Covid 4/15: Are We Seriously Doing This Again
post by Zvi · 2021-04-15T13:00:01.288Z · LW · GW · 37 commentsContents
The Numbers Predictions Deaths Cases Vaccinations Vaccine Passport Hype Vaccines Still Work In Other News None 37 comments
Yes we are. It can happen here.
THIS IS LITERAL ONE IN A MILLION AND MUCH LESS THAN THE BASE RATE WHAT THE ACTUAL FUCK IS WRONG WITH YOU DID YOU NOT SEE WHAT HAPPENED LAST TIME ARE YOU COMPLETE MORONS OR ARE YOU MUSTACHE-TWIRLING VILLIANS YOU CAN’T NOT BE BOTH, AS IN IF YOU’RE NOT MORONS AND I LOOK AT PHOTOGRAPHS I WILL SEE MUSTACHES AND YOU PEOPLE WILL BE TWIRLING THEM:



If any of them don’t have mustaches, we need to get them some clip-on ones, because while lots of people die at least they should get to enjoy the pleasures of twirling.
Yes I am fully aware that it is technically a particular rarer blood clotting disorder that is happening here and thus in that subclass it is above the base rate and that there’s an argument this might be ‘real’ in some sense and no I do not care even a little bit about any of that and no I am not going to treat this with the dignity and respect that it does not in any way even potentially deserve. There are scientific details and if you find them interesting by all means read about them but I am ignoring them because like the points They. Do. Not. Matter.
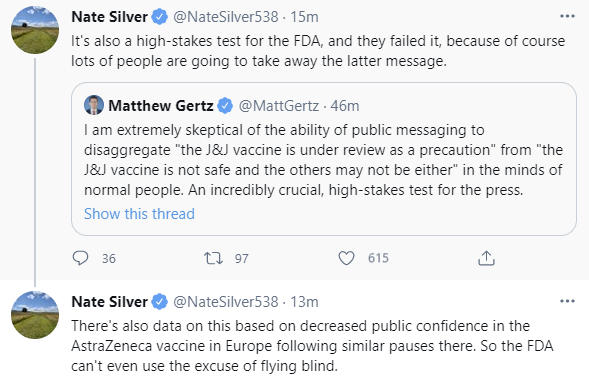
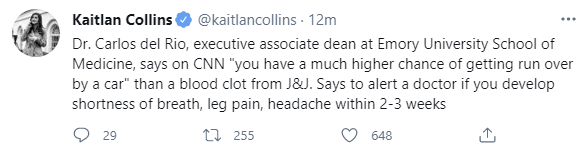
In case you were wondering how people were going to react or what this would do to public confidence, these are from less than an hour after the announcement:
I mean, they’re wrong, but I can’t fault their reasoning from where they sit, if you asked me the ‘which is more likely’ game back in 2019 I would most definitely have not have gone with ‘no really they’re doing this in a pandemic because of six cases.’
Again, seems logical to conclude they were rushed if they act in a way that would only make sense if they actually did rush.
The first time around with AstraZeneca, I could sort of understand the argument for the other side of the hesitancy effect when I squinted, that this would look like the Very Serious People Take Vaccine Safety Seriously and therefore we should now expect the people to trust the FDA more, and being untrustworthy stewards who kill a bunch of people in order to fool the public into thinking we are trustworthy is a tradeoff they thought we should make, but we ran the experiment on that hypothesis, and, yeah, no.
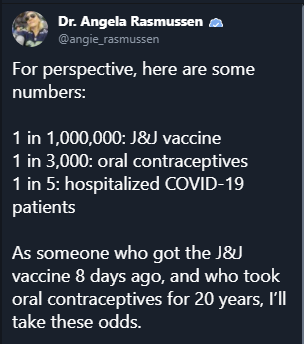
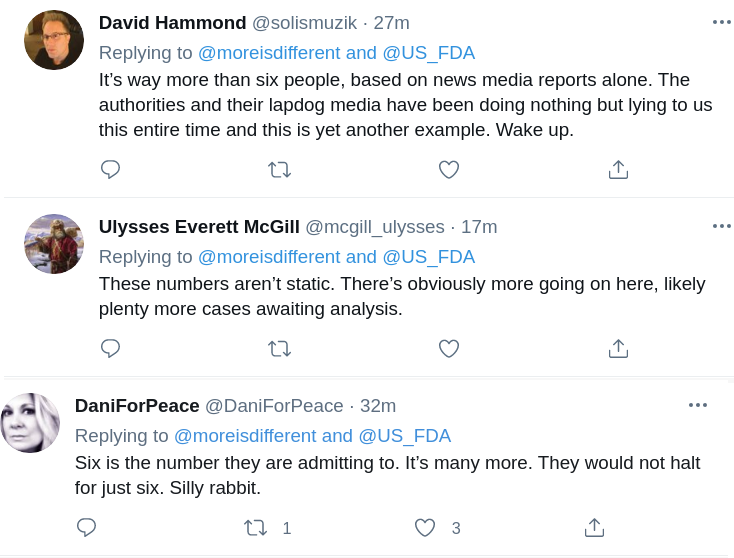
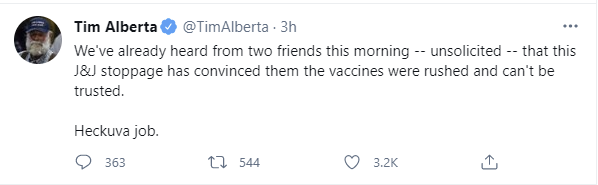
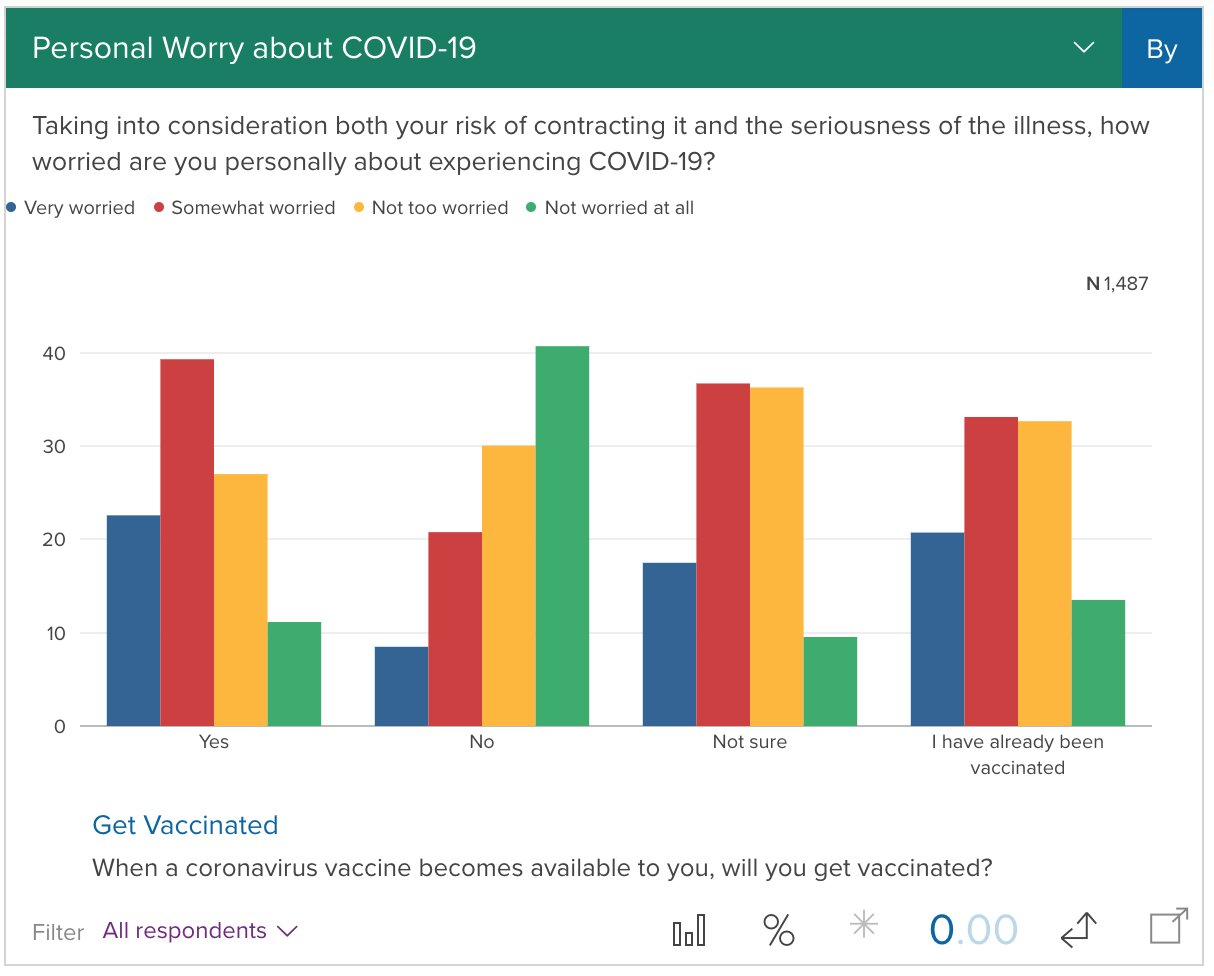
Seriously, people are not so stupid:
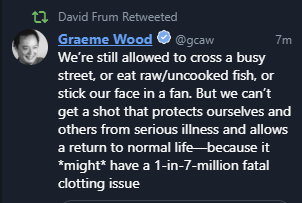
Also, when you keep saying loudly that any adverse things that happen will destroy your credibility, consider your credibility preemptively destroyed already because you’re either right or wrong:

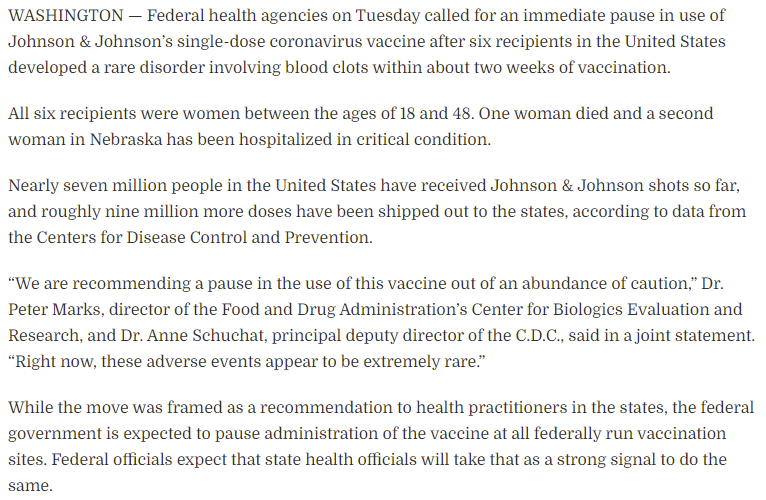
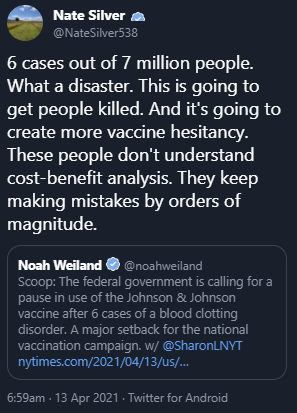
This is going to permanently supercharge the anti-vax movement, not only on Covid but also in general, and kill a huge number of people. Over six cases. Note deaths. Cases. Six.
You know how many people died?
ONE. F***ing ONE.
No, this was not ‘going to come out.’ It was going to completely correctly get ignored. All they had to do was put it in the list of side effects and note it was extremely rare.
This is the Washington Post’s attempt to chronicle what was going through their minds, it’s sympathetic but doesn’t make the decision look any less absurd if you actually think about the physical situation at all or how real people would react to it.
If I had to steelman the case being made, it’s a combination of believing that acting over-the-top paranoid about side effects makes people feel more confident rather than less confident, that a pause to inform people can meaningfully impact care for this rare type of blood clot, and thinking that until one looks at the data who knows how big the problem might be and one shouldn’t assume the math is right until you check it, so we should halt and catch fire for a day and then quickly convene a meeting to confirm that this is only going to kill one person in six million.
Even in a world in which the initial pause wasn’t crazy, there was a meeting the next day to go over the information, and the decision was made to wait 7-10 days and then meet again without making a choice about the pause (and obviously, here, if you choose not to decide you still have made a choice). They didn’t even make the ‘compromise’ decision of halting for young women (and yes, ‘people who are in the subpopulation that is often on birth control which causes orders of magnitude more blood clots than this seems like it’s a hint on what’s happening) and continuing for everyone else, since you can then swap doses between different groups and keep up your pace of vaccinations while you ‘investigate further’ whatever that means here. The failure to at least make that decision is obviously completely bonkers even if you somehow think the initial decision to halt and catch fire was reasonable, as laid out in this thread by someone who supported the first decision but at least supported the ‘compromise’ option at the meeting.
Here’s an argument that this isn’t so bad in the United States, as it will mostly only destroy faith in Johnson & Johnson, rather than faith in the mRNA vaccines as well, or all vaccines generally:
FDA Delenda Est. The FDA must be destroyed.

At a minimum, while we prepare to do that, we can at least implement Tyler’s modest proposal.
Let’s run the (other, not equal to one or six) numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 5.9% (up 0.4%) and deaths decline by 8%.
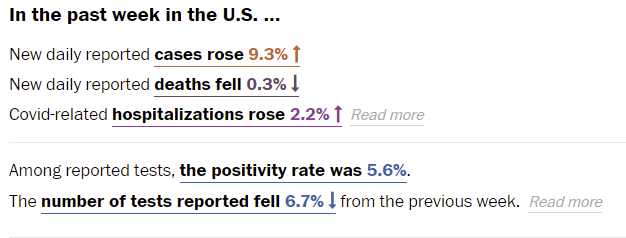
Once again Washington Post’s numbers baffle me, although this being six rather than seven days later makes them not impossible. Somehow tests fell, cases rose, and the positivity rate barely budged.
A key question whenever one gets good news on deaths is whether this is good news or whether it’s time shifted. If it’s cases shifting into the future, it means the next week looks doubly worse and on top of that you were fooled by what looked like a downward trend. Similarly, bad news can be a mirage from old cases. It now looks like the death rate decline has stalled out, which is unfortunate.
Predictions for next week: Positivity rate of 5.8% (up 0.2%) and deaths unchanged.
Deaths
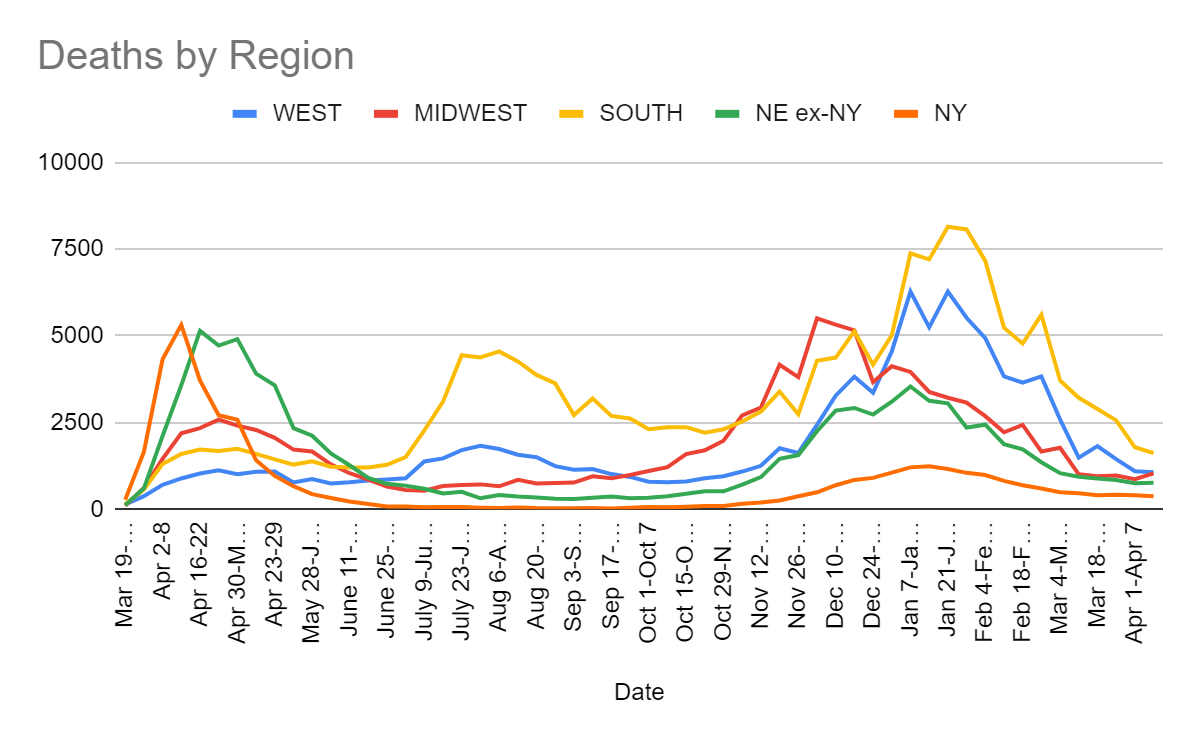
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Feb 25-Mar 3 | 3834 | 1669 | 5610 | 1958 | 13071 |
| Mar 4-Mar 10 | 2595 | 1775 | 3714 | 1539 | 9623 |
| Mar 11-Mar 17 | 1492 | 1010 | 3217 | 1402 | 7121 |
| Mar 18-Mar 24 | 1823 | 957 | 2895 | 1294 | 6969 |
| Mar 25-Mar 31 | 1445 | 976 | 2564 | 1262 | 6247 |
| Apr 1-Apr 7 | 1098 | 867 | 1789 | 1160 | 4914 |
| Apr 8-Apr 14 | 1070 | 1037 | 1621 | 1145 | 4873 |
Half or more of the Midwest increase is quirky data in Missouri, but that doesn’t make any of this good news, and it’s likely deaths are going to now be stable or go slightly up, along with cases, until we get enough vaccinations to turn things around.
Cases
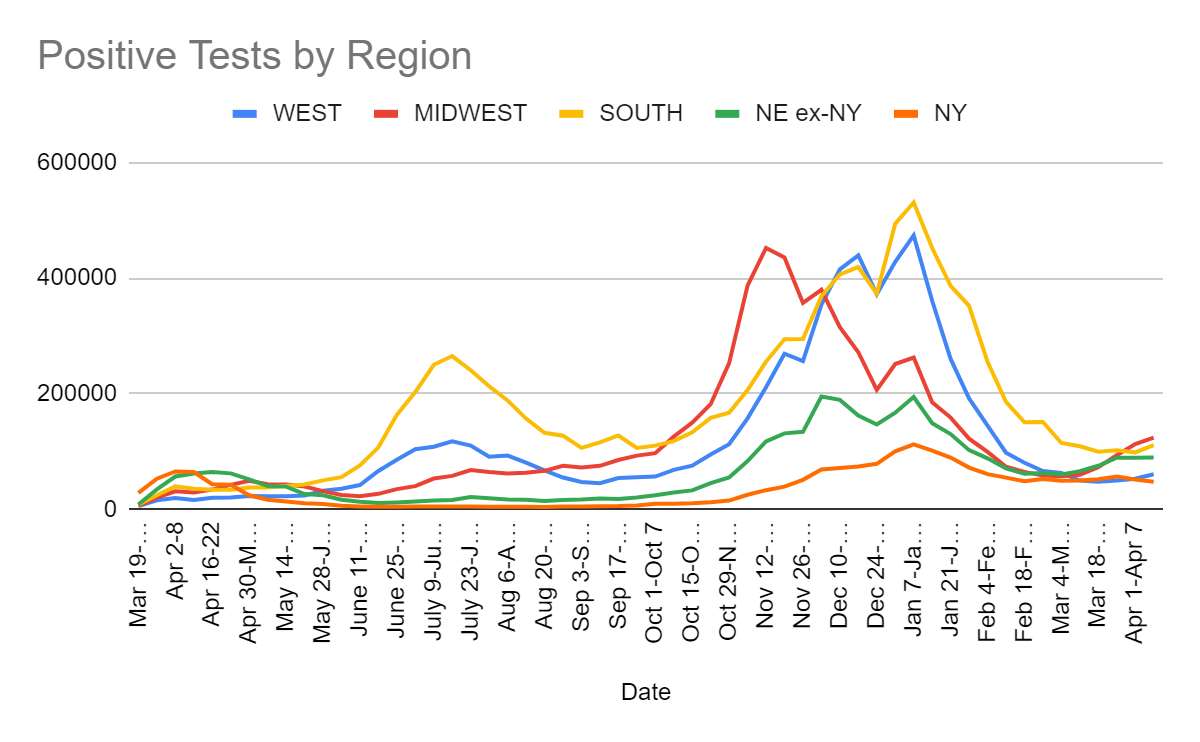
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Feb 25-Mar 3 | 66,151 | 58,295 | 151,253 | 115,426 |
| Mar 4-Mar 10 | 62,935 | 57,262 | 114,830 | 109,916 |
| Mar 11-Mar 17 | 49,696 | 59,881 | 109,141 | 115,893 |
| Mar 18-Mar 24 | 47,921 | 72,810 | 99,568 | 127,421 |
| Mar 25-Mar 31 | 49,669 | 93,690 | 102,134 | 145,933 |
| Apr 1-Apr 7 | 52,891 | 112,848 | 98,390 | 140,739 |
| Apr 8-Apr 14 | 60,693 | 124,161 | 110,995 | 137,213 |
Looking at this chart, it seems clear the Midwest’s problems are real. The finale wave is out in force there, even if it’s relatively tame in other places.
Given the increase in positive tests, and the report of a continued decline in test counts, I’m willing to believe that positive rates did go up ~0.4% in the past week, which Johns Hopkins confirms (although they have lower numbers on both ends than WaPo does), so the prediction miss was mostly about doing it based on Friday’s number or some similar quirk (or a math error on their end somewhere).
Things in many places other than the United States are quite bad. In India, they surpassed 200,000 cases per day and things are rapidly getting worse, and there are many other places that have big problems. Aside from the places that successfully did full suppression, the places doing actively well are the ones with strong vaccination campaigns. Facing the new strains while not keeping up in vaccinations is a very bad place to be right now.
Vaccinations

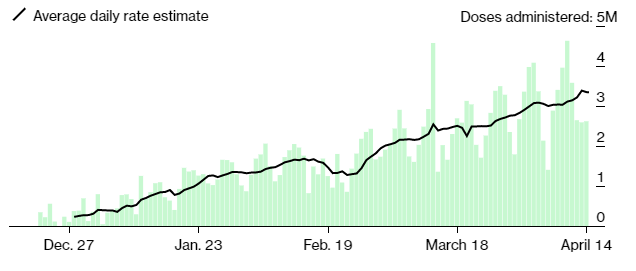
That small decline at the end might have something to do with the J&J suspension, or it could mostly be a random quirk. Either way, even without J&J, we still should be able to continue slowly expanding our vaccination rates until we hit a wall where we run out of people who want a shot put into their arm. There are signs this is starting to be an issue in some places, but mostly there’s still plenty of people eager to put the pandemic behind them.
As furious as I am at the J&J suspension, and as many people as it’s going to kill (most of which will be from disadvantaged groups and areas, which J&J’s one shot at room temperature made much easier to reach), it is important not to lose perspective. J&J was a small portion of our vaccine effort, and case growth is not that rapid, so it’s not going to kill hundreds of thousands of people, at least not in America. If we’re lucky, it will only kill thousands.
Vaccine Passport Hype
Washington Post reports on New York’s Excelsior pass, the first one of its kind. Conclusion was that it’s relatively easy to use and isn’t got reasonable privacy protections given the circumstances, but that unless you’re counting on ID to catch fraud it’s trivial to fake it via copying someone else’s pass. That sounds about right. It’s clear by now that there isn’t going to be a national system and that New York is the exception rather than the rule. That doesn’t render the questions moot, but it lowers their urgency and importance quite a lot.
Tyler’s position is that we should be planning full reopening, and that passports seem more likely to hinder that than help. That’s one of the key disagreements. Is the alternative to passports a full reopening, or is it more restrictions? My guess remains that not being able to check leads to more restrictions in the medium term (next few months), but there’s a point when that flips, and things that would have fully reopened without checking would, if given the opportunity to easily check vaccine status, continue to check that status for a while longer. We then have to balance these needs. My guess is that the ‘overtime’ period’ is 50% to last at least two months or so, but highly unlikely (<10%) to last for six, and that the ‘extra game time’ period when passports would help starts now and has at least three months to go most (75%) of the time, and there’s a decent chance (25%) it’s six months or more in at least many blue areas, so one can do a cost/benefit calculation with this plus all the other objections. Here I’m counting the extra restrictions as pure downside, because even with them the net risk is likely higher than with the pass, unless we’re checking physical cards at the door, which is a different cost/benefit tradeoff.
The other half of that is the argument from focus. If the country and discourse only have so many focus points (Imperial Focus Points!), which seems basically right, then it’s plausible that all the work on passports delays the full reopening not because of lowering the costs of not reopening fully, but by preventing the attention and blame pressure required to generate the reopenings. Doing anything at all, in this model, has high opportunity costs. I don’t think I value this as highly as Tyler but I’ve likely not been giving it its due.
Vaccines Still Work
The J&J suspension goes hand in hand with the ongoing campaign to convince the public that vaccines work, but don’t work in the sense of accomplishing anything for people. In the name of some combination of proving one’s Very Serious Person credentials, maximizing the quantity of economic harm and scaring people as much as possible, there’s a competition on how to give the impression that being out there is unsafe for the fully vaccinated.
Zeynep points us to an especially creative entry here:
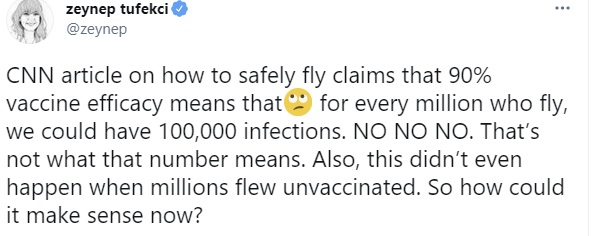
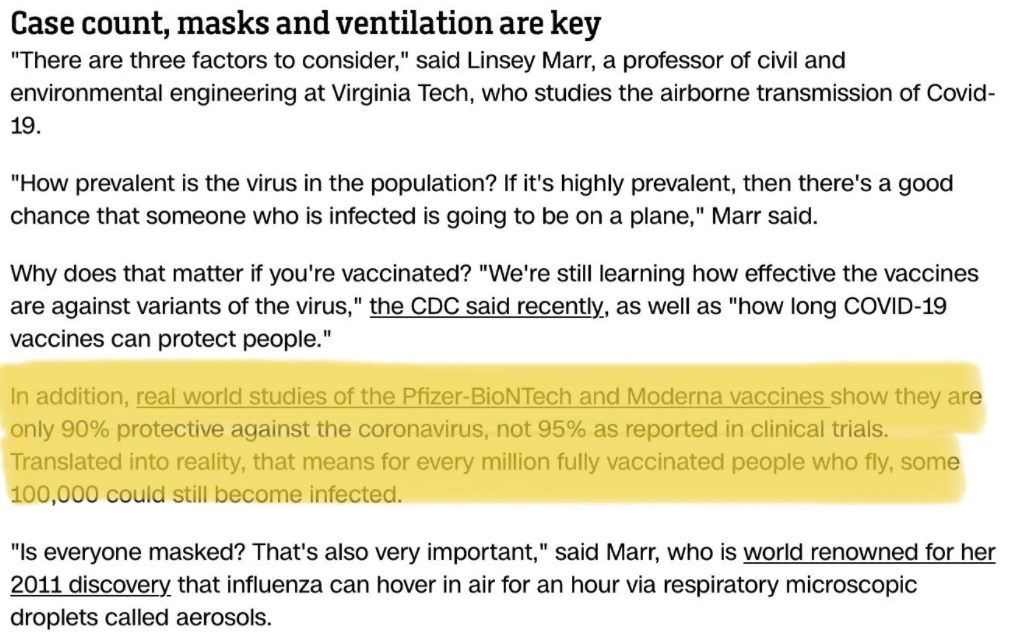
What CNN is saying might be technically correct. A model where 90% of people who are vaccinated are fully safe, while 10% remain at similar risk to before vaccination, is simplified but mostly plausible. What CNN is technically saying here is that there are 100k people who are being exposed to possibly getting infected (look around, could it be you?) and Zeynep is pointing out that this is damn well written to give the ordinary person the impression that if we didn’t Do Something About It that one in ten people who fly vaccinated would get infected, so if you’re vaccinated and fly that way there’s a 10% chance you get infected, which is of course complete nonsense.
Even without this willful mislead it’s still terrible and leads to scaremongering, but this here is something special. There should be some kind of award for such things.
Also, Nate Silver is correct here, and it would be dishonest to treat ‘we don’t know if vaccinated people can transmit’ FUD spreading as anything but gaslighting.
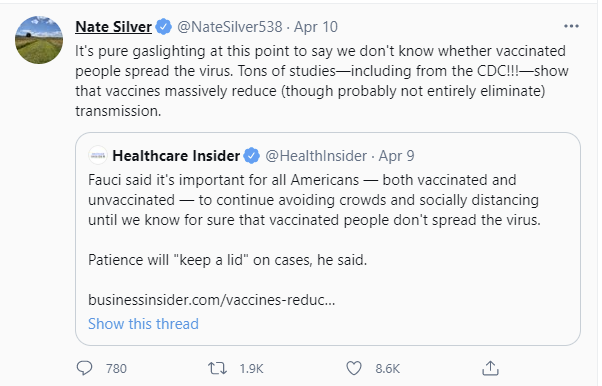
Here’s the Business Insider article linked there, which notes:
Vaccinated people are almost certainly less infectious when they do get infected, on top of not getting infected. The reduction in risk to others is ‘we don’t know’ to the extent that it might be much safer than the 90-95% range in which it reduces risk of infection.
Anyone who tells you otherwise is either lying to you, or is believing the lies told to them by others. Those who continue to treat vaccinated people as risky to others, and avoid living life on that basis, are making a choice to not live life in order to send some sort of social message or tell themselves a story about the type of person they are, or some other not-physical-reality based motivation. Or they just aren’t that into you and it’s a convenient excuse.
That doesn’t mean risk for the vaccinated is zero, precautions that are cheap are worth taking and ‘stupid stuff’ is worth avoiding, and one should follow mask norms for social reasons cause it’s really not that big a deal, but on this ‘we don’t know if it works’ thing, seriously: Stop. Just stop.
Similarly, Zeynep has a thread here about wildly misleading headlines about effectiveness of the vaccines against variants. Studies that find the vaccines work fine are being reported as ‘vaccines don’t work as well’ in a way that has nothing to do with any practical implications. The practical implications are that they work just fine, thanks, and it’s so clear I’m not even going to go into it beyond that. Attempts like this one to scare people about this are pure gaslighting.

And act more like this (video, which is living its best life):
Which is why this is basically where we are:
That’s before the whole Johnson & Johnson mess.
In Other News

I mean, at least it’s true.
More support for first doses first. As Tyler notes, it’s too late for America to benefit from this, but the rest of the world still could. The same goes for fractional dosing. From what I’ve seen, a lot of people are having a really unpleasant day or two after the second dose of Moderna, and my strong hunch is the severity is caused by using a dose that’s twice as big as it needs to be, and it would be actively better for them to get half doses plus we’d have twice as many doses to give out.
Canadians return home via taxis from Buffalo to avoid quarantine. They did indeed solve for the equilibrium.
Australia might not open its borders even after full vaccination. The hypothesis that Australia succeeded because it was using good epistemics to make decisions is not holding up well in the endgame.
Covid Tracking Project offers thoughts on data source issues. I miss them deeply.
37 comments
Comments sorted by top scores.
comment by danohu · 2021-04-15T18:08:46.572Z · LW(p) · GW(p)
There's another big reason for the jump in vaccinations in Germany (and the rest of the EU): We've just started a new quarter.
Yes, really.
The discussion on manufacturers vaccine production schedules have largely been on numbers per quarter. Given that the EU is scapegoating them for delays, the manufacturers really really want to avoid missing their targets. And that leads to weirdness at the boundaries of the quarters.
Here's the data on deliveries in Germany
At Biontech, production is going well, and they are comfortably meeting their Q1 commitment (~12m doses). But they have promised to almost quadruple that in Q2. So through March they delivered a steady 1m doses per week. Then in April, when we start counting against their Q2 target, the deliveries jump to 2.7 million per week.
AstraZeneca are the opposite. They are behind schedule. So they squeezed in a huge delivery at the end of Q1 (actually a couple of days later, but it's being counted as Q1), like maybe 5x what they usually deliver in a week.
It's rational behaviour from both companies. When you're dealing with a short-tempered and annoying customer, you CYA by fulfilling the letter of your contracts, even at the cost of a worse outcome for the customer. And that's the position the EU have put Biontech and AZ into
[EDIT: I should add that this is entirely speculation, but I do think it fits the facts and the (non-altruistic parts of the) motivations of everybody involved]
comment by Cesare · 2021-04-15T14:16:29.478Z · LW(p) · GW(p)
Thank you. It resonated with me.
I hope that, eventually, in the distant future, someone holds someone else accountable.
↑ comment by romeostevensit · 2021-04-16T00:02:29.359Z · LW(p) · GW(p)
This highlights an, I think, neglected angle of analysis of civilizational problems. I almost want a deity of diffusion of responsibility. One of Moloch's most faithful servants.
When looking back on an earlier era one has the benefit of conceptual distinctions that didn't exist at the time. Looking back on our era, I think people will be surprised that we had dim understanding of responsibility and credit taking being able to diverge, and in fact optimized to diverge.
Replies from: adrian-arellano-davin↑ comment by mukashi (adrian-arellano-davin) · 2021-04-16T03:14:30.723Z · LW(p) · GW(p)
I hope so too. A perverse effect of letting every state/region/city handle the pandemics by themselves is that, in most countries, those states/regions/cities are normally governed by different parties. When everyone is responsible for the disaster no one is!
As you say, we need to wait for the distant future for some justice.
comment by Measure · 2021-04-15T14:43:15.899Z · LW(p) · GW(p)
Can people who are prevented from getting the J&J vaccine due to the suspension and later get Covid sue the FDA?
Replies from: jimrandomh↑ comment by jimrandomh · 2021-04-15T15:46:09.275Z · LW(p) · GW(p)
No. The FDA is fully immune to lawsuits related to its decisions, no matter how moronic.
Replies from: Daniel_Eth, None↑ comment by Daniel_Eth · 2021-04-20T20:28:23.591Z · LW(p) · GW(p)
This is probably a good thing - I'd imagine that if you could sue the FDA, they'd be a lot more hesitant to approve anything.
Replies from: jimrandomh↑ comment by jimrandomh · 2021-04-20T22:40:45.572Z · LW(p) · GW(p)
Certainly if lawsuits were allowed for approving things but not allowed for failing to approve things, that would be a disaster. But the issue here isn't that they approved something they shouldn't have, it's that, faced with extremely time-sensitive approval decisions, they keep dragging their feet and waiting weeks while not appearing to do anything in the mean time, ie failing to do their job promptly. If they could be sued for that, it would likely be an improvement.
Replies from: Daniel_Eth↑ comment by Daniel_Eth · 2021-04-20T23:06:09.718Z · LW(p) · GW(p)
I think in practice allowing them to be sued for egregious malpractice would lead them to be more hesitant to approve, since I think people are much more likely to sue for damage from approved drugs than damage from being prevented from drugs, plus I think judges/juries would find those cases more sympathetic. I also think this standard would potentially cause them to be less likely to change course when they make a mistake and instead try to dig up evidence to justify their case.
↑ comment by [deleted] · 2021-04-15T21:17:11.192Z · LW(p) · GW(p)
Technically speaking that isn't true but practically speaking it is. (Just like technically speaking you could write a letter of complaint to Stalin)
Congress could find their behavior so egregious they pass a law authorizing you to sue.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-04-20T09:41:55.218Z · LW(p) · GW(p)
Well, if we are involving Congress there are even better remedies than litigation.
comment by Adam Zerner (adamzerner) · 2021-04-15T16:52:44.322Z · LW(p) · GW(p)
Any updates regarding your thoughts on herd immunity?
Replies from: CraigMichael↑ comment by CraigMichael · 2021-04-16T00:02:52.051Z · LW(p) · GW(p)
Would like to hear about this too.
comment by GeneSmith · 2021-04-16T04:19:10.882Z · LW(p) · GW(p)
I think Garret Jones's tweet is potentially misleading. One of the people in the comments mentioned that BioNTech increased their vaccine deliveries by 2.5x coinciding with the approval to vaccine at doctor's offices.. I tried to independently verify this but wasn't able to find an article. However I checked the profile of the guy who tweeted it and he seems to pretty regularly publish updates about the vaccine reserves in Germany, so my guess is he's credible.
Perhaps Germany allowed general practitioners to administer the vaccine precisely because they finally had too many vaccines to be used by the specialty clinics?
comment by agc · 2021-04-15T15:33:52.161Z · LW(p) · GW(p)
Things i have wondered about this week:
- The UK has vaccinated a larger share than the US, although America is catching up. Still, US states seem to be opening up to all adults very soon, while the UK is only going to 45+. Why is that? My current theory is that the UK has much higher vaccine take up among older people.
- Why is Japan doing so few vaccinations? They could afford afford it and surely have the organizational capacity. Are they so confident that they can control the virus that they don't bother? Are kindly letting the west have the vaccine first since we clearly need it?
- Are there factories out there that could be making COVID vaccine but aren't? In theory there shouldn't be because Pfizer, AstraZeneca, J&J and others should rationally be subcontracting to others to manufacture for them. Worldwide demand should be easily big enough to justify it. Yet I'm not sure.
↑ comment by Zac Hatfield-Dodds (zac-hatfield-dodds) · 2021-04-16T02:10:34.839Z · LW(p) · GW(p)
Worldwide demand should be easily big enough to justify [subcontracting manufacturing]
If it was legal to sell vaccines for the market price, or anywhere near their actual value, of course. Thanks to monopsony purchasers (i.e. irrationally cheap governments), we instead see massive underproduction.
↑ comment by Tom Richards (tom-richards) · 2021-04-17T09:54:33.795Z · LW(p) · GW(p)
Anti-vax sentiment is much rarer in the UK than in the US (or indeed most countries). It would be very surprising if uptake in the UK were not significantly higher.
There is as yet no significant national policy response to the prospect of possible escape variants. In particular, the current plan is to use August to vaccinate children, when I think a better use of the infrastructure at that point would probably be to give Pfizer/Moderna/Novavax to people who got AZ first time round in a bid to stave off a potential Autumn wave of B.1.351, B.1.617 or some other variant (assuming AZ's apparent underperformance against B.1.351 is real and generalizes to other similar variants, as I think likely).
↑ comment by Cesare · 2021-04-15T17:23:09.675Z · LW(p) · GW(p)
The real answer is Astrazeneca. More than half of vaccinated people in the UK have been vaccinated with Astrazeneca... and they are concerned about the actual effectiveness of this vaccine, and possible variant outbreaks (there have been three instances of "surge testing" where they go door-to-door following an outbreak: https://www.gov.uk/guidance/surge-testing-for-new-coronavirus-covid-19-variants). According to Eric Topol (whose opinion is based on a few studies), Astrazeneca is not effective against B.1.3.5 (south-african variant).
Due to effectiveness of Pfizer and Moderna, the US (and Israel) can afford to relax restrictions much more than their european counterparts.
↑ comment by gjm · 2021-04-16T02:12:56.566Z · LW(p) · GW(p)
I think you're answering a different question from the one agc is asking. Unless I misunderstood, agc was asking why the UK isn't yet vaccinating people younger than 45. Being able to relax restrictions more in the US wouldn't explain that.
I think the actual answer is that the UK very promptly secured a pretty decent quantity of vaccines (mostly AstraZeneca), enough to vaccinate quite a lot of its population, but that while the US was slower it then got hold of more relative to population size, and now the US has more plentiful supply than the UK.
Replies from: Cesare↑ comment by Cesare · 2021-04-16T11:12:40.598Z · LW(p) · GW(p)
I didn't word it very well, the original thought got lost along the way, thanks for pointing it out!
I meant to conclude that since the UK cannot afford to lift restrictions for vaccinated people then they follow the logical route of vaccinating by age cohorts: this will keep deaths as low as they can be.
However, in the US they are actually enabling vaccinated people to do stuff... which will boost the economy significantly, and they can afford to do so due to the degree mRNA vaccines seem to block transmission. So it makes sense to allow anyone that wants to be vaccinated to do that, instead of the inevitable slowdown caused by using an age restrictive criterion.
comment by tkpwaeub (gabriel-holmes) · 2021-04-20T09:40:07.384Z · LW(p) · GW(p)
I agree that it was probably a mistake to pause for a whole week. However, they were correct to look into the matter. May I reframe this a bit? (I still plan on writing my own, more comprehensive piece on all this - your posts are helping me sort this out).
Deep breath - here goes.
-
We are asking people to get vaccinated for the common good - because there's an emerging consensus that all the vaccines help mitigate transmission.
-
It really does appear that for some vaccines (the ones using adenovirus vectors), there's an increased risk of a very rare type of blood clot for some people (women 18 to 55). The personal risk of death from Covid for that group is lower than it is for the general population.
In other words, we're asking some people to put their lives on the line for the common good. Yes, the absolute numbers are small, but that shouldn't be a distraction. Women between 18 and 55 need to be offered mRNA vaccines first. Everybody else should consider it their civic duty to get an adenovirus vector vaccine. And women between 18 and 55 who get one of the adenovirus vector vaccines need to be fully informed and at the very least sincerely thanked - possibly with money.
Replies from: philh↑ comment by philh · 2021-04-20T17:15:02.419Z · LW(p) · GW(p)
In other words, we’re asking some people to put their lives on the line for the common good.
As a note, this doesn't yet follow from your (1) and (2). It would follow from a stronger version of (2), in which these people are more likely to die if they get this vaccination than if they don't. (Roughly, more likely to die from this vaccination than from Covid - but the vaccine risk is conditional on getting vaccinated, and the Covid risk is conditional on not getting vaccinated, not conditional on getting Covid.)
Replies from: gabriel-holmes, gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-04-21T00:53:12.836Z · LW(p) · GW(p)
Fair enough. I believe that it's been noted that in some places (Australia) the stronger version of (2) really does hold. I'm not sure if (1) still holds, but it's conceivable that it could. Either way, you're comparing two very small numbers and my meta-point is that it's still something that bears analyzing. Thanks for keeping me on my toes.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-04-21T00:55:16.171Z · LW(p) · GW(p)
I could also add #3 - non-pharmaceutical interventions are still perfectly legit.
comment by Vitor · 2021-04-17T10:27:35.540Z · LW(p) · GW(p)
News from Switzerland: health authorities have made the decision that people who had covid should only get one vaccine shot, 6 months after recovery. This sounds sensible to me, but I'm worried what this means regarding different strains: if someone was infected by the milder variant, aren't they still at high risk from the newer strains? Anyplace else pursuing similar policies?
comment by Zac Hatfield-Dodds (zac-hatfield-dodds) · 2021-04-16T02:04:25.422Z · LW(p) · GW(p)
The hypothesis that Australia succeeded because it was using good epistemics to make decisions is not holding up well in the endgame.
From Australia, this hypothesis was only ever plausible if you looked at high-level outcomes rather than the actual decision-making.
We got basically one thing right: pursue local elimination. Without going into details, this only happened because the Victorian state government unilaterally held their hard lockdown all the way back to nothing-for-two-weeks, ending our winter second wave. Doing so created both a status quo and (having paid higher-than-if-faster costs) a very strong constituency for elimination.
Victoria remains the only area with non-negligible masking. Nationwide, we continue to make expensive and obvious mistakes about handwashing, distancing, quarantine, and appear to be bungling our vaccine rollout.
Zero active cases and zero local transmission covers a multitude of sins. I attribute the result as much to good luck as epistemic skill, and am very glad that COVID is not such a hard problem that we can't afford mistakes.
Replies from: adrian-arellano-davin↑ comment by mukashi (adrian-arellano-davin) · 2021-04-16T03:05:59.656Z · LW(p) · GW(p)
Strongly disagree. Australia has done many things right:
- Close the borders early (and close them for real)
- Very efficient contact tracing. Even after months with 0 cases, we still are asked to sign up to every bar we visit
- 2 weeks supervised quarantines for returning Australians
- Very quick reactions as soon as one case is detected in the community, e.g. Queensland lockdown from a few weeks ago
- Tons of testing
Etc
Handwashing has no effect on the transmission of the virus. Distancing is meaningless if there are no cases.
I will concede though that the vaccine rollout is being inefficient, but it does not have such a high cost: people are not dying in the thousands. Australia can afford that.
Deaths in the USA (correcting per population) are 50 times higher than in Australia.
Replies from: zac-hatfield-dodds↑ comment by Zac Hatfield-Dodds (zac-hatfield-dodds) · 2021-04-16T05:35:06.623Z · LW(p) · GW(p)
I don't think we're actually disagreeing much about outcomes (which I agree have been great!), or even that Australia has competently executed at least enough of the important things to get right. Of the five items you mention I'd include borders, quarantine, snap-lockdowns, and testing as part of the local elimination policy; we haven't done them perfectly but we have done them well enough.
I understand "using good epistemics to make decisions" to require that your decisions should be made based on a coherent understanding and cost-benefit analysis of the situation, even if both might change over time. "Merely" getting good outcomes doesn't count!
For example, we still encourage pointless handwashing and distancing while iffy on masks or ventilation - and because we got to zero transmission in other ways, that's OK. Similarly, it's true that Australia's slow vaccine rollout hasn't cost many lives so far and I hope that neither winter nor variants change that. The cost-in-expectation of an unlikely outbreak should still drive faster vaccination efforts IMO, especially when e.g. increasing local production is not zero-sum.
comment by cistran · 2021-04-19T06:57:32.957Z · LW(p) · GW(p)
Here is another ironman for FDA decision based on nothing at all. What if they are scared of unknown long term effects and take any confirmed problem as a red flag pointing to unknown long term effects. This would push them away from moustache twirling villains category.
comment by Primer (primer) · 2021-04-16T20:16:29.683Z · LW(p) · GW(p)
Why are we saying "stopping J&J and AstraZeneca is a terrible idea, even if it was for younger women only" but on the other hand we don't question that around 20% of the population (those younger than 18yrs) will not get any vaccine at all in 2021?
Replies from: cistran↑ comment by cistran · 2021-04-19T06:53:15.535Z · LW(p) · GW(p)
People between 12 and 16 not getting vaccines by the end of 2021 is not even a 90% proposition. Studies are already underway for this age cohort, and it is plausible that a vaccine will be available for teenagers as soon as September of this year.
Replies from: primer↑ comment by Primer (primer) · 2021-04-29T17:31:54.003Z · LW(p) · GW(p)
The clinical trials on children by Moderna and Biontech have end dates somewhere in 2022, thus I had supposed we won't see any approval in 2021. That assumption seems to be wrong and I'm happy to stand corrected.
I still believe we're missing something when we complain about the "abundance of caution" concerning 19 year old women, but hardly talk at all about the abundance of caution delaying vaccinations of a 15yo.
comment by jo lima (jo-lima) · 2021-04-19T21:14:25.743Z · LW(p) · GW(p)
What weirds me out most about this is that we find this pattern in so many countries - this article states that 18 countries have halted the use of AstraZeneca. (As far as I know some have started again, others have limited the use to certain demographics and others have stopped its use all together).
Are they really all simply "COMPLETE MORONS" or is there a better explanation?
Replies from: jo-lima↑ comment by jo lima (jo-lima) · 2021-04-19T21:32:02.393Z · LW(p) · GW(p)
Just calculated one answer to my question: for me as a 30 year old the chance of dying of Covid19 is about 200 / 1.000.000 - IF I get it. Currently in Berlin the chance of infecting myself is around 5% according to https://covid-o-mat.de - so these two possibilities multiplied are 0,0001 or 0,001 %. If I take Astra Zeneca my chance of getting a serious brain thrombosis seem similar. If you just look at these possibilities it seems more understandable why governments don't want to take the responsibility to advise younger people to take the vaccine. (In Germany I think I can still get it - on my own risk and after counselling a doctor).
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-04-20T09:47:59.750Z · LW(p) · GW(p)
Yup, especially if you keep up the non-pharmaceutical interventions.