Omicron Post #6
post by Zvi · 2021-12-13T18:00:01.098Z · LW · GW · 30 commentsContents
South Africa Denmark United Kingdom Other Places Laboratories and Experiments Threads Prediction Markets Probability Updates Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 75% → 85%. Chance that Omicron will displace Delta as most common strain: 96% → 98+%. Chance that Omicron is importantly more virulent than Delta: 4% → 3%. Chance that Omicron is importantly less virulent than Delta: 55% → 60%. Will the CDC label Omicron a variant of high concern before 2022? 12% → 11%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 60% → 50%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 25% → 25%. Will Omicron be >1% of all cases by the end of the year? 94% → 97%+. None 30 comments
Previous posts: #1, #2, #3, #4, #5, last weekly post
Well, that escalated quickly. Omicron has already escalated quickly in log terms, and will soon escalate quickly in linear terms. The core questions remain the same, and we continue to continuously get better data to allow us to make better guesses and projections.
There are three central places where population-level information is available first:
- South Africa, because Omicron has taken over already and they have good data.
- Denmark, because they do all the sequencing.
- United Kingdom, because of S-gene-deletion data and good sequencing.
We also have a few African countries like Zimbabwe with giant spikes. But in other European countries and in the United States, the lack of sequencing makes it impossible to know how far along things are or how fast they are moving.
Thus, we must rely on what data we have, and give thanks to those who provide it.
Uncertainty abounds but there is no known link between ‘has more Omicron infections’ and ‘has ability and willingness to monitor Omicron cases’ so we should start with the assumption that Denmark and the United Kingdom are typical western countries for this, adjusted for the state of Covid-19 under Delta there relative to other places.
All of that can and should be complemented by experimentation and lab results. Alas, as per usual, challenge trials and most non-natural experiments remain illegal, so we have orders of magnitude less knowledge and certainty from these sources, and everyone is much worse off, than we could if we cared more about saving lives and making people’s lives better and actual ethics, and prioritized those considerations over ‘biomedical ethics.’ So mostly the useful findings lie elsewhere.
Here’s two charts of overall cases and positive test percentages in various places, for context. The rise in Denmark does reflect some Omicron cases, they’d still be under 1,000 on this graph without it, and the UK rise as well.


South Africa
The most hopeful news would be if South African cases peaked all of a sudden for no clear reason, the same way cases of Delta in India did, and started heading downward. We did see a blip for a few days, but was it more than a blip? My read on it is no, and there are signs of issues with data reporting to explain it.
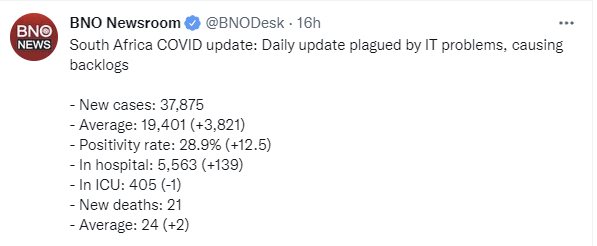
The news on this front is still good, because it’s possible things are improving, and in the worst scenarios things should have continued to get rapidly worse. The positivity rate sticking around 30% would be actively great news.
As you can see on the graph above, the 7-day averages haven’t stopped rising, at least once Our World In Data corrected for temporary data errors. I do still find the lack of a steeper rise to be good news.
Here’s a short explanation of why it’s still too early to draw any conclusions from the death rate. Still need another week or so due to lag.
There are a bunch of threads about South Africa in the Threads section below. They basically all note that a lot of cases continue to be incidental and severity looks low, but that it’s too early to know for sure for reasons I went into on Thursday.
Here’s a video interview with Dr. Angelique Coetzee of the South African Medical Association from December 12. Most optimistic case presented so far. I want to update more but I still don’t feel like this clarifies things much.
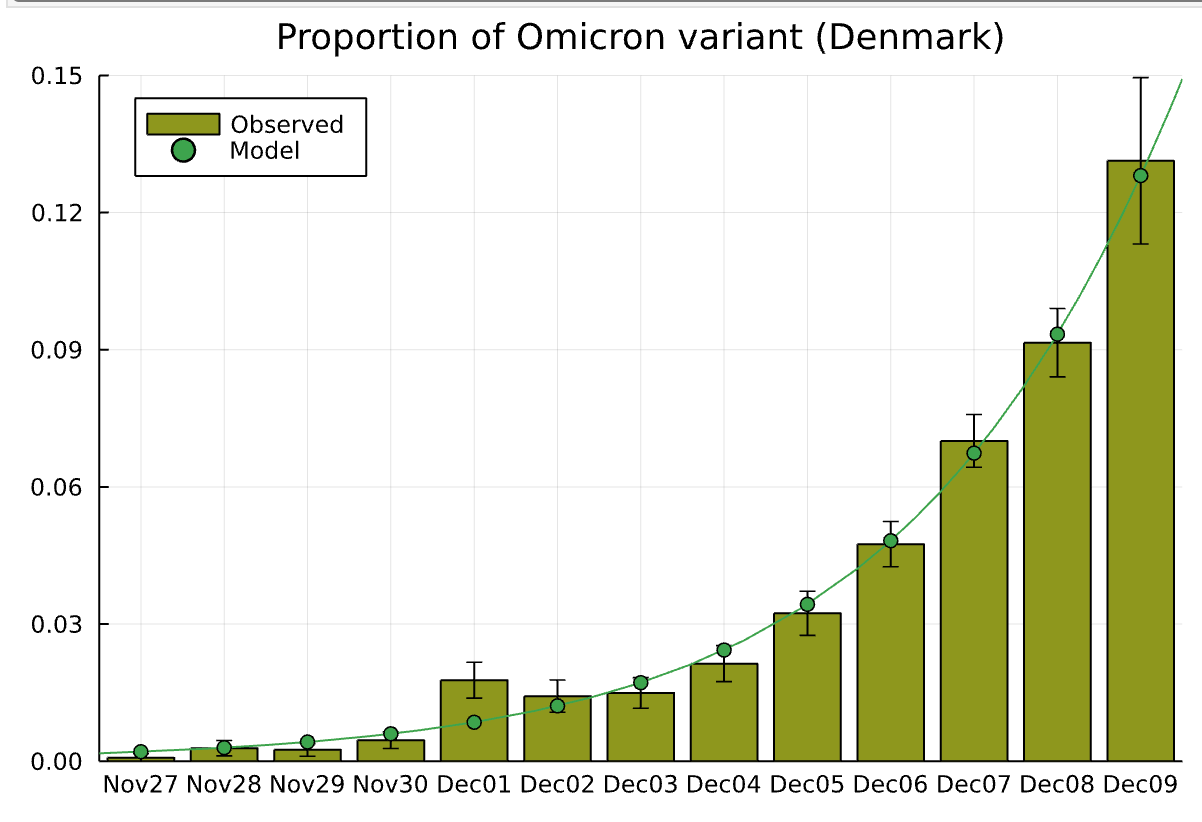
Denmark
Denmark has the world’s best sequencing. It also has the largest number of known Omicron cases as a share of population by a lot, which is not a coincidence. And it knows cases are growing exponentially, also not a coincidence.
Here’s an update from yesterday.

For speed reasons I didn’t double check the math, but the principles are right and the answer is roughly correct. This is happening, and it is happening fast, and places that aren’t observing the same should still expect to be experiencing the same soon after.
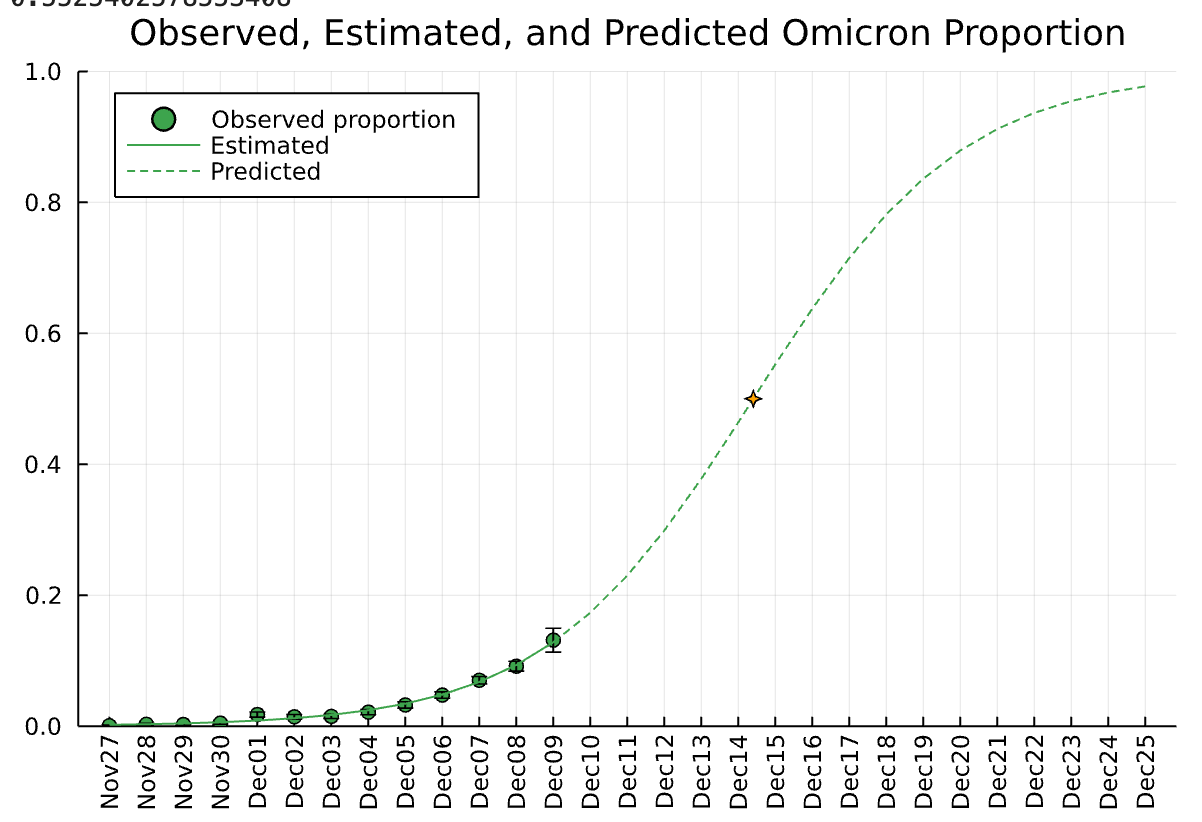
Here is the official government projection from December 13:
United Kingdom
An announcement from Boris Johnson, urging everyone to get boosted and aiming to finish the job by the end of the year. Compared to the messaging I’m used to, this is quite good. The issue is not what is here, the issue is what is not here – any effort to get Omicron boosters, or any attempt to improve options for testing and treatment.
Here’s an analysis of a lagged update on the situation in the United Kingdom up through December 3.
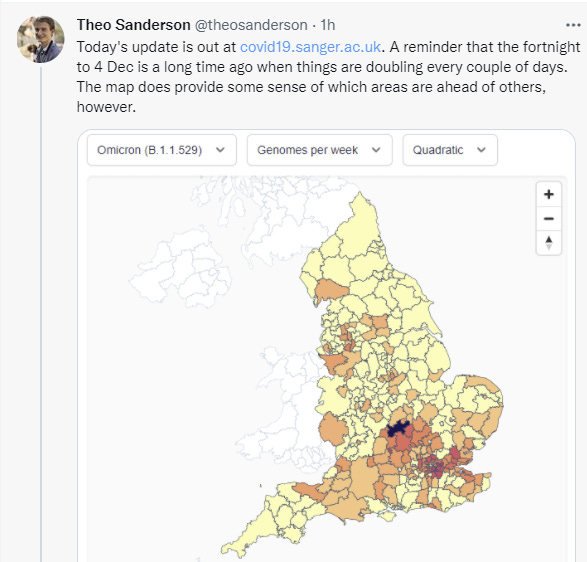
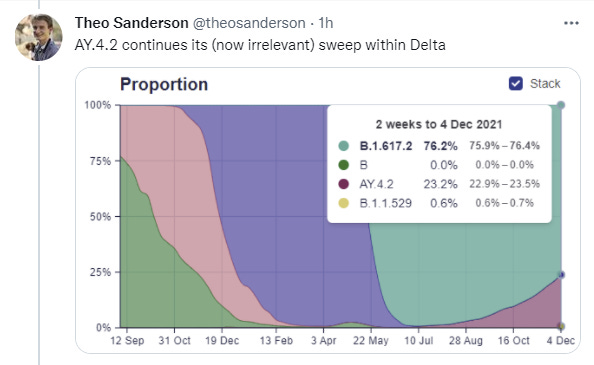
AY.4.2 is irrelevant in the sense that it’s going to be overwhelmed by Omicron soon, but it’s also common enough and growing rapidly enough that it represents a higher previous baseline of infectiousness. It’s also relevant for looking into the future, to know that trouble of a lesser kind was already on the horizon and approaching rapidly, and starting to meaningfully impact case counts.
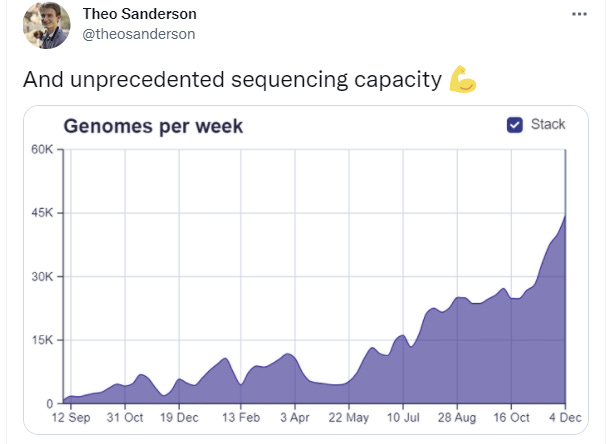
This is excellent and seems to have started before Omicron, which highlights how hard it is to pivot into such responses after you know you need them.
The key estimate is 0.6% for Omicron in the two weeks ending December 3, up from 0.0% before that, while remembering that December 3 is ten days ago.
We should adjust this down slightly for rapidly increasing sequencing, since Omicron cases would be sampled more from the later portion of the period, and for the choice of what to sequence not being entirely random, but these are unlikely to be large effects given the numbers involved. Let’s call it 0.5%.
How does that constrain possibility space?
Since the previous calculation was also over a two-week period, there’s a broad range of possible growth rates, which we can make work by adjusting the rate already infected on 11/21.
In the optimistic case, which also corresponds to the reports of doublings every three days, we can say 0.1% coverage already on 11/21, have a daily R0 of 1.23 (doubling every 3 days would be 1.26), and still get to about 0.5% for this period, which would have Omicron become the majority strain on Christmas Eve, minus the lag in cases from infections, so we’d have about a week. There will be a large natural adjustment in behaviors even if Boris doesn’t cancel Christmas and otherwise go around ruining life, but is a mostly vaccinated population going to lock down sufficiently hard to adjust for this kind of transmission advantage? I don’t see them doing it voluntarily, nor should they, so the question is whether one can be imposed by force and sustained.
On December 10 Guardian reports that while the government had instituted Plan B, and had noticed that Plan B would be the goggles and essentially do nothing, there remain no plans to implement Plan C. Which is good, since even if it temporarily worked Plan C is unsustainable on the timeline it would be needed, there is no sign of rushing to get Omicron boosters and/or Paxlovid to the scene fast enough to matter, and the costs of a somehow sustained Plan C that might get us that far seem clearly higher than the costs of doing nothing.
Note that the official reports (WaPo) have Omicron taking over this week, rather than next week, so why the difference? The answers here are very sensitive to exact doubling times and starting conditions, so the difference is less substantial than it might look at first glance.
Here’s some data from Scotland, from December 10, not updated yet. Direct source, dug briefly but didn’t find an updated version. Each line is one day.
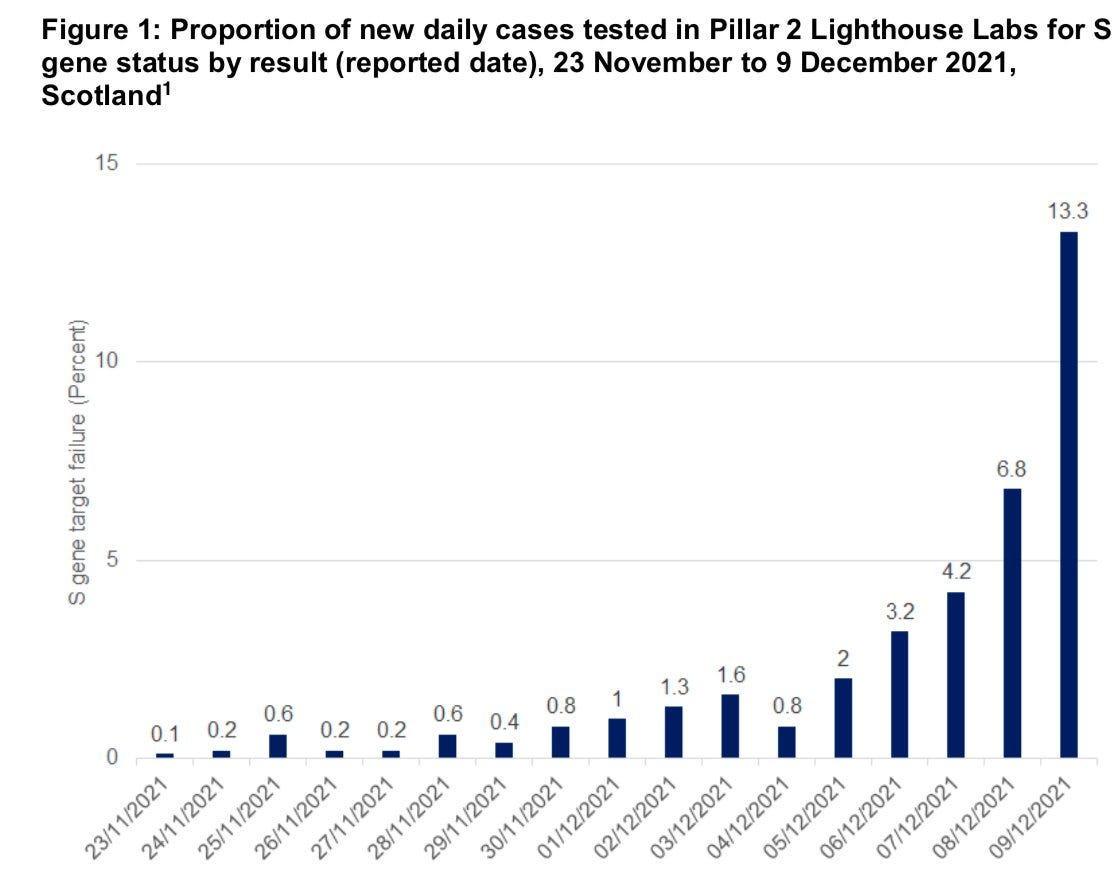
Ten days is a long time ago given how fast things are moving. That’s three or more doubling periods.

This is reported cases. The 21st is a Tuesday, and well before Christmas, so should have full reporting. Let’s say we can expect 750 Delta cases per million people, or about 50k Delta cases, on a weekday. So this is mostly asking if Omicron will substantially surpass Delta by then, which is approximately a coin flip between the later two categories. I’m impressed by the poll responses.
Reported first on December 13: A patient known to have Omicron in the United Kingdom has died. One death obviously means little, but zero and one are highly different numbers, and cases and deaths typically lag by three weeks, so this is disappointing news.
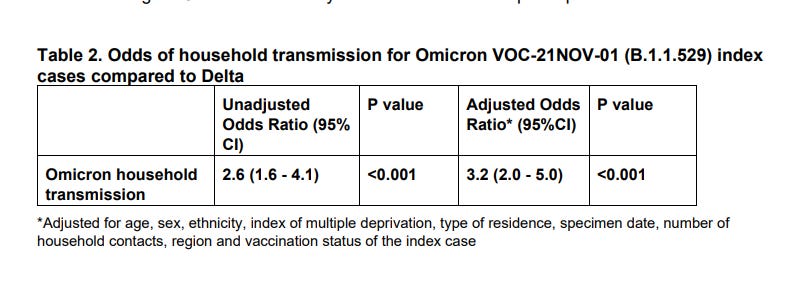
UK also offers this helpful report (direct link) showing Omicron with a huge household transmission advantage.
Other Places
USA dates first known Omicron patient symptoms to November 15.
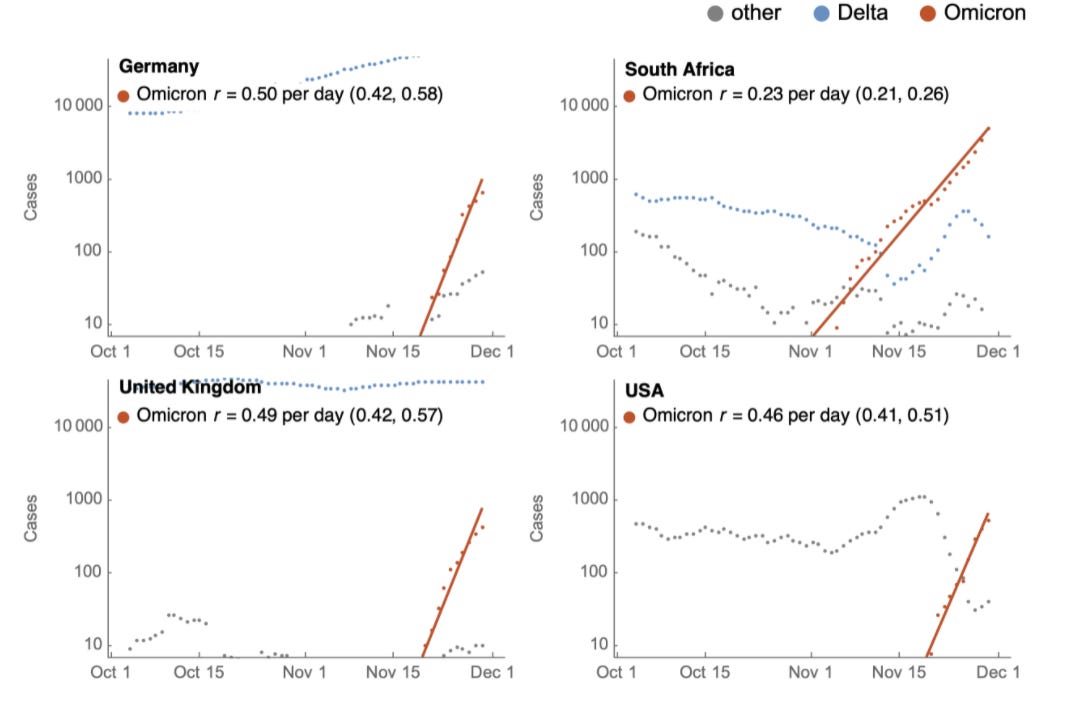
Trevor Bradford looks at data from USA and Germany and attempts to directly estimate rate of spread, building off previous thread about South Africa that was relatively optimistic about possibility things might peak relatively soon there.

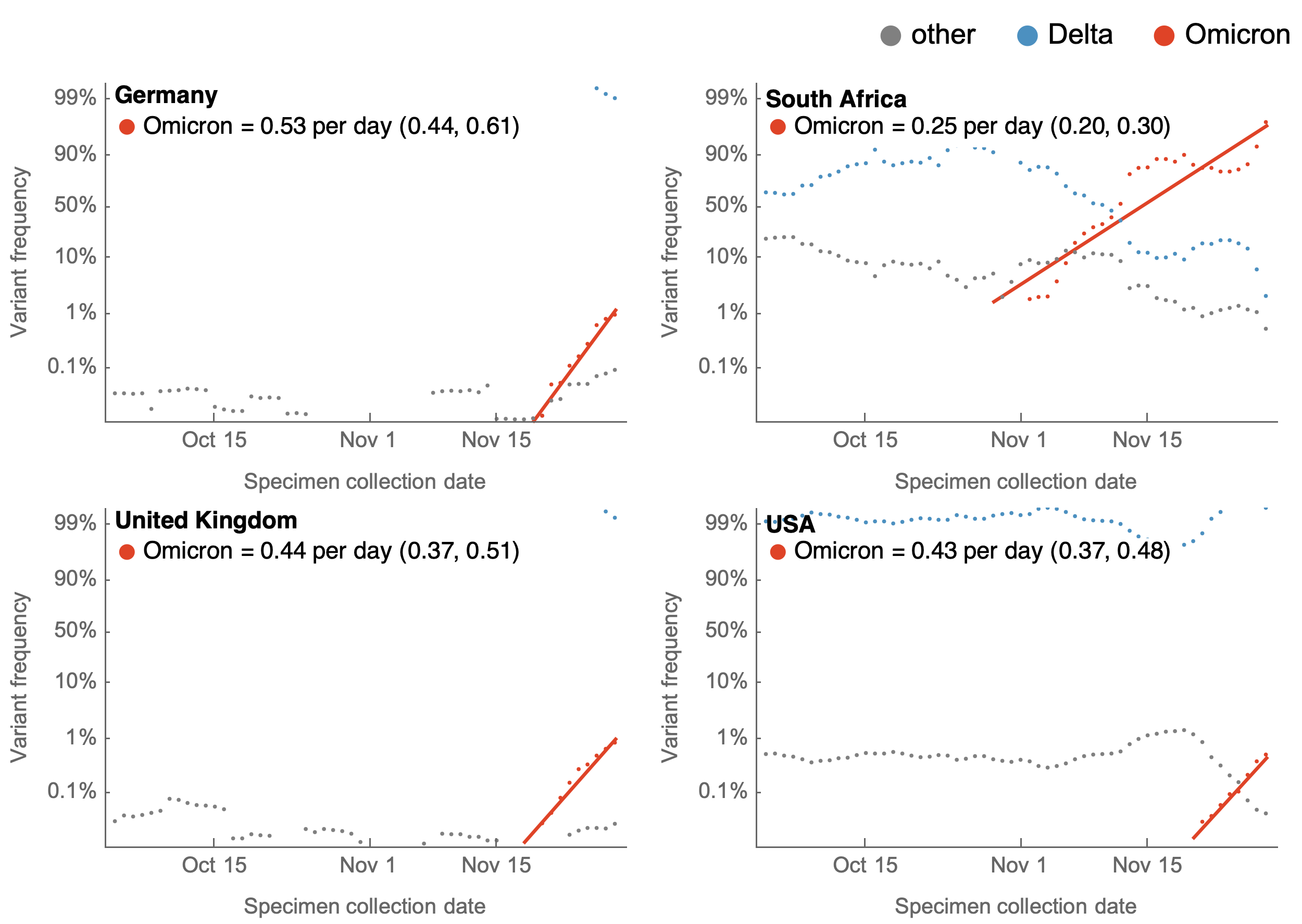
To extent we have data for the USA and Germany, this superficially looks is saying it largely matches the UK’s data, which should be our baseline assumption, but the Rt calculation comes in somewhat lower. Still very far above 1.
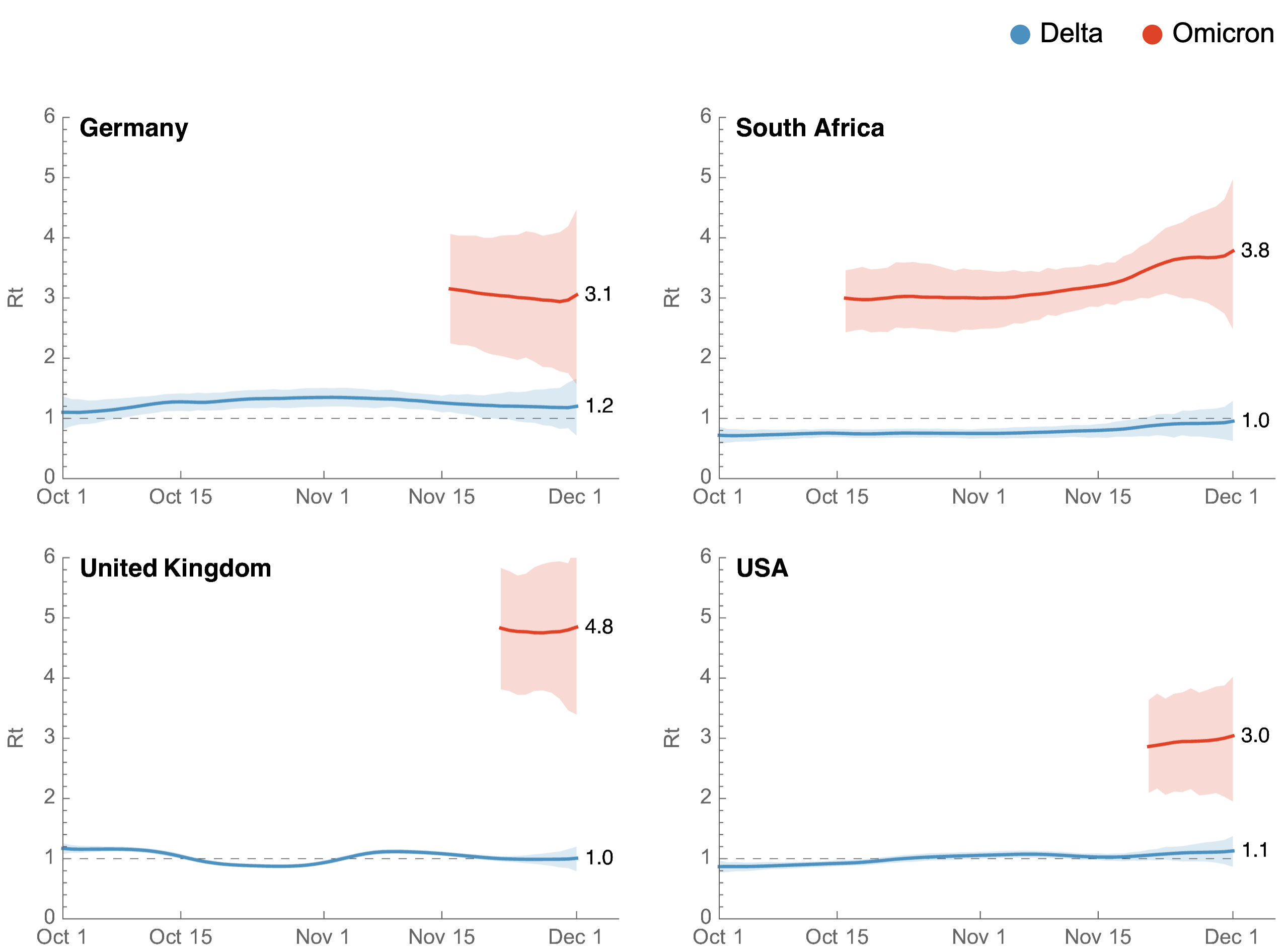

Link to methodology. You can find updated figures here as per his link. At press time here are the estimates, which have gotten faster/worse:
Norway, where we earlier saw a superspreader event get noticed, is ramping up measures:
Laboratories and Experiments
Confirmation from Michael Mina that rapid antigen tests work on Omicron.
Concern that inactivated virus vaccines will fail against Omicron.
Threads
December 10 what-we-know thread from Tom Friedman, seems right but without new insight.
December 10 overview of UK government report.
December 9 summary thread from Derek Thompson, nothing new at this point. Optimistic on severity, but with appropriate caution.
December 9 thread from Andrew Lilley about severity based on South African data, no new data, cautious optimism. December 10 thread from John Burn-Murdock about the same topic, more reserved. And December 10 one from Shabir Madhi.
December 13 thread from Trevor Bradford noting that Omicron might not displace Delta, and it’s possible both will continue to circulate. I don’t see this as likely, but it is possible.
December 13 thread from Bloom Lab about subvariants of Omicron, and their relative levels of escape.
Prediction Markets
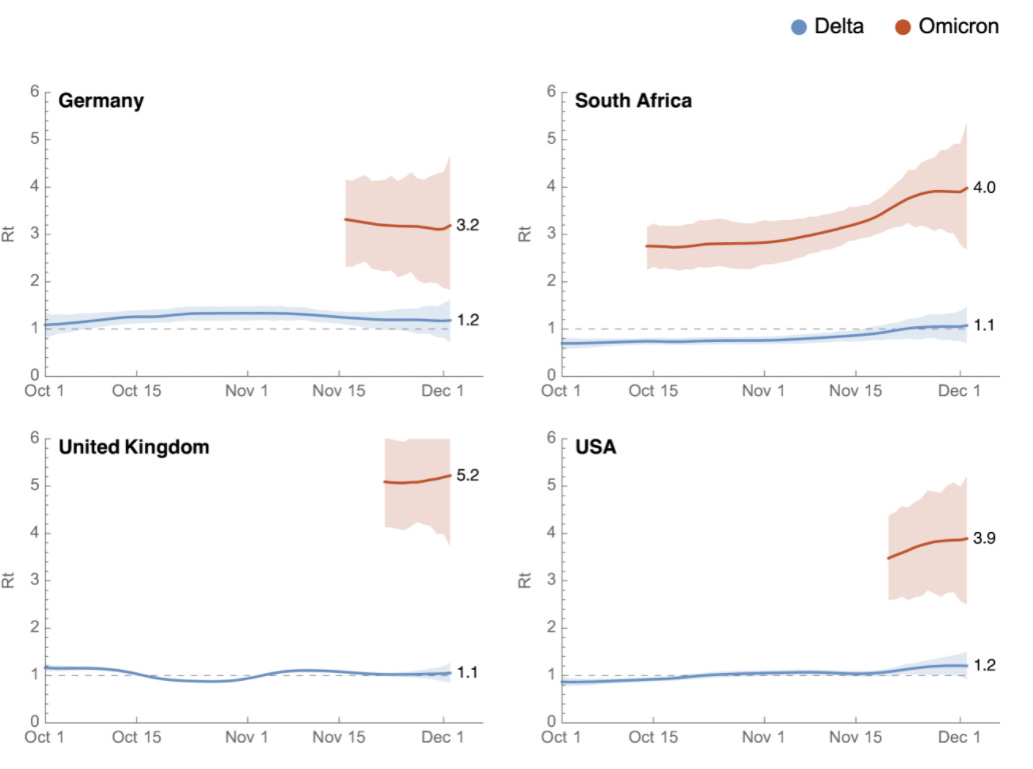
Here’s what’s happening at Polymarket.
Paxlovid approval by end of the year is back up to 35% based on there being a plausible schedule, and the others are interesting, but I will focus here on the Omicron ones.
Variant of High Consequence remains at 12%. Given no movement towards doing this and the month ending one day at a time, this likely should be declining faster than it has, but I thought it was a little low before. I have no problem with it now.
The Omicron-share-of-American-cases markets, are now:
1% of cases by year’s end: 93%.
10% of cases by year’s end: 77%.
50% of cases by year’s end: 20%.
These all seem low. We are going to go over 50% of cases well before year’s end in Denmark and the United Kingdom, and growth in the United States doesn’t seem that much slower. The 1% line is reflective of prediction markets not handling extreme odds well due to capital issues, this should be much higher. The 10% level also seems like it would be pretty strange if we don’t hit it, and I’d definitely buy this to at least 85% and would have my fair at least at 90%. For the 50% threshold, it’s hard for me to understand why this is an underdog at this point, given the data source is aiming to be backward-looking. I do want to give some respect to the market, but I still see this as at least 50% to happen. I wouldn’t bet against it happening at almost any price unless I had a way to hedge.
Probability Updates
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 75% → 85%.
We know for a fact it has a much bigger than 100% advantage right now in the West. That includes the potentially large advantage for being new, so how confident to be here depends on the spirit of the question. But with this much escape, it seems increasingly hard for this to be wrong.
Chance that Omicron will displace Delta as most common strain: 96% → 98+%.
The graphs are very clear. This is going to happen. I will stop reporting on this one unless it goes down.
Chance that Omicron is importantly more virulent than Delta: 4% → 3%.
Chance that Omicron is importantly less virulent than Delta: 55% → 60%.
The evidence slowly adds up, but that’s mostly what one would expect. The one English death is disappointing. We won’t know much for a while.
Will the CDC label Omicron a variant of high concern before 2022? 12% → 11%.
No movement so notching this downward.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 60% → 50%.
I’m lowering this back down because of the comments that Omicron boosters might be unnecessary, and a general sense that authorities don’t care much about this happening. They might well try to pretend this isn’t necessary to avoid a mess of some kind.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 25% → 25%.
I need to game this out more to get a better idea of what would trigger this kind of response, regardless of whether anyone wants to do it or has any intention of doing it before the crisis happens. So I notice I’m not confident in this estimate but I don’t have a better one.
Will Omicron be >1% of all cases by the end of the year? 94% → 97%+.
The timing seems like it’s baked in and this may well have already happened. I’m putting on a plus to indicate that I’m including model error and cowardice a bit in not going higher, which means I’d never accept a bet against this happening at anything like these odds.
30 comments
Comments sorted by top scores.
comment by Charlie Steiner · 2021-12-15T14:12:59.287Z · LW(p) · GW(p)
I think the best antidote to "cowardice" is thinking about probabilities on a log scale once you get close to 0 or 1. The same likelihood ratio moves your log odds the same amount no matter the starting point, which basically means that going from 90% to 99% and going from 99% to 99.9% are steps of the same size.
Thus, I present the "number of nines" technique. Probability 0.9 (a.k.a. 90%) is one nine. Once you're at one nine, further evidence should be measured in "number of nines" (number of powers of 10 in the likelihood ratio) E.g. "the growth rate data from Denmark and the UK provides about 1.3 nines of evidence (likelihood ratio something like 15:1) that Omicron is taking over before the end of the year." Then to add up your evidence, you just add up the number of nines. Four nines = probability 0.9999.
It's easy to end up over-confident with this technique if you accidentally double-count evidence, but it's a really good antidote to feeling like you have to stop all of your probability estimates at 99%. Between seeing South Africa and Denmark and UK data, I think we are at >3 nines for Omicron being more than 1% in western countries by the end of the year.
comment by arunto · 2021-12-13T19:56:05.618Z · LW(p) · GW(p)
Bredford's new data for Germany are quite interesting. An Rt of 3.2 with widespread mask mandates, compulsory testing for many public situations and something like a partial lockdown for unvaccinated persons (even though the vaccination status may not be that important for the spread of Omicron, locking down any 25%+ of the population should have a meaningful effect) leads me to the following predictions:
1. To stop the spread of Omicron (if that is what one really wants given the costs associated with it) a more or less full lockdown of all nonessential social activities would be necessary (whether that would be sufficient is a different question). - 75%
2. Since the German healthcare system (and those of many other European states) is near the limit of its capacity (primarily because of staffing shortages for intensive care beds), there will be a lockdown in Germany starting before January 15. - 55% (even if 1. were true, Omicron could be significantly less virulent).
3. Given the seasonality of the virus and the US being about 1 month behind Central Europe when it comes to the onset of autumn, the Rt in the US will increase to 4.5 or higher (more in the direction of the Rt in the UK). - 75% (could be lower if the control system kicks in fast).
comment by avturchin · 2021-12-14T19:48:50.362Z · LW(p) · GW(p)
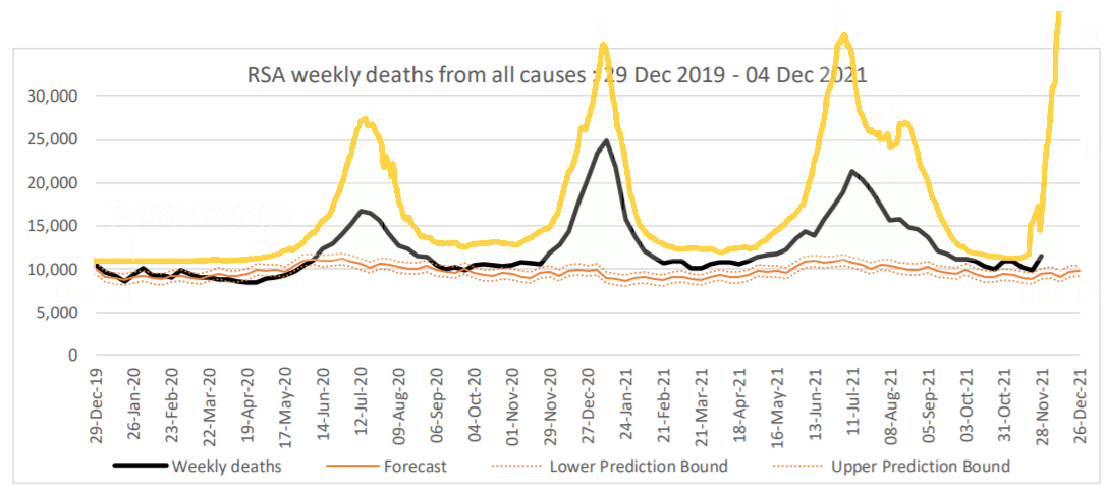
Excess mortality is growing is South Africa, for last week of November, it was 1000 above trend. https://www.samrc.ac.za/sites/default/files/files/2021-12-08/weekly4Dec2021.pdf
Replies from: simon↑ comment by simon · 2021-12-15T20:03:15.954Z · LW(p) · GW(p)
Overlay comparing with new cases from https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/south-africa/ (yellow line). I think I have reasonably accurate x-axis scaling, not sure about x-axis position. Y axis position and scaling is arbitrary (scaling based on preserving aspect ratio of original charts, position for easy visual comparison to line for total deaths).
comment by Eric Neyman (UnexpectedValues) · 2021-12-14T03:59:20.839Z · LW(p) · GW(p)
For personal reasons it made sense for me to calculate the percentage of Londoners who will have COVID this Thursday, the 16th. The number I got was much higher than I intuitively expected: 10%. Please point out any errors you see!
- Among specimens collected in London 5 days ago, about 8000 were positive. This is relative to 4000 before the recent rise in cases, suggesting about 4000 are Omicron. Source
- Omicron doubles at a rate of 2.5 days in the UK. Source
- So among specimens collected Monday, we’d expect ~16k Omicron cases. Among specimens collected Thursday the 16th that should be ~35k.
- As a ballpark guess, we might guess that about half of cases are caught, so that’s ~70k.
- The typical time period between someone catching COVID and getting tested is 5 days. So the number of Londoners who will catch COVID on Thursday is ~280k, since they’ll typically get tested 5 days (two doublings) after that. That’s about 3% of the population of London.
- Omicron grows by a factor of ~1.3 per day, so (3/1.3)% will catch COVID on Wednesday, and so on. The total percentage of Londoners who will have COVID on Thursday is thus ~10% (summing the appropriate geometric series).
Thoughts?
Replies from: Lukas_Gloor, gabriel-holmes↑ comment by Lukas_Gloor · 2021-12-14T10:19:25.342Z · LW(p) · GW(p)
For reference, the Zoe symptoms app project estimates around 1.3-2% prevalence of symptomatic Covid for London burrows: https://covid.joinzoe.com/data
I think asymptomatic cases are maybe 40%? Have seen it be a bit higher, but I doubt the higher numbers for asymptomatic cases. Going with 50% asymptomatic, this would indicate prevalence of 2.6-4%. That's for today. Your estimate is 2 days in the future, so plausible but maybe a bit high?
Under the assumption that Omicron is 50% of cases today, and doubling time 2.5 days, maybe that would give 5-6% on the 16th.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-14T10:14:03.863Z · LW(p) · GW(p)
R0 will go down a bit as more people become immune to Omicron, but...sure.
comment by tkpwaeub (gabriel-holmes) · 2021-12-14T10:10:53.339Z · LW(p) · GW(p)
On the matter of Paxlovid not having been approved yet, I'm considering writing to the CDER Ombudsman:
https://www.fda.gov/about-fda/cder-contact-information/cder-ombudsman
And cc'ing my elective reps. As a hedge, and so as not to be accused of foul play if I decide to jump into any of the prediction markets, I might bet against my preferred outcome (rapid approval)
comment by davelaing · 2021-12-15T22:37:35.244Z · LW(p) · GW(p)
It looks like there might be an Omicron variant which doesn't have the S gene dropout [1]. I'm wondering how that might impact various modelling efforts, but haven't had time to think it through.
[1] https://www.abc.net.au/news/2021-12-08/qld-coronavirus-covid-omicron-variant/100682280
comment by tkpwaeub (gabriel-holmes) · 2021-12-15T21:07:30.736Z · LW(p) · GW(p)
Does anyone have any leads on the idea that attrition could be making Omicron appear milder? Are the least "Covid-hardy" humans being picked off?
Replies from: Zvi↑ comment by Zvi · 2021-12-15T21:38:30.865Z · LW(p) · GW(p)
Effect size here should be quite small, but not zero.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-20T17:47:04.434Z · LW(p) · GW(p)
I hope you're right about the effect size being small, I wish you'd given me a convincing argument that it's zero using some sort of brilliant sophistry, and I wish I was the only person speculating this. Sadly I'm not:
https://twitter.com/tomtom_m/status/1472561128240824324?t=PjtsZrO-mIrUWzdjTsF3Gw&s=19
comment by tkpwaeub (gabriel-holmes) · 2021-12-16T09:58:06.039Z · LW(p) · GW(p)
I would actually rate the probability of a "pancoronavirus vaccine sometime in 2022" at 60%, which is why I doubt there's going to be an Omicron specific vaccine. Evusheld will probably be updated for Omicron, however.
comment by philip_b (crabman) · 2021-12-13T20:47:39.140Z · LW(p) · GW(p)
The two plots of the proportion of Omicron among new cases of Covid-19 you posted are from Denmark and the region around Washington. They show that in these locations now or in the next few days approximately half of new cases are Omicron. I am from a country that doesn't really track statistics of Omicron vs Delta. Is it a good idea to assume that the situation here is approximately the same as in these plots? More specifically, how was the decision to include these plots in this post made? Were these plots included specifically because they look scary or are they more like a truly random sample of locations?
Replies from: Zvi, npostavs↑ comment by Zvi · 2021-12-14T09:44:12.346Z · LW(p) · GW(p)
They are the only plots I have seen. If anyone has known others I would like to know.
Replies from: Vitor↑ comment by Vitor · 2021-12-15T09:45:25.711Z · LW(p) · GW(p)
data from Switzerland: https://www.covid19.admin.ch/en/epidemiologic/virus-variants
↑ comment by npostavs · 2021-12-14T13:34:50.945Z · LW(p) · GW(p)
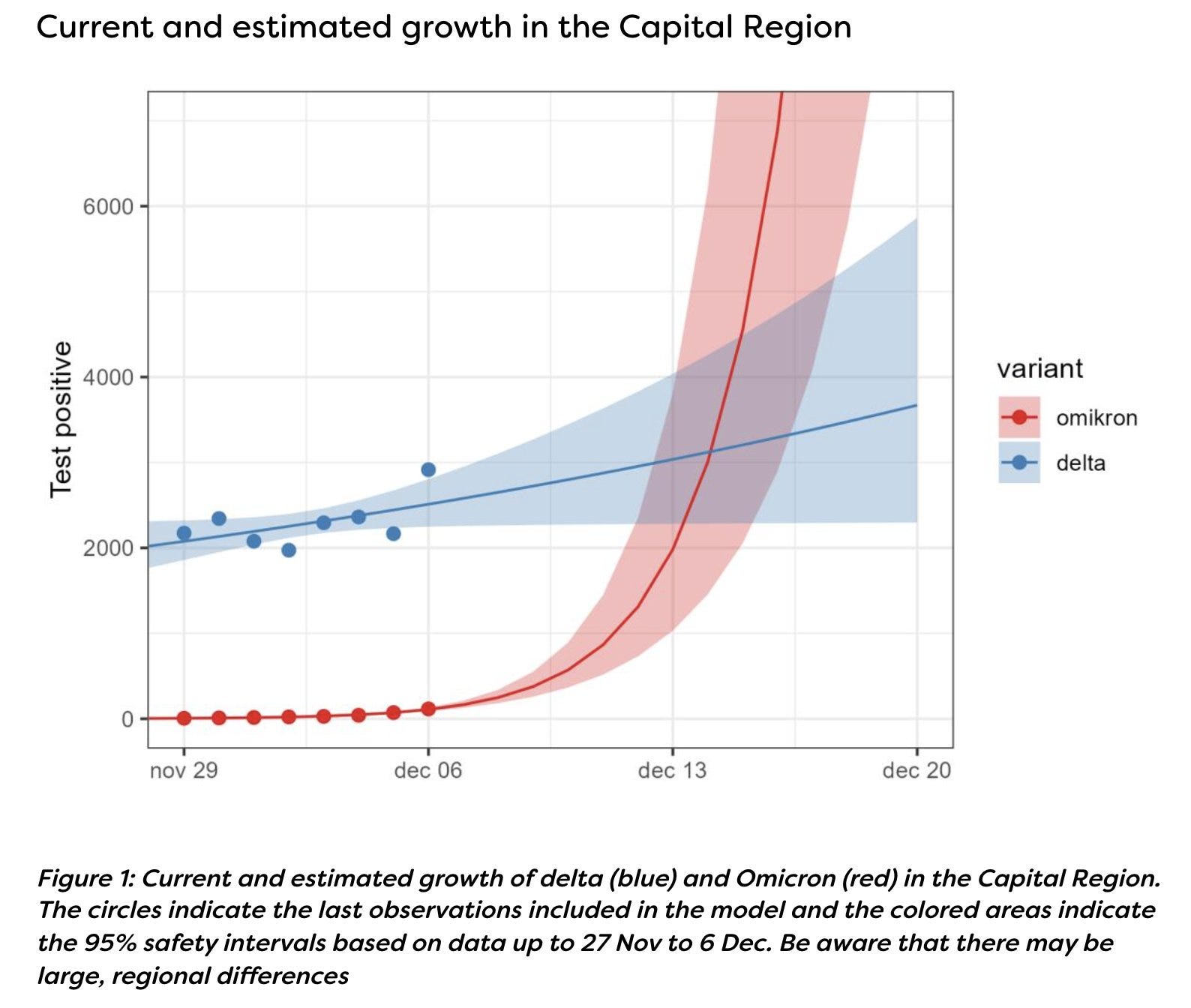
If by "region around Washington" you meant the graph labeled "Capital Region", I think that refers to the capital of Denmark.
Replies from: crabman↑ comment by philip_b (crabman) · 2021-12-14T13:52:37.812Z · LW(p) · GW(p)
Oh, indeed.
comment by Gurkenglas · 2021-12-13T18:30:09.172Z · LW(p) · GW(p)
What probability do you assign that half a year from now you'll think that we really, really should have closed most borders for the duration of the peak to avert more variants sweeping the globe?
Replies from: Zvi↑ comment by Zvi · 2021-12-14T09:45:46.304Z · LW(p) · GW(p)
Basically zero. This isn't sustainable in a way that could work.
Replies from: Gurkenglas↑ comment by Gurkenglas · 2021-12-14T10:56:15.958Z · LW(p) · GW(p)
The idea was that if it's sustainable for a month, we might notice the death rate suddenly going up different amounts in 3 countries, accompanied by the sound of Overton windows breaking. You don't think a sufficiently lethal and salient pandemic would have everyone declare the atmosphere a no-fly zone at turretpoint?
Replies from: jaspax, Zvi↑ comment by jaspax · 2021-12-14T16:38:06.707Z · LW(p) · GW(p)
They key phrase in your comment is "sufficiently lethal", and COVID ain't.
Replies from: Gurkenglas↑ comment by Gurkenglas · 2021-12-14T18:29:04.495Z · LW(p) · GW(p)
Yet! But "the ~90% of the world that haven't been infected yet won't spawn lethal variants" is the kind of expert prediction that I can buy. :)
Replies from: cistrane↑ comment by cistrane · 2021-12-19T14:03:54.875Z · LW(p) · GW(p)
On what data do you base the estimate that 90% of the world population haven't been infected by the novel coronavirus by now?
Replies from: Gurkenglas↑ comment by Gurkenglas · 2021-12-19T15:28:03.375Z · LW(p) · GW(p)
I googled "covid cases worldwide" for ~3% and thought "probably a bunch of cases are never tested". Do you think even more people have been infected?
Replies from: cistrane↑ comment by Zvi · 2021-12-14T16:00:43.515Z · LW(p) · GW(p)
Omicron isn't like that. So your proposal is to do this pre-emptively, before the threat arises, and sustain that forever? Yeah, not happening, and not going to feel bad about not doing it.
Replies from: Gurkenglas↑ comment by Gurkenglas · 2021-12-14T18:27:13.699Z · LW(p) · GW(p)
It wouldn't have to be forever. It would on the mainline be the about one-month duration of the peak, after which one would see that there are no new catastrophic variants. If there actually is a new catastrophic variant, then one can keep borders closed around that country for the... half a year? it takes to develop/distribute vaccines/treatment.
Replies from: Zvi↑ comment by Zvi · 2021-12-14T19:29:09.993Z · LW(p) · GW(p)
I'm confused what you think this accomplishes - by the time you know to close the border the new variant is already in your border. Even if a new variant arose during the month you're closed, you probably open up before you know it exists, and lose anyway.
Replies from: Gurkenglas↑ comment by Gurkenglas · 2021-12-14T19:42:34.215Z · LW(p) · GW(p)
Yes I'm not talking about reacting to a new variant by closing, only about closing in advance. If a variant will spread across borders months before it is discovered because we can't afford to sequence every case, then I agree this doesn't work. I assume we don't have a poolable test that excludes known variants.