Omicron Post #12
post by Zvi · 2022-01-04T15:50:01.288Z · LW · GW · 21 commentsContents
Vaccine Effectiveness Treatment Quarantine, Isolation and Travel Disruptions other than Hospitals Spread Severity Hospitals Threads Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? %? → 50%. Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 60% → 55%. Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 85% → 90%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% → 20%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 10% → 5%. Generation time (serial interval) of Omicron is 3.5 days or less: 85% → 87%. Daily cases in the the United States have peaked by February 1, 2022: ?% → 85%. None 21 comments
It involved a backlog, but the USA reported over 1 million cases yesterday. That’s a lot of cases, and we’re missing a ton more of them. Schools, hospitals and all businesses face massive disruptions from people unable to work, even with the new CDC isolation guidelines.
So far, we’re holding up well, better than I expected even after previous severity estimates were adjusted. Things are going to be severely disrupted for a while, but not as severely as we might have feared, and even if we get a median outcome that is much better than the mean outcome given the tail risk of true disaster.
Still, brace yourself, and choose how you want to handle the next month or two. If you’re serious about trying to avoid Omicron, now is the time to show it.
Vaccine Effectiveness
A Danish study from earlier found large negative vaccine effectiveness. Large negative effectiveness is not a thing, we would know about it and the world would look very different, but anti-vax people are of course jumping on it and the attempt to explain isn’t going all that well. Which it mostly shouldn’t, in my view, because when you get nonsense results that are clearly nonsense results but you don’t control properly and so you publish anyway, what else do you expect?
I looked at the paper. They control for the basics, including geographical region.
VE was calculated as 1-HR with HR (hazard ratio) estimated in a Cox regression model adjusted for age, sex and geographical region, and using calendar time as the underlying time scale.
I’ve heard reasons that make it possible for vaccine effectiveness to go negative, but those reasons don’t seem compatible with large positive effectiveness shortly after two doses, and large positive effectiveness again after a booster shot.
More than that, check the sections on severity and hospitalization below. They make it very clear that being vaccinated offers a lot of effective protection and is very much a good idea, and getting boosted is an even better idea.
Treatment
CDC lifts the pause on anti-Delta monoclonal antibodies, says they can be used if Delta is still in your region and there aren’t other options available. My guess is there are still some places in America where this makes sense, since even a small chance of getting the old effectiveness is better than doing nothing, but this window is ending rapidly.
Quarantine, Isolation and Travel
Instead of ending all travel-based quarantines because they no longer make any sense, many new travel restrictions are being imposed.
This is deeply stupid. It makes sense to make someone quarantine if they are at much higher risk than the surrounding population, and there’s some hope of stopping the spread. Two places having mutual travel restrictions usually means both are making a mistake. These quarantines are quite expensive (as are the required PCR tests, which given the need for reliable results often cost hundreds).
What prompted this was that I noticed that France added the United States to their ‘red list’, including the first comment as a ‘same energy’ to indicate the mindset.

France has twice as many cases per capita as the United States right now, and about two thirds of the death rate.
At this point, quarantines even for people with large known exposures seem questionable. If you learn you’ve been exposed to Covid-19, you have not received that many bits of information, and it’s not clear how much behavior change is justified. Not zero, especially if you’re going to potentially see vulnerable people, but if you used the old thresholds for quarantine you would (quite literally) never leave the house.
At least it’s better than universal isolation, such as the curfews in Quebec:

Whereas Princeton is telling its students they can’t leave the county after they arrive on campus. Not the country, the county. I am confused how they think this will help.
Delhi is locking down for the weekend. I have no idea what this hopes to accomplish. Reported cases in India are up 488% in a week (presumably they’re missing most of them), but what good will three days do? Allow the countryside to catch up a bit?
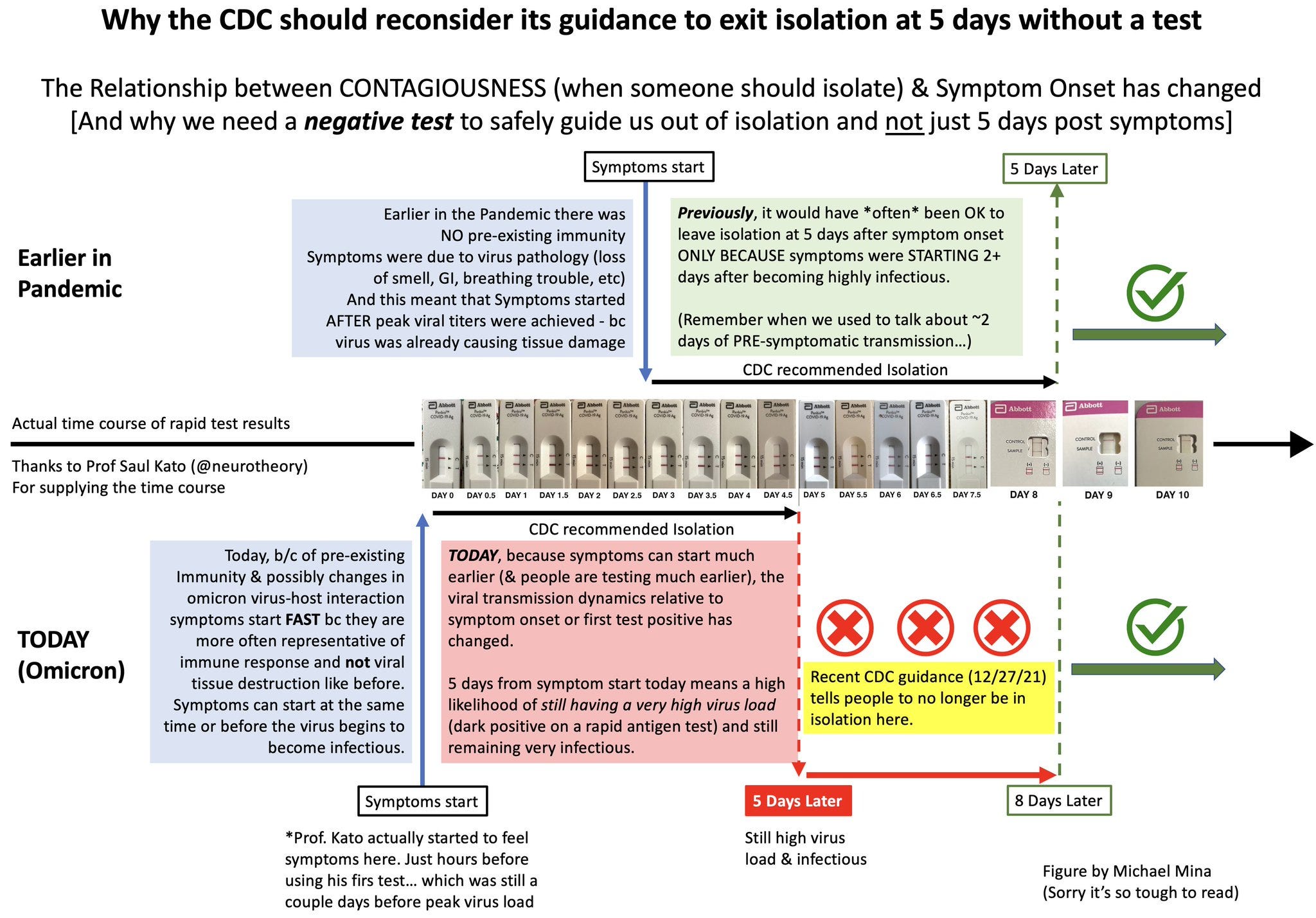
Here’s a graphical argument liked by Mina from Saul Kato for why you need a negative test before you end isolation (the thread contains more details, but we’ve seen those before).
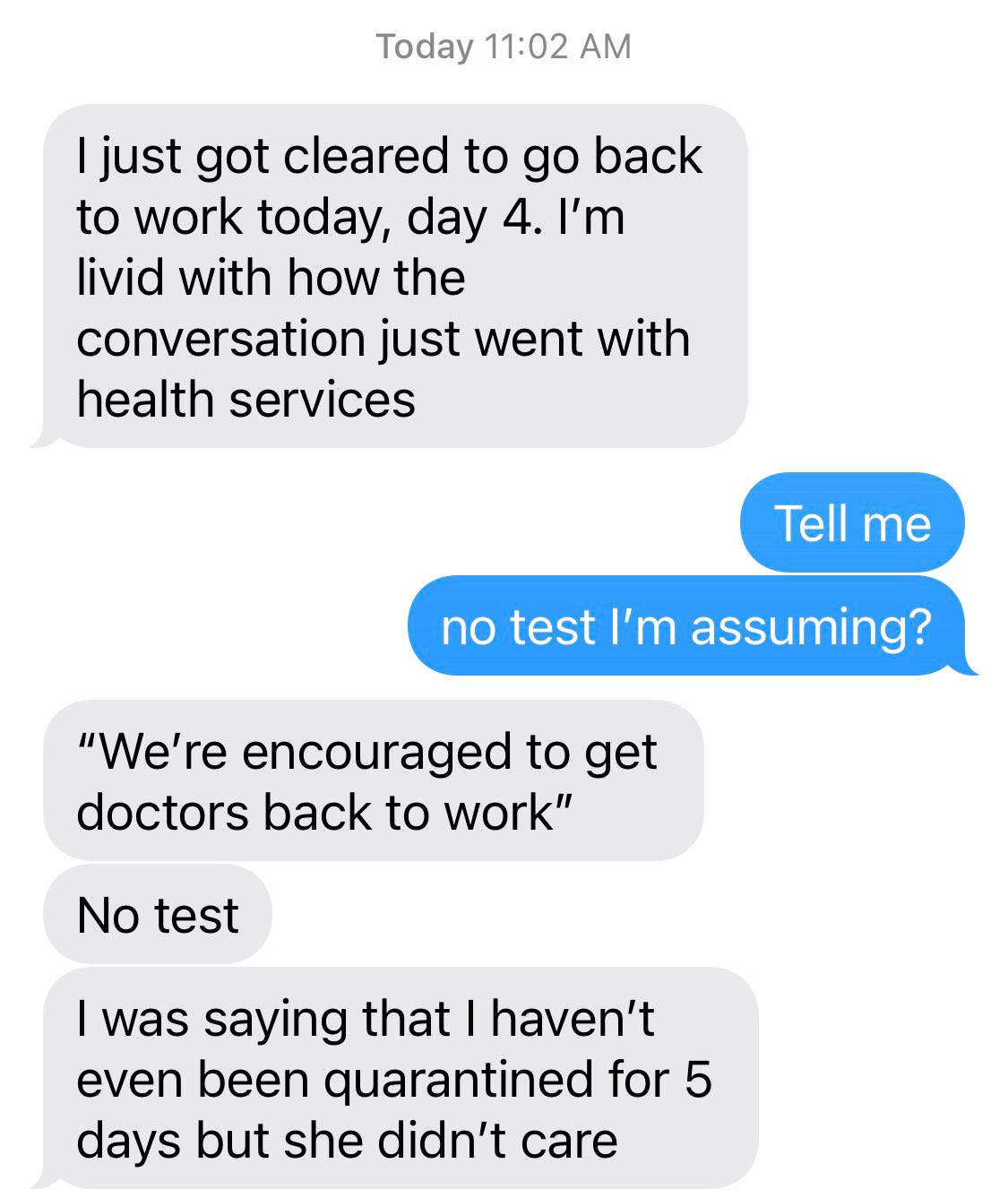
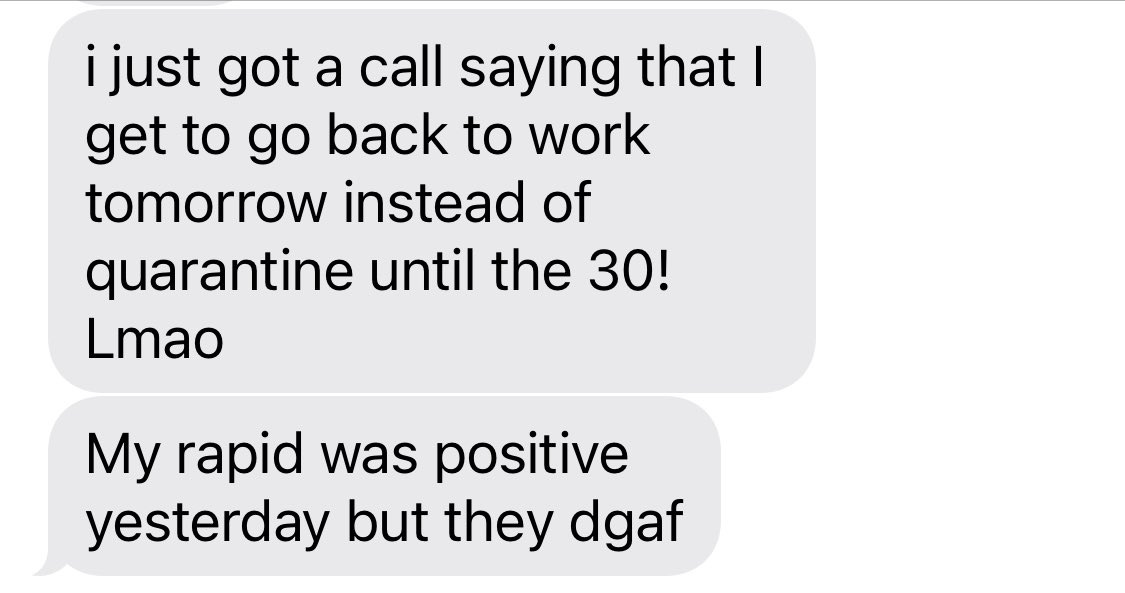
The CDC’s guidance is definitely having an impact, for better and for worse.

If you tell someone who is symptomatic to come back to work, the results to your business are not, in expectation, going to be what you are hoping for.
Yes, some amount of this was inevitable from the new guidelines, especially given the lack of a testing requirement, but restaurants have been making sick people come in when they very much should not come in (even if it means closing the place down for a bit) for a long time and they are not about to stop now.
There are some who are going to treat the CDC requirements as a minimum, without which doing anything is crazy. Others are going to treat it as a maximum, and then make compromises. You do have to set the requirements knowing both of these things will happen. It’s a hard problem.
Doctors being told to come back in four days with no test means they’re going back while still infectious. Is that better or worse than having patients go without care due to lack of staffing? I don’t know.
I do know that this Colbert clip shows how symbolic the whole thing is. Colbert can come back in five days if he wears a mask at all times including during the monologue when he’s dozens of feet away from the nearest person (or if not, he certainly could be) but otherwise he needs to wait ten and she doesn’t tell him to test. The need to pretend that the guidelines make sense forces director Walensky into Obvious Nonsense territory. She did have the decency to nervously force herself to laugh.
Disruptions other than Hospitals
Staffing shortages shut things down. A substantial portion of local restaurants have been shut down at some point by now, for example, along with several subway lines.
When we check in on our ‘not an alarmist’ account, we see these: A county in Maryland cancels school bus routes. Multiple school districts close entirely. Milwaukee going to virtual schooling due to staffing shortages. So is Newark. A prediction that almost all schools will close during January. All NYC Apple stores are closed. A third of Philadelphia classrooms forced to go remote on Tuesday.
I updated a small amount in favor of things being somewhat less disrupted than I expected, because given the information networks available, I would have expected the account to find more and bigger examples of school disruptions. Still, Milwaukee is big, and Philadelphia is big.
So far, both my children’s schools remain open, albeit with large drops in attendance and a bunch of michegas regarding testing.
There’s a reasonable argument that I buy, which says that if you believe school is what its advocates say it is, schools should be kept open as long as possible. NYC Mayor Eric Adams (man saying that is such a relief) definitely buys that, saying that ‘the safest place for our children is in a school building. We are going to keep our schools open.’
The claim that a school is ‘the safest place for our kids’ in a pandemic is grade-A Obvious Nonsense, and presumably comes from this logic:
- We must always do The Safest Thing for our kids.
- We need to open the schools.
- Therefore, the schools are The Safest Thing.
The problem is that people mostly aren’t willing to let such things ‘muddle through’ in any sense, so this kind of will often won’t generate a way.
Schools aren’t going to be allowed to say ‘yes, the school is going to involve a lot of Covid-19’ and instead imposes lots of tests, which finds cases, which forces isolations and shuts down classrooms. Even without that, staffing shortages would still make it impossible to keep many schools and classrooms open, because the system does not have enough slack for such an event.
Businesses and other activities that can survive with limited on-site staff by muddling through, or that are important enough that people should come in anyway if it comes to that, should mostly be able to stay open.
Those that cannot take that approach are going to face a lot of disruption over the next few weeks. Be ready.
Ideally we can find the right balance of shutting versus muddling. It’s difficult.
Spread
One million cases reported in one day. Wow. Backlogs from New Year’s and the weekend were involved, to be sure, but still, wow.
Georgia didn’t update because too much data overwhelmed the system, so you can guess how well things are going there.
Seattle offers some strange graphs, where if we use SGTF deletion as our guide, we see Omicron fading away and Delta increasing. I was told this was from Trevor Bedford, who has otherwise been an excellent data source, but there’s simply no way the graphs are indicating what they say they are. One possibility is that the other version of Omicron, that doesn’t have SGTF deletion, is rising in relative terms.
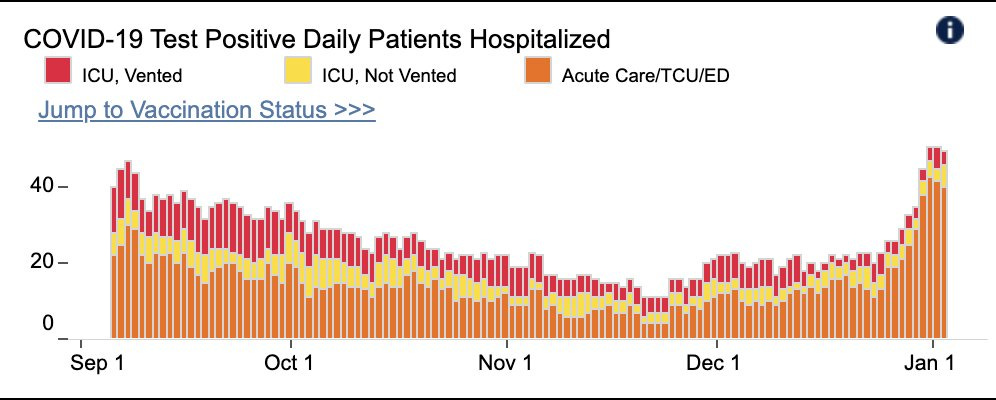
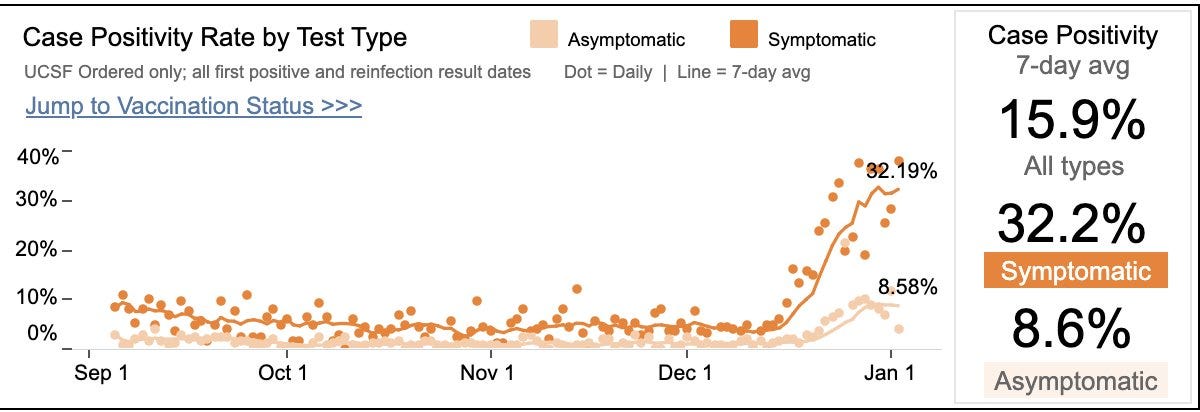
San Francisco infections may already be peaking. My guess is this is premature, but we are seeing data points in this direction. Could be the same holiday-related fluctuations, as well.
New York is going to start having hospitals report how many people are hospitalized ‘with Covid’ versus ‘for Covid’ starting in five days. This will be a great source of data, hopefully exactly in time to not much matter.
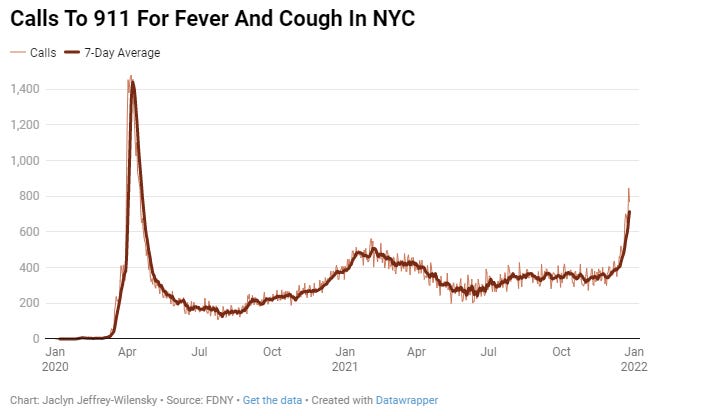
This article highlights that 30% of EMS workers in NYC are currently out sick. The thing is, they’re not all out sick, they’re all sick or isolating.
Amid the spike in calls, 30% of the city’s 4,400 emergency medical services (EMS) staff were out sick as of Wednesday, according to Frank Dwyer, an FDNY spokesperson. He added that the surge in people out sick was a combination of COVID-positive workers, those who’d been exposed and staff awaiting test results.
That means we can’t use the 30% to estimate prevalence, and it also means that we’re holding too many people back. If you’re an EMS worker, yes, you’ve been exposed. That’s the job when 10%+ of the city has Covid-19 at once, how could you not be exposed?
Having such people isolate after an exposure or while waiting for test results is going to do far more harm than good at this point. It’s also fully incompatible with ending isolation after a positive test after only five days without a negative test, although I assume the EMS is ignoring that suggestion and requiring the negative tests anyway.
Nate Silver notes a decline in Google searches for Covid symptoms in NYC.

My guess is that at this point everyone’s already Googled a lot, and a lot of this is pseudo-random, but it is an interesting data point. Nate also notes that the positive test rate has stabilized at 23%, which seems like stronger evidence that we may be at or near the peak.
Severity
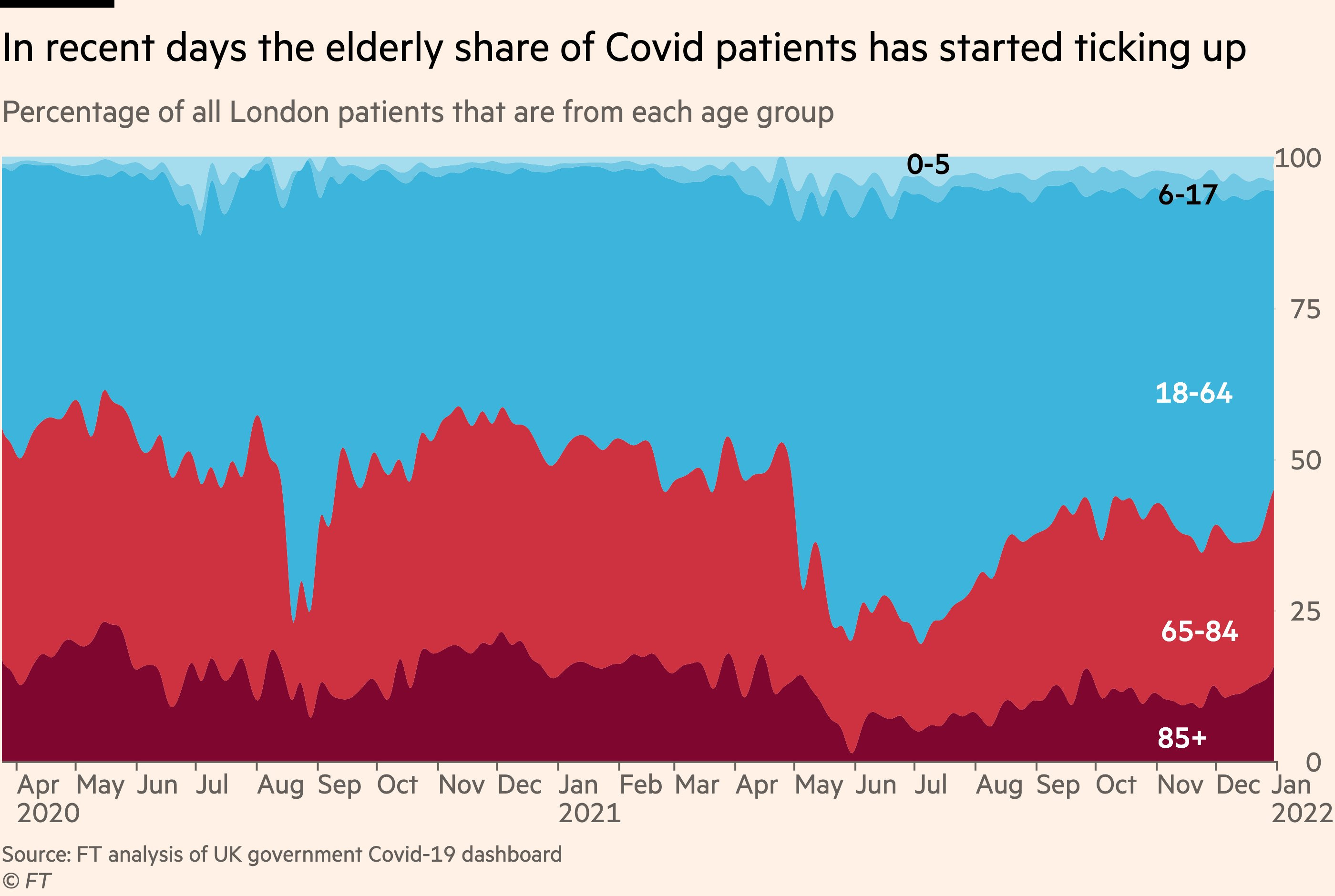
There’s been enough time that if John’s adjustment is remotely reasonable, the cohort that got sick earlier was at little risk. The question now is what will happen with the elderly, for whom not as much time has passed.
This is the data from Gauteng:
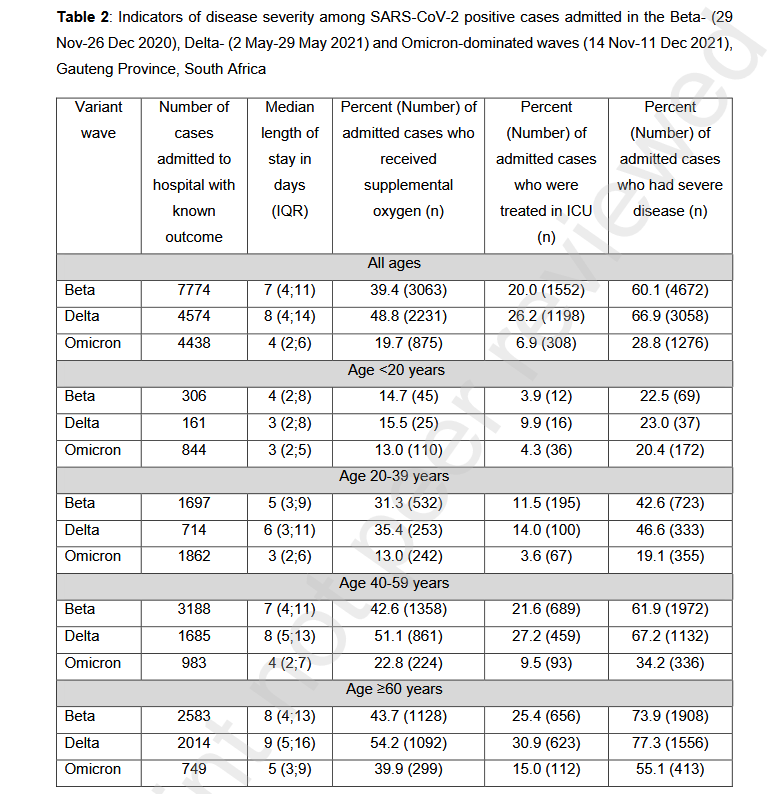
The >60 year old category there definitely shows a much lower drop-off.
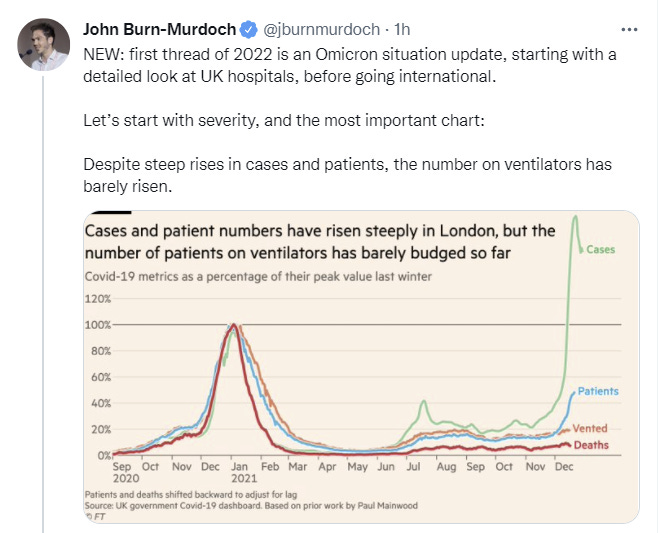
From there the thread pivots into what’s happening to hospitals, including reference to this additional thread on that. I’ll cover that in the next section. That other thread does refer to severity in elderly patients, and finds it substantially improved:
It then pivots back.
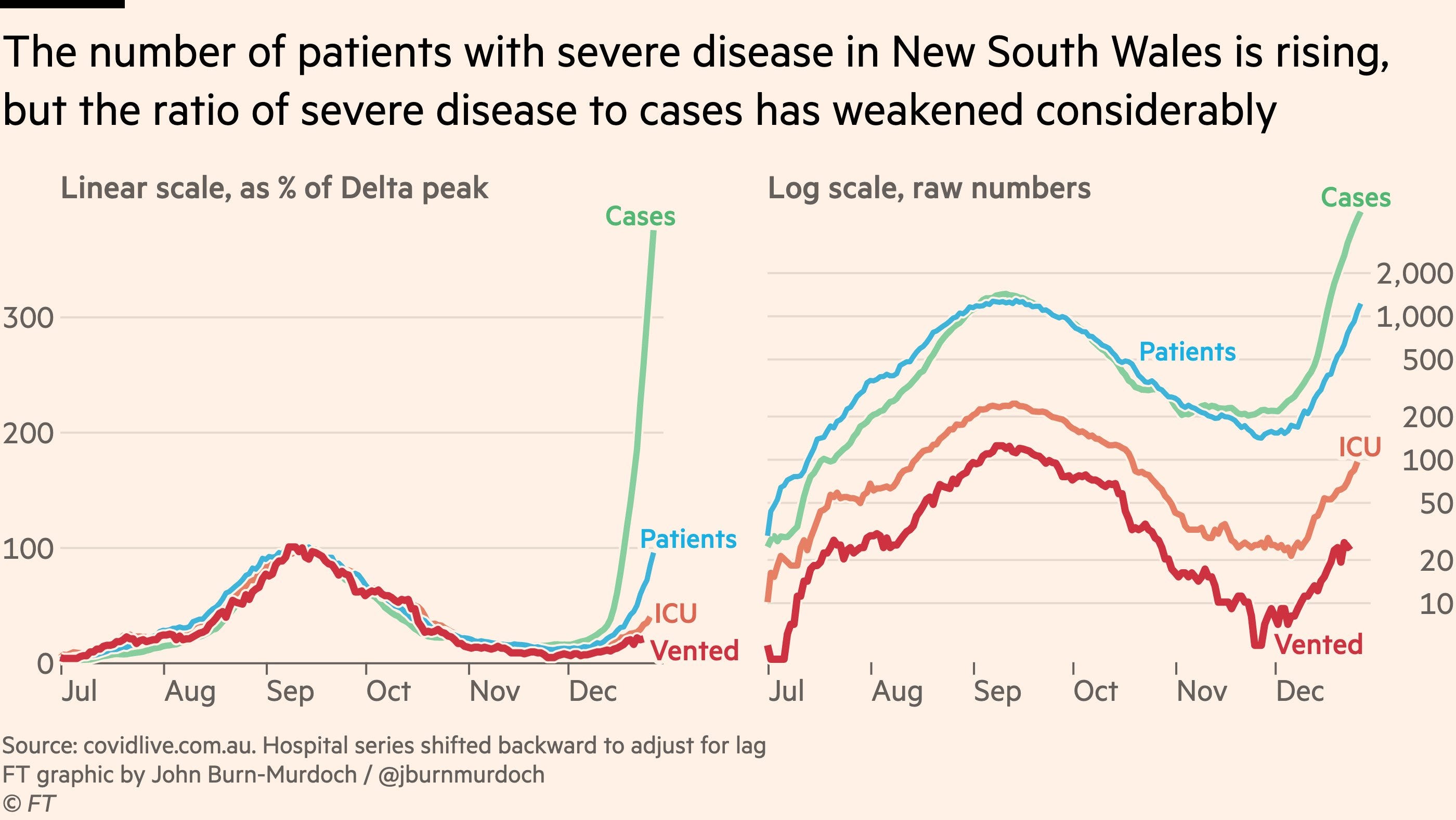
The log scale on the right means that it’s the gap between the lines we should pay most attention to, and it clearly does indicate good news.

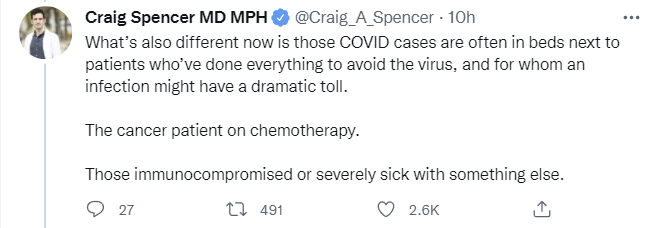
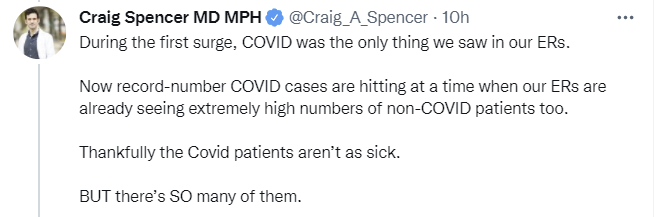
Similarly, this thread is on the situation in the hospitals and draws clear contrasts of those boosted, those vaccinated but not boosted, and the unvaccinated.
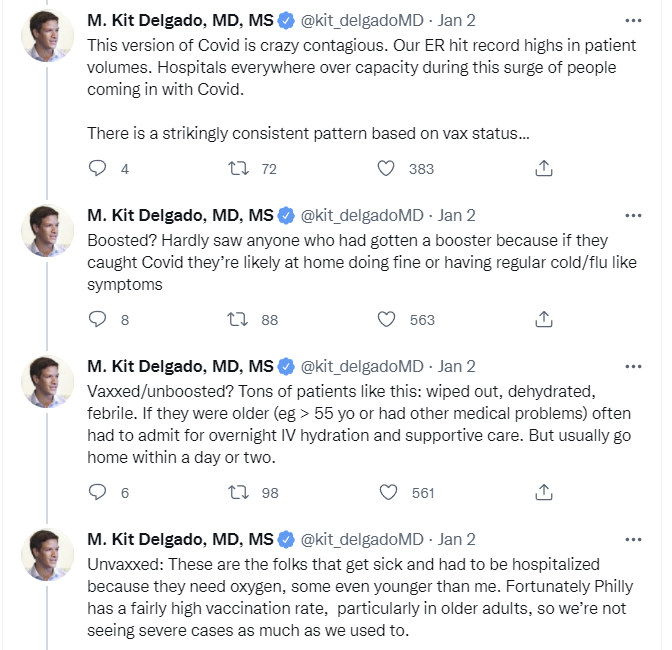
Hospitals
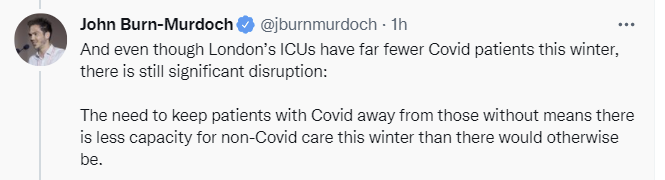
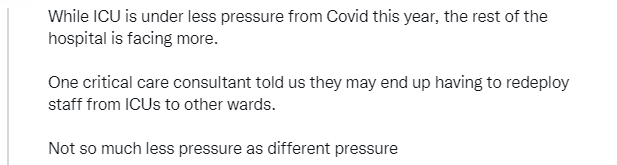
Our hospitals in many places were already under severe strain due to Delta. Now there’s a shortage of staff due to illness, and lots of Omicron patients showing up. Those patients mostly aren’t landing in the ICU, but the situation remains under tremendous strain on both sides of the pond.

UK hasn’t lowered their isolation requirements yet, which is compounding the problem there.
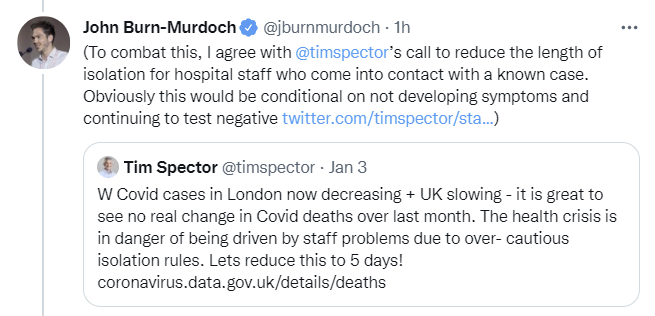
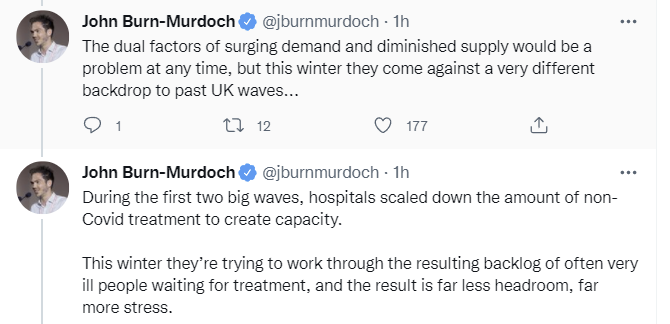
Backlogs persisting for months is entirely consistent with my model of the dynamics here. We never got our slack back from when we gave it up, because that would mean giving up permanently on patients.

Here’s the summary from the linked thread above.
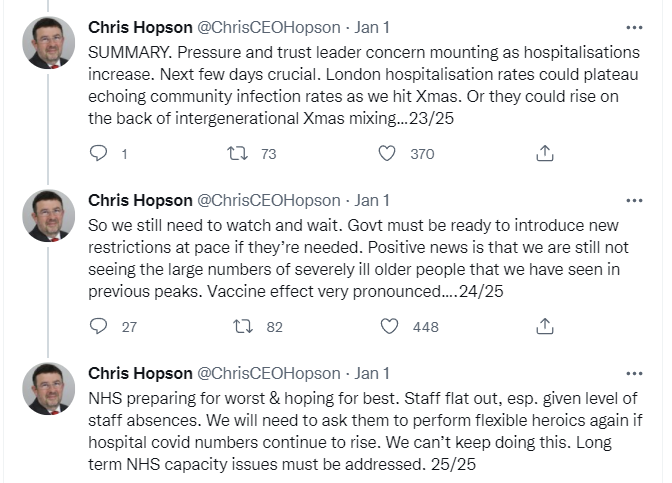
This seems right. Hospitals are in a bad way but holding. The scary scenario is if cases among the elderly are only now picking up and severity is much less reduced in that group while also starting out at a higher level, and things then get much worse. Cases are accelerating full blast and will peak very soon in the first-hit areas like New York and London if they haven’t already, but it will take another cycle or two before the effective risks start declining.
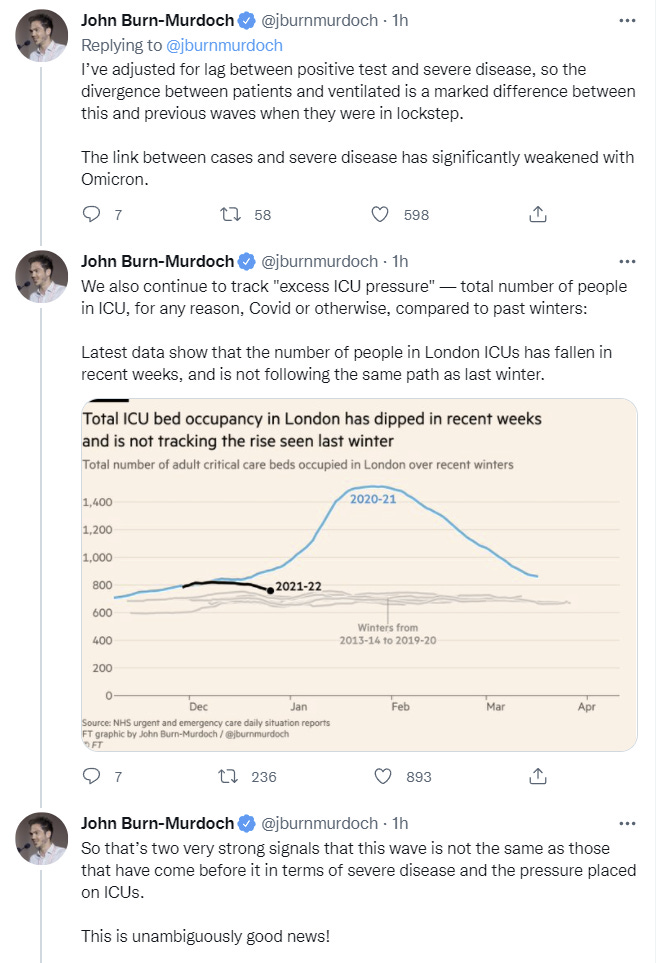
Hopson then had another updated thread on 3 January, which gives more hope that the scenario can be handled. Situation continues, and the problems in London are being seen elsewhere as well, but London isn’t getting that much worse.
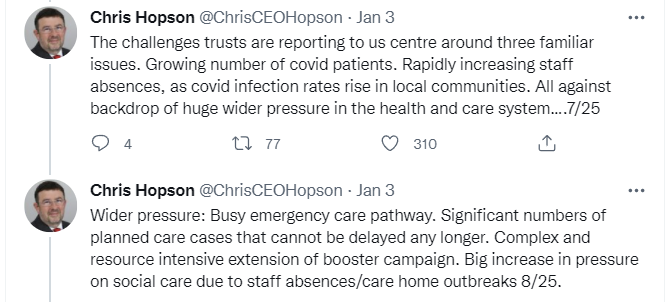
The news is good. The center is holding:
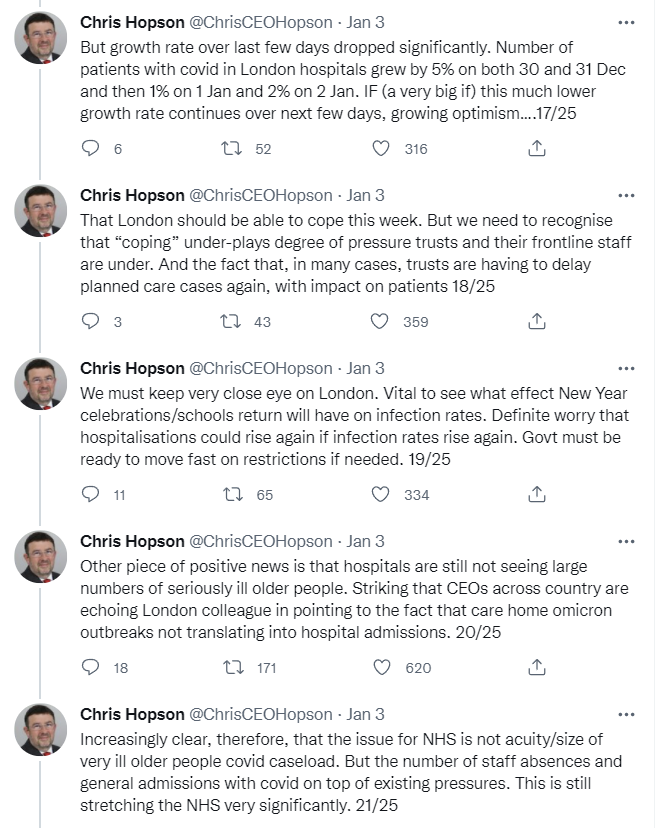
It’s not over yet, and it’s going to get worse before it gets better. Similar story from Philadelphia (see full thread for more details).
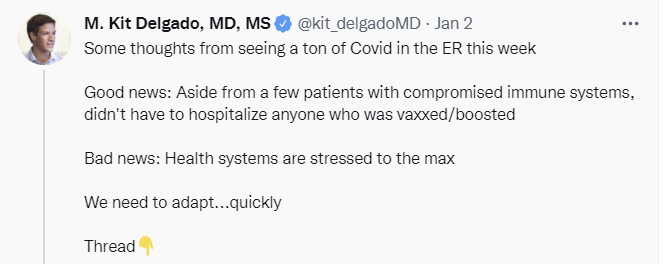
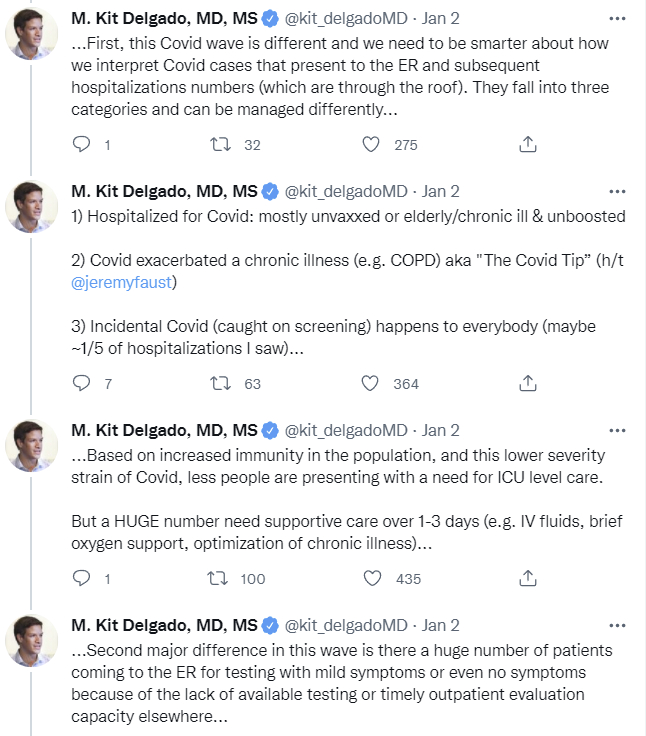
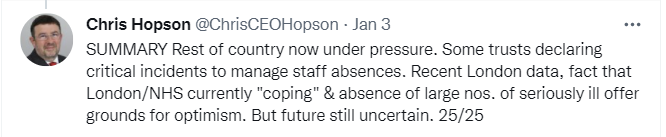
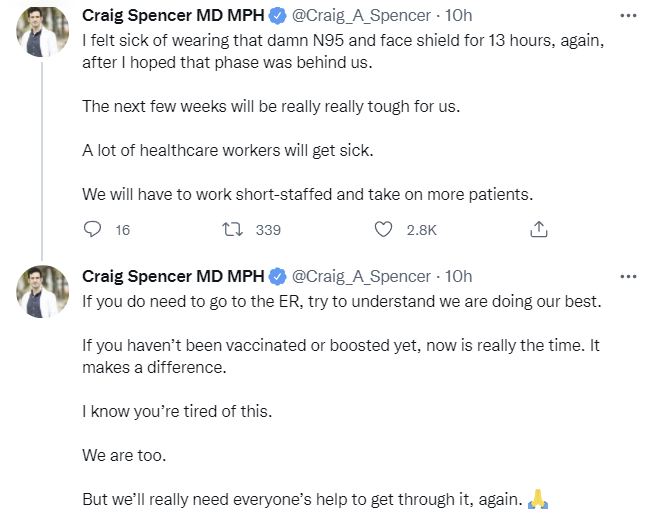
If I needed a test, and didn’t have much in the way of symptoms, I’d stay the hell away from the ER right now. That seems like a very good way for you to test negative today and then get your symptoms two or three days later. We need to do better warning essentially healthy people to keep their distance, not only for the system’s sake but for their own. This also seems like an excellent prescription if we are capable of doing it:
Link to that article. A lot of this is much worse due to a failure of professionals to talk logistics. I’m guilty of this too, in the sense that I don’t focus on forward-looking logistics often enough. Long term I need to remember to talk logistics more. After all, as Hunter S. Thompson pointed out, when the going gets weird, the weird turn pro.
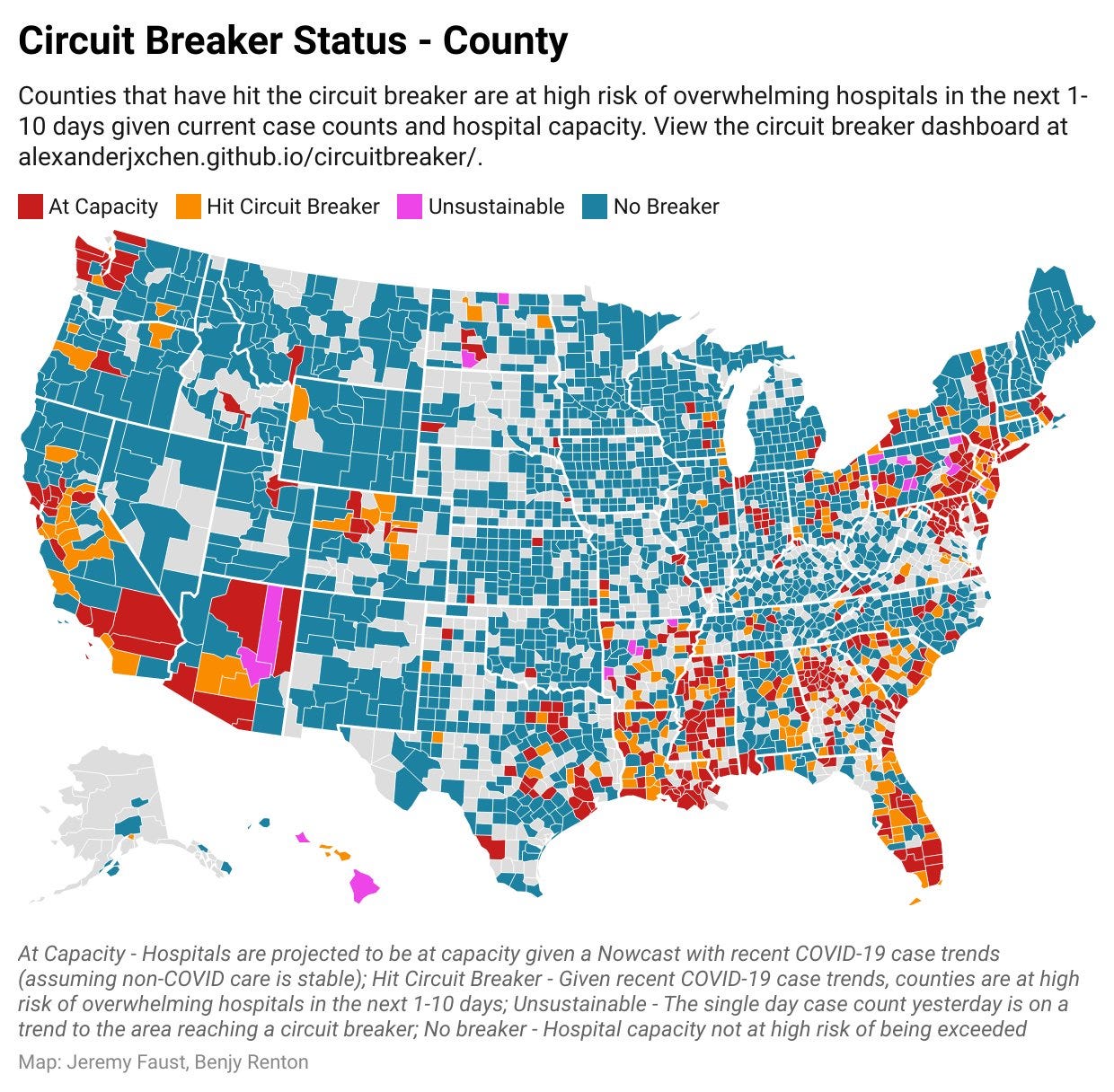
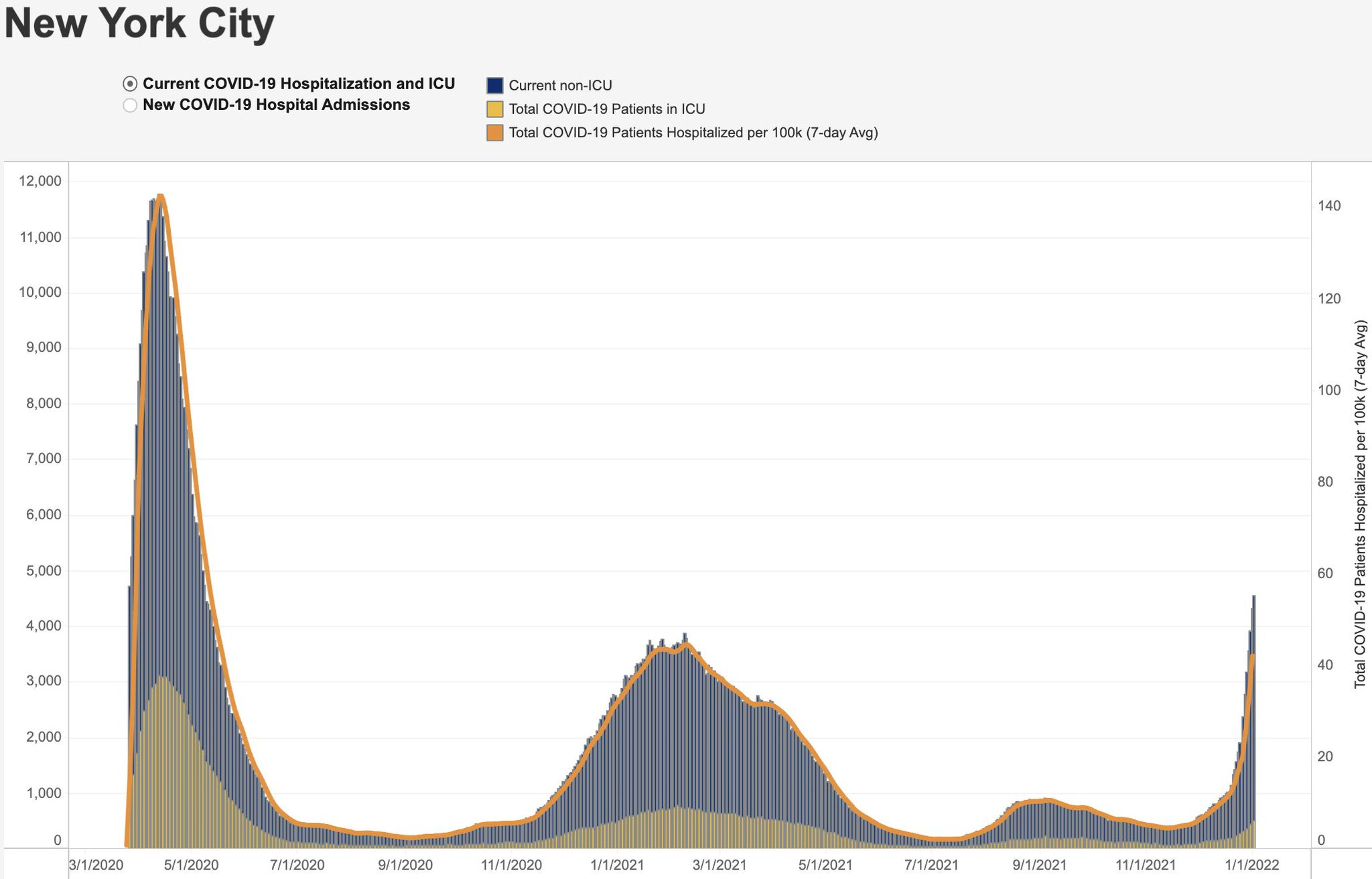
There’s a lot of population in the red and yellow areas here, but it’s not about whether you go over, it’s about how far you go over, and how bad the consequences will be for how long.
Here’s a thread about the situation in New York City. A lot of similar observations. I’m worried about this observation, which is the flip side to other places where it’s proving logistically difficult to administer care due to the need to avoid it:
Overall, same patterns.

Given how much downside risk there was initially, I’ll take this level of pressure.
It’s going to suck, a lot. But it looks like we’ll mostly make it through. If it was going to be a complete collapse, we would know by now.
Threads
Could we be looking at the Pi variant in France? This reply convincingly says no, this one is less kind, this isn’t new and if it had anything like Omicron’s infectiousness then we would know. Level of concern here very low.
This is what the quarantine looks like in Xi’an, where you’re not allowed to go outside for any reason so you’re dependent on government food deliveries, and they disinfect the streets anyway. This seems like Maximum Containment and it’s at best going to be close. This doesn’t seem sustainable.
Zeynep thread pointing out that exponential math eventually causes massive disruptions no matter what, in context of NYC.
Gottlieb predicts the wave will take two months, that NYC will peak within two weeks, most other areas within four weeks. If anything I expect it to be faster.
The question is how much more exponential growth is left before it’s over, and how much we should be focused on the hospitalization number versus the ICU number (because potentially we have a ton of people ‘with Covid’ instead of being there ‘for Covid.’)
Thread calling for more effort to slow spread on the basis of ‘millions being crippled by Long Covid’ and claiming that getting Covid now makes you more susceptible in the future by ‘creating pre-existing conditions.’ This is very much not my view, but if I did believe that Long Covid was this bad, the rest would indeed follow. I don’t see any evidence cited here that would cause me to update on my view of Long Covid.
Prediction Updates
Adding this, from Nate Silver (here’s Metaculus):
I hope soon to be able to expand my work with prediction markets, and also we’ll have everyone’s 2022 predictions to play off. Going to be a fun ride.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? %? → 50%.
Metaculus has the median for lifting this requirement in August, which roughly agrees with Nate. I’m more optimistic about not needing a mask mandate on planes, but also more skeptical that it will get lifted. Is your tray table up and your seatbelt in the full upright position? Have you met the TSA and their machines that they assure us no longer cause cancer (and that I still opt out of)?
Since this is a slow-moving one, I will only update it every so often. If you’re curious where I’m at, you can give me a nudge, but this should stay roughly here for a while.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 60% → 55%.
I messed up the math last time and said 70% before adjusting to 60%, but our starting point this week is 60%. On reflection, after adjusting for early advantage and looking at when things are stabilizing, my guess is that this is going to be close, and we may never know for sure.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 85% → 90%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 20% → 25%.
The news out of the hospitals seems clear. Unless something very strange is happening, Omicron is substantially more mild than Delta. I don’t expect us to hit the 75% threshold, but the news keeps being good on that front, so for now I’m creeping a bit higher.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% → 20%.
Israel is going with their fourth shot, but otherwise things seem to be settling into full complacency. I didn’t define who ‘we’ is here, but I meant the broad ‘we’ as in I personally have the legal option to get one, I’ll be 43 years old and technically have a risk condition but am not immunocompromised. Note that even if I’m allowed to get one, I don’t intend to get one if the peak has already passed.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 10% → 5%.
We’ve made our position clear. It’s going to be difficult to get care of any kind for a month, but we’ve picked ‘muddle through’ and we’re sticking to it.
Generation time (serial interval) of Omicron is 3.5 days or less: 85% → 87%.
This continues to be the best fit of the data and I’m creeping the number up a bit, but my guess is we will never find out for sure (unless it’s super not close) because experimentation remains illegal.
Daily cases in the the United States have peaked by February 1, 2022: ?% → 85%.
This seems like more than enough time to be on our way back down, but you can sustain a lot of cases for a long time. Feels right to express my degree of certainty about this. I’m curious how confident other people are on this.
I’ll open the floor to suggestions. What would be the most high-value things to put in the predictions section at this point? Links to Metaculus are always a bonus, or better yet real-money prediction markets. Mostly I plan to wait until I see the other 2022 prediction threads, and play off of those, like I have in the past.
21 comments
Comments sorted by top scores.
comment by Peter S (peter-s) · 2022-01-04T21:23:30.695Z · LW(p) · GW(p)
The Danish paper on negative effectiveness can be because Denmark required proof of vaccination to attend large events. If some of those events were superspreader events you would see an apparent negative effectiveness.
Same sort of result out of Canada, which also required vaccination for large events:
https://www.medrxiv.org/content/10.1101/2021.12.30.21268565v1
Replies from: CraigMichael↑ comment by CraigMichael · 2022-01-05T01:58:04.478Z · LW(p) · GW(p)
So the idea is the boosted/double-vaxxed risk-compensate with their behavior to an extent that they’re at more risk than, perhaps, a more isolated unvaccinated person?
Replies from: kjz↑ comment by kjz · 2022-01-05T03:26:57.084Z · LW(p) · GW(p)
That may contribute as well, but I think Peter was implying that if enough cases overall take place during superspreader events where ~all of the attendees were vaccinated, vaccinated people may be more likely to test positive just because they were substantially more likely to be attending those superspreader events than unvaccinated people.
Replies from: NormanPerlmutter↑ comment by NormanPerlmutter · 2022-01-05T08:01:24.492Z · LW(p) · GW(p)
How is that different from what CraigMichael said? Attending that sort of event is a type of risk compensation.
Replies from: kjz, tivelen↑ comment by kjz · 2022-01-05T17:55:44.022Z · LW(p) · GW(p)
I agree that attending large events is a type of risk compensation, and we may be referring to similar behavior patterns using different words here. But I'm trying to distinguish between these two types of infection:
- Infections resulting from people going about their daily activities (e.g. getting exposed at work, in a store or restaurant, other small gatherings, etc.) Here, individuals might indeed change their behavior based on their own vaccination status and risk tolerance. But since Omicron is so widespread at this point, the probability that an infected person was vaccinated should be close to the base rate of vaccination among the overall population (although somewhat lower, since the vaccines still prevent some transmission of Omicron). In other words, P(vaccinated | type-1 infection) is a little less than P(vaccinated).
- Infections resulting directly from attending large superspreader events where proof of vaccination was required. In this case, while P(vaccinated | type-2 infection) won't be exactly 1 due to the possibility of fake vaccine ID cards or weak enforcement of the policy at the event, I think it would still be quite close to 1.
If type-2 infections are a high enough percentage of overall infections, this could make it look like vaccinated people are more likely to get infected (which would be true at the population level!) even though getting vaccinated makes it less likely for any individual to get infected (assuming their behavior after vaccination remains the same).
Apologies if much of this is obvious or redundant - I'm still trying to understand the gears behind this dynamic better myself. I agree there is likely a component coming from "vaccinated people take on more risk in general", but I hadn't considered that policies which only allow vaccinated people (to a first approximation) to attend large potentially-superspreading events could lead to increased transmission among the vaccinated relative to the unvaccinated, which could lead to negative perceived vaccine effectiveness, until seeing Peter's post.
Replies from: NormanPerlmutter↑ comment by NormanPerlmutter · 2022-01-10T03:24:19.725Z · LW(p) · GW(p)
Thank you, good explanation. But see also my response to tivelen below.
↑ comment by tivelen · 2022-01-05T16:21:02.516Z · LW(p) · GW(p)
Suppose 50% of vaccinated people would attend this event, and so would 50% of unvaccinated people, after considering the risks (ergo, there is no risk compensation). However, only vaccinated people are allowed to go to the event. Then the vaccinated people could have increased rates of Covid compared to unvaccinated people because of being more likely to attend superspreader events, even though they did not increase their level of risk compared to the unvaccinated population.
Whether this is the actual reason for the apparent negative effectiveness would depend on the actual percentages, and how common/dangerous superspreader events really are.
↑ comment by cistrane · 2022-01-06T01:13:33.193Z · LW(p) · GW(p)
But effectively, the unvaccinated were not allowed to have the same level of risk as vaccinated if they couldn't come to the event, right?
Replies from: tivelen↑ comment by tivelen · 2022-01-06T16:20:13.451Z · LW(p) · GW(p)
A vaccination requirement could result in lower apparent effectiveness; so could risk compensation. In order to determine how much risk compensation occurred, we have to determine how much the vaccination requirement lowered the effectiveness. Without that analysis, concluding that risk compensation has a big enough effect to cause or contribute significantly to negative effectiveness is premature.
I am otherwise unsure of what you are trying to get at. The unvaccinated were prevented from doing a risky activity, and the vaccinated were allowed to do the activity (with a lower risk due to their status), yes.
↑ comment by cistrane · 2022-01-08T19:12:01.927Z · LW(p) · GW(p)
Well, if this is consistently applied across many events, the unvaccinated will not be allowed risky activities and the vaccinated will be allowed risky activities. Which means in practice consistently higher number of risky activities available for the vaccinated. I agree that this effect might not be significantly big and more measurements would be needed.
↑ comment by NormanPerlmutter · 2022-01-10T03:25:30.968Z · LW(p) · GW(p)
This is true to an extent. Unvaccinated people are still able to attend. They just would need to forge their vaccination card. I think this is not particularly hard to do, though it's not trivially easy and many unvaccinated people would not do it for ethical reasons.
comment by Brendan Long (korin43) · 2022-01-04T18:01:03.682Z · LW(p) · GW(p)
I'm not sure if there's enough information to make these predictions, but things I want to know are:
-
Does budesonide help with COVID? (Will the FDA approve budesonide as a COVID treatment / will it be considered 'standard of care' by some metric by some date)
-
Will there be another variant that infects some suitably large % of the population this summer / next winter?
comment by agc · 2022-01-04T17:34:29.067Z · LW(p) · GW(p)
The claim that a school is ‘the safest place for our kids’ in a pandemic is grade-A Obvious Nonsense
I'm not sure about that. Covid isn't all that dangerous for children, and possibly a good portion of them would otherwise be in some unsafe kind of childcare.
Note that even if I’m allowed to get one, I don’t intend to get one if the peak has already passed.
Why is that? If I somehow make it through the next 4 months without getting Covid I wouldn't mind an other booster, to top up fading immunity and protection in case there is a more virulent Omicron-derived variant in the future.
Replies from: philh↑ comment by philh · 2022-01-07T21:16:59.281Z · LW(p) · GW(p)
I don't know Zvi's reasoning, but you'd be able to get such a booster upon news of that variant, which might be better than getting it several months before the variant. (But perhaps worse than "long enough before that you can get a fifth shot when it arrives".)
I have some abstract concern about the possibility of developing immune reactions to mRNA shots so that we can only get a limited number of them over a lifetime. I haven't looked into it in depth or even what experts think, it's not right now gonna stop me from getting a shot that seems important, but it might swing me to no on a just-in-case.
comment by Pattern · 2022-01-04T18:28:40.547Z · LW(p) · GW(p)
Large negative effectiveness is not a thing,
What's being measured? If people go out of lockdown and interact more after being vaccinated, I could see it. That does require the people who aren't vaccinated to not do that stuff too though.
Replies from: GWS↑ comment by Stephen Bennett (GWS) · 2022-01-05T00:18:32.673Z · LW(p) · GW(p)
Iirc they also did not control for previous infection. My model of why “VE” went negative is due to “natural” versus vaccinated immunity, with natural immunity lasting longer and/or generalizing better to new variants (at the cost of much higher disease burden coming into present conditions). I was confused about what how exactly they computed VE, however, so I might just be missing something.
I’ll note that even with waning immunity, I expect vaccination to have been and remain a clear net positive to my health. I’m more on the fence for boosters because I am young male and healthy, and omicron may well be milder than some future variant, and I expect it to provide better immunity in the future. If I’m wrong about any points in that chain of “and”s, however, I expect to be wrong in a way that favors getting boosted.
comment by rosyatrandom · 2022-01-05T10:14:26.699Z · LW(p) · GW(p)
On quarantining/geo-boxing:
Even if the different regions have similar numbers of cases, is there an argument to be made for confinement in that it keeps variants more isolated?
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2022-01-07T07:11:18.731Z · LW(p) · GW(p)
I've wondered about that too. And not just for Covid
comment by Bucky · 2022-01-04T19:29:13.667Z · LW(p) · GW(p)
More “for Covid” vs “with Covid” from England:
https://www.bbc.co.uk/news/health-59862568
Ratio in October was 3:1 (for:with) but this has gone down to 2:1. “For” cases are rising but at a lower fractional rate than “with” cases.
comment by CraigMichael · 2022-01-05T02:09:52.433Z · LW(p) · GW(p)
I basically agree with Rachel Thomas on everything, but I think she’s overestimating the risk of long Covid and hire much we can realistically do at this point to stop Omicron.
Would also like to see fluvoxamine mentioned along with paxlovid.