Long Covid Is Not Necessarily Your Biggest Problem
post by Elizabeth (pktechgirl) · 2021-09-01T07:20:05.374Z · LW · GW · 40 commentsContents
Personal Stuff Caveats Data Long term outcomes correlate with short term outcomes Odds of acute outcomes Odds of long term outcomes Comparison to other diseases Conclusion Change my mind None 40 comments
At this point, people I know are not that worried about dying from covid. We’re all vaccinated, we’re mostly young and healthy(ish), and it turns out the odds were always low for us. We’re also not that worried about hospitalization: it’s much more likely than death, but maintaining covid precautions indefinitely is very costly so by and large we’re willing to risk it.
The big unknown here has been long covid. Losing a few weeks to being extremely sick might be worth the risk, but a lifetime of fatigue and reduced cognition is a very big deal. With that in mind, I set out to do some math on what risks we were running. Unfortunately baseline covid has barely been around long enough to have data on long covid, most of it is still terrible, and the vaccine and Delta variant have not been widespread long enough to have much data at all.
In the end, the conclusion I came to was that for vaccinated people under 40 with <=1 comorbidiy, the cognitive risks of long covid are lost in the noise of other risks they commonly take. Coming to this conclusion involved reading a number of papers, but also a lot of emotional processing around risk and health. I’ve included that processing under a “personal stuff” section, which you can skip if you just want the info but I encourage you to read if you feel yourself starting to yell that I’m not taking small risks of great suffering seriously. I do encourage you to read the caveats section before deciding how much weight to put on my conclusions.
Personal Stuff
This post took a long time to write, much longer than I wanted, because this is not an abstract topic to me. I have chronic pain from nerve damage in my jaw caused by medical incompetence, and my attempts to seek treatment for this continually run into the brick wall of a medical system that doesn’t consider my pain important (tangent: if you have a pain specialist you trust, anywhere in the US, please e-mail me (elizabeth@acesounderglass.com)). I empathize very much with the long covid sufferers who are being told their suffering doesn’t exist because it’s too hard to measure and we can’t prove what caused it.
Additionally, I’m still suffering from side effects from my covid vaccine in April. It’s very minor, chest congestion that doesn’t seem to affect my lung capacity (but I don’t have a clear before picture, so hard to say for sure). But it’s getting worse and while my medical practitioners are taking it seriously, this + the experience with dental pain make me very sensitive to the possibility they might stop if it becomes too much work for them. As I type this, I am taking a supplement stack from a high end internet crackpot because first line treatment failed and there aren’t a lot of other options. And that’s just from the vaccine; I imagine if I actually had covid I would not be one of the people who shakes it off the way I describe later in this post.
All this is to say that when I describe the long term cognitive impact of covid as being too small to measure with our current tools against our current noise levels, that is very much not the same as saying it’s zero. It’s much worse than that. What I’m saying is that you are taking risks of similar levels of suffering and impairment constantly, which our health system is very bad at measuring, and against that background long covid does not make much of a difference for people within certain age and health parameters.
A common complaint when people say “X isn’t dangerous to the young and healthy” is that it implies the death and suffering of those who aren’t young and healthy don’t matter. I’m not saying that. It matters a lot, and it’s impossible for me to forget that because I’m very unlikely to be one of the people who gets to totally walk covid off if I catch it. But from looking at the data, there don’t seem to be very many of us in my age group.
Caveats
Medical research in general is really bad, research of a live issue in a pandemic is worse, you should assume these are low quality studies unless I indicate otherwise.
This research was compiled for LessWrong and Redwood Research, with the goal of assessing safety for their office spaces populated by mostly-but-not-entirely-healthy people 25-40, who were much more interested in the cognitive and fatigue sequelae than the physical. Much of this research is applicable outside that group or the sources can be used in that way, but you should know that’s what I focused on.
There isn’t any data on long covid in vaccinated people with breakthrough delta-variant infections. Neither vaccines nor delta have been around long enough for that to exist. Baseline covid has barely been around long enough to have long-term data. What I have here is:
- Data showing that strength of acute infection correlates with long term impact, although not perfectly
- Data on the long term impact of baseline covid, given the strength of an initial infection
- Data on how the vaccine impacts the strength of acute infections
- Data on how delta impacts the strength of acute infections
Data
Long term outcomes correlate with short term outcomes
By far the best study (best does not mean good) comes out of the UK, where the BBC coincidentally started an online intelligence test in January 2020 (giving them a pre-covid baseline) and in May began asking participants if they’d had covid and if so how bad a case. When I said “assume the studies are terrible unless I note otherwise”, this is the study I wanted to highlight as reasonably good. Because they can compare test-takers in a given time period with and without covid they can control for some of the effects of changing a study population over time, which would be the biggest concern. Additionally, my statistical consultant described the paper as “not having any errors that affect the conclusion”, which is extremely good for a medical paper. This study was not ideal for determining sequelae persistence, but they did check if size of effect was correlated with time since symptom onset, and it wasn’t (but their average was only 2 months).
This study showed a very direct correlation between the severity of the acute infection and cognitive decline. I don’t trust its absolute numbers, but the pattern that more severe disease -> more severe persistent effects is very clear
A second study in Wuhan, China (hat tip Connor Flexman) examined long term outcomes of hospitalized patients, based on the intensity of their care (hospitalization, supplemental oxygen, ventilation) found an increase in acute severity was correlated with an increase in sequelae, although it didn’t hold for every symptom (there are a lot of symptoms and the highest-intervention group is small), and they barely looked at cognitive symptoms.
Taquet et al used electronic health records to get a relatively unbiased six figure sample size, that also showed a strong correlation between acute and long term outcomes, which we’ll talk about more below.
From this I conclude that your overall risk of long covid is strongly correlated with the strength of the initial infection.
Odds of acute outcomes
Sah et al estimate that 35% of covid cases (implied to be baseline and pre-vaccination) are asymptomatic, with large variation by age. Children (<18) are 46% likely to be asymptomatic, adults 18-59 are 32% likely, adults >=60 are 20% likely. I’m going to round the non-elderly adult number to ⅓ to make the math easier.
The Economist has a great calculator showing your pre-vaccine, pre-Delta risk of hospitalization and death, given your age, sex, and comorbidities. Note that this calculator only includes diagnosed cases, so it excludes both asymptomatic cases and those that did have symptoms but didn’t drive people to seek medical care. Here’s a few sample people:
- A healthy 30 year old man has a 2.7% chance of hospitalization, and <0.1% risk of death
- A healthy 30 year old woman has a 1.7% chance of hospitalization, and <0.1% risk of death
- A 25 year old man with asthma has a 4.2% risk of hospitalization, and <0.1% risk of death
- A 40 year old woman with obesity has a 6.5% risk of hospitalization, and 0.1% risk of death.
- Risk of hospitalization rises steadily with age but the risk of death doesn’t really take off until 50, at which point our healthy man has a death risk of 0.4% and our health woman has a risk of 0.2%
If you’d like, you can use your own numbers in this guesstimate sheet.
And again, that’s only for officially diagnosed and registered cases. If you assume ⅓ of infections in that age group are asymptomatic, the risk drops by ⅓.
If you are hospitalized, your risk of being ventilated is currently very, very low even if you’re in a high risk category. The overall average percent of hospitalized patients who were ventilated was 2.0% in the last week for which data was available (2021-03-24), after dropping steadily for most of the plague. We can assume that’s disproportionately among the elderly and people with severe comorbidities, so if that’s not you your odds are better still. I’m going to count the risk of intubation for our cohort as 0.5%, although that’s likely still an overestimate.
How do vaccines change these odds? According to CDC data from a time period ending 2021-05-01 (so before delta took off), 27% of breakthrough infections that reached the attention of the CDC were asymptomatic, and only 7% were hospitalized due to covid (another 3% were hospitalized for non-covid reasons). It’s very likely that the CDC is undercounting asymptomatic cases, so we’ll continue using our ⅓ number for now. The minimum age of reported breakthrough infection deaths was 71, so we’ll continue to treat the risk of death as 0% for our sample subjects. Additionally, given the timing most vaccinated participants would be elderly or front line workers, raising their risk considerably. A CDC press release goes much farther, saying vaccinated people > 65 had 7% of the hospitalizations of age-matched controls.
How does delta change these odds? A Scottish study estimated delta had 2x the risk of hospitalization as alpha, which a Danish study estimated as having 1.42x the risk of hospitalization as baseline covid. So very roughly, we’re looking at 3x the risk of hospitalization from delta, relative to baseline.
So for our sample cases above, we have the following odds (note I updated these on the night it was posted, due to a math error. Thanks to Rob Besinger for catching it):
| Risk given vaccine, delta | Hospitalized | Intubated |
| Healthy 30yo man | 0.38% = 2.7*.07*3*2/3 | .002% = 0.38*.005 |
| Healthy 30yo woman | 0.24% = 1.7*.07*3*2/3 | .002% = 0.24*.005 |
| Asthmatic 25yo man | 0.58% = 4.2*.07*3*2/3 | .003% = 0.58*.005 |
| Obese 40yo woman | 0.92% = 6.5*.07*3*2/3 | .005% = 0.92*.005 |
That’s not so far from the rate of hospitalization in that age range for the flu (0.6%), with some caveats (the CDC sample includes unvaccinated people and the bucket is 18-49 years old, with the higher end presumably carrying more of the disease burden).
There is concern that vaccine effectiveness wanes over time, which I haven’t incorporated here.
Odds of long term outcomes
In general I ignored studies that merely tracked number of persistent sequelae but not their severity or type, which made it impossible to distinguish between “sense of smell still iffy” from “permanent intellectual crippling”, and studies that didn’t track how long the sequelae persisted. This was, unfortunately, most of them.
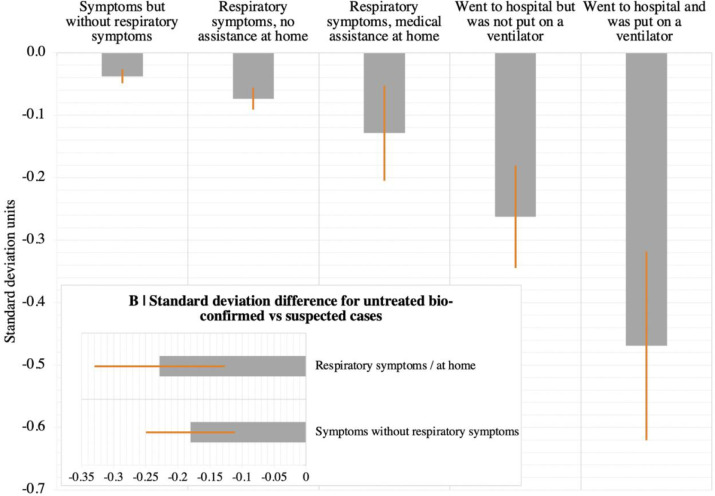
We talked about the Great British Intelligence Test above. I initially found this study quite scary. The study used its own tests rather than IQ, but if you assume a standard deviation in their tests is equivalent to a standard deviation in an IQ test, the worst category (ventilation) is equivalent to a 7 point IQ loss. That’s twice as bad as a stroke in this study (although I suspect sampling bias). I suspect the truth is worse still, because the worse your recently acquired cognitive and health issues are, the less likely you are to take a fun internet test advertised as measuring your intellectual strengths. However as I noted above, you are extremely unlikely to be put on a ventilator.
For people with “symptoms, but not respiratory symptoms”, the cognitive damage is ~equivalent to 0.6 IQ points. For “medical assistance at home”, it’s 1.8 points. These are both likely to be overestimates given that the study only included known (although not necessarily formally diagnosed) cases. Additionally, while the paper claims to control for education, income, etc, bad things are more likely to happen to people in worse environments, and it’s impossible to entirely back that out.
Taquet et al used electronic health records to get a relatively unbiased six figure sample size, and found unhospitalized diagnosed covid patients (pre-Delta, pre-vaccine) had a 11% likelihood of a new neuro or psych diagnosis after their covid diagnosis, hospitalized patients had a 15% likelihood, and ICU patients had 26% likelihood. The majority of these were mood disorders (3.86%/4.49%/5.82% for home/hospitalized/ICU) and anxiety (6.81%/6.91%/9.79%). This seems quite bad, until you compare it to the overall numbers for depression in the time period, a naive reading of which suggests that covid had a protective effect
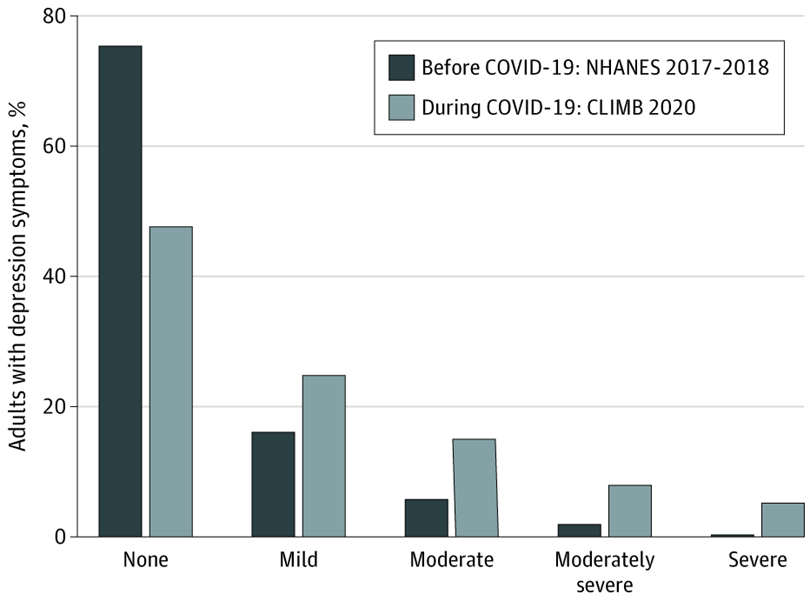
These numbers aren’t directly comparable. The second study is much lower quality and includes rediagnoses (although the total depression diagnosis numbers for the covid patients are 13.10%/14.69%/15.43%- still under the total increase in depression in the general population study).
Overall this seems well within what you’d expect from getting a scary disease at a scary time, and not evidence of widespread neuro or psych impact of covid. Even if you take the numbers at face value, they exclude most people who were asymptomatic or treated at home without a formal diagnosis.
A UK metareview found the prevalence at 12 weeks of symptoms affecting daily life ranged from 1.2% (average age: 20, minimum 18) to 4.8% (average age: 63). The cohort with average age 31 had a mean prevalence of 2.8%. This is based on self-reports on survey data, which will again exclude asymptomatic cases- if you use the ⅓ figure and assume no long covid among the asymptomatic, that becomes 1.8% of 25-45 year olds with covid developing long covid that affects their daily life, which is well within the Lizardman Constant.
On the other hand, medicine is notoriously bad at measuring persistent, low-level, amorphous-yet-real effects. The Lizardman Constant doesn’t mean prevalences below 4% don’t exist, it means they’re impossible to measure using naive tools.
Comparison to other diseases
The Taquet study did compare covid patients to those with other respiratory diseases (including the flu, not controlling for disease severity or patient age), and found covid to be modestly worse except for myoneural junction and other muscular diseases, where covid 5xed the risk (although it’s still quite low in absolute terms). Dementia risk is also doubled, presumably mostly among the elderly.

Additionally, cognitive impairment following critical illness, and especially following intubation, is a well known phenomenon. This puts the Great British Intelligence Test numbers in perspective- being/needed to be ventilated is quite bad, but it’s always been that bad, there doesn’t appear to be any unique-to-covid badness.
Conclusion
My tentative conclusion is that the risks to me of cognitive, mood, or fatigue side effects lasting >12 weeks from long covid are small relative to risks I was already taking, including the risk of similar long term issues from other common infectious diseases. Being hospitalized would create a risk of noticeable side effects, but is very unlikely post-vaccine (although immunity persistence is a major unresolved concern).
I want to emphasize again that “small relative to risks you were already taking” doesn’t necessarily mean “too small to worry about”. For comparison, Josh Jacobson did a quick survey of the risks of driving [LW · GW] and came to roughly the same conclusion: the risks are very small compared to the overall riskiness of life for people in their 30s. Josh isn’t stupid, so he obviously doesn’t mean “car accidents don’t happen” or “car accidents aren’t dangerous when they happen”. What he means is that if you’re 35 with 15 years driving experience and not currently impaired, the marginal returns to improvements are minor.
And yet. I have a close friend who somehow got in three or four moderate car accidents in < 7 years, giving her maybe-permanent soft tissue damage (to answer the obvious question: no, the accidents weren’t her fault. Sometimes she wasn’t even driving). Statistically, that friend doesn’t exist. No one gets in that many car accidents that quickly without it being their fault. And yet the law of large numbers has to catch up with someone. Too small to measure can be very large.
What this means is not that covid is safe, but that you should think about covid in the context of your overall risk portfolio. Depending on who you are that could include other contagious diseases, driving, drugs-n-alcohol, skydiving, camping, poor diet, insufficient exercise, too much exercise, and breathing outside. If you decide your current risk level is too high, or are suddenly realizing you were too risk-tolerant in the past, reducing covid risk in particular might not be the best bang for your buck. Paying for a personal trainer, higher quality food, or a HEPA filter should be on your radar as much as reducing social contact, although for all I know that will end up being the best choice for you personally.
Change my mind
My own behavior and plans have changed a lot based on this research, so I’m extremely interested in counterarguments. To make that easy, here’s a non-exhaustive list of things that would change my mind:
- Evidence that long covid gets worse over time, rather than slowly improving (note that I did look at data from SARS 1 and failed to find this).
- New variants increase the risk to what it was or was feared to be in April 2020
- Evidence of more severe vaccine attenuation than we’re currently seeing.
- Credible paths through which the risk could drop shortly in the next six months.
Thanks to LessWrong and Redwood Research for funding this research, and to Connor Flexman and Ray Arnold for comments on drafts.
40 comments
Comments sorted by top scores.
comment by Ruby · 2021-09-02T15:22:10.879Z · LW(p) · GW(p)
[A little late, but still worth saying.] (Speaking as a moderator). We've varied our policy of frontpaging Covid content over time. Initially we frontpaged Covid content at the beginning of the Pandemic (an exception to the general "timelessness" requirement for frontpage posts) since the info was important and in demand. As thing quietened down, we relegated Covid content back to Personal blog.
Since Long Covid is a topic of great concern for many, I am again making an exception and frontpaging top posts that discuss Long Covid like this one and Covid 9/2: Long Covid Analysis [LW · GW].
As always, you can modify your frontpage tag settings to either ensure you see all Covid posts, never see Covids, or something in between.
↑ comment by Eli Tyre (elityre) · 2021-09-05T10:03:11.645Z · LW(p) · GW(p)
Thank you for being thoughtful about how to serve the community's needs!
comment by Ruby · 2021-09-06T02:46:19.628Z · LW(p) · GW(p)
Curated. Our usual policy is to only draw attention to posts that are "timeless" (not just of interest at a particular time); however, we have been making exceptions for exceptional posts about Covid that might significantly impact decisions people are making.
comment by Naryan Wong (naryan-wong-1) · 2021-09-13T21:30:57.701Z · LW(p) · GW(p)
Wanted to share another (IMO) decent review of long covid risks from Thomas Pueyo: https://unchartedterritories.tomaspueyo.com/p/long-covid-chronic-fatigue-syndrome
I think his relevant conclusion looks something like this: Long COVID can look remarkably similar to Chronic Fatigue Syndrome, which REALLY sucks and you do not want to get it, but for a double-vaxxed person who catches COVID, the risks of this kind of outcome are between 0.20%-0.75%.
For anyone interested, he's also got some fresh sources to back up his thinking.
Replies from: Sameerishere↑ comment by Sameerishere · 2021-09-13T22:39:13.130Z · LW(p) · GW(p)
Thanks for sharing this! Added it to my post of summary snippets here: https://www.lesswrong.com/posts/jfHZR6Ykmc5DBSLCp/cliffs-notes-how-much-should-fully-vaccinated-people-care [LW · GW]
Seems like Pueyo's conclusion would support a similar level of risk tolerance as Elizabeth's analysis, would you agree?
comment by Josh Jacobson (joshjacobson) · 2021-09-20T23:23:12.147Z · LW(p) · GW(p)
It’s very likely that the CDC is overcounting asymptomatic cases, so we’ll continue using our ⅓ number for now.
Shouldn't this say "undercounting"?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-21T07:01:48.540Z · LW(p) · GW(p)
yes, thank you
comment by Isaac King (KingSupernova) · 2021-09-06T16:11:03.859Z · LW(p) · GW(p)
so it includes both asymptomatic cases
I think that "includes" should be "excludes"?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-06T18:03:50.188Z · LW(p) · GW(p)
You're right, thank you. I fixed it on my blog and thought LW had picked it up but apparently not.
comment by MichaelStJules · 2021-09-01T12:37:45.323Z · LW(p) · GW(p)
Thanks for writing this!
My impression is that we're much less likely to catch other infectious diseases that are nearly as severe in the long term (except maybe Lyme?), and unless your probability of catching COVID is very low, your risks from COVID seem worse than driving. This is based on a few people's separate BOTECs for long COVID [LW · GW] and my own (vague and personal, not well-researched) impression of how common and bad other infectious diseases are.
Note that a lot of other infectious diseases have become rarer under lockdowns, too, and that's something to account for. If someone has had an infectious disease in the past month, I'd guess it's reasonably likely to be COVID, given its high transmissibility. If someone who's been fully vaccinated for > 1 month has had an infectious disease in the past month, I'm not sure, I'd have to do the math. Going forward, COVID seems likely to be one of the most common infectious diseases going around.
What (similarly addressable or more easily addressable) risks do you think add up to being worse? Or, do you have an overall risk estimate to compare?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-01T21:23:47.272Z · LW(p) · GW(p)
What (similarly addressable or more easily addressable) risks do you think add up to being worse? Or, do you have an overall risk estimate to compare?
This question feels like a type error to me. My claim isn't "we precisely measured a bunch of risks and covid didn't make the top 5", it's "our measures of damage are not sufficiently precise to measure the danger of breakthrough covid against the accumulated risks we take elsewhere". Additionally, which risks are worth lowering depends heavily on the individual, both what risks they were already taking and how much joy those risks bring them.
That said, I personally am focusing my energy on exercise, air quality, fixing the vaccine-induced chest congestion, and diet.
Replies from: MichaelStJules↑ comment by MichaelStJules · 2021-09-02T07:24:21.455Z · LW(p) · GW(p)
Sorry, I was responding to this, but forgot to quote it:
My tentative conclusion is that the risks to me of cognitive, mood, or fatigue side effects lasting >12 weeks from long covid are small relative to risks I was already taking, including the risk of similar long term issues from other common infectious diseases.
(emphasis mine)
My expectation is that compared to other infectious diseases, (long) COVID is
- Much much worse, but less common (e.g. cold), or
- Much worse and about as common (e.g. flu), or
- Not as bad, but much much more common.
And these together make it seem reasonably likely to me that (long) COVID risk is not small relative to (long) risks from other common infectious diseases together.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-04T19:42:05.403Z · LW(p) · GW(p)
Some very quick numbers (populations may overlap):
- 13.15 CFS diagnoses per 100,000 person-years (13.58 if you include idiopathic fatigue)
- 430 fibromyalgia diagnoses per 100,000 person-years
- 10-20% chance of "failure to treat" acute Lyme, given Lyme
- 30-80% chance of post-ICU syndrome, given admission to ICU (but that's not tracking the counterfactual). There are ~4 million ICU admissions in the US per year, although those have a heavy long tail.
- Lifetime chance of 30% for shingles (which is a manifestation of dormant chicken pox), although that should be trending down with the chickenpox vaccine. 10%-18% of people who develop shingles will develop postherpetic neuralgia (another source has lifetime chance of postherpetic neuralgia at 20%).
- 500 traumatic brain injuries per 100,000 person-years (albeit concentrated amoung children) of which 26-30 will create a long term disability and 17 will cause death.
↑ comment by MichaelStJules · 2021-09-06T15:03:42.721Z · LW(p) · GW(p)
Ok, ya, some of these seem roughly within an order of magnitude of long COVID (higher or lower, since there's a lot of uncertainty).
I think it's worth mentioning that some of the risks here are more concentrated in older people, but can still be within an order of magnitude of COVID risk for people around my age (28). I would guess only Lyme and CFS would be concerning for a healthy person in their early 20s who doesn't take excessive risks of physical injury (low brain injury and post-ICU syndrome risk). I do wonder about recreational drug use, especially binge drinking (I never drank, so this was never a risk for me) and bike riding.
I'm not sure what I can do about CFS, fribromyalgia and shingles other than maintain a healthy lifestyle (diet, sleep and exercise), which I already am trying to do (but I suppose could be doing more), and I recognize is part of the point of your article. Maybe there's some link between CFS and viral infections (Epstein-Barr, herpes), so I could try to avoid those. I've already had chickenpox, so I'm not sure what else I can do about shingles.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-07T09:40:54.406Z · LW(p) · GW(p)
This isn't cruxy for me, but:
- 95% of healthy people have been infected with Epstein-Barr, it just doesn't have acute symptoms in many people
- Both Epstein-Barr and chickenpox are herpes viruses, all of which establish residence in your cells forever. "Postherpetic" doesn't necessarily mean HSV1/2, it includes multiple viruses that are (EB, cytomegalovirus) or were (chickenpox, pre-vaccine) nearly impossible to avoid without living in a bubble.
comment by George3d6 · 2021-09-10T18:18:56.967Z · LW(p) · GW(p)
Tangential but: sorry to hear about the nerve endings damage thing :/ I got something like that because I made the (in hindsight potentially dumb) move to pull out a wisdom tooth and adjecent tooth.
Dentist was not the best and the tug fucked up a nerve.
Not as bad as your case, but occasionally it gives a very "creepy" feel and a bit of pain.
What I can stay is that being mindful to the pain always seems to drive it away, this doesn't work with other types of pain. So unlikely but if you can't find anything else, it might be worth a shot to see if close examination can "cure" it.
comment by jmh · 2021-09-08T03:47:09.479Z · LW(p) · GW(p)
I just scanned the post and comments so may well have missed it. I would think these studies are looking at early in the pandemic patients (perhaps wrong to think that) so just wonder if there is any control over the treatment of the patients in the early days that might have biased the results at all?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-08T09:41:38.999Z · LW(p) · GW(p)
Quite possibly- the frequency of intubation certainly went down over time, and my overall impression is we've gotten better at treating covid over time.
comment by MichaelStJules · 2021-09-02T19:12:16.045Z · LW(p) · GW(p)
This is based on self-reports on survey data, which will again exclude asymptomatic cases- if you use the ⅓ figure and assume no long covid among the asymptomatic, that becomes 1.8% of 25-45 year olds with covid developing long covid that affects their daily life, which is well within the Lizardman Constant.
On the other hand, medicine is notoriously bad at measuring persistent, low-level, amorphous-yet-real effects. The Lizardman Constant doesn’t mean prevalences below 4% don’t exist, it means they’re impossible to measure using naive tools.
1.8% seems similar to the lower risk difference estimates between cases and controls I've seen (EDIT: 1.8% is the absolute risk, not a difference with controls), and I would guess the point with the Lizardman Constant you make here might not apply to risk differences between cases and controls, unless you want to claim that the constant differs between these two groups. I don't think this is entirely implausible, although I'd lean against it accounting for most of these risk differences, and I'd guess selection effects or controls that aren't good enough would be the most likely ways to explain away most of the long COVID risk difference estimates as actually nothing.
I'm guessing it's so low because of the "affects their daily life" (so risk difference estimates are measuring things not as severe or less frequent, and you filtered these out), or maybe just noise, studies from some samples being unrepresentative, etc.. This should give us a rough upper bound on the risk difference.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-02T19:57:11.921Z · LW(p) · GW(p)
For this metareview it's the absolute percentage, not a comparison. I'm interested in the other studies you think show a similar number relative to a control group.
Replies from: MichaelStJules, Lanrian↑ comment by MichaelStJules · 2021-09-02T21:12:53.226Z · LW(p) · GW(p)
For this metareview it's the absolute percentage, not a comparison.
Woops, sorry, I didn't mean to suggest otherwise.
I'm interested in the other studies you think show a similar number relative to a control group.
Hmm, I only remember this one with a similar number and controls, off the top of my head (I might have been thinking of similar numbers for something else):
https://www.nature.com/articles/s41586-021-03553-9 (I'm focusing on Positive cases in figure 3, who are not hospitalized; I think this paper has gotten relatively more attention in the community; see this comment [LW(p) · GW(p)])
Some others are discussed here, mostly higher estimates, like 5x-10x higher, though:
- https://www.medrxiv.org/content/10.1101/2021.03.18.21253633v2.full-text, also discussed here [LW(p) · GW(p)] and in a reply here [LW(p) · GW(p)] (healthcare workers)
- https://jamanetwork.com/journals/jama/fullarticle/2778528 (healthcare workers)
- https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1april2021 / https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1007511/S1327_Short_Long_COVID_report.pdf, two links for the same study on a UK sample, specifically these quotes and column ONS-CIS [3][6] in Table 1 in the second link:
Among a sample of over 20,000 study participants who tested positive for COVID-19 between 26 April 2020 and 6 March 2021, 13.7% continued to experience symptoms for at least 12 weeks. This was eight times higher than in a control group of participants who are unlikely to have had COVID-19, suggesting that the prevalence of ongoing symptoms following coronavirus infection is higher than in the general population.
Of study participants who tested positive for COVID-19, symptom prevalence at 12 weeks post-infection was higher for female participants (14.7%) than male participants (12.7%) and was highest among those aged 25 to 34 years (18.2%).
In contrast, the ONS study compared persistent symptoms lasting 12+ weeks using a survival analysis approach between confirmed COVID-19 cases and age- and sex-matched non-COVID controls, with estimates of 13.7% in cases and just 1.7% in controls.
Prospective versus retrospective data collection: Prospective data collection on ongoing symptoms on a daily basis was uniquely performed in the COVID Symptoms Study, which had the lowest estimates of proportions of cases affected, (2.3% for >12 weeks symptoms).[1] Unpublished analysis of the same individuals asked retrospectively about symptoms using the same questionnaire as in CONVALESCENCE cohorts (inclusive method) revealed very similar proportions with symptoms lasting >12 weeks, ranging from 6% of COVID+ cases in men aged 20-30 to 16% in women aged 40- 50. The COVID Symptoms Study did not count symptoms re-emerging after a week of reporting no symptoms, but although relapse rates were higher in the case population (16.0%) versus non-COVID controls (8.4%; P < 0.0005), this does not account for the difference in reporting rates and suggests that recall bias may operate in retrospective self-reports of symptom duration. The ONS study of persistent symptoms in confirmed infections was based on prospective data [3](symptoms experienced in the last week, collected each week for the month from enrolment and then each month for up to a year); whereas symptom durations for the population prevalence estimate [6] is based on retrospective reporting of the initial (confirmed or suspected) infection.
Another I got from Scott's article (which summarizes risk estimates from several and discusses biases): https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2776560
↑ comment by Lukas Finnveden (Lanrian) · 2021-09-02T20:18:59.515Z · LW(p) · GW(p)
The 1.8% number comes from your own calculations, though, right? Shouldn't we be comparing the lizardman constant with the reported percentages, rather than this calculated number?
In this case, that might be 2.8%. But I don't know what the methodology of the survey was. If they just asked a bunch of random people and got them to self-report whether they had covid; maybe we should actually use the percentage of people who claimed to have long covid among everyone asked, which could be lower than 1.8%.
Of course, all of these numbers are smaller than the lizardman constant anyway.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-03T17:59:22.112Z · LW(p) · GW(p)
You're right, will make this correction in the main article and then get LW to pull it over.
comment by simongcox@gmail.com · 2021-09-19T19:03:57.729Z · LW(p) · GW(p)
Thanks for the article. I was particularly interested to hear your vaccine side-effects. I have been having the same response - chest congestion - for the last couple of months. I've not been able to find much information on this subject as the web is full of covid conspiracy theories rather than good science. The CDC and WHO list no chronic side effects. Have you been able to find any good information on this? Which vaccine did you have?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-19T19:39:55.129Z · LW(p) · GW(p)
When I went to urgent care over this they said they were seeing a lot of people with post-vaccine complaints (no denominator, obviously) and kept being surprised I didn't have fatigue. I think they also expected brain fog but am less certain of that. I haven't looked very actively for more because the signal: noise ratio is so bad.
My doctor gave me a glutathione nebulizer and I went on a vitamin stack I'll be writing up at my blog soon (and will probably make its way to LessWrong) and have talked about a little on twitter already.
I had Pfizer, with typical scheduling.
comment by Algernoq · 2021-09-09T05:41:34.991Z · LW(p) · GW(p)
Mad-Eye Moody had once worked out how long it had taken him, in retrospect, to achieve what he now considered a decent level of caution - weighed up how much experience it had taken him to get good instead of lucky - and had begun to suspect that most people died before they got there.
You are here to learn how to defend yourselves against the Dark Arts. Which means, let us be very clear on this, defending yourselves against Dark Wizards.
My sense is that the political risk exceeds the disease risk.
comment by t0ben · 2021-09-01T08:27:45.609Z · LW(p) · GW(p)
My cold response and heart rate variability has also changed very significantly / https://physoc.onlinelibrary.wiley.com/doi/10.1113/JP281888
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-01T08:58:57.539Z · LW(p) · GW(p)
They don't explicitly give dates for data collection, but based on "8 months after the disease was declared a pandemic" and the age of the participants, it would be shocking if they were vaccinated.
comment by Jonathan_Graehl · 2021-09-01T08:51:02.846Z · LW(p) · GW(p)
Your contrary cite notwithstanding, I predict Delta will end up less damaging on average and more cases will go uncounted due to its mildness. This may also drive some overestimation of its virulence. It does appear to spread well enough that is a question of when not if you'll be exposed.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-09-01T09:00:16.495Z · LW(p) · GW(p)
What are you basing that lower virulence on?
comment by ChristianKl · 2021-09-01T14:04:53.717Z · LW(p) · GW(p)
Credible paths through which the risk could drop shortly in the next six months.
In India, Uttar Pradesh (population of 204.2 million) managed to reduce COVID incidence by 3 orders of magnitude since the start of May.
Currently, there's no political willingness to copy their policies to reduce COVID in the US or in Europe but it's plausible that after additional studies or public discussion we will copy their policies and get the same results.
Replies from: pktechgirl, dave-orr↑ comment by Elizabeth (pktechgirl) · 2021-09-01T19:22:24.486Z · LW(p) · GW(p)
What's the QALY (including emotional and financial) hit of the policies necessary to achieve that drop?
Replies from: ChristianKl↑ comment by ChristianKl · 2021-09-02T07:42:10.661Z · LW(p) · GW(p)
The metastudy we have suggests that low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by an average 86% (95% confidence interval 79%–91%).
Uttar Pradesh gives everybody prophylatic ivermectin so it's plausible that it's the determining factor for the success that they have.
Ivermectin is out of patent and can be produced relatively cheaply so that an Indian region with a lot of poor people can afford to give it to everyone. It's unclear how much it would cost given how Western states buy medicine. There's little emotional cost involved.
There are currently a few Ivermectin studies that are running and them reporting results might shift Western policy.
Replies from: Mitchell_Porter, pktechgirl↑ comment by Mitchell_Porter · 2021-09-02T08:10:20.186Z · LW(p) · GW(p)
Uttar Pradesh gives everybody prophylatic ivermectin
All I can find is that when people show symptoms or have been exposed, they are given a home isolation kit with 7 days of medical supplies that include ivermectin. Is that what you mean?
Replies from: Lanrian, ChristianKl↑ comment by Lukas Finnveden (Lanrian) · 2021-09-02T20:08:02.422Z · LW(p) · GW(p)
This page (I don't know how trustworthy it is) claimed on 19th May:
“Three days [ago] Goa issued a Government Order for mass prophylaxis using ivermectin for the people of Goa”, said Dr Suryakant. Goa is the first state in India to use ivermectin in this way, he emphasised. Uttar Pradesh was the first state to issue a Government Order for the use of ivermectin for treatment and prophylaxis for asymptomatic and mild cases of covid-19 and for prophylaxis of health care workers and home contacts.
↑ comment by ChristianKl · 2021-09-03T12:00:19.766Z · LW(p) · GW(p)
When I last looked more into Ivermectin and India I found that both https://www.newindianexpress.com/nation/2021/may/12/covid-19-uttarakhand-govt-to-distributeivermectin-tablets-to-allresidents-2301677.html and https://indianexpress.com/article/india/goa-prescribes-ivermectin-for-all-above-18-irrespective-of-symptoms-7310158/ are about decisions to generally give it to all people.
https://www.palmerfoundation.com.au/india-mumbai-move-for-ivermectin-prophylaxis-while-uttar-pradesh-smashes-covid-19-but-drugs-use-suppressed-in-media/ unfortuantely doesn't say exactly how often it was used in Uttar Pradesh but suggest it's use for prophylaxis at the end of May was enough to have a big effect. In my own reasoning them predicting three months ago that their strategy involving invermectin does the job matters.
↑ comment by Elizabeth (pktechgirl) · 2021-09-02T20:04:15.253Z · LW(p) · GW(p)
I downvoted this because, while I haven't ruled out ivermectin as a treatment and am actively angry at people dismissing it as a horse drug instead of engaging with the claims, I object to the way this comment slid the assumption that ivermectin was good but politically suppressed under the radar instead of stating it explicitly and making the case for it.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-09-03T06:32:48.089Z · LW(p) · GW(p)
Whether or not ivermectin is the cause for the point, doesn't really matter. If there another factor that's responsible for cases falling in an Indien state that still suggests that Delta cases falling is possible.
I object to the way this comment slid the assumption that ivermectin was good but politically suppressed under the radar instead of stating it explicitly and making the case for it.
It's following the classic advice of "politics is the mindkiller". Focus on the fact that there's something getting the cases down without pointing to the political charged part.
I do think it's good if people take an unbiased look at the fact that Uttar Pradesh managed to bring their case count down by three orders of magnitude.
Replies from: finolex1↑ comment by finolex1 · 2021-09-03T13:02:22.972Z · LW(p) · GW(p)
Isn't the more likely reason that about 75% of people in Uttar Pradesh had already been exposed to the virus or vaccinated by late July, as shown by the national serological survey findings?
https://indianexpress.com/article/explained/explained-icmr-covid-fourth-serosurvey-findings-7413949/
Other north indian states also show similar drastic drops, and I doubt all of them administered prophylactic invermectin.
↑ comment by Dave Orr (dave-orr) · 2021-09-01T18:20:18.755Z · LW(p) · GW(p)
I think seasonality is going to push in the other direction for a while. I think in 7-8 months things could plausibly be much better, in fact I think it's likely, but February is still very winter.