Taking Initial Viral Load Seriously
post by Zvi · 2020-04-01T10:50:00.542Z · LW · GW · 45 commentsContents
Category 1: Better Information Category 2: Things Individuals or Small Groups Can Do Bird’s Eye View How Many Infections are High Versus Low Load Now? One’s Own Risk Two to Tango Three is a Crowd Category 3: What Society Can Easily Do (Beyond Gathering Data) Category 4: Bold Action Conclusion None 45 comments
In part a response to (Overcoming Bias): Variolation May Cut Covid19 Deaths 3-30X
Also related: This is an expansion of parts of this debate with Robin Hanson.
Epistemic Status: Thinking out loud. Food for thought. Not an expert.
Initial viral load seems likely to have a large impact on severity of Covid-19 infection. If we believe this, we should take this seriously, and evaluate both general policy and personal behavior differently in light of this information. We should also do our best to confirm or deny this hypothesis as soon as possible.
Robin Hanson and I had a debate [LW · GW] on Sunday regarding his proposal of variolation: Deliberate Covid-19 infection of volunteers, using small viral loads, followed by isolation of those volunteers until recovery. I felt it was an excellent discussion. As with all such discussions, some key points are glossed over, lost or not stated as well as one would like in hindsight, there are areas that never come up, and one thinks of important additional things afterwards.
What evidence do we have that viral load matters?
Three classes of evidence seem strong.
The first is that we have a strong mechanism story we can tell. Viruses take time to multiply. When the immune system detects a virus it responds. If your initial viral load is low your immune system gets a head start, so you do better.
The second category is the terrible outcomes in health care workers on the front lines. Those who are dealing with the crisis first hand are dealing with lots of intense exposures to the virus. When they do catch it, they are experiencing high death rates. High viral load is the only theory I know about so far for why this is the case. Their cases are presumably handled at least as well as others, in terms of detection, testing, treatment and what the infected do themselves. The only other issue I can think of is that they might be reluctant to rest given how urgently their help is needed.
The third category is historical precedents.
Robin’s proposal for variolation is similar to what was historically done with smallpox. Parents infected their children with what they hoped was exactly the minimum dose required to get them sick enough to develop antibodies and gain immunity. Sometimes this went wrong and the child would get sick. Thus this form of inoculation was dangerous and 1%-2% of patients died. But of those who got smallpox infections in other ways, 20%-30% of patients died. Those rates are well established.
Another classic example is measles. We have a study that says that the first child in a family to contract the disease was relatively safe, whereas other children in the same family were 14 times as likely to die. That’s another huge gap. This is from a study of 126 children, so much less certain, but effect sizes that big are not accidents.
Finally for SARS, we have the Hong Kong high rise where proximity to the index patient played a crucial role. Here we see a factor of three difference. SARS being so deadly that 70%+ of highly exposed patients died could be a reason the ratio of deaths between high and low viral load was only three to one.
There are also claims that we can observe higher viral loads from lockdowns making things worse and increase death rates, allowing us to be more confident that viral loads have a big impact. I do not find this convincing because of likely reverse causation and other highly non-random factors that determined where lockdowns happened earlier. Later on I’ll analyze the likely impact of lockdowns on viral load, where I get a different answer than Robin’s.
It’s worth noting that we have vaccines for smallpox and measles, and the SARS virus in question was contained, so none of these three are remotely candidates for variolation no matter the true ratios.
What is the evidence against viral load having a big impact?
The evidence of absence is the absence of further evidence. Yes, the effects observed were very big. Yes, they are all the result of natural experiments and we have been ethically precluded from doing randomized trials or other better studies, so the lack of those trials doesn’t mean much. But how likely is it we didn’t find more natural experiments where viral load would have differed in an observable way? Publication bias here could be a large effect.
These effect sizes are super large. It seems odd for them to hold for some viruses, and not to have a large effect in most others. But if that’s true, how is it we are not observing them? Maybe we really don’t ever look so it’s never come up. But it definitely seems odd.
There’s also the small sizes for the measles and SARS studies, which have about 200 patients between them. That does not seem like enough to draw general conclusions with any confidence.
The smallpox case represents the best case, but it also represents an engineered best case of exactly the minimum dose in exactly the right way, along with awareness of the situation versus a society that otherwise had little idea how to handle infections. It also represents the case in which things went so well that ordinary people managed to fight through all the barriers and actually do the thing. It makes sense to assume this was an unusually large effect size.
We have to ask why smallpox was a unique event, and we never used this method for any other virus. Did we even ever consider it?
My prior at this point is that the difference between a low and high initial viral load of Covid-19 is large. The theory makes too much sense. But with high uncertainty.
Suppose we agree that it is likely. At a minimum, there is a large chance of a large effect, and essentially zero chance of a backfiring effect – at worst, a low dose is the same as a high one.
What should we do? How do we take this seriously?
Four categories of things one might do.
- There are things we could do to get better information.
- There are things individuals or small groups can do to improve their situation.
- There are things society as a whole could try to do that don’t have big downsides.
- We could take bold action, potentially including variolation.
Category 1: Better Information
The failure to collect more and better information about Covid-19 has been atrocious, shameful, expensive and deadly.
We shouldn’t only be doing a crash project for a vaccine and ramping up testing much faster and immediately testing every treatment that shows any promise.
We should be collecting extensive population-level data everywhere. Mostly we’re not collecting any data at all that isn’t massively biased.
We should be studying with experiments how Covid-19 spreads, and how likely each method is to work, using controlled experiments. Yes, this involves infecting individuals. Considering how many lives are at stake and the ability to test using young healthy volunteers who are then isolated, I fail to see how anyone who objects on the basis of ‘ethics’ knows what that word means, or why we should listen to them.
We should use those experiments, and additional experiments if necessary, to study effects of viral load. Because again, that knowledge would save so many lives, in addition to tons of economic distress that could force horrible choices upon us.
We can shut down the entire economy, force people to stay home and create double digit unemployment. And we can’t do this? Really?
The more I think about the Covid-19 situation, the more I think the highest leverage thing most people reading this can do is to find ways to get our hands on better data.
Better information would (of course) make it much easier to know whether it made sense to take other action, know which actions made sense, and gain support for the right ones, across the board. As we go over what else we might do, all of that will emphasize how valuable more information would be.
My current best thought for how to do experiments quickly is medical cruise ships in international waters. We even have lots of spare cruise ships lying around with nothing to do right now, which we could convert if we needed to. Medical cruise ships are already an established way to do things without running into regulatory problems. We could do things properly, in a way that would give trustworthy results and would allow others to trust the data. The tests required are not expensive or difficult to produce if no FDA regulations get in one’s way. Such projects are well within the ‘Bill Gates decides to just go ahead and do this’ price range.
Still, one must be realistic. Given we likely won’t get much good information soon, and time is very short, I’ll proceed as if we are physically prevented from information gathering.
Category 2: Things Individuals or Small Groups Can Do
Bird’s Eye View
Things individuals can do are a good place to start, because ‘scale up what an individual should do’ is an excellent hypothesis for much of what a society should do. I agree with Robin Hanson that people who are at risk, and say they are more concerned with infecting others than becoming infected, are usually wrong about that. I still think most people care a lot about preventing others from becoming infected. Incentives, in most places, are not so misaligned.
The first question one would ask is, what infection methods result in a high load, versus which methods result in a low load. Or to be more granular, what lowers or raises such loads.
The default model is that the longer and more closely you interact with an infected person, especially a symptomatic infected person, the larger your viral load.
In-household infections are presumed to be high viral load, as in the case of measles. So would be catching the infection while treating patients.
Most out-of-household infections that aren’t health care related are presumed to be low viral load. Anything outdoors is probably low viral load. Most methods that involve surfaces are probably low viral load. Infection via the air from someone there half an hour ago, to the extent this is a thing, is low viral load. Quick interactions with asymptomatic individuals are probably low viral load.
Knowledge would of course be far better than supposition. If anyone has actual information on any of this, please do share it in the comments.
The only method that seems highly ambiguous is the fecal-oral transmission route. We don’t know how dangerous it is either in terms of infection probability or likely viral load. It could be anything from almost harmless to very dangerous.
To a first approximation, we can say that a typical person (who is not a health care worker) should consider it more deadly to be infected via household transmission. They should consider it less deadly to be infected out-of-household.
We can also consider it relatively more deadly when the infection risk from a given source was otherwise high, or one might be infected from multiple sources at once. When one is exposed to a low-probability infection from a small number of sources, expected viral load is low.
How Many Infections are High Versus Low Load Now?
One place I disagree with Robin Hanson’s analysis is that he is comparing an intervention to create universal low viral loads to an alternative of mostly high viral loads.
I believe he is discounting the extent to which many infections are already low viral load. Consider our intuitive model, and infection rates from the poorly named category ‘close contacts.’
If you had an infected ‘close contact’ in Wuhan, your probability of infection was only 2.5%. Close contacts within the household were much more likely than those outside it to pass along the infection. If we focus on asymptomatic close contacts outside the household, we match our intuition that infection is possible but any given person is unlikely to infect us – the paper gives the probability of infection from each asymptomatic ‘close contact’ that wasn’t all that close at only 0.03%!
Under current lock down conditions, where anyone who got this far into this post (again, who doesn’t have an essential job that prevents this) is presumably avoiding anyone symptomatic, and most symptomatic people are self-isolating or seeking help, it does not seem so hard for most of us to avoid direct out-of-household interaction with highly symptomatic people.
Thus, let’s simplify the baseline for those taking ‘ordinary precautions.’ Out of household transmission is low load. Inside of household transmission is high load. To balance this out, let’s presume that if anyone in a household gets infected, they are probably going to infect the rest of the household, and we’ll set that probability at 100%.
If you are the only member of your household, unless you take big risks or something highly unlikely happens, you’re going to have a low viral load.
If you are one of two members, then one of you will get a low load, and one of you will then probably get a high load.
Overall infection rates are unknown due to inexcusably poor data, but we do know that the probability of infection on a given day for a given person who is taking precautions is low even if many are currently infected around them. Thus, unless household members are exposed from the same source at the same time, the probability of simultaneous infection that gets them both a low viral load is very low and can be rounded off to zero.
The biggest factor thus effectively becomes, how big is your household?
The average household size in the United States of America is about 2.6 people. If we exclude children, the average household size is 2.02 people, which we’ll round to 2.
Children can spread the infection, but they probably are not as effective at it and they do not have essential work outside the home. It should mostly be easy, once schools have closed, to avoid having them get infected before other household members. If they are infected in-household, we don’t care much if they have high viral loads since their risk remains very low.
Thus, of those that matter and who reside in a household, approximately 50% will get low viral loads in a lock down. This will briefly be false in the first week of a lock down, since you clamp down on out-of-household infections but not inside-of-household infections during that period. But longer term, the impact of higher-probability inside-of-household transmission does not matter very much, because the probability of inside-of-household transmission, once someone got infected, was so high already. The only effective defense is to stop out-of-household transmission so everyone in the household stays uninfected in the first place.
Lock downs seem like they would decrease viral load conditional on an out-of-household infection, as long duration in-person indoor interactions, and other ways to get a high viral load, seem to be down a lot more than other out-of-household transmission vectors. So intuitively, lock downs are actually net good for viral load.
The exception is if they change household size, by causing people to shelter together, which brings us back to what groups can do.
We also need to consider what to do about those in institutions, especially nursing homes. That could drive these numbers higher, if such people are effectively inside the same household, and that can’t be fixed.
Looking at a 50% low risk, 50% high risk scenario, we can only save 50% of what we could save if we started in a 50% high risk scenario. So a range of factors of 3-30, which I already discounted because of selection bias in the evidence, can further be cut in half. That gives us a reasonable range of room for improvement of about a factor of 1.5-10. Still a big win! That could be higher if we could do even lower initial loads than what we are calling ‘low load’ but a procedure that is <0.1% to infect you already seems likely to functionally be close to the minimum dose.
One’s Own Risk
If you are living alone, that seems great.
By definition, you can’t be infected inside-of-household with a household size of one. Thus, unless you need to do other high-risk activity, your viral load will be low.
If you are already mostly self-isolating, then you can worry less about incoming holes in your containment procedures. If you do get infected, you’re unlikely to pass it along, your risk will be lower than you would otherwise calculate,
There is an argument that if you’re alone and not going outside for a month conditional on getting packages, and you are young and healthy, you can stop worrying about getting Covid-19 from those packages. If it did happen, you are perhaps doing a solid approximation of variolation, after which you will be immune. That might actively be better than wiping the packages down or letting them sit for three days.
Two to Tango
If there are two people in the household, the calculus changes. We also get some non-intuitive results – since infecting anyone in the household probably infects everyone, protecting the more vulnerable member of the household means you want them to be infected first.
The first thing to note is that, in theory, sufficiently correlated risk to both individuals seems actively great. Both of you getting infected at the same time means you both get low viral loads. This is not easy to pull off, since most risks worth taking are low probability even when they are risky (e.g. <1% chance of infection even if the close contact is infected) so the chance of actually catching it at the same time is still low. But it could be worth thinking about.
The second thing is that people may be allocating infection risk backwards by default. Suppose you have a high risk old individual in poor health, and a low risk young individual in good health. You can’t get groceries delivered and supplies are running low, so someone has to run to the store. Who goes?
Intuition says of course the individual in good health should take the risk. But if we take the whole model seriously, that seems wrong now! If the healthy individual gets infected first then you have a low-risk infection in a low-risk individual (small win) who then infects the high-risk individual and puts them at high-risk again (big loss). You would want to reverse that process.
The counterargument here is that there is some evidence that higher risk individuals are also going to catch the virus more easily, which could prevent the situation from reversing. Again, we need better data!
The third thing is that social distancing within the household starts to look more valuable. Viral load depends on the exact interactions that take place. It makes sense to place at least some value on minimizing infection exposures between household members, even if you are mostly resigned to the infection eventually happening once anyone gets infected. There is still something important to win.
A household with varying risk levels due to age or health, to the extent possible, might choose to concentrate as much within-household exposure as possible in the less risky direction. For example, perhaps the person at high risk should be doing most of the cooking.
If one person does show symptoms first, precautions then become super valuable, even if they probably ultimately fail to prevent spread.
Three is a Crowd
Larger households mean bigger risk of high viral loads. Such groups have both a higher risk of infection at all (since any of them could get infected) they also carry a bigger risk via higher expected viral loads. Thus, as a group scales higher, precautions become even more important.
The obvious strategy is to break up large households. If you have more than two adults in a group, consider that an even higher cost. If you have a lot more than two, this gets extreme. And as before, if you have low-risk individuals together with high-risk ones, having the low-risk individuals take all the risks looks pretty bad. If you do that, it might make sense to consider social distancing within the household where feasible, if it can turn potential inner-household transmissions into effectively out-of-household transmissions. This is especially true if you have reason to believe someone may have been exposed recently.
If there are multiple households considering interacting with each other, that now looks like a bigger additional risk as well. Those types of interactions could effectively be inner-household style contacts.
For those with family members or housemates who insist on taking risks, you should be even more worried than before. The people living with the risk-taker are now at greater risk than the risk-taker themselves. It becomes that much more important to do something about such actions.
Category 3: What Society Can Easily Do (Beyond Gathering Data)
If we think there are things individuals should do, society’s first job is to encourage those people to do those things. Thus, everything in category two could be added to existing lists of recommendations.
But that’s not a practical answer. Bandwidth is limited. People are already overloaded with information, and with disinformation.
If you only get about five words [LW · GW], those five words need to be something like “socially distance, wash hands, mask.” Even not touching your face wouldn’t make the cut. We still have major organizations continuing to actively spread disinformation against even that level of response.
Everything we go over here is therefore probably far too subtle. It also risks muddling the messaging on more important matters. Any intervention for the public as opposed to people who read long analytical blog posts needs to have a focused simple message that could be attached at the end of the current list of simple useful interventions.
Another argument against spending bandwidth on this is that minimizing an individual’s viral load does not much help bend or smash the curve, and anything that reduces R0 is higher leverage and takes priority over other actions. The obvious retort is that lots of people in my circles and other circles are focusing on ventilators.
The simple message of minimize household size seems like a reasonable candidate. Since a large percentage of infections are within-household, this seems like a strong intervention even without viral load concerns. Perhaps we want to emphasize this more. We could use the viral load argument as an additional justification for an already good intervention.
A second strategy would be to ban activities that lead to high viral loads but not ban those that lead to low viral loads. This could make infections less deadly while doing less economic damage. The risk is that there are still a lot of large households out there. It seems beyond our abilities to say “people living alone and not working in a highly interactive position can do X, but not people living with others or working in ways that interact with others.” I would love to be wrong about that. Still, some amount of adjustment of what we do and don’t permit or encourage, on the margin, would be helpful.
It seems hard to do more than that on a broad basis until we have much better data. So again, the most low-hanging fruit is to gather data. Run experiments. Do more and faster science to it.
Category 4: Bold Action
Suppose we manage to gather better data and it turns out viral loads are a big deal.
Say, we become confident that minimal loads have a 0.1% death rate with proper medical care and high loads have a 2% death rate with proper medical care, and lock down conditions have a roughly 50/50 mix of both and a 1% death rate. That’s a bigger effect than I expect, but very much in the realm of the possible.
That difference is a really, really big deal. It’s a much bigger deal than getting enough ventilators. It’s potentially a bigger deal than having a medical system at all. Alternatively, it’s potentially a bigger deal than the difference between 100% infection rates and the infection rate a few weeks from now (or in some places like Spain or New York City, potentially the infection rate today). It’s not enough to overcome both of those differences at once.
It is certainly a big enough difference to justify bold action to minimize high viral load infections among our most vulnerable populations.
Suppose we got our act together. We want to do more than nudge individual behavior. We are willing to do things that people find instinctively repugnant, provided they save lives while at least not hurting the economy. How could we accomplish this?
The possibilities I can see are subsidizing household divisions, strategic variolation of individuals, variolation of the young and healthy, or variolation of the old and vulnerable.
Subsidizing household divisions means exactly what it sounds like. We could offer tax or other incentives, up to and including providing housing and forcing people to use it, in order to break up sufficiently large groups of adults, or sufficiently large groups of adults that contain at least one at-risk member (e.g. someone over the age of 60, or 70). Given the economic costs of shutdown, actions that involve spending large amounts of money and/or using large amounts of coercion are being underconsidered in general. We are already using lots of coercion and paying gigantic economic costs! The difference is we are doing so passively, via preventing actions, rather than actively via causing actions. That’s not a hill I want us to (literally) die on.
Then there are variolation strategies, where we deliberately infect individuals. Or alternatively, if we find out-of-household infections are low enough viral load, perhaps we could do this passively via allowing those in single-adult households to do things that cause them to infect each other in such ways, while otherwise taking strong precautions so they avoid infecting others.
There are a lot of bad objections to such policies. I won’t waste space addressing them other to note that they present practical barriers to implementation, and that they force us to be sure to do all of this carefully and correctly to have a chance of avoiding being shut down or worse.
One very strong objection is that our medical system is about to be overwhelmed. Anyone we expose now will either take needed resources away from others, or go without those resources. Thus, we either need to be in a world in which everyone is already going to get infected while the system is overwhelmed and we can’t stop it (in which case perhaps the best we can do is get remaining people low viral loads and hope for the best), or a world in which the virus has been contained for now but where we don’t have a long term plan that can keep it that way (e.g. some places can squash and keep their medical systems stable for a while, but they can’t stop reintroductions while reopening the economy, and the economic costs of doing this for long enough to wait for a vaccine or other solution are not an option).
Infecting the young and healthy is the natural first thing to model. The young are at relatively low risk. That risk is not zero, even if we assume big impacts from low viral loads, screening for comorbidities and ensure good at-home care. But if such people will eventually probably get infected anyway, we can reduce their net risk while allowing them to return to work and other activity much faster. Then that slows the further spread of the virus, hopefully allowing more high-risk individuals to never get infected at all.
Robin’s current best concrete suggestion, once we have established the safety and value of the procedure via testing, is to create variolation villages. Those who voluntarily participate and are deemed healthy enough would be isolated and infected, we would verify the infection and then allow them free access to the village until they were safely cured and non-infectious. Then they could return to their lives and move freely.
One could respond that this is exactly backwards. If low viral loads are a big win, why are we protecting those who least need that protection? Why aren’t we protecting those who most need it? This argues that, given we will have limited capacity, we should instead look to variolate the old and at risk, since we are reducing risk and they benefit from this the most.
Going down this path means we’ve concluded that protecting them, via herd immunity from the young or via general suppression or otherwise, is not realistic. These are exactly the people who ideally we don’t let get infected at all. If they do get infected, even carefully, they will need a lot of care. Doing this requires even more ideal conditions than infecting the young. We either need a lot of spare medical resources without having much hope of long term containment, or we need to have essentially no hope of stretching things out very far before most are infected.
Those who are capable of sustained safe isolation would want to avoid participating even under the best conditions.
That leaves what I am calling strategic variolation. Rather than taking whoever volunteers, or sorting by age and health, we choose people who (both volunteer and) provide superior leverage. Look for those who would otherwise be forced to expose themselves to high viral loads or lots of interactions. Alternatively, look for activities that cannot be done while social distancing, but which have very high value. Focus on those categories of individuals and at least give them priority. Alas, many would consider this an even worse look than a general call for volunteers, so much so that I am not naming anyone I would prioritize. If we got farther along this path, there would be plenty of time to discuss that.
Conclusion
Viral loads are not being taken seriously. We should take them seriously.
On an individual and household level, that means thinking carefully about how to avoid high viral load infections especially for those most at risk.
On a societal level, that means gathering much better data about how impactful this factor is and how it works (and about all other aspects of what is happening, of course), so we can consider taking bold action if appropriate. It also likely means encouraging smaller household groups during the pandemic.
Remember, I am not an expert. This is only me thinking out loud.
45 comments
Comments sorted by top scores.
comment by [deleted] · 2020-04-01T14:40:53.341Z · LW(p) · GW(p)
It should be noted that a big part of smallpox variolation was not the viral dose, but the means by which it entered the body - a scratch instead of an orifice.
Replies from: matthew-lewis, jmh↑ comment by Matthew Lewis (matthew-lewis) · 2020-04-04T18:39:42.371Z · LW(p) · GW(p)
I proposed in a another thread that variolation of the GI tract, where there are known cell populations expressing ACE2, might be preferred to lung. Avoiding the lung infection from the the apical surface of AT2 lung cells sounds like a good idea.
Replies from: Davidmanheim, None↑ comment by Davidmanheim · 2020-04-05T19:00:13.487Z · LW(p) · GW(p)
It's unclear to me that you wouldn't end up with a worse clinical course in this case - perhaps you wouldn't, but I'm not sure why you'd assume it's safer.
Replies from: None↑ comment by [deleted] · 2020-04-06T08:16:28.504Z · LW(p) · GW(p)
It's a superficially plausible idea, assuming you don't always burp or vomit the virus up into your lungs anyway or get very slight viremia getting them there anyway too which is COMPLETLEY possible given what we know. And assuming you somehow get it into your gut without getting it into your throat. Huge numbers of assumptions, dosage unknown, methods unknown, effectiveness unknown. Superficially plausible and right now a very bad idea. You absolutely CANNOT assume it's safer, but it could be something to look for in case studies of natural infections, seeing if people who first manifest with intestinal issues have lower levels of pneumonia.
If you COULD somehow reliably restrict viral replication to the gut rather than the lungs... I don't think many first-world (or, to expand the sample, American) COVID patients have died of the diarrhea.
EDIT: "Patients with COVID-19 who have digestive symptoms were shown to have a worse prognosis than those without."
Replies from: Davidmanheim↑ comment by Davidmanheim · 2020-04-06T11:35:32.123Z · LW(p) · GW(p)
I'm more concerned about increased rates of central nervous system impacts and cytokine storms, both of which are rare in typical COVID cases, but seem closely related to high fatality rates in the minority where they occur.
↑ comment by jmh · 2020-04-01T17:23:41.235Z · LW(p) · GW(p)
Wouldn't the entry means it self function a bit like a control on the viral load?
However, that point is clearly something that should matter to the larger point I think is being made.
Replies from: None↑ comment by [deleted] · 2020-04-02T01:10:23.963Z · LW(p) · GW(p)
You could plausibly construct a chain of reasoning that lets you imagine that being exposed to the virus in the intestines first might decrease the odds of getting a lung infection. There is little to no actual *evidence* of this at this time, but it could be a thing to look at in case studies.
EDIT: "Patients with COVID-19 who have digestive symptoms were shown to have a worse prognosis than those without."
comment by Connor_Flexman · 2020-04-06T19:19:48.521Z · LW(p) · GW(p)
I think the common factor between COVID and smallpox is their long incubation times, which isn't shared by something like 95% of current ambient disease (not sure about historically).
This makes sense with the proposed mechanism. There must be some short length of incubation period where your immune system wouldn't have time to get much stronger even if given double the notice, some longer period where it can definitely grow much stronger given double the notice, and some even longer period where the body has ample time to react no matter the starting load. It also fits the immune response time relatively well: the short term response of IgM antibodies takes around a week, so diseases that took around 1-3 weeks of progression would be right in the sweet spot of getting substantially more exponential response from your immune system from advance notice of a few doublings (several days of viral growth).
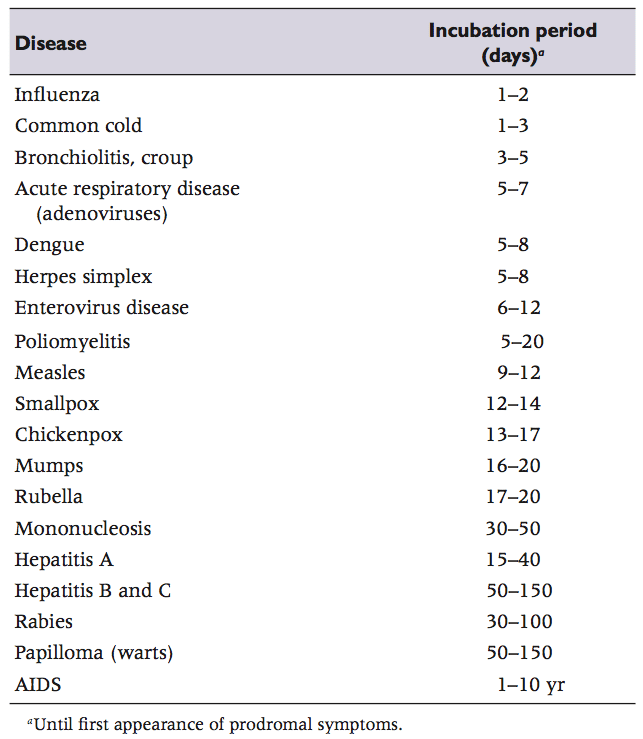
The one countervailing consideration is that the incubation periods for a lot of diseases are a bit longer than I had thought. I can't tell if this is an artifact of them including outliers rather than just the middle 95% or something. But it still seems like the difference between a 4-day and 10-day incubation period could explain why viral load doesn't matter much in most diseases. It also suggests that chickenpox, rubeola, rubella, whooping cough, and mumps are good places to look for outcome dependence on initial viral load.
Replies from: leggi↑ comment by leggi · 2020-04-07T07:16:08.593Z · LW(p) · GW(p)
COVID and smallpox is their long incubation times, which isn't shared by something like 95% of current ambient disease
I'm not sure what current ambient disease means.
Where do you get the figure of 95% from?
If you're talking about "colds and flu" then yes they do have short incubation times but many other viruses have long incubation times for example HIV, hepatitis causing viruses
https://www.virology.ws/wp-content/uploads/2014/10/Screenshot-2014-10-07-13.18.17.png
{kind=link}
Some figures for incubation periods for various diseases:
Replies from: Connor_Flexman↑ comment by Connor_Flexman · 2020-04-07T17:51:22.893Z · LW(p) · GW(p)
The second link was meant to be to incubation times, now fixed.
I meant ~95% of the times you become sick, i.e. mostly "colds and flus".
comment by Rob Bensinger (RobbBB) · 2020-04-01T17:12:35.235Z · LW(p) · GW(p)
Rob Wiblin: "A problem with healthcare workers is they're going to be run off their feet, lacking sleep, etc. That could worsen outcomes. They are also at higher risk of being exposed to multiple pathogens simultaneously (e.g. get COVID and flu from patients the same day)."
comment by avturchin · 2020-04-01T18:40:57.529Z · LW(p) · GW(p)
Any animal data on small viral loads effects?
Replies from: leggi↑ comment by leggi · 2020-04-01T21:17:59.666Z · LW(p) · GW(p)
viral titer/titre is the technical term for "viral load" so would be more useful if looking for studies.
2 human studies I've quickly found....
Assessment of correlation between serum titers of hepatitis c virus and severity of liver disease
Dengue Viremia Titer, Antibody Response Pattern, and Virus Serotype Correlate with Disease Severity
comment by Bundle_Gerbe · 2020-04-02T22:24:34.192Z · LW(p) · GW(p)
We have to ask why smallpox was a unique event, and we never used this method for any other virus. Did we even ever consider it?
There are two strains of smallpox, one of which is much less deadly than the other. People practicing variolation tended to use variolous material from a mild cases, including those successfully variolated. Some of the success of smallpox variolation was probably due to this practice and the resulting tendency for the inoculations to contain variola minor.
comment by Vaniver · 2020-04-02T01:21:50.203Z · LW(p) · GW(p)
The biggest change that this suggests, I believe, is that people should not isolate with their families if they become sick. (Basically for the same reason that the first kid with measles is ok, but their siblings are in trouble.)
The 'temporary hospitals', where someone with COVID goes there to recover and hopefully doesn't infect anyone else (or get too much additional virus from the other patients), seem like they get around this.
comment by Decius · 2020-04-12T08:05:11.276Z · LW(p) · GW(p)
I'll just note that the implied course of action is to send a bunch of immunocompromised people out on lots of cruise ships with known infected individuals to compare their death rates in different circumstances, to try to determine IF variolation and low viral load benefit those groups.
If you can't see why someone would have ethical concerns about that, I think you should perform a full stop on anything that is critically important until you can at least understand the ethical objections (even if you disagree with them and think that the sacrifice is worthwhile and also think that you can get volunteers without coercion of any kind existing).
comment by habryka (habryka4) · 2020-04-02T19:32:03.871Z · LW(p) · GW(p)
Promoted to curated: I generally want to make sure to not spam all of our curated posts with coronavirus related stuff, but this post is good enough to add to our current curation list. I think it analyzes a really important consideration, that has pretty direct implications for many people reading LessWrong, and does so in a transparent and understandable way.
I expect there are probably quite a few errors in this analysis, just because that's how it goes when people try to write things like this quickly and without a lot of domain expertise, but I am pretty confident the overall point is at the very least important to consider.
comment by jacob_cannell · 2020-04-01T20:31:34.241Z · LW(p) · GW(p)
The first is that we have a strong mechanism story we can tell. Viruses take time to multiply. When the immune system detects a virus it responds. If your initial viral load is low your immune system gets a head start, so you do better.
The problem with this story is that it assumes that immune system detection time is not dependent on viral load, which seems highly unlikely. The more viral particles, the more likely they will be detected. How that interacts with viral load's more obvious direct effects is complex and probably virus strain dependent.
The second category is the terrible outcomes in health care workers on the front lines. Those who are dealing with the crisis first hand are dealing with lots of intense exposures to the virus. When they do catch it, they are experiencing high death rates.
Evidence/source?
Your third category on analogy evidence from other viruses makes sense, with the single example from the other SARS coronavirus carrying more weight as it's a much closer relation than smallpox or measles.
comment by Raemon · 2021-12-04T23:56:43.318Z · LW(p) · GW(p)
I haven't followed the covid discourse that'd indicate whether this post's ideas turned out to make sense. But, I really appreciated how this post went about investigating its model, and explored the IF-THEN ramifications of that investigation.
I like how it broke down "how does one take this hypothesis seriously?", i.e:
- There are things we could do to get better information.
- There are things individuals or small groups can do to improve their situation.
- There are things society as a whole could try to do that don’t have big downsides.
- We could take bold action, potentially including variolation.
I like how it highlighted a really key failure of "man, we really should be doing better science and gathering more data here", as well as discussing how this hypothesis might have some pretty counterintuitive implications (i.e. maybe old people should be making themselves more exposed), while being sensible about what sort of steps would make sense for actually taking that sort of bold action.
I'd appreciate a more in-depth review by someone can review both our current state of the knowledge about the initial-viral-load hypothesis, as well as some review of whether all the logical inferences here made sense at the time.
comment by Elizabeth (pktechgirl) · 2020-04-09T23:25:16.518Z · LW(p) · GW(p)
I think 30X for initial viral load might be too high, because it's comparing symptomatic cases of smallpox to all cases of smallpox. The fair thing is to compare variolation against everyone who was exposed to smallpox, whether they developed symptoms or not.
Internet seems divided on whether or not subclinical smallpox even exists, so this probably isn't a very large factor. I write it out mostly so if someone else has the same idea they don't have to duplicate work.
comment by Lucent · 2020-04-02T17:31:10.472Z · LW(p) · GW(p)
Is it possible we already have a lot of information about the impact of viral load and just don't realize it? Ever since we switched to agriculture and civilization, the human population has had a large fraction wiped out dozens of times. I don't think we're descendants of merely lucky or biologically "sturdy" people, but of people whose behaviors optimized viral load or had personality traits that helped them avoid it entirely.
Could we be looking at two distinct, competing behaviors which help survival that have evolved out of the ashes of the plagues that devastated humanity? One may be mysophobia/OCD, a behavior pattern about things we cannot see. If this trait has a large hereditary component, that would be strong evidence of why it came about.
The competing strategy may be deliberately attempting to introduce a small viral load frequently to avoid a large load from something like a sneeze to the face. Based on the quantity of recent memes lamenting difficulty in not touching one's face, perhaps there's a genetic component to it. It seems like a stretch to suggest a face-touching gene, but with how many droplet contagious diseases have killed so many of us, one would think it would be selected against by now if it didn't have some redemptive factor.
I'd be most convinced if population modeling showed mysophobia and frequent face-touching were rarely traits that occurred in the same person, suggesting they were opposing strategies, an attempt to avoid exposure entirely and an attempt to deliberately take on a small exposure. Would a combination of both traits compromise survival? Do people at different ages have differing severity of mysophobia or face-touching corresponding to their immune system strength? Does the quantity of each trait in comparison to its population density or type of historical plague correlate strongly enough to these traits to draw any conclusions?
Are we saying "don't touch your face" to people who've specifically evolved to do just that because it got their ancestors through dozens of plagues?
comment by ChristianKl · 2020-04-01T18:12:16.986Z · LW(p) · GW(p)
We have to ask why smallpox was a unique event, and we never used this method for any other virus. Did we even ever consider it?
If you can give someone immunity by giving them a small smallpox infection the logical next step is to give them dead smallpox virus that's enough to get an immune reaction to produce immunity but that in most cases won't produce infection. That's the crudest form to do vaccination.
I see no reason why you would want to give a patient living smallpox virus over giving them dead smallpox virus if you have a decent amount of resources. The same goes for other viruses.
Policy-wise it might make more sense in third-world countries where you have neither the resources to self-quarenteen people nor to give everybody dea smallpox virus as a vaccine.
comment by leggi · 2020-04-01T15:31:36.502Z · LW(p) · GW(p)
Question - why is the term variolation being used?
Unless I am very much mistaken variolation is specific to smallpox.
Edited to add. I am not mistaken, I was just trying to be polite in some ill-attempt not to get voted down so quickly and hidden out of sight, but since that didn't work:
THE USAGE OF THE TERM "VARIOLATION" IN THIS SITUATION SHOWS A DISTINCT LACK OF UNDERSTANDING OF WHAT THE WORD MEANS.
Shockingly poor practice IMO. I find it disappointing at how readily it's been accepted, repeated and defended without any apparent thought.
EDITED TO ADD INFORMATION I'VE PUT IN OTHER COMMENTS:
using a live (unmodified) virus to stimulate immunity is still a VACCINATION.
with a"live vaccine"
Different routes of administration have also got names.
by scratch is known as
"scarification" , or "percutaneous vaccination" or "scratch vaccination"
other routes of vaccine administration include:
intranasal, intraocular, intramuscular, subcuteneous , intraperitoneal, oral, sublingual ...
Using variolation exposes the lack of basic medical/immunological knowledge of the author/s.
IF lesswrong wants to be taken seriously on this subject using the correct terminology would help significantly.
My comments are of no benefit to me - they are for lesswrong.
And down-votes are not going to stop me wanting to help, but do provide some amusement at the rat-reactions to being challenged.
Replies from: kevinpet, orthonormal↑ comment by kevinpet · 2020-04-07T05:42:24.677Z · LW(p) · GW(p)
Words are used to convey meaning. No one who has read more than a sentence on this topic thinks that Robin and Zvi are proposing the use of dried scabs. Vaccination is a word in common use for all diseases despite originally referring specifically to inoculation by cowpox ('vacca' = 'cow'). And it has a highly relevant parallel twin that refers specifically to the inoculation by the live dangerous virus, variolation.
Replies from: leggi↑ comment by leggi · 2020-04-07T07:05:33.708Z · LW(p) · GW(p)
I've edited the post you answered to include stuff I've posted in other comments.
Words are used to convey meaning.
I totally agree. Which is why I've been pushing the point that the meaning of variolation is not what people here seem to accept it as.
Vaccination is a word in common use for all diseases
Indeed. And it's the word that should be used here.
A starting point for increasing knowledge of the subject: live-vaccines (edit to add: not a good link for differentiating between true live and live attenuated/modified vaccines, my mistake.)
highly relevant parallel twin that refers specifically to the inoculation by the live dangerous virus, variolation.
NO.
Using a live virus is a known as a "live virus vaccination".
Can you find ANY evidence that variolation is an acceptable term for any disease other than smallpox?
Replies from: kevinpet↑ comment by kevinpet · 2020-04-08T09:16:26.320Z · LW(p) · GW(p)
No it isn’t. Quoting your own source “ Live vaccines contain a weakened or attenuated form of a virus or bacteria.”. That is not what is suggested here.
Intentional infection through controlled means with the contagious virus hasn’t been used since Smallpox (as opposed to pox parties). There is no accepted term. The meaning was immediately clear to me on first reading it. It appears to be a successful reintroduction if a word for an analogous purpose. It’s even unique enough to be googleable.
Replies from: leggi↑ comment by leggi · 2020-04-08T12:06:30.841Z · LW(p) · GW(p)
A true "live vaccine" is different from "live-attenuated" vaccine. (you're right re the link, it doesn't make the differentiation clear and is poor referencing on my part.)
Due to the increased risks of "live vaccines" (and the ability to attenuate the infective agent in the majority of cases) they are rare but they do exist and are the subject of research.
For example:
Used for military personnel: Adenovirus vaccine contains live adenovirus
adenovirus type 4 and type 7 vaccine, live
Adenovirus Type 4 and Type 7 Vaccine, Live, Oral contains live viruses that are shed in the stool and can cause disease if transmitted.
The virus strains have not been attenuated. (in section 11 DESCRIPTION)
and:
A Study to Assess the Safety of Live Intranasal Sendai Virus Vaccine in Children and Toddlers
a live, unmodified intranasally administered Sendai virus vaccine
(for "croup" rather than disease caused by sendai virus)
Using a live unattenuated dose of COVID to stimulate immunity would fall into the live vaccination category.
↑ comment by orthonormal · 2020-04-02T20:45:34.318Z · LW(p) · GW(p)
Robin Hanson started it. [EDIT: he wasn't the first; see FactorialCode's reply.]
Replies from: FactorialCode, leggi↑ comment by FactorialCode · 2020-04-05T17:17:47.954Z · LW(p) · GW(p)
No he didn't. The idea and terminology has been bouncing around the rat-sphere a bit earlier than that. [LW · GW]
Replies from: leggi↑ comment by leggi · 2020-04-05T18:53:48.612Z · LW(p) · GW(p)
Thanks for that info.
It makes a bit more sense why "variolation" is the term being knocked around since the post refers to giving the vaccination by scratching the skin but variolation shouldn't be used when talking about viruses other than smallpox.
This method of administration is known as:
"scarification vaccination" or "percutaneous vaccine"
↑ comment by leggi · 2020-04-03T08:47:53.834Z · LW(p) · GW(p)
Thank you for replying and for the link.
To quote the article by Robin Hanson:
" Variolation is an inoculation technique whereby a scab or pus from an individual with a mild smallpox infection is introduced into the nose or mouth of healthy individuals."
Which is missing some key points about variolation. wikipedia.org/wiki/Variolation
Firstly to expand on the definition Robin used:
The Chinese practiced the oldest documented use of variolation, dating back to the fifteenth century.
According to such documentation, mild smallpox cases were selected as donors in order to prevent serious attack. The technique used scabs that had been left to dry out for some time. Fresh scabs were more likely to lead to a full-blown infection. Three or four scabs were ground into powder or mixed with a grain of musk and bound in cotton. Infected material was then packed into a pipe and puffed up the patient's nostril.
Variolation is usually thought of in the (English-speaking) medical world as:
The procedure was most commonly carried out by inserting/rubbing powdered smallpox scabs or fluid from pustules into superficial scratches made in the skin.
Variolation is about smallpox. A term that should not be applied to covid19 or any other virus/disease.
What Robin describes as "deliberate low dose infection" is the process of vaccination using a live virus (as apposed to live-attenuated or dead virus vaccine).
comment by Sammy Martin (SDM) · 2020-04-03T18:20:17.459Z · LW(p) · GW(p)
How much is the data we're currently working off of influenced by high/low viral load effects? This table from Imperial college seems to contain the hospitalisation risk estimates by age that everyone has converged on: https://mobile.twitter.com/anderssandberg/status/1239923496916058112.
The data is based on adjusted results from Wuhan which would suggest... what? I would think that under Lockdown conditions you would get more in home infections? Perhaps we are working with estimates of hospitalisation risk that already account for a large fraction of cases being high viral dose.
If there's a really really large difference between high and low viral dose risk, but only half the exposure in Wuhan was high dose (as in the OPs example) , then as a rough approximation you should multiply those risks by 2 if you're high dosed.
Second, one of Rob Wiblin's sources suggested that the dominant effect might not be at home vs outside but a virtuous or vicious circle - severe illnesses release more virus and are more likely to provoke severe illness in the same household, while mild illness provokes mild illness: https://m.facebook.com/story.php?story_fbid=887350766835&id=204401235&anchor_composer=false#
That story could fit some of the data we've seen, especially doctors and care homes, but imply groups of young healthy people have much less to fear, as they just expose each other to mild or asymptomatic illness and don't make each other much sicker.
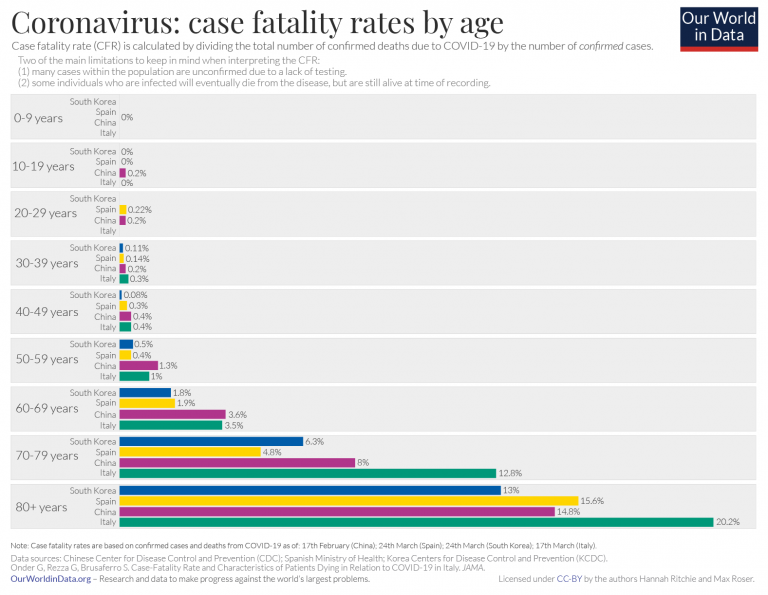
Hanson argued that viral load before and after Lockdown was the main factor affecting differing fatality rates between countries and I agree with the OP that this probably isn't the case. As additional evidence, we can see that the death rates for under 50s seem to be more consistent between countries than those over 50, https://ourworldindata.org/uploads/2020/03/COVID-CFR-by-age-768x595.png. That's harder to fit with the viral load story, unless we assume older people are more sensitive to differences in viral load
{kind=link}
comment by jimmy · 2020-04-01T23:59:37.871Z · LW(p) · GW(p)
Looking at a 50% low risk, 50% high risk scenario, we can only save 50% of what we could save if we started in a 50% high risk scenario.
I don’t think this is right.
It’s worth noting that the 14x difference between the risk for the first kid in the house and the second is a (noisy) lower bound on the degree to which the risk depends on dose. For example, this data is consistent with the toy model that the risk vs dose is a step function going from 0% to 100% at a certain point; it would just require that the kid bringing the disease into the house is 14x less likely to have crossed that threshold. With intentional inoculation we don’t know how much lower the risk can be driven, nor do we know how much of the exceptionally bad cases are simply due to exceptionally high initial dose of the virus. It’s entirely possible that even in your “50% low risk 50% high risk” scenario, all or most of the low risk people that die are because of unusually high viral loads given their risk grouping, and that with careful titration of dosage we can do much better than shifting people from one crude grouping to another.
I’m also quite skeptical that we should find the absence of more evidence to be particularly damning. Where would it come from? Ethics boards aren’t going to be happy about intentionally infecting people with deadly diseases, and it’s hard to get more than a very crude guess at the initial dose of cases caught “in the wild”. Furthermore, if you’re going to intentionally inject people with non-potent virus in order to build antibodies, you’d normally want to go all the way and do an actual vaccine. How many people have been thinking about what to do in case there’s a pandemic where you can’t wait for a real vaccine, and how many of them have been studying variolation? I wouldn’t think many.
To me, it sounds like taking volunteers to empty cruise ships sounds like an easy and potentially big win. There are plenty of young people who aren’t concerned and aren’t at high risk to begin with, and you can offer them both a lower risk (because they’re likely to get it anyway), a free party, and a way to feel like they’re helping instead of hurting other people. In return we get data, a step towards herd immunity, and workers which can safely treat other patients or run nursing homes. Once we need to scale up we can start thinking on how to triage people who are wanting to take this risk. For now, it seems like we just want to rush to get this idea accepted and tried somewhere.
comment by Andrew_Clough · 2020-04-04T15:48:17.325Z · LW(p) · GW(p)
From my understanding of how the learned immune response works an infection has to grow to a certain size before it really starts to kick in. That would tend to suggest that, if a dose is enough to cause an infection in the first place, danger will remain roughly constant up to some inflection point before starting to become less dangerous.
Of course as doses go down the chance that the innate immune system cleans it up or none of the viruses manage to find an ACE2 receptor goes up. But in those cases you won't be training the immune system.
comment by esamgood · 2020-04-04T05:32:02.056Z · LW(p) · GW(p)
"let’s presume that if anyone in a household gets infected, they are probably going to infect the rest of the household, and we’ll set that probability at 100%."
Curious what the logic was here to use 100% instead of doing our best to try and find what the household secondary attack rates have been. Below is a study from Mar 4th putting it at 15%
https://www.medrxiv.org/content/10.1101/2020.03.03.20028423v1.full.pdf (4 Mar, N=391, Shenzhen cases) Household secondary attack rate was 15%
Even if it was in the 30-40% ballpark, it seems like that would be enough to heavily weigh us towards recommending for younger people to take the task of grocery shopping, no?
Replies from: habryka4↑ comment by habryka (habryka4) · 2020-04-04T00:54:47.745Z · LW(p) · GW(p)
See this [LW · GW] for some commentary on that study (and others)
comment by K2msmith · 2020-04-03T05:24:35.181Z · LW(p) · GW(p)
If covid-19 can be fought with inoculation then aren't we much closer to developing a proper vaccine, which is a much safer approach to treating the population ? This is what happened with smallpox (over a longer time frame).
Replies from: ChristianKl↑ comment by ChristianKl · 2020-04-03T15:06:24.347Z · LW(p) · GW(p)
We have developed proper vaccines and are currently in the process of testing them.
comment by ike · 2020-04-02T16:12:52.139Z · LW(p) · GW(p)
https://www.nytimes.com/2020/04/01/opinion/coronavirus-viral-dose.html
Nice to get some of this into NYT
comment by jmh · 2020-04-01T17:43:23.983Z · LW(p) · GW(p)
I liked a lot of the suggestion and thoughts expresses.
The central issue though is data and I don't quite see a solution offered there other than we should be collecting and studying the larger set of data. But if getting that were simple the question then is why? If it really is "We just haven't thought of doing that in all the madness" should be simple to start moving that forward.
However I suspect that is not the right description of the situation. So perhaps a better starting point here might be to look at where the binding constraints (as John has so often pointed out to us) are and think about how to relax those constraints.
Clearly both activities, just recording and providing the additional information or identifying existing constraints limiting that effort, will include opportunity costs. But the opportunity costs for generating the data within the existing constraints versus identifying binding constraints that would allow the data to be more easily generated will likely be quite different. As such the relative payoff will be different with regard to the increased data I would think.
comment by Gurkenglas · 2020-04-01T15:03:49.740Z · LW(p) · GW(p)
Who knew that after all this time my grandmother would be right. Homeopathy is the answer.
Replies from: wizzwizz4↑ comment by wizzwizz4 · 2020-04-02T20:54:06.668Z · LW(p) · GW(p)
Don't dilute it that much, or it won't work. We should give this a name: “reduced-strength homeopathy”, maybe, or perhaps “variolation” (because it's a variant of homeopathy).
Oh hey, look, there's a Wikipedia article on Variolation:
The success of variolation led many, including medical professionals, to overlook its drawbacks. Variolation was practiced on the basis that it protected against smallpox for life, and was far less likely to kill than natural infection. In some cases however, natural smallpox or variolation failed to protect from a second attack. These cases were a result of a lapse of immune "memory", while others may have been misdiagnosed (experts often confused smallpox with chickenpox). Variolation also required a level of skill and attention to detail which some physicians lacked. Many physicians failed to take note of local redness and discharge to assure the variolation had taken, resulting in inadequate treatment. However, it was its great risk to others that led to the end of the practice. The collateral smallpox cases spread by variolated subjects shortly after variolation began to outweigh the benefits of the procedure.
Hmm… We'd have to be careful.
Replies from: Gurkenglas↑ comment by Gurkenglas · 2020-04-03T11:58:44.367Z · LW(p) · GW(p)
Well of course from a public perspective we should only do this if we expect everyone to contract it anyway. A straightforward way to avoid the danger of unilateralism is for each state to decide whether to recommend such measures as not being careful about touching things to the populace.