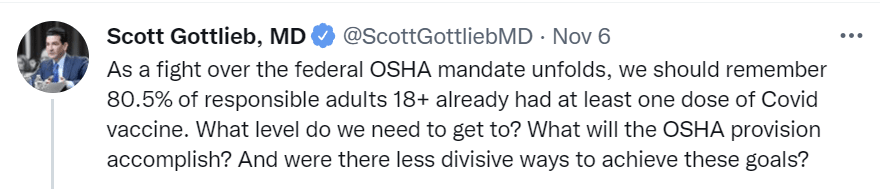
This also seems to implicitly echo multiple other fallacies, which I know Scott knows better than. There is no ‘level we need to get to,’ there are only benefits to marginal improvements, and the existence of other ways to raise levels that we aren’t doing doesn’t change the question of the OSHA rule unless we can choose those options, nor does ‘divisiveness’ represent the obviously primary cost of policy.
Meanwhile in Singapore, they’re done paying for Covid-19 treatment for the ‘voluntarily unvaccinated.’
But the Singaporean government said Monday that it will no longer cover the medical costs of people “unvaccinated by choice,” who make up the bulk of remaining new coronavirus cases and covid-19 hospitalizations in the city-state.
…
The government now foots the bill for any Singaporean citizen, permanent resident and holder of a long-term work pass who is sick with covid-19, unless they tested positive shortly after returning from overseas.
“This was to avoid financial considerations adding to public uncertainty and concern when covid-19 was an emergent and unfamiliar disease,” the Health Ministry said in its statement.
Then there’s Greece, where there’s fun being had with low social trust.
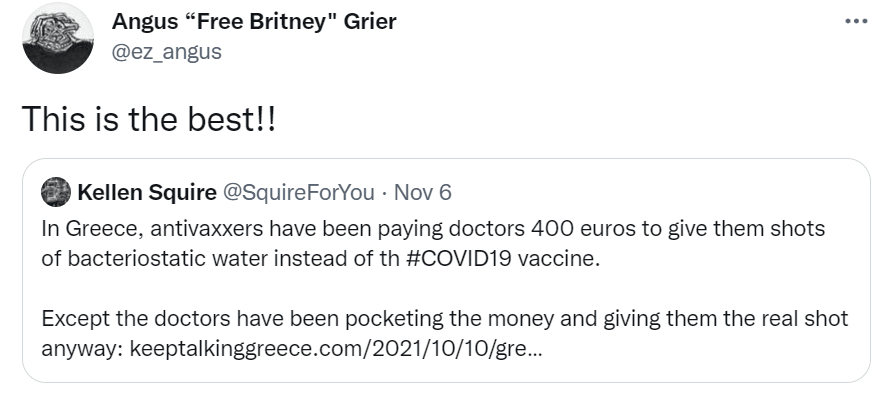
It turns out that giving out the real vaccine protects the doctors from getting in trouble for taking bribes to not administer the vaccine, but that doesn’t mean not taking the bribe, that would be crazy talk, who turns down perfectly good bribe money.
In terms of humor value and schadenfreude value, I can’t argue with Agnus’s evaluation.
But maybe this is actually… not the best? And we shouldn’t be happy about people getting vaccinated while the doctor tells them they’re getting water, regardless of the bribery and the attempted fraud, because the one does not make the other okay?
It’s Over
Last week’s title was The After Times, and I made much more explicit my position that for all practical purposes that involve actual meaningful health risks, the pandemic for most people reading these posts is over now that booster shots are available and kids can get the vaccine as young as five.
So basically this, except without the surprise.

That doesn’t mean we’re done with NPIs. There will be masks and tests and distancing and other such precautions and you and especially your children will be caught up in all that, perhaps for quite a while and perhaps at great cost. So it wasn’t fully over.
In any case, perhaps I should have waited a week, because Pfizer’s anti-Covid pill Paxlovid has interim results, and modulo the time it takes to ramp up production they can be summarized this way:

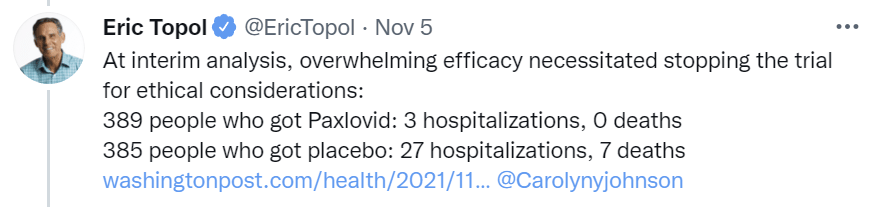
Washington Post write-up is here Here’s the AP rounding up to make it sound better, also they have a quote saying it’s ‘100% effective against death’ which is not the correct conclusion from 7 vs. 0 deaths. Here’s the Pfizer announcement.
The trial was stopped due to ‘ethical considerations’ for being too effective. You see, we live in a world in which:
- It is illegal to give this drug to any patients, because it hasn’t been proven safe and effective.
- It is illegal to continue a trial to study the drug, because it has been proven so safe and effective that it isn’t ethical to not give the drug to half the patients.
- Who, if they weren’t in the study, couldn’t get the drug at all, because it is illegal due to not being proven safe and effective yet.
- So now no one gets added to the trial so those who would have been definitely don’t get Paxlovid, and are several times more likely to die.
- But our treatment of them is now ‘ethical.’
- For the rest of time we will now hear about how it was only seven deaths and we can’t be sure Paxlovid works or how well it works, and I expect to spend hours arguing over exactly how much it works.
- For the rest of time people will argue the study wasn’t big enough so we don’t know the Paxlovid is safe.
- Those arguments will then be used both by people arguing to not take Paxlovid, and people who want to require other interventions because of these concerns.
- FDA Delenda Est.
I propose the Law of Efficacy, which states that the requirement to halt a trial due to a drug being ‘too effective’ is that the drug has been approved for public use by the regulatory authorities.
If it’s so damn obvious that the drug is safe and effective that we don’t need more data, then the authorities can make that determination. Until then, no halting trials.
You can tell me that there’s one set of ‘ethics’ for people intertwined with randomness or who are in front of your face, and another for those who aren’t, and I will note that such arguments are obvious nonsense. I reject the Copenhagen Interpretation of Ethics.
Merck’s pill was much less effective than Pfizer’s, and it was still a huge deal. Pfizer’s pill, by all rights, should change the whole game. An additional 89% reduction in hospitalization and death, on top of the gains from vaccination including booster shots, in vulnerable populations.
There is still far too much uncertainty in how effective Paxlovid is, due to the trial being halted early – the idea that we know what we need to know here already is absurd. But we do know enough that this should become the standard treatment, and it should mostly replace prevention efforts other than vaccination.
Once Pfizer’s pill is widely available, and most who catch Covid-19 can get the treatment, on top of widely available safe, free and effective vaccines and booster shots, I can’t see any reasonable case for prevention measures that meaningfully interfere with the living of life. The cost-benefit on that does not make any sense, any more than we already interrupt our lives for the flu or any other disease. Stay home when you’re sick, get tested if you might have it and treated if you do, and all that, but that’s it. It’s a marginal concern, but that’s all it is, a marginal concern.
Note that this means that the case for medium-term caution if a winter wave does hit is much stronger this week than it was last week. If you wait, you do get meaningfully more protected, and there’s greater plausibility that life could mostly return to the old normal within a reasonable time frame. Similarly, there’s a less stupid policy case for doing more to contain the spread and stop the wave, since stopping the wave now buys time for a meaningful change.
I do not agree with those cases for those who have had booster shots, I think they still fall far short, but it is important to note that the arguments in favor did get substantially better. It’s a sign of how overdetermined things were before that I’m not close to changing my mind on this.
Think of the Children
Big Bird got vaccinated for Covid-19 this week. Here’s a clip of him getting vaccinated back in 1972, so none of this is new. Yet somehow when he Tweeted (yes, Tweeted, which for a Big Bird does seem rather appropriate) about his vaccine shot, this was a big news item for a bit this week, as according to various sources such as Ted Cruz this was government propaganda being used to push the Covid-19 vaccine on children.
A lot of the responses to this from the anti-vaccine crowd are dark. Also dark humor, which only benefits from the author quite likely taking themselves seriously.

I mean the framing on that, the attention to detail. Chef’s kiss.
Ted Cruz’s offering is much less refined, but the concept is even better, so I say it still wins. I mean, that’s great stuff, only I don’t think it sends the message he has in mind.
Is this whole operation government propaganda? No, absolutely not, HBO and Sesame Workshop did this on their own. Is it propaganda? I mean, yeah, sure, I guess, if you want to call it that, is there a problem?
Yes, there’s a problem. This horrible photographer thought a picture to remember forever justified spending a minute outside without a mask, and I’m glad I taught my daughter better than that, says proud area mother.
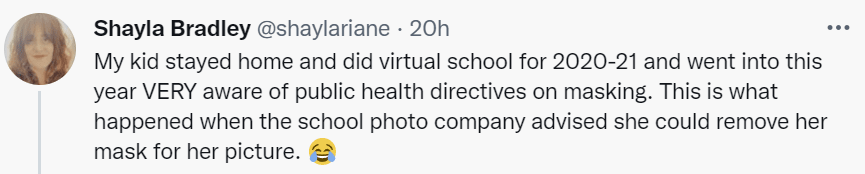

Once again, that photo, I mean look at her eyes, chef’s kiss. Future meme. Let this moment be remembered for exactly what it is. She has no mouth, and she must scream.
Therefore, Emily asks the tough questions about masks.
A number of pieces have also been written about the evidence of the protective value of masks in schools. Not everyone agrees on that topic. But today I want to look at what we know about the other side of the coin, which is actually the question I get most frequently from parents: Are there any downsides to mask wearing for kids in school or child care?
I mean. Open mouth. Close mouth. Boggle. I mean, sure, measure the magnitude of the downside, but asking whether there are any downsides at all? I mean, seriously, have you met a child? Have you even met a human being? What in the world?
When people discuss possible concerns with masks for kids, there are a few key issues that are raised:
Interference with breathing/respiratory health
Interference with social development (ability to read emotions and interact with friends)
Interference with intellectual development (learning to speak, learning to read, learning in general)
Concerns about students with disabilities
Yes, yes, all of that is good, that is an excellent list of some of the downsides one should measure. It reminds me of nothing so much as an Effective Altruist trying to measure the advantages of an intervention to find things they can measure and put into a report. Yes, they will say, here is a thing called ‘development’ so it counts as something that can be put into the utility function and we can attach a number, excellent, very good. Then we can pretend that this is a full measure of how things actually work, and still imply that anyone who doesn’t give enough money is sort of kind of like Mega-Hitler, especially given all these matching funds.
If you think you need to talk about Charles Darwin and the role of facial expressions in emotional development to understand that it’s not a free action to have to wear a mask all day, I’m sorry, I don’t think you have met a human being, I notice I am confused, what is even going on. No, that’s wrong. You’ve met a human, and you think that human hasn’t met any humans, or is willing to act as if they have not met any humans, and you’re reacting accordingly. And then, in this case, you’re forced to conclude that you can’t prove anything in terms of magnitude, so maybe masks are fine and don’t matter?
Burden of proof is a hell of a drug. So are demands for this kind of “scientific” rigor.
Ministry of Truth
In potential blog movement news, as my previous post noted, I’m considering moving to Substack, and I’m now also considering Ghost. If you have thoughts on that, please comment on the linked post rather than here. This includes if anyone has a good source for making the block editor or comment section on WordPress not terrible, or a recommended comment solution for Ghost since it requires you to pick one.
One of my considerations is potential future censorship, as this blog’s statements would doubtless have been suppressed and probably outright censored on major social networks and distribution channels such as Facebook or YouTube. Wordpress and Ghost allow self-hosting and are effectively immune. Substack so far has taken a strong anti-censorship position, but history tells us we should worry how long that will last.
Usually when I mention these concerns people will respond that no, that’s ridiculous, such actions aren’t taken in such cases, they have much bigger things to worry about. Except, well, no:

This is Cochrane. They are the gold standard on reviews of the medical literature. I’ve had my disagreements with them over the years, but it’s not like there’s anyone out there doing it better, unless there’s something I don’t know, in which case definitely let me know. Here is their Instagram, which has been declared dangerous and unmentionable due to ‘repeated posting of false information.’
So yeah. I’m going to continue worrying about such things.
In Other News
This story talks about trouble in the CDC, and I can’t figure out what it thinks went wrong beyond ‘political missteps’ and some sort of failure to get the White House to kowtow further to the CDC? It says there’s a ‘credibility problem’ and points to a few places where they outright proved not credible (e.g. said that which was not, and then couldn’t pretend they hadn’t done that) but didn’t seem to get into the systematic actual problems.
Twitter thread from Kelsey Piper about how much one can poison the well on an intervention by suggesting people actually use it, repeatedly and loudly, simply because it probably works. Also she points out that the guidelines for using Fluvoxamine still haven’t been updated.
19 comments
Comments sorted by top scores.
comment by Pattern · 2021-11-11T17:30:49.696Z · LW(p) · GW(p)
Trial was halted because medical ‘ethics’ is crazy and decided we couldn’t study the pill because it was too effective.
That...almost sounds reasonable. "It works!" "Great, trials over, now we know it's effective. Let's get this thing out there."
I propose the Law of Efficacy, which states that the requirement to halt a trial due to a drug being ‘too effective’ is that the drug has been approved for public use by the regulatory authorities.
If only.
comment by Daniel V · 2021-11-11T18:45:55.576Z · LW(p) · GW(p)
There is still far too much uncertainty in how effective Paxlovid is, due to the trial being halted early – the idea that we know what we need to know here already is absurd.
The chi-squared statistic (df=1) on hospitalization is 20.23, p<.00001. This is strong evidence against non-efficacy. What's your prior on non-efficacy? Or how unstable do you think these sample proportions are at this N? I've got a (non-Bayesian) 95% CI on treatment efficacy against hospitalization at (64%, 97%), so sure there's uncertainty in how effective it is, but I think we know what we need to know here - it easily meets the efficacy bar for approval, and it's highly effective. Would it be nicer to narrow our confidence interval more? For the sake of basic knowledge, sure, but meh. If there were other treatment options hitting in the same ballpark pre-hospitalization and we wanted to be choosy among them, then yes, but there aren't (correct me?), so what's the complaint here?
it should mostly replace prevention efforts other than vaccination.
It's a treatment, not a prophylaxis. This prevents hospitalization/death, not infection. So for preventing infections (if that is a goal), NPIs are still relevant.
To end on a positive note: good post, as always.
Replies from: localdeity, Zvi↑ comment by localdeity · 2021-11-12T00:23:32.282Z · LW(p) · GW(p)
it should mostly replace prevention efforts other than vaccination.
It's a treatment, not a prophylaxis. This prevents hospitalization/death, not infection. So for preventing infections (if that is a goal), NPIs are still relevant.
The treatment means that it's less bad if you get infected. Therefore it decreases the benefits of preventing infection. Therefore, infection-prevention efforts that were previously justified in a cost-benefit analysis might no longer be justified (on the margin).
For sake of illustration, if the treatment had negligible cost and total availability and was 100% effective at eliminating all COVID symptoms, then it would be essentially pointless to make any prevention efforts anymore.
Replies from: Daniel V↑ comment by Zvi · 2021-11-12T12:52:10.607Z · LW(p) · GW(p)
On the effectiveness question, I think 64% and 97% are hugely different numbers - they are an order of magnitude difference in remaining risk. So a CI that wide to me very much screams not enough data in terms of deciding how to act. I expect tons of expensive prevention efforts to be justified by that 64% number, that would be much harder to justify if we could be confident in 89%, and if it was known to be 97% would be much harder still.
On treatment versus prophylaxis, yes I understand that, but treatment and prophylaxis can be either complements or substitutes depending on the situation - if you have a good enough treatment it makes it less important to do prophylaxis (and vice versa).
comment by Josh Jacobson (joshjacobson) · 2021-11-11T17:13:48.516Z · LW(p) · GW(p)
Thought about the timing of Pfizer pill availability for ~2 minutes, current guess is that it will be similar to the vaccines last year. Late this year very limited availability, becoming more and more available in the early months next year, easy to get around April or May.
comment by arunto · 2021-11-14T10:44:49.610Z · LW(p) · GW(p)
"The question is not whether cases will continue increasing, but rather whether the increase will accelerate and by how much. "
Looking at what is currently happening here in Germany and its neighboring countries (e.g. Netherlands, Austria, Denmark) the increase is highly likely to accelerate.
Why can a look at these European countries be somewhat predictive for the US? Berlin and Amsterdam lie further north than Montreal or Toronto. And the climate table for Berlin in September is similar to the climate table for Chicago in October. Therefore I think that the behaviour of the delta variant due to seasonality here in Europe now can to some extent give an indication what is going to happen in the northern half of the US in about a month. And the vaccination rates here are higher than in the US (completely vaccinated: US 58.5%, Germany 67.1%, Netherlands 64.8%, Austria 64.9%, Denmark 75.7% - numbers are based on NPR and ECDC; there are slightly different numbers für the European countries depending on the source I look at, but the general picture is clear, I think.)
Given those vaccination numbers and what is happening here (see below) I believe that parts of the US Midwest are quite likely to be hit hard by a next wave at the end of the year with current vaccination rates of 53.9% (Michigan), 52.3% (Ohio) or 50.1% (Indiana). And even the high vaccination rates in the New England states (e.g. Vermont 71.8%) could not be enough to prevent a next wave without at least some countermeasures against transmissions beeing in place.
Germany
Germany is back into exponential growth. The seven-day-R-value in Germany has been fairly constant at about 1.2 since mid October. However the growth rates differ between the states by their vaccination rates (from 57.4% fully vaccinated in Saxony to 79.1% in Bremen). I have calculated the correlation between vaccination rates and 7-day-infection-rate of the 16 German states, the results were r = -.78, p < .001. The steepest rise was in Saxony with an increase in infections over one month of nearly 500% and in Thuringia with about 400% (RKI).
The states with lower vaccination rates, Saxony (57.4%), Thuringia (61.4%), Bavaria (65.4%), and Baden-Wuerttemberg (65.5%), report massive problems with their hospitals due to shortages in intensive care capacity. Currently, they are able to compensate this with transfers to other hospitals within state but they expect to be forced to transfer patients to other states soon. There are on a regular basis reports from different states about outbreaks in nursing homes with half a dozen fully vaccinated (2x) inhabitants dying of covid.
This development has happened within the following regulatory framework: Germany has maintained mask mandates in public places (however not in most schools). For many situations, e.g. bars and restaurants, there has been a rule of "3G" (geimpft, genesen, getestet = vaccinated, recovered in the last 6 months, recently tested), although there are increasing regulations with "2G" (only vaccinated or recovered, no entry for unvaccinated). There are no vaccination mandates, e.g. for the healthcare sector.
It is not clear yet which additional measures will be implemented. There is talk about possibly changing to "2G+" (only vaccinated or recovered, but both with an additional recent test) and about reintroducing home office mandates for business.
Netherlands
The Netherlands had stopped most countermeasure (mask mandates, social distancing) on September, 25, but has reintroduced those measures after seeing a strong increase in infections. This weekend they opted for a partial lockdown (e.g. shops and restaurants closing at 8:00 pm, max 4 visitors at home, home office if possible) - an announcement that has lead to massive public protests (France24).
Austria
In Austria with a higher incidence than in Germany some states are imposing a lockdown for unvaccinated persons. It is planned to extend this lockdown for the unvaccinated nationwide (France24).
Denmark
Denmark with its high vaccination rate hasn't had problems on the scale of the other countries mentioned above. They lifted their restrictions mid-September but a recent surge of infections has forced them to reconsider reintroducing some countermeasures (CNN).
Of course, the vaccination rates between Europe and the US can't be compared without adjustments because e.g. the rates of natural immunity due to a prior infection can be different. But nevertheless, there are many parts of the northern half of the US with vaccinations rates so low that it seems unlikely that they will not have a massive infection wave. And Denmark with its very high vaccination rate shows that even the high vaccination rates in the New England states probably won't be enough without additional countermeasures to escape the next wave.
Replies from: arunto↑ comment by arunto · 2021-11-14T19:33:01.424Z · LW(p) · GW(p)
Additional information:
A couple of hours ago Austria has decided to implement a lockdown for unvaccinated citizens in all its states (Reuters).
And I have looked at the numbers for their two states with low vaccination rates:
Upper Austria: 55.89 % fully vaccinated (1), 415% increase in the Covid incidence in the last 4 weeks
Salzburg: 57.06% fully vaccinated (1), 490% increase in the Covid incidence in the last 4 weeks
Sources: Coronavirus in Österreich, AGES Dashboard.
Which closely mirrors the growth rate for the German states with similiarily low vaccination rates (Saxony, Thuringia).
(1): Here, fully vaccinated does not imply a third, booster shot.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-17T05:20:32.417Z · LW(p) · GW(p)
Austria is also allowing for recovery from natural infection within the last 180 days.
I'm kind of hoping that when the Biden administration's mandates get to the SCOTUS, instead of invalidating them completely, they demand a tweak like that (natural immunity). That would give that position the appearance of compromise.
comment by Robbo · 2021-11-12T11:18:24.772Z · LW(p) · GW(p)
I'm curious about this passage:
Yes, yes, all of that is good, that is an excellent list of some of the downsides one should measure. It reminds me of nothing so much as an Effective Altruist trying to measure the advantages of an intervention to find things they can measure and put into a report. Yes, they will say, here is a thing called ‘development’ so it counts as something that can be put into the utility function and we can attach a number, excellent, very good. Then we can pretend that this is a full measure of how things actually work, and still imply that anyone who doesn’t give enough money is sort of kind of like Mega-Hitler, especially given all these matching funds.
This seems like it's alluding to a more detailed, strongly-held, and (if correct) damning assessment of (at least early-years) effective altruism. I'd like to understand that position more. Have you written about this elsewhere?
Replies from: The Scary Black Hundreder↑ comment by The Scary Black Hundreder · 2021-11-16T13:00:33.030Z · LW(p) · GW(p)
Moreover, it is unclear to me what point the OP is making about the list of potential downsides of wearing masks. Perhaps it helps to already know his position on that matter?
comment by Jody Lanard · 2021-11-21T23:54:27.065Z · LW(p) · GW(p)
Re: >Meanwhile in Singapore, they’re done paying for Covid-19 treatment for the ‘voluntarily unvaccinated.’<
The linked article makes pretty clear that all Singapore did was revert the unvaccinated to the pre-pandemic way of paying for their health care, without the pandemic exception of the government paying for COVID-related health care.
The only Singaporeans who are getting "free" COVID health care now are those who are vaccinated, and have not traveled recently, and catch COVID.
If we want to see this "free COVID care" as a reward for being vax'd and not taking risks like traveling outside Singapore, that's fine: see it as a reward.
But it's not fine to imply that taking away "free" COVID health care for unvax'd Singaporeans is a punishment.
The unvax'd are just going back into the general population of Singaporeans who pay for their own health care, out of their own insurance and medical savings mechanisms. This includes vaccinated Singaporeans who pay for their own non-COVID related healthcare.
Much of the western media covering this story conveyed the impression that Singapore is "punishing" the unvax'd by not paying for their COVID-related health care. I think this is a kind of mis-information. Even though Zvi links to an article that partially explains this, Zvi's short excerpt still gives this false impression.
With great respect and admiration for Zvi and LessWrong,
Jody Lanard MD (on Twitter: @EIDGeek )
comment by 3arthsea · 2021-11-20T21:49:05.952Z · LW(p) · GW(p)
I don't think I entirely agree with your characterization of the situation and would like to push back a bit.
> 2. It is illegal to continue a trial to study the drug, because it has been proven so safe and effective that it isn’t ethical to not give the drug to half the patients.
Sorry, but where are you getting this from? I am pretty sure it is not illegal to continue a trial if it crosses an efficacy or futility boundary in the interim (happy to be corrected on this point). In fact, when futility boundaries are crossed in interim analyses (ie, when it seems a drug is most likely to be ineffective), the trials are often continued after discussion by the data monitoring committee. There are specific ways to handle this--statistically this means setting up a "non-binding" interim analysis boundary. In other words, you can choose to continue the trial even if the drug is deemed "too ineffective" (or "too effective) in an interim analysis.
The reason trials rarely (never?) continue after crossing an efficacy boundary in the interim is because there's no incentive for the sponsor (ie, the drug company) to continue once a drug has been deemed effective. And to recruit more patients costs time and money for essentially no added benefit. You can choose to read this uncharitably (Big Pharma is skimping on money) or charitably (they are shortening time to approval and helping more people earlier).
3. Who, if they weren’t in the study, couldn’t get the drug at all, because it is illegal due to not being proven safe and effective yet.
4. So now no one gets added to the trial so those who would have been definitely don’t get Paxlovid, and are several times more likely to die.
As I see it, the two possible scenarios are this: 1) You stop a trial early and submit data for FDA approval. This gets the drug in the hands of the masses earlier. 2) You run the full trial and then submit data for approval. Wider access to the drug is delayed, costing lives.
The first option is better because I think we can reasonably assume that the time it takes for FDA to approve the drug is same in both of the cases (and so equal no. of people will be harmed while waiting for the FDA to approve the drug). However, wider access to the drug is established quicker in the first scenario, thus saving more lives over the long run.
6. For the rest of time we will now hear about how it was only seven deaths and we can’t be sure Paxlovid works or how well it works, and I expect to spend hours arguing over exactly how much it works.
7. For the rest of time people will argue the study wasn’t big enough so we don’t know the Paxlovid is safe.
8. Those arguments will then be used both by people arguing to not take Paxlovid, and people who want to require other interventions because of these concerns.
IMO, this makes your critique kind of incoherent to me. Should the FDA be more conservative in this scenario or not? If you wait for more precise treatment estimates by running a full trial, then there's a delay which costs lives (as I outlined previously). Or you could be less conservative given the circumstances, make do with the best statistical methods you've got and accept results from an interim analysis.
FWIW, the statistical literature on stopping trials early is indeed mixed (eg, you're prone to over-estimating effect sizes although there are ways to adjust for it now but it's an ongoing area of research and so on). However results from interim analysis are deemed perfectly acceptable by drug regulatory authorities and ideally, stopping early should not be inflating Type-I error etc. (statistical methods try to take this into account) So, results from an interim analysis should be as good as running a "full" clinical trial.
I think most of us agree that FDA should be less conservative (especially during covid) and that's exactly what it's doing by accepting results from interim analyses. This is actually one of the few instances where FDA's decision making is anti-conservative. And again, like I said before, it is not illegal to run full trials if you get positive results from interim analyses.
So, to summarize, I am kind of confused by your characterization of the situation. I think FDA should definitely be doing better in emergency situations but the specifics of your criticism here don't seem convincing to me. What is the proposed alternative here? Don't accept interim analyses? Force drug companies to continue the trial if interim analyses are beneficial while waiting for drug approval?
comment by cistrane · 2021-11-13T09:26:18.201Z · LW(p) · GW(p)
Looks like Quebec government is seriously concerned that unvaccinated medical workers will quit.
https://globalnews.ca/news/8346947/quebec-drops-vaccine-mandate-among-health-care-workers/
Replies from: Zvi↑ comment by Zvi · 2021-11-13T10:11:57.741Z · LW(p) · GW(p)
Looks like they managed to get a 97% vaccination rate, but found that not good enough, so they abandoned the mandate and permanently sacrificed everyone's credibility but especially their own, whereas places without a mandate usually end up far lower. So the news here is that Quebec defected and burned the commons?
Replies from: The Scary Black Hundreder, cistrane↑ comment by The Scary Black Hundreder · 2021-11-16T13:19:58.533Z · LW(p) · GW(p)
Even assuming we live in a world where there is a reasonable hope of eradicating covid with the vaccines that we have, it still wouldn't be enough to simply rely on a gentleman's agreement for various parties to implement mandates. Different parties have different incentives, and even dictatorships have to spend political capital to impose policy. And if the imposed policy turns out to be much less effective than promised, there is even less political capital to impose the next policy.
↑ comment by cistrane · 2021-11-14T19:02:11.040Z · LW(p) · GW(p)
Plus the 3% of holdouts (14 thousand in absolute numbers) are critically important , apparently they cannot afford to lose anyone at all. Which is very strange. There are less than 9 million people in Quebec and according to their numbers, 420 thousand are employed in healthcare which is 10% of their employed population.