Covid 1/21: Turning the Corner
post by Zvi · 2021-01-21T16:40:00.941Z · LW · GW · 41 commentsContents
The Numbers Predictions Deaths Positive Test Percentages Positive Tests Test Counts Covid Machine Learning Project Vaccinations Europe The English Strain The Other New Strains But What Do We Do Now? You’re Vaccinated, Now What? Yes, We Can Agree Andrew Cuomo Is The Worst The Quest to Sell Out of Covid Vaccine Vaccine Allocation By Politics and Power Prioritization by Lack of Virtue Would you like a vaccine? If so, check this box. Useful Resources How Bad is it Out There Right Now? You Should Know This Already In Other News For Those Who Actively Want to Give Me Money None 41 comments
Aside from worries over the new strains, I would be saying this was an exceptionally good week.
Both deaths and positive test percentages took a dramatic turn downwards, and likely will continue that trend for at least several weeks. Things are still quite short-term bad in many places, but things are starting to improve. Even hospitalizations are slightly down.
It is noticeably safer out there than it was a few weeks ago, and a few weeks from now will be noticeably safer than it is today.
Studies came out that confirmed that being previously infected conveys strong immunity for as long as we have been able to measure it. As usual, the findings were misrepresented, but the news is good. I put my analysis here in a distinct post, so it can be linked to on its own.
We had a peaceful transition of power, which is always a historic miracle to be celebrated.
Vaccination rollout is still a disaster compared to what we would prefer, with new disasters on the horizon (with several sections devoted to all that), but we are getting increasing numbers of shots into increasing numbers of arms, and that is what matters most. In many places we have made the pivot from ‘plenty of vaccine and not enough arms to put shots into’ to the better problem of ‘plenty of arms to put vaccine into, but not enough shots.’ Then all we have to do is minimize how many shots go in the trash, including the extra shots at the bottom of the vial, and do everything we can to ramp up manufacturing capacity. Which it seems can still be meaningfully done.
The problem is that the new strains are coming.
The English strain will arrive first, within a few months. That’s definitely happening, and the only question is how bad it’s going to get before we can turn the tide. We are in a race against time.
The South African and Brazillian strains are not coming as fast, but are potentially even scarier. There are signs of potential escape from not only vaccination but previous infection, potentially allowing reinfection to take place. See the section on them for details, and if you can help provide better information, please do so. We need clarity on this, and we need it badly.
There are also all the other new strains being talked about, which are probably nothing, but there’s always the chance that’s not true.
But first, the good news, and it is very, very good. Let’s run the numbers.
The Numbers
Predictions
Prediction last week: 14.0% positive rate on 11.7 million tests, and an average of 3,650 deaths.
Results: 11.9% positive rate on 11.3 million tests, and an average of 3,043 deaths.
Both numbers are hugely pleasant surprises, and this is the biggest directional miss I’ve had on deaths.
Last week we were at 3,335 deaths per day, and I figured things would keep getting worse for another week or two. Instead, things are already on their way to rapid improvement, unless there were massive shifts in when deaths were reported that made last week look worse than it was.
For infections, I did predict a drop (last week was 15.2%) and we got a much more dramatic drop than I expected. This was wonderful news, and it seems like this should continue.
The caveat is that Tuesday and Wednesday of this week both look suspiciously good on both stats, such that I suspect missing data. I don’t know if somehow Martin Luther King Day actually mattered to reporting, or the inauguration and fears of disruptions around it were distracting, or what, but we should worry that this is getting a bit ahead of ourselves, even though test counts would indicate otherwise.
Test count predictions don’t seem worth doing, so going to stop doing those.
Prediction: 10.5% positive rate and 2,900 deaths per day. I’m being conservative because I worry about the drops from this week being data artifacts, but I am confident things are improving for now. Starting next week I’ll be expecting the IFR to start dropping substantially due to selective vaccinations.
Deaths
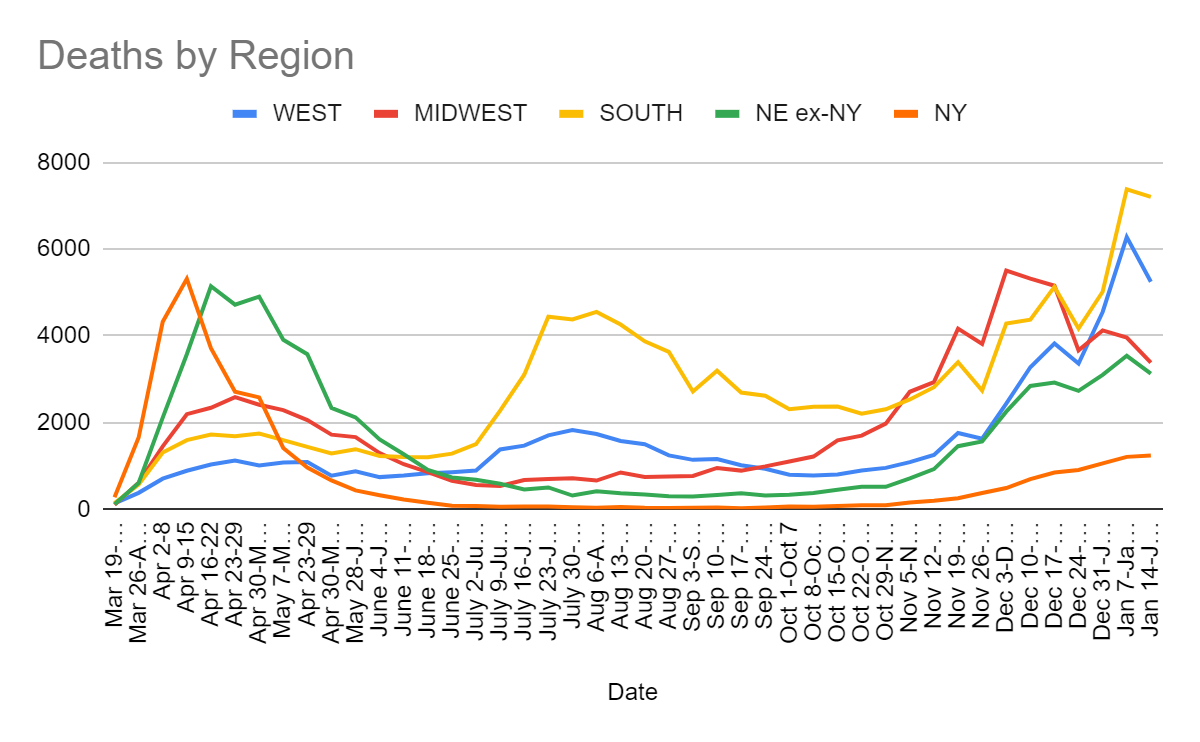
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Nov 19-Nov 25 | 1761 | 4169 | 3396 | 1714 |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
| Dec 17-Dec 23 | 3826 | 5158 | 5131 | 3772 |
| Dec 24-Dec 30 | 3363 | 3668 | 4171 | 3640 |
| Dec 31-Jan 6 | 4553 | 4127 | 5019 | 4162 |
| Jan 7-Jan 13 | 6280 | 3963 | 7383 | 4752 |
| Jan 14-Jan 20 | 5249 | 3386 | 7207 | 4370 |
As noted above, this was expected to get much worse, and instead things started improving, although they’re still in a worse spot than two weeks ago. This is very good news, and it sheds new light on what has been happening in the past few weeks. If everything we’d seen previously had been fully reflective of the situation on the ground, we would not have seen a decline in deaths this week.
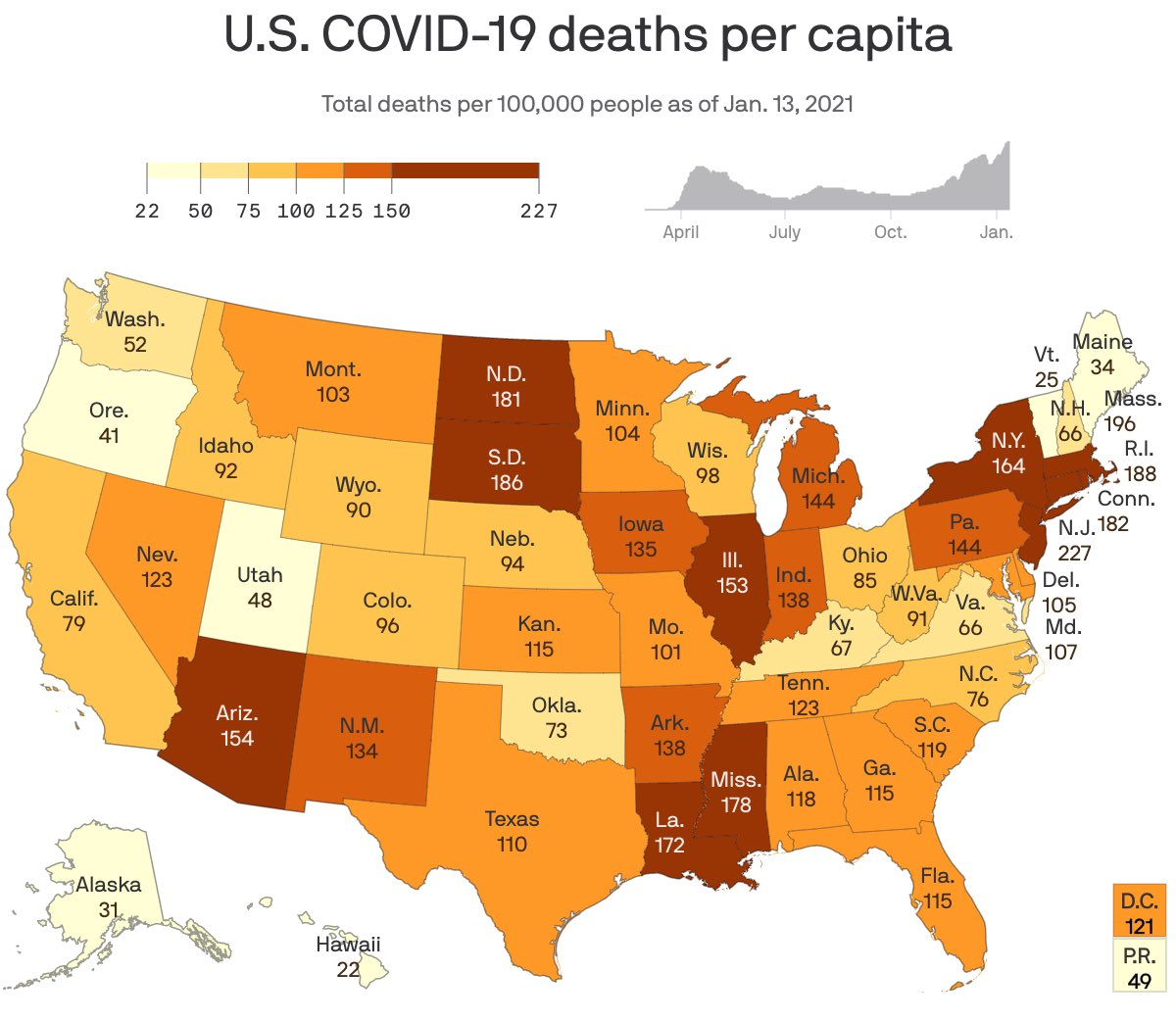
This graphic of cumulative deaths comes courtesy of Venkesh Rao on Twitter, seemed crisp and useful enough to include, from a few days ago:
Positive Test Percentages
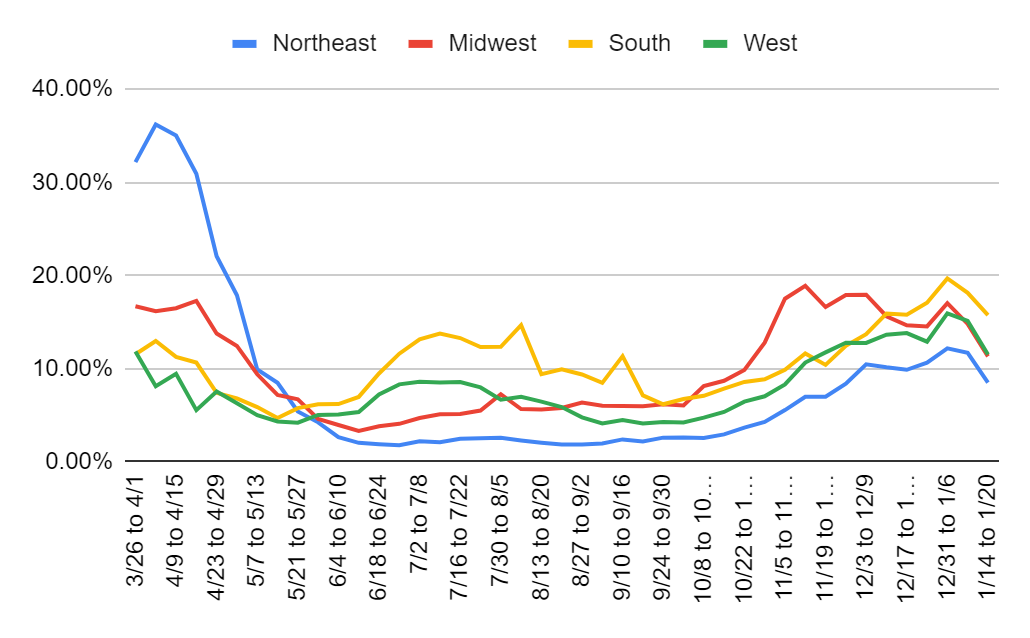
| Percentages | Northeast | Midwest | South | West |
| 11/26 to 12/2 | 8.38% | 17.90% | 12.45% | 12.79% |
| 12/3 to 12/9 | 10.47% | 17.94% | 13.70% | 12.76% |
| 12/10 to 12/16 | 10.15% | 15.63% | 15.91% | 13.65% |
| 12/17 to 12/23 | 9.88% | 14.65% | 15.78% | 13.82% |
| 12/24 to 12/30 | 10.65% | 14.54% | 17.07% | 12.90% |
| 12/31 to 1/6 | 12.18% | 17.03% | 19.69% | 15.94% |
| 1/7 to 1/13 | 11.70% | 14.81% | 18.14% | 15.12% |
| 1/14 to 1/20 | 8.50% | 11.32% | 15.75% | 11.53% |
Test counts are up, positive test rates are down everywhere. Great numbers.
Positive Tests
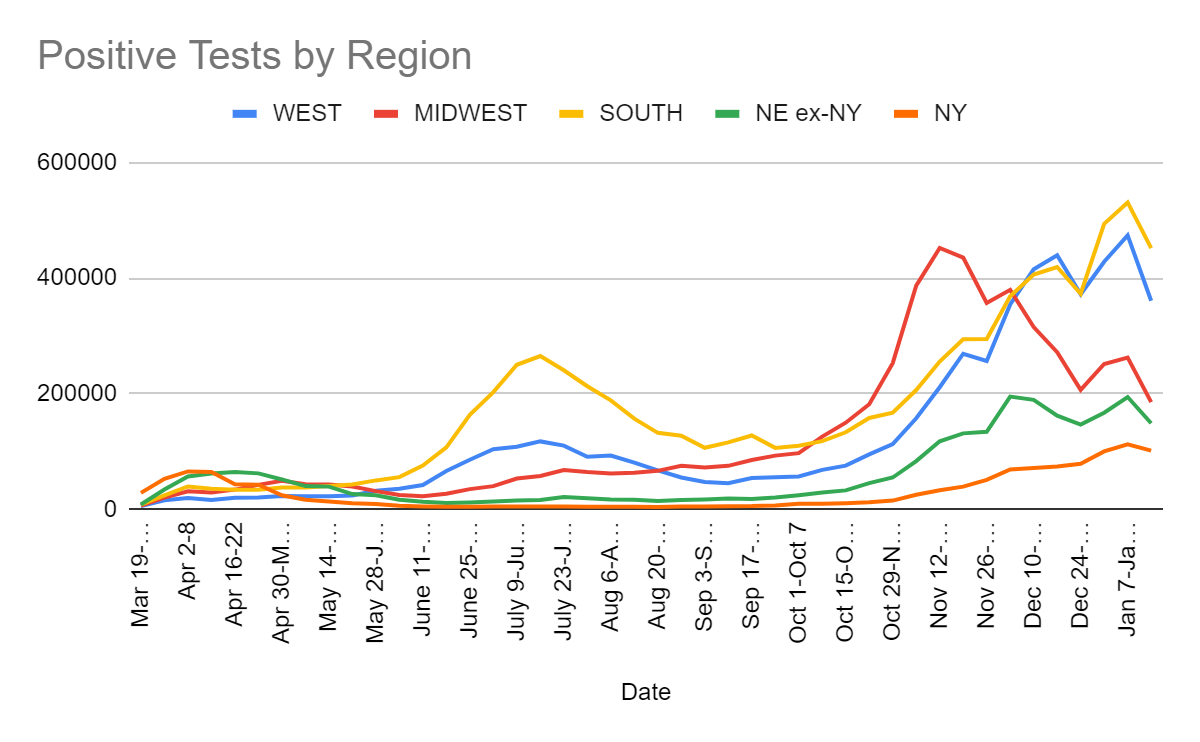
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Dec 3-Dec 9 | 354,397 | 379,823 | 368,596 | 263,886 |
| Dec 10-Dec 16 | 415,220 | 315,304 | 406,353 | 260,863 |
| Dec 17-Dec 23 | 439,493 | 271,825 | 419,230 | 236,264 |
| Dec 24-Dec 30 | 372,095 | 206,671 | 373,086 | 225,476 |
| Dec 31-Jan 6 | 428,407 | 251,443 | 494,090 | 267,350 |
| Jan 7-Jan 13 | 474,002 | 262,520 | 531,046 | 306,604 |
| Jan 14-Jan 20 | 360,874 | 185,412 | 452,092 | 250,439 |
Good news all around, and overall test count was even up about 2%.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Nov 19-Nov 25 | 10,421,697 | 11.8% | 1,373,751 | 2.9% | 3.88% |
| Nov 26-Dec 2 | 9,731,804 | 11.8% | 1,287,010 | 4.0% | 4.23% |
| Dec 3-Dec 9 | 10,466,204 | 13.9% | 1,411,142 | 4.9% | 4.67% |
| Dec 10-Dec 16 | 10,695,115 | 13.9% | 1,444,725 | 4.9% | 5.12% |
| Dec 17-Dec 23 | 10,714,411 | 13.7% | 1,440,770 | 5.1% | 5.57% |
| Dec 24-Dec 30 | 9,089,799 | 13.8% | 1,303,286 | 6.0% | 5.95% |
| Dec 31-Jan 6 | 9,334,345 | 16.4% | 1,365,473 | 7.3% | 6.42% |
| Jan 7-Jan 13 | 11,084,291 | 15.2% | 1,697,034 | 6.6% | 6.93% |
| Jan 14-Jan 20 | 11,300,725 | 11.9% | 1,721,440 | 5.9% | 7.35% |
In addition to the numbers listed, hospitalizations are also finally on the decline. I don’t generally track hospitalizations because I worry the limiting factor is often hospital beds, but seeing a decline is definitely a very good sign.
Covid Machine Learning Project
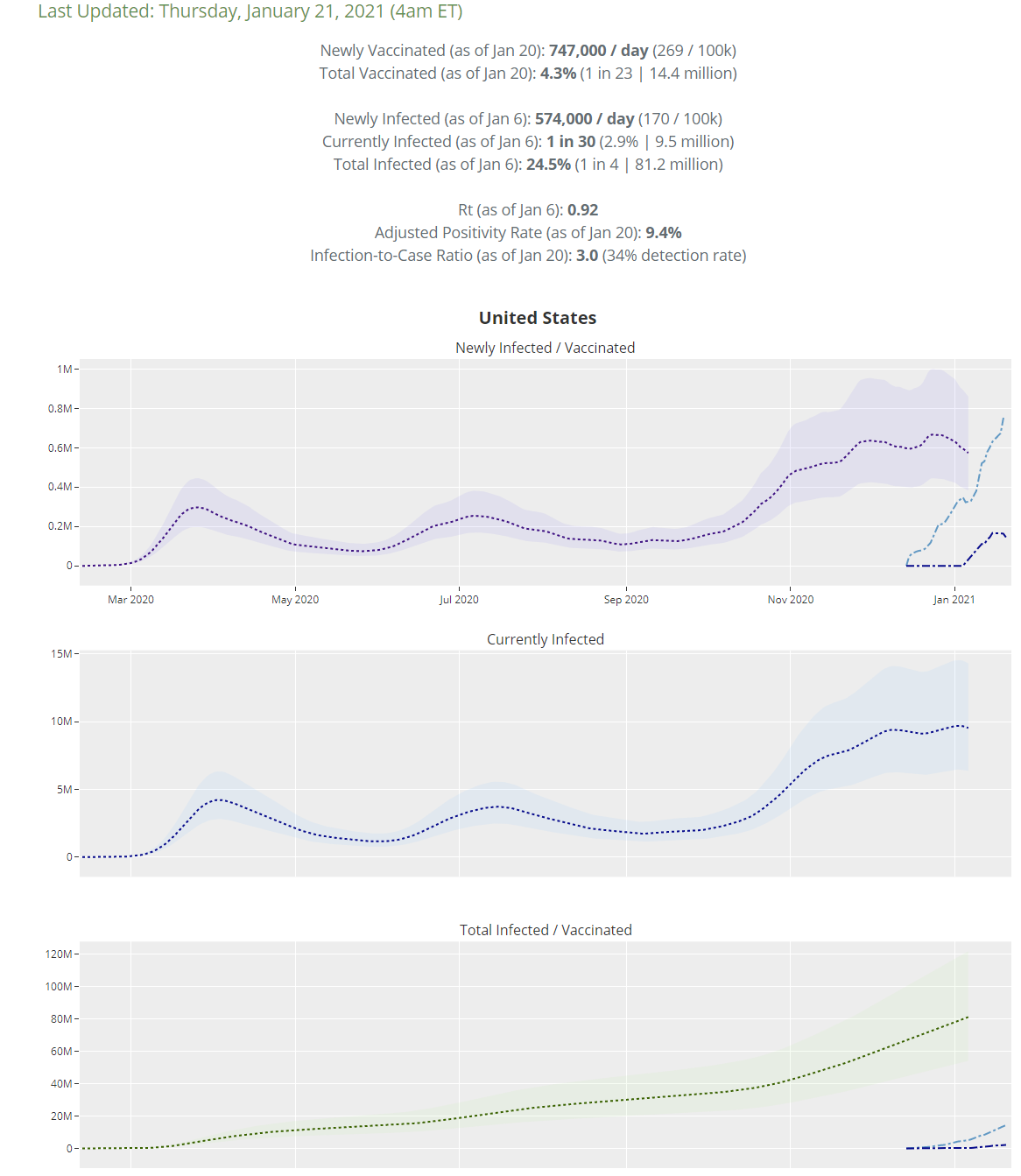
Look at that vaccination line shoot upwards and the newly infected line start heading downwards. You love to see it.
As of January 6 these projections had us at 24.5% infected, versus 23.4% a week before. This continues to be my rough lower bound for how many people have been infected. Herd immunity from infection is having a big and growing impact.
Vaccinations
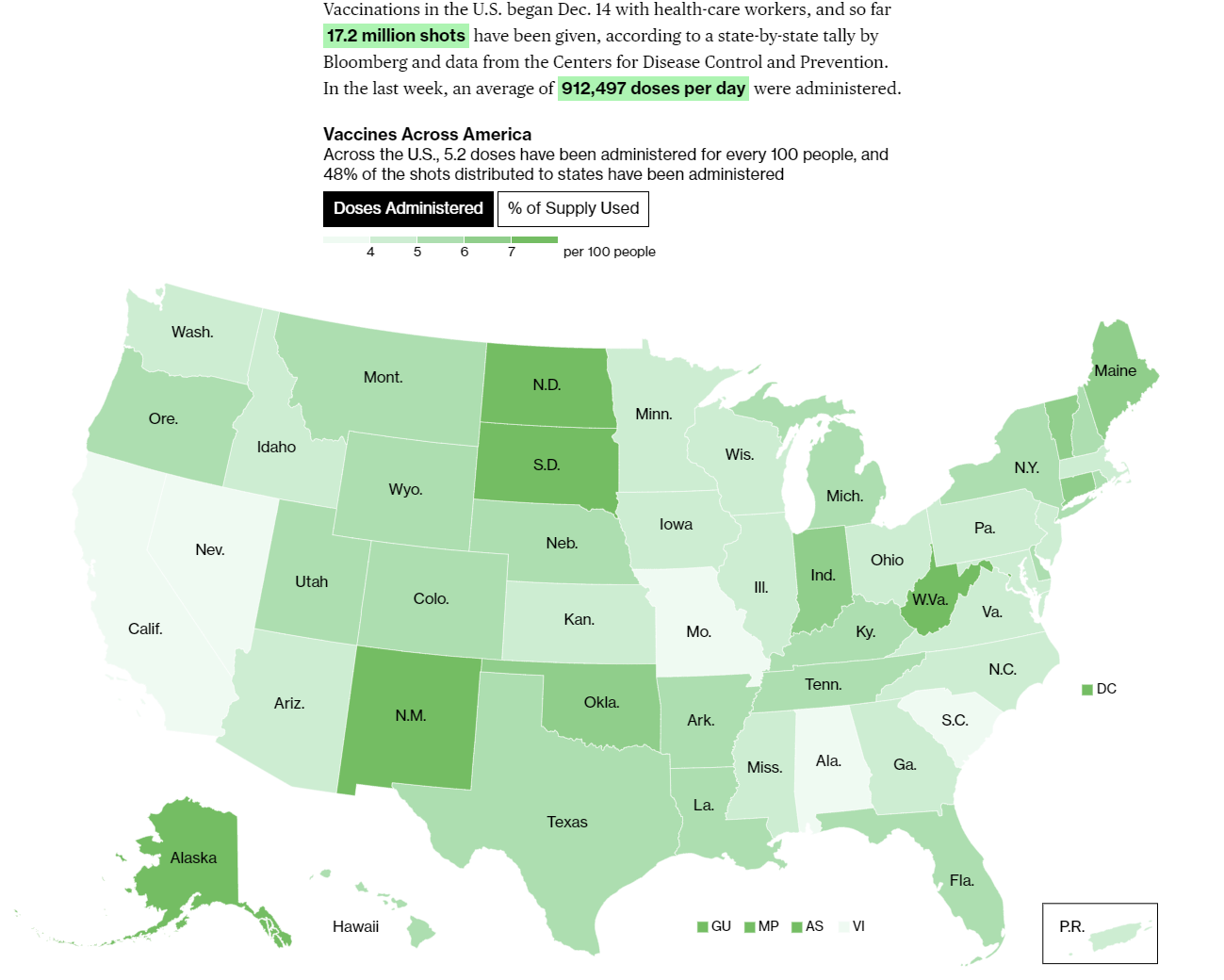
Relative regional progress remains unchanged. If you were behind last week, you’re almost certainly even further behind now. California continues to do an unusually disgraceful job with its vaccine rollout, which will be discussed extensively later. New York, for all the complaining that gets done about it, is doing relatively fine.
The headline number is 912k doses per day over the course of the week, the bulk of which were first doses. That’s not great, and it isn’t improving that quickly, but it’s much less disastrous than the worst scenarios that were being pondered. It’s also enough that we should start seeing the effect of those vaccinations in both infections and deaths soon if we aren’t seeing it already.
Europe
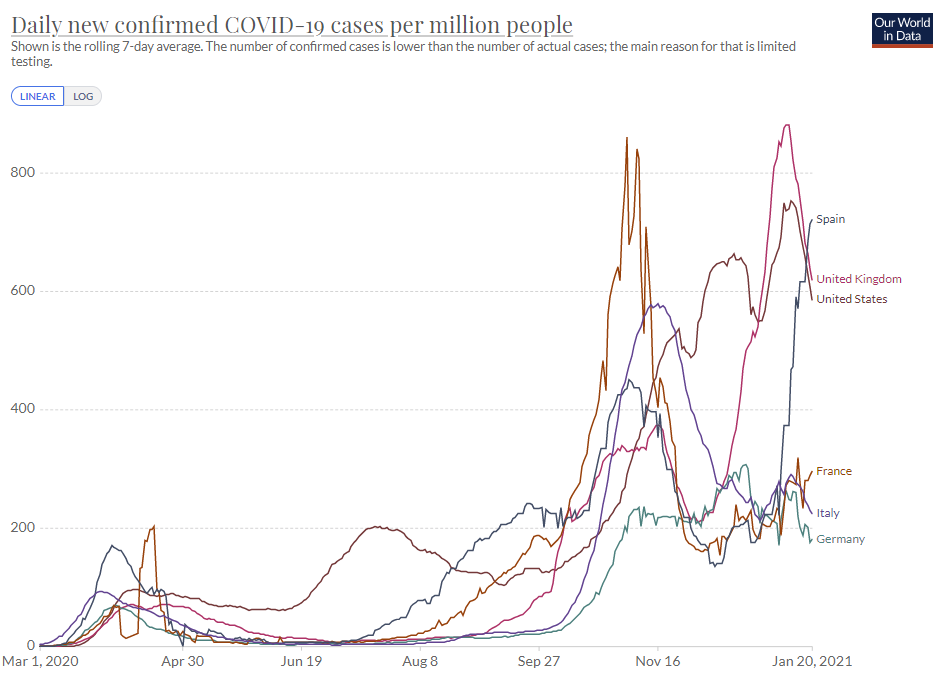
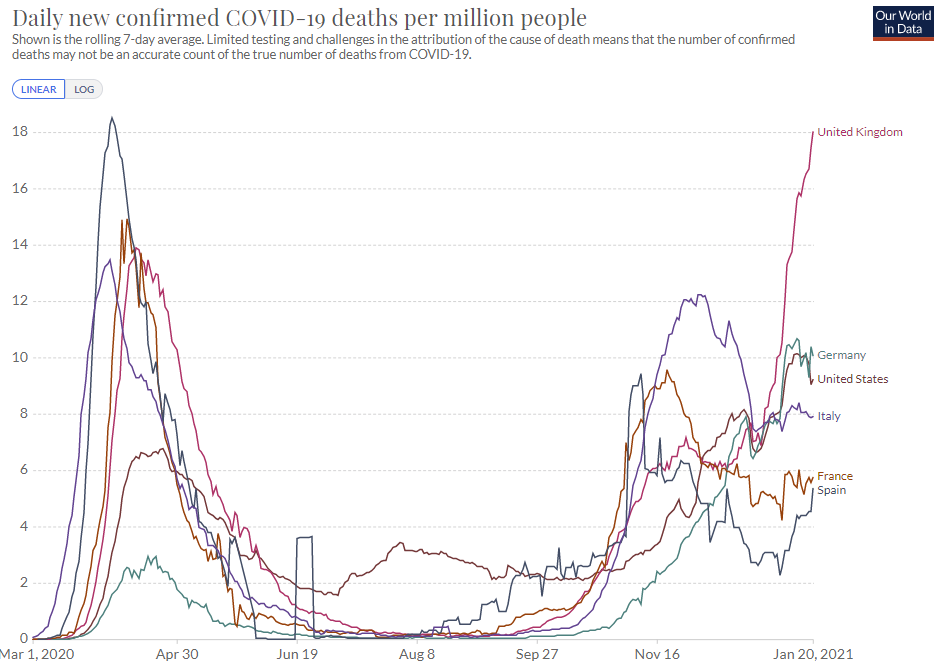
The first graph’s story is: All hail the control system. The United Kingdom is on its way back down in infections once again, despite the domination of the new strain. The peak was January 9th. Ireland is not pictured, but it peaked on the 10th at an even higher rate and is following a similar curve.
The second graph’s story is that the new strain is still killing an awful lot of people before that happens. We are currently 12 days past the peak of infections, so the line should keep going up for a few more days.
Now Spain is out of control. I don’t know if that is partly because of the English strain taking over, or entirely for other reasons.
It seems clear that yes, with sufficiently strong restrictions and private reactions, the United Kingdom at least can stabilize the infection level against the new strain. I still am not sure if America could or would do the same under the same conditions. We’ll find out soon, with conditions that in some ways will be substantially more favorable, with more people vaccinated and more people having already been infected.
The English Strain
Scott Gottlieb reached the same core conclusion I did, at least by January 17, that the new strain will likely double every week, so we’ll see a few weeks of declines and then things start getting worse again. So did Eric Feigl-Ding, and many others, including the CDC itself. It seems that my core conclusions of December 24 are now rapidly becoming the official Very Serious Person perspective.
The CDC is out with their analysis, accepting the basic premise of increased transmission and modeling outcomes. They are assuming a baseline of 0.5% of cases are the new strain at start of the year, which seems reasonable. I did some toy modeling, and they are doing some toy modeling, except with more toys and less models.
They split into the R0=1.1 and R0=0.9 scenarios for the current situation.
Note that they are assuming only 25% of cases are reported, so their immunity effect from infections is larger.
Without vaccinations, they
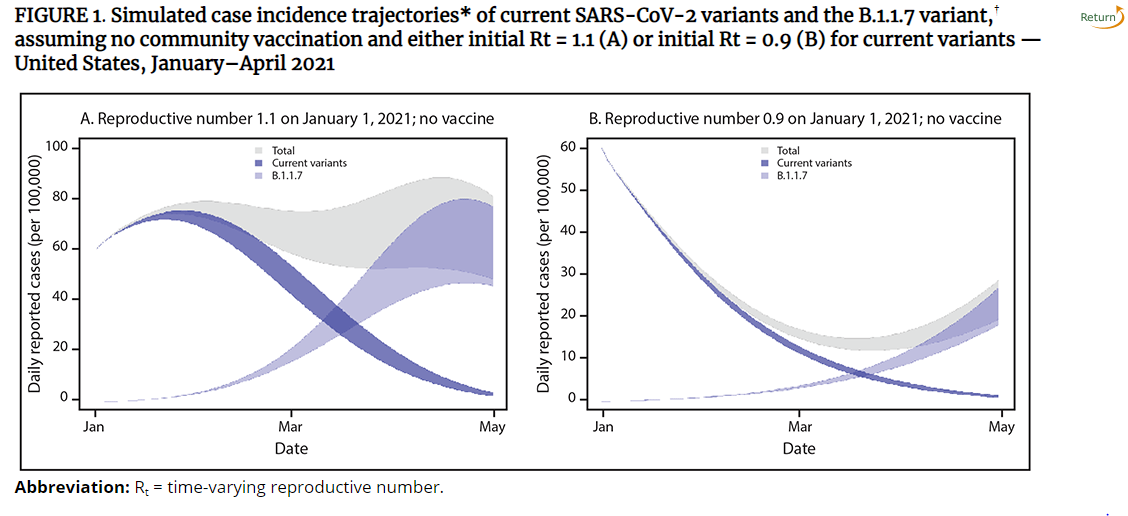
Then here it is with vaccination of 0.15% of the population per day (e.g. shots per day equal to 0.3% of the population, with two shots per person) or about the same as my model’s assumption:
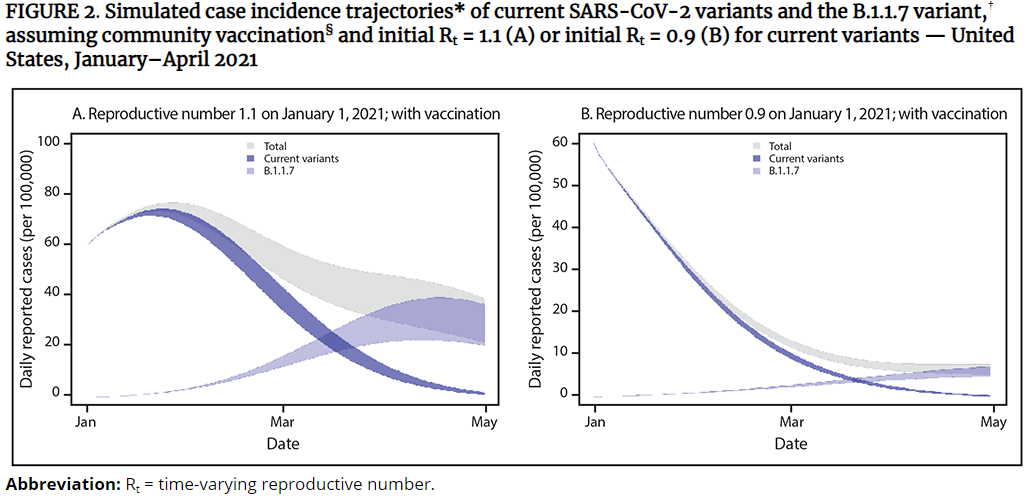
For those who criticize me for not respecting the control system, the CDC says, what’s a control system and how do we talk to the people in charge?
Their recommendation, of course, is the same as it is for anything else. Universal compliance with existing policies, and more vaccinations. Thanks, CDC!
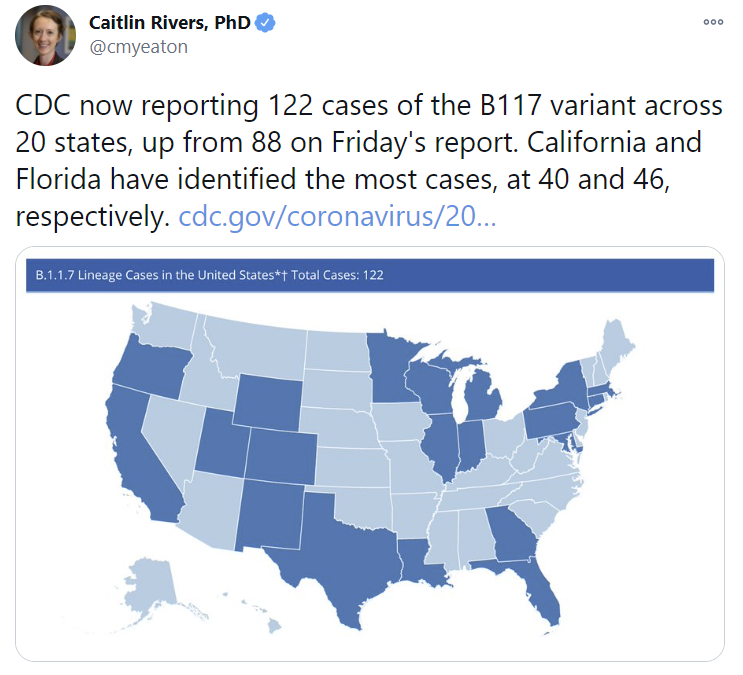
Here’s how things are progressing, right on schedule (CDC link):
The vaccines are confirmed to work on the English strain and I won’t bother sharing further similar findings unless they put this finding into doubt.
The Other New Strains
What about all these other new strains, which many claim are even worse than the English strain? How likely is it that things are even worse? What do we know about these other strains?
Early in the week, we knew a lot of things that were possibly scary, but nothing definite. I know experimentation is illegal when it has to be done on people, but in this case the experiments we need can be done in a laboratory in approximately zero time for approximately zero dollars with approximately no risk to anyone – you see whether neutralizing antibodies from various sources are effective against various strains – so it’s (to put it politely) rather frustrating when no one runs the tests.
The test did get done later in the week, at least for the South African strain, and the results were quite alarming. I’ll get to that later in the section.
A question that isn’t getting enough attention is: Why suddenly all these strains now?
I see a bunch of people saying things like this, starting a high quality infodump thread:
And few if any of them are acting at all suspicious about the whole thing. Whereas my instincts whisper: This Is Not a Coincidence Because Nothing Is Ever a Coincidence.
As I noted last week, the timing seems highly suspicious. There are new mutations every day. Why are there suddenly so many scary new strains?
It can’t be the vaccinations, because the timing doesn’t work on that. If conditions changed, it happened earlier, and it was something else.
Could it be more use of masks or social distancing somehow applying stronger selective pressure for greater infectiousness? Seems like a stretch.
This was Trevor’s guess on the 14th, from later in the thread:
That’s plausible, but doesn’t explain why the chronic infections hadn’t done this earlier, and the English strain doesn’t escape immunity in this way (and we don’t know about the others) so I notice it doesn’t feel like it explains things.
There are more people getting infected now than before, so it could be having more viruses around to mutate, but this seems too sudden for that alone to explain things.
There are also more people who are immune, thus increasing selective pressure to escape from that (Stat News which seems high quality):
This makes sense as an escalating factor, but once again it does not seem like it could be escalating fast enough to explain the sudden phase shift. There are lots of places that were previously very infected, more infected than many of the places where the new strains are now emerging.
Perhaps what changed is largely our perception of what is scary? Which raises the question of whether we’re right to be terrified now, or were right before to mostly not be concerned?
Until the English strain, everyone was treating ‘there’s a new variant out there’ as nothing to be concerned about. Suddenly, every day there’s a new headline announcing another strain or travel restriction.
The new Brazillian strain is potentially terrifying. This scared the English so badly that they banned travel from not only fifteen countries in Latin America, but Portugal as well.
There are warnings that the Brazillian variant could have outright escaped not only the vaccine, but the immunity from previous infections. This would be very different from the English strain:
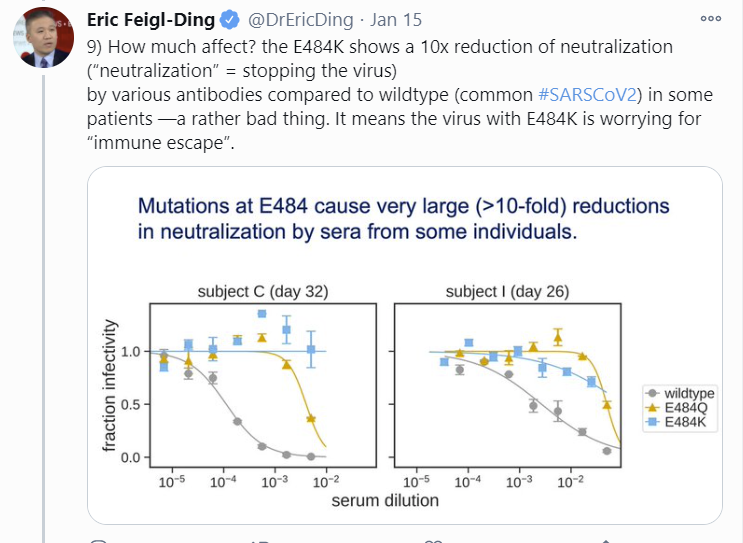
Supporting this is that areas of Brazil that were previously very hard hit, including Manaus with 75% seroprevalence, are being hit again. Now Eric Feigl-Ding says (in a long thread of good data) there are two Brazil variants but both can escape antibodies:
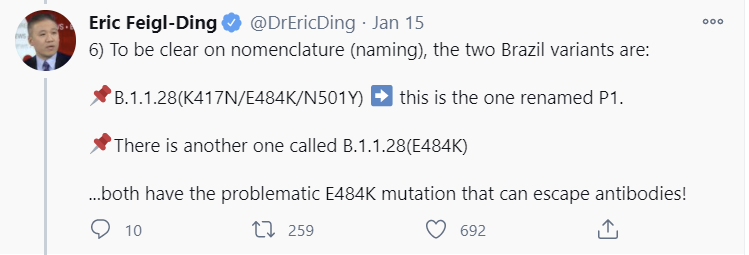
There’s no weasel ‘may’ in that claim, although I suppose ‘can’ still leaves room for a ‘mostly doesn’t.’
Under these circumstances, halting travel as a precautionary principle seems wise. Even if the probability of full escape remains low, the consequences are beyond dire. And as noted above, we should run the tests required to know the real situation.
There’s reports of a new strain in California, 452R:
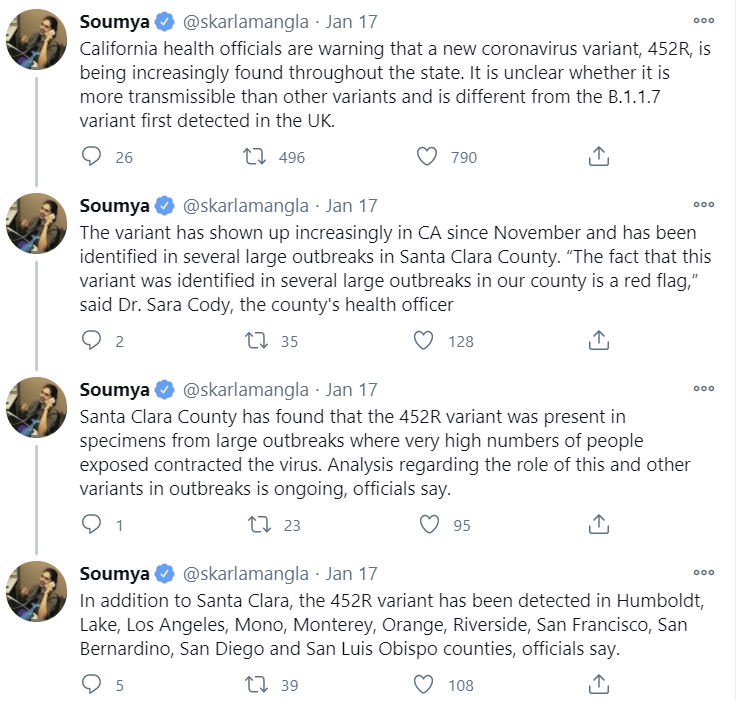
This feels like exactly the kind of thing that months ago would have been met with a giant shrug, a ‘mutations be mutating, what you gonna do’ and reminders of the importance of random factors, until more data shows up and we can run the necessary tests.
That’s especially true given this:

The problem is, California is rather large and has a lot of infections, and you need to explain this along with California having it especially bad right now:

Given that the strain was identified in Denmark in March, it seems unlikely that it could be that much more infectious, or we would already know. One case in California in May, doubling every week, would have fully infected the country if the control systems hadn’t kicked in at some point.
There’s also the standard ‘we don’t know if the vaccine works on this variant’ talk because this modifies the spike protein. So again, we need to run the tests, but it seems unlikely that there’s a problem. It’s not like California is doing much selecting for vaccine resistance.
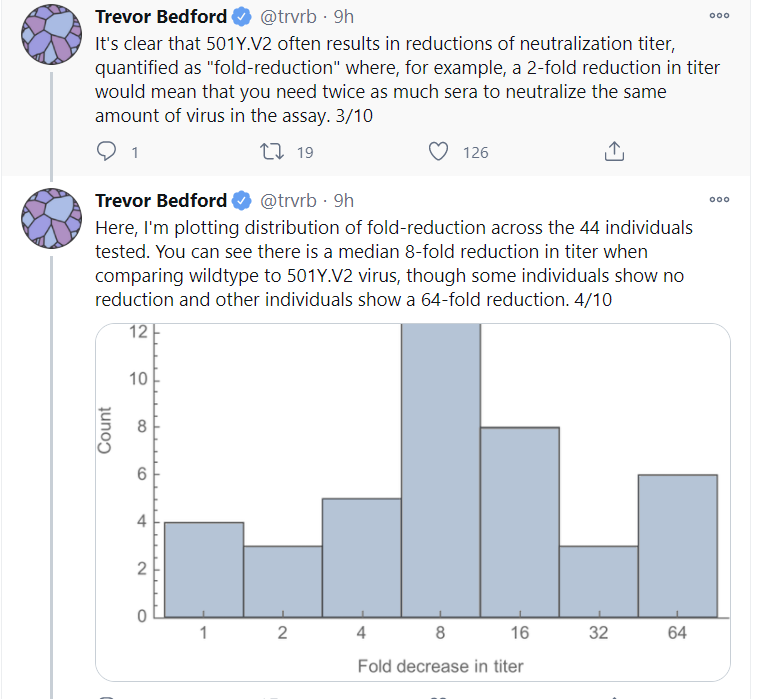
The really scary one, at this point, is the South African strain, because it looks a lot like it reduces neutralization capacity (study preprint), which likely means it can reinfect people. It’s worth quoting a lot of Trevor’s thread:
From what I’ve seen, the expectation is that the vaccine won’t work as well as before, but should still work, and could easily be updated if needed. This is from one of the authors:
As more people are vaccinated and more people have been infected, the selection pressure for strains that escape the vaccine and/or escape prior infection intensifies, and so does the danger of leaving more people only partially protected via vaccination. With the new strains, it is becoming less clear that it would be wise to delay second doses for too long. I’d still be very strongly in favor of not holding second doses in reserve but am becoming more receptive to the precautionary principle, which suggests that we might not want to let people wait around for many months. Either we have the vaccine capacity required to re-vaccinate, in which case we can afford to give everyone two doses, or we don’t, in which case we won’t be able to re-vaccinate quickly if we need to do that.
South Africa’s CDC has issued a rather dire warning:
That’s the kind of thing a CDC would be inclined to say in terms of behavioral prescriptions, whether it was appropriate or not. What’s important and terrifying is that there was so much loss of antibody effectiveness.
Of course, all of this only emphasizes how important it is now to increase capacity. If we spent a few billion to ramp up mRNA vaccine production capacity now, then by the time the South African strain becomes a problem, we’d have the ability to fix this via re-vaccination, and without effectively taking those doses away from the third world.
Also of course, we should have very strict travel restrictions around South Africa so we can slow the problem down long enough to get to that point.
But What Do We Do Now?
An interesting pivot seen this week is from ‘everyone wears a mask’ to ‘everyone wears an effective mask.’
Until this year, the battle to get people to even pick up a piece of cloth was so much trouble that there was little attempt to do more than that. Periodically we’d say that a surgical mask or N95 was better than a cloth mask, but the overwhelming agreement was to emphasize ‘mask at all.’ If you pressure people to choose better masks, it risks making people throw up their hands and not care at all.
Now a variety of sources have decided that this won’t cut it, slash certain forces are out of the picture, and we now need to step up our game and push for better masks.
I’m happy to get behind this attempt by the control system to stay on target. There is an abundance of high-quality masks available for sale on Amazon, and I was quickly able to find one that didn’t feel substantially more annoying than a cloth mask. So I encourage everyone who hasn’t yet done so to up their mask game.
Note that there is most definitely a More Dakka version of this where you get the fully effective $2,000 filtration systems going, and it’s overwhelmingly correct to just do that, if anyone actually does use them can you share your experiences?
What about we as in the new administration? This seems to be a list of day one actions:
So out of 23 things, 3 of them concern Covid, whereas 9 concern Racial Equity, one of which involves a fully written bill being sent to Congress. One of the 3 concerning Covid is to not leave the W.H.O. The second is a mask mandate for the places a president can issue a mask mandate, which is better than not doing it. The third is to establish a structure for future action. Arguably the two economic actions are also Covid-related.
This is better than doing actual nothing for months on end, but for now it’s also remarkably similar.
You’re Vaccinated, Now What?

Israel is seeing the impact and no that can’t be the lockdown:
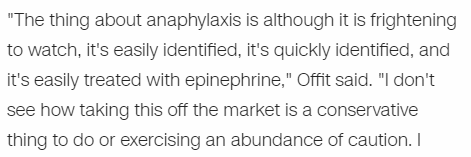
Yet, as was pointed out last week, many are telling the vaccinated they still have to engage in the same behaviors as everyone else, including avoiding indoor gatherings and maintaining social distancing. These Very Serious People are looking for any way to get people to take any precaution. The Sacrifices to the Gods must continue.
To prove this, they say there is “no evidence” that vaccines prevent transmission. Then if necessary they’ll retreat to “no proof” that they prevent transmission. Then they’ll retreat to the inner motte of “no proof that they entirely 100% prevent transmission.”
Of course they prevent transmission. Not 100%, we don’t know the exact percentage, but a lot.
A long term worry on this is that it will make people not want the vaccine, since what’s the point if you still can’t live your life. Then again, one could reasonably say if one were in the “lying to the American people for their own good” business, that’s a problem for Future America. Right now, there are more people who want the vaccine than there are vaccine doses. Which is true in all places that are open to those over 65. We can then turn around and tell other lies later, to solve those future problems, such people would say, and no we are not worried about our credibility, we are the authorized official sources and anyone who disagrees with us should be censored on social media.
I have exactly PoliMath’s position on masks after vaccination:
Here’s Nate Silver, who also occasionally does some math and also has some understanding of public messaging:
I intend to wear my mask after vaccination, if I can be vaccinated in time for that to matter, in order to reinforce mask norms. It’s easy to wear a mask. There’s even some tiny chance it might physically matter, and again, it’s easy to do. As opposed to continuing to do costly social distancing, and yeah, no.
This is the attempt to both be honest and split the needle:
This uses the weasel framing of “can” in the third claim, which is technically correct but is chosen to scare people. It is possible that this plane will crash, better drive instead.
Meanwhile, they call saying the vaccine prevents transmission “hiding the truth”:
The difference here is that this would be “hiding the truth” to say things are safe, which is not fine, as opposed to “hiding the truth” to say things are not safe, which is encouraged.
The one point of evidence potentially pointing the other way comes from Israel, where we’re getting some truly bizarre and troubling data about positive test rates for the recently vaccinated. I couldn’t locate the original study, so I’m going by the news report, if you can link to the study please do so in the comments.
Here’s my summary of key data points:
Tests up to 7 days after vaccination had a 5.4% positive rate. Vaccine shouldn’t be protecting them, so consider this a baseline, out of 100,000 tested.
Tests between days 8 and 14 had an 8.3% positive rate, which is super high, higher than baseline. Perhaps those who get vaccinated go out and have parties quickly? This is out of 67,000 tested.
Tests between days 15 and 21 still had a 7.2% positive rate. Still super high. This is out of 20,000 tested.
Tests between days 22 and 28 were 2.6% positive, including some people vaccinated twice, although the second dose hadn’t had much time to work. This is out of only 3,200 tested.
We don’t know how they determined when and whether to test people. If testing was only done when there was a reason, these numbers don’t worry me. If testing was done at random, then this is rather alarming. The declines in numbers of tests run could be because people are being vaccinated in real time, or because they were only testing people when it seemed necessary, and therefore as time went by they tested less people.
The 100,000 number is very suspiciously round, making me think that testing was randomized. Israel’s general positive test rate has been rising recently up to about 7%, so that seems like a stretch – testing at random should cause a lower positive rate than that, but perhaps they stopped collecting results after 100k of them? The rise in the second week makes sense if you think those 67,000 tests weren’t at random, or the timing could be weird as the situation was changing rapidly. In any case, without better data, hard to tell.
We know from elsewhere that there’s a lot of protection by day 10, but the positive test rates here did not decline much until substantially after that.
Without the original source, a lot of key information is lacking, so it’s hard to interpret the information we do have.
They did also show that antibody responses were robust:
Ideally I’d withhold analysis until I had a better understanding here, but we don’t have that luxury these days. In any case, it’s data that needs to be explained.
Yes, We Can Agree Andrew Cuomo Is The Worst
In good New York State news, the state continues to open and operate additional vaccination sites. The fifth was in SUNY Albany on the 15th. They’ll need to close or slow down soon due to lack of supply, but that’s the right problem to have.
Cuomo somehow managed to mangle the restrictions sufficiently that restaurants suing for the right to provide indoor dining won in court, so Cuomo is now largely giving up on the zone-based restrictions:
This is part of the general sudden pivot from ‘we must contain the virus’ to ‘we must save the economy’ that is happening in many places right now. The timing seems, shall we say, suspicious, but also a lot is changing quickly.
Cuomo will pay the legal action forward by threatening to sue the Biden Administration to get more vaccine doses:
The entire NYS budget is split in two, with Cuomo demanding Washington give him money or else, and saying ‘look what you’d make me do if I didn’t have the money.’
The entire system is a giant mess and puts seniors in an impossible position, although to be fair I’ve seen reports that this is mostly true in other places as well:
The Quest to Sell Out of Covid Vaccine
Good news, everyone. We’re much closer to successfully using all our doses than previously expected, because that reserve of vaccine that Secretary Azar claimed we’d be releasing? It never existed. There were no held back second doses, the government now claims, instead we had far fewer doses than we were led to believe:
The whole thread is wild. Despite the administration shipping out its entire reserve, Pfizer released a statement saying it has second doses on hand for everyone who needs them:
If the government now claims to not have a reserve, after previously claiming it was going to release that same reserve, but Pfizer claims that instead it has the reserve ready to go, what the hell is actually going on?
And it’s not only the feds, the states and Pfizer, potentially counties and cities could have their own reserves. New York City does!
It isn’t clear to me whether there was never any reserve of second doses on a mass scale, or if there was a reserve but it’s already gone, or there were two reserves of second doses sitting around idle and now one of them has been deployed, or even possibly if there were three or more distinct reserves of second doses because yes we really are that dumb, and it seems states are talking about distinct distributions of “their” first and second doses and took delivery in two sections, or something? Then combine that with city or county reserves.
I don’t think there were an average of two distinct reserves let alone three or more, but it’s so confusing I can’t rule anything out.
None of the potential answers cover us in glory.
The quest of then selling out what has been distributed goes better in some places than others.
Here’s one theory of what went wrong. (Link to WSJ)
New York City is now crossing over into the camp that has successfully sold out (while of course holding onto a complete reserve of second doses for everyone who got a first dose):
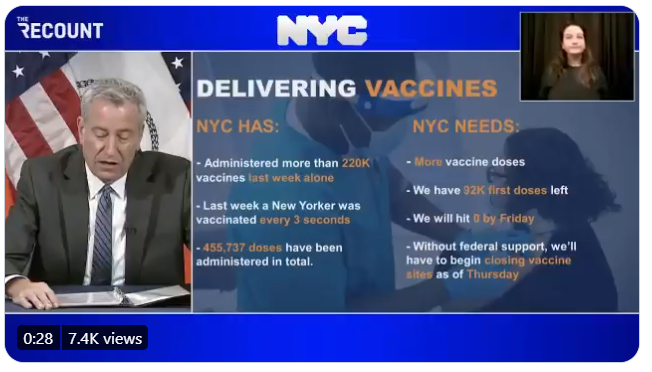
This in fact happened, and Thursday and Friday first dose appointments were cancelled en masse.
How are some places doing the rollout much faster than others? Here’s a CNN article about that, suggesting what matters is basic logistics and planning in advance, and an emphasis on speed. If you focus on allocation to where vaccine can be used, it gets used. Makes sense to me. I’d also add that such techniques require de-emphasizing prioritization, and not threatening people with huge penalties for giving the wrong person a vaccine shot.
If you don’t want to succeed, there are always plausible ways to not succeed. For example,
California has decided to not administer what seems to be hundreds of thousands of doses in a giant Moderna shipment, while they ‘investigate possible severe allergic reactions,’ all of which occurred at only one location, and while as far as I can see none of the other states that got the rest of that shipment (almost a million doses have been given out) either are halting use or reporting any concerns.

This seems like the latest variation on ‘make vulnerable elderly people sit together indoors in close quarters for observation after getting vaccinated, to monitor for extremely rare reactions, thus exposing them to infection right before they become immune.’
The new administration looks to be moving ahead as quickly as possible to distribute via pharmacies, which seems ideal, and also to use FEMA and the National Guard for distribution, which doesn’t seem like it should be necessary but given how things are going, sure, why not try throwing everything at the wall and seeing what sticks.
The math on selling out via pharmacies on their own seems rather strong:
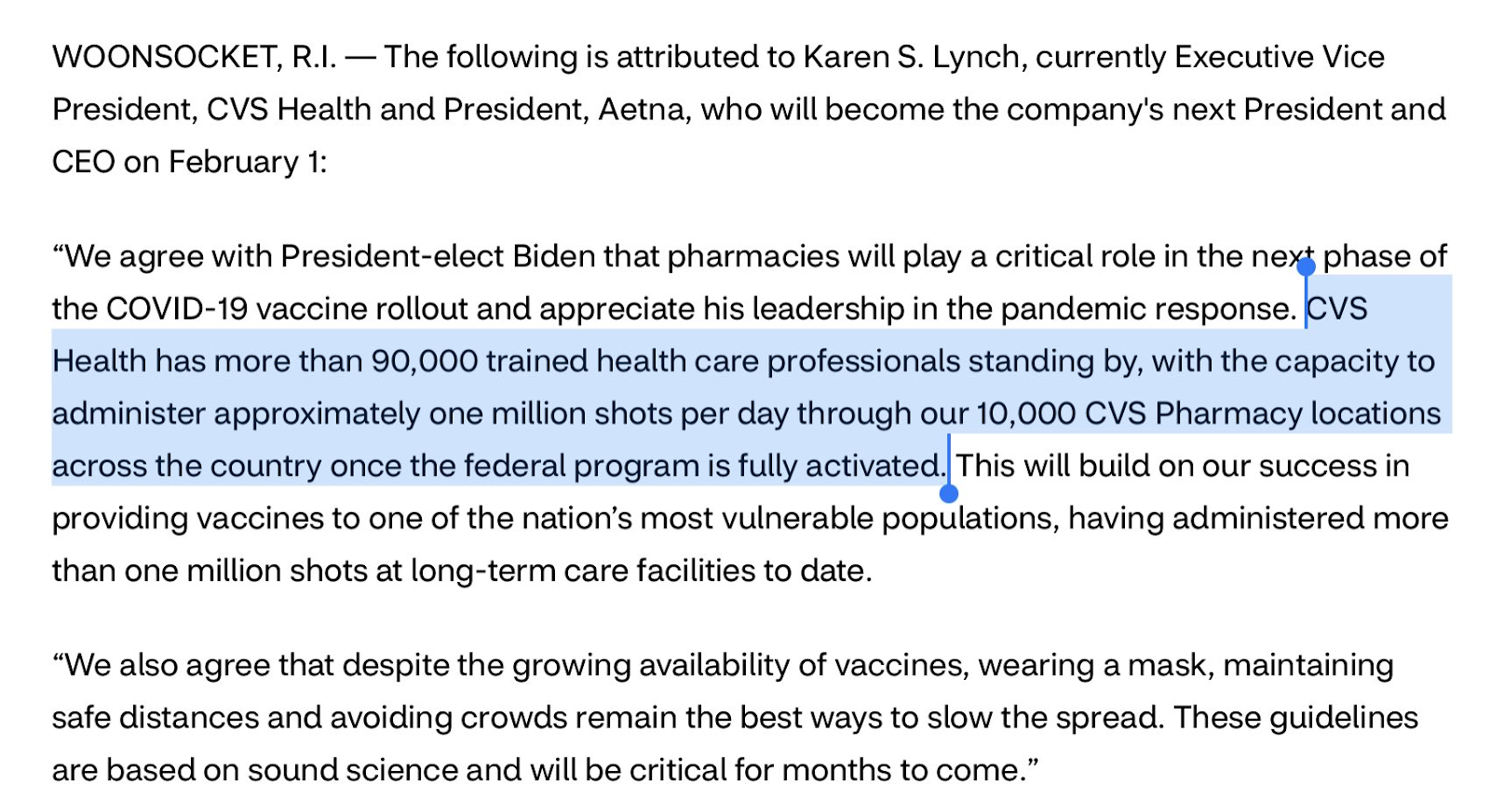
If CVS can do a million shots a day, that alone is the entire goal of Biden’s 100 million shots in 100 days.
CVS has less than 10,000 pharmacies in the United States, out of a total of about 88,000 pharmacies. That seems eminently doable, with the limiting factor being supply.
Here’s a thread on all the people who could put shots in arms now, if we had both shots and arms but needed professionals to bridge the gap. 752k practicing physicians, 3.1mm registered nurses, 125k physician’s assistants, 265k paramedics and EMTs, 322k pharmacists, 422k pharmacy technicians. Professionals simply are not the limiting factor. Full stop.
How is the experience trying to book an appointment for your elderly parents? It could be compared to trying to get concert tickets. We’ve gone over problems in New York, and it seems similar issues exist everywhere. Information is in different places, confusing and contradictory. Everything is booked, no one has supply, the people who want it make tons of calls and try lots of methods. That link has information by state, including links to everyone’s websites and phone numbers. Hopefully that can help.
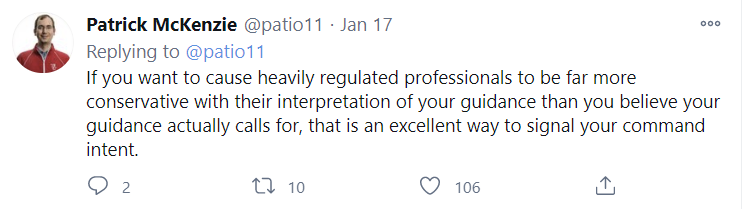
Vaccine Allocation By Politics and Power
Patrick McKenzie sums up what happens when you go around threatening anyone who disrupts the properly ethical priority order with personal ruin, as New York and California have done:
When you emphasize how bad it is to ‘jump the line’ you also get stories like this:
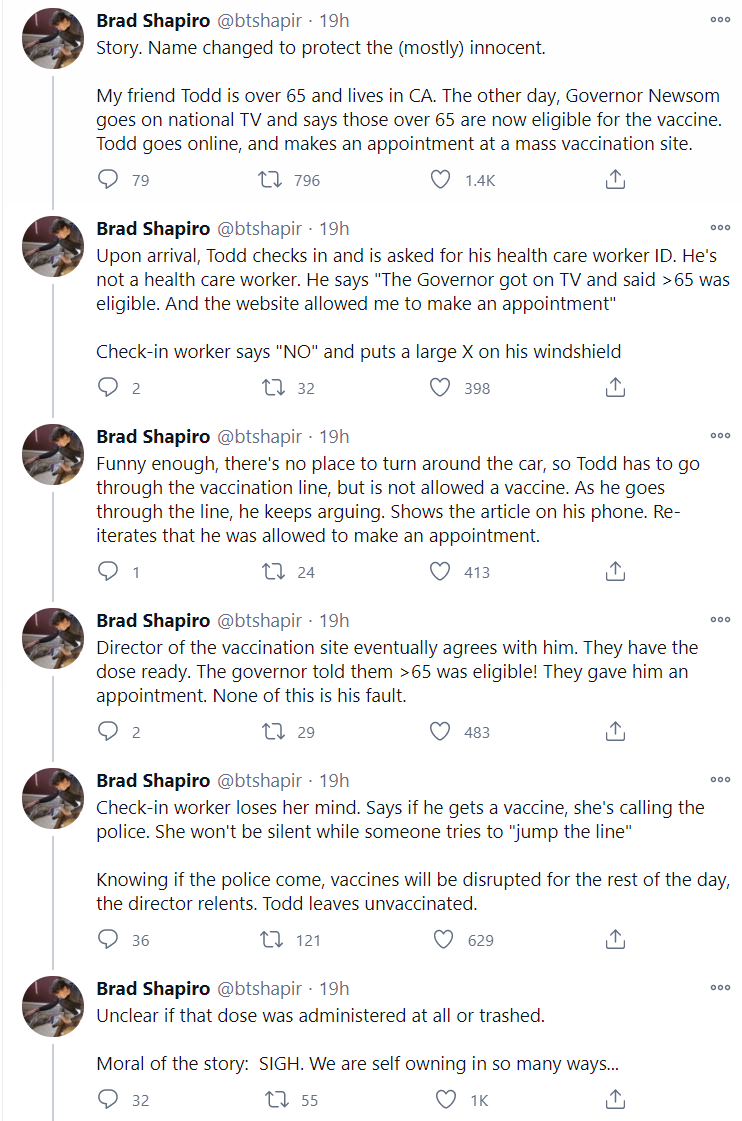
Or this, from of all places TMZ:
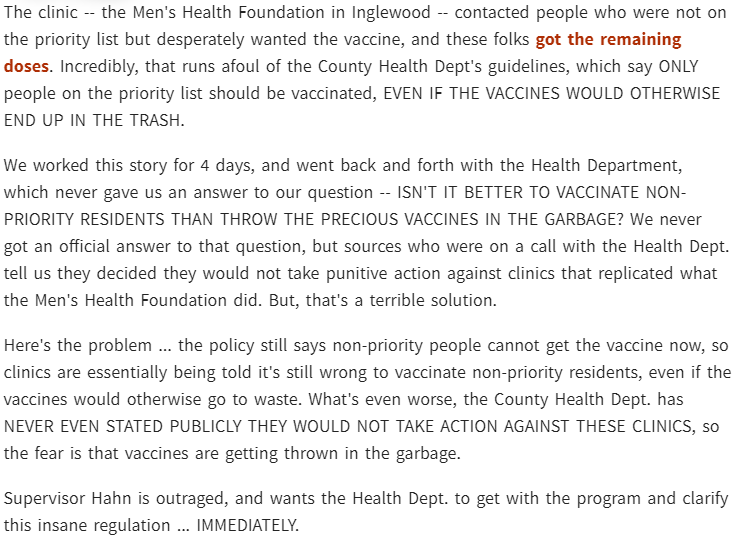
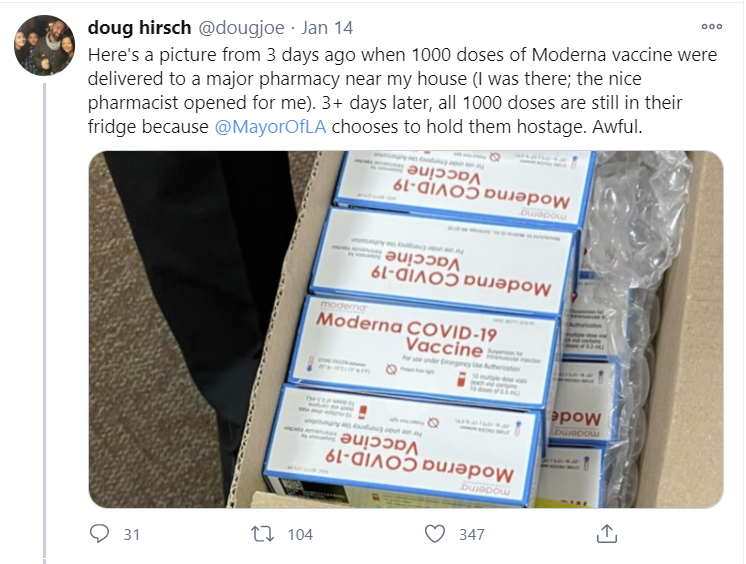
That’s also how you get outcomes like this via the LA Times:
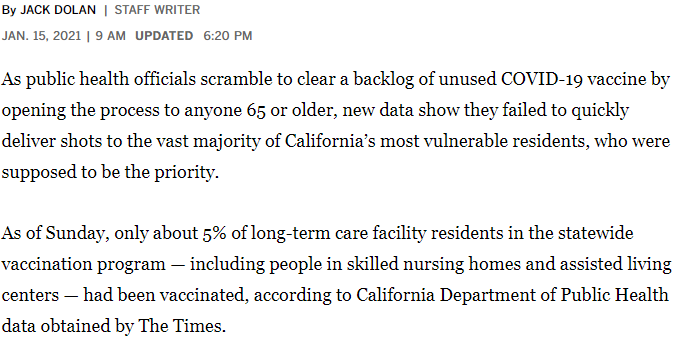
To summarize, emphasis on prioritization has led to large amounts of vaccine sitting around unused because people are waiting for ‘authorization’ to use it, to people blocking valid appointments at vaccination sites, and also to only 5% of the actual most vulnerable people, the group that is 1% of the population and over a third of the deaths, getting their shots a month into the campaign.
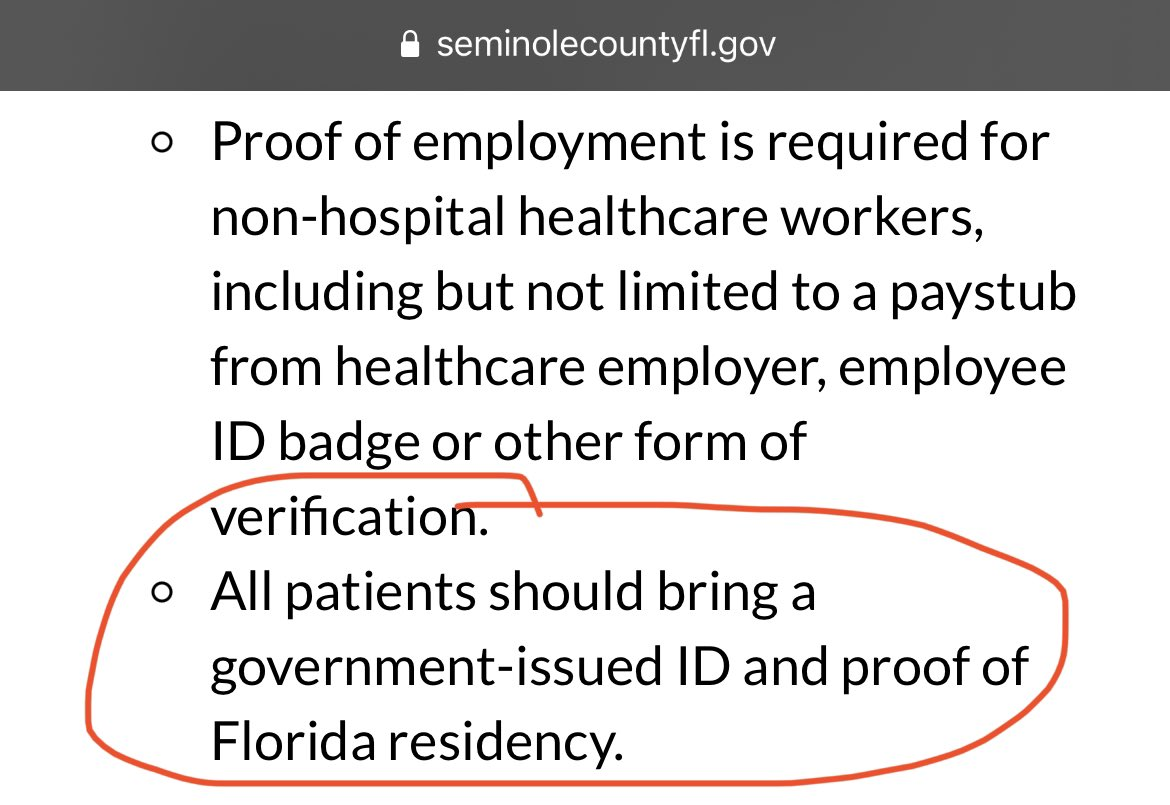
Meanwhile, in Florida, they’re requiring government ID and proof of residency to get vaccinated, to avoid accidentally giving doses to undocumented immigrents, or to people who noticed Florida was doing a decent distribution job and came down to get vaccinated. Nebraska is attempting to exclude immigrants as well. This will doubtless trip up numerous people, especially poor people, who lack or forget or are afraid of using proper documentation:
Meanwhile,in Wales (Twitter HT), they are delaying vaccinations so the curve of vaccination times is smoother for each individual vaccine type, no really they are literally doing that, what more do I have to say:
Prioritization by Lack of Virtue
What do politics and power reward and punish, in the end?
At some point, the system stops pretending it is rewarding virtue and punishing lack of virtue.
Then, at some point, the system stops pretending it is not punishing virtue, and starts punishing virtue and rewarding lack of virtue.
The official CDC recommended guidelines suggest prioritizing those with various ‘chronic conditions’ and include giving priority to smokers.
This is being followed in at least Alabama, Nevada, New Jersey, Mississippi and Washington D.C.
In other words: If you, on a regular basis, pay for and then consume poison, then that puts you at higher risk, so we will prioritize that you get life-changing and life-saving medicine before others who do not on a regular basis consume poison.
Every year, the poison in question kills more people, and costs more years of life, than Covid-19 was responsible for in 2020. It is highly plausible that, should this guideline be followed, smoking would gain status, people would have a new excuse for their smoking or not quitting, and this act alone could result in sufficiently more smoking to be a bigger health cost than the entire Covid-19 pandemic.
I expect that, for the rest of time, anyone who wants to justify smoking, or not having a healthy weight, or any other issue they don’t want to deal with, will often pull out “hey, at least it’ll get me priority health care!”
In addition, did you know you can just lie about this? It’s not as if they check in any way whatsoever. So…

In addition, there’s the question of whether you are sufficiently shameless to use the fact that you smoke to step in line ahead of an elderly person who is at actual risk in a way that has nothing to do with their life choices. So in that sense they are prioritizing the selfish and shameless.
Most of all, they are prioritizing liars.
You don’t even have to say what you’re lying about! In DC you can simply say you have one of the conditions, never mind which one, and get vaccinated at age 17:

Here’s the actual prioritization scheme they’re about to have in Washington, DC, then:
Would you like a vaccine? If so, check this box.
At that point, what are the ethics of checking that box? Should this kind of rule be respected?
Do you think people will respect such a rule? What will that do to their respect for such rules in general?
Once you add obesity as a chronic condition, everybody knows that the dice are loaded, the system’s sole purpose is to punish he honest and honorable, and we’d wish there was no prioritization at all:
Note that starting at 25 not only includes the majority of people, thus making sure that the elderly can’t get vaccinated any time soon, it also doesn’t make physical sense at all even if you buy the supposed premise of people being at higher risk:

This is the ultimate result of allocation by politics and power. Those who learn to work the system, to invest their resources in such games, to be comfortable using special rules and appropriating from others, get the scarce resources.
Those who play by ‘the rules’ and do ‘what is fair’ are left out in the cold. If you did what the Responsible Authority Figures said to do, you’re now behind most other people and will have to spend additional months of your life hiding at home while those who smoke or are overweight or just decided to lie about it frolic around town like it is nothing.
So let’s be clear. If you don’t want to have priority, you can just… not have priority. Allocate by willingness to make phone calls or stand in lines or reload web pages. Find out who is willing to destroy more real resources.
You could also allocate by willingness to pay more real resources rather than destroy more real resources, but whenever I talk about the only known good way to allocate scarce resources people get into demon threads complaining about how that is Just Awful, so once again I’m not going to suggest that.
I strongly suspect (and hope) that there will be a lot of vaccination sites that are told that this is the priority list, but if you call them and say you’re eligible because you are a smoker or have a BMI of 27, suddenly there won’t be any appointments available and you’ll be put on a waiting list and never called back.
Luckily, it seems the majority of states realize what these CDC guidelines imply, and are mostly disregarding them.
I considered not writing this section to avoid highlighting the issue, because highlighting the issue risks accelerating the negative consequences involved, and it didn’t seem like anyone was noticing this. Then Nate mentioned it, and I wrote the section.
On reflection, I shouldn’t have hesitated.
This is not a small effect. This could easily, where adopted, delay an honest and honorable person’s vaccine access by several months.
Not mentioning destructive behaviors because the noticing of such behaviors creates destruction is a horrible, horrible incentive that leads to harmful crimes being continuously covered up and rewarded. If one sees something, one must say something. If the law is unjust, one should not keep quiet about that out of fear that more others will then notice the law is unjust and might take advantage of it.
The silver lining of such policies is they absolutely create enough eligible arms in which to put all the shots. This is systematic injustice for injustice’s sake, but at least it does get shots into arms.
Useful Resources
VaccinateCA is a project that calls hospitals and pharmacies in California daily, and checks which are currently administering vaccines. I heard about it from several sources, originating with Patrick McKenzie.
Here’s how necessary that project is from another angle:


Here’s a similar project in Massachusetts.
Here’s a similar project in Texas.
Here’s the start of something similar for New York City.
If you’d like to direct few-questions-asked funding to a similar operation to VaccinateCA in another state, I know someone looking to do that, and I’m happy to direct you to that person if you contact me via email, Twitter DM or LessWrong PM.
Or, if you know about existing similar places for other states, share in the comments, and I’ll include in future updates.
This CNN article linked above has some useful phone numbers and websites to try.
Note that different locations have decided to use different standards for who they will vaccinate. Some are allowing anyone 65+, others are only allowing 75+. Of interest to many readers, Alameda County’s three cites are all (as of writing this section on Tuesday) only doing 75+. Other areas are place after place with no supply.
To get an appointment in New York State from the state’s facilities (as opposed to other places, or using NYC’s system) you are officially asked to start here. It looks like some upstate places have appointments available. It’s up to you to decide how far you’re willing to travel. My answer would be quite far.
If you’re looking in NYC you could try starting here or look here but I expect best answers to change. There is also now the NYC vaccine list above.
How Bad is it Out There Right Now?
It’s so bad that the states are starting to turn to actual logistics experts. No, not Amazon. Starbucks!
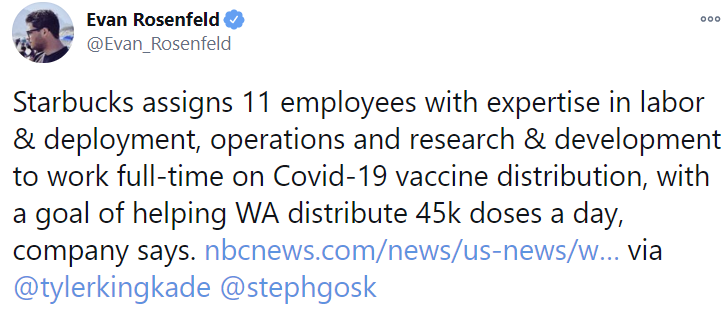
To be clear, I do not say this to mock. This is a very very good development. Let the experts do what they do best.
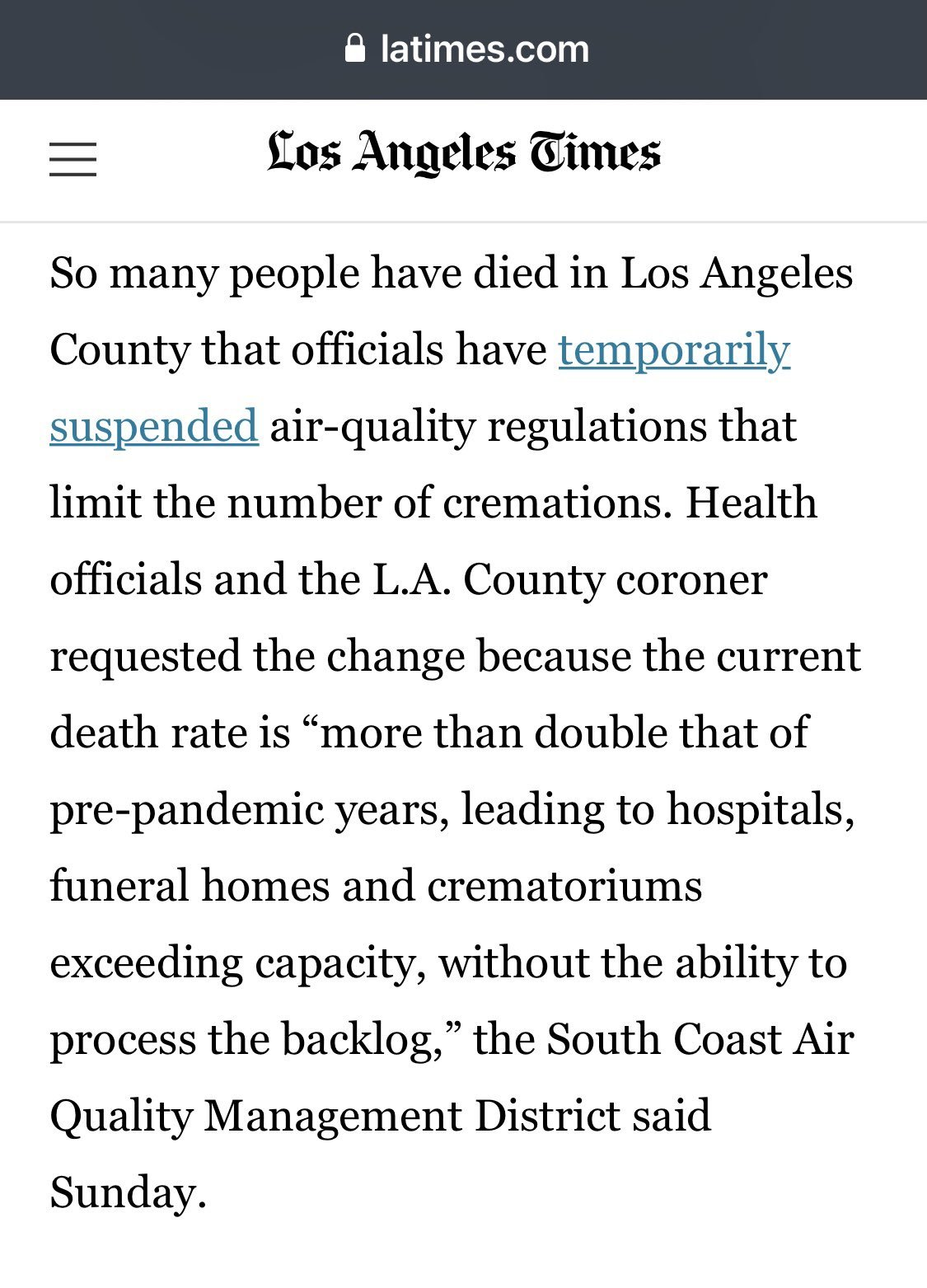
Meanwhile, in Los Angeles, we have moved on from leaving people to die without transporting them to hospitals, to then having to temporarily suspend air-quality regulations in order to cremate them when they die:
You Should Know This Already
There are extra vaccine doses in the vials, but you can only fully extract them with a low dead space syringe and we are not reliably using such syringes, wasting a substantial percentage of all potential vaccine doses. This could plausibly be a much bigger loss than throwing unused doses away at day’s end.
Once again, do not throw doses in the garbage. In an important sense this is the most important thing to care about, for most people, on the margin. Of course, the hospital gets attacked for breaking with ‘priority’ and also roasted alive for wasting doses, meaning that they keep everything quiet and destroy all records of what happened. The key is to choose the side to be on in the dark.
Matt Yglesias makes the case for vaccine challenge trials. He makes a strong and clear case, which is admittedly easier when something is overwhelmingly obviously correct. In any case, additional voices on this are always welcome.
Mentioned from another source above, but reminder: Israeli study on Pfizer vaccine sees 100 of 102 develop significant antibodies, editor says participants likely won’t spread virus further.
Periodic reminder: Pay for something and you get more of it, well, maybe, but yeah, you do: Utilization of the United Kingdom’s Covid subsidies by region correlates to cases of Covid (pdf).
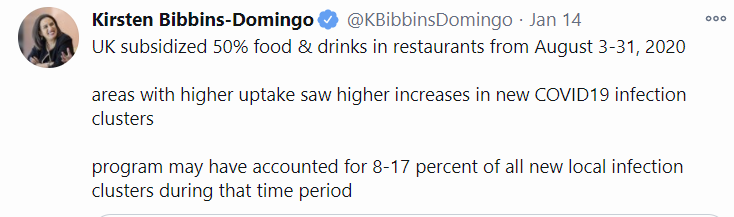
(Not the biggest concern these days, but can we stop using the word ‘may’ and then providing a range? Studies show I may have between 2 and 17 burgers for lunch next Tuesday.)
The program details were even worse than you know:

This is, shall we say, most definitely not how any of this works (via MR) and explaining why would only insult your intelligence:
Your periodic entirely correct rant that we should consider allocating scarce resources by price rather than by politics and power, and letting people do the things they want to do to stop the pandemic because that would actually work, from The Grumpy Economist John Cochrane.
Europe has been informed that it will get fewer vaccine doses from Pfizer than expected for a while, so that they can upgrade their factory and produce more doses in the future. That’s an excellent reason to temporarily produce fewer doses, given you are in a world where there’s no better way to increase production capacity that you already implemented months ago for trivial amounts of money. It seems that Europe negotiated a lower price point in exchange for going to the back of the line, so now they’re going to the back of the line.
The Very Serious People will always criticize anyone who does not defer to the Very Serious People, even when they are obviously wrong, as we are reminded this week by two old Guardian links from Marginal Revolution.
First, the Very Serious People declared that since Brexit was in defiance of them and their dictates, that bad things must follow, so they declared pulling out of the European Medicines Agency would slow down the UK’s vaccine rollout. Because, somehow, the union that spends all day telling people what they cannot do and how exactly they must do everything that is still done, and being unable to make any decisions, would obviously get the vaccine first. By implication it is unforgivable therefore to leave since that will deny your people the vaccine. Instead you should participate in the EU’s plan to… negotiate a lower price in exchange for going to the back of the line.
Then in July, when the United Kingdom decided not to take part in the European Union’s plan of paying less for vaccines in exchange for going to the back of the line while putting lots of regulatory hurdles in place, that was called ‘unforgivable’ because it would ‘set the UK up as a competitor’ and because the UK might decide to secure more doses rather than less doses:

What is morally unforgivable to the Very Serious People? Not going along with their schemes (the title of the Guardian article actually calls it a “scheme” by name) and deciding instead to attempt to create better outcomes rather than worse outcomes, instead of their explicit calls to aim for worse outcomes rather than better outcomes. No wonder, for example, that every single super-rich person was terrified to be seen actually helping. I know it’s easy to not see such statements but perhaps consider that they could be literally true?
Your periodic reminder that people are crazy and the world is mad and none of the rules make about children make any sense:
In Other News
With the new administration, the CDC will now review all of its guidance on everything:
There are two recent studies out about immunity to Covid coming from past infection. My analysis of those studies is available in its own post rather than as part of this post, so it is easy to link to.
Israel had already secured vaccines in part by promising to provide good data in return. Now it seems they’ve struck another data-for-vaccine deal. For everyone who says there are no more doses to be had, it’s gotta be odd that more doses keep being had.
Meanwhile the W.H.O. thinks that countries and companies should stop making deals entirely, so they can direct all the vaccine shots wherever they think is best. Anyone who disagrees with this, they declare, is deeply unethical. How dare people with money pay for things to be created, and then take delivery of those things! The horror. Yes, that logic has other implications. Remember to be consistent.
Could it be happening? Please?
If the attack on the plan is ‘how dare this not have happened sooner’ then that’s perfect, let’s do it now and yell at each other about how awful and political the timing was, come on, everyone, we can do this:
You know who isn’t wasting doses or time? The Department of Corrections!
PoliMath assumes this is a data error, but my presumption is that this is no error. There are extra doses in each vial, so it’s perfectly reasonable to get a few percent more shots in then there were doses allocated to you. That should be the standard by which one is judged.
Via MR, this long detailed post goes over the mRNA vaccine supply chain. Most of the steps, while non-trivial in an important sense, seem straightforward to scale as far as we’d need to scale them, including making the mRNA itself. It’s known tech.
The limiting factor seems, according to this article, to be Lipid Nanoparticle (LNP) production. I don’t know anything about that process beyond what is seen here, so I don’t know how much that could be scaled or at what cost. There weren’t any indications we were punching anywhere near the limits of what could be done.
Studies suggest saliva tests are as accurate as swab tests while being cheaper and easier to use (synthetic review 1, review 2).
It is almost certainly safe to be vaccinated while breastfeeding.
Marginal Revolution links to a Reason interview of Alex Tabarrok on First Doses First.
Claim that NSAIDs dampen immune response to Covid in mice.
This seems like a good method of explaining how to stay safe:
For Those Who Actively Want to Give Me Money
An increasing number of people have asked about giving me money, to show appreciation for these posts and the work required to create them. You really really don’t have to do this! I don’t need the money! I don’t do this for money, I have a day job and I don’t need to worry about money any time soon.
But if you choose to contribute, I believe this would be motivating rather than demotivating, and you have my thanks.
If you wish to do this on a small scale, I have set up a Patreon for the blog as a means to do that. There won’t be any rewards beyond things like ‘I am happy and motivated, and I respond more to your comments.’ There won’t be any locked posts.
If you want to give enough that the fees involved in Patreon are worth avoiding, you can PM me on LessWrong or DM me on Twitter, or email me, and I’ll provide details for PayPal or the relevant crypto address.
Once again, please do not consider yourself under any obligation whatsoever to do this. It brings me joy that others are finding these updates useful, and ideally spreading the word about them and putting the information and ideas into practice, and that we are building better models of the world together. That’s what is important.
Until next week.
41 comments
Comments sorted by top scores.
comment by mingyuan · 2021-01-21T20:04:52.176Z · LW(p) · GW(p)
My house has been calling and driving around CA for the past few days to try to get information, and I find it really disheartening. I'm not sure a single site we visited (and there have been 30+ at this point) had even vaccinated all of its healthcare workers. All government-run sites are closed on weekends and holidays, and no sites of any kind were open other than during normal business hours (at most 12 hours a day, often more like 8 hours). We ran into an old man at a closed site who hadn't been able to get any kind of information from the vaccination site, and watched another old man do 30 full minutes of paperwork before getting his shot. Some of the older/wiser people in my house aren't as depressed as I am after each excursion, because they say they already knew the world was inadequate, and this isn't an update. Doesn't mean it's not a fucking disaster.
My mom is a teacher and 64, but since she's not a K-12 teacher and is younger than 65, she's in Tier 5 along with healthy 16-year-olds. Fuck that. She lives in Wisconsin, for which I have been completely unable to find any information on how a person might get vaccinated. (Let me know if you have info, please.)
Meanwhile in Arizona, a friend's grandma got vaccinated at 2:24 AM, because they're open 24/7 like some kind of sane people.
tl;dr everything is terrible and the faith in humanity I felt as a child is but a dim memory as my heart and soul are ground into the dust and shat on
Replies from: MondSemmel↑ comment by MondSemmel · 2021-01-22T08:43:33.152Z · LW(p) · GW(p)
Have you seen VaccinateCA, a volunteer effort that hopes to help CA citizens make sense of the mess in that state?
Replies from: mingyuancomment by Rob Bensinger (RobbBB) · 2021-01-25T04:34:10.118Z · LW(p) · GW(p)
I've put Zvi's COVID posts in a sequence, so they're easier to browse and link to: https://www.lesswrong.com/s/rencyawwfr4rfwt5C [? · GW]
comment by noggin-scratcher · 2021-01-21T19:04:39.751Z · LW(p) · GW(p)
(the title of the Guardian article actually calls it a “scheme” by name)
The word "scheme" doesn't have quite the same negative connotations in the UK as I gather it does in the US. Government (or otherwise large-scale) programs and projects being described as "schemes" is fairly common.
Describing a person as "scheming" carries the association of being devious and underhand, but somehow not so much for big organisations.
Replies from: Zvi↑ comment by Zvi · 2021-01-21T19:11:07.336Z · LW(p) · GW(p)
Interesting. Thank you for the note, in America that would definitely have had big negative connotations. So when they say scheme is it closer to our 'plan'?
Replies from: johnlawrenceaspden, noggin-scratcher↑ comment by johnlawrenceaspden · 2021-01-23T20:28:45.262Z · LW(p) · GW(p)
Am British, confirm.
↑ comment by noggin-scratcher · 2021-01-21T19:38:56.570Z · LW(p) · GW(p)
Yes, plan would be similar.
comment by MondSemmel · 2021-01-21T23:19:33.199Z · LW(p) · GW(p)
It's amazing how many problems were caused by using a political rather than monetary prioritisation scheme for the scarce vaccines.
Lots of head-meets-wall moments this week. Like every week. My "favorite" as an EU citizen was the EU criticizing the UK for trying to secure more than way-too-few vaccines. The notion that an entire first-world continent somehow failed so epically in one of the single most important challenges of 2020 (namely, securing enough vaccine) indicates that our leaders somehow weren't living anywhere close to reality.
And that no leaders worldwide thought of any non-zero-sum solutions to the problem (like paying to increase vaccine production capacity) does not bode well for our ability to solve more difficult coordination problems.
comment by Douglas_Knight · 2021-01-21T21:02:33.755Z · LW(p) · GW(p)
My (highly speculative!) hypothesis is that the emergence of these variant viruses arises in cases of chronic infection during which the immune system places great pressure on the virus to escape immunity and the virus does so by getting really good at getting into cells. 11/19
That’s plausible, but doesn’t explain why the chronic infections hadn’t done this earlier, and the English strain doesn’t escape immunity in this way (and we don’t know about the others) so I notice it doesn’t feel like it explains things.
That isn't plausible to me. Not only does it not explain everything, I don't think it explains anything. There are two traits, immune escape and infectiousness, which is pretty much the same as fitness. It makes sense that chronic infection causes immune escape, but we aren't looking at immune escape. There might be tons of strains with immune escape out there, but we won't notice until we achieve substantial herd immunity, at which point they will have increased fitness. If that happens, and we need to explain immune escape in future strains, then this is a possibility. But I see no reason to believe it about these strains. We are filtering by increased fitness, so we need to explain increased fitness. Immune escape is probably a side effect of increased fitness, because it's a potential side effect of any change.
Fitness is fitness. There is no need for a weird environment to explain selection for fitness, because it's the main story. In fact, this is exactly backwards. If there is any trade-off between reproduction between hosts and reproduction in hosts, then selection by chronic infection will favor the latter at the expense of the former and probably move away from optimal fitness. Whereas it appears, as Bedford claims, that these mutations are a free lunch. This is quite plausible for a young parasite that hasn't finished adapting to its new host. But then what does a weird selection pressure explain? Every infection should be an opportunity to develop this. What matters is the number of roughly the number of virus-host-days. A virus trapped in one individual for 100 days is under roughly the same selection pressure as a virus passing through 20 individuals under the same time. I've seen a lot of people call that "fast evolution" because 20x as much selection happens in the host, but it's not any faster in time.
Bedford seems to allude to this view, but he also uses similar points to make a different argument, which is that the UK variant appeared out of nowhere with a lot of mutations, without the intermediate forms being observed. Arising from a chronic infection would explain this. But we also know that all the mutations have arisen before, without seeming to do much on their own. So we know that it only took off when it reached the magic combination, which explains why we didn't see the intermediate forms. I don't think chronic infection adds much to this, although I could imagine a scenario in which the individual changes happen to be selected for in chronic infection at the slight expense of general fitness. So it needs the different landscape of a chronic infection to cross the valley and reach the final form. But this seems like excess detail to me.
Replies from: Zvi↑ comment by Zvi · 2021-01-21T22:27:36.610Z · LW(p) · GW(p)
All makes sense, but I would note that if a strain had escaped sufficiently to fully reinfect, that would be a huge advantage already, 20%+ of the population has already been infected including most of those taking them most risks.
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2021-01-22T04:37:45.824Z · LW(p) · GW(p)
Dynamically, that predicts that the advantage would rise over time, as a substantial proportion of the population got infected by the original strain. I think we've been monitoring the UK variant enough to see that this is not a large portion of its advantage.
Even statically, I think it's difficult to make the numbers work out. The idea that the population has heterogeneous risk makes a lot of sense, but it doesn't seem born out by the basic prediction that HIT is much lower than predicted by initial R. I suppose the control system might make it hard to observe how close we are getting to HIT, but I'm skeptical. And you need zero cross-immunity. But then wouldn't the observed reinfections skyrocket and be obvious? Maybe if the reinfections are asymptomatic, but just as contagious. I guess that this very specific scenario predicts that the new variant has passed through the riskiest portion of the London population and no longer has an advantage there.
comment by Rasmus Faber-Espensen (rasmus-faber-espensen) · 2021-01-21T20:59:30.077Z · LW(p) · GW(p)
Denmark's SSI is now estimating the relative reproduction number for B.1.1.7 to 1.36. Since Denmark now has R=0.6 with the current restrictions, this should mean that B.1.1.7 infections here is currently falling.
In less good news: Denmark was from the beginning extracting 6-7 doses per vial of the Pfizer/BioNTech vaccine, sensibly ignoring EMA's guidelines only permitting 5 doses per vial. The Danish plan for vaccinations thus took the extra doses into account. But Pfizer has now informed Denmark that since they are extracting extra doses from the vials, they will reduce the deliveries accordingly (since the contracts specified number of doses and not vials), thus forcing Denmark to make a new slower plan.
As for that plan, I can't help getting a bit worried when I see the jump in expected weekly vaccine deliveries jump from 85,000 in week 13, the last week with confirmed deliveries, to 750,000 in week 14, the first week with only forecasts.
Replies from: Zvi, rasmus-faber-espensen↑ comment by Zvi · 2021-01-21T22:29:08.599Z · LW(p) · GW(p)
Wow, Pfizer actively punishing countries for extracting extra doses is one even I didn't see coming.
Replies from: rasmus-faber-espensen↑ comment by Rasmus Faber-Espensen (rasmus-faber-espensen) · 2021-01-21T22:34:54.473Z · LW(p) · GW(p)
To be fair, Pfizer has reduced deliveries to all countries that follow EMA guidelines, even those that haven't been able to consistently extract 6 doses per vial. I guess they are just hard-pressed to deliver the vaccines they have promised, and are thus seizing this as an excuse to reduce the deliveries.
↑ comment by Rasmus Faber-Espensen (rasmus-faber-espensen) · 2021-01-26T19:33:15.105Z · LW(p) · GW(p)
The newest report estimates the reproduction number (R) for all types of Covid-19 in Denmark to 0.64 (95% CI [0.56 ; 0.73]) and for B.1.1.7 to 1.07 (95% CI [0.83 ; 1.32]). This translates to a relative reproduction number of 1.67. B.1.1.7 is now 12.1% of tested samples. It looks like it will dominate in 3-4 weeks at which point we should expect infections to start rising again.
The report also contains some interesting details about how they estimate the reproduction numbers (rolling poisson regression with beta correction).
comment by billzito · 2021-01-28T00:04:58.751Z · LW(p) · GW(p)
Was your prediction that cases would go down and then up also for the UK in addition to the US? I thought the new strain prevalence was already pretty high in parts of England according to the pre-print, so it seems like cases going down by a lot there is a big update towards the pre-print potentially being wrong? The UK's last wave doesn't look naively out of distribution compared to e.g. Spain and the U.S.
[To clarify: I think this was worded somewhat incorrectly -- I didn't update much on the probability of the pre-print being wrong, but I did update significantly on the implications of the higher transmissibility.]
Replies from: Zvicomment by habryka (habryka4) · 2021-01-21T19:28:39.684Z · LW(p) · GW(p)
Mod note: this is frontpaged, which is an exception to our usual rules. See here for explanation [LW(p) · GW(p)].
Replies from: Pongo, Chris_Leong↑ comment by Chris_Leong · 2021-01-23T07:46:27.682Z · LW(p) · GW(p)
Will all comments by you be green or just a special class of mod comments?
Replies from: Raemoncomment by bardstale · 2021-01-22T13:26:15.533Z · LW(p) · GW(p)
I intend to wear my mask after vaccination, if I can be vaccinated in time for that to matter, in order to reinforce mask norms. It’s easy to wear a mask. There’s even some tiny chance it might physically matter, and again, it’s easy to do. As opposed to continuing to do costly social distancing, and yeah, no.
Wearing a mask after vaccination would reduce the spread of other diseases such as the flu, thus freeing additional healthcare resources for COVID-19 patients.
comment by MalcolmOcean (malcolmocean) · 2021-01-26T11:29:51.447Z · LW(p) · GW(p)
🇨🇦 People liked my Canada update last week [LW(p) · GW(p)], so here's another one. I thought I wouldn't have much to say but apparently I wrote some stuff!
I made it its own post for better linkability. I'm honestly not sure if that's better, but that's what I did.
Covid Canada Jan25: low & slow [LW · GW]
comment by TheMajor · 2021-01-22T10:23:06.839Z · LW(p) · GW(p)
It was pointed out to me that it is really not accurate to consider the UK daily COVID numbers as a single data-point. There could be any number of possible explanations for the decrease in the numbers. Some possible explanations include:
- The current lockdown and measures are sufficient to bring the English variant to R<1.
- The current measures bring the English variant to an R slightly above 1, and the wild variants to R well below 1, and because nationally the English variant is not dominant yet (even though it is in certain regions) this gives a national R<1.
- The English strain has spread so aggressively regionally that group immunity effects in the London area have significantly slowed the spread, while not spreading as quickly geographically.
Most notably, hypotheses 2 & 3 predict that the stagnation will soon reverse back into acceleration (with hypothesis 3 predicting a far higher rate than 2), as the English variant becomes more prevalent throughout the rest of the UK. Let's hope the answer is door number 1?
comment by Matt Goldenberg (mr-hire) · 2021-01-21T23:49:48.578Z · LW(p) · GW(p)
The whole section assuming the vaccine rollout should be based on reward and punishment seems bizarre to me and the product of a horrifying world view.
The vaccine rollout should be based on saving lives not on reward and punishment. Of course, the current rollout is neither but substituting a scheme that "rewards virtuous people" would be evil in the deepest sense of the word.
Replies from: Zvi↑ comment by Zvi · 2021-01-22T00:46:06.042Z · LW(p) · GW(p)
I was observing what happens when you allocate via politics, rather than endorsing the opposite solution, which isn't being proposed by anyone that I can see. I was not suggesting we should reward virtuous people over non-virtuous people. Rather, I was pointing out that the current system systematically rewards non-virtuous people with life saving medicine, at the expense of virtuous people, using the criteria of non-virtue. If "are you willing to lie?" is the test one must pass to get vaccine, that seems like it should be highlighted, and that it is not a good policy.
Centrally, I was pointing out (and to) the implications and consequences of doing that. I was not suggesting reversed stupidity - e.g. I would not support withholding vaccine from the people in question.
I think I have made my first best solution very clear, and also have made my second best realistic suggestion (age bands only) also very clear.
I commit to saying no more on the subject of this section, since it has major demon thread potential.
Replies from: mr-hire↑ comment by Matt Goldenberg (mr-hire) · 2021-01-22T01:06:50.546Z · LW(p) · GW(p)
Hmm, it wasn't clear to me from that section what you were suggestion. I tend to skim these posts and find areas that are relevant because they're very long, so if you talk about it in a different part I suppose I have egg on my face here.
comment by alkjash · 2021-01-21T22:28:19.790Z · LW(p) · GW(p)
re: why are there more scary new strains now:
Have people have already accounted for the fact that the more virus there is in the world, the more likely it is for one of these viruses to mutate? If there's 5x as many cases of covid floating around right now than in September, a strain as bad as the UK strain will emerge 5x as quickly in expectation.
Replies from: alkjash↑ comment by alkjash · 2021-01-21T23:16:22.499Z · LW(p) · GW(p)
Adding onto this a little, here's a toy model of viral genetic diversity based on my high-school level biology.
Suppose the virus' DNA starts out as 000 (instead of ACTG for simplicity), and it needs to mutate into 111 to become stronger. Each individual reproduction event has some small probability p of flipping one of these bits. Some bit flips cause the virus to fail to function altogether, while others have no or negligible effect on the virus. As time goes on, the number of reproduction events starting from a given bitstring grows exponentially, so the likelihood of getting one more 1 grows exponentially as well. However, each time you jump from 000 to 100, it's not as if all other copies of 000 turn into 100, so making the next jump takes a while of waiting on lots of copies of 100 to happen. And then some 101 appears, and there's no jump for a while again as that strain populates.
The upshot is that you imagine the viral population to be "filling out the Hamming cube" one bitflip at a time and the weight of each bitstring is the total number of viruses with that code, and a genuinely new strain only appears when all 3 bits get flipped in some copy. But:
(a) The more total copies of the virus there is, the faster a bad mutation happens (speed scaling linearly).
(b) Assuming that some mutations require multiple independent errors to occur (which seems likely?), the virus population is "making incremental research progress" over time by spreading out across the genetic landscape towards different strains, even when no visibly different strains occur.
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2021-01-22T05:21:47.287Z · LW(p) · GW(p)
Given the high dimension of the search space, I think (b) is negligible and the linear model (a) of your first comment is better. In low dimension the boundary of the unit sphere is small and you can have a lot of copies on the inside, having to pass through the sphere to reach new terrain. Whereas, in high dimensions, the population will quickly thin out and all be unique, so what matters is the total volume of space explored, not how long it takes to get anywhere.
Replies from: alkjash↑ comment by alkjash · 2021-01-22T21:54:18.036Z · LW(p) · GW(p)
I'm not totally convinced this is the right way to think about it, any given useful mutation will depend on some constant number of coordinates flipping, so in this high-dimensional space you're talking about, useful mutations would look like affine subspaces of low codimension. When you project down to the relevant few dimensions, there's probably more copies of virus than points to fit in, and it takes a long time for them to spread out.
I guess it depends on the geometry of the problem, whether there are a small number of relevant mutations that make a difference, each with a reasonable chance of being reached, or a huge number of relevant mutations each of which is hard to reach.
comment by Zian · 2021-01-22T01:44:29.290Z · LW(p) · GW(p)
Another vaccination call center website : https://www.covid19vaccinemi.com/
comment by MondSemmel · 2021-01-21T23:21:39.884Z · LW(p) · GW(p)
Missing text:
- There's a paragraph that only says "Without vaccinations, they "
- There's another paragraph that ends with a comma: "If you don’t want to succeed, there are always plausible ways to not succeed. For example," But maybe that's intentional to lead into the following paragraph with "California has decided to [...]".
comment by agc · 2021-01-21T18:00:55.195Z · LW(p) · GW(p)
For why new strains now, the English strain was first detected in September but nobody cared much until Christmas. Now that strains are a hot topic they get reported more. I'm not sure that explains the whole explosion in new strains, but maybe part of it.
I wonder if there was a new and more infectious strain in Europe last spring. They could explain part of why it spread so much faster in Europe and the Americas than in East Asia. Although in that case I would have expected the European strain to have reached Asia eventually.
I feel like restaurants suing so they can have indoor dining says something bad about America. European restaurants just don't do that, so restrictions don't need to be lawsuit-proof. That said the UK had the very inadvisable "Eat Out to Help Out" scheme in August, so maybe different countries just decide that boosting restaurants outweighs everything else at different times.
I think you're being unfair on the smokers thing. It's the kind of thing that happens when you take a general principle (vaccinate people with chronic conditions) and don't add a bunch of exceptions. We don't have time for exceptions. Just going by age would still be better, but getting shots into arms is more important, so let's not get outraged about some undeserving smokers getting vaccinated.
Just as a side note, the word "scheme" doesn't have a negative connotation in the UK.
Replies from: RobbBB, arunto, agc↑ comment by Rob Bensinger (RobbBB) · 2021-01-21T19:04:28.645Z · LW(p) · GW(p)
As of Jan. 21 2021, Our World in Data reports that ~52% of all confirmed COVID cases in the world have happened since Nov. 1, and ~74% have happened since Sep. 1. This maybe makes it a bit less surprising that we'd see more mutations over the past five months, since the amount of circulating virus in the world is much higher.
(Though there's also more testing now than there was in the past.)
↑ comment by arunto · 2021-01-21T19:45:13.373Z · LW(p) · GW(p)
I feel like restaurants suing so they can have indoor dining says something bad about America. European restaurants just don't do that, so restrictions don't need to be lawsuit-proof.
Not all of Europe's restaurants don't do that. In Germany there have been in most states lawsuits against Covid restrictions of all types, e.g. against restaurant closures.
↑ comment by agc · 2021-01-21T23:39:13.637Z · LW(p) · GW(p)
The White House has released a "National Strategy for COVID-19" (pdf) that should be worth critiquing along with the day 1 priorities. I will take it as a good sign that the tweet has "aggressive, coordinated" before "equitable".
On an other note, I wonder what your current best estimate for the increase in R with the new strain is. Has the UK managed to get R below one because the different is smaller than the 0.7 we thought, or just because the control system / lockdown is so powerful?
comment by Angela Pretorius · 2021-01-24T07:40:50.783Z · LW(p) · GW(p)
My (highly speculative!) hypothesis is that the emergence of these variant viruses arises in cases of chronic infection during which the immune system places great pressure on the virus to escape immunity and the virus does so by getting really good at getting into cells. 11/19
That’s plausible, but doesn’t explain why the chronic infections hadn’t done this earlier, and the English strain doesn’t escape immunity in this way (and we don’t know about the others) so I notice it doesn’t feel like it explains things.
Here is a National Geographic article on how new therapies may have allowed chronic patients to be kept alive for longer and with higher viral loads, and may have influenced viral evolution. In particular, the article cites a preprint on Medrxiv which finds that convalescent plasma therapy leads to rapid changes in spike proteins and to the evolution of antibody resistance.
comment by CraigMichael · 2021-01-22T20:05:05.541Z · LW(p) · GW(p)
lol imagining Very Serious People telling us to eat out. Like someone named Colonel Angus.
I mean... are other 80s/90s kids laughing at 'eat out to help out' and then feeling old? Because I am.