Covid vaccine safety: how correct are these allegations?
post by DPiepgrass · 2021-06-13T03:08:23.858Z · LW · GW · 93 commentsContents
96 comments
One month ago I clumsily tried to persuade my 74-year-old father that Tucker Carlson is probably wrong about Covid vaccines killing 3000 people, and if not, my father should get the vaccine anyway because he is in a high-risk group.
Well, move over lab-leak discussion, because this video is a tad more explosive: it alleges an ongoing and almost systematic censorship of information about vaccine side-effects, and it manages to do so in a way that fails to trip my BS detectors. While the LessWrong community isn't known for its expertise in vaccine science and epidemiology, it's usually pretty good about separating the true from the false, so here I am to ask for your comments. While the video is extremely long, the most controversial claims come near the beginning.
It's hosted by Bret Weinstein who (says Wikipedia) 'came to national attention during the 2017 Evergreen State College protests' and 'is among the people referred to collectively as the "intellectual dark web"'. The video description says Robert Malone is "the inventor of mRNA Vaccine technology"; he doesn't have a Wikipedia page, but he is mentioned on the page about mRNA vaccines as having 'developed a high-efficiency in-vitro and in-vivo RNA transfection system using cationic liposomes, which were used "to directly introduce RNA into whole tissues and embryos", as well as various cells types' in 1989. Finally there's Steve Kirsch, a red-tribey-sounding serial entrepreneur who mostly does tech firms but has been "researching adverse reactions to COVID vaccines". Steve frequently interrupts the other two, but at least seems very knowledgeable and well-connected (not to mention wealthy).
At first I was going to make this a 'question', but there's a lot to unpack and I think it could generate a lot of discussion, so I made it a 'post' instead.
Summary of the video's main points & discussions:
- 3:40 Prophylactic ivermectin is about "100% effective at preventing people from contracting Covid when taken properly" (an "Argentina study" is mentioned in support of this)
- 8:00 Bret gushes in the beginning about Steve's "article in Trial Site News". Here is a list of Steve's (seven) articles in Trial Site News. (edit: the original article was removed from there, albeit still accessible via direct link, and was later put behind a paywall with Kirsch's name removed.)
- 11:12 Steve became interested in the issue of vaccine safety because he talked to his carpet cleaner, who said he had a "heart attack" two minutes after taking the Pfizer vaccine and was "still feeling bad about it" (18:40 he talks about these side effects, how the press ignores victims of serious side effects, and how this has cost his carpet cleaner $30,000). Meanwhile, his wife started to suffered from serious hand shaking after taking the vaccine. This was like "lightning striking twice", "impossible" if the vaccine is safe. (my thought: a 'bad batch' could explain clustering in Steve's community)
- 12:30 Steve heard from to Byram Bridle about how, according to Japanese Government data, the spike protein generated by "the vaccine" doesn't stay in the arm like a typical vaccine, but spreads throughout the body. 14:02 The FDA knew about the biodistribution, and it's most concentrated in the ovaries (edit: this is false [LW(p) · GW(p)]), though the FDA did not believe it was dangerous at the time.
- 13:39 Dr. Malone: "The spike protein itself, we now know, is cytotoxic" (and "very dangerous", adds Bret) and Malone alerted the FDA about this risk "months and months and months ago, and we had a discussion"... "Their determination was, they didn't think that was sufficient documentation of the risk that the spike was biologically active." (edit: a least 4 fact checkers reject this)
- 14:40 Bret: if the protein lodged in "the membrane of the cells doing the transcribing" as intended, it would be a lot less destructive; Dr. Malone agrees, and says the "prior literature that was put out by the people that developed [the vaccine]" acknowledges this risk. They did "limited, non-clinical studies" to show "it stays stuck, we engineered it to stay stuck, and they published it." But "that's generally not good enough in non-clinical data package...in the normal situation where we're not in a rush, we have some really rigorous tests that have to be done on animals, and revealing that spike gets cleaved off of expressed cells and becomes free is something that absolutely should have been known and understood well before this ever got put into humans."
- 17:08 Dr. Malone says "cellular cytotoxicity" is actually what "really provides the protection... so you're getting CTLs against it" yada yada technical jargon.
- 19:07 Bret says groups about vaccine side-effects are censored. Steve says "200,000 users were wiped off the planet" (Facebook?); Dr. Malone jumps in to say "the censoring has been going on for well over a year, it's well documented, it's unequivocal, and my argument is that by implementing censoring, what we're doing is making it so that signals can't be detected, people's voices can't be heard [...] we have to have full disclosure of risks, and when you censor this, you cannot have this." Steve argues that because everyone is trained to think the vaccine is safe, doctors routinely deny that any side-effects were caused by the vaccine and do not enter information in the VAERS system as they should (note: the CDC web site says that "FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS," but I don't know if there are any reporting requirements for other side-effects.)
- 21:28 Bret was talking to everyone he encountered - Dentist, Doctor, hairdresser - and "the number of people who had a frightening story was alarmingly large. In fact, I believe it is the case that the only people who didn't have some anomalous reaction was my parents and Heather's mom" (this is the most BS-sounding thing in the video, but it could be that Bret misspoke and actually meant that "most people who are public-facing [interact with many people] in his community know someone who has had an anomalous reaction to a Covid vaccine", which is still a big allegation.)
- 22:30 Dr. Malone says his FDA friends "in senior positions... were aware back when we were doing [RCTs] that these adverse events were occurring—many of them were oddly delayed and atypical for a vaccine trial. .... one of our assumptions here is that this is like every other vaccine...and it's not"
- 23:57 Dr. Malone talking about his alarm about a "data package...that Canadians acquired from foya (?)", and he shared it with a "regulatory affairs professional" who found more issues, like the absence of the "reprotox" (reproductive toxicology) package and genotoxicity package. But he's heard "Pfizer has submitted a new data package in the last couple weeks, so...we have to take those data with a little bit of a grain of salt because they may have been updated"
- 26:52 The FDA lied by telling people that no corners were cut (they used an analogy of a road in which they have straightened out the curves and reduced paperwork); informed consent is being elided. Bret: "everybody who is getting these vaccines is part of an experiment that we are running, which is actually wildly overgenerous of me to say, because in order for it to be an experiment, we would have to systematically collect data on what happened to them, and our ... system isn't so systematic ... voluntary reporting with stigma attached"
- 28:23 Steve "did a survey on Nextdoor, and 3% had persistent troubling symptoms that haven't gone away" (Lizardman constant, one wonders? Coincidental illness? But I wonder which state these three people are in, and whether one vaccine is implicated more than the others. Pfizer and Moderna are both mentioned in the video and, for the most part, they don't clarify which vaccine(s) they are talking about.)
- 28:47 "Nobody knows about [the VAERS system] and people aren't reporting" and "we've had reports reversed without the doctor's consent"
- 30:32 Chart showing death reports in the VAERS system. There are less than 205 deaths every year before 2021, then 4561 for "Covid vaccines". (edit: OpenVAERS data disagrees: it shows 605 deaths after vaccinations in 2019 [? · GW])
- 32:07 Steve: "Nobody can explain why they've removed reports from the VAERS system, because what we found is that the reports that were put in by people and [snaps fingers] they disappeared, so this is a conservative estimate, because what about those reports that they took out that we can't see?"
- 32:35 Dr. Malone "this morning" called friends at the FDA about "the databases and database analysis" who said "it's chaotic, it's disorganized, they are not analyzing the data efficiently, they're understaffed, they're overwhelmed" .... "If our goal is to ensure safety, the bias has to be to assume that there is some association and then take the time to track it down, and therein lies the rub ... the FDA had the latitude to require that the vaccine sponsors/developers implement more rigorous data capture for safety ... and they made a conscious decision not to ... [after] authorization for Emergency Use Authorization [EUA] ... under an [EUA], normally ... the sponsors are still required to carefully capture safety and efficacy information; you're still an experimental product ... in this case, I'm not aware they implemented any requirements for the sponsors to capture those data." (I wonder: what about the rest of the world?)
- 39:44 the info we have (e.g. VAERS) is almost worthless. In the vaccine cost-benefit equation, the "benefit" calculation requires you to look at the full set of alternatives; Steve talks about how elites are ignoring major results showing fluvoxamine and ivermectin "works". Steve: "This information is being suppressed, and it's unfair..." says Tess Lawrie submitted something (at 51:14 he says it's a "systematic review and meta-analysis" for ivermectin) to a journal and got it peer-reviewed and "it's probably going to be published tomorrow". He says there's been systematic review and meta-analysis - "the highest level of evidence" and Bret adds that "the evidence is overwhelming". It sounds like ivermectin has stronger evidence than fluvoxamine. But at 40:38 Steve raises my eyebrows by saying a p=0.05 result "proves that it really works" as Bret nods vigorously. Edit: Lawrie's paper was published 7 days later with 6 co-authors, concluding "Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using ivermectin". I notice that Lawrie is also the Director of the "Evidence-Based Medicine Consultancy" that calls for "an immediate halt to the [Covid] vaccination programme"; notably, this document lacks cost/benefit analysis and ignores base rates (i.e. it ignores the number of adverse health events that would normally occur in a large population in the absence of any vaccines). Theresa Lawrie also founded the BIRD website (registered 2021-03-07), which "[brings] together clinicians, health researchers and patient representatives...to advocate for the use of ivermectin". Co-authors Dowswell and Fordham are affiliated with the EBMC and BIRD respectively.
- 43:19 Dr. Malone says, at doses effective against Covid-19, ivermectin is safe. Masks are mandated under the precautionary principle despite a low level of evidence for efficacy, and yet for ivermectin all authorities are saying we can't use it despite all the evidence. Note: the FDA has published an article titled "Why You Should Not Use Ivermectin to Treat or Prevent COVID-19" — don't take my word for it, but its arguments are weaksauce.
- 51:35 Steve alleges that NIH doesn't take 'saving lives' into consideration when making decisions; Dr. Malone disagrees, but before he can explain is interrupted by Bret who speaks of an "emergent phenomenon" similar to regulatory capture but without the usual hallmarks. "We are trying to grapple with what it is that's doing this. It is very tempting to imagine that there must have been a meeting in which people decide it was okay for tens of thousands, hundreds of thousands, possibly millions to die needlessly given a pandemic we might be able to end if we just simply decided to do it [...] but [instead] it can be a function of the underlying drivers."
- 56:37 Bret: "Merck...very conspicuously attacked the safety of its own drug ivermectin even though they knew from four decades of work" that it was safe, citing no evidence to the contrary. "Why? Well, it turns out they have another drug headed rapidly for an [EUA]. Well, what does the [EUA] require? It requires that there is no safe and effective therapy existing because if there was, you wouldn't take the risk of fast-forwarding this process" and also they're partnered with Johnson & Johnson to produce their vaccine. Dr. Malone suggests that the usual "rigorous terms and conditions" for disclosure of conflict of interest were not followed in this case.
- 59:20 recap by Bret. Dr. Malone adds "my colleagues are telling me they're extremely frustrated because they can't make heads or tails out of the data"; Steve says the U.S. government commissioned a study on VAERS that estimated "there could be only 1%" of adverse events being reported, and alleges that none of the deaths in VAERS have been explained or investigated. Also says Tess Lawrie's study is self-funded, so no conflict of interest.
- 1:07:55 Steve asks "the OpenVAERS people" what they think the true number of deaths from the vaccine is, "and they told me that of course nobody truly knows, but based on their analysis they put it around 20,000 deaths". Edit: it turns out Steve asserted on May 25 that the vaccines "likely killed over 25,800 Americans" [edit 2: omitted 'likely' in first edit, sorry]). My objections: one, if this were true, where are the lawsuits against the vaccine makers? and two, how likely is it that all vaccines are equally dangerous? Steve seems to have done nothing to try to distinguish the safety of each vaccine individually. Edit 3: the blog he indirectly linked to, by Austin Walters, retracted the claim about 25,800 deaths on June 18. Steve did not retract his claim, but (based on Wayback Machine records) on August 3 the link to the claim disappeared and most of the article went behind a paywall, after the author's name changed on July 29 from "Steve Kirsch" to "Vaccine Truth", now spelled "vaccinetruth". The profile of vaccinetruth says it "is a group of people"; Malone is one of the 5 names listed, but Kirsch is not.
- 1:11:10 A UK document of "The Evidence-Based Medicine Consultancy Ltd" shows a high rate of adverse events and says "The MHRA now has more than enough evidence on the Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans."
- 1:14:43 Bret: "it is becoming clear to clinicians that long-haul Covid, Covid and post-vaccine syndrome are closely related." Dr. Malone: "for me the thing that's alarming is that there's no alarm."
- 1:16:39 The V-safe system is not transparent at all, not even to FDA data analysis specialists (or 1:19:18 "responsible, qualified third parties")
- 1:19:22 Discussion of "unprecedented" social media censorship. Also, lamentation of political polarization.
- 1:25:30 Steve: "when I posted this to Trial Site News I had a scientific advisory board of 14...very high-powered academics, all of them resigned...saying that what I was doing was irresponsible, that it will cause vaccine hesitancy... that they didn't want to associate me any more.... I said 'I'm sorry you're resigning, but could you please point out an error, and I will correct it... and they gave me nothing... factual that was wrong with my article." (Edit: I am skeptical that Steve ever corrects claims in his previously-published articles. Surely someone told him that his headline claim about 25,800 deaths was retracted with an explanation by the person who originally made it, and I don't see how he himself could have failed to notice that his claim about ovaries was false... it's quite a blatant error.)
- 1:28:19 Lamenting people being sent home from the ER without treatment, possibly infecting family members, being told "don't come back until your lips are blue". Steve refers to a "little practice" of "George Fareed and Bryan Tyson" having treated 6500 patients averaging 60 years old with "like zero" hospitalizations except in cases where "somebody comes up to us really late"; they use a treatment protocol with hydroxychloroquine, ivermectin and fluvoxamine. Dr Malone stresses that Steve isn't just talk, he walked the walk, having funded a fluvoxamine study at Wash U.
- 1:33:09 Dr Malone: Some front-line doctors are doing a great job trying to understand what's going on and tinkering with ways to treat their patients.
- 1:38:38 Dr Malone, in a discussion on perverse financial incentives, says "I lived this. I set up a company, Theric Pharmaceuticals, for Zika, and I worked closely with the DoD and developed a portfolio of drugs, repurposed drugs, many of which are now being applied to Covid because they're antivirals, okay? I went bankrupt. The investment community had zero interest because there was no way to make a buck... so I have direct personal experience validating the thesis that the financial incentives around drug repurposing are such that it doesn't get done." Steve adds that "we" called drug companies and offered to "pay for all your expenses" and they still weren't interested. "even if I had their phase-3 trial that they need, which I do have now, I still would not be able to get an [EUA] on a repurposed drug."
- 1:40:50 Bret asks Malone about doing a quick RCT on ferrets to show safety and efficacy of ivermectin for Covid. Malone says we really need evidence in humans. He says Andy Hill tells him "there are large trials pending" but he's decided to stop releasing interim results, and results are "scheduled to come in in September". Steve says there's never been a case where a systematic review and meta-analysis has been overturned by another one, so existing evidence for ivermectin is sufficient.
- 1:49:19 Dr Malone says a common criticism of ivermectin data is that small studies across the world on ivermectin have not been peer-reviewed, but this is because "it has become wicked hard to get anything through peer review involving repurposed drugs". Malone set up a "special edition of frontiers of pharmacology for repurposed drugs, and then it got killed" arbitrarily. He doesn't clarify this point, but adds "we've never encountered a situation like this, where it has become this difficult to get anything through peer review, and anything that has to do with repurposed drugs is...almost impossible". Malone agrees with Steve that there is a negative reporting bias where only negative reports can be published, noting that this is the opposite of the usual bias.
- 1:52:18 Steve is frustrated at hospitals avoiding repurposed drugs, giving an anecdote (not about Covid?) of a drug treatment where "you go from lungs that are like, dark, to fully clear in 48 hours, and the physicians say 'we've never seen anything like this'... happens about 50% of the time", but he personally jumped through hoops and couldn't get El Camino hospital to prescribe this for a hospitalized acquaintance in "bad shape, on ICU". "People have gone to court to force doctors to give ivermectin and the hospital doesn't want to do it, because if the hospital gives a drug which has not been approved by the NIH, they are liable if something happens... so the hospital doesn't want to give you stuff that would save your life". "Outpatient doctors are always trying new things, so if they reported to the FDA, that's all we need... because...you can see, holy moly, the doctors that are giving the ivermectin-fluvoxamine, they've got like no hospitalization, repeatedly." Dr Malone says the idea of a "system to enable patient-reported outcomes and physician-related outcomes...is a profound statement. We have nothing like that. My friends at the FDA also came to that conclusion, and they're frustrated because it doesn't exist." Malone blames administrators/MBAs for preventing drug repurposing at hospitals, not just because of liability but also because they make more money prescribing in-patent drugs like remdesivir ("6 or 8 thousand dollars... for a treatment course") rather than older ones.
- 2:01:41 Steve says there's another drug "which we funded the work on, which is GS 441524", an antiviral "sort of the precursor to remdesivir, and it works really really well, but it's being pursued by Victoria Yan (?) who's just an individual, [who has] raised some money privately to do this"; one patient was amazed how effective this was as treatment for her severe long-haul Covid... "and Gilead is doing nothing!" even though it's "much safer and much easier to produce".
- 2:03:15 Bret: doctors had fewer tools in the past, but they had the virtue of acting as scientists, being able to gather more local information and being allowed to do more with that information. Modern legal and corporate structures have shut down those virtues.
- 2:08:04: Steve argues multiple drugs should be used at once as a Covid treatment. "Treat this virus like your life depended on it" (because it might just). Dr Malone agrees and is pursuing multi-drug trials but facing "immense" challenges. In their strategy they would "learn form David Ho". "Almost all the agents you've been talking about are acting at the level of anti-inflammatories, not antivirals", because antivirals have a poor track record of treating pulmonary viral infections, because it's too hard to treat early enough, so the second phase of dangerous inflammation must be treated. But "the thought leaders who have set public strategy in the drug space have decided...to emphasize direct-acting antivirals, and they have sought to test those, most often, in a late-stage Covid environment...it doesn't work".
- 2:14:13: Dr Malone "In my correspondence with the agency advocating for an ivermectin-containing arm in this study, I had to write...the justification for mechanism of action for ivermectin... I've never disclosed this publicly, I don't have...authorization to say so... but the truth is, that I wrote this big long section, summarized the different potential mechanisms of action of ivermectin, most of which are anti-inflammatory. The agency wrote back and said 'you have to do the studies in cell culture to prove the mechanism of action before we will allow you to proceed with the trial', and our decision was to just drop it.... and it gets to this point of another data point" (apparently he means 'another anomaly in how authorities are acting'.)
- 2:17:34 discussion of reproductive harms begins with chart from a article by Steve. I looked up the displayed URL, which begins with a statement that "these vaccines have killed over 25,800 Americans and disabled at least 1,000,000 more", which links indirectly to a blog post by Austin G. Walters. Steve and Dr. Malone agree that the graph (for "Pfizer mRNA Vaccine BNT162") is "consistent with the primary data". It shows the concentration of a "lipid nanoparticle" that is the delivery mechanism of the vaccine, "the box in which the mRNA" is housed. The graph shows about 10 times higher concentration in the ovaries than most other organs after 48 hours. (edit: this is very misleading [LW(p) · GW(p)]) "On some level it's not safe for women at all," Bret says. The high concentration in bone marrow is also worthy of study. There is no signal in the testes.
- 2:28:30 Bret asks Malone about "the hazard of the vaccines because they create a very concentrated evolutionary push on spike protein alone, that vaccinating into a pandemic rather than in advance of a pandemic, is liable to cause the evolution of escaped mutants, and that it could...make a much worse pandemic in the end". Malone immediately responds "this isn't a theoretical, this is a real." (I will leave this argument in the video because it doesn't make sense to me; evolution doesn't have goals and shouldn't evolve its spike protein appreciably faster just because people are getting vaccines. I don't think this is meant as an anti-vax argument, though I would assume some people will use it that way.)
- 2:31:55 Bret worries about "antibody-dependent enhancement". Normally antibodies are supposed to stick to antigens to neutralize them, but apparently there are cases where antibodies make the infection worse, and "this is why the second bout of dengue [fever] is worse". Dr. Malone responds that "all of the prior attempts to develop human coronavirus vaccines have failed due to ADE.... The [interesting thing] about the current ones is they are showing so much efficacy ... I was watching for an ADE signal, I'm not seeing it".
- 2:39:29 Dr Malone chose to take the vaccine. He had Covid already, and only took the vaccine to meet travel requirements, after waiting for an ADE signal.
- 2:44:29 Dr Malone: "The thing that is the hallmark of the modern FDA is the response to Thalidomide... that has guided the whole legislative structure and organizational structure of the FDA, and that's all about reproductive toxicity... and I hope that Pfizer has submitted to Peter a comprehensive genotoxicity and reproductive toxicity panel in the nonclinical studies, but even then, rats are not humans. What we've learned is that reproductive risks don't always manifest in the first generation. So I don't mean to scare, but I do mean to speak honestly and with integrity, and...if you were to ask me, 'Robert, do you know what the reproductive consequences are for this signal?' I would have to tell you 'no I don't'... if you then ask me 'has there been any examples in the past of reproductive effects of agents in female reproductive tissue that were not anticipated by the animal model testing?' I would have to say yes there is.... My position on all of this goes back to the bioethics... there has to be full and open disclosure... it's your body... the burden is on the government... to convince us... they do have an obligation... to full and open disclosure.... we as a public health community should err on the side of transparency and disclosure, and trust the American people and the people all over the world ... to make decisions for our own health... I do feel pretty strongly ... the strategy 'we're going to give out ice cream to get the kids to get vaccinated', that's just wrong." Bret adds, "it's tantamount to evil."
- 2:49:59 Steve: "If I had known what I know today, I never would have vaccinated my three young daughters..." ... "I know one of the cabinet ministers of the Biden administration, and I brought this to his attention numerous times, and he has tried to get the attention of the proper people, and ... it doesn't register because it's against the narrative..." ... "If you want to criticize what I've written, tell me what's wrong and I'll fix it." ... "This is why people can't speak out, because the narrative is so strong..."
- 2:56:57 Dr Malone: "This is always the case when you're at the tip of the spear. There's the parable 'don't be a pioneer; all you get is arrows in the ass'. This is a paradigm-shift problem, and the lovely thing about medicine is that we've been through multiple cycles of this. The classic one is gastric ulcers, and the bacterial basis for gastric ulcers." (hm, years ago a climate dismissive used 'ulcers' on me to justify his eternal support of the minority position on climate, but point taken.)
- 2:58:38 Bret: "the work I did that revealed there was a flaw in the drug safety system [what flaw, Bret?], that bell still hasn't rung, that was 2002... this is par for the course except the stakes are really high here"... "you've got all of these anomalous signatures... I can make a defense for [EUAs] for a vaccine is not well-enough tested in the face of an emergency... [but] I can't make that argument when there's perfectly safe therapies that are available for us off-the-shelf, and I never could have made that argument for people that have already had Covid..." ... "we've got all these signals of...'extended regulatory capture' where regulatory capture reaches into not just regulatory agencies, it reaches into journals...universities...social media...organizations of doctors...the [WHO]... it is self-censorship, but the point is but the point is, I don't think there's any way to beat that going through the front door... what you're finding out [Steve]... is that that's not going to work because there are so many layers protecting it" [the others agree].
- 3:01:06 Bret suggests this is the perfect opportunity for Elon Musk to gain practice saving planet Earth. "the greatest defect [in] our economic and political system [is] it can allow you to evaporate trillions of dollars of wealth in the pursuit of billions of dollars of wealth." ... "there's a bitter pill here... we can't solve the problem perfectly, we're going to have to accept something ugly... we need to buy out the interests of those who are doing it. If they've got an [EUA] for an untested, dangerous new drug and that's the reason they're thwarting our ability to talk about the solutions that are available to us, let's just fuckin' buy them out already." ... "it's a hell of a lot easier than going to Mars... [Elon] is way smart enough to look at the same data we've looked at and reach the only conclusion you could reach if you looked at it..."
- 3:06:31 Dr Malone: "we're facing a future where pharmaceuticals and vaccines are largely produced offshore... as a consequence of this kind of kookiness" (um ... why would regulatory capture drive big pharma away?)
- 3:08:56 Steve's solution is simpler: Elon should tweet a link to the video saying "Everybody should watch this. This is very very very important." Another solution... "everybody has a social...moral...ethical responsibility to retweet this, share it..." (wow, the longest chain letter I've ever seen) "The doctors who want to speak out, cannot, because they don't have a voice, especially if you got any kind of NIH funding... you will never see a dime... I just got a tweet yesterday from a woman who runs a support group and 'one of our members committed suicide' because no one is listening to her..."
- 3:13:42 Dr Malone: "the irony is, the RNA story went through this same thing where it got suppressed and shut down, it was considered to be crazy talk... I'm in close contact with the long-hauler community, and like your story a member of that community recently committed suicide... if we can't allow these people to even have a voice, then they're completely disempowered... we must let these people who have no voice to at least speak to each other."
{kind=link}
Edit: After reviewing everything, I'm seeing some signs of BS, mainly centered around Steve, who takes some rather extreme interpretations as fact (the summary above omits Steve's many interjections demonstrating this). One example is that he acts like it's crazy that everybody hasn't already accepted the greatness of ivermectin, even though the best evidence is said to be in a paper that hasn't been published yet. Also, his May 25 article (linked twice above already) has even more extreme claims than this video. And yet, Bret thinks Steve's article is great (assuming the URL at 2:17:34 is the one he gushed about in the beginning). While Dr. Malone occasionally disagrees, it's rare; for the most part he explicitly agrees, nods, or expresses no skepticism. So my main point of concern is that the three of them are very credulous about the strongest claims, and don't take seriously the possibility that they could be wrong. Plus, they show no interest in possible differences between the vaccines. Pfizer-BioNTech and Moderna are both mRNA-based, but this hardly guarantees the same risks for both. But they speak about all vaccines (4 brands in 2 categories) as a singular entity, "the vaccine".
As I noted a month ago, it is required to report deaths after vaccine administration to VAERS, so if it's more common to give a Covid vaccine to elderly and ill patients than it was to give seasonal flu vaccines to elderly and ill patients, this could explain the VAERS data. If the reporting requirement is new or more publicized, that could help explain it too. And if a vaccine is causing these deaths, where are the lawuits? Alleging "the" vaccine has killed tens of thousands of people, with no sign of having considered any alternative hypotheses, is a big red flag and if Steve proves to be incorrect, his efforts will probably cause deaths, because surely there are many elderly people like my parents who have chosen to stay unvaccinated due to messages like this. If Steve is correct, it is still important to do a cost-benefit analysis of vaccination vs no vaccination, particularly in regard to high-risk groups like my parents, and Steve did not attempt to do that either in the video or on his blog.
Also important is how little evidence is directly presented; mostly it's just alluded to. Don't extraordinary claims require extraordinary evidence? They seem to think that they themselves having seen some evidence is enough, so there's little need to present it to their audience. Since the number of views has topped 350,000, I encourage interested people to see if they can debunk, support or clarify some of these claims. While I suspect the claims about vaccine deaths are overstated (perhaps dramatically), I think there's a lot of common-sense reasoning in this video that will stand the test of time.
The video was deleted for 'Violating YouTube's Terms of Service'. See below for alternate links.
P.S. Here are the results of Canada's voluntary Covid-19 vaccine safety survey. It would be nice if they offered more detail on the more major side-effects, but...
93 comments
Comments sorted by top scores.
comment by paulfchristiano · 2021-06-14T00:04:14.528Z · LW(p) · GW(p)
I read the start of Kirsch's article here since I'm slightly interested in vaccine skepticism and have never dug into it before. (I'm not sure if this is the article that Bret is gushing about.)
The first claim in the article is that there are many more deaths reported by VAERS. I ignored this because without some other context it seemed unsurprising and uninformative that VAERS is used more for the covid vaccine than for the flu vaccine (and the absolute numbers of deaths reported are negligible given the number of people who have taken the vaccine). The inference of "at least 20,000 deaths due to the vaccine" looks like it's probably bullshit but it would take a few minutes to establish that and so I moved on.
The next claim about harms was "82% miscarriage rate in first 20 weeks", which links here. But this number seems to be computed as "Amongst pregnancies that ended, how many were miscarriages?" The table was published in April 21 about people who were vaccinated December 14 - February 28, and it looks like there shouldn't have bee enough time for anyone to have a healthy live birth if they were vaccinated in the first 20 weeks.
The authors of the letter-to-the-editor acknowledge this as saying "We acknowledge this rate will likely decrease as the pregnancies of women who were vaccinated <20 weeks complete but believe the rate will be higher than 12.5%," but it's unclear why they believe this (the study reports 96 spontaneous abortions amongst something like 1000 people who were vaccinated in the first trimester, which seems like it may be right on track). And of course that wouldn't make the 82% number less dubious.
So as far as I can tell this datapoint is very misleading, and this should have been obvious to anyone who took a cursory look before including it in an article. It's also such an extreme and bizarre claim that it should certainly have warranted a cursory look.
I didn't look into any of the other claims because it would probably be more valuable to instead read some more credible vaccine skeptic.
Replies from: markus-plesner-dalin↑ comment by Markus Plesner Dalin (markus-plesner-dalin) · 2021-08-21T18:50:12.449Z · LW(p) · GW(p)
There is an interesting critique of the miscarriage claims (and some of the other claims) in this Medium post:
https://medium.com/rebel-wisdom/on-vaccine-safety-ivermectin-and-the-dark-horse-podcast-an-investigation-f32491d4c970
comment by MichaelLowe · 2021-06-13T11:42:11.107Z · LW(p) · GW(p)
As others have said, I strongly dislike posting of 3 hour videos without any timemark or summary of the main points. This is making the community do the work of extracting the information; on top of that people will not watch most (or any) of the video before commenting, so discussion quality will be low.
To not be completely negative, I watched the section on "Vaccine suffers censored" (there are time marks in the description on youtube) where all three of them claim explicitly that there is no monitoring. This is clearly inaccurate, for example we know that Israel has recently reported that myocarditis might be occurring more often than expected in young men. In addition, I know that Germany has the SafeVac app to make it easier for people to report side effects after vaccination.
Replies from: Vanilla_cabs↑ comment by Vanilla_cabs · 2021-06-13T13:03:56.542Z · LW(p) · GW(p)
there are time marks in the description on youtube
As timestamps go, I found these ones to be well-made and more useful than the usual:
00:00 Introductions
02:20 This must be discussed
03:13 Will herd immunity be reached?
07:58 Spike protein is very dangerous
13:45 FDA knew it could be toxic if it didn't stay stuck
18:09 Vaccine sufferers censored
23:26 Reviewing the FDA data package
26:41 Corners were cut
27:52 Steve looking at VAERS
32:37 Robert's friends at the FDA and the emergency use authorisation
37:38 Risk benefit and quality life years
40:18 Alternative to vaccines
44:19 Mask wearing RCT
45:28 Three anomalies around vaccines
46:05 Fluvoxamine trials
51:00 Two million dollar offer and the NIH
52:13 Robert's view of the NIH
53:00 Regulatory capture
54:41 Fauci's emails
56:30 Merck on Ivermectin
59:24 Emergent phenomenon
01:01:42 Vaccine deaths
01:03:24 Tess Lawrie's vaccine safety data
01:04:43 Difference between the gene therapy vaccines
01:06:40 Self reported deaths from vaccines
01:09:18 Adverse reactions
01:17:12 Robert on V-safe database
01:19:30 Social media censorship
01:22:20 Steve's experience with denial
01:24:17 Two teams
01:28:20 "Don't come back until your lips are blue"
01:30:52 "Treat people early with drugs"
01:32:11 Ignoring frontline doctors
01:35:39 Financial incentives
01:37:28 Response to demand for RCT on ivermectin
01:38:39 Robert's personal experience with repurposing drugs
01:40:52 Mink and ferrets lab research
01:43:53 Robert on animal model for COVID treatment
01:46:33 Ivermectin works
01:49:13 Repurposing drugs
01:52:17 Doctors ignoring treatments
01:55:31 Effective treatments for long haulers
01:56:45 Robert's response on incentives and hospital liability
02:01:42 Additional antiviral and Gilead overlooking it
02:03:13 Communication is forbidden
02:04:53 Using antivirals as soon as virus presents
02:06:41 Multiple drugs at once and Dr Drew
02:11:02 Trials with drug combinations
02:13:53 Criticism of Fauci and mechanisms of action for ivermectin
02:17:35 Pfizer data on where the vaccine spike protein goes
02:20:42 Spike protein in the ovaries and bone marrow
02:22:12 FDA signals of risk from vaccines and auto-immune issues
02:27:41 Bret summarises and discusses additional harms
02:28:31 Vaccines possibly causing escape mutants
02:31:56 Antibody dependent enhancement (ADE)
02:38:19 Why did Robert and Steve get vaccinated?
02:40:54 Summary of risks including coagulation problems
02:42:41 FDA, thalidomide, and reproductive toxicity
02:48:12 Vaccinating adolescents
02:50:00 Steve on vaccinating his children and the response he receives
02:56:38 Don't be a pioneer, you'll get arrows in the ass
03:00:01 Extended regulatory capture
03:01:10 Can Elon Musk save the planet?
03:05:17 Pharmaceutical industry offshore
03:08:59 Steve's solution, plea to big tech employees, and vaccine long haulers
03:13:41 Robert speaking to big tech employees
03:15:55 Wrap up
comment by gilch · 2021-06-13T07:22:37.626Z · LW(p) · GW(p)
Don't know yet. I've watched about half so far. My first impressions are similar to DPiepgrass.
Typical conspiracy theorists are fairly easy to recognize. They seem to take the axiom that everything happens on purpose. They don't notice the inconsistencies in their own models, and their bald assertions often don't stand up to easy verification, if you bother to check.
These are not crazy conspiracy-theory types. (That doesn't make them right.) They understand scientific thinking, are using the biology vocabulary correctly, and are trying to use gears-level models. They understand how the vaccines work, and what might go wrong. They accept the possibility that this isn't happening on purpose, but is just a bad outcome of incentives, something we already believe happens [? · GW].
Kirsch (blue shirt guy) seems less careful than the other two, and may or may not be a crackpot. This doesn't necessarily make his concerns wrong. We should still try to verify their claims. Are these guys who they say they are? Do they have valid credentials? Does the spike protein break off so it could have systemic effects? How toxic is it? The vaccine might still win a cost-benefit analysis.
I've watched IDW videos before. They're an interesting bunch, some of them might even be rationalist adjacent, but this varies. They seem to like long conversations.
Whether or not this case has merit, the systematic censorship thing seems real to me. We've had measles outbreaks here in the U.S., despite having an effective vaccine. This is mainly due to the antivaxxers swallowing bullshit, and there's been a mainstream pushback. But Arguments Are Soldiers [? · GW], so even when the antivaxxers have a point, the mainstream isn't allowed to admit it, especially in the face of the clear and present danger posed by the current pandemic.
The media's recent about-face on the lab-leak hypothesis is a recent example of this effect: it was on the "wrong" side politically, even though it had merit. Weak evidence is still evidence, and the truth doesn't become a lie just because the Enemy says it. Social media has been (fairly) blamed for spreading conspiracy theories, and so under pressure to take responsibility, they're trying to control the damage using blunt instruments, even if that means causing some collateral damage themselves.
How is a rational scientist supposed to navigate this environment? Often the answer has been "study something that isn't (politically) radioactive instead". That's not good enough this time.
Replies from: ChristianKl, greylag↑ comment by ChristianKl · 2021-06-13T21:14:57.213Z · LW(p) · GW(p)
Kirsch (blue shirt guy) seems less careful than the other two, and may or may not be a crackpot.
We should still try to verify their claims. Are these guys who they say they are? Do they have valid credentials?
Without having watched the video my prior before this conversation from what Steve Kirsch did before:
Steve Kirsch was listening to Corona virus experts (experts that studied Corona viruses before the pandemic) and organizing funding clinical trials for the drugs those experts considered promising (and invested significant personal money into it). He's one of the few people who scored A+ in 2020 at fighting COVID-19 by being sensible.
When we discuss whether he's a crackpot we should also discuss whether all those people in power who initially said masks don't work listening to think tanks instead of the most qualified experts should be considered crackpots. I think the case for Fauci being a crackpot is a lot better then for Kirsch.
Robert Malone wrote https://www.pnas.org/content/86/16/6077 which is a paper about using mRNA from 3 decades ago. When it comes to inventing mRNA vaccines there were a lot of steps on the way and it's unclear whether any single person should be considered "The Inventor" but he seemed to played part in it.
Replies from: gilch↑ comment by gilch · 2021-07-17T23:12:19.151Z · LW(p) · GW(p)
How safe is the covid vaccine? is making me update toward Kirsch being a crackpot.
Replies from: ChristianKl, DPiepgrass↑ comment by ChristianKl · 2021-07-18T20:52:36.988Z · LW(p) · GW(p)
It's quite unclear why it makes you update about personal instead of the thesis. The vaccines likely don't do as much damage as Kirsch first claimed but that's not the same thing as he being a crackpot.
The article also makes some strange leaps. It assumes that death due to suicide couldn't be due to the vaccine. Lipid nanoparticles get used as a vehicle to transfer drugs through the blood-brain barrier so it's plausible that there are cases were the vaccine goes into the brain, a bunch of neurons expressing spike proteins, getting killed of by the immune system and that leading downstream to suicide in rare cases.
There's the general idea in the post that it's vaccines vs. no vaccines. To the extend that it is it's only because the US government and the EU is not willing to buy and approve Novavax and doesn't maximize vaccinating as many people as possible by giving different options. If the government would have been willing to engage in a non-tribalistic response Bred might have increased overall vaccination at the cost of pushing it back for a few months just like he convinced more people to take COVID-19 seriously.
Ideally the US would also just allow vaccines like RaDVaC but in contrast buying and approving Novavaxx would be easily possible if the NIH, CDC and FDA would be staffed by people who take the pandemic more seriously then tribal fights.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-07-19T04:32:54.285Z · LW(p) · GW(p)
I haven't seen Kirsch advocate for Novavax, does he? Might U.S. officials be thinking to themselves "we bought plenty enough vaccines for everyone already, no need to buy more"? How do you conclude that the mRNA vaccines cross the blood-brain barrier? Do you have safety concerns with the J&J vaccine?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-07-19T10:23:54.980Z · LW(p) · GW(p)
I haven't seen Kirsch advocate for Novavax, does he?
In the linked video, it's quite clear that both Kirsch and Bret are generally pro-vaccine and object to new vaccine technology. They do say in the video that more conventional vaccine technology could be better. They don't speak explicitely about Novavax.
How do you conclude that the mRNA vaccines cross the blood-brain barrier?
mRNA vaccines use lipid nanocoating. That same technology is used in other context to get drugs to cross the blood-brain barrier.
Do you have safety concerns with the J&J vaccine?
Safety-wise I would expect that side-effects follow some distribution. A vaccine that's going to make a substantial portion of the people that take it too ill the next day to work is likely to have more serious bad effects then a vaccine that makes very few people to ill to work the next day.
My safety concerns personally started with Stöcker having nobody of >100 people that he vaccinated being ill the next day. https://www.lesswrong.com/posts/RfdCJZtE7gPisjXFC/how-do-the-side-effects-of-novavax-compare-to-other-covid-19 [LW · GW] was how I was trying to find out whether Novavaxx as a traditional platform manages to have less side-effects and it actually has.
I haven't read about the J&J vaccine side-effects specifically, but even if it would have less safety issues a single dose vaccine is not going to give you the same protection against COVID-19 and that matters.
Generally viral vector vaccines and the mRNA vaccine get your body to attack some of it's own cells in a way that a vaccine where the protein (or subsection) is injected doesn't. There are arguments that this is going to make the vaccine more effective as it allows the immune system to do additional things. It however comes at the cost of the vaccine having more side effects because a few of your cells get actually killed by your immune system.
The results of Novavaxx suggest that this is not needed to have an effective vaccine for COVID-19.
Given the way the economics of drug development work, pharma companies are incentivized to push for a maximum in clinical effects at the cost of side effects because that increases the chances of drug approval. With vaccines that scientists do for their own protection like RaDVaC or Stöcker's vaccines the incentives are the other way around and safety is a primary consideration. It's quite ironic how the FDA's safety processes of requiring those trials give us less safe vaccines.
Might U.S. officials be thinking to themselves "we bought plenty enough vaccines for everyone already, no need to buy more"?
Yes and that would be pretty stupid in a world where people might be willing to take a vaccine with less side-effects then the one's already on the market but not those already on the market.
This both goes for the people who are afraid of missing a day of work after taking the vaccine and those who are concerned about the new technology platforms.
I will still get my second shot with the BioNTech vaccine this week but I'm annoyed that I can't have Novavaxx and might spend 1-2 days without the ability to do anything for no good reason.
Replies from: DPiepgrass, DPiepgrass↑ comment by DPiepgrass · 2021-07-19T20:41:11.585Z · LW(p) · GW(p)
mRNA vaccines use lipid nanocoating. That same technology is used in other context to get drugs to cross the blood-brain barrier.
I'm no biologist, but I know all kinds of things have lipid membranes (including bacteria), so I doubt that simply being lipid-covered is all you need to cross the barrier.
I haven't read about the J&J vaccine side-effects specifically
Well, it's important to Kirsch's position. After all, J&J has 568 deaths attributed to it according to OpenVAERS even though J&J is not mRNA-based (curiously, OpenVAERS is now reporting dramatically higher death numbers for Pfizer over Moderna, whereas they were ~equal one month ago [LW(p) · GW(p)]).
I calculated that according to the latest numbers, 3.9% of vaccines injected were J&J vaccines (which is 8% of people "fully vaccinated" since you only get one dose of J&J).
Now, if my thesis is correct that the VAERS deaths are ordinary deaths that would have happened anyway, then approximately 3.9% of the deaths should be attributed to J&J. In fact, OpenVAERS (updated July 9) assigns 5.2% of deaths to J&J. Does this mean that actually there is a greater chance of death associated with non-mRNA vaccine shots? (well, the numbers are probably 2-3 weeks out of sync with each other, as the VAERS data lags behind. Perhaps this could account for the difference. Historical data is available, but not in an easy-to-read form. So I used the Wayback Machine instead, and found that ... er, 3.8% of vaccine shots had been J&J on July 1. No significant difference.)
The same sort of hypothesis can be applied to non-death VAERS reports, of course, but I leave that analysis for someone else who cares enough to do it.
Yes and that would be pretty stupid in a world where people might be willing to take a vaccine with less side-effects then the one's already on the market but not those already on the market.
Perhaps... but if I'm right, Novavax would end up getting VAERS death reports at roughly the same rate as other vaccines. If most people who are reluctant to take a vaccine are (like my father) getting their beliefs from people like Kirsch who harp on VAERS, Novavax might not end up being perceived as safer even if it is. So a relevant question, I think, is whether we could expect right-wing news outlets to effectively communicate "Novavax has less side effects / is safer" (because I don't think an article in The Atlantic would sway the likes of my dad. edit: so I just Googled "side effects" Novavax site:foxnews.com and the first result is a video subtitled "Kurt 'The CyberGuy' Knutsson tells ‘Fox and Friends Weekend’ how he accidentally joined the Novavax trial coronavirus vaccine and what side effects surprised him the most." The side effects weren't bad, but the anecdotal approach being taken is not encouraging.)
Edit: btw, I totally agree that FDA needs reform, and it certainly wouldn't hurt to deploy small amounts of Novavax to test demand.
Replies from: ChristianKl, ChristianKl, alexey-lapitsky↑ comment by ChristianKl · 2021-07-20T14:47:16.405Z · LW(p) · GW(p)
When it comes to VEARS my main hypothesis is that VEARS used to be pretty bad at actually tracking side effects. One of the key arguments for it being bad is that if you look at history only a minute amount of the side effects that you would expect given what happens in clinical trials end up in VEARS.
It's likely that some people who are responsible for VEARS thought that it's very important that it's good at picking up on side-effects given how we deployed the vaccines and the increased amount of VEARS cases is simply because the system was improved to get doctors to report cases more often.
Unfortunately, the sphere of people who are interested in making that argument is quite small given that it's about admitting past flaws in vaccine safety.
↑ comment by ChristianKl · 2021-07-19T22:51:31.980Z · LW(p) · GW(p)
I don't think that Kirsch is as focused on VAERS as you assume. Kirsch is a VC for whom strong opinions-loosely held is central. That's why he could easily switch from running an NGO that has vaccination as part of it's mission to speaking up against the vaccines.
The article in The Atlantic won't convince your dad but "we should use Novavaxx instead of mRNA vaccines" is a contrarian position that's open to be argued especially when it's an actual choice for people to take. It won't be argued by real antivaxxers like Mercola but there's no reason for it not to be argued by Chris Martenson, Steve Kirsch or Bret Weinstein. It also makes a good story for Tucker (for Tucker it doesn't even need to be true to make a good story).
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-09-25T18:36:30.980Z · LW(p) · GW(p)
So, my dad is continuing to refuse vaccines, and while he's not naming any of the people he trusts on this issue, one of his claims is about "infertility" and the only original source of infertility claims I'm aware of is Steve Kirsch. So I'd like to ask for your perspective on this.
Kirsch was praised by Bret Weinstein for continuing to update his anti-vax article as he found new information. And yet, Kirsch's headline claim about the danger of vaccines - the very first claim he makes, the claim that the vaccines "likely killed over 25,800 Americans" - was retracted on June 18 by the person to whom Kirsch linked as evidence of that claim, Austin Walters. Walters also explained why his claim was wrong. But Kirsch didn't change the beginning of his article at all. So Kirsch was supposedly keeping his article up-to-date, but he made an exception for the 25,800 deaths claim (and then, of course, he removed his name from the article and other names including Robert Malone appeared instead.)
Also, Steve said this: "Biodistribution of lipid nanoparticles which carry the mRNA show that the ovaries get the highest concentration" ... but this is clearly untrue [LW(p) · GW(p)].
My question is, does this reduce the credibility you attach to Steve Kirsch and Robert Malone? If not, why not?
Also, do you know of any other original (not parroted) sources of infertility claims other than Steve Kirsch?
(On the other hand, if it does reduce their credibility... Yuri Deigin says he was a friend of Bret Weinstein before all of this started, and says that he told Bret about how Steve was misreporting the data re: ovaries (among other things). Do you know if Bret has ever backpedaled about this claim or otherwise distanced himself from Steve Kirsch? And if not, does it speak to Bret's credibility?)
Replies from: ChristianKl↑ comment by ChristianKl · 2021-09-26T07:15:38.390Z · LW(p) · GW(p)
Even if what Steve is saying about the vaccines producing problems in the ovaries which can cause infertility would be true, that shouldn't matter to your dad because he doesn't have ovaries. I haven't heard any claims for male infertility.
Also, Steve said this: "Biodistribution of lipid nanoparticles which carry the mRNA show that the ovaries get the highest concentration" ... but this is clearly untrue [LW(p) · GW(p)].
My question is, does this reduce the credibility you attach to Steve Kirsch and Robert Malone? If not, why not?
My view of Kirsch is at the moment is that he strongly pattern matches and this seems to both result in fast detection of issues and also in overmatching and seeing patterns where there are none.
Here there's more concentration in the ovaries then in most other tissues according to the EMA documents but saying it's the highest concentration is overstating it.
Generally, I haven't meet anyone who had clear negative consequences from the vaccine in the way Kirsch describes so I find the thesis that the side effects are so common falsified.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-09-26T10:55:40.880Z · LW(p) · GW(p)
I take that as a no. That is, you judge his specific hypotheses but refrain from judging his credibility.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-09-26T13:47:49.358Z · LW(p) · GW(p)
Credibility is a quite complex thing. There's a tradeoff between taking no action and requiring a lot of evidence and taking action based on too little evidence.
Besides the lying one of the problems with people in the establishment like Fauci is that they require a lot of evidence and as a result we still haven't updated our vaccines to the delta spike protein. Kirsch is one the other hand of that spectrum.
Taking a lot of bets and not needing all to payoff is likely what makes him a good venture capitalist. I do think it's worthwhile to listen to people on all parts of that spectrum.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-09-26T15:23:53.132Z · LW(p) · GW(p)
Steve appears to have two separate and very different evidence thresholds. In the "25,800 deaths" case, he accepts evidence in one direction readily while ignoring evidence from the same source in the other direction.
Also, he should have known that the ovaries statement was false from the first time he said it (and the fact that he chose neither to show the original source data, nor link to it, nor even be specific about where he got the information, suggests that he knew what he was doing.)
It's puzzling that your analysis ignores the facts I put before you.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-09-27T15:19:55.402Z · LW(p) · GW(p)
Steve appears to have two separate and very different evidence thresholds. In the "25,800 deaths" case, he accepts evidence in one direction readily while ignoring evidence from the same source in the other direction.
Anyone who's serious about medicine has different evidence thresholds for risks and safety of drugs. That's why the FDA takes a lot of evidence to allow a new drug to be marketed while at the same time withdrawing a drug from market.
Replies from: DPiepgrass, DPiepgrass↑ comment by DPiepgrass · 2021-09-30T16:20:45.395Z · LW(p) · GW(p)
I just learned that my Dad's unvaccinated brother died with Covid-19 yesterday.
One thing I didn't mention before was that my Dad knew his brother was in hospital with Covid on a ventilator, and still refused to take a vaccine because he claims it has caused "100,000" deaths (plus justifications that don't apply to him, like "infertility!" and "harms children!").
Now I suppose Kirsch isn't the one using the number 100,000; he was saying 25,800 four months ago and now the Malone/Kirsch/etc group is saying things like this:
[...] the death toll is over 40,000 people.
[...] the vaccine is more likely to kill you than save you. For example, Pfizer’s own study showed deaths from COVID were reduced by a factor of 2, but this saving was more than offset by deaths from cardiac arrest which went up by 4X.
(Of course, the details of both of these claims are behind a paywall, though the first one was published before the paywall went up so interested parties can see it on the Wayback Machine. I googled for a little while for these claims, finding Snopes and Politifact reporting "False" and "pants on fire" for a claim of 45,000 deaths, though I found no one else making or analyzing the second claim, just NYT saying "Heart Problem More Common After Covid-19 Than After Vaccination". FWIW I got a new permanent heart problem after contracting Covid and before getting the vaccine, but there's a strong chance it's unconnected.)
Regardless of who said "100,000", Kirsch helped get the ball rolling, and now my uncle and former legal guardian is dead.
But people like you, and probably even my Dad, can't bring themselves to consider that maybe, just maybe, Kirsch et al are not acting in good faith (or are otherwise epistemically compromised). Why is that? I really can't fathom it. I mean, sure, there's outgroup hate and ingroup love, but to risk your life without allowing even a seed of doubt in your mind that you could be wrong?
Replies from: Benito, ChristianKl↑ comment by Ben Pace (Benito) · 2021-09-30T18:10:10.771Z · LW(p) · GW(p)
I'm sorry to hear about your uncle, DP.
↑ comment by ChristianKl · 2021-09-30T17:13:29.812Z · LW(p) · GW(p)
I really can't fathom it. I mean, sure, there's outgroup hate and ingroup love, but to risk your life without allowing even a seed of doubt in your mind that you could be wrong?
I'm vaccinated. To the extend that I'm making currently choices about risking COVID-19 it's a combination of not ordering Ivermectin from India, not taking my taffix and chosing to go to events where there are other people.
I'm thinking I'm arguing for more doubt on most of the major issues involved. The expecation is the lab leak hypnothesis where I think there's less doubt than many other people but that's not directly medical policy.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-09-30T19:33:15.510Z · LW(p) · GW(p)
Kirsch is also fully vaccinated. You're still deflecting not answering the questions I ask.
↑ comment by DPiepgrass · 2021-09-28T17:45:55.916Z · LW(p) · GW(p)
Lest you forgot, the two pieces of evidence in question are the assertions (1) "X" and (2) "my assertion X was wrong and here's why" on the same blog post. You're saying it is reasonable to conclude from (1) and (2) that X is true.
Moreover the blog post is written specifically by a fan of Kirsch (it linked back to Kirsch for its claim that "the Pfizer mRNA vaccine will have the highest concentration in the ovaries and bone marrow") so Kirsch should have no reason not to trust (2).
↑ comment by Alexey Lapitsky (alexey-lapitsky) · 2021-07-21T18:39:51.297Z · LW(p) · GW(p)
even though J&J is not mRNA-based
The core point is that even J&J is not a traditional vaccine. It's also genetic (DNA-based) with a classic non-LNP delivery mechanism using an adenovirus. From what I understand, it penetrates a different subset of cells (using ACE receptors, afaik) that get killed by the immune system in the same way as with mRNA-vaccines.
↑ comment by DPiepgrass · 2021-12-30T00:01:52.682Z · LW(p) · GW(p)
They don't speak explicitely about Novavax.
Kirsch has now done so in his article "15 things everyone needs to know about COVID". The first thing he says everyone needs to know is "Avoid all the COVID vaccines, even Novavax. The data shows that these vaccines kill more people than they save."
↑ comment by DPiepgrass · 2021-07-18T01:52:19.331Z · LW(p) · GW(p)
Yes, particularly this bit:
Austin Walters issued a correction to his blog post, after seeing this problem. Steve Kirsch took 25 minutes of debate before giving some half-hearted concession that his claim probably isn’t true. He still hasn’t updated his own writing or videos, and continues to tell people that the vaccine is causing mass casualties.
I have been criticizing Kirsch (and Lawrie) for not considering more than one hypothesis that could explain the data. But it's likely to be much worse: that people are going to him with better explanations and he chooses to ignore them. Classic denier: one who does not respond to evidence (unless confirmatory).
But charitably, maybe nobody's going to him with good arguments. Like, I randomly listened to a little of that 5-hour debate with Avi. At 36:11 Steve asks Avi what caused those deaths in VAERS and Avi's first thought is to suggest that maybe there's lots of false reports, based on just one example of a false report? ugh. (I looked at 37 reports elsewhere in this thread and didn't suspect any of them were simply made up. I did wonder if sometimes multiple reports sometimes happened for the same person, but didn't try to check.) Edit: or extra charitably, Steve's totally found good answers to the issues I raised and I just never happened to see evidence of that.
↑ comment by greylag · 2021-06-13T10:13:23.318Z · LW(p) · GW(p)
Whether or not this case has merit, the systematic censorship thing seems real to me... when the antivaxxers have a point, the mainstream isn't allowed to admit it
”Social media trying to tackle disinformation with blunt instruments and causing collateral damage” seems to me very much true. Censorship of information about side-effects…? Well, it seems like “the covid vaccine makes you feel terrible 24-48 hours afterwards for some people” seems like common knowledge; I’m sure I’ve been advised after the flu vaccine to stay still & nearby for ten minutes to check I don’t react badly to it. More pointedly, the low-but-detectable-risk-of-blood-clots problems with the adenovirus vaccines resulted in rollout of those vaccines being paused/delayed by some countries for certain demographic groups, and while there was controversy about what was justified (pause vaccine rollout? Only give those vaccines to older people at less risk of blood clots?), “systematic censorship” is not an accurate description of what was happening.
Replies from: gilch↑ comment by gilch · 2021-06-13T19:08:28.445Z · LW(p) · GW(p)
Informed consent is important. I don't recall being informed about accumulation in bone marrow or ovaries, or the risk of myocarditis or the risk of brain fog at the time I got my shots. Maybe some of these side-effects weren't known at the time. But that the vaccine didn't stay in the muscle and therefore might have systemic effects was news to me, and they're asserting that this was known at the time.
I've been experiencing persistent palpitations recently. It had not occurred to me that this could be due to the vaccine until I watched this video. I believed the mainstream line that the vaccines are safe and effective. I still think they're effective. The evidence for that is very strong. I'm less confident that they're safe now.
Confirmation bias is a serious concern when reactions are this delayed though. People develop health issues all the time for all sorts of reasons. If they're primed to think the vaccine could have long-term side effects, they'd probably attribute all sorts of things to the vaccine that are mere coincidence. So individual anecdotes are pretty weak evidence, but this noisy data is still worth collecting to see if any patterns emerge. On the other hand, if we've all been primed to think the vaccines are safe (and we have been), then we won't make the connection at all and don't even report the data, and this is one of the main concerns from the video. The issue has become too politicized for society to be objective about it. Legitimate concerns get you labeled as an antivaxxer.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-13T21:03:49.683Z · LW(p) · GW(p)
Yes, as I said in my letter to my dad: elderly people already die often (big number nationally), so if vaccines are being given to millions of elderly people, we should expect a tiny percentage to die soon afterward from natural causes. A key thing to look at is whether it used to be rare (and in 2021 became common) to give the vaccines to ill elderly people, which could explain the increase in VAERS.
Still, why are blood clots given lots of attention but not VAERS reports? And if the FDA is so understaffed, why?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-06-15T00:10:53.807Z · LW(p) · GW(p)
Blood clots are not independent from VEARS reports. VEARS reports are how the FDA gets the data about the Blood clots.
The VEARS reports give them reports about many different kinds of issues and if there are many issues to look into and they are understaffed it's reasonable to put more attention on the blood clots issue then other issues given that blood clots in the brain are a serious issue.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-15T19:01:24.092Z · LW(p) · GW(p)
How is it more reasonable to focus on VAERS blood clots than VAERS deaths?
Replies from: Lukas_Gloor, ChristianKl↑ comment by Lukas_Gloor · 2021-06-15T19:19:02.750Z · LW(p) · GW(p)
One obvious candidate explanation: For the reason you explain in the letter to your dad – probably those deaths were roughly what you'd expect among the vaccinated demographic if the vaccine is benign. By contrast, the specific blood clots are generally rare.
↑ comment by ChristianKl · 2021-06-15T22:03:30.693Z · LW(p) · GW(p)
Because you rather focus on investigating the thing that causes the most deaths then investigating deaths in general.
comment by [deleted] · 2021-06-13T21:48:04.123Z · LW(p) · GW(p)
While I agree that there is insufficient attention paid to ivermectin as a possible treatment in Western nations, I have seen far too much shoddy and conflicting data in the studies that are brought forward proposing it as prophylaxis and think the hype is a spiral that has amplified nonsense into prominence. People LOVE the idea of a panacea. While there is quite possibly something interesting going on there it has been hyped to the moon and back in a way it should not be.
The animal data I have seen that I trust the most (since it avoids many of the pitfalls of observational trials, and few people are doing randomized trials that are actually good and not shoddy as hell after chloroquine sucked all the oxygen out of the room) suggests there could be something there, but not in a way that would block epidemics. Animals that are infected and then dosed have no difference in viral levels but recover their sense of smell significantly faster and when you take tissue samples the levels of inflammatory and tissue-destroying signaling molecules are lower while the ones that are more classically associated with antiviral responses are higher. Leans me towards the idea that it could decrease severity and odds of falling into downwards spirals. I have been following the in vitro work on this from the beginning and my conclusion is that you're probably looking at immunomodulatory effects that can help you not fall into the pathological attractors, and deal with long infections better, rather than doing anything about viral binding or replication, if any of it pans out.
See, as an example, https://www.biorxiv.org/content/10.1101/2020.11.21.392639v1.full
This being said, given the safety profile of the drug I say the risk to reward ratio is pretty good if you pay close attention to contraindications and I see no reason for it to not be used and studied more.
With regards to repurposing drug studies being almost impossible, I am much much more angry that there are no good studies, and no studies at all outside India, for indomethacin. A much more promising and well defined antiviral mechanism there against cytoplasmic RNA viruses via host factors that works STUNNINGLY well on canine intestinal coronaviruses in vivo, and sars and sars-2 in culture, and when you dig carefully through the literature being already on it by prescription is associated with much lower covid hospitalization risk.
Replies from: mngreen↑ comment by mngreen · 2021-06-14T03:49:22.747Z · LW(p) · GW(p)
My reading on ivermectin is that the concentrations required to be effective outside of in vitro would be extremely high. For what it's worth, here are a few articles. Science is an evolving understanding of complex systems. Time and testing will tell.
"Laboratory studies using monkey cells in a test tube (as opposed to clinical studies in human patients) have shown ivermectin can shut down the replication of SARS-CoV-2, the coronavirus that causes COVID-19, within 24-48 hours of exposure to the drug.
Ivermectin is thought to inhibit the virus by preventing viral proteins moving in and out of the host cell’s nucleus, which is essential for replication of the coronavirus.
The problem is this process requires very high concentrations of ivermectin – well above the recommended dose for humans. This means ivermectin’s virus-killing powers would be unlikely to be harnessed inside the human body."
(there are several linked references from within the article as well)
This next link is excellent - it delves into the molecular science w/out becoming incomprehensibly dense and there are three updates appended to the end showing promise.
https://blogs.sciencemag.org/pipeline/archives/2020/05/11/whats-up-with-ivermectin
Another very useful article:
mng
Replies from: None, Dentin↑ comment by [deleted] · 2021-06-14T19:14:14.301Z · LW(p) · GW(p)
The mechanisms stopping growth in vitro at obscene concentrations I agree are probably not operative in vivo, or at the very best not in the same way. However there are other bits of data regarding the drug as an immunomodulator in other viral infections, and this virus in particular has much of its pathogenesis having to do with badly regulated immune reactions.
Basically I am at the awkward position where I think the risk to potential reward ratio is favorable and that good research is needed while thinking most of the existing research is super shoddy.
↑ comment by Dentin · 2021-06-14T20:41:56.871Z · LW(p) · GW(p)
One other thing to consider is that even small differences in replication rate might actually matter. Consider that it takes a week for the virus to really ramp up, and that's a large number of doubling periods. Even just getting a larger or smaller initial dose seems linked to how sick people get. Even a few percent difference may allow the immune system to stay ahead in the arms race, and result in a nonlinear change in death rate.
Note that I'm not saying this happens; I'm saying that because this is an exponential growth attacker (the virus) versus and exponential growth responder (the immune system), even small differences in growth rates might have a large impact.
comment by Vanilla_cabs · 2021-06-13T07:34:14.041Z · LW(p) · GW(p)
Could you make a digest of their main points? That might help get everybody on the same page to start the discussion.
Edit: Ok, TBH, I just don't feel like watching a 3-hour long video ATM. But others might prefer to have the original debate in full rather than a digest.
Edit 2: Thanks for listing noteworthy points. I'm in the process of passively listening to the video bit by bit.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-13T11:31:27.960Z · LW(p) · GW(p)
Okay, I'll review the video again and add a list of controversial and interesting bits.
comment by DPiepgrass · 2021-06-17T00:26:44.844Z · LW(p) · GW(p)
So, I decided to head on over to OpenVAERS, do some searches and look at some reports. Here are the number of results for a few queries for deaths in 2021:
5997 results in 2021 (all vaccines)
5869 results in 2021 with Vax Name "covid19"
3607 results in 2021 for 65+ (all vaccines)
3543 results in 2021 for 65+ with Vax Name "covid19"
1673 results in 2021 for 65+ with Vax Name "moderna"
1691 results in 2021 for 65+ with Vax Name "pfizer"
165 results in 2021 for 65+ with Vax Name "janssen" (Johnson & Johnson)
1061 results in 2021 for <65 (all vaccines)
1023 results in 2021 for <65 with Vax Name "covid19"
406 results in 2021 for <65 with Vax Name "pfizer"
458 results in 2021 for <65 with Vax Name "moderna"
214 results in 2021 for <45 with Vax Name "covid19"
101 results in 2021 for <35 with Vax Name "covid19"
37 results in 2021 for <25 with Vax Name "covid19"
Edit: for comparison, the average annual death rate in the United States in 2018 and 2019 was 719 per 100,000 or 0.719%. Since the population is about 328 million, the expected number of deaths in a normal year is about 2,358,000, and in a typical week, 45,228. Now, 51.56% of the population has received at least one vaccine shot as of June 10 (one week ago). Therefore, if it were the case that someone filed a VAERS report for every death that was not caused by the vaccine but happened within one week of vaccine administration, we would expect to see much more than 5869 death reports, perhaps 23,300 (or higher, because some people have received multiple vaccine shots and because older people are more likely to have been vaccinated). This is relevant because I read that "FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS", which explains why we see e.g. two deaths by gunshot wound in my roundup below.
Since there are only 37 deaths nationwide for age 24 and under, I decided to summarize all of them. Because I could. At least in this category we can rule out age-related illness. I will put the actual summaries of these reports in a separate message in the hope that LessWrong's display algorithm will be more likely to "collapse" that information.
I have divided these deaths into mutually exclusive prioritized categories. This means that if a death was in both categories B and D, I only listed it under category B which is listed first.
- Suicides: 4 (though in one case the person was also ill)
- Other reports with indications that the death is probably not vaccine-related: 2
- Death reports more than 14 days after vaccine: 4
- No information about time between vaccine and death: 1
- Death within 14 days, but serious pre-existing illness: 8
- Death within 14 days, seemingly no serious pre-existing illness: 2
- Death within 14 days, level of pre-existing illness unclear: 16
Most of the "within 14 day" reports were also within 7 days.
An interesting indicator would be how many people are getting each vaccine. If the numbers of deaths for each vaccine is exactly proportional to the number of people receiving each vaccine, it would suggest that the vaccines are all equally safe, and if so, the most probable safety level is "very safe". (wrinkle: if e.g. J&J is a 'rising star', the death report curve is likely to lag behind the vaccination rate curve.) But where do I find that data?
Replies from: DPiepgrass, sil-ver, DPiepgrass↑ comment by DPiepgrass · 2021-06-17T00:27:43.230Z · LW(p) · GW(p)
Detailed summaries:
Suicides
- 958443 - self inflicted gun shot wound
- 1243487 - VAX DATE: 13 April 2021 | DATEDIED: 21 April 2021 - Patient Committed Suicide with a firearm.
- 1307657 Death by suicide [4 days after taking vaccination]
- 1349598 VAX DATE: 19 April 2021 | ONSET DATE: 19 April 2021 | DATEDIED: 23 April 2021 - he was COVID positive... patient did not have COVID prior to vaccination [sic].... patient...received the first dose of...PFIZER...on 29Mar2021... headache, sore arm, lethargic.... 19Apr2021, the patient received the second dose, and the patient was sick that day, headache/tired, diarrhea. On Tuesday (20Apr2021), the patient slept all day, headache, chills, diarrhea, no appetite, said he didn't feel right.... Friday (23Apr2021) diarrhea - took his own life by hanging himself. The patient did not have history or signs of depression, anxiety, or mental illness.
Other reports with indications that the death is probably not vaccine-related
- 1166062 - DATEDIED: 20 March 2021 - patient received second dose of Pfizer vaccine on March 17, 2020 while at work... her 5 month old breastfed infant developed a rash and within 24 hours was inconsolable...developed a fever. Patient brought baby to local ER... passed away. Diagnosis of TTP. [It sounds like the baby did NOT receive a Covid vaccine]
- 1347547 VAX DATE: 15 April 2021 | ONSET DATE: 16 April 2021 | DATEDIED: 21 April 2021 - The injury that led to the death occurred within 1 day of the decedent receiving the vaccine
Deaths more than 14 days after vaccine
- 1076949 - VAX DATE: 29 January 2021 - Patient admitted on 2/21/21 and died in hospital on 2/22/2021. Patient had a significant, lifelong underlying medical condition.
- 1074788 - [This report appears to be for a fetus that died more than a month after the mother received the vaccine]
- 1372120 - VAX DATE: 01 May 2021 | ONSET DATE: 01 June 2021 | DATEDIED: 01 June 2021 - Pt called 911 for shortness of breath...Patient with sob, saying she can not breath , states it came on suddenly about a half hour ago and pt has not been feeling ill prior to this... became pulseless and apneic... no medical history other than anemia... J and J covid 19 vaccine recently. ... copious amounts of vomit, suction enroute to ed.
- 1366320 - VAX DATE: 10 March 2021 | ONSET DATE: 11 March 2021 | DATEDIED: 06 May 2021 - he died [Jesus Christ, that's all you have to say?]
No information about time between vaccine and death
- 1353097 - On an unknown date, the patient received second dose...Moderna...1 dosage form. On an unknown date, the patient experienced CARDIAC ARREST... It is unknown if an autopsy was performed... Follow up not possible as no contact details available
Death within 14 days, but major pre-existing illness
- 960841 - VAX DATE: 17 January 2021 | ONSET DATE: 19 January 2021 | DATEDIED: 21 January 2021 - 104.4 temp approximately 48 hours after being given the vaccine....treated with antibiotics, IV fluids, cooling methods...cardiac arrest on 1/21/21. HISTORY: ventilator dependent, anoxic encephalopathy, seizure disorder. OTHER_MEDS: Amantadine, clonazepam, clobazam, lovenox, dextroamphetamine-amphetamine, famotidine, gabapentin, keppra, robinul, polyethylene glycol, propanolol, sertaline, senna, valproic acid, vimpat, cefepime
- 1105115 - VAX DATE: 14 February 2021 | DATEDIED: 28 February 2021 - POC observed abscesses in the arm, groin, thigh and knees after the first vaccination. After the second dose, he was hypoactive. ...POC removed the sheet, she observed that her mouth and nose were full of secretions. HISTORY: Portal hypertension (secondary to portal vein thrombosis), Leukopenia, Thrombocytopenia, Epilepsy, Splenomegaly, Esophageal Varices, Asthma, Pancytopenia and Severe mental retardation.
- 1105146 - VAX DATE: 30 January 2021 | ONSET DATE: 30 January 2021 | DATEDIED: 02 February 2021 - 1/19 began vomiting and was hospitalized. On 1/30 he was discharged and later received the vaccine.... [later] He started coughing up foul-smelling secretions.... HISTORY: Epilepsy, Hydrocephalus, and Multiple Sclerosis
- 1199455 VAX DATE: 02 April 2021 | DATEDIED: 10 April 2021 - Patient reported difficulty breathing and chest pain... cardiac arrest... HISTORY: spina bifida, spinal meningocele, VP shunt, scoliosis, neurogenic bladder, constipation
- 1273475 VAX DATE: 28 April 2021 | DATEDIED: 29 April 2021 - Resident was checked at 1830 and found to be at baseline status. At approximately 1855, resident was found pulses and apneic. CPR initiated... Resident expired 1939. CUR_ILL: Anoxic Brain Injury, History of MI, Uterine rupture, dysphagia, PEG TUBE, Tracheostomy. HISTORY: Anoxic Brain Injury
- 1343614 VAX DATE: 18 May 2021 | ONSET DATE: 20 May 2021 | DATEDIED: 24 May 2021 - presented to ED dept confused, incr n/v, weakness. Received palliative care... deceased. CUR_ILL: fibrolamellar hepatic carcinoma with metastatic disease OTHER_MEDS: xarelto, methadone, morphine, prochlorperazine, lorazepam, ondansetron, protonix
- 1349127 - VAX DATE: 19 March 2021 | DATEDIED: 04 April 2021 - Concurrent medical conditions included Traumatic brain injury, Movement disorder, Seizures (since she was a baby at 11 months old) and Speech loss. Concomitant products included CLONAZEPAM, OXCARBAZEPINE (TRILEPTAL) and GABAPENTIN for an unknown indication.... cause of death was not reported. An autopsy was not performed.... death certificate said... natural causes.
- 1365075 - VAX DATE: 10 March 2021 | ONSET DATE: 12 March 2021 | DATEDIED: 19 March 2021 - father said his son began throwing up 2 days after injection. They took him to the ER and patient was given some medication to stop emesis... Patient was reported to throw up everyday until his death on day 9. HISTORY: Cerebral Palsy legally blind Epileptic Seizures deteriorating bones in hips Hydrocephalus Shunt in head
Death within 14 days, no major pre-existing illness
- 1121695 - VAX DATE: 10 March 2021 | 01 March 2021 (sic) ...no significant past medical history...very severe diabetic ketoacidosis one week after receiving the vaccine...severe metabolic encephalopathy, aspiration pneumonia...
- 1255787 - DEATH; BLOOD COAGULATION...the patient was very healthy...date not reported for...vaccination...On an unspecified date...patient developed blood coagulation...patient subsequently died 10 days after vaccination; the cause of death was not provided...
Death within 14 days, seriousness of pre-existing illness is not clear
- 1067765 - VAX DATE: 08 February 2021 | DATEDIED: 08 February 2021 - died in his sleep through the night; This is a spontaneous report from a contactable consumer received via a Pfizer sales representative... Medical history included muscular dystrophy. HISTORY: ...Muscular dystrophy [This report is confusing: it says he received the vaccine Feb 8 and died the same day, even though he died in his sleep?]
- 1078352 - VAX DATE: 02 March 2021 | DATEDIED: 05 March 2021 - Developed fatigue, body aches, headache 1 day after vaccination on 3/3. The morning of 3/5 complained of chest pain. Took Tylenol at 8:30 am. At 10:30 am his family found him unresponsive.
- 1140258 - VAX DATE: 26 March 2021 | DATEDIED: 27 March 2021 - Patient contacted 911 complaining of not feeling well and difficulty breathing... patient was found by EMS in cardiac arrest.
- 1187918 I am the PICU attending who cared for the patient after her cardiac arrest which we believe was about 3-4 days after her second Moderna Vaccine
- 1198540 VAX DATE: 01 April 2021 | DATEDIED: 11 April 2021 - Patient...unresponsive and not breathing...outside on the grounds of the campus. A rented scoter was next to him... There was no sign of trauma.
- 1204016 VAX DATE: 09 April 2021 | DATEDIED: 13 April 2021 - HE DIED SUDDENLY !!!!! JUST COLLAPSED !!!! [that's the entire description]
- 1206323 VAX DATE: 10 April 2021 - Pt received vaccine at 1130 on 4/10... Awoke at approx 0100 4/11, reported not feeling well, vomited, returned to bed. Found by housemate at appox 2100 4/11 unresponsive.
- 1209903 VAX DATE: 06 March 2021 | DATEDIED: 13 March 2021 [no symptoms, story or history provided]
- 1225942 VAX DATE: 19 March 2021 | ONSET DATE: 28 March 2021 - cardiac arrest at home... Patient placed on ECMO and imaging revealed bilateral large pulmonary embolism
- 1242573 VAX DATE: 18 April 2021 | ONSET DATE: 19 April 2021 | DATEDIED: 20 April 2021 - Heart failure
- 1243791 - VAX DATE: 10 April 2021 | DATEDIED: 12 April 2021 - found dead...at his home. HISTORY: History of clotting disorder at age 16 with Xarelto treatment and hospitalization
- 1261766 VAX DATE: 08 April 2021 | DATEDIED: 10 April 2021 - increased body temperature, seizure, death
- 1321517 VAX DATE: 30 April 2021 | DATEDIED: 01 May 2021 - He did not told me about any symptoms. He just died the next day of the vaccine.
- 1346657 VAX DATE: 18 February 2021 | DATEDIED: 19 February 2021 - deceased in bed, no known symptoms, undetermined cause and manner of death
- 1355039 VAX DATE: 22 May 2021 | ONSET DATE: 23 May 2021 | DATEDIED: 25 May 2021 - Cardiac Arrest
- 1372338 - VAX DATE: 21 May 2021 | ONSET DATE: 21 May 2021 | DATEDIED: 22 May 2021 - HISTORY: Asthma Anxiety/Depression/Panic
↑ comment by Rafael Harth (sil-ver) · 2021-06-19T11:22:36.641Z · LW(p) · GW(p)
This is relevant because I read that "FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS"
How does this square with OpenVaers's claim that only about 1% of injuries are reported?
Without knowing the reporting rate, it's difficult to interpret the data. If we take the 1% and 5869 numbers at face value, it implies that the vaccines killed about 560.000 people, whereas if we assume 100% reporting rate, it looks like they're an amazing preventer of unrelated causes of death. Is there any reasonable way to estimate what % to use?
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-19T19:26:51.599Z · LW(p) · GW(p)
(Edit: a more direct answer to this question, according to this page, is that the "1%" claim comes from misreading a report conducted before 2010 called "Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS)". This was not a report about vaccines, and (being a misread) it was never true. Regardless, it makes sense that the rules about reporting deaths would be more strict than the rules for reporting minor side effects.)
Well, Google led me to the HHS VAERS FAQ which says
Healthcare providers are required by law to report to VAERS:
- Any adverse event listed in the VAERS Table of Reportable Events Following Vaccination that occurs within the specified time period after vaccination
- An adverse event listed by the vaccine manufacturer as a contraindication to further doses of the vaccine
Healthcare providers are strongly encouraged to report:
- Any adverse event that occurs after the administration of a vaccine licensed in the United States, whether or not it is clear that a vaccine caused the adverse event
- Vaccine administration errors
Vaccine manufacturers are required to report to VAERS all adverse events that come to their attention.
Covid vaccines aren't explicitly mentioned in the PDF so the final list of reporting requirements seems to apply ("Any new vaccine recommended by the [CDC] for routine administration to children"):
A.Shoulder Injury Related to Vaccine Administration (7 days)
B. Vasovagal syncope (7 days)
C. Any acute complication or sequelae (including death) of above events (interval - not applicable)
D. Events described in manufacturer’s package insert as contraindications to additional doses of vaccine (interval - see package insert)
Interesting, this isn't as clear as the CDC's statement that "FDA requires healthcare providers to report any death..." Now, if the FDA/CDC/HHS sent memos/bulletins/checklists to hospitals/clinics, these might be the sorts of instructions that front-line staff pay the most attention to. But, don't know how to see those.
↑ comment by DPiepgrass · 2021-06-18T00:24:55.451Z · LW(p) · GW(p)
An odd fact: search results on OpenVAERS disagree with this claim:

It says there were 4561 deaths for "covid vaccines" as of May 28 and less than 210 every year before 2021. But as of June 17, OpenVAERS disagrees (note: OpenVAERS says its data is "through June 4, 2021"):
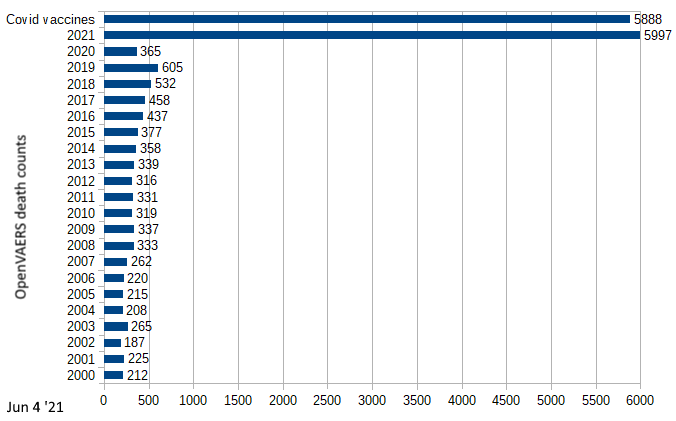
In OpenVAERS there is an upward trend since 2012 that peaks at 605 deaths in 2019. So while the covid death counter has increased 29% in this dataset (possibly due to the passage of time), it also shows 234% more deaths in 2019. Not sure what to make of this.
Replies from: ndr↑ comment by ndr · 2021-06-18T09:58:39.648Z · LW(p) · GW(p)
Thy disagree, but in which direction? The second chart seem to report numbers higher than the first chart but I'm not sure they are about the same data. What's your read? Can you put some links for the second graph source?
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-18T21:54:17.952Z · LW(p) · GW(p)
I constructed the second graph manually, by recording the number of results of 22 queries at OpenVAERS. OpenVAERS (which I learned about through Steve K) says it provides the same data as the government.
Edit: I'm inclined to think that a major reason that the number for 2021 is higher in my chart is because I produced my chart 3 weeks later. As of Jan 17 2022, the number of deaths reported by OpenVAERS for "covid19" in 2021 is 21,427, giving an average rate of 412 weekly death reports. I was surprised to learn that only 46% of these were for age 65+, but it turns out that only 16% of these are for under age 65, so apparently 38% of the deaths occurred in people with no age whatsoever. Also, while the number of death reports is greater in the second half of the year, there has been a dramatic increase in ageless death reports since June. Hmm... it seems like about 15,558 of the reports were filed since I last checked in June, of which about 6800 of the new reports are ageless (44%). That is pretty weird. And indeed, the first report I clicked on at random, said that a person of unknown age and gender in an unknown state, with unknown medical history, suffered from an unknown cause of death on an unknown date after taking a JANSSEN vaccine! I don't think this is what Weinstein and Kirsch had in mind when they talked about underreporting!
comment by ndr · 2021-06-16T09:36:10.256Z · LW(p) · GW(p)
The whole video is painful to watch, it gets more bearable after the 2:11 mark when Kirsch (the blue shirt guy) slows a bit down.
The following is a recap of what I've understood them saying and some unpacking. I'm not educated in anything medical and still have a bunch of open question. If you spot any error or know the answer to these questions please let me know.
TL;DW
They seem to be making 3 main points:
- Ivermectin prevents and treats SARS-CoV-2. It's extremely safe, common and cheap.
- Vaccines were rushed. Long term adverse reactions are unknown, some adverse reactions are now noticeable and worrying.
- Pharmaceutical companies have economical incentives to push for new drugs/vaccines and against out of patents ones. These incentives are skewing media reporting, social media policies and basic research to push pro-vaccine content, and to censor warnings on vaccine safety or potentially safer drug alternatives that might result in vaccines losing their Emergency Use Authorization (EUA).
Bret Weinstein's idea to solve the issue is to find some deep-pocketed sense-making individual or set of people who can buy the pharmaceutical companies out. He thinks that would kill the economical incentives and allow sense to be made.
That was, I think, a fair representation of what they were trying to say and I don't necessarily buy any of it.
Before I try to unpack it note that I've listened to Bret (the host) a fair bit, and he has a positive influence on my priors.
Robert Malone: I didn't know anything about him until I watched this. He sounds balanced, knowledgeable and well connected. His historical involvement with mRNA vaccinology checks out. His recent gigs are way less transparent.
Steve Kirsch: sounds obnoxious and cranky. I'd tend to be dismissive but both Malone and Weinstein seem to see past his style and to agree on his content. From the conversation it seems he's well off and financed some trials on Fluvoxamine out of his own pocket.
1. Ivermectin
It's many smallish studies, and if you think their biases cancel out you come out thinking an effect cannot be there by chance. I don't know of any big study, but at this point I buy that IVM is unreasonably good.
The probability that an ineffective treatment generated results as positive for the 55 studies to date is estimated to be 1 in 23 trillion (p = 0.000000000000043). The consistency of positive results across a wide variety of cases has been remarkable. It is extremely unlikely that the observed results could have occurred by chance.
Source: The mechanisms of action of Ivermectin against SARS-CoV-2: An evidence-based clinical review article, on Nature's The Journal of Antibiotics, quoting ivmmeta.com which collects a bunch of studies.
Other resources:
- Ivermectin for prevention and treatment of COVID-19 infection: a systematic review and meta-analysis, another metastudy by Bryant and Lawrie
- NIH has some official criticism to some of these studies. Typically that they're either small or non blinded.
2. Vaccines
Lack of animal trials
Malone claims the current vaccines skipped animal trials. Humans are the first animals. Some animal testing would have shown the spike protein is an actual active agent, in lack of this knowledge FDA just gambled it wasn't.
On LinkedIn he wrote:
Second big inconvenient truth is that the spike protein is the actual active agent, in terms of eliciting an immune response. And in the case of the traditional vaccines, the dose of spike protein is defined relatively precisely. With the genetic vaccines, it is not (to the best of my knowledge). I know of no data wherein the mean, median, range etc of total amount of spike protein produced in a patient after administration of the COVID genetic vaccine has been defined. Usually, the FDA is quite persnickety about such things, but I am not aware of this key variable having been determined. Therefore, the range and severety of adverse events potentially attributable to the level of expressed spike protein may reflect patient to patient differences in genetic transfer efficiency and subsequent spike expression.
Is the spike protein toxic?
I don't know.
They say "we now know", but I can't tell.
There's a bunch of papers that mention cytotoxicity but I'm not quite sure of what that means. Most of the related points they make seem speculations on top of this point, see next point
Free spike protein?
They claim the vaccine antigen/debris is supposed to stay around the injection point. I don't know why that would need to be the case.
They found circulation
(paper), and the worry seems to come from their claim that now you have the toxic S protein circulating.
That could explain coagulation problems, even though the mechanism is not clear to me.
They are particularly worried about the accumulation in bone marrow and ovaries 48h after taking mRNA vaccines.
They mention a cautionary tale, Thalidomide, Malone denounces the lack of reproductive toxicology.
They claim that the circuation wasn't originally made public say they originally found this via FOIA request to some Japanese authority (pdf).
Pfizer vs Moderna: dosage
Phase 3 trials are optimized to prove efficacy, not to find the minimal dose to have sufficient effect. I find this reasonable on its own.
Malone recommends Pfizer over Moderna as it has lower dosage and similar efficacy. Presumably because adverse reactions are proportional to dosage?
Antibody-dependent enhancement? (ADE)
ADE are new behaviors that viruses get after they bind to antibodies.
In particular the "tail" of the antibody can bind to things that virus alone can't bind to, so if you have circulating antibodies bound to the virus you can circulate the virus in many more places.
This happens in Dengue, you get a minor disease up on first infection, and risk a much worse one on re-infection.
Malone claims we don't yet see ADE induced by vaccines (which is good), but that all previous attempts to create an anti-coronavirus vaccine failed due to ADE.
I had no way to verify this yet.
Should you get vaccinated?
Kirsch has a post about this, collecting much of the material, the tone is similar as in the video.
In the video they go as far as saying that if you're young or a woman the risk/benefit seems to be against vaccination.
3. Pharmaceutical companies
The analysis sounds like a conspiracy.
One of the most glaring point in their favor is the standard that was applied to Remdesivir, a still-under-patent repurposed drug. FDA required a single study (n=1063) to give it EUA, which is a much lower standard than applied to IVM.
Of course it doesn't mean there is a conspiracy, but it might very well be the net-resulting force of one sided nudging.
This ended up much longer than I anticipated. I didn't like the style of all of this, but the content seems interesting.
Replies from: dachamian↑ comment by dachamian · 2021-06-22T18:50:04.596Z · LW(p) · GW(p)
As I mentioned in my post, blog posts by David Gorski systematically address most of the issues you've highlighted ( https://sciencebasedmedicine.org/ivermectin-is-the-new-hydroxychloroquine-take-2/ )
Ivermectin:
"The mechanisms of action of Ivermectin against SARS-CoV-2:" this paper is explicitly critiqued, not least the sensational claim of a 1 in 23 trillion chance of the positive effect being random. (this isn't how statistical analysis works, apparently...)
There's also criticism of the Bryant and Lawrie paper.
On twitter recently Malone has acknowledged his mistake having been presented with evidence of dosing analysis by Pfizer ( https://twitter.com/RWMaloneMD/status/1406555309200531458 )
The key paper that shows cytotoxicty from the spike protein is with regards to the spike protein found in sars-cov-2, according to Gorski and the papers he cites the s-protein created via the mrna vaccines is modified to attach to cells in the muscle rather than freely circulating. (Its since been found that there are circulating levels of spike protein post mrna vaccine but in extremely small quantities, far lower than you'd get via an infection, and that the clearance of the protein is as expected for the proper functioning of the vaccine. ( https://blogs.sciencemag.org/pipeline/archives/2021/06/15/the-novavax-vaccine-data-and-spike-proteins-in-general ) )
The Japanese biodistribution data is also debunked, the study is in rats, the percentage build up in the ovaries is exceptionally small and studies have been completed looking specifically at ovarian function post mrna vaccine with no issues found. The Japanese data is at the center of Byram Bridle's claims, which is systematically debunked here https://byrambridle.com/ .
I'm also unware of any info on ADE.
I've been vaccinated with one dose of Pfizer with no side effects. I'm waiting on the imminent CDC emergency panel on myocarditis to gauge whether it makes any sense getting a second dose.
There's a lot of talk about the molnupiravir being invested in (a Merck product I believe) and concerns about an Alzheimer's drug that the FDA have recently approved despite apparently scant evidence and evidence of toxicity.
Replies from: DPiepgrass, ndr↑ comment by DPiepgrass · 2021-06-27T01:59:02.929Z · LW(p) · GW(p)
I may not have time to read through all of that, but thanks for the links. I quickly learned some new things by following a few links there + googling around.
Most notably, some key evidence presented by Steve K that took center stage in the video, both evidence of the dangers of "the vaccines" and evidence of the effectiveness of ivermectin, comes from groups led by the same person, Theresa Lawrie.
- Lawrie apparently founded a web site for ivermectin advocacy (registered March 7, 2021) after presenting evidence on Ivermectin's efficacy on January 13 (to "13 clinicians" and 7 others)
- Lawrie is the director of a group of 4 people calling itself "The Evidence-Based Medicine Consultancy" that called for "an immediate halt to the [Covid] vaccination programme" on June 9
- Lawrie published the meta-analysis Steve was raving about (with 6 co-authors), which found "Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using ivermectin" (published June 17 but, obviously, completed earlier)
Now, is Lawrie just one of those productivity superheroes vying for a Nobel prize? Or is there something suspicious about too much evidence and advocacy coming from the same person?
What makes me the most suspicious is that
- the anti-vaccine document performs no cost/benefit analysis before concluding that all three vaccines are too dangerous to use.
- it includes no analysis of base rates (the number of adverse health events that would normally occur in a large population in the absence of any vaccines).
- Edit 1: seriously, what are the chances that all three vaccines are both dangerous and equally so? Has that ever happened in history? I think not. (4 different vaccines are implicitly demonized by the video since it talks about US and UK data, but this document is UK-specific; the UK and US have used 3 vaccine brands each)
- Edit 2: I don't say this enough, but one must also consider the reaction of other experts. Large numbers of other experts think the vaccines are safe (safe enough to deploy widely, anyway) and that ivermectin is an interesting treatment but unproven. When experts in high places thought there was a risk of rare blood clots, they were often willing to halt the use of a vaccine even when doing so would lead to a larger number of overall Covid deaths. And of course, while regulatory agencies were understandably in a hurry, separate phase-3 trials were completed on each vaccine (in multiple countries) and showed adequate safety as usual. So the idea that these same experts and agencies are ignoring a wide variety of side-effects, including death, seems preposterous. The only argument I've seen against these numerous other visible experts comes from my father, who claimed the media is hiding information because they are controlled by George Soros, and from this video, which explains it as groupthink & social norms. As if scientists but not conservatives do groupthink & social norms.
I only skimmed the document, but I don't see any lip service paid to any of these issues or objections. And these are obvious objections, aren't they? So why wouldn't they be considered?
In the absence of other information, I assume that the lack of care demonstrated in this document is typical for Lawrie.
Unfortunately, my post ended up doing something I disapprove of: it listens to a handful of outspoken scientists (one in particular, it turns out) while utterly ignoring the majority who disagree. I hoped other LessWrong users would tell me how other scientists/experts are arguing the other side, but I got less of that than I hoped.
Replies from: ndr↑ comment by ndr · 2021-06-27T15:59:37.807Z · LW(p) · GW(p)
- seriously, what are the chances that all three vaccines are both dangerous and equally so?
Malone/Weinstein say they seem to have minor differences, at least in mechanism/effect. Their point being that if you get the S p circulating you're in trouble. All the three seem to produce that effect.
- One must also consider the reaction of other experts [...] When experts in high places thought there was a risk of rare blood clots, they were often willing to halt [...]
Well done, this is a very well put and good point. I don't know what drove the craze on blood clot (very few instances too?) against AZ and J&J. It's weirdly inconsistent with the reaction on myocarditis for mRNA vaccines, they only (reasonably?) halted on young population? It looks like a different standard than for AZ/J&J.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-27T20:36:12.629Z · LW(p) · GW(p)
Well, Moderna and Pfizer's are both mRNA-based, but presumably different in some ways because they were made by different teams (and I thought I saw Bret or Dr. Malone say he would have preferred Pfizer over Moderna, though it's not in my summary). But AstraZeneca and J&J are "adenovirus vector vaccines", using chimpanzee adenovirus ChAdOx1 and serotype 26 (HAdV-D26) respectively; the latter was "under investigation as [a] protective platform against HIV, Zika, RSV infections and are in Phase-III clinical trials for Ebola" in early 2019. Now, adenovirus vector technology is pretty new. Even so, it would be an impressive coincidence if the risks were both substantial and the same for a ChAdOx1-based vaccine, a HAdV-D26-based vaccine and both RNA vaccines. Sure, they all use the spike protein in some way — probably it's necessary for the immune system to recognize the spike protein — but (i) eventually our bodies will encounter the spikes, either via SARS-Cov-2 or via vaccine, and I've seen no one make a case that a live, replicating virus is safer, and (ii) the evidence/argument for the protein itself being dangerous hasn't been made clear in any of the stuff I've seen.
But my main point is the seeming lack of interest from Lawrie, Dowswell, Kirsch et al. in the question of relative safety, because this is a known failure mode of anti-vaxxers all the way back to the Wakefield study. That infamous paper apparently linked the MMR vaccine to autism, yet many anti-vaxxers acted like there was some fully general link between all vaccines and autism.
↑ comment by ndr · 2021-06-23T19:45:18.313Z · LW(p) · GW(p)
There's also criticism of the Bryant and Lawrie paper.
What's an actual criticism of that paper from that article? That meta-studies are garbage-in-garbage-out? That's weak at best, the author seems to have spent no time in spot checking any of the papers included to check whether this actually happened.
The Japanese data is at the center of Byram Bridle's claims, which is systematically debunked ...
... by a nameless "Concerned Scientist". I don't want to play ranking authorities, but it's obvious someone is mad at Bridle enough to steal his name to put up that website. It's hard to read that website assuming good faith, at least Bridle seems courageous enough to argue his points in the open under his own name, like any "Scientist" should do, especially "Concerned" ones.
Regarding the spike protein toxicity, my understanding is that the claim is a bit more nuanced. A recent tweet from Malone says:
The SARS-CoV-2 spike protein is cytotoxic. That is a fact. Who says so? Multiple peer reviewed references. The Salk Institute.
It is the responsibility of the vaccine developers to demonstrate that their expressed version is not toxic. Show us.
And then links to this Salk article.
Basically claiming that we know SARS-CoV-2 spike protein is cytotoxic and unless proven otherwise it's fair to assume the version expressed by vaccines is similarly cytotoxic.
All the "fact-checker" linked from that website are "we have no evidence that [...]", and this is very much a case in which absence of evidence is not evidence of absence.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2022-01-18T00:34:50.843Z · LW(p) · GW(p)
A recent tweet from Malone says:
The SARS-CoV-2 spike protein is cytotoxic. That is a fact. Who says so? Multiple peer reviewed references. The Salk Institute.[...]
And then links to this Salk article.
I've seen this paper used over, and over, and over by antivaxxers. But a coauthor of that paper, who was horrified about how it was being used, says:
Congrats to @OgataAlana on this important study. Many asked how much spike protein gets into circulation after vaccination. Turns out to average ~30-40 pg/mL for a few days then disappears. FYI: This is ~100,000x less than used in our paper (4 ug/mL). https://academic.oup.com/cid/advance-ar
I challenge anyone to name any vaccine or protein (or whatever) that is safe at the normal dosage and ALSO safe at a dose 10,000x or 100,000x higher. An extreme dose being hazardous is not surprising. It logically follows that if an extreme dose is harmful, it doesn't mean a dose 100,000x lower is harmful.
comment by Vanilla_cabs · 2021-06-18T08:21:56.211Z · LW(p) · GW(p)
Aaaand the video's gone.
Edit: Available at either
https://odysee.com/@GatheringOfEagles:9/how-to-save-the-world-ivermectin:b
Replies from: philovivero, DPiepgrass↑ comment by philovivero · 2021-06-18T20:12:08.753Z · LW(p) · GW(p)
One of the main take-aways I got from the video is that the censorship around this issue has gotten out of hand. I wonder why the video is gone? One hopes not due to censorship. Did the speakers have a change of mind, and remove the video?
Replies from: devin-brenton↑ comment by Devin Brenton (devin-brenton) · 2021-06-18T20:56:28.665Z · LW(p) · GW(p)
It was removed for violating youtube's "terms" and the channel was given a strike. Same thing happened to another video on the channel about the research and data on Ivermectin.
↑ comment by DPiepgrass · 2021-06-18T21:36:36.485Z · LW(p) · GW(p)
Meh. It won't do much to harm the popularity of the video's message, since Tucker Carlson was promoting "Covid vaccines dangerous!" a more than month before this video arrived. And since the video was at 350K views last I checked, I'd guess it reached 500,000 by the time it was taken down.
While "Covid vaccines killed 20,000 people!" doesn't have good evidence behind it and, I think, will get people killed, I'm not sure taking down the video is actually helpful. Many viewers will notice that the censorship they were warned about has come to pass. Distrust of Big Tech, the MSM, and Covid vaccines will be bolstered.
But if you're YouTube, what do you do? Get into the debunking business, post a response video? Nah—there's no profit in it. Deleting is easy, and they don't even have to give a clear reason.
comment by huey · 2021-06-19T10:14:37.660Z · LW(p) · GW(p)
This is an interview with Edward Mills, who is running trials on repurposed drugs.
https://www.halifaxexaminer.ca/featured/whats-the-deal-with-ivermectin-and-covid/
He seems more measured in his assessment of Ivermectin. Ultimately, he thinks there will be a small positive treatment effect, but not one that merits calling it a "miracle drug."
Contrast that with Bret Weinstein or Pierre Kory, who think this will end the pandemic.
comment by philovivero · 2021-06-16T14:58:00.416Z · LW(p) · GW(p)
From another comment:
When we discuss whether he's a crackpot we should also discuss whether all those people in power who initially said masks don't work listening to think tanks instead of the most qualified experts should be considered crackpots. I think the case for Fauci being a crackpot is a lot better then for Kirsch.
From You:
Don't extraordinary claims require extraordinary evidence? They seem to think that they themselves having seen some evidence is enough, so there's little need to present it to their audience.
They seem to be advocating for the type of science and evidentiary methods from 2019 and earlier. It seems to me, the extraordinary claims are originating starting around February 2020 from some folks who have a lot of friends in mass media. Masks absolutely do not work, and you will be banned from public discourse if you disagree. This was the ordinary claim made with ordinary evidence, and we all agreed with it and abided by it because we had to.
A few weeks later, the ordinary claim made with ordinary evidence was masks are absolutely required. Some time later, two masks are better than one. I still remain unconvinced.
If I have to choose between the enforced beliefs-from-above mass media controllers and these three guys, with their... "extraordinary claims" without "extraordinary evidence," I'm going with these three guys. Would prefer some sane discussion, though, since this is a somewhat serious disease causing somewhat serious problems for our global society.
Related, although I have sympathy with Kirsch's position and views, when I read his "paper" or whatever it is, it reads like a manic schizophrenic. And as another commenter pointed out, I think he is too quick to include some anecdata or shoddy studies into his mountain of evidence, which is a huge "conspiracy theorist" tell. I'm not sure I want Kirsch on my side, save for the fact that he has collected all this stuff together, while no-one else did. I suppose the flawed hero is better than no hero at all.
Replies from: mngreen↑ comment by mngreen · 2021-06-18T03:19:27.286Z · LW(p) · GW(p)
Without relying on mass media, i've seen far too many simulations and demonstrations (various camera and imaging types) and far too many detailed articles specifying particle size, mechanisms of viral distribution, viral load and the like to convince me that there is sufficient efficacy to warrant their use.
Yes, this includes discussions with people I know that work or who have worked in front-line medical positions. Yes, how the wearer uses / fits a mask, touches / adjusts it, disposes / reuses, which type of masks and how much other protocols are followed will all influence the degree of mask effectiveness.
Yes, there are no large double-blind, peer-reviewed studies to support mask use (non that I could find anyway). I'm not a "chicken little". I do believe there has been far too much conflation by some of prudence to mean cowardice, panic or being overwrought.
Re: the video ... I found far too many instances of where the other two were putting words into Malone's mouth, or were quick to over-interpret something he said.
I really would love for someone who understands the deep bioscience to take a very hard look at their ppl virology claims. At face value, the assertions would be very concerning, and while I would prefer for them to be wrong, I would rather see analysis as to whether they are or not. Pseudoscience is based on a whole lot of very very credible information and takes a sudden turn that is virtually impossible for non-specialists to unravel.
comment by DPiepgrass · 2021-07-19T05:10:26.023Z · LW(p) · GW(p)
One of the Ivermectin-supporting studies included in Lawrie's metastudy has been retracted due to glaring issues. This study (Elgazzar et al 2020) was the 5th largest study on Ivermectin by sample size (N=200) listed in the Bryant & Lawrie metastudy. Based on Figure 3 it looks like Elgazzar et al was one of only two studies that favored ivermectin without including the no-benefit line in the confidence interval.
Meanwhile, 6 other studies appeared to favor ivermectin but included the no-benefit line in their confidence interval, 1 study favored the control group and 2 studies sat in the middle. One of those, Fonseca 2021, had an especially narrow confidence interval centered around zero effect. This was not achieved via large sample size (N=167), but Fonseca 2021 was one of the few studies that ticked all the boxes for avoiding bias in Figure 2.
Now, it's well known that there is often a positive publication bias in science, but Dr. Malone put his weight behind the claim that in this case there's a negative publication bias. So, it's still plausible that ivermectin helps, but it hardly looks like a slam dunk based on the metastudy's Figures (I don't have time to read the text so much).
Replies from: ndrcomment by CraigMichael · 2021-06-14T22:15:59.710Z · LW(p) · GW(p)
- 28:47 "Nobody knows about [the VAERS system] and people aren't reporting" and "we've had reports reversed without the doctor's consent"
I don't buy this. I got a hand out about the VAERS system, created and account and reported everything that happened (and I did have weird side effects).
Replies from: ndr↑ comment by ndr · 2021-06-15T22:17:33.532Z · LW(p) · GW(p)
Nobody is very likely an exaggeration, I suspect is severely under used, but I have no idea about the reversals.
Did you report to VAERS yourself or via your doctor?
How do you know whether your report made it through?
↑ comment by CraigMichael · 2021-06-17T02:34:07.341Z · LW(p) · GW(p)
I might have been mistaken. I was thinking VARES was part of vSafe, but they may be different. I did for sure report it to vSafe.
comment by dachamian · 2021-06-22T18:14:00.505Z · LW(p) · GW(p)
I am a big, long time fan of Bret Weinstein, was impressed by the stoicism and apparent knowledge of Malone, and alarmed at the extreme claims Kirsch made. I've been following the ivermectin story over the past month or so, listening also to Dr John Campbell's seemingly sober and impartial analysis. I'd reached the point where I believed there was financially motivated suppression of ivermectin research, believed that it likely had generic antiviral properties (via "blocking" the ACE2 receptor), believed that adverse reactions to mRNA vaccines were under-reported and were likely caused via the human cell generated spike protein circulating in the body, that the particularly serious adverse reactions could be plausibly explained by accidental intravenous injection of the vaccine, and that Dr Tess Lawrie's BIRD group meta-analysis and Dr Pierre Kory's meta-analysis were being unfairly rejected by top journals. I find Bret's evolutionary argumentation compelling and I don't have a background in biology let alone virology. I imagine I'm not alone in coming to that position.
I became increasingly skeptical once Goa dropped ivermectin from its home kits (after being touted as an ivermectin success story). Then I came across an interview by The Halifax Examiner with the leader of the TOGETHER trial on repurposed drugs for covid treatment in Canada, Dr Edward Mills. In it he dampens enthusiasm for ivermectin's efficacy, its still part of their ongoing trial but he, without naming him, criticizes the intensity of Kory's invermectin advocacy:
"That particular group who authored that article [Kory's meta-analysis in The American Journal of Therapeutics] have a well understood agenda promoting ivermectin, and no amount of evidence is likely to change their mind — whether that be favorable or negative evidence — I don’t think it’s going to change their mind. So one of the problems with the ivermectin topic is that the advocate groups around ivermectin have overcalled the importance of this drug. You can’t go around promoting a drug, calling it a miracle drug that will end the pandemic, when you don’t even have a good clinical trial to support it, and that’s exactly what they did. If indeed this drug has a treatment effect — and I am very optimistic that it will — it will just be one component of the interventions that we need. It’s not going to end the pandemic. And that’s illustrated in India at the moment where Goa did recommend ivermectin, and just over the last few days it was recommended that it actually should stop being used."
This opened cracks in my confidence in the various narratives supported by Bret around covid and ivermectin, I started reading the comments to his recent tweets looking at the pushback he receives and so came across Dr David Gorski, whose blog posts on ScienceBasedMedicine.org systematically debunk the claims made around ivermectin, the toxicity of the spike protein (the one generated in human cells after mrna vaccination, not sure what the technical term is to distinguish it from the spike protein from sars-cov-2) and the lab leak hypothesis. I don't think its settled, but to me the criticisms made my Gorski are robust and would be of interest to people trying to reason about these issues for themselves. (https://sciencebasedmedicine.org/ivermectin-is-the-new-hydroxychloroquine-take-2/). I'd also be interested if people are aware of good faith counter-arguments to Gorski's counter-arguments.
Replies from: drobbs↑ comment by drobbs · 2021-06-28T08:27:05.561Z · LW(p) · GW(p)
The problem is, Bret is one of the few non-conspiracy adjacent vanguards fighting against the established "science". Because of his prior experiences being driven off campus by mob politics, he's become "anti-fragile" so to speak, willing to fight because he has found success by being true to his set of values & principles, which is admirable. But, the burden should not fall on him, we should have a system that welcomes open debate. To me, this is obvious. Truth wins through proving something to be true, not through conjecture, mass manipulation, and isolating anyone with a hint of skepticism. The dangers are obvious, America is in ruins from this rapacious empire, we have a seriously destructive society. It's impossible to not blame media for the state of the country (who are heavily influenced by various governmental & business actors).
That's what is so angering to me about this entire situation, never in the history of the world has there ever been a propaganda machine quite like the United States, its the most powerful element to the American empire. Its been able to hold the veneer of political credibility through "democracy & openness", when its really a lightly managed democracy, whose leadership class will use fear & deception to rule. Its not a "right-left" thing either, there is no doubt a class of oligarchs who move between the two parties seamlessly (ahem, Bloomberg). They are all entirely open about their desire to control humanity with vaccine passports, digital currency run by the IMF out of Switzerland, and an entirely new surveillance economy in the West to compete against China's surveillance economy.
I've slowly become totally distrustful of any established narrative, because the longer you live, the more obvious it becomes just how powerful the propaganda machine in America is. They have managed to lie the country into endless wars, lied the country into a mass surveillance program with the Patriot Act, allowed the Financial Crisis to play out where millions lost their homes & nothing happened to those at fault, to now the complete nonsense ever since Covid broke out. Its just impossible to believe the state of the country represents anything remotely close to truth or reality. Now, the way people put up signs in their laws saying "In this house we believe in science", its just feels like something out of a totalitarian society. Somehow they've turned this blind faith in "the science" because the media says so, into a full blown religion among a certain upper class of society. It's just so creepy & makes me believe people like Bret are probably far closer to the truth than Fauci & his cronies are.
comment by gilch · 2021-06-15T23:20:10.759Z · LW(p) · GW(p)
I've watched the whole thing now, at 2x speed. We've also got your summary with time index.
There are a lot of points in there, and we could try to verify each one. Anything particularly salient that you'd like us to focus on first?
To call the vaccines harmful on net, we have to compare that to the alternatives. Even if we accept (for the sake of argument) that the vaccine is toxic, presumably an actual infection has the potential to be much worse, since it produces the same spike protein. In my view, a lot of this case hinges on the availability of an effective prophylactic option as an alternative to the vaccines, or on the possibility that mass vaccination is somehow worse than the risk of infection.
So, in particular,
- is Ivermectin (or some cocktail containing it) effective enough to be a viable alternative to vaccination?
- Is the risk of female reproductive harm from the vaccines any worse than the risk from infection?
↑ comment by Mateusz Bagiński (mateusz-baginski) · 2021-06-16T07:22:01.184Z · LW(p) · GW(p)
As far as I understand, they claim think that since spike proteins in the actual virus particles are embedded in the particle (as opposed to "free"/"detached" when produced after getting the vaccine), they do not accumulate in the tissues, at least not to the same extent. Possibly, after a virus particle has been destroyed, some of its spike proteins circulate freely (or attached to some smaller segments of the virion) and then can get into tissues and accumulate.
↑ comment by DPiepgrass · 2021-06-16T21:54:55.757Z · LW(p) · GW(p)
The thing I wonder most is how we can work out whether or not the VAERS deaths can be mostly attributed to natural causes, and secondarily, whether there's some way to tell if there is a strong underreporting of deaths (contrary to FDA regs) as Steve alleges (and, says Steve, OpenVAERS).
↑ comment by ndr · 2021-06-16T13:27:42.697Z · LW(p) · GW(p)
Is the risk of female reproductive harm from the vaccines any worse than the risk from infection?
That is a brilliant question. Data from Israel and UK (both high vaccination rates) should reveal useful, but I do wonder how much data is required to make that claim.
In the UK (ONS) 1.7 males died for each dead female in the 15-45 age bucket. It's 2.3 in the 20-25 age bucket. This suggests female (young especially) are less prone to be badly affected, but it says nothing of other fertility-related adverse reactions.
Regarding Ivermectin, see my top level reply [LW(p) · GW(p)].
Also from the FLCCC website, it looks like there is still no data about taking IVM during pregnancy.
comment by gilch · 2021-08-10T04:50:17.396Z · LW(p) · GW(p)
I stumbled across the Better Skeptics "Ground Truth Challenge" which offered prize money for identifying false statements in this and three other related podcasts, judged by three referees including our own ciphergoth [LW · GW].
Results are here.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-08-24T22:25:35.099Z · LW(p) · GW(p)
This site puts the burden of proof on critics to prove that statements by the anti-vax leaders are false. I think this is problematic because most of the claims coming out of the mouths of Weinstein, Kirsch, etc. are...
- unfalsifiable claims (e.g. "the [VAERS] reports were put in by people and [snaps fingers] they disappeared")
- speculation ("vaccinating into a pandemic rather than in advance of a pandemic, is liable to cause the evolution of escaped mutants, and that it could...make a much worse pandemic in the end"*)
- vague motte-and-baily type claims (e.g. "the spike protein is dangerous"), whose goalpost is unclear so that whether the claim is falsified is very much in the eye of the beholder.
- difficult or impossible to prove false on a budget less than the reward amount of $100, especially as lots of the claims do not identify any source they are based on.
Also, the fact that 123 out of the 126 submissions were unsuccessful suggests that the judges were very strict in their judgements.
I can't tell what reasoning they used to reject 123 of the entries; most of the links away from the result page are dead links that just say "File is in owner's trash".
Edit: in fact there is a category called "Unsupported claim" which seems to have a lower burden of proof (reward: $50); still, somehow 98% of submissions were unsuccessful. Also, the official rules limit submissions to four specific podcast episodes; they don't accept challenges to source material such as Steve's blog, and I didn't initially realize this so I did challenge Steve's blog here.
But let's consider, for example, Steve's claim that "these vaccines have likely killed over 25,800 Americans", which links to Walters, who explicitly admits that his claim about 25,800 deaths was incorrect. Does this prove Steve's claim is false under these rules? Maybe not, because Steve says he confirmed it "3 different ways", so first you'd have to figure out what the other two ways Steve used to "confirm" this information and disprove both of those. Steve doesn't clearly spell out what these 3 different ways are, though. We could speculate that one of the other "ways" was VAERS data, but even if the judges accept this interpretation, how do you prove that ~7,000 deaths in VAERS does not correspond to 25,800 deaths in reality? Sure, I've made arguments that this is likely to be nonsense, but clearly proving it could be hard-to-impossible depending on how the judges judge.
Another issue is that a challenge can only be successful if the claim is "non-corrected". (edit: looks like the rules don't clarify what non-corrected means). So, Steve claimed the vaccines have "disabled at least 1,000,000" Americans. Hypothetically, let's say this blog post was read by 2,000,000 people, but then Steve "corrects" this claim in a different post read by 10,000 people. Would that make the original claim ineligible to be challenged? Hard to say - once again it's up to the judges.
Just a couple of hours ago I noticed that Steve K's big article contradicts itself; it states that "Biodistribution of lipid nanoparticles which carry the mRNA show that the ovaries get the highest concentration" and it also states that "the vaccine takes about 15 minutes to set fire to every part of your body at the same time (and the biggest fire is in your ovaries)". But data in a chart in the same article shows this to be false! (see also this [LW(p) · GW(p)].) So, why is it that none of the successful challenges demonstrated that this claim is false? Well, if we can't look at the rejected submissions, I guess all we can do is unfalsifiable speculation ;)
* by the way, isn't vaccination during a pandemic completely normal? e.g. annual Flu vaccines, and the early days of smallpox and polio vaccination. Not to mention that the alternative — waiting for the pandemic to be over before vaccinating people — is silly.
comment by gilch · 2021-08-10T01:54:23.924Z · LW(p) · GW(p)
Yuri Deigin recently did a point-by-point takedown on Rebel Wisdom: https://www.youtube.com/watch?v=GwzfnZfo-rU
Bret's thesis rests on two pillars: the mRNA vaccines are dangerous and Ivermectin is a safer alternative. If either of these aren't true, then vaccination is the better option.
According to Yuri, basically all of the important claims are false. Neither pillar holds. The case on Dark Horse for the dangers of the vaccine and the safety and efficacy of Ivermectin is misleading at best. It requires cherry-picking studies of poor quality, and then misrepresenting what they actually say. Unless Yuri is outright making stuff up, I don't know what Bret is thinking. My estimation that Bret is being either rational or honest is diminishing.
I mentioned previously of conspiracy theorists that
They don't notice the inconsistencies in their own models, and their bald assertions often don't stand up to easy verification, if you bother to check.
Both Bret and Steve seem to show this failing now, and despite Bret's earlier record of scientific thinking and correct contrarianism, I think he's out of touch.
comment by gilch · 2021-08-08T22:48:04.181Z · LW(p) · GW(p)
Sam Harris [who was also counted in the IDW originally] responded to this (as well as vaccine hesitancy in general) in a recent podcast https://www.youtube.com/watch?v=7jQfNzk_CFk
Sam's main point seems to be that even if we steelman the claims against the mRNA vaccines, it's still a clear-cut choice when you do a cost-benefit analysis because the risks from COVID are so much higher than from (mRNA) vaccines. But the vaccines are still obviously safe and effective and maybe Bret is confused. Also, Sam still considers Bret a friend.
DarkHorse Podcast reply: https://www.youtube.com/watch?v=AsnXoe1EBaE
Bret says that Sam failed to engage with his real arguments, and that past disputes of fact about this pandemic puts Bret in what we'd call the correct contrarian cluster, [LW · GW] so take this a bit more seriously, please? Also, Bret still considers Sam a friend.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2022-05-03T17:46:49.199Z · LW(p) · GW(p)
Yeesh. No wonder Bret wasn't impressed - I've heard the first 45 minutes and they still haven't talked about any of the misinformation in Bret's podcast. Will they eventually get around to talking about it? Who knows, I can't be bothered to sit through the whole thing. At least at the 40 minute mark they implicitly discussed base rates in VAERS, which seems to be a totally invisible concept to anti-vaxxers.
But at the same time, they're saying "in the clinical trial no one died" and then talk about the "12 thousand VAERS deaths" without discussing the fact that anti-vaxxers dispute these basic facts. For example I see Kirsch saying, in a "Pfizer 6 month trial" that there were 21 deaths in the vaccine group vs. 17 in placebo (no doubt true but irrelevant); Kirsch also claims there is an enormous underreporting factor (42? I forget) for deaths post vaccination in VAERS (ridiculous, but he has an excuse for making the claim). At 47:20 there's finally a (forceful but weak) rebuttal of something Bret said.
So the podcast is engaging with anti-vax arguments a little, but the Dark Horse podcast I summarized here is 3 hours long and I can be pretty sure, without hearing the rest, that Sam hasn't addressed most of the claims made there, let alone everywhere else.
Replies from: ndr↑ comment by ndr · 2022-05-16T13:08:44.353Z · LW(p) · GW(p)
It wasn't really intellectually honest, to the point he received enough criticism from his own wife and granted that much
You can check out the initial few minutes of the following AMA
I don't feel like dealing with too many specifics here. One criticism I do take to heart if only because it came in one form from my wife is that despite my saying that I wanted to remain non judgmental and try to produce a document that the vaccine averse could actually receive without feeling denigrated in any way. I didn't try hard enough and certainly my guest Eric didn't try hard enough there. I would have to say we are guilty as charged and in truth, I'm not even sure it's the right target. I mean there's something patronizing about the claim that in order to reach the vaccine hesitant, you have to walk on eggshells. So as to not make them feel judged. Nevertheless, I do see the depressing results of the last podcast all around me. Those who were disposed to agree with me absolutely loved it and we're grateful. And those are worried about the Covid vaccines and taken in by what they've heard on Bret Weinstein's podcast or tucker Carlson, wherever thought Eric and I were totally clueless about the state of the conversation that's happening over there. I don't actually know what the solution is here because some people asked why not just have Brett on the podcast to talk about all this, But I think that would be a bad idea, not because I don't think they're adequate answers to the kinds of points he would raise. But like so many debates on fairly fringe topics, classic conspiracy theories, religious fundamentalism, many points can't be addressed in real time. Many anomalies can't be fully explained, right?
comment by DPiepgrass · 2021-07-21T14:53:05.174Z · LW(p) · GW(p)
The claim that the concentration of LNP (lipid nanoparticles) is highest in the ovaries after 48 hours appears to be not only false, but a "pants on fire" kind of lie: the linked source shows the concentration as being 259 times higher at the injection site, and 170 times higher in the liver.
The chart showing the concentration as being highest in the ovaries simply leaves out the data for the injection site, for the liver, and for the spleen (which has over 10x higher concentration than the ovaries).
Edit: I had been investigating the claim about ovaries on Austin G. Walters' blog, which is the first thing Steve Kirsch links to his own post. It claims "after a 48 hour period, the Pfizer mRNA vaccine will have the highest concentration in the ovaries and bone marrow". No wonder, as Kirsch did say that "Biodistribution of lipid nanoparticles which carry the mRNA show that the ovaries get the highest concentration". However, although Steve shows the same chart as Austin, and the same chart was also featured in the Bret W / Steve K video, Steve's blog post shows another chart that includes Liver and Spleen (but still excludes injection site!) Oddly, this chart shows only 2x concentration in liver and spleen after 48 hours (rather than 170x). Note that in both cases the data is from rats.
So, why the difference? Well it turns out that both numbers are correct, and I used incorrect wording above. While the amount of LNPs is 259x higher at the injection site, 170x higher in the liver, and 10x higher in the spleen, the concentration of particles is only 13x higher at the injection site and 2x higher in the liver and spleen. The liver is way bigger than the ovaries, so a 2x higher concentration translates to a 170x higher total amount of LNPs.
Something else that I noticed is that Austin's and Steve's posts each link to the other, each one giving readers the impression that the link to the other is evidence for a claim. Which is... pretty weird.
How the chart would have looked if Kirsch had included the injection site:

comment by Marve Flexnes (marve-flexnes) · 2021-06-19T11:46:50.808Z · LW(p) · GW(p)
"And if a vaccine is causing these deaths, where are the lawuits?"
Vaccine manufacturers are actually exempt from such lawsuits.
↑ comment by DPiepgrass · 2021-07-21T16:45:57.178Z · LW(p) · GW(p)
[Citation needed [LW(p) · GW(p)]]
comment by Rafael Harth (sil-ver) · 2021-06-19T11:28:27.703Z · LW(p) · GW(p)
This is the video, right? You could link to that instead of the removed youtube link.
comment by Jonathan_Graehl · 2021-06-14T20:33:58.687Z · LW(p) · GW(p)
'If this were true, where are the lawsuits against the vaccine makers?'
Surely they've been shielded from liability so there won't be any.
Replies from: DPiepgrass, TAG, DPiepgrass↑ comment by DPiepgrass · 2021-07-07T17:39:29.409Z · LW(p) · GW(p)
This is possibly outdated, but I saw a publication by "National Research Council (US) Division of Health Promotion and Disease Prevention" from 1985 stating that "A manufacturer who produces and sells a defective vaccine that creates a risk of significant injury to the recipient is liable to any person injured by that defect under the principles stated in section 402A of the Restatement of Torts. This is thought to be the law in every American jurisdiction".
↑ comment by DPiepgrass · 2021-06-16T21:58:03.630Z · LW(p) · GW(p)
If that's true (??), I guess lawsuits would be directed at the FDA instead. It'd be shocking if everybody involved had immunity (against lawsuits, I mean).
Replies from: philovivero↑ comment by philovivero · 2021-06-18T20:16:48.184Z · LW(p) · GW(p)
Whether or not you agree with the people who were concerned about the USA 2020 election irregularities, one thing you absolutely can conclude is that an entire class of people can have their lawsuits ignored with "lack of standing," if there is any political will. This goes all the way to the Supreme Court.
Those who aren't happy with the vaccines largely overlap with that previous group who were summarily kicked out of the judicial system. I predict there will be no lawsuits, whether or not millions of people desire there to be.
Replies from: DPiepgrass↑ comment by DPiepgrass · 2021-06-18T21:50:11.751Z · LW(p) · GW(p)
I think you're saying that a Supreme Court with two-thirds Republican appointees won't give popular Republican ideas a fair shake, and that the concept of "standing" has been corrupted by "political will". Political will in the judicial branch? How does this work exactly?
comment by zby · 2022-05-22T08:10:30.882Z · LW(p) · GW(p)
I am surprised that nobody linked to Scott Alexander on ivermectin: https://astralcodexten.substack.com/p/ivermectin-much-more-than-you-wanted (plus: https://astralcodexten.substack.com/p/higlights-from-the-comments-on-ivermectin?s=r). For me it more or less settles the subject - the most probable hypothesis is ivermectin de-warms people and it has a huge positive outcome on peoples health when people have warms (independently from covid - or maybe even dependently - because the warms decrease immune response fighting the virus) and unfortunately in many places on Earth worms are still prevalent enough that it shows in covid related trials.
But on the other hand I am pretty much sure that much of vaccines related info is now suppressed - not through a centralized censorship but via an emergent mechanism.
The clustering is pretty telling - anyone who claims that vaccines are dangerous also claims that ivermectin or HCQ treats covid, everyone who rejects ivermectin will also reject any claims about adverse effects of vaccines.
Yet another clustered subject is vaccine efficacy - it is pretty clear that injected vaccines don't prevent getting ill and spreading the virus. Vaccination can limit the time of virus shedding - but actually the dangerous case is when we shed the virus when hot having other symptoms and for all we know vaccines might even increase the durability of that infection phase. This is something that is admitted by the 'main stream' - but the implication of that is that "vaccine passports" are silly, because vaccinated persons can still spread the virus and that will never be accepted by the 'pro-vaccines' side (which is now main stream).
It is also pretty clear now that the current vaccines are less effective against the new variants - the problem is that the 'pro vaccine side' does not want to admit that, and 'the other side' does not want to admit that the right conclusion is that we need new vaccines (maybe the nasal onese - that would provide sterilizing immunity): https://erictopol.substack.com/p/the-covid-capitulation?s=w
comment by RichardBentley · 2022-03-20T02:10:26.598Z · LW(p) · GW(p)
I have just read a short blog entry by Steve Kirsch and my BS detectors went into overdrive. That is what put me on the search to find this particular piece. At the first mention of 'cover-up' or any other kind of conspiracy to keep 'unwanted' information from the public you had better start washing off the shoe that stepped in it. Also, I keep seeing VAERS 'data' being thrown around. That so-called 'data' is of very limited usefulness because people can report anything without any cause-and-effect evidence and thus separating signal from common background noise is very difficult.
comment by Sara Smith (sara-smith) · 2022-05-22T06:03:14.426Z · LW(p) · GW(p)
Now, with the benefit of hindsight, we find >95% of the claims on this video to be not just accurate, but peer reviewed.
Also, you describe Steve Kirsch as "red-tribey" - he is in fact a classic liberal, a quick public records search revealed that he gave the maximum donations to Obama, Hillary, and even Biden in 2020 (but not to any Republicans). Recently he has expressed extreme disappointed in the Democratic party (as have I), but spend any amount of time reading his stuff and you will find him to be pretty left leaning, but bipartisan and open minded in his dialogue (I have seen several examples where he gracefully accepts a fact-check, as long as it's evidence based). I have also found that for his videos & articles, he extends more invitations to pro-vaxxers than anti-vaxxers.
comment by cata · 2021-06-13T06:57:58.976Z · LW(p) · GW(p)
It's really hard to take seriously a thesis that is only presented in the form of a 3-hour YouTube hangout conversation, presumably because the participants are more interested in promoting their brand than communicating information to anyone.
If these guys give a shit maybe they should write down their opinions.
Replies from: ChristianKl, SolAlium↑ comment by ChristianKl · 2021-06-13T21:10:57.321Z · LW(p) · GW(p)
This is an unfounded allegation. Kirsch writes down his position at https://trialsitenews.com/should-you-get-vaccinated/ and that's linked in the video description. This video is not the only time they talk about it.