Covid 12/10: Vaccine Approval Day in America
post by Zvi · 2020-12-10T14:20:02.012Z · LW · GW · 31 commentsContents
The Numbers Predictions Deaths Positive Tests Test Counts Positive Test Percentages Covid Machine Learning Projections Europe No, Not That Pandemic Vaccine, That Other Pandemic Vaccine All I Want For Christmas Are a Covid Vaccine and a PS5, But They Underpriced Them And Now They’re All Sold Out Scream If You Wanna Go Faster For Me But Not For Thee The Ramsey Tax Is Too Damn High All Masks Are Not Created Equal In Other Covid News Winter is Coming None 31 comments
Today, the FDA is meeting to discuss Pfizer’s Covid-19 vaccine. By the time many of you read this, they will have hopefully given the vaccine, and perhaps Moderna’s as well, emergency use authorization. If that happens, distributions to the states can begin, and some people will be vaccinated as early as tomorrow.
That is excellent news. Alas, supplies remain highly limited and the vaccine takes a month to work. States are getting smaller allocations of the vaccine than they expected. The situation for the holiday season remains unchanged, and most of us will likely not become immune until some time around May.
Two weeks ago, I noted data was about to get weird. A week ago I observed that the data was weird. What I didn’t note was that the Covid Tracking Project had written a post about exactly in what ways they expected it to be weird, which were different in places from the ways I expected. Lots of good observations in there. The post makes a convincing case that I was underestimating expected delays and bottlenecks.
Despite that, we saw a big jump in positive test percentage on Tuesday, December 2, exactly when I’d expected one. That could mostly be a coincidence. Perhaps that was more of a shift in timing of reporting, with the real surge from Thanksgiving coming later. I certainly buy the augment that such super-spreader events infect people in multiple waves, as those infected take the virus home, and we should expect an unusually high effective R0 in the week after Thanksgiving.
That will not give us much time to recover before Christmas and New Year’s Eve give their one-two punch. It seems unlikely we will turn the corner until after those get to play out. Despite previous holidays not showing up much in the data, these big three seem like a huge deal to me, especially now. People are sick of it all.
People are also sick, period. Death rates are up. Positive test rates are up. Cases are up.
This week’s post attempts to limit Twitter links. In cases where the link is serving as a source but is otherwise inessential, I’m going to link it explicitly and purely as a source, so there’s no need to click unless you want to verify it. Any other Twitter links didn’t have a good substitute I could find easily.
Let’s run the numbers.
The Numbers
Predictions
Last week’s prediction: My unconfident prediction is a 14.8% positive rate on 10 million tests, and an average of 2,200 deaths to account for at least some amount of catching up in reporting. But, again, wider than usual error bars all around.
Results: We got a 13.7% positive rate on 10.4 million tests, and an average of 2,276 deaths. So somewhat better positive rate than I expected, but not as good as one might hope.
Next week: My baseline prediction is a 14.3% positive rate on 11 million tests, and an average of 2,550 deaths per day.
Deaths
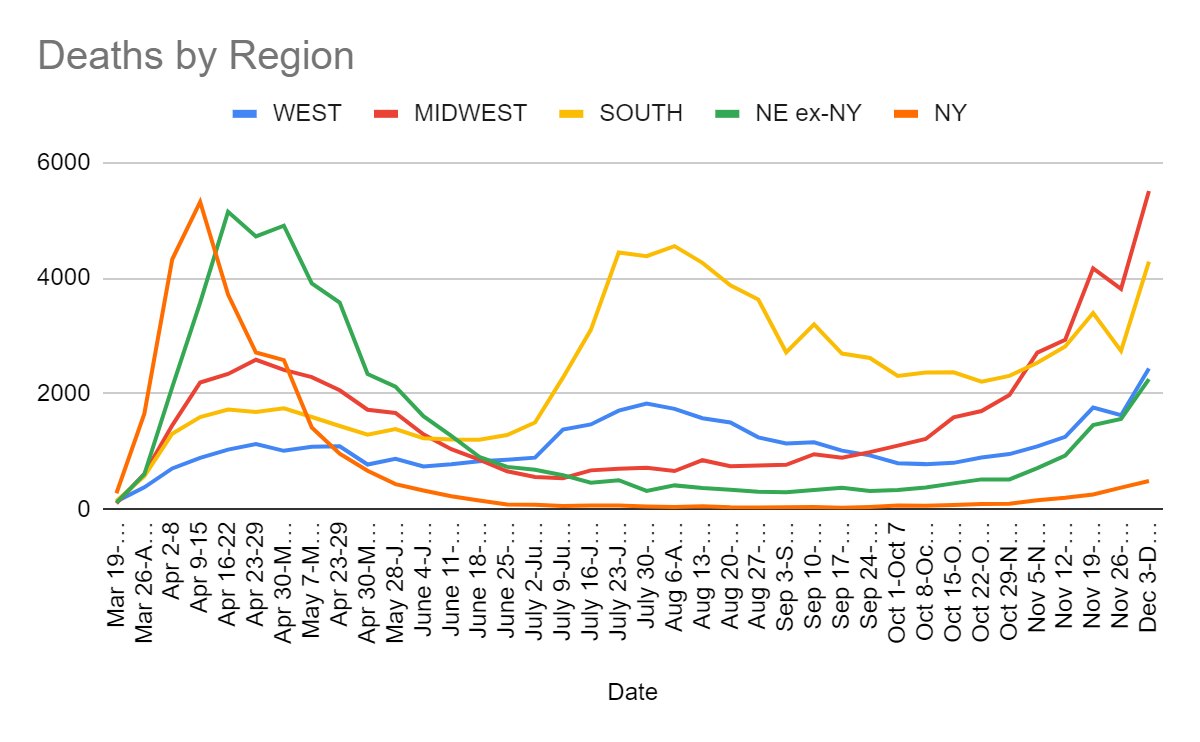
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 8-Oct 14 | 782 | 1217 | 2366 | 436 |
| Oct 15-Oct 21 | 804 | 1591 | 2370 | 523 |
| Oct 22-Oct 28 | 895 | 1701 | 2208 | 612 |
| Oct 29-Nov 4 | 956 | 1977 | 2309 | 613 |
| Nov 5-Nov 11 | 1089 | 2712 | 2535 | 870 |
| Nov 12-Nov 18 | 1255 | 2934 | 2818 | 1127 |
| Nov 19-Nov 25 | 1761 | 4169 | 3396 | 1714 |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
If anything, deaths continue to lag infections, likely due to holiday effects, so this is likely an underestimate of how bad things are out there. Even at face value, things are clearly quite bad. The Midwest number is higher than any previous peak, the South is not far behind and the total death count is at an all time high, with numbers going up dramatically everywhere.
Positive Tests
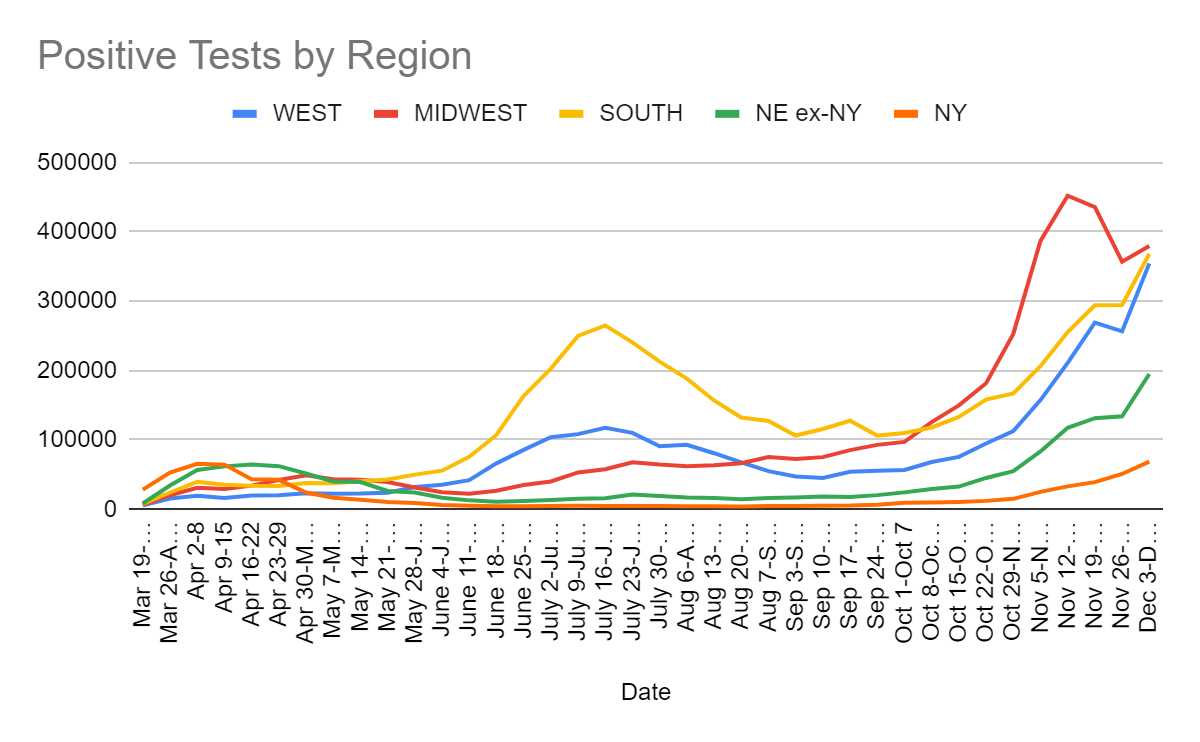
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 8-Oct 14 | 68284 | 125744 | 117995 | 38918 |
| Oct 15-Oct 21 | 75571 | 149851 | 133238 | 43325 |
| Oct 22-Oct 28 | 94983 | 181881 | 158123 | 57420 |
| Oct 29-Nov 4 | 112684 | 252917 | 167098 | 70166 |
| Nov 5-Nov 11 | 157495 | 387071 | 206380 | 108581 |
| Nov 12-Nov 18 | 211222 | 452265 | 255637 | 150724 |
| Nov 19-Nov 25 | 269230 | 435688 | 294230 | 170595 |
| Nov 26-Dec 2 | 256629 | 357102 | 294734 | 185087 |
| Dec 3-Dec 9 | 354397 | 379823 | 368596 | 263886 |
Outside of the Midwest, it seems clear things continue to rapidly get worse, and last week was a data hiccup as expected. In the Midwest, it looks plausible from this graph that things have peaked, but positive test percentages will be the judge of that.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Oct 1-Oct 7 | 6,009,923 | 5.2% | 763,935 | 1.3% | 2.28% |
| Oct 8-Oct 14 | 6,322,326 | 5.7% | 850,223 | 1.1% | 2.39% |
| Oct 15-Oct 21 | 6,440,150 | 6.5% | 865,890 | 1.2% | 2.52% |
| Oct 22-Oct 28 | 6,933,155 | 7.5% | 890,185 | 1.4% | 2.67% |
| Oct 29-Nov 4 | 7,246,068 | 8.6% | 973,777 | 1.6% | 2.86% |
| Nov 5-Nov 11 | 8,285,598 | 10.6% | 1,059,559 | 2.4% | 3.13% |
| Nov 12-Nov 18 | 8,917,701 | 12.4% | 1,155,670 | 2.9% | 3.47% |
| Nov 19-Nov 25 | 10,430,055 | 11.6% | 1,373,751 | 2.9% | 3.83% |
| Nov 26-Dec 2 | 9,788,446 | 11.5% | 1,287,010 | 4.0% | 4.18% |
| Dec 3-Dec 9 | 10,458,813 | 13.7% | 1,411,142 | 4.9% | 4.61% |
Test counts have recovered back to their peak and should presumably resume going up now. That positive rate is one ugly number, and it looks like New York is rapidly ceasing to be that much safer than the rest of the country, although it does run way more tests than most places.
The cumulative positives number is getting quite substantial, especially given how many infections are being missed, and that those infected are not a random sample. Without immunity from those already infected, we would likely be seeing growth now like we saw back in March.
Positive Test Percentages
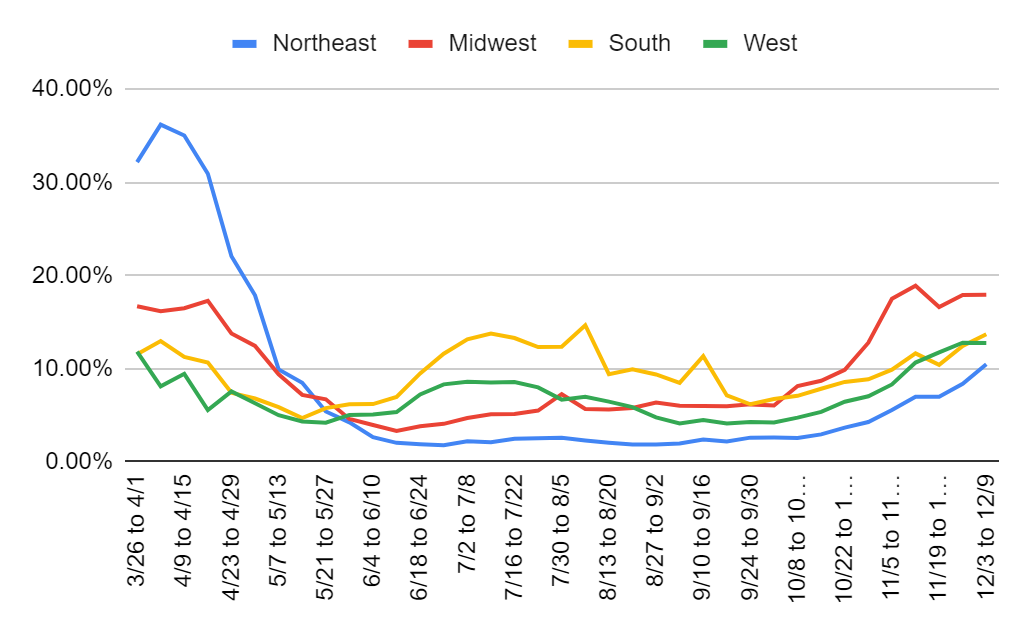
| Percentages | Northeast | Midwest | South | West |
| 10/8 to 10/14 | 2.57% | 8.14% | 7.09% | 4.75% |
| 10/15 to 10/22 | 2.95% | 8.70% | 7.85% | 5.36% |
| 10/22 to 10/28 | 3.68% | 9.87% | 8.58% | 6.46% |
| 10/29 to 11/4 | 4.28% | 12.79% | 8.86% | 7.04% |
| 11/5 to 11/11 | 5.56% | 17.51% | 9.89% | 8.31% |
| 11/12 to 11/18 | 6.99% | 18.90% | 11.64% | 10.66% |
| 11/19 to 11/25 | 7.00% | 16.62% | 10.41% | 11.75% |
| 11/26 to 12/2 | 8.38% | 17.90% | 12.45% | 12.79% |
| 12/3 to 12/9 | 10.47% | 17.94% | 13.70% | 12.76% |
I am ready to believe the story that the Midwest is more or less peaking now. Their test percentages have been in a narrow range for the last five weeks, and their immunity effects are rapidly increasing. The West’s number is encouraging, but it is on vastly more tests. That many more tests should drive down percentages enough to account for this, or alternatively disproportionally many negative tests got reported late and are warping the curve there a bit. Optimism seems premature.
In the Northeast and South, trends do not look good, and the Northeast especially looks quite bad, as if a combination of holidays and colder weather has broken the control system, and things are likely to get substantially worse before they get better. Time to bunker down.
My best guess is that the likely overall true peak is after the effects of Christmas and New Year’s, so the measured peak of infections should be some time in mid-January, with deaths closer to the end of January. Early vaccinations will assist a little with this, but not much, as they are going to the vulnerable and deserving rather than to those most likely to spread the disease, and there are not that many doses.
Note that I continue to not list hospitalizations in these charts. They continue to rise, but that seems to me to still say more about how hospitals are handling things than about how many are infected or sick. Even if things were improving and there were plenty of beds, hospitalizations would still be rising now, because there would be more people getting sick now than are ready to leave the hospital, as discharges are going to lag cases by quite a bit. So while it’s certainly something I look at as a sanity check, I don’t know what it can teach us.
Covid Machine Learning Projections
For those interested, here’s a closer look at the Covid-19 Projections website’s nowcast model for true prevalence. Layman summary by him on Twitter here. Can be compared to his earlier write-up here. Seems intuitively like reasonable approximations. What it doesn’t look like is the output of a machine learning algorithm, which is interesting. It looks a lot like something I would create if I was trying to plausibly fit a bunch of curves and generate reasonable claims in a smooth consistent manner, except that this uses a suspiciously large number of round numbers. I have some experience with this sort of thing.
The machine learning project doesn’t know about Thanksgiving and its warping effects on data, so it still thinks there was a brief downward blip in infections a few weeks ago, although it now recognizes that things resumed getting worse shortly thereafter. If you smooth that out, answers here continue to seem sane and they see us as having had 630k infections per day two weeks ago, with 2.6% infected at that time and 17.3% of the population having been infected at some point, or over 20% by today. I continue to think that answer is on the very low end of plausible.
Europe
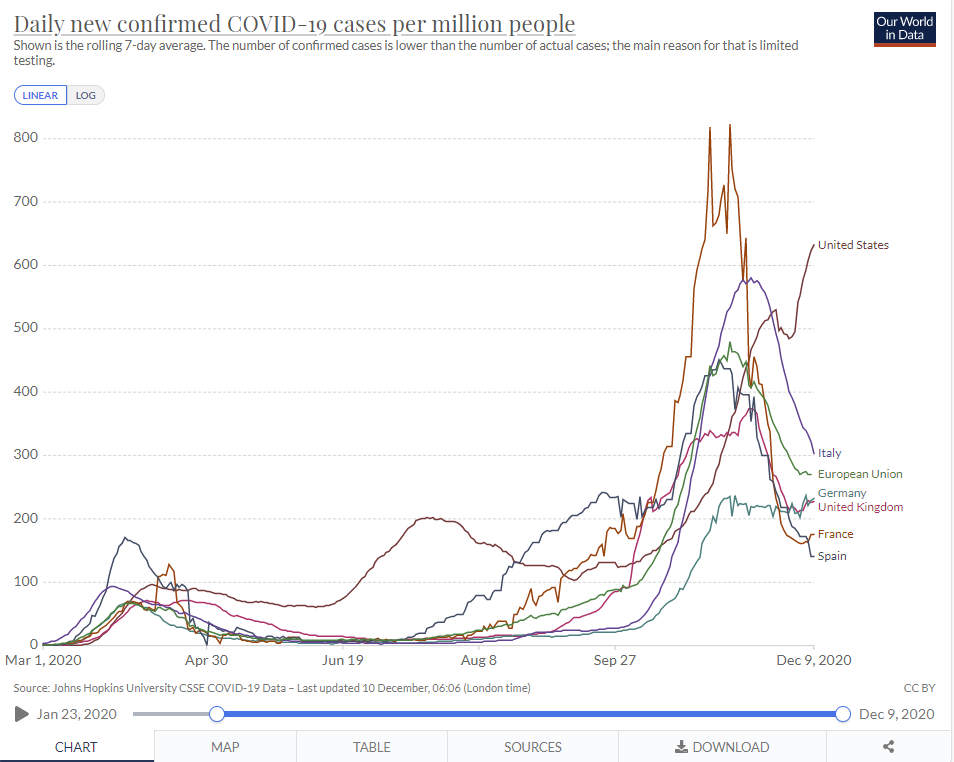
Germany continues to be stable. Many others have seen dramatic declines from their peaks, and the United States once again has a far worse Covid problem than Europe.
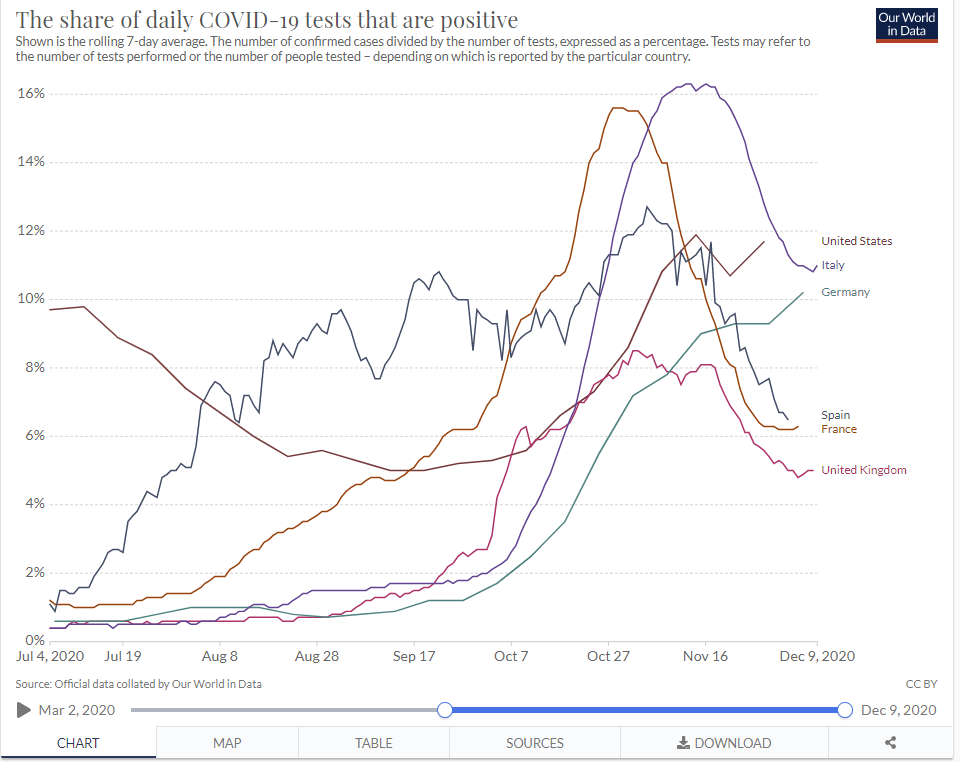
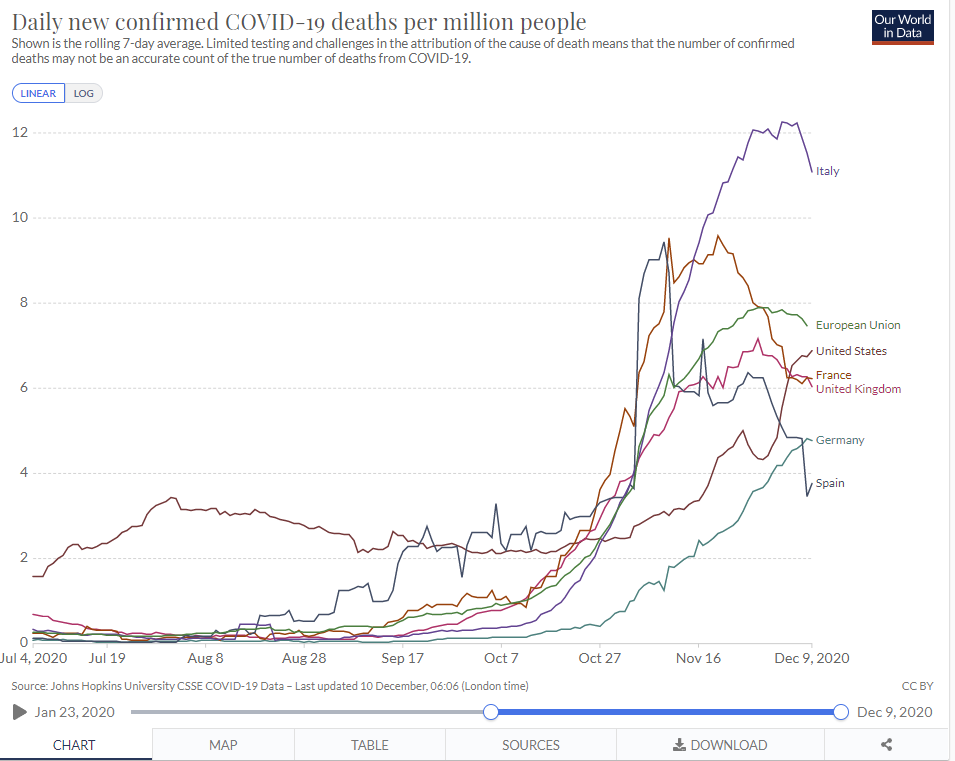
My news sources have not seen much happening in Europe this week, and the charts seem straightforward. Countermeasures have worked in at least containing things and preventing them from getting worse, but no one is aiming at suppression, instead they are waiting for the vaccine.
No, Not That Pandemic Vaccine, That Other Pandemic Vaccine
Team behind Oxford Covid jab start final stage of malaria vaccine trials. This is excellent news. Also a reminder that the world is smaller than it appears, as the same team behind one of three Covid-19 vaccines also produced this one. Given how most of the time and effort involved in vaccines seems to involve testing them and overcoming regulatory barriers, it should not be surprising that teams that make one vaccine can also make more.
Malaria is kind of a big deal, killing over 400,000 people a year. Bed nets are one of the prototypical Effective Altruist causes. Whether or not the best strategy would be to instead eradicate malaria in Africa the way it was eradicated in America, that is not happening at the moment. Barring that, a cheap and widely available vaccine seems like an excellent way to go.
“A lot more people will die in Africa this year from malaria than will die from Covid. I don’t mean twice as many, probably 10 times,” Hill said. The vaccine “is going to be available in very large amounts, it works pretty well. And it’s going to be very low priced.”
The vaccine could be in use by 2024 if the final human trials are successful, he said.
So we are now entering the final stage of trials, which means we are only three years away from starting vaccinations. Some time next year, 4,800 children will be vaccinated, then we will wait a very long time, likely in part because we only vaccinated 4,800 children. This is what people mean when they say what a great achievement the Covid-19 vaccines have been in terms of speed. Here we have a vaccine that likely could save over a million people if we sped up its release and distribution by three years, and we are not doing that because of reasons.
All of you Effective Altruists who were already working hard on malaria, is there any way to push on this and make it go faster? Perhaps you can arrange for a larger trial that will gather more data faster? Perhaps you can fund scaling up production or distribution faster in advance? What about Bill Gates, who is very involved with malaria and funded pre-production of Covid-19 vaccines? By the end of 2021, we should have sufficient doses of Covid-19 vaccines, which leaves years to handle production on this one even if they are in conflict. It does not appear this is getting the level of urgency it deserves.
All I Want For Christmas Are a Covid Vaccine and a PS5, But They Underpriced Them And Now They’re All Sold Out
What does everyone else want for Christmas?
A PS5, yes. And thanks to my good friend Seth Burn, I got one! Section title will have to change.
For a slim majority, also a Covid vaccine.
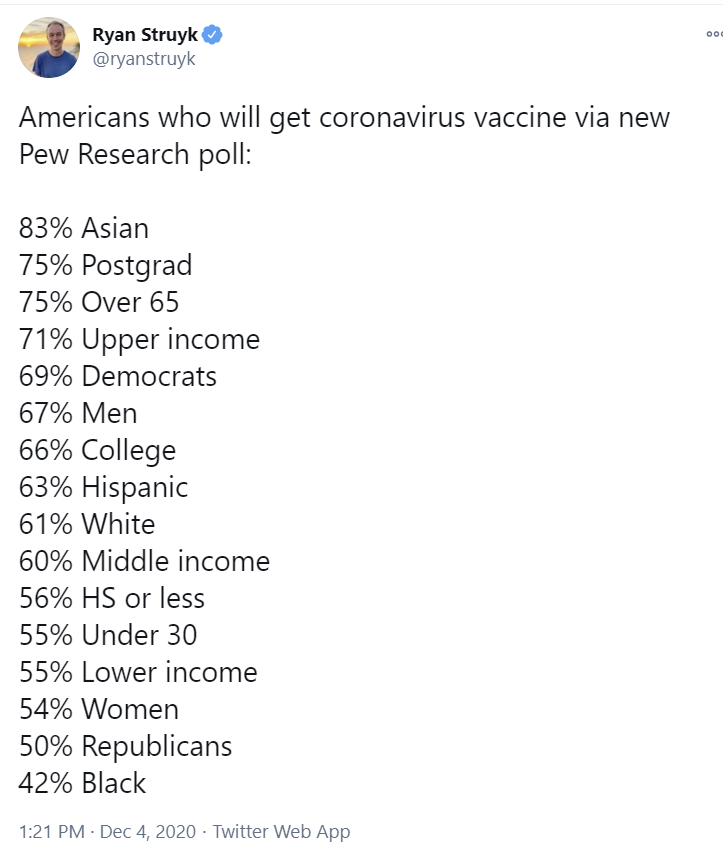
There was a Pew Research survey this week on who intends to get the vaccine.
For those who want to guess who wants it more before looking, the categories are Male, Female, Postgrad, College, HS or less, Upper income, Middle income, Lower income, Over 65, Under 30, White, Black, Hispanic and Asian.
Answers are at the end of the section via screenshot (or Twitter source here).
To help convince the hesitant ones to change their minds, at least some skin in the game is officially here: Former Presidents Obama, Bush and Clinton volunteer to get coronavirus vaccine publicly to prove it’s safe. I would assume Biden as well. Trump already had Covid-19, but if the goal is to show it is safe rather than effective, it would be great if he joined them anyway. I haven’t seen this actually suggested anywhere? Will be a while before it matters much, given the severe shortage of doses.
You know who should likely get the Covid vaccine early? Airline pilots.
So naturally, the FAA is currently telling them that if they get their vaccine, they will lose their medicals, and not be allowed to fly. They are monitoring the FDA’s decisions closely, but pilots are not allowed to get vaccinations that don’t have full approval. I would never have predicted this particular plot point, but on a meta-level I find it entirely unsurprising. It makes sense that there would be government regulations that ban the vaccine from getting to some of the people who need it most. That the best we can hope for is that some such authorities try to kill us less aggressively some of the time.
Scream If You Wanna Go Faster
The vaccine even works faster than we thought! From the FDA report: Looks like efficacy even for one dose might be 88.9%. Here’s the graph.
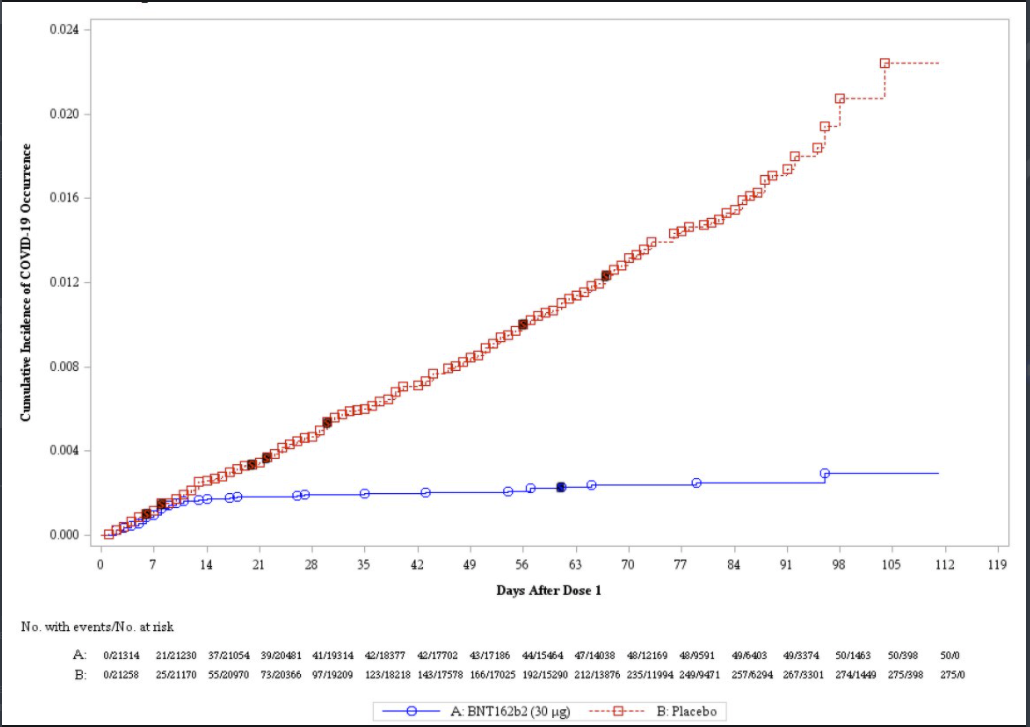
That doesn’t mean we can do only one dose per person for a while until we have enough doses, because we don’t know the consequences of a longer wait or whether the immunity from only one dose would last, but it’s still great news. It also puts people in a profoundly weird spot, since they’re mostly immune now, but will be much more immune soon. How safe do you play it during that period?
Business insider asks why the United States is behind the United Kingdom in approving the vaccine. Here is the functional explanation they give:
The regulatory process involves experts reviewing “thousands of pages” of technical information, an FDA representative told Axios on Tuesday.
The agency also has to evaluate the manufacturing process, check statistical analyses, and look at the effect of the vaccine on groups of people with high risk of side effects, the representative said.
The FDA and the Medicines and Healthcare products Regulatory Agency, the UK regulator, have different processes to review vaccines, Dr. Penny Ward, a visiting professor in pharmaceutical medicine at King’s College London, told The New York Times.
The FDA asks drugmakers for raw data, which it reanalyzes, while British regulators rely more heavily on reports produced by the drugmakers.
An alternative hypothesis is that the FDA is delaying the process intentionally. With the cover story that this is being done ‘in order to be careful’ so as to prevent fear that the vaccine was rushed. I strongly agree that there are approximately zero people who are going to look at the gap between application for approval and when the FDA approves the application, and use that as a true objection that justifies not taking the vaccine. To the extent that this group has non-zero members, the group Tyler points out, that takes the delay as worrisome and uses that as its true objection, is not obviously smaller.
The simpler explanation is that there was already a meeting scheduled for December 8-10, people had holiday plans, and the FDA simply did not care enough about doing this faster to move the meeting.
In other Tyler modeling news, while the cause of faster vaccine approvals is clearly righteous, I do not think we can model a day’s delay in approval as delaying vaccine production by one day. The story flat out makes no sense to me. Pfizer is not going to produce vaccine slower, at any point, because the FDA gives formal approval on December 10 instead of November 30. The vaccine is already approved in the UK, so there is a guaranteed place to sell more doses than they can possibly produce this month, in the worst case scenario. The probability of approval by the FDA isn’t 100%, but given their knowledge of the data, it’s close. Every sign points to the approval being a formality. So I hold strongly that the damage done is that current doses are shipped with a delay, not that all doses are delayed.
Still, that’s pretty bad. It looks plausibly like a third of all deaths are of nursing home residents that could be reached in the first wave. So they all are getting vaccinated two weeks late, which means the cost here is something like 1,000 additional deaths per day of delay from that alone. Then add in the healthcare workers, and their new ability to actually do their jobs fully and also avoid turning hospitals into outbreaks. So yeah, it’s a lot of blood, but giving them every death between application and approval isn’t fair.
After I wrote that section, Tyler wrote a post even more explicitly disagreeing with this, essentially claiming that yes approval would accelerate other tasks substantially, which I continue to mostly not buy. I think his argument holds when approval is truly uncertain, but not when it is a formality. I do understand and share the frustration with those who use constraint X to justify not working to remove constraint Y, which we don’t work on because constraint Z, which we don’t work on because constraint X. Yes, we should be working on the other constraints. But that doesn’t change the answer to the question.
Switzerland is going even slower, making the usual noises about the need for ‘caution.’ My read is that this is because they did not order vaccine doses early enough, and now they are all sold out, so why not spin that by not approving the vaccine for a while and calling it ‘caution?’
As we know from last week, the Europeans are taking it relatively slow, despite knowing the answer already:

The impression it gives to me is not that officials were taken by surprise. It is that they had a choice to make, and made it.
Cell asks how we might speed up future vaccine development in case of a new pandemic. The strategy is based on it not being that hard to predict where future pandemics come from. If most are going to be variations on a few existing virus families, we can do a lot of the work in advance. They suggest that for only a few billion dollars, we can do advance Phase I and Phase II trials for vaccines designed for each virus family that could plausibly cause a future pandemic, stockpile doses, and be ready to proceed to Phase III right away.
If we had the vaccine in question ready to go on day one, then the phase III could begin the equivalent of February, then all we’d have to do is wait for enough infections.
What they do not say is that we could do much better than this by using human challenge trials. If we were willing to do such trials, and had already gathered safety data, there is no reason we could not know the vaccine’s effectiveness and safety within a few weeks of identifying the new pathogen. Remember, Moderna created their vaccine in two days. Then all that is left is to scale production.
Cell does not suggest this, instead taking the need for a regular Phase III as a fixed law of nature that cannot be changed even when preparing in advance for a future threat.
And that’s valuable! I am glad that people are taking seriously the question of “if the people and procedures in charge of slowing down and stopping development must be accommodated, how can we do that as quickly as possible?” Very good question. I only wish we could also fully ask an even better one.
The vaccine is the ultimate case of More Dakka. However much we are spending on it, it won’t be enough. We should spend more. That was true before. It’s still true now. The case for going big remains overwhelming. This whole time, we could have built far more capacity in exchange for (in context) trivial amounts of money. Pfizer offered us 200 million doses of vaccine in July, but we balked at the price tag, and only ordered 100 million doses. Then this week the Trump administration tried to buy more, but Pfizer informed us that other countries bought those other doses instead, and they won’t have capacity for more until next June. Whoops. Then Trump issued some sort of executive order demanding that the doses go to us instead, because America, to which the chief scientist of Operation Warp Speed has said, “I literally don’t know” what it means. And in an evergreen statement, “The White House is doing what the White House is doing.”
I don’t think this is going to slow us down much once Moderna is added to the picture, but if this mistake costs us all an extra month or two of our lives, it would be one of the worst times someone has walked away from an obviously great deal. If I was told my available dose was in June rather than April, I don’t think I personally take that much extra risk given how perilous a state the hospital situation might be in for the next few months, but it definitely feels like a plausible last straw for many. In particular, being given one timeline, then having a delay for such a stupid reason, seems very much a ‘screw it I’m done with this’ moment. Again, I’m not doing that if this happens. But if others do that, I totally get it.
The Money Illusion has thoughts, speculating that bureaucracies are simply incapable of adjusting on the fly when the things that change matter. In Sumner’s proposed model, what you enter the crisis with is mostly what you are stuck with unless you force their hand, and we forced it but not enough.
The Grumpy Economist wants to go fastest of all. He suggests the obviously correct answer, which is to allow free market vaccines and to distribute them by price, starting in February for those willing to buy it under those conditions. He claims this would have prevented the pandemic, which is going too far, since scaling up production and convincing enough people to take it would have taken months.
If we wanted to prevent the pandemic in the first place, that requires going much further. We would have needed to allow free market testing.
Let us be clear. Government bans on private action are entirely responsible for the entire pandemic in the West. Period.
Meanwhile in India, they rejected the emergency use authorization for AstraZeneca’s vaccine. Which seems entirely unsurprising, given that there are all sorts of problems with the studies so far, which is why they didn’t even attempt such a thing in the West. But of course, it’s also, from an expected value position, completely insane. The vaccine is super cheap and the safety data seems ironclad. So what if we don’t know how effective it is? It’s weird to pick on India here. If anything, they deserve praise for making it worthwhile to ask the question at all. They might have gotten the right answer, even though they didn’t.
For Me But Not For Thee
Austin Mayor Steve Adler (source):
Late Show Host Steven Colbert (source):
The Ramsey Tax Is Too Damn High
I think this calculation by Tyler Cowen, viewing Covid-19 as a “Ramsey tax problem,” is not only importantly wrong but exactly backwards and rather perverse, in ways worth exploring.
The whole point of saying we are overreacting, to say that the costs of Covid-19 are not that high, is exactly to argue that the costs borne have been extraordinarily high. The claim is that the costs from infection are low, and that we are making a mistake to bear such high costs, such huge deadweight losses. There hasn’t been a huge non-health loss as a law of nature. There’s been a huge non-health loss because we made choices. Why must we accept those choices as given, and thus assume that the non-health costs must be so high relative to counterfactual health costs, if that is the current situation? And why are such people being accused of making moral claims when they are making efficiency arguments?
In particular, why is “talking people out of their high elasticity” equivalent to the statement “Don’t leave NYC just because the taxes are going up! It will wreck the city.”? Tyler’s sentence is calling for sacrifice by the individual on behalf of the group. Whereas talking people out of their high elasticity is more like “you would be better off living your life mostly as you lived it before, and accepting that you are likely to get Covid-19 at some point, because life is short.” If anything it’s the opposite of the group sacrifice. What is going on here?
The better educated tend to be staying safer than the lower educated, as Tyler says. That seems like a distinct argument.
He then goes on to note this:
As a side point, note that in the 1968/1957 pandemics elasticities of adjustment were way lower, because you couldn’t switch things to Zoom, Amazon, and so on. So those pandemics were closer to being a “lump sum tax” on human life and thus they were cheaper, and had lower deadweight loss, probably in per capita terms as well. From the framework on welfare economics, that is. The value of human lives was lower then too.
That does not seem like a side point! It seems like it’s going even farther, and saying that we are worse off because we have the choice to use Zoom and Amazon, and choices are bad. In this case, in part because the choice creates a Copenhagen effect. It seems clear to me that in general having the option to overpay for safety is quite bad. The option to have us collectively do this is even worse. If Tyler is explicitly agreeing that if we lacked this choice, we would have all been better off, then what is he actually arguing for?
There is a distinct argument offered that those with better educations tend to be taking more precautions. To some extent this is obviously unfair, since those with higher educations are often those better able to work from home, and those with better financial cushions. They are also those who tend to listen more to authority, and worry more about looking responsible and safe, and they tend to be members of the blue tribe. The idea that they are doing this because they are smarter or make better decisions is… one hypothesis, sure. Definitely not the whole story.
Also worth saying that an individual cannot decide to not pay the Ramsey tax here, and accept the Covid risk. That choice is unavailable at this time. The world around you is not going to let you do the old normal things. Thus, one can realize that given one’s remaining options it makes sense to play it safe, while also preferring the world in which no one played it safe and you did not either.
It is also perfectly fine to do any or all of these things, while also preferring the world in which we did proper suppression.
If we knew at the beginning what we know now but were restricted to the choices of “pay more costs” or “pay less costs” a lot of people would choose “pay less costs,” both as a collective and as individuals.
Both for society in general, and for themselves in particular.
All Masks Are Not Created Equal
Robin Hanson asks why we treat all masks as the same, simply saying ‘wear a mask,’ when it is very clear that N-95 and surgical masks are more effective than cloth ones:
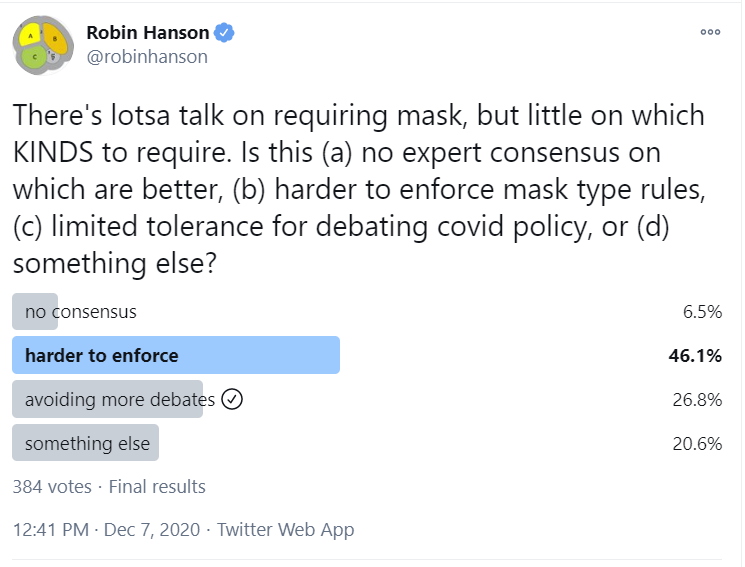
In my model, all three of these explanations play a meaningful part in the debate.
There is still a huge lack of consensus on how much better surgical is than cloth. That’s what happens when you ban experiments. It makes it hard to learn things.
There is clearly very limited tolerance for debating Covid policy, and even less for advocating such policy to the public, or even getting them the message.
That’s one of two central things going on, in my mind. You Have About Five Words [LW · GW]. We can maybe tell people “Social distance, outside, wear masks.” We don’t want to burn another word here.
There’s also what happens when you make that higher ask of people. If you count cloth masks that one can reuse as needed and are in plentiful supply, and that in my experience are relatively comfortable and look relatively normal, you have made a highly reasonable ask, which a lot of people still treat as unreasonable. You can even customize your cloth mask as a fashion statement or other signal of affiliation.
If you instead were to say, it needs to be N-95 or surgical (and if you allow both, then it’s not only one word of your five that you’re burning here), then there would be a lot of ‘nope, not reasonable, not doing that.’ Then they’ll often wear no mask at all.
Or they’ll wear a mask, but less often, especially when it actually matters. For the most part, that trade-off isn’t worth it.
The public doesn’t have the ability to process ‘sort of works’ or ‘this works, but this works better.’ They can’t handle ‘this is somewhat safe, but this other thing would be safer.’ You get to say, these things are safe, do those, these other things are unsafe, don’t do those, with clear markings. That’s it. Try to be detailed and there will be a huge demand for “Do cloth masks work, or not? Well? Stupid so-called ‘experts.’” Or they’ll think asking that question owned the libs.
They certainly would not take kindly to being told the most important thing is a cloth mask, then the moment there are enough other masks, changing tunes (after initially lying about masks working at all) and demanding better.
So instead we wisely took the option for a clean, simple message. Wear a mask, period. If you’re on the ball enough to upgrade to N-95, great, that’s even better.
This is a whole section because this logic extends to all our other strategies and policies, including outside of Covid-19.
In Other Covid News
CDC recommends this week that Americans wear masks indoors when not inside their own homes. Let that sink in. Until last week, the CDC had not recommended this. Still, better ludicruously late than never, even for the single most important thing to be doing. Thank you, CDC.
Taleb notes: Masks work, says Danish study people described as not saying that masks work.
New York City vaguely aware sewage data might be helpful, but not so aware as to release said data anywhere I’m aware of, or to make any effort to isolate locations or otherwise use it to contain the virus.
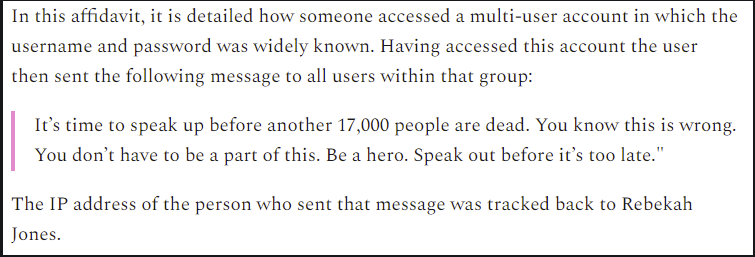
Police were sent to seize the laptop and phone of Rebekah Jones. That was her account via Twitter, alternatively two news report are here and here. She was responsible for Florida’s Covid-19 database before she was fired. She claims (credibly, as far as I can tell) that she was fired by Florida for refusing to falsify Covid-19 statistics early in the pandemic. She has spent the time since then trying to provide accurate data and expose corruption. For this, the police pointed a gun in her face and the face of her children, and seized her devices, claiming it was about a security breach. Which, one way or another, I suppose it was. In particular, they cite this particular breach, which was accomplished by ‘no one bothered to change the login credentials’ (direct source):
If you’d like to get involved, the thread linked to has details on how you can help.
Yet another cheap, fast, easy and seemingly reliable method of Covid-19 testing that, if it works and was implemented, would end the pandemic. This one uses the microscope on your smartphone and can even give you viral load information. So of course I barely registered this news at all because I assumed there was almost no chance the test would be allowed. FDA delenda est.
There’s also this method of testing (source):
Seems great and I have little doubt we will never do anything of the kind.
A rather complete takedown, as far as I can tell, of an often-cited paper that concluded lockdowns are highly effective and saved three million lives in Europe. It’s a lot of words that mostly aren’t necessary, because it suffices early in the takedown to point out that the paper assumes its conclusion. If you presume that the only things that ever change transmission rates are non-pharmaceutical government interventions, then the alternative to such interventions is that almost everyone quickly gets infected while hospitals are completely overwhelmed, and that’s how you get three million lives saved. So, sure. If there are no control systems and people don’t adjust behavior except when the government issues an order, at which point they instantly adjust to the new transmission rate (which is what the paper assumes), then of course you are going to conclude that all credit must go to the only thing that ever changes anything. This is the level of scientific literacy and interaction with physical reality that even relatively competent Western governments and policy makers (e.g. European ones) seem to be employing these days.
California is locking down hard.
Here’s the order for Los Angeles. Everyone must stay in their homes. Among other details, podcasts are explicitly exempt, religious services must be outdoors but are otherwise all right, and protests are explicitly allowed. Malls open, playgrounds closed. I think I sense a protest coming on.
It’s unclear to me how this is supposed to work out. Do they think people are going to obey rules where they can’t meet a single other person while socially distanced, unmasked and outside? Do they not understand that if you push unreasonably far, people stop listening to you? How would one even begin to enforce such a rule? How long do they intend to maintain things this severely? Conditions elsewhere are probably not going to be much better until at least February or so at the earliest. The full turnaround will likely take months beyond that. Is the plan to shut down the city completely that whole time, on top of what has already been done and not worked?
Ohio High School Athletic Association coronavirus rules: Students can wrestle, but can’t shake hands. On the one hand this is obviously absurd. If shaking hands is not safe, what exactly do the decision makers think is happening when kids wrestle? On the other hand, shaking hands is a purely symbolic action that you need to stop across the school, whereas wrestling is a compact activity providing value.
Paper claims that a region in Brazil has 75% overall infection rate. About half by the epidemic peak, the rest after. Raw test numbers were not that high, but they feel confident correcting for waning antibody counts, and the implied IFRs are not unreasonable. They have some speculations on how the numbers got this high, but nothing satisfying. My best guess is quite simple, that the region was unusually vulnerable and also mostly young and taking few if any precautions, and it got hit hard enough to far overshoot its immunity threshold.
Winter is Coming
In other More Dakka news, we want to meet everyone outdoors and go on walks, but baby it’s cold outside. Sounds like a problem. In a move I delayed for too long, I’ve ordered the warmest coat known to man. Should have done it last month, but better late than never. I was going to go with the third warmest coat known to man because for my needs that was definitely enough dakka, but in a running theme these days, they underpriced them and now they’re all sold out, so instead I am ready, if necessary, for a cozy winter in Winnipeg. Which was the motivation behind my friend Seth Burn finding out about this coat in the first place, which he loves. I’ll report back when it arrives. Not cheap. But if it works, totally Worth It.
Until next week.
31 comments
Comments sorted by top scores.
comment by Mitchell_Porter · 2020-12-11T10:56:04.242Z · LW(p) · GW(p)
Now that western governments are scrambling to approve and deploy vaccines, it must be the beginning of the end of the pandemic in the west, and I am glad of that. But I am concerned that I don't have a coherent understanding of so much of what happened this year.
Mainstream media reporting is a jumble of anecdotes and numbers without context, but overall their big picture is that this is a disaster and we should all obey the public health restrictions until the authorities tell us that it's over and we're safe.
I have a sociological explanation for why this is the mainstream narrative: As the Trump/Brexit years of western populism have made clear, western mainstream media speak from a particular class standpoint - I could describe it as 'boardroom progressivism' - and the vaguely upper-middle-class stratum who are the social base for this worldview, are the social class who are least affected by the lockdowns - information-age professionals who are happy to work from home, and who can afford to do so for long periods. They can afford an approach of maximal precaution, and so the media and politicians who represent them, are all about erring on the side of caution, having lots of restrictions and keeping those restrictions for as long as it takes.
(This explanation could be wrong; I don't belong to this class, this is just my attempt to read between the lines.)
Meanwhile, in social media one may find the contrarians who maintain that there has been an enormous overreaction. I find this plausible, but that raises the question, what would have been a commensurate reaction; especially when one takes into account the uncertainty which existed in the early days. E.g. suppose that a public health strategy of vitamin D for the masses and 'focused protection' for the vulnerable would have been a viable and far less costly alternative to the lockdowns; what are the odds that someone could have figured it out in time?
One of the key issues in the debate between the mainstream and the contrarians, is that most of Covid's victims have been elderly. I think we all know the argument: that tens of millions of people who are at almost no risk from Covid, are making major sacrifices to protect other people who are at the end of their lives anyway. I find it hard to think straight about this. I'm a transhumanist who would like to see aged care homes become rejuvenation centers, so in principle I'm in favor of more life for the elderly, but obviously the masterminds of contemporary public health policy are not coming from this position. The critics of the mainstream Covid policy say, flu season always kills many of the old and infirm, but we never before shut down society to prevent this from happening, so why do it now?
There is not only a normative question here, the question of the right policy; there is also a simple question of fact: how and why did lockdowns become the default response to Covid? I could say that it caters to the alleged hegemonic social class of boardroom progressives that I mentioned, but I'm not sure I believe that's the reason... Alex Berenson has written a small book on the origin of the lockdown strategy. I haven't read it, but it sounds important for those wanting to understand how that became the standard response worldwide.
There's a lot that I puzzle over, this is just part of it. Meanwhile, Zvi has worked hard to give us detailed numbers for America and an analysis of what they mean. At some point I'll have to re-read his entire sequence from the beginning, and see what big picture it implies.
Replies from: TAG↑ comment by TAG · 2020-12-11T16:03:37.457Z · LW(p) · GW(p)
Lockdowns aren't actually good for the PMCs, they're just less bad. That being the case, the default explanation that lockdowns are to protect the elderly holds.
Replies from: Mitchell_Porter↑ comment by Mitchell_Porter · 2021-01-01T21:54:42.873Z · LW(p) · GW(p)
lockdowns are to protect the elderly
Let's suppose we're trying to understand why almost every society on Earth engaged in unprecedented society-wide lockdowns, over a virus which is certainly highly lethal e.g. for people in their 80s, but which is mostly harmless for people in the prime of life.
I like the theory above - that the lockdowns are to protect the elderly - because of its simplicity. If it's true, it should be possible to present an account of what happened in 2020, in which that thought and intention is central.
But to develop that account, further nuances need to be brought out. For example, if we focus just on western countries for a moment, would the more nuanced explanation be, that it was largely about protecting the parents of the progressive managerial class? (is that what PMC stands for?) - in the sense that this is the social stratum whose sensibilities make the difference between one policy and another, in many cases.
But then we would want to explain that countries as different as China, India, Saudi Arabia, and South Africa also engaged in lockdowns. Was the same logic at work in all of them? But in East Asia they also had the experience of the far more lethal 2003 SARS (and, it now occurs to me, Saudi may have had the analogous experience of MERS, to encourage swift severe lockdowns).
With respect to global use of lockdowns, I think WHO and the G20 did a lot to encourage it, so that would be part of the chain of cause and effect... And another aspect of understanding how the year unfolded, would be to think of the public health response in each country, as something constantly in evolution, and also contested.
So maybe my provisional explanation is that there was a convergence of practice between SARS-terrified Asia and the elites of the information-age West, and that this then became a new global norm via bodies like WHO and G-20.
Replies from: TAG↑ comment by TAG · 2021-01-02T22:27:51.657Z · LW(p) · GW(p)
unprecedented
The unprecedented part is the global,not the lockdowns. Staying inside during plagues is well attested historically.
But to develop that account, further nuances need to be brought out
Maybe, you are not really saying what is is wrong with the simple account. You keep harping on about the professional managerial classes, but you still don't have evidence that lockdowns are benefitting them, or that they are not benefitting the relatives of poorer people.
Wanting to make sacrifices to protect your elderly relatives is not weird.
Replies from: Mitchell_Porter↑ comment by Mitchell_Porter · 2021-01-03T14:18:44.223Z · LW(p) · GW(p)
you still don't have evidence that lockdowns are benefitting them
I was struck by the case of a political columnist who tweeted an appeal to ordinary people, to just let their businesses fail, rather than risk orphaning their kids; while she herself went about organizing a new online business venture involving dozens of colleagues.
Lockdowns are hardest on those who are already vulnerable, and on people who can't work from home. But digital society is run by affluent people who spend their working days in front of a computer. It makes sense that they would be much less sensitive to the drawbacks of a stay-at-home policy.
Replies from: TAG↑ comment by TAG · 2021-01-03T17:46:44.483Z · LW(p) · GW(p)
And it still doesn't follow from that , that anything untoward is going on.
The events match the narrative where the evil PMCs screw everyone else over, but they also match the narrative where lockdowns are the best solution for everybody.
So you still need to disprove that.
Replies from: Mitchell_Porter↑ comment by Mitchell_Porter · 2021-01-06T15:56:27.989Z · LW(p) · GW(p)
At this point, I am not trying to show that lockdowns were an overreaction, so much as I am just trying to understand why events unfolded as they did.
How did the idea of a national lockdown enter public health contingency plans all over the world? (the idea existed before Covid, but I think people usually envisaged it as a response to a much deadlier pandemic). What are the attributes of Covid which made people regard it as dangerous enough to warrant national lockdowns? (e.g. a lethal respiratory disease, of a kind for which no vaccines existed). What made national lockdowns the global norm? (e.g. was it because WHO advised it and many countries follow WHO recommendations, or was it more a matter of public health officials in diverse countries independently coming to the same conclusion, because it really was the appropriate response).
So, just seeking the basic cause and effect of how the global pandemic response unfolded.
comment by orthonormal · 2020-12-16T17:30:14.299Z · LW(p) · GW(p)
Not the most important thing, but Adler and Colbert's situations feel rather different to me.
Colbert is bubbled with a small team in order to provide mass entertainment to the nation... just like sports teams, which you endorse.
Adler is partying for his own benefit.
Replies from: Zvicomment by romeostevensit · 2020-12-11T06:58:24.357Z · LW(p) · GW(p)
I'd like to be commenting on these more, unfortunately most of the things that occur to me to say are prosecutable under the insurrection act.
comment by Rana Dexsin · 2020-12-10T18:24:16.579Z · LW(p) · GW(p)
There was a Pew Research survey this week on who will get the vaccine.
To confirm, this is about who intends to seek out the vaccine, yes? The study mentioned by this article on the Pew Research site? Some of the text (especially the Twitter screenshot) was easy to initially read as “to whom the system will choose to allow the vaccine” instead.
Replies from: rockthecasbah↑ comment by Tim Liptrot (rockthecasbah) · 2020-12-10T19:52:35.693Z · LW(p) · GW(p)
Intends is correct.
Replies from: Zvicomment by maia · 2020-12-10T23:01:00.187Z · LW(p) · GW(p)
Here’s the order for Los Angeles. Everyone must stay in their homes. Among other details, podcasts are explicitly exempt, religious services must be outdoors but are otherwise all right, and protests are explicitly allowed. Malls open, playgrounds closed. I think I sense a protest coming on.
They reopened playgrounds. Source
comment by Alexei · 2020-12-11T05:27:26.077Z · LW(p) · GW(p)
If someone got COVID how long do they need to wait to get tested so that the test correctly identifies them as positive?
Replies from: adamzerner↑ comment by Adam Zerner (adamzerner) · 2020-12-11T05:35:05.242Z · LW(p) · GW(p)
I haven't spent much time looking into it, but I recall coming across this:
In the report on the findings published May 13 in the journal Annals of Internal Medicine, the researchers found that the probability of a false negative result decreases from 100% on Day 1 of being infected to 67% on Day 4. The false negative rate decreased to 20% on Day 8 (three days after a person begins experiencing symptoms). They also found that on the day a person started experiencing actual symptoms of illness, the average false negative rate was 38%. In addition, the false negative rate began to increase again from 21% on Day 9 to 66% on Day 21.
- https://www.hopkinsmedicine.org/news/newsroom/news-releases/covid-19-story-tip-beware-of-false-negatives-in-diagnostic-testing-of-covid-19
comment by George3d6 · 2020-12-12T20:08:53.399Z · LW(p) · GW(p)
If you can send back the jacket and get your money I'd seriously consider doing that.
Lookup any serious mountaineering guide and you'll see one thing regarding clothing:
LAYERING
Layering, layering, layering. Be it in the city or at 8000 meters high, layering seems like the most reasonable way to protect yourself.
After all, temperature variations of 5-10 degrees during a day and depending on if you're traveling or not they can carry by 20-110 degrees throughout the year, so what are you going to do? Have a special wardrobe for all temperatures? **** No
Skin-tight shirt, normal shirt, Merino sweater, fluffy warm jacket, sky/boating coat.
Merino leggings, some normal pants, potentially some fluffy pants (overkill usually, ankle socks are enough), and skying/boating pants (by which I mean, **** that is made to keep you warm in 100+km/h wet wind)
In my experience, you can get the equipment needed for 4k in the alps for < 300$ (granted, this summer had great sales), it pains me to see people spend 1000$ on a city jacket.
***
Also, the places where you "feel" cold are your face, hands, and feet. By the time your abdomen feels uncomfortably cold you've made a mistake and need to get the fuck to safety as soon as possible because permanent damage is setting in (unless you got your chest wet or something).
But you'll feel horrible pain from your hands and feet and face a dozen hours or even days before your "core" body temperature starts dropping enough for you to feel it. Granted, keeping the core warm will allow it to keep normal blood circulation in the hands/feet/face (thus warming them up)... but it's a secondary effect and you're walking a tight line between warm and sweating.
If you're uncomfortable with the cold, I'd bet at 5/1 odds that you'll feel better with:
1.
- Very very thick woolen socks, maybe 2 pairs, and some warm boots
- Thick gloves
- A mask (the kind bad guys wear in movies) over your face, and a hat, and a scarf, and some glasses (or some other more reasonable face-protection)
Even if your core is exposed (e.g. just a light jacket and some leggings under your pants).
Than with
2.
A very thick jacket but more exposed peripheries.
Replies from: Ericf↑ comment by Ericf · 2020-12-16T17:53:27.638Z · LW(p) · GW(p)
Anecdotally, I was comfortable walking around in no-wind winter NYC (so, in the 40s) in normal clothes & a coat + scarf, but felt super cold if I left off the scarf.
For temps in the low 60s, I didn't even need the coat, just a scarf with my t-shirt + long pants + sandals. Conversely, Jacket over the same is insufficient.
comment by AnnaSalamon · 2020-12-10T21:48:49.881Z · LW(p) · GW(p)
This is a nitpick, but to me it seems to overstate things to say:
and the United States once again has a far worse Covid problem than Europe
According to worldometers, the United States has so far had ~903 covid deaths for every 1M people, while in Europe, the UK has had 912 deaths/1M; Italy has had 1,036; Spain 1,012; Germany 253; France 871; Greece 324; etc. The US has a far worse problem than Germany or Greece or Finland, but a comparably bad problem to the UK or Italy or Spain or France. I guess I feel a bit picky on this point because I've seen a lot of news articles that assume the US is worse because they fail to do "per capita", and because there seems to be a general attempt to discredit our institutions so that they'll collapse, which doesn't obviously seem crazy or misguided to me, but doesn't obviously seem right either given the downside risk.
(Or do you think the death estimates are wrong?)
Replies from: Zvi↑ comment by Zvi · 2020-12-10T22:56:11.324Z · LW(p) · GW(p)
I meant cases going forward, not cumulative deaths. Was pointing to europe having higher infection rates a few weeks ago by a lot, but getting it relatively under control.
Replies from: AnnaSalamon↑ comment by AnnaSalamon · 2020-12-10T23:57:27.873Z · LW(p) · GW(p)
Oh; sorry. I thought your "again" was referring to the earlier covid wave.
comment by Ofer (ofer) · 2020-12-11T16:39:27.309Z · LW(p) · GW(p)
Regarding comparison of mask types, the best source I'm aware of is: https://examine.com/topics/coronavirus-masks/
comment by Annapurna (jorge-velez) · 2020-12-14T19:17:32.866Z · LW(p) · GW(p)
Zvi, what do you think of The United Arab Emirates opening up vaccination centers for anyone who wants to get the Sinopharm vaccine without phase 3 trial results being published?
https://www.gulftoday.ae/news/2020/12/10/covid-19-vaccine-shots-are-available-all-across-the-uae-find-out-your-nearest-vaccination-centre
Replies from: Zvi↑ comment by Zvi · 2020-12-15T01:13:25.598Z · LW(p) · GW(p)
From the post it sounds like they're only giving it to those on state health care, so you can't go there for vaccine tourism. Which is a shame, because I would totally, totally do that if I could, or at least strongly consider it depending on logistics. Is that your read as well?
Replies from: jorge-velez↑ comment by Annapurna (jorge-velez) · 2020-12-15T15:47:05.416Z · LW(p) · GW(p)
Zvi my sister lives in Dubai and she's booking an appointment. Shes in her late 20s and doesn't work in health care. So they are opening up appointments for regular folks. I also know that it is free for residents of the UAE, not sure if non-residents can get it.
Replies from: Zvicomment by Kevin Liu (Pneumaticat) · 2020-12-14T18:12:38.839Z · LW(p) · GW(p)
A bit late on reporting back, but last week's post convinced me to sign up for a vaccine trial. Happy to report I've joined the Johnson & Johnson ensemble study (which in my area was actually 1 dose, not 2). I decided to go with J&J because a 50% chance of getting the vaccine now seemed net positive, and apparently they're hoping to get results back fairly soon (January-Feb).
A few non-obvious things I noticed:
- For signing up, I never got an email back after the initial application online. It seems like the play is to sign up on the website, and then call the number of the trial site they give to you. Then, you'll be able to complete their screening form and schedule a first visit.
- The researchers are actually totally fine with you dropping out to take a different approved vaccine if it happens to become available. Obviously they won't encourage it, but because of ethical guidelines you're free to drop out at any time, and they'll tell you if you got the placebo or not.
- It's not entirely clear right now whether, if you got the placebo, they'll prioritize giving you the real vaccine when it becomes approved. Looking at the Pfizer vaccine, it seems like Pfizer at least wants to, and another option being considered is a blind crossover, where all study participants are called back in when they would be eligible for a vaccine normally and given the opposite of what they got originally (so either the vaccine, or a placebo).
Overall a nice experience! Happy to answer questions if anyone has any.
comment by Vitor · 2020-12-13T05:03:59.601Z · LW(p) · GW(p)
> Switzerland is going even slower, making the usual noises about the need for ‘caution.’ My read is that this is because they did not order vaccine doses early enough, and now they are all sold out, so why not spin that by not approving the vaccine for a while and calling it ‘caution?’
This "read" of yours is quite far reaching, going on very little information. It is also completely wrong: Switzerland has contracts with all 3 major vaccine providers, the first of which was signed way back in August, securing 4.5 million doses (covering ~25% of the population).
Source (in german): <https://www.srf.ch/news/schweiz/moderna-impfdosen-gesichert-schweiz-steigt-ins-rennen-um-einen-moeglichen-impfstoff-ein>
So, yes, these delays are indeed because the swiss health authorities are being cautious. The vaccines are going through expedited but otherwise normal approval processes.
Replies from: Zvi↑ comment by Zvi · 2020-12-14T15:18:20.886Z · LW(p) · GW(p)
That sources says they don't have enough vaccine! Also consider this one: https://www.nature.com/articles/d41586-020-03370-6.
None of that considers timing. I don't know when what vaccine they have managed to buy will arrive. But August was rather late in the game to be doing one's first contract.
Even with all deals combined, Switzerland doesn't have 2 doses per person. They have half the European Union average before deal expansion, one third after potential EU deal expansion.
UK, US, Canada have the most, with 5+ doses per person, and all three are moving quickly to approve.
None of this seems like a coincidence to me.
Replies from: Vitor↑ comment by Vitor · 2020-12-20T12:06:07.540Z · LW(p) · GW(p)
So, the Swiss just approved the Pfizer vaccine. I think this clearly proves you wrong. However, as I was already planning to write an answer before this new development, let me give you that answer for completeness' sake (better late than never).
Your original claim sounded a lot stronger than what you're now saying, where it seems you simply disagree with the exact quantity that is being ordered.
Do you consider it obvious that 5+ doses per person would be optimal? For starters, only about half the population even wants to get vaccinated. Also, the first million doses are clearly worth much more than each additional million. These decisions were made in a very high uncertainty environment, before the effectiveness numbers were known. Switzerland obviously doesn't have the same market power as other, larger countries, etc. I'm not saying I disagree with your position, just that it is far from obviously correct.
But your original comment went much further than just claiming the swiss ordered the wrong quantity. You implied that Swissmedic (the body in charge of approval) basically has no political independence, and that both the head of Swissmedic and the health minister were brazenly lying to the public when they claimed that they were moving as fast as possible towards approval.
My priors say that these things are pretty unlikely. The delay is much more easily explained by the fact that there is no emergency approval process in Switzerland, which yields a huge status-quo bias for the regular process. To move any faster, new laws would have had to be passed.
So yes, I do think that you made a very far reaching read based on very little information.