COVID/Delta advice I'm currently giving to friends
post by Rob Bensinger (RobbBB) · 2021-08-24T03:46:09.053Z · LW · GW · 31 commentsContents
1. Figure things out for yourself 2. Be much more wary of COVID when hospitals are full 3. Consider mostly not worrying about it 4. If you do worry about it... 5. Try to get triple-vaccinated 6. Right now is the safe time 7. Small exposures are better than large exposures, and maybe better than no exposure? 8. Be aware of possible signs of COVID 9. Be prepared for if you get pretty sick 10. Take care of yourself if you get sick None 31 comments
[Epistemic status: US-centric. gathering various impressions even though I haven't deeply investigated this topic and am not an expert, so it's all in one place and others can better use or critique the claims.]
1. Figure things out for yourself
Figure out what risk level you're comfortable with, and use microCOVID.org to get a sense of what policy makes sense for you personally.
Consider sharing your Fermi estimates with others (e.g., make a small Facebook group or chat for the purpose, or a LW thread if you're happy to do it publicly). This is a way to compare notes, get feedback, and share info without there needing to be a single big Policy Proposal For Everyone blog post people are passing around.
2. Be much more wary of COVID when hospitals are full
Keep an eye on confirmed COVID-19 cases, hospitalizations, and deaths in your area, and put effort into avoiding catching or transmitting COVID-19 if it looks like hospitals in your area will be overloaded 2-4 weeks from now.
3. Consider mostly not worrying about it
For young healthy vaccinated people in places with relatively good health care and relatively high vaccination rates (e.g., the US), if it doesn't look like your local hospitals will be overloaded in the next few weeks, then I think COVID-19 is mostly not worth worrying about right now.
(Likely exceptions: you're spending a lot of face-to-face time with an immunocompromised friend; you're visiting your seventy-five-year-old parents for the holidays in two weeks; etc.)
I emphasize this point mostly because my friends are in left/liberal spaces, where I think social forces encourage people to voice their "worry more" thoughts and keep quiet about their "worry less" thoughts.
This makes it extra valuable to speak up about "worry less" when you think it's true. (Though, again, all of this is too individual-specific for a public blog post to be able to say much about the exactly correct level of "worry".)
People in my social circle have mostly been taking large precautions throughout the pandemic. I see rationalist friends worrying a lot about whether it's OK to host get-togethers without rapid-testing all attendees (which I'd tentatively guess is not worth the trouble for the vast majority of gatherings). I see non-rationalist friends posting about how sad they are to not get to see friends again until things 'go back to normal'.
What I don't see are rough quantitative arguments for why the benefits are worth the costs here, especially ones that take into account the importance of social distancing's emotional costs (cf. Scott Alexander's Things I Learned Writing The Lockdown Post).
I don't see explanations of what 'going back to normal' looks like, and why we should expect that to happen at all (cf. Alyssa Vance on "we should distance until X").
Daniel Filan tells me that he initially locked down in response to COVID, but when he took the time to do a quick Fermi on the risks of COVID (around August 2020), he was surprised to find how costly his precautions were compared to their benefit:
[... M]y estimate [in late 2020] was that I should pay up to tens of cents to avoid a uCOVID.
I wasn't really modelling externalities well, and I'm still not totally sure how to do that right.
[...] TBC, the Fermi was something like "look up p(death | covid) given my age and sex, then estimate cost of other side effects as equal to cost of death, then add the cost of being normally sick for one week".
[T]hat being said, paying $100k to definitely not get covid seems pretty pricey.
My current guess: the cost per uCOVID [in late 2020] came out to under 10c, and I rounded up for caution or something.
See also Connor Flexman's Delta Strain: Fact Dump and Some Policy Takeaways [LW · GW], which (with a bunch of caveats and uncertainty) estimates that given Delta's ubiquity, a healthy vaccinated thirty-year-old who would otherwise live a full life now loses something like the equivalent of 1 hour of life for every 1,000–5,000 microCOVIDs they get.
I think the vaccines are remarkably effective (both vs. infection and vs. severe-symptoms-given-infection, which correlates with long COVID and death risks), and COVID wasn't a large risk for young healthy people in the first place (though Delta is a bigger risk than Alpha, ignoring effects of vaccination).
(Added Aug. 24: I think COVID risk for young vaccinated people isn't that different from the risk you face from other widespread viruses. In particular, my impression is that many (if not all?) viruses cause long-term symptoms similar to long COVID. Though at least in unvaccinated people, it seems that COVID causes long-term issues more often than the typical virus.
I know some people whose conclusion from this is "I'll try to avoid all viruses", including people who were taking such precautions pre-COVID. For healthy individuals, I don't have a strong view on whether that's more or less reasonable than mostly-ignoring this risk. But I am suspicious of the view that only and exactly COVID is worth worrying about.)
4. If you do worry about it...
... I would especially prioritize doing things outdoors.
I also think in-person friend groups, events, and group houses should consider restructuring to cater to people with this or that risk tolerance. The typical especially at-risk person, IMO, shouldn't be trying to get a huge community of people to all match their needs. Nor should they be bunkering down to "wait out COVID" and avoiding in-person socializing until then (unless they really don't want or need in-person socializing). Rather, I'd propose planning around the assumption that things will stay at least this risky for years to come, and build connections with other people who want to keep their risk low on that timescale.
(Added Aug. 24: The older you are, the higher your COVID risk generally is. Mayo Clinic says other major risk factors are: obesity, diabetes, heart disease (including hypertension), lung problems, cancer, sickle cell anemia, weakened immune system, chronic kidney or liver disease, and Down syndrome.)
5. Try to get triple-vaccinated
J&J seems to be much less effective than Pfizer/Moderna, so people who received J&J should especially prioritize getting two mRNA shots ASAP. But mRNA recipients should probably also get a third shot if their second shot was 4-6 months ago.
Will Eden re 'should people get a third shot, and if they had Pfizer/Moderna the first time should they try to have J&J this time around?':
The mechanisms for cell entry are a bit different, but they all end up using RNA to encode the S protein on the cell surface, so the nature of the immunity is basically the exact same mechanism. J&J is also going to immunize you against the vector virus, making it harder to receive future AAV vaccines/gene editing in the future, so personally I would stick to the mRNA vaccines only.
From the Israeli data it seems like a third shot is probably most effective around 5 months later for little or no lapse in coverage? I would recommend it personally and have to others already. Doing third shots is in trials, as is mixing different vaccines, both appear to work well.
In response to Zvi Mowshowitz's criticism of the Israeli data [? · GW], Will adds:
I do think there’s a reasonable point about the denominator problem, and how outbreaks began in more heavily vaccinated areas thus skewing the results downwards. But he also admits this means there are enough vaccine breakthroughs to cause a pandemic!
On the flip side, the discrepancy between protection against symptomatic COVID vs hospitalization/death I don’t agree with him on. I think a straightforward view of the data, especially the effectiveness of vaccine vs month of administration released by Israel, suggests that you need high circulating antibodies to prevent the infection from taking root at all, but prevention of severe disease is more reliant on cellular immunity and your body mounting a quick response after exposure, which is the benefit provided by vaccination. (On the other hand, this is why I want mucosal immunity - an optimal vaccine would even prevent infection + spread, and clearly the current vaccines don’t.)
Moderna seems to be better than Pfizer, perhaps because it uses a higher dose.
CNBC reports:
The United States will begin widely distributing Covid-19 booster shots next month as new data shows that vaccine protection wanes over time[...] U.S. agencies are preparing to offer booster shots to all eligible Americans beginning the week of Sept. 20, starting eight months after their second dose of Pfizer or Moderna’s vaccines.
But this seems too slow to me, given the next section. (My family and peers would nearly all have to wait till Nov/Dec/Jan.) So I still suggest trying to get a third shot sooner.
6. Right now is the safe time
COVID seems to be quite seasonal -- it spreads a lot more in the winter. To think about the coming months, I looked at COVID rates where I'm living:
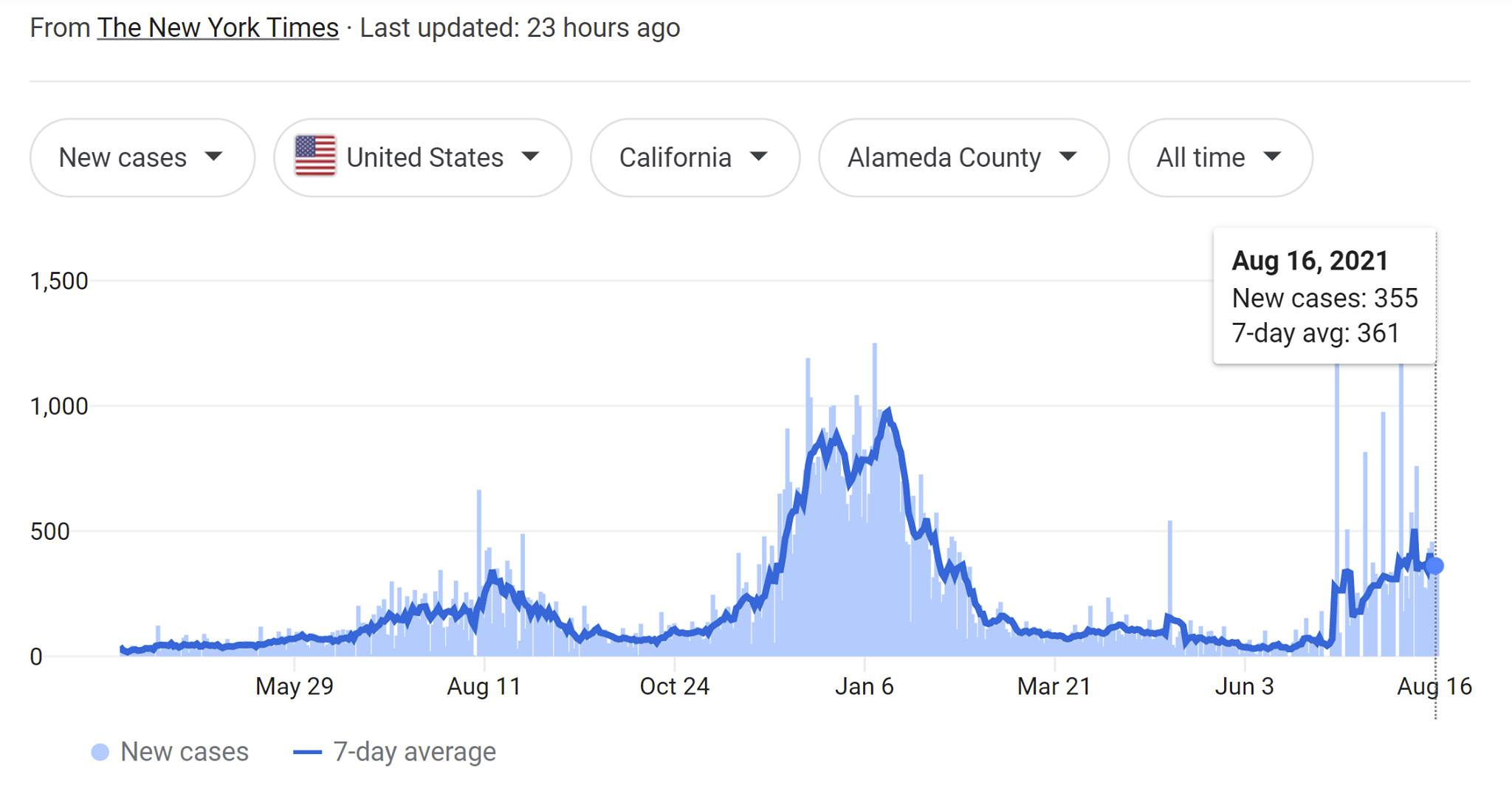
Based on this, I expect this coming Nov/Dec/Jan/Feb to be way worse again around SF. Except the baseline is much higher now, so I expect the elevated case rate to likewise be much higher.
I think most people who track these things are looking at the current COVID rates, seeing they're a lot higher than in the past, and concluding that we should be buckling down temporarily right now.
Except that the rise is because Delta took over, and Delta is the new normal going forward. So if you're planning to throw some parties before March 2022, now is very likely the best time to do it. If you're planning to "buckle down temporarily" and "temporarily" means "a few months" rather than "a few years", you may want to reconsider whether things will actually look any better five or ten months from now.
Eyeballing NYC, it looks like things may be bad in some parts of the US even in May?

Beyond seasonality, other things that may make things worse in the future include:
- Fading vaccine efficacy, if that's a thing. Even if you personally get more shots, others may not.
- In general, my tentative default guess (if something like the status quo continues) is that people's willingness to get more COVID booster shots will drop off a lot over the coming months and years. (Because it will feel more like an annoying regular chore than like a miracle cure.)
- New COVID strains.
- Regulatory hurdles inhibiting and delaying vaccine roll-out.
I'm not especially worried about long COVID, because I expect long COVID frequency and severity to track symptom severity pretty closely -- if vaccines protect against severe symptoms, they'll tend to reduce long COVID risk too.
Even in the best-case scenario, there's a delay between "new COVID strain evolves" and "new vaccine targeted at that strain rolls out," and a further delay before we get data on long COVID in people infected by that strain (either for vaccinated or unvaccinated people), which makes it harder to be confident about the risks.
Or perhaps not. The future could hold a lot of things. But in my own planning, I'll be acting like most of the probability mass is on 'things stay about the same for a long time, or get worse'. I mostly am planning around the expectation that this is life going forward, and I'm not going to shut down my life indefinitely -- but I can plan around taking more risks during warmer months, and fewer risks during colder ones.
7. Small exposures are better than large exposures, and maybe better than no exposure?
This is a probably a relatively good time to get infected if the trend "COVID evolves to be more dangerous and high-viral-load" continues. Getting infected with a lower viral load is better, and may confer a lot of immunity against future variants.
By the same logic, if you expect to get infected with Delta regardless in the next few months (as a large portion of the US presumably will), it's better if your exposures tend to be in low-risk settings where you'll get a small initial viral load. (And it's better to get sick when you know hospitals won't be overloaded.)
8. Be aware of possible signs of COVID
(Added Aug. 24.)
According to CBS, an August CDC study found that the most common symptoms of Delta are still "cough, headache, sore throat, myalgia [muscle pain], and fever". Oddly, the COVID Symptom Study instead found that the most common Delta symptoms were runny nose, headache, sneezing, sore throat, and loss of smell.
But: don't assume people are COVID-free just because they're showing no symptoms. COVID is often asymptomatic (or the symptoms are hard to notice), and people with COVID transmit the illness a lot before they start showing symptoms.
If you might have COVID, self-isolate and try to get tested. PCR tests are the most reliable, but they have to be sent to a lab and normally take days to give back a result. Also, Connor Flexman suspects [LW · GW] that PCR tests may still have a ~40% false negative rate, which is much higher than usually advertised. Antigen tests have something like a ~50% false negative rate, but can be done fully at home and give much faster results (within a few minutes). LAMP tests like Lucira are also fast, and are in-between PCR and antigen tests in efficacy, according to Connor. (Flagging that these are very off-the-cuff numbers with minimal due diligence done; I'll revise them if the situation becomes clearer.)
Consider taking zinc lozenges soon after COVID exposure or symptom onset. (They should taste bad if they're working.)
9. Be prepared for if you get pretty sick
Things to buy now for if you get sick: Pedialyte or gatorade powder, acetaminophen or ibuprofen, oral thermometers, and a finger pulse oximeter.
Maybe also: over-the-counter inhalers, a humidifier, mucinex/guaifenesin, pseudoephedrin.
10. Take care of yourself if you get sick
(section in progress)
31 comments
Comments sorted by top scores.
comment by Rob Bensinger (RobbBB) · 2021-08-24T04:16:56.248Z · LW(p) · GW(p)
Response from Alex Altair to a social media post I wrote containing some of the claims above:
Replies from: moridinamael, malcolmocean, viking_math, ESRogsI feel quite strongly confused about why someone would think that future COVID risk might be permanently as high as it currently is. (You didn't say literally this, but you've said/shared a bunch of things that make me think that's what you believe; please correct me if I'm wrong!)
I will grant that it is physically possible; like, I'm not laboring under the illusion that there is some natural baseline risk that reality equilibrates to. The world could at any time become permanently more dangerous.
But like... that basically just doesn't seem to happen with diseases? Over the bazillion years of human history, a lot of pandemics have occurred, and none of them proceeded to continuously exist at the risk level that COVID is currently occurring. The flu did mutate and stick around mightily, but annual flu deaths are an order of magnitude lower than COVID.
I do fully expect COVID to become endemic at this point, and I don't think I ever believed we were going to eradicate it. But almost all diseases somehow end up receding to a very low level of daily risk, and I have no reason to think that COVID is different. So to me, the current case rates are clearly a spike of risk worth changing my behavior for, and worth waiting out. Not going to indoor unmasked parties is one of the easiest ways to reduce that risk.
[...]
I could imagine that the amortized case rates don't go down much over the next few years, but I do expect it to continue having these exponential rises and falls, such that one can efficiently reduce most of the risk (the current spike being one of those times).
↑ comment by moridinamael · 2021-08-24T12:27:28.435Z · LW(p) · GW(p)
I feel like the “diseases just naturally become not-dangerous” perspective neglects smallpox and other extremely deadly endemic viruses which we have used vaccination to control or eradicate.
↑ comment by MalcolmOcean (malcolmocean) · 2021-08-24T08:03:47.751Z · LW(p) · GW(p)
The flu did mutate and stick around mightily, but annual flu deaths are an order of magnitude lower than COVID.
Maybe this is what you're already saying, but I want to highlight something specific:
My understanding is this isn't about the virus mutating to become less deadly, but more because endemic viruses encounter non-naive immune systems, which is true for flus but not for sars-ncov-2 (so far). T-cells have basically lifetime memory I think (longer than antibodies?). This is similar to how european diseases were so devastating to indigenous folk (and I think vice versa in one case?) because of naive immune systems.
And this prepared defense effect might be stronger for people who actually got sick than folks who got the vaccine (I feel like I saw this somewhere but am very unsure) but in either case the odds of this being worse than the flu are now pretty low and it seems to me vaccinated folks should at this point treat covid roughly like the flu—get a shot now and then, and don't visit your grandparents if you think you might have it, but otherwise don't worry about it.
I'm getting much of this from this source, which bases its reasoning on various claims I'm not qualified to assess. Would love to hear others thoughts: Why COVID-19 Is Here to Stay, and Why You Shouldn’t Worry About It
↑ comment by viking_math · 2021-08-25T15:30:48.274Z · LW(p) · GW(p)
Hold on. That seems to be very wrong. The world became permanently more dangerous when smallpox, cholera, typhoid, measles, mumps, and the flu jumped to humans. That only stopped being true when vaccines were developed. I think it bodes pretty well for the outlook of COVID, if we keep vaccinating. But so far as I know, it's definitely not the case that smallpox ever became less deadly on its own.
↑ comment by ESRogs · 2021-08-24T16:54:02.273Z · LW(p) · GW(p)
I agree with Alex's first points, but it's not clear to me that this part follows:
So to me, the current case rates are clearly a spike of risk worth changing my behavior for, and worth waiting out.
It seems likely that there will be a spike this winter, but then by next summer (and the following winter) COVID will have faded to just being a flu-like minor consideration.
In which case, yeah this is not the new normal forever, but also it'll probably get worse one more time before it gets better.
Replies from: ESRogscomment by Dave Orr (dave-orr) · 2021-08-24T18:22:40.166Z · LW(p) · GW(p)
Based on this, I expect this coming Nov/Dec/Jan/Feb to be way worse again around SF. Except the baseline is much higher now, so I expect the elevated case rate to likewise be much higher
I'd like to register a prediction that in the Bay Area and in CA, rates will be drastically below where they are today in a couple of months.
The reason I think that is that everywhere else, we've seen delta skyrocket, and then collapse once the control system kicks in and herd immunity thresholds are reached as vulnerable people get infected. I think the same thing will happen here.
So contra the advice that this is the best time to do things, I think it's worth waiting. If I'm right we should see evidence in the next few weeks.
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2021-08-24T19:32:14.281Z · LW(p) · GW(p)
Could you quantify 'in a couple of months'? I don't have a strong view on exactly what Delta will look like between now and November -- I could pretty easily imagine it being about the same on average, slightly lower, slightly higher, or a decent amount higher, if no major surprises (e.g., a new strain displacing Delta) happen.
Off the cuff: In Alameda County, I'd maybe put 2/3 probability on at least 85% of weeks being between 5000 official new cases per day and 80,000 official new cases per day, until November?
And I'd separately predict with 70% probability the conjunction: (1) the average number of new Alameda County cases each day between Dec 15 and Jan 15 will be at least 1.5x the average number of cases in the last week of September; and (2) this Dec 15 - Jan 15 average will be at least 50,000 cases per day.
I wouldn't be at all surprised if there's a rise, followed by a collapse, followed by another (seasonally mediated) rise. I would be surprised if the collapse takes us far below 5000 official new cases per day -- I'd more expect the collapse to take us approximately back to present levels, or somewhat higher than present levels? But I don't feel super confident of any of this (hence my giving probabilities like 2/3).
Replies from: RobbBB, dave-orr↑ comment by Rob Bensinger (RobbBB) · 2021-10-03T04:55:49.956Z · LW(p) · GW(p)
In Alameda County, I'd maybe put 2/3 probability on at least 85% of weeks being between 5000 official new cases per day and 80,000 official new cases per day, until November?
Oops! I said "Alameda County" here, but I think I must have been thinking of CA, since I remember setting my lower bound (5000) at somewhat below case count at the time (in the chart I was looking at), whereas 5000 would have been massively higher than anything we've ever seen for Alameda. Hence my saying:
I would be surprised if the collapse takes us far below 5000 official new cases per day -- I'd more expect the collapse to take us approximately back to present levels, or somewhat higher than present levels
(There were ~400 new confirmed cases in Alameda County on the day I posted this comment, vs. 11,000 new confirmed CA-wide cases.)
Likewise, the second prediction doesn't make sense for Alameda County.
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2022-01-30T23:14:20.562Z · LW(p) · GW(p)
Replacing 'Alameda County' with 'California':
I could pretty easily imagine it being about the same on average, slightly lower, slightly higher, or a decent amount higher, if no major surprises (e.g., a new strain displacing Delta) happen.
A new strain did replace Delta.
In [California], I'd maybe put 2/3 probability on at least 85% of weeks being between 5000 official new cases per day and 80,000 official new cases per day, until November?
Looking at each Monday from Aug 23 through Nov 1 for what the NY Times says the weekly average was that day, I get:
- Aug: 16k, 14k
- Sep: 13k, 11k, 9k, 8k
- Oct: 7k, 6k, 6k, 4k, 9k
By that accounting, 10/11 = ~91% of weeks were in the 5000 - 80,000 range.
And I'd separately predict with 70% probability the conjunction: (1) the average number of new Alameda County cases each day between Dec 15 and Jan 15 will be at least 1.5x the average number of cases in the last week of September
Average in the last week of September was ~7241. 1.5x that is ~10862. On Dec 15 new cases were only 5365, so my prediction is falsified. Dec 20 cases jumped from 3582 to 19084, so CA cases have been in the range I mentioned starting Dec 20 rather than Dec 15. (And I expected a climb to start in early November, like it did in 2020, rather than in late December -- I mentioned 'Dec 15' because I expected this to give me more than enough buffer for seasonality effects to take over.)
and (2) this Dec 15 - Jan 15 average will be at least 50,000 cases per day.
Eyeballing the NYT graph, looks to me like the average was ~30k at the end of Dec, 50-60k first week of Jan, and 100k+ for most of Jan. (And again, with Omicron rather than Delta.)
↑ comment by Dave Orr (dave-orr) · 2021-08-24T22:00:06.479Z · LW(p) · GW(p)
Off the cuff: In Alameda County, I'd maybe put 2/3 probability on at least 85% of weeks being between 5000 official new cases per day and 80,000 official new cases per day, until November?
That's a good way to think about it. My 2/3rds confident window looks something like 1.5k-25k per day for most weeks until November. So substantially lower than yours.
For example, if we had the same infection rate as the UK (cases are down from delta peak) it would be 500 cases/day in Alameda county. The UK might be trending back up now, but the slope is much lower. Their vaccination rate is a little higher than Alameda county but our vaccines are better, so that's probably ~ a wash, or maybe slightly in the UK's favor.
this Dec 15 - Jan 15 average will be at least 50,000 cases per day
In other words, you think the average for that month will be equivalent to the worst week last winter before anyone was vaccinated? Definitely seems high to me. Delta is much worse, yes, but vaccines really do help quite a bit, I think.
I buy that seasonality is a thing for covid, but I think it will be more like 15kish rather than 50k for that month.
Replies from: RobbBB↑ comment by Rob Bensinger (RobbBB) · 2021-08-25T22:58:17.091Z · LW(p) · GW(p)
That seems reasonable to me, and updates me some toward your view. I feel confused about how rapidly cases fell in the UK. If this has something to do with levels of natural immunity in the UK, I could imagine that meaning the Bay Area has less protection. (~9.7% of the UK has been confirmed-infected, vs. I think ~6.3% of Alameda County.)
I'm also curious how 'lockdown culture' differs between Alameda County and the UK—Berkeley has seemed pretty COVID-cautious to me (which makes me think the control system could be more trigger-happy, resulting in fewer cases), but I'm not sure how to compare that to the UK.
comment by MichaelStJules · 2021-08-24T06:54:34.261Z · LW(p) · GW(p)
3. Consider mostly not worrying about it
There wasn't much discussion of long COVID here. At what risk of long Covid (including possibly chronic fatigue and brain fog lasting >6 months, up to the end of study periods, and possibly much longer) would you change your mind about this? I suppose it would still depend on your personal preferences, and how much you get out of certain activities (enjoyment and mental and physical health).
In my specific case (in Canada), I've decided to move out of my current dorm-style residence, since although it's pretty empty now, I would have been sharing a kitchen with 17 other people (although I've been told less than half of residents ever really use the kitchen), and a bathroom with 3 other people. I'd also expect there to be parties with outsiders here, too. I think it's likely that almost everyone would be vaccinated, though.
I think the evidence is somewhat ambiguous on long COVID rates at this point, even among the studies with actual comparisons/controls. A few of the higher quality studies with comparisons/controls were discussed here:
- https://www.nature.com/articles/s41591-021-01292-y
- https://jamanetwork.com/journals/jama/fullarticle/2778528
- https://www.medrxiv.org/content/10.1101/2021.03.18.21253633v2.full-text
- https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1april2021
I'd somewhat lean towards lower risk estimates, since I think higher ones are more likely to be biased due to poorly matched controls, selection bias or unrepresentative samples. On the higher end of studies with controls, one of them (of healthcare workers) had small/insignificant differences in mental health between positive and negative cases, but (most worrying to me)
Neurological symptoms of statistical significance included problems sleeping through the night (60.7% vs 51.5%), forgetfulness (35.0% vs 19.0%), confusion/brain fog/trouble focussing attention (
20.7%27.9% vs 14.7%), trouble trying to form words (15.7% vs 9.2%), short-term memory loss (20.7% vs 5.6%) and, less frequently, difficulty swallowing (6.4% vs 2.4%), twitching of fingers and toes (5.7% vs 2.4%) and trembling (5.7% vs 1.7%). Respiratory symptoms of interest included unusual fatigue/tiredness after exertion (39.3% vs 17.5%), breathlessness after minimal exertion (25.7% vs 10.2%), chest tightness/pain (18.6% vs 8.2%), fits of coughing (13.6% vs 6.5%) and breathlessness at rest (9.3% vs 2.8%).
See Table 2. Positive cases were more likely to be patient-facing frontline clinical healthcare workers (51.7% vs 23.0%), though, and maybe they were more exhausted and this explains it, but you'd think this would show up in their mental health, too. None of the cases were hospitalized for COVID.
See also this post on vaccination and long COVID [LW · GW] and this post in Bountied Rationality on Facebook.
From the Bountied Rationality post, these two were shared, among others:
- In a (small) sample of 39 breakthrough infections among fully vaccinated healthcare workers, 19% had symptoms lasting > 6 weeks. I haven't gone through in detail, but it doesn't look like they had a comparison group for this one.
- A large study of long COVID in non-hospitalized patients estimated risks and excess burdens of symptoms at 6 months. See Figure 3 where "Positive" indicates "non-hospitalized individuals with COVID-19". Dividing the excess burdens by 1000, fatigue looks like <2%, and they're all < 2.5%. EDIT: I misread; they're not checking whether they still have the symptoms only at 6 months, but whether they have them at any point 30 days to 6 months post-infection. From the paper:
Outcomes were ascertained from day 30 after COVID-19 diagnosis until the end of follow-up.
For another analysis, see this comment [LW(p) · GW(p)].
My best guess is that you have at least an additional ~1% risk of fatigue lasting > 6 months (and who knows how long) if you're vaccinated and catch COVID than if you don't catch COVID at all. My upper estimate is around 10%, but as I mentioned above, I give more weight to lower estimates, since I expect them to be less biased.
↑ comment by Owain_Evans · 2021-08-31T09:50:06.711Z · LW(p) · GW(p)
Re: the healthcare workers study. This seems like one of the best studies because of the matched control group and the fact that it's median 7.5 months after people had Covid. My main takehomes from this study:
1. 3% of Covid cases self-described has having ongoing symptoms at least 6 months out. This is only 4 people and so error bars are large. The inferred prevalence would be lower for men as this sample is skewed to women. 11% of cases had sporadic symptoms, but this seems significantly less bad than ongoing symptoms.
2. There were differences in between Covid cases and controls in self-reported symptoms that weren't picked up by (1). The really big affect is loss of smell/taste (which I don't see as very concerning). The neurological effects MichaelStJules cites seem less concerning. 15% of people without Covid are complaining of brain fog and 28% with Covid. I'm a bit puzzled about 15% of non-Covid people saying this. But given that they self-describe as having brain fog on (IMO) flimsy grounds, it's not that surprising that 13% more of Covid cases would report this (even if actual rates were only a few % different). This could be explained by demographic differences in front-line workers vs office/tech staff. Or from people hearing that Covid causes brain fog. Or from having brain fog during Covid and then being primed to notice it.
Some concerns about the study:
1. Selection bias in who filled out the survey (e.g. people who think they have Long Covid more likely to fill out the questionnaire, people with worst cases of Long Covid less likely to fill out survey).
2. The % among non-Covid with neurological symptoms is absurdly high and so it's clear the self-report methodology is very noisy/confusing. (These are all people employed in healthcare and skew younger so I'd expect serious neurological symptoms to be rare).
3. Different demographics of Covid cases vs non-Covid cases.
4. Only ~100 Covid cases and so can't detect rare effects.
5. The survey asked explicitly about Long Covid and so primed people about it.
6. These healthcare workers who had Covid all knew they had it (lab confirmed). An ideal study would look at people who never got a positive test.
7. They excluded people who had Covid less than 6 months ago. That might induce some bias for prevalence estimates (but not sure).
↑ comment by MichaelStJules · 2021-08-31T20:17:21.836Z · LW(p) · GW(p)
The high prevalence of neurological symptoms could be related to working in healthcare during a pandemic. Mental health also looked bad, but didn't differ significantly between cases and controls.
↑ comment by MondSemmel · 2021-08-26T10:41:49.330Z · LW(p) · GW(p)
One perspective on this, from a comment on the SSC reddit:
Replies from: MichaelStJulesBut this makes me think two things:
(1) Prior to covid, I was underrating how risky it is to get sick, because I was not accounting for the risk of chronic illness. I needed to update that prior, and take more general precautions against getting sick, period.
(2) Because chronic illness is not a unique or even (apparently) particularly special risk of COVID, fear of chronic COVID specifically should not change my risk calculus or precautions overall.
So I am simultaneously being more careful than I was before the pandemic, and less careful than my friends who still think "long COVID" poses a unique and novel threat that requires extra-special risk avoidance.
↑ comment by MichaelStJules · 2021-08-29T20:59:46.096Z · LW(p) · GW(p)
I think long COVID is particularly bad because I think you are much more likely to get it from pretty normal activities if you're not careful. Lyme disease, which the author of that comment mentions (citing this article), also looks common:
Recent estimates using other methods suggest that approximately 476,000 people may get Lyme disease each year in the United States.
I would guess that there aren't that many others nearly as bad, but I haven't really looked into it. I think colds, flus and food poisoning are much less severe and less common than COVID-19.
↑ comment by MichaelStJules · 2021-08-24T21:34:08.322Z · LW(p) · GW(p)
I also worry that it could become basically chronic and lifelong. It's surprising that we still presumably see effects 6 months after, and if 6 months isn't long enough to get better, that's reason for me to believe that these people won't get better. And it's possible to catch COVID multiple times (although you become more immune each time), so each time you may face a risk of long COVID.
If they do longer studies, maybe we'll see more people getting better, and with future studies, we'll have more reliable statistics. For now, I plan to continue being somewhat cautious and avoid large indoor crowds and high-traffric indoor areas.
Replies from: ChristianKl, cistrane↑ comment by ChristianKl · 2021-08-25T06:58:43.074Z · LW(p) · GW(p)
Given that the SARS side-effects were still there years later there's nothing surprising about still seeing effects 6 months later.
Replies from: Owain_Evans↑ comment by Owain_Evans · 2021-08-31T09:51:12.433Z · LW(p) · GW(p)
But the IFR for SARS is order of magnitudes higher and we know that severe illness is more likely to cause long-term effects.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-08-31T10:51:01.518Z · LW(p) · GW(p)
An order of magnitude less then SARS would still be a lot.
we know that severe illness is more likely to cause long-term effects.
How do we know that? We did have some long-COVID studies that suggest this isn't the case.
If the long-term effects are due to the immune system "learning" to attack native cells that can happen without severe illness.
↑ comment by cistrane · 2021-08-27T20:58:30.231Z · LW(p) · GW(p)
When you say that each consecutive time you catch covid you become more immune, do you implicitly estimate that each consecutive infections comes with lower risk of long covid?
Replies from: MichaelStJules↑ comment by MichaelStJules · 2021-08-29T05:31:05.114Z · LW(p) · GW(p)
This is what I was thinking, yes. The vaccines themselves reduce your risk of long COVID conditional on catching COVID, and more vaccines seem to be better (even after 2).
On the other hand, maybe there could be cumulative damage from repeated infections and there's some kind of threshold effect.
↑ comment by MichaelStJules · 2021-08-25T23:21:45.167Z · LW(p) · GW(p)
I've edited my comment, since I misinterpreted one of the studies. See also this comment [LW(p) · GW(p)] and this separate estimate based on different studies.
comment by Josh Jacobson (joshjacobson) · 2021-08-24T05:16:52.251Z · LW(p) · GW(p)
There seems to be a strong consensus that the Mayo Clinic study was highly flawed (assuming this is the source for your Pfizer vs Moderna claim… it’s paywalled). I haven’t seen many people actually address their takeaways beyond that, except one in our community who said they’d bet on ~equal effectiveness still rather than Moderna having higher effectiveness.
I’d be interested in additional takes, or maybe I’ll look into this myself.
comment by Jonathan_Graehl · 2021-08-24T03:57:40.636Z · LW(p) · GW(p)
agree. thanks
comment by Rob Bensinger (RobbBB) · 2021-08-24T04:21:15.743Z · LW(p) · GW(p)
Response from Connor Flexman to a social media post I wrote containing some of the claims above:
I think the arguments for [throwing a party now rather than later, if you're going to throw one anytime in the next seven months] are basically correct—it's not very bad to do it now, and it's not clear it will get better bc of increased infectiousness of Delta.
I think the best counterargument is to say [...] that it's likely we have some dip for some reason by Mar 2022, especially toward the end of that. Cases are currently just above average (keeping in mind that early in the pandemic we were failing to catch most cases and tests were likely worse). But we've never seen a 7-month period where cases didn't drop super low. Last winter, Feb/Mar had gotten way safer. Further, if we're at 1% cases now and they're cycling 1/wk (bc Delta is faster), that means over the next 30 weeks 30% of the population will get it—which means either we get pushed *substantially* toward herd immunity, or else it has to drop under current levels at some point.
The obvious counterargument is that herd immunity is no longer meaningful, since Delta seems to breakthrough against vaccines like 20-40% of the time and natural immunity isn't that much better, and the control system means that as we get closer to "herd immunity" then people will start making out more and more until we still miraculously have the same number of infections.)
Overall, I'd probably still do it now, but I could certainly imagine many people with lower risk tolerances wanting you to wait until the statistically-reasonably-likely time that risk has gone down 4x.
[...]
comment by Evan Sandhoefner (evan-sandhoefner) · 2021-11-12T18:58:43.575Z · LW(p) · GW(p)
Can anyone help me understand this bit?
"J&J is also going to immunize you against the vector virus, making it harder to receive future AAV vaccines/gene editing in the future, so personally I would stick to the mRNA vaccines only."
comment by Josh Jacobson (joshjacobson) · 2021-08-24T17:14:26.371Z · LW(p) · GW(p)
Be much more wary of COVID when hospitals are full
Keep an eye on confirmed COVID-19 cases, hospitalizations, and deaths in your area, and put effort into avoiding catching or transmitting COVID-19 if it looks like hospitals in your area will be overloaded 2-4 weeks from now.
I’ve had a vague impression that this hasn’t meaningfully led to worse outcomes, though I could be wrong. Know of any analysis on it?
Additionally, even if we added the hospitalization % to the death percent (pretended all hospitalizations were deaths), I think impact would still be dwarfed by long COVID?
comment by Florin (florin-clapa) · 2021-08-24T05:35:33.634Z · LW(p) · GW(p)
4. If you do worry about it...
...wear effective PPE (elastomeric respirator + eye protection or PAPR) and never worry about it again.