Omicron Post #7
post by Zvi · 2021-12-16T17:30:01.676Z · LW · GW · 41 commentsContents
United Kingdom Denmark South Africa Elsewhere The Lab on Vaccines The Lab on Spread Severity Official Statements Response The Lab Leak Hypothesis Part 2 Probability Updates Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 85% → 90%. Chance that Omicron is importantly more virulent than Delta: 3% → 3%. Chance that Omicron is importantly less virulent than Delta: 60% → 60%. Will the CDC label Omicron a variant of high consequence before 2022? 11% → 11%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 50% → 30%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 25% → 35%. Will Omicron be >1% of all cases by the end of the year? 97%+ → 99.9%+ None 41 comments
Here are some better worlds we might have lived in, but don’t.
- In a better world, I could focus on this full time and also maybe even hire a research assistant, and be better able to scour for information.
- In a better world than that, there would be a department at a newspaper, or some other such place, that scoured the world for data sources like SGTF deletion counts and wastewater concentrations that could help us understand spread, called the sources to attempt to get the best data possible, and complied it all in nice form.
- In an even better world than that, there would be funding, either public or private, for the actual gathering of additional data.
- In an even better world than that, we’d have run challenge trials the moment Omicron was detected, and we’d already have all our answers.
Alas, instead, we live in this world, where none of those things are true. I am grateful to all my news sources and those who help gather the information together, and everyone working tirelessly in the lab, but the whole thing is still a slapstick hodgepodge, and we know so much less than we could know so much slower than we could know it.
Still, we do the best we can.
This time out, we have a few new places whose data has been located, to supplement the United Kingdom and Denmark. We also have several important new lab results.
There is some uncertainty about how far along things are. There is uncertainty regarding how much milder Omicron is than Delta, from it being essentially the same (but much better on a per-case basis due to who it infects) to there being a substantial or even large difference.
But the main uncertainty that I’m now wondering about, that feels central, is how we will react.
What will happen when the rice grains on the chessboard suddenly get fully out of hand, stuff hits the fan and the hospitals overflow? Not if. When. How will governments react? How will the people react?
Last year, I created a toy spreadsheet to model how the rise of Alpha might go, and whether the control system (governments and individuals reacting to the levels of cases, hospitalizations and deaths by scaling up or down prevention measures) combined with vaccinations could handle it. I invite everyone to copy, modify, mess around and find out, and create their own toy models. There are a bunch of things in column AH that you can modify to see what they imply. Note that this sheet is designed for my own use rather than public consumption; it seemed useful to share it anyway but it’s very much not optimized for that.
Prediction markets believe and I even more strongly believe that Omicron will become the majority of cases by year’s end in the USA and most of Europe. The question is what happens after that. Will we be able to make the straight line on a logarithmic graph bend before things get completely out of hand, one more time? Or will this be the time it’s too much and we fail?
What are we willing to do to try and not fail? What are we willing to do to be able to claim that we were trying not to fail, even if failure is inevitable? These are the questions.
Meanwhile, there’s still the question of exactly where we are and what are the physical rules of the game, so let’s review the evidence.
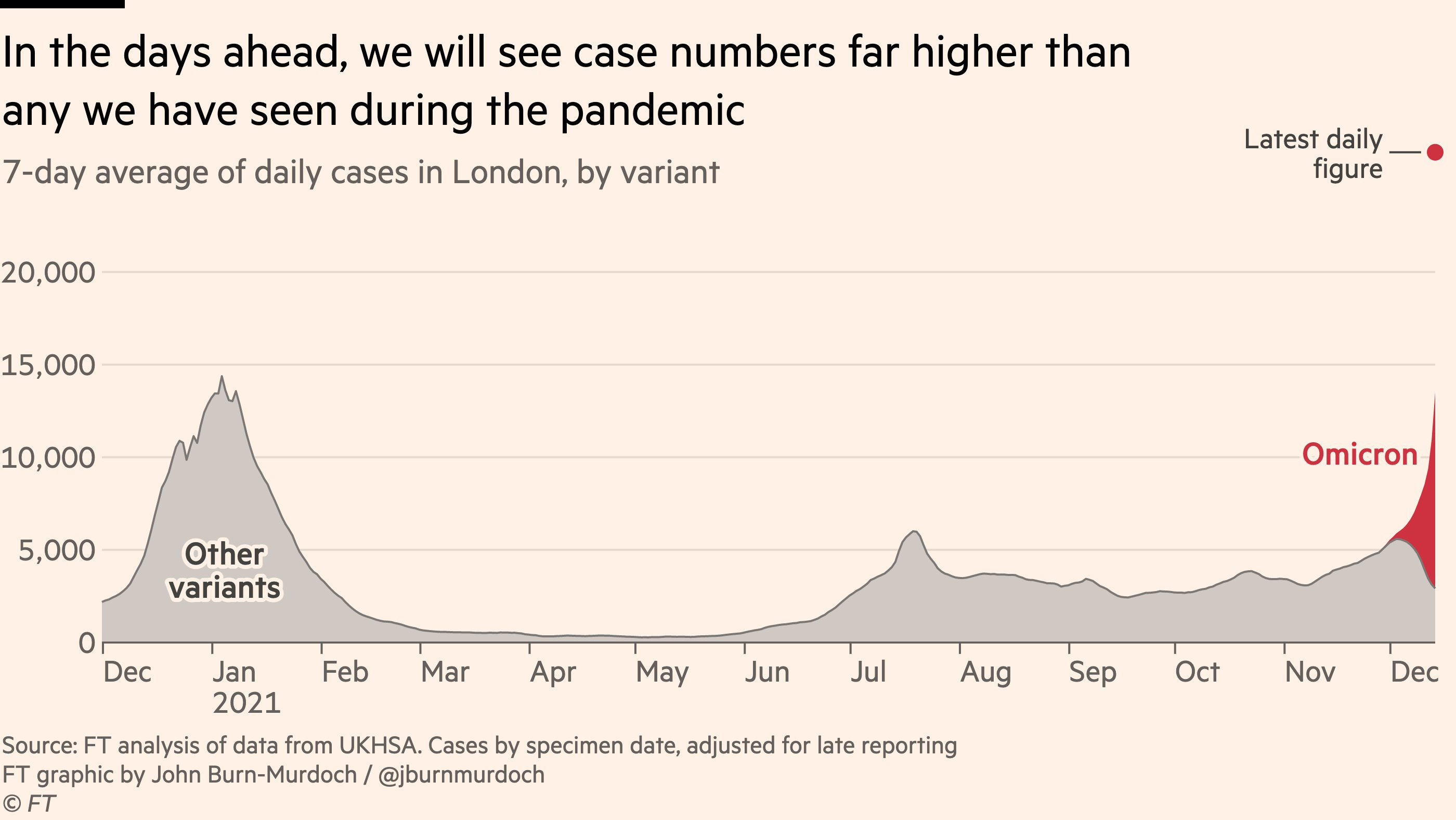
United Kingdom
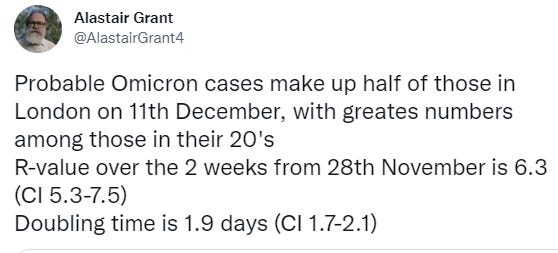
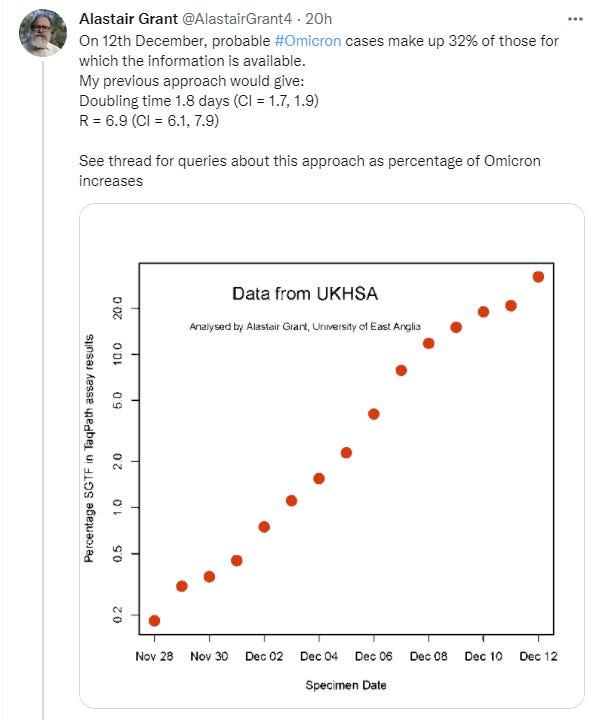
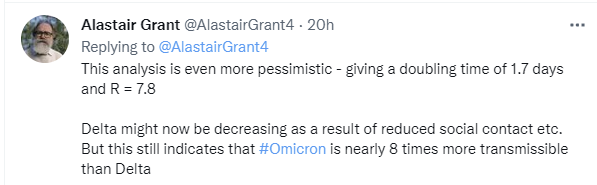
50% Omicron yesterday in London, 60% today, stunning growth rate, the daily cases chart’s last three days are still incomplete.
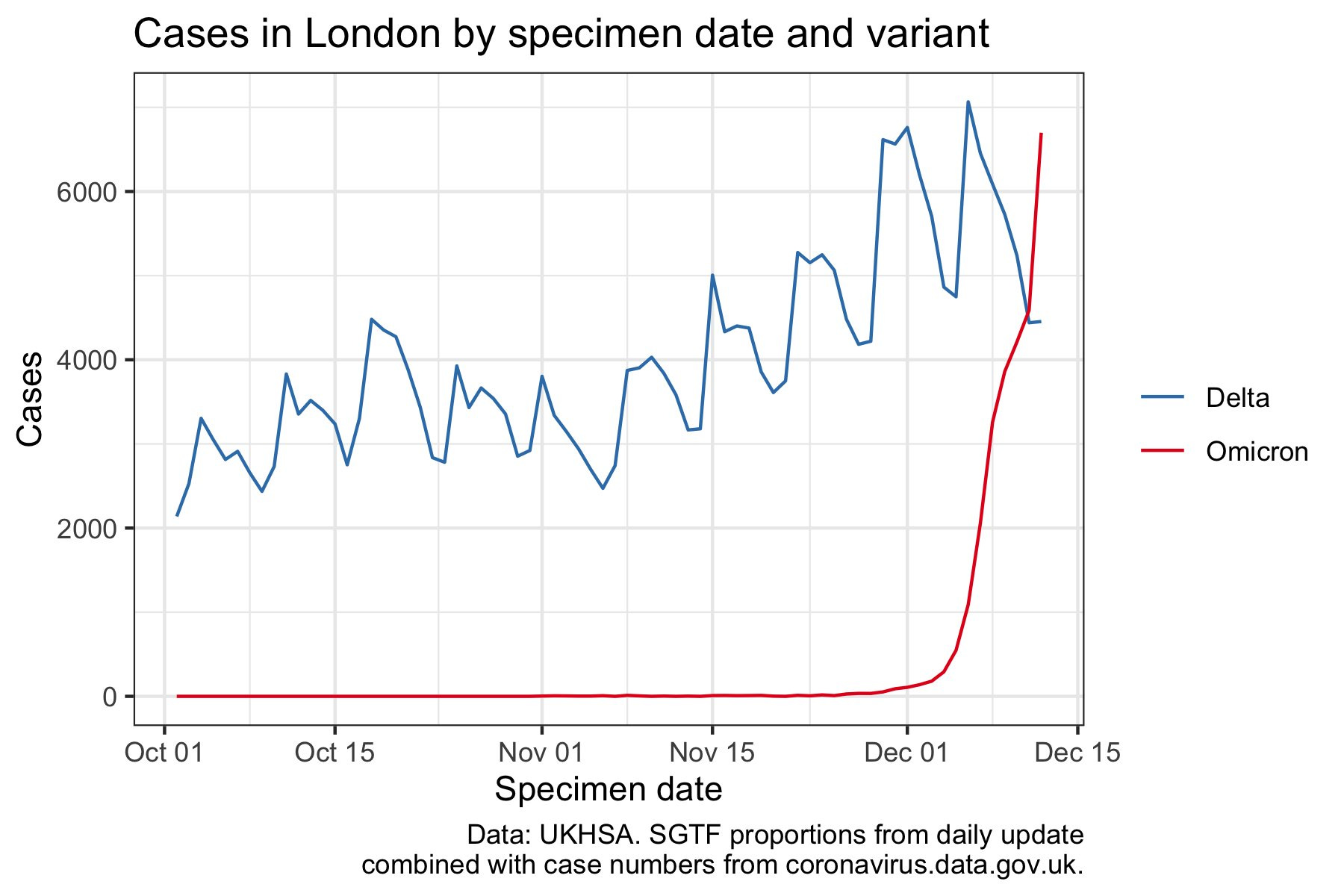
Other regions too, but not as dramatically, here’s the data source:
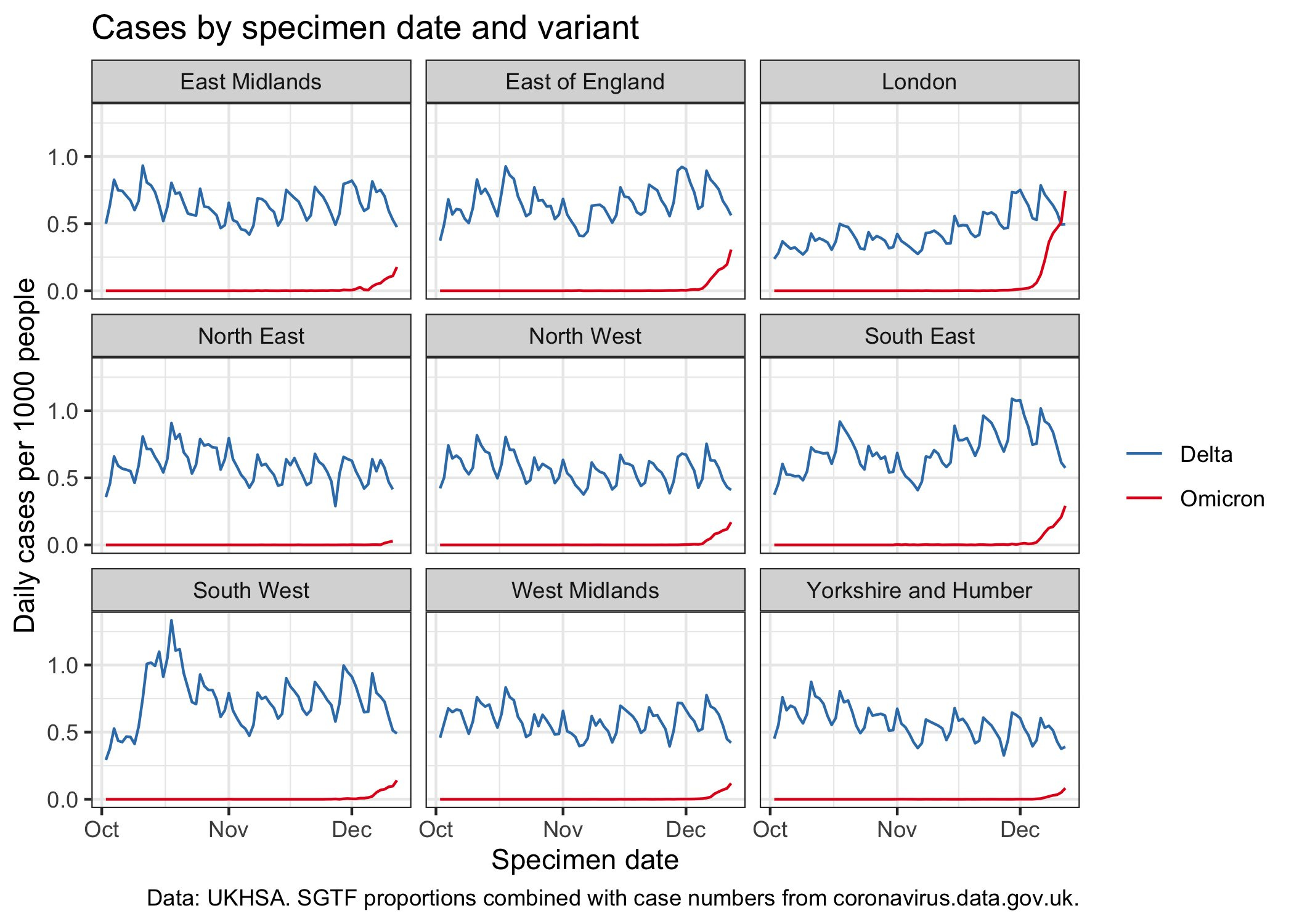
A day older but better labeled:
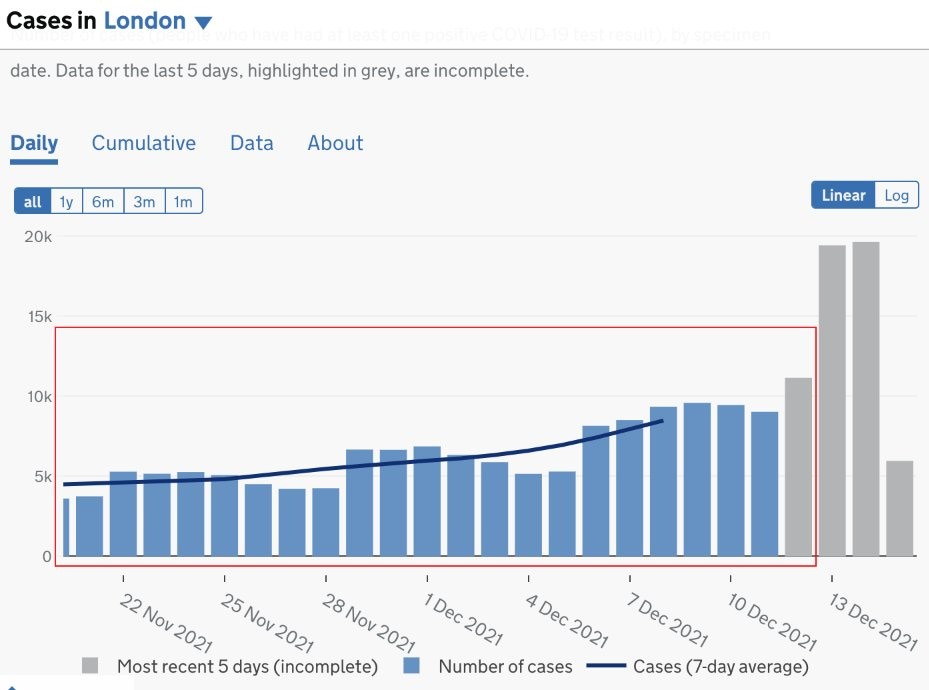
And finally another illustration for London from one day ago:
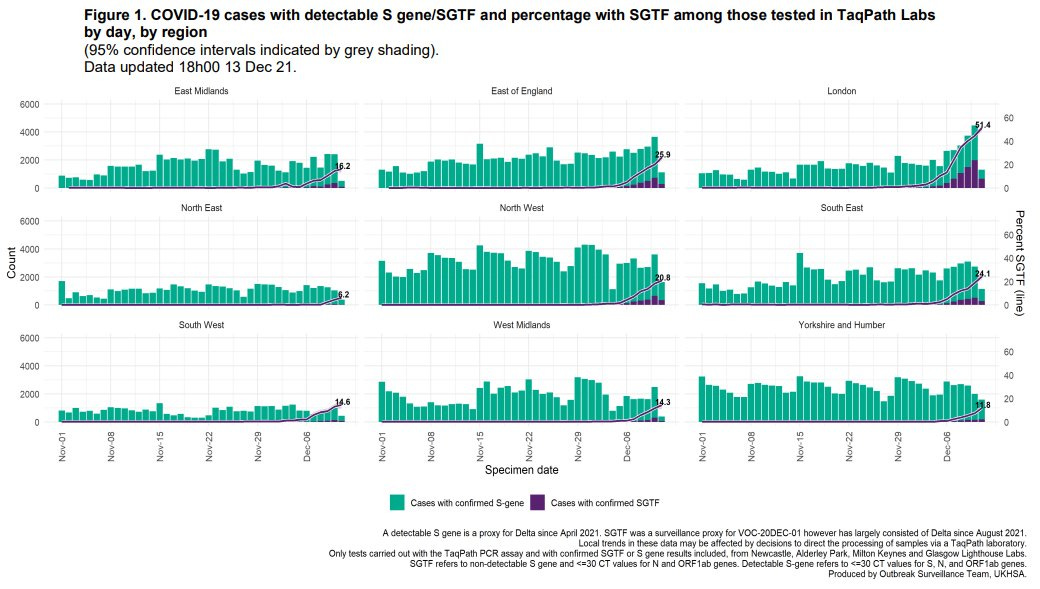
And the synthesis for the nation.
It’s a strange dynamic where Delta is stable in London and stable outside of London, yet in London Omicron goes vertical much faster than elsewhere. It’s a big hint as to how the physical dynamics work, with Delta cases in London even declining rapidly at this point as people adjust. But then again, maybe that’s simply a head start from more international travel, and I’m squinting at graphs wrong. Hard to say.
It also looks like London cases are spreading into older groups.
If you live in London, you have a choice to make right now that is similar to the one many others will likely have to make soon. Do you want to make a real effort to not be infected? We had over 30,000 reported cases in one day out of a population of 9 million or so, with a doubling time of every two days, with several days lag between infection and positive test. It’s reasonable to assume that the number of new infections is now more than 1% of the city per day and probably still increasing fast. If you go about your business as usual, you’re going to get infected. If you don’t want that to happen, extreme prevention measures need to happen now. The good news is that this is not sustainable – by definition you can’t have 1% infection rates per day for very long, and you can have 2% rates per day half as long as that, and so on, assuming no rapid reinfections occur. But it’s crunch time, and decision time.
Denmark
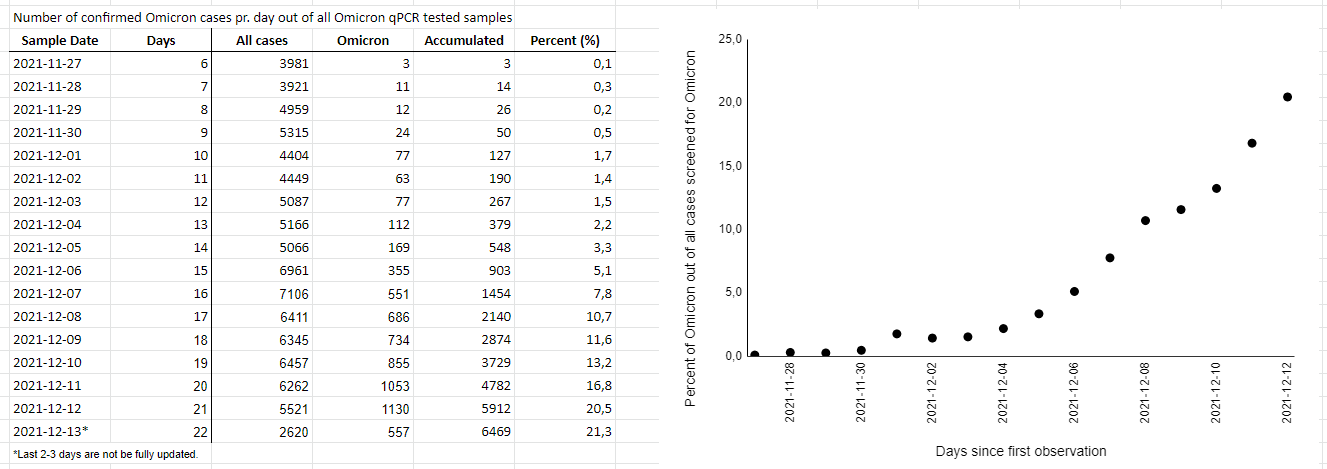

This is a good news style update, as I on average expected things to go faster than this. Best guess is that extra prevention is helping, although it shouldn’t help differentially against Omicron versus helping against Delta. Note the decline in Delta numbers starting on the 8th.
This continues to be our best information source. If things continue to be relatively under control here, that will be very good news.
Note that the UK data and Denmark’s data seem like they live in different universes, with very different relative R0s for Delta versus Omicron. It’s a mystery, and I don’t yet know how to reconcile them.
South Africa
The first real world results are in.
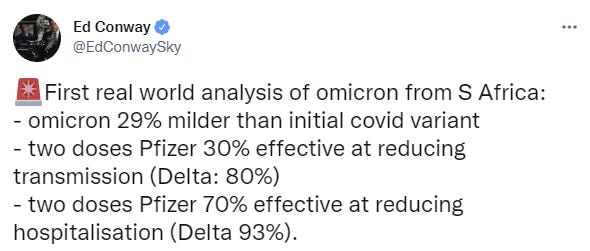
I’m running low on time, so not going to do a deep dive now, but there’s a great thread here for further analysis.
Elsewhere
General roundup of raw case counts:
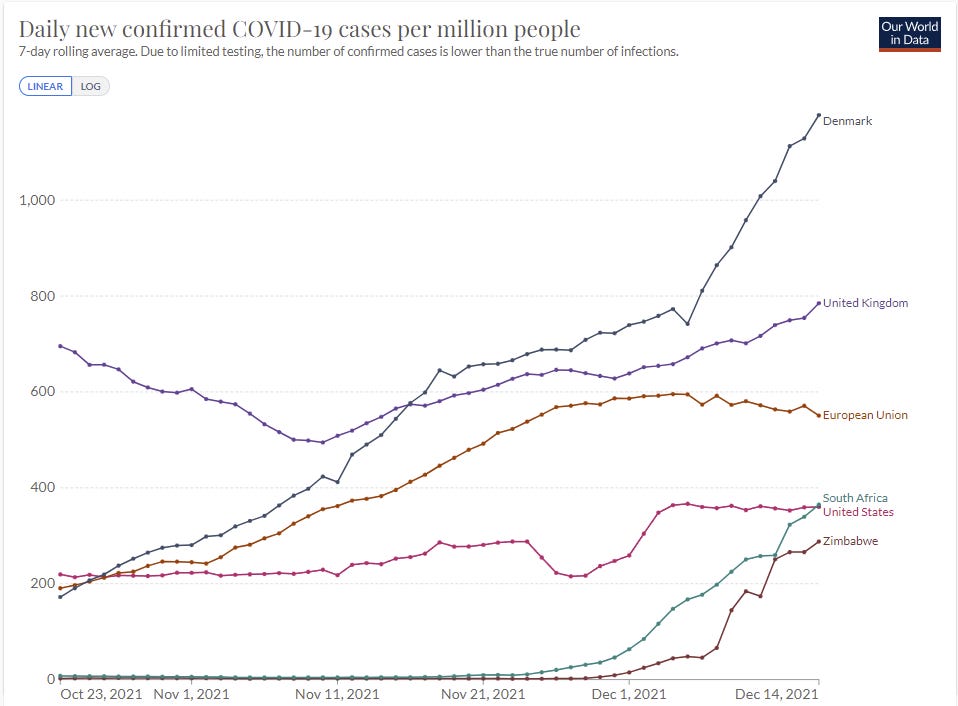
With time, better information sources are available in more places, so this is the round-up. To those who have been sharing sources in the comments, many thanks.
The CDC has a nowcast, which is more like a thencast given it reflects a bunch of lag, but it also appears to be a good faith attempt to synthesize the evidence and estimate what was happening in a given week.
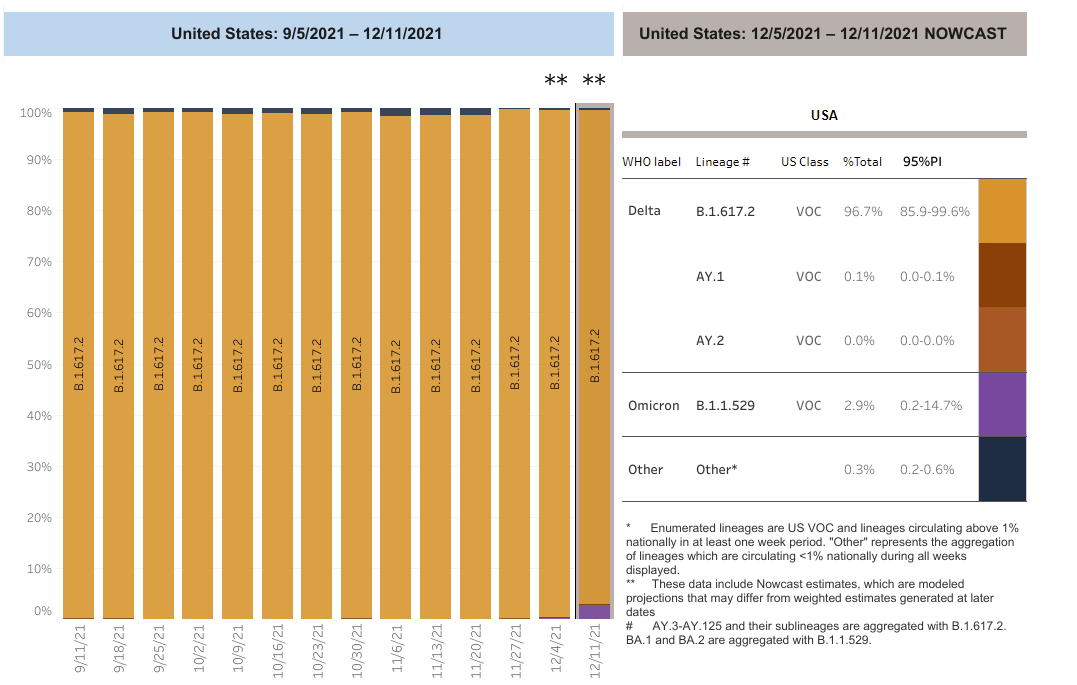
They have Omicron at 2.9% of infections already last week, after being only 0.4% the previous week, which is almost three doublings in seven days. Five days later, if trends continue, this predicts that we should already be at about 20% Omicron cases, because exponentials.
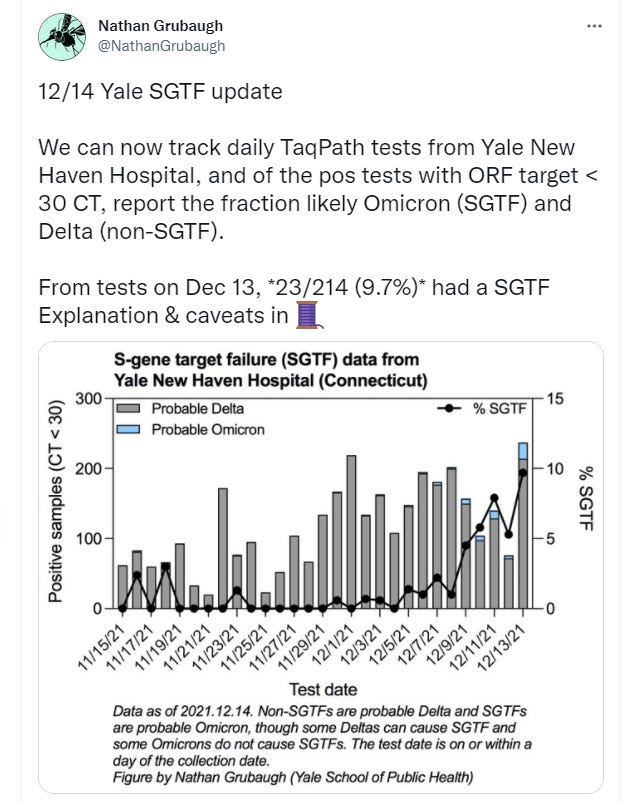
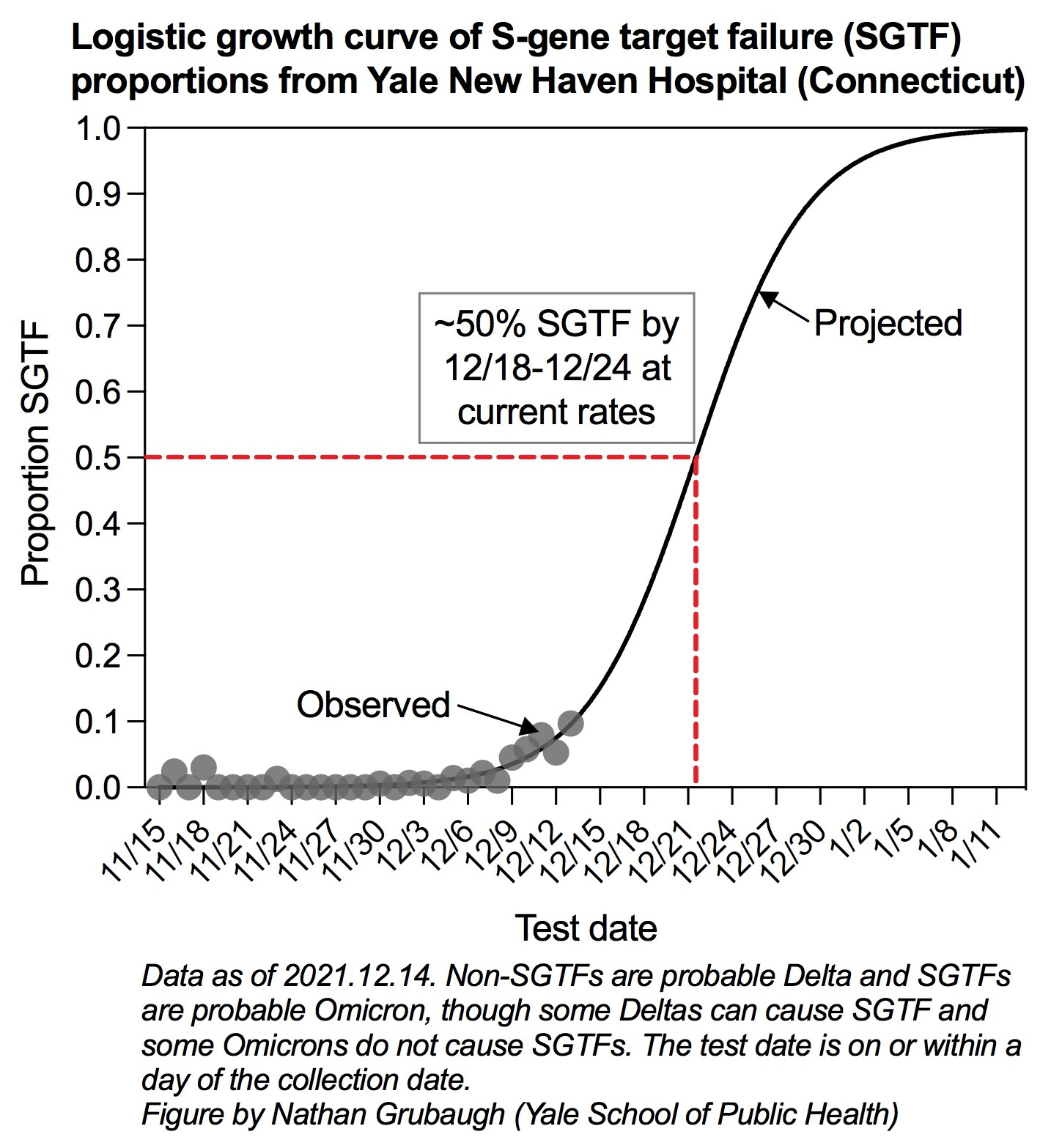
Here’s the word from Seattle. Here’s the University of Washington dashboard, for future reference, things are still too small to show up there, but here’s the SGTF graph. And here’s the updated word.
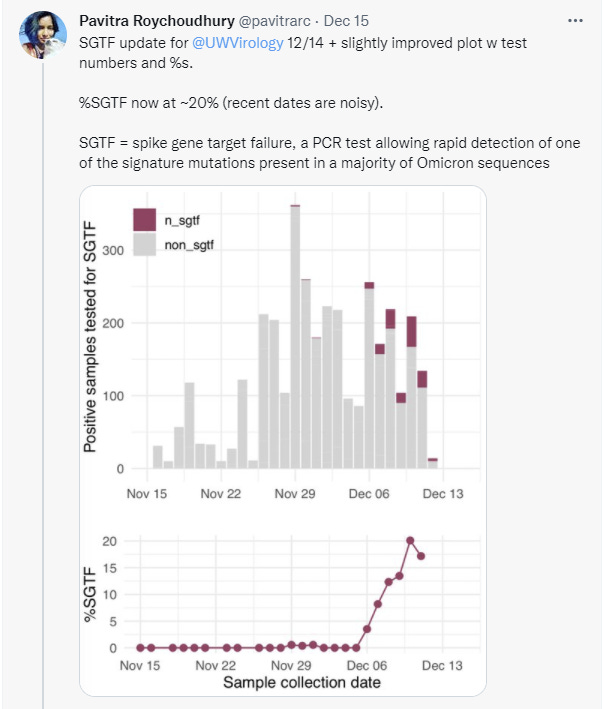


A doubling time of 3.8 days is actually super comforting and good news relative to other places. It can get way worse.
How much worse? Here’s the word from Ontario and all I can say here is holy f*** this is bad, that’s R0 = 7.7 when Delta would be stable, how in the world:
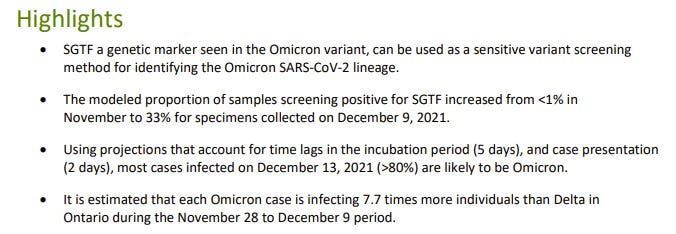
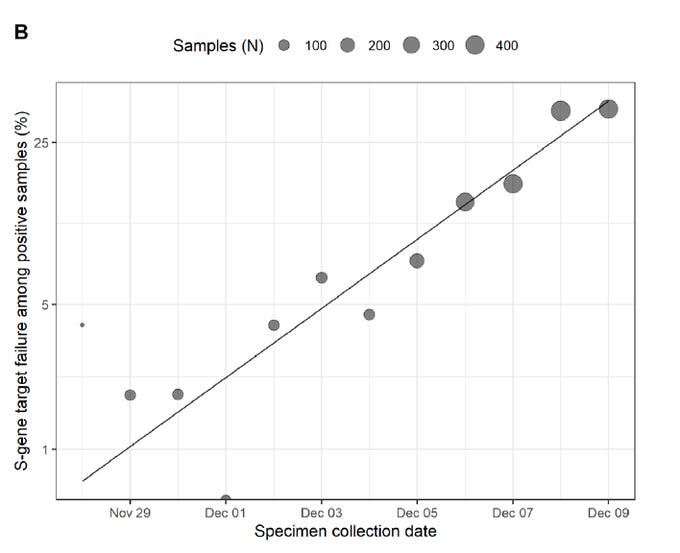
Given our other observations I’d happily take the under on 80%, or on the 7.7 multiplier, but if they’re even remotely close then there are no more reservations about how these exponential curves always blunt themselves and no the whole population won’t actually get infected by the end of February. If these numbers are accurate, it’s game over, man, game over. That doesn’t mean there’s nothing to be done, but it does mean you lose, good day sir, let’s try to do it with dignity and save as many people as we can.
Here’s an EU assessment of what’s likely to come, without predicting how many cases this is. It has the takeover point a week or two into January, which seems increasingly overly optimistic.
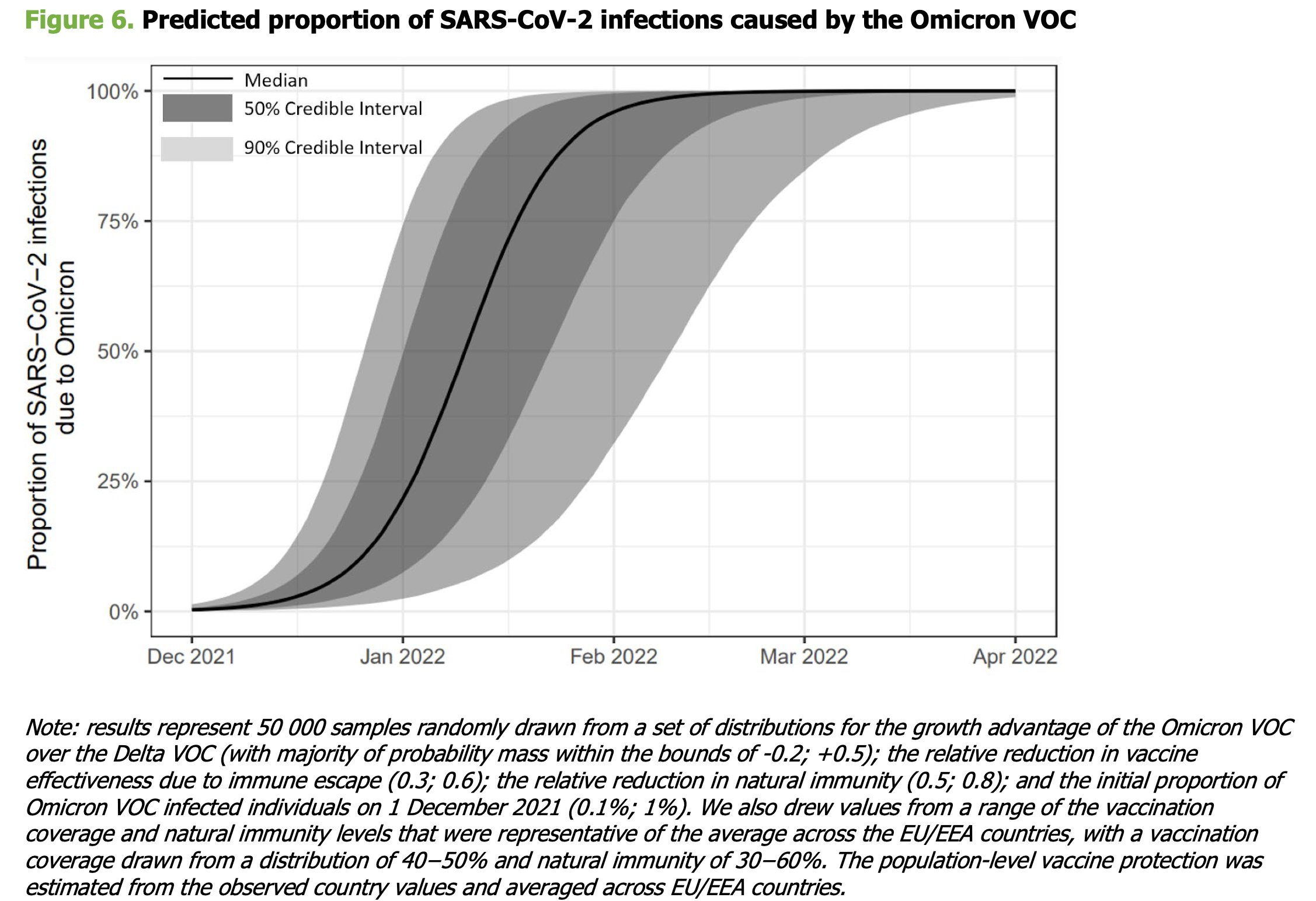
Kai gives a good thread summarizing the report. Here’s their projection for deaths:
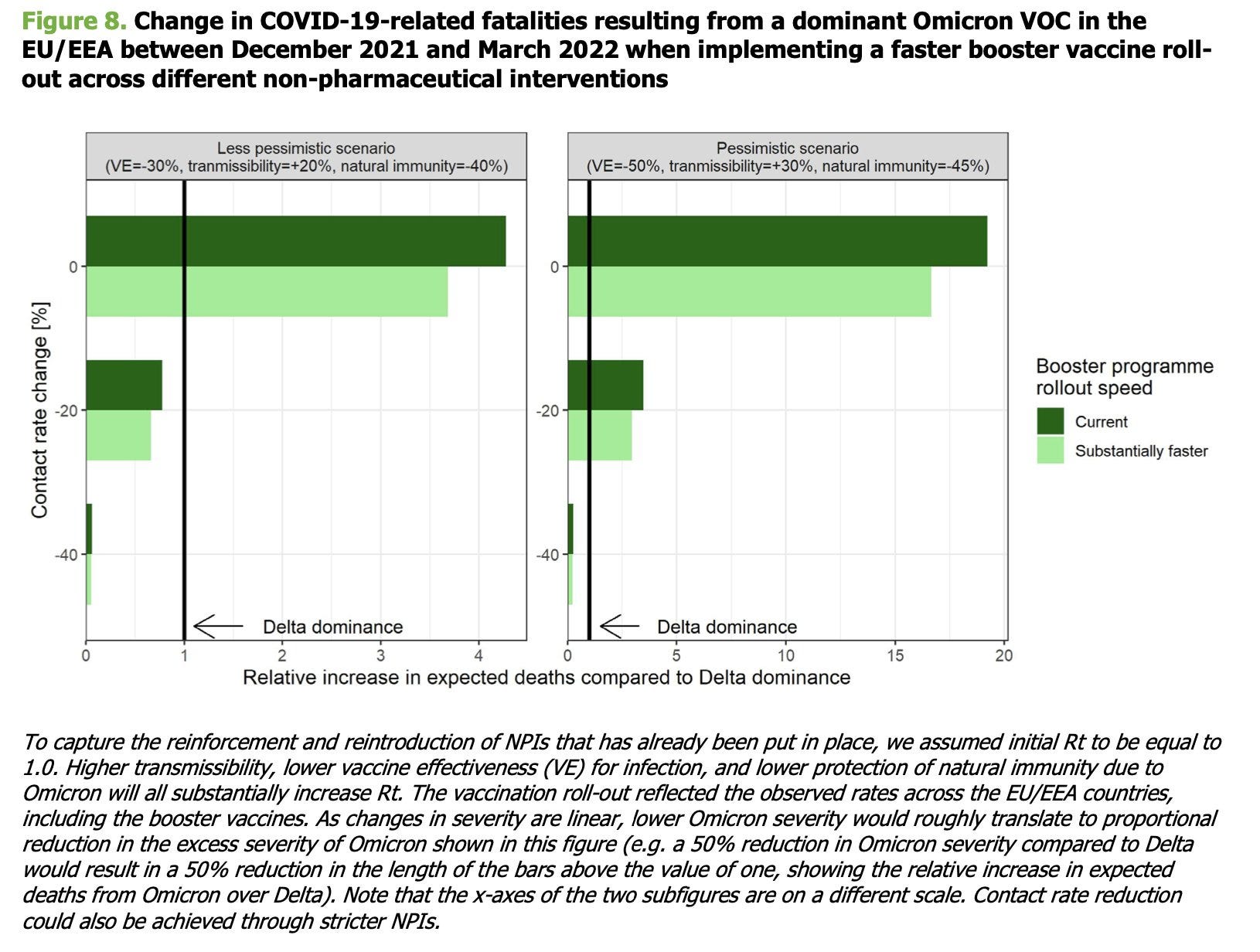
This is not an especially pessimistic scenario. It could happen, but it’s definitely nothing like the worst thing that could plausibly happen.
An interesting speculation on how information sources will change as things evolve.
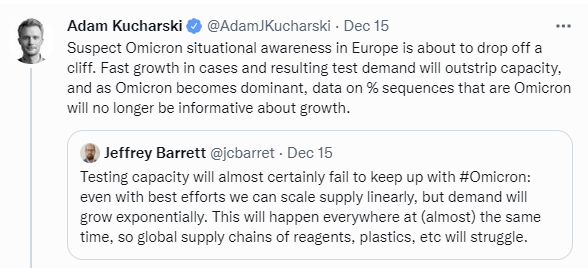
Even in the most optimistic scenarios we run out of tests, and have to adjust to things like positivity rate to estimate number of cases. However, the idea that hospitalizations will provide an alternative data source seems even less hopeful. The number of people in the hospital, even in relatively good scenarios, is going to be more a measure of how many beds there are in the hospital for patients to use, rather than a measure of how many people need those beds. In the good scenarios we manage to give everyone who sufficiently urgently and badly needs a bed a bad, but when we most need to know what’s going on, this won’t help us.
Deaths will tell us, but that’s a month in the rear view mirror, which is an eternity in context.
We’ll continue to get better data continuously everywhere for a while. Then when testing is overwhelmed, we’ll start to have to extrapolate. I still expect to better know where Omicron is at in a month than I do now, but we’ll be solving a very different set of puzzles to figure that out.
Here’s the variant data from Switzerland, which should be a better data source over time, for now maybe they’re behind and maybe they’re not measuring enough.
Omicron is spreading in China. Given their vaccination situation and lack of prior infections this could get ugly quickly. The techniques they used before likely won’t work now, although we’ve been wrong about that before. Definitely one to watch, but not much to go on yet.
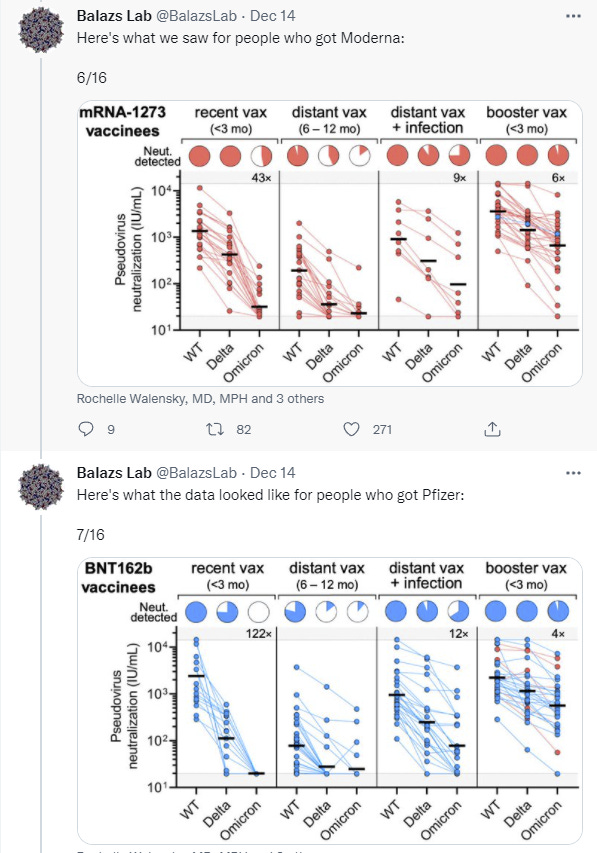
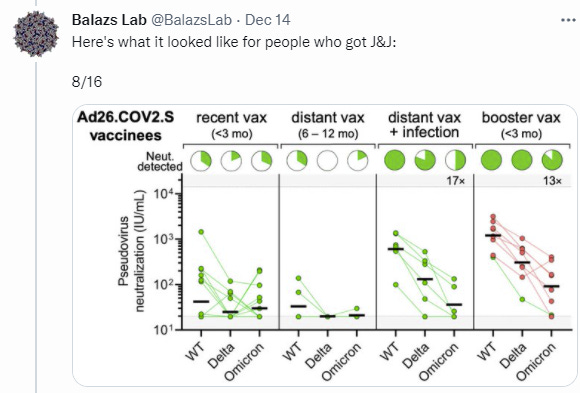
The Lab on Vaccines
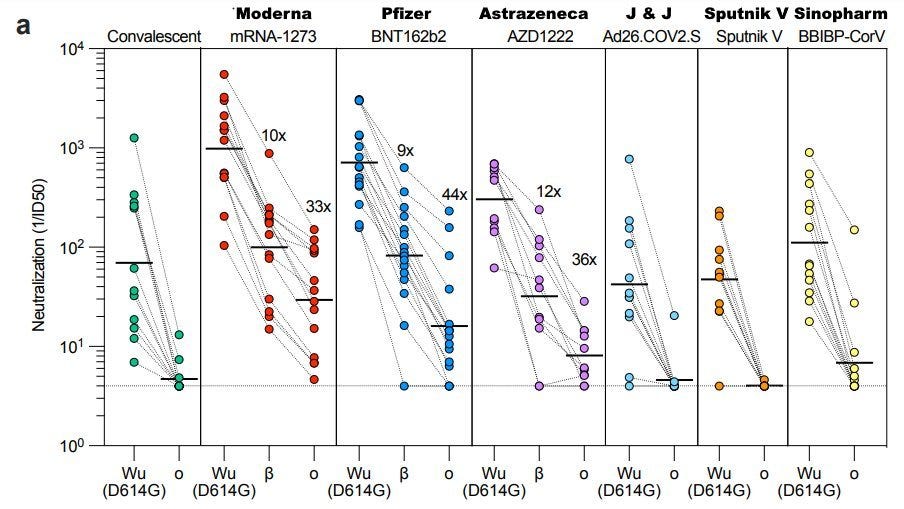
How effective are various vaccines against Omicron after various numbers of doses? We got some good data (paper).

Here is a very good but long analysis thread of another study. Here’s a link to the lab’s thread. There’s lots of very good diagrams.


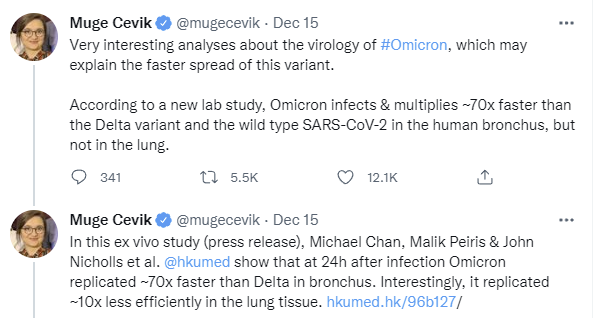
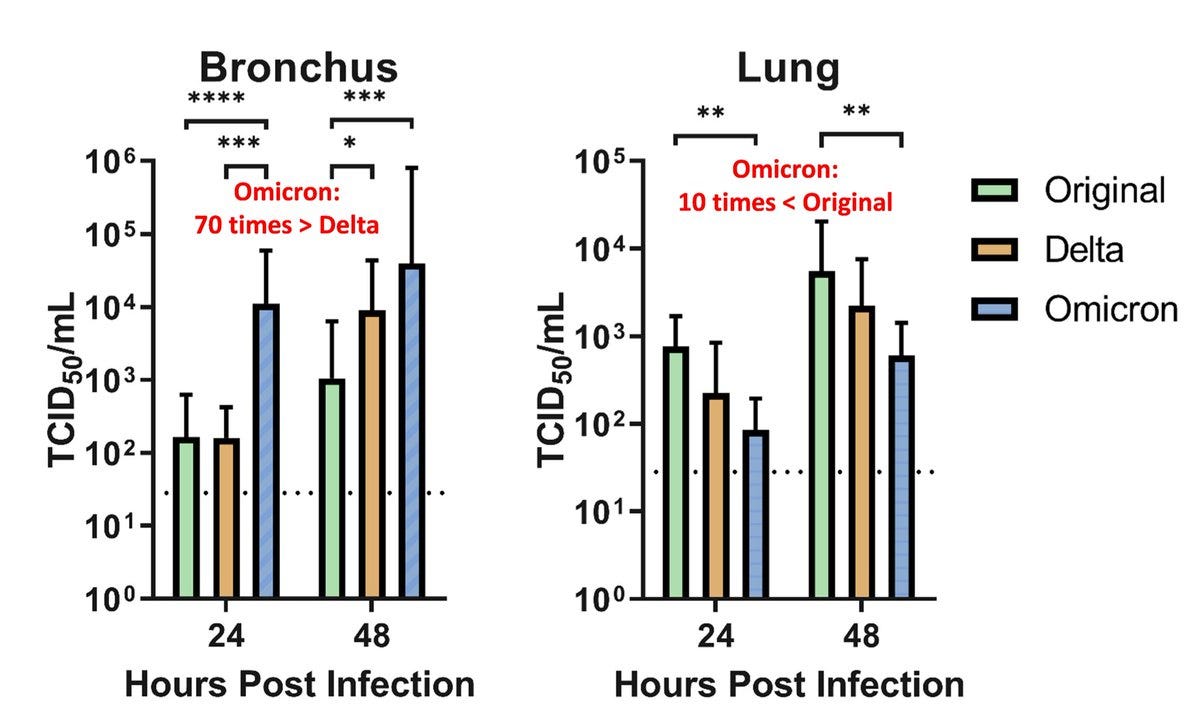
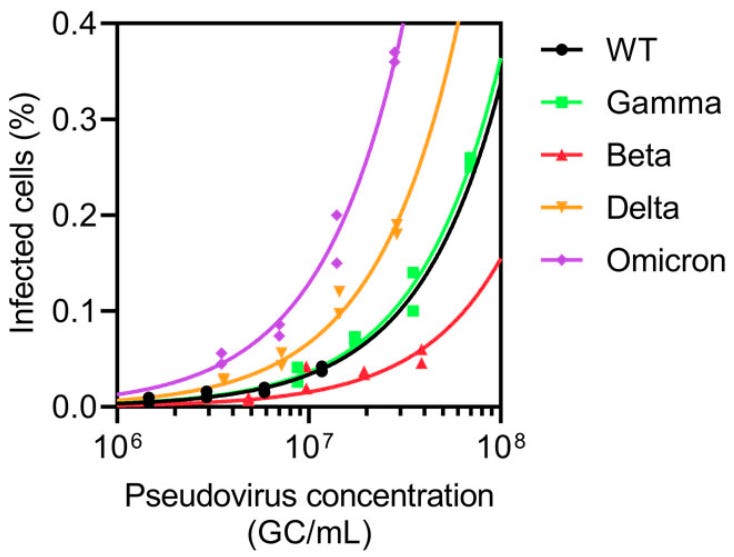
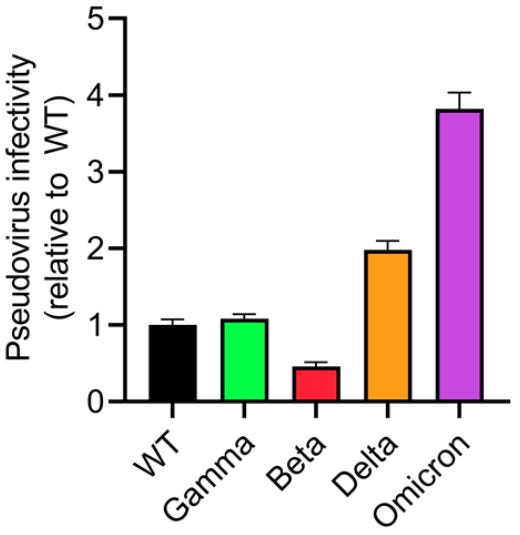
The Lab on Spread
We’re starting to get more color on why Omicron is spreading so fast. It’s not purely that it has escape properties. A lot more is going on. The graphs here are originally from the Balazs Lab study and thread.

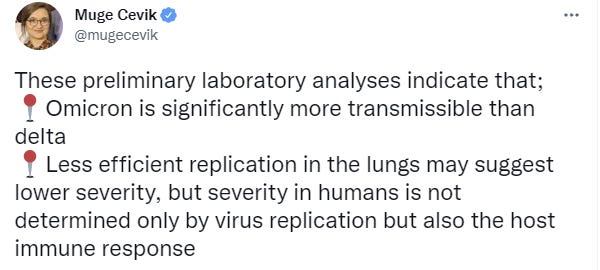
Severity
Andrew Lilley responds to arguments against his case that Omicron is indeed less severe even if you take into account all the other factors, in his analysis they can’t add up to enough and arguments otherwise are increasingly convoluted special pleading.
Official Statements
December 14 statements by Dr. Fauci on Omicron.
He nails the central question of virulence, for which we still lack clarity.
“The real question is, is that an inherent diminution of virulence of the virus or is it because there are so many people in the population who have already been infected and now have residual post-infection immunity — which is not protecting them from getting infected, but is protecting them from getting severe disease?”
He also is clear about what’s going to happen, up to a point.
“Whatever it is, the disease seems to be less severe. Whether it’s inherently less pathogenic as a virus or whether there’s more protection in the community, we’re just going to have to see when it comes in the United States. And for sure … it is going to be dominant in the United States, given its doubling time.”
What he isn’t then quoted as saying is anything regarding what happens when it does become dominant. There’s still pure denial about the size of the wave that is going to hit soon thereafter, and no attempt to prepare for it or reckon with the consequences. The correct answer could easily be to let it happen, but one still needs to be ready to do that.
It’s also worth noting that post changes even Fauci’s ‘is going to become dominant’ to a meaningless statement of what might happen, rather than an accurate statement of what will happen, by starting like this.
What will happen next with the omicron coronavirus variant? It might become the country’s most dominant COVID-19 strain, according to Dr. Anthony Fauci.
For some reason this kind of thing is happening a lot with Fauci in particular, where reporters change his words in ways that importantly distort their meanings. I notice it because he’s a simulacra-level-2 player whose words are intended to convey meaning and whose position makes those meanings important, so I parse them carefully. It’s possible that this position also makes reporters distort Fauci more readily, but I doubt this. It’s much more likely that this is standard procedure and reporters will report you as having said whatever they feel like, even when the direct quote provided says something different. They don’t believe words have meanings.
That’s one reason it’s often better to have transcripts, like this one from an interview Fauci gave on December 8. That’s a little old at this point but there are several telling passages. First, the attitude towards family gatherings, where vaccination makes life ‘possible’ and we are all called upon to police those around us:
Well, yes, that is just the reality of the situation. I mean, one thing vaccinated people can feel comfortable–for example, let’s take the holiday setting. You’re with your family. You have grandparents and parents and children. When you get vaccinated and you have a vaccinated group and you are in an indoor setting, you can enjoy, as we have traditionally over the years, dinners and gatherings within the home with people who are vaccinated.
And that’s the reason why people should, if they invite people over their home, essentially ask and maybe require that people show evidence that they are vaccinated, or give their honest and good faith word that they have been vaccinated.
Then there’s the new information, which is how he’s thinking about Omicron boosters.
You ask about the regulatory requirements. You know, I don’t want to step ahead of the FDA about what they would do, but I think in broad, contextual terms, if the level of protection with the boost against the original ancestral strain goes low enough–and whatever that cutoff point is–that’ll be up to the FDA, whether that’s below 50 percent or what have you. Then, it is likely we would need to at least look seriously at a variant-specific boost. But I hope we don’t need that. I hope we can continue to elevate the response by boosting with the original vaccine.
I’ve been in a few conversations about how to get Omicron boosters working faster, perhaps fast enough to get to the vulnerable before the wave becomes a tsunami, and had debates over whether that was the right focus. Everyone I know who thinks about this considers starting the process as fast as possible both important and a no brainer. Instead, everyone with any power over the situation seems to have suddenly decided that there’s no point, so it isn’t going to happen until far too late, and our entire ability to update the vaccines for a variant was effectively fake. We can’t actually do this until after we know we needed to have already done it. That’s marginally better than nothing, but it’s a lot closer to nothing.
It seems like, when there’s a strain that spreads three times as fast as the original or more, a vaccine that works about half the time is considered good enough, and good enough to force people to take it. This isn’t people modeling and thinking about the physical world and plotting exponential growth curves. This is moralistic thinking, or worse.
Finally, he makes it clear for those who weren’t sure that ‘fully vaccinated’ is a term of art that’s used to motte-and-bailey between ‘as much vaccination as would give you maximum protection’ and ‘what we require people to do or else.’
Well, you know, fully vaccinated is a technical term, Frances. It relates to the requirement of showing that you’re vaccinated to be able to go into a location, be it a college or a university or a workplace, to say I am now officially within this category so I can proceed. I don’t see that changing in the immediate future, but one thing is clear, that, from a personal standpoint, optimal protection is with a booster. When that gets changed to be the official definition of fully vaccinated, I think that certainly is on the table and is going to be seriously considered.
Response
What can we then do?
Here’s a thread about messaging to the people, pointing out that giving people ‘hope’ makes them more likely to support restrictions and adhere to guidelines. So you avoid showing them things like this projection from Denmark that was making the rounds last week.
Instead you show them things like this, from messaging about Alpha.
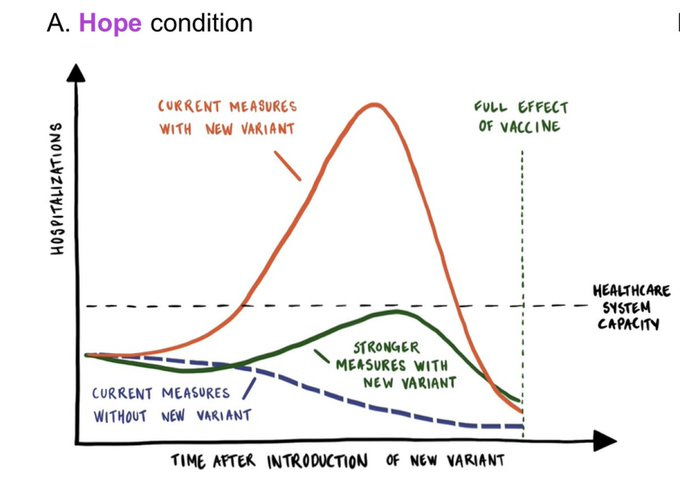
With this result:

It’s good to know what is effective but what if there is no hope, and even with maximum realistic prevention it’s still a disaster? One response is ‘then we don’t want them adhering to the guidelines’ but you still do want people adhering to the right guidelines, whatever those are. Although if you’re standing outside the guideline-choosing process and they choose bad guidelines, as they likely will, then perhaps it would be better to have people ignore guidelines because the many of the guidelines are pointlessly destructive.
Here’s a thread covering the policy statement of the Global Preparedness Monitoring Board.
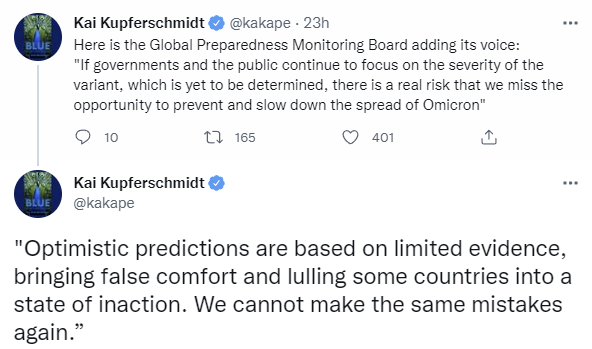

Once again, we have a generic call to, in Dido’s words, do the things we usually do. This is mostly the same measures they would have called for without Omicron. It contains nothing that has any hope of actually stopping Omicron. If you’re not willing to close schools, the game is already super over. Yes, it’s good to prepare the health systems and have good surveillance data available, and absolutely we should work on new vaccines and therapies and distribution of vaccines, that’s all very good, but how does all of that possibly help us in time?
The answer of course (aside from ‘prepare the system’ as best you can so it fails less hard, it’s simply not equipped for the scale of this) is that it doesn’t, but no one has anything else to do and one must Call For Action, so call for action it will be.
Kai notes in this thread that the UK seems to not be taking the WHO’s ‘vaccines and’ message to heart. I still don’t know what would be in the ‘and.’
Science article on what we know, seems reasonable but nothing new, once again downplaying the actually bad scenarios. Even when saying ‘I don’t think we got the message through’ I think ‘true, but I also think you didn’t get the message either.’
The Lab Leak Hypothesis Part 2
So, yeah. This happened.
This just dropped and I’m out of the time necessary to look into this for today. Maybe it’s all wrong, so don’t read too much into it until it’s been examined carefully.
But if this comes from a mouse I do not believe in that level of coincidence. There may not be a fire alarm for artificial general intelligence, but other things have constantly ringing really loud alarm bells and maybe we should stop doing the sort of thing that can lead to this outcome. The next time this happens we might not be so lucky. It has to stop.
It’s a developing story, so more on this later. For now, let’s wrap with the probability changes.
Probability Updates
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 85% → 90%.
It’s pretty hard to look at the UK data and draw any other conclusion. I hold out the possibility that this is an early-stage thing enough that it might not break 100% exactly, but this doesn’t seem like an interesting question anymore, since at most we are ‘talking price’ and the better question is our best guess as to exactly how big an advantage. I’ll think about what the best replacement is.
Chance that Omicron is importantly more virulent than Delta: 3% → 3%.
Chance that Omicron is importantly less virulent than Delta: 60% → 60%.
The data from Denmark and South Africa point in opposite directions here. Saying ‘oh well they cancel out’ is the coward’s way out for sure, but until I have more time to process that’s where I am at. I’ll probably update at some point soon off no new information when I decide what it all means.
Will the CDC label Omicron a variant of high consequence before 2022? 11% → 11%.
I mean they should based on what I think it means, but whether or not they will doesn’t have much to do with that. Still waiting.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 50% → 30%.
Fauci is outright saying we don’t need an updated booster ‘at this time.’ That definitely kills any super rapid response but in the later part of the window it still seems plausible.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 25% → 35%.
The data in the UK and Ontario, and the data now coming in from various American cities, and the CDC nowcast, all point in the direction that this is happening fast. There’s no sign of a robust policy response anywhere, so maybe we really will let it burn, but I have no idea how we actually do it. Then again, I have no idea how we do another set of lockdowns. Something has to give. I notice that I don’t expect to do indoor dining (or, given the winter, much dining out at all) for much longer, but will it go further than that? I notice increasingly that I don’t have a good handle on how to think about the policy response that we’ll actually get because neither do any of the policymakers. I don’t think they’re thinking about it much at all.
Will Omicron be >1% of all cases by the end of the year? 97%+ → 99.9%+
This already happened. It’s done.
41 comments
Comments sorted by top scores.
comment by Randomized, Controlled (BossSleepy) · 2021-12-17T19:24:22.222Z · LW(p) · GW(p)
The Lab Leak Hypothesis Part 2
Feel like you buried the lede here, Zvi. If this is a lab leak (potentially a second one for covid) seems like it has huge+urgent implications for biosecurity policy and us-all-not-dying etc.
Even if covid itself turns out to be a nothingburger on the larger scale of things, if we're this eagerly stepping on rakes, maybe we should think harder about picking up all the rakes rather than deciding to start jumping around.
Replies from: Zvi↑ comment by Zvi · 2021-12-18T17:11:16.878Z · LW(p) · GW(p)
I haven't had time to examine the study nor have I seen confirmation from a source I would trust to do it for me, so I don't want to jump to conclusions too fast. Also, Omicron is about to hit us hard within weeks, and addressing this problem is a longer term problem.
I agree that there's a good chance I have very much buried the lead here, but I want to be sure. I did try to start this ball rolling in at least one other way.
comment by Chris_Leong · 2021-12-16T22:24:51.346Z · LW(p) · GW(p)
"In a better world, I could focus on this full time and also maybe even hire a research assistant, and be better able to scour for information."
Have you tried applying for funding from anywhere?
↑ comment by Zvi · 2021-12-17T00:23:42.198Z · LW(p) · GW(p)
I have a job that I'm passionate about, with a lot of upside, with people who I care about who rely on me, making the Emergents TCG (https://emergentstcg.com/) and associated things. I'm not about to give that up lightly, although there is always a price.
I have not applied for funding, beyond setting up ways to accept gifts (e.g. Twitter tips, Patreon, Substack), which is mainly because people actively wanted to give me small amounts. It doesn't provide serious funding, or at least it hasn't yet. Money here does make a motivational difference, but please no one should feel obligated in any way at all (and if it's a large amount, let's make sure we use a no-fee method, if necessary PM me).
Part of the problem is that my opportunity costs are very high, and also that I don't know how to hire assistance well (as I noted in the SFF post [LW · GW]). And applying for large amounts of funding when you're already well off doesn't feel great. And I worry about the social dynamics and incentives, and worry that the thing where we go around asking each other for grant money isn't great (again, see SFF post).
Replies from: Chris_Leong, Chris_Leong, Ericf↑ comment by Chris_Leong · 2021-12-17T04:44:06.332Z · LW(p) · GW(p)
Oh, and maybe you could clarify? Is it that you don't want to accept funding from institutions? Or is it that you don't want to go actively looking for funding? How would things work in the world in the world where you were funded and felt good about it?
How would you feel about a model where a foundation offered matching funds instead of a direct grant? Or what if another org hired the research assistant and loaned them out to you for the period so that the money never touched your hands?
↑ comment by Zvi · 2021-12-17T15:08:30.382Z · LW(p) · GW(p)
I very much don't want to go actively looking, for reasons that I've gestured at a lot in various places, but gifts are always helpful. If institutions (or individuals) want to offer me of their own accord a retrospective grant/gift, or a prospective grant/gift with no strings attached at all (e.g. MacArthur grant style), and do so of their own accord, I'd be happy to accept. If strings were attached I might consider it, but it would have to be very large.
Different orders of magnitude of funds impact me in different ways.
If people want to loan me a research assistant and/or personal assistant and/or an expense account to make things easier, with or without direct funding, I'd welcome that too and would try it out, while noting that it's hard to find good help that actually pays dividends.
Another thing that worries me is that the whole Covid thing could be over within a few months. I do want to write other stuff anyway, but it'll be a very different product that might not still be something the person would want to be paying for (or it might be something they want even more, who knows).
Replies from: Chris_Leong↑ comment by Chris_Leong · 2021-12-17T17:15:56.586Z · LW(p) · GW(p)
How would you feel about someone else putting in an application on your behalf supposing that you wouldn't have any involvement with writing it, apart from giving permission?
Replies from: Zvi↑ comment by Zvi · 2021-12-17T18:26:06.277Z · LW(p) · GW(p)
I don't want any sort of 'hard sell' and who knows what I'll be doing by the time such a process finishes, but if you want to tell someone else 'hey have you considered giving Zvi a check?' I'm not exactly going to say no.
Replies from: Chris_Leong↑ comment by Chris_Leong · 2021-12-18T05:29:23.192Z · LW(p) · GW(p)
What if I submitted an intentionally 'soft sell' grant application? Think along the lines of what Scott Alexander used to have on his Patreon?
Replies from: Zvi↑ comment by Chris_Leong · 2021-12-17T04:27:56.444Z · LW(p) · GW(p)
"I'm not about to give that up lightly, although there is always a price"
Even if your price would be too high, I would be surprised if you couldn't obtain funding for a research assistant. That might solve: "And applying for large amounts of funding when you're already well off doesn't feel great".
↑ comment by Ericf · 2021-12-17T04:01:16.517Z · LW(p) · GW(p)
It sounds like if there is an unemployed reader out there with some experience in doing research, there is an opportunity here to make a Patreon account and explicitly solicit donations in a "If I can make $X,000 per month I will spend 40 hours a week doing research on important topical issues and provide the raw data for analysis" kind of way.
Most of us have jobs already, but it only takes one...
↑ comment by Nicolas Lacombe (nicolas-lacombe) · 2021-12-17T00:01:42.727Z · LW(p) · GW(p)
also: how much funding do you think it would take? i'd be interested in sending more money if i knew it would have a marginal impact
Replies from: CraigMichael↑ comment by CraigMichael · 2021-12-17T19:40:25.056Z · LW(p) · GW(p)
Subscribed to his substack today. Would do more than that even if it would help.
comment by bfinn · 2021-12-16T20:32:02.980Z · LW(p) · GW(p)
One possibly relevant difference between London and Denmark is that fully one-third of Londoners are completely unvaccinated. No jabs at all.
(Something that most of the media here didn't seem to notice until yesterday.)
Replies from: bfinn, Pattern↑ comment by bfinn · 2021-12-19T13:12:27.194Z · LW(p) · GW(p)
BTW the reason the media hasn't highlighted this before seems to be because the UK and London government haven't done so either, and that's because the unvaccinated are mainly first- or second-generation immigrants who they don't want to be seen as criticizing.
Hence also for the last year the unvaccinated have been characterized (on the UK media I follow) as 'vaccine hesitant' rather than 'anti-vaxxers', with detailed explanations for why they might not want to be vaccinated. Which is reasonable, and actually a rare example of (in effect) steelmanning in the media.
↑ comment by Pattern · 2021-12-19T06:18:52.213Z · LW(p) · GW(p)
Where's Denmark at with vaccination?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-12-19T09:49:16.848Z · LW(p) · GW(p)
https://lmgtfy.app/?q=vaccination+rate+denmark
80% at least one dose, 77% two doses, and 27% three doses.
comment by tkpwaeub (gabriel-holmes) · 2021-12-19T18:20:07.998Z · LW(p) · GW(p)
This New York Times article seems to have an important clue about the increased transmissibility of Omicron (I boldfaced the key points):
The buzzing activity Dr. Amaro and her colleagues witnessed offered clues about how viruses survive inside aerosols. The mucins, for example, did not just wander idly around the aerosol. The negatively charged mucins were attracted to the positively charged spike proteins. Charged atoms such as calcium fly around the droplet, exerting powerful forces on molecules they encounter.Dr. Amaro speculated that the mucins act as a shield. If the virus moves too close to the surface of the aerosol, the mucins push them back in, so that they aren’t exposed to the deadly air.
“What we think is that it’s actually covering itself in these mucins, and that’s acting like a protective coating for it during flight,” Dr. Amaro said.
This discovery may help explain how the Delta variant became so widespread. Delta’s spike proteins have a more positive charge than those on earlier forms of the coronavirus. As a result, mucins huddle more closely around them. That attraction could potentially make the mucins a better shield.
Every now and then, one of the simulated coronaviruses flipped open a spike protein, surprising the scientists. “The Delta variant opens much more easily than the original strain that we had simulated,” Dr. Amaro said.
A simulation of the Delta variant’s spike protein suggests that it opens wider than the original coronavirus strain, which may help explain why Delta spreads more successfully.
Once a coronavirus enters someone’s nose or lungs, the Delta spike’s wide opening may make it better at infecting a cell. But Dr. Amaro suspects that it’s bad for a coronavirus to open a spike protein when it’s still inside an aerosol, perhaps hours away from infecting a new host. “If it opens too soon, it could just fall apart,” Dr. Amaro said.
Some of the molecules that are abundant inside aerosols may be able to lock the spike shut for the journey, she said. Certain lung surfactants can fit into a pocket on the surface of the spike protein, preventing it from swinging open.
To test that idea and explore others, Dr. Amaro and her colleagues are stretching out the time frame of their simulation a hundred times, from ten billionths of a second to a millionth of a second. They’ll also investigate how the acidity inside an aerosol and the humidity of the air around it may change the virus.
Dr. Amaro and her colleagues are making plans to build an Omicron variant next and observe how it behaves in an aerosol. They want to wait for structural biologists to work out the three-dimensional shape of its spike proteins before getting started. But just looking at the early findings about Omicron, Dr. Amaro already sees one important feature: “It is even more positively charged,” she said.
Because Omicron’s spike proteins are even more positively charged than Delta’s, it may build a better mucin shield in aerosols. And that may help make it even more transmissible.
In other words, Delta lasts longer in the air than the original strain (which itself could last in the air for as long as three hours) and Omicron is even hardier. This seems to track pretty well with increased spread in households and across hotel corridors. In the latter example, the prevailing theory seems to be that it passed from one occupant to the other when they were getting their meals. I find it much easier to imagine the increased transmission resulting from a build-up of Omicron in the air, which then seeped through a gap in the door, rather than Omicron having developed sentience and seeking out new hosts during fleeting encounters. Doors to hotel rooms aren't exactly airtight. Together with the aforementioned 70-fold replication speed in the bronchus, that would tie up the transmissibility question quite nicely - infected people are spewing a lot more virus, which lasts longer in the air. We are all super-spreaders now.
The "air hardiness" also makes the jump from wild mice that much more plausible. With a virus that survives such a long time in the air, it's a lot easier to imagine zoonosis and reverse zoonosis occurring, without having to get terribly close to an infected animal.
Another corollary of all this would be that you should assume that you're going to get infected if you live in a multi-family residence with any shared indoor spaces whatsoever. Or consider getting an indoor air purifier, even if you live alone. Scratch that; if you haven't already gotten an air purifier it's probably too late.
God help us.
Replies from: gwillen, Kenny↑ comment by gwillen · 2021-12-20T22:58:04.303Z · LW(p) · GW(p)
In other words, Delta lasts longer in the air than the original strain (which itself could last in the air for as long as three hours)
This is tangential, but it's been fascinating to me to watch the spread of that "three hours" factoid. I believe it originally comes from this paper: https://www.medrxiv.org/content/10.1101/2020.03.09.20033217v1.full.pdf (Note that "HCoV-19" was referring to what is now designated "SARS-CoV-2", i.e. COVID-19.)
I very gently criticized it at the time for having a quite misleading abstract, regarding the "three hours" figure:
https://twitter.com/gwillen/status/1237854407007457280 https://twitter.com/DrNeeltje/status/1237895661967642626 https://twitter.com/gwillen/status/1237896626355593221
This abstract, as far as I can tell, is where the "three hours" factoid originated, which has now become gospel that appears on public health pages like your link above. In reality, the abstract said they detected the virus in aerosols for "up to three hours" because that was the duration of the experiment. It's obvious from graphs, as well as their computed half-life figure -- which is coincidentally pretty close to three hours -- that if they had continued the experiment, they would have kept detecting viable virus for a multiple of that time. (Of course, this figure is also kind of meaningless anyway, since the initial quantity of virus they're experimenting on was arbitrary! Only the half-life is really meaningful, but that doesn't make good headlines.)
It feels very weird to me to have "been there at the beginning" for this. I have no specific qualifications for interpreting this paper, beyond being smart and careful. It's a little depressing (but that's the COVID story.)
(I would love for someone to correct my story here, and find some other explanation for where this factoid came from, or argue that I'm wrong about it being misleading to the point of error. I really don't like this story or what it implies.)
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-21T06:48:42.976Z · LW(p) · GW(p)
So 3 hours was too low even for the original strain??? Jesus, no wonder so many cases are untraceable.
↑ comment by Kenny · 2021-12-20T16:56:54.072Z · LW(p) · GW(p)
Thanks for some possible details about the relevant 'gears'!
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-20T22:03:06.935Z · LW(p) · GW(p)
Gears! I love it!
Replies from: Kennycomment by Connor_Flexman · 2021-12-20T04:42:45.967Z · LW(p) · GW(p)
I can't confirm you didn't talk about this, but the only thing of importance I haven't seen you mention in these is that the serial interval might be much smaller (eg as mentioned here), so that R0 and number of secondary infections is not so vastly higher even as we see incredibly fast doubling times. I think people don't realize how much this effect played a part in Delta's containability, even while Delta overtook other variants very quickly and it seemed pretty concerning at the beginning.
Specifically, if Omicron is tearing through vaccinated populations because it has 5x higher immune escape than Delta, 2/3 the serial interval, and 1.5x the transmission (which I think roughly fits the SA data), then we might see the Omicron wave ending up surprisingly containable—only needing behavior to curb the 1.5x transmission and to go back to pre-vaccine (Jan 2021) measures to fix the immune escape.
I don't put much probability on this since I don't know a ton about omicron and I haven't heard people talking about it much, but it seems like it's still an overlooked phenomenon re Delta and so I wouldn't be surprised if it made omicron a lot more containable than I've seen implied. Admittedly people seem very done with countermeasures at this point, so we still might be screwed (and screwed quickly if serial interval is in fact a big driver), but I wouldn't actually be all that surprised if the control system kicked in in a few weeks and the wave peaked fairly quickly.
Replies from: Zvi↑ comment by Zvi · 2021-12-20T14:44:25.622Z · LW(p) · GW(p)
I haven't talked about it recently, I did discuss it with regard to Delta, whose interval was shorter than the original strain. It would be surprising for Omicron, which didn't come from Delta, to be faster even than Delta, but perhaps it is possible. It would take a lot of this to be enough, but it would certainly help.
Replies from: Connor_Flexman↑ comment by Connor_Flexman · 2021-12-27T05:50:34.340Z · LW(p) · GW(p)
Given that serial interval is a very effective way to amplify an already-high R0 to great evolutionary advantage, and common colds/flu etc all have developed serial interval of more like 1-2 days showing there's plenty of room for COVID to climb in this regard, I would expect lots of new dominant strains to show shortened serial interval regardless of heritage.
Not sure if there's publication bias or measurement bias here but the first link on google shows a study estimating Omicron serial interval at 2.2 days in South Korea.
comment by aaqofib · 2021-12-17T09:44:23.761Z · LW(p) · GW(p)
Regarding the Danish hospitalization numbers:
The non-omicron variants column in the hospitalization table of the daily Danish omicron reports (which one can found on here, with the most recent one via the big "Download her" button and the older ones under "Arkiv") was changed from the previous one to the last report. Until the report from the December 15, they only reported cases for which a variant PCR test was carried out, i.e. hospitalizations of people who tested positive for coronavirus, but where no variant PCR test result is available was not counted (which makes sense, as it is then not known whether the case is omicron or not!). Starting with the current report from December 16 they are counting positive tests without a variant PCR result as "other variants". At least that is how I understand the explanation on page 1. So here is how I read the two tables:
| Report | Column | Which cases are counted |
|---|---|---|
| Dec 15 | Other variants | PCR test positive, variant PCR result negative for Omicron |
| Dec 15 | Omicron | PCR test positive, variant PCR result positive for Omicron |
| Dec 16 | Other variants | PCR test positive, variant PCR result negative for Omicron OR no variant PCR result available |
| Dec 16 | Omicron | PCR test positive, variant PCR result positive for Omicron |
The previous report had 95,245 other variant cases of which 715 were hospitalized with positive tested earlier than 48 hours after (abbreviated <48h from now on), and 4 with test after (48+h). Now, with one extra day of data plus the added cases that did not have a variant PCR done (or no result available yet), they report 115,017 other variant cases with 1,560 (<48h) and 222 (48+h) of those hospitalized cases. This doesn't make sense unless a large number of hospitalized cases did not have a variant-PCR test done? In particular, those could still turn out to be omicron, so this makes concluding things about virulence from the new table more difficult. It confuses me why (even though the total number of other variant cases went up only moderately by the change in definition for that column, corresponding to the fact that variant PCR test coverage in general is very high) so many hospitalized cases seem not to have a variant PCR result, with the difference particularly drastic in the 48+h category. The only explanation I can come up with that fits this is the following: Hospitals have their own labs to analyze covid tests they carry out. Originally, in February / early March 2020, I think tests were essentially done in those labs, now the mass testing program has two big central labs in which the PCR tests for the whole country is analyzed. But presumably hospitals still analyze their own PCR tests in their own labs. Perhaps hospitals tend to not be equipped with the variant PCR test? I think this would explain the data. Up to the report before the current one, the numbers in the 48+h category were not changing much for other variants and omicron, (eg. staying at 8-9 cases for omicron). I dimly remember in the early days of omicron (1-2 weeks ago) that it was said (in a press conference or interview for the news) by someone responsible for contact tracing that there had been an omicron outbreak at a hospital, so that is probably why there originally were a couple of omicron cases identified in the 48+h category. My conclusion is that the 48+h row in that table is essentially useless to compare variants, as there seems to be very little variant testing to be done for those cases so far, or with a big delay (I would assume that the hospital labs are either going to set up variant tests or forward positive tests to the central labs for variant testing, but this might introduce extra delays, so this is not really reflected in the data yet?). In the <48h row there also must be quite a few cases that don't have a variant result, though the difference is less drastic than for the 48+h row. Which makes sense because <48 hours includes tests done at the hospital (which I suspect correlates strongly with no variant PCR test result available) as well as tests done before admission (for which there seems to be good coverage of variant PCR tests, though with a little extra delay until results are ready).
The previous table from the December 15 report shows 0.6% of omicron cases being hospitalized in the <48h category and 0.8% of non-omicron cases being hospitalized in the <48h category, which is quite disappointing regarding virulence; as omicron is still rapidly rising and hospitalizations are delayed we would expect a lower rate currently even if virulence is the same, so this little difference in hospitalization is not good news.
The table from December 16 report still shows 0.6% of the omicron cases hospitalized (<48h) and 1.4% of the other variant cases (<48h). But by my discussion above I think the additional difference likely can be explained by people who were tested positive at the hospital and for which we don't (yet) have a variant PCR test result.
Thanks for writing these posts on corona Zvi, I really appreciate them!
comment by toner · 2021-12-17T03:49:24.050Z · LW(p) · GW(p)
Data from NSW, Australia. Delta was stable at 150-300 cases/day, so recent spike is likely omicron. 93% of people aged 16 or over are double-vaccinated. https://covidlive.com.au/report/daily-cases/nsw
comment by TheMajor · 2021-12-17T09:36:07.091Z · LW(p) · GW(p)
The link on severity of Omicron infections (https://www.nrk.no/urix/tall-fra-danmark_-omikron-forer-til-like-mange-innleggelser-som-delta-1.15769977) raises an interesting question. They deduce the severity by comparing the number of hospitalisations from Omicron with the spread of the variant 5 to 6 days prior to hospitalisation, which is the correct thing to do if we assume it takes 5 days from infection to developing symptoms severe enough to be admitted to the hospital. My two questions:
- Are other news sources doing this consistently as well? If they are comparing hospitalisations today with case numbers today that gives the wrong answer by approximately two doubling times, underestimating severity.
- Is there a reason to believe Omicron may develop symptoms slower/faster than older variants, so that we need to correct these figures?
Since the doubling time of Omicron is so short this has serious knock-on effects.
As an aside, the link does not claim anywhere the patients were admitted for Omicron, just that they were admitted, and diagnosed with Omicron. So for now I'm withholding updating on this.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-20T17:40:36.039Z · LW(p) · GW(p)
On the other hand, everyone seems to have given up on tracking full recoveries, so maybe the two things cancel one another out, so we end up just using the most naive approach possible?
comment by ardavei · 2021-12-17T19:56:35.941Z · LW(p) · GW(p)
In addition to the data from Denmark, an analysis of the data from England found no significant association between Omikron and hospitalization: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-49-Omicron/
Note that this doesn't say anything about need for intensive care or ventilation, which seemed to be lower among hospitalized patients in the South African data.
Still, given this data, and the caveats of the South African data (younger patients, very high levels of natural immunity), I would set the chance that Omikron is significantly less virulent than Delta at more like 20-30% at this point.
comment by Oskar Press Mathiasen (oskar-press-mathiasen) · 2021-12-17T00:45:51.783Z · LW(p) · GW(p)
this link is in Norwegian, not danish
comment by teageegeepea · 2021-12-20T03:01:28.364Z · LW(p) · GW(p)
I couldn't see which tweet Robert Walker was linking to, and the images here as just images rather than links to tweets, so I tried to link them here, but it's not letting me submit a comment.
Replies from: teageegeepea↑ comment by teageegeepea · 2021-12-20T03:01:58.357Z · LW(p) · GW(p)
I went to his account via a different link here and found this:
https://twitter.com/DoomsdayDebunks/status/1471204307609477123
which links to this:
https://twitter.com/SetteLab/status/1469007626306392064
comment by Riffer · 2021-12-17T19:17:58.937Z · LW(p) · GW(p)
"In an even better world than that, we’d have run challenge trials the moment Omicron was detected"
I personally would have spent the first week of December figuring out how to home-brew an Omicron-tailored booster if I were at-risk.
Replies from: kamil-pabis↑ comment by Kamil Pabis (kamil-pabis) · 2021-12-19T11:14:43.040Z · LW(p) · GW(p)
Given the data we have getting an "illicit" fourth booster shot might be the safer play. The mRNA vaccines continue to work, especially against severe disease, the effect is just much diminished.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-19T14:54:48.536Z · LW(p) · GW(p)
That's what I did. I'll let you know how it works out. See you on the other side.
comment by CScrewtape · 2021-12-17T12:10:36.342Z · LW(p) · GW(p)
What is the Taiwan link saying? It is blocked for me. Officially their are only two cases on the mainland, split between Tianjin Guangzhou. How the Tianjin cluster develops will probably be the earliest read we can get on how quarantine procedures hold up. Those sort of workers get daily tests. Workers on average hospitals seem to be on a three day testing schedule. So I’m pessimistic, but they have held out longer than I expected and used the time wisely.
comment by Yandong Zhang (yandong-zhang) · 2021-12-19T07:57:35.381Z · LW(p) · GW(p)
It is easy to make simple things complicate. It is extremely difficult to simplify the complicate issues. It is ever more difficult to understand the conclusion that looks simple.
Two years ago, I CONCLUED that the COVID can only be controlled by N95 or even better physical protection equipment. The posts I provided looks like a joke (someone do said it is a joke).
https://www.lesswrong.com/posts/xGHh4zeWJHp6tMzQ5/a-proof-of-the-existence-of-the-ending-moment-of-the-covid [LW · GW]
https://www.lesswrong.com/posts/QZtt9q6u7vaBjXgu3/equilibrium-point-of-the-social-evolution-under-the [LW · GW]
Today, do those posts look more reasonable? The key point is: the mutation of COVID is very fast and uncontrollable (at this stage). This is an obvious, but not easy to understand fact.
Replies from: yandong-zhang↑ comment by Yandong Zhang (yandong-zhang) · 2021-12-21T15:29:08.942Z · LW(p) · GW(p)
With the speed of double 1-3 days, I did not believe other details/aspects played any significant role. Only the transmission control/observe has relationship with the true reality.