Covid 10/14: Less Long Cvoid
post by Zvi · 2021-10-14T14:20:01.250Z · LW · GW · 22 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Vaccinations Vaccine Mandates Long Covid NPIs Including Mask and Testing Mandates In Other News None 23 comments
The pandemic has become predictable, which is the world we much prefer to live in. Cases and deaths continue their slow but steady declines, vaccine approvals for boosters and children continue to slowly move forward. Mandates continue to make people angry but mostly work when used, while also not that often being used. Same old, same old.
The big news story was that one of the studies of Long Covid was revealed to be vastly overestimating frequency due to a methodological ‘error.’ It’s an important update.
Executive Summary
- Cases and deaths declining as expected.
- Approvals progressing slowly as expected.
- Long Covid study had important error, see discussion later in post.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 560k cases (-10%) and 11,500 deaths (-8%).
Results: 547k cases (-12%) and 11,051 deaths (-12%).
Prediction for next week: 481k cases (-12%) and 9,835 deaths (-11%).
We are still in a low-variance situation, with no reason to expect any big surprises for at least several more weeks.
Deaths
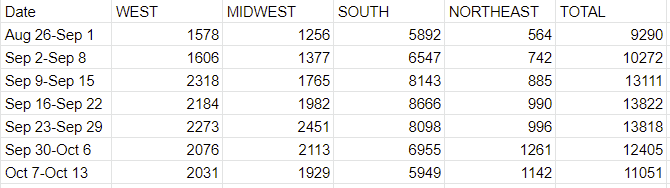
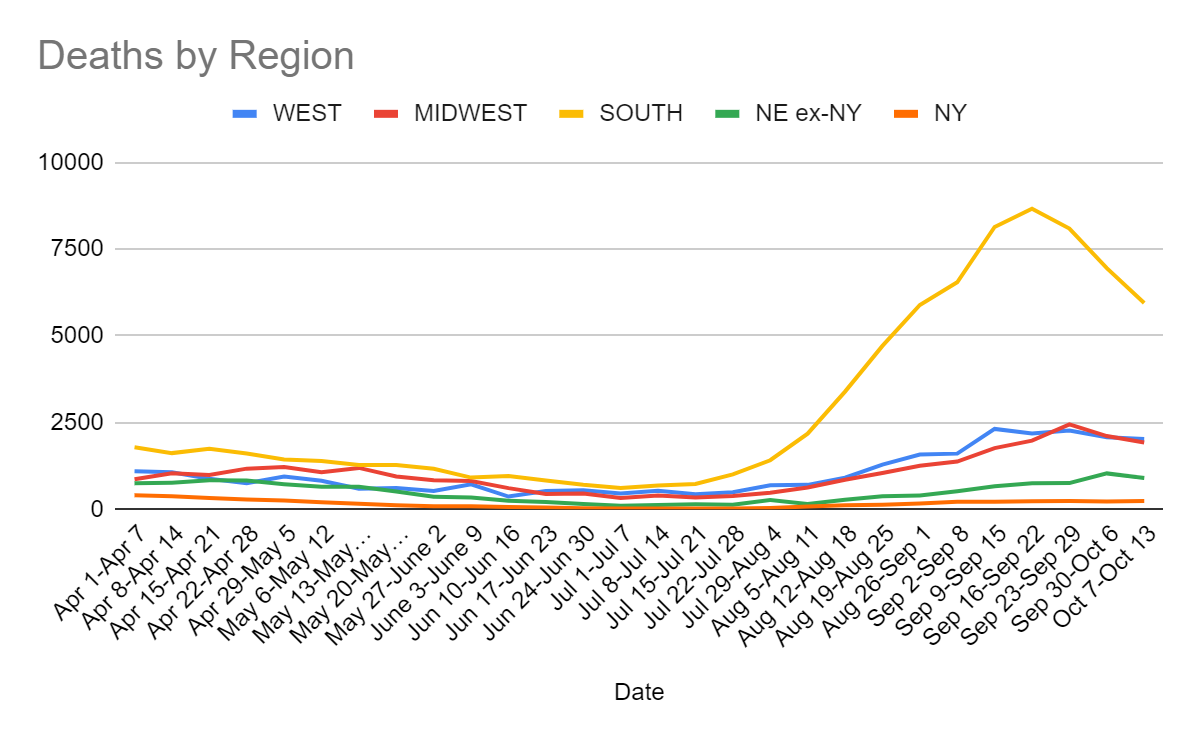
The exact rate of decline here was a pleasant surprise, but we’ve gotten to the point where this is a lagging indicator, so the times when it is surprising are mostly about data gathering issues, either holidays or changes in the ways in which we do testing. Expect this trend to continue, and continue to mirror cases with a lag.
Cases
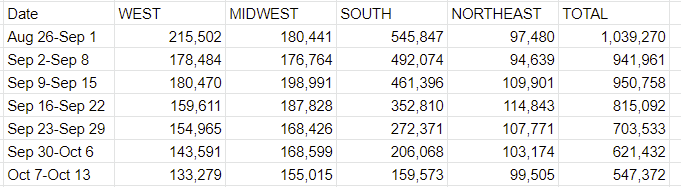
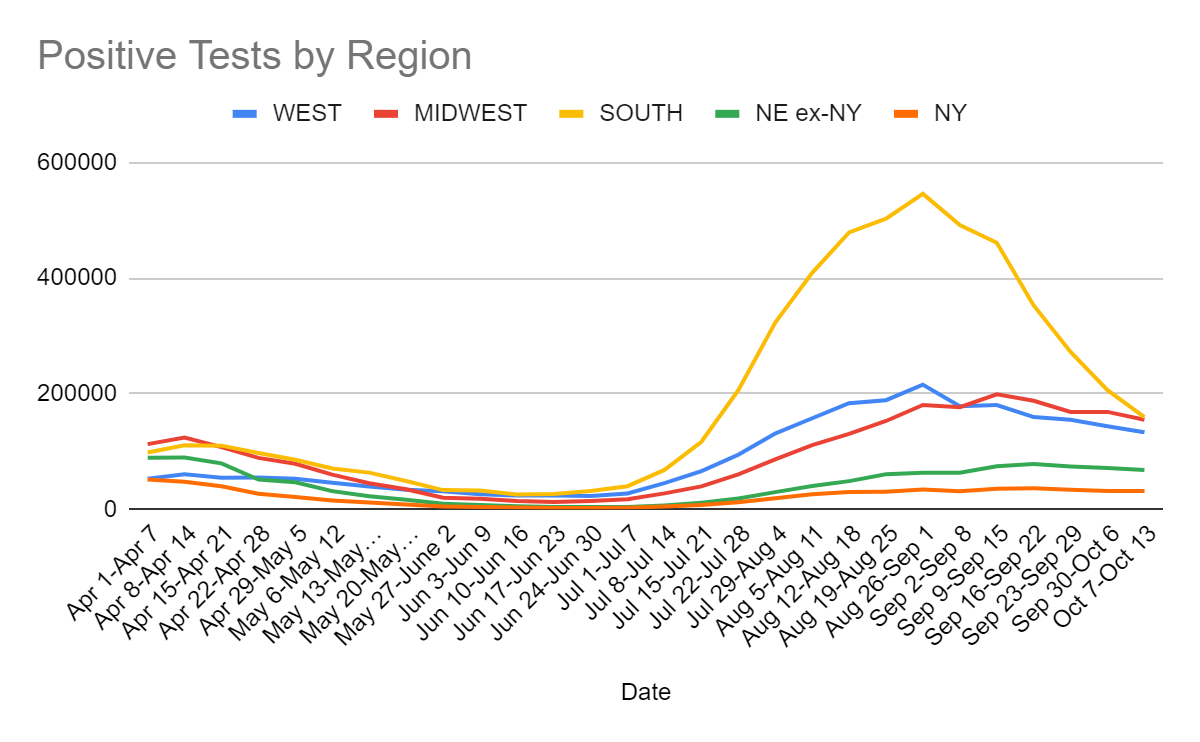
This is pretty much exactly what we would have expected. The Northeast number is slightly disappointing, others were slightly better than expected, but no real surprises.
Vaccinations
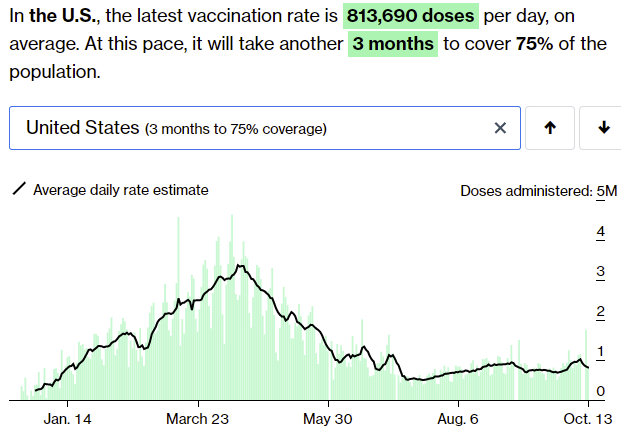
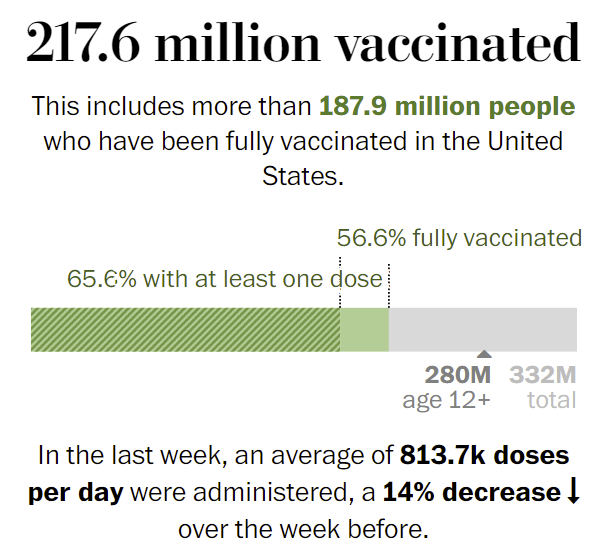
The rate of vaccinations continues to not change much, and it’s clear that the positive bump wasn’t the start of a surge. That continues not to tell us much about how much work the mandates are doing here. My impression is that the mandates that have teeth work, but that few of them have teeth.
In his podcast interview this week with FiveThirtyEight, former FDA Commissioner Dr. Scott Gottlieb asks where the cost-benefit analyses are on the vaccine mandates, since there don’t seem to be any. He estimates that we could use mandates to go from something like 80% adult vaccination rates to 84%, and asks how much that really accomplishes.
My answer is that this change would be worth quite a lot, but how much depends heavily on how we would react to the two scenarios.
Cutting the number of unvaccinated adults by 20% wouldn’t cut transmission by 20%, since there is some spread by non-adults and some spread by the vaccinated. It’s still a major percent drop in transmission if behavior didn’t adjust, at least 10%. Cutting transmission by 10% means a 10% cut in cases every four days or so if behavior doesn’t adjust, which is a rather big game, cutting cases in half each month.
Behaviors would of course adjust, which is a big benefit. We’d get to increase our equilibrium amount of Covid-19 risk by 10%, which is a substantial percentage of the way back to regular life. If we used this to eliminate ‘stupid prevention’ selectively the win would be even bigger.
Alternatively, if we didn’t adjust our behaviors, then we get full suppression before too long, or damn close to it, at which point the adjustments happen no matter what any ‘public health experts’ or government officials might want. If we’re looking at under 10k cases per day, as we likely are within a few months, people outside of some particular institutions going to go back to normal, and even in those few places there’d be increasing pressure over time.
The intuition pump here is that putting us over the top is a huge deal, and that this is plausibly exactly what we need to get over the top, and if this doesn’t get us there it still gives us a bunch of extra slack to spend. Plus it creates new ‘safe spaces’ where everyone is vaccinated. And of course, it lowers average severity that much more, as well.
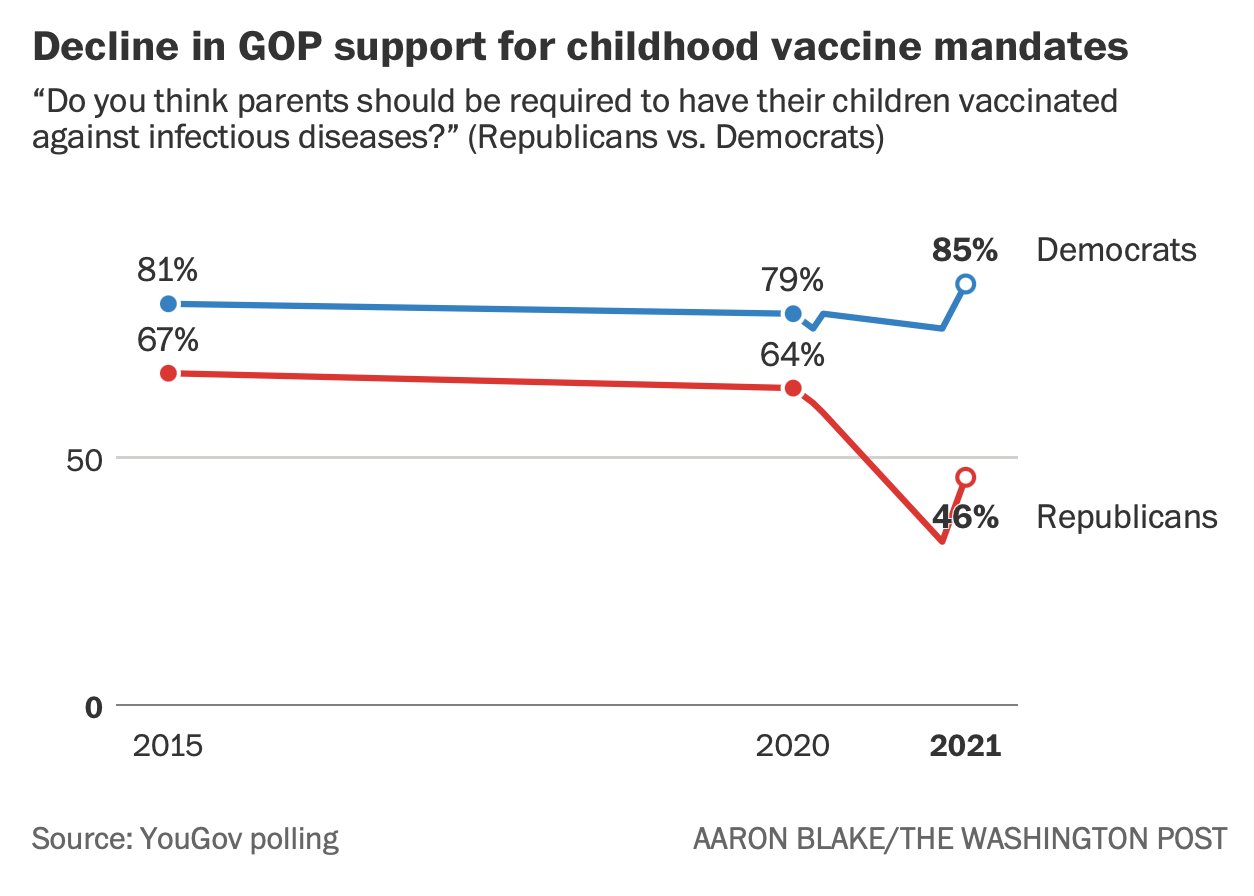
One big cost of all this is that Republicans are turning against vaccinations and vaccine mandates in general, which is a big problem, but the timing seems to correspond to the vaccine rollout rather than to the mandates. Not clear to what extent the mandates will contribute to this, but would be rather disastrous if red states stopped requiring childhood immunizations.
Looks like mix and matching vaccines is going to be shown once again to be effective, but this time the results come from America, so maybe they will count.
Vaccine Mandates
The mandate conflict this week is that Texas mandated a lack of vaccine mandates by any entity at all, to combat Biden’s mandate that there be mandates for large corporations, putting the two in direct conflict. There’s still a technical way out of that for corporations, which is that the Biden rule allows frequent testing as an alternative. Alternatively, one can take a side and say that the Texas rule is invalid, which is what the Biden administration is claiming, and the major airlines seem to have adopted this policy.
Mostly we didn’t hear about much in the way of new mandates this week. The mandates that are already in place or being put in place seem to be proceeding smoothly, but there isn’t much appetite to add new ones.
Meanwhile, given the lack of enthusiasm for surprise, ruthless efficiency or fanatical devotion to the Pope, some vaccine advertisements turn to fear.
In other places, some countries are actively halting or scaling back use of Moderna, despite it being clearly the most effective vaccine, due to relatively trivial concerns. I can’t even get angry about it anymore, but all the more reason to get your shots while you can to be safe on multiple fronts.
The FDA is moving forward with child vaccine approval (after which it will presumably become mandatory right away in many places) but isn’t comfortable yet that it has inserted enough delays to make everyone feel comfortable, so the delays continue for now.
Long Covid
Via an excellent comment [LW(p) · GW(p)], we have an important discovery about the Long Covid data.
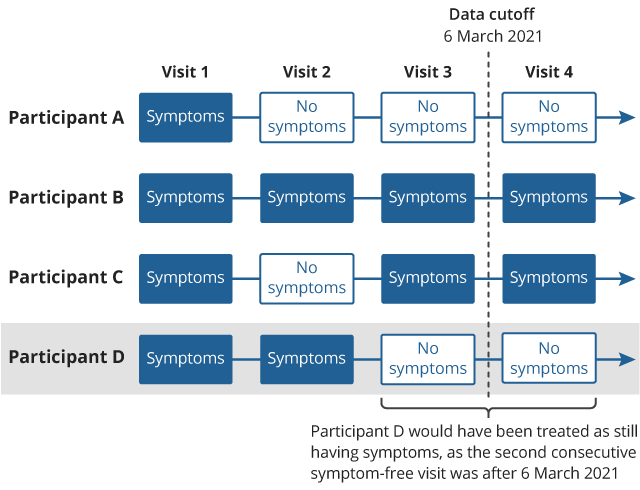
A major source for the previous pessimistic LC estimates, like Scott Alexanders (the UK’s giant ONS survey) published an update of their previous report which looked at a follow-up over a longer time period. Basically they only counted an end to long Covid if there were two consecutive reports of no symptoms, and lots of their respondents had only one report of no symptoms before the study ended, not two, so got counted as persistent cases. When they went back and updated their numbers, the overall results were substantially lower. This graphic explains their original mistake:
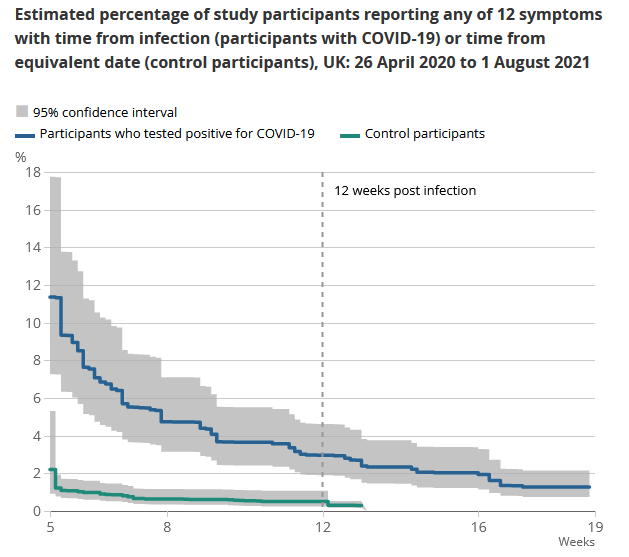
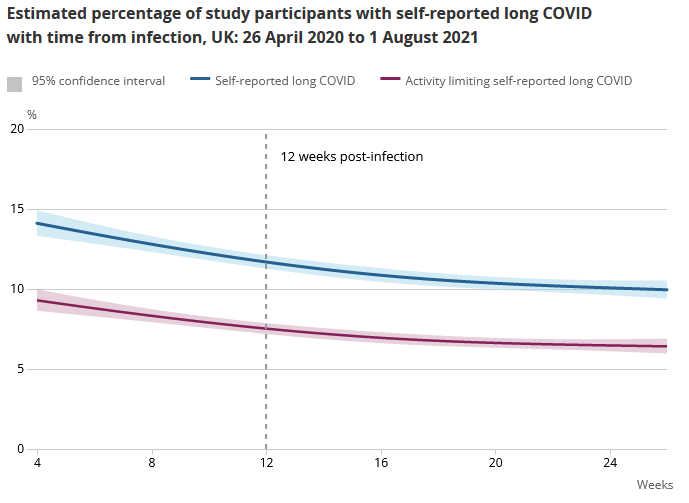
The new headline result is 7.5% of Covid-19 patients had ‘some limitation’ of daily activities after 12 weeks if you ask them if they had long Covid-19. If you go by asking if there were any symptoms from a given list, the rate is lower (like 3%). The full reportis here. What’s notable is that a lot of participants reported LC symptoms with no Covid-19 positive test.
They break it down by age and sex in the full report, but you should treat these numbers as numbers for mostly double vaxxed AZ and some mixture of single/double vaxxed Pfizer/Moderna for younger groups, since that’s how it worked in the UK.
This is a pretty dumb error, a very dumb way to get a lot of people very scared and destroy a lot of value. Many thanks to the team for correcting the error, whether or not it was intentional and whether or not they should never have made the mistake. And whether or not the mistake was a reasonable one to be making, which it pretty much wasn’t. Error correction is a big deal. Basically what they did, as far as I can tell, was this:
- If you report symptoms, that means for now you have Long Covid.
- If you report no symptoms twice in a row, congratulations, you don’t have long Covid.
- If you report no symptoms then symptoms, we still assume the symptoms are due to Covid, and you therefore still have Long Covid.
- If your last report was no symptoms, you’re still considered to have Long Covid until you report in again with no symptoms.
- A lot of people didn’t feel the second no-symptom report was a terribly urgent thing to be doing.
- A lot of people simply hadn’t had the chance to report a second time once their symptoms had cleared up.
- Yet they still counted the period that included their report of no symptoms, as a length of time that they had Long Covid.
To be blunt, they cheated (intentionally or otherwise), it was a massive effect, and we should have caught it, but to my knowledge none of us did. They have now fessed up.
If you ask people to pick from a list of common symptoms, only 3% report that they have one. The larger numbers are mostly or entirely what happens when people are asked if there is anything wrong with them at all, and would they like to blame it on Covid-19. Also the percentages declined a lot over time, so chances are few of the cases would be permanent or semi-permanent. Even if you buy one of the larger numbers, this is a substantial improvement.
Given how many people have already had Covid if you go by the antibodies present in various populations or what I would otherwise guess, this seems far more plausible, that Long Covid while real is relatively rare.
NPIs Including Mask and Testing Mandates
The other thing I wanted to highlight from Gottlieb’s podcast interview this week with FiveThirtyEight was that when cloth masks were first proposed as a solution, everyone involved (according to his account) agreed that cloth masks probably worked, and agreed they were widely available, but that they pushed back hard because if people were told they could use masks, they wouldn’t listen to demands that they stay inside. So that’s the type of thinking we are dealing with there. Scott Gottlieb is very much in the ‘level with the people and it will work out’ camp, and I continue to wonder about the alternative world where he had still been in charge at FDA in 2020.
Lateral Flow Tests looking more effective in practice than we previously thought.
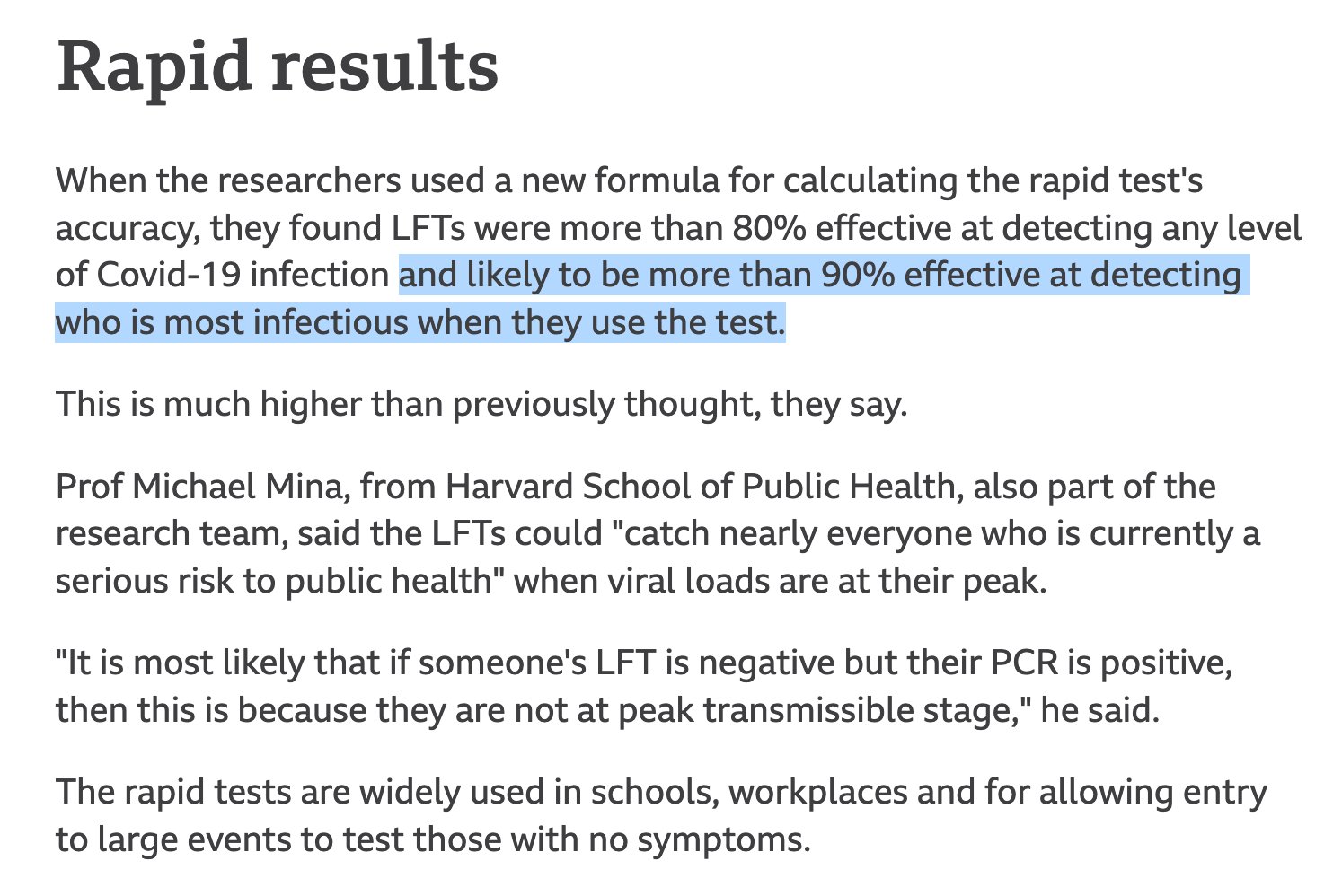
Good thing we blocked them due to being insufficiently good, leaving many people without any access to testing when it mattered most.
In Other News
There were a bunch of flights cancelled in Florida, over some combination of a lack of pilots due to protests against vaccine mandates, a lack of air traffic controllers due to protests over vaccine mandates, and bad weather, depending on who you believe. In the mainstream media this has been treated with something that’s hard not to describe as a media blackout, where a big event happened with both practical short-term and potential long-term impact, and everyone somehow decided not to cover it. It seemed to reflect prioritizing something other than reporting newsworthy events or providing useful information to listeners and readers.
On the other side, this was seen as some glorious sign of revolt and things to come, which also seems mostly wrong to me. Such disruptions seem both rare and mostly not that impactful, with this being news exactly because it had any meaningful impact at all. Whereas supply chain issues caused by actual Covid-19 disruptions are increasingly dire.
Ivermectin studies looking more and more like outright fraud, as in the study never happened and they copied lines of data a lot levels of fraud.
Another reminder of how bad it’s been that we’ve groundlessly scared pregnant women to the point where they’re largely not getting vaccinated, and now they’re filling ICUs.
Dr. Sanjay Gupta appeared on the Joe Rogan Experience. Due to time limitations I haven’t yet had a chance to listen, I hope to be able to report back on this next week.
22 comments
Comments sorted by top scores.
comment by Daniel_Eth · 2021-10-14T23:42:10.645Z · LW(p) · GW(p)
"Mandates continue to make people angry"
True for some people, but also worth noting that they're popular overall. Looks like around 60% of Americans support Biden's mandate, for instance (this is pretty high for a cultural war issue).
"Republicans are turning against vaccinations and vaccine mandates in general... would be rather disastrous if red states stopped requiring childhood immunizations"
Support has waned, and it would be terrible if they stopped them, but note that:
- Now republicans are split ~50:50; so it's not like they have a consensus either way
- Republicans being split and others (including independents) being in favor means that majority is clearly in favor, even in red states
- Republican support has recovered somewhat already, and I'd expect support will continue to revert closer to pre-COVID levels as we progress further (especially years out); we might not reach pre-covid levels, but I'd be surprised if the general view of republicans was against several years from now (though OTOH, perhaps those against are more strongly against, so you could wind up in a single-issue voter type problem)
"3%"
This seems to be at the 12 week mark, which is somewhat arbitrary. Even according to the same study, looks like long covid rates are closer to 1% after 19 weeks.
"To be blunt, they cheated (intentionally or otherwise)"
Flagging that I don't like this language, for a couple reasons:
- I think it's inaccurate/misrepresentative. "Cheating", in my mind, implies some dishonesty. Yes, words can obviously be defined in any way, but I'm generally not a fan of redefining words with common definitions unless there's a good reason. If, on the other hand, your claim is that they were indeed being dishonest, then I think you should come out and say that (otherwise what you're doing is a little motte-and-bailey-ish).
- I think it's unnecessarily hostile. People make mistakes, including scientists making dumb mistakes. It's good that they corrected their mistake (which is not something lots of people - including scientists - do). The fact that none of us caught it shows just how easy it is to make these sort of mistakes. (Again, this point doesn't stand if you are trying to imply that it was intentional, but then I think you should state that.) I similarly don't think it's apt to call it "fessing up" when they correct their mistake.
Looks like this dropped after your post here so you wouldn't have been able to incorporate it – advisors to the FDA are recommending moderna boosters for the same group of people that are getting pfizer boosters (65+, risk for health reasons, or risk for job), and also this will be at half dose. They should make a recommendation on J&J tomorrow.
comment by DanArmak · 2021-10-14T15:38:14.068Z · LW(p) · GW(p)
Title typo: cvoid.
Replies from: quintin-pope↑ comment by Quintin Pope (quintin-pope) · 2021-10-15T02:31:08.315Z · LW(p) · GW(p)
Also typo: “reportis” (“is” belongs to a hyperlink, so the typo may look like “report[is” depending on your editor).
comment by Jackson Wagner · 2021-10-14T19:39:05.458Z · LW(p) · GW(p)
Zvi, what are your thoughts on covid in the USA during the winter?
On the one hand:
- The delta wave is ending, and there are no new variants on the horizon.
- Vaccinations rates are high and slowly rising.
- The overall rate of immunity (from vaccines + natural infection) is high and probably rising (although this is a fight between fading vaccine effectiveness vs natural infections & vaccine booster shots).
On the other hand, winter is traditionally the worst time for colds and flus, including the monster covid wave of 2020. It seems hard to believe we'll skate through winter 2021 without somewhat of a bump in covid cases.
If you have thoughts about the course of covid beyond this winter (like the prospect for future variants or how necessary it will be for most of the population to take booster shots at a regular cadence), I'd be interested in that too.
One thing that I think will be consequential, in a kind of hilarious way, is that we're probably going to skip two flu seasons in a row, which will possibly set us up for a whopper flu season down the road. Last winter the flu was practically nonexistent, crowded out by covid. This winter, based on my read of this Metaculus forecast, the flu season is expected to be only half as intense as a typical pre-covid year -- peaking at around "4% ILI" instead of around 8%.
https://www.metaculus.com/questions/7621/peak--ili-in-va-during-2021-2022-flu-season/
https://www.vdh.virginia.gov/epidemiology/influenza-flu-in-virginia/influenza-surveillance/
If we get a whopper flu season in 2022 or 2023 (perhaps 2-3x worse than normal), it will be interesting to watch how the media and culture responds -- will they go into covid-esque hysterics about the overcrowded hospitals and demand flu lockdowns? Or will it act as a nudge in the other direction, convincing people that the lockdowns and NPIs have got to stop somewhere? Or, perhaps we'll never get a whopper flu season -- maybe Delta will remain the transmissibility king of all the infectious viruses, even after stabilizing and going endemic? Perhaps our transition to remote work, covid-caution in shared indoor spaces, and mRNA vaccines means a permanently more hygienic world?
Overall, I'm very interested in the question of whether covid cases ever crash to suppression levels (as would perhaps have happened in a world without the Delta variant), versus only very slowly trailing off into the background of ordinary pre-covid colds & flus. I think this is very important for predicting how culture will evolve going forwards. A sharper transition from pandemic to negligible covid would encourage more of a snap-back to pre-covid "normality": more mass concerts, more comfort visiting shared indoor spaces, fewer masks and NPIs, less remote work. Versus a world where covid lingers interminably and there's no sharp transition into the post-pandemic world will make it harder for culture to coordinate a "return to normal".
I'm not sure which side I'm cheering for, but it's clearly an important question regardless. (Remote work and better tech adoption across the board have been highlights of pandemic culture. A slightly increased focus on scientific progress is obviously welcome. And the pre-covid world sometimes strikes me as being a little too heavy on present consumption, like travel vacations, with not enough long-term focus. But of course all the masking and social distancing and reduced socializing has been miserable, and the madness of constantly-changing restrictions is terrible for both business and living an enjoyable human life.)
Replies from: cistrane, gabriel-holmes↑ comment by cistrane · 2021-10-15T10:15:38.273Z · LW(p) · GW(p)
By late 2022 and much more probable by 2023 mRNA flu vaccines will be available and they will be just as effective as covid vaccines.
Replies from: demost↑ comment by demost · 2021-10-16T18:59:42.061Z · LW(p) · GW(p)
I don't think it's clear that mRNA flu vaccines will be as effective as mRNA corona vaccines.
One reason why SARS-CoV2 is an "easy" target for vaccine is that it has a very low mutation rate (as do other corona viruses). Influenza viruses evolve much faster. A standard problem of flu shots is that they are not designed against the virus that circulates in the winter, but rather against viruses that circulated half a year ago. For the corona virus, this does not make a big difference, but for flu viruses, it can render the vaccine (partially) useless.
The mRNA technology has some advantages because the cycle of development and production is shorter. But it is still long enough that the problem does not go away completely. We should not expect mRNA flu vaccines to be as effective as mRNA corona vaccines.
Replies from: cistrane↑ comment by cistrane · 2021-10-19T08:30:50.635Z · LW(p) · GW(p)
The big promise of mRNA technology is that a vaccine can be made against several strains in the same shot
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2021-10-26T16:54:15.969Z · LW(p) · GW(p)
Flu shots already target 4 strains. The size of mRNA vaccines are so small that they could put 100 in one shot, but could the immune system handle it? But the short development time of mRNA vaccines means that they can target better. The same should be true of recombinant protein vaccines—the real promise of mRNA is that it's new and sexy and the FDA will let them try. But targeting is only a small part of the flu vaccine problem. Good targeting raises the effectiveness from 30% in mismatch years to 50% in match years. The problem is the flu vaccine isn't that good even when it is matched.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-10-15T09:36:58.634Z · LW(p) · GW(p)
I actually think we should be mandating flu shots in addition to covid shots.
Biden administration: "Mandates work! Get a covid shot or else!" Also Biden administration: "Pretty please, get your flu shot"
(Seriously though, get your flu shot)
comment by samjlord · 2021-10-15T18:24:52.700Z · LW(p) · GW(p)
I found the Rogan episode with Gupta (and especially the one with Berenson) was painful. I had to stop listening and I don’t think I’ll listen to Rogan anymore. When I know the details of the studies that Rogan throws around I get really frustrated with his lack of really deep understanding of the science. He is quick and smart, but his lack of depth leads him far astray when it comes to complex things like vaccines and medical science.
For example, he kept telling Gupta about the Hoeg myocarditis preprint (https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1) and repeatedly read from a news story about it that boys are more likely to get myocarditis from the vaccine than to get hospitalized by covid. But this misunderstands that the preprint was comparing vaccine risk to covid risk *assuming you had a fairly low chance of getting covid in the first place*. It wasn’t comparing vaccine risk to covid risk conditional on actually getting covid.
Gupta really stumbled and neither made the point that all kids are likely to eventually be exposed to the virus now that it is likely to become endemic, so the net risks from the disease are much higher than the Hoeg preprint estimates, nor did he flesh out that hospitalizations that result from covid are likely to more dangerous than myocarditis, which is often easily treatable.
The Berenson episode was this times a million. Most of the data they showed was “real,” but completely lacking context and depth/understanding to the point of being misinformation. It really reminds me of the numbers games (wrong denominator, failing to compare to other risks, failing to balance risk of an action/policy with risk of the alternatives) Berenson used to fight against when they were coming from covid fearmongers. Now he’s using identical tactics to spread fear about the vaccines.
I wish folks would point out to Rogan that he applies a different standard to vaccines (they must be proven totally safe over decades of testing) than he does to other medications and natural remedies. How can he know that Ivermectin won’t just cause SARS-CoV-2 to go dormant in people’s spinal columns for a decade only to reemerge to kill them? Vaccines hold a special fear in our collective psyche, because we’ve all been exposed to decades of anti-vaxx propaganda. Even those of us very pro-vaxx can’t help falling prey to the emotional fear of jabbing our kids.
Replies from: CraigMichael↑ comment by CraigMichael · 2021-10-15T19:25:25.416Z · LW(p) · GW(p)
I'm in the middle of listening to it and have a somewhat similar feeling. I don't like the trick of bringing up a paper about Covid-19 when it looks like there's about 4.4 million scholarly articles, and would then assume another order of magnitude more broadly in "the news." Sure, some are more important than others, but "hey there's this one study you didn't see and I'm going to ask you to evaluate it in real time" is a jerkass move under the circumstances. If there's something you want to bring up, should give people a week or more to get familiar with the content.
comment by Sammy Martin (SDM) · 2021-10-15T11:45:08.887Z · LW(p) · GW(p)
If you ask people to pick from a list of common symptoms, only 3% report that they have one. The larger numbers are mostly or entirely what happens when people are asked if there is anything wrong with them at all, and would they like to blame it on Covid-19.
Also the percentages declined a lot over time, so chances are few of the cases would be permanent or semi-permanent. Even if you buy one of the larger numbers, this is a substantial improvement.
The result that I mentioned in that original comment was the one for rates of 'some limitation' of daily activities, not just if they had long covid at all. I could tell a story where the 7.5% number (which was indeed declining, though slowly, since it was still at 6% after 24 weeks) is a better estimator than the 3% (which declined to 1% by 19 weeks) rate of specific symptoms.
The study didn't list 'brain fog' as a symptom, so if people are fairly honest in saying whether their daily activities are limited, and mostly they're limited by things like brain fog that didn't appear on the symptom list, the rate could look more like that 7.5%.
However, I'm not sure if I buy this argument. The study authors mention it briefly:
The 12 symptoms in our survival analysis approach do not include all those often associated with long COVID such as heart palpitations, chest pain, sleep disruption, cognitive impairment, and depression and anxiety. This may have downwardly biased the estimates. We are exploring options for adding additional symptoms to the CIS questionnaire to address this gap.
And then they give some reasons to think that the higher estimates are more accurate because long covid relapses:
The self-reported long COVID response may better capture the relapsing nature of long COVID symptoms. Of participants who were classed as experiencing symptom discontinuation (two successive symptom-free visits) in our survival analysis approach in Section 4, 14.1% reported at least one of the 12 symptoms in a subsequent follow-up visit. Some of these participants may still describe themselves as having long COVID in our analysis in Section 5 if, from their past experience, they expect periods of improvement to be followed by relapse.
Furthermore, the percentage of participants with symptoms persisting for at least 12 weeks using the survival analysis approach increased to 6.1% when we defined symptom discontinuation as being three rather than two successive symptom-free visits (see the data tables) for full sensitivity analysis results).
It is also likely that the 12 symptoms included in the survival analysis approach do not include some symptoms often associated with long COVID, which may further explain the disparity between the estimates.
On the other hand, are we getting into 'dragon in the garage' territory at this point? If long covid is really nonspecific, comes and goes and random and can only be accurately assessed with subjective reports, you've just introduced a few huge sources of upward bias.
So overall, I'd treat that 7.5% as an upper limit and the 3% as a lower limit on rates after 12 weeks.
comment by James_Miller · 2021-10-14T15:38:04.025Z · LW(p) · GW(p)
How confident are we that being vaccinated for COVID reduces the likelihood that you will transmit COVID to another especially given that vaccination will change your behavior, e.g. if you don't even notice you have symptoms you don't stay home in bed when you are infected? This paper is likely relevant: https://www.medrxiv.org/content/10.1101/2021.07.31.21261387v4
Replies from: samjlord↑ comment by samjlord · 2021-10-15T00:31:09.710Z · LW(p) · GW(p)
This study of actual transmission seems to indicate a substantial reduction in transmission from vaccinated people. But that benefit also seems to fade. I don't know if the fading is real or how much is from confounding effects (like more and more "unvaccinated" having immunity from prior infection). Someone with more experience in these types of studies than I could dig into that.
https://www.medrxiv.org/content/10.1101/2021.09.28.21264260v1
comment by YimbyGeorge (mardukofbabylon) · 2021-10-15T09:27:45.433Z · LW(p) · GW(p)
Why doesn't this trial get more publicity?
https://www.togethertrial.com/trial-specifications
Ivermectin was dropped for futility, Fluvoxamine trial stopped for superiority! Fluvoxamine rules!
Replies from: ChristianKl, CraigMichael↑ comment by ChristianKl · 2021-10-15T20:33:19.373Z · LW(p) · GW(p)
The page says "manuscript in development". Without even a preprint it's hard to say anything about the trial.
↑ comment by CraigMichael · 2021-10-15T17:18:50.098Z · LW(p) · GW(p)
I am surprised and not surprised that fluvoxamine hasn’t gotten more coverage. I think it’s because the attention has went to the Merck pill.
comment by DPiepgrass · 2021-10-27T23:25:04.417Z · LW(p) · GW(p)
Ivermectin studies looking more and more like outright fraud, as in the study never happened and they copied lines of data a lot levels of fraud.
This link is not about ivermectin or repurposed drugs.
comment by J Mann · 2021-10-14T20:29:25.967Z · LW(p) · GW(p)
The link for "Ivermectin studies looking more and more like outright fraud" seems to go to a discussion of mix and match routines.
Thanks again for doing these - I look forward to them all week!
↑ comment by CraigMichael · 2021-10-15T17:23:31.317Z · LW(p) · GW(p)
I noticed this too. Looks like maybe it was the wrong link.
comment by theme_arrow · 2021-10-14T18:48:18.305Z · LW(p) · GW(p)
With regards to mandates, something that happened this week is that big federal contractors, including Boeing and Lockheed Martin, formally announced their plans to comply with the contractor mandate.