Covid 12/17: The First Dose
post by Zvi · 2020-12-17T14:20:01.106Z · LW · GW · 29 commentsContents
The Numbers Predictions Deaths Positive Tests Test Counts Positive Test Percentages Covid Machine Learning Projections Europe All I Want For Christmas is a Covid Vaccine Everything Matters Versus Nothing Matters Further Research Is Needed You Should Know This Already (Inessential Reminders) In Other News None 29 comments
The Pfizer vaccine is being deployed to health care workers and long-term care facility residents. The Moderna vaccine is close behind, with the full FDA report already out. There were some small extra delays thrown in for good measure, on the order of a few days, that doubtless killed a few people but shouldn’t delay the overall path of events. We are now in the vaccination stage of the pandemic. If the trial results are to be believed in detail, by the end of next week those getting the first dose will largely already be immune, and the population immunity effects can begin to compound and help turn the tide. They will start out small, but soon start growing faster, and every little bit helps.
There even seems to be a good chance that overall new infections would have already peaked if not for worries about Christmas and New Year’s coming up soon. Positive test percentages seem to be starting to even out or slowly decline as we get clear of Thanksgiving, and death rates are not rising as much as they would be rising in the scenario where data snags and testing issues were the only reason we didn’t notice things getting even worse than they are. If anything, death rates suggest a better picture than the positive test counts.
In other great news, Over the counter $30 Covid-19 test approved by FDA. It’s official. Woo-hoo! Three million over the counter tests this month, then they ramp up production. We could have done this a long time ago and solved the whole pandemic, and instead it’s going to be a drop in the bucket that shows up late to the party, but every little bit helps.
Alas, as always, none of that changes the short term situation much. There’s lots of Covid-19 out there, and if anything there are even more reasons to play it safe right now. Large Christmas gatherings or New Year’s parties are a profoundly bad idea.
In many ways, it seemed like this week was mostly ‘cut to one week later’ with few if any surprises, except for the approval of the first at-home Covid-19 test.
Let’s do the numbers.
As a bonus, here is someone else running their version of the numbers on a state level. He does this monthly, and they’re useful graphs with solid commentary. It’s a generally good newsletter.
(Technical note: Brief uncredited screenshots whose source isn’t obvious are from CNBC live update page or CNN live update page. I’m experimenting with this as a quick way to get sourced info across, let me know if you think it’s a good idea to keep doing this.)
The Numbers
Predictions
We got a peak. Test count and deaths were close, the positive rate went small down instead of small up.
Last week’s prediction: I predicted a 14.3% positive rate on 11 million tests, and an average of 2,550 deaths per day.
Results: We got a 13.5% positive rate on 10.95 million tests, and an average of 2,617 deaths per day.
Prediction: 13.1% positive rate on 11.5 million tests, and an average of 2,850 deaths per day.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 15-Oct 21 | 804 | 1591 | 2370 | 523 |
| Oct 22-Oct 28 | 895 | 1701 | 2208 | 612 |
| Oct 29-Nov 4 | 956 | 1977 | 2309 | 613 |
| Nov 5-Nov 11 | 1089 | 2712 | 2535 | 870 |
| Nov 12-Nov 18 | 1255 | 2934 | 2818 | 1127 |
| Nov 19-Nov 25 | 1761 | 4169 | 3396 | 1714 |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
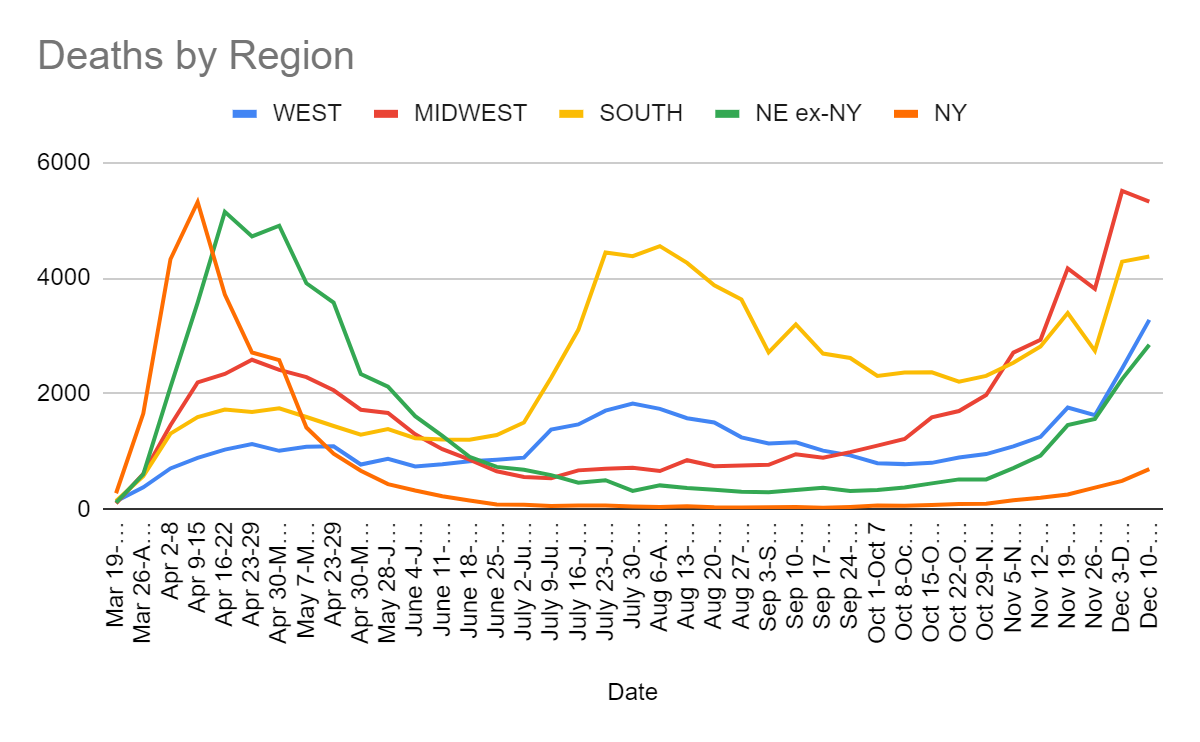
I interpret this as a backlog of deaths from previous weeks showing up in the Dec 3-Dec 9 reporting in the Midwest and South, with the numbers we see this week being about where the real death rates are once again, and things still getting worse everywhere given the lag. The Northeast and West numbers came in a little higher than I expected, which cancelled out, but nothing here seems too surprising. Peaks outside of the Midwest are likely still at least a few weeks away, but I do not expect things to get that much worse than they are now before they turn around.
Positive Tests
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 15-Oct 21 | 75571 | 149851 | 133238 | 43325 |
| Oct 22-Oct 28 | 94983 | 181881 | 158123 | 57420 |
| Oct 29-Nov 4 | 112684 | 252917 | 167098 | 70166 |
| Nov 5-Nov 11 | 157495 | 387071 | 206380 | 108581 |
| Nov 12-Nov 18 | 211222 | 452265 | 255637 | 150724 |
| Nov 19-Nov 25 | 269230 | 435688 | 294230 | 170595 |
| Nov 26-Dec 2 | 256629 | 357102 | 294734 | 185087 |
| Dec 3-Dec 9 | 354397 | 379823 | 368596 | 263886 |
| Dec 10-Dec 16 | 415220 | 315304 | 406353 | 260863 |
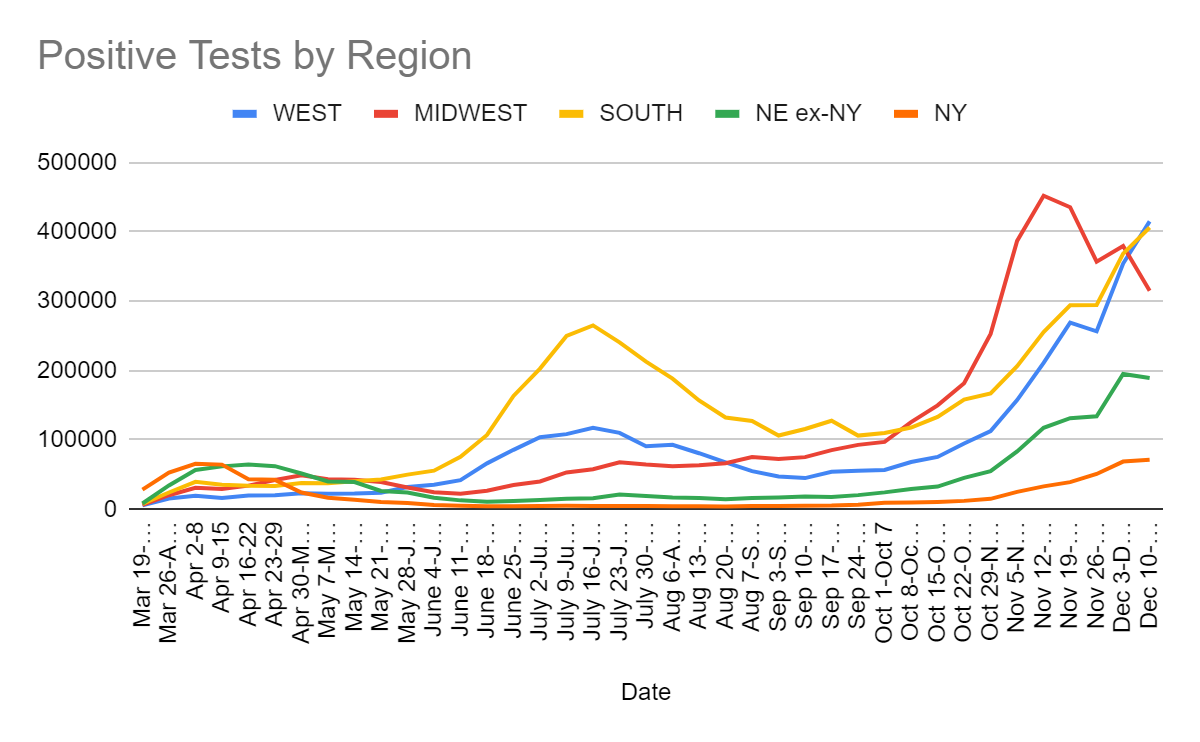
Seems clear the Northeast got ahead of itself last week and that has now been smoothed out but is still getting worse, the Midwest has peaked, and the West and South are in trouble. As usual, I rely more on the test percentages
Test Counts
Positive Test Percentages
| Percentages | Northeast | Midwest | South | West |
| 10/15 to 10/22 | 2.95% | 8.70% | 7.85% | 5.36% |
| 10/22 to 10/28 | 3.68% | 9.87% | 8.58% | 6.46% |
| 10/29 to 11/4 | 4.28% | 12.79% | 8.86% | 7.04% |
| 11/5 to 11/11 | 5.56% | 17.51% | 9.89% | 8.31% |
| 11/12 to 11/18 | 6.99% | 18.90% | 11.64% | 10.66% |
| 11/19 to 11/25 | 7.00% | 16.62% | 10.41% | 11.75% |
| 11/26 to 12/2 | 8.38% | 17.90% | 12.45% | 12.79% |
| 12/3 to 12/9 | 10.47% | 17.94% | 13.70% | 12.76% |
| 12/10 to 12/16 | 10.15% | 15.63% | 15.91% | 13.65% |
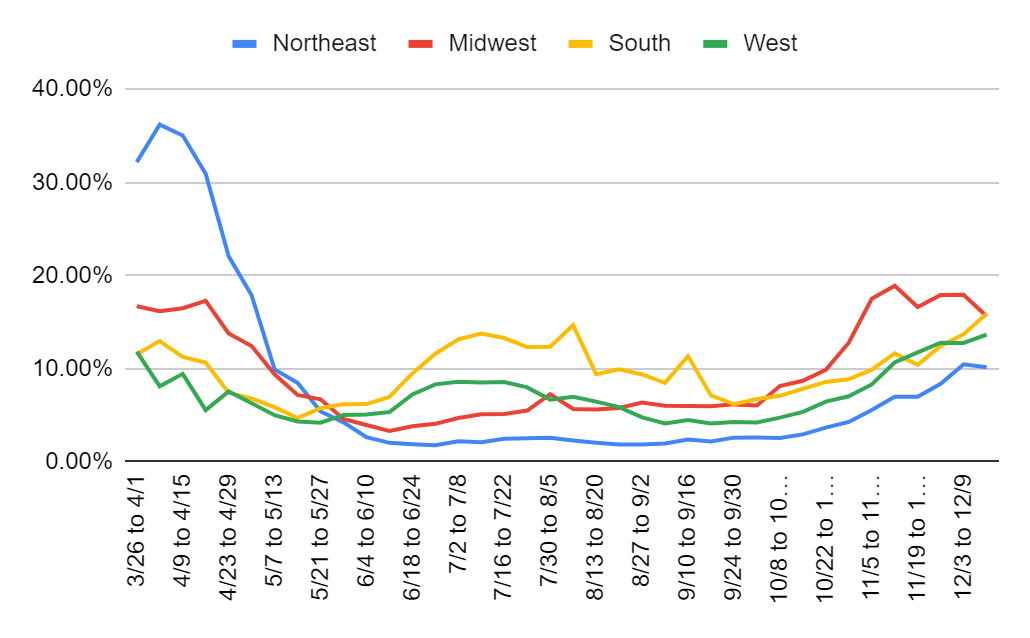
I’m ready to believe the Midwest is headed in the right direction. I am not ready to believe the Northeast is following suit quite yet. That seems much more likely to be a blip and nothing more, although the snowstorm outside my window at the moment might slow things down a bit – being forced inside is not great but no one leaving the house at all is actively useful. Thus I think the baseline scenario is that the Midwest continues to drop. The South is the opposite case, with this number coming in a bit ‘too high’ so I expect it to level off a bit next week despite the true number of infections likely still rising a bit.
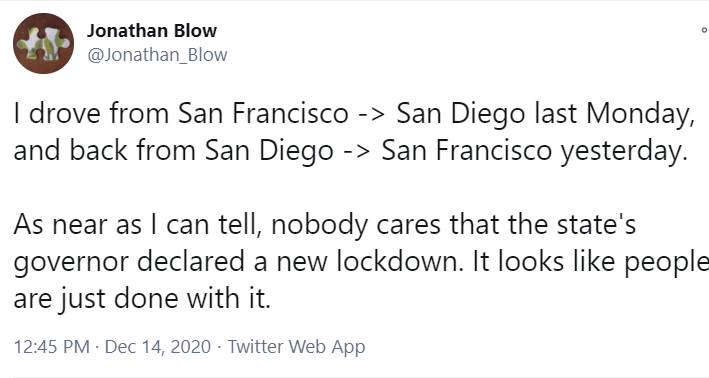
It is worth noting that California is now at 11.9% positive tests. The attempts to lock things down aren’t working, presumably because they are not locking things down due to being sick of it all, and also because they’re going after the wrong things too harshly with no end date in sight, and forcing people into all-or-nothing choices. That’s also despite weather that shouldn’t create as big a winter crisis as other areas. The counter-argument is that things might have been about to go the way of Arizona (32%), Colorado (28%), Idaho (47%) or Nevada (40%), but Oregon (5%) and Washington (8%) seem like better parallels and thus a strong counter-argument to that.
Covid Machine Learning Projections
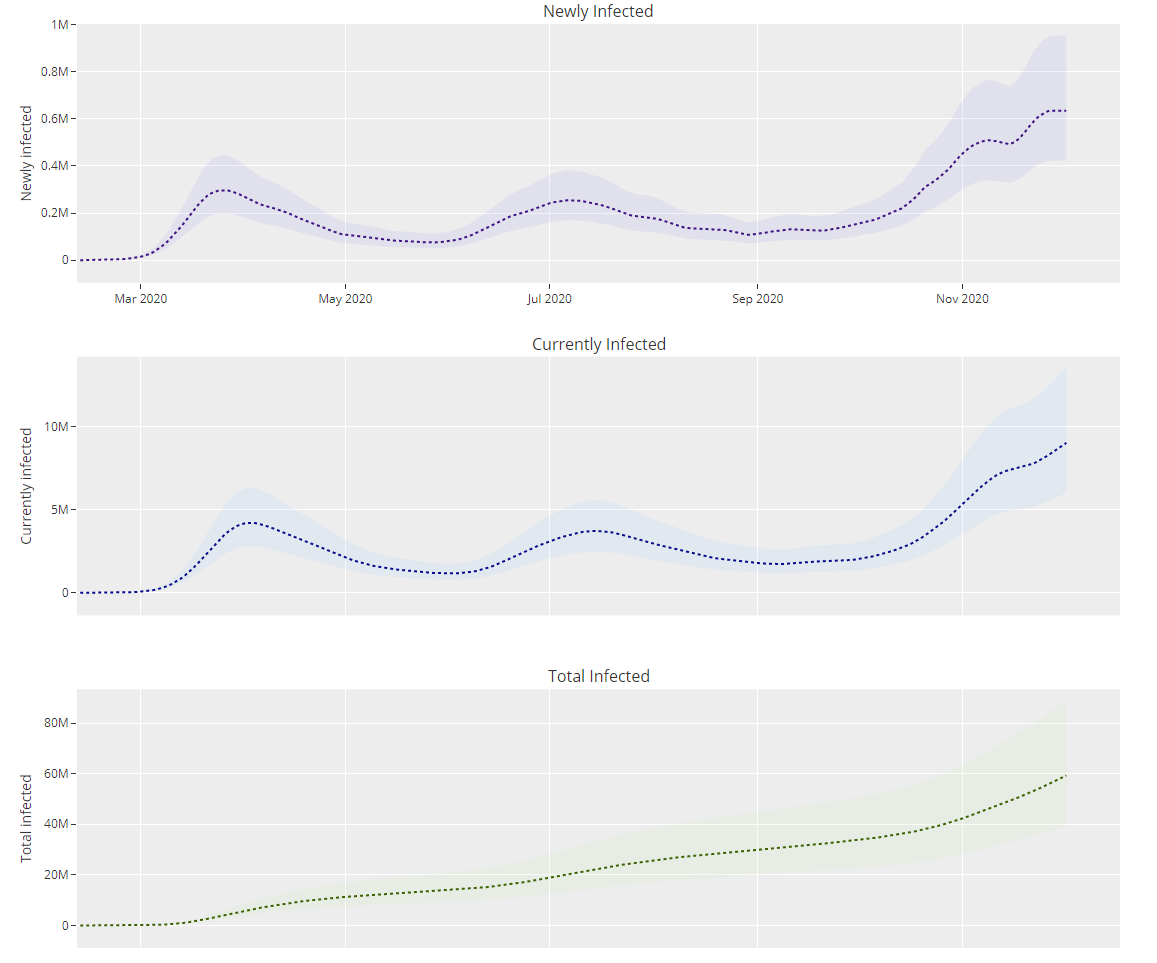
Predicted total infected 17.9% on December 2, 634k new infections per day.
Remember, those numbers are several weeks behind, and in general I consider them to be soft lower bounds.
Europe
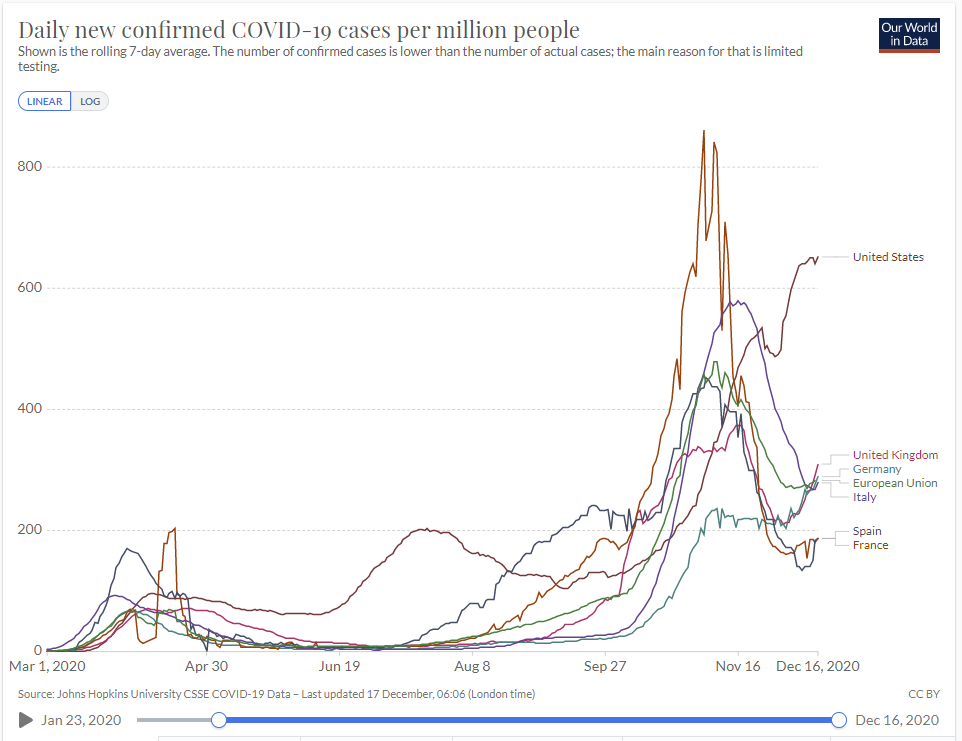
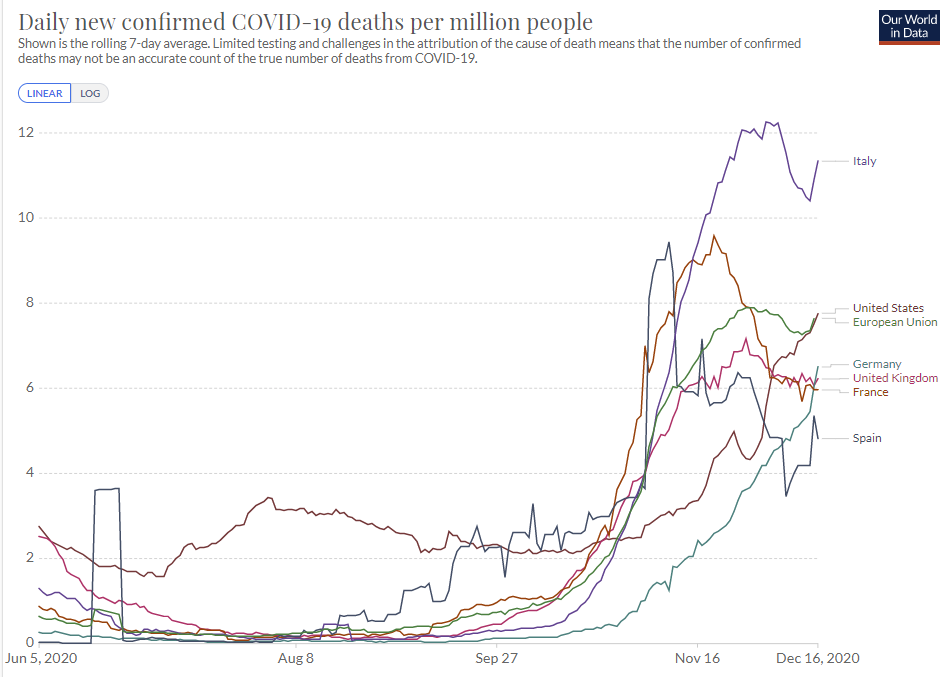
America now has twice as many infections as any of the European nations tracked here. Germany and the United Kingdom once again seeing more infections. Italy rapidly improved on that front but is still seeing a lot of deaths due to lag. The European strategies seem to continue to oscillate between being harsh to get things under control, and at other times letting things get worse. This does not seem obviously worse or better than the de facto American strategy of doing nothing.
All I Want For Christmas is a Covid Vaccine
It seems all it took to get the FDA to approve the vaccine on Friday, only one day’s worth of deaths after their panel had taken its sweet time to meet and give its seal of approval, was for Mike Meadows to tell the head of the FDA to resign if they didn’t give approval by the end of the day. It seems things were being held up because they had not prepared a proper “fact sheet” for the vaccine, which prompted Alex Tabarrok to calmly suggest maybe getting that done in advance next time.
The FDA denies that the pressure impacted their timetable:

He has to say that, because of the mindset ‘this was either due to science or due to pressure’ rather than the pressure being used to get around stupid red tape after the scientific job was already done (including lots of other stupid red tape), and also to save face. I am very confident he is lying here.
Calling for the head of the FDA if he doesn’t find a way to assemble a fact sheet by end of business is exactly the type of thing one does when giving such questions the urgency they deserve. We still didn’t vaccinate people until Monday, but things could have slipped even further. It’s also worth noting that the vaccine didn’t begin shipping until after every prior step was completed, which caused an additional unnecessary delay.
Early vaccinations seem to be running into some snags. Here’s a report from Florida. Hospitals are getting lots of doses, yet only using a few percent of them each day. That does not seem like the right sense of urgency. It also says that due to production concerns future shipments are on hold, which is a lot scarier. I haven’t seen other indications of things being on hold, but that would be very bad news.
Other shipments seem to have issues with being… too cold? Not sure exactly what goes wrong when that happens.
Credit where credit is due: Looks like Moderna is being allowed to submit with 7-week instead of 8-week safety data, and without full verifications (source):
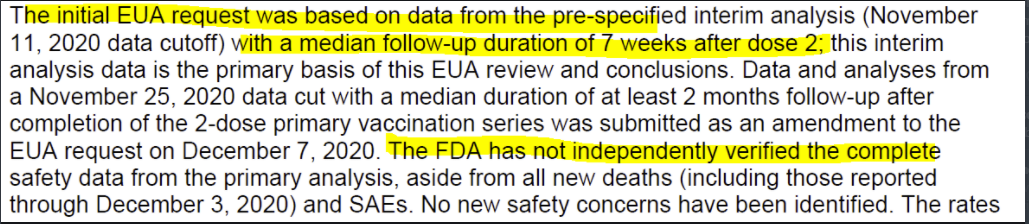
Once again, it’s all minor in the grand scheme, provided this did not slow down production or vaccination.
What matters is the long term path. That seems to still mostly be on track for early spring. We just bought another 100 million doses of the Moderna vaccine. By waiting, we gave ourselves the chance to save a tiny bit of money, and in exchange we slowed getting back to normal by a month. Not maxing out vaccine purchases was a supremely costly decision in terms of expected lives lost and lives ruined. I originally wrote it was a “mistake,” but on reflection that implies things about decision makers that I don’t endorse. Not a mistake.
Well, you should know this already, but FDA Delenda Est:
The full FDA report on the Moderna vaccine is here.
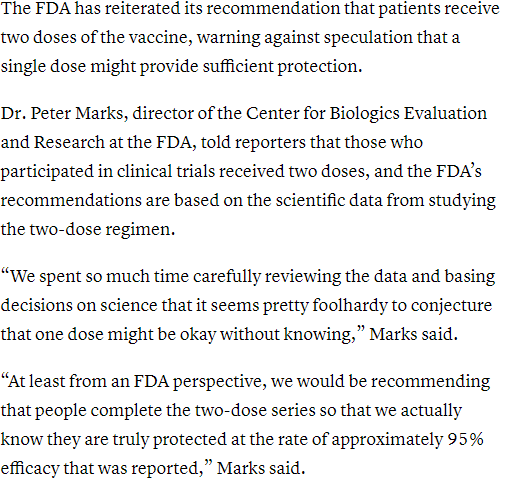
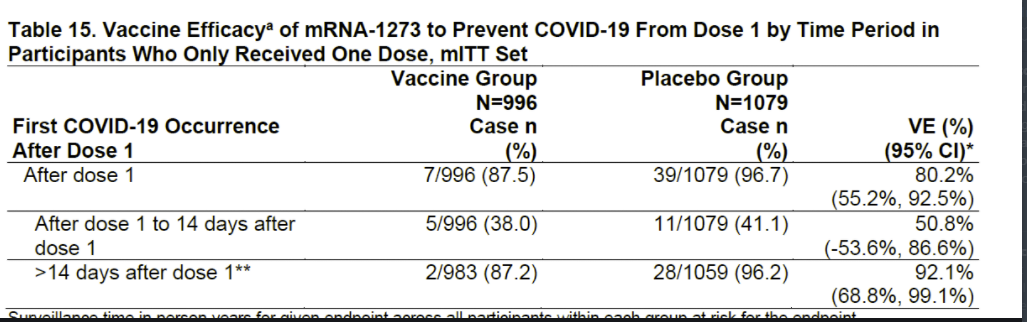
Also, um, have you seen the one-dose efficacy data because, I mean, holy shit:
Guess who said the Pfizer vaccine was safe and effective after one dose? Yep. The FDA.
In what world is giving the second dose to the same person, raising them from 87% to 96% protected, a higher priority than vaccinating a second person?
Guess who is the Only One Man brave enough to step up for this obviously correct strategy? Who is the most ridiculed of them all? It is, of course, the quintessential Florida Man, Governor DeSantis. Remember when DeSantis was history’s greatest villain for not closing beaches while Andrew Cuomo was a hero despite literally forcing nursing homes to take in people who were Covid-positive? Huh.
I do want to note the counterargument to this, which is that if an individual is 86% protected they have to decide whether to resume normal life while waiting for their second shot, whereas at 95% anyone not at high risk can safely take a lot more risk. At a societal level, of course, this if anything backfires further, but at the individual level there are definitely gains to concentrating your immunity.
You know what would be another way to get more people vaccinated? Use our entire supply of the vaccines! As in, the bottles provided are so overfilled that pharmacists can extract one or sometimes even two extra doses out of each five-dose vial. That is quite a bit of extra vaccine going to waste by default! Which is fine for a vaccine or other medicine with abundant supply, where avoiding contamination and ensuring a buffer against spillage or other surprises is important, but is totally not fine here. Luckily for us, the FDA has decided to declare using these extra doses “acceptable,” although as of the article’s publication that guidance was not yet official, opening the door for the extra doses to be used.
There’s still this, though:
Both Pfizer and FDA said that leftover vaccine from multiple vials should not be mixed, because of the contamination risk.
To which I would like to reply, that’s an interesting answer, can you please show your work?
It seems to imply strongly that the risk of contamination for any given injection is sufficiently high that multiplying that risk by two or three makes it net negative to administer the vaccine. That would mean it is eating up a large fraction of the gains from vaccination, as opposed to us essentially never hearing about contamination issues.
If we presume that a vial right now has a random amount of leftover vaccine, then by default the average vial should have about half a dose remaining after administering all full doses. That means that if we average six doses otherwise, we can expand supply by another 8% or so by combining those doses, or 6% or so if we are willing to combine up to two vials but not three. We are throwing that away because it would increase “risk of contamination” and again I very much want to see their work.
I love this gem:

I will gladly accept this particular demand for subgroup analysis if it keeps us from utterly wasting vaccinations on people who already have the immune response the vaccine is designed to create. Even if the vaccine was 100% effective in this group with zero side effects, that’s obviously hugely wasteful. Yet it looks like hospitals are mandating that such people get vaccinated anyway.
How fast could we have gone? Remember how we learned last week how the Moderna vaccine was designed in two days? I was surprised by that because my father said he could have done it in one, and it looks like Pfizer agrees with his timetable.
COVID-19 Vaccine Allocation Dashboard by Benjamin Renton tells us where America’s vaccine doses are headed. The first shipment seems to be allocated by population, as expected, but later in December the numbers quickly diverge, and it’s not obvious what is driving this. There isn’t an obvious political economy story here, and one could plausibly credit a lot of the differences to shipments not having been catalogued yet. It seems like consistently 6-7% or so of the population is getting vaccinated in the places that are getting the most, and there are a lot of ‘null’ entries here, so the hope is that this represents roughly a 6.5% of population vaccination distributed smoothly by the end of December. That would match previously announced quantities. If we did get that, then combining it with growing immunity from other sources, the tide should turn rapidly in January, unless sufficient additional control systems set in to un-turn it.
In other vaccine news around the world, The Oxford/AstraZeneca Vaccine Efficacy Data is in. The whole process seems to have been quite the royal mess, making it hard to be at all confident in the efficacy numbers. The standard Very Serious Person response is to re-run the trials, including checking to see if the mistaken half-dose given in the UK was a random stroke of genius. There does seem to be a plausible theory of how that might be true. My guess is that efficacy is something like 75%, in between the two trial results, and the half-dose makes only a small difference either way, but given we have limited vaccine supply I’d definitely go with the initial half dose for now.
The big (alas mostly rhetorical) question remains, why haven’t we approved this vaccine? The safety data seems very solid and I still can’t believe people continue to fret about a single person out of tens of thousands getting sick with something, anything despite not even having a mechanistic story of how the vaccine could be related, let alone it happening often enough for us to want to care. Our confidence interval for effectiveness should presumably be something like at least 50% effective and at most 90% effective, and if it’s 50% effective then we should get on this yesterday, obviously. Which we of course will not do.
Similarly, I was reminded this week that many arab countries have approved the Chinese vaccine, and was asked why this is so. I replied this was so because it probably works. There is no mystery to explain.
Perhaps we should consider trading vaccines with the Russians? Their consumer watchdog is asking those who get vaccinated to refrain from alcohol for two months, as Russians, in Russia, during the winter. I totally get how this can help build up immunity but come on. This is what one calls ‘not going to happen in a million years.’ Bring them vodka or bring them death, and if it’s both or neither for arbitrary values of vodka and relatively low levels of death, I’m pretty sure we already know their revealed preference.
My guess, of course, is that the watchdog is trying to use this as an excuse to get Russians to drink less, with the breakdown between ‘Russians drink way way too much and it’s worse for them than Covid-19 so getting them to cut down by any means is important’ and ‘Very Serious Person gets to take away only joy in people’s lives and is not about to miss that opportunity’ left as an exercise to the reader. Some actions are overdetermined.
I, on the other hand, have not had a drink of alcohol in years. May I suggest free trade?
They’re also experimenting with combining the Sputnik vaccine with the one from AstraZeneca. Given the issues with the first dose building up immunity to the vector needed for the second dose, it makes sense that mixing and matching could be good. I’m glad they are trying this. However, this also points out the obvious, which is that combining vaccines is on priors more effective than only doing one, and if that’s true and the safety data is in, why are we not taking all of the vaccines?
Sanofi vaccine given in insufficient doses in Phase I/II trials, and only generated what confidently looks like sufficient response in 18-49 year olds. Here’s a less detailed news report that also mentions delays in another vaccine. So they’re going to redo the studies, and while doing so they will not be doing a Phase III on 18-49 year olds, even though there are plenty of other vaccines that can serve the older cohort while we give Sanofi’s vaccine to the young. On top of that, they tested a lower dose and it seemed to work in the young, so that lets us get more people vaccinated faster! Perhaps we should be going a step further, and considering that maybe younger people need smaller doses of other vaccines as well. That would be another way to get this done faster. Not that anyone will ever give any of that the slightest consideration.
I do genuinely feel for regulators sometimes. Even when they want to do the right thing, they face horrible incentives, blamed only for individual bad things that result from the things they do, without getting credit for anything good or being blamed in any meaningful way for holding things up. Consider this throwing under the bus of India’s regulatory authority. It spends most of its time blaming them for approving things improperly, or letting trials happen that had individual adverse events. You see, these things ‘undermine confidence.’ It does not mention, at all, failure to run challenge trials or use other methods, including simply ‘run more and bigger trials sooner’ to get results faster, or its failure to actually do the job of ensuring the manufacturing of its full capacity of 3 billion doses per year of vaccine.
Everything Matters Versus Nothing Matters
A paper, phylogenetic analysis of SARS-CoV-2 in Boston highlights the impact of superspreading events, studies several such events. In particular, it seems that one conference held in Boston was responsible for a large percentage of all Covid-19 cases in the area for months afterwards, and subsequently for almost 2% of nationwide cases if you count all cases that derive from a virus variation that originated at the conference. That sounds like a really terrible conference.
The catch is that, like everything else in this pandemic, all those cases are intertwined with the control system. The counterfactual where the conference was cancelled does not contain 2% fewer Covid-19 infections or 2% fewer deaths. As people notice the extra infections, they adjust their behaviors, and governments adjust their rules. If you assume only fully naive SIR-model-style immunity effects from only detected cases, by now immunity has reduced new infections by 58%. If you started off 2% higher, those effects start off 2% stronger, and a majority of the increase cancels out. Then adjust that for the infections we miss, and the selection effects of who gets infected, and combine with the other aspects of the control system.
These are the two pandemic perspectives. On the one hand, every new infection permanently increases the infection rate, which then moves exponentially, so the conference is responsible for 2% of infections. On the other hand, control systems, so it’s not clear that the conference had a meaningful overall long term impact at all. In the extreme, if the control system was always destined to break down in November as the weather got colder, making things worse earlier can potentially build up immunity earlier, which prevents hospital overload and gives us a smaller peak number of infections, which minimizes overshooting after the corner gets turned and gets people overall better treatment. So being careless is either deeply irresponsible, actively saving lives, or something in between. Life is confusing like that.
Further Research Is Needed
Fast Grants and Marginal Revolution provide suggestive early results that fluvoxamine, and perhaps SSRIs and sigma-1 receptors more broadly, could provide an effective treatment for Covid-19. Given robust safety records, these do look promising, with the downside that fluvoxamine is reported to be difficult to quit. This is the kind of thing we would have known in April if we had our act together. Instead, even if these treatments work, we won’t be confident enough to use these treatments widely until most deaths have already happened. The sample and effect sizes here are quite small, so it could easily go either way.
You Should Know This Already (Inessential Reminders)
Yes, Moderna’s vaccine prevents transmission. One dose is good for reducing infection by 63%, two by over 90%.
CDC Delenda Est:

Our government is still hard at work slowing down the vaccination process:
As a reminder, if you only give someone one dose, nothing bad happens, and you can give out the second dose later with full benefits therefrom. This large of a reserve only has one purpose.
Reddit is asked: why is there an explicit line between Phase 3 and roll out of a vaccine? The responses point to bureaucratic, regulatory and “ethical” justifications aplenty, most of which readers will already be familiar with. Under normal circumstances they would even make sense.
More confirmation of what is important to “bioethics.”
Here’s another confirmation that what scares such people most is that things of value might be allocated to those who value them most, as measured by their willingness to pay, or who might go on to produce the most value. You see, it’s a scandal and tragedy when we prioritize treating the President of the United States over more ‘ethically deserving’ others, and we have to watch out before we allocate resources where they might be useful. If we’re not careful, next thing you know we’ll have an entire economy full of producing useful things and allocating them where they are valued most and can produce the most value. That would be the worst.
Household gatherings are driving a lot of the spread, but contact tracing works if and only if there are contacts one can easily trace, and assumes that the contact was the source. It’s still worth doing, and still provides useful information. But one must be careful with interpretation:
T
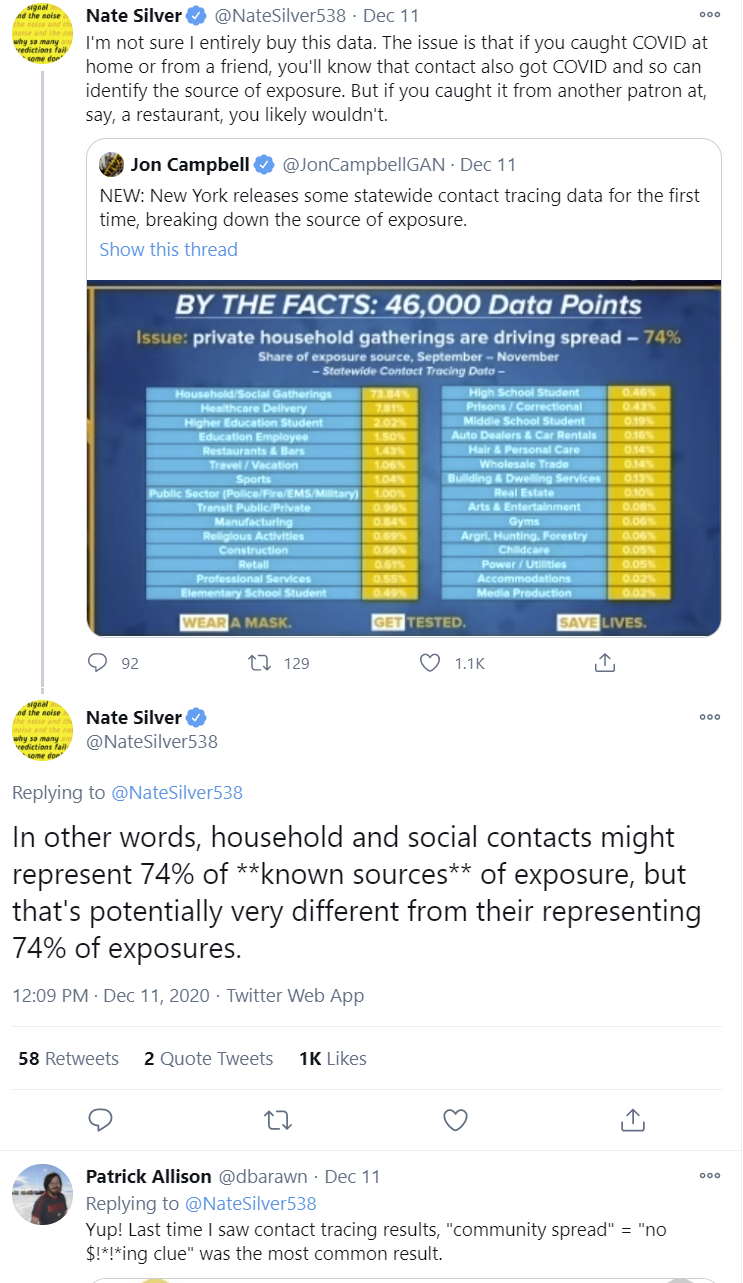
Thus, Nate and Patrick make strong points here, but it is even worse than the initial impression. Even if one has a contact that tests positive, and the timeline works out that they could have infected you, that doesn’t mean that was the source of your infection. Thus, it’s not that 74% of known sources come from households and social gatherings, and then some cases have no known source. It’s that of the cases where there is a known source, 74% of those involve households and social gatherings, but we don’t know how often that is actually the source.
I do think it’s right that social gatherings and exposure within households are the largest source of cases, and likely the majority of them, but the data we have is not sufficient to reach such conclusions.
Here is an analysis of why the west failed so utterly at contact tracing and other places succeeded. This all seems simple. Most nations did not attempt (the word ‘try’ is so overloaded I’m going to mostly taboo it) contact tracing. At maximum, they attempted to take symbolic action that they could cite as an attempt to do contact tracing. Between privacy concerns, distrust of government, and a complete unwillingness to ever compel anyone to go anywhere, do anything or reveal any information unless they’ve been arrested for a crime, or to spend money on things like getting people places to safely and comfortably quarantine even when they wanted to do so, and fearing (I think correctly) that if they did any of that people would not get tested and otherwise go crazy, they settled for symbolic action. There was not even an attempt to scale up to numbers of tracers that might plausibly have been adequate. Then case numbers quickly got out of hand, and one thing the places that succeeded via contact tracing had in common is they did so early, before things got out of hand.
So we did nothing, while Vietnam did this (source that includes more):
There’s also this inessential lighter side twitter video link about the joys of contact tracing. I was amused.
Non-essentially, more restating “ethical” and otherwise nonsensical reasons why we should not do the things we obviously should do, via MR. Not doing these things has caused and will cause many, many people to die, and many lives to be destroyed, and all of us to be dramatically worse off.
Should kids get snow days off during remote learning? New York City mayor DeBlasio, owner of a true zero percent approval rating, has picked the side you would expect, saying ‘snow days are over.’ He’s also saying New York should prepare for a ‘total shutdown’ after Christmas.’ Joy is the enemy and must everywhere be destroyed.
Should those instructed at home get snow days? Depends on what snow days are, and what schools are. Rather than restate my views I’ll let everyone ponder on their own.
Or, if you don’t know the following particular thing already, then we need to fix that, because the WHO says so:
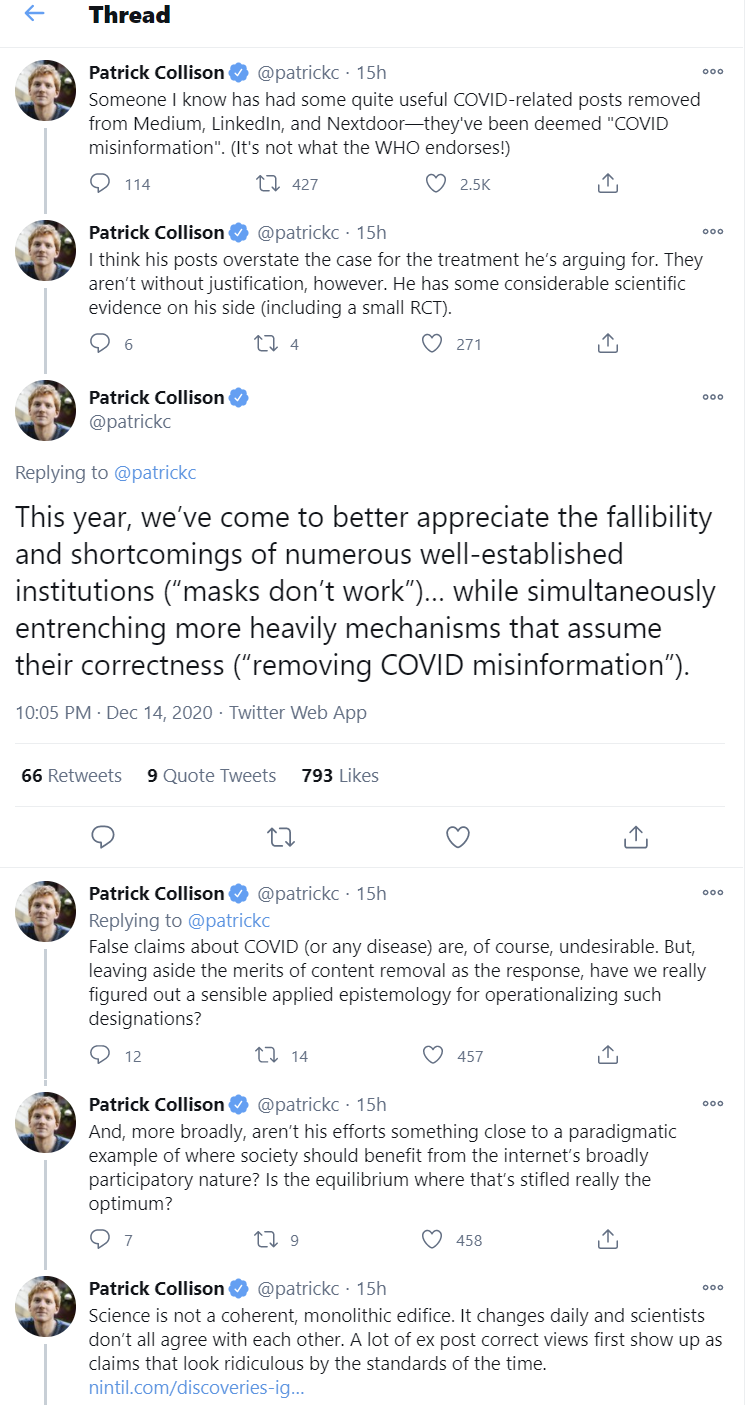
Many platforms have a principle that if you disagree with the WHO or CDC (also known as ‘the lying liars who said masks don’t work and have similarly only admitted fact after fact months after they had become clear’) that your posts and videos will be taken down. WordPress does not have such a principle, so I should be safe here, but if I did not have LessWrong as an automatic backup (and my drafts saved in Google as a second backup) I would be sure to stash additional copies. If I was posting this content to places like YouTube, Facebook or Medium, my expectation is that at least some posts would have been taken down.
Even the Internet Archive does not seem reliable, as they have announced plans to begin putting warnings on past content rather than offer up the web purely as it was. That pretty much signals that at some point, perhaps reasonably soon, they will start taking down records of things that powerful people sufficiently dislike.
Like most modern rules, this rule is not reliably and fairly enforced. If it was, it would be obvious that the rule was absurd and unacceptable. Instead, the rule is that when people are inclined to take something down, it is considered a valid excuse to cite disagreement with official sources, despite the known unreliability of those official sources.
If you tell people they aren’t allowed to go to the office, they’ll find offices where they may, such as in the quiet cars of the Long Island Railroad.
When you don’t let people get treatment until they prove they are sick enough for it, at which point the treatment is being given too late, you end up not using it:
In Other News

Russian Doll is in fact excellent. Thought experiment: If this happened to you, other than making a killing in various markets, what would you do? Would you be able to stop the pandemic?
Non-Covid: FDA also approves genetically modifying pigs. They don’t fly.
FDA panel member explains her vote against approval of Pfizer vaccine, potentially ‘undermining confidence,’ because the panel recommended it be given to 16-17 year olds in addition to those over 18, without having enough specific evidence for that, and the panel member fully supporting vaccinations in those over 18, and the obvious fact that no one under 18 is going to get a vaccination for a long time either way.
FAA generously decides to not attempt to murder its pilots at this time:

In welcome news, Pelosi denounces all her policy positions:
Carbone, which pre-pandemic was the only restaurant in New York that I both wanted to dine in and couldn’t get a table at when I wanted one, is taking outdoor dining to the next level. That next level appears to be ‘indoor dining,’ which they are claiming does not technically count so long as the ground it is built upon is legally a sidewalk.

Germany confirms they are engaging in triage (in German).
If you don’t need to be quarantined, you can have your own line at the airport.
Skin in the game:

San Mateo County in the San Francisco area declines to Sacrifice to the Gods and shut everything down in ways known to not be effective, explains its reasoning in detail.
Not that anyone should expect people to obey the new California lockdowns, which is one reason why they definitely won’t work (source):
In a cool little piece rounding up views on techno-optimism, we get this perspective:
It is obviously correct that given the restrictions placed upon us, the disruptions we suffered in 2020 would be a drop in the bucket compared to attempting similar restrictions in the year 2000 for a similar length of time. Mobile and internet technology has proven its value many times over.
But that doesn’t mean we would have had worse outcomes! It seems highly plausible we would have had much better outcomes on at least some fronts.
On the economic front, we would have had to choose either to actually suppress the virus, in which case we get much better outcomes all around, or to accept that the virus couldn’t be stopped, which also produces better economic outcomes.
Our technological advancement gave us the choice to make massively larger Sacrifices to the Gods rather than deal with the situation. And as we all know, choices are bad. We also are, in my model, much more inclined to make such sacrifices now than we were in the past, even when the trade-offs are similar, which ties into my view that simulacra and maze levels are higher, with a larger role played by fear of motive ambiguity. We might have been willing to do challenge trials or other actual experiments, and have had a much better handle on things quicker on many levels.
Here’s a quote from Tyler Cowen yesterday that illustrates the issue quite well, while also showing how much else we have lost:
Here is my earlier Bloomberg column rejecting the notion of forced quarantine of individuals for Covid-19, mostly on rights grounds, though I add some consequentialist arguments. I would not trade in the American performance for the Chinese anti-Covid performance if it meant we had to weld people inside their apartments without due process, for instance, as the Chinese (and Vietnamese and others) did regularly.
Seriously, what the hell, hero? You wouldn’t make that trade, in hindsight, knowing that their method would work and our method would be this awful?
I think not making this trade, under these conditions of assured outcomes for both choices, and given only these choices, is utterly completely insane.
The civilization that chooses thus, does not survive long.
It is an open question whether being forced to give up on containment entirely, and accepting a lot of deaths, would have been a better outcome than over a year of Covid lockdowns of varying severity that we got instead. One could make a reasonable case for both sides even in hindsight.
But to outright say, no, we’d rather fail than use the means that work because we might do things without “due process”? Did you see anyone using “due process” this whole time for anything other than regulatory interference with those trying to solve the problem? I didn’t. I saw a bunch of fiat restrictions of freedom with no legislative backing that were much bigger and didn’t work, instead of restrictions that in total were much smaller and did work, together with lots of restrictions on doing anything useful.
One thing we definitely wouldn’t have had in the year 2000 would be mRNA vaccines.
It is good to be reminded that the vaccine effort was extraordinarily fast, innovative, safe and effective. That doesn’t cancel out the fact that it could have been much faster and much more effective if the people saying it couldn’t be done had interfered less with the people doing it. And while that interference was a huge problem, the interference with other things like testing (or masks, or things as simple as ordinary life) was far worse.
Both are important. And there is a very optimistic take that combines both. If we did all of this despite the best efforts of many of the most powerful people and organizations and dynamics, then imagine what we could do if we took those gloves off!
I am not expecting this outcome, but we should keep shouting it from the rooftops, as soon as we are done shouting for one-dose vaccinations. If we can use the pandemic as an impetus to move from telling people it cannot be done and they are not allowed to do it, for most worthwhile new values of it, to providing subsidies or even giving people the freedom to act at all, across a variety of other domains, than perhaps the whole of 2020 will have been worthwhile after all.
29 comments
Comments sorted by top scores.
comment by Sammy Martin (SDM) · 2020-12-18T19:19:39.528Z · LW(p) · GW(p)
On the economic front, we would have had to choose either to actually suppress the virus, in which case we get much better outcomes all around, or to accept that the virus couldn’t be stopped, *which also produces better economic outcomes. *
Our technological advancement gave us the choice to make massively larger Sacrifices to the Gods rather than deal with the situation. And as we all know, choices are bad. We also are, in my model, much more inclined to make such sacrifices now than we were in the past,
So, by 'Sacrifices to the Gods' I assume you're referring to the entirety of our suppression spending - because it's not all been wasted money, even if a large part of it has. In other places you use that phrase to refer specifically to ineffective preventative measures.
'We also are, in my model, much more inclined to make such sacrifices now than we were in the past '- this is a very important point that I'm glad you recognise - there has been a shift in values such that we (as individuals, as well as governments) are guaranteed to take the option of attempting to avoid getting the virus and sacrificing the economy to a greater degree than in 1919, or 1350, because our society values human life and safety differently.
And realistically, if we'd approached this with pre-2020 values and pre-2020 technology, we'd have 'chosen' to let the disease spread and suffered a great deal of death and destruction - but that option is no longer open to us. For better, as I think, or for worse, as you think.
You can do the abstract a cost-benefit calculation about whether the other harms of the disease have caused more damage than the disease, but it won't tell you anything about whether the act of getting governments to stop lockdowns and suppression measures will be better or worse than having them to try. Robin Hanson directly confuses these two in his argument that we are over-preventing covid.
We see variations in both kinds of policy across space and time, due both to private and government choices, all of which seem modestly influenceable by intellectuals like Caplan, Cowen, and I...
But we should also consider the very real possibility that the political and policy worlds aren’t very capable of listening to our advice about which particular policies are more effective than others. They may well mostly just hear us say “more” or “less”, such as seems to happen in medical and education spending debates.
Here Hanson is equivocating between (correctly) identifying the entire cost of COVID-19 prevention as due to 'both private and government choices' and then focussing on just 'the political and policy worlds' in response to whether we should argue for less prevention. The claim (which may or may not be true) that 'we overall are over-preventing covid relative to the abstract alternative where we don't' gets equated to 'therefore telling people to overall reduce spending on covid prevention will be beneficial on cost-benefit terms'.
Telling governments to spend less money is much more likely to work than ordering people to have different values. So making governments spend less on covid prevention diminishes their more effective preventative actions while doing very little about the source of most of the covid prevention spending (individual action).
Like-for-like comparisons where values are similar but policy is different (like Sweden and its neighbours), make it clear that given the underlying values we have, which lead to the behaviours that we have observed this year, the imperative 'prevent covid less' leads to outcomes that are across the board worse.
Or consider Sweden, which had a relatively non-panicky Covid messaging, no matter what you think of their substantive policies. Sweden didn’t do any better on the gdp front, and the country had pretty typical adverse mobility reactions. (NB: These are the data that you don’t see the “overreaction” critics engage with — at all. And there is more where this came from.)
How about Brazil? While they did some local lockdowns, they have a denialist president, a weak overall response, and a population used to a high degree of risk. The country still saw a gdp plunge and lots of collateral damage. You might ponder this graph, causality is tricky and the “at what margin” question is trickier yet, but it certainly does not support what Bryan is claiming about the relevant trade-offs.
So, with the firm understanding that given the values we have, and the behaviour patterns we will inevitably adopt, telling people to prevent the pandemic less is worse economically and worse in terms of deaths, we can then ask the further, more abstract question that you ask - what if our values were different? That is, what if the option was available to us because we were actually capable of letting the virus rip.
I wanted to put that disclaimer in because discussing whether we have developed the right societal values is irrelevant for policy decisions going forward - but still important for other reasons. I'd be quite concerned if our value drift over the last century or so was revealed as overall maladapted, but it's important to talk about the fact that this is the question that's at stake when we ask if society is over-preventing covid. I am not asking whether lockdowns or suppression are worth it now - they are.
You seem to think that our values should be different; that it's at least plausible that signalling is leading us astray and causing us to overvalue the direct damage of covid, like lives lost, in place of concern for overall damage. Unlike Robin Hanson, though, you aren't recommending we attempt to tell people to go off and have different values - you're simply noting that you think our tendency to make larger sacrifices is a mistake.
...even when the trade-offs are similar, which ties into my view that simulacra and maze levels are higher, with a larger role played by fear of motive ambiguity. We might have been willing to do challenge trials or other actual experiments, and have had a much better handle on things quicker on many levels.
There are two issues here - one is that it's not at all clear whether the initial cost-benefit calculation about over-prevention is even correct. You don't claim to know if we are over-preventing in this abstract sense (compared to us having different values and individually not avoiding catching the disease), and the evidence that we are over-preventing comes from a twitter poll of Bryan Caplan's extremely libertarian-inclined followers who he told to try as hard as possible to be objective in assessing pandemic costs because he asked them what 'the average American' would value (Come on!!). Tyler Cowen briefly alludes to how woolly the numbers are here, 'I don’t agree with Bryan’s numbers, but the more important point is one of logic'.
The second issue is whether our change in values is an aberration caused by runaway signalling or reflects a legitimate, correct valuation of human life. Now, the fact that a lot of our prevention spending has been wasteful counts in favour of the signalling explanation, but on the other hand there's a ton of evidence that we in the past, in general, valued life too little. [There's also the point that this seems like exactly a case where a signalling explanation is hard to falsify, an issue I talked about here,
I worry that there is a tendency to adopt self-justifying signalling explanations, where an internally complicated signalling explanation that's hard to distinguish from a simpler 'lying' explanation, gets accepted, not because it's a better explanation overall but just because it has a ready answer to any objections. [LW(p) · GW(p)] If 'Social cognition has been the main focus of Rationality' [LW · GW] is true, then we need to be careful to avoid overusing such explanations. Stefan Schubert explains how this can end up happening:
I think the correct story is that the value shift has been good and bad - valuing human life more strongly has been good, but along with that its become more valuable to credibly fake valuing human life, which has been bad.
Replies from: Zvi, habryka4↑ comment by Zvi · 2020-12-18T22:09:45.723Z · LW(p) · GW(p)
Agree with habryka that I don't agree with all of this but it's well stated. I don't think it much disagrees with the claims in OP, even the implied claims, rather it's making a different argument.
I think the opening of the comment interprets my claim about how much of our current response is unproductive in a way that I didn't intend and don't endorse. I agree that some of our spending has been worthwhile on the margin, if the only alternative was to do nothing beyond preventing action. And I agree that if government is determined to prevent useful private action (e.g. "We have 2020 values"), it does not then have the means to prevent local private costly preventative action, so doing basically no prevention isn't a real option.
Which is that under 2020 values and 2020 technology, and with the only choice being 'prevent more' or 'prevent less' that preventing less backfired on all fronts when nations tried it, because preventing less meant more private prevention that proved more expensive e.g. Sweden and Brazil. Because that's the only thing we are capable of executing - the government can shut down useful private responses and not do anything itself, but in terms of realistic choices we can talk about, it can neither do better useful things or allow others to do them, only do more of standard-issue-prevention or less.
I do think that if you compare different US state responses, you get a different answer than comparing Sweden to Norway (which I understand why people think is fair but is a very high bar to clear). I don't know to what you compare Brazil, a country that has had shrinking GDP and a death spiral economy for many years now. Is this economic response bad? E.g. EWJ is +10% YoY, which underperforms Argentina but outperforms Mexico. Argentina was previously growing, and shrunk more in Q2 than Brazil, etc etc.
Anyway, that's all for me here, calling the comments to a close for the week for Shabbat.
↑ comment by habryka (habryka4) · 2020-12-18T20:58:22.826Z · LW(p) · GW(p)
While I disagree with substantial portions of this, I found it really clear and valuable, and strong-upvoted it. Thank you for writing down your arguments in such a clear way!
comment by Shmi (shminux) · 2020-12-18T01:55:24.885Z · LW(p) · GW(p)
Building on "choices are bad": the Covid-19 mortality rate is at the Goldilocks zone for allowing (bad) choices:
- If the mortality rate was 20+%, the choices of herd immunity, doing slow full-scale trials or doing nothing would not be on the table. It would be "let's try everything, anything, now, now, now!" and the vaccines made in February would have been produced and used before summer.
- If the mortality rate was within an order of magnitude of the annual flu (0.1% or so), "do nothing" would have been the only choice
As it is, 0.5%-3% mortality rate is exactly the wrong number, since the right decision is not immediately obvious to everyone. And so we have the largest number of overall deaths and the largest damage to the economy possible from anything short of Oryx & Crake-style plague.
Replies from: jaspax↑ comment by jaspax · 2020-12-18T10:24:47.765Z · LW(p) · GW(p)
I had the exact same thought. COVID inhabits a liminal zone in which it's simultaneously true that vigorous action could save hundreds of thousands of lives, but many people would individually look at the infection and fatality rates and determine that it wasn't worth it to cancel their entire lives. Given existing political cleavages, it was also entirely predictable that this would wind up splitting down partisan lines.
comment by TAG · 2020-12-19T18:20:08.581Z · LW(p) · GW(p)
Here’s another confirmation that what scares such people most is that things of value might be allocated to those who value them most, as measured by their willingness to pay
Thus is bad logic. Willingness to pay only translates to value if everyone has a ton of money. Since that is not the case, it is possible to value something without being able to afford it.
comment by gjm · 2020-12-17T14:39:50.368Z · LW(p) · GW(p)
You seem to have an off-by-two error in the title.
Replies from: Zvi↑ comment by Zvi · 2020-12-17T21:14:49.649Z · LW(p) · GW(p)
What's funny is that I looked at that and thought "Third Dose? Negative One Dose? Huh?" until someone in the OP outright pointed out I'd placed this in October.
Replies from: adamzerner↑ comment by Adam Zerner (adamzerner) · 2020-12-18T01:30:50.531Z · LW(p) · GW(p)
I made a similar mistake. I thought gjm was referring to "Third Dose".
comment by Timothy Johnson (timothy-johnson) · 2020-12-17T22:34:11.267Z · LW(p) · GW(p)
Several months ago, some people argued that trying to develop a vaccine for COVID-19 was pointless, because the "common cold" includes several types of coronaviruses, which have never had a successful vaccine.
Now that we have multiple successful vaccines for COVID-19, could we use the same methods to produce a vaccine for the common cold?
Five minutes of research suggests to me that it would be worth it to try. (Caveat: I picked the first numbers I found from Google, and I haven't double-checked these.)
- The common cold costs $40 billion per year in the US alone, after including the cost of lost productivity: Cost of the Common Cold: $40 Billion (webmd.com). (Article from 2003, but I don't imagine this has changed significantly.)
- The US government contributed $9 billion to developing COVID-19 vaccines: How Much Will It Cost to Get a COVID-19 Vaccine? (healthline.com). As I understand it, that includes both the costs of funding the research and, at least in some cases, pledging to buy hundreds of millions of doses.
- Coronaviruses cause around 15% of cases of the common cold: Common cold - Wikipedia.
Spending $9 billion to save $6 billion per year (15% of $40 billion, assuming all types of colds have roughly the same severity) sounds like a good deal to me. And chances are that the cost of development could be much lower in a non-emergency situation, since we don't need so much redundancy.
This article makes it sound like the main difference is that we've never tried mRNA vaccines before: Fact-checking Facebook post comparing COVID-19 vaccine research to HIV, cancer, common cold - HoustonChronicle.com. But now that we know it works, I don't see what's stopping us.
Replies from: romeostevensit↑ comment by romeostevensit · 2020-12-18T01:48:34.436Z · LW(p) · GW(p)
looks like we're getting an mrna vaccine for HSV out of all this, so there's that.
Replies from: crabman↑ comment by philip_b (crabman) · 2020-12-18T18:15:13.842Z · LW(p) · GW(p)
Can you elaborate? Where can I read about it?
Replies from: romeostevensitcomment by charlesoblack · 2020-12-18T19:02:49.039Z · LW(p) · GW(p)
In what world is giving the second dose to the same person, raising them from 87% to 96% protected, a higher priority than vaccinating a second person?
I'm not sure I agree with this point. There's no hard evidence that the second dose is not necessary: nobody was only vaccinated once in the trials (as far as I'm aware). Of course, we do have a prior for the immunity continuing, but we also have examples of other vaccines that require booster shots (HPV, meningitis, hep A/B); so I'd say that we should absolutely explore the one-dose option, but in the meantime, continue vaccinating people twice.
I don't think this would affect the overall outcome either, since - as you said - the overall distribution of the vaccine works exponentially. If we start a one-dose trial now, I'm sure we'd have results soon enough that it would still be massively useful to switch gears and start doing one-dose vaccinations.
Is there a further argument for believing one-dose is sufficient? I may have missed it.
comment by Adam Zerner (adamzerner) · 2020-12-17T19:32:25.219Z · LW(p) · GW(p)
I wonder how much risk compensation will happen for people who get vaccinated. If you start dining indoors instead of having MODified hangouts with friends, that's something like 300x the risk according to the microCOVID Project whereas the vaccine gives you something like a 10x reduction in risk.
Replies from: Ericf↑ comment by Ericf · 2020-12-17T19:49:31.300Z · LW(p) · GW(p)
It might be 300x the risk of transmission, given one infected person, but if everyone is vaccinated the chance of any attendee being infected is reduced for every interaction they had leading up to the hangout.
Replies from: adamzerner↑ comment by Adam Zerner (adamzerner) · 2020-12-17T20:08:22.142Z · LW(p) · GW(p)
Yeah, I don't mean to imply that I think vaccinations will be a net negative for society due to risk compensation. I think they'll be a net positive. People's lifestyles are already risky enough such that at a society level, there isn't room to 300x the risk.
comment by Joe Collman (Joe_Collman) · 2020-12-17T16:39:11.957Z · LW(p) · GW(p)
Thanks again for these.
Typo: "...net negative to administer the virus".
comment by Baisius · 2020-12-17T18:07:40.335Z · LW(p) · GW(p)
Am I the only one who doesn't understand the Moderna Efficacy Table you screencapped?
39/1079 is an infection rate of 3.61% (They have 96.7%, which I assume means virus free? But that doesn't match)
They say 7 out of 996 got infected who got one dose of the vaccine. That's an infection rate of 0.703%. 0.703% / 3.61% = 19.4%, which I would call an 80.6% "effective" vaccine. They show a percentage of 87.5%?
None of this really matters, I guess, because the overall point is the same. Obviously one dose is ~pretty effective for varying definitions of "pretty". But it's still not clear to me what kind of math they're doing.
Replies from: Joe_Collman, Joe_Collman, Daniel V↑ comment by Joe Collman (Joe_Collman) · 2020-12-17T21:47:00.112Z · LW(p) · GW(p)
It's also worth looking at the next table for Moderna one-dose severe-COVID-prevention efficacy:
Vaccine group: 2 / 996
Control group: 4 / 1079
Efficacy: 42.6% (-300.8, 94.8) [95% CI]
Huge error bars and little data, but certainly doesn't support a guess of ~80% efficacy at preventing severe cases. In the end it's the transmission that matters, but I suppose there's a danger based on public perception: if one dose turns out to have under 50% efficacy for severe cases it's not going to make anyone feel safe. If the sub 50% applies to deaths too, then you'll have many reports of "X took the vaccine, caught Covid and then died".
I assume Moderna wouldn't be crazy about this either. Not great PR if everyone broadly remembers that vaccines stopped Covid, but specifically remembers that Moderna's failed to save their friend's granny.
While there's short supply, it doesn't particularly matter if a load of people don't want to take it. Once there's a large supply, that changes - and if there's a largely baked-in misperception that the vaccine(s) suck(s), it's likely to be unhelpful.
In some sense it's analogous to the mask situation:
[Take action likely to reduce confidence in X] ---> [Free up supply of X to allow efficient targeting] ---> [Suffer consequences of longer-term low confidence in X]
Here the confidence-reducing action wouldn't be a lie, but that's not the only consideration.
↑ comment by Joe Collman (Joe_Collman) · 2020-12-17T19:40:11.199Z · LW(p) · GW(p)
My best guess on that table, looking at the full report (caveat: I am emphatically not an expert):
1) The VE calculations look correct: they're almost precisely what I get by division of my naïve incidence rate calculations. I assume the small discrepancy is due to the data's being discrete: if you have 7 cases out of 996, your best prediction of incidence rates won't be precisely 7/996.
2) From my guess the numbers in brackets in the first two columns aren't percentage rates at all. Rather they are "Surveillance time in person years for given endpoint across all participants within each group at risk for the endpoint". This description is at the bottom of the table, without any asterisk or similar. I assume that this is an error: there was supposed to be an asterisk for that from the bracketed number in the first two columns.
This seems plausible for the data: the pre-14-days numbers are under half of the post-14-days numbers, and the median follow-up time was 28 days.
But it's entirely possible that I'm wrong.
↑ comment by Daniel V · 2020-12-17T20:45:44.850Z · LW(p) · GW(p)
I'm having trouble with it too and I think Zvi misinterpreted it as well- the far right column is the VE.
Replies from: Joe_Collman↑ comment by Joe Collman (Joe_Collman) · 2020-12-17T20:54:49.406Z · LW(p) · GW(p)
Ah yes, I think you're right.
To me it seems that one dose efficacy is approx 80% from that table, and the two dose is still the old approx 95%. So it's more like an 80% to 95% upgrade than 87% to 97%.
Zvi's main point likely still stands, but the personal immunity question is less clear [ETA even on a population level it's somewhat less clear, once you consider the confidence intervals: given 55% to 92% CI, one-shot efficacy could turn out to be below 70%, in which case things depend a lot on the homogeneity of populations, the precision of your targeting, and post vaccination behaviour changes]
↑ comment by Zvi · 2020-12-17T21:14:14.319Z · LW(p) · GW(p)
I was responding to other people saying what the numbers were and didn't attempt to read the chart in detail - it was more 'oh grab the primary source and that looks about right' because as usual things move quickly.
But yes, the first dose being much more than half the total is all it takes to draw the same conclusion.
comment by jmh · 2020-12-19T03:04:44.368Z · LW(p) · GW(p)
Regarding the late to the party home tests, perhaps one very positive aspect is the test approval has presumably set a precedence for some future infectious madness that shows up for some future party.
Anyone know if the actually mechanism might be flexible enough to allow a quick response for test kits? I would think possibly so but have not yet looked into that question. However, suspecting someone here might I have I ask. (Guessing that it's some type of DNA/RNA "fingerprinting" type of test so once the fingerprint is known the device can be loaded with the needed chemistry.)
comment by wangscarpet · 2020-12-18T15:53:00.054Z · LW(p) · GW(p)
In what world is giving the second dose to the same person, raising them from 87% to 96% protected, a higher priority than vaccinating a second person?
One benefit of 96 vs 87 is that the former could allow you to live an un-quarantined life, while the latter wouldn't result in much behavioral change. Clearly, the one-dose is better for net deaths etc, but the QALY calculation looks a little different.
I still agree with you. But it's worth considering the above reasoning for completeness.
Replies from: Zvi↑ comment by Zvi · 2020-12-18T16:21:22.602Z · LW(p) · GW(p)
Agreed that this is the counter-argument, if you think that 87% wouldn't be enough to allow changes in behavior - which of course can also be an advantage, since now you really did reduce that person's risk by 87%, and the risk of them infecting others too.
Note that when I ask, for myself, whether 87% now (with 96% coming in 4-6 months) would be enough for me to un-quarantine, I get a strong yes. I would still not take 'stupid' risks but would mostly e.g. see friends freely.