Covid 2/4: Safe and Effective Vaccines Aplenty
post by Zvi · 2021-02-04T14:50:01.552Z · LW · GW · 25 commentsContents
The Numbers Predictions Deaths Positive Tests Test Counts Covid Machine Learning Project Vaccinations Europe South African Strain English Strain The Pfizer and Moderna Vaccines The AstraZeneca Vaccine The Johnson & Johnson Vaccine The Novavax Vaccine The Russian Vaccine The Amazing Race Vaccine Allocation By Politics And Power Covid Tracking Project Calls It Quits Your Periodic Reminders (You Should Know This Already) We Can Still Agree: Andrew Cuomo Is The Worst In Other News None 25 comments
The vaccine data is in. It’s pretty great.
We now have six known safe and effective Covid-19 vaccines: Pfizer, Moderna, AstraZeneca, Novavax, Johnson & Johnson and Sputnik.
Pfizer and Moderna are amazingly safe and effective. They have been approved and are being distributed. The problem is that due to our unwillingness to properly fund the process of scaling up, we are stalling out at about 1.3 million doses per day for a population of 330+ million people each of whom needs two doses. That won’t do, the vaccine rollout is going about the way you would expect if you’ve been paying attention so far, and the English and other variant strains are rising fast.
The other vaccine approvals are not in. It’s pretty terrible.
Johnson & Johnson and Novavax are also safe and effective, far better than we need them to be. They both held onto their data longer than they would have in a sane world, and took longer to collect it than they would have in a sane world, but there’s nothing other than bureaucratic delays now standing in our way. Johnson & Johnson is expected to get its approval at some unspecified date, presumably this month. Yet there is no sense of urgency.
AstraZeneca is even more egregious. There are doses ready to go, it has been approved by major regulatory agencies elsewhere, and the main objections seem to be “the data isn’t from Americans” and “we’re mad at you about previous mistakes so we need to punish that somehow.” We are still going to wait until April or so for the American data, plus the delays after that, unless something changes and the new administration and/or the FDA see themselves as sufficiently blameworthy for not approving the vaccine. This badly needs more outrage. There’s an increasing amount, but so far it’s nowhere near enough.
Sputnik is the least egregious. Not using it is going to get a lot of people killed, but it’s a Russian project largely motivated by national pride, that never held out any hope of convincing us to trust it and always planned to distribute its doses in Russia and then the third world, so I can sort of understand this one. I’ll settle for the other five.
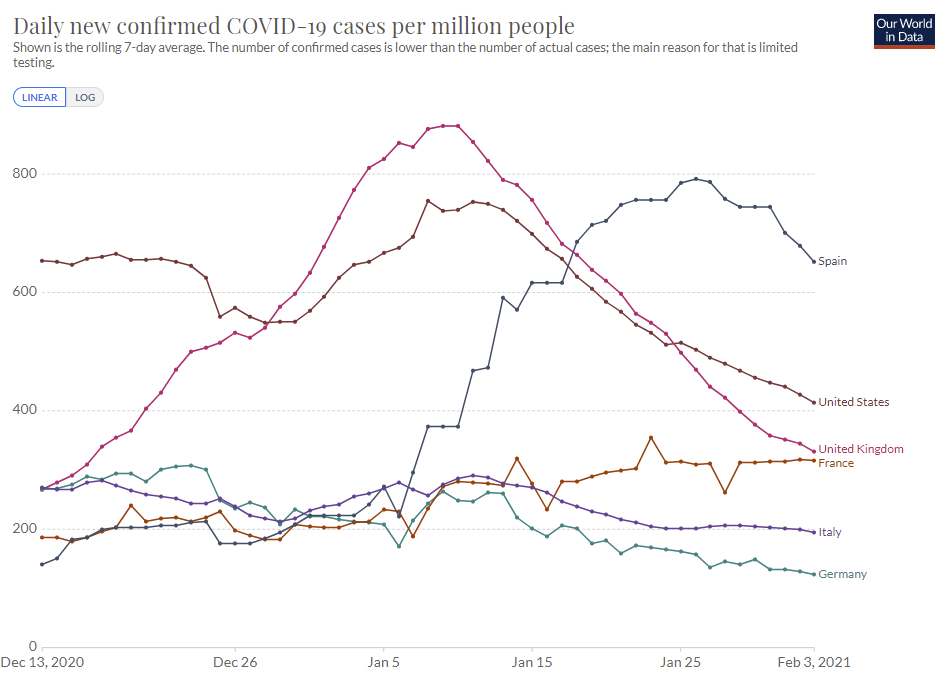
The short term situation is clearly headed in a positive direction. Death counts are being remarkably stubborn, but are on their way down along with hospitalizations, case counts and positive test percentages. By all metrics, every day we are a percent or two safer than the day before, with politicians hard at work to bring the control systems back online. The problem is that in the medium term, the English strain is coming fast and our current pace of vaccinations isn’t going to make much impact.
The news on those strains is very much not the best possible news. It looks like the English strain is more virulent than the old one, and also it seems to be picking up the mutations that allow the other new strains to partially escape immunity from previous infections. If we don’t get our act together quickly, things could turn quite ugly quite fast.
Things should still have a few weeks of improvement left before that next crisis hits us, but we’ll have to pick up the vaccination pace a lot if we want that next crisis to not happen or not be so bad. It’s likely going to be close.
We’ll also be losing the Covid Tracking Project soon. I hope that they’ll guide me to alternative data sources that do the job, but it could get considerably harder to stay on top of things.
Let’s run the numbers.
The Numbers
We have a complication. The Covid Tracking Project has changed the way their data is presented. This forces a choice between using a set of test percentages that is obviously too high, or one that is substantially lower than the one I previously thought was most accurate. I’ll be using the smaller numbers. Presumably this is a difference like counting somewhat duplicative tests instead of not counting them, but I’m not sure.
Thus, the numbers that use Covid Tracking Project need to be recalibrated. I’ve copied the old sheet so we still have it, but the new sheet backfills all data with the new numbers.
Also, I looked at the data downloads I used to use to calculate regional positive test percentages, and there’s enough uncertainty and missing data points that I don’t think it makes sense to try and fix it with the site going down in a month. I’ll keep an eye out for another source of that data that’s in reasonably nice form, if you know of one please drop a line in the comments.
In the meantime, one can rest assured that test percentages on the regional level are roughly moving with test counts, as the testing situation seems to have stabilized as far as I can tell. It’s fine to ignore this issue for a while, but I wouldn’t want to ignore it for months on end, so we’ll need a fix.
Predictions
Using the previous scale of test percentages:
Last Week’s Number: 11.9% positive rate on 11.3 million tests, and an average of 3,043 deaths.
Last Week’s Prediction: 10.5% positive rate and 2,900 deaths per day.
Using the new scale of test percentages:
Last Week’s Number: 8.8% positive rate on 12.8 million tests, and an average of 3,257 deaths.
Last Week’s Implied Prediction (using same ratios week over week): 7.8% positive rate and 3,103 deaths per day.
Results under the new system: 7.7% positive rate on 12.7 million tests, and an average of 3,041 deaths per day.
Thus, once you recalibrate, we are on the scheduled path.
Prediction for next week: 6.9% positive rate and an average of 2,750 deaths. Current trends should continue, with minimal impact yet from new strains, changed policies or increased vaccinations.
Deaths
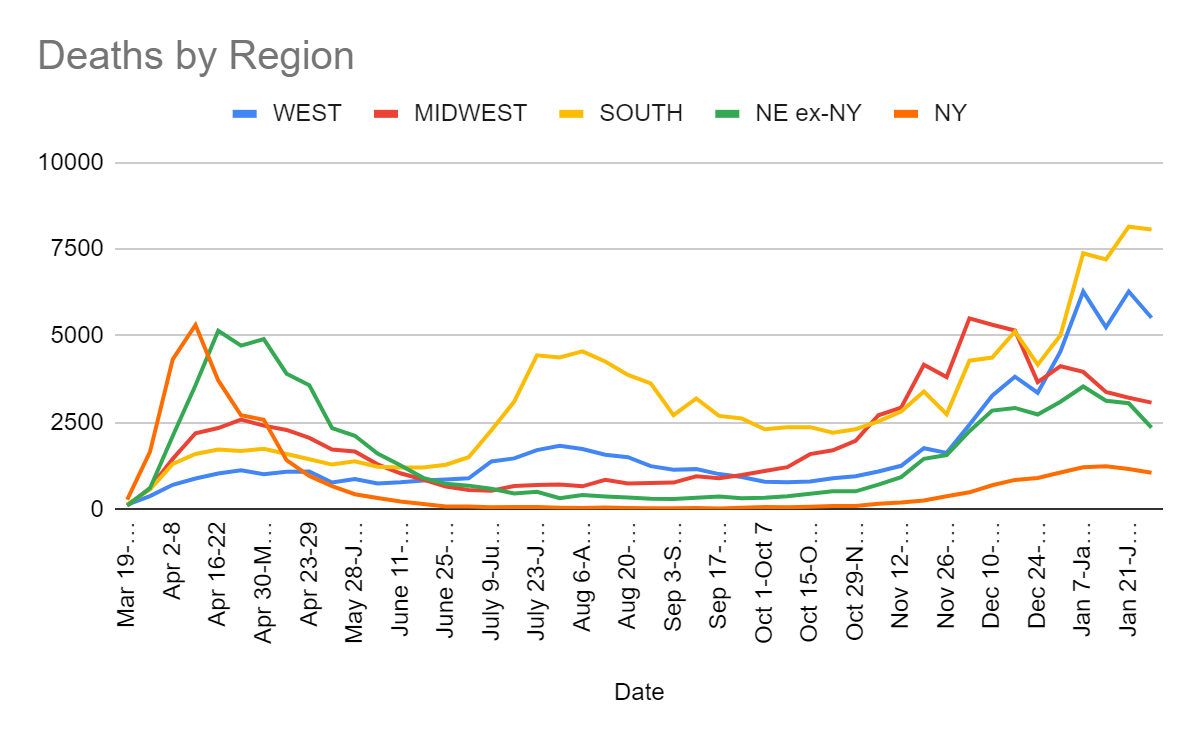
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
| Dec 17-Dec 23 | 3826 | 5158 | 5131 | 3772 |
| Dec 24-Dec 30 | 3363 | 3668 | 4171 | 3640 |
| Dec 31-Jan 6 | 4553 | 4127 | 5019 | 4162 |
| Jan 7-Jan 13 | 6280 | 3963 | 7383 | 4752 |
| Jan 14-Jan 20 | 5249 | 3386 | 7207 | 4370 |
| Jan 21-Jan 27 | 6281 | 3217 | 8151 | 4222 |
| Jan 28-Feb 4 | 5524 | 3078 | 8071 | 3410 |
There was quite the storm in the Northeast but I don’t think that was driving the drop in deaths that much but it likely contributed a little due to delayed reporting. Mostly I think this is all real and even the South has now peaked.
Positive Tests
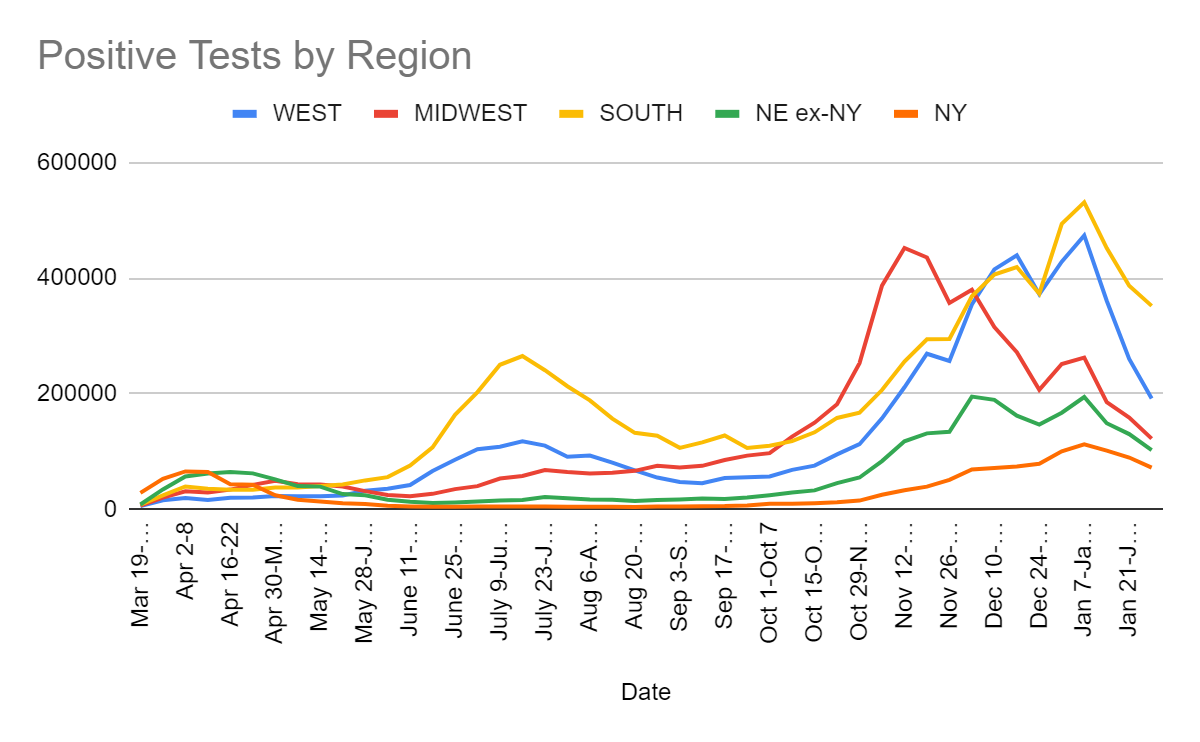
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Dec 17-Dec 23 | 439,493 | 271,825 | 419,230 | 236,264 |
| Dec 24-Dec 30 | 372,095 | 206,671 | 373,086 | 225,476 |
| Dec 31-Jan 6 | 428,407 | 251,443 | 494,090 | 267,350 |
| Jan 7-Jan 13 | 474,002 | 262,520 | 531,046 | 306,604 |
| Jan 14-Jan 20 | 360,874 | 185,412 | 452,092 | 250,439 |
| Jan 21-Jan 27 | 260,180 | 158,737 | 386,725 | 219,817 |
| Jan 28-Feb 3 | 191,804 | 122,259 | 352,018 | 174,569 |
We see clear improvement all around. One needs to remember that things remain at a very high level even with the drops so far, and will continue to do so for a while. It’s easy to mistake improvement for being at a good level, and we’re not at a good level. We should continue to see another few weeks of improvement along similar lines, at the end of which we still won’t be at comfortable overall levels, but it will be substantially better than now.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Dec 10-Dec 16 | 13,438,613 | 11.1% | 1,444,725 | 4.9% | 5.14% |
| Dec 17-Dec 23 | 13,363,172 | 11.1% | 1,440,770 | 5.1% | 5.60% |
| Dec 24-Dec 30 | 11,300,924 | 11.2% | 1,303,286 | 6.0% | 5.98% |
| Dec 31-Jan 6 | 11,649,640 | 13.3% | 1,365,473 | 7.3% | 6.45% |
| Jan 7-Jan 13 | 13,911,529 | 12.2% | 1,697,034 | 6.6% | 6.97% |
| Jan 14-Jan 20 | 14,005,720 | 9.7% | 1,721,440 | 5.9% | 7.39% |
| Jan 21-Jan 27 | 12,801,271 | 8.8% | 1,679,399 | 5.3% | 7.73% |
| Jan 28-Feb 3 | 12,257,123 | 7.7% | 1,557,550 | 4.6% | 8.02% |
Note the change in the old numbers, and recalibrate what the numbers mean going forward. This is good news, but it isn’t great news or as good as it looks, and it isn’t enough to overcome the new strain. Previously we measured the peak at 16.4%, now it’s being measured at 13.3%.
Covid Machine Learning Project

The model sees the control system kicking in and edging our R0 back up to 0.92 by January 20. It seems clear it’s still below 1, but not that much below 1. We see the stalling out of first vaccine doses, as the number of available doses is scaling up painfully slowly and more doses get diverted to second doses.
As of January 20 this sees 26.6% of the population as having been infected, up from 25.7% on January 13.
Vaccinations
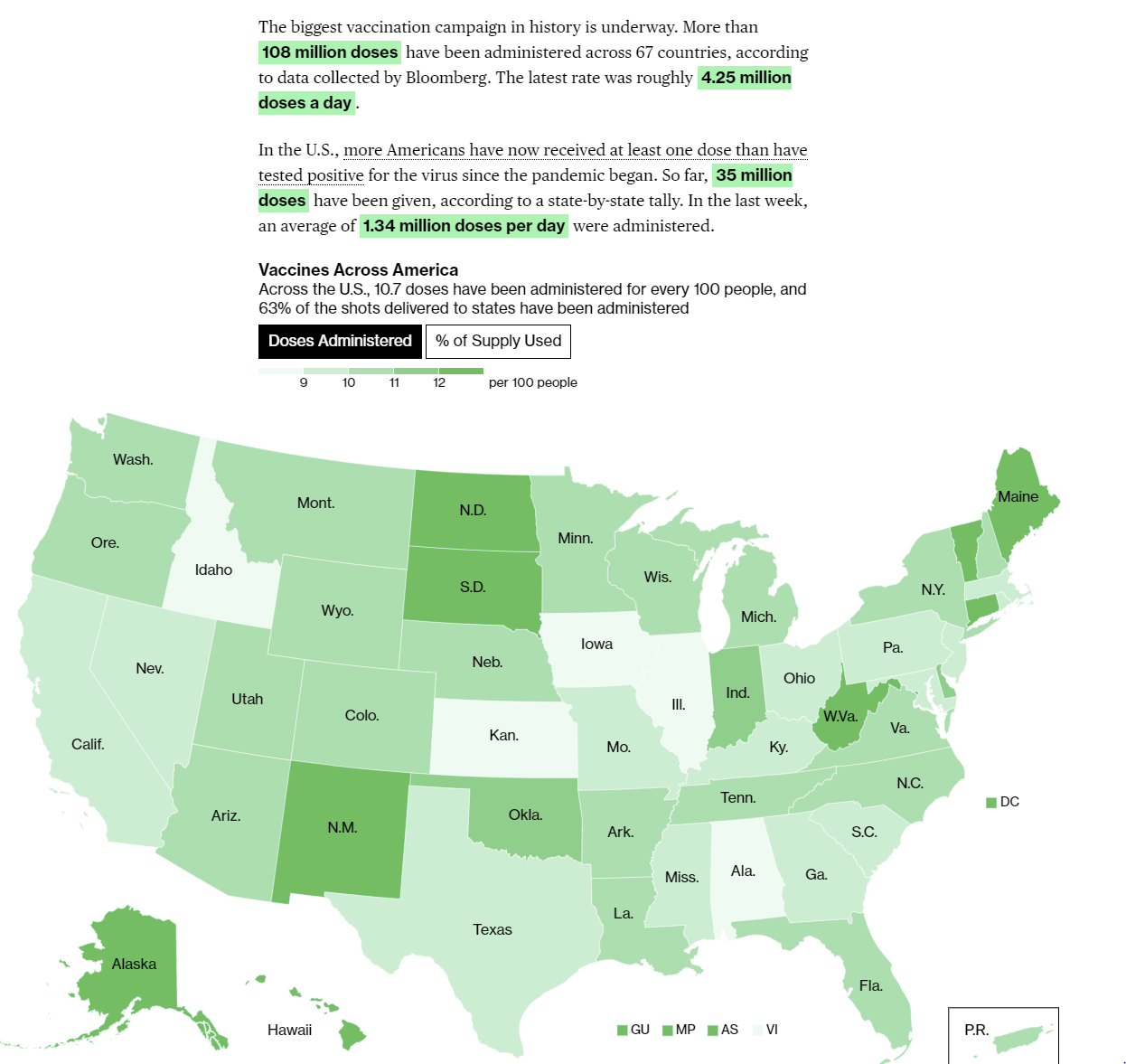
The average is up to 1.34 million doses per day versus 1.21 million doses per day last week, but the increase is in second doses many of which were held back in various places (despite instructions not to do this, I’m confident this was frequently ignored). Even worse, the averages have stalled out over the past few days. We should expect things to pick up in March and April for multiple reasons, but the near term outlook isn’t great.
Europe
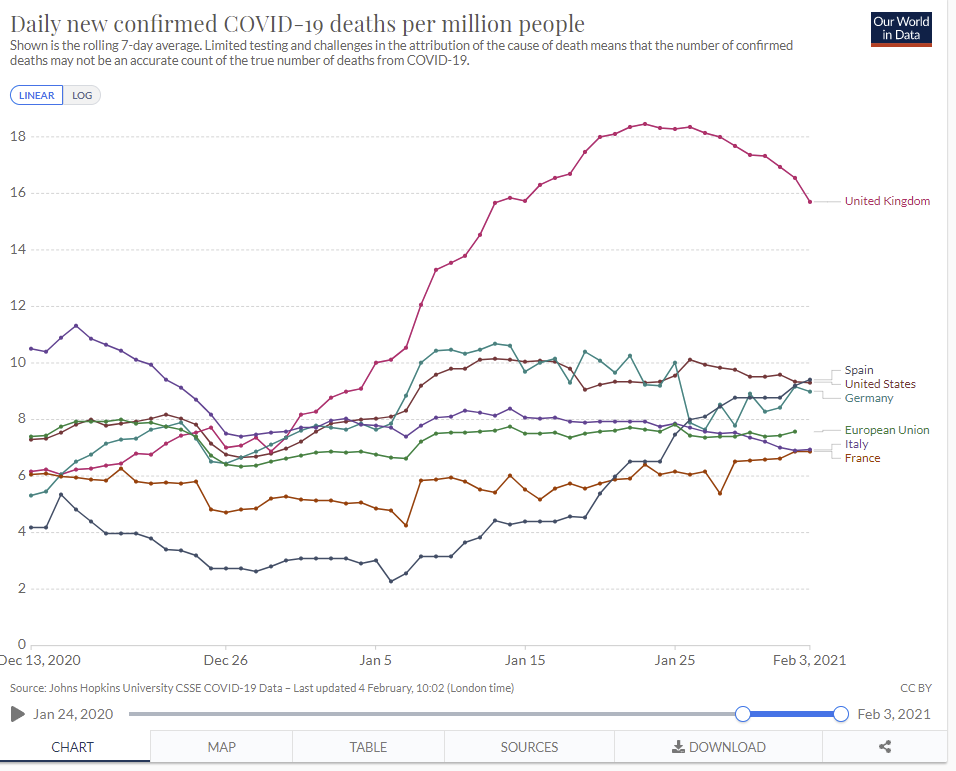
The United Kingdom’s case counts started declining on January 9, so we’re finally starting to see the corresponding improvement in deaths. Everything seems to be a continuation of previous trends.
South African Strain
It looks increasingly like the South African strain reduces, but does not eliminate, efficacy of vaccines and of previous infection. Here’s a thread discussing, which links to another few good threads as well. The Novavax vaccine’s effectiveness dropped off substantially but less than half, and we see similar results from Pfizer and Moderna.
Worth keeping in mind that in all these cases, effectiveness versus severe disease, hospitalization and death is higher than effectiveness against all reinfections.
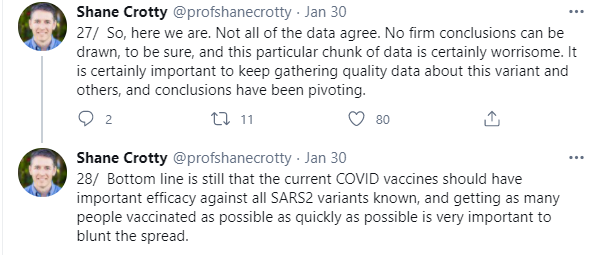
There were a lot of reinfections in the South African study. This thread does a good job going over the details but misses the obvious interpretation:




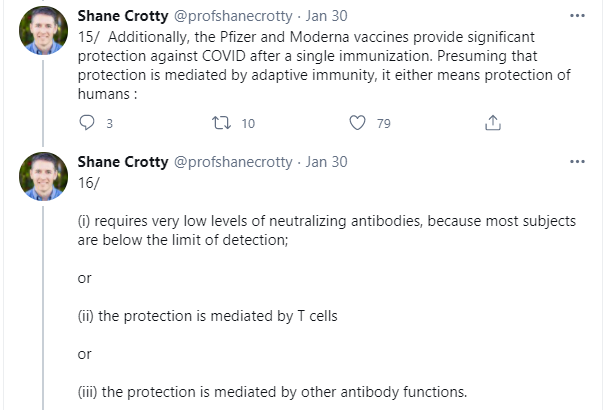
The obvious thing that Crotty is missing here, which I keep having to point out because everyone constantly ignores it, is that people do not get infected with Covid-19 at random. People get infected proportional to the amount of risk they take. The people who previously got Covid-19 both were previously taking more risk as a group, because that’s how they got infected, and also were likely taking even more risk now, because they had multiple reasons to think themselves relatively safe.
So if we get equal rates of infection between the previously infected and the previously not infected, that is entirely consistent with 50% protection. What we actually learned here is that the two effects likely have similar size. The chance of reinfection by the South African variant is roughly the same ratio as the risk profile of people who were previously infected versus previously not infected. If we can solve for one, we can solve for the other, which seems pretty exciting actually.
From Crotty’s thread, we know that from antibodies alone we might estimate 50% protection is retained against the SA strain from previous infections, but we also should expect mediation by T Cells and other methods, so we should expect more than 50% protection to remain. That also jives with any reasonable estimate of relative risk-taking, since both have to give the same answer. It would shock me if the ratio of risk between the infected and non-infected wasn’t more than 2:1.
One reasonable prior for the actual ratio is that the J&J vaccine’s relative effectiveness should apply. Thus, against symptomatic infection, we have 72% effective in America versus 57% effective in South Africa, for immunity being 79% as effective. That would imply somewhat under a 4:1 risk ratio for the infected versus non-infected (since they should match the asymptomatic risk ratio, which should show less effectiveness), which also makes sense to me and if anything seems a little low.
Also, the South African strain is here, and there’s community spread, identified in South Carolina (WaPo).
English Strain
More evidence that it’s more virulent, although the overall virulence on display here is not high:
Even worse, it looks like it’s acquiring the mutation from the South African strain, because that mutation is inevitable under current conditions…

In Denmark they have a lockdown that is rapidly bringing down cases, and thanks to frequent sequencing we know that it is almost good enough to stop the English Strain (B117) but not quite, with estimated R at 1.06, again Kai in this thread from this Science article. Given that it’s still the heart of winter and we can get help from more vaccinations, it seems like Denmark should be able to ‘win’ the endgame, but at the cost of months of additional hard lockdown.
The Pfizer and Moderna Vaccines
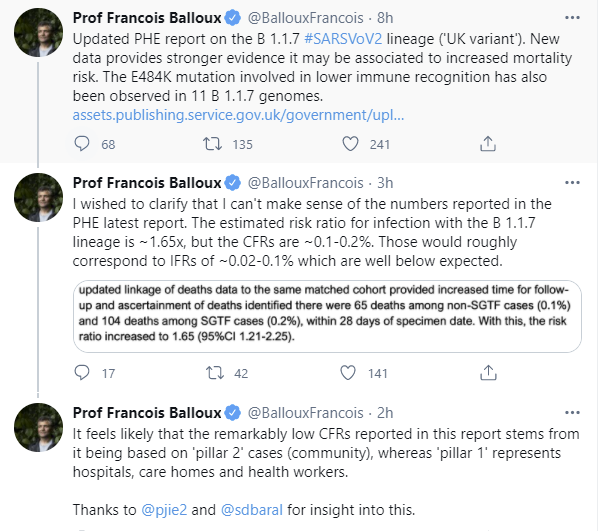
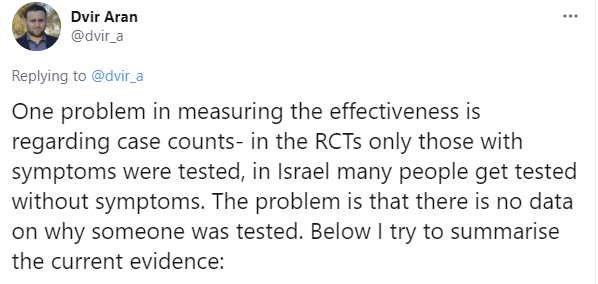
There’s more data coming out of Israel, because Israel collects data. It looks highly disappointing, likely because there’s a lot of asymptomatic cases being picked up, where effectiveness is lower, but also lots of confounding stuff going on in all directions:





There’s a big push by everyone, and I am no exception to this, to boil down the effectiveness of a vaccine to one number. It increasingly looks like it does not work that way. The vaccines are better thought of as being protective at each stage of the disease. Thus, they protect you from being infected, then if you are still infected they protect against symptoms, then against severity, then against hospitalization, then against death. You’re in a better position the whole way.
That means that you are personally very very protected from the worst outcomes and vaccinated people are going to be at minimal risk themselves, but their chance of being infected won’t improve as much. What about infecting others? That will be somewhere in the middle. All infections are not created equal, and any given infection of someone who was vaccinated is less likely to be symptomatic, and so almost certainly similarly less likely to be infectious slash likely to be less infectious, at any given time.
This does update me against acting as if fully vaccinated people don’t pose risk to not-yet-vaccinated others, so precautions in those situations look more sane, as does the case for continuing mask wearing and social distancing in general until things are suppressed. If all parties involved are vaccinated, that’s another story.
If you’re running out of vials in which to put your vaccine, you should put as much as possible into each vial, and also yes more money would have accelerated vaccine production and more money still could do so. Moderna is therefore asking the FDA permission to put more doses in the vials, which somehow they need to do, and also the answer wasn’t ‘yes of course do that I know technically you had to ask but this really, really isn’t a question.’ The contrast with Pfizer’s ‘I know you’re using that sixth dose so we don’t have to give you as much vaccine’ is rather stark.
We’ll get right on that request, Moderna!
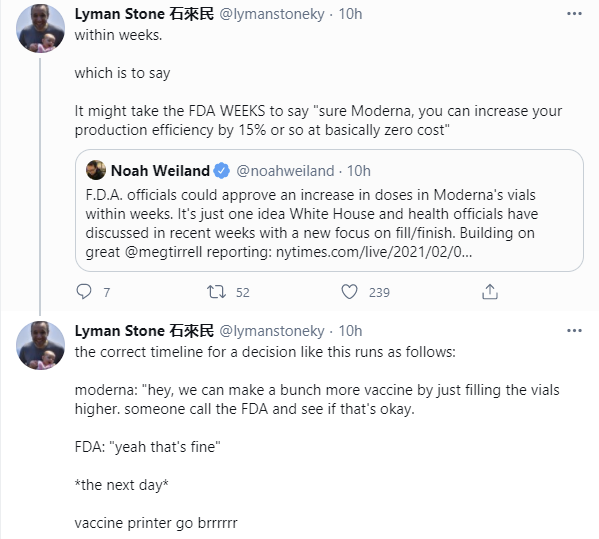
I think this is being too charitable. The correct timeline involves not having to check at all, and correct timeline where approval is necessary to avoid other stupid cases doesn’t waste the day confirming and you get a yes during the call. Also, note that this is saying the FDA could approve it within weeks, but also might not. We’re supposed to think this is fast and praiseworthy for literally ‘put more of the same liquid into the same vials.’ That’s the standards we’re judging ourselves against these days.
Also, this anecdote is not exactly comforting:
This is also food for thought:
The AstraZeneca Vaccine
At least Europe has approved the vaccine, even if they didn’t look at all the data, and took way too long to look at the data, while fighting in public about not getting their fair share for a vaccine they hadn’t even approved yet and which they delayed by months haggling over pennies, and with the potential hesitations to use it on people who need it most because ‘no evidence’ in older people.
But, seriously, good decision.
On the issue of pregnancy, they issue this stark warning:
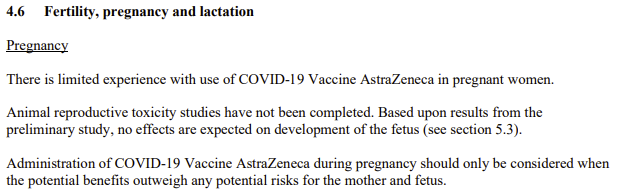
Yes, I agree. We should only consider doing things when the benefits outweigh the risks.
The benefits outweigh the risks.
Delaying the second dose appears to actively make the second dose more effective. Which is common for vaccines.
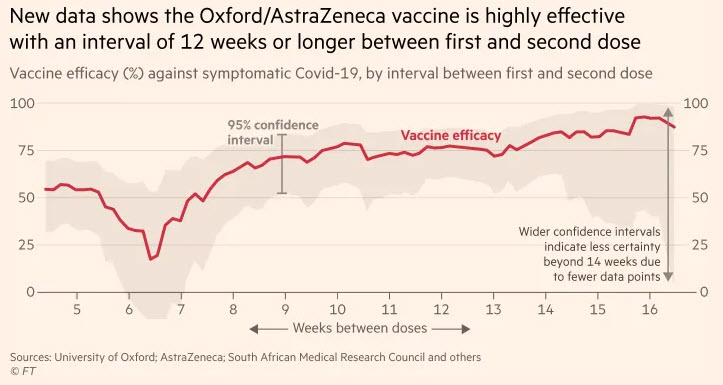
Thus, the admission that delaying it is ‘reasonable.’ If we were considering switching to faster second doses, rather than the other way around, ‘experts’ would consider it reckless and irresponsible.
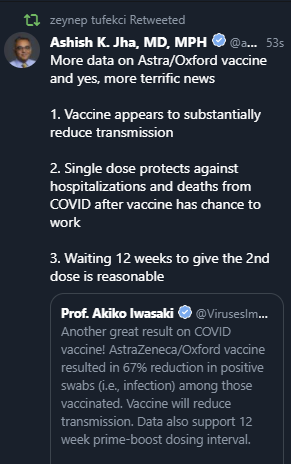
In the meantime, the single dose alone is 76% effective, presumably against symptomatic infection (WaPo) and was found to be 67% effective against further transmission. Because we need a study to generate headlines or quotes like these:


What the hell is up with the word “may” in these sentences, anyway? I’m pretty sure we don’t need a study to know that vaccines “may” prevent transmission.
Unless AstraZeneca is committing outright fraud, the data shows the AstraZeneca vaccine is safe and effective, and every day that we do not approve it will cost lives for no reason whatsoever.
AstraZeneca has not applied for emergency use authorization, because it has been told not to do so. If told to apply, they would doubtless quickly apply. Or you could of course approve it without an application. The regulatory norms were made for man, not man for the regulatory norms.
The good news is that the factory is running despite our failure to act. We are sitting on tens of millions of doses of a proven safe and effective vaccine. They’re sitting around in Baltimore waiting for approval.
How long it takes us to approve this vaccine is a major test of the Biden administration.
A test they have clearly already failed, and continue to fail. We must make it clear how unacceptable this is. The only way to give the people involved a path to doing the right thing is to let them point to how blameworthy they would be for not doing the right thing, within the next two weeks. To that extent, I am interested in assigning blame.
So I’m in favor of such true and culturally heartwarming summarizes as:
To that end, there’s even a planned protest at the FDA building to call for vaccine approvals. Whether or not anyone shows up or listens, it’s a great idea.
The Johnson & Johnson Vaccine
As always, every headline writer has a choice to make.
Option one is to point out that the Johnson & Johnson vaccine is inferior to the Pfizer and Moderna vaccines. One can say something based on “J&J Vaccine 66% Effective Against Moderate to Severe Covid-19.”

Which, while a hell of a lot better than 0%, is definitely not 95%. This sets up a deeply silly ‘should we approve it?’ debate and a (slightly less silly given you could potentially hold out for something better personally) ‘should you want this vaccine?’ debate. As a bonus, one gets to set up permanent fear, uncertainty and doubt, so you can demand indefinite Sacrifices to the Gods despite vaccinations.
Another option is to take sides and lead with the takeaway conclusion despite not understanding how good the J&J vaccine is, because a much worse version would still be good enough:

Or, you could go with something like this Bloomberg headline instead (twitter link, data):

Not only no deaths but also no hospitalizations in the treatment group is pretty great. If you get this vaccine and wait a month, you definitely have to worry that you might then infect other non-vaccinated people, but you do not have to worry about dying from Covid-19.
I’d pay a substantial amount to get Pfizer or Moderna instead of J&J if I could get either one today, but given the choice between waiting and taking what’s available, I will happily accept the J&J vaccine now rather than hold out for Pfizer or Moderna.
Thus, as something we can give to the whole population, as a one dose vaccine that only requires regular refrigeration and can be produced in massive quantities – J&J is promising 100 million doses by April and a billion within the year – this will do nicely.
It is worth noting that the one dose Johnson & Johnson vaccine shows similar benefits to the first shot from Pfizer or Moderna. The difference is that Pfizer and Moderna then give you a second shot.
Thus, Johnson & Johnson has done us the valuable service of not testing their vaccine with a second shot, thus allowing us to do First Doses First and get on with vaccinations twice as fast. If we decide later that we should double back and give a second shot to make it more effective, once we have sufficient supply, that’s great.
Given our current ‘medical ethics’ regime, it is important to test exactly those options that it would be good to enact, and to not test anything that else. Whenever you have another option, that option can create ethical obligations, and also choices are bad because they make you blameworthy for all opportunity costs. Better to only have the one good option.
Of course, if had turned out that J&J’s vaccine worked with a second shot but didn’t with only one shot, and we only tested one shot, that would have been quite bad. The good news is that early phase trials are very good at testing for antibody response, so we already knew the answers before we started the test.
The bad news of course is that thanks to the FDA, we (once again) had to wait for the test anyway, and then wait for the evaluation, which we are (once again) still waiting for, despite ‘hot damn look at this chart’ and meaningful side effects best described as ‘none whatsoever.’ Despite that, I’m writing this section on Sunday, and I would be shocked if I have to go back and edit it.
While we wait, the FDA is doing its usual thing of not releasing its information yet. It typically releases two days before the meeting.
Moderna scientist who worked on their vaccine agrees that J&J’s vaccine is ‘darn good’ and warns to let the perfect be the enemy of the good.
Eric Topol looks at the results and reaches similar conclusions, that J&J vaccine might have issues with continued asymptomatic transmission but offers great protection to the person vaccinated and is a ‘very effective’ vaccine.
Unless Johnson & Johnson is committing outright fraud, the data shows the Johnson & Johnson vaccine is safe and effective, and every day that we do not approve it will cost lives for no reason whatsoever.
How long it takes us to approve this vaccine is a major test of the Biden administration.
The Novavax Vaccine
Let’s not forget that there was another vaccine that came out with results this past week. Novavax was found to be 89.3% effective for preventing symptomatic Covid-19, which as we’ve learned presumably means less than that against asymptomatic Covid, but far more effective against hospitalization and death. A post-hoc analysis found 95.6% effective versus old variant and 85.6% effective versus the new strain, and there was only 60% efficacy against the South African strain in the South African leg of the study. It seems clear that the SA variant partially escapes, but does not fully escape.
Did anyone else notice that the South African leg’s headline was “90% of cases attributed to escape variant” to make people think about 90%, then in the non-bold print it mentions the 60% efficacy?
Alas, there is a major problem, which is that the study wasn’t conducted in the United States.
Therefore, they are ‘in talks’ with the FDA about asking for emergency use authorization, but it has yet to announce that it will even seek approval before its ‘Prevent-19’ American study is complete. But that study is still recruiting patients, so it’ll presumably be a few months, at which point the vaccine will be mostly unneeded here (but will still do a lot of good elsewhere). You see, last year the FDA graciously said that outside data could be submitted, but you need to talk to the FDA first on a case by case basis.
The lack of reciprocity in approvals between the US and UK/EU or other first world nations is senseless and costs lives and money and stifles innovation, but at least I understand it. You don’t want to trust your regulatory decisions to another country. Easy thing to get. But it’s worth periodically pointing out that this thing where we don’t have data reciprocity is completely insane.
First we mandate detailed three-step data collection. Then we ban any efficient method of data collection. Then we ban any method of data collection that isn’t done here in the United States, out of some bizarro FUD that Our Humans Are Different or something. Which sort of makes sense for Japan under normal circumstances, if you don’t do cost-benefit analysis, but enforcing it here on English data during a pandemic is something else.
Then, of course, we mandate where the vaccines are made. Even more vaccine nationalism.
Unless Novavax is committing outright fraud, the data shows the Novavax vaccine is safe and effective, and every day that we do not approve it will cost lives for no reason whatsoever.
How long it takes us to approve this vaccine is a major test of the Biden administration.
When we see an article called “Biden’s Latest Move Just Handed The Vaccine Market To These Two Companies” it should be about how they won’t approve anyone else’s vaccine, not about how Biden wisely is buying enough doses from those two companies alone to vaccinate everyone if necessary. We should do that several times over to be safe.
The Russian Vaccine
Beep. Beep. Sputnik works too. Data source here.
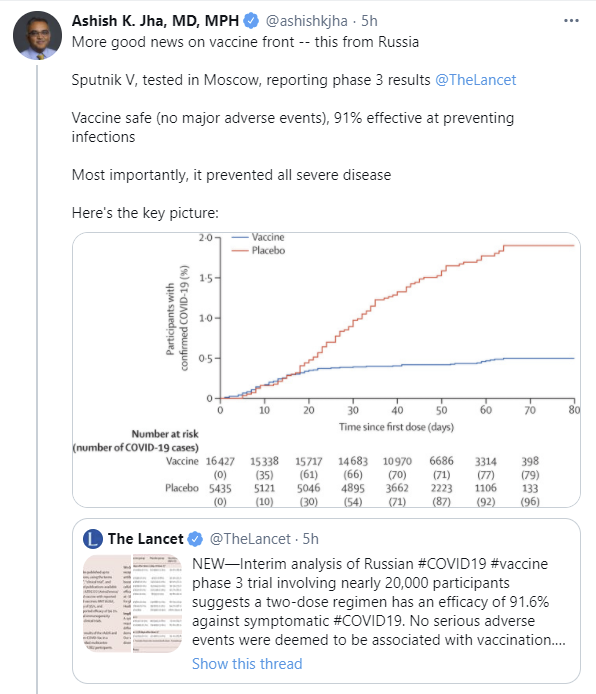
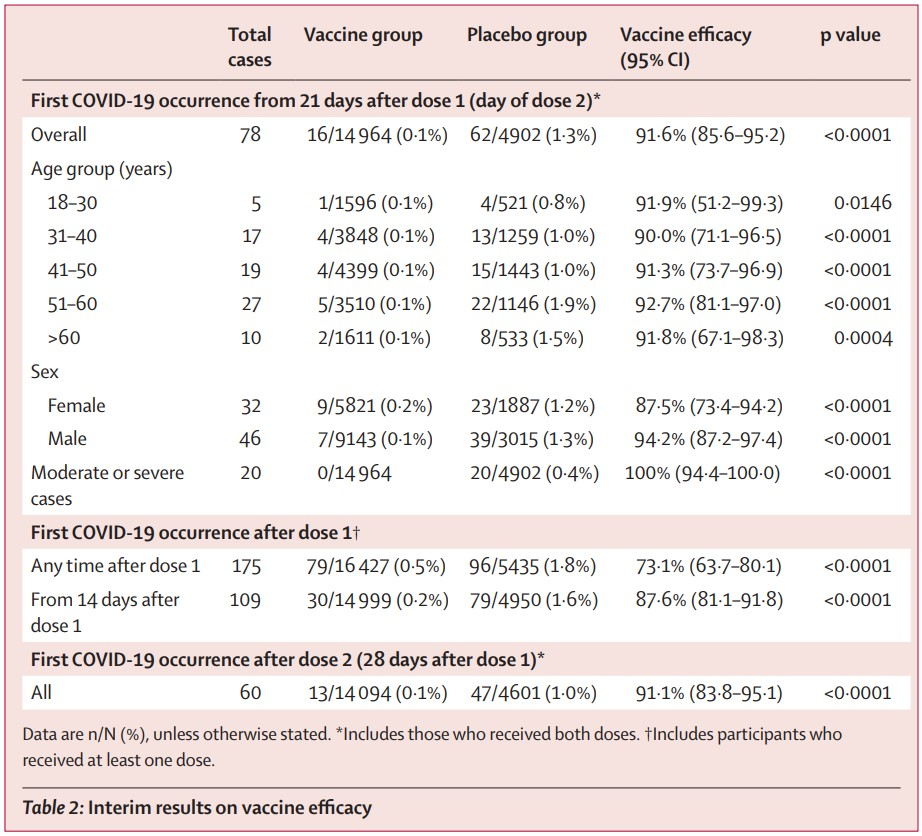
That chart sure looks familiar. 90%+ effective against detected infections (at this point, I expect effectiveness versus all infections to be somewhat lower, but for a bunch of asymptomatic and largely not so infectious infections to get missed and for those to be prevented less often, slash more infections are contained before they become detected.)
And once again, prevents all cases of severe disease. Nice.
There’s also a New Yorker article on Sputnik’s development.
That article explains that we must deny approval to this vaccine because the people involved did not Follow Proper Procedure, and therefore must be punished:
Don’t get me wrong. There are some details that are indeed rather suspicious, and some process decisions that are highly suspicious. Putin and company are highly, and highly suspiciously, motivated to show good results quickly. Timing in several cases seemed motivated by getting there first, or not being outdone, or modifying effectiveness to match others’ results; see the full post for details.
And suspicious one should therefore be. All of this must be verified. Which won’t happen, in part because given that we wouldn’t approve things anyway, they’re not about to give us that ability.
But also the author is completely correct on this:
That’s the test. Would you put it in your arm rather than do nothing? And if the answer here is no, then, please, show your work.
I’m fully aware of the reality that we’d never use a Russian vaccine no matter how good the evidence and likely neither will Europe, purely because it is Russian, but there’s nothing stopping us from doing so, and there being no chance of actually approving the vaccine (to the extent that there won’t be an application) doesn’t make the words any less true, so…
Unless the Russians are committing outright fraud, or there are side effects of which I’m unaware or that they are hiding (in this case, that caveat does seem necessary), the data shows the Sputnik vaccine is safe and effective, and every day that we do not approve it will cost lives for no reason whatsoever.
How long it takes us to approve this vaccine is a major test of the Biden administration.
The Amazing Race
We had another episode this week (WaPo), as a lucky late-night freezer failure in Seattle sent hundreds into a frenzy.
By morning, they’d used all their vaccine shots. It doesn’t always quite work out that way, but it is the default result, despite people not planning for such situations and engaging in what is clearly full improvisation.
For those who don’t think we’d get up in the middle of the night to get a vaccine shot, not only would we do that, some of us will get up in the middle of the night to look for an appointment for a vaccine shot:

Also, they want to make it clear that this is not the hospital’s fault, it’s our fault because everyone was ‘getting used to’ the requirements:
Overall, I strongly approve of the conclusion:

Except I would then, you know, have them implement it anyway.
Vaccine Allocation By Politics And Power
When you allocate by politics and power, you also allocate technological contracts and logistics the same way. Some places were so foolish they decided to use the CDC’s software to schedule appointments, that it paid $44 million to create. That turned out about as great as you’d expect.

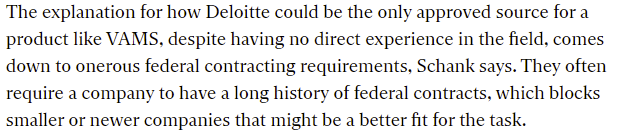
You see, there is only one company responsible enough (read: connected enough slash paying enough bribes) to be able to do this job:
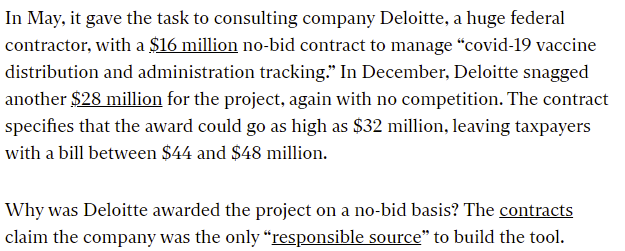
The whole article is full of failure, so kind of read the whole thing but also kind of no need.
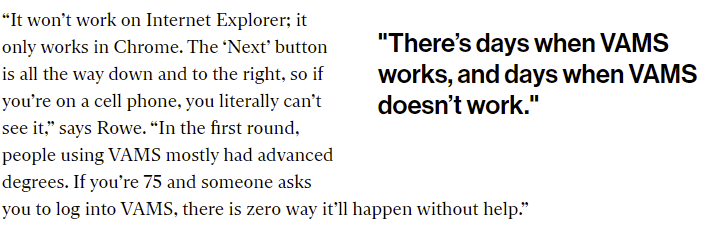

As usual, when something fails a lot of people, that is cited as an ‘equity’ concern rather than a ‘failing lots of people’ concern.
This is all business as usual. I’m not exactly surprised or outraged, but I want to make it clear that this is business as usual so maybe don’t give these people our business:

They let counties set their own additional requirements, on top of anything from the states.
Some counties decided to engage in vaccination nationalism, excluding anyone from outside the county, putting pressure on others to follow suit. There’s also outrage about people travelling within counties, such as between parts of Manhattan, where all vaccination sites are now scrambling to promise they’ll prioritize the way the powerful people want rather than by which eligible people attempt to get appointments.
There’s also the issue that counties in New York aren’t allowed to vaccinate seniors or anyone not on their particular priority list, even if those people are eligible. That’s a different department.
My grandparents are getting told that they can’t make appointments outside their county, but their own county allows outside appointments, so there aren’t any appointments available in their own county either. A prisoner’s dilemma that everyone saw coming.
This was the report this week from Arnold Kling:
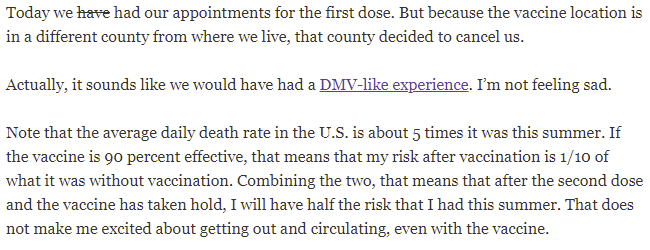
So little text, so many failures. First, we let him make the appointments, then we cancelled them over a spat between counties. I wonder how often such cancellations get replaced in time.
Then we managed to downsell the vaccine and botch the distribution and stories about distribution so much that he’s not even feeling sad about it. Let alone outraged. He’s under the impression that the vaccine is maybe 90% effective, when it’s 95% effective against symptomatic Covid, and more effective than that against hospitalization and death. But even relatively attention-paying people don’t realize.
Then there’s the story he linked to, about a Maryland couple waiting hours indoors on a line to get their shots. This is not par for the course, but it’s scary to even hear about, and given I haven’t heard that many vaccine stories, someone I read reporting back this way is a pretty bad sign.
If you don’t have the connections or savvy to get an appointment or on the approved lists, you try whatever you can think to do, which results in having to tell people to stop calling 911 for a vaccine appointment.
Or you can sit there clicking over and over, hoping for the best:
Or, if you’re a senior who lacks strong computer skills, you’re effectively out of luck and behind others who are at much less risk but who have the ability to navigate such problems.
Covid Tracking Project Calls It Quits
I’ve relied on them as my source of data all the way through, so it’s pretty scary to suddenly see this:
This was their post explaining their decision. At core, they say this is a government job, and now that the government will actually do it, they can stop. I wish I shared their confidence. They’ll be spending the next few weeks telling people like me where to go to find the data elsewhere, which hopefully will work out.
A big thank you to everyone involved in the project. You’ve been invaluable over this past year, and you’ve done it all on a volunteer basis. I’m sure it has cost many of you dearly, and I can’t be at all upset about the decision on finally hanging up the hat.
Still, if we can take up a collection and change the answer, I’m definitely up for contributing.
Your Periodic Reminders (You Should Know This Already)
The Pfizer and Moderna vaccines are super duper effective, in practice much more than 95%.
We should at most give those who already got infected one vaccine dose, for reasons that should be obvious. Now we have a study backing that up, for those who deny knowledge outside of studies can exist.
We should give Dolly Parton her vaccine shot. This waiting until other people to get it first despite being instrumental in funding the vaccine thing might seem noble but she’s 75 years old, and also people who are instrumental in funding the vaccine need to get first crack and if we don’t give them that then we really don’t deserve her. Especially if her shot in arm could help get people to accept the vaccine. What we actually deserve, it seems on every front, is a Super Bowl ad about having a gig economy side job for which she re-recorded her hit song as “working 5 to 9.” Therefore, that’s what we are going to get. Go Chiefs.
We should approve more vaccines and vaccinate more people faster (MR).
We should work to expand vaccine manufacturing capacity by spending more money (paper).
We should do human challenge trials and not doing so is a massive fail.
We should at least not let trivial issues massively slow down the world’s most important activity. From the New Yorker article on Sputnik, on how one incident cost us over a month on the only AZ trial the FDA will accept because it’s the only American one:
We should approve the Lilly antibody cocktail.
We should be doing more rapid testing and almost everyone arguing against them is either deeply confused about what matters and/or is arguing in bad faith. They work wonders. Also the arguments keep repeating and I don’t want to write the same thing each week.
We should consider that the FDA’s current actions are likely government in America at its theoretical best. Anything else you ask it to do, it will probably do worse than this.
We shouldn’t do what the link does and make our headlines and top cares about who is and isn’t blameworthy, but we totally should let Merck and anyone else without a working vaccine manufacture the approved vaccines. And put in large orders. If any of the original developers objects, pay them full price and also pay Merck full price. I really, really don’t care about that, any more than I care about who is to blame or whether they would have backed these proposals three months ago. And also they offer support for approving (and even better, for subsidizing) any and all rapid tests.
Not that it would be that easy. There’s a bottlenecked step, the creation of Lipid Nanoparticles (LNPs) for the mRNA vaccines, which the other companies can’t obviously help with. At least, not right away, but I’m betting they could help scale up, although you could also just pay Pfizer and Moderna more money. Also, this week we learned that Moderna literally is out of vials and is asking the FDA permission to fill them higher, and is waiting around for a few weeks on that, so yes a little help might be in order. As a fallback, the pharma companies whose candidates failed don’t need to produce the mRNA vaccines from Pfizer and Moderna, if they can’t do that, but I strongly suspect that if they had the right to produce the Oxford vaccine, or the Johnson & Johnson or Novavax vaccines, that would go rather smoothly, because that’s a more standardized process.
Then again, the person saying it cannot be done should never interrupt the person doing it:

You can go to a pharmacy or other location doing vaccinations, and offer to take a dose that’s going to be otherwise thrown away. Sometimes this works. The media and other Very Serious People, of course, will call you a ‘vaccine hunter’ and ‘line jumper’ who isn’t being ‘fair.’ What those people should have done, these experts say, is let those doses get thrown into the garbage. Much better, and you definitely totally shouldn’t get vaccinated with an otherwise-to-be-discarded dose, because that would be very unethical and inequitable, and that stuff matters so much more. You selfish bastard.
This was actually a case of a failure to zero out. Physicists tried to model everything that happened on campus, the distances between students, and dangers of each activity. They made an insanely complicated model, which they thought had room for error. The problem is that once your model tries to model something, if you miss any components or mess up any components, now you get the wrong answer. One ludicrously wrong input – in this case assuming everyone would follow the rules, despite everyone being college students – and your results are meaningless.
That’s why I try to stick to much simpler models that allow us to take into account the factors that we can’t model directly, by using inputs that incorporate those factors. It’s the only way. Even if they hadn’t made this particular dumb mistake, they doubtless had lots of other mistakes, and lots of other places where they had to guess because we banned experiments and don’t know the answer.
All the modeling efforts talked about in the write-up are doomed because they don’t understand the role of the control system, and I couldn’t bring myself to read the whole thing because it’s very long and boring.
Those taking mass transit need to wear masks. The CDC has now caught on and announced a mandate, and only about a year late and after the President signed an explicit executive order.
A reasonable case against Dr. Fauci. It is a good question what would have happened if he hadn’t tried to ‘handle’ Trump and instead spoken out using his authority in his field. The weird thing about this case is portraying Fauci as ‘truth teller who compromised to keep his job’ instead of ‘strategic liar who knows the truth, who compromised that approach to keep his job’ which I think is closer to accurate. Either way, there are reasonable arguments for and against Fauci’s tactical decisions.
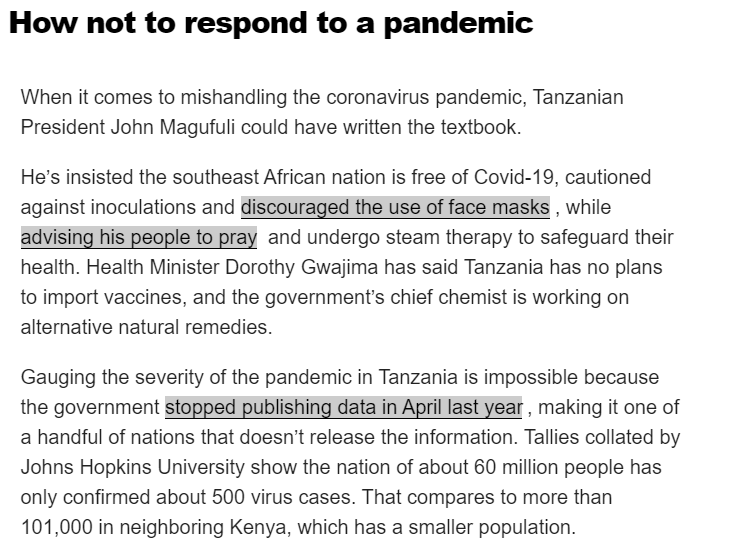
And finally, never forget that it can always, always, always get so much worse:

No, really, it can always get worse (from my Bloomberg daily Covid update email):
We Can Still Agree: Andrew Cuomo Is The Worst
Credit where credit is due, I don’t want to defend him either but it’s only fair, sometimes stopped clock successfully tells time, I don’t trust them either:
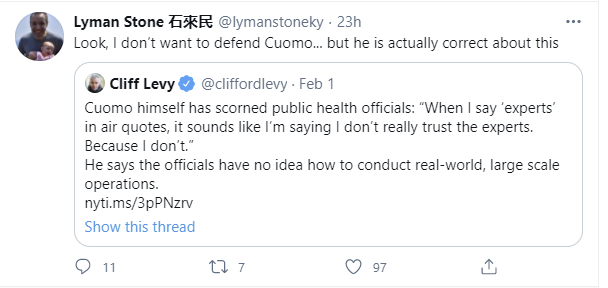
Then again, in practice this means he scorned the people explicitly in charge of planning distribution of a vaccine in exactly this situation, and instead improvised something new based on those closest to him on the fly (NYT so no link), which doesn’t seem like it would be expected to be better.
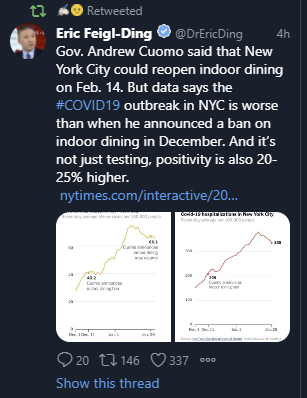
Cuomo is reopening indoor dining, despite conditions being worse than when he banned indoor dining, and there being a higher payoff to staying safe now than before due to vaccination progress, and despite the new variant coming soon that’s easier to transmit:
To justify this, he’s distorting data in a way that would shock even psychiatric researchers.
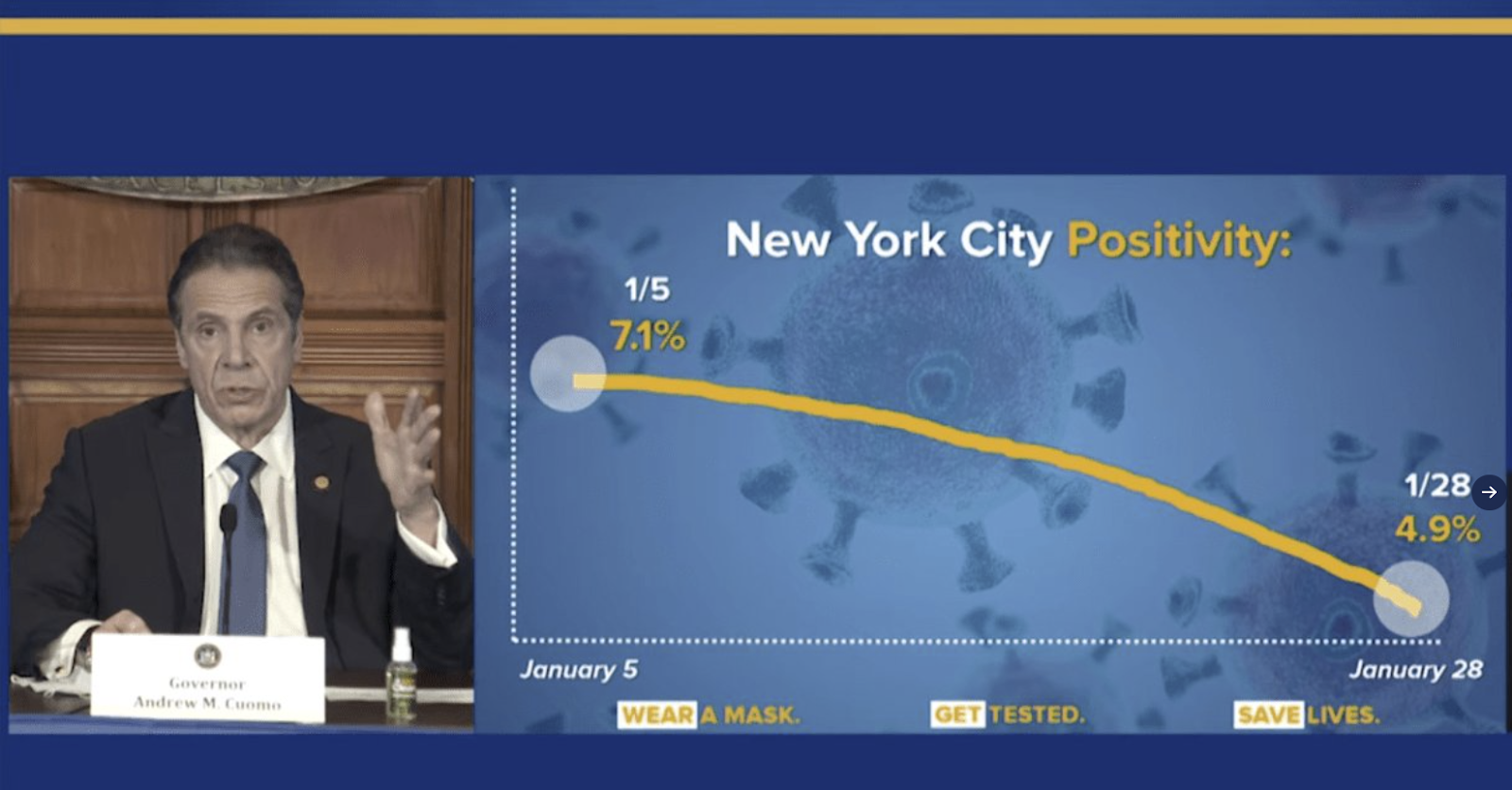
If you don’t want to call this fraud or lying, what would you like to call it instead?
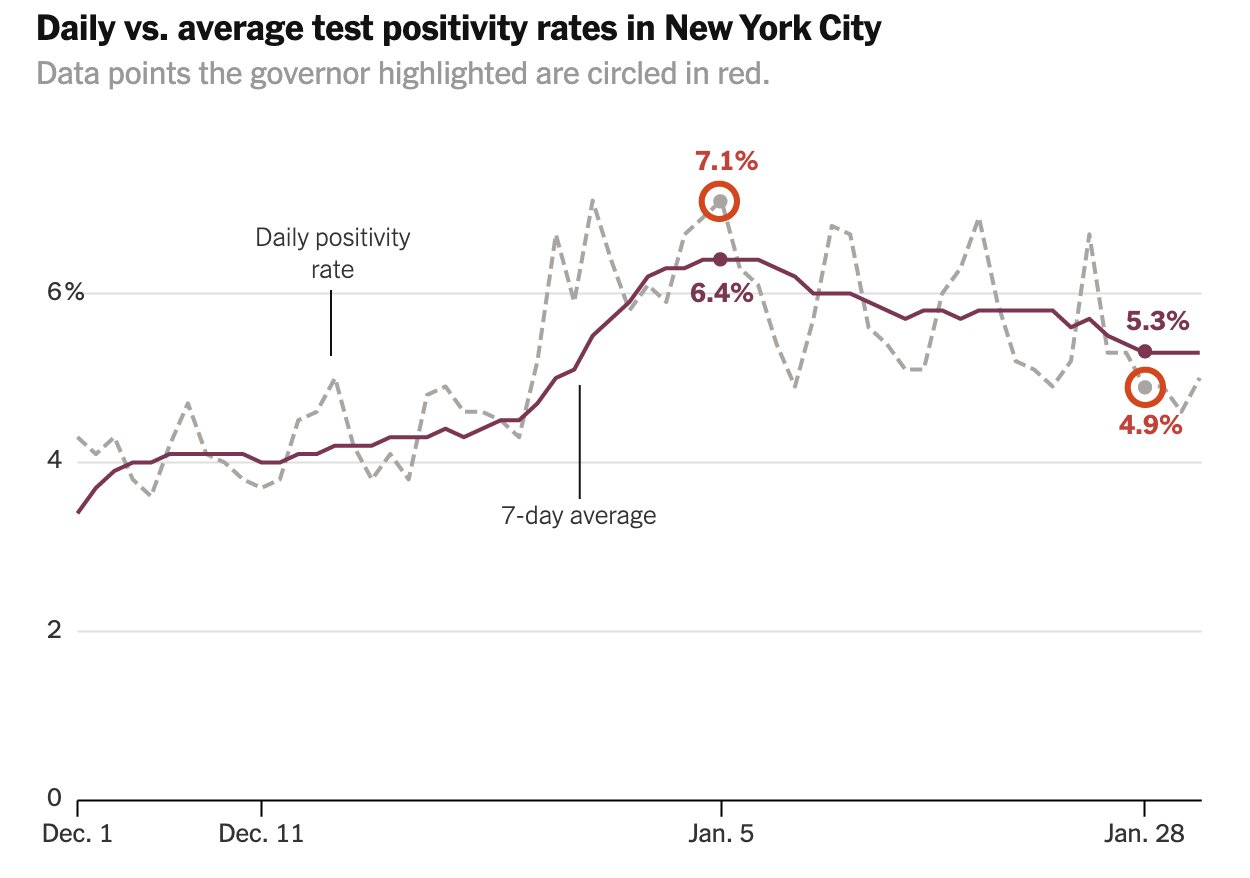
When called out on it, he issued this “corrected” graph:
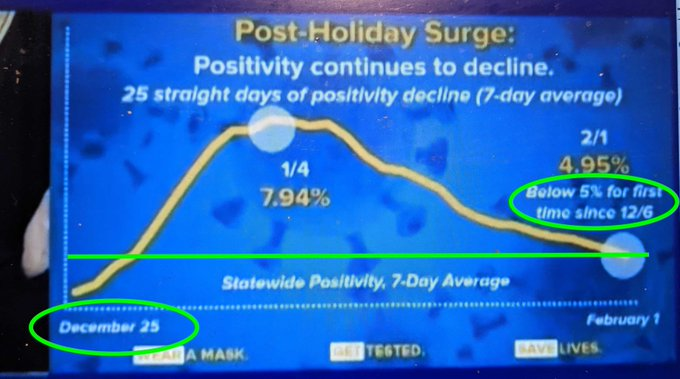
The green circles are a hint, as is that the graph starts lower than it finishes. Huh.
I leave ‘spot all the other ways this graph is wrong’ as an exercise to the reader.
In Other News
A report this week of someone making their own vaccine [LW · GW]. The question is whether it will work (and of course, whether it is entirely safe). This is pretty great in the context of doing it For Science. Plausible experiments are almost always positive expected value given how they can scale. In terms of whether it’s a good idea to do this for your own benefit, it seems like it’s rather late in the game for that, but I’m not going to attempt to render a verdict.
Biden continues to do some of the obvious things pure wins we weren’t doing before, even if they’re not the most important ones:

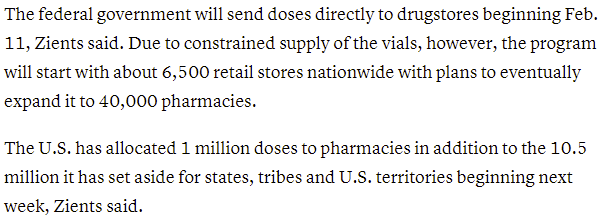
In context I can’t tell if this is talking about the constrained supply of vaccine doses, or referring to the real actual shortage of vials to put vaccine doses into, which is awaiting the FDA hopefully agreeing only a few weeks from now to let Moderna put more doses into each vial.
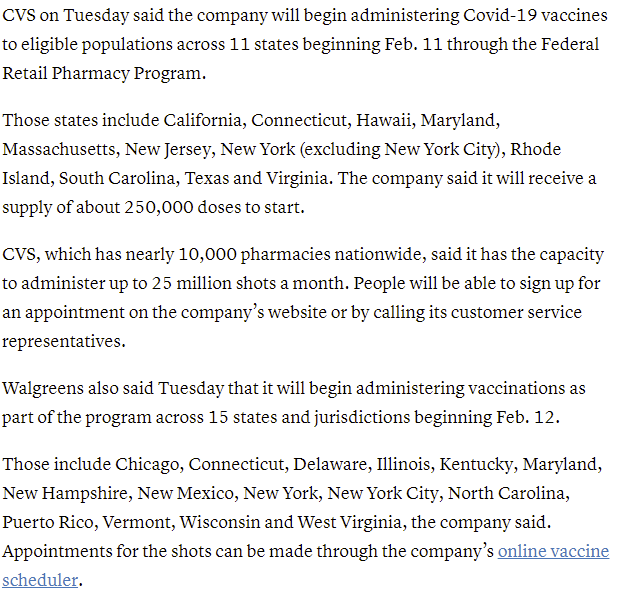
Also we’re finally doing this:

Here’s the scope of what to expect, looks like CVS can’t quite do our entire current pace on its own, we’d need to also use RiteAid and/or Walgreens:
Teachers’ unions in many areas continuing to fight for the right to not teach children:
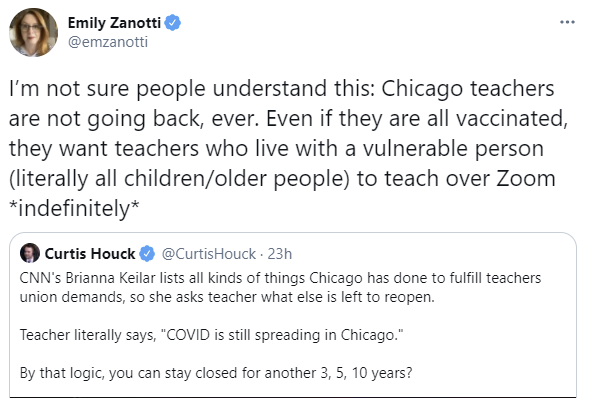
As always I’m torn because I consider school as it existed in 2019 in America a prison and a dystopian nightmare, but somehow remote learning has managed to be much worse, and it might never end, or at least go on for years, for those who can’t afford private school. The kids are not going to be alright.
There’s a disturbing pattern of people who get Covid-19 also getting diabetes, both Type I and Type II (WaPo). Unclear how often those people remain diabetic, but it’s one more reason to not want to get Covid.
Canada doesn’t seem to be following up that often to check on whether travellers are quarantining. But of the 3% or so they do follow up with, they claim that over 99% are complying with the rules. Would they like to buy a bridge, or perhaps Niagara Falls?
Pasteur Institute abandons its effort to create a vaccine after disappointing test results. Presumably it was too late to matter anyway, better to scale up what we have. Story seems to mostly be about French national pride and how they no longer have any.
Far right anti-vaccine protesters blocked access to the mass vaccination site at Dodger Stadium, forcing it to shut down for a day. Somehow we did not simply physically remove them. Instead, major news outlets are asking what sites helped organize it (in this case, it seems, Facebook) so they can demand censorship.
Global forecast for who will get vaccines this year. Thread discussing it here.
I’d like to thank Scott Sumner of The Money Illusion, author at EconBlog, writer of the excellent Great Depression gold standard book The Midas Paradox and top relentless advocate of the obviously correct Fed policy of NGDP targeting that I wouldn’t know about if not for him, for sending people over to my posts. He’s worth reading if his interests are relevant to your interests. He should also know that I’ve been unable to load The Money Illusion for months now but still read it through my RSS feed. His econLog posts are on average better anyway, as he readily admits. Some highlights of his on Covid are Selective Outrage, Markets Are Good At Allocating Resources and Regulation It’s Much Worse Than You Think. The titles say it all but the details are solid if you want them.
Curative is providing massive amounts of testing, and wants to test asymptomatic people because it’s called testing. The FDA is pushing back and warning against this, because there is a ‘risk of false negatives’ which is concentrated on weeks-old infections. It’s not even clear whether these ‘false negatives’ are an advantage or disadvantage, since detecting that someone was infected two months ago mainly shuts down activity without reducing risk much. What matters is active Covid. The FDA certainly seems from this reading to be demanding that the tests become so sensitive that they detect completely inert quantities of virus left over from old infections, and force such people into needless isolation, on pain of not allowing people to learn about their status at all. The good news is, as the article notes, lots of asymptomatic people are getting these tests anyway, despite the FDA’s best efforts to get us all killed.
It’s important to make disaster movies so that people only act as dumb as the stupid people in disaster movies, becuase otherwise they don’t realize they’re not supposed to be even stupider:
Matt Levine continues to be on fire, it’s important to remember there’s life outside of Covid-19, and I continue to recommend subscribing to his newsletter. In addition to coverage of the entire GameStop saga, this was an example yesterday of “Matt says thing Zvi frequently says, but incidentally says it better when covering today’s financial news”:
The news allowed me to scale things back a bit this week, a trend that will hopefully continue. I do not expect many surprises over the next few weeks. Then again, that’s often how surprises work.
25 comments
Comments sorted by top scores.
comment by Rasmus Faber-Espensen (rasmus-faber-espensen) · 2021-02-06T08:02:39.967Z · LW(p) · GW(p)
So it is clear that B.1.1.7, the English strain, is more transmissible than the old strain.
But what do we know about the methods of the increased transmissibility?
Do you need less exposure to the new strain to get infected? (Less time? Less amount of virus?) Do the virus persist in the air for longer time? Do the virus transmit more via different pathways?
We started out by using the protections that worked best against the flu: lots of handwashing, disinfecting surfaces etc. We adjusted this when we learned more about Covid-19: masks reduces transmission etc. Is there anything we can adjust to protect better against the English strain? Is it just strictly more infectious, or is it also that it is better than the old strain at transmitting through a specific pathway that we have not been protecting as much?
Replies from: rasmus-faber-espensen↑ comment by Rasmus Faber-Espensen (rasmus-faber-espensen) · 2021-02-11T13:04:41.958Z · LW(p) · GW(p)
I have tried to investigate and after much search (and having a question on r/askscience about it closed due to this being easily googleable) this is a summary of what I have found:
Apparently the mutation in the spike protein and the receptor binding domain lets the virus 'easier' bind to the ACE2 receptor sites and thus infect the cells.
So for a given amount of exposure you have a higher risk of getting infected with B.1.1.7 as compared to the old strain.
So bad news, I guess. There does not seem to be any low-hanging fruit here. Only harder restrictions (and more vaccinations) will help.
Best sources was this: https://www.medrxiv.org/content/10.1101/2020.12.24.20248822v2.full.pdf and this: https://www.reddit.com/r/askscience/comments/kjo7zm/how_do_experts_come_to_know_that_the_recent/
comment by IlyaShpitser · 2021-02-08T14:14:49.581Z · LW(p) · GW(p)
"That’s the test. Would you put it in your arm rather than do nothing? And if the answer here is no, then, please, show your work."
Seems to be an odd position to take to shift the burden of proof onto the vaccine taker rather than than the scientist.
---
I think a lot of people, you included, are way overconfident on how transmissible B.1.1.7. is.
↑ comment by ChristianKl · 2021-02-10T20:26:37.499Z · LW(p) · GW(p)
I think a lot of people, you included, are way overconfident on how transmissible B.1.1.7. is.
Do you mean with overconfident that it's likely more transmissible or likely less transmissable?
comment by ejacob · 2021-02-04T21:07:22.920Z · LW(p) · GW(p)
I showed the bit about Cuomo's graphs to some friends, and one of them responded with "If he will not open now, what he will close later?"
I think it was meant as a joke, but it might be a deep insight into the decision-making process behind reopening the restaurants now. If his majesty and King of New York Governor Cuomo expects things to get worse later, and knows that he needs to (i) have something to point to as the cause and/or (ii) have some action to take to make it look like he is reacting with Courage and Wisdom, reopening restaurants now makes sense.
On the other hand I think even according to his own data and justifications, NYC indoor dining wasn't even contributing much to cases to begin with, so maybe the decision is okay even if the epistemology is a joke.
comment by MalcolmOcean (malcolmocean) · 2021-02-07T17:42:05.436Z · LW(p) · GW(p)
🇨🇦 Canada update: we are WAY behind on vaccines (2.7% of population) and the bottleneck is very clear: we don't have the doses.
The "why" is also becoming a bit more clear: we never even tried to create a big manufacturing plant for it last year and instead just tried to partner with everybody, including a deal with China that was announced last May and started going sideways 3 days later but we're just finding out now that it completely fell through and is a nonstarter! Wtf.
A couple articles to read on that front:
- Canada-China vaccine collaboration began to fall apart days after Ottawa announced clinical trials (Globe & Mail)
- LILLEY: Britain's vaccine success the path Canada should have followed (Toronto Sun)
Not sure what we can do about any of that now though, unlike the USA where Zvi points at many obvious mistakes being made in the present, or choice points around approvals.
Meanwhile cases continue to trend downward (restrictions are mostly working) but there's no reason I'm aware of to think we aren't still going to gradually see growth of the UK strains and others.
Here's a longer update I wrote awhile ago: Covid Canada Jan25: low & slow [LW · GW]
comment by skybrian · 2021-02-05T06:23:58.602Z · LW(p) · GW(p)
AstraZeneca has not applied for emergency use authorization, because it has been told not to do so.
That resolves a mystery for me if true. How do you know this?
(I was wondering if maybe they are selling all they can make in other countries.)
Replies from: Zvi, TheSimplestExplanation↑ comment by TheSimplestExplanation · 2021-02-06T11:18:49.805Z · LW(p) · GW(p)
After reading the article i'm wondering why they aren't selling all they can make in other countries.
Replies from: danohu↑ comment by danohu · 2021-02-08T11:30:53.897Z · LW(p) · GW(p)
They are currently being keelhauled by the EU for having allegedly* diverted vaccine from the EU (which had not approved it) to the UK (which had).
They are committed to not making a profit from the vaccine. So there is no financial incentive for getting more vaccine out into the world, and plenty of reputational risk for doing so.
(*) AFAICT they did not even do this, and still their reputation is being trashed.
comment by Dave Orr (dave-orr) · 2021-02-05T00:18:28.651Z · LW(p) · GW(p)
The reinfection rates for the SA variant are indeed concerning. Do we have any data on whether previous infection prevents deaths or severe infection? The vaccines in general seem to do a great job of stopping the really bad outcomes regardless of how well they do on preventing all infections, so possibly something similar could be going on with the SA variant. Any data either way?
Replies from: Zvi↑ comment by Zvi · 2021-02-05T12:33:16.817Z · LW(p) · GW(p)
As far as I can tell, no data either way, but also not reports of people dying the second time around. I would expect substantial protective effects on severity (which also might mean we are underestimating how often such folks are technically re-'infected' in a mostly harmless way).
comment by Radford Neal · 2021-02-04T19:51:17.275Z · LW(p) · GW(p)
It's not clear what happened at Dodger Stadium. You say that "Far right anti-vaccine protesters blocked access to the mass vaccination site at Dodger Stadium, forcing it to shut down for a day.". But if you read this account:
https://www.fox5dc.com/news/anti-vaccine-protesters-temporarily-shut-down-covid-19-vaccine-site
and try to read between the lines, it's not clear. They say that "The Los Angeles Fire Department shut the entrance to the vaccination center at Dodger Stadium about 2 p.m. as a precaution". That doesn't actually sound like the protesters prevented people from entering. It sounds more like they waved signs and shouted, and the authorities thought that they might become violent, so they shut things down (for an hour, not the whole day).
comment by Douglas_Knight · 2021-02-08T21:04:14.537Z · LW(p) · GW(p)
All the modeling efforts talked about in the write-up are doomed because they don’t understand the role of the control system
Is that a forward-looking prediction? What consequences was UIUC doomed to? The article ends its coverage of UIUC in early September, declaring it a failure. But, in fact, it achieved its goal of keeping infections below 5k. You could credit that to "the control system," the panic caused by the early spike that got all the news coverage, but it's still a success.
comment by cistran · 2021-02-10T08:33:44.398Z · LW(p) · GW(p)
There are two Indian vaccines close to finishing their trials in India. On that note, Pfizer was denied approval in India since it did not use Indian subjects in their trials. There is a Chinese vaccine. There are one or two more versions of Russian vaccines still going through trials hopefully crossing every t because Russia does want to play by the rules and sell in EU at least. it just wanted to protect their population more.
comment by skybrian · 2021-02-05T06:09:31.132Z · LW(p) · GW(p)
I'm not sure about this statement in the blog post:
In the meantime, the single dose alone is 76% effective, presumably against symptomatic infection (WaPo) and was found to be 67% effective against further transmission.
I read another article saying that this is disputed by some experts:
With a seductive number, AstraZeneca study fueled hopes that eclipsed its data
Media reports seized on a reference in the paper from Oxford researchers that a single dose of the vaccine cut positive test results by 67%, pointing to it as the first evidence that a vaccine could prevent transmission of the virus. But the paper, which has not yet been peer-reviewed, does not prove or even claim that — although it hints at the possibility.
[...]
If a person tests negative, Andrew Pollard, one of the study authors and a professor of pediatric infection and immunity at the University of Oxford, told STAT via email, “then it is a reasonable assumption that they cannot transmit.”
But it is a big and unjustified leap, outside experts agree, from that suggestion to proof of decreased transmission from people who are vaccinated.
“The study showed a decrease in [viral] shedding, not ‘transmission,’” said Carlos del Rio, a professor of infectious diseases at the Emory University School of Medicine. “The bottom line is, no, one cannot draw a conclusion or straight line.”
Unfortunately the article doesn't say specifically why these experts consider this an unreasonable inference while the study's author thinks it's a reasonable inference. The closest thing is "There are too many, in my view, moving variables."
I can imagine one possibility for a counterintuitive result. Suppose the vaccine turns severe cases into asymptomatic cases, and transmissions happen mostly in asymptomatic cases?
Also, I was unable to tell from the paper when they do PCR+ tests. I have read that in some studies, they only do tests when a test subject shows symptoms, which would mean that some asymptomatic cases might be missed?
As a non-expert, I think we need to hedge our bets when experts disagree.
↑ comment by skybrian · 2021-02-06T05:20:33.463Z · LW(p) · GW(p)
I found an answer on the PCR question here:
But there is something good to say about their data collection: since the UK study that’s included in these numbers tested its subjects by nasal swab every week, regardless of any symptoms, we can actually get a read on something that everyone’s been wondering about: transmission.
comment by TheSimplestExplanation · 2021-02-04T22:54:32.768Z · LW(p) · GW(p)
A report this week of someone making their own vaccine. The question is whether it will work (and of course, whether it is entirely safe). This is pretty great in the context of doing it For Science. Plausible experiments are almost always positive expected value given how they can scale. In terms of whether it’s a good idea to do this for your own benefit, it seems like it’s rather late in the game for that, but I’m not going to attempt to render a verdict.
As long as you have not been infected it's not to late.
comment by TheSimplestExplanation · 2021-02-04T22:38:32.900Z · LW(p) · GW(p)
not test anything <s>that</s> else
comment by tomconerly · 2021-02-04T18:56:41.391Z · LW(p) · GW(p)
What's your best guess at how prevalent the English strain is in the US now? Is there any new data on that?
Replies from: Zvicomment by Yoav Ravid · 2021-02-04T16:18:23.618Z · LW(p) · GW(p)
Typo:
Replies from: ZviDelaying the second dose was found to actively appears to make the second dose more effective. Which is common for vaccines.