Covid 4/22: Crisis in India
post by Zvi · 2021-04-22T13:40:01.676Z · LW · GW · 25 commentsContents
The Numbers Predictions Deaths Cases Vaccinations India Vaccines Still Work Pausing Vaccines For No Reason Still Doesn’t Work The Next Strain: P.1 In Other News None 25 comments
The United States appears to have turned the corner. Despite our determination to sabotage vaccination efforts, they have taken only minor damage, and we are starting to see declines again in the number of cases. Unless a new strain more dangerous than the English one reverses things once again, we should soon start to see steady declines in cases.
Other places without our access to vaccines are not as lucky, and in particular India is in crisis. Things there are worse than they’ve ever been and rapidly getting worse, with the hospitals on the verge of collapse. This is likely to be the biggest human cost of the entire pandemic, plausibly by a very large margin given how many people live in India, and it is entirely the our responsibility for not accelerating vaccine production in time to help them. Even when we have vaccine we are unwilling to use, we refuse to use it to help where it is needed.
Actions have consequences. In particular, a lot of death.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 5.8% (up 0.2%) and deaths unchanged.
Result:
The number of tests continues to crater, and also the numbers continue to not make much sense as reported here, since if tests fall 26.5% and cases fall 11.9%, that should imply the positive test percentage is higher rather than lower. I still don’t get how that one keeps happening.
Johns Hopkins has the rate declining from 5.2% to 4.7%, so I suppose that decline is real, and the 26.5% number isn’t real and I should chalk this kind of thing up to systematic reporting delays.
Can you tell that I really, really miss the Covid Tracking Project?
The trick as always is whether this is a data error that self-corrects, or the start of a trend which in this case would be the beginning of the final phase barring a new strain worse than the English one. I’m going to cautiously say it’s more likely to be mostly real, but likely got a little ahead of itself because graphs should be smooth.
Deaths should continue to slowly decline as vaccinations work, but it’s a slow process.
Prediction: Positivity rate of 5.1% (down 0.2%) and deaths decline by 4%.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Mar 4-Mar 10 | 2595 | 1775 | 3714 | 1539 | 9623 |
| Mar 11-Mar 17 | 1492 | 1010 | 3217 | 1402 | 7121 |
| Mar 18-Mar 24 | 1823 | 957 | 2895 | 1294 | 6969 |
| Mar 25-Mar 31 | 1445 | 976 | 2564 | 1262 | 6247 |
| Apr 1-Apr 7 | 1098 | 867 | 1789 | 1160 | 4914 |
| Apr 8-Apr 14 | 1070 | 1037 | 1621 | 1145 | 4873 |
| Apr 15-Apr 21 | 883 | 987 | 1747 | 1168 | 4785 |
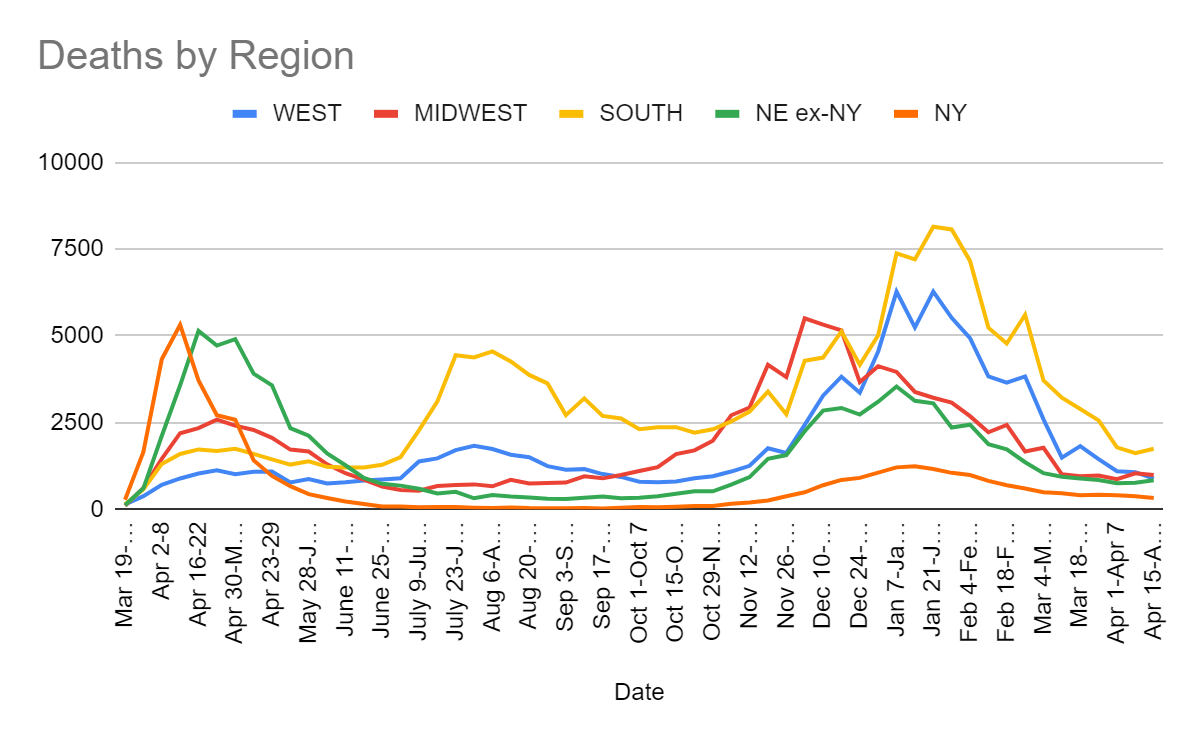
Things will bounce around due to random fluctuations and data timeshifting, but the default should continue to be a slow decline in deaths until cases have had several weeks of declines, at which point the drop should accelerate.
Cases
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Mar 4-Mar 10 | 62,935 | 57,262 | 114,830 | 109,916 |
| Mar 11-Mar 17 | 49,696 | 59,881 | 109,141 | 115,893 |
| Mar 18-Mar 24 | 47,921 | 72,810 | 99,568 | 127,421 |
| Mar 25-Mar 31 | 49,669 | 93,690 | 102,134 | 145,933 |
| Apr 1-Apr 7 | 52,891 | 112,848 | 98,390 | 140,739 |
| Apr 8-Apr 14 | 60,693 | 124,161 | 110,995 | 137,213 |
| Apr 15-Apr 21 | 54,778 | 107,700 | 110,160 | 119,542 |
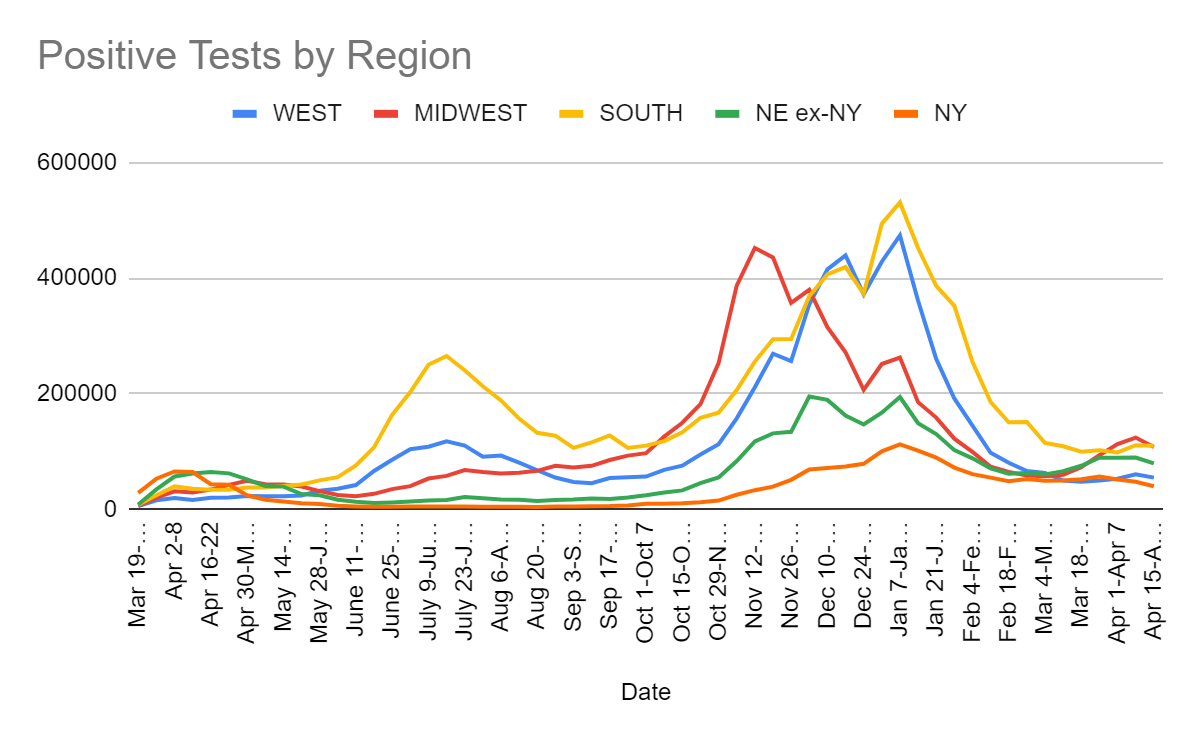
Clearly the corner has been turned. We will see if it can be sustained.
Vaccinations
You know what’s not good for vaccination rates? Suspending the use of vaccines. I hear that’s bad for vaccination rates.

That number was greatly boosted by a +15% acceleration in California. Most states had double digit declines.
Without Johnson & Johnson, and with the increased vaccine hesitancy, things are going to be harder from here on in, and I have little hope that J&J vaccinations will be allowed to resume, nor do I expect us to agree to export the doses to a place that would actually use them any more than we’re letting go of our AZ doses. It’s at least kind of murder, and all kinds of foolish and destructive.
There are those who say that the slowdown has multiple causes, and that we’re starting to run into the wall where there aren’t enough people who want vaccinations, making supply not the limiting factor in many places and making the second half of the job harder and presumably much slower as well. I do acknowledge this is a real dynamic, but also we intentionally hurt demand via the suspension of J&J, both in terms of increasing hesitancy, and in terms of taking away a one-shot-only vaccine that was logistically far easier to deal with, thus making harder to reach people that much harder to reach and making those who dread shots or ‘this new mRNA technology’ that much more hesitant.
Thus, while I do think it’s unfair to attribute the entire deviation from the previous upward trend as being due to the suspension of J&J, I do think that’s most of it. At a minimum, I would be very surprised if we would have otherwise seen a decline in the rate of progress rather than a plateau.
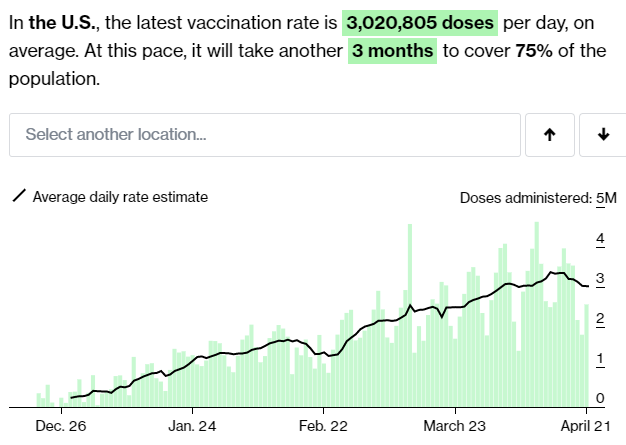
For next week, my expectation is that it will drop below 3 million doses per day, let’s say a median prediction of 2.9 doses per day, assuming that J&J remains suspended, as it appears that it will be. I do still expect all the second doses to happen on schedule, which should prevent the number from dropping too dramatically, as the number of scheduled second doses should still be rising.
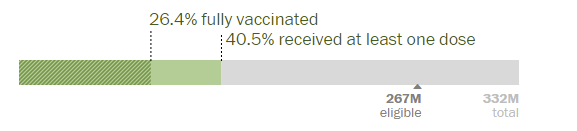
Note of course that this still represents a steady stream of additional vaccinations, and that our situation will continue to improve. Even if we decline to 2 million doses a day, and all of them are from 2-dose vaccines, that’s still 1 million extra immune people per day, or an extra 2% protected every week. With 40%+ of the population and 50%+ of the adult population already having at least one dose, that should lower the weekly spread of Covid by a compounding 5% or so a week. The results of that should still be good enough.
Others, however, are not so lucky. In particular, the situation in India looks very, very bad.
India

It looks very, very bad (Financial Times).


They’re still barely below the United States in confirmed cases per capita, but the graph looks like this:
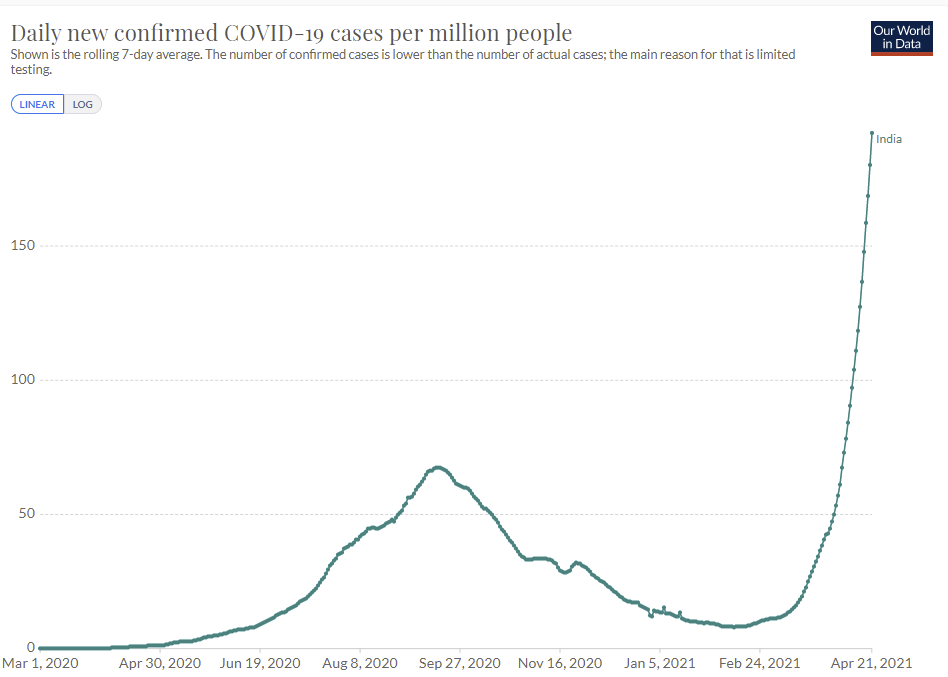
With no signs of stopping, and no reason to doubt that this is a massive undercount.
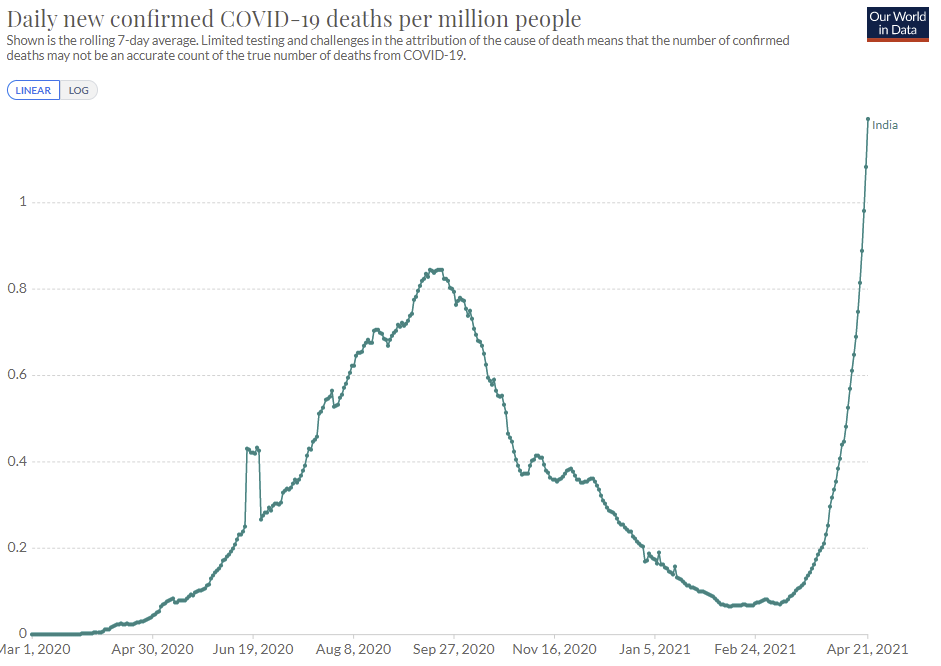
Official deaths are lower than in the United States as well, but likely much, much higher than reported, and going vertical:
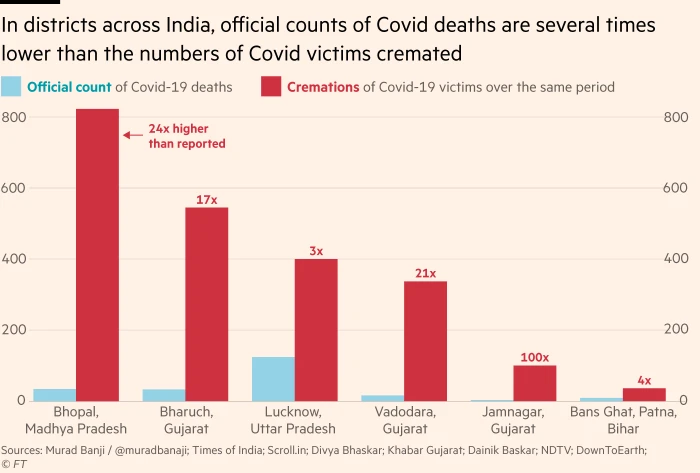
Here’s the comparison (from FT) to cremations of Covid victims, it’s really bad out there:
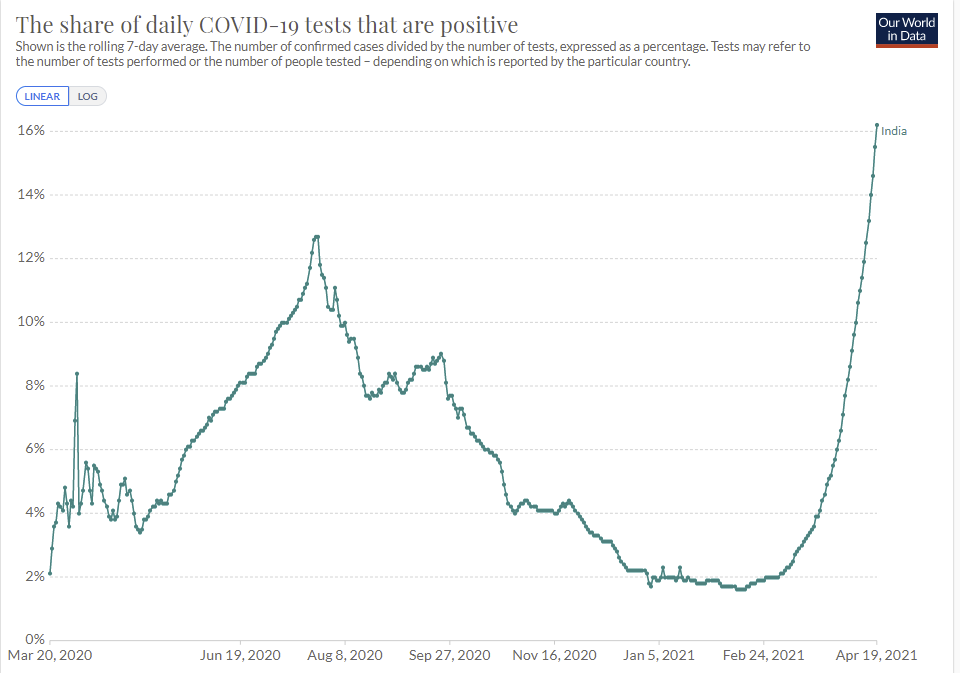
As always, share of positive tests is a key metric, and it has the same straight line. Yikes.
The hospital system is on (at least) the verge of collapse.What happened? And what is going to happen now?
As there usually is, there’s a variant involved, this time it’s B.1.617.
The thing is that being vaccine evasive wouldn’t explain what’s happening, because India doesn’t have that many people who are vaccinated. Even if it had full escape from all immunity, that wouldn’t explain what’s happened here. India’s old positive test percentages were never that high, so it’s that much more unlikely there were massive previous waves we didn’t notice. To the extent that this strain is the cause, it’s pure additional infectiousness doing most of the work. That doesn’t preclude escape, but it means we don’t have much reason to expect escape either.
I haven’t been tracking India, but I don’t have any reason to think there was a large behavioral change since February that could take us from static to doubling every week. What could this be other than the variant? So I went looking for what we know.
Here’s a Forbes explainer, which also notes that the variant has arrived in California. It seems there are a lot of different mutations in B.1.617 that are contributing to it being a bigger problem, part of which is making immune response more difficult. Forbes also reports that Israel found eight cases, and that the Pfizer vaccine still works but has ‘reduced efficacy’ against it.
This from the Indian Express covers the basics but doesn’t have insight into the questions we need answered. This from The Guardian is similar, with those quoted thinking this likely isn’t as dangerous a variant as the Brazillian or South African ones.
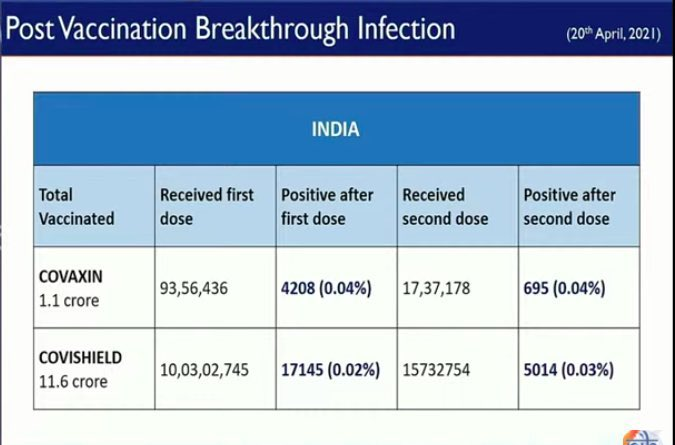
Zaynep comes through and hooks us up with the good news that the vaccines still look effective against B.1.617:

That thread also points out the obvious. Yes, we need to worry about and think about the possibility that the variant will cause trouble on our shores and for ourselves personally, but the main thing for the world is that there’s a huge disaster happening right now, in India, and no one seems to care to do much about it. Certainly our vaccine policy has given little or no thought to getting doses for the third world, despite it protecting us against variants and buying massive goodwill while being super cheap. To the extent that anyone ever says anything, it’s ‘let’s get rid of the IP incentives that created the vaccines’ rather than ‘let’s pay more money and make more vaccine doses.’
This from Science Media Center is the standard thing where ‘experts’ refuse to speculate until they have all their data lined up, and act like the variant both taking over and taking over while cases explode all of a sudden aren’t together much evidence, and there’s no reason yet to call this a ‘variant of concern.’ I’d say I’m concerned.
I know that jumping to conclusions can backfire. But if something is probably concerning, that’s concerning. One shouldn’t remain unconcerned until there’s proof, that’s not how this works, that’s not how any of this works.
I’m putting it at about 85% that the surge in India’s primary cause is that the B.1.617 variant is far more infectious than their previous variant. I’d go higher, but the possibility that lots of cases have been missed for a long time, together with my lack of detail knowledge in India, makes me not want to make too strong an assumption yet. I could easily get higher quickly.
What happens now, unfortunately, is presumably the collapse of India’s hospital system. I don’t see a likely way around that, since they’d have to stall things in their tracks right here without another doubling. The only way this doesn’t happen is if individuals react dramatically, and cut their exposures by almost half within the next few days, or perhaps it would even need to have already happened several days ago. Either way, seems unlikely, as I don’t think India or its people have that kind of slack.
This was always on the table as an outcome, from the very beginning. There’s a maximum amount of baseline infectiousness, beyond which adjustment to stop it is not practical, and the control system breaks down. It’s that much easier to hit the breaking point in a country that’s much poorer, and thus has much less effective hospital capacity. We’ll find out soon if India has reached that point.
The flip side is that there have been places with much higher positive test rates for quite a while. Mexico spent a long time around 50%, and many places in the United States may have been in worse spots than India is now, and turned things around or at least stabilized them via behavioral adjustments.
Vaccines Still Work
Some perspective, I didn’t do the math myself but seems reasonable even if the other person is unvaccianted, cars are rather unsafe:
Before you say we can’t pause cars, we paused seeing other humans for a year, so we can do a lot of things.
Some lack of perspective, if you’d prefer that instead. If you have a vaccine that is only 95% effective, and there are 71 people who catch the virus post-vaccination none of whom die, you could always do something like this, including having officials ‘urge caution’:

Pausing Vaccines For No Reason Still Doesn’t Work
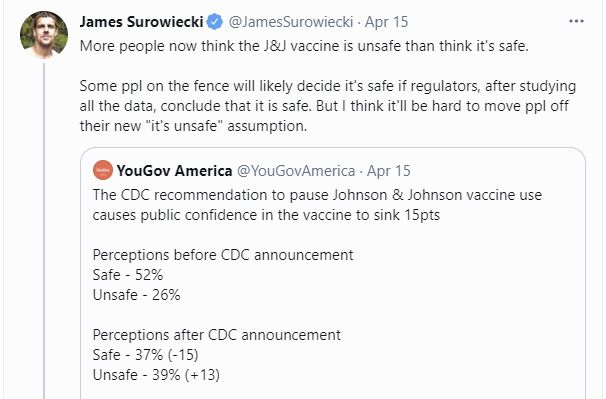
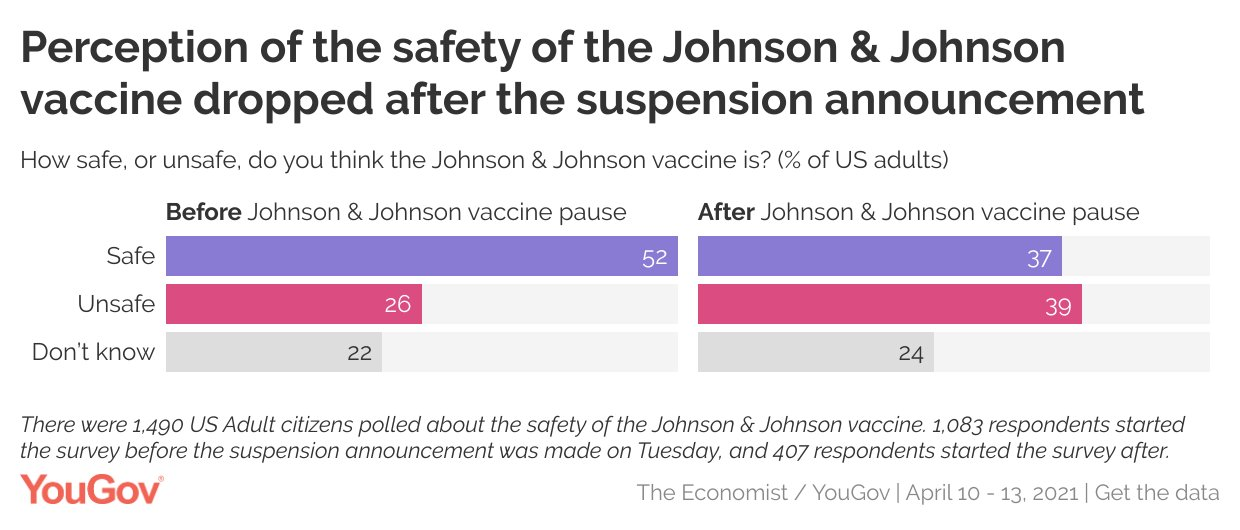
Damage to public confidence was done quickly, and will be hard to reverse.
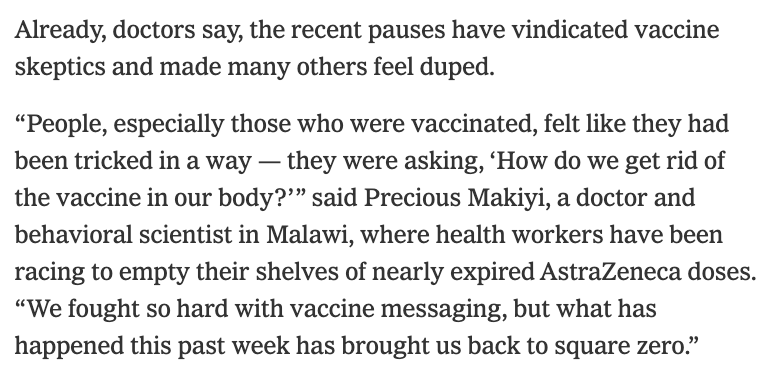
Also:
As noted last week, a brief pause was something that could be steelmanned. If you had a very different model of how the public reacts to news, and assumed the news would always get out, then you could argue for a brief pause.
You can’t argue for our current policy of keeping the blanket pause in place for weeks. We could mitigate most of the damage by restricting the ban to young women, putting a fig leaf over the whole thing and moving doses around between populations, but we aren’t even doing that.

Matt Yglesias points out how much whiplash is involved here, as every consideration is either mandatory and total, or forbidden to even speak its name:

Again, what is this new data we’re looking for? What about the current data is insufficient to reach the necessary conclusions?
This seems like a good intuition pump:
When you’ve lost Eric Topol on your abundance of caution (WaPo), and he’s calling it a ‘deadly mistake,’ you know you messed up. Unless, of course, you didn’t.
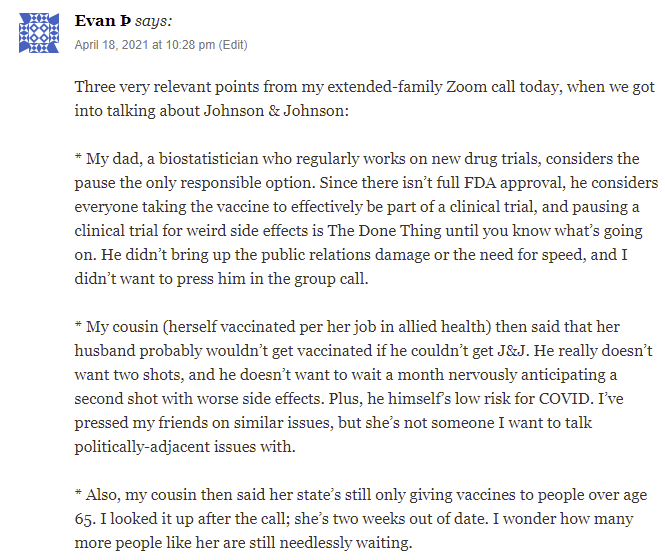
This comment on last week’s post kind of says it all:
There’s also this, which is now increasingly causing direct damage by giving the impression that things were rushed:

It also has the standard splash damage that when a completely insane standard is applied in one area, it makes it impossible to think clearly about other areas, resulting in things like this:
That’s not to take any position on firearms, any more than one would call for a pause on slicing bread. You could argue for a pause in actual almost anything if all it has to do is unintentionally kill two people when done millions of times.
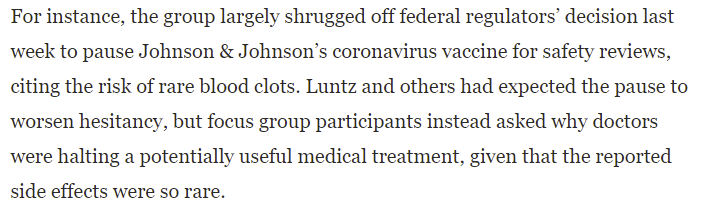
There’s this claim today that the AZ and J&J pauses did not increase vaccine hesitancy. I do not think this reflects what’s going on at all, as willingness to get vaccinated naturally increases over time as people can see others doing it and everything going well, but it’s at least saying that this hasn’t been that large of a disaster in terms of the threshold that counts. I’m still highly confident things are going substantially worse than in the counterfactual.
The Next Strain: P.1
Eliezer Yudkowsky asks the obvious question. Only about a third of the population is covered, but there are also a lot of children:
Thread contains a bunch of real data (as usual, he has to follow up with a Tweet saying “please only respond with actual data) that led to James Babcock pointing out the CDC’s variant data, which he then put into this spreadsheet.
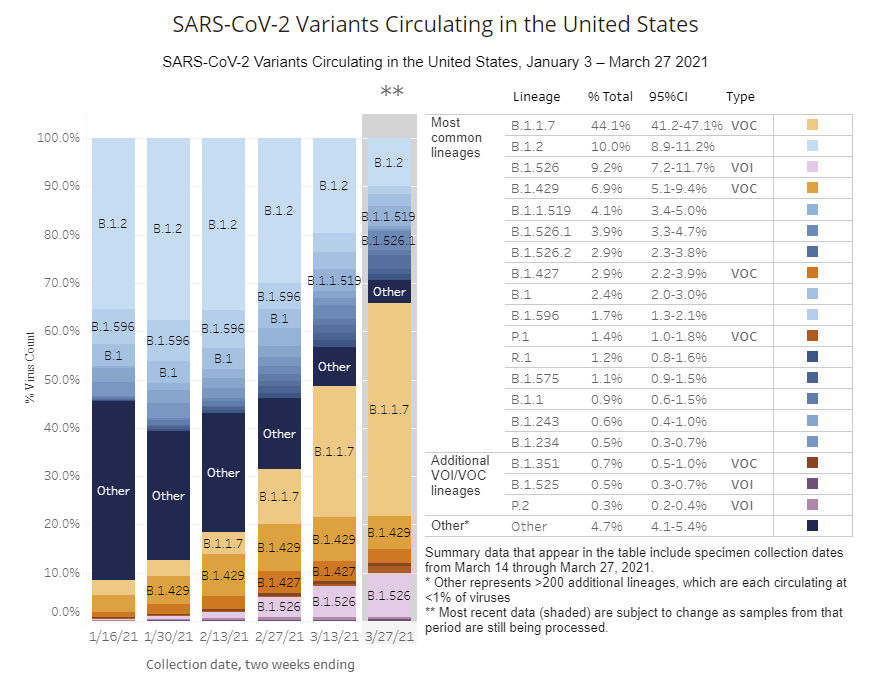
The end of March was when B.1.1.7 was taking over, going from 11.4% of cases on 2/27 to 44.1% of cases on 3/27. Thus, in April, strains with a competitive advantage are growing, other cases continue to shrink, and the shift from one to the other has cancelled out our vaccinations. The good news is that B.1.1.7 can only hit 100%, whereas vaccinations can also hit 100%, and that’s a battle vaccines win. If that was the whole story, we’d be in great shape, and confident we can turn things around soon.
The bad news is that P.1 is growing as well, potentially faster than B.1.1.7 (there’s enough measurement error here that I wouldn’t be confident in that), and its advantages likely involve some amount of immune escape. If that’s true, even if (as it seems from this and what other data we have on the question) that’s mostly about evading immunity from infections rather than from vaccinations, it will be the dominant strain in several months, and we’ll have to up our game another level if we want to stay ahead.
The good news is that, unless the immune escape is much stronger than we think it is, we can totally get there, even with our vaccination pace slowing down due to regulatory sabotage. Or at least, we can definitely get there in areas without a lot of vaccine hesitancy, which also is up due to that same sabotage.
It’s worth stopping to contrast these two world views.
In the first corner, we have Dustin Moskovitz, who works on projects he hopes will make humanity thrive. He notes how amazing it is we’ll be able to immunize essentially the entire population of many areas.
In the second corner, we have the reporter from The New York Times, who points out how Just Awful some places are, and then associates the whole thing with Donald Trump. Classy.
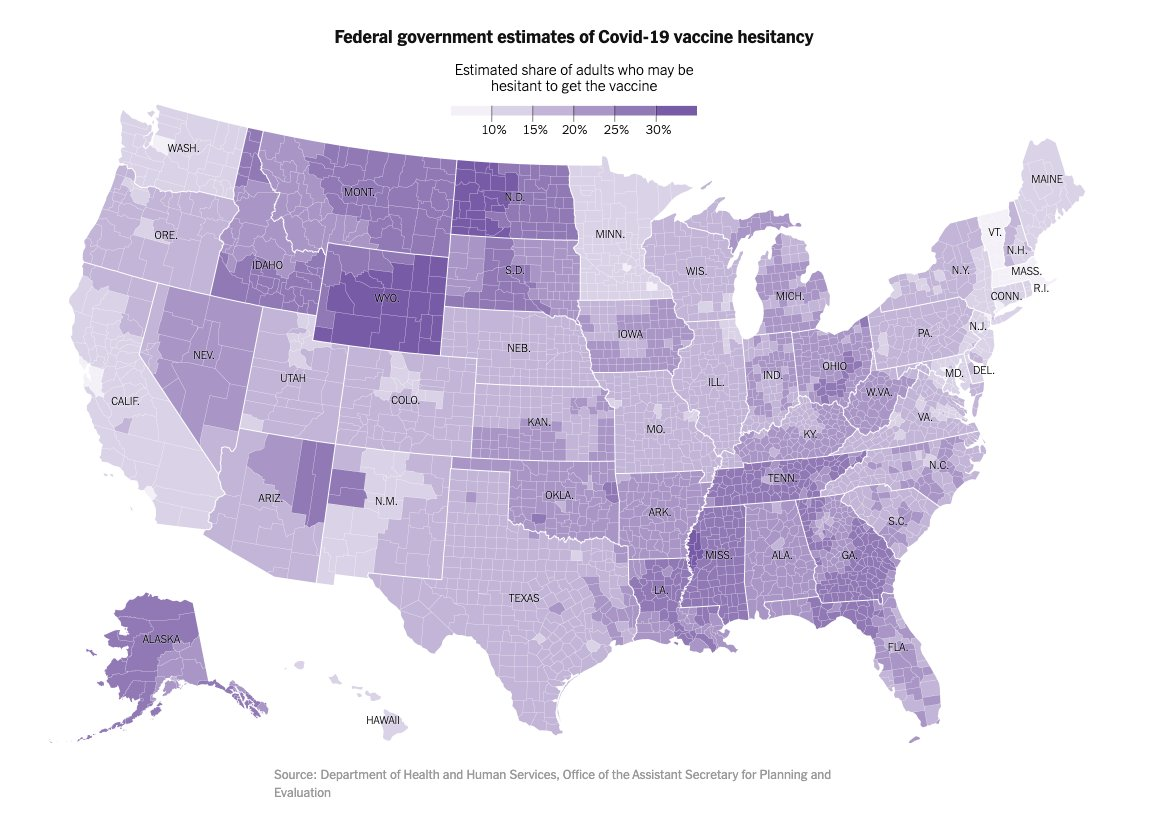
I wonder what magic is taking place along state borders in many places, especially Wyoming, but mostly the graph should not surprise us. I’m not sure how much of the detail I would have guessed on first principles, but certainly a lot of it.
The number of people who live in areas where the refusal rate is going to be 30%+ looks very low. The worst this gets for places with a lot of people in them is roughly 20-25%, which means (if these calculations are correct) they can still get to 75-80% vaccinations. That should still be enough. We might still be left with some states where things stay bad for a while, but when there’s almost zero cases in the Northeast and still a lot of cases in the places people aren’t vaccinating, I have a feeling we’ll see some people change their minds.
If you’re looking to help change those minds, here’s some good advice (WaPo article):
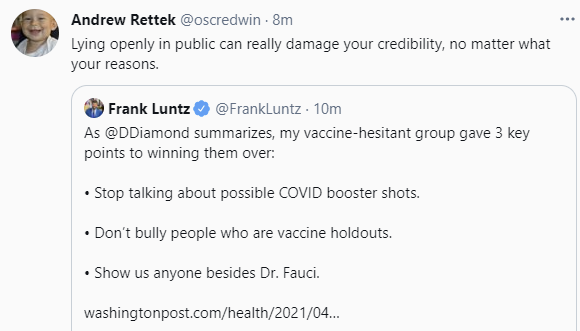
From that article, it turns out that even vaccine skeptics can do math better than the FDA, and but haven’t figured out that this is true and important:
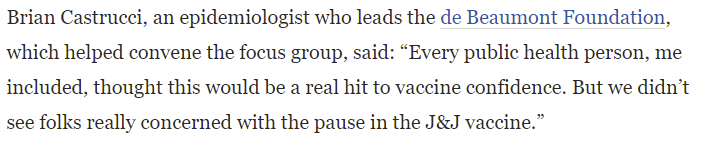
It took less than a week for us to go from ‘pause is important to keep people confident in the vaccines’ to ‘every public health official, me included, thought this would be a big hit to vaccine confidence.’ I don’t even get whiplash anymore. (And yes, I know that if you steelman their position there’s a way to reconcile those two statements, where the alternative would have been worse.)
What I found most interesting was also surprising to those who ran the focus group, which is that talk of booster shots pisses off such people:
I fail to understand why people can’t live like that. A vaccine shot every year is that bad? In a world in which, by definition, Covid is still around? All right then.
On the other hand, there’s this other thing they found that they did not expect, and yeah they should totally have expected it and I’m not sure why they didn’t:
You thought people who didn’t want to get vaccinated wouldn’t want fake vaccination cards when the cards are required in order to do things? Really?
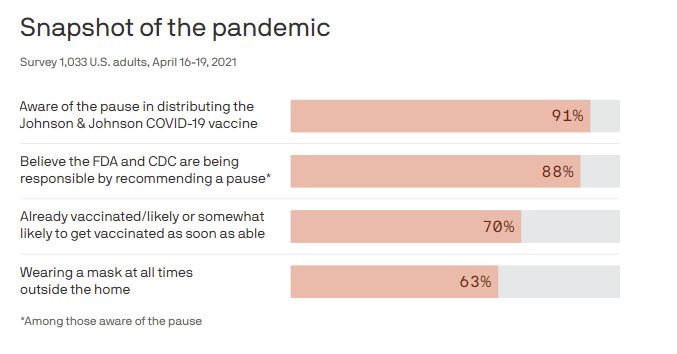
Finally, it’s worth noting that this is a place where regular people, most people, still are willing to take the FDA’s word for things. The problem is that what they’re taking the FDA’s word for is that the vaccines might not be safe, but either way, public support for the announcement is strong.
That’s in contrast to the people I talk to and respect, who universally think of this decision the same way I think of this decision.
In Other News
Bill Maher offers his weekly new rule to not mix politics with our health. Well said, and good luck with that.
Washington state denies people vaccinations on the basis of the color of their skin.
Researchers in Belgium register a trial of Moderna half-doses, which I expect will produce less side effects, almost identical protection and double the number of people protected; I’d put the chance of a success here around 90% if the study is well-designed. Thing is, it’s only 200 people, so all they can measure is immunogenicity, which the clinical trials already checked. So what’s likely going to happen is they note ‘immune response is almost identical’ and then everyone says ‘yes, but what if somehow it’s not as effective’ and continues actively wasting half the doses.
Pirate Wires preaches it: “Science” and safety porn.
Nate Silver thread reminding us of the pattern where when we play up dangers, we scare the people who are already safe while alienating the ones who are taking real risks.
Child shows up at their facility daily so they can perform required labors remotely on their computer anyway in an overflow room. Yes, you can have the worst of all worlds at once.
Interesting analysis says that English Strain’s relative infectiousness likely declined greatly over time, and at a minimum we have no idea how much more infectious it actually is despite ‘experts’ pretending otherwise on the basis of, as he essentially puts it, two points and a line between them. One could reply that we know a lot because the strain did indeed take over everywhere more or less within the predicted time frame, but it’s good to look from additional angles. There’s definitely some weird data here. There’s also reason to think that restrictions could alter the relative infectiousness levels. The English strain is slower to spread and slower to go away, and it produces higher viral loads. Various restrictions could be more or less effective at stopping the different strains, and the timing could also give a misleading impression.
Demand falling below supply at University of Arizona. Seems to be steadily happening in more places. If still need to get vaccinated, there are lots of places to go if you look around.
If you’re 50+ in NYC, you can walk in and get a vaccine without an appointment, here’s a list of where to go.
Soon you’ll also be able to go to Alaska, and get vaccinated at the airport. It’s part of a plan to reinvigorate the Alaskan tourist industry, via getting as many unvaccinated visitors as possible.
A paper reporting on (spoiler alert: complete lack of) lockdown effectiveness, and on benefits versus costs.
United Kingdom has a day with only one Covid death. New goal is a day with only one death of any kind. Fund anti-aging research!
25 comments
Comments sorted by top scores.
comment by GeneSmith · 2021-04-22T21:17:10.975Z · LW(p) · GW(p)
Sometimes I read these posts and feel like I am standing on an island of sanity among a sea of insane people. That 88% support of Johnson & Johnson vaccine pause just seems totally nuts.
If you're looking for something useful to do, call your senators and congresspeople and ask them to send our Astra Zeneca doses to hard hit parts of India.
Replies from: JesperO, hamnox↑ comment by JesperO · 2021-04-23T03:41:40.553Z · LW(p) · GW(p)
On the bright side, that 88% of people may not be as insane as they seem. The vast majority of people don't think for themselves on most topics. Rather people outsource thinking to trusted institutions and specialized individuals. That makes sense. Unless you've focused a lot on how to think well it's going to be far too expensive and ineffective to figure out (most things) by yourself.
Unfortunately, when the institutions are bad and spread insane views, this outsourced thinking causes the trusting majority to share those insane views.
↑ comment by Vladimir_Nesov · 2021-04-23T08:25:08.486Z · LW(p) · GW(p)
when the institutions are bad and spread insane views, this outsourced thinking causes the trusting majority to share those insane views
Or alternatively, with the model of institutions as competent but dishonest, the takeaway from an action with an implausible-sounding explanation (pausing vaccination out of "an abundance of caution") is to make up your own explanation that would make the action seem reasonable (there are issues that are actually serious), and ignore all future claims from the institution on the topic ("we checked and it seems fine").
Thus conspiracy theories, grounded in faith in the competence of institutions. With how well they manage to keep the evidence behind the real explanations secret, they must be pretty competent!
↑ comment by hamnox · 2021-04-23T14:13:55.481Z · LW(p) · GW(p)
I do kind of see it as being the responsible action, I just do not think this is the same thing as it being the right or even reasonable action.
It's trying to be "responsible" despite not actually having the kind of control over the situation that makes things your responsibility.
comment by Sam Marks (samuel-marks) · 2021-04-22T17:33:32.561Z · LW(p) · GW(p)
I wouldn't trust the vaccine hesitancy data at the sub-state level. From the methodology here, the state level data come from the Household Pulse Survey (HPS), and the local estimates are produced by adjusting these data using sociodemographic factors:
Our statistical analysis occurred in two steps. First, using the HPS, we used a logistic regression to analyze predictors of vaccine hesitancy using the following sociodemographic and geographic information: age, gender, race/ethnicity, education, marital status, health insurance status, household income, state of residence, and interaction terms between race/ethnicity and having a college degree.
Second, we applied the regression coefficients from the HPS analysis to thedata from the ACS [a survey with local demographic information] to predict hesitancy rates for each ACS respondent ages 18 and older. We then averaged the predicted values by the appropriate unit of geography, using the ACS survey weights, to develop area-specific estimates of hesitancy rates.
Note in particular that "state of residence" is one of the variables in the regression.
More info can be found here.
Replies from: JesperOcomment by CraigMichael · 2021-04-24T06:58:34.590Z · LW(p) · GW(p)
Paras Chopra, who I met on Twitter because of a common interest in GPT-3, posted a Tweet with recommendations on what Americans can do to help India.
https://twitter.com/paraschopra/status/1385834938545557507?s=20
Paras Chopra (@paraschopra) Tweeted: Donate: https://t.co/1fErNmgAys
Petition your govt (if in US) to release the embargo on exporting vaccine supplies to India.
And retweeted the following from @Sidin
COVID FUCKING SUCKS. What can you do you NRI, international legend with Forex?
GIVEINDIA have several campaigns: https://indiafightscorona.giveindia.org
FOOD: KhaanaChahiye: https://fundraisers.giveindia.org/fundraisers/khaanachahiye-mumbai-is-battling-hunger-along-with-covid-19-again
OXYGEN: Its Hemkunt baby! https://linktr.ee/hemkuntfoundation
...
Is there ways to share this with EAs?
Replies from: evhub↑ comment by evhub · 2021-04-24T21:40:09.114Z · LW(p) · GW(p)
Is there ways to share this with EAs?
You could write a post about it on the EA Forum.
Replies from: CraigMichael↑ comment by CraigMichael · 2021-04-25T01:22:22.216Z · LW(p) · GW(p)
Woah. It looks just like LessWrong. :)
comment by lsusr · 2021-04-22T15:43:25.983Z · LW(p) · GW(p)
Great post. India will be a disaster for human welfare. I predict at 90% confidence that one or more new strains are responsible for the exponential growth of infections in India. Only three other things could cause it:
- Summer. Seasonal change doesn't make sense because infections ought to go down, not up.
- A change to testing or reporting. Possible but unlikely.
- Complete breakdown of society on the scale of a civil war. If this happened I would have heard about it.
I predict with 98% confidence that the exponential growth is caused by a new strain, new strains, and/or sampling bias (testing + reporting).
If [you] still need to get vaccinated, there are lots of places to go if you look around.
This is true where I live. I am in the youngest adult age bracket and live in a Blue city. I got my first vaccination yesterday by taking a ferry to a nearby Red district.
Replies from: TheSimplestExplanation↑ comment by TheSimplestExplanation · 2021-04-22T19:57:35.279Z · LW(p) · GW(p)
Summer. Seasonal change doesn’t make sense because infections ought to go down, not up.
AFAIK seasonality works different in the tropics. It's worst in the rainy season.
Complete breakdown of society on the scale of a civil war. If this happened I would have heard about it.
Weren't there religious & political events that may have contributed?
I predict with 98% confidence that the exponential growth is caused by a new strain,
Yes I came across this graph 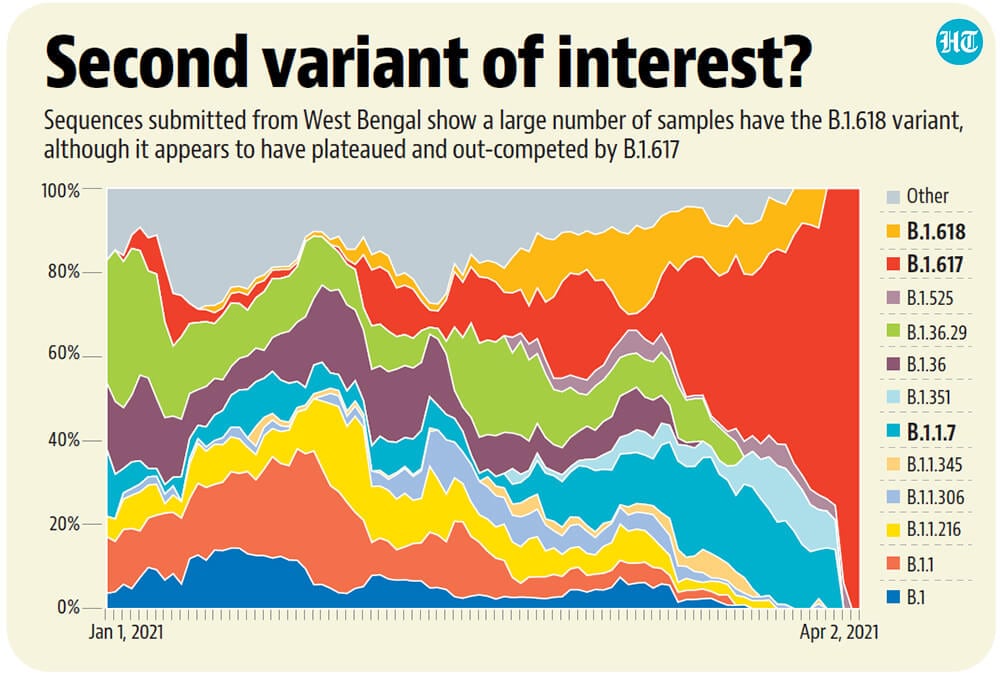
↑ comment by lsusr · 2021-04-22T23:00:58.156Z · LW(p) · GW(p)
Good point about the tropics. I could be wrong about the seasonal directionality. I had an unstated assumption that even if direction of the effect was inverted the change wouldn't be significant enough to account for the data. That was my real crux.
My reference point for religious rituals was Christmas in the United States. India's biggest religious rituals take place outside. Even if India's religious rituals were much bigger, they wouldn't cause a takeoff as fast as we observed in Zvi's graph.
That's a informative variant graph. I'm updating my probabilities to 98% it's one or more strains and 99% it's one or more strains and/or a change to the measurement. I'm going to add another prediction: 95% confidence that India fails to get B1.617 under control before it burns through the population.
But experts say India is unlikely to meet its target of covering 250 million people by July, especially as cases continue to surge.
―Covid-19 vaccination: How is India's inoculation drive going from BBC News via Yahoo News
India is hosed. I wonder what happens when B1.617 hits other countries that haven't vaccinated their populations yet?
Replies from: TheSimplestExplanation↑ comment by TheSimplestExplanation · 2021-04-23T09:35:09.662Z · LW(p) · GW(p)
I had an unstated assumption that even if direction of the effect was inverted the change wouldn’t be significant enough to account for the data.
I agree.
or a change to the measurement
Given the apparent under reporting, I'd say no.
95% confidence that India fails to get B1.617 under control before it burns through the population.
It seems like people will panic and isolate. Don't know how much that could or will change in India though.
According to OWD the reproduction rate is 1.5 . So non pharmacological interventions might make a difference, conversely abandoning non pharmacological interventions might have contributed to the current outbreak.
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2021-04-23T12:50:58.456Z · LW(p) · GW(p)
Seconded. The situation in India looks worse, but kind of comparable, to the rapid spikes in South Africa and the UK when new variants arose there. In both cases, the strong reaction induced by the threatening situation led to things stabilizing. It's true that things might be worse for India, but 95% seems really quite high. Maybe you have a detailed model of why the situation is much different and worse in India now? If so, I'd be curious about the reasoning. (JTBC, I also think it's likely that things will be completely bad, but I don't immediately see why >60% for a worst-case scenario seems obviously warranted. There's a chance that if I looked into this for 2h or heard some convincing arguments, I'd also update to >90% now. )
Replies from: lsusr↑ comment by lsusr · 2021-04-23T15:42:15.936Z · LW(p) · GW(p)
Maybe you have a detailed model of why the situation is much different and worse in India now? If so, I'd be curious about the reasoning.
My model of the Indian subcontinent is it's a poor region of huge dense population centers administered by weak central governments.
comment by Jozdien · 2021-04-24T09:00:46.018Z · LW(p) · GW(p)
I haven’t been tracking India, but I don’t have any reason to think there was a large behavioral change since February that could take us from static to doubling every week. What could this be other than the variant?
I’m putting it at about 85% that the surge in India’s primary cause is that the B.1.617 variant is far more infectious than their previous variant.
I don't have much better data about how much to attribute the surge to the variant because as far as I've seen there isn't any, but in the weeks before the surge began, there was a sizeable contingent of people predicting that cases would go up very badly in April even before news of the variant, because of religious festivals (Kumbh Mela in mid-April saw millions of people in crowds without masks after many of the priests tested positive) and regional elections (standard practice to have huge crowds of people surrounding candidates on the road as they pass by, most places didn't stop this year) happening at the same time.
This article gives a bit of credence to the possibility that some countries had populations with higher prior immunity than others. I can't say whether this is true or not, but if so, it's possible that's where the new variant differs. And because India was hit far less hard than people expected, many weren't following mask and distancing protocols by April, which meant new viral loads would have been very opportune.
comment by Kenoubi · 2021-04-24T00:48:16.311Z · LW(p) · GW(p)
I have little hope that J&J vaccinations will be allowed to resume
Seems like you were finally too pessimistic about something. https://www.washingtonpost.com/health/2021/04/23/johnson-and-johnson-vaccine-blood-clots/, headline is "Federal agencies lift pause on use of Johnson & Johnson vaccine, saying benefits outweigh risks". (I agree entirely with your points on the merits (more specifically, lack thereof) of suspending it in the first place.)
comment by Sherrinford · 2021-04-23T13:32:27.503Z · LW(p) · GW(p)
Certainly our vaccine policy has given little or no thought to getting doses for the third world, despite it protecting us against variants and buying massive goodwill while being super cheap.
What about COVAX?
comment by NoSignalNoNoise (AspiringRationalist) · 2021-04-23T04:02:17.177Z · LW(p) · GW(p)
The important question about Alaska opening up vaccines to tourists is whether non-Americans will be able to get in.
comment by Mitchell_Porter · 2021-04-22T21:01:44.704Z · LW(p) · GW(p)
On India
it is entirely our responsibility for not accelerating vaccine production in time to help them
India is the world's biggest vaccine producer, and the cornerstone of the Gavi plan to supply Covid vaccines to poor countries. And when this second wave became evident, I believe they quickly started redirecting their national Covid vaccine production for domestic use. I am not sure what the exact cause of the Indian second wave is, but I don't think you can blame it on America, unless you think it was America's responsibility to foresee and preempt all problems worldwide in beating the pandemic.
Replies from: GeneSmith, CraigMichael↑ comment by CraigMichael · 2021-04-23T19:05:05.723Z · LW(p) · GW(p)
“I don't think you can blame it on America, unless you think it was America's responsibility to foresee and preempt all problems worldwide in beating the pandemic.”
A world where we accepted and followed through with these kinds of responsibilities would, overall, be a better one.
comment by Pattern · 2021-04-22T17:52:01.916Z · LW(p) · GW(p)
With no signs of stopping, and no reason to doubt that this is a massive undercount [on the right side of this graph, and what's going is much worse.]
All the negatives in the second part of the sentence take a while to parse.
Certainly our vaccine policy has given little or no thought to getting doses for the third world, despite it protecting us against variants and buying massive goodwill while being super cheap.
'even though it would protect us'. Past tense suggests an event has taken place. The way to suggest that it would have, had we done it (counterfactual past?): 'despite that it would have protected....bought massive goodwill...and been super cheap.'
What I found most interesting was also surprising to those who ran the focus group, which is that talk of booster shots pisses off such people:
A really strong response to rent seeking?
comment by tkpwaeub (gabriel-holmes) · 2021-04-28T09:27:21.755Z · LW(p) · GW(p)
Have you been following some of the research linking poor clinical outcomes in Covid-19 patients to CMV?
https://immunityageing.biomedcentral.com/articles/10.1186/s12979-021-00218-z
And then compare the map (note the high incidence of congenital CMV in India, South Africa, and Brazil):
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3553672/#!po=6.72043
Upshot: we might need to get a handle on CMV in order to quash Covid-19.
comment by Dale Udall · 2021-04-23T08:23:15.440Z · LW(p) · GW(p)
We now have a Philippines strain to worry about, there will be more until we solve this globally, yet there is no sense of urgency whatsoever.
The urgency went away with the restaurants, the jobs, the summer protests and the winter elections. "Two weeks to slow the curve" became "Let's make sure the poorest people with the most vulnerable relatives still have to ride the NYC subway to work because a city survives on its underclass, and hey let's stick COVID patients in nursing homes." The pandemic became the one thing that's poison to a news cycle: boring.